jim laging, tips and trick for transition to home ...€¦ · hospital to home opportunities time...
TRANSCRIPT

7/10/2019
1
Tips and tricks for transitioning from hospital to home
Jim Laging RRT Philips Ventilation Solutions
Disclosure
I work for Philips Healthcare North AmericaThat’s how I can go on road trips!
Harvard Business ReviewOctober 2013
“In healthcare, the overarching goal for the providers, as well as for every other stakeholder, must be improving value for patients, where value is defined as the health outcomes achieved that matter to patients relative to the cost of achieving those outcomes.”
“Improving value requires either improving one or more outcomes without raising costs, or lowering costs without compromising outcomes, or both.
Failure to improve value means, well, failure.”
Learning objectives
• Overview of Non Invasive Ventilation (NIV)
• Discuss potential Uses of new modes for hospital and home use
• How can NIV help with your COPD needs
1 2
3 4

7/10/2019
2
Goals of NIV• Alleviate respiratory distress by
• Improving gas exchange
• Reducing work of breathing Decrease rapid shallow breathing
• Augmenting alveolar ventilation
• Achieve patient-to-ventilator synchrony
• Reverse atelectasis
• Minimize risks and avoid complications associated with endotracheal intubation
Clinical keys to success• Early intervention
• Consider NIV as the first mode of ventilator support
• The earlier the initiation, the higher the success rate
• Availability of equipment and staff
• Trained staff
• Appropriate interface
• High performance equipment
• Cardiopulmonary monitoring
Patient selection considerations• Strong evidence
• CHF
• COPD exacerbation
• Facilitating weaning of COPD
• Immunocompromised patients
• Moderately strong evidence
• Asthma
• Cystic fibrosis
• Postoperative RF
• Avoidance of extubation failure
• DNI patients
Strong = multiple controlled trials
Moderately strong = single controlled trial or multiple case series
Weaker = a few case series or case reports
Acute Applications of Noninvasive Positive Pressure Ventilation; T. Liesching, H. Kwok, N. Hill; Chest 2003;124:699-713
• Weaker evidence– Partial UAW – ARDS– Trauma
Interface selection• Estimate length of use
• Compatibility with device
• Safety features
• Facial features• Skin condition
• Facial abnormalities
5 6
7 8

7/10/2019
3
Failure to fit and apply the mask appropriately
• Even if the mask is not too tight, it must fit and be applied appropriately
• If the mask is uncomfortable or leaking Patients will become agitated and remove the mask
Or they may not settle down which leads to NIV failure
Selecting the appropriate size mask or a one size fits all mask may lead to increased patient comfort and acceptance
New Modes in NIV
• PCV (Hospital)
• C-Flex (Hospital / Home)
• AVAPS (Hospital)
• AVAPS-AE (Hospital / Home)
Difference between S/T and PCV modes• In PCV all breaths look the same, as machine determines I-time
• In S/T each breath is different, patient determines I-TimeP
cmH2O
20
0
. . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . .
PcmH2O
20
0
. . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . .
PCV on the V60 versus an ICU ventilator
• PCV on an ICU ventilator is PEEP compensated
• If PEEP is 5 cmH2O and set pressure is 15 cmH2Oo PIP is 20 cmH2O
• On the V60 as well as on all dedicated NIV ventilators, PEEP is not compensated
• If EPAP is 5 cmH20 and IPAP is 15 cmH20o PIP is 15 cmH2O
• Changes in EPAP without an equal change to IPAP
• Results in a change in pressure support (delta pressure)
9 10
11 12

