jiun/adjunctive medical knowledge the complementary
TRANSCRIPT
Too often a single noninvasive imaging techniquefails to provide enough information to permit a diagnosis to be made, whereas a judicious combination
of two or more techniques will frequently provideenough data to obviate the need for such invasiveprocedures as angiography or exploratory laparotomy. In this article we shall endeavor to correlatethe use of nuclear medicine techniques with sonography in several organ systems. In most instances webelieve that nuclear medicine and ultrasound shouldplay complementary roles, although one or the othermay be uniquely suited to the diagnosis of someconditions. We will attempt to put these noninvasiveprocedures in perspective and develop a guide totheir most efficient utilization. Certain conditions arebest diagnosed by sonography, such as obstetricproblems and abdominal aneurysms. Since ultrasound cannot pass through gas or bone, pulmonaryand bone lesions must be investigated by nuclearmedicine or radiologic techniques. Most organs inthe abdomen, thyroid, and breast can be examinedadvantageously with both nuclear medicine andultrasound. We will consider only those conditionswherein both these techniques can be used with mutual benefit, and not those where one or the otherhas little or no role. This communication will beconcerned with an assessment of how the two modalities should be used together for best patient management in these areas.
KIDNEY
Genitourinary diagnosis involves several problemsin which ultrasound and nuclear medicine play important complementary roles. Kidneys not visualizedadequately on excretory urography (IVP) in thepresence of renal failure should be studied next withultrasound to exclude bilateral hydronephrosis orpolycystic kidneys (Fig. I ) (1 ). In both conditions
the kidneys will be enlarged and numerous cysticareas will be present. Differentiation between thetwo conditions is usually simple: the cysts in a polycystic kidney vary markedly in size and in thesmoothness of the wall, whereas several characteristic ultrasonic configurations may be seen in hydronephrosis when it is severe (2). Multiple cystic structures of similar size radiating from the center of thekidney occur if the bulk of the pressure changes havebeen borne by the calyces, or, if the pelvis is mostaffected, a large cystic “sac-like―area surrounded bya small rim of renal parenchyma will be seen. Athird configuration occurs in hydronephrosis due toobstruction of the ureteropelvic junction : both theextrarenal and intrarenal pelves dilate, causing twoadjacent cystic areas with a “dumbbell―shape.
Although ultrasound is sufficiently reliable for thediagnosis of hydronephrosis (1 ), only anatomic
changes are shown, and the degree of renal functioncannot be assessed. If some renal function persists,nuclear techniques are helpful in three ways:
1. A e9mTc-DTPA scan allows one to detectthe level of the obstruction. Only severelydilated ureters can be visualized with ultrasound.
2. A 9OmTc..DMSAscan delineates the amountof functioning parenchyma in each kidney(3) and permits the surgeon to decidewhether a drainage procedure is indicated.
3. A sonographicdiagnosisof polycystickidney can be supported if numerous areas ofdecreased uptake are seen within the renal
outline (3) (Fig. 1).
Received Aug. 18, 1976; original accepted Sept. 21, 1976.For reprintscontact: Roger C. Sanders, Dept. of Radiol
ogy, Johns Hopkins Medical Institutions, 601 N. Broadway,Baltimore, MD 21205.
Volume 18, Number 3 205
jIUn/ADJUNCTIVE MEDICAL KNOWLEDGE
The Complementary Use of B—Scan Ultrasound and
Radlonuclide Imaging Techniques
AngelitaDingcongSandersandRogerC.Sanders
Johns Hopkins Medical Institutions, Baltimore, Maryland
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from
SANDERS AND SANDERS
4
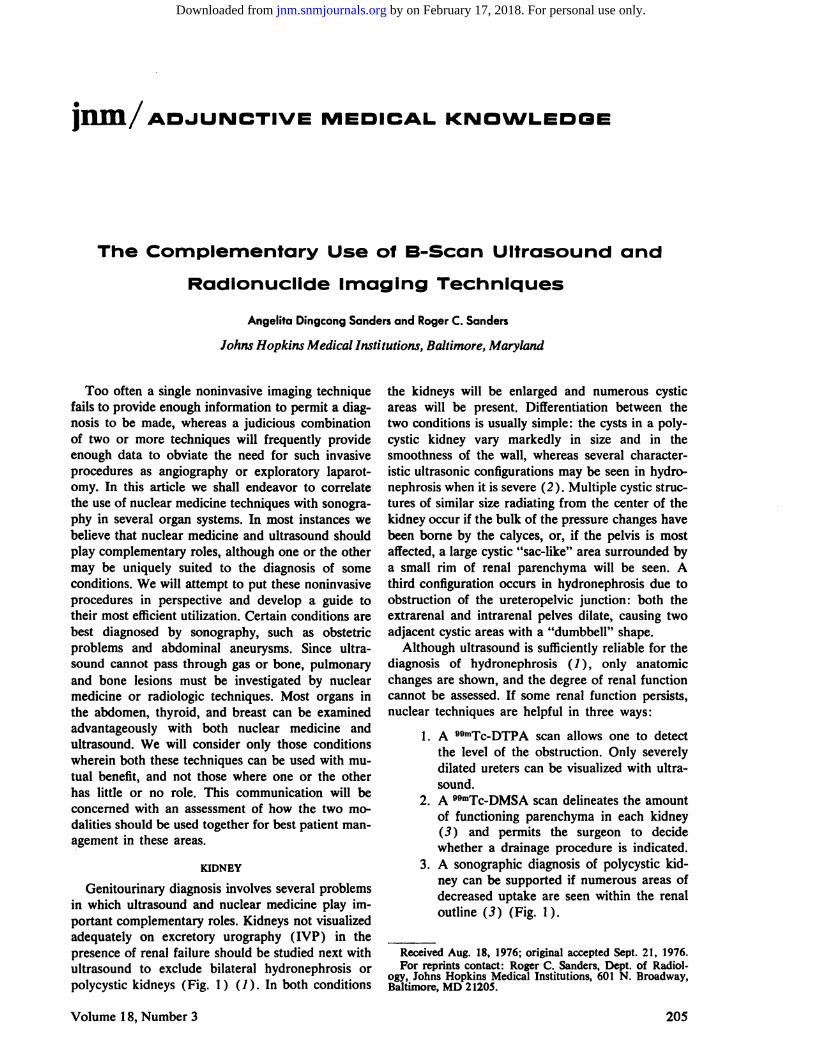
FIG. 1. Polycystickidney.(Top)Transversepronesection,5 cmabov iliac crest, showstypical sonographic changes of polycystickidneys. Both kidneysare markedly enlarged with multiple cysts(C)of varying sizes. Pelvicalyceal echoes (P), although disorganized, arestill recognizable. Sound.obsorbingstructure between two kidneys
(S) is vertebral column. Arrows indicate septa. (Bottom) Right pos.tenor oblique and left posterior oblique views of @Tc-DM$Ascan on same patient showstypical appearance of polycystickid.neys: distortion of renal outline with multiple defects correspond.in9 to cystsseenon sonogram.
Renal failure due to vascular disorders (e.g.,thrombosis) may be diagnosed if the kidneys arefound to be small or normal in size by ultrasoundand if there is no perfusion to the renal bed by aø9mTcO4flow study. In acute renal failure, the degreeof ‘311-Hippuranconcentration in the kidneys maybe of diagnostic significance regarding eventual renalfunction (4) . In end-stage renal failure, where ultrasound has shown small but otherwise normal kidneys, there is as yet no means of distinguishing amongthe many causes, such as chronic pyelonephritis,chronic glomerulonephritis, or renal artery stenosis,since all will show diminished flow on the 9omTc@DTPA flow study. End-stage kidneys retain someperfusion but show equally poor function.
In the absence of renal failure, a single kidneyfailing to visualize on excretory urography shouldfirst be studied with ultrasound, since hydronephrosis can be diagnosed easily and a number of theother possible causes have typical appearances (5).In addition, ultrasound provides information aboutneighboring organs which may not be available witha 99mTc-DTPA scan (Fig. 2). The sonographic appearance of multicystic kidney is that of a cysticmass with multiple cysts of varying sizes within it(6). Sincetherenalarteryisatretic,a 9DmTc@DTPAflow study will show no perfusion on the affectedside. If a neoplastic mass occupies the whole kidney,the sonogram will show distortion of the renal outline and central pelvic echoes and, in general, extraechoes within the renal parenchyma. A recent unilateral renal infarct causes little change in the sono
graphic appearance of the kidney, but a oomTc@DTPAflow study will show absence of perfusion to theaffected kidney (Fig. 2). A small end-stage kidneyis usually detectable by ultrasound if the kidney is
not too small (below approximately 3 cm) . A 9omTc@DTPA flow study will show a very little or absentperfusion to the affected side. If none of these mdications is seen, a sonographic search should be made
for an ectopic kidney in the pelvis. Should none befound, perhaps because of overlying bowel gas, aODmTc-DTPA scan with flow study, done in the antenor projection using a diverging collimator, willshow both renal beds and the pelvis, where an cctopic kidney might be.
