john matheson director of finance, ehealth and pharmaceuticals
TRANSCRIPT

John MathesonDirector of Finance, eHealth
and Pharmaceuticals

• NHSScotland– 5 million people– £12 billion– 14 Health Boards– 8 Support Boards– Integrated delivery– Moving towards
social care integration

Health and Wellbeing
Local Government
Finance
EducationJustice
Administration
Infrastructure and Capital Investment
Rural Affairs
Culture and External Affairs
Other
Spending – by portfolio
• 33% Local Government• 34% Health and Wellbeing• 8% Education and Lifelong
Learning
• £34 billion• £6,500 for each person in
Scotland• £93 million per day• £129 million per working day

Aims
To deliver the highest quality healthcare services to the people of Scotland
For NHSScotland to be recognised as world-
leading in the quality of healthcare it provides

• Person-Centred - Mutually beneficial partnerships between patients, their families, and those delivering healthcare services which respect individual needs and values, and which demonstrate compassion, continuity, clear communication, and shared decision making.
• Effective - The most appropriate treatments, interventions, support, and services will be provided at the right time to everyone who will benefit, and wasteful or harmful variation will be eradicated.
• Safe - There will be no avoidable injury or harm to patients from healthcare they receive, and an appropriate clean and safe environment will be provided for the delivery of healthcare services at all times.
The Healthcare Quality Strategy for ScotlandThe Healthcare Quality Strategy for Scotland

EVERYONE IS ABLE TO LIVE LONGER HEALTHIER LIVES, AT
HOME, OR IN A HOMELY SETTING
Our ‘2020 Vision’Our ‘2020 Vision’

ROUTE MAP TO THE 20:20 VISION
Primary Care
Quality of care
Integrated Care
Safe Care
Unscheduled & Emergency Care
Health of the Population
Prevention
Early Years
Health Inequalities
Value & Financial Sustainability
Efficiency & Productivity
Innovation
Workforce
12 PRIORITY AREAS FOR ACTION
11/02/13
Person Centred Care
Care for Multiple & Chronic Illnesses

“Give me six hours to chop down a tree and I will spend the first four sharpening the axe”
Abraham Lincoln1809-1865

Efficiency and Productivity Workstreams
Alignment of workstreams with the ‘20:20’ Vision
Prevention and Early Intervention
Health Behaviour Change Smoking Cessation Lifestyle Interventions
Evidence Based Care Low Value Clinical Interventions
Evidence Based Clinical Thresholds NICE/ HIS Standards Patient Safety
Support and Enablers:
• Identify and share good practice
• Innovative approaches to data to identify productive opportunities
• Tools for demonstrating productive gain and benefits realisation
Outpatients, Primary and Community Care
Acute Flow and Capacity Management
Prescribing Shared ServicesProcurement
Productive GP
RTC Community
Reshaping Care
Outpatients
SAS Modernisation
PMS QoF Indicators
Ophthalmic Referrals
LTC eHealth
Demand and Capacity Planning
Day/ Short Stay Surgery/ Ambulatory Care
Enhanced Recovery
Inpatient Capacity and Flow
Orthopaedics
Theatres
National Therapeutic Indicators
PAPS, Formulary and Advisory Network
Secondary and Primary Care Interface
Repeats, Waste and Polypharmacy
Performance Management and Incentives
National Approach and Consistency
HR Services
Facilities
Finance
Social Work
Good Practice
Intensive Improvement Activity
National Contracts Review
Regional Consortia
Dashboards
Workforce Capacity and Modernisation
Leadership and Capability Governance and Engagement
Information and Analytics Benchmarking Baselining Productive
OpportunityWhole Systems
Analysis
Core
W
orks
trea
ms
Enab
ling
Wor
kstr
eam
sCr
oss-
cutti
ng
Wor
kstr
eam
s

“The Scottish Patient Safety Programme is without doubt one of the most ambitious patient safety
initiatives in the world – national in scale, bold in aims, and disciplined in science. It harnesses the
energies and wisdom of Scotland’s health care leaders –NHS executives, QIS experts, clinical
professionals, civil servants, and more – all aligned toward a common vision, making Scotland the
safest nation on earth from the viewpoint of health care.”
Don Berwick

