job satisfaction: how do social workers fare with …
TRANSCRIPT

OMEGA, Vol. 49(4) 327-346, 2004
JOB SATISFACTION: HOW DO SOCIAL WORKERS
FARE WITH OTHER INTERDISCIPLINARY
TEAM MEMBERS IN HOSPICE SETTINGS?
JACQUELYN MONROE, L.S.W., M.S.W., Ph.D.
ROENIA JITTAUN DELOACH, L.M.S.W., M.S.W., Ph.D.
The Ohio State University
ABSTRACT
The purpose of this study was to investigate job satisfaction among hospice
interdisciplinary team members, which included social workers, nurses, and
other professionals (i.e., home health aides and spiritual care providers.)
Interdisciplinary team members (N = 76) from four hospices in the midwest
participated in the study. One way analysis of variance (ANOVA) revealed
that significant differences in satisfaction resulted in the areas of distributive
justice, autonomy, and opportunity between social workers, nurses, and other
interdisciplinary team members.
Collaborations between interdisciplinary members have been a part of hospice
settings since Cicely Saunders of England first developed the “team” concept
in 1967 (Kulys & Davis, 1986). Joint efforts of this nature between diverse
professionals and organizations are essential in the provision of quality services to
ill individuals and have been found to be an important element in improving
service delivery (Cheung, 1990; Fowler, Hannigan, & Northway, 2000). This is
particularly true for terminally ill patients and their families who are involved
with hospice organizations. Since its inception in the United States in 1974,
hospices have utilized interdisciplinary teams, which are typically composed of
the social worker, nurse, chaplain, physician, volunteer director, and patient care
coordinator (Kulys & Davis, 1986). Over the years, however, the allied health
327
� 2004, Baywood Publishing Co., Inc.

professionals on these teams have evolved into what many view as primary
members, while social work has evolved into what some view as ancillary to
these professionals (Abramson, 1993; Reese & Sontag, 2001), which may have
implications for job satisfaction for the social work professional.
This study investigates job satisfaction—the degree to which an individual
experiences pleasure in his or her work (Price & Mueller, 1986a) among social
workers, nurses, and others (i.e., home health aides and spiritual care providers)
who work as interdisciplinary team members in hospice settings. Specifically, the
degree of job satisfaction among social workers in hospice settings is compared
and contrasted with other interdisciplinary team members. The authors also make
recommendations to hospice organizations on how to increase job satisfaction
among social workers in hospice settings based on statistically significant job
satisfaction variables: distributive justice, autonomy, and opportunity.
HOSPICE ORGANIZATIONS
According to the National Hospice and Palliative Care Organization (NHPCO),
there are over 3200 operational hospices in the United States including the District
of Columbia, Puerto Rico, and Guam (NHPCO, 2003). Hospice’s mission is
to meet the multitude of needs and desires of those who are terminally ill for
whom acceptable curative medicinal options have been exhausted. Distinctive to
hospice’s mission is its subsumption of the palliative care philosophy. Palliative
care in hospices is centered on physical, psychological, spiritual, and psycho-
social symptom relief (Kulys & Davis, 1986; NHPCO, 2003). Palliative care
service delivery by hospices is considered the gold standard in care for the
dying patient whose life expectancy is usually six months or less (Ferrell &
Borneman, 2002; Walter, 2003; Wright, 1999). Hospice’s goal is to ensure a “good
death,” which requires allowing for client self-determination while maintaining
the integrity of the whole dying process (Wright, 1999, p. 136). Contrary to
popular belief, hospice’s focus is not on death; hospices actually focus on life
during a person’s last days.
Like all organizations, hospices have evolved over time. These changes involve
trends in service delivery and organizational characteristics (Abel, 1986;
Banaszak-Holl & Mor, 1996; Jennings, 1997; Kaye & Davitt, 1998; Paradis &
Cummings, 1986; Tehan, 1985). In the past, hospice was viewed as unique in that
it offered services that the traditional health care system had neglected, which
included: 1) being a safe haven for the terminally ill; 2) providing supportive
services for the dying patient and his or her families; and 3) delivering services
specific to the needs of dying patients (Rutledge, 2003). Abel (1986) reports that
hospices have become part of the mainstream heath care system nowadays and
consequently have lost some of their uniqueness. Banaszak-Holl and Mor (1996)
list four different types of hospice programs that have emerged. They tend to be
either hospital based or free standing, or centered on skilled nursing or home
328 / MONROE AND DELOACH

health care. Regardless of the type of hospice program, most hospices actually
serve patients in a variety of settings which include patients’ homes, long-term
facilities, and hospitals. All Medicare certified hospices that are regulated by the
Joint Commission for Accreditation of Healthcare Organizations (JCAHO)
mandate that hospice interdisciplinary teams consist of the following core
members: the social worker, registered nurse, pastoral or other counselor, and
physician (Kovacs & Bronstein, 1999; U.S. Department of Health and Human
Services [USDHHS], 2003a, 2003c, 2003d, 2003e, 2003f). The home health aide
is also considered to be an important member of the interdisciplinary team.
Encompassed under “other services” in Medicare terms, these members must
work with registered nurses on interdisciplinary teams to meet the needs of
patients (USDHHS, 2003b).
INTERDISCIPLINARY TEAM MEMBERS (IDT)
In hospice organizations, social workers, nurses, home health aides, and
spiritual care providers tend to be core members on interdisciplinary teams
because they provide direct care on a day-to-day basis. The physician, volunteer,
and medical director are also part of the direct care team, but are not considered
to be core team members because their involvement tends to be on an as needed
basis (Dove, Schneider, & Gitelson, 1985; Hospice Institute of the Florida Sun
Coast, 1996). The IDT provides a variety of services whereby each team member
provides services based on their professional or instructional training. This care
emphasizes communication and collaboration between the patient, family, and
hospice IDT members, which is consistent with the holistic approach to care
(Fowler et al., 2000).
Social Workers
Operating from the social systems perspective whereby the impact of the larger
social system on the client system is always taken into consideration when
working with the individual (Reese & Sontag, 2001), the licensed and oftentimes
Master’s level social work professional provides psychosocial support to patients
and the family in health care settings (Foliart, Clausen, & Siljestrom, 2001;
Mizrahi, 1992). Officially recognized as a “licensed health care profession” by
both Medicaid and Medicare (Mizrahi, 1992), the hospice social worker also
makes clinical assessments, provides referrals, facilitates discharge planning,
ensures continuity of care, serves as an advocate, offers crisis intervention, and
serves as a counselor (Kulys & Davis, 1986). Conducting assessments along with
supportive and therapeutic counseling of patients, in particular, is seen by most
social workers in the social work profession as a primary responsibility (Cowles &
Lefcowitz, 1995). Therapeutic counseling in hospice settings, however, tends to
be minimal due to the debilitating nature of the illness of most hospice patients.
DIFFERENCES IN SATISFACTION / 329

