japanese encephalitis
TRANSCRIPT

A 20 year-old Spanish man, without relevant past medical history, travelled to Thailand on 25 January 2013 to participate in a martial art competition. The expected duration of the trip was a month and a half. He had not attended a travel clinic before departure and was not prescribed or did not take malaria chemoprophylaxis.Upon arriving in Thailand, he visited Bangkok during two days where he stayed in a hotel. On 28 January he travelled by bus to Surat Thani, and on the same day he took the ferry to Koh Samui island.He stayed at bungalows in the beach (Chaweng and Lamai beaches) during all the stay. In Koh Samui, he trained every day but he also visited rural areas, went in the forest and visited waterfalls where was bitten by mosquitoes.
Case study
On 21 February, he was admitted to a local hospitalin Koh Samui with a 48 hours history of fever (38‹C), myalgia, �malaise and headache. Twenty-four hours after admittance, his condition worsened and photophobia, vomiting and decreased level of consciousness occurred.Physical examination revealed neck stiffness and Glasgow coma score (GCS) 11.Forty-eight hours later the patient presented seizures, V and VII left peripheral nerves palsy with right hemiparesis, and GCS decreased to nine.Intubation and invasive mechanical ventilation were required. Empiric treatment was initiated with ceftriaxone, doxycycline, acyclovir, dexamethasone and phenytoin.After five days the patient was tetraparetic and did not respond to simple commands. A tracheotomy was made and weaning from mechanical ventilation was started.
Initial full blood count, urine test and chest X-ray were normal. A cerebral computed tomography (CT) showed meningeal enhancement. Cerebrospinal fluid (CSF) analyses revealed a clear fluid with 960 leucocytes/mm3 (norm: 4,000–10,000/mm3) with 86% of mononuclear cells, and normal glucose and proteins.Multiple bacterial cultures including mycobacteria, polymerase chain reaction (PCR) for herpes virus, varicella-zoster virus, enterovirus, and rabies virus, blood and CSF Cryptococcus antigen, malaria blood smear and serological tests for human immunodeficiency virus (HIV), dengue virus, Leptospira species, Rickettsia species and Burkholderia pseudomallei were negative.
Lab IX ?

Real time-polymerase chain reaction (RT-PCR) for Japanese encephalitis virus (JEV) in CSF was negative. The result of IgM against JEV in serum was positive using an IgM capture enzyme-linked immunosorbent assay (ELISA) (IgM in CSF was not performed).

Japanese Encephalitis&
KFD
Dr Naresh T Chauhan

Introduction
• Encephalitis is an acute inflammatory process affecting the brain• Viral infection is the most common and important cause, with over
100 viruses implicated worldwide• Symptoms
– Fever– Headache– Altered level of consciousness– Focal neurologic deficits– Seizures– Behavioral changes
• Incidence of 3.5-7.4 per 100,000 persons per year
Causes of Viral Encephalitis
• Herpes viruses – HSV-1, HSV-2, varicella zoster virus, cytomegalovirus, Epstein-Barr virus, human herpes virus 6
• Adenoviruses• Influenza A• Enteroviruses, poliovirus• Measles, mumps, and rubella viruses• Rabies• Arboviruses – examples: Japanese encephalitis; St. Louis
encephalitis virus; West Nile encephalitis virus; Eastern, Western and Venzuelan equine encephalitis virus; tick borne encephalitis virus
• Bunyaviruses – examples: La Crosse strain of California virus• Reoviruses – example: Colorado tick fever virus• Arenaviruses – example: lymphocytic choriomeningitis virus

What Is An Arbovirus?
• Arboviruses = arthropod-borne viruses • Arboviruses are maintained in nature through
biological transmission between susceptible vertebrate hosts by blood-feeding arthropods
• Vertebrate infection occurs when the infected arthropod takes a blood meal

http://www.cdc.gov/ncidod/dvbid/arbor/schemat.pdf
Japanese Encephalitis
• Most important cause of arboviral encephalitis worldwide, with over 50,000 cases reported annually
• Transmitted by culex mosquito, which breeds in rice fields– Mosquitoes become infected by feeding
on domestic pigs and wild birds infected with Japanese encephalitis virus. Infected mosquitoes transmit virus to humans and animals during the feeding process.

