j infect dis. 2010 parker fiebelkorn 1520 8
DESCRIPTION
nTRANSCRIPT

1520 • JID 2010:202 (15 November) • Parker Fiebelkorn et al
M A J O R A R T I C L E
Measles in the United Statesduring the Postelimination Era
Amy Parker Fiebelkorn, Susan B. Redd, Kathleen Gallagher, Paul A. Rota,Jennifer Rota, William Bellini, and Jane SewardDivision of Viral Diseases, National Center for Immunization and Respiratory Diseases, Centersfor Disease Control and Prevention, Atlanta, Georgia
Background. Measles affected entire birth cohorts in the prevaccine era but was declared eliminated in theUnited States in 2000 because of a successful measles vaccination program.
Methods. We reviewed US surveillance data on confirmed measles cases reported to the Centers for DiseaseControl and Prevention and data on national measles-mumps-rubella (MMR) vaccination coverage during post-elimination years 2001�2008.
Results. During 2001�2008, a total of 557 confirmed cases of measles (annual median no. of cases, 56) and38 outbreaks (annual median no. of outbreaks, 4) were reported in the United States; 232 (42%) of the cases wereimported from 44 countries, including European countries. Among case-patients who were US residents, thehighest incidences of measles were among infants 6–11 months of age and children 12–15 months of age (3.5 and2.6 cases/1 million person-years, respectively). From 2001 through 2008, national 1-dose MMR vaccine coverageamong children 19–35 months of age ranged from 91% to 93%. From 2001 through 2008, a total of 285 US-resident case-patients (65%) were considered to have preventable measles (ie, the patients were eligible for vac-cination but unvaccinated). During 2004–2008, a total of 68% of vaccine-eligible US-resident case-patients claimedexemptions for personal beliefs.
Conclusions. The United States maintained measles elimination from 2001 through 2008 because of sustainedhigh vaccination coverage. Challenges to maintaining elimination include large outbreaks of measles in highlytraveled developed countries, frequent international travel, and clusters of US residents who remain unvaccinatedbecause of personal belief exemptions.
Measles is a highly infectious, acute viral disease that
causes rash, respiratory symptoms, and fever. Severe
complications, which may result in death, include
pneumonia and encephalitis. In the decade before the
national measles vaccine program was implemented in
Received 2 April 2010; accepted 10 June 2010; electronically published 7October 2010.
Potential conflicts of interest: none reported.Disclaimer: The findings and conclusions in this article are those of the authors
and do not necessarily represent the views of the Centers for Disease Controland Prevention, US Department of Health and Human Services.
Financial support: No external funding sources were used to gather the data,analyze the data, or write up the findings.
Presented in part: 46th annual meeting of the Infectious Diseases Society ofAmerica, Washington DC, 25–28 October 2008 (oral presentation); PediatricAcademic Societies Annual Conference, Honolulu, Hawaii, 3–6 May 2008 (platformoral presentation).
Reprints or correspondence: Amy Parker Fiebelkorn, CDC/NCIRD MS A-47, 1600Clifton Rd, Bldg 16, Atlanta, GA 30333 ([email protected]).
The Journal of Infectious Diseases 2010; 202(10):1520–1528This article is in the public domain, and no copyright is claimed.0022-1899/2010/20210-0010DOI: 10.1086/656914
1963, it was estimated that 3–4 million people in the
United States acquired measles each year [1]. Of the
∼500,000 measles cases reported annually, 500 resulted
in death, 48,000 resulted in hospitalization, and 1000
resulted in permanent brain damage due to measles
encephalitis [1].
Achieving a high level of population immunity is the
best way to prevent measles. Accordingly, 2 doses of
measles-mumps-rubella (MMR) vaccine are recom-
mended for all US children [2]. The first dose should
be administered at 12–15 months of age and the second
dose at 4–6 years of age. Laws in every state require
age-appropriate vaccination of children enrolled in
child care facilities and documentation of evidence of
measles immunity at the time of entry into kindergarten
or first grade [3]. As the vaccinated cohorts age, all
children in kindergarten through grade 12 should be
covered by the requirements [3]. For adults without
evidence of measles immunity, one dose of MMR vac-
cine is recommended. Two doses are recommended if
by guest on Decem
ber 23, 2014http://jid.oxfordjournals.org/
Dow
nloaded from

Measles in the Postelimination Era • JID 2010:202 (15 November) • 1521
the adult is in a high-risk group (ie, healthcare workers, in-
ternational travelers, or students at post–high school educa-
tional institutions) [2].
Because of the success of the measles vaccine program in
achieving and maintaining high 1- and 2-dose MMR vaccine
coverage in preschool and school-aged children and improved
control of measles throughout Central and South America,
measles was declared eliminated from the United States in 2000
[4] and from the World Health Organization (WHO) Region
of the Americas in 2002 [5]. Elimination is defined as the
absence of transmission of endemic disease (ie, no epidemio-
logical or virological evidence that measles virus transmission
is continuously occurring in a defined geographical area for
�12 months). However, in 2008, it was estimated that there
were 20 million cases of measles worldwide and 164,000 related
deaths [6]. Importation of measles virus from abroad continues
to test the status of elimination in the United States. In this
report, we summarize the epidemiology of measles in the
United States during measles postelimination years 2001–2008.
METHODS
Reporting of measles cases to public health authorities by
healthcare providers and clinical laboratories is legally man-
dated in all states. Measles cases are identified and classified
using standard case definitions and case classifications [7]. A
confirmed case of measles is either laboratory confirmed or
epidemiologically linked to a patient with laboratory-confirmed
measles infection [7]. State health departments electronically
transmit data on confirmed cases of measles to the Centers for
Disease Control and Prevention (CDC) via the National No-
tifiable Diseases Surveillance System. The CDC performs mo-
lecular typing of measles viruses according to WHO-recom-
mended protocols [8–10]. Molecular epidemiologic data
obtained from viral isolates are used to confirm the links to
outbreaks occurring in other countries. Viral isolates that are
genotyped are categorized by the WHO region (ie, African
Region, Region of the Americas, South-East Asia Region, Eu-
ropean Region, Eastern Mediterranean Region, or Western Pa-
cific Region) from which the virus was imported.
