jim dunford, md city of san diego medical director (ems ... · pdf filechildren 12-19 yo 60+...
TRANSCRIPT

Jim Dunford, MD
City of San Diego Medical Director (EMS)
Professor Emeritus, UCSD Emergency Medicine
President, San Diego AHA Board of Directors

Introduce 2020 AHA National Goals
Describe two valuable AHA tools ◦ Life’s Simple 7 - quantifies individual’s CV health
◦ GWTG-Outpatient – HER data extraction software
Describe Vision for San Diego EMS ◦ Two examples of successful partnerships
◦ New opportunities for accountable, meaningful care

Primordial prevention
Primary prevention
Secondary prevention
Emergency response




Circulation 2010; 121: 586-613

2020 Impact Goals
- Improve CV health of all Americans by 20% - Reduce death from heart disease stroke by 20%
20 % positive difference on measurable health gains
20 % negative difference on death rates

Define ideal CV health
Provide tool to objectively measure health
Quantify health along continuum ◦ Poor --- Intermediate --- Ideal
Support and assist

Goal/Metric Ideal Cardiovascular Health Definition Current Smoking Adults ≥20 yo Never or quit >12 months ago Children 12-19 yo Never tried; never smoked whole cigarette
Total Cholesterol Adults ≥20 yo <200 mg/dL* Children 6-19 yo <170 mg/dL*
Blood Pressure Adults ≥20 yo <120/<80 mm Hg* Children 8-19 yo <90th percentile*
Fasting Glucose Adults ≥20 yo <100 mg/dL* Children 12-19 yo <100 mg/dL*
*Untreated

Ideal CV Health Behaviors
Goal Ideal CV Health Definition BMI Adults ≥ 20 yo <25 kg/m2 Children 2-19 yo <85th percentile
Physical Activity
Adults ≥ 20 yo 150+ min/wk mod or 75+ min/wk vigorous
Children 12-19 yo 60+ min mod. or intense vigorous daily
Healthy Diet Adults ≥ 20 yo 4-5 components Children 5-19 yo 4-5 components

Goal/Metric Poor Health Intermediate Health Ideal Health Current Smoking
Adults ≥20 yo Yes Former <=12 months Never or quit >12 months
Children 12-19 yo Tried prior 30 days Never tried; never whole cigarette
Body Mass Index
Adults ≥20 yo ≥30 kg/m2 25-29.9 kg/m2 <25 kg/m2
Children 2-19 yo >95th percentile 85th-95th percentile <85th percent ile
Physical Activity
Adults ≥20 yo None
1-149 min/wk moderate or 1-74 min/wk vigorous or 1-149 min/wk mod + vig
150+ min/wk mo derate or 75+ min/wk vigorous or 150+ min/wk mod + vig
Children 12-19 yo None >0 and <60 min of moderate or vigorous daily 60+ min of mod or vig daily
Healthy Diet Score
Adults ≥20 yo 0-1 components 2-3 components 4-5 components
Children 5-19 yo 0-1 components 2-3 components 4-5 components
Total Cholesterol
Adults ≥20 yo ≥240 mg/dL 200-239 mg/dL or treated to goal <200 mg/dL
Children 6-19 yo ≥200 mg/dL 170-199 mg/dL <170 mg/dL
Blood Pressure
Adults ≥20 yo SBP ≥140 or DBP ≥90 mm Hg SBP120-139 or DBP 80-89 or Rx to goal <120/<80 mm Hg
Children 8-19 yo >95th percentile 90th-95th percentile or SBP ≥120 or DBP ≥80 mm Hg <90th percentile
Fasting Plasma Glucose
Adults ≥20 yo ≥126 mg/dL 100-125 or treated to goal <100
Children 12-19 yo ≥126 mg/dL 100-125 <100

http://mylifecheck.heart.org/

http://mylifecheck.heart.org/



17

0
5
10
15
20
25
30
35
All Uses
Male Uses
Female Uses
Avg. Heart Score
Avg. Male HS
Avg. Female HS



Instituted 2001
1500 hospitals
2 million patient records
>55 peer-reviewed publications


0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Performance Measure
Co
mp
lia
nc
e
Baseline 82.1% 83.3% 77.9% 68.8% 72.1% 62.6% 76.9% 56.1%
Current 90.0% 94.2% 94.2% 92.0% 92.0% 98.6% 92.5% 85.2%
ASA within
24 Hours
ASA at
Discharge
Beta Blockers
at Discharge
ACEI or ARB at
D/C for LVSD
Lipid Lowering
Therapy at D/C
for LDL > 100
Smoking
Cessation
Counseling
Composite
Performance
Measure
100%
Compliance
Measure