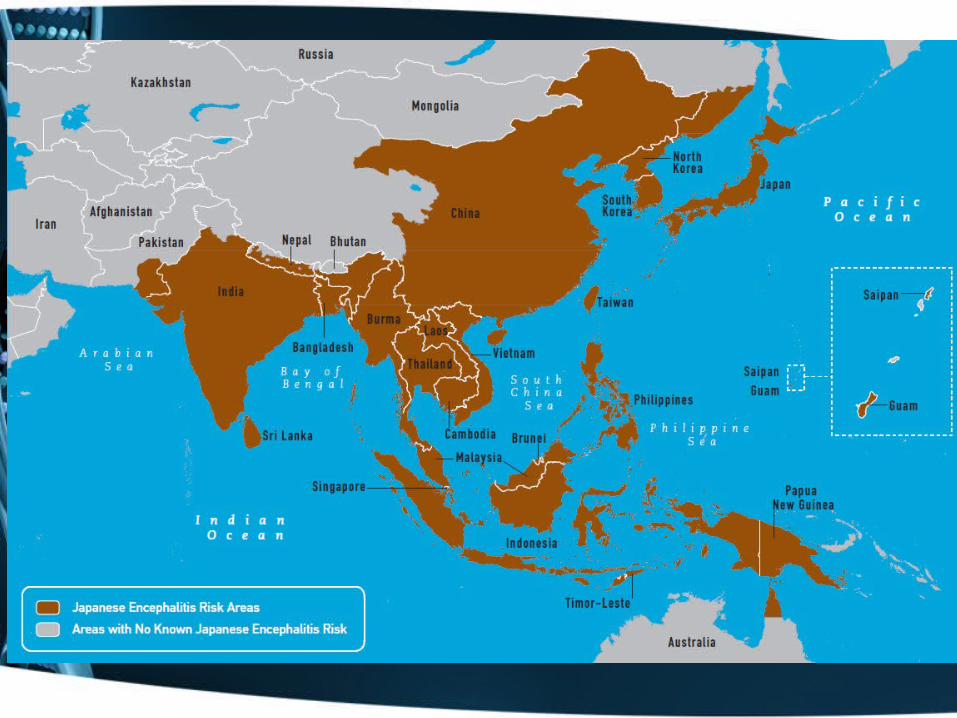
Epidemiology
• Primarily a disease of rural Asia– Vector mosquitoes proliferate in close
association with birds and pigs– Birds and pigs are the major amplifying
hosts• Culex tritaeniorhynchus the principal vector
but many other mosquitoes are competent and can transmit– C. pipiens– C. quinquefasciatus– Species of Aedes, Anopheles

