johnston,2012
TRANSCRIPT
1
TABLE OF CONTENTS PREFACE 3
1 TORTURE 4
TORTURE 4 1.1 CENTRE FOR THE STUDY OF VIOLENCE AND RECONCILIATION (CSVR) 5 TRAUMA AND TRANSITION PROGRAMME (TTP) 5 STATUS OF PEOPLE TORTURED IN THEIR COUNTRY OF ORIGIN 6
2 EFFECTS OF TORTURE 7
2.1 COMMON EFFECTS OF TORTURE 7 OTHER PSYCHOLOGICAL SYMPTOMS 8 2.2 EFFECTS ON FAMILIES 8 CHILDREN’S REACTIONS 9
3 WORKING WITH SURVIVORS OF TORTURE 9
TALKING ABOUT THE TRAUMA 9 SECONDARY TRAUMA IN THE SERVICE PROVIDER 10 WORKING WITH INTERPRETERS 10 THE THERAPEUTIC TRIANGLE 10 SKILLS FOR PROVIDERS 11 SKILLS FOR INTERPRETERS 11 WORKING WITH SURVIVORS OF TORTURE: PSYCHO-‐SOCIAL, LEGAL, MEDICAL AND HUMANITARIAN & ECONOMIC 11
4 WORKING WITH VICTIMS OF TORTURE: A GUIDE FOR MENTAL HEALTH WORKERS 12
4.1 INTRODUCTION 12 GUIDELINES FOR ADAPTING SERVICES 12 4.1.1 ROLES AND RESPONSIBILITIES OF CLIENT AND SERVICE PROVIDER 12 4.2 HEALING 13 4.2.1 STAGES OF RECOVERY 13 4.2.2 FAMILIAR STRATEGIES USED BY MENTAL HEALTH WORKERS TO HELP TORTURE SURVIVORS 13
5 SOME RESOURCES FOR MENTAL HEALTH PROFESSIONALS WORKING WITH VICTIMS OF TORTURE 16
6 WORKING WITH VICTIMS OF TORTURE: A GUIDE FOR MEDICAL PROFESSIONALS 19
6.1 INTRODUCTION 19 6.2 EVIDENCE OF TORTURE 19 6.3 MEDICAL HISTORY 20 6.4 PHYSICAL EXAMINATION 20 6.5 MEDICAL REPORT 21
2
6.6 ETHICAL ISSUES 22 6.7 RIGHTS TO MEDICAL TREATMENT OF PEOPLE IN CUSTODY IN SOUTH AFRICA 23
7 SOME RESOURCES FOR MEDICAL PROFESSIONALS WORKING WITH VICTIMS OF TORTURE 24
8 WORKING WITH VICTIMS OF TORTURE: A GUIDE FOR CARERS IN THE CONTEXT OF HUMANITARIAN ASSISTANCE 28
8.1 INTRODUCTION 28 8.2 SKILLS OF CARERS 28 8.3 PRACTICE OF CARERS 29 SOME QUESTIONS FOR CARERS TO ASK THEMSELVES 29 8.4 ABOUT CARER’S HEALTH AND WELL BEING 30 8.5 ACCOUNTABILITY 30 8.6 SETTING AND MAINTAINING BOUNDARIES 30 8.7 OPPORTUNITIES TO STRENGTHEN CARERS IN PRACTICE 31 8.8 ORGANISATIONAL CULTURE AND BUREAUCRACY 31 8.9 OBSTACLES TO PROFESSIONAL HUMANITARIAN CARING PRACTICE 31 CORRUPTION 31
9 SOME RESOURCES FOR HUMANITARIAN CARERS WORKING WITH VICTIMS OF TORTURE 32
10 WORKING WITH VICTIMS OF TORTURE: A GUIDE FOR LEGAL PRACTITIONERS 37
10.1 INTRODUCTION 37 WHAT IS TORTURE? 37 PERSONS VULNERABLE TO TORTURE IN SOUTH AFRICA 38 10.2 STATES HAVE AN OBLIGATION TO PROTECT GROUPS THAT ARE ESPECIALLY VULNERABLE TO TORTURE 38 10.3 SOUTH AFRICA’S DOMESTIC OBLIGATIONS 39 10.4 PROVIDING LEGAL SERVICES TO VICTIMS OF TORTURE IN SOUTH AFRICA 39 CONSULTING WITH YOUR CLIENT 39 10.5 LEGAL RECOURSE FOR VICTIMS OF TORTURE 40 10.6 THE ROLE OF THE LEGAL PRACTITIONER BEYOND CLIENT REPRESENTATION 40
11 SOME RESOURCES FOR LEGAL PRACTITIONERS WORKING WITH VICTIMS OF TORTURE 41
12 APPENDICES 43
12.1 APPENDIX 1 43 12.2 APPENDIX 2 46
3
Preface This book is an introduction to torture and working with torture survivors. It aims to encourage service providers to treat survivors of torture with dignity and respect, and to promote their empowerment. It is intended as a tool for provoking thought and facilitating learning. It is not an instruction manual. Pravilla Naicker from the Trauma Clinic at the Centre for the Study of Violence, compiled sections one, two and three, Torture; Effects of torture; Working with survivors of torture. These sections were compiled by gathering content from Healing the Hurt a publication of The Centre for Victims of Torture in the USA, and from Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa, a publication of SANToC, The South African No Torture Consortium. Pravilla Naicker also compiled Section four, Working with victims of torture: a Guide for mental health workers by drawing on the content of Healing the Hurt a publication of The Centre for Victims of Torture in the USA, and on Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa, a publication of SANToC, The South African No Torture Consortium. Marivic Garcia from the Trauma Clinic at the Centre for the Study of Violence compiled section five, Working with victims of torture: A Guide for medical professionals by drawing on the content of International Rehabilitation Council for Torture Victims publication entitled Model Curriculum on the Effective Medical Documentation of Torture and Ill-‐Treatment, Educational Resources for Health Professionals Students, Prevention through Documentation Project 2006-‐2009, and from Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa, a publication of SANToC, The South African No Torture Consortium. Josie Adler, social development consultant, and Libby Johnston, supervisor at the Refugee Aid Organsiation, wrote Section six, Working with victims of torture: a guide for carers in the context of humanitarian assistance. They wrote this section based on an interview Josie Adler conducted with Libby Johnston. Nicola Whittaker of Human Rights and Democratisation in Africa, University of Pretoria, wrote section 7, Working with victims of torture: a guide for legal practitioners. Eulinda Smith clinical manager, Boitumelo Kekana and Gaudence Uwizeye of the Trauma Clinic, Centre for the Study of Violence and Reconciliation, provided input and support for the production of this book. Megan Bantjes community manager at the Trauma Clinic, Centre for the Study of Violence and Reconciliation provided assistance and guidance on important data contained in the book. This book was made possible by the generous financial assistance of USAID.
4
1 TORTURE
The United Nations Convention against Torture and other Cruel, Inhuman and Degrading Treatment of Punishment (UNCAT, 1984) defines
Torture as “…any act by which severe pain or suffering, whether physical or mental, is intentionally inflicted on a person for such purposes as obtaining from him or a third person information or a confession, punishing him for an act he or a third person has committed, or intimidating or coercing him or a third person for any reason based on discrimination of any kind, when such pain or suffering is inflicted by or at the instigation of or with the consent or acquiescence of a public official or other person acting in an official capacity”.1
Torture • Causes severe mental and/or physical pain or suffering; • Is intentionally inflicted; • Is inflicted for a purpose or reason; • Is committed by, or, at the instigation of, or with the consent of, or compliance of a
public official or other person acting in an official capacity.
Who tortures? • Police • Military • Paramilitary forces • Special forces/intelligence personne • Prison officials • Death squads • Health professionals (including psychologists) • Co-‐detainees • Rebel forces
Who is being tortured? Anyone who is deprived of their liberty is vulnerable to being tortured, that is, people held involuntarily in places such as:
• places of safety for children • police holding cells, prisons • lock up psychiatric hospitals • drug rehabilitation centres • holding facilities for migrants (for example Lindela) • war captives/hostages • people are also tortured in their homes, in public places (like at political rallies or in the
street) • anyone is vulnerable to torture if torture is perpetrated in the country in which they live in,
for example Zimbabwe and South Africa • Women, men, children 2
1 United Nations Convention Against Torture and other Cruel, Inhuman and Degrading Treatment or Punishment (UNCAT), adopted and opened for signature, ratification and accession by General Assembly Resolution 39/46 of 10 December 1984. 2 Megan Bantjes, Community Manager, CSVR (powerpoint presentation).
5
1.1 Centre for the Study of Violence and Reconciliation (CSVR) Trauma and Transition Programme (TTP)
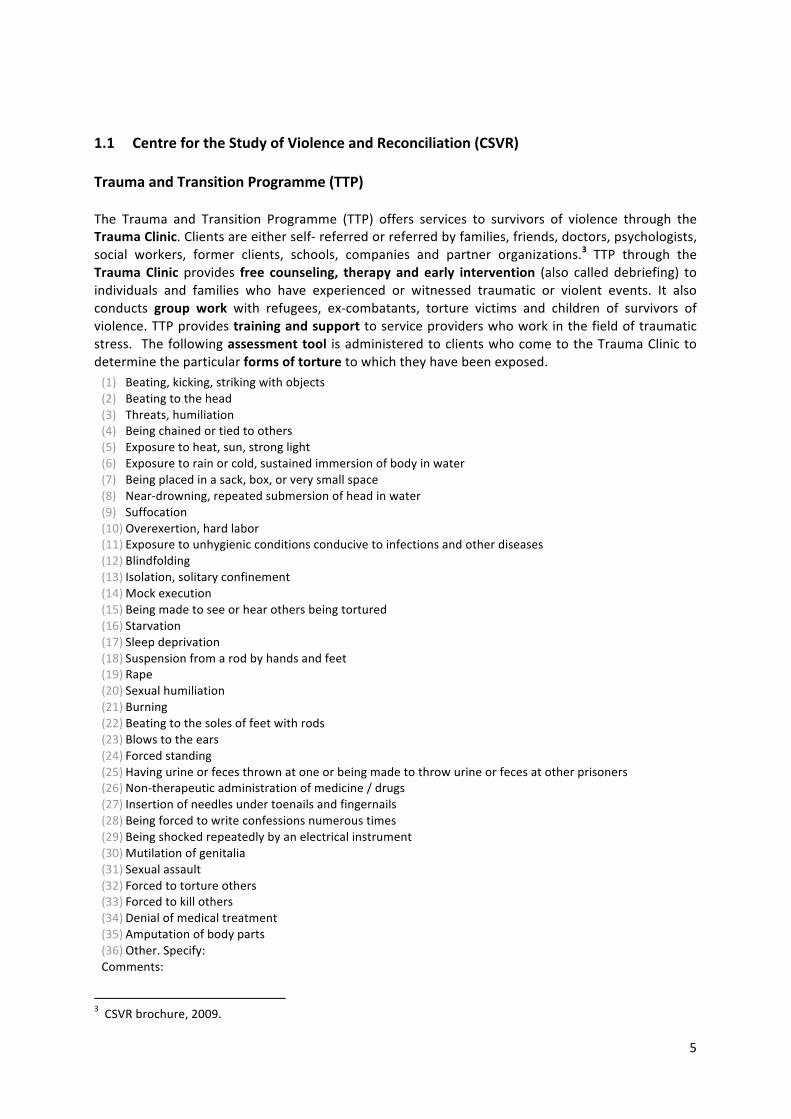
The Trauma and Transition Programme (TTP) offers services to survivors of violence through the Trauma Clinic. Clients are either self-‐ referred or referred by families, friends, doctors, psychologists, social workers, former clients, schools, companies and partner organizations.3 TTP through the Trauma Clinic provides free counseling, therapy and early intervention (also called debriefing) to individuals and families who have experienced or witnessed traumatic or violent events. It also conducts group work with refugees, ex-‐combatants, torture victims and children of survivors of violence. TTP provides training and support to service providers who work in the field of traumatic stress. The following assessment tool is administered to clients who come to the Trauma Clinic to determine the particular forms of torture to which they have been exposed.