In the United States, an outbreak of measles is defined as a
chain of transmission with �3 confirmed cases. Cases are clas-
sified either as internationally imported (ie, measles cases in
which exposure to measles virus occurred outside the United
States 7–21 days before the onset of rash and in which rash
developed within 21 days of entrance into the United States,
with no known exposure to measles occurring in the United
States during that time) or acquired in the United States (US-
acquired cases; ie, case-patients either had not been outside the
United States during the 21 days before the onset of rash or
were known to have been exposed to measles within the United
States). US-acquired cases were subclassified into 4 mutually
exclusive groups: (1) import-linked cases (ie, any case in a chain
of transmission that was epidemiologically linked to an inter-
nationally imported case), (2) imported-virus cases (ie, cases
in which an epidemiologic link to an internationally imported
case was not identified but viral genetic evidence indicated an
imported measles genotype within the chain of transmission),
(3) endemic cases (ie, cases in which transmission of measles
virus was continuous for �12 months within the United
States), and (4) unknown source cases (ie, cases in which an
epidemiological or virological link to importation or to en-
demic transmission within the United States could not be es-
tablished after a thorough investigation) [7, 11].
We analyzed all cases of measles reported in the United States
during 2001–2008. However, we differentiated between US
case-patients and “foreign-visitor” case-patients (ie, foreign
tourists, international students, new international adoptees, re-
cent immigrants, refugees, and cruise ship employees) when
we calculated incidence, so we could use 2008 US Census data
as the denominator [12], as well as when we reported vacci-
nation status, because the US vaccination recommendations
apply only to its US residents. This distinction allowed the
differentiation of cases that would have been preventable had
the recommended vaccination policy been implemented. Non-
preventable cases were defined as measles cases that occurred
among US residents who either (1) had received �1 dose of
measles-containing vaccine, (2) were vaccinated as recommended
if traveling internationally, (3) were not vaccinated but had other
evidence of immunity (ie, were born before 1957 and therefore
were presumed to be immune from natural disease in childhood,
had laboratory evidence of immunity, or had documentation of
physician-diagnosed disease), or (4) belonged to a category (such
as infants !1 year of age) for whom vaccination is not routinely
recommended. “Personal belief exemptors” were defined as per-
sons who were vaccine eligible, according to recommendations
of the Advisory Committee on Immunization Practices (ACIP)
[2] or the WHO [6], but remained unvaccinated because of
personal or parental beliefs.
We examined the rates of national 1-dose measles vaccina-
tion coverage among children 19–35 months of age from 2001
through 2008, as well as those of 2-dose coverage among ad-
olescents from 2006 through 2008 (the only years for which
data were available), using data from the National Immuni-
zation Survey, which supplies provider-verified, population-
based rates of immunization with 95% confidence intervals.
RESULTS
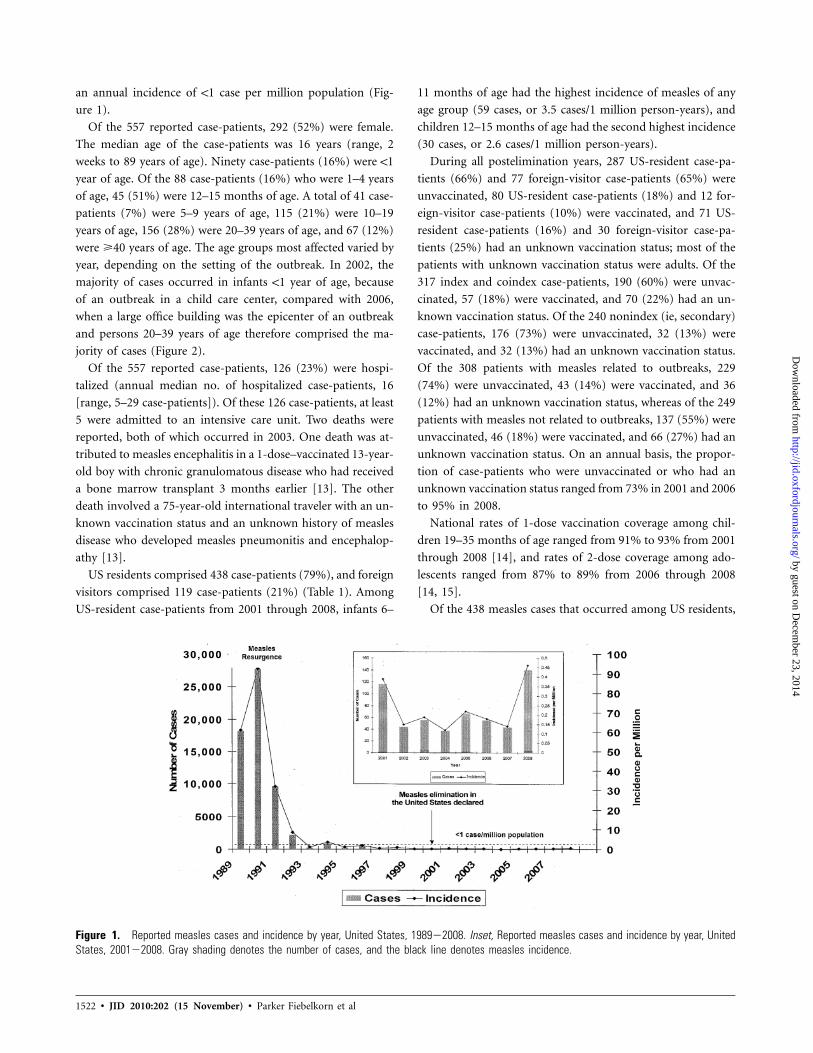
In the United States, from 2001 through 2008, a total of 557
confirmed measles cases were reported from 37 states and the
District of Columbia (annual median no. of cases reported, 56
[range, 37 cases in 2004 to 140 cases in 2008]), representing
by guest on Decem
ber 23, 2014http://jid.oxfordjournals.org/
Dow
nloaded from
1522 • JID 2010:202 (15 November) • Parker Fiebelkorn et al
Figure 1. Reported measles cases and incidence by year, United States, 1989�2008. Inset, Reported measles cases and incidence by year, UnitedStates, 2001�2008. Gray shading denotes the number of cases, and the black line denotes measles incidence.
an annual incidence of !1 case per million population (Fig-
ure 1).