Supporting counseling in these settings is the norm. Other responsibilities of
hospice social workers involve assisting families to constructively cope with
issues surrounding death and dying, which includes helping the family to utilize
community, financial, and legal resources (Dane & Simon, 1991; Hospice Institute
of the Florida Sun Coast, 1996; Rusnack, Schaefer, & Moxley, 1988).
Nurses
The nurse’s primary responsibility is to provide for the patient’s physical
condition and comfort. Therefore, hospice nurses must be highly skilled in
physical assessments and symptom management. They also help to transition
dying patients from curative treatment to palliative treatment (Rutledge, 2003;
Wright, 1999). Using the medical model as a framework, hospice nurses view
illnesses from the disease model.
Responsibilities of the hospice nurse include educating the patient and family
on physical care, medication administration, skin care, nutrition, and equipment
management (Munley, 1983). They also engage in crisis intervention tasks,
advocacy work, and psychoeducational responsibilities like relaying infor-
mation on advanced directives (Kaye & Davitt, 1998; Kulys & Davis, 1986).
Moreover, some function in the role as a therapeutic counselor, the direct care
giver, and a discharge planner in hospice settings (Cowles & Lefcowitz, 1995;
Lafferty, 1998; Wright, 1999).
Home Health Aides
The home-health aide or nurse’s aide provides physical care when there is
a need. From a hierarchal perspective, they are the least trained of nurses. They
typically acquire 75 or more hours of instruction in the basics of health care service
delivery from a high school, vocational-technical school, or community college.
At this level of nursing, home-health aides are required to be certified when
employed by agencies receiving reimbursement from Medicare (Bureau of Labor
Statistics, 2004-05) as in the case of hospice organizations. This team member
tends to provide personal care assistance with activities of daily living (ADLs).
Their duties may include bathing, grooming, mouth care, skin care, and transfers.
Home-health aides may also provide light housekeeping, shopping, and respite
for caregivers. Educating family members on basic care is also one of their
responsibilities as well as providing support and relief for the primary caregiver
(Buckingham, 1985; “RNS, LPNS, and NAS—Oh My!” 2001; Sankar, 1991).
Spiritual Care Providers
Due to Dr. Cicely Saunders’ vision of the connectedness between medicine and
religion, a spiritual component has been part of hospice since its early beginnings
(Driscoll, 2001). Although the professional chaplain has become a key player for
330 / MONROE AND DELOACH

spiritual care delivery in hospice settings, spiritual care delivery still tends to be
the responsibility of the whole team. This explains why some hospice social
workers and nurses feel that pastoral or bereavement counseling is one of their
many responsibilities as interdisciplinary team members (Carroll, 2001; Kulys
& Davis, 1986; Reese & Sontag, 2001). The official spiritual care providers on
most health care teams, nonetheless, tend to be board-certified chaplains who are
called to offer spiritual care and education to patients, their relatives, and staff
(Driscoll, 2001; Wright, 2001). They are responsible for direct counseling,
coordinating care with the patient’s own clergy, offering prayers, assisting in
rites and rituals (e.g., baptisms) of the patient and his or her family, as well as
bereavement services for the dying (Foliart et al., 2001; Lentz, 1999; Sankar,
1991; Wright, 2001).
Although Christian chaplains still dominate the landscape of most organizations
in this country, including the prison system, the military, police departments,
universities, and hospices, they all have started to recognize the diversity
of humans’ spiritual needs (Bellandi, 2000; Coeyman, 2000; Friedman, 2003;
Lapwood, 1982; “Navy Chaplain Named to Serve US Senate,” 2003; Zoba, 2000).
According to chaplains’ code of ethics, chaplains employed in secular institutions
like hospices must refrain from proselytizing or attempting to convert patients to
their faith, but instead they are charged with offering hope and encouragement
to those of any faith or no faith at all (Driscoll, 2001). Spiritual care in hospice
transcends religions and faiths. Hospice’s philosophy of spiritual care is non-
judgmental and focuses on healing, forgiveness, and acceptance (Munley, 1983).
Even an atheist or agnostic can be spiritual according to hospice’s philosophy
(Carroll, 2001). Therefore, the spiritual intervention in hospice is geared toward
helping the patient and family address, deal, or wrestle with spiritual concerns,
questions, or crises (Derrickson, 1996).
METHODS
Agency Selection and Participation
Interdisciplinary team members from four Medicare certified and JCAHO
accredited hospices in the Midwest were asked to participate in the study. These
particular hospices were selected for this study because they were the only
organizations in the area that were adult-based and adhered to the regulatory
guidelines mandated by Medicare and JCAHO. IDT members from these agencies
were also direct-care practitioners who worked with patients in diverse settings
which included the home, long-term care (LTC) facilities, and hospitals. By
selecting these particular hospices, the researchers increased the likelihood of
accessing interdisciplinary team members from all four disciplines (e.g., social
work, nursing, spiritual care, and home-health aide) for inclusion in this study.
DIFFERENCES IN SATISFACTION / 331