3 CSVR brochure, 2009.
(1) Beating, kicking, striking with objects (2) Beating to the head (3) Threats, humiliation (4) Being chained or tied to others (5) Exposure to heat, sun, strong light (6) Exposure to rain or cold, sustained immersion of body in water (7) Being placed in a sack, box, or very small space (8) Near-‐drowning, repeated submersion of head in water (9) Suffocation (10) Overexertion, hard labor (11) Exposure to unhygienic conditions conducive to infections and other diseases (12) Blindfolding (13) Isolation, solitary confinement (14) Mock execution (15) Being made to see or hear others being tortured (16) Starvation (17) Sleep deprivation (18) Suspension from a rod by hands and feet (19) Rape (20) Sexual humiliation (21) Burning (22) Beating to the soles of feet with rods (23) Blows to the ears (24) Forced standing (25) Having urine or feces thrown at one or being made to throw urine or feces at other prisoners (26) Non-‐therapeutic administration of medicine / drugs (27) Insertion of needles under toenails and fingernails (28) Being forced to write confessions numerous times (29) Being shocked repeatedly by an electrical instrument (30) Mutilation of genitalia (31) Sexual assault (32) Forced to torture others (33) Forced to kill others (34) Denial of medical treatment (35) Amputation of body parts (36) Other. Specify: Comments:
6
TTP’s offers services to people who have been tortured in South Africa and, or, to people who have been tortured in their country of origin.
Torture in South Africa In South Africa there is irrefutable evidence that links torture to repressive rule under apartheid4. Post apartheid the democratic South African government took a position against torture by:
• Enshrining the right not to be tortured, not to be treated or punished in a cruel inhuman or degrading way in the SA Constitution (Section12)
• Signing and ratifying UNCAT and • By participating in drawing up the Robben Island Guidelines, which provide guidelines and
measures for the prohibition and prevention of torture and cruel, inhuman or degrading treatment and punishment in Africa.
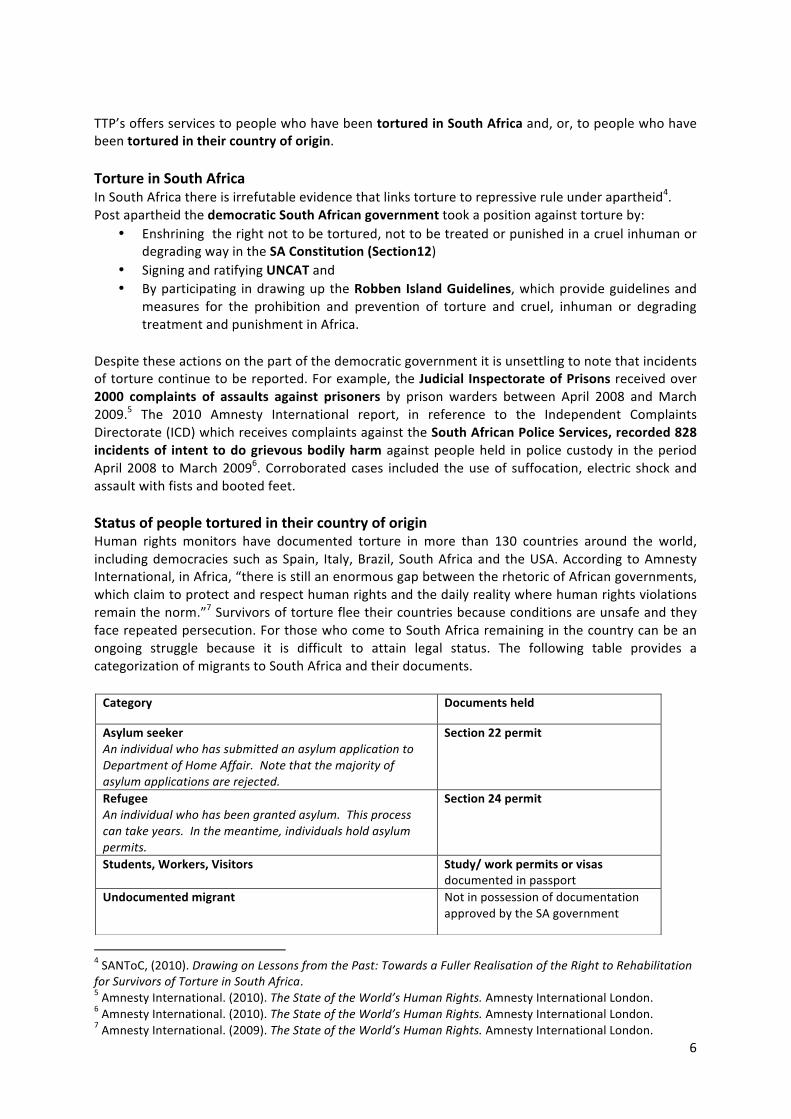
Despite these actions on the part of the democratic government it is unsettling to note that incidents of torture continue to be reported. For example, the Judicial Inspectorate of Prisons received over 2000 complaints of assaults against prisoners by prison warders between April 2008 and March 2009.5 The 2010 Amnesty International report, in reference to the Independent Complaints Directorate (ICD) which receives complaints against the South African Police Services, recorded 828 incidents of intent to do grievous bodily harm against people held in police custody in the period April 2008 to March 20096. Corroborated cases included the use of suffocation, electric shock and assault with fists and booted feet. Status of people tortured in their country of origin Human rights monitors have documented torture in more than 130 countries around the world, including democracies such as Spain, Italy, Brazil, South Africa and the USA. According to Amnesty International, in Africa, “there is still an enormous gap between the rhetoric of African governments, which claim to protect and respect human rights and the daily reality where human rights violations remain the norm.”7 Survivors of torture flee their countries because conditions are unsafe and they face repeated persecution. For those who come to South Africa remaining in the country can be an ongoing struggle because it is difficult to attain legal status. The following table provides a categorization of migrants to South Africa and their documents.
4 SANToC, (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa. 5 Amnesty International. (2010). The State of the World’s Human Rights. Amnesty International London. 6 Amnesty International. (2010). The State of the World’s Human Rights. Amnesty International London. 7 Amnesty International. (2009). The State of the World’s Human Rights. Amnesty International London.
Category Documents held
Asylum seeker An individual who has submitted an asylum application to Department of Home Affair. Note that the majority of asylum applications are rejected.
Section 22 permit
Refugee An individual who has been granted asylum. This process can take years. In the meantime, individuals hold asylum permits.
Section 24 permit
Students, Workers, Visitors Study/ work permits or visas documented in passport
Undocumented migrant Not in possession of documentation approved by the SA government

7
2 EFFECTS OF TORTURE
Torture affects individual survivors, their families and whole societies. Extensive work and research with people who have been tortured, and work in repressed societies and communities, whose members have been tortured, identifies common and unique physical and psychological symptoms and effects on families and societies. It is important to remember that torture survivors do not present with either physical or psychological symptoms. Torture impacts on the psyche and the body simultaneously and its effects extend beyond the individual to impact on families and communities.
2.1 Common effects of torture 8 Posttraumatic stress disorder Depression Physical Symptoms Reliving the trauma: Nightmares Bad thoughts or memories of the torture come into your mind Acting or feeling like the torture is happening all over again flashbacks) Avoiding the trauma: Trying to forget the torture, trying not to think about it Staying away from anything that reminds you of the torture Cannot remember important things that happened during the torture Numbness: Feeling like you do not care about life or what happens to you Feeling like no one understands or cares about you, like you are alone and cut off from others Feeling numb, like there are no feelings inside you Feeling like you have no future or that you may die sooner than most people Heightened arousal: Difficulty falling asleep or staying asleep at night Feeling angry a lot, easily upset Difficulty concentrating Can’t relax or feel comfortable, often afraid something bad will happen
Feeling sad or angry Difficulty thinking or making decisions Difficulty concentrating or Feeling worthless or Hopeless Feeling excessive guilt Feeling that you do not care about life, that you are not interested in things Feeling too hungry or not hungry at all, gaining or losing a lot of weight without trying to Sleeping too much or too little Feeling tired a lot, not having energy Thinking about death a lot, thinking about killing yourself (suicidal thoughts)
Headaches Feeling dizzy, faint or weak Chest pain Heart beats very fast Stomach hurts or feeling sick in the stomach Shaking or trembling Hands or feet feel cold Hot or burning feelings Numb or tingling sensations Sweating Diffuse or generalized sense of pain, weakness, misery Other pains in the body
8 The Centre for Victims of Torture. (2005). Healing the hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt.
8
Posttraumatic stress disorder and depression are amongst the better known and named effects of torture. It is important to remember that not all torture survivors have posttraumatic stress disorder or all of the symptoms of posttraumatic stress disorder. This does not mean they have not been affected. There are diverse psychological and emotional symptoms they may experience including. Other psychological symptoms
• Anxiety• Unusual fears and phobias • Feeling self blame • Feeling ashamed • Feeling aggressive towards others • Unable to relate to others resulting in breakdown in inter-‐personal relationships • Unable to engage in intimate relationships • Substance abuse disorders including drug and alcohol addiction
The physical symptoms with which torture survivors present can be results of actual damage done to their bodies by torturers and can be bodily expressions of emotions. Symptoms of physical damage include: Head injuries; Spinal cord injuries; Loss of vision; Loss of hearing; Bone fractures; Muscle damage Dislocation of joints; Weakness in limbs; Skin damage; Difficulties urinating; Difficulties in moving bowels; Damage to sexual and reproductive organs – uterus, vagina, breast, penis, scrotum; Venous problems, necrosis in the feet or toes.
