joanne klevens hhs public access a sarah beth l. … · exploring policies for the reduction of...
TRANSCRIPT
Exploring policies for the reduction of child physical abuse and neglect☆
Joanne Klevensa, Sarah Beth L. Barnetta, Curtis Florencea, and DeWayne Mooreb
aCenters for Disease Control and Prevention, Division of Violence Prevention, Atlanta, GA, USA
bClemson College of Business and Behavioral Science, School of Psychology, Clemson, SC, USA
Abstract
Policies can be powerful tools for prevention given their potential to affect conditions that can
improve population-level health. Given the dearth of empirical research on policies' impacts on
child maltreatment, this article (a) identifies 37 state policies that might have impacts on the social
determinants of child maltreatment; (b) identifies available data sources documenting the
implementation of 31 policies; and (c) utilizes the available data to explore effects of 11 policies
(selected because they had little missing data) on child maltreatment rates. These include two
policies aimed at reducing poverty, two temporary assistance to needy families policies, two
policies aimed at increasing access to child care, three policies aimed at increasing access to high
quality pre-K, and three policies aimed at increasing access to health care. Multi-level regression
analyses between within-state trends of child maltreatment investigation rates and these 11
policies, controlling for states' childhood poverty, adults without a high school diploma,
unemployment, child burden, and race/ethnicity, identified two that were significantly associated
with decreased child maltreatment rates: lack of waitlists to access subsidized child care and
policies that facilitate continuity of child health care. These findings are correlational and are
limited by the quality and availability of the data. Future research might focus on a reduced
number of states that have good quality administrative data or population-based survey data on
child maltreatment or reasonable proxies for child maltreatment and where data on the actual
implementation of specific policies of interest can be documented.
Keywords
Child physical abuse; Child neglect; Policy evaluation
☆Partial data collection was conducted under contract with the Center for the Study of Social Policies with funding from the Doris Duke Charitable Foundation, in partnership with the CDC Foundation, and the Division of Violence Prevention of the Centers for Disease Control and Prevention. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Correspondence to: Joanne Klevens.
HHS Public AccessAuthor manuscriptChild Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Published in final edited form as:Child Abuse Negl. 2015 February ; 40: 1–11. doi:10.1016/j.chiabu.2014.07.013.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Introduction
Research on and use of public policies to prevent child maltreatment is surprisingly scant. A
recent review conducted to identify gaps in child maltreatment prevention found only three
studies examining public policies (Klevens & Whitaker, 2007). Two of these studies
examined the impact of welfare policies on child physical abuse and neglect (Fein & Lee,
2003; Paxson & Waldfogel, 2002, 2003), and one study looked at the impact of legislation
banning corporal punishment (Durrant, 1999). Other policies with prevention potential
examined in the literature not identified by Klevens and Whitaker (2007) include legislation
criminalizing fetal exposure to drugs (Chavkin, Wise, & Elman, 1998), child exposure to
partner violence being considered child neglect (Edleson, Gassman-Pines, & Hill, 2006),
increasing access to abortion (Bitler & Zavodny, 2004; Seiglie, 2004; Sen, Wingate, &
Kirby, 2012), and housing policies' effects on stability for children and availability of child
care (McAllister, Thomas, Wilson & Green, 2009).
This limited research on policies is problematic because policies can be powerful tools for
prevention given their potential to affect the conditions in which people are born, grow, live,
and work (i.e., social determinants) and improve population-level health (Commission on
Social Determinants of Health [CSDH], 2008). Even policies that are not formulated with
health in mind often have health consequences. For example, the Earned Income Tax Credit
has been associated with decreases in infant mortality (Arno, Sohler, Viola, & Schechter,
2009). Providing income support to families in poverty has been associated with decreases
in children's externalizing behaviors (Gennetian, Castells, & Morris, 2010), young adult
substance abuse (Costello, Erkanli, Copeland, & Angold, 2010), and delinquency (Akee,
Copeland, Keeler, Angold, & Costello, 2010).
Given the potential for prevention and dearth of empirical research on policies' impacts on
child maltreatment, we aimed to (a) identify state policies that might have impacts on the
social determinants of child maltreatment; (b) identify available data sources documenting
the implementation of these policies; and (c) utilize the available data to explore effects of a
selected set of policies on child maltreatment investigation rates. The first section of this
article describes our approach and findings for the first two aims. The second section
presents the methods and findings for the third aim. The final section will summarize the
findings, identify the limitations of our data, and suggest directions for future efforts. This
work may encourage other child maltreatment prevention researchers to go beyond
individual and family-level interventions and consider more research on policies' impacts.
Identification of Policies, Theoretical Links, and Data Sources
The term policy, as used in this study, includes any law, regulation, procedure,
administrative action, incentive, or voluntary practice of governments and other institutions
(Centers for Disease Control and Prevention, 2013). This study focuses on state-level
policies for two reasons. First, states and local governments contribute to two thirds of all
public spending on children (Isaacs, Hahn, Rennane, Steuerle, & Vericker, 2011), and
therefore, state-level public policies have substantial impacts on children. Second, the
variation across states and small but measurable change over time in the selection and
Klevens et al. Page 2
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

implementation of policies offered multiple “natural experiments” which could facilitate the
evaluation of the impact of policies.
To identify state policies that might affect the social determinants of child maltreatment
rates we consulted with nine individuals identified by the Center for the Study of Social
Policy (CSSP) as policy experts in the area of child and family welfare, economics, public
health, health care, or environment and discussed with them how these policies might be
theoretically linked to child maltreatment. For the consultants, we defined social
determinants as the circumstances in which people are born, grow, live, work, and age
(CSDH, 2008). These consultants also provided suggestions for available data on state-level
policies. Internet searches and interviews with key informants identified by CSSP were used
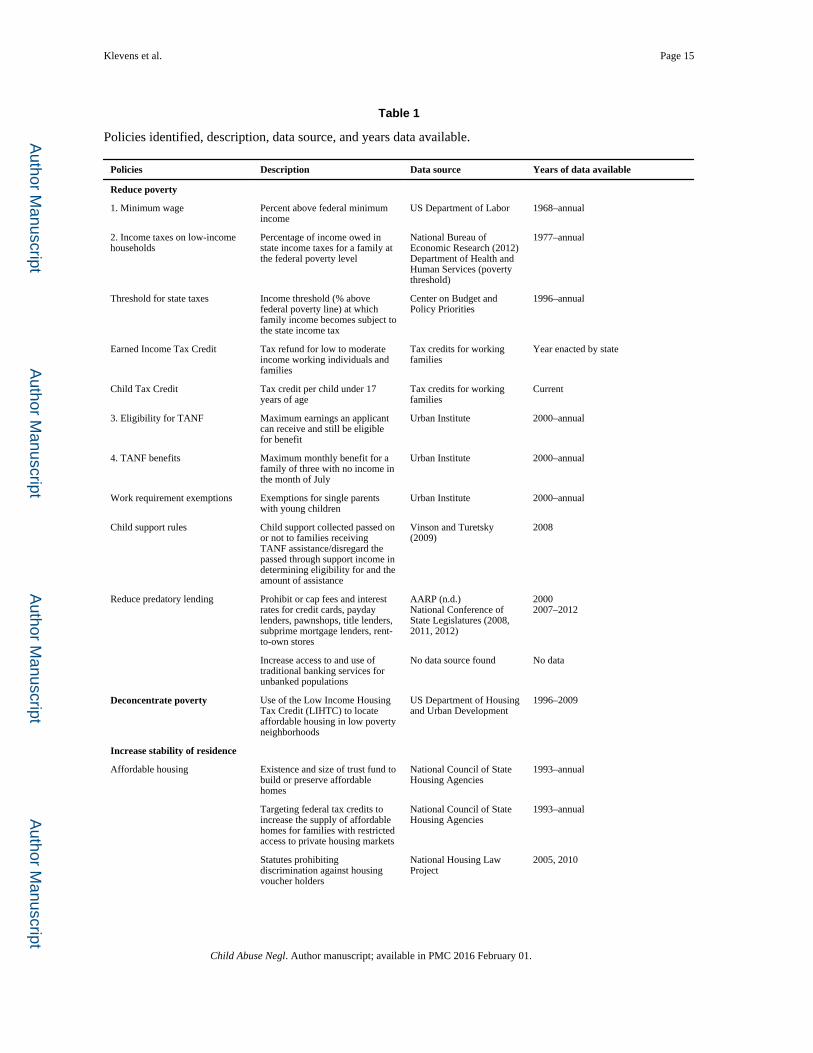
to identify other available data on state-level policies. Table 1 presents the list of state
policies identified and, if found, the year(s) and source for which data were available on
their implementation.