During team meetings at each respective hospice, a total of 65 IDT members
completed a self-administered survey. Eleven members who were absent during
initial team meetings mailed in their completed surveys. The final response rate
was 90% (n = 76).
Sample
Seventy six participants completed surveys. As shown in Table 1, females made
up 89.5% of the respondents, while males made up 10.5% of the respondents.
African Americans represented 5.3% of respondents and Caucasians constituted
94.7% of the sample. Nearly 60.5% of the respondents indicated that they were
nurses, 18.4% were social workers, while 21.1% were either home-health aides
or spiritual care providers.
Instrumentation
For the purposes of this study, the dependent variable job satisfaction was
measured using a six-item index adapted by Price and Mueller from Brayfield and
Rothe’s (1951) 18-item index. This instrument measures the global aspect of job
satisfaction. The statements included in this scale were: 1) I find real enjoyment
in my job; 2) I like my job better than the average worker; 3) I am seldom bored
with my job; 4) I would not consider taking another job; 5) Most days I am
enthusiastic about my job; and 6) I feel fairly well satisfied with my job. Response
options on this scale are: 1 = Strongly Agree to 5 = Strongly Disagree. The scores
were summed. The scores ranged from 6 to 30 with a low score (<15) indicating
a high degree of job satisfaction and a high score (15+) indicating a low degree
of satisfaction. Convergent validity and the reliability of this scale have been
established in the literature (Agho, 1989; Price & Mueller, 1986b; Wallace, 1992).
Agho (1989) reported a high level of reliability (Cronbach’s alpha = .90).
The independent variables in this study were pay, distributive justice, internal
labor market, supervisory support, autonomy, integration, opportunity, task sig-
nificance, work motivation, positive affectivity, negative affectivity, role over-
load, role conflict, role ambiguity, and routinization, along with demographic
variables (i.e., age, race/ethnicity, job title,1 education, length of time in current
position, number of years working in hospice settings, employment status, sex,
and ethnicity). Table 2 is an illustration of the variables, definitions, measurements
and the number of items included in the instrumentation used to operationalize
the variables in this study.
As seen in Table 2, several measures were used in the operationalization of
the variables in this study. For the sake of brevity, however, only three of the
332 / MONROE AND DELOACH
1 Home-health aides and spiritual care providers were subsequently combined for the purposes of
data analysis and recoded as “other” because of their low representation in the sample (N = 16).

variables will be examined here. They include distributive justice, autonomy,
and opportunity.
The distributive justice variable was measured using the four-item index
developed by Price and Mueller (1986b) which included questions like: 1) When
compared to the other employees on your team, how do you relate to the fairness
with which you have been treated by your employer in the distribution of the
DIFFERENCES IN SATISFACTION / 333
Table 1. Description of Sample
Respondents N Percent Respondents N Percent
Sex
Females
Males
Total
Ethnicity/Race
African American
Caucasian
Total
Age
26-34
35-44
45-54
55-64
Missing
Total
Job Title
Social worker
Nurse
Other
Total
Level of Education
Advanced
Non-advanced
Total
Employment Status
Full-time
Part-time
Contingency
Total
68
8
76
4
72
76
9
23
32
11
1
76
14
46
16
76
19
55
76
61
11
3
76
89.5
10.5
100.0
5.3
94.7
100.0
11.8
29.3
42.7
14.7
1.3
100.0
18.4
60.5
21.1
100.0
25.0
72.9
100.0
80.3
14.5
3.9
100.0
Number of Years Working
in Hospice Settings
Less than 1 year
1 to 5 years
6 to 10 years
More than 10 years
Total
Length of Time in
Current Position
Less than 1 year
1 to 5 years
6 to 10 years
More than 10 years
Total
Pay (in dollars)
0-5,000
5,000-9,999
10,000-19,999
20,000-29,999
30,000-39,999
40,000-49,999
50,000-59,999
60,000+
Missing
Total
12
29
19
16
76
13
37
17
9
76
2
1
5
12
20
19
11
4
2
76
15.8
38.2
25.0
21.1
100.0
17.1
48.7
22.4
11.8
100.0
2.7
1.3
6.7
16.0
26.3
25.3
14.5
5.3
2.7
100.0

Tab
le2
.D
ep
en
den
tan
dIn
dep
en
den
tV
ari
ab
les
Vari
ab
les
Defin
itio
ns
Measu
rem
en
tin
dex
No
.o
fitem
s
Jo
bsatisfa
ctio
n
Op
po
rtu
nity
Au
ton
om
y
Ro
leam
big
uity
Ro
leco
nflic
t
Ro
leo
verl
oad
Dis
trib
utive
justice
Su
perv
iso
rysu
pp
ort
Ext
en
tto
wh
ich
an
ind
ivid
ualis
ple
ased
with
his
or
her
job
.
Accessib
ility
too
ther
po
sitio
ns
ext
ern
alto
the
org
an
izatio
n.
Th
eext
en
tto
wh
ich
ind
ivid
uals
are
free
tom
ake
decis
ion
s
ab
ou
tth
eir
wo
rk.
Havin
gu
ncle
ar
un
ders
tan
din
go
fth
eexp
ecta
tio
nre
qu
ired
for
on
e’s
role
.
Inco
mp
atib
ility
betw
een
the
ind
ivid
ual’s
role
an
dw
hat
is
exp
ecte
do
fth
em
.
Havin
gto
om
an
yta
sks
toacco
mp
lish
an
dn
ot
en
ou
gh
tim
e
or
reso
urc
es
toco
mp
lete
them
.
Ind
ivid
uals
’p
erc
ep
tio
no
ffa
iran
dju
st
rew
ard
san
dp
un
ish
men
t.
Th
ed
eg
ree
tow
hic
hsu
perv
iso
rp
rovid
es
assis
tan
ce.
Pri
ce
&M
uelle
r(1
98
6b
)
Pri
ce
&M
uelle
r(1
98
6b
)
Tetr
ick
&LaR
occo
(19
87
)
Riz
zo
et
al.
(19
70
)
Riz
zo
et
al.
(19
70
)
Riz
zo
et
al.
(19
70
)
Pri
ce
&M
uelle
r(1
98
6b
)
Ho
use
(19
81
)
6 4 3 4 4 5 4 6
334 / MONROE AND DELOACH