In the absence of hematuria, demonstration orsuspicion of a renal mass on an 1W should lead toan ultrasonic examination to determine whether themass is cystic or solid (7) . Cystic lesions show largeposterior-wall echoes, smooth walls, and no internalechoes. Solid lesions, although they usually containnumerous echoes, may also be more or less echofree; however, their posterior-wall echo is smallbecause sound has been absorbed. An attenuatedposterior-wall echo has been found to correlate withsolid avascular neoplasms (8) , and the accuracy indistinguishing cysts from solid lesions has been reported as 95% (9). Solid lesions are due to neoplasms and arteriography is required to establish the
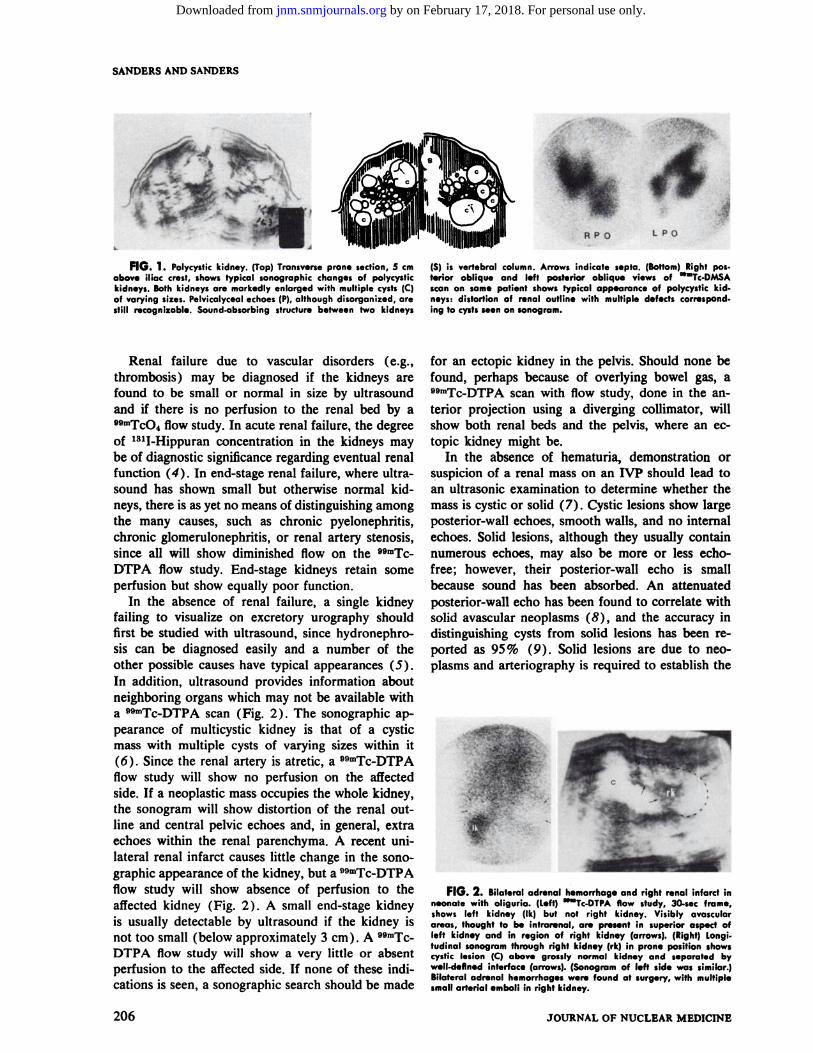
FIG.2. Bilateraladrenalhemorrhageandrightrenalinfarctinneonate with oliguria. (L.ft) “@Tc.DTPAflow study, 30.sec frame,shows left kidney (1k) but not right kidney. Visibly avascularareas, thought to be intrarenal, are present in superior aspect ofleft kidney and in region of right kidney (arrows). (Right) Longi.tudinal sonogram through right kidney (rk) in prone position showscystic lesion (C) above grossly normal kidney and separated byw.ll.deflned interface (arrows).(Sonogramof left side was similar.)Bilateral adrenal hemorrhages were found at surgery, with multiplesmallarterial emboli in right kidney.
206 JOURNAL OF NUCLEAR MEDICINE
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

ADJUNCTIVE MEDICAL KNOWLEDGE
pattern of vascular supply and the presence or absence of inferior vena caval involvement. The lowerlimits of consistent visualization of cysts using grayscale equipment is about 1.5 cm, although 1-cmcysts may sometimes be seen. Solid lesions less than2 cm in diameter may not be shown by ultrasoundbut may be detected by a renal image taken with°9mTcDM5A(dimercaptosuccinicacid), especiallyif the lesion is peripherally located. The o9mTc@DMSA accumulatesin the proximaland distal convoluted tubular cells and thus normally outlines theextent of the renal cortex (10) ; consequently, masslesions in the cortex will be visualized. Small lesionsdeeper in the kidney and close to the pelvicalycealsystem may not be detected with a DMSA scan (3).Ultrasound is probably more sensitive in detectingdeep lesions, particularly if they distort the pelvicechoes. Occasionally a suspected intrarenal mass isdue to a hypertrophied column of Bertin. Sonography and radionuclide imaging will show the presenceof cortical tissue instead of the decreased activitythat would accompany a true mass (11).
A lesion at the upperpole of the left kidneymaybe difficult to detect by ultrasound because of overlying ribs and lung. Should the NP indicate a massin this area and if the sonogram is negative, a @mTc@DMSA scan is helpful.The upperpole of the rightkidney does not pose the same problem for sonography because it can be examined with the patientsupine, with the liver providing a transonic path.
Locating the kidney for percutaneous biopsy isbest done with ultrasound (12). It gives an accurateguide as to the depth and direction to which theneedle should be introduced and can show the location of the kidney even in the presence of severeuremia.
Monitoring renal transplants is another area whereradionuclides and ultrasound play complementaryroles. Radioactive fibrinogen and @mTc@sulfurcolbid have been reported to accumulate in a graftundergoing rejection (13,14), but both need furtherevaluation. Also, a9mTc_sulfur colloid was seen toconcentrate in acute tubular necrosis. Perfusion andfunction in the allograft have been assessed using1311-Hippuran, with or without imaging (15—18). Amore recent method, which provides an indicationof the overall status of the transplant, is the 99mTc_DTPA flowstudy (15). Interpretationwiththis procedure, however, is made more difficult by the lackof a normal side for comparison. Moreover, manyof the problems that can arise produce very similarclinical pictures, so that at times only subtle differences in the 9@Tc-DTPA study are seen. Since onlyone kidney is visualized, the degree of perfusion isassessed by using the aorta for comparison. A base
FIG.3. Lymphoc.le.(Left) @Tc-DTPAscanshowslargeavascular area (arrows) above transplant (1). (Right) Transvsrse sono.graphic ssction through renal transplant shows irregularly shapedcysticlesion(C)with septumin its lower aspect(arrow).
line study for perfusion and function should be ohtamed within 24 hr of renal transplantation to assessacute tubular necrosis. This also provides a convenient comparison with future studies so that acuterejection or other complications can be detectedearly (15). Acute tubular necrosis (ATh) is characterized on the scan by good perfusion and disproportionately poor function, with gradual improvement of function over a period of time, depending onits severity. The prognosis appears to be related tothe duration of ischemia during transplantation (18).Any subsequentdecreaseof perfusionand concomitant loss of function, compared with the initial study,should indicate a high probability of acute rejection,but arterial stenosis or renal-vein thrombosis andobstruction must be excluded. The graft can be measured sonographically to look for the increase in sizethat occurs in acute rejection, but the problem ofobtaining ultrasonic scans at exactly the same levelon serial examination makes it a difficult procedureto perform accurately (20). Another sonographiccriterion for the diagnosis of rejection is a decreasein the amplitude of the pelvicalyceal echoes, but thisfinding too is difficult to quantify on serial examinations by the currently available methods, and it couldbe produced artifactually by differences in timecompensated gain and output settings. Failure ofthe patient to improve with therapy for rejectionshould raise the possibility of arterial stenosis; angiography is then necessary to make the diagnosis.
Both °°@‘Tc-DTPAimaging and ultrasound candiagnose obstruction, but with at least fair functionof the transplant the radionuclide study shows thelevel of obstruction more reliably. If transplant function is poor, however, the ultrasonic study is bettersince it depends on anatomic rather than functionalchange. Delayed images, obtained 1—2hr after tracerinjection, may be used to exclude obstruction if activity is seen in the bladder but not in the ureter and
Volume 18, Number 3 207
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from
SANDERS AND SANDERS
@@2: ..
@- :4
r •@3amiri
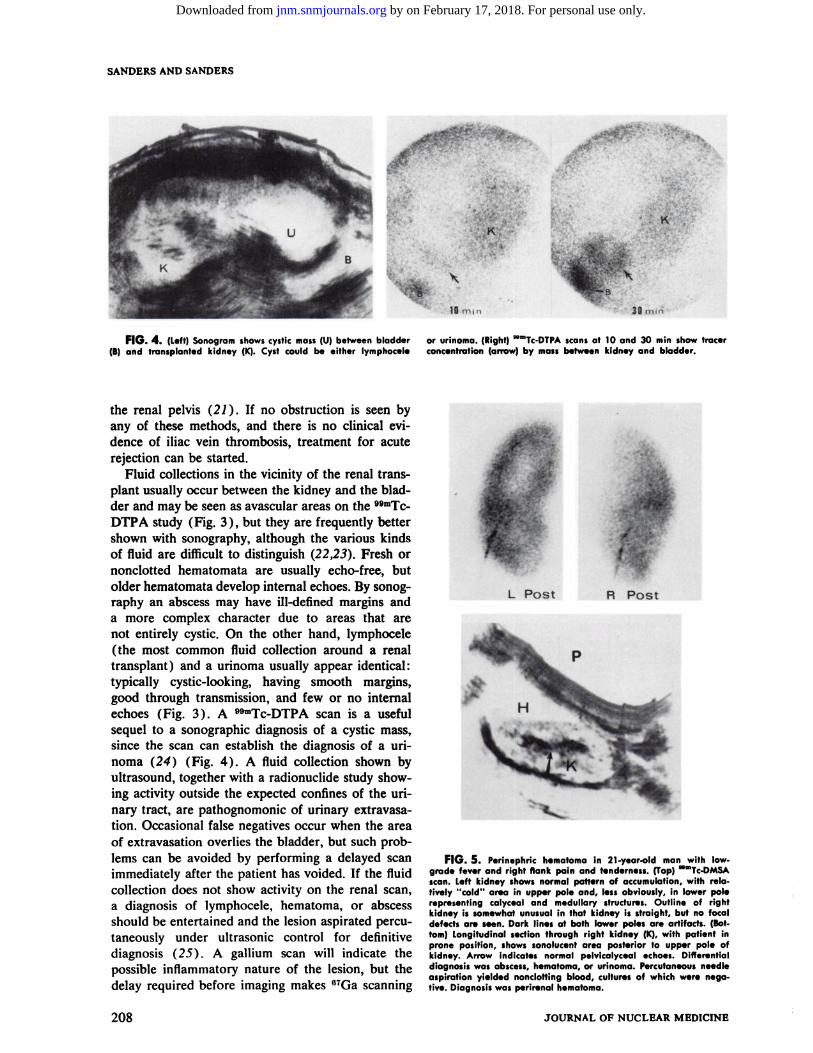
or urinoma. (Right) @mTc-DTPAscansat 10 and 30 mm show tracerconcentration (arrow) by mass between kidney and bladder.
FIG.5. Perinephrichematomain [email protected] fever and right flank pain and tenderness.(lop) mmTc.DMSAscan. Left kidney showsnormal pattern of accumulation,with rela.fively “cold―area in upper pole and, lessobviously,in lower polerepresenting calyceal and medullary structures. Outline of rightkidney is somewhat unusual in that kidney is straight, but no focaldefects are seen. Dark lines at both lower poles are artifacts. (Bot.tom) Longitudinal section through right kidney (K), with patient inprone position, shows sonolucent area posterior to upper pole ofkidney. Arrow indicates normal pelvicalyceal echoes. Differentialdiagnosiswas abscess,hematoma,or urinoma. Percutaneousneedleaspiration yielded nonclotting blood, cultures of which were negative. Diagnosis was perirenal hematoma.