The first group of policies identified addressed the issues of low income and poverty. Low
income has long been associated with maltreatment (Stith et al., 2009). The mechanisms
through which poverty or low income might increase child maltreatment include increased
parental stress as a result of perceived hardships (Gershoff, Aber, Raver, & Lennon, 2007;
Mistry, Vandewater, Huston, & McLoyd, 2002; Slack, Holl, McDaniel, Yoo, & Bolger,
2004; Yeung, Linver, & Brooks-Gunn, 2002), increased number of negative life events
(Gershoff et al., 2007), or because of poverty's effects on parents' mental health and
relationships with partners (Yeung et al., 2002).
Policies related to concentration of poverty were also proposed. Concentrated neighborhood
poverty is consistently associated with higher rates of child maltreatment (Coulton,
Crampton, Irwin, Spilsbury, & Korbin, 2007; Freisthler, Merritt, & LaScala, 2006).
Neighborhood disadvantage might increase child maltreatment through its effects on
parental depression (Mair, Diez Roux, & Galea, 2008), social capital (Zolotor & Runyan,
2006), willingness to rely on neighbors for child care (Garbarino & Sherman, 1980) or other
needs (Ernst, 2001), increased social disorder resulting in lack of social controls on
behaviors (Freisthler et al., 2006), or decreased access to resources and formal supports.
Housing policies were suggested because they affect access to affordable housing and
residential stability. Homelessness is a stronger predictor than parental substance abuse or
mental illness for out-of-home placements for children (Cowal, Shinn, Weitzman,
Stojanovic, & Labay, 2002). Whether a direct result of low income or its correlates,
homelessness or residential instability is in itself a stressor and it affects a parent's ability to
develop and maintain a local support network. In turn, weak or lack of social support is a
consistent risk factor for child maltreatment (Stith et al., 2009).
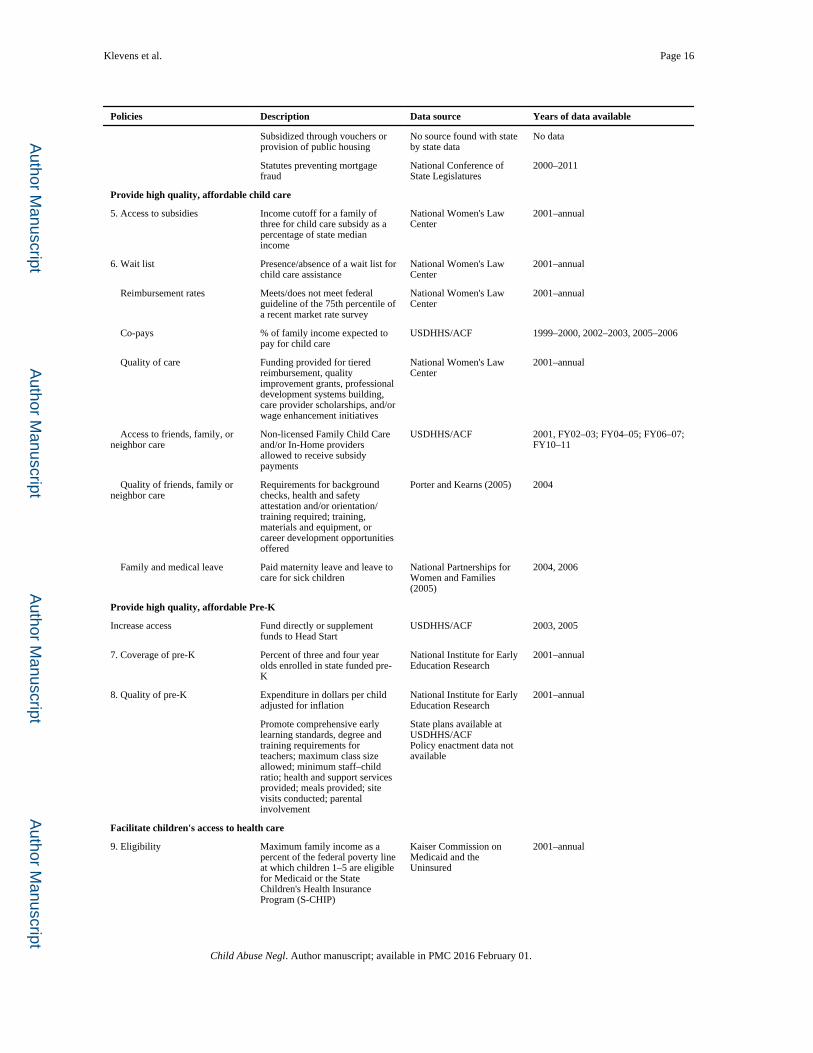
Policies related to access to high quality affordable childcare were proposed for two reasons.
First, childcare assistance can affect families' ability to work and earn sufficient income
(Schulman & Blank, 2004); as described previously, insufficient income may lead to child
maltreatment through various mechanisms. Second, enriched early experiences in high-
Klevens et al. Page 3
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
quality care settings can reduce childhood and adolescent behavioral problems (Vandell et
al., 2010) which may trigger abusive parenting.
Evidence suggesting that pre-K programs involving parents may reduce child maltreatment
(Reynolds & Robertson, 2003) led to consideration of policies increasing access to high
quality pre-K. States vary considerably in the strategies pursued to increase the quality of
child care (e.g., allowing tiered reimbursement; and providing funding for quality
improvement grants, professional development systems building, care provider scholarships,
and/or wage enhancement initiatives) and pre-K programs (e.g., promoting comprehensive
early learning standards or parental involvement, establishing degree and training
requirements for teachers, setting maximum class size allowed and minimum staff–child
ratio, requiring that health and support services and meals be provided, and conducting site
visits).