2.2 Effects on families
The effects of torture on individuals radiate into the family system. Survivors with altered identities, lost dignity and shame find it difficult to take up their previous positions and roles in the family system. Where survivors lose occupational functioning financial burdens create added tensions. Pain, anger and grief not processed, are acted out in verbal or physical abuse. Family members themselves cannot bear to hear stories of trauma reinforcing the silence, and thereby negating the survivor’s experience. Without family support symptoms are reinforced. 9 As a result there can be MARITAL OR INTERGENERATIONAL CONFLICT. PARENTAL FUNCTIONING IS AFFECTED with the result that parents are often less emotionally attuned and attentive to children. Parents have LOW TOLERANCE for negative emotions. For example a parent can’t stand to hear a baby cry because it may reminds the survivor of other prisoners’ screams. There is SILENCE WITHIN the family regarding the torture and other trauma leading to confusion misunderstanding, multiple versions of what happened, and unaddressed blame, shame, anger, disappointment, and sadness. PARENT-‐CHILD ROLE REVERSAL occurs because parents experience disempowerment due to trauma-‐related symptoms and the loss of their traditional roles in a new culture. Children prematurely assume adult roles due to more rapid language acquisition and acculturation. Children’s IDENTITY DEVELOPMENT is affected. Children experience LOSS OF BASIC TRUST. There can be PRESSURE ON CHILDREN to be immune to effects of the family’s ordeals, to succeed and to makeup for what the family lost. 10
9 SANToC, (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa. 10 The Centre for Victims of Torture. (2005). Healing the hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt.
9
Children’s reactions
Anxiety Psychosomatic symptoms Sleeping problems Problems in school Depressive features Problems in the family Regressive features Behavioural changes11
3 WORKING WITH SURVIVORS OF TORTURE
The first ethical obligation of service providers and professionals is to ensure no harm to patients or clients. This includes not causing further psychological or emotional harm through the way that torture survivors are treated, and ensuring that state officials do not expose them to torture.
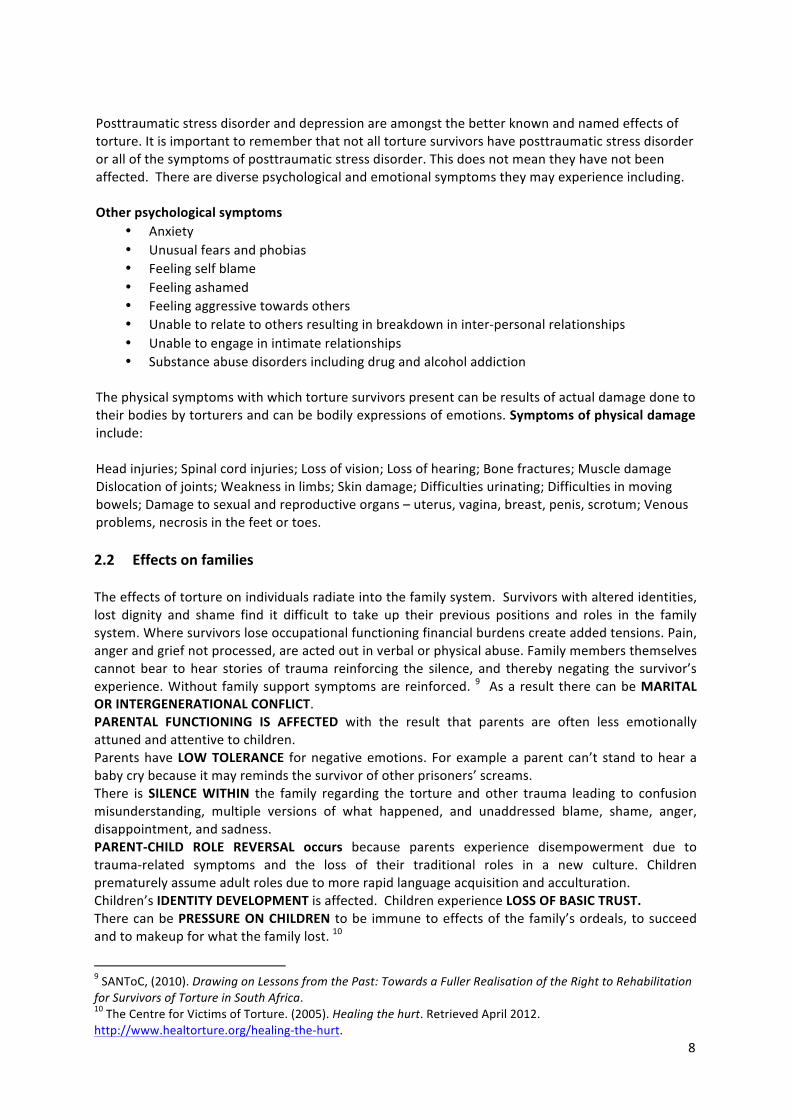
Knowledge of the life experiences and resettlement issues of refugees and asylum seekers before, during, and after the violence is important. The Triple Trauma Paradigm describes three phases of traumatic stress that apply to torture survivors – pre-‐flight, flight and post-‐flight12.
Pre -‐flight
Harassment/intimidation Fear of unexpected arrest Loss of job/livelihood Loss of home and possessions Disruption of studies, life dreams Repeated relocation Living in hiding/underground Societal chaos/breakdown Prohibition of traditional practices Lack of medical care Separation, isolation of family Malnutrition Need for secrecy, silence, Being followed or monitored Imprisonment Torture and other violence Witnessing violence
Flight Fear of being caught or returned Living in hiding Detention borders Loss of home, possessions Loss of job/schooling Illness Robbery exploitation: bribes, falsification Physical assault, rape, or injury Witnessing violence Lack of medical care Separation of family Malnutrition Crowded, unsanitary conditions Uncertainty about future
Post-‐flight Low social and economic status Lack of legal status Language barriers Transportation, service barriers Loss of identity, roles Un-‐/under-‐employment Racial/ethnic discrimination Inadequate, dangerous housing Repeated relocation/migration Social and cultural isolation Family separation/reunification Unresolved losses Conflict: marital, family Unrealistic expectations from home Shock of new climate, geography Symptoms often worsen
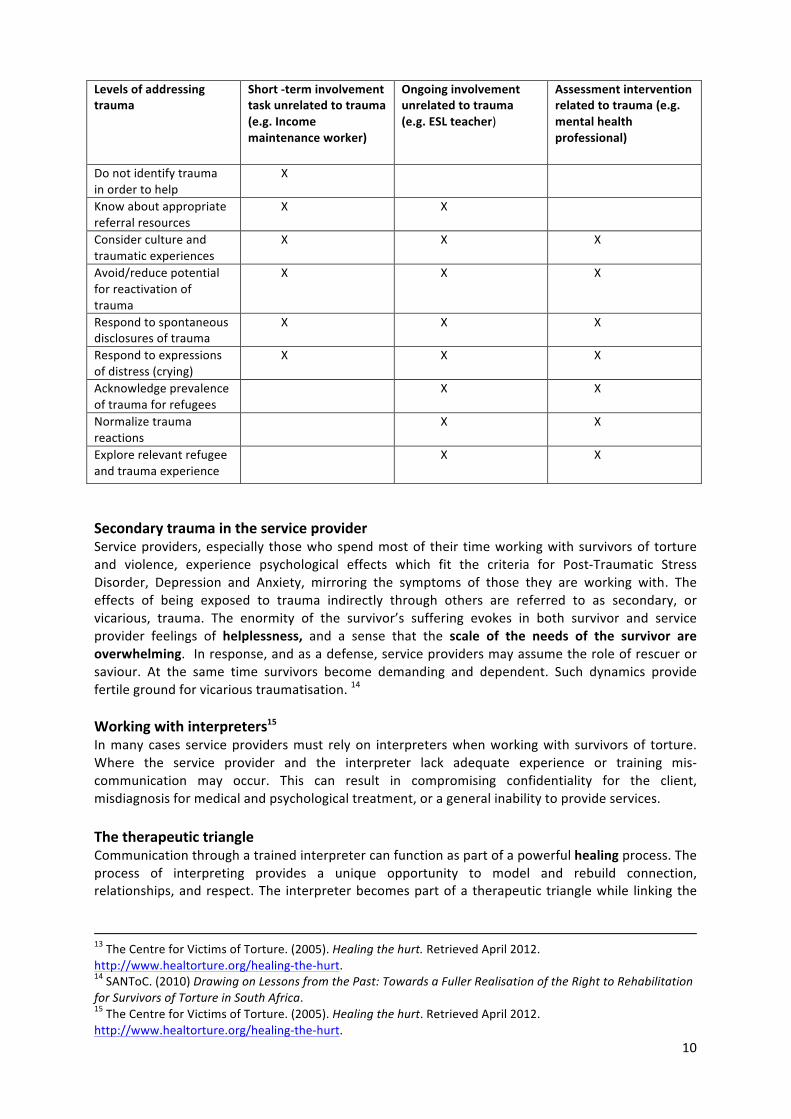
Talking about the trauma
Comprehension of torture and its long-‐term effects on survivors, their families, their community is vital. However, it is not always necessary or even appropriate to address the trauma directly. Addressing torture trauma must be tailored to the setting and the services provided. Minimizing the potential for re-‐traumatization can be addressed through: • Short-‐term involvement • Ongoing involvement unrelated to trauma symptoms, and • Involvement that specifically addresses some aspect of the trauma, whether expressed or not. 13
11 The Centre for Victims of Torture. (2005). Healing the hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt 12 The Centre for Victims of Torture. (2005). Healing the hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt
10
Levels of addressing trauma
TRAUMA
Short -‐term involvement task unrelated to trauma (e.g. Income maintenance worker)
Ongoing involvement unrelated to trauma (e.g. ESL teacher)
to Trauma
Assessment intervention related to trauma (e.g. mental health professional)
Do not identify trauma in order to help
X X
Know about appropriate referral resources
X X
Consider culture and traumatic experiences
X X X
Avoid/reduce potential for reactivation of trauma
X X X
Respond to spontaneous disclosures of trauma
X X X
Respond to expressions of distress (crying)
X X X
Acknowledge prevalence of trauma for refugees
X X
Normalize trauma reactions
X X
Explore relevant refugee and trauma experience
X X
Secondary trauma in the service provider Service providers, especially those who spend most of their time working with survivors of torture and violence, experience psychological effects which fit the criteria for Post-‐Traumatic Stress Disorder, Depression and Anxiety, mirroring the symptoms of those they are working with. The effects of being exposed to trauma indirectly through others are referred to as secondary, or vicarious, trauma. The enormity of the survivor’s suffering evokes in both survivor and service provider feelings of helplessness, and a sense that the scale of the needs of the survivor are overwhelming. In response, and as a defense, service providers may assume the role of rescuer or saviour. At the same time survivors become demanding and dependent. Such dynamics provide fertile ground for vicarious traumatisation. 14 Working with interpreters15 In many cases service providers must rely on interpreters when working with survivors of torture. Where the service provider and the interpreter lack adequate experience or training mis-‐communication may occur. This can result in compromising confidentiality for the client, misdiagnosis for medical and psychological treatment, or a general inability to provide services. The therapeutic triangle Communication through a trained interpreter can function as part of a powerful healing process. The process of interpreting provides a unique opportunity to model and rebuild connection, relationships, and respect. The interpreter becomes part of a therapeutic triangle while linking the
13 The Centre for Victims of Torture. (2005). Healing the hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt. 14 SANToC. (2010) Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa. 15 The Centre for Victims of Torture. (2005). Healing the hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt.