0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Performance Measure
Co
mp
lian
ce
Baseline 69.7% 90.1% 81.2% 87.3% 77.4% 80.1% 60.1%
Current 89.8% 97.3% 92.3% 92.4% 96.6% 93.2% 84.7%
Discharge
Instructions
LV Function
Measurement
ACEI or ARB at
D/C for LVSD
Beta Blocker at
D/C for LVSD
Smoking Cessation
Counseling
Composite
Performance
Measure
100% Compliance
Measure

0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Performance Measure
Co
mp
lian
ce
Baseline 27.6% 87.9% 65.9% 92.7% 52.9% 39.7% 44.3% 70.5% 40.2%
Current 70.0% 96.0% 93.2% 97.4% 93.5% 85.1% 95.7% 92.7% 83.8%
tPA < 3hr with
Arrival < 2hr after
Onset
Early
Antithrombotic
DVT Risk
Management
Antithrombotic Tx
at
Discharge
Anticoag. Tx at
Discharge for Afib
Lipid Lowering
Therapy at D/C for
LDL > 100
Smoking Cessation
Counseling
Composite
Performance
Measure
100% Compliance
Measure

CONFIDENTIAL – American
Heart Association 2009

Duke Clinical Research Institute
EHR A
Performance
reports
Patient
data sent
via EHR
EHR B

Internal Medicine
Family Medicine
Osteopathic Medicine
OB/GYN
Cardiology
Neurology
Geriatric Medicine
Etc.
Patients 18 and Over

Demographics
Risk Factors
Medical History
Hospitalizations
Labs
Vital Signs
Medications
Contraindications
Mortality
*full list of elements can be found on americanheart.org/outpatient

AMA/PCPI/ACC/AHA Measures
◦ Coronary Artery Disease
◦ Heart Failure
◦ Tobacco Use and Counseling
CMS/NCQA
◦ Pneumonia Vaccination
◦ Flu Shots for Older Adults
CMS/SCRIPT
◦ Medication Management
PQRI Measures
◦ Screening – Preventive Care
◦ Diabetes Mellitus
◦ CAD
PQRI
◦ Heart Failure
AHA/ACC 2009 Measures
◦ Primary Prevention
◦ Atrial Fibrillation – 2007
◦ Pending Heart Failure
Management to Goal
See GWTG-O handout - FAQ



33
Simplifies data extraction
Quarterly reports
Aligns with incentive-based programs
National recognition
Allows participation in research
Access to AHA resources clinical support; professional & patient education

Stanford
Northwestern


Goal: < 8 min (90%)
First responder: 1 paramedic
3 EMTs
Ambulance: 1 paramedic
1 EMT
Requirement: < 12 min (90%)
San Diego EMS

• Seamless emergency care
• Uniform training and education
• Oversight and transparency
Rural/
Metro
City of
San
Diego

In partnership with the
community, we shall provide
innovative and quality medical
care

Paramedic 1st response
Medical call center
Field operations
CQI
CE
Ambulance personnel
Supplies and maintenance
Financial management
Capital infusion
Non-911 transportation BLS, CCT, wheelchair, bariatric
Sharp Healthcare
Kaiser
Palomar-Pomerado



10 (acute status)
8%
20 (ALS care
provided)
14%
30 (ALS monitor)
15%
40 (BLS care)
21%
50 (alt. transport
would have been
approp.)
19%
No Transport
23%
10 (acute status)
20 (ALS care provided)
30 (ALS monitor)
40 (BLS care)
50 (alt. transport would
have been approp.)
No Transport


Hospital
Detox
Jail

18 months UCSD & Scripps Mercy 312 EMS transports 417 ED visits
$1,476,000 Dunford J. Report to the SDPD Homeless Outreach Team. 1997

In Reno one man ran up >$1 million in medical bills and still died on the streets
Gladwell M. “Million Dollar Murray”. The New Yorker. Feb 13, 2006

San Diego Police Department
San Diego EMS
Mental Health Systems, Inc.
SD Sheriff’s Department
SD County Alcohol and Drug Services
SD City Attorney
Office of the Public Defender
Superior Court
St. Vincent de Paul Village