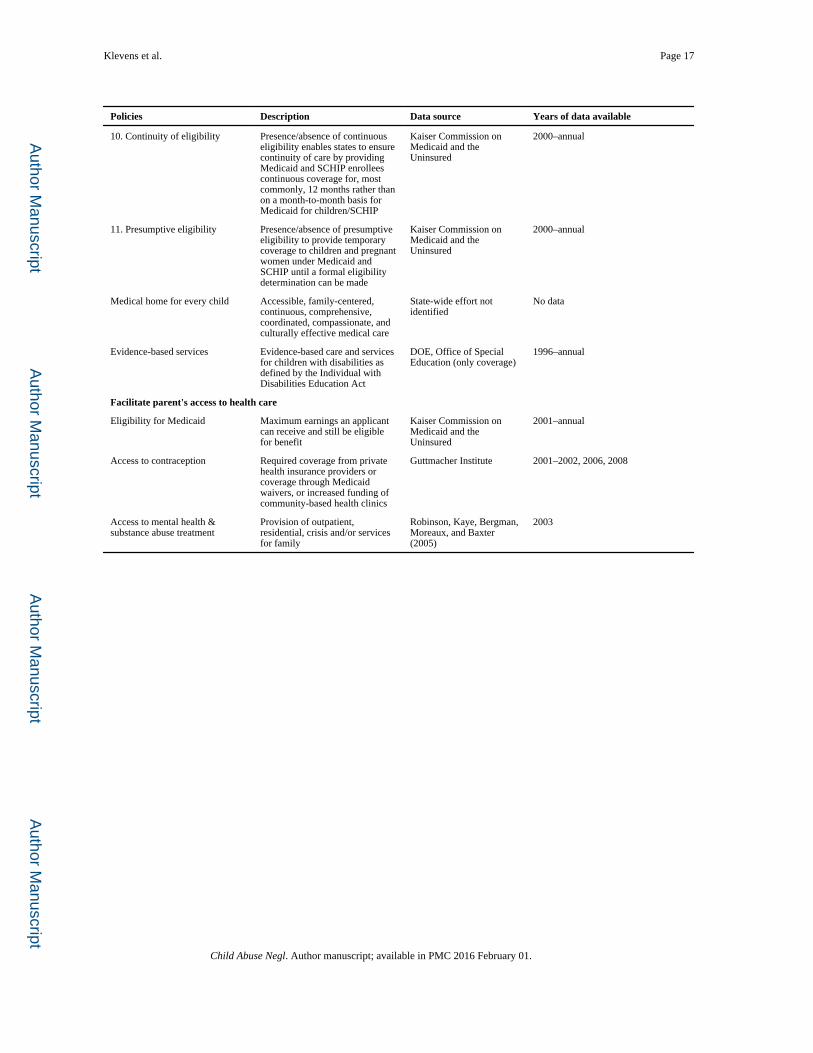
Policies related to state provision of children's health care insurance (SCHIP) were proposed
because without insurance children are less likely to receive health services in a timely
manner (Institute of Medicine, 2002) which might lead to medical neglect. In addition to
considering increased thresholds for eligibility for lower income families, policy experts
proposed continuous eligibility and presumptive eligibility policies. Continuous eligibility
policies were considered because these enable states to ensure continuity of care by
providing Medicaid and SCHIP enrollees' continuous coverage for longer periods of time
rather than on a month-to-month basis. Presumptive eligibility policies enable states to
provide temporary coverage to children and pregnant women under Medicaid and SCHIP
until a formal eligibility determination can be made.
Policies related to parents' health insurance and access to mental health care, substance
abuse treatment, and contraception were also suggested. Such policies were included
because anxiety, depression, psychopathology, substance abuse, and unplanned pregnancies
are risk factors for child maltreatment (Stith et al., 2009).
Exploration of Potential Effects of Policies on Child Maltreatment Investigation Rates
We examined the potential statistical effects of the 11 policies that had the most complete
set of state-level yearly data for 2000 to 2009. The 11 policies selected for these analyses are
numbered in the first column of Table 1 along with a description and the sources of data
used to document these policies.
Methods
Variables
The dependent variable for these policy analyses, state-level child maltreatment
investigation rate, was based on the U.S. Department of Health and Human Services'
(DHHS) Administration for Children and Families (2002, 2003, 2004, 2005, 2006, 2007,
2008, 2009, 2010a, 2010b) annual reports on child abuse and neglect. These reports contain
data on the number of referrals (or allegation of maltreatment) to Child Protective Services
(CPS), the number of cases screened in (i.e., investigated), and the number of cases
determined to be maltreated or substantiated by CPS for the 50 states and the District of
Klevens et al. Page 4
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Columbia. We chose to utilize cases screened in (per 1,000 children in each state) as the
outcome for various reasons. A screened in referral means that an allegation of child abuse
or neglect met the State's standard for investigation. The rate of investigations in the United
States has remained constant for at least the past five years (DHHS, 2010), which suggests
some level of consistency in this determination despite changes in response (e.g., the
development of differential response models). Screened in cases include both substantiated
and unsubstantiated cases. Although including unsubstantiated cases in our rates might seem
counterintuitive, there is growing recognition in the field that this inclusion provides a better
indicator of child maltreatment given that multiple studies find little or no difference
between substantiated and unsubstantiated cases in regards to risk factors or future risk
(Drake, Jonson-Reid, Way, & Chung, 2003; English, Marshall, Brummel, & Orme, 1999;
Hussey et al., 2005; Jonson-Reid, Drake, Kim, Porterfield, & Han, 2004; Kohl, Jonson-Reid,
& Drake, 2009). It also avoids the problem of substantiation rates changing as a result of
new procedures or response decisions implemented by child protective services (e.g.,
alternative response tracks). We refer to this dependent variable as child maltreatment
investigations throughout the manuscript.
The independent variables were the 11 policies identified as havinig the most complete data
set. These variables included:
(a) state minimum wage (U.S. Department of Labor, 2013),
(b) the percentage of income owed in state income taxes (tax burden; calculated
with version 9.0 of TAXSIM; Feenberg & Coutts, 1993; National Bureau of
Economic Research, 2012) for families at the federal poverty line (U.S.
Department of Health and Human Services, 2011a,b),
(c) the maximum earnings applicants could receive and still be eligible for TANF
benefits in each state (maximum monthly earnings and still eligible) (Rowe,
McManus, & Roberts, 2004; Rowe & Murphy, 2006, 2009; Rowe, Murphy, &
Kaminski, 2008; Rowe, Murphy, & Williamson, 2006a, 2006b; Rowe, Murphy,
& Mon, 2010; Rowe & Roberts, 2004; Rowe & Russell, 2004; Rowe &
Versteeg, 2005),
(d) monthly benefits for a family of three, both adjusted for 2009 dollars (Rowe et
al., 2004; Rowe & Murphy, 2006, 2009; Rowe et al., 2008; Rowe et al.,
2006a,b; Rowe et al., 2010; Rowe & Roberts, 2004; Rowe & Russell, 2004;
Rowe & Versteeg, 2005),
(e) the income cutoff for child care subsidies for a family of three in each state
(Blank, 2001; National Women's Law Center, 2004, 2006, 2007, 2008, 2009),
(f) existence of a waitlist for child care in each state (Blank, 2001; National
Women's Law Center, 2004, 2006, 2007, 2008, 2009),
(g) percent above the federal poverty line at which children one to five years old
were eligible for Medicaid/SCHIP (eligibility for Medicaid/SCHIP; Kaiser
Commission on Medicaid and the Uninsured, 2000, 2002, 2003, 2004, 2005,
2007, 2008, 2009a,b),
Klevens et al. Page 5
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
(h) continuity of eligibility for Medicaid/SCHIP (Kaiser Commission on Medicaid
and the Uninsured, 2000, 2002, 2003, 2004, 2005, 2007, 2008, 2009a,b),
(i) presumptive eligibility for Medicaid/SCHIP (Kaiser Commission on Medicaid
and the Uninsured, 2000, 2002, 2003, 2004, 2005, 2007, 2008, 2009a,b),
(j) percent of 3- and 4-year olds in pre-K (National Institute for Early Education
Research, 2003, 2004, 2005, 2006, 2007, 2008, 2009), and
(k) expenditures per child in pre-K in each state (available for 2001–2009; National
Institute for Early Education Research, 2003, 2004, 2005, 2006, 2007, 2008,
2009).
Thus, the data consisted of 510 potential observations (where an observation is a state/year
pair), representing 50 states and the District of Columbia during 10 years. There were 63
instances of missing state child maltreatment investigation rates (12%). Missing data for the
policy analyses ranged from 157 observations (31%) for state pre-K expenditures to 42
observations (8%) for state minimum wage. All analyses treated missing data as missing.