11
provider and client in communication. A relationship of confidence and trust amongst those involved can help the survivor to experience the safety needed to engage effectively in treatment.
Skills for providers There is a need for frequent and thorough communication between provider and interpreter. Most training sources stress the importance of attending to three sequential stages of work for providers and interpreters: before, during, and after the use of an interpreter with a given client or patient.
Skills for interpreters Interpreting for torture survivors requires knowledge of words and concepts commonly transmitted during the course of medical, mental health, legal, or social services work, and understanding of the cultures of clients as well as their experiences of trauma. Sensitivity and resilience in working with people (both clients and providers) are essential. While each agency should provide thorough training for its interpreters, interpreters must assume responsibility for expanding their knowledge base (See Annexure 1 for some of the common vocabulary used in work with torture survivors). Working with survivors of torture: psycho-‐social, legal, medical and humanitarian & economic Striking the right balance in working with torture survivors requires awareness, trust and acceptance. Some argue that service providers must take their cue from survivors allowing them to dictate the pace of giving testimony. Being able to do this requires sensitive judgment that can only come with a good grasp of torture and its effects. Working holistically and co-‐operation amongst service specific professionals will provide the survivor with a more positive outcome and a better transition/re-‐integration into society. It can also enhance the healing process. 16 The UN Voluntary Fund for Victims of Torture describes holistic services provided to victims of torture as follows:17 Psychological assistance is provided to enable victims of torture to overcome the psychological trauma they have experienced. Medical assistance treats the physical after-‐effects of torture. Following diagnosis by a general practitioner, treatment is provided by medical specialists in the fields of orthopaedics, neurology, physiotherapy, paediatrics, sexual health, urology as well as traditional healing and complementary medicine. Social assistance complements the above-‐mentioned forms of assistance by providing various services to reduce the sense of marginalization that many victims experience Legal assistance may be provided in a number of ways including covering the costs of lawyers, courts, translations and legal proceedings. Financial assistance enables victims to meet their basic needs and to gain access to other types of assistance, such as health care.
16 SANToC. (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa. 17 United Nations Human Rights: http://www.ohchr.org/EN/Issues/Pages/TortureFundAssistance.aspx
12
4 WORKING WITH VICTIMS OF TORTURE: A GUIDE FOR MENTAL HEALTH WORKERS
4.1 Introduction Work with torture survivors requires mental health professionals to adapt their conventional models of counseling and psychotherapy to include case management, advocacy and accompaniment. 18 Guidelines for adapting services
• SLOW DOWN or become more comfortable with a slower pace. Information that a provider is accustomed to getting quickly, for example getting a person’s date of birth, can take much longer due to interpretation, cultural differences, and psychological symptoms.
• MONITOR AND/OR REDUCE the number of questions asked, especially in the beginning of treatment. Being asked many questions can remind clients of the interrogation experience.
• CHECK IN WITH CLIENTS regularly to see how they are doing and offer breaks. • HELP CLIENTS MODERATE the pace of telling their trauma stories. • ACTIVELY ADDRESS evidence of re-‐experiencing symptoms or other distress, allowing as
much time as it takes for clients to feel comfortable enough to proceed. This sometimes means letting go of interview protocols.
• ALLOW AT LEAST TWICE as much time for sessions with interpreters. • ALLOW ADEQUATE TIME at the end of sessions for closure and for joint planning regarding
self-‐care of clients after meetings and between sessions. • ADAPT TREATMENT GOALS to the long processes many survivors face in rebuilding their
lives in a new country.
4.1.1 Roles and responsibilities of client and service provider For torture survivors, who may attribute enormous amounts of power to authorities, it is important to clarify the provider role, that is, the limits of power and what the provider offers. It is critical to explain who the provider is and how they can help in terms directly linked to the survivor’s situation and/or needs.19
• EXPECTATIONS: What can the survivor expect next? What does the provider expect next? • CONFIDENTIALITY: What is it and how does it work? What are its limits? Discuss how
confidentiality applies to all role-‐players (interpreter, client, provider, bicultural worker, receptionist). Torture survivors may wonder about possible connections between the provider or clinic and governmental authorities. It is helpful to address this openly.
• PURPOSE: What are the goals of the work together? • PSYCHOLOGICAL SERVICE: What it is, how it works, how it can help? • PSYCHIATRIC MEDICATIONS: Common issues include concerns about addiction or
dependency, discontinuing medication, sharing medication with others, changing dosages, difficulty paying for medication and knowing how and where to fill prescriptions.
• CLIENTS’ RIGHTS: Torture survivors may or may not be familiar with the concept of “rights.” • SLOW THE PACE: A core effect of trauma is that the body and mind are overwhelmed. A
healing experience for a torture survivor involves adapting interventions to a pace that is
18 The Centre for Victims of Torture. (2005) Healing the hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt. 19 SANToC. (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa.

13
tolerable for the survivor. This pace may change throughout treatment and needs continuous monitoring.
• SYSTEMS AND INSTITUTIONS: How they (for example, social services, health care, education, employment, legal services, etc.) relate to working together is an important issue for clients. The success of a multidisciplinary approach to rehabilitation and advocacy requires people working within particular disciplines to have, at the very least, a basic awareness of the issues and priorities that their counterparts address.20
4.2 Healing
4.2.1 Stages of recovery Herman (1992), quoted in Healing the Hurt by the Centre for Victims of Torture describes the following stages in trauma recovery:21
I. Establishment of safety and stabilisation II. Remembrance and mourning: coming to terms with trauma and its effect on one’s life III. Reconnection: rebuilding one’s life and future
Progress through these stages is neither linear nor unidirectional and can be affected by ongoing stress. Moving through the stages can take anywhere from months to years. Herman notes, each survivor “must be the author and arbiter of her own recovery”.22 A torture survivor may define a successful recovery as constituting one, two, or all three of these stages. 4.2.2 Familiar strategies used by mental health workers to help torture survivors While working with torture survivors requires expansion of traditional models it is important for mental health workers to know that their existing repertoire of skills and previous training is relevant. The following strategies used in work with torture survivors may sound familiar to those who have worked with other forms of trauma:
• Provide information to survivors about the psychological effects of trauma and normalise and validate these reactions.
• Provide a safe, therapeutic environment and listen, receive, and endure the emotions with the survivor.
• Help survivors learn to calm and soothe themselves by teaching specific anxiety-‐management strategies.
• Help survivors identify their beliefs about torture and persecution and begin to examine which beliefs were imposed under torture (for example, “I was responsible for what was done to my family.”).
• Foster the establishment or re-‐establishment of trust in others and in the world.
20 SANToC, (2010) Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa. 21 The Centre for Victims of Torture. (2005). Healing the Hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt. 22 Herman, J.L. (1992) Trauma and Recovery: The aftermath of violence from domestic abuse to political terror. Basic Books, p. 133. In The Centre for Victims of Torture. (2005). Healing the Hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt.
14
• Promote positive connection or reconnection with others.
• Address pre-‐ and post-‐torture trauma experiences, which may be significant.
• Assist survivors through the mourning of multiple losses.
• Assist survivors with their adjustment to a new environment and the re-‐establishment of
occupational and educational plans, familial roles, and responsibilities.
• Help survivors anticipate and cope with potentially re-‐traumatisng experiences or with unexpected experiences of re-‐victimisation (for example, crime, racism, arrest by local authorities etc.).
• Foster the eventual connection or reconnection with meaningful return to one’s social,
cultural, political, and economic roles, to whatever extent is desired by the client.
• The qualities of genuineness, warmth, high positive regard, responsiveness, consistency, and respect are as important in working with torture survivors as with any other clients. Many survivors highlight the value of feeling heard and believed as the most healing aspect of their treatment.
The following effects of torture may affect survivors to varying degrees depending on cultural and individual differences23: Distrust Torture survivors have experienced deliberate cruelty and betrayal under highly intimate conditions. Many torturers knew their victims personally, and torture often involves intimate contact. Those in positions of authority who were supposed to protect people perpetrated torture. Understandably, many survivors resolve never to trust another human being. Showing understanding and acceptance of distrust in torture survivor is a powerful intervention. Distrust affects the length of time it takes for someone to acknowledge what happened, and it will affect the survivor’s ability to build relationships with the service provider and with others. For torture survivors, rebuilding trust is a long-‐term recovery goal. Silence and self-‐expression Torture is highly effective at silencing individuals and communities. Torture affects people’s thinking and willingness to express themselves. Their fundamental views of the world, other people, and self are altered to accommodate what they experienced when tortured, which is usually bizarre, sadistic, and incomprehensible. Words often seem inadequate for explaining what one experienced. Survivors find it difficult enough to understand and believe their own experiences, so the task of explaining them to someone who was not there can seem overwhelming or pointless. Disempowerment and helplessness Empowerment is a fundamental principle of trauma recovery. Survivors of torture experience unpredictability, helplessness, and lack of control under torture. Torturers control their victims’ most intimate and basic bodily functions, such as eating and elimination. Victims under detention live for long periods with the feeling of not knowing what is going to happen next, of not knowing when
23 The Centre for Victims of Torture. (2005). Healing the hurt. Retrieved April 2012. http://www.healtorture.org/healing-‐the-‐hurt.