FIG.4. (Left)sonogramshowscysticmass(U)betweenbladder(B) and transplanted kidney (K). Cyst could be either lymphocel.
the renal pelvis (21 ) . If no obstruction is seen byany of these methods, and there is no clinical cvidence of iliac vein thrombosis, treatment for acuterejection can be started.
Fluid collections in the vicinity of the renal transplant usually occur between the kidney and the bladder and may be seen as avascular areas on the v9mTc_DTPA study (Fig. 3), but they arefrequentlybettershown with sonography, although the various kindsof fluid are difficult to distinguish (22,23). Fresh ornonclotted hematomata are usually echo-free, butolder hematomata develop internal echoes. By sonography an abscess may have ill-defined margins anda more complex character due to areas that arenot entirely cystic. On the other hand, lymphocele(the most common fluid collection around a renaltransplant) and a urinoma usually appear identical:typically cystic-looking, having smooth margins,good through transmission, and few or no internalechoes (Fig. 3). A 9°―Tc-DTPAscan is a usefulsequel to a sonographic diagnosis of a cystic mass,since the scan can establish the diagnosis of a un
noma (24) (Fig. 4). A fluid collection shown byultrasound, together with a radionuclide study showing activity outside the expected confines of the unnary tract, are pathognomonic of urinary extravasation. Occasional false negatives occur when the areaof extravasation overlies the bladder, but such problems can be avoided by performing a delayed scanimmediately after the patient has voided. If the fluidcollection does not show activity on the renal scan,a diagnosis of lymphocele, hematoma, or abscessshould be entertained and the lesion aspirated percutaneously under ultrasonic control for definitivediagnosis (25) . A gallium scan will indicate thepossible inflammatory nature of the lesion, but the
delay required before imaging makes 6TGa scanning
L Post A Post
p
208 JOURNAL OF NUCLEAR MEDICINE
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from
ADJUNCTIVE MEDICAL KNOWLEDGE
nation is to Sort out the anatomic relationships of themass and show that it is separate from the kidney(Fig. 6) . At times it is impossible to decide whethera large mass is primarily intrarenal on is extrarenaland invading the kidney, but once a renal origin hasbeen excluded, the extent of the mass is determined.The ultrasonic scanning must be performed with thepatient both prone and supine: the prone scan shoulddefine the relationship of the mass to the kidneyswhile the supine scan explores its relationship to thegreat vessels and searches for a possible extensionacross the midline. Absorption by the vertebraemakes the supine position the one of choice for theevaluation of retroperitoneal nodes or retroperitonealfibrosis. Under sonographic examination, retroperi
r
20 sec
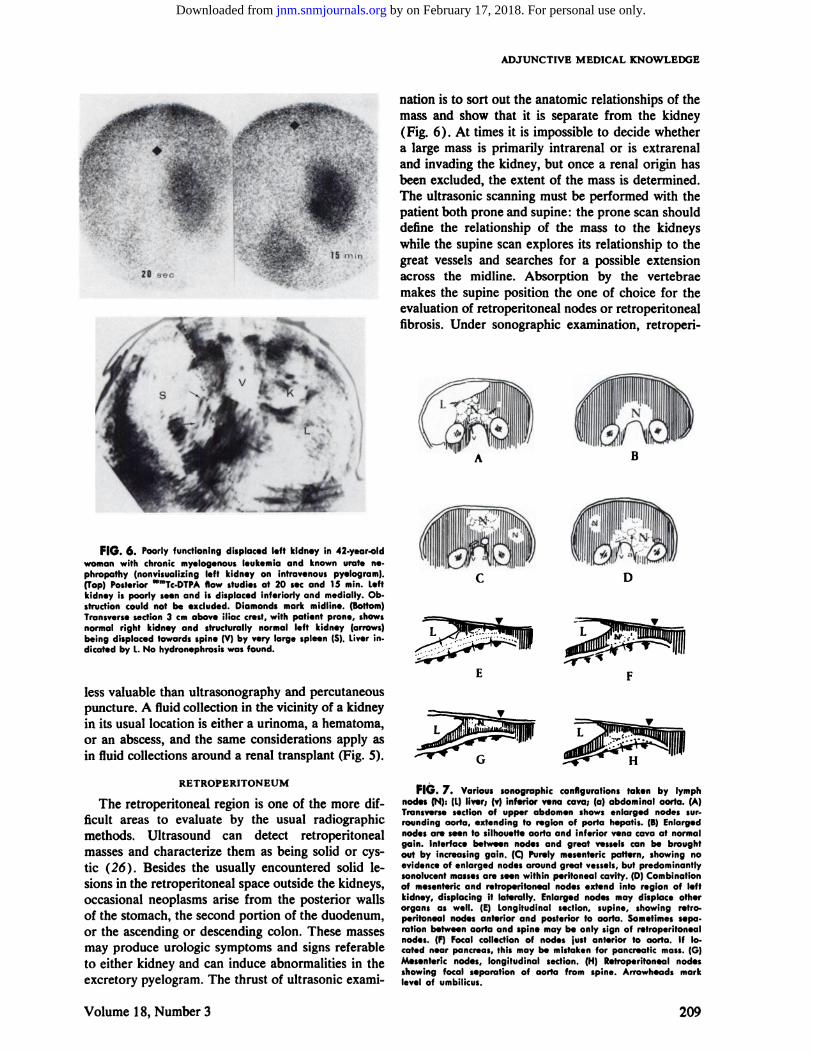
FIG.6. Poorlyfunctioningdisplacedleftkidneyin42.year.oldwoman with chronic myelog.nous leukemia and known urate nephropathy (nonvisualizing left kidney on intravenous pyelogram).(Top)PosteriormmTc.DTPAflow studiesat 20 secand 15 mm. Leftkidney is poorly seen and is displaced inferiorly and medially. Ob.structioncould not be excluded.Diamondsmark midline. (Bottom)Transversesection3 cm above iliac crest,with patient prone, showsnormal right kidney and structurally normal l.ft kidney (arrows)being displaced towards spine (V) by very large spleen (S). Liver in.dicated by L. No hydronephrosis was found.
less valuable than ultrasonography and percutaneouspuncture. A fluid collection in the vicinity of a kidney
in its usual location is either a urinoma, a hematoma,or an abscess, and the same considerations apply asin fluid collections around a renal transplant (Fig. 5).
C D
E F
RETROPERITONEUM
The retropenitoneal region is one of the more difficult areas to evaluate by the usual radiographicmethods. Ultrasound can detect retropenitonealmasses and characterize them as being solid or cystic (26). Besides the usually encountered solid lesions in the retropenitoneal space outside the kidneys,occasional neoplasms arise from the posterior wallsof the stomach, the second portion of the duodenum,or the ascending or descending colon. These massesmay produce urologic symptoms and signs referableto either kidney and can induce abnormalities in theexcretory pyelogram. The thrust of ultrasonic exami
FIG.7. Varioussonographicconfigurationstakenbylymphnodes (N): (L) liver; (v) inferior vena cava; (a) abdominal aorta. (A)Transverse section of upper abdomen shows enlarged nodes surroundingaorta, extending to region of porta hepatis.(B)Enlargednodesare seento silhouetteaorta and inferior venacavaat normalgain. Interface between nodes and great vesselscan be broughtout by increasing gain. (C) Purely mesenteric pattern, showing noevidence of enlarged nodes around great vessels, but predominantlysonolucentmassesare seen within peritoneal cavity. (D) Combinationof mesentericand retroperitoneal nodes extend into region of leftkidney, displacing it laterally. Enlarged nodes may displace otherorgans as well. (E) Longitudinal section, supine, showing retroperitoneal nodes anterior and posterior to aorta. Sometimes sepa.ration between aorta and spine may be only sign of retroperitonealnodes. (F) Focal collection of nodes just anterior to aorta. If located near pancreas,this may be mistakenfor pancreatic mass.(0)Mesenteric nodes, longitudinal section. (H) Retroperitoneal nodesshowing focal separation of aorta from spine. Arrowheads marklevel of umbilicus.
Volume 18, Number 3 209
!@•,@ @i.;*@
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

SANDERS AND SANDERS
ANT A LAT
FIG.8. Subcapsularliverhematomain 36-year.old woman with history of cho.lecystectomy1 year previously, with profuse bleeding at surgery. (lop) Liver scanwith @Tc.sulfurcolloid shows large coldarea (arrows) in superior posterior aspectof right hepatic lobe. (Bottom, left) Flowstudy using mmlc.sulfurcolloid showscolddefect (arrows) seen on static scans to beavascular. (Boftom, right) Transverse sec.tion 1 cm blow ziphisternum showslargecystic area (C) with irregular margins (arrows) in posterior superior aspect of righthepaticlobe, correspondingto focal defecton radionuclide scan. Large subcapsularhematomawas evacuated at surgery.
.,-@
R.Ant
@t@1@
toneal fibrosis presents a symmetric mantle-like relatively echo-free mass enguffing the great vessels, withsmooth margins and without lobulations (27) . Retropenitoneal nodes may appear similar but are morelikely to be asymmetric, lobulated, and to havemesenteric and intraperitoneal components. Enlargedabdominal nodes present several ultrasonic patterns;one simulates retroperitoneal fibrosis, and others areschematically shown in Fig. 7. When nodes “silhouette―the aorta and the margins of the aorta cannotbe delineated, the nodes may be confused with anabdominal aortic aneurysm; however, increasing thegain will cause low-level echoes to become visiblein the nodes and the aortic interface to become discernible (28). Ultrasound is less sensitive than lymphography in detecting lymph-node enlargement cxtending less than 3 cm along the external iliac orperiaortic lymph-node chains. Since nodes along theinternal iliac chain, within the mesentery, or aroundthe pancreas are in “blind―areas for conventionallymphography, ultrasound may be helpful.