7/10/2019
4
Patients who may benefit from using PCV
• Patients who may not be able to sustain a breath
• Neuromuscular disorders Muscular dystrophy, ALS
• Chronic disease processes Restrictive diseases
• Patients who are not tachypneic and are experiencing muscle fatigue, may VT by time at IPAP pressure
C-Flex
• The amount of pressure relief is determined by the C-Flex setting and the expiratory flow of the patient
• The higher the setting number (1, 2 or 3)
• And the greater the expiratory flow
• The greater the pressure relief o During the active part of exhalation only
C-Flex
Reduces pressure at the beginning of exhalation and returns to therapeutic pressure just before inhalation
Pressure relief varies on flow and C-Flex setting
C-Flex: Potential new indications
• Acute settings• Acute respiratory failure in OSAS• Acute respiratory failure in OHS
• Chronic settings• OSAS to improve tolerance and use
•Should not be used in patients requiring CPAP for oxygenation purposes
Just remember – it’s CPAP!
13 14
15 16
7/10/2019
5
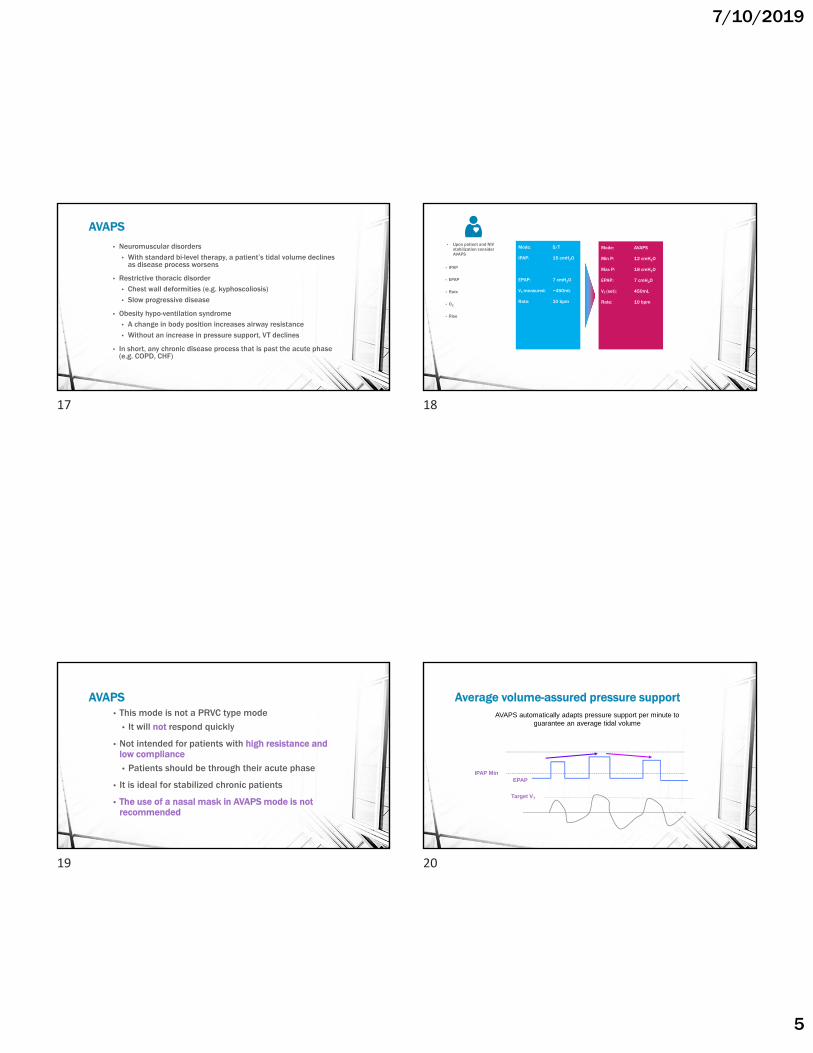
AVAPS
• Neuromuscular disorders• With standard bi-level therapy, a patient’s tidal volume declines
as disease process worsens
• Restrictive thoracic disorder• Chest wall deformities (e.g. kyphoscoliosis) • Slow progressive disease
• Obesity hypo-ventilation syndrome• A change in body position increases airway resistance• Without an increase in pressure support, VT declines
• In short, any chronic disease process that is past the acute phase (e.g. COPD, CHF)
• Upon patient and NIV stabilization consider AVAPS
• IPAP
• EPAP
• Rate
• O2
• Rise
Mode: S/T
IPAP: 15 cmH2O
EPAP: 7 cmH2O
VT measured: ~450mL
Rate: 10 bpm
Mode: AVAPS
Min P: 12 cmH2O
Max P: 18 cmH2O
EPAP: 7 cmH2O
VT (set): 450mL
Rate: 10 bpm
AVAPS• This mode is not a PRVC type mode
• It will not respond quickly
• Not intended for patients with high resistance and low compliance
• Patients should be through their acute phase
• It is ideal for stabilized chronic patients
• The use of a nasal mask in AVAPS mode is not recommended
Average volume-assured pressure supportAVAPS automatically adapts pressure support per minute to
guarantee an average tidal volume
IPAP MinEPAP
Target VT
17 18
19 20