Of the 557 reported case-patients, 292 (52%) were female.
The median age of the case-patients was 16 years (range, 2
weeks to 89 years of age). Ninety case-patients (16%) were !1
year of age. Of the 88 case-patients (16%) who were 1–4 years
of age, 45 (51%) were 12–15 months of age. A total of 41 case-
patients (7%) were 5–9 years of age, 115 (21%) were 10–19
years of age, 156 (28%) were 20–39 years of age, and 67 (12%)
were �40 years of age. The age groups most affected varied by
year, depending on the setting of the outbreak. In 2002, the
majority of cases occurred in infants !1 year of age, because
of an outbreak in a child care center, compared with 2006,
when a large office building was the epicenter of an outbreak
and persons 20–39 years of age therefore comprised the ma-
jority of cases (Figure 2).
Of the 557 reported case-patients, 126 (23%) were hospi-
talized (annual median no. of hospitalized case-patients, 16
[range, 5–29 case-patients]). Of these 126 case-patients, at least
5 were admitted to an intensive care unit. Two deaths were
reported, both of which occurred in 2003. One death was at-
tributed to measles encephalitis in a 1-dose–vaccinated 13-year-
old boy with chronic granulomatous disease who had received
a bone marrow transplant 3 months earlier [13]. The other
death involved a 75-year-old international traveler with an un-
known vaccination status and an unknown history of measles
disease who developed measles pneumonitis and encephalop-
athy [13].
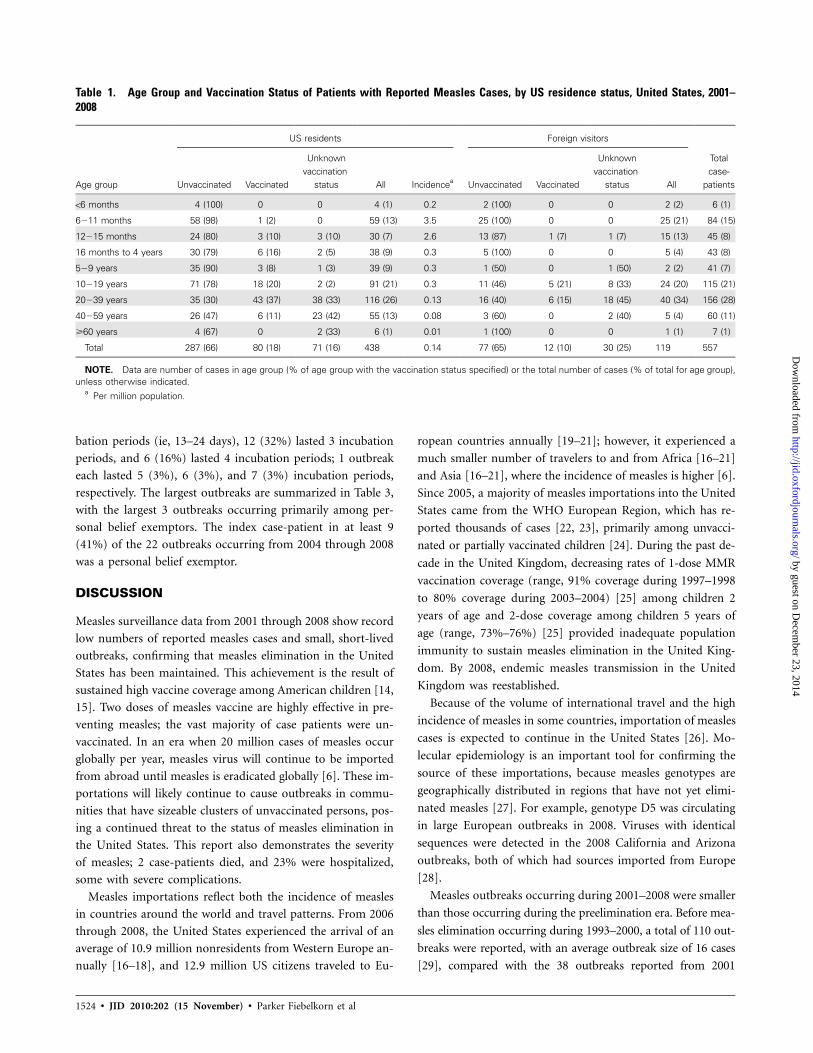
US residents comprised 438 case-patients (79%), and foreign
visitors comprised 119 case-patients (21%) (Table 1). Among
US-resident case-patients from 2001 through 2008, infants 6–
11 months of age had the highest incidence of measles of any
age group (59 cases, or 3.5 cases/1 million person-years), and
children 12–15 months of age had the second highest incidence
(30 cases, or 2.6 cases/1 million person-years).
During all postelimination years, 287 US-resident case-pa-
tients (66%) and 77 foreign-visitor case-patients (65%) were
unvaccinated, 80 US-resident case-patients (18%) and 12 for-
eign-visitor case-patients (10%) were vaccinated, and 71 US-
resident case-patients (16%) and 30 foreign-visitor case-pa-
tients (25%) had an unknown vaccination status; most of the
patients with unknown vaccination status were adults. Of the
317 index and coindex case-patients, 190 (60%) were unvac-
cinated, 57 (18%) were vaccinated, and 70 (22%) had an un-
known vaccination status. Of the 240 nonindex (ie, secondary)
case-patients, 176 (73%) were unvaccinated, 32 (13%) were
vaccinated, and 32 (13%) had an unknown vaccination status.
Of the 308 patients with measles related to outbreaks, 229
(74%) were unvaccinated, 43 (14%) were vaccinated, and 36
(12%) had an unknown vaccination status, whereas of the 249
patients with measles not related to outbreaks, 137 (55%) were
unvaccinated, 46 (18%) were vaccinated, and 66 (27%) had an
unknown vaccination status. On an annual basis, the propor-
tion of case-patients who were unvaccinated or who had an
unknown vaccination status ranged from 73% in 2001 and 2006
to 95% in 2008.