Transmission cycle of the Japanese encephalitis virus
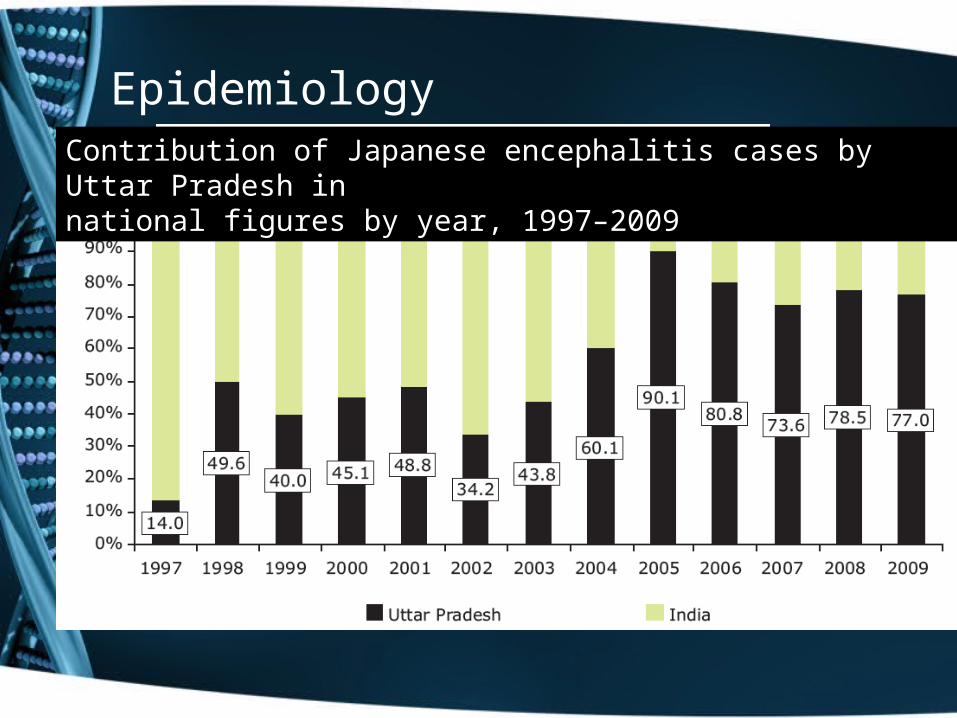
EpidemiologyBiharContribution of Japanese encephalitis cases by Uttar Pradesh in
national figures by year, 1997–2009
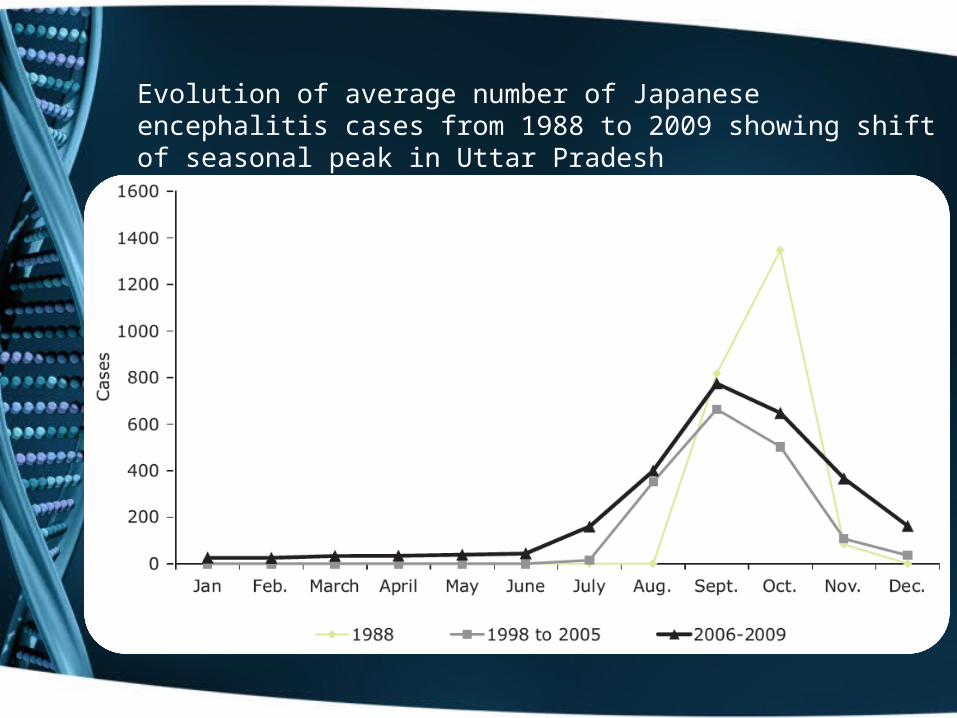
Evolution of average number of Japanese encephalitis cases from 1988 to 2009 showing shift of seasonal peak in Uttar Pradesh

Distribution of Japanese encephalitis cases by age and sex, Gorakhpurdivision, Uttar Pradesh 7A: Distribution of JE cases by age/sex, Gorakhpur, 2009