7/10/2019
6
AVAPS= so far promising results in obesity-hypoventilation in STABLE patients
Benefits of AVAPS in ICU
Benefits of AVAPS in ICU
Clinical
• Lowest pressure support to achieve target volume
• Less sedation1
• Improves gas exchange1,2,3
• Small changes to PaCO2 lead to significant
outcomes
• Improves patient comfort and compliance1
• Improved Health-Related Quality of Life (HRQL)3
• Improved sleep quality3
AVAPS for the COPD patient during sleepSupplemental Oxygen Needs During Sleep. Who Benefits? Robert L. Owens, MDRespir Care 2013;58(1):32-44.
• With lung disease, changes in ventilation lead to Nocturnal Oxygen Desaturation.
• Up to 70% of COPD patients with awake oxygen saturation of 90-95% experience substantial desaturation at night, particularly during REM sleep.
• In those with severe COPD, the desaturation during sleep is more profound even than during exercise.
• Alveolar hypoventilation likely accounts for most of the oxygen desaturation.
Clinical Benefits of Bi-Level with Volume Assured
• Maintains ventilatory support and tidal volume during
• progressive ventilatory changes of the patient
• positional changes during sleep
• Alarms to indicate that tidal volume is not being maintained
21 22
23 24

7/10/2019
7
AVAPS-AE
AVAPS-AE is a auto-titration mode of noninvasive ventilation designed to better treat respiratory insufficiency patients (OHS, COPD and NMD) in the hospital and homecare environments
• Proven performance of AVAPS
– Maintains targeted tidal volume
• Auto EPAP
– Maintains patent upper airway at comfortable pressure
• Auto backup rate
– Applies an auto backup rate near a patient’s resting rate
25
AVAPS: proven effective • Automatically titrates pressure support
• Changes in body position
• Sleep stage
• Changes in respiratory mechanics
• Delivers average tidal volume
• Within the night
• Long-term progression
• AVAPS produces results comparable to sleep lab titration of PS1
• CO2 reduction
• Health-related quality of life
• Sleep quality
26
1Murphy, PBThorax thoraxjnl-2011-201081: Published Online First: 1 March 2012 doi:10.1136/thoraxjnl-2011-201081
EPAP
Target Vt
IPAPPS min
PS max
AVAPS-AEMaintaining tidal volume and airway patency
EPAP min
EPAP max
Resistance
27
AVAPS-AE suggested settings
OHS* COPD – OSA*Vt Target 6 -8 ml/Kg of ideal
bodyweight6-8 ml/Kg of ideal
bodyweight
Max P 35 cmH2O 30 cmH20
PS Max 19- 35 cmH2O 30 cmH2O
PS Min 14 -19 cmH2O 12 cmH2O
EPAP Max 14 cmH20 14 cm H2O
EPAP Min 4 cmH2O 4 cm H2O
Breath Rate Auto Auto
AVAPS Rate 2 5
28
25 26
27 28

7/10/2019
8
AVAPS-AE Settings
Settings Range Trilogy v 13.0
Rate From 1.0 AVAPS to 5.0 cmH2)/min in 1.0 cmH2O increments
Tidal volume 50 – 2000ml
Maximum pressure 6 – 50 cmH20
Pressure support Max 2 – 40 cmH20
Pressure support Min 2 – 40 cmH20
EPAP Max pressure 0/4 – 25 cmH20
EPAP Min pressure 0/4 – 25 cmH20
Breath rate Auto/0 – 60BPM
AVAPS-AE suggested settingsOHS* COPD – OSA*
Vt Target 8 -10 ml/Kg of ideal bodyweight
6-8 ml/Kg of ideal bodyweight
Max P 35 cmH2O 30 cmH20
PS Max 19- 31 cmH2O 26 cmH2O
PS Min 14 -19 cmH2O 12 cmH2O
EPAP Max 14 cmH20 14 cm H2O
EPAP Min 4 cmH2O 4 cm H2O
Breath Rate Auto Auto
AVAPS Rate 5
* AVAPS-AE protocol Dr. N. Hart, Dr. P. Murphy, Lane Fox Respiratory unit, St. Thomas’ Hospital London UK* AVAPS-AE Multi Center Trial protocol l,Prof Jean François MUIR, France
Proven to reduce readmissions
*All receiving NIV and meeting program eligibility requirements. All subjects were admitted at least twice in the prior 12 months before enrollment.1. Coughlin S., Liang WE, Parthasarathy S. RetrospectiveAssessment of Home Ventilation to Reduce Rehospitalization in Chronic Obstructive Pulmonary Disease. J Clin Sleep Med. 2015 Jun 15;11(6):663-70.
88% reductionIn a review of 398 COPD patients*
in hospitalreadmissions1
Managing COPD patients is a major issue
SOURCE: American Lung Association.
Growing COPD population Changing COPD reimbursement
Medicare has recently made readmissions a major performance
indicator needed for full reimbursement
12 millionMore than
Americans diagnosed
24 millionUp to
May be undiagnosed
29 30
31 32