National rates of 1-dose vaccination coverage among chil-
dren 19–35 months of age ranged from 91% to 93% from 2001
through 2008 [14], and rates of 2-dose coverage among ado-
lescents ranged from 87% to 89% from 2006 through 2008
[14, 15].
Of the 438 measles cases that occurred among US residents,
by guest on Decem
ber 23, 2014http://jid.oxfordjournals.org/
Dow
nloaded from

Measles in the Postelimination Era • JID 2010:202 (15 November) • 1523
Figure 2. Percentage of case-patients with measles, by age group (by year), in the United States, 2001�2008. Striped diagonal bars denote infants!1 year of age. This age group had the highest percentage of measles cases in 2002, when an outbreak occurred in a child care center. Black barsdenote children 1–4 years of age. This age group had the highest percentage of measles cases in 2004, when a multistate outbreak occurred amongtoddlers adopted from China. Striped vertical bars denote those 5–19 years of age. This age group had the highest percentage of measles cases in2003, 2005, and 2008, when large outbreaks occurred among unvaccinated school children. Gray bars denote adults 20–39 years of age. This agegroup had the highest percentage of measles cases in 2006, when a large outbreak occurred in an office building. Dark gray bars denote adults �40years of age.
285 (65%) were considered preventable (Table 2). More than
two-thirds (196 [69%]) of the preventable cases were acquired
in the United States. Of the 119 US-resident case-patients who
traveled internationally, 94 (79%) were unvaccinated or had an
unknown vaccination status; of these case-patients, 89 (95%)
were considered to have preventable measles, including 20
(21%) who were 6–11 months of age (Table 2). During 2004–
2008, a total of 110 (68%) of 162 vaccine-eligible US-resident
case-patients were known to be unvaccinated because they or
their parents self-declared a personal belief exemption. (Data
on reasons for remaining unvaccinated were not systematically
collected until 2004.)
During 2001–2008, a total of 232 cases (42%) were imported
from 44 countries (annual median no. of cases imported, 26
[range, 18 cases in 2002 to 54 cases in 2001]). Of the 123 im-
ported cases from 2001 through 2004, the majority (68 [55%])
were from the WHO Western Pacific Region (Figure 3), including
28 cases from China, 23 from Japan, and 10 from the Philippines.
Whereas, of the 109 imported cases from 2005 through 2008,
the WHO European Region contributed the largest number (42
cases [39%]), including 7 cases each from Italy and the United
Kingdom and 6 cases imported from Ukraine. However, India
was the country from which the largest number of imported
cases came from during 2005–2008, with 20 cases. A median of
29 US-acquired cases were reported annually (range, 10 cases in
2004 to 115 cases in 2008). The 325 US-acquired cases reported
during 2001–2008 were classified as follows: 167 (51%) were
import-linked cases, 94 (29%) were imported-virus cases, 0 were
endemic cases, and 64 (20%) cases were of an unknown source.
The transmission setting was known for 235 (72%) of the 325
US-acquired cases. Transmission occurred in the home for 71
cases (30%), in the community for 35 (15%), at church for 26
(11%), in a healthcare facility for 23 (10%), at school/college/
boarding school for 21 (9%), at a child care center for 14 (6%),
at work for 14 (6%), at home school for 10 (4%), and at other
locations for 21 cases (9%). The measles genotypes identified
during 2001–2008 were D3-D9, H1, H2, and B3. These genotypes
are found in various Asian, African, and European countries.
During 2001–2008, there were 38 outbreaks (annual median
no. of outbreaks, 4 [range, 2–10 outbreaks]). Of the 557 case-
patients reported from 2001 through 2008, a total of 308 (55%)
were outbreak-related cases. The average outbreak size was 9
cases (median no. of outbreak cases, 5 [range, 3–34 cases]).
Outbreak duration (ie, the time between the onset of rash in
the first case and that in the last case) ranged from 3 to 79
days (median outbreak duration, 27 days). Of 38 outbreaks
occurring from 2001 through 2008, a total of 6 (16%) lasted
1 incubation period (ie, �12 days), 11 (29%) lasted 2 incu-
by guest on Decem
ber 23, 2014http://jid.oxfordjournals.org/
Dow
nloaded from
1524 • JID 2010:202 (15 November) • Parker Fiebelkorn et al
Table 1. Age Group and Vaccination Status of Patients with Reported Measles Cases, by US residence status, United States, 2001–2008
Age group
US residents Foreign visitors
Totalcase-
patientsUnvaccinated Vaccinated
Unknownvaccination
status All Incidencea Unvaccinated Vaccinated
Unknownvaccination
status All
!6 months 4 (100) 0 0 4 (1) 0.2 2 (100) 0 0 2 (2) 6 (1)
6�11 months 58 (98) 1 (2) 0 59 (13) 3.5 25 (100) 0 0 25 (21) 84 (15)
12�15 months 24 (80) 3 (10) 3 (10) 30 (7) 2.6 13 (87) 1 (7) 1 (7) 15 (13) 45 (8)
16 months to 4 years 30 (79) 6 (16) 2 (5) 38 (9) 0.3 5 (100) 0 0 5 (4) 43 (8)
5�9 years 35 (90) 3 (8) 1 (3) 39 (9) 0.3 1 (50) 0 1 (50) 2 (2) 41 (7)
10�19 years 71 (78) 18 (20) 2 (2) 91 (21) 0.3 11 (46) 5 (21) 8 (33) 24 (20) 115 (21)
20�39 years 35 (30) 43 (37) 38 (33) 116 (26) 0.13 16 (40) 6 (15) 18 (45) 40 (34) 156 (28)
40�59 years 26 (47) 6 (11) 23 (42) 55 (13) 0.08 3 (60) 0 2 (40) 5 (4) 60 (11)
�60 years 4 (67) 0 2 (33) 6 (1) 0.01 1 (100) 0 0 1 (1) 7 (1)
Total 287 (66) 80 (18) 71 (16) 438 0.14 77 (65) 12 (10) 30 (25) 119 557
NOTE. Data are number of cases in age group (% of age group with the vaccination status specified) or the total number of cases (% of total for age group),unless otherwise indicated.
a Per million population.
bation periods (ie, 13–24 days), 12 (32%) lasted 3 incubation
periods, and 6 (16%) lasted 4 incubation periods; 1 outbreak
each lasted 5 (3%), 6 (3%), and 7 (3%) incubation periods,
respectively. The largest outbreaks are summarized in Table 3,
with the largest 3 outbreaks occurring primarily among per-
sonal belief exemptors. The index case-patient in at least 9
(41%) of the 22 outbreaks occurring from 2004 through 2008
was a personal belief exemptor.