Incidence and Prevalence
• Ratio of apparent to inapparent infection ranges from 1:300 to 1:1000
• Ratio affected by age, virulence of the strain of virus, cross protective immunity from other Flaviviruses (dengue)
• Risk to travelers 1 case per 50,000 months of exposure
History of Japanese Encephalitis
• 1871s – recognized in Japan• 1924 – Japan epidemic. 6125 cases,
3797 deaths• 1935 – virus isolated in brain of
Japanese patient who died of encephalitis
• 1938 – virus isolated from Culex mosquitoes in Japan
• 1948 – Japan outbreak• 1949 – Korea outbreak• 1966 – China outbreak

Flaviviruses
Japanese Encephalitis Virus
St. Louis encephalitis virus
West Nile Virus

Overview of Flaviviruses
• RNA viruses related to Yellow Fever virus• At least 80 different ones, over 40 can infect
humans• Most are arthropod borne, • One with the greatest impact on human health
– Yellow fever virus– Dengue fever virus– Japanese encephalitis virus– West Nile virus– St Louis encephalitis virus
Pathogenesis
• Pathology• Usually gray matter is involved. Lesions are seen
in thalami, substantia nigra, cerebral cortex, cerebellum, Ammon’s horn, and anterior horn of spinal cord

Clinical Manifestations
• Incubation 6-16 days. Spectrum from mild febrile headache to severe encephalitis
• Headache, fever, nausea, vomiting, drowsiness. Abdominal pain and diarrhea common in children
Clinical manifestation
• Symptoms and signs of infection: • Symptoms and signs of focal brain damage due to
infection• Symptoms and signs of raised intracranial tension: • Symptoms and signs of meningeal irritation• Non-neurologic signs

Developing Signs
• Altered LOC – mild lethargy to deep coma.• AMS – confused, delirious, disoriented.• Mental aberrations:
– hallucinations– agitation– personality change – behavioral disorders – occasionally frank psychosis
• Focal or general seizures in >50% severe cases.
• Severe focused neurologic deficits.

Clinical Manifestations
• Death in 5-40%• Children under 10 more likely to
die or have residual neurological defects
• Poor prognosis associated with– Respiratory dysfunction– Babinsky’s sign– Frequent or prolonged
seizures– Prolonged fever– Albuminuria– High viral replication in the
brain
Neurologic Signs
• Most Common– Aphasia– Ataxia – Hemiparesis with hyperactive tendon reflexes– Involuntary movements– Cranial nerve deficits (ocular palsies, facial
weakness)

Neuropsychiatric Sequelae
• Occur in 45-70% of survivors, particularly severe in children
• Parkinsonism• Seizures• Paralysis• Mental retardation• Psychiatric disorders

Differential Diagnosis
• Distinguish Etiology– Bacterial infection and other infectious conditions– Parameningeal infections or partially treated bacterial
meningitis– Nonviral infectious meningitides where cultures may be
negative (e.g., fungal, tuberculous, parasitic, or syphilitic disease)
– Meningitis secondary to noninfectious inflammatory diseases
• MRI– Can exclude subdural bleeds, tumor, and sinus thrombosis
• Biopsy

Standard Case definition
Suspect (History)• A person of any age at any time of year with
acute onset of fever and change in mental status AND/OR new onset of seizures (Exclude SFS)
Probable (History and clinical Exan)• A suspect case that occurs in close geographical
and temporal relationship to a laboratory confirmed case of JE, in the context of an outbreak
Confirmed (laboratory Test)• Presence of JE virus specific Ig-M antibodies
Laboratory Diagnosis
• Diagnosis is usually based on CSF – Normal glucose– Absence of bacteria on culture. – Viruses occasionally isolated directly from CSF– IgM-capture ELISA
• Polymerase Chain Reaction techniques– Detect specific viral DNA in CSF
Treatment
• ‘ABCs’ of resuscitation• Seizure management: • For raised intracranial tension: • Prevent and treat pain • Nutrition and fluids • Antibiotics to be used as and when necessary.