In the evaluation of retroperitoneal masses, nuclear medicine is best used to assess possible renal,hepatic, or splenic involvement and to evaluate patients with known or suspected lymphoma (or metastasis) who might be saved a staging laparotomy ifliver and spleen involvement can be proven by a9OmTc..sulfuncolloid study. Moreover, in a patientwho is technically difficult to examine ultrasonicallydue to excessive obesity or the presence çfbowelgas, a gallium study may detect abnormal concentrations of activity in lymph nodes and organs (29).Some metastases from lymphomas accumulate galhum quite avidly, predominantly the histiocytic type
and Hodgkin's; lymphocytic lymphonia is less avid(30). Radionuclide lymphography with 198Au(31,32)has been reported to correlate well with biopsy findings in lymphomas and some metastases, but thetechnique needs further evaluation.
LWER
Radionuclide imaging with a labeled colloidalagent such as 9OmTc..sulfurcolloid should be the firstdiagnostic step in the evaluation of possible liverdisease, since information is obtained about both thestructure and the function of this organ. Since thespleen can always be imaged concurrently, the correlation of the two organs usually makes the scanmore specific than otherwise.
Diffuse disease of the liver, the condition mostfrequently encountered, often appears in the earlystages as hepatomegaly, with or without inhomogeneity of tracer uptake in the various parts of theliver. Gross hepatomegaly is easily detected but themilder degrees of liver enlargement are more difficultto judge. A subjective impression of hepatomegalycan be obtained when the usual sharp points in theliver outline assume a rounded contour, e.g., alongthe inferior margin, especially on the night side. Theliver volume can be estimated by constructing thebest elliptical shape around the liver in the anteriorand lateral projections, but this method requiresexperience because of the variability of liver shapesand contours (33—35). Sonographic determinationof liver volume has been proposed by Rasmussen(36), but his method does not appear to be any moreaccurate than the scintigraphic method. The spleenmay appear normal in early diffuse liver disease, but
210 JOURNAL OF NUCLEAR MEDICINE
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

ADJUNCTIVE MEDICAL KNOWLEDGE
as this progresses, the spleen will show increasinguptake of colloidal radiopharmaceuticals (37) aswell as a progressive increase in size. With stillgreater severity of the liven disease, the tracer willaccumulate in the bone marrow and eventually inthe lungs (38). The combination of hepatomegaly,inhomogeneous hepatic uptake of tracer, decreasedliver-to-spleen uptake ratio with or without splenomegaly, and bone-marrow activity is highly suggestive of cirrhosis, but it may also be seen in severefatty metamorphosis (39). One may also diagnosethe more florid examples of diffuse liver disease withsonography, but the modality is less sensitive thanthe 99mTc@sulfur colloid scan. Fatty infiltration andcirrhosis both give diffuse strong echoes throughoutthe liver (40). With cirrhosis and portal hypertension, however, the extrahepatic veins in the portalsystem are dilated, venous collaterals may be seen,and the spleen is usually enlarged (41).
Focal disease in the liver, such as primary or metastatic tumor, abscess, cyst, or hematoma, usuallyappears as a “cold―area on the colloid scan. “Hot―spots have been reported with superior vena cavaobstruction (42), portocaval shunts (43), hemangioma (44), hepatic-vein occlusive disease (45),and following misdirected central venous pressurecatheters (46). Dynamic imaging (flow study) willassist in differentiating lesions without Kupifer cellsbut with normal or even greater than normal vascularity (hepatoma, hemangioma, and a few metastases) from lesions that have no phagocytic cells andlittle or no vascularity (hematoma, cirrhotic pseudotumor, most metastases, cyst, and abscess) (47)(Fig. 8). Further information can be obtained byimaging with 67Ga citrate, which accumulates in mosthepatomas, inflammatory lesions, and lymphomasand in some metastatic neoplasms (48,49).
Although ultrasound can detect focal intrahepaticlesions down to 2 cm in size if done very systematically and thoroughly by a skilled operator (50), theinherent tediousness, the great variability of the technique, and the lower sensitivity in detecting diffusedisease (51 ) make it a much less satisfactoryscreening procedure than nadionuclide scintigraphy(52) . However, in patients with a strong clinicalsuspicion of focal liver disease, complementary studies will be beneficial (53,54). Nuclear medicine techniques are more sensitive in detecting lesions closeto the surface but may miss those deeper in theparenchyma (55), which ultrasound can demonstrate(Fig. 9). Gamma imaging may be less helpful indetecting lesions of the left lobe, which normally hasmuch less activity than the right lobe because of itsthinness (56) and which cannot be imaged satisfactorily from the posterior projection (Fig. 10). In the
R
ant r lat
FIG.9. Livermetastasisin65-year-oldwomanwithrightupperquadrant pain for previous 10 months and gastric mass seen on up.per 01 series. (Top) Transverse sonogram taken at level of xiphisternum shows relatively large anechoic area (arrows). (L) Normal liverparenchyma.This large lesionhascompletelysonolucentcenter(N)representingnecrotictumor; two smaller metastaticareas (M) of de.creasedechoescan be seen.(Bottom)Scantaken with “@Tc.sulfurcolloid of sameliver showslarge “cold―area (arrows)corresponding to large lesion in right hepatic lobe seen on sonogram.Smallerlesion in left lobe (arrowhead) was recognized only in retrospect.Lesion in caudate lobe seen on sonogram is not seen at all onradionuclidescan.At surgery,patient had leiomyosarcomaof stomach with metastases to liver.
diagnosis of liver disease, the major role of ultrasound should be that of determining whether a lesionfound by radionuclide imaging is solid or cystic (57),whether it is intrahepatic or perihepatic, and whetherthere is superimposed focal disease in those liverswith inhomogeneous patterns of activity.
Sonographically, the normal liver shows diffuselow-level echoes throughout, with occasional tubularstructures (branches of the portal or hepatic venoussystems) that can be traced to the inferior vena cavaor to the porta hepatis (40) . Focal lesions that havecharacteristics of a cyst (no internal echoes, strongposterior-wall echoes) are usually due to benign disease, either simple cyst, abscess, or hematoma. Thesecyst-like lesions may appear similar, with smooth mangins, but abscesses usually have some internal echoesdue to debris within the cavity and may be surroundedby a zone of decreased echoes, compared with the restof the liver, due to inflammation (Fig. I 1). Abscessescan be differentiated from cysts and hematomas bygallium imaging, which usually shows increased activity in the case of a pyogenic abscess but decreased
Volume 18, Number 3 211
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

SANDERSANDSANDERS
@1AN TERIOR
FIG. 10. Normalvariantliver.(Left)‘°mlc-sulfurcolloidscanofliver showing suspiciouslesion at junction between right and leftlobes of liver (arrows). (Right) Transverse sonogram 3 cm below
activity in an amebic abscess (58,59). Frequently, discrepancies are observed in abscess size as measuredby sonography and by imaging with either DamTc@sulfur colloid or 67Ga (Fig. 11) . The discrepancy isprobably due to the demonstration by ultrasound ofonly the fluid-filled cavity without the surroundingzone of inflammation, whereas this zone is usuallypart of the focal defect seen on o9mTc scan or thearea of abnormal accumulation of gallium. For thisreason, it is better to evaluate the adequacy of drainage from an intrahepatic abscess by sonography,since it is less likely to give a false-positive result ofresidual pus collection (60). The continuing decreased or absent activity of the reticuloendothelialcells and the increased uptake of gallium due to nesolving inflammation may be misinterpreted on thesulfur colloid and gallium scans (61 ) . Hematomasmay have irregular margins (Fig. 8) and may have
ant
xiphisternumshowssizable gap (arrow) between right (R) and leftlobes (L) of liver. No abnormality could be found. Inferior venacava (V) and aorta (A) are seen.
some internal echoes if clots are present; they mayalso differ in appearance depending on how recentlythe bleeding occurred. A recent hematoma may showa flat fluid interface that always stays parallel withthe table regardless of the patient's positioning. Thiseffect is probably due to the setthng of the solidelements in the blood to the lowest portion of thecavity. Unfortunately, this finding is not specificsince it has also been seen in abscesses. Chronichematomas may be entirely cystic, but they oftendevelop a number of echoes within their substance.
The sonographic appearance of solid lesions in theliver can range from (A) echo-free areas that canbe mistaken for cysts (but which have poor transmission and fill with echoes as the transducer's output is increased), to (B) areas with fewer echoesthan surrounding parenchyma, and (C) highly echogenic areas (62). Metastases most commonly show
.. @. ..@ -
ant
lesion is an area of decreased acousticdensity (arrowheads).Scanwas interpreted as showing intrahepatic abscesswith surroundingarea of decreased echoes representing inflammation. (Right) GalIium.67 scan of liver showsdiseased area seen on the @mTcscanand on sonographyto concentrategallium (A). Black line representscostal margin. Other less well-defined areas of abnormal galliumaccumulation are seen. Large hepotic abscess in right lobe nearnormal gallbladder was drained at surgery. Inflamed liver tissuecorrespondingto other gallium-avid areas could not be drained.
212 JOURNAL OF NUCLEAR MEDICINE
f .@.
FIG. 11. lntrahepaticabscessesin21-year-oldmanwithfever,leukocytosis,and right upper quadrant pain and tenderness.(Left) Anterior mmTcsulfur colloid scan of liver shows cold―area(arrows) in region of gallbladder fossa. Black line representscostalmargin. Whether this lesion was intrahepatic or not was uncertain.Smaller areas of decreased activity in left lobe (arrowheads)werenot originally appreciated. (Middle) Transversesectionshowsirregu.larly shaped cystic area (arrows) with multiple internal septationsin anterior aspect of right lobe of liver. Surrounding this cystic
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

ADJUNCTIVE MEDICAL KNOWLEDGE
areas of decreased echoes (Fig. 9) ; metastases fromadenocarcinoma are reported to form a bull's eyeappearance: an echogenic area surrounded by echofree rim (62). With a nadionuclide flow study,those metastases having greater vascularity than thesurrounding parenchyma may be confirmed. Mostmetastases, however, seem to be avascular (47).