Quarterly Clostridium difficile Infection cases
in Patients aged 65 and over
January – March 2007 to July-September 2012
Cases have decreased by 1,410 – 79.4%
(from 1,775 cases in Jan-Mar 2007 to 365 in Jul-Sept 2012)

The Early Years Collaborative - Ambition
To make Scotland the best place in the world to grow up in by improving outcomes, and reducing inequalities, for all babies, children, mothers, fathers and families across Scotland to ensure that all children have the best start in life and are ready to succeed.
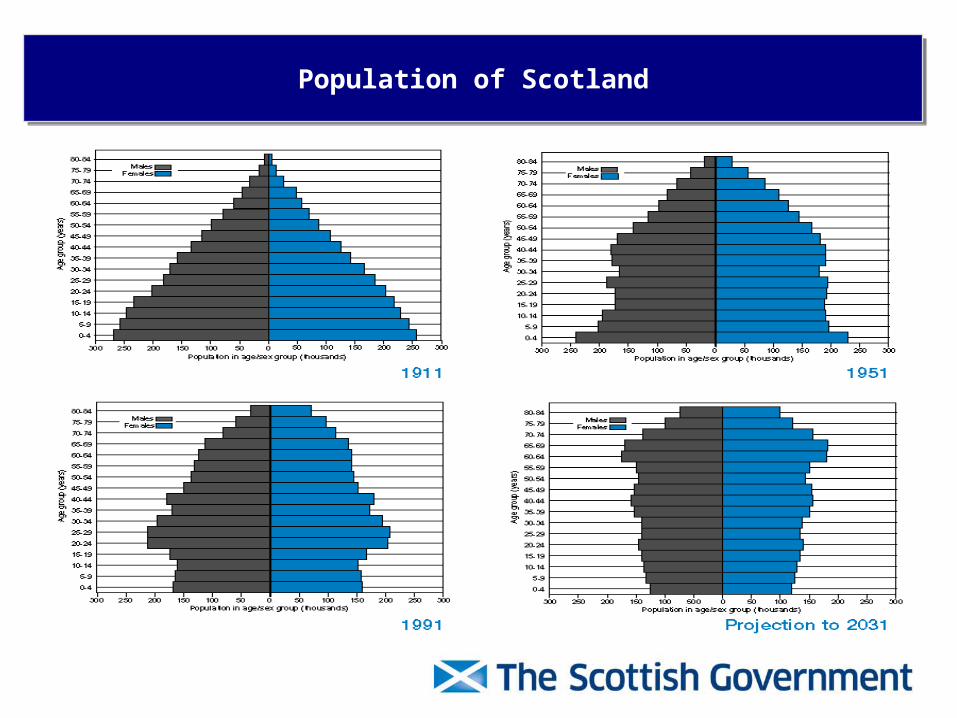
Population of ScotlandPopulation of Scotland

0
1
2
3
4
5
6
7
Glasgow
City
Inverclyde
West D
unbartonshire
Midlothian
Eilean S
iar
East R
enfrewshire
Edinburgh, C
ity of
Renfrew
shire
East Lothian
Scottish B
orders
East D
unbartonshire
Aberdeen C
ity
Dundee C
ity
Argyll &
Bute
South A
yrshire
Highland
Aberdeenshire
West Lothian
Moray
South Lanarkshire
Perth &
Kinross
North A
yrshire
North Lanarkshire
Falkirk
East A
yrshire
Dum
fries & G
alloway
Fife
Orkney Islands
Angus
Stirling
Clackm
annanshire
Shetland Islands
75+
Bed
day
s p
er c
apit
a
ISD 2010/11 IRF mapping data

Public Finances – Fall in Government ExpenditurePublic Finances – Fall in Government Expenditure

Doomed, we’re all doomed
Vision
• People are supported to live well at home or in the community for as much time as they can
• They have a positive experience of health and social care when they need it