DISCUSSION
Measles surveillance data from 2001 through 2008 show record
low numbers of reported measles cases and small, short-lived
outbreaks, confirming that measles elimination in the United
States has been maintained. This achievement is the result of
sustained high vaccine coverage among American children [14,
15]. Two doses of measles vaccine are highly effective in pre-
venting measles; the vast majority of case patients were un-
vaccinated. In an era when 20 million cases of measles occur
globally per year, measles virus will continue to be imported
from abroad until measles is eradicated globally [6]. These im-
portations will likely continue to cause outbreaks in commu-
nities that have sizeable clusters of unvaccinated persons, pos-
ing a continued threat to the status of measles elimination in
the United States. This report also demonstrates the severity
of measles; 2 case-patients died, and 23% were hospitalized,
some with severe complications.
Measles importations reflect both the incidence of measles
in countries around the world and travel patterns. From 2006
through 2008, the United States experienced the arrival of an
average of 10.9 million nonresidents from Western Europe an-
nually [16–18], and 12.9 million US citizens traveled to Eu-
ropean countries annually [19–21]; however, it experienced a
much smaller number of travelers to and from Africa [16–21]
and Asia [16–21], where the incidence of measles is higher [6].
Since 2005, a majority of measles importations into the United
States came from the WHO European Region, which has re-
ported thousands of cases [22, 23], primarily among unvacci-
nated or partially vaccinated children [24]. During the past de-
cade in the United Kingdom, decreasing rates of 1-dose MMR
vaccination coverage (range, 91% coverage during 1997–1998
to 80% coverage during 2003–2004) [25] among children 2
years of age and 2-dose coverage among children 5 years of
age (range, 73%–76%) [25] provided inadequate population
immunity to sustain measles elimination in the United King-
dom. By 2008, endemic measles transmission in the United
Kingdom was reestablished.
Because of the volume of international travel and the high
incidence of measles in some countries, importation of measles
cases is expected to continue in the United States [26]. Mo-
lecular epidemiology is an important tool for confirming the
source of these importations, because measles genotypes are
geographically distributed in regions that have not yet elimi-
nated measles [27]. For example, genotype D5 was circulating
in large European outbreaks in 2008. Viruses with identical
sequences were detected in the 2008 California and Arizona
outbreaks, both of which had sources imported from Europe
[28].
Measles outbreaks occurring during 2001–2008 were smaller
than those occurring during the preelimination era. Before mea-
sles elimination occurring during 1993–2000, a total of 110 out-
breaks were reported, with an average outbreak size of 16 cases
[29], compared with the 38 outbreaks reported from 2001
by guest on Decem
ber 23, 2014http://jid.oxfordjournals.org/
Dow
nloaded from

Measles in the Postelimination Era • JID 2010:202 (15 November) • 1525
Table 2. Number of Patients with Preventable and Nonpreventable Reported Measles Cases ( ) among USn p 438Residents, by Age, Travel History, and Measles Vaccination Status, United States, 2001�2008
Case-patients, by age group or case type
International travel No international travel
TotalVaccinated
Not vaccinatedor unknown
vaccination status Vaccinated
Not vaccinatedor unknown
vaccination status
!6 months 0 0 0 4 46�11 months 1 20a 0 38 5912�15 months 1 11a 2 16 3016 months to 4 years 2 8a 3 25a 385�9 years 1 5a 1 32a 3910�19 years 3 9a 15 64a 9120�29 years 2 10a 12 27a 5130�39 years 13 10a 16 26a 65�40 years 2 21b 4 34c 61
Total case-patients 25 94 53 266 438Total with preventable cases 0 89 0 196 285Total with nonpreventable casesd 25 5 53 70 153
a Case-patients with preventable measles were case-patients for whom vaccination was recommended by the Advisory Committee onImmunization Practices but who had not received �1 dose of measles-containing vaccine.
b Sixteen of the 21 cases were preventable; 5 cases occurred in persons born before 1957 and were classified as nonpreventablebecause measles-containing vaccine is not recommended for that age group.
c Of the 34 cases, 22 were preventable; the other 12 cases occurred in persons born before 1957 and were classified as nonpreventablebecause measles-containing vaccine is not recommended for this age group.
d Cases were defined as nonpreventable if they occurred among US-resident case-patients who had received �1 dose of measles-containing vaccine, were vaccinated as recommended if traveling internationally, or were not vaccinated but had other evidence of immunity(ie, were born before 1957 and therefore were presumed to be immune from natural disease in childhood, had laboratory evidence ofimmunity, or had documentation of physician-diagnosed disease) or for whom vaccination is not recommended.
through 2008, for which the average size was 9 cases. Outbreak
duration during 1993–2000 ranged from 3 to 131 days (median,
29 days); in the postelimination era, outbreaks had a shorter
range (from 3 to 79 days; median, 27 days). Whereas 93% of
outbreaks (35 of 38) occurring in 2001–2008 lasted �4 incu-
bation periods (ie, �48 days), only 73% (80 of 110) outbreaks
occurring in 1993–2000 lasted �4 incubation periods.
Mathematical models show that maintaining measles elim-
ination requires that the proportion of susceptible individuals,
which is estimated using rates of MMR vaccine coverage in the
population and rates of effectiveness of the vaccine, is less than
the epidemic threshold [30]. The limited size and duration of
recent measles outbreaks in the United States can be attributed
to several factors. First, levels of national measles vaccination
coverage among preschool-aged and school-aged children are
high [14, 15]. Second, MMR vaccine is highly effective (ie, 2
MMR vaccine doses administered after 12 months of age are
95%–100% effective in preventing measles [31–33]). Finally,
there is an aggressive and effective public health response to
reported measles cases in the United States that helps limit
further disease transmission.