Dexamethasone
• Synthetic adrenocortical steroid • Potent anti-inflammatory effects• Dexamethasone injection is generally
administered initially via IV then IM• Side effects: convulsions; increased ICP after
treatment; vertigo; headache; psychic disturbances

Prevention
• Personal protective measures and mosquito elimination are the most important
• travellers going to endemic areas may consider vaccination

• Keep all drains free from blockage
• Cover tightly all water containers, wells and water storage tanks
• Top up all defective ground surfaces to prevent the accumulation of stagnant water
Prevent mosquito breeding
• Put all used cans and bottles into covered dustbins
• Change water for plants at least once a week, leaving no water in the saucers underneath flower pots
Prevent mosquito breeding

Prevention of Mosquito Bites
• Avoid going to rural area during dusk and dawn when the mosquitoes are most active
• Wear light-colored, long-sleeved clothing and trousers
• Apply DEET-containing mosquito-repellents over exposed parts of the body and clothes every 4 to 6 hours
• For DEET products used by children, its concentration should be less than 10%
Prevention of Mosquito Bites
• hang mosquito screens around your bed, use insecticides or coil incenses to repel mosquitoes
• Place of accommodation should have air-conditioners or mosquito nets; or
• Install mosquito nets to doors and windows so that mosquitoes can’t get in
Vaccination
– Appears to be 91% effective– There is no JE-specific therapy other than
supportive care – Live-attenuated vaccine developed and
tested in China • Appears to be safe and effective
– Vero cell-derived inactivated vaccines have been developed in China
Vaccines for JE virus
– Inactivated vaccine grown in primary hamster kidney cells
– Live attenuated vaccine (SA14-14-2) grown in hamster kidney cells
– Licensed as JE-VAXR – Three subcutaneous injections over a
month with a booster at 3 years– 91% efficacy in a large field trial in
Thailand

References
• A review of Japanese encephalitis in Uttar Pradesh,India, Roop Kumaria, Pyare L Joshib WHO South-East Asia Journal of Public Health 2012;1(4):374-395
• Japanese Encephalitis, Potharaju Nagabhushana Rao,Indian Pediatrics 2001; 38: 1252-1264
• Doti P, Castro P, Martinez MJ, Zboromyrska Y, Aldasoro E, Inciarte A, Requena A, Milisenda J, Fernandez S, Nicolas JM, Munoz J. A case of Japanese encephalitis in a 20 year-old Spanish sportsman, February 2013. Euro Surveill. 2013;18(35)
• JE ICMR document• Map of geographical distribution WHO• Japanese encephalitis: a review of the Indian perspective Sarika Tiwari,
Rishi Kumar Singh, Ruchi Tiwari, Tapan N. Dhole. braz j infect dis. 2012;16(6):564–573
Kyasanur Forest Disease

History …..
• Heavy mortality in two species of monkey
( Langur & Red faced bonnet ) in 1955 in forests of Shimoga led to the discovery of KFD
• Mortality in monkeys was followed by acute febrile prostrating illness among villagers and few human deaths

History …….Autopsy on monkeys
Place of reporting of First monkey death in march 1957

Kyasanur forest disease• Found in India• Limited originally to
Shimoga district in Karnataka (800 sq km
• Newer foci in 3 more districts namely U.kannada,D. Kannada and Chikmangaluru
( 6000 sq km )• Serosurveys reveal KFD
in Kutch & Saurashthra

Problem statement
The outbreak during 1983-1984 is the largest with 2167 cases and 69 deaths.
In 1997 the cases came down to75 and deaths to 4.
The number of human deaths varied between 4-15% of the cases
Even today few hundreds of cases and some deaths are reported

Agent factors ..
• Kyasanur forest disease (KFD) is a febrile disease associated with hemorrhages caused by an arbovirus flavivirus.
• KFD virus is a member of group B togaviruses
• Belongs to Russian spring summer encephalitis (RSSE) group of viruses

HOST FACTORS
• Age :majority between 20 and 40 years.• Sex: males• Occupation: Cultivators who visit forest with cattle
or cutting wood.• Epidemic correlates with peak human activity in
forests i.e between January and June
Natural hosts & reservoirs
• Circulates in small mammals rats, squirrels, shrews and bats are the main reservoirs .
• Neutralizing antibodies have also been found in cattle, buffaloes, goats and porcupines
• Maintenance hosts – maintain the infection in nature
Natural hosts & reservoirs
• Monkeys are the amplifying hosts for the virus.
• Amplifying hosts --- multiplication of the virus takes place at very high levels such that the intensity of infection is very high.