Inte
rnalla
bo
rm
ark
et
Task
sig
nific
an
ce
Inte
gra
tio
n
Pay
Ro
utin
izatio
n
Wo
rkm
otivatio
n
Po
sitiv
eaffectivity
Neg
ative
affectivity
Th
eext
en
tto
wh
ich
ind
ivid
uals
can
mo
ve
up
with
inth
e
org
an
izatio
nan
dh
ave
the
op
po
rtu
nity
toco
ntin
ue
toin
cre
ase
his
or
her
skill
san
dkn
ow
led
ge.
Th
eext
en
tto
wh
ich
the
ind
ivid
ual’s
job
isim
po
rtan
tto
the
org
an
izatio
n.
Clo
se
rela
tio
nsh
ipw
ith
oth
ers
on
the
job
.
Mo
ney
receiv
ed
by
the
ind
ivid
ualin
exc
han
ge
for
serv
ice
pro
vid
ed
toth
eo
rgan
izatio
n.
Deg
ree
tow
hic
ha
job
isre
petitive.
Th
ed
eg
ree
tow
hic
han
ind
ivid
ualm
akes
his
or
her
job
am
ain
part
ofth
eir
life.
Th
eext
en
tto
wh
ich
an
ind
ivid
ualco
ntin
uo
usly
exp
eri
en
ces
hig
hle
vels
ofp
ositiv
eem
otio
ns.
Th
eext
en
tto
wh
ich
an
ind
ivid
ualco
ntin
uo
usly
exp
eri
en
ces
hig
hle
vels
ofn
eg
ative
em
otio
ns.
Ag
ho
(19
89
)
Mo
ttaz
(19
81
)
Pri
ce
&M
uelle
r(1
98
6b
)
Self-r
ep
ort
Pri
ce
&M
uelle
r(1
98
6b
)
Kan
un
go
(19
82
)
Wats
on
et
al.
(19
88
)
Wats
on
et
al.
(19
88
)
3 4 3
Cate
go
ries
5 4
10
10
DIFFERENCES IN SATISFACTION / 335

following rewards?; and 2) When compared to other employees not employed
by hospice, how do you rate the fairness with which you have been treated by
hospice in the distribution of rewards? Questions were computed into one scale.
The scores were summed. The reliability (Cronbach’s alpha of .95; Agho, 1989)
as well as the convergent and discriminant validity for this index have been
demonstrated in the literature (Agho, 1989; Brooke & Price, 1989; Iverson, 1992;
Price & Mueller, 1981).
Autonomy was operationalized using a three-item index adapted by Iverson
(1992) from Tetrick and LaRocco’s (1987) six-item index. Statements for this
scale included: 1) I never control the scheduling of my work; 2) I have little or no
influence over things that affect me on the job; and 3) I have a lot of input in
deciding what tasks or parts of tasks I will do. Statements were computed into
one scale. The scores were summed. The reliability and validity of this scale are
supported in the literature (Iverson, 1992; Tetrick & LaRocco, 1987). Jo (1995)
reported a moderate to high level of reliability (Cronbach’s alpha of .70).
The opportunity variable was measured using a four-item index developed by
Price and Mueller (1986b). Questions for this scale included: 1) How easy would it
be for you to find a job with another employer in this geographical area that is as
good as the one you now have?; 2) How easy would it be for you to find a job with
another employer in the local job market that is better than the one you now have?;
3) How easy would it be for you to find a local job market that is as good as the one
you now have? and; 4) How easy would it be for you to find a job with an employer
outside the local job market that is better than the one you now have? Statements
were computed into one scale for this variable as well. The scores were then
summed. The reliability (Cronbach’s alpha of .87; Agho, 1989) and discriminant
validity of this scale have been demonstrated (Agho, 1989; Iverson, 1992; Price &
Mueller, 1981, 1986a).
RESULTS
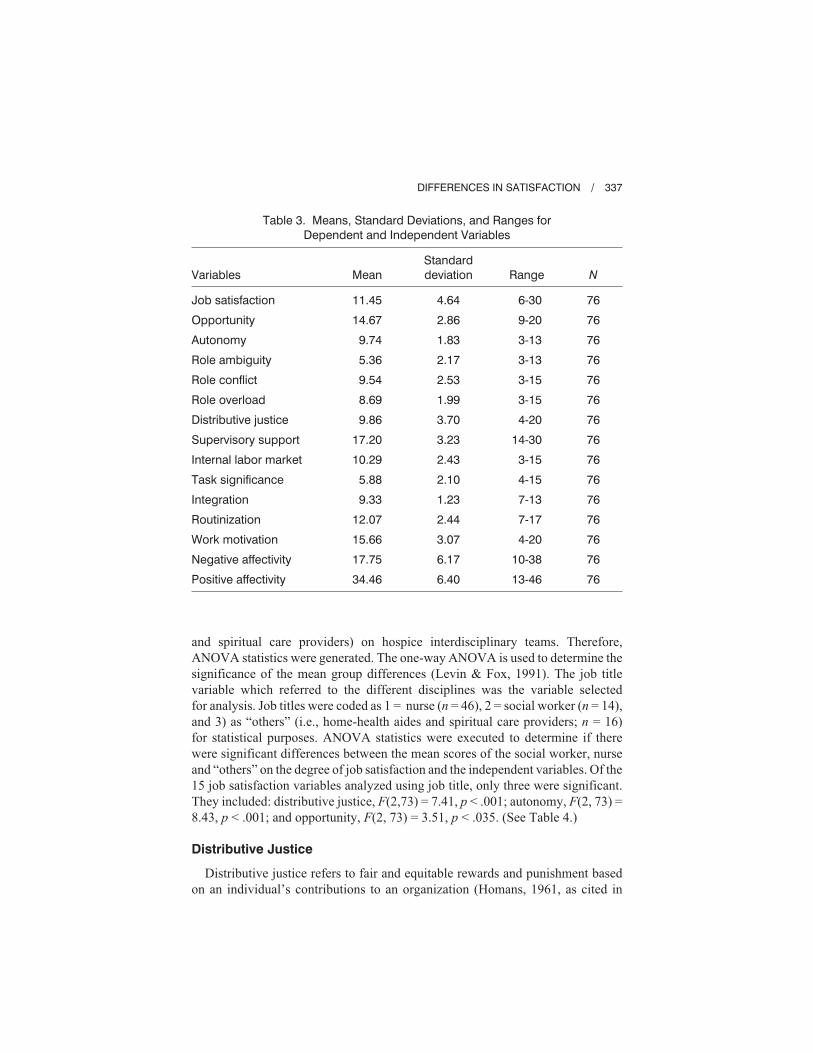
Table 3 shows the means, standard deviations, and ranges for all of the vari-
ables. According to Table 3, respondents reported experiencing a high degree of
satisfaction with their jobs (M = 11.45, SD = 4.64). The possible range for the
measure was from 6 to 30 with a low score (<15) indicating a high degree of job
satisfaction. Specifically, social workers had a mean of 12.57, nurses had a mean
of 11.46, while other professionals had a mean of 10.38. This means that other
team members (i.e., home-health aides and spiritual care providers) as a whole
expressed the most satisfaction with their jobs while nurses followed. Social
workers, however, although satisfied as a whole, were not as satisfied as their
counterparts.
After determining that hospice workers were indeed satisfied, these researchers
sought to determine if differences existed in the degree of job satisfaction
between social workers, nurses, and other professionals (i.e., home-health aides
336 / MONROE AND DELOACH
and spiritual care providers) on hospice interdisciplinary teams. Therefore,
ANOVA statistics were generated. The one-way ANOVA is used to determine the
significance of the mean group differences (Levin & Fox, 1991). The job title
variable which referred to the different disciplines was the variable selected
for analysis. Job titles were coded as 1 = nurse (n = 46), 2 = social worker (n = 14),
and 3) as “others” (i.e., home-health aides and spiritual care providers; n = 16)
for statistical purposes. ANOVA statistics were executed to determine if there
were significant differences between the mean scores of the social worker, nurse
and “others” on the degree of job satisfaction and the independent variables. Of the
15 job satisfaction variables analyzed using job title, only three were significant.
They included: distributive justice, F(2,73) = 7.41, p < .001; autonomy, F(2, 73) =
8.43, p < .001; and opportunity, F(2, 73) = 3.51, p < .035. (See Table 4.)
Distributive Justice
Distributive justice refers to fair and equitable rewards and punishment based
on an individual’s contributions to an organization (Homans, 1961, as cited in
DIFFERENCES IN SATISFACTION / 337
Table 3. Means, Standard Deviations, and Ranges for
Dependent and Independent Variables
Variables Mean
Standard
deviation Range N
Job satisfaction
Opportunity
Autonomy
Role ambiguity
Role conflict
Role overload
Distributive justice
Supervisory support
Internal labor market
Task significance
Integration
Routinization
Work motivation
Negative affectivity
Positive affectivity
11.45
14.67
9.74
5.36
9.54
8.69
9.86
17.20
10.29
5.88
9.33
12.07
15.66
17.75
34.46
4.64
2.86
1.83
2.17
2.53
1.99
3.70
3.23
2.43
2.10
1.23
2.44
3.07
6.17
6.40
6-30
9-20
3-13
3-13
3-15
3-15
4-20
14-30
3-15
4-15
7-13
7-17
4-20
10-38
13-46
76
76
76
76
76
76
76
76
76
76
76
76
76
76
76