15
death might come. The complete control that torturers have over victims is not just physical but also mental. Mental forms of torture include sleep deprivation, mind games, direct threats, psychological abuse, brainwashing, pharmacological torture, and many other psychological methods. This type of powerlessness undermines people’s ability to assert themselves. Even questions such as “Do you understand what I said to you?” or “Are you feeling all right?” are difficult for torture survivors to answer. They try to assess what is the right answer or what the authority figure wants to hear. They answer yes because they do not want anyone to be upset with them. This places providers in a very difficult position. It is important not to confuse these responses with passivity and indifference. What the provider might be seeing is the chronic fear and helplessness created by torture and repression. Shame and humiliation Torturers intentionally produce feelings of shame and humiliation that undermine identity and prevent survivors from talking about what happened to them. For example, forced nakedness is one technique commonly used under captivity. This act strips away personal identity and shames victims through indecent exposure to others. Other forms of sexual torture result in shame and humiliation. Even survivors who appear quite willing to talk about their experiences will not reveal their most shaming experiences. Providers can never assume they know the worst of what a survivor experienced. In some cultures, it is unacceptable to disclose sexual torture. Female survivors are concerned they will lose their husbands or their communities of support. Because of the potential social and economic consequences, rape survivors may not be able to disclose this to anyone. Similarly, men who are victims of sexual torture struggle with extreme feelings of shame, humiliation, and emasculation. Many survivors say they will have to live with the effects of sexual torture their entire lives. When shame becomes intolerable the effects of this type of torture can be severe, including suicide. Denial and dis-‐belief Simply put, torture is difficult to believe. Torturers tell their victims no one will believe them even if they live to tell the story. Sometimes the torture is so sadistic and bizarre that survivors find it easy to accept that, indeed, no one else will believe what happened. Torturers use torture to distort victims’ sense of reality. The world turns upside down. The incomprehensible and unbelievable become true, and social norms and the rules of logic or common sense in the culture no longer apply. For these reasons, survivors deny, distort, or repress memories of the torture. Torture survivors may fear laughter or disbelief if they talk about the torture. They are sensitive to the slightest gesture from a provider that may imply doubt, disbelief, or denial. Disorientation and confusion Under torture, the assault on the senses and the strangeness of everything that is happening confuses victims. Torturers manipulate the environment to create illusions and fears of losing one’s mind. Under captivity, even if it is only a matter of hours, people lose their sense of time. This is especially true when there is also sensory deprivation (for example, blindfolding, imprisonment in complete darkness), multiple episodes of similar interrogation and torture, or solitary confinement. Survivors may lack memories of what happened under captivity. They do not remember start and end dates of imprisonment. Confusion and disorientation influence the ability to recall events, creating inconsistencies and gaps in their stories. Some torture survivors have experienced pharmacological torture or loss of consciousness. Providers should use caution when interpreting memory issues, and be aware that memory gaps and inconsistencies are common among torture survivors. Rage Rage is a common response to the violations of torture. Many survivors suppressed rage for a long time. The force of their own rage often frightens survivors. Survivors may feel more rage or anger

16
toward a current situation than would normally be expected, given the situation. Conversely, they may shut down when upset, in order to protect themselves from their feelings. They may be able to discuss their fear of their anger but are often at a loss as to what to do with it. They are embarrassed or ashamed, recognizing what they are feeling is out of proportion to the present situation and feel helpless against their own fury. Trauma-‐related rage interferes with the ability to remember, to think clearly, and to express oneself, especially in threatening situations where survivors either feel out of control or fear losing control. Providers may witness behaviors that the torture survivors used during their torture to survive. Psychiatric sequelae Many torture survivors meet criteria for one or more psychiatric disorders. However, use of the term disorder or any concept that so labels the survivor is a very sensitive matter. Some survivors are relieved to know that what they suffer has a name, a history of professional study, and treatment options. Other survivors feel misunderstood or misrepresented by individual diagnoses. They are acutely aware that torture is fundamentally a political and social problem, which receives little attention or acknowledgement worldwide. Survivors suffer from normal, expected human reactions to extremely abnormal and disturbed sets of events and environments. Providers need to communicate this understanding to survivors and to normalize the effects of the torture in ways that have meaning for survivors. Diagnoses, while useful, focus on particular symptoms and on individuals. They do not cover the full range of effects on survivors, their families, and communities.
5 SOME RESOURCES FOR MENTAL HEALTH PROFESSIONALS WORKING WITH VICTIMS OF TORTURE
Centre for the Study of Violence and Reconciliation – Trauma Clinic Physical Address: 4th Floor, Braamfontein Centre 23 Jorrisen Street, Braamfontein Tel: 011 403 5102 Fax: 011 403 7532 E-‐mail: [email protected] Services: 1. Individual and group counselling to survivors of violence and
torture 2. Facilitates support groups 3. Training workshops on complex trauma and trauma management 4. Specialist services for the psychiatric management of survivors of
complex trauma and torture 5. Community outreach programmes to raise awareness of trauma
and PTSD Islamic Careline Physical Address: 32 Avenue Road, Fordsburg Tel: 011 373 8080 Fax: 011 373 8099 Services: Counselling for abused women and children, marital and family
counselling, trauma debriefing, play therapy, HIV and Aids counselling.
Fees: Donation preferred for face-‐to-‐face counselling. Jesuit Refugee Services (JRS) Physical Address: 7th Floor Royal Place Building
85 Eloff Street Tel: 011 333 0980

17
Fax: 011 333 0119 Email: [email protected] Services: 1. Provides limited accommodation and assistance for new arrivals
and vulnerable groups 2. Writes referral letters to hospitals and clinics 3. Provides Support and Counselling to refugees infected and
affected by HIV/Aids 4. Limited Funeral Assistance 5. Assists with micro loans, depending on availability of funds. Johannesburg Child Welfare Physical Address: 41 Fox Street, Cnr West Street, Johannesburg Tel: 011 298 8500 Fax: 011 298 8590 Services: Sexual abuse unit for children under 12 years, counselling and
therapy. Johannesburg Parents and Child Counselling Centre Tel: 011 484 1734 Services: Telephone counselling traumatised children and women Lifeline Physical Address: 2 The Avenue, Corner Henrietta Street, Norwood. 24 hr Crisis Line: 011 728 1347 Fax: 011 728 3497 Services: Rape Counselling for survivors and family, domestic violence
counselling and trauma counselling. Face to face counselling per appointment.
Fees: Donations accepted. Mother Teresa Home Physical Address: No 76 St Georges Street, Yeoville, Johannesburg Tel: 011 648 6315 Services: Shelter for women and children, Spiritual support. Food and
counselling. Mthwakazi Arts and Culture Advice Office Physical Address: 214 Geldenhuys, 33 Jorissen Street, Braamfontein Tel: 011 492 2352492 00000002352 Services: Information workshops, sustainable peace building, legal advice and
referrals. Vocational advice training for migrants, asylum seekers, refugees and their families.
People Opposing Women Abuse (POWA) Physical Address: Confidential Tel: 011 642 4345/6 Fax: 011 484 3195 Services: Telephonic and individual counselling for women, legal advice and
court preparation, and shelters for abused women Fees: R1 – R5 on a sliding scale depending on income.
18
Refugee Ministry Centre Physical Address: Baragh House St. Mary’s Cathedral Cnr Wanderers and Plein Streets, Johannesburg Tel: 011 333 3392 Services: 1. Advocates on behalf of refugees with departments of health and
home affairs 2. Limited paralegal assistance 3. Psychosocial counselling to refugees and refugee torture survivors South African Depression and Anxiety Group Tel: 0800567567 Services: Telephone support for depression and anxiety. Women Refugee Care (WORECA) Physical Address: 19 Lilly Ave, Berea Tel: 076 186 1137 Services: Assists refugee and migrant woman through pregnancy and post
natal. Southern African Centre for the Survivors of Torture (previously known as ZTVP) Physical Address: Field North Building 1st Floor
23 Cnr Jorrisen & De Beer Streets, Braamfontein Services: The Southern African Centre for Survivors of Torture is
a rehabilitation centre that documents human rights violations and offers holistic medical and psychological rehabilitation services to victims/survivors of organised violence and torture perpetrated within the Southern African Development Community (SADC) region.
Southern African Women’s Institute for Migration Affairs (SAWIMA) Physical Address: 513 Heeringracht Building 87 De Korte Street Braamfontein Tel: 011 339 3900 (office hours) 079 873 9021/ 011 211 3269 (after hours) Email: [email protected] Contact Person: Joyce Dube Services: Counseling, HIV/AIDS Paralegal desk Zimbabwe Political Victims Association Physical Address: 114 Rissik Street Methodist House Braamfontein Tel: 072 517 6066 Services: Welfare assistance, paralegal assistance, counselling referrals Sophiatown Community Psychological Services Physical Address: 4 Lancaster Street Westdene Tel: 011 482 8530/482 2117 Services: Counselling ; Couple counseling; Family counseling; Training; Groups
19
6 WORKING WITH VICTIMS OF TORTURE: A GUIDE FOR MEDICAL PROFESSIONALS
6.1 Introduction Health professionals who encounter survivors of torture may do so in different capacities, and they may thus have slightly different but convergent duties24:
• The health professional that is asked to examine an individual expressly for the purpose of providing a medical opinion in a report for a court or other judicial body will be fulfilling a forensic (medico-‐legal) role.
• A health professional who is acting as a care giver to an individual and who in the course of
routine work notes signs and symptoms of ill-‐treatment, or to whom the individual complains of being previously subjected to ill-‐treatment, may need to make an accurate medical record of the findings in the medical notes.
• A health professional that forms part of a team visiting places of detention may record
findings of ill treatment in individuals, but this information may be used more generally in a report on the place of detention without actually forming part of a medico-‐legal report.
• Health professionals in primary care or emergency departments to whom the individual
complains of ill treatment or who note signs of torture. In such cases the health professional may not necessarily have to write a report, but may just need to know how to make a proper examination and a good set of medical notes, which document the care.
• Health professionals in hospitals or clinics who may be asked by, for example, police or
military, to examine a detainee.
• Health professionals examining individuals in a specialist centre for survivors of torture. 6.2 Evidence of torture
• Torture as practiced around the world has many features in common, almost invariably including beating, slapping and kicking and more sophisticated techniques.
• Increasingly across the world torture methods are devised, sometimes with the help of
doctors that produce maximum pain with minimum external evidence. For example, physical evidence of beating may be limited when wide, blunt objects are used for beatings. Similarly, victims are sometimes covered by a rug, or shoes in the case of falaka, to distribute the force of individual blows. For the same reason, wet towels may be used with electric shocks. Other cases of maximum pain and suffering with minimal evidence include forced deprivation.
• Taking a detailed history is essential to ensure that, during the subsequent physical
examination, signs in the relevant areas of the body are not missed and that a correct differentiation from accidental or self-‐inflicted injury is made. For this reason it is necessary to review, at length, some of the techniques employed in different countries before outlining the symptoms and signs to be expected during history-‐taking and physical examination.
24 International Rehabilitation Council for Torture Victims. (2011/12). Model Curriculum on the Effective Medical Documentation of Torture and Ill-‐Treatment, Educational Resources for Health Professionals Students, Prevention through Documentation Project 2006-‐2009. Copenhagen. Accessed May 2012 from http://phrtoolkits.org/wp-‐content/uploads/ downloads/2011/12/MODEL-‐CURRICULUM.pdf
20
• Of particular value in assessing the severity of the attack is a history of loss of consciousness,
though this should be elaborated by questions aimed at finding out whether unconsciousness was caused by blows to the head, asphyxiation, unbearable pain or exhaustion.
• It is difficult to separate physical from psychological torture, as each has a component of the other; for example, hooding not only impedes normal breathing, but also produces disorientation and fear. In addition, physical forms of torture and ill treatment will generally produce both physical and psychological sequelae, and psychological forms of torture and ill treatment often result in psychological sequelae, but may also produce physical sequelae as well. 25
6.3 Medical history The physician should obtain a complete medical history, including information about prior medical, surgical or psychiatric problems. 1. Be sure to document any history of injuries, medical conditions and surgery before the period of
detention and any possible after-‐effects 2. Avoid leading questions 3. Structure inquiries to elicit an open-‐ended, chronological account of the events experienced
during detention 4. Specific historical information may be useful in correlating regional practices of torture with
individual allegations of abuse. Examples of useful information include descriptions of torture devices, body positions, methods of restraint, descriptions of acute or chronic wounds and disabilities and identifying information about perpetrators and places of detention
5. An individual who has survived torture may have trouble expressing in words his or her experiences and symptoms. In some cases, it may be helpful to use trauma event and symptom checklists or questionnaires.