Ultrasonic examination is very helpful in differentiating scan defects due to intrahepatic lesionsfrom those produced by disease in adjacent structuresand from defects due to unusual variations in theliver shape (Fig. 10) . The radionuclide defects mostdifficult to interpret are usually located (A) in theregion of the gallbladder fossa; (B) posteriorly in thevicinity of the kidney; (C) laterally where the ribsmay produce indentations; (D) superiorly where thehepatic veins emerge from the liver and where anenlarged heart may exert extrinsic pressure; (E) inthe region of the porta hepatis; (F) in the fossa ofthe inferior vena cava; or (G) in the areas where theliver is normally thin such as in the left lobe or dome(Fig. 10). Sonography can demonstrate (A) normal,but thin liver parenchyma; (B) a normal structureoccupying the supposed defect (such as a gallbladderor hepatic veins) ; (C) an intrahepatic lesion; (D)extrinsic pressure from abnormal adjacent structuressuch as polycystic or hydronephrotic kidneys or gallbladder empyema; and (E) extrinsic masses. Occasionally, the liver has unexpected dips and elongations along the periphery, particularly in patientswith cirrhosis or asymmetric hypertrophy of the liver.The sonogram is helpful in verifying that there are nomasses along the periphery and that the variationsare merely due to an irregular borden. In cirrhotic patients who may be suspected of superimposed hepatoma, sonography will frequently show the presenceor absence of a neoplasm within the liver. Galliumimaging can also be very helpful in these patientssince the vast majority of hepatomas concentrate thatradionuclide (49) . Similarly, patients with a focalhepatic defect due to previous irradiation can beinvestigated by ultrasound for possible recurrent tumon. An alternative approach is to use a radiopharmaceutical excreted by hepatocytes, such as 1311-rosebengal, since hepatocytes are less sensitive to irradiation than the neticuloendothelial cells. This methodis not foolproof, however, as hepatocytes can alsobe damaged by sufficient radiation. Comparing theshapes of the lesion as shown by the uamTc@sulfurcolloid scan and by the 131I-rose bengal scan can behelpful. If they have the same geometric shape, conforming to the radiation port, the lesion is muchmore likely due to irradiation rather than to neoplasm.
PANCREAS
Lesions of the pancreas are more accurately detected and characterized by sonography (63,64) thanby scintigraphy with T5Se-methionine. In one reportradionuclide imaging was 67% accurate in the detection of pancreatic neoplasms greater than 2 cmin size, compared with an accuracy of 84% withultrasound (65). Radionuclide pancreatography ishampered by the difficulties of separating the pancreas from the left lobe of the liver, the variabilityof pancreatic shape, the high percentage of falselypositive or negative scans (66,67), and the nonspecificity of an abnormal finding (68,69). Sonographically, the contour of the pancreas is irregularlyexpanded, and reduced echoes are seen in areas involved with neoplasm. Similar findings may also beseen, however, with focal chronic pancreatitis. Although the accuracy of sonography in diagnosingpancreatic carcinoma is no greater than that of pancreatic duct cannulation or angiography (65), thegreater patient acceptability of ultrasound and itslack of morbidity give it a distinct advantage as ascreening procedure. While some neoplasms in thepancreas may be seen, many of those responsible forjaundice are unfortunately less than 2 cm in diameter and are therefore unlikely to be visualized. Once
a pancreatic mass is detected by ultrasound, a definitive diagnosis may be obtained by percutaneousneedle biopsy of the mass under ultrasonic control(70) . Pancreatitis,if generalized,is readily diagnosable (Fig. 12), but, if focal, it may be confusedwith neoplasm. Since ultrasonic scanning may not beable to distinguish a mass near the pancreas from atrue pancreatic lesion, a normal radionuclide pan
creatognam can be helpful in confirming the extrapancreatic lesion.
Sonography is the procedure of choice for detecting and following pancreatic pseudocysts (71 ), andits diagnostic reliability is virtually 100% . Othertechniques, such as radionuclide pancreatic scansand upper GI series, can indicate that a mass is present, but the advantage of sonography is that it cancharacterize the lesion as cystic. Pancreatic pseudocysts may change size abruptly if they discharge
spontaneously into neighboring viscera. Such changescan be followed with sonography.
SPLEEN
Both radionuclide images and sonography definespleen size well (Fig. 12), but a small spleen maybe difficult to find with sonography. Detection ofpossible accessory spleen is best resolved with aspleen scan. As with the liver, the focal defects ohserved on radionuclide images can be characterized
Volume 18, Number 3 213
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

SANDERSANDSANDERS
newer agents as OamTc..HIDA, but a partially obstructed bile duct cannot be distinguished from apatent duct (77). Sonography is the procedure ofchoice to differentiate between jaundice due to hepatocellular disease or cholestasis and jaundice due toextrahepatic biliary obstruction. Abnormally largeintrahepatic biliary radicles can be seen if the ductsare sufficiently dilated (78) ; in practice, this impliesa bilirubin value of 6—8.A dilated common bile ductcan sometimes be traced, which provides a crude ideaof the level of obstruction (79). The undistended cornmon bile duct is not normally seen, but an enlargedone may be seen as a tubular structure coursingsomewhat@ obliquely anterior to the portal veinthroughout most of its course. Even with experience,the common bile duct may not be demonstrable fortechnical reasons such as obesity or overlying bowelgas. Ducts once dilated can remain chronically enlarged after the obstructive lesion is no longer present (77).
Several possible causes of obstruction may be identilled. In general, gallstones are readily seen withultrasound even when they are as small as 2 mm indiameter (80). Stones within the gallbladder produce discrete strong echoes in the dependent portionof the gallbladder, and they are frequently so soundattenuating that an acoustic “shadow―is cast behindthem (81 ). In contrast to calcification within thewall of the gallbladder, they fall to the most dependent portion of the gallbladder when the ultrasonicexamination is performed in the upright position.Small stones are difficult to differentiate from bilesludge.
Choledochal cyst, usually diagnosed in childhood(82), is a rare cause of jaundice and can be easilydetected with ultrasound (83). Pancreatic pseudocysts may also cause obstructive jaundice when theyare located in the head of the pancreas. Differentiation between choledochal cysts and pancreatic pseudocysts is best made using such hepatocyte-excretedradiopharmaceuticals as 1811-rose bengal (82). Overa period of hours this agent will concentrate in acholedochal cyst and not in a pancreatic pseudocyst.
If intrahepatic bile duct dilatation is not detectedby ultrasound and the bilirubin is markedly elevated,significant extrahepatic obstruction is unlikely. Investigation should then be pursued for diffuse liverdisease or multiple focal lesions that can cause intrahepatic obstruction and cholestasis. As mentioned inthe section on the liver, radionuclide procedures areto be preferred for this type of study.
Sonography is still valuable if the bilirubin is lowbut obstruction is suspected, because the outline ofa large gallbladder may suggest distention. Cholelithiasis or pancreatic neoplasm may be present, even
.. S@@ ‘;@r—.i I@'@ ,@.
A
4@ -
ANT
,. ,4_
FIG. 12. Splenic-veinthrombosissecondaryto pancreatitisin33-year-old alcoholic man admitted with left upper quadrant painand tendernessand palpable left upper quadrant mass.Liver function testswere abnormal. Serumamylase was normal. (Top) Anterior“@“Tc-sulfurcolloid scan showsnormal-sized liver with inhomogene.ous tracer uptake and markedly enlarged spleen without evidenceof increasedactivity. (Bottom)Transversesection4 cm below xiphi.sternum again shows markedly enlarged spleen (5) and diffuselyenlarged pancreas (p) containing fewer echoes than normal; thispattern is typical of pancreatitis. (a) Aorta; (V) inferior vena cava.Angiography showedsplenic-veinthrombosis.
by sonography as cystic or solid. Solid lesions aredue either to infarction or to metastatic disease,whereas cystic lesions are due to splenic cyst, abscesses, or hematomas. In subcapsular hematomathe spleen scan usually shows a filling defect orsplaying of the spleen outline, the so-called “doubledensity―sign ( 72 ) or “spleniccrowding―Sign (73).Combined liver—spleenand lung scanning may showseparation between the spleen and the lower lobeof the left lung, particularly if the injury is to theupper pole of the spleen. Experience with sonography for splenic trauma is less extensive, but if thefindings on a spleen scan are questionable, sonography may help in that it may show a cystic lesion(74,75). Both modalities may occasionally show theactual rent in the splenic tissue along its margin.
BILIARY SYSTEM
In clinical jaundice a9mTc_sulfurcolloid scans canshow dilated bile ducts, but only the grossest changesare detectable (76) . Dilated ducts can at times bemistaken for focal defects. Complete biliary obstruction can be diagnosed with 1311-rose bengal and such
214 JOURNAL OF NUCLEAR MEDICINE
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

ADJUNCTIVE MEDICAL KNOWLEDGE
though the ducts are too small to be visualized byultrasound.
Several complementary imaging techniques areavailable for the diagnosis of acute cholecystitis. Infusion cholangiogram (a procedure that usually requires tomography) will visualize the biliary tree butnot the gallbladder and cystic duct, a combinationthat nearly always indicates acute or chronic diseaseof the gallbladder. However, infusion cholangiography is time-consuming and carries a relatively highrisk of an allergic reaction to the contrast medium.Ultrasound may be helpful in the diagnosis of acute
R
cholecystitis. When the wall of the gallbladder isinflamed and edematous, irregularity and a doublecontour to the gallbladder may be seen; it is unclearhow often this finding occurs in acute cholecystitis.Inflammation-causing disease within the gallbladder,such as gallstones, will be detected.
Masses that arise from the gallbladder, such aspolyps and carcinoma, distort the wall and have thedifferent acoustic texture of neoplasia to distinguishthem from the liver parenchyma. Inability to visualize the gallbladder sonographically, in a patient with
a nonvisualizing gallbladder on reinforced oral cholecystogram, is strong evidence of a chronically diseased gallbladder.
Radionuclide techniques are useful in acute cholecystitis. Cystic duct obstruction can be excluded ifthe tracer accumulates in the gallbladder. Radiolabeled rose bengal has been the most used radiopharmaeutical for this purpose, but 9°―Tc-labeledhepatobiliary agents with much better imaging characteristics are now in development (84) . One ofthese, HIDA, has been reported useful even whenthe bilirubin is significantly elevated (77).
Empyema of the gallbladder is difficult to distinguish from acute cholecystitis by radiologic or radionuclide procedures, since neither the contrast medianor the radioactive agents will enter the gallbladder.Gallium-67 imaging, however, will show uptake inthe gallbladder area. Ultrasonic findings may besuggestive. When the common bile duct or cystic ductis obstructed and the gallbladder wall is producingpus, a “tense―configuration is adopted: the gallbladder is enlarged and the wall is rounded. To datewe have no good standards to tell us when a gallbladder, under ultrasonic examination, is too largeto be considered normal. If the gallbladder is fibrosedbefore the attack of acute cholecystitis or empyema,a smaller size may be abnormal. In empyema thesurrounding liver may well be affected by an inflammatory response and show an altered ultrasonic texture with decreased echoes.