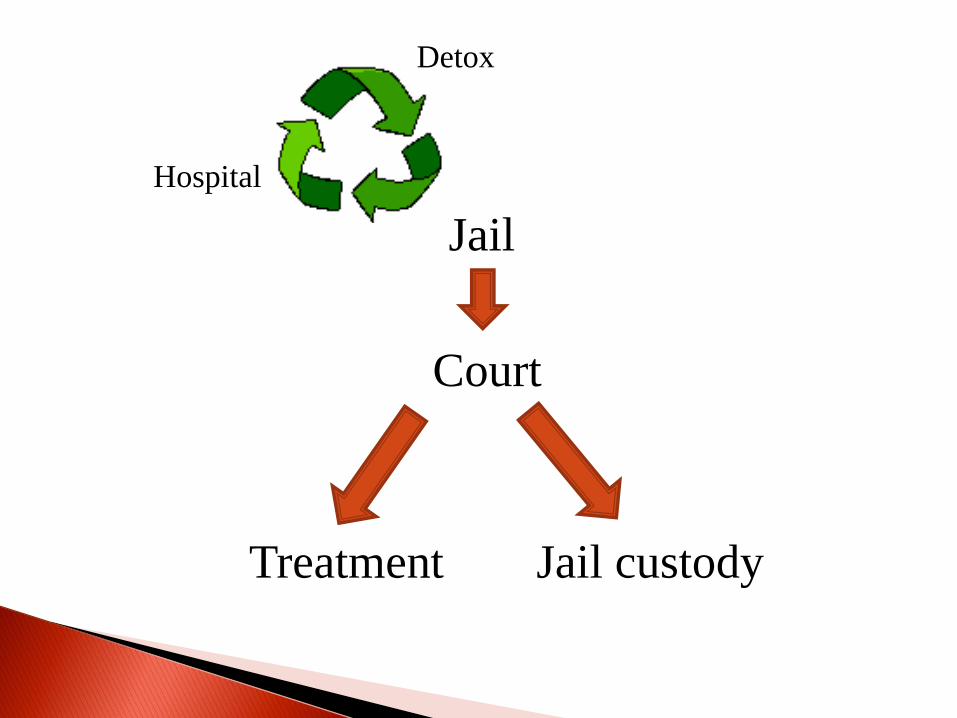
Hospital
Detox
Jail
Treatment
Court
Jail custody

529 patients
EMS, ED IP billing data
2000 – 2004
UCSD & Scripps Mercy
Impact of SIP on utilization of medical resources
Dunford JV et al. Ann Emerg Med. 2006;47(4):328-336

Charges Payments %
EMS $1,276,977 $176,725 13.8
ED $2,530,398 $389,286 15.4
IP $13,939,910 $2,742,850 19.7
Total $17,747,245 $3,308,861 18.6
Dunford JV et al. Ann Emerg Med. 2006;47(4):328-336

-60,000
-50,000
-40,000
-30,000
-20,000
-10,000
0
EMS ED In-pt.
- $73,552/mo
Dunford JV et al. Ann Emerg Med. 2006;47(4):328-336

-200%
0%
200%
400%
600%
800%
1000%
accept decline
EMS
ED
In-pt.
953%
Dunford JV et al. Ann Emerg Med. 2006;47(4):328-336

“… we’ve unearthed evidence-based
research that allows us to make policy and provide investment in
these projects”.

Acute care
Health management
Fully integrated
Identify & modify risk
Monitor community health
August 1996

1%

90%
10%

21
48 48
82
0
10
20
30
40
50
60
70
80
90
Private
insurance
Uninsured Medicare Medicaid
ED
vis
its p
er
100 p
ers
on
s
CDC/NCHS. National Hospital Ambulatory Medical Care Survey. 2006

214 patients
3126 transports ◦ 4% of all transports in City!

EMS
SDPD PERT
HHSA

736
199
33
459
143
30
0
100
200
300
400
500
600
700
800
EMS ED IP
Pre-RAP
Post-RAP
Tadros A et al. 2010 APHA Annual meeting

$689,743
$413,410
$687,386
$468,394
$360,779
$646,881
$-
$100,000
$200,000
$300,000
$400,000
$500,000
$600,000
$700,000
$800,000
EMS ED IP
Pre-RAP
Post-RAP
Tadros A et al. 2010 APHA Annual meeting

Hospital
Home
Clinic
EMS

Hospital
Home
Clinic
EMS

EMS

In Camden New Jersey, 1% of patients account for a third of the city’s medical costs
Gawande A. “The Hot Spotters”. The New Yorker. January 24, 2011

Heidenreich PA. Circulation 2011;123:00-00
0
100
200
300
400
500
600
700
800
900
Indirect
Direct


EMS
Hospital Hospital
Hospital
Hospital
Hospital
Hospital
Hospital
Hospital
Hospital Hospital Hospital Hospital
Hospital
Hospital
Hospital
Hospital
Hospital
Hospital
1 million
patient records


Serra J. SDSU MPH thesis, 2011.

Serra J. SDSU MPH thesis, 2011.

Serra J. SDSU MPH thesis, 2011.