6.4 Physical examination The physical examination is usually the last component of a medical evaluation of an alleged torture victim, after the acquisition of all background information, allegations of abuse, acute and chronic symptoms and disabilities, and after the psychological evaluation, if, in fact, the psychological evaluation is performed by the same clinician who is assessing physical evidence and conducting the physical examination.
• It is essential to obtain the individual’s informed consent prior to the physical examination. • The physical examination must be conducted by a qualified physician. • Whenever possible, the patient should be able to choose the gender of the physician and,
where used, interpreter. If the doctor is not the same gender as the patient, a chaperone who is of the same gender as the patient should be used unless the patient objects.
• The patient must understand that he or she is in control and has the right to limit the examination or to stop at any time. 26
25 International Rehabilitation Council for Torture Victims. (2011/12). Model Curriculum on the Effective Medical Documentation of Torture and Ill-‐Treatment, Educational Resources for Health Professionals Students, Prevention through Documentation Project 2006-‐2009. Copenhagen. Accessed May 2012 from http://phrtoolkits.org/wp-‐content/uploads/ downloads/2011/12/MODEL-‐CURRICULUM.pdf 26 International Rehabilitation Council for Torture Victims. (2011/12). Model Curriculum on the Effective Medical Documentation of Torture and Ill-‐Treatment, Educational Resources for Health Professionals Students, Prevention through Documentation Project 2006-‐2009. Copenhagen. Accessed May 2012 from http://phrtoolkits.org/wp-‐content/uploads/ downloads/2011/12/MODEL-‐CURRICULUM.pdf

21
Acute Symptoms • The individual should be asked to describe any injuries that may have resulted from the
specific methods of alleged abuse. For example: bleeding, bruising, swelling, open wounds, lacerations, fractures, dislocations, joint stress, haemoptysis (coughing up blood), pneumothorax (lung puncture), tympanic membrane perforation, genitourinary system injuries, burns (including colour, bulla or necrosis according to the degree of burn), electrical injuries (size and number of lesions, their colour and surface characteristics), chemical injuries (colour, signs of necrosis), pain, numbness, constipation and vomiting.
• The intensity, frequency and duration of each symptom should be noted. • The development of any subsequent skin lesions should be described and whether or not
they left scars. 27 Chronic Symptoms
• Elicit information of physical ailments that the individual believes were associated with torture or ill treatment.
• Note the severity, frequency and duration of each symptom and any associated disability or need for medical or psychological care.
• Even if the after-‐effects of acute lesions are not observed months or years later, some physical findings may still remain, such as electrical current or thermal burn scars, skeletal deformities, incorrect healing of fractures, dental injuries, loss of hair and myofibrosis.
• Common somatic complaints include headache, back pain, gastrointestinal symptoms, sexual dysfunction and muscle pain. Common psychological symptoms include depressive affect, anxiety, insomnia, nightmares, flashbacks and memory difficulties.28
6.5 Medical report Careful documentation of physical evidence plays a critically important role in verifying that torture has occurred, in supporting legal claims and contributing to human rights campaigns. The medical practitioner requires: knowledge of torture methods and their effects; familiarity with methods of torture designed to leave little physical evidence; skills in detecting hidden and chronic effects of torture; knowledge of patterns of torture in particular localities; understanding of appropriate diagnostic tests; thorough understanding of ethical principles and obligations; acquaintance with relevant national legislation and protocols; and international human rights legislation, and a capacity for empathy. 29 The report on the findings of the medical examination includes a photographic record of injuries and a completion of a form containing standard anatomical drawings on which findings of the investigation can be shown. In South Africa this form is known as the J88. Standards for effective medical evaluation recommended by the Istanbul Protocol provide a guideline for the report (see Appendix 2). The report should include the following details:
27 International Rehabilitation Council for Torture Victims. (2011/12). Model Curriculum on the Effective Medical Documentation of Torture and Ill-‐Treatment, Educational Resources for Health Professionals Students, Prevention through Documentation Project 2006-‐2009. Copenhagen. Accessed May 2012 from http://phrtoolkits.org/wp-‐content/uploads/ downloads/2011/12/MODEL-‐CURRICULUM.pdf 28 International Rehabilitation Council for Torture Victims. (2011/12). Model Curriculum on the Effective Medical Documentation of Torture and Ill-‐Treatment, Educational Resources for Health Professionals Students, Prevention through Documentation Project 2006-‐2009. Copenhagen. Accessed May 2012 http://phrtoolkits.org/wp-‐content/uploads/ downloads/2011/12/MODEL-‐CURRICULUM.pdf 29 SANToC. (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa.

22
• Case information which details the name of the professional, date of the evaluation, referral source, evidence of informed consent, biographical details of the patient, whether an interpreter was used, other parties present, details of any restrictions on the examination and to whom the report was given;
• Credentials of the examiner including qualifications and experience; • Background history of the patient; • Allegations of torture. Details on the torture will depend on the purpose of the report. Some
lawyers note that a general description is sufficient so that another version is not provided for cross-‐examination. For the purposes of human rights advocacy a detailed account provides important data for identifying patterns of torture;
• Current symptoms and disabilities; • Findings of the physical examination; • Results of diagnostic tests including radiology reports and blood tests; • Interpretation of findings; • Recommendations; • Opinion on the association between findings and allegations of torture30. •
6.6 Ethical Issues Apart from the obvious importance of medical examination to guide treatment of torture survivors, medical evidence is significant for legal action and for advocacy against torture. Lawyers acting on behalf of torture survivors place a high value on medical evidence, which some describe as ‘incontrovertible’, meaning that it can be used to prove beyond reasonable doubt that torture took place. Similarly, medical evidence that clearly reveals the physical damage done by torture is used effectively to expose that torture occurred, and to advocate for its prevention.31 Despite the importance of medical proof for legal action and torture prevention, the first ethical obligation of medical doctors, who come into contact with survivors of torture, and of cruel, inhuman or degrading treatment, is to the patient. This means that the practitioner has a duty to examine and treat the survivor guided by the ethical principles of:
• autonomy, by obtaining consent and protecting privacy and maintaining a practitioner-‐patient confidentiality;
• non-‐maleficence by doing no harm; • justice by ensuring fair treatment, and • beneficence, by ensuring that the survivor’s overall care, protection and well-‐being is
considered by the health professional, who must also ensure that the survivor does not face discrimination due to his or her vulnerability, and that he or she will be treated with dignity at all times.32
Similarly, health professionals are under obligation to examine and treat people held in the custody of state officials and institutions with the same standard and quality of care that they would offer to any other patient. In other words doctors are obliged to avoid unfair discrimination and should administer fair treatment irrespective of the social or legal status of the patient.
30 SANToC. (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa. 31 SANToC. (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa. 32 SANToC. (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa.

23
Collusion with torture In South Africa the HPCSA and SANC are statutory bodies that guide and regulate the ethical conduct of health practitioners and nurses respectively and advocate the prohibition of participation in, collusion with, and, or facilitation of torture. The Istanbul Protocol states that it is a ‘gross contravention’ of ethics for health care professionals to participate in torture, whether actively or passively33 What are the duties of health professionals who suspect or have evidence that torture has been perpetrated against the patient, or, suspect that the patient may be at risk?
• A central principle of the practitioner-‐patient relationship is that the practitioner must act in the best interests of the patient.
• Given this the practitioner, even if employed by the State, must retain professional independence.
• The doctor has a duty to protect the patient, to report evidence of torture or cruel, inhuman or degrading treatment and to make or support efforts to ensure that torture or ill treatment is not continued.
• The practitioner must consider the safety of the patient and the risks of reprisal that may arise from such actions. In such situations the doctor is caught between the obligation to report torture and promote justice, and the obligation to ensure the safety of the patient.34
The Istanbul Protocol suggests that medical doctors seek advice from professional bodies and notes that the World Medical Association calls on national and local professional associations to support doctors.35 6.7 Rights to medical treatment of people in custody in South Africa Section 35 of the South African Constitution protects the right of access to medical treatment for people held in state custody. The South African Police Service has internal regulations, referred to as ‘Standing Orders’, which provide for the medical examination of individuals who are arrested and detained. For example Standing Order 349 provides for urgent medical attention to individuals who are injured at a crime scene, guidelines for responses to detainees requesting medical attention, and prohibitions on the issuing of medication to detainees without the consent of a medical practitioner. The Correctional Services Act 111 of 1998 provides for the medical treatment of prisoners. Correctional Service institutions, or prisons, are required to provide medical facilities. Prisoners may request treatment at which request they should be accompanied or transferred to the hospital or health care facility of the prison. Additionally the Correctional Services Act provides for the protection of prisoners from treatment and interventions without their consent and from medical abuse. 36
33 United Nations. (2004). Istantbul Protocol Manual for the Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment. Professional Training Series, No 8/Rev.1. Geneva. 34 SANToC. (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa. 35 United Nations. (2004). Istantbul Protocol Manual for the Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment. Professional Training Series, No 8/Rev.1. Geneva. 36 SANToC. (2010). Drawing on Lessons from the Past: Towards a Fuller Realisation of the Right to Rehabilitation for Survivors of Torture in South Africa. SANToC. (2010).
24
7 SOME RESOURCES FOR MEDICAL PROFESSIONALS WORKING WITH VICTIMS OF TORTURE
Central Methodist Church Physical Address: Cnr Pritchard and Smal Streets, Johannesburg Tel: 011 337 5938 Service: 1. Makes referrals for emergency accommodation for new arrivals 2. Makes medical referrals for torture survivors 3. Provides counselling to refugees infected and affected by HIV and
Aids.
MEDECINS SANS FRONTIERES (DOCTORS WITHOUT BORDERS) Physical Address: Orion Building-‐3rd Floor 49 Jorissen Street Braamfontein Tel: 011 403 4440 Fax: 011 403 4443 Email: [email protected] Website: www.msf.org.za Services: MSF is a medical humanitarian organization that delivers emergency
aid to people affected by conflicts, epidemics, natural disasters and man-‐made disasters, or exclusion of health care.