Price & Mueller, 1981, 1986b). Individuals contribute to the organization in a
variety of ways such as hard work, experience, and education. The number of
rewards and punishment is not the important element in distributive justice.
Rather, it is the relationship between the two and the individual’s input that
signifies distributive justice (Price & Mueller, 1981). Increased distributive justice
increases the likelihood of an individual being satisfied (Agho, 1989; Price &
Mueller, 1981).
For the relationship between job title and the extent of distributive justice, the
mean was 8.65 for nurses, 11.00 for social workers, and 12.19 for “others.” The
range was 4-20. Low scores mean that the participants perceived the allocation of
benefits to be fair. Therefore, the mean for nurses indicated that this group
perceived the benefits to be the most fair. Nurses, unlike social workers and the
other professionals on the interdisciplinary team felt very satisfied with the way
they were rewarded or penalized (distributive justice) for their contributions to the
agency. This means that these IDT members felt like their contributions to
the agency were equitably rewarded. Social workers and other professionals,
338 / MONROE AND DELOACH
Table 4. Analysis of Variance by Job Title and Satisfaction Variables
Variables Job title / Means
Sum of
squares df
Means
squared F Sig
Distributive
Justice
Social worker / 11.00
Nurse / 8.65
Other / 12.19
Between
Within
Total
171.90
846.87
1018.78
2
73
75
85.95
11.60
7.41 .001
Note: Scores for distributive justice ranged from 4-20 with a low score suggesting fair
distributive justice and a high score suggesting that distributive justice is not fair.
Autonomy Social worker / 9.43
Nurse / 10.33
Other / 8.38
Between
Within
Total
46.96
203.29
250.25
2
73
75
23.48
2.78
8.43 .001
Note: Scores for autonomy ranged from 3-15 with a low score denoting low autonomy
and a high score denoting a lot of autonomy.
Opportunity Social worker / 16.14
Nurse / 14.67
Other / 13.44
Between
Within
Total
54.66
567.76
622.42
2
73
75
27.33
7.78
3.51 .035
Note: Scores for opportunity ranged from 4-20 with a low score suggesting a lot of
opportunity and a high score suggesting little opportunity.

however, did not feel as positive about how they were being rewarded for their
contributions to their respective agencies. They appear to have felt devalued to
some degree.
Autonomy
Autonomy is defined as the degree to which an individual is free to make
decisions about his or her work environment (Van de Ven & Ferry, 1980).
Furthermore, autonomy is viewed as the perceived power that an individual has in
determining how to do his or her job. An individual is perceived to have low
autonomy if others within the organization have control over what and how the job
is done (Agho, 1989). For example, a hospice social worker who is able to
determine how he or she will provide service to a particular patient with little to no
input from a supervisor demonstrates a fair amount of autonomy. In contrast, a
hospice social worker who is instructed on how and when to offer services to
patients demonstrates little autonomy.
For the relationship between job title and the degree of autonomy, nurses had
a mean of 10.33, social workers had a mean of 9.43, and “others” had a mean of
8.38. The range was 3-15. A high score on autonomy means that a participant
believed that he or she had a lot of autonomy. Thus, nurses reported having
the most autonomy while social workers ranked second. The gap between the
means between IDT members for this variable, however, was narrower. Thus,
the means for this variable suggest that social workers and other profes-
sionals (i.e., spiritual care providers and home-health aides) appeared to feel
as though they did not have the same freedom as hospice nurses when it came
to controlling their work environments and making decisions on how to do
their jobs.
Opportunity
Opportunity is referred to as the extent to which jobs are available in the
organizational environment (Price & Mueller, 1986b). The amount of opportunity
that is available depends on the external labor market. The organization in which
the individual is employed has no control over the availabilities of outside jobs.
However, the individual’s personal qualifications may have an effect on the
number of job opportunities available to him or her (Agho, 1989; Price & Mueller,
1981). The literature suggests that few opportunities negatively influence job
satisfaction (Iverson, 1992; Price & Mueller, 1986b).
For the relationship between job title and the degree of opportunity, social
workers had a mean of 16.14, nurses had a mean of 14.67, and “others” had a
mean of 13.44. The range was 4-20. A high score here means that participants
felt that they had few opportunities in the external labor market. Hence, social
workers reported having the least opportunity among the three groups. Thus,
they were the least of the three groups to voice satisfaction about external job
DIFFERENCES IN SATISFACTION / 339