The following variables were considered potential confounders: state percentages of
childhood poverty (U.S. Census Bureau, 2011c), population over 18 years of age with high
school diploma (U.S. Census Bureau, 2011a), proportion of Black and Latino population
(U.S. Census Bureau, 2011b), annual average unemployment rate (U.S. Department of
Labor, 2012), and the state ratio of children 0–17 to adults 18–64 (U.S. Census Bureau,
2012).
Analyses
To establish potential effects of policies on states' rates, multi-level regression model
analyses was used to estimate the within state trends in child maltreatment investigation
rates as a function of a specific policy controlling for all confounders mentioned previously.
In addition, we also estimated models with up to three policies of similar nature to adjust for
these simultaneously (e.g., TANF eligibility and TANF benefits were in the same model).
For descriptive purposes, there was evidence of substantial clustering of measurement
occasions (Level 1) within states (Level 2). For all variables, the proportion of state level
variance was substantial (assessed by treating each predictor as a dependent variable in an
intercept only model to establish intraclass correlation coefficients (ICCs)). All ICCs were
over .50, except for the measure of child care quality (ICC = .14), indicating over half of the
variation in the assessments occurred across states. Multi-level models were selected to
adjust for the clustering of time within states.
We focus on the results for the Level 1 predictors. All Level 1 predictor variables were
centered around the state mean (Hoffman & Gavin, 1998). Values that deviated by more
than 4.5 standard deviations from the expected value were excluded from the analyses to
reduce error and avoid excess influence on effects. The time trend in child maltreatment
investigation rates was included as a fixed effect. The policy variables were measured as
differences from the state mean for the study period in order to control for unobservable
state differences that are constant during the study period. A state-level random effect
(random intercept) was also included to model unexplained variation across states in child
Klevens et al. Page 6
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
maltreatment investigation rates. Because trends over time were likely to vary by state we
also model a random slope for time. Fit statistics based on the reduction in the −2 Restricted
Log Likelihood (REML was used instead of ML estimation) and Schwarz's Bayesian
Criterion (BIC) indicated improvement in fit by modeling a random slope using the
unstructured option for the covariance structure.
Given the large number of policies examined and the potential for collinearity among the
policy variables, all 11 policy variables were not entered into the model simultaneously.
Instead, separate models were estimated with each policy individually. As a sensitivity
analysis, models were also estimated that included all policies in a given policy category,
such as all state Medicaid policies.
Results of Policy Analyses
Between 2000 and 2009, the rate of child maltreatment investigations ranged from 7.77 to
97.2 per 100,000 children (M = 26.7, SD = 10.3). Overall, these rates tended to decrease
over the time period.
Table 2 presents descriptive statistics for the selected policies, standardized β regression
coefficients and marginal effects (for each policy alone and, in parentheses, adjusted for
similar policies) derived from the multi-level regression models controlling for demographic
confounders. Marginal effects are calculated as the change in the dependent variable
associated with a one-unit change in the policy variable. Standard errors for marginal effects
are presented in Table 3. The absence/presence of wait lists to access child care had a
statistically significantly association with child maltreatment investigation rates. More
specifically, the presence of wait lists to access subsidized child care was associated with an
increase in maltreatment investigations of 3.13 per 1,000 children.
States' continuity of eligibility for Medicaid/SCHIP was statistically significant and
associated with lower child maltreatment investigation rates. States with continuous
eligibility for Medicaid/SCHIP have child maltreatment investigation rates that are 2.55 per
1,000 lower than states without continuous eligibility.
Discussion
In this article, 37 different policies are identified that might have impacts on the social
determinants of child maltreatment. For 31 of these policies, there is at least one data point
documenting their existence at the state-level. Multiple years of data are readily available for
some unevaluated policies such as the Earned Income Tax Credit, work requirements for
single parents with young children, and those aimed at increasing availability of affordable
housing. This list is not exhaustive but suggests several opportunities for child maltreatment
prevention researchers and others interested in policy evaluation. It may also be of interest to
those concerned with child well-being in general.
We also examined the statistical relationship between child maltreatment investigation rates
and four policies targeting poverty reduction, two policies facilitating access to child care,
two policies facilitating access to early childhood education (pre-K), and three policies
Klevens et al. Page 7
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
facilitating children's access to health care. We found a statistically significant negative
effect of waitlists to access subsidized child care and a statistically significant positive effect
for policies that facilitate continuity of child health care insurance which are consistent with
the expectation that greater access to child care and continuous access to health care could
potentially decrease child maltreatment rates.
Our models control for a wide array of demographic confounders, the presence of similar
policies, and the policy variables are measured as deviations from the state mean to control
for time-invariant state-level unobservables and common trends in reports of child
maltreatment. We report only within state trends to avoid issues with the variation in state
definitions of what constitutes child maltreatment and who is mandated to report. However,
there may be other confounders we have not controlled for that may be time-variant within
states and potentially correlated with these state policies. On the other hand, given that
policies might be more effective if implemented as part of a larger package, controlling for
similar policies occurring simultaneously may be considered excessive.
Our statistical analyses have other limitations that warrant cautious interpretation for both
the significant findings as well as the nonsignificant findings. Although the data reported by
the Administration for Children and Families are extremely useful, there are many issues
related to using child maltreatment reports to CPS (Fallon et al., 2010). Administrative
protocols, regulations, and definitions vary across states. In addition, we chose to focus only
on allegations of child abuse or neglect that met the State's standard for investigation (i.e.,
screened in). However, because we only report within state trends, these issues would be of
concern if they vary within states over time.
Our use of official reports is also a potential limitation. Reports to CPS underestimate the
occurrence of child maltreatment (Theodore et al., 2005), and future research should
examine policies' impacts on self-reported child maltreatment.
These statistical analyses are also limited by the indicators or data used to measure the
implementation of a policy. We have no information on how well the policies were
implemented, what proportion of the population targeted was covered or actually complied,
or whether the policies affected those at highest risk. We also lack information on the
implementation of competing policies or contextual factors that may have influenced
implementation or child maltreatment investigation rates. In addition, we have no
information on whether these policies effectively achieved their purpose, and if they did,
whether there was a time lag between the implementation of the policy and this
achievement. Future research should try to collect this type of information in order to be
able to know whether the absence of effects is because of poor implementation, reduced
coverage, inequitable coverage, a time lag, competing policies or contextual factors, or
ineffective policies.
Another limitation to consider is that the associations identified occur at the state level and
not at the family or child level. Thus, although we report a significant association between
increased state rates of child maltreatment investigations and the presence of child care
waiting lists, we cannot conclude that a child being on a child care waiting list is associated
Klevens et al. Page 8
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
with that child's increased risk for being investigated for child maltreatment. However, state-
level time trend analyses can suggest a potential relationship between policy changes and
maltreatment reports that deserves further exploration. Future research using different
research designs is needed to understand the pathways by which policy changes may be
linked to child maltreatment.
Finally, it is important to acknowledge that our study design does not permit us to draw
conclusions about causality from the analyses. Although the longitudinal design and our
ability to adjust for confounders in our analyses add strength to our conclusions, these
strategies do not overcome key potential biases inherent to quasi-experimental studies. For
this reason, our findings should be viewed as correlational.
Although the randomized controlled trial is the most robust form of evidence of
effectiveness and is increasingly used to evaluate policies (Ludwig, Kling, & Mullainathan,
2011), in many instances, the costs, time constraints, complexity of the policy, or ethical
concerns makes randomized designs impractical to evaluate public policies. In these cases,
natural experiments offer good opportunities for examining policies' impacts. Future
research might focus on a reduced number of states that have good quality administrative
data or population-based survey data on child maltreatment or reasonable proxies for child
maltreatment and where data on the actual implementation of specific policies of interest
could be documented. Combining qualitative methods with quantitative might contribute to
a better understanding of how a policy is implemented and in what context. Such data could
go a long way towards addressing the issues raised above and would contribute to a better
evidence base to inform policies that might affect child maltreatment.