Doctors Dr Mbobo & Associates Physical address: 2nd Floor Becker House, Hospital and De Korte Street, Hillbrow Tel: 011 720 0666 Services: Wellness Clinic, HIV/AIDS testing and pre counselling, VCT Dr M.M. Bhikhoo Physical Address: 74 Queens Road Mayfair Tel: 011 837 5771 Fax: 011 837 7607 Email: [email protected] Dr Robbie Potenza Physical Address: Suite 10 St Joseph’s Wing Wits Donald Gordon Medical Centre 21 Eton Road Parktown Dr. Ebrahim Joosuf Physical Address: Burton Court Shop 16 8 Pretoria Street Hillbrow Tel: 011 725 2281 Fax: 011 720 4980 Email: [email protected] Dr T.A.A. Essay

25
Physical Address: Townsview Medical Centre 72 Main Street Rosettenville Tel: 011 436 1983 Dr S.A. Bhoora Physical Address: 635 Julies Street Malvern Tel: 011 615 7291 Dr S. Brower Physical Address: 120 Hey Street Turffontein Tel: 011 615 7291 Dr S.W. Maphisa Physical Address: Cnr Banket & Bruce Streets Hillbrow Tel: 011 484 0305 Dr M.N. Mabasa Physical Address: 5463 Riverside Matlhako street Kagiso Tel: 011 410 6353 Dr M.C. Maharaj Physical Address: House No 41 Kagiso Avenue Extension 6 Kagiso Tel: 011 410 6336 Dr M.D. Kgalamono Physical Address: 3801 Themba Drive Hills View Kagiso 2 Tel: 011 410 6784 Dr B. Jivan Physical Address: 25 Park Street Randfontein Tel: 011 692 1221 Dr T Diphoko Physical Address: 2124 Ralerata Street Mohlakeng 011 414 5561 Dr D. L. Cumes Physical Address: 25D Kenmere Street Yeoville Tel: 011 683 8263
26
Dr G.M.P.V. De Oliveira Physical Address: 131 8th Avenue Bez Valley Tel: 011 614 6951 Dr Z. Bham Physical Address: 114 D Twist Street Hillbrow Tel: 011 484 0151 Physiotherapists Ashira Singh (Physiotherapist) Physical Address: House No1 Garden City Clinic 35 Bartlett Road Mayfair Tel: 011 495 5353 Fax: 011 8378883 Email: [email protected] Sello Matona (Physiotherapist) Physical Address: New Kensington Medical Centre 23 Roberts Avenue Kensington Mobile phone: 082 794 4444 Email: [email protected] Clare Cresswell (Physiotherapist) Physical Address: 2 Firth Avenue Parktown North Tel: 011 880 7112 Email: [email protected] Roxanne Ashkar (Physiotherapist) Physical Address: Thrupps Illovo Centre 204 Oxford Road Illovo Tel: 011 268 0331/0297 Email: [email protected] E.C. Speechly (Physiotherapist) Physical Address: 24 12th Avenue Linksfield West Tel: 011 485 1882 G.M. Bogoshi (Physiotherapist) Physical Address: Johannesburg Hospital Parktown Tel: 011 488 3258

27
L.B. Lelaka (Physiotherapist) Physical Address: 2 Bunting Road Netcare Rehabilitation Hospital Auckland Park Tel: 011 489 1226 Dawn Hansen (Physiotherapist) Physical Address: Milpark Hospital Suite 2 Lower Level Parktown West Tel: 011 726 1512 Email: [email protected] J.N. Mare (Physiotherapist) Physical Address: 38 Fairfield Road The Hill Tel: 011 435 9840 Email: [email protected]
28
8 WORKING WITH VICTIMS OF TORTURE: A GUIDE FOR CARERS IN THE CONTEXT OF HUMANITARIAN ASSISTANCE
8.1 Introduction Service providers, be they receptionists, administrators and volunteers, counsellors, facilitators, and professionals are responsible to support the healing and restoration of the self-‐esteem and self-‐confidence of victims of torture with whom they work. What do we hope will come out of our intervention with regard to the self-‐esteem, self-‐respect, goals, independence, and economic development of victims of torture?
Our hope as carers is that we assist victims of torture on their way to becoming self-‐empowered, self-‐sufficient individuals, with working knowledge of places they can go and things they can do independently.
What beliefs, attitudes, values, knowledge, skills, and tools do we value, nurture and sustain in order to make us competent and effective carers whose practice can achieve the hoped-‐for outcome?
The person who has suffered torture doesn’t want to come to your office, into a dependent, welfare situation. Victims of torture are embarrassed by their situation. They are already victimised. They don’t want to be in the situation where they have to beg organisations for assistance
The humanitarian carer’s interaction creates and sustains an environment which:
• Avoids a situation in which the ability of the client to think and act is diminished. The carer’s approach will avoid ‘taking the problem away’ from the person whose problem it is. The locus of control is placed and remains firmly in the hands of the victim. The relationship with the carer is established to promote independence;
• Encourages the person to feel like someone who is recognised and regarded as a respected and active partner in the relationship. The victim of torture may have any number of negative feelings including embarrassment, fear, confusion, suspicion, hostility and aggression. The carer’s open, non-‐judgmental and interested attitude together with a skilled, firm and steadfast holding to the agreed objectives, will initiate a process to support and guide the victim of torture in growing insight into the possibilities of co-‐operating and assuming a journey on a path to independence.
8.2 Skills of carers The skills of the professional carer are acquired through academic study, internship, practice and accumulated experience. This is built upon in organisations by shared collegial experience, strengthened by broader learning in meetings, seminars, conferences and professional development courses. Support personnel in organisations who work with victims of torture, including receptionists, administrators, counsellors and facilitators, acquire their skills and competencies through training and exposure to the ethos of the organisations.
29
8.3 Practice of carers As carers we have to work on our own self-‐confidence in decision-‐making. This means not being so academically oriented. Yes, you learn everything in university and school. You know the laws and human rights and what should be done. To become a successful carer there also has to be some thinking outside of the box; not everything can be learned from a book. You have to have your own judgments, and confidence.
Carers encounter victims of torture in situations that require multi-‐pronged responses incorporating: • respect • listening • compassion • patience and insight • application of critical skills and analysis in assessing the situation • seeking additional expertise and information • formulating an appropriate plan for intervention that includes assistance, support, treatment
and ongoing joint reflection and evaluation of progress to closure. Some questions for carers to ask themselves
• In my first meeting with a victim of torture, do I meet a new person in my life with authentic interest? Or am I starting a ‘new case?
• Within the first ten minutes of a meeting, do I know what is the most important thing in the life of this person? Or has my total focus been on the completion of all the details on the intake form?
• At the end of the first meeting, will the victim of torture feel they have met someone whom they have a sense of, who they can work with? Or have they met a person packaged in a uniform?
• Am I confident that the parameters of the interaction have been set, including the limits of any assistance I may be able to offer?
• How many times did I smile? • Have I become aware of anything that may cause me personal discomfort, or loss of my
confidence? How will I address this? • In what ways has my confidence as an independent decision-‐maker in my work with victims
of torture increased? Has my academic training supported my feelings of being a competent and effective professional? Have I experienced situations where there is a conflict or contradiction between what I feel should be an approach or decision regarding a victim of torture; between what I have learnt; what my organisation says is right; and what I believe is the right way to do things? How have I proceeded in such instances? What have I felt about the outcome, as it relates to my own development, personally and as a carer?
• How is my independent thinking encouraged, facilitated and supported by my colleagues and organisation? What instances are there where I worked on ‘my mistakes’ in a way that has led to my personal growth and professional development? What have I done when I have felt failed either in making a good decision, or that I have let the client or my organisation down?
• Do I know and always practice “The Iron Rule”? (Never do for people what they can do for themselves). People are capable and the carer can promote self-‐sufficiency by showing ‘tough love’ wherever possible.
• Who cares for the carers?
30
8.4 About carer’s health and well being A carer’s caseload may involve 10 interviews and consultations a day, each requiring intense listening and counselling. The interviews are followed by research, problem solving and preparation of plans of action. The accounts presented to the carer are traumatic and the person’s condition may present in disturbed behaviour. Such intense encounters impact on the carer’s mental and emotional capacity.
One of the impediments to carers achieving optimal results may lie in stress for which there are numerous causes. In addition to the emotional impact of listening to survivor’s stories, there may be factors in the carer’s personal life; for example, situations involving family members, financial strains, or worries about personal competency in the workplace. In organisations where shortages of funding hang over everyone’s heads, carers may become anxious. ’Physician, heal thyself’ captures the role of debriefing for the humanitarian worker in regenerating energy and preventing ‘burnout’. Debriefing sessions help avoid the transfer of trauma from the carer onto clients. Debriefing requires frankness and openness. Humanitarian staff need to realise their need for debriefing. It is not something someone else can identify; one has to assume personal responsibility to know the need for it, deal with any inclination to avoid or postpone it for whatever reason (for example, heavy workload, personal resistance or fear of cultural stigma). In the absence of debriefing sessions humanitarian carers may experience loss of emotional and mental fitness, rendering them unable to help someone who is dealing with emotional trauma. Carers have been attacked, verbally, physically and emotionally or have been subjects of attempts at extortion. It can be surprising to any practitioner to find themselves feeling helpless, angry, confused, frustrated, disappointed. It is important to develop and maintain mental, emotional and physical wellbeing, and to recognise one’s own limits.
8.5 Accountability Carers are required to make independent decisions while remaining accountable to legal parameters, organisational policies and financial constraints. From time to time carers may make the ‘wrong’ decision or act ambivalently. This usually arises where carers are reluctant to acknowledge they can’t fix problems. Or, they may not want to give someone who is desperate bad news. Accountability is a critical strength of humanitarian professional practice. However, accountability can be perceived as threatening -‐ as exposure of vulnerability, loss of self-‐esteem and possible loss of one’s job. In reality, the practice of accountability affords an opportunity to share experience, expand and strengthen working knowledge and build a trusting environment that fosters and rewards growth and independent practice.
8.6 Setting and maintaining boundaries How do carers avoid stepping in to ‘rescue’ the victim of torture whilst showing compassion until the client is able to assume responsibility and the ability to jointly work on addressing problems? This process is difficult and can take time. An important attribute for carer’s to develop is to refrain from allowing personal feelings of responsibility to dominate and to resist the desire fix’. To manage this process the carer requires commitment to "The Iron Rule" -‐ never do for people what they can do for themselves. Setting and maintaining boundaries are vitally important tools for the carer in order to:
• Avoid creating dependency • Maintain the balance between nurturing the client’s empowerment and retaining the carer’s
mental, emotional and physical energy.
31
8.7 Opportunities to strengthen carers in practice Disappointment, manipulation, misappropriation of resources and theft of money are part of the territory in humanitarian care. To keep strong carers have to:
• Keep the goals of the work in sight • Retain a professional balance by being objectively assessing situations and simultaneously
being aware of the risks • Make use of collegial support.
Participation in mentored reflection designed to foster development of professionals, and participation in support groups, can build a body of knowledge, which may strengthen carers and the organisations within which they work.
8.8 Organisational culture and bureaucracy While the broad vision of the caring sector is dedicated to rehabilitation of victims of torture, there exist diverse ‘cultures’ in organisations, depending on whether they are non-‐governmental organsiations, religious, or government agencies. Inevitably organisational cultures have unintended consequences. For example, as proficiency and expertise develops, there may also grow some sense of ‘knowing the answers’. As a result, responses and interventions may appear or become mechanical. As working systems and processes -‐ which are important for good governance -‐ are established, particularly in organisations dealing with referrals and resource management and distribution, bureaucratic requirements may become onerous and seem endless. In addition to being faced with trying to fulfill bureaucratic requirements victims of torture seeking help may encounter bureaucratic attitudes that can be intimidating and discouraging. Factors that can deplete the already diminished energies of victims of torture and violence are the time spent being referred from office to office, or waiting in queues. When this happens, as can be seen in long lines at government documentation and processing offices, frustration and resentment can build up in individuals and groups, which exacerbates the already present sense of victimisation.