P
ABSCESS DETECTION
A possible cause of fever is an intra-abdominalabscess, and there may be no signs pointing to aspecific region. Gallium-67 has a great affinity forinflammatory lesions and is the screening agent ofchoice (85,86). The major disadvantage of galliumimaging is the substantial delay following injectionbefore the study can be performed (87) ; occasionallyrepeat studies are necessary at 24, 48, and even 72hr. In cases where bowel cleansing cannot be used(e.g., in a patient who has inflammatory bowel disease or immediately following bowel surgery) , areasof gallium accumulation may be difficult to interpret,
FIG.13. Pyelonephritisin18-year.oldmanwithfeverandrightupper quadrant pain and tenderness. Subphrenic, intrahepatic, orperinephric abscesswas clinically suspected. (Top) Gallium.67 ci.trate scan shows abnormal gallium accumulation in right upperquadrant, seen best on posterior view. Without moving patient,repeat scanwas taken of same area with “ETc-sulfurcolloid. Abnormal gallium accumulation is below liver and in region of rightkidney. (Middle) @Tc-DMSAscan of kidneys done next day showsfocal defect in upper pole of right kidney. Together with findingsin gallium scan, this defect was interpreted as renal abscess. (Right)Longitudinal sonogram 6 cm to right of midline showsslight distortion of upper-pole calyces of right kidney (arrows) but noevidence of cystic area. Because of absence of fluid collection,pyelonephrltis was diagnosed. Patient subsequently improved onconservativetherapy with antibiotics.
Volume 18, Number 3 215
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from
SANDERS AND SANDERS
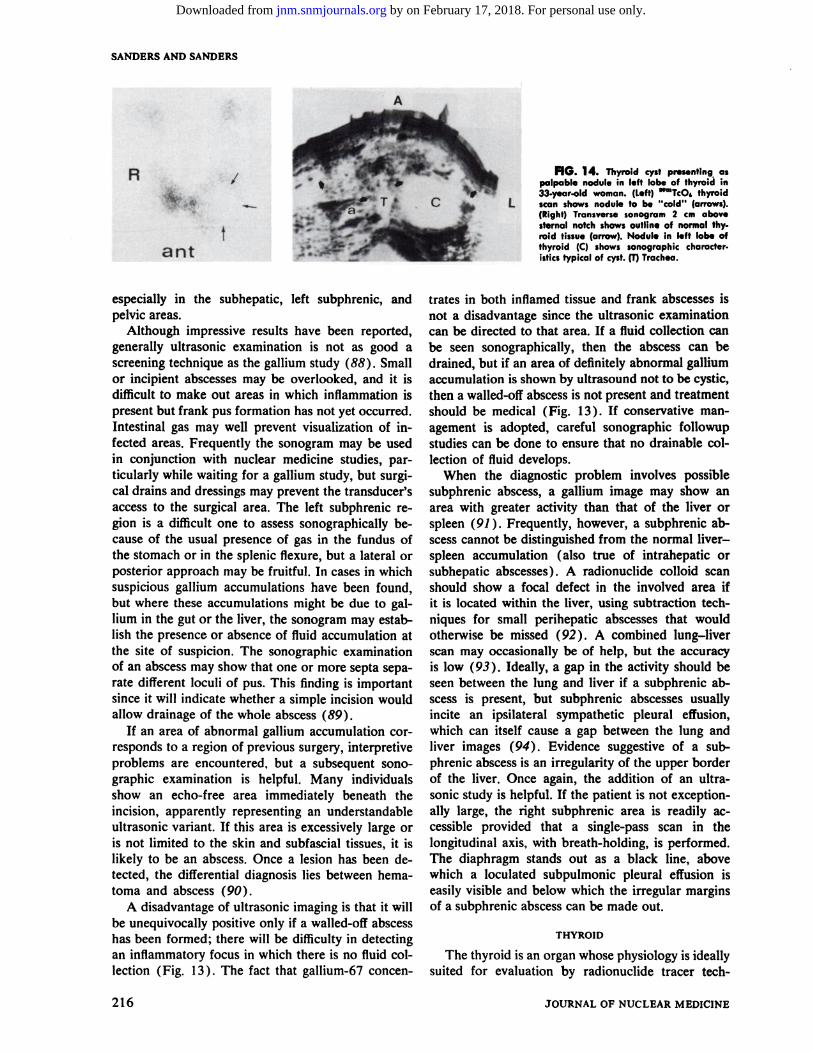
FIG. 14. Thyroidcystpresentingaspalpable nodule in left lobe of thyroid in33-year-old woman. (Left) ‘@TcO@thyroidscan shows nodule to be “cold―(arrows).(Right) Transversesonogram 2 cm abovesternal notch showsoutline of normal thyroid tissue (arrow). Nodule in left lobe ofthyroid (C) shows sonographic characteristicstypical of cyst.(I) Trachea.
A
ant
I
especially in the subhepatic, left subphrenic, andpelvic areas.
Although impressive results have been reported,generally ultrasonic examination is not as good ascreening technique as the gallium study (88) . Smallor incipient abscesses may be overlooked, and it isdifficult to make out areas in which inflammation ispresent but frank pus formation has not yet occurred.Intestinal gas may well prevent visualization of infected areas. Frequently the sonogram may be usedin conjunction with nuclear medicine studies, particularly while waiting for a gallium study, but surgical drains and dressings may prevent the transducer'saccess to the surgical area. The left subphrenic region is a difficult one to assess sonographically because of the usual presence of gas in the fundus ofthe stomach or in the splenic flexure, but a lateral orposterior approach may be fruitful. In cases in whichsuspicious gallium accumulations have been found,but where these accumulations might be due to gal
hum in the gut on the liver, the sonogram may establish the presence or absence of fluid accumulation atthe site of suspicion. The sonographic examinationof an abscess may show that one or more septa separate different loculi of pus. This finding is importantsince it will indicate whether a simple incision wouldallow drainage of the whole abscess (89).
If an area of abnormal gallium accumulation corresponds to a region of previous surgery, interpretiveproblems are encountered, but a subsequent sonographic examination is helpful. Many individualsshow an echo-free area immediately beneath theincision, apparently representing an understandableultrasonic variant. If this area is excessively large oris not limited to the skin and subfascial tissues, it islikely to be an abscess. Once a lesion has been detected, the differential diagnosis lies between hematoma and abscess (90).
A disadvantage of ultrasonic imaging is that it willbe unequivocally positive only if a walled-off abscesshas been formed; there will be difficulty in detectingan inflammatory focus in which there is no fluid collection (Fig. 13 ) . The fact that gallium-67 concen
trates in both inflamed tissue and frank abscesses isnot a disadvantage since the ultrasonic examinationcan be directed to that area. If a fluid collection canbe seen sonographically, then the abscess can bedrained, but if an area of definitely abnormal galliumaccumulation is shown by ultrasound not to be cystic,then a walled-off abscess is not present and treatmentshould be medical (Fig. 13). If conservative management is adopted, careful sonographic followupstudies can be done to ensure that no drainable collection of fluid develops.
When the diagnostic problem involves possiblesubphrenic abscess, a gallium image may show anarea with greater activity than that of the liver orspleen (91 ) . Frequently, however, a subphrenic abscess cannot be distinguished from the normal liverspleen accumulation (also true of intrahepatic orsubhepatic abscesses) . A radionuclide colloid scanshould show a focal defect in the involved area ifit is located within the liver, using subtraction techniques for small perihepatic abscesses that wouldotherwise be missed (92). A combined lung—liverscan may occasionally be of help, but the accuracyis low (93). Ideally, a gap in the activity should beseen between the lung and liver if a subphrenic abscess is present, but subphrenic abscesses usuallyincite an ipsilateral sympathetic pleural effusion,which can itself cause a gap between the lung andliver images (94). Evidence suggestive of a subphrenic abscess is an irregularity of the upper borderof the liver. Once again, the addition of an ultrasonic study is helpful. If the patient is not exceptionally large, the right subphrenic area is readily accessible provided that a single-pass scan in thelongitudinal axis, with breath-holding, is performed.The diaphragm stands out as a black line, abovewhich a loculated subpulmonic pleural effusion iseasily visible and below which the irregular marginsof a subphrenic abscess can be made out.
THYROID
The thyroid is an organ whose physiology is ideallysuited for evaluation by radionuclide tracer tech
216 JOURNAL OF NUCLEAR MEDICINE
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

ADJUNCTIVEMEDICALKNOWLEDGE
niques, by both imaging and in vitro studies. Function in terms of T4 and T3 output and its complexrelationship with various factors are easily assessed,as also are organ size, shape, and the presence of hotor cold nodules. Although ultrasound can be usedto measure the thyroid volume by means of serialscans and the formula proposed by Rasmussen (95),assessing the thyroid size by radionuclide imaging
R
L
FIG. 15. Thyroidadenomain42-year-oldwomanwithpalpa.ble thyroid nodule. (lop) mmTcO4thyroid scan showsarea of de.creased activity (arrow) in lower pole of right lobe of thyroid carresponding to palpable nodule. (Middle) Transversesonogram 3.5cm above sternal notch shows normal thyroid tissue (arrows), cxtending across trachea (T) anteriorly: (V) jugular vein; (a) carotidartery. Posterior aspect of right lobe has sonolucent area (N).Unlike typical cysts, however, sonolucentstructuresdid not havegood through transmissionand posterior-wall echoes are notprominent. (Bottom)Transversesection 3.5 cm above sternumwithincreased gain shows similar normal structures as scan throughsame level (Fig. 15B). However, previously noted sonolucentarea(N) has developed internal echoesas expected for solid homogeneous lesion, whereas really cystic structures(e.g., vessels)have remained echo-free. Diagnosiswas thyroid adenoma.
FIG. 16. Malignantascites.Transversesonographicsection4cm below umbilicus shows multiple fluid collections (a). Intestines(b) lie mostly in dependent portion, but bowel loop is adherent toanterior abdominal wall (arrowheads),a commonfinding in malignant ascites.Patient had disseminatedcarcinomaof ovary.
is so much easier that this aspect of thyroid evaluation is best left to nuclear medicine except when theuptake of tracer by the gland is so poor that theborders are not defined.
The role of ultrasound in the evaluation of thyroiddisease is confined to situations where a solitary coldnodule is revealed by radionuclide techniques (Figs.14 and 15). The nodulecan then be classifiedassolid or cystic by ultrasound and, if cystic, it can beaspirated under ultrasonic control and the cell contents of the fluid examined.