7/10/2019
9
COPD is now part of Medicare’s Hospital Readmissions Reduction Program• Chronic obstructive pulmonary disease (COPD) ranks 4th among the most
costly hospital readmissions, with the rate of readmission for Medicare beneficiaries at 23% within 30 days post-discharge.
• Medicare beneficiaries with two or more chronic conditions, including COPD and asthma, accounted for almost 98% of all hospital readmissions in 2010 at a cost of $300 billion, according to an analysis of Medicare claims data.
• Effective October 1, 2014, COPD was added to Medicare’s Hospital Readmissions Reduction program and hospitals will face a 3% payment penalty if they are not able to reduce the rate of excess readmissions.
• www.aarc.org
Preventable COPD readmissions remain high
1. Jencks et al. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418-28.
Of 1 million COPDadmissions for acute exacerbation in 2012
23%were readmitted to the
hospital within
And your institution may be financially responsible
SOURCES: http://khn.org/news/half-of-nations-hospitals-fail-again-to-escape-medicares-readmission-penalties/ and http://kff.org/medicare/issue-brief/aiming-for-fewer-hospital-u-turns-the-medicare-hospital-readmission-reduction-program/.
2592In 2016, Medicare fined a record
number of hospitalsnationwide
77 of hospitals were penalized
%
Hospital to Home OpportunitiesTime For Disease Management
• COPD was predicted to be #3 cause of death by 2020
• It reached this milestone in April 2011 according to CDC
• Population >65 will increase 73% by 2025• Baby Boomers are over 80 million strong.
• PCP shortages of 20-27% by 2025.• Allergists, PCP, anesthesiologists.
• There are over 100 Million patients in the US classified as having chronic conditions
Kallstrom, T. “The Long Term Implications of the Affordable Care Act”. AARC Times, Oct 2012. pg 20-21
33 34
35 36
7/10/2019
10
Pulmonary Issues Aren’t Going Away!Respiratory have Opportunities
RT as a Physician Extender• Work in PCP office assessing patients
RT as Case Managers and RT Navigators• Teach self management• Modify patients behavior at home• Coach, encourage and give advice• Regular communication between patient and RT• Identify unmet health needs• Keeps patients:
• Out of Hospital
• Out of ED
• Out of Physician office
RT case managers are the lifeline for COPD Management
Home Health
Rehab
Long Term Care
Durable Medical
Equipment
Improved Care in Hospital
Treat Exacerbation
Address Root Causes:-medication skills-smoking cessation-other
CARE PROTOCOL
