jennifer hunter - national institute of complementary medicine university of western sydney -...
TRANSCRIPT

Delivering on the benefits of ancillary services in
PHI cover
Dr. Jennifer HunterBMed, MScPH, PhD

Ancillary Services
• Ancillary services and the benefits in health promotion
• The impact of low cover products on community ratings
• Review of the PHI rebate for homeopathy
• Evidence based science and natural remedies

PHI in Australia
• Hybrid (½ UK : ½ USA) disconnected healthcare system
• Regulations and tax incentives distorting market signals
• No direct financial return for improving patient outcomes
• Unsustainable projections for public and private healthcare
• And so on….

Ancillary care is a doctor-‐centric term
Ancillary Care refers to the wide range of healthcare services provided to support the work of a primary physician.
Ancillary definition:adjective 1. subordinate; subsidiary2. auxiliary; assisting

Allied Health refers to the wide range of healthcare services professionals able to operate autonomously
Ally definition:verb1. To formally cooperate, combine or unite a resource or commodity with another for mutual benefit
Allied Health a better term than ancillary?

Doctor-‐centric model of healthcareStrengths• Acute medicine • Specialised• High-‐tech• Curative
Weaknesses• Increasingly expensive• Chronic disease• Disease prevention• Health promotion

Time bomb chronic disease
• Aging population
• Physical, psychological, cognitive
• Many have multiple chronic diseases
• Unsustainable healthcare model
“we have an acute disease system for an aging, chronic disease population”

“You can make bad decisions now that will have massive repercussions”
Warwick Thornton(Samson & Delilah)The future is unforgiving
Anna Schwartz GalleryMelbourne 17 July – 22 August 2015

Allied Health services and the benefits in health prevention
• Who are they?
• What do they do?Allied health practitioners work autonomously within their scope of practiceHuge list of APHRA registered along non-‐registered practitioners
Physiotherapist, Chiropractors, Osteopaths, Massage therapistsAcupuncturists, TCM herbalistsNaturopaths, Nutritionists, DietitiansPsychologists, Occupational therapistsPharmacists, Podiatrists, Optometrists and so on…

Australian Health Practitioner Regulation Agency 2015National Infrastructure Audit CM Practitioners 2015 (unofficial)
Australian healthcare workforce Doctor15%
Dentist3%
Nurse Midwife55%
Pharmacist4%
Psychologist5%
CM registered2%
CM unregistered6%
Other allied health10%
≈27% Allied Health

Underutilised Allied Health for chronic disease management
• Bullet points
40%
9% 7%
30%
10% 10%20%17%
Australian Health Survey ABS 2011-‐2012

healthinsurancecomparison.com.au

Intergenerational Report 2015
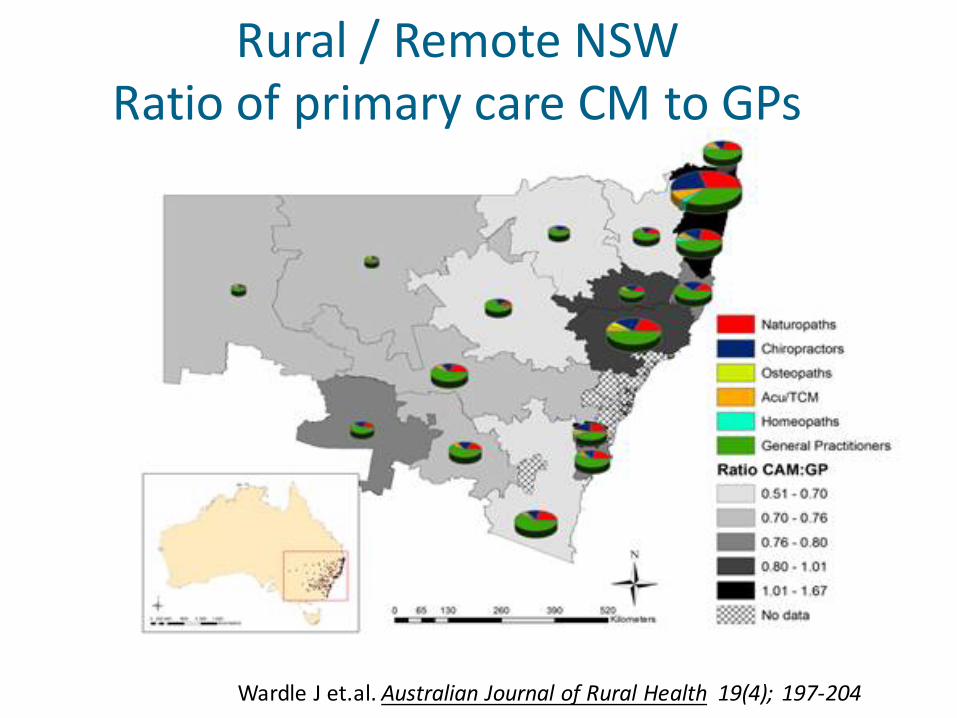
Wardle J et.al. Australian Journal of Rural Health 19(4); 197-‐204
Rural / Remote NSWRatio of primary care CM to GPs