MISCELLANEOUS
Large amounts of free intrapenitoneal fluid can bediagnosed by plain radiographs of the abdomen,liver—spleen scintigraphy, and sonography. An avascular area is observed around the liver and spleenon the radionuclide images, and they frequently reveal poor definition of the margins. On sonographya fluid collection is seen first along the inferior margin of the liver and then surrounding the bowel inincreasing amounts. Quantities of free fluid as smallas 100 cc can be accurately detected by using A modeand placing the transducer near the umbilicus withthe patient in a knee—handposition (96). Smallamounts of loculated intraperitoneal fluid and loculation within a large free effusion can only be diagnosed by ultrasound. This information indicates thatthe ascites is either of an inflammatory or malignantnature and allows accurate localization@for paracentesis (Fig. 16).
Ultrasound has been found useful in classifyingmasses within the breast into three types: cysts, benign masses, and malignant masses. The accuracyrate is said to be as high as that obtained with mammography (97). Bone-seeking radiopharmaceuticals
Volume 18, Number 3 217
V a f •.@
R@ N T@ V
. @p -
V d@ ‘@‘@
R@ L@ ‘4
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

SANDERS AND SANDERS
(e.g., oomTc@labeled phosphates) have been reportedto accumulate in breast tumors (98,99), but theymay also accumulate in normal breast tissue and inbreasts with benign disease. Indium-i 11-bleomycinwas found 74% accurate in predicting malignancyof palpable breast masses in 3 1 patients. Technetium-99m has been reported to be fairly reliable inpredicting malignancy ( 88 % accurate in 16 cancers)but its use is limited by the righ rate of false positives(29 % ) in benign breast disease. Gallium-67 is muchless sensitive as an indicator of breast malignancy,
being positive in only 5 out of 10 breast carcinomas(100).
REFERENCES
1. SANDERSRC, JECKDL: B-scan ultrasound in the evaluation of renal failure. Radiology 119: i99—202, 1976
2. SANDERSRC, BEARMANS: B-scan ultrasound in thediagnosis of hydronephrosis. Radiology 108 : 375—382, 1973
3. HANDMAKERH, YOUNGBW, LOWENSTEINJM: Clinical experience with mmTc-DMSA (dimercaptosuccinic acid),a new renal-imaging agent. J Nuci Med 16: 28—32,1975
4. STAAB EV, HOPKINS J, PATTON DD, et al. : The use
of radionuclide studies in the prediction of function in renalfailure.Radiology106:141—146,1973
5. SANDERSRC: The place of diagnostic ultrasound inthe examination of kidneys not seen on excretory urography.I Urol114:813—821,1975
6. BEARMANSB, HINE PL, SANDERSRC: Multicystic kidney: A sonographic pattern. Radiology I 18: 685-688, 1976
7. SANDERSRC: Renal ultrasound. Radio! Clin North Am18: 417—434,1975
8. MAKLAD NR, CHUANG VP, DOUST BD, Ct al. : Solidrenal lesions : Ultrasonic and angiographic correlation.American Institute of Ultrasound Presentation, WinstonSalem, North Carolina, Oct., 1975
9. LEOPOLDGR, TALNER LB, ASHERWM, et al. : Renalultrasonography: An updated approach to the diagnosis ofrenal cyst. Radiology 109: 671—678,1973
10. ENLANDERD, WEBERPM, nos REMEDIOSLV: Renalcortical imaging in 35 patients: Superior quality with mmTcDMSA. I NucIMed 15:743—749,1974
11. POLLOCKHM, EDELL S, MORALESJD: Radionuclideimaging in the diagnosis of renal pseudotumors. Radiology111:639—644,1974
12. BOLTONWK, TULLY Ri, LEWIS EJ, et al. : Localization of the kidney for percutaneous biopsy. A comparativestudy of methods. Ann Intern Med 81 : 159—164,1974
13. SALAMENJR: Use of radioactive fibninogen for detecting rejection of human renal transplants. Br Med I 2:517—521,1970
14. GEORGEEA, CODDJE, NEWTONWT, et al. : Furtherevaluation of mmTc sulfur colloid accumulation in rejectingrenal transplants in man and a canine model. Radiology116: 121—126,1975
15. FRICKMP,LOKENMK, GOLDBERGME, etal.: UseofesmTcsulfur colloid in evaluation of renal transplant cornplications.I NucI Med 17:181—183,1976
16. DUBOVSKYEV, LoGic JR, DIETHELM AG, et al.:Comprehensive evaluation of renal function in the transplanted kidney. I Nuc! Med 16: 1115—1120,1975
17. ROSENTHALLL, MANGELR, LISBONAR, et al.: Diagnostic applications of radiopertechnetate and radiohippurate
imaging in post-renal transplant complications. Radiologylii:347—358,1974
;18. HOLLENBERG NK, B1RTcH A, RAsHiD A, et al. : Relationships between intrarenal perfusion and function : Serialhemodynamic studies in the transplanted human kidney.Medicine5l:95—106,1972
19. HöR0, PABSTHW, PFEIFERKJ, et al. : Radionuclidesin renal transplantation. I Nuci Med 13: 795—800,1972
20. BARTRUM RJ, SMITH EH, D'On.si CJ, Ct al.: The ultrasonic determination of renal transplant volume. I Clin Ultrasound2:281—285,1975
21. PAVELDG, JoNAssoNOM, ANDERSON0, et al.: Improved diagnosis of post renal transplant collecting systemabnormalities by radionuclide studies. I NucI Med 16: 557,1975
22. NESBITR, BLAKEDD, EKSTRANDK, et al. : Lymphocele following renal transplantation: Value of ultrasonography in diagnosis and follow-up studies. South Med I 69:303-304, 1976
23. SANDERSRC,HILLMC: “Cystic―massdifferentiationby grey scale B-scan ultrasonic pattern. Presented atWorld Federation of Ultrasound in Medicine and Biology,San Francisco, August, 1976
24. HADENHT, STACYWK, WOLFJS,et al.: Scintiphotography in diagnosis of urinary fistula after renal trans
plantation.I NucI Med 16:612—615,197525. S@ioos D, CAPEK V: Ultrasonically guided percu
taneous aspiration of lymphoceles following renal transpiantation: A diagnostic and therapeutic method. I Clin Ultrasound4: 45—46,1976
26. LEOPOLD GR, ASHER WM : Diagnosis of extraorganretroperitoneal space lesions by B-scan ultrasonography. Radiology104:133—138,1972
27. JACOBSONJB, REDMANHC: Ultrasound findings in acase of retropenitonealfibrosis. Radiology 113: 423—424,1976
28. FREIMANIS AK: Echographic diagnosis of lesions ofthe abdominal aorta and lymph nodes. Radio! Clin NorthAm 13:557—572,1975
29. TURNERDA, PINSKYSM, GOTrSCHALKA, Ct al. : Theuse of ‘TGascanning in the staging of Hodgkin's disease.Radiology104:97—101,1972
30. GREENLAW RH, WEINSTEIN MB, BRILL AB, et al.:VGa-citrate imaging in untreated malignant lymphoma: Preliminary report of cooperative group. I Nuci Med 15: 404—407, 1974
31. GLASSBURNJR, PRASAVINICHIA5, Nuss RC, et al.:Correlation of 1mAu abdominal lymph scans with lymphangiograms and lymph node biopsies. Radiology 105: 93—96,1972
32. KAZEN I, ANTONIADESJ, [email protected], et al. : Clinicalevaluation of lymph node scanning utilizing colloidal gold198.Radiology90:905—911,1968
33. MCAFEE JO, AUSE RG, WAGNERHN: Diagnosticvalue of scintillation scanning of the liver. Arch Intern Med116:95—110,1965
34. MOULDRF: An investigation of the variations in normal liver shape. Br I Radio! 45: 586—590,1972
35. WINSTONMA, KARELITZJ, WEIss ER, et al. : Vanation in the appearance of the lateral liver scan with patientposition. Radiology 102: 665—666,1972
36. RASMUSSENSN: Liver volume determination by ultrasonic scanning. Br I Radio! 45: 579—585, 1972
37. EDDLESTONALWF,BLENDISLM, OsBoaNSB,et al.:Significance of increased “splenicuptake― on liver scintiscanning. Gut 10: 711—716, 1969
218 JOURNAL OF NUCLEARMEDICINE
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from
ADJUNCTIVE MEDICAL KNOWLEDGE
scanning in acute hepatic amebic abscess. I Nucl Med 15:561—563,1974
60. Mor'utoE LS, LEOPOLD GR, BROWN JW, et al. : Theultrasonic scan in the management of amebic hepatic abscess.Am I Dig Dis 16: 523—528,1971
61. Cu@oN A, GORDON F, MUNOZ R, Ct al. : Scanning ofthe hepatic blood pool in liver amebiasis. Am I Roentgeno!Radium TherNuc!Med 117: 373—379,1973
62. BREER, STANLEYCT, GOLDSTEINHM, et al.: Thespectrum of findings in hepatic neoplasms. Presented atWorld Federation of Ultrasound in Medicine and Biology,San Francisco, 1976
63. SAMPLE WF, Po JB, GRAY RK, et al. : Gray-scaleultmasonography techniques in pancreatic scanning. App!Radio! 5: 63, 1975
64. DousT BD: Ultrasonicexaminationof the pancreas.Radio! C!in North Am 13: 467—478,1975
65. WALLS WJ, GONZALEZ 0, MARliN NL, et al. : B-scanultrasound evaluation of the pancreas. Radiology 114: 127—134,1975
66. WATANABEK, KAWAHIRAK, MATSUURAK : Scintigraphy as a screening test for carcinoma of the pancreas.Acta Radio! 15: 57—64,1974
67. ESPIRITU CR, ROLFS HE: Diagnostic accuracy ofpancreaticscanning.Am I Dig Dis 17:539—543,1972
68. MCCARThYDM, BROWNP, MELMEDRN, Ctal.: ThSeselenomethionine scanning in the diagnosis of tumors of thepancreas and adjacent viscera : The use of the test and itsimpact on survival. Gut 13: 75—87,1972
69. MIALE A, RODRIGUEZ-ANTUNEZA, GILL WM: Pancreas scanning after ten years. Semin Nucl Med 2: 201—219,1972
70. HANCKE5, HOLM HH, KOCH F: Ultrasonically guidedpercutaneous fine needle biopsy of the pancreas. Surg Gynecol Obstet 140: 361—364, 1975
71. LEOPOLDOR: Pancreatic echography: A new dimension in the diagnosis of pseudocyst. Radiology 104 : 365—369,1972
72. BERGBC: The use of radionuclide imaging in diagnosis and management of the “acute―or traumatized patient. In Diagnostic Nuclear Medicine, Gottschalk A, Potchen EJ, eds. Baltimore, Williams & Wilkins, 1976, pp 550—563
73. O'MARARE, HALLRC, DOMBOWSKIDL: Scintiscanfling in the diagnosis of rupture of the spleen. Surg GynecolObstet131.:1077—1084,1970
74. ASHERWM, PARVINS. VIRGIu0 RW, et al.: Echographic evaluation of splenic injury after blunt trauma.Radio!ogy118:411—415,1976
75. KRISTENSENJK, BUEMANNB, KUHL E: Ultrasonicscanning in the diagnosis of splenic haematomas. Ada ChirScand137:653—657,1971
76. HECKLL, GOTFSCHALKA: The appearanceof intrahepatic biliary duct dilatation on the liver scan. Radiology99: 135—140,1971
77. RYAN J, ISIKOFF M, NAGLE C, et al. : The combineduse of Tc-99m HIDA and ultrasound in differential diagnosis of jaundice. I Nuc! Med 17: 545, 1976
78. TAYLORKJ, CARPENTERDA, MCCREADYVR : Ultrasound and scintigraphy in the differential diagnosis of obstructive jaundice. I Clin Ultrasound 2: 105—116, 1974
79. PERLMUTrEROS, GOLDBERGBB: Ultrasonicevaluation of the common bile duct. I Cli,; Ultrasound 4: 107—Ill,1976
80. DOUST BD, MAKLAD NF: Ultrasonic B-mode examination of the gallbladder. Technique and criteria for the
38. GOODRICHJK, HALIBAN M, WiuuNsoN R, et al. : Extrahepatic ‘@mTcsulfur colloid distributions: Indicator ofliver disease. In Hematopoietic and Gastrointestinal Investigations with Radionuclides. Springfield, Ill., C. C. Thomas,1972,pp 400—414
39. GESLIENGE, PINSKYSM, P0THRK, et al.: The sensitivity and specificity of @“Tc-sulfurcolloid liver imagingin diffuse hepatocellular disease. Radiology 1 18 : 115—119,