ImprovedPatientEducation
HOSPITAL
COMMUNITY CARE
Rea
dmis
sio
n
Admission
Discharge
MD TreatmentWhen/IfOffice Visit Occurs
Identify asCOPD Patient
ER Used As Solution to Problems
Transition
• Third visit to the Emergency Room in 2 months complaining of increasing shortness of breath
• This visit reveals extreme dyspnea, hypercarbia, and hypoxemia via ABG
Familiar patient
37 38
39 40
7/10/2019
11
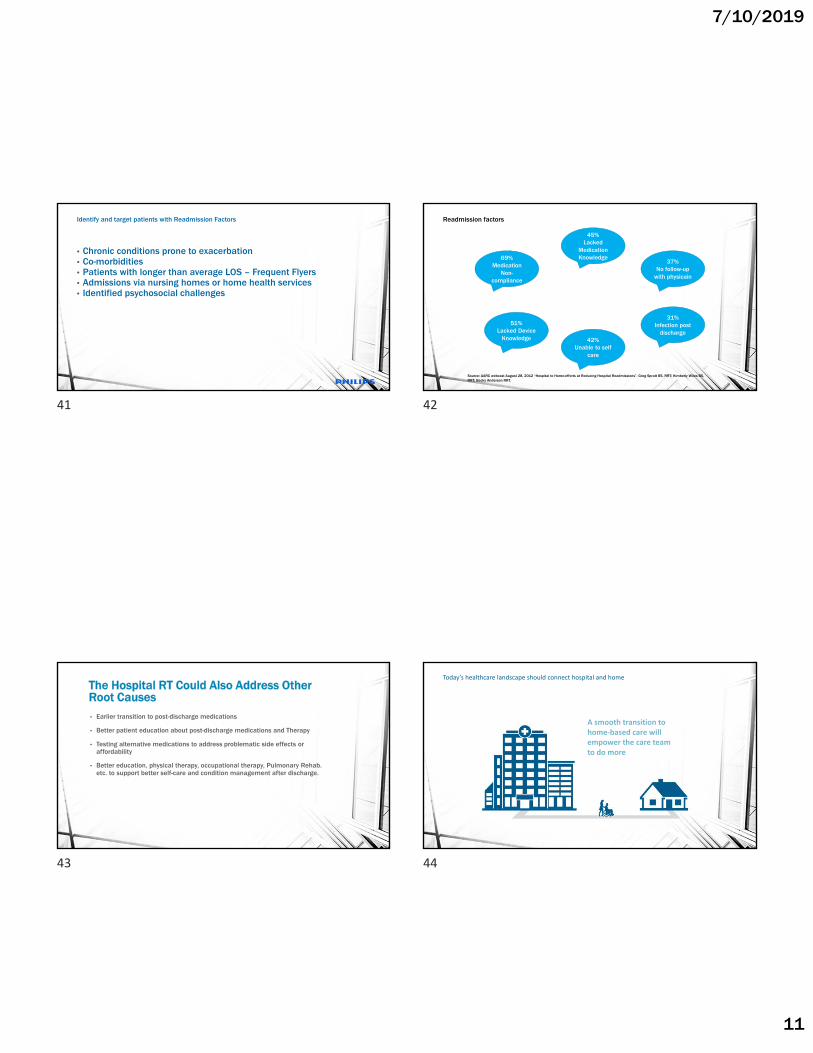
Identify and target patients with Readmission Factors
• Chronic conditions prone to exacerbation• Co-morbidities• Patients with longer than average LOS – Frequent Flyers• Admissions via nursing homes or home health services• Identified psychosocial challenges
Readmission factors
Source: AARC webcast August 28, 2012 “Hospital to Home-efforts at Reducing Hospital Readmissions”. Greg Spratt BS, RRT; Kimberly Wiles BS, RRT; Becky Anderson RRT.
69%Medication
Non-compliance
51%Lacked Device
Knowledge
45%Lacked
Medication Knowledge
42%Unable to self
care
37%No follow-up
with physicain
31%Infection post
discharge
The Hospital RT Could Also Address Other Root Causes• Earlier transition to post-discharge medications
• Better patient education about post-discharge medications and Therapy
• Testing alternative medications to address problematic side effects or affordability
• Better education, physical therapy, occupational therapy, Pulmonary Rehab. etc. to support better self-care and condition management after discharge.
Today’s healthcare landscape should connect hospital and home
A smooth transition tohome‐based care will empower the care team to do more
41 42
43 44

7/10/2019
12
Comprehensive solution
Durable Medical Equipment
-5365
-365
0 1530
Long Term Care
Home Health
Rehab
Long Term Care
RT Navigator/COPD Case
Manager
Systematic approach for COPD management
RT’s can take the lead with COPD Patients hospital to home transition. Education is KEY Effective COPD Management Plans
Ultimate Goals
Prevent and treat exacerbations
Prevent and treat complications
Moderate mortality
Overall Goals
Ultimate Goals
Stable COPD Patient
Overall Goals
Inhibit disease progression
Alleviate symptoms
Increase exercise tolerance
Improve health status
45 46
47 48

7/10/2019
13
Leading the way to a healthy society
Our role
Failed Approach
ED - ICU General ward Home Repeat
Noninvasive ventilation…
A safe effective way to successfully ventilate or oxygenate and manage
many patients and decrease readmissions
[email protected] 773-573-9155
A1A2
49 50
51
Slide 51
A1 Author, 7/5/2019
A2 Author, 7/5/2019