References
Akee RK, Copeland WE, Keeler G, Angold A, Costello EJ. Parents' incomes and children's outcomes: A quasi-experiment using transfer payments from a casino profits. American Economic Journal: Applied Economics. 2010; 2:86–115. [PubMed: 20582231]
Arno PS, Sohler N, Viola D, Schechter C. Bringing health and social policy together: The case of the earned income tax credit. Journal of Public Health Policy. 2009; 30:198–207. [PubMed: 19597453]
Bitler MP, Zavodny M. Child maltreatment, abortion availability, and economic conditions. Review of Economics of the Household. 2004; 2:119–141.
Blank, H. State developments in child care, early education, and school-age care, 2000. 2001. No longer accessible as of September 18, 2013
Centers for Disease Control and Prevention. Definition of policy. 2013. Retrieved from http://intranet.cdc.gov/od/adp/od/policyDef.htm
Chavkin W, Wise PH, Elman D. Policies towards pregnancy and addiction. Sticks without carrots. Annals of the New York Academy of Sciences. 1998; 846:335–340. [PubMed: 9668420]
Costello EJ, Erkanli A, Copeland W, Angold A. Association of family income supplements in adolescence with development of psychiatric and substance use disorders in adulthood among an American Indian population. Journal of the American Medical Association. 2010; 303:1954–1960. [PubMed: 20483972]
Coulton CJ, Crampton DS, Irwin M, Spilsbury JC, Korbin JE. How neighborhoods influence child maltreatment: A review of the literature and alternative pathways. Child Abuse & Neglect. 2007; 31:1117–1142. [PubMed: 18023868]
Cowal K, Shinn MB, Weitzman BC, Stojanovic D, Labay L. Mother–child separations among homeless and housed families receiving public assistance in New York City. American Journal of Community Psychology. 2002; 30:711–730. [PubMed: 12188057]
Klevens et al. Page 9
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
CSDH. Final report of the Commission on Social Determinants of Health. World Health Organization; Geneva: 2008. Closing the gap in a generation: Health equity through action on the social determinants of health.
Drake B, Jonson-Reid M, Way I, Chung S. Substantiation and recidivism. Child Maltreatment. 2003; 8:248–260. [PubMed: 14604173]
Durrant JE. Evaluating the success of Sweden's corporal punishment ban. Child Abuse & Neglect. 1999; 23:435–448. [PubMed: 10348380]
Edleson JL, Gassman-Pines J, Hill MB. Defining child exposure to domestic violence as neglect: Minnesota's difficult experience. Social Work. 2006; 51:167–174. [PubMed: 16858922]
English D, Marshall D, Brummel S, Orme M. Characteristics of repeated referrals to child protective services in Washington state. Child Maltreatment. 1999; 4:297–307.
Ernst JS. Community-level factors and child maltreatment in a suburban county. Social Work Research. 2001; 25:133–142.
Fallon B, Trocmé N, Fluke J, MacLaurin B, Tonmyr L, Yuan YY. Methodological challenges in measuring child maltreatment. Child Abuse & Neglect. 2010; 34:70–79. [PubMed: 20053453]
Feenberg DR, Coutts E. An introduction to the TAXSIM model. Journal of Policy Analysis and Management. 1993; 12:189–194.
Fein DJ, Lee WS. The impacts of welfare reform on child maltreatment in Delaware. Children and Youth Services Review. 2003; 25:83–111.
Freisthler B, Merritt DH, LaScala EA. Understanding the ecology of child maltreatment: A review of the literature and directions for future research. Child Maltreatment. 2006; 11:263–280. [PubMed: 16816324]
Garbarino J, Sherman D. High-risk neighborhoods and high-risk families: The human ecology of child maltreatment. Child Development. 1980; 51:188–198. [PubMed: 7363733]
Gennetian LA, Castells N, Morris PA. Meeting the basic needs of children: Does income matter? Children and Youth Services Review. 2010; 32:1138–1148. [PubMed: 20689675]
Gershoff ET, Aber JL, Raver CC, Lennon MC. Income is not enough: Incorporating material hardship into models of income associations with parenting and child development. Child Development. 2007; 78:70–95. [PubMed: 17328694]
Hoffman DA, Gavin MB. Centering decisions in hierarchical linear models: Implications for research in organizations. Journal of Management. 1998; 24:623–641.
Hussey JM, Marshall JM, English DJ, Knight ED, Lau AS, Dubowitz H, Kotch JB. Defining maltreatment according to substantiation: Distinction without a difference? Child Abuse & Neglect. 2005; 29:479–492. [PubMed: 15970321]
Institute of Medicine. Health insurance is a family matter. National Academy Press; Washington, DC: 2002.
Isaacs, J.; Hahn, H.; Rennane, S.; Steuerle, CE.; Vericker, T. Kids' share 2011: Report on federal expenditures on children through 2010. Brookings Institution and Urban Institute; Washington, DC: 2011.
Jonson-Reid M, Drake B, Kim J, Porterfield S, Han L. A prospective analysis of the relationship between reported child maltreatment and special education eligibility among poor children. Child Maltreatment. 2004; 9:382–394. [PubMed: 15538037]
Kaiser Commission on Medicaid and the Uninsured. Making it simple: Medicaid for children and CHIP: Income eligibility guidelines and enrollment procedures. Findings from a 50-state survey. 2000. Retrieved from http://kff.org/medicaid/report/making-it-simple-medicaid-for-children-and/
Kaiser Commission on Medicaid and the Uninsured. Enrolling children and families in health coverage: The promise of doing more. 2002. Retrieved from http://kff.org/medicaid/report/enrolling-children-and-families-in-health-coverage/
Kaiser Commission on Medicaid and the Uninsured. Preserving recent progress for health coverage of children and parents: New tensions emerge. 2003. Retrieved from http://kff.org/medicaid/report/preserving-recent-progress-for-health-coverage-of/
Kaiser Commission on Medicaid and the Uninsured. Beneath the surface: Barriers threaten to slow progress on expanding health coverage of children and families. 2004. Retrieved from http://kff.org/medicaid/report/beneath-the-surface-barriers-threaten-to-slow/
Klevens et al. Page 10
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Kaiser Commission on Medicaid and the Uninsured. In a time of growing need: State choices influence health coverage access for children and families. 2005. Retrieved from http://kff.org/medicaid/poll-finding/in-a-time-of-growing-need-state/
Kaiser Commission on Medicaid and the Uninsured. Resuming the path to health coverage for children and parents: A 50-state update on eligibility rules, enrollment and renewal procedures, and cost-sharing practices in Medicaid and SCHIP in 2006. 2007. Retrieved from http://kff.org/medicaid/poll-finding/resuming-the-path-to-health-coverage-for/
Kaiser Commission on Medicaid and the Uninsured. Health coverage for children and families in Medicaid and SCHIP: State efforts face new hurdles. 2008. Retrieved from http://kff.org/medicaid/report/health-coverage-for-children-and-families-in/
Kaiser Commission on Medicaid and the Uninsured. Challenges of providing health coverage for children and parents in a recession: A 50 state update on eligibility rules, enrollment and renewal procedures, and cost-sharing practices in Medicaid and SCHIP in 2008. 2009a. Retrieved from http://kff.org/medicaid/report/challenges-of-providing-health-coverage-for-children/
Kaiser Commission on Medicaid and the Uninsured. A foundation for health reform: Findings of an annual 50-state survey of eligibility rules, enrollment and renewal procedures and cost-sharing practices in Medicaid and CHIP for children and parents during 2009. 2009b. Retrieved from http://kff.org/medicaid/report/a-foundation-for-health-reform-findings-of/
Klevens J, Whitaker D. Primary prevention of physical abuse and neglect: Gaps and promising directions. Child Maltreatment. 2007; 12:364–377. [PubMed: 17954942]
Kohl PL, Jonson-Reid M, Drake B. Time to leave substantiation behind: Findings from a national probability study. Child Maltreatment. 2009; 14:17–26. [PubMed: 18971346]
Ludwig L, Kling JR, Mullainathan S. Mechanism experiments and policy evaluations. Journal of Economic Perspectives, American Economic Association. 2011; 25:17–38.