• The Reshaping Care Change Fund is a key element within the Scottish Government’s preventative spend strategy – £300 million will be invested over the period 2011-12 to 2014-15.
• Health and Social Care Partnerships across Scotland are using the Fund as bridging finance to make better use of their total combined resources for older people’s services.
• Evidence shows that the Fund is already helping to redesign care services for Scotland's growing older population - helping to prevent delays, provide more proactive community-based services and better care and support at home.
• In line with the Scottish Government's proposals to integrate adult health and social care, the Reshaping Care Change Fund to 2014-15 is now explicitly linked to delivery of joint commissioning strategies.
Reshaping Care Change FundReshaping Care Change Fund

Principles of integration
Services should be planned so that they:
•Are integrated from the point of view of recipients
•Take account of the particular needs of different recipients
•Take account of the particular needs of recipients in different parts of the area in which the service is being provided
•Are planned and led locally in a way which is engaged with the community and local professionals
•Best anticipate needs and prevent them arising, and
•Make the best use of the available facilities, people and other resources

Why integrate resources?
• To share the challenges of managing service delivery in the context of demographic change across primary, secondary and social care, with a real focus on reducing demand and managing services to maximise quality, capacity and effectiveness
• To understand total resource use and patterns of spend and activity, to recognise and address variation that works against principles of wellbeing, and to help identify areas of service that bring the greatest opportunity for redesign to support preventative and anticipatory care, reduce unplanned care and to improve efficiency and effectiveness
• To create a shared incentive that engages all the key players in addressing the continuing pressure in growth and demand throughout the entire system
• To ensure that the most expensive care is used appropriately and maximised at every opportunity

• Evidence– planning for populations, not delivery structures or
functions– pooling resources to support the population based plan– “Hegemony of acute care” - Northern Ireland
• Strategic planning– Each integrated partnership must prepare a strategic
plan setting out how its integrated arrangements will achieve the national health and wellbeing outcomes (s23)
An approach based onintegrated strategic planning

• We must ensure:– provision of safe, sustainable high quality care– shared service planning and delivery more effectively rooted in preventative and
anticipatory care– shared, transparent understanding of spend, activity and variation across the
entire journey of care, particularly for the growing frail older population– strategic planning arrangements that give real traction on the totality of resource
to the integrated partnerships, to deliver a shift in the balance of care and outcomes
– incentives for localities: delivering better outcomes with less use of institutional care must result in a benefit for localities in terms of capacity to invest in preventative care
– local ability to plan using overall spend for defined populations and user groups and to use budgets flexibly
– services designed with and for people and communities, not “delivered top down for administrative convenience”
Challenges (1)

• We must avoid:– planning in terms of historic functional activity rather than
population need– failing to improve on the status quo in terms of unwarranted
variation and the balance of care– opaque understanding of activity and outcomes inhibiting
opportunities to plan for better use of total resources – destabilising management of hospital services– unnecessary transactional complexity– punishment for good performance: delivering better outcomes
with less use of institutional care must be in the best interests of all parties (integrated partnerships; local authorities; health boards)
Challenges (2)
Public Bodies (Joint Working) (Scotland) Bill
• Consultation on health and social care – May to Sept 2012 • Public Bodies (Joint Working) (Scotland) Bill laid before
Scottish Parliament 29 May 2013• First Reading – stage 1 will begin Autumn 2013;
subsequent stages contingent on progress• Second reading - • Enactment – Spring 2015
Still to come: • Secondary legislation• Regulation• Statutory guidance

Legislation Aims to Address
• Inconsistency in the quality of care for people, and the support provided by carers across Scotland particularly in terms of services for older people and adults who access a range of support services across health and social care;
• Unnecessary delays in hospital when people are clinically ready for discharge; and
• Prompt availability of services to enable people to stay safely at home in order to avoid admissions to hospital or care home wherever possible.