197640. CARLSENEN: Liver, gallbladder and spleen. Radio!
ClinNorthAm 13:543—556,197541. LEOPOLD OR: Gray scale ultrasonic angiography of
upper abdomen. Radiology 117: 665—671,197542. KRISHNAMURTHYGT, WINSTON MA, WEiss ER, et al.:
Demonstrations of collateral pathways after superior venacaval obstruction with the scintillation camera. I Nucl Med12:189—191,1971
43. HOLMQUESTDL, BURDINEJA: Caval—portalshuntingas a cause of a focal increasein radiocolloiduptake in normal livers. I Nucl Med 14: 348—351, 1973
44. VOLPE JA, JOHNSTONOS: “Hot―hepatic hemangioma: A unique radiocolloid-concentrating liver scan lesion.JSurgOncol2: 373—377,1970
45. WOOD EJ, TAVILL AS: Liver and spleen scanning:Some physical and clinical aspects. Br I Radio! 44: 402,1971
46. HOLBIG HD : Focal iatrogenic increased radiocolloiduptake in liver scan. I Nuc! Med 14: 354—355, 1973
47. FREEMANLM, MANDELLCH : Dynamicvascularscmtiphotography of the liver. Semin Nuci Med 2: 133—138,1972
48. LITTENBERG RL, ALAzit@KI NP, TAKETA RM, et al.:A clinical evaluation of gallium-67 citrate scanning. SurgGyneco! Obstet 137: 424—430,1973
49. LOMASF, DIBOS PE, WAGNERHN : Increased specificity of liver scanning with the use of °@galliumcitrate.NEnglJMed286: 1323—1329,1972
50. TAYLORKJ, CARPENTERDA, MCCREADYVR: Greyscale echography in the diagnosis of intrahepatic disease.JClin Ultrasound 1: 284—287,1973
51. LOMONACOA, KLINE P. HALPERN S, et al. : Nuclearmedicine and ultrasound : Correlation in diagnosis of disease of liver and biliary tract. SeminNuc! Med 5: 307—324,1975
52. LEYTON B, HALPERN5, LEOPOLD0, et al. : Comelation of ultrasound and colloid scintiscan studies of the
normal and diseased liver. I NucI Med 14: 27—33,197353. GARRETT WJ, KOSSOFF 0, UREN RF, Ct al. : Gray
scale ultrasonic investigation of focal defects on mmTc sulphur colloid liver scanning. Radiology I 19: 425—428,1976
54. LEE GC, WILsoN RL, WAXMAN AD, et al. : Comrelation of scintigraphic and sonographic findings in focal liverdisease.JNuclMed15:511,1974
55. VIDRIH VE, HIGGINS HP: Accuracy of liver scintiphotography using a plastic and water phantom. Can J Surg14:273—279,1971
56. COVINGTON EE: Pitfalls in liver@ photoscans. A m IRoentgenol Radium Ther Nuci Med 109 : 745—748,1970
57. THIJS LG, SNELLP: Diagnosisof cystic lesions of theliver with special reference to the value o1@iagnostic ultra
sound. Neth I Med 18: 234—244,197558. KUMARB, COLEMANRE, ALDERSONP0: Gallium
citrate Ga 67 imaging in patients with suspected inflamma
tory processes. Arch Surg I 10: 1237—1242,1975@59. GESLIENGE, THRALLJH, JOHNSONMC: Gallium
219Volume 18, Number 3
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

SANDERSANDSANDERS
diagnosis of gallstones. Radiology I 10: 643—647,197481. HUBLITZ UF, KAHN PC, SELL LA: Cholecystosonog
raphy: An approach to the nonvisualized gallbladder. Radiology 103: 645—649,1972
82. ROSENFIELD N, GluscoM NT: Choledochal cysts:Roentgenographic techniques. Radiology 114: 113—119, 1975
83. FILLY RA, CARLSENEN: Choledochal cyst: Reportof a case with specificultrasonographicfindings.I Clin U!-trasound4: 7—10,1976
84. HANDMAKER H: Nuclear medicine in the evaluationof the patient with jaundice. JAMA 23 1: 1172—1176, 1975
85. ThATES CD, HUNTER JO : Gallium scanning as ascreening test for inflammatory lesions. Radiology 1 16: 383—387,1975
86. LIi-FENBERGRL, TAKETA RM, ALAZRAKI NP, et al.:Gallium-67 for localization of septic lesions. Ann internMed79: 403—406,1973
87. HoPKINS GB, KAN M, MENDE CW: Early @Gascmtigraphy for the localization of abdominal abscesses. I NucIMed 17:990—992,1975
88. MAKLADNF, DOUST BD, BAUM JK : Ultrasonic diagnosis of postoperative intra-abdominal abscess. Radiology113:417—422,1974
89. UHRICHPC, SANDERSRC: Ultrasoniccharacteristicsof pelvic inflammatory masses. I Clin Ultrasound 4: 199—204, 1976
90. SMITH EH, BARTRUM RJ : Ultrasonically guided percutaneous aspiration of abscesses. Am I Roentgeno! RadiumTherNuclMed 122:308—312,1974
91. BLAIR DC, CARROLLM, SILVAJ, et al. : Localizationof infectious processes with gallium citrate Ga 67. JAMA230:82—85,1974
92. DAMRON JR, BEmN RM, SELBY JB, et al.: Galliumtechnetium subtraction for the localization of subphrenicabscess. Radiology 113: 117—122,1974
93. GOLD RP, JOHNSON PM: Efficacy of combined liverlung scintillation imaging. Radiology 117: 105—111, 1975
94. SANDERSRC : Post-operative pleural effusion and subphrenic abscess. Clin Radio! 21 : 308—312, 1970
95. RASMUSSEN SN, HJORTH L: Determination of thyroid volume by ultrasonic scanning. I Clin Ultrasound 2:143—147,1974
96. GOLDBERGBB, GOODMAN GA, CLEARFIELD HR:Evaluation of ascites by ultrasound. Radiology 96: 15—22,1970
97. COLE-BEUGLET C, BEIQUE RA: Continuous ultrasound B-scanning of palpable breast masses. Radiology 117:123—128,1975
98. WEINRAUB JM, ROSENBERG R, IRWIN GAL: Technetium-99mpolyphosphatein differentialdiagnosisof breastmasses. I NuclMed 16: 581, 1975
99. HOLMES RA, MANOLI RS, ISITMAN AT: Tc-99mlabeled phosphates as an indicator of breast pathology.I Nucl Med 16: 536, 1975
100. RICHMAN SD, BRODEY PA, FRANKEL RS, et al.:Breastscintigraphywith‘5―Tc-pertechnetateand “Ga-citrate.INuc!Med 16:293—299,1975
(@ SNMTECHNOLOGISTSECTION24th Annual Meeting
June20—23,1977 McCormick Place Chicago,Illinois
SIXTHCALLFORTECHNOLOGISTSCIENTIFICEXHIBITSTheTechnologistProgramCommitteejnvjtesthesubmissionof abstractsof exhibitsfor the24thAnnual
Meeting. Applications are welcomed from all technologists. The Committee also welcomes exhibits thatcompliment presented papers on the program.
All exhibits will be illuminated by availableroom light. Therewill be no provisionsfor transillumination, e.g.,viewboxes.The exhibit should be mounted on poster board not exceeding 30x 30in. No morethan two boardsmaybeenteredforasubject.Exhibitsshouldbeclearlytitled.Submitthefollowinginformationwithyourapplication:exhibitor'snameandaffiliation,title of exhibit(10wordsmaximum),abstract(100words),dimensions(maximum of 2 boards not exceeding 30 x 30 in.).
First, Second, and Third place awards will be presented to the three most outstanding exhibits. These will bejudgedon the basisof scientificmerit,originality,displayformat,andappearance.
For additional information contact Joan A. McKeown,MercyCatholic MedicalCenter,PhiladelphiaSchoolof Nuclear Medicine Technology, Lausdown & Bailey Road, Darby, PA 19023.
DEADLINE: April 10, 1977
220 JOURNAL OF NUCLEAR MEDICINE
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from

1977;18:205-220.J Nucl Med. Angelita Dingcong Sanders and Roger C. Sanders The Complementary Use of B-Scan Ultrasound and Radionuclide Imaging Techniques
http://jnm.snmjournals.org/content/18/3/205.citationThis article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1977 SNMMI; all rights reserved.
by on February 17, 2018. For personal use only. jnm.snmjournals.org Downloaded from