prospects in the organizational environment. Subsequently, many felt that job
opportunities were limited outside their current positions and therefore would
most likely remain in their current positions.
DISCUSSION
According to the Revised Casual Model of Job Satisfaction (Agho, Mueller,
& Price, 1993), which was adapted from Price and Mueller’s Model of Job
Satisfaction (1986b), the following variables contribute to job satisfaction. They
include those that are economical (e.g., pay, distributive justice, and internal labor
market), sociological (e.g., supervisory support, autonomy, integration, oppor-
tunity, and task significance), psychological (e.g., work motivation, positive
affectivity, and negative affectivity), and physiological (e.g., role overload, role
conflict, role ambiguity, and routinization) in nature. In other words, this con-
ceptual framework purports that hospice IDT workers are more likely to be
satisfied with their jobs when they are pleased with their salaries, feel rewarded
for their contributions to the agency, and have potential for other jobs in the
agency. Having supportive supervisors while having flexibility in job respon-
sibilities, having collegial relationships with co-workers, having opportunities
for advancement in one’s skills, and feeling that one’s roles are valued are
also contributors to job satisfaction according to this model. Moreover, being
motivated to work, having positive emotions toward work, having manageable
caseloads, and having distinct roles and a variety of job responsibilities have
also been linked to job satisfaction according to Price and Mueller’s Job Satis-
faction Model.
The purpose of this study, then, was twofold. First, the researchers wanted
to determine if social workers, nurses, and other team members (i.e., home-health
aides and spiritual care providers) were satisfied with their jobs in hospice settings,
and second, to determine if any one group of team members was more satisfied.
The results revealed that all hospice interdisciplinary team members in this
study were satisfied with their jobs, but social workers were the least satisfied
of the three groups. Using ANOVA statistics, significant differences between
professionals emerged along the lines of distributive justice, autonomy, and
opportunity. Specifically, social workers did not feel as satisfied about how
they were rewarded for their contributions to the agency as some of their
counterparts, nor were they as satisfied as their nursing counterparts in their
degree of autonomy. They also reported that they did not feel like they had
as many opportunities for gainful employment external to the organization as
their counterparts. Consistently nurses were more satisfied than social workers
on all three variables. In summation, hospice social workers in this study were
satisfied as a whole, but they did report less satisfaction than their counterparts
on most occasions.
340 / MONROE AND DELOACH

Implications for the Social Work Profession
and Hospice Organizations
The results of this study have implications for the social work profession and
hospice organizations. These implications lie in the practice, administration,
and research arenas. At the practice level, the social worker is vital to the
interdisciplinary process as a core member of hospice interdisciplinary teams. This
is evidenced by Medicare’s requirement of their participation on IDT teams
(Kovacs & Bronstein, 1999). Moreover, social workers perform vital roles in
hospice settings—which include but are not limited to conducting assessments,
counseling, making referrals, advocating for needed services, and discharge
planning (Cowles & Lefcowitz, 1995; Kulys & Davis, 1986)—which are essential
services to terminally ill patients and their families. Therefore, it is important
that individuals with responsibilities of this nature enjoy their work so that
high quality services can be delivered to the patient and his or her family.
As previously mentioned, social workers reported feeling less rewarded
(distributive justice) than their nursing counterparts for their contributions to the
agency. With this in mind, it is critical that interdisciplinary-based agencies like
hospices work harder to validate the paradigm and practices in which social
workers adhere to by developing a healthy appreciation for the unique training
and expertise that these licensed and highly trained social workers bring to the
table as counselors, brokers, advocates, and educators. The development of an
appreciation for social workers’ value system as well as other interdisciplinary
members’ value systems can be achieved, for instance, through interdisciplinary
education. Interdisciplinary education has shown to be an effective strategy for
developing knowledge, appreciation, understanding, and clarity of professional
identities between interdisciplinary team members (Fowler et al., 2000). Increas-
ing social workers’ sense of distributive justice can also be potentially achieved
through 1) higher salaries, 2) professional recognition in the form of awards and
announcements, and 3) professional recognition via acknowledgments at the
agency and/or collegial level, which suggests that social workers’ contributions
are significant and vital to the overall functioning of the organization.
Second, the degree of autonomy in how the professional conducted their affairs
also resulted as being significantly different between IDT members in this study.
Having autonomy is certainly central to social workers, as it is to all IDT members,
due to the fact that a large amount of documentation is required of them due to
Medicaid and Medicare requirements. When hospice agencies allow for autonomy
in the workplace, this energizes practitioners because it conveys a sense of
confidence in the clinician’s abilities and it allows for creativity in intervention
strategies. This ultimately contributes to job satisfaction.
Last, social workers reported that they had fewer opportunities for career
advancement outside their organizations than their colleagues. As a remedy,
hospices must re-examine the medical hierarchy inherent in its agencies and
DIFFERENCES IN SATISFACTION / 341