Mair C, Diez Roux AV, Galea S. Are neighborhood characteristics associated with depressive symptoms? A review of the evidence. Journal of Epidemiology and Community Health. 2008; 62:940–946. [PubMed: 18775943]
McAllister C, Thomas T, Wilson P, Green B. Root shock revisited: Perspectives of early head start mothers on community and policy environments and their effects on child health, development, and school readiness. American Journal of Public Health. 2009; 99:205–209. [PubMed: 19059871]
Mistry RS, Vandewater EA, Huston AC, McLoyd VC. Economic well-being and children's social adjustment: The role of family process in an ethnically diverse low income sample. Child Development. 2002; 73:935–951. [PubMed: 12038561]
National Bureau of Economic Research. [Accessed 15.12.12] TAXSIM version 9.0. 2012. http://www.nber.org/~taxsim/taxsim-calc9/index.html
National Institute for Early Education Research. Preschool yearbook. 2003. Retrieved from http://nieer.org/yearbook2003/pdf/yearbook.pdf
National Institute for Early Education Research. Preschool yearbook. 2004. Retrieved from http://nieer.org/yearbook2004/pdf/yearbook.pdf
National Institute for Early Education Research. Preschool yearbook. 2005. Retrieved from http://nieer.org/yearbook2005/pdf/yearbook.pdf
National Institute for Early Education Research. Preschool yearbook. 2006. Retrieved from http://nieer.org/yearbook2006/pdf/yearbook.pdf
National Institute for Early Education Research. Preschool yearbook. 2007. Retrieved from http://nieer.org/yearbook2007/pdf/yearbook.pdf
National Institute for Early Education Research. Preschool yearbook. 2008. Retrieved from http://nieer.org/yearbook2008/pdf/yearbook.pdf
National Institute for Early Education Research. Preschool yearbook. 2009. Retrieved from http://nieer.org/yearbook2009/pdf/yearbook.pdf
National Women's Law Center. State child care assistance policies 2001–2004: Families struggling to move forward, states going backward. 2004. Retrieved from http://www.nwlc.org/resource/child-care-assistance-policies-2001-2004-families-struggling-move-forward-states-going-back
National Women's Law Center. State child care assistance policies 2005: States fail to make up lost ground, families continue to lack critical support. 2006. Retrieved from http://www.nwlc.org/
Klevens et al. Page 11
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

resource/child-care-assistance-policies-2005-states-fail-make-lost-ground-families-continue-lack-cri
National Women's Law Center. State child care assistance policies 2006: Some steps forward, more progress needed. 2007. Retrieved from http://www.nwlc.org/resource/state-child-care-assistance-policies-2007-some-steps-forward-more-progress-needed
National Women's Law Center. State child care assistance policies for 2008: Too little progress for children and families. 2008. Retrieved from http://www.nwlc.org/resource/state-child-care-assistance-policies-2008-too-little-progress-children-and-families
National Women's Law Center. State child care assistance policies 2009: Most states hold the line, some lose ground in hard times. 2009. Retrieved from http://www.nwlc.org/resource/state-child-care-assistance-policies-2009-most-states-hold-line-some-lose-ground-hard-times
Paxson C, Waldfogel J. Work, welfare, and child maltreatment. Journal of Labor Economics. 2002; 20:435–474.
Paxson C, Waldfogel J. Welfare reforms, family resources, and child maltreatment. Journal of Policy Analysis and Management. 2003; 22:85–113.
Porter, T.; Kearns, S. Supporting Family, Friend and Neighbor Caregivers: Findings from a Survey of State Policies. Bank Street College of Education; New York: 2005. Retrieved from: http://www.bankstreet.edu/gems/ICCC/surveypaperfinal.pdf
Reynolds AJ, Robertson DI. School-based early intervention and later child maltreatment in the Chicago longitudinal study. Child Development. 2003; 74:3–26. [PubMed: 12625433]
Robinson, G.; Kaye, N.; Bergman, D.; Moreaux, M.; Baxter, C. State Profiles of Mental Health and Substance Abuse Services in Medicaid. U.S. Department of Health and Human Services; 2005. Retrieved from: http://store.samhsa.gov/product/State-Profiles-of-Mental-Health-and-Substance-Abuse-Services-in-Medicaid/NMH05-0202
Rowe, G.; McManus, K.; Roberts, T. Welfare rules databook as of July, 2001. 2004. Retrieved from http://www.urban.org/UploadedPDF/311110_DP 04-07.pdf
Rowe, G.; Murphy, M. Welfare rules databook as of July, 2006. 2006. Retrieved from http://anfdata.urban.org/databooks/Published%202006%20Databook.pdf
Rowe, G.; Murphy, M. Welfare rules databook as of July, 2008. 2009. Retrieved from http://anfdata.urban.org/databooks/Databook%202008%20FINAL.pdf
Rowe, G.; Murphy, M.; Kaminski, J. Welfare rules databook as of July, 2007. 2008. Retrieved from http://anfdata.urban.org/databooks/Databook%202007%20Final%20Draft%20December%202008.pdf
Rowe, G.; Murphy, M.; Mon, EY. Welfare rules databook as of July, 2009. 2010. Retrieved from http://www.urban.org/UploadedPDF/412252-Welfare-Rules-Databook.pdf
Rowe, G.; Murphy, M.; Williamson, M. Welfare rules databook as of July, 2004. 2006a. Retrieved from http://anfdata.urban.org/databooks/Published%202004%20Databook.pdf
Rowe, G.; Murphy, M.; Williamson, M. Welfare rules databook as of July, 2005. 2006b. Retrieved from http://anfdata.urban.org/databooks/Published%202005%20Databook.pdf
Rowe, G.; Roberts, T. Welfare rules databook as of July, 2000. 2004. Retrieved from http://www.urban.org/UploadedPDF/311111_DP 04-08.pdf
Rowe, G.; Russell, V. Welfare rules databook as of July, 2002. 2004. Retrieved from http://www.urban.org/UploadedPDF/311109_DP 04-06.pdf
Rowe, G.; Versteeg, J. Welfare rules databook as of July, 2003. 2005. Retrieved from http://www.urban.org/UploadedPDF/411183_WRD_2003.pdf
Schulman, K.; Blank, H. Child care assistance policies 2001–2004: Families struggling to move forward, states going backward. National Women's Law Center; Washington, DC: 2004. Retrieved from http://www.nwlc.org/sites/default/files/pdfs/statechildcareassistancepolicies2004.pdf
Seiglie C. Understanding child outcomes: An application to child abuse and neglect. Review of Economics of the Household. 2004; 2:143–160.
Sen B, Wingate MS, Kirby R. The relationship between state abortion-restrictions and homicide deaths among children under 5 years of age: A longitudinal study. Social Science & Medicine. 2012; 75:156–164. [PubMed: 22497846]
Klevens et al. Page 12
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Slack KS, Holl JL, McDaniel M, Yoo J, Bolger K. Understanding the risks of child neglect: An exploration of poverty and parenting characteristics. Child Maltreatment. 2004; 9:395–408. [PubMed: 15538038]
Stith SM, Lui T, Davies C, Boykin EL, Alder MC, Harris JM, Som A, McPherson M, Dees JE. Risk factors in child maltreatment. A meta-analytic review of the literature. Aggression and Violent Behavior. 2009; 14:13–29.