Why do people use CM?
• Adjuvantnot a replacement for ‘medical care’
• Wellness (51%)1
• Wellness and disease management (35%) 1
• Manage top 5 priority health conditions 2
1. National Health Interview Survey, USA 2007 2. National Health Survey, Australia 2004-‐05

Who uses complementary medicine -‐ CM?
• 20 primary care; up to 70% use generally
• 25 -‐64 y.o, female, educated, wealthier
• Less illness, better self reported health, healthier lifestyle
• PHI extras cover60% who saw a CM practitioner in last 2 weeks had PHI extras(compared to 41% total population)
National Health Survey, Australia 2004-‐05

Extras Cover – which one will you choose?

Imagine PHI providers as leaders inhealth and people care (not just disease care)
• Build strong, healthy, resilient, vital people who areactively participating in our community
• New and innovative ways to encourage and reward healthy living
• Holistic approach -‐ physical, cognitive, emotional, social, occupational, financial, spiritual
• Patient-‐centred, individualised services
• Practitioner incentives to promote health that is more than the absence of disease

1.9M same day procedures (+6%)1.4M overnight procedures (+2.5%)Hospital treatment $1,206, or $3,217 per episodeApprox. $25M increase hospital costs
85M allied health services (+3.4%)10M physiotherapy (+4.1%)5.7M natural therapies services (+6.1%)$52 per natural therapy consultationApprox. $2,7M increase natural therapy
Private Healthcare Australia 28 May 2015

Evidence based science and natural remedies

Is there any CM Evidence?• Under funded researched topic
• Difficult to undertake high quality research
• Increasing scientific evidence

Acupuncture in combination with conventionaltreatment for chronic lower back pain
1. Systematic review Cochrane 2005 -‐ 35 RCT, 2861 patients [1]
2. Cost effectiveness Economic modelling for Australia [2]
3. Clinical guidelines2013 American College of Physicians & American Pain Society: Rec.72009 NICE: Section 1.6.1
[1] Spine 2013 Nov 15;38(24):2124-‐38.[2] Pain Pract. 2013 Oct 21 [Epub ahead of print]
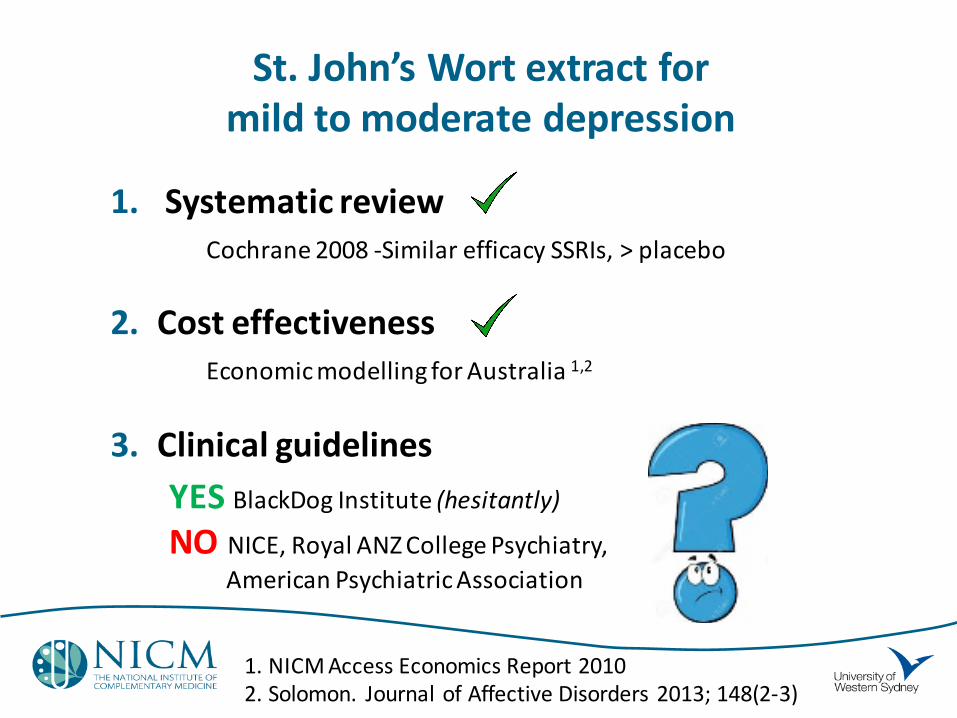
St. John’s Wort extract for mild to moderate depression
1. Systematic review Cochrane 2008 -‐Similar efficacy SSRIs, > placebo
2. Cost effectiveness Economic modelling for Australia 1,2
3. Clinical guidelinesYES BlackDog Institute (hesitantly)
NO NICE, Royal ANZ College Psychiatry, American Psychiatric Association
1. NICM Access Economics Report 20102. Solomon. Journal of Affective Disorders 2013; 148(2-‐3)