Despite high overall rates of measles vaccination at the na-
tional and state levels [14, 15], there are communities and coun-
ties where vaccine exemption rates are several times higher than
state averages [34, 35]. Clustering of susceptible persons in such
communities may result in population immunity below the herd
immunity threshold of 93%–95% [36] and an increased risk of
outbreaks [37, 38]. In the measles postelimination era, a majority
of the measles outbreaks that occurred in the United States were
among personal belief exemptors [28, 37, 39–41]. Salmon et al
[42] found that the most common reason that parents claimed
vaccine exemptions was fear that the vaccine might cause harm.
As the incidence of a vaccine-preventable disease like measles
decreases, the public perception tends to shift to a belief that the
severity of the disease and susceptibility to the virus have also
decreased [43]. Concurrently, over the past decade, public con-
cern about real or perceived adverse events associated with vac-
cines has increased [42, 44, 45].
Enactment and enforcement of school immunization laws
has been shown to be an important factor in achieving high
immunization coverage [3]. However, in many states, home-
schooled children are not covered by school-entry vaccination
requirements. Between 1991 and 2004, the average proportion
of schoolchildren whose parents claimed exemptions from vac-
cination because of personal belief exemptions increased [46].
All 50 states allow medical exemptions from vaccination before
school entry, 48 states allow religious exemptions (Mississippi
and West Virginia do not), and 20 states allow philosophical/
personal belief exemptions for entry into primary school [47].
States that allow personal belief exemptions have higher non-
by guest on Decem
ber 23, 2014http://jid.oxfordjournals.org/
Dow
nloaded from

1526 • JID 2010:202 (15 November) • Parker Fiebelkorn et al
Figure 3. Importations of measles to the United States, by World Health Organization region, 2001�2008. “Unknown” denotes importations ofunknown origin.
Table 3. Largest Measles Outbreaks in the United States during 2001�2008
YearCases,
no. Primary setting of outbreakMedian age ofcase-patients Source (genotype)
Vaccination status ofindex case-patient
Reason index casewas not vaccinated
Total number(%) of PBEs
2005 34 Church, home 13 years Romania (D4) Unvaccinated PBE 28 (82)2008 30 Home school, household 10 years Italy (D4) Unvaccinated PBE 28 (93)2008 19 Household, school, church 12 years Possibly Japan (D5) Unvaccinated PBE 17 (89)2006 17 Work 36 years India (D8) Unvaccinated Not specified 02008 14 Healthcare 20 years Switzerland (D5) Unvaccinated PBE 3 (21)2001 14 Community (exposed in or-
phanage abroad)11 months China (unknown) Unvaccinated Too young 0
2008 13 Multiple settings 15 months Israel (D4) Unvaccinated Delayedvaccination
2 (15)
2002 13 Child care center 10 months The Philippines (D3) Unvaccinated Too young 02003 13 Community 12 months Unknown (H1) Unvaccinated Not specified Unknown2008 12 Healthcare, household,
school6 years Switzerland (D5) Unvaccinated PBE 8 (67)
2003 11 Boarding school 17 years Lebanon (D4) Unvaccinated Unknown but vac-cine eligible
Unknowna
2001 11 Community 16 years Korea (H1) Unvaccinated Unknown but vac-cine eligible
Unknownb
NOTE. PBE, personal belief exemption.a However, 4 were unvaccinated and vaccine eligible.b However, 3 were unvaccinated and vaccine eligible.
medical exemption rates than states that only offer religious ex-
emptions. States that easily grant exemptions have higher ex-
emption rates than states with moderate and difficult processes
for granting exemptions [46].
Measles virus is highly infectious and can cause severe com-
plications or death [1]. Susceptible individuals who remain un-
vaccinated may be unaware of the potential risk of acquiring
measles disease. Once a person becomes infected, there is the
risk of the virus being spread to other susceptible persons,
including those for whom vaccination is not recommended
because of medical reasons or those who are too young for
vaccination. From 2001 through 2008, infants 6–11 months of
age had the highest age-specific incidence (3.5 cases/1 million
person-years); infants in this age group are not recommended
for MMR vaccination unless they are traveling internationally.
Compared with vaccinated persons, individuals who are exempt
from vaccination are 22–224 times more likely to become in-
fected with measles [34, 48, 49].
Healthcare providers play an important role in influencing par-
ents as to whether they vaccinate their children. Nearly 40%
of parents who change their minds after considering delaying
or refusing a vaccine for their child credit information they
by guest on Decem
ber 23, 2014http://jid.oxfordjournals.org/
Dow
nloaded from

Measles in the Postelimination Era • JID 2010:202 (15 November) • 1527
receive from the child’s healthcare provider as the reason they
decided not to delay or refuse [50]. Healthcare providers play
an important role in sustaining elimination by maintaining a
high awareness of measles in international travelers and un-
protected populations and by rapidly implementing isolation
precautions if measles is suspected in a patient. In addition,
providers can facilitate measles prevention by encouraging pa-
tients who are planning international travel to be up to date
with immunizations.
The epidemiology of measles in the United States during the
postelimination era highlights the importance of implementing
existing policy recommendations. Of the 119 US-resident case-
patients who traveled internationally and were vaccine eligible,
89 (75%) were unvaccinated. Had existing MMR vaccine rec-
ommendations been followed, 285 US cases (65%) could have
been prevented. Because the second-highest age-specific inci-
dence among US residents in the postelimination era occurred
among those 12–15 months of age, providers should be en-
couraged to offer vaccination as soon as possible once children
reach 12 months of age. In addition, vaccination recommen-
dations for adults should be followed, because several sizeable
outbreaks primarily affected adults.