Theodore A, Chang JJ, Runyan DK, Hunter WM, Bangdiwala SI, Agans R. The epidemiology of the physical and sexual maltreatment of children in the Carolinas. Pediatrics. 2005; 115:e331–e337. [PubMed: 15741359]
U.S. Census Bureau. Data ferret. 2011a. Retrieved from http://dataferrett.census.gov/
U.S. Census Bureau. Population by sex, race, and Hispanic origin. 2011b. Retrieved from http://www.census.gov/popest/data/state/asrh/2009/SC-EST2009-03.html
U.S. Census Bureau. Small area income and poverty estimates. 2011c. Retrieved from http://www.census.gov/did/www/saipe/data/statecounty/data/index.html
U.S. Census Bureau. Population estimates: State intercensal estimates (2000–2010): Sex and age. 2012. Retrieved from http://www.census.gov/popest/data/intercensal/state/ST-EST00INT-02.html
U.S. Department of Health and Human Services. The 2009 HHS federal poverty guidelines. 2011a. Retrieved from http://aspe.hhs.gov/poverty/figures-fed-reg.cfm
U.S. Department of Health and Human Services, Administration for Children and Families. Child maltreatment 2000. 2002. Retrieved from http://www.acf.hhs.gov/programs/cb/pubs/cm00/cm2000.pdf
U.S. Department of Health and Human Services, Administration for Children and Families. Child maltreatment 2001. 2003. Retrieved from http://www.acf.hhs.gov/programs/cb/resource/child-maltreatment-2001
U.S. Department of Health and Human Services, Administration for Children and Families. Child maltreatment 2002. 2004. Retrieved from http://www.acf.hhs.gov/programs/cb/resource/child-maltreatment-2002
U.S. Department of Health and Human Services. Administration for Children and Families. Child maltreatment 2003. 2005. Retrieved from http://www.acf.hhs.gov/programs/cb/resource/child-maltreatment-2003
U.S. Department of Health and Human Services. Administration for Children and Families. Child maltreatment 2004. 2006. Retrieved from http://www.acf.hhs.gov/programs/cb/resource/child-maltreatment-2004
U.S. Department of Health and Human Services. Administration for Children and Families. Child maltreatment 2005. 2007. Retrieved from http://www.acf.hhs.gov/programs/cb/pubs/cm05/cm05.pdf
U.S. Department of Health and Human Services. Administration for Children and Families. Child maltreatment 2006. 2008. Retrieved from http://www.acf.hhs.gov/programs/cb/pubs/cm06/cm06.pdf
U.S. Department of Health and Human Services. Administration for Children and Families. Child maltreatment 2007. 2009. Retrieved from http://www.acf.hhs.gov/programs/cb/pubs/cm07/cm07.pdf
U.S. Department of Health and Human Services. Administration for Children and Families. Child maltreatment 2008. 2010a. Retrieved from http://www.acf.hhs.gov/programs/cb/pubs/cm08/cm08.pdf
U.S. Department of Health and Human Services. Administration for Children and Families. Child maltreatment 2009. 2010b. Retrieved from http://www.acf.hhs.gov/programs/cb/resource/child-maltreatment-2009
U.S. Department of Health and Human Services. Administration for Children and Families. Child maltreatment 2010. 2011b. Retrieved from http://www.acf.hhs.gov/programs/cb/resource/child-maltreatment-2010
U.S. Department of Labor. Regional and state unemployment (annual). 2012. Retrieved from http://www.bls.gov/schedule/archives/all_nr.htm#SRGUNE
Klevens et al. Page 13
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
U.S. Department of Labor. Changes in basic minimum wages in non-farm employment under state law. 2013. Retrieved from http://www.dol.gov/esa/whd/state/stateMinWageHis.htm
Vandell DL, Belsky J, Burchinal M, Steinberg L, Vandergrift N, NICHD Early Child Care Research Network. Do effects of early child care extend to age 15 years? Results from the NICHD Study of Early Child Care and Youth Development. Child Development. 2010; 81:737–756. [PubMed: 20573102]
Vinson, M.; Turetsky, V. State child support pass-through policies. Center for Law and Social Policy. 2009. Retrieved from http://www.clasp.org/admin/site/publications/files/PassThroughFinal061209.pdf
Yeung WJ, Linver MR, Brooks-Gunn J. How money matters for young children's development: Parental investment and family processes. Child Development. 2002; 73:1861–1879. [PubMed: 12487499]
Zolotor AJ, Runyan DK. Social capital, family violence, and neglect. Pediatrics. 2006; 117:e1124–e1131. [PubMed: 16740814]
Klevens et al. Page 14
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Klevens et al. Page 15
Table 1
Policies identified, description, data source, and years data available.
Policies Description Data source Years of data available
Reduce poverty
1. Minimum wage Percent above federal minimum income
US Department of Labor 1968–annual
2. Income taxes on low-income households
Percentage of income owed in state income taxes for a family at the federal poverty level
National Bureau of Economic Research (2012)Department of Health and Human Services (poverty threshold)
1977–annual
Threshold for state taxes Income threshold (% above federal poverty line) at which family income becomes subject to the state income tax
Center on Budget and Policy Priorities
1996–annual
Earned Income Tax Credit Tax refund for low to moderate income working individuals and families
Tax credits for working families
Year enacted by state
Child Tax Credit Tax credit per child under 17 years of age
Tax credits for working families
Current
3. Eligibility for TANF Maximum earnings an applicant can receive and still be eligible for benefit
Urban Institute 2000–annual
4. TANF benefits Maximum monthly benefit for a family of three with no income in the month of July
Urban Institute 2000–annual
Work requirement exemptions Exemptions for single parents with young children
Urban Institute 2000–annual
Child support rules Child support collected passed on or not to families receiving TANF assistance/disregard the passed through support income in determining eligibility for and the amount of assistance
Vinson and Turetsky (2009)
2008
Reduce predatory lending Prohibit or cap fees and interest rates for credit cards, payday lenders, pawnshops, title lenders, subprime mortgage lenders, rent-to-own stores
AARP (n.d.)National Conference of State Legislatures (2008, 2011, 2012)
20002007–2012
Increase access to and use of traditional banking services for unbanked populations
No data source found No data
Deconcentrate poverty Use of the Low Income Housing Tax Credit (LIHTC) to locate affordable housing in low poverty neighborhoods
US Department of Housing and Urban Development
1996–2009
Increase stability of residence
Affordable housing Existence and size of trust fund to build or preserve affordable homes
National Council of State Housing Agencies
1993–annual
Targeting federal tax credits to increase the supply of affordable homes for families with restricted access to private housing markets
National Council of State Housing Agencies
1993–annual
Statutes prohibiting discrimination against housing voucher holders
National Housing Law Project
2005, 2010
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Klevens et al. Page 16
Policies Description Data source Years of data available
Subsidized through vouchers or provision of public housing
No source found with state by state data
No data
Statutes preventing mortgage fraud
National Conference of State Legislatures
2000–2011
Provide high quality, affordable child care
5. Access to subsidies Income cutoff for a family of three for child care subsidy as a percentage of state median income
National Women's Law Center
2001–annual
6. Wait list Presence/absence of a wait list for child care assistance
National Women's Law Center
2001–annual
Reimbursement rates Meets/does not meet federal guideline of the 75th percentile of a recent market rate survey
National Women's Law Center
2001–annual
Co-pays % of family income expected to pay for child care
USDHHS/ACF 1999–2000, 2002–2003, 2005–2006
Quality of care Funding provided for tiered reimbursement, quality improvement grants, professional development systems building, care provider scholarships, and/or wage enhancement initiatives