Plethora of clinical guidelines
Often do not consider CMeven when good evidence
Lack transparency about the decision to exclude CM
Rarely make a strong recommendation to either to use or not use CM
Eur. J Integrative Medicine. 2014;6(2):164-‐75.
Clinical guidelines about CM use

NHMRC review of natural therapists
• Claim bastions science, delivered low quality methods
• Narrow search terms -‐> no evidence
• Incorrect definitions and criteria
• Medical professions would alsofail the test
• Only 9% oncology practice guidelineshigh level of evidence 1
1. J Clin Oncol. 2011;29(2):186-‐191

Efficacy is only one component of scientific evidence-‐based medicine
• RCTs strive for high internal validity
• Narrow inclusion / exclusion criteria
• Randomisation and blinding
• BUT low external validityaka low generalisability forreal world scenarios

“There is no such thing as an ever valid hierarchy of evidence.
There is only evidence that has a higher level of internal validity, and
evidence that may have a higher level of external validity.”
Walach,H & Loef,M J Clinical Epidemiology (2015), doi: 10.1016/j.jclinepi.2015.03.027.

Comparative Effectiveness Research
• RCTs >2 active (non-‐placebo) intervention arms
• Database studies
• Observational studies
• Model-‐based studies
• Decision analysis

0
10
20
30
40
50
60
70
80
Treatment Comparison Treatment Comparison Treatment Comparison
Artifacts/Natural history Non-‐specific effects/Placebo Specific treatment effect
Trend suggestingdifference
Nodifference
Pre-‐existing belief in efficacy increases non-‐specific effects and placebo effect
Consecutive positive results increases non-‐specific effect
Significant difference
TIME -‐-‐>
Walach,H & Loef,M J Clinical Epidemiology (2015), doi: 10.1016/j.jclinepi.2015.03.027.

Placebo/ sham treatments that work
• Four placebo tablets work better than two in gastric ulcers
• Pink dummy pills are better at maintaining concentration than blue ones
• Placebo injections are more effective than placebo pills
• Placebo painkillers work better if they're believed to be costly than if they're believed to be cheap
• Placebo surgery works for people with knee pain
• Sham acupuncture for pain is better than doing nothing
Bad Science, Ben Goldacre, Fourth Estate, 2008

When is placebo a bad thing?
• Pretend it’s not
• Expensive
• Side effects
• Unsafe
• Opportunity costs

Review of the PHI rebate for homeopathy
• NHMRC review of reviews(poor quality methodology)
• Excluded studies promoting health or wellbeing (disease only)
• Is the jury is still out?
• The clinical trials continue
• Quality of trials improving

Individualized homeopathic treatment verses fluoxetine for moderate to severe depression
• 133 peri & post menopausal women
• Randomized, double-‐dummy, double-‐blind, placebo-‐controlled trial
• 3 groups: homeopathy, fluoxetine, placebo
• Homeopathy & fluoxetine > placebo for depression
• Homeopathy > placebo for menopausal symptoms
• Fluoxetine = placebo for menopausal symptoms
PLoS One. 2015; 10(3): e0118440

Homeopathy as adjuvant for Rheumatoid Arthritis
• Randomised, double-‐blind, placebo trial
• 83 adults with active stable RA receiving conventional therapy
• Evidence for effectiveness homeopathic consultation
• Fund homeopaths but not the homeopathic medication?
Rheumatology (Oxford). 2011 Jun; 50(6): 1070–1082.

0
10
20
30
40
50
60
70
80
Treatment Comparison Treatment Comparison Treatment Comparison
Artifacts/Natural history Non-‐specific effects/Placebo Specific treatment effect
Trend suggestingdifference
Nodifference
The consultation will increase the non-‐specific / placebo effect
Significant difference
Walach,H & Loef,M J Clinical Epidemiology (2015), doi: 10.1016/j.jclinepi.2015.03.027.


How can PHI promote health & reduce costs?• Think outside the box –
allied health, traditional & natural medicine, lifestyle medicine, self-‐care, antenatal & children, employers
• Catch the horse that has bolted –secondary disease prevention interventionsmaximise health, minimise disease complications
• Reward healthy behaviour –without compromising community rating & ethics
• BE CREATIVE!

Thank You