develop ways to increase the marketability of all of its team members. Specif-
ically, offering opportunities to improve clinical, research, administrative, and
leadership skills of social workers are ways to achieve this. In-services at the
agency level or within the community are also ways to build social workers’ skill
levels. Supporting IDT members’ attendance at local, national, and international
conferences is an excellent venue in which to improve social workers’ skill levels.
Diversifying job responsibilities like appointing more social workers to adminis-
trative posts in hospice settings would also help the social work clinician to
develop a more marketable repertoire of skills.
Recommendations for Future Research
Most studies on hospice settings tend to focus on nurses and other medical
personnel resulting in a major gap in the literature on issues and concerns of social
workers. At this juncture, the literature is scant with information on social workers
in hospice settings despite their preeminent roles on hospice interdisciplinary
teams. Large scale studies are highly suggested as well as qualitative efforts.
Qualitative studies in particular will help the researcher to glean into the core
issues and concerns of hospice social workers. Thus, studies of this nature and
magnitude may be instrumental in helping administrators to better meet the needs
of hospice social workers employed in their organizations, which may have
implications for service delivery.
Limitations
The findings in this study should be judiciously interpreted due to the limita-
tions imposed by the study’s design. For instance, the use of only four adult-based
hospice organizations in the Midwest limits the generalizability of the study.
Any generalizability to hospice interdisciplinary team members in hospices other
than those selected in this study are based on the reader’s interpretation of
similarities and applicability. The researchers involved in this study had no way
of knowing if participants were representative of the many hospice interdisci-
plinary team members employed in hospice settings across the nation. Moreover,
combining home health aides with spiritual care providers and subsequently
re-coding them as “others” because of their low representation in the sample
prevented the researchers from differentiating between members in the final
analyses. Therefore, the results of the study do not reflect the differences in
satisfaction that may or may not exist between these IDT members.
Despite these limitations, these researchers feel that this study is rich in content
and has raised a number of significant issues related to job satisfaction among
hospice social workers and other IDT members. Replication of this study using
more hospices and a larger sample of IDT members from each discipline is
recommended.
342 / MONROE AND DELOACH

REFERENCES
Abel, E. (1986). The hospice movement: Institutionalizing innovation. International
Journal of Health Services, 16(1), 71-85.
Abramson, J. S. (1993). Orienting social work employees in interdisciplinary settings:
Shaping professional and organizational perspectives. Social Work, 38(2), 152-157.
Agho, A. (1989). The determinants of employee job satisfaction: An empirical test of a
causal model. Unpublished doctoral dissertation, University of Iowa, Iowa.
Agho, A., Mueller, C., & Price, J. (1993). Determinants of employee satisfaction: An
empirical test of a causal model. Human Relations, 46(8), 1007-1027.
Banaszak-Holl, J., & Mor, V. (1996). Differences in patient demographics and
expenditures among Medicare hospice providers. Hospice Journal: Physical,
Psychosocial, and Pastoral Care of the Dying, 11(3), 1-19.
Bellandi, D. (2000). A prayerful experience. Modern Healthcare 30(30), 14-16.
Brayfield, A., & Rothe, H. (1951). An index of job satisfaction. Journal of Psychology,
35, 307-311.
Brooke, P., & Price, J. (1989). The determinants of employee absenteeism: An
empirical test of a casual model. Journal of Occupational Psychology, 62, 1-19.
Buckingham, R. (1985). Hospice team practice. In P. Lecca & J. McNeil
(Eds.), Interdisciplinary practice: Issues and trends (pp. 78-93). New York: Praeger
Publishers.
Bureau of Labor Statistics: U.S. Department of Labor. (2004-2005). Occupational
outlook handbook, 2004-05 edition: Nursing, psychiatric, and home health aides. Retrieved
April 11, 2004 from, http://www.bls.gov/oco/ocos165.htm
Carroll, B. (2001). A phenomenological exploration of the nature of spirituality and
spiritual care. Mortality, 6(1), 81-99.
Cheung, K. (1990). Interdisciplinary relationships between social work and other
disciplines: A citation study. Social Work Research & Abstracts, 26(3), 23-30.
Coeyman, M. (2000). Jewelnel Davis: University Chaplain—Columbia University,
New York. Christian Science Monitor, 93(22), 14.
Cowles, L., & Lefcowitz, M. (1995). Interdisciplinary expectations of the medical
social workers in the hospital setting: Part 2. Health & Social Work, 20(4), 279-287.
Dane, B., & Simon, B. (1991). Resident guests: Social workers in host settings. Social
Work, 36(3), 208-213.
Derrickson, B. S. (1996). The spiritual work of the dying: A framework and case
studies. Hospice Journal: Physical, Psychosocial, and Pastoral Care of the Dying, 11(2),
11-30.
Dove, H., Schneider, K., & Gitelson, D. (1985). Identifying patients who need social
work services: An interdisciplinary analysis. Social Work, 30, 214-218.
Driscoll, J. (2001). Spirituality and religion in end-of-life care. Journal of Palliative
Medicine, 4(3), 333-335.
Ferrell, B., & Borneman, T. (2002). Community implementation of home care
palliative care education. Cancer Practice, 10 (1), 20-27.
Foliart, D., Clausen, M., & Siljestrom, C. (2001). Bereavement practices among
California hospices: Results of a statewide survey. Death Studies, 25, 461-467.
Fowler, P., Hannigan, B., & Northway, R. (2000). Community nurses and social
workers learning together: A report of an interprofessional education initiative in South
Wales. Health and Social Care in the Community 8(3), 186-191.
DIFFERENCES IN SATISFACTION / 343