National Women's Law Center
2001–annual
Access to friends, family, or neighbor care
Non-licensed Family Child Care and/or In-Home providers allowed to receive subsidy payments
USDHHS/ACF 2001, FY02–03; FY04–05; FY06–07; FY10–11
Quality of friends, family or neighbor care
Requirements for background checks, health and safety attestation and/or orientation/training required; training, materials and equipment, or career development opportunities offered
Porter and Kearns (2005) 2004
Family and medical leave Paid maternity leave and leave to care for sick children
National Partnerships for Women and Families (2005)
2004, 2006
Provide high quality, affordable Pre-K
Increase access Fund directly or supplement funds to Head Start
USDHHS/ACF 2003, 2005
7. Coverage of pre-K Percent of three and four year olds enrolled in state funded pre-K
National Institute for Early Education Research
2001–annual
8. Quality of pre-K Expenditure in dollars per child adjusted for inflation
National Institute for Early Education Research
2001–annual
Promote comprehensive early learning standards, degree and training requirements for teachers; maximum class size allowed; minimum staff–child ratio; health and support services provided; meals provided; site visits conducted; parental involvement
State plans available at USDHHS/ACFPolicy enactment data not available
Facilitate children's access to health care
9. Eligibility Maximum family income as a percent of the federal poverty line at which children 1–5 are eligible for Medicaid or the State Children's Health Insurance Program (S-CHIP)
Kaiser Commission on Medicaid and the Uninsured
2001–annual
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Klevens et al. Page 17
Policies Description Data source Years of data available
10. Continuity of eligibility Presence/absence of continuous eligibility enables states to ensure continuity of care by providing Medicaid and SCHIP enrollees continuous coverage for, most commonly, 12 months rather than on a month-to-month basis for Medicaid for children/SCHIP
Kaiser Commission on Medicaid and the Uninsured
2000–annual
11. Presumptive eligibility Presence/absence of presumptive eligibility to provide temporary coverage to children and pregnant women under Medicaid and SCHIP until a formal eligibility determination can be made
Kaiser Commission on Medicaid and the Uninsured
2000–annual
Medical home for every child Accessible, family-centered, continuous, comprehensive, coordinated, compassionate, and culturally effective medical care
State-wide effort not identified
No data
Evidence-based services Evidence-based care and services for children with disabilities as defined by the Individual with Disabilities Education Act
DOE, Office of Special Education (only coverage)
1996–annual
Facilitate parent's access to health care
Eligibility for Medicaid Maximum earnings an applicant can receive and still be eligible for benefit
Kaiser Commission on Medicaid and the Uninsured
2001–annual
Access to contraception Required coverage from private health insurance providers or coverage through Medicaid waivers, or increased funding of community-based health clinics
Guttmacher Institute 2001–2002, 2006, 2008
Access to mental health & substance abuse treatment
Provision of outpatient, residential, crisis and/or services for family
Robinson, Kaye, Bergman, Moreaux, and Baxter (2005)
2003
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Klevens et al. Page 18
Table 2
Range and mean scores (SD), adjusted standardized regression coefficients and marginal effects of each policy
alone (and adjusted for similar policies) on child maltreatment investigations.
Policies (unit of measurement) n Range M (SD) Standardized β policy alone/adjusted for similar
policiesa
Marginal effects of policy alone/adjusted
for similar policiesa
Reducing poverty
Minimum wage (% above federal minimum wage)
468 −17 to 54 8.42 (13.67) .02/.01 0.625/0.536
State tax burden ($) for family of 3 at federal poverty line
443 −0.10 to 0.03 −0.005 (0.02) −.05/−.05 −18.111/−17.107
TANF policies
Maximum monthly earnings and still be eligible (US2009$)
459 0.0–1696.86 820.54 (340.31) −.04/−.03 −0.014/−0.014
Maximum monthly benefits for family of 3 (US 2009$)
459 169.40–1149.93 468.41 (176.91) −.04/−.03 −0.002/−0.0001
Access to child care
Income cutoff for child care subsidies for family of 3 (% of state median income)
408 33.82–95.30 57.76 (12.62) −.01/−.01 0.009/−0.030
Wait list for child care (no/yes) 404 0–1 .38 (.49) .07/.07** 3.127**/2.238*
Access to quality pre-K
Enrollment in pre-K for 4-year olds (%) 354 0–71 12.71 (15.97) .02/.01 −0.017/−0.022
Enrollment in pre-K for 3-year olds (%) 354 0–27 2.43 (4.51) .02/.02 0.056/0.087
Expenditure per child in pre-K (US 2009$)
353 0–11,797 3417.54 (2812.41) .02/.01 0.0002/0.0002
Access to health care
Eligibility for Medicaid/SCHIP for children 1–5 years old (% of federal poverty limit)
457 133–300 162.65 (44.10) .01/.03 0.012/0.012
Continuity of eligibility for Medicaid/SCHIP (no/yes)
408 0–1 .32 (.47) −.047*/−.03 −2.551*/−2.504*
Presumptive eligibility for Medicaid/SCHIP (no/yes)
408 0–1 .16 (.37) −.03/−.03 −0.435/−0.271
Notes: Regression coefficients adjusted for state level percent of childhood poverty, high-school graduation among population > 18, unemployment, Black, and Latino population, and the child dependency ratio. Marginal effects represent the change in the child maltreatment investigation rate associated with a one unit change in the independent variable.
aAdjusted for policies in same category (e.g., eligibility, continuity, and presumptive eligibility for Medicaid/SCHIP included in one model).
*p < .05.
**p < .01.
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Klevens et al. Page 19
Table 3
Adjusted standardized regression coefficients and marginal effects and standard errors of each policy alone
(and adjusted for similar policies) on child maltreatment investigations.
Policies (unit of measurement) Standardized β policy alone/adjusted for
similar policiesa
Marginal effects of policy alone/adjusted for similar policies Standard errors in parentheses
Reducing poverty
Minimum wage (% above federal minimum wage) .02/.01 0.625(3.07)/0.536(3.08)
State tax burden ($) for family of 3 at federal poverty line −.05/−.05 −18.111(35.66)/−17.107(35.73)
TANF policies
Maximum monthly earnings and still be eligible (US2009$) −.04/−.03 −0.014(0.01)/−0.014(0.01)
Maximum monthly benefits for family of 3 (US2009$) −.04/−.03 −0.002(0.004)/−0.0001(0.004)
Access to child care
Income cutoff for child care subsidies for family of 3 (% of state median income)
−.01/−.01 0.009(0.05)/−0.030(0.04)
Wait list for child care (no/yes) .07/.07** 3.127**(1.10)/2.238*(1.02)
Access to quality pre-K
Enrollment in pre-K for 4-year olds (%) .02/.01 −0.017(0.03)/−0.022(0.03)
Enrollment in pre-K for 3-year olds (%) .02/.02 0.056(0.21)/0.087(0.21)
Expenditure per child in pre-K (US2009$) .02/.01 0.0002(0.0003)/0.0002(0.0003)
Access to health care
Eligibility for Medicaid/SCHIP for children 1–5 years old (% of federal poverty limit)
.01/.03 0.012(0.01)/0.012(0.01)
Continuity of eligibility for Medicaid/SCHIP (no/yes) −.04*/−.03 −2.551*(1.13)/−2.504*(1.14)
Presumptive eligibility for Medicaid/SCHIP (no/yes) −.03/−.03 −0.435(1.05)/−0.271(1.05)
Notes: Regression coefficients adjusted for state level percent of childhood poverty, high-school graduation among population > 18, unemployment, Black, and Latino population, and the child dependency ratio. Marginal effects represent the change in the child maltreatment investigation rate associated with a one unit change in the independent variable.
aAdjusted for policies in same category (e.g., eligibility, continuity, and presumptive eligibility for Medicaid/SCHIP included in one model).
*p < .05.
**p < .01.
Child Abuse Negl. Author manuscript; available in PMC 2016 February 01.