CONCLUSION
Despite its status as an eliminated disease in the United States,
measles importation is continuing to occur and occasionally
leads to outbreaks. Because of the widespread circulation of
measles virus, especially in highly traveled European countries,
the ease and volume of international travel, and the geographic
clustering of unvaccinated persons in the United States, the risk
for imported measles virus and subsequent spread remains. To
maintain elimination, it will be necessary to sustain high rates
of 2-dose measles vaccination coverage at the national and local
levels, understand attitudes about vaccines and parents’ ratio-
nales for exemptions, work with healthcare providers to reach
out to persons who have questions about vaccines, find im-
proved methods to communicate vaccine safety information,
and continue with rapid public health containment measures
when importations of measles virus occur.
Acknowledgments
We thank Cedric Brown and Claudia Chesley for their assistance withthis manuscript.
References
1. Strebel PM, Papania MJ, Dayan GH, Halsey NA. Measles vaccine. In:Plotkin SA, Orenstein WA, eds. Vaccines. Philadelphia: Elsevier, 2008:353–98.
2. Watson JC, Hadler SC, Dykewicz CA, Reef S, Phillips L. Measles,mumps, and rubella—vaccine use and strategies for elimination of
measles, rubella, and congenital rubella syndrome and control ofmumps: recommendations of the Advisory Committee on Immuni-zation Practices (ACIP). MMWR Recomm Rep 1998; 47:1–57.
3. Centers for Disease Control. School immunization requirements formeasles—United States, l982. Morb Mortal Wkly Rep 1982; 31:65–7.
4. Katz SL, Hinman AR. Summary and conclusions: measles eliminationmeeting, 16–17 March 2000. J Infect Dis 2004; 189:(Suppl 1):S43-7.
5. Pan American Health Organization. Area of Family and CommunityHealth, Immunization Unit. Public. Absence of transmission of the D9measles virus in the region of the Americas, November 2002–May 2003.Epidemiol Bull 2003; 24:24.
6. World Health Organization. Measles fact sheet. Geneva: World HealthOrganization. http://www.who.int/mediacentre/factsheets/fs286/en/index.html. Accessed 4 June 2010.
7. Centers for Disease Control and Prevention. Measles (rubeola): 2009case definition. http://www.cdc.gov/ncphi/disss/nndss/casedef/measles_2009.htm. Accessed 24 February 2010.
8. Ratnam S, Tipples G, Head C, Fauvel M, Fearon M, Ward BJ. Per-formance of indirect immunoglobulin M (IgM) serology tests and IgMcapture assays for laboratory diagnosis of measles. J Clin Microbiol2000; 38:99–104.
9. Expanded Programme on Immunization (EPI). Standardization of thenomenclature for describing the genetic characteristics of wild-typemeasles viruses. Wkly Epidemiol Rec 1998; 73:265–9.
10. New genotype of measles virus and update on global distribution ofmeasles genotypes. Wkly Epidemiol Rec 2005; 80:347–51.
11. Papania MJ, Seward JF, Redd SB, Lievano F, Harpaz R, Wharton ME.Epidemiology of measles in the United States, 1997–2001. J Infect Dis2004; 18(Suppl 1):S61–8.
12. US Census Bureau. General demographic characteristics: 2008 popula-tion estimates. http://factfinder.census.gov/servlet/QTTable?_bmpy&-qr_namepPEP_2008_EST_DP1&-geo_idp01000US&-ds_namepPEP_2008_EST&-_langpen&-formatp&-CONTEXTpqt. Accessed26 February 2010.
13. Centers for Disease Control and Prevention. Epidemiology of mea-sles—United States, 2001—2003. Morb Mortal Wkly Rep 2004; 53:713–6.
14. Centers for Disease Control and Prevention. Immunization Coveragein the U.S. National Immunization Survey (NIS)—children (19–35months). http://www.cdc.gov/vaccines/stats-surv/imz-coverage.htm#nis. Accessed 4 June 2010.
15. Centers for Disease Control and Prevention. National, state, and localarea vaccination coverage among adolescents aged 13–17 years—Unit-ed States, 2008. MMWR Morb Mortal Wkly Rep 2009; 58:997–1001.http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5836a2.htm. Ac-cessed 4 June 2010.
16. Office of Travel and Tourism Industries, International Trade Admin-istration, US Department of Commerce. 2008 Monthly tourism sta-tistics. 2008 Monthly arrivals to the United States—table C. Washing-ton, DC: US Department of Commerce, 2008. http://tinet.ita.doc.gov/view/m-2008-I-001/index.html. Accessed 26 February 2010.
17. Office of Travel and Tourism Industries, International Trade Admin-istration, US Department of Commerce. 2007 Monthly tourism sta-tistics. 2007 Monthly arrivals to the United States—table C. Washing-ton, DC: US Department of Commerce, 2008. http://tinet.ita.doc.gov/view/m-2007-I-001/index.html. Accessed 26 February 2010.
18. Office of Travel and Tourism Industries, International Trade Admin-istration, US Department of Commerce. 2006 Monthly tourism sta-tistics. 2006 Monthly arrivals to the United States—table C. Washing-ton, DC: US Department of Commerce, 2008. http://tinet.ita.doc.gov/view/m-2006-I-001/index.html. Accessed 26 February 2010.
19. Office of Travel and Tourism Industries, International Trade Admin-istration, US Department of Commerce. Final U.S. citizen air trafficto overseas regions, Canada & Mexico 2008. Washington, DC: USDepartment of Commerce, 2008. http://tinet.ita.doc.gov/view/m-2008-O-001/index.html. Accessed 26 February 2010.
by guest on Decem
ber 23, 2014http://jid.oxfordjournals.org/
Dow
nloaded from

1528 • JID 2010:202 (15 November) • Parker Fiebelkorn et al
20. Office of Travel and Tourism Industries, International Trade Admin-istration, US Department of Commerce. Final U.S. citizen air trafficto overseas regions, Canada & Mexico 2007. Washington, DC: USDepartment of Commerce, 2008. http://tinet.ita.doc.gov/view/m-2007-O-001/index.html. Accessed 26 February 2010.
21. Office of Travel and Tourism Industries, International Trade Admin-istration, U.S. Department of Commerce. Final U.S. citizen air trafficto overseas regions, Canada & Mexico 2006. Washington, DC: U.S.Department of Commerce; 2008. http://tinet.ita.doc.gov/view/m-2006-O-001/index.html. Accessed 26 February 2010.