Friedman, G. (2003). Chaplaincy: Facing new—and old—challenges. Corrections
Today, 65(5), 90-91.
Hospice Institute of the Florida Sun Coast. (1996). The Hospice Institute Certification
Program. Largo, FL: Author.
House, J. (1981). Work stress and social support. Massachusetts: Addison-Wesley.
Iverson, R. (1992). Employee intent to stay: An empirical test of a revision of the Price
and Mueller Model. Unpublished doctoral dissertation, University of Iowa, Iowa.
Jennings, B. (1997). Individual rights and the human good in hospice. Hospice
Journal: Physical, Psychosocial, and Pastoral Care of the Dying, 12, 1-7.
Jo, D. (1995). Employee attachment among teachers in South Korea: A comparative
analysis with U.S. teachers. Unpublished doctoral dissertation, University of Iowa,
Iowa.
Kanungo, R. (1982). Measurement of job and work involvement. Journal of Applied
Psychology, 67, 341-349.
Kaye, L. W., & Davitt, J. K. (1998). Comparison of the high-tech service delivery
experiences of hospice and non-hospice home health providers. Hospice Journal: Physical,
Psychosocial, and Pastoral Care of the Dying, 13(3), 1-20.
Kovacs, P., & Bronstein, L. (1999). Preparation for oncology settings: What hospice
social workers say they need. Health & Social Work, 24(1), 57-65.
Kulys, R., & Davis, M. A. (1986). An analysis of social services in hospices. Social
Work, 31, 448-456.
Lafferty, C. L. (1998). Transformational leadership and the hospice R.N. case
manager: A new critical pathway. Hospice Journal: Physical, Psychosocial, and Pastoral
Care of the Dying, 13(3), 35-48.
Lapwood, R. (1982). Chaplain to casualty. British Medical Journal, 285, 194-195.
Lentz, R. (1999). Good counsel. Hospitals & Health Networks, 73(7), 20-22.
Levin, J., & Fox, J. A. (1991). Elementary statistics in social research (5th ed.). New
York: HarperCollins.
Mizrahi, T. (1992). Social work in health care regulation and legislation. Health &
Social Work, 17 (2), 87–92.
Mottaz, C. (1981). Some determinants of work alienation. Sociological Quarterly, 22,
515-529.
Munley, A. (1983). The hospice alternative: A new context for death and dying. New
York: Basic Books.
National Hospice and Palliative Care Organization [NHPCO]. (2003). Facts and
Figures. Retrieved October 20, 2003 from,
http://nhpco.org/i4a/pages/index.cfm?pageid=3362&openpage=3362
Navy chaplain named to serve U.S. Senate. (2003). Christian Century, 120(14), 15.
Paradis, L., & Cummings, S. (1986). The evolution of hospice in America toward
organizational homogeneity. Journal of Health and Social Behavior, 27(4), 370-386.
Price, J., & Mueller, C. (1981). Professional turnover: The case of nurses. New York:
SP Medical and Scientific.
Price, J., & Mueller, C. (1986a). Absenteeism and turnover among hospital employees.
Greenwich, CT: JAI Press.
Price, J., & Mueller, C. (1986b). Handbook of organizational measurement.
Cambridge, MA: Allinger.
344 / MONROE AND DELOACH

Reese, D. J., & Sontag, M. (2001). Successful interprofessional collaboration on the
hospice team. Health & Social Work, 26(3), 167-175.
Rizzo, J., House, J., & Lirtzman, S. (1970). Role conflict and ambiguity in complex
organizations. Administrative Science Quarterly, 15, 150-163.
RNs, LPNs and NAs—Oh my! (2001). Regional Review 11(3), 14.
Rusnack, B., Schaefer, S. M., & Moxley, D. (1988). “Safe Passage”: Social work roles
and functions in hospice care. Social Work in Health Care, 13(3), 3-19.
Rutledge, D. (2003). Models of palliative care: Moving beyond hospice. ONS News,
18(10), 106.
Sankar, A. (1991). Ritual and dying: A cultural analysis of social support for
caregivers. Gerontologist, 31(1), 43-50.
Tehan, C. (1985). Has success spoiled hospice? The Hastings Center Report, 15(5),
10-13.
Tetrick, A., & LaRocco, J. (1987). Understanding, prediction, and control as
moderators of the relationship between perceived stress, satisfaction, and psychological
well-being. Journal of Applied Psychology, 72(4), 538-543.
U.S. Department of Health and Human Services [USDHHS]. (2003a). Centers for
Medicare & Medicaid Services—Condition of Participation: Counseling Services. Code of
Federal Regulations [42CFR418.88], 42(2), 750-751.
U.S. Department of Health and Human Services [USDHHS]. (2003b). Centers for
Medicare & Medicaid Services—Condition of Participation: Home Health Aide and
Homemaker Services. Code of Federal Regulations [42CFR418.94], 42(2), 751.
U.S. Department of Health and Human Services [USDHHS]. (2003c). Centers for
Medicare & Medicaid Services—Condition of Participation: Interdisciplinary Group. Code
of Federal Regulations [42CFR418.68], 42(2), 748.
U.S. Department of Health and Human Services [USDHHS]. (2003d). Centers for
Medicare & Medicaid Services—Condition of Participation: Medical Social Services.
Code of Federal Regulations [42CFR418.84], 42(2), 750.
U.S. Department of Health and Human Services [USDHHS]. (2003e). Centers for
Medicare & Medicaid Services—Condition of Participation: Nursing Services. Code of
Federal Regulations [42CFR418.82], 42(2), 750.
U.S. Department of Health and Human Services [USDHHS]. (2003f). Medicare and
Medicaid Programs; approval of the Joint Commission on Accreditation of Healthcare
Organizations (JCAHO) for deeming authority for hospices. Federal Register, 68(104),
32528-32529.
Van de Ven, A., & Ferry, D. (1980). Measuring and assessing organizations. New
York: Wiley-Interscience.
Wallace, J. (1992). Employee attachment among law firm lawyers: A study of
organizational commitment and intent to stay. Unpublished Doctoral Dissertation,
University of Iowa, Iowa.
Walter, T. (2003). Hospices and rituals after death: A survey of British hospice
chaplains. International Journal of Palliative Nursing 9(2), 80-85.
Watson, D., Clark, L., & Tellegen, A. (1988). Development and validation of brief
measurement of positive and negative affect: The PANAS scale. Journal of Personality and
Social Psychology, 54(6), 1062-1070.
Wright, M. (2001). Chaplaincy in hospice and hospital: Findings from a survey in
England and Wales. Palliative Medicine, 15, 229-242.
DIFFERENCES IN SATISFACTION / 345
Wright, P. (1999). Expanding the role of the home health nurse: Recognizing the
hospice-eligible patient. Journal of Hospice and Palliative Nursing, 1(4), 135-140.
Zoba, W. (2000). More than a badge and a gun. Christianity Today, 44(12), 101-104.
Direct reprint requests to:
Jacquelyn Monroe, L.S.W., M.S.W., Ph.D.
The Ohio State University
College of Social Work
225B Stillman Hall
1947 College Road
Columbus, OH 43210-1162
e-mail: [email protected]
346 / MONROE AND DELOACH