Natural cycle
• In enzootic states the infection is maintained in small mammals and also in ticks
• When monkeys come in contact with infected ticks , they get infected , amplify and disseminate the infection in “hot spots ”of infection
• Humans in these hot spots are infected by bite of infected anthrophilic ticks like H. spinigera
VECTORSFemale tick laying eggs
Virus has been isolated from 16 species of ticks but Hard tick species of the genus Haemophysalis particularly H.spinigera and H.turtura are the main vectors
Ticks act as both as vectors and reservoirs of infection in KFD
Vector bionomics and seasonal transmission of KFD
• Adult Ticks become active after few monsoon rains in June
• Adult population reaches peak during July & August and gradually declines in September
• Larval activity builds in post monsoon Oct-Dec
• Nymphal activity high from January to May
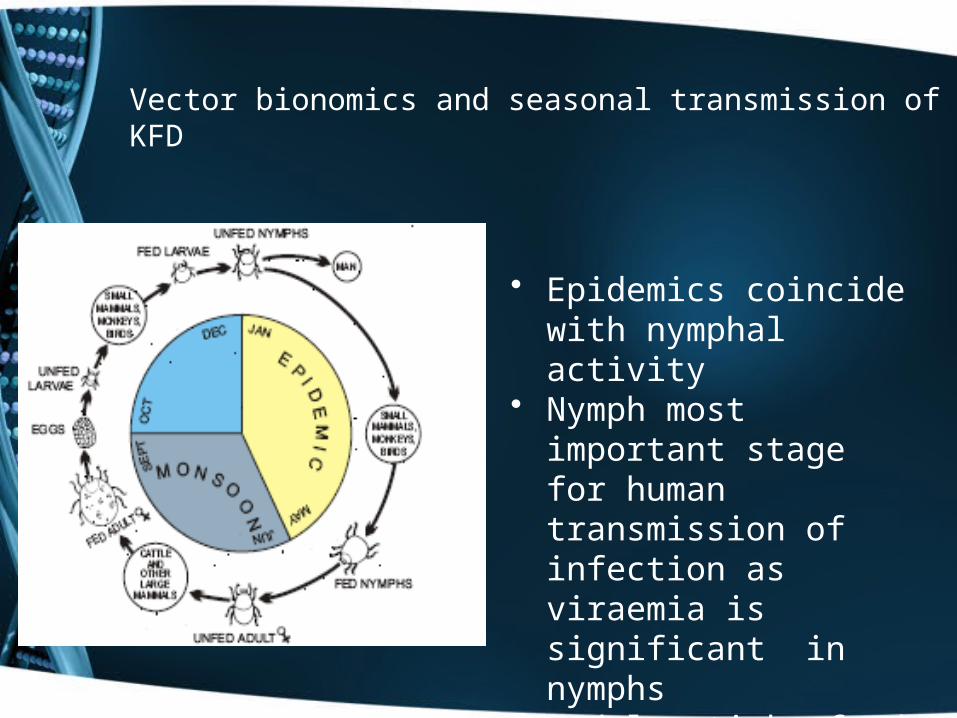
Vector bionomics and seasonal transmission of KFD
• Epidemics coincide with nymphal activity
• Nymph most important stage for human transmission of infection as viraemia is significant in nymphs
• Adults ticks feed on cattle and viraemia is not significant
Environmental factors
Tropical evergreen, deciduous forests
Clearing of forests for cultivation and other developmental activities leads to change in tick flaura and fauna and is an important determinant for outbreaks
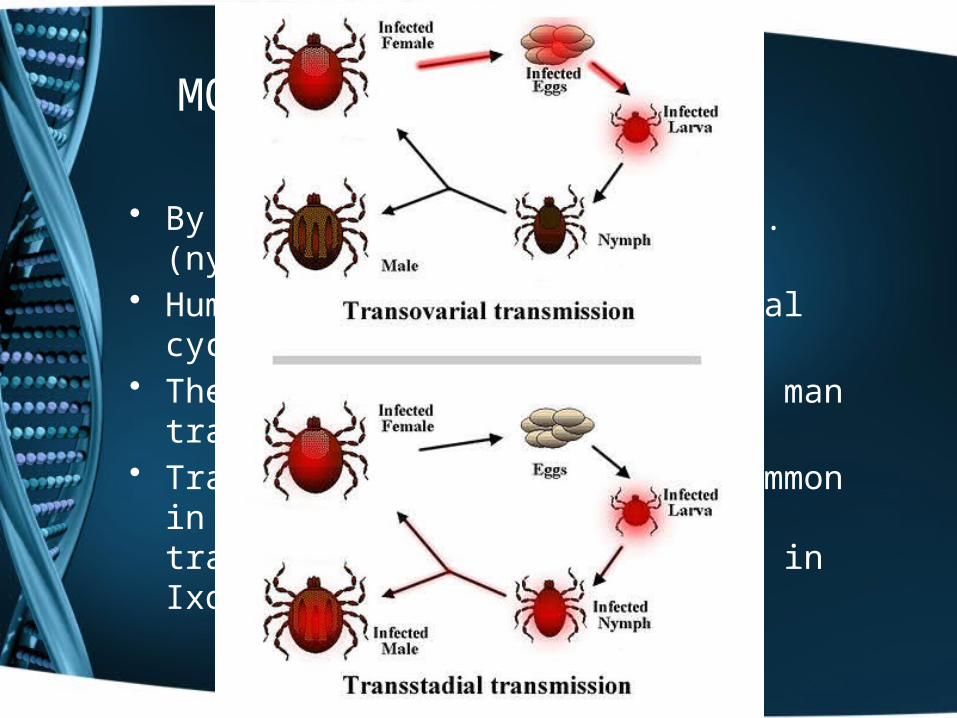
MODE OF TRANSMISSION
• By the bite of infective ticks.(nymphal stage )• Human is dead end in the natural cycle • There is no evidence of man to man
transmission • Transtadial transmission is common in ticks but