Models (Section 1 SS 4)
Body Corporate• Delegation of functions by the local authority to a body corporate that is to
be established by order under section 9 ( an “integration joint board) and delegation of functions by the health board to the integrated joint board”
Delegation between partners• Delegation of functions to local authority to the health boardor• Delegation of functions to health board to the local authority or• Delegation of functions to local authority to the health board and by health
board to the local authority
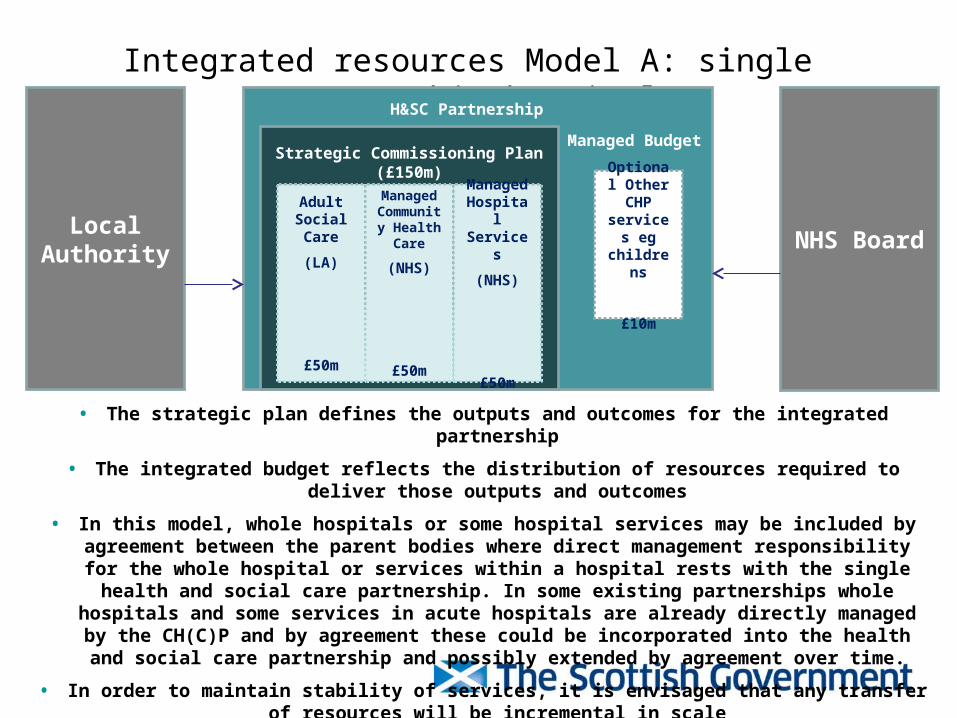
Integrated resources Model A: single partnership hospital
Adult Social Care
(LA)
£50m
Managed Community Health
Care
(NHS)
£50m
Managed Hospital Services
(NHS)
£50m
H&SC Partnership
Optional Other CHP
services eg
childrens
£10m
Strategic Commissioning Plan (£150m)Managed Budget
Local Authority
NHS Board
• The strategic plan defines the outputs and outcomes for the integrated partnership
• The integrated budget reflects the distribution of resources required to deliver those outputs and outcomes
• In this model, whole hospitals or some hospital services may be included by agreement between the parent bodies where direct management responsibility for the whole hospital or services within a hospital rests with the single
health and social care partnership. In some existing partnerships whole hospitals and some services in acute hospitals are already directly managed by the CH(C)P and by agreement these could be incorporated into the health
and social care partnership and possibly extended by agreement over time.
• In order to maintain stability of services, it is envisaged that any transfer of resources will be incremental in scale

NHS Board
Integrated resources Model B: multiple partnership hospital
Local Authority
• The scope of the Strategic Commissioning Plan is the same in Model A and B
• Resource flows are driven by delivery of the agreed Strategic Commissioning Plan
• To avoid disaggregation of hospital services within a single site, the operational management and budgetary responsibility for unscheduled care remains with NHS Board
• The hospital budget for all services in scope of the SCP will be fully transparent to the Chief Officer
Local Authority
Local Authority
Adult Social Care
(LA)
£50m
Managed Community Health
Care
(NHS)
£50m
Managed Hospital Services
£10m
H&SC Partnership
Optional Other CHP
services eg
childrens
£10m
Strategic Commissioning Plan £150mManaged Budget
Hospital Services
£40m
Hospital Services
£40m

• A position statement on managing integrated resources to be agreed by the SG, NHS and local government
• Ongoing work to support effective strategic planning locally – particularly local articulation of agreed objectives to shift the balance of care
• Technical guidance for managing integrated resources
What next?

• Protected Self Interest
• Imbedded Culture
• Tokenistic Change
• No Change at Grass Roots
• Cash Cows
• Clock is Ticking
• Needs recognition that one size just doesn’t fit all
Current IssuesCurrent Issues

Questions?