22. Muscat M, Bang H, Wohlfahrt J, Glismann S, Mølbak K. Measles inEurope: an epidemiological assessment. Lancet. 2009; 373:383–9.
23. World Health Organization. WHO calls for scaling up of measles vac-cination. Children in affluent European countries have a higher risk ofinfection. http://www.euro.who.int/en/what-we-publish/information-for-the-media/sections/press-releases/2009/02/who-calls-for-scaling-up-of-measles-vaccination.-children-in-affluent-european-countries-have-a-higher-risk-of-infection. Accessed 26 February 2010.
24. Measles once again endemic in the United Kingdom. Euro Surveill2008; 13:18919.
25. The National Health Service (NHS) Information Centre. NHS Im-munisation Statistics England 2008�09: The NHS Information Centre.2009. http://www.ic.nhs.uk/statistics-and-data-collections/health-and-lifestyles/immunisation/nhs-immunisation-statistics-england-2008-09. Accessed 26 February 2010.
26. Oster NV, Harpaz R, Redd, SB, Papania MJ. International importa-tion of measles virus—United States, 1993–2001. J Infect Dis 2004;189(Suppl 1):S48–53.
27. Rota PA, Featherstone DA, Bellini WJ. Molecular epidemiology of mea-sles virus. Curr Top Microbiol Immunol 2009; 330:129–50.
28. Centers for Disease Control and Prevention. Measles—United States,January 1–April 25, 2008. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm57e501a1.htm. Accessed 25 February 2010.
29. Yip FY, Papania MJ, Redd SB. Measles outbreak epidemiology in theUnited States, 1993–2001. J Infect Dis 2004; 189(Suppl 1):S54–60.
30. MacIntyre CR, Gay NJ, Gidding HF, Hull BP, Gilbert GL, McIntyrePB. A mathematical model to measure the impact of the Measles Con-trol Campaign on the potential for measles transmission in Australia.Int J Infect Dis 2002; 6:277–82.
31. Marin M, Nguyen HQ, Langidrik JR, et al. Measles transmission andvaccine effectiveness during a large outbreak on a densely populatedisland: implications for vaccination policy. Clin Infect Dis 2006; 42:315–9
32. Watson JC, Pearson JA, Markowitz LE, et al. An evaluation of measlesrevaccination among school-entry-aged children. Pediatrics 1996; 97:613–8.
33. Vitek CR, Aduddell M, Brinton MJ, Hoffman RE, Redd SC. Increasedprotections during a measles outbreak of children previously vaccinatedwith a second dose of measles-mumps-rubella vaccine. Pediatr InfectDis J 1999; 18:620–3.
34. Salmon DA, Haber M, Gangarosa EJ, Philips L, Smith NJ, Chen RT.
Health consequences of religious and philosophical exemptions fromimmunization laws: individual and societal risk of measles. JAMA1999; 282:47–53.
35. Washington State Department of Health. Immunization program CHILDprofile: summary of immunization coverage for school entry grade.http://www.doh.wa.gov/cfh/Immunize/documents/kindercoverag08.pdf.Accessed 26 February 2010.
36. Meissner HC, Strebel PM, Orenstein WA. Measles vaccines and thepotential for worldwide eradication of measles. Pediatrics 2004; 114:1065–9.
37. Parker AA, Staggs W, Dayan GH, et al. Implications of a 2005 measlesoutbreak in Indiana for sustained elimination of measles in the UnitedStates. New Engl J Med 2006; 355:447–55.
38. Smith PJ, Chu SY, Barker LE. Children who have received no vaccines:who are they and where do they live? Pediatrics 2004; 114:187–95.
39. Centers for Disease Control and Prevention. Outbreak of measles—San Diego, California, January–February 2008. MMWR Morb MortalWkly Rep 2008; 57:203–6.
40. Dayan GH, Ortega-Sanchez IR, LeBaron CW, Quinlisk MP, Iowa Mea-sles Response Team. The cost of containing one case of measles: theeconomic impact on the public health infrastructure—Iowa, 2004. Pe-diatrics 2005; 116:e1-4.
41. Centers for Disease Control and Prevention. Update: measles—UnitedStates, January—July 2008. MMWR Morb Mortal Wkly Rep 2008; 57:893–6.
42. Salmon DA, Siegel AW. Religious and philosophical exemptions fromvaccination requirements and lessons learned from conscientious ob-jectors from conscription. Public Health Rep 2001; 116:289–95.
43. Omer SB, Salmon DA, Orenstein WA, deHart MP, Halsey N. Vaccinerefusal, mandatory immunization, and the risks of vaccine-preventablediseases. N Engl J Med 2009; 360:1981–8.
44. Kennedy AM, Gust DA. Measles outbreak associated with a churchcongregation: a study of immunization attitudes of congregation mem-bers. Public Health Rep 2008; 123:126–34.
45. Salmon DA, Sotir MJ, Pan WK, et al. Parental vaccine refusal in Wis-consin: a case-control study. Wisconsin Med J 2009; 108:17–23.
46. Omer SB, Pan WK, Halsey NA, et al. Nonmedical exemptions to schoolimmunization requirements: secular trends and association of statepolicies with pertussis incidence. JAMA 2006; 296:1757–63.
47. National Conference of State Legislatures. States with religious and phil-osophical exemptions from school immunization requirements. July2010. http://www.ncsl.org/programs/health/SchoolExempLawsChart.htm. Accessed 17 September 2010.
48. Feikin DR, Lezotte DC, Hamman RF, Salmon DA, Chen RT, HoffmanRE. Individual and community risks of measles and pertussis associatedwith personal exemptions to immunization. JAMA 2000; 284:3145–50.
49. Van den Hof S, Conyn-van Spaendonck MA, van Steenbergen JE. Measlesepidemic in Netherlands, 1999–2000. J Infect Dis 2002; 186:1483–6.
50. Gust DA, Darling N, Kennedy A, Schwartz B. Parents with doubts aboutvaccines: which vaccines and reasons why. Pediatrics 2008; 122:718–25.
by guest on Decem
ber 23, 2014http://jid.oxfordjournals.org/
Dow
nloaded from