transovarial transmission is absent except in Ixodides species
CLINICAL FEATURES
• Acute phase with sudden onset of fever, headache ,severe myalgia with prostration lasting for 2 weeks.
• GI disturbances and hemorrhagic manifestations in severe cases
• Second phase characterized by mild meningoencephalitis after an afebrile period of 7- 21 days.
• Case fatality varies between 4-16%

Treatment
Conservative
• Antipyretics • Analgesics • Supportive therapy

Diagnosis
• Diagnosis by suspicion by clinical signs and symptoms
• H/O occupation/travel in forests • Detecting the presence of virus in blood.• Serological evidence by haemagglutination and
immunofloresence

CONTROL
• Timely control decreases morbidity and mortality in humans
CONTROL OF TICKS• By aircraft mounted equipment to dispense
lindane , cabaryl fenthion at 2.24 kg / hectare at forest floor
• Spraying carried out within 50m around hot spots • Restriction of cattle movement brings reduction in
vector population

CONTROL
Personal protection • Adequate clothing • Insect repellants such as DMP, DEET provide 90-
100% protection against tick bites • Examine themselves for ticks and promptly
remove them• Health education
CONTROL
Vaccination • Inactivated chick embryo tissue culture
vaccine developed by NIV, Pune • Neutralizing antibodies in 70% of vaccinated
persons • Vaccinating at risk population i.e villagers
living near forests , forest workers , occupational personnel concerned with forests
Bio safety concerns
• One of the highest risk category pathogens
• Bio safety level 4
• One of the potential bioterrorist weapon

THANKS