8.9 Obstacles to professional humanitarian caring practice
Corruption Corruption is pervasive in South Africa. Humanitarian carers may be confronted with temptations, which are difficult to resist. What are the duties and responsibilities of carers to strengthen good governance, compliance and accountability?
Good Governance Put the systems in place, for example, policies and codes of conduct, in the organisation and ensure that everyone knows what they are. Compliance and accountability Ensure that checks and balances are in place to facilitate compliance and accountability, for example management and administration meetings, regular reporting and inspections and effective financial reporting. Proper use of the funding and resources entrusted to the organisation for the purposes of its humanitarian work requires everyone in the organisation to have fiduciary responsibility (An individual/organisation in whom the utmost trust and confidence has been placed to care
32
for, manage and protect property or money for the purpose for which it is intended. The term "fiduciary" is derived from the Latin term for "faith" or "trust.") By adhering to due process and taking prompt action where standards are not upheld, organisations build up social capital:
• The organisation is recognised for its good governance and compliance • People employed within the organisation are strengthened in the work they do • Other people and organisations feel confident about their interactions with the
organisation and its representatives • The organisation is able to meet its commitments and continue to secure funding.
9 SOME RESOURCES FOR HUMANITARIAN CARERS WORKING WITH VICTIMS OF TORTURE
Coordinating Body for Refugee Communities (CBRC) Physical Address: 11th Floor, Auckland House, Braamfontein Tel: 011 403 4429 Fax: 011 403 8075 Service: Provides emergency accommodation for new arrivals. Makes referrals to relevant service providers Facilitates contacts with other refugees. Refugee Aid Office (RAO) Physical Address: Markade Mall-‐Ground floor 84 President Street (corner Kruis) City Centre (Johannesburg office) Tel: 072 785 3959 Physical Address: IDASA Building 357 Visagie Street Pretoria (Pretoria office) Tel: 012 320 2943 Fax: 012 320 2949 Email: admin@refugee-‐aid.org Services: Provides physical, medical, spiritual and educational needs of
refugee clients. Financial assistance is not guaranteed and will only be provided as a contribution to the family in need; not a full payment of rent and food.
Jesuit Refugee Services (JRS) Physical Address: 7th Floor Royal Place Building 85 Eloff Street Johannesburg Tel: 011 333 0980 Fax: 011 333 0119 Services: 1. Provides limited accommodation and assistance for new arrivals
and vulnerable groups 2. Writes referral letters to hospitals and clinics 3. Provides support and counselling to refugees infected and
affected by HIV/Aids
33
4. Limited Funeral Assistance 5. Assists with micro loans, depending on availability of funds. Lutheran Church of Johannesburg (Church of Peace) Physical Address: Cnr Kaptein and Claim Streets, Hillbrow, Johannesburg Tel: 011 720 7011 Services: Spiritual support and healing for victims of torture and humanitarian
support Email: [email protected] Mother Teresa Home Physical Address: No 76 St Georges Street, Yeoville, Johannesburg Tel: 011 648 6315 Services: Shelter for women and children, Spiritual support. Food and
counselling. Papillon Development Centre Physical Address: Cnr Mabel and Lily Streets, Rosettenville Tel: 011 435 9799/1117 Email: [email protected] Services: 1. English Classes 2. Computer training 3. Feeding Scheme; Mondays – Fridays between 12h00 and 13h00 4. Distributes clothing to orphans and the poor who attend the
feeding scheme. People Opposing Women Abuse (POWA) Physical Address: Confidential Tel: 011 642 4345/6 Fax: 011 484 3195 Services: Telephonic and individual counselling for women, legal advice and
court preparation, and shelters for abused women Fees: R1 – R5 on a sliding scale depending on income. Women Refugee Care (WORECA) Physical Address: 19 Lilly Ave, Berea Tel: 076 186 1137 Services: Assists refugee and migrant woman through their pregnancy and
after delivery. Southern African Centre for the Survivors of Torture Physical Address: 23 Cnr Jorissen and De Beer streets Field North Building First Floor Braamfontein Tel: 011 339 4476 Services: The Southern African Centre for Survivors of Torture is
a rehabilitation centre that documents human rights violations and offers holistic medical and psychological rehabilitation services to victims/survivors of organised violence and torture perpetrated

34
within the Southern African Development Community (SADC) region.
African Migrants Solidarity Physical Address: 20 Cnr Albert & Eloff Streets Standard Building 8th floor Office 817 Johannesburg Services: Amis assists and orients its clients to access services such as
IT/Computer training, English courses & others Migrant women’s sexual and reproductive health education and
protection Facilitation and orientation of migrants in terms of studies or
education in South Africa Ant-‐poverty initiatives for migrants and local communities. African Diaspora Forum Physical Address: 47 Corner Sauer and President Streets Johannesburg Tel: 011 633 2140 Fax: 011 636 8274 Email: [email protected] Services: Humanitarian assistance Integration and reintegration assistance Central Methodist Church Physical Address: Corner Pritchard and Small Streets Johannesburg Tel: 011 333 7672 Fax: 011 333 3254 Email: [email protected] Contact person: Pastor Kim Alexander/Bishop Paul Verryn Services: Emergency accommodation for new arrivals Medical assistance for immigrants Counseling to refugees infected by HIV/AIDS Pre-‐school and School run at the church SHELTERS Bethany Shelter Physical Address: Cnr Millburn Road and Viljoen Street, Bertrams Tel: 011 614 3245 Restrictions: For Abused Women Bienvenue Shelter Physical Address: 36 Terrace Road, Bertrams Tel: 011 624 2915 Restrictions: For women and minors only. Email: [email protected] Door of Hope Physical Address: 17 Doris Street, Berea. Tel: 011 432 2913 Restrictions: Assists newborn abandoned street children. Email: [email protected]
35
Ekhaya Overnight Shelter Physical Address: Cnr Quartz and Kotze Streets, Hillbrow Tel: 011 725 6531 Fax: 011 725 6572 Restrictions: Men only. Freda Hartley Shelter for Women Physical Address: 97 Regent Street, Yeoville Tel: 011 648 6005 Restrictions: For women only. Email: [email protected] Jabulani Khakibos Kids Centre Physical Address: Cnr Claim and Pietersen Streets, Joubert Park Tel: 084 6201 465 Restrictions: For boys who have been on the streets. Abused, abandoned, or
orphaned boys. Offers accommodation and education. Email: [email protected] Jesse Mission Physical Address: 74 Joel Street, Berea Tel: 011 642 4422 Restrictions: For men only. Call to check availability of rooms. Place of Refuge Physical Address: Diagonal Street, La Rochelle Tel: 011 435 7867 Restrictions: For men and women. St Francis de Sales House Physical Address: 50 Buston Street, Doornfontein Tel: 082 754 1959 Restrictions: Per referral from JRS, Maximum stay of 3 months. Must follow rules
and participate in community activities. Strabane Mercy Shelter Physical Address: 98 Kerk Street, Johannesburg Tel: 011 336 2476/8 Fee: R3 per day Restrictions: Only men and women between 30 and 60 years old. The House Physical Address: 60 Olivia Road, Berea Tel: 011 642 4358 Restrictions: For girls between 12 and 18 years only. Three months limit. Also
daily drop in programme with food, showers and washing facilities. Usindiso Sanctuary Physical Address: 80 Albert Street, Johannesburg Tel: 011 334 1143 Restrictions: For abused women and girls, especially those with children. Email: admit@usindiso ministries.co.za Ikayha Le Themba
36
Physical Address: 176 Smit Street Braamfontein Tel: 011 242 3038 Fax: 011 242 3017 Contact Person: Merita Ground Email: [email protected] Services: 24 hour residential sanctuary and shelter for abused women and
their children Counseling for survivors of abuse Nazareth House Physical Address: Nazareth House 1 Webb Street Yeoville Tel: 011 648 1002 Fax: 011 487 3643 Contact Person: Sister Lorraine Akal Email: [email protected] Services: Caters for:
Abandoned HIV + babies and children The financially burdened and destitute frail aged Mentally challenged Destitute, terminally ill adults with AIDS Rosebank Mercy Centre Physical Address: 17 Sturdee Avenue Rosebank Tel: 011 447 4399 Restrictions: Single Men Fee: R5 per night SOUP KITCHENS Christ the King Cathedral Physical Address: Saratoga Avenue, Joubert Park Holy Trinity Catholic Church Physical Address: 16 Stiemens street Braamfontein Tel: 011 339 2826 Fax: 086 528 9538 Email: [email protected] Gauteng Council of Churches Physical Address: St Albans Church Schoeman Street Pretoria Tel: 012 323 5187/8 Restrictions Food parcels once per month Newcomers must register with the council and present proof of asylum or refugee documents and
proof of residency in Pretoria Trinity Congregating Church Physical Address: Cnr Muller and Bedford Streets Yeoville

37
10 WORKING WITH VICTIMS OF TORTURE: A GUIDE FOR LEGAL PRACTITIONERS
10.1 Introduction This guide is intended to assist legal practitioners in working with victims of torture in South Africa. It unpacks the definition of torture; identifies the persons who are vulnerable to torture in South Africa; provides the international legal framework that governs torture; details South Africa’s domestic obligations regarding torture; as well as provides practical steps for providing legal services to victims of torture. What is torture? The United Nations Convention Against Torture (UNCAT)37 outlaws torture; as well as cruel, inhuman and degrading treatment or punishment. South Africa ratified the UNCAT in 1998. It is thus bound by the CAT and must adhere to the provisions contained therein. The UNCAT defines torture in Article 1 as ‘any act by which severe pain or suffering, whether physical or mental is intentionally inflicted on a person for such purposes as obtaining from him or a third person information or a confession, punishing him for an act he or a third person has committed or is suspected of having committed, or intimidating or coercing him or a third person, or for any reason based on discrimination of any kind, when such pain or suffering is inflicted by or at the instigation of or with the consent or acquiescence of a public official or other person acting in an official capacity. It does not include pain and suffering arising only from, inherent in or incidental to lawful sanctions’. The UNCAT does not define cruel, inhuman or degrading treatment or punishment. However; it requires states to prevent cruel, inhuman, degrading treatment or punishment.38 Legal practitioners should have regard to case law, both national and international, to assist in distinguishing torture from cruel, inhuman or degrading treatment or punishment. In unpacking Article 1 of the UNCAT, the elements of torture are as follows:
• An act or omission that inflicts severe pain or suffering: o Such as causing physical pain or suffering; o Such as intentionally withholding food or medical treatment from detainees;
• That is inflicted intentionally: o The act or omission must be intentional; o If an official forgets to provide a detainee with food; this would not be torture.
Rather, if food is withheld from a detainee in order to solicit a confession or to discriminate against the detainee – this would amount to torture.
• Must be inflicted for a specific purpose: o The UNCAT lists purposes for which torture is inflicted: to obtain information; to
obtain a confession; as punishment; as intimidation or coercion; discrimination. o The list is not exhaustive.
37 The Convention Against Torture was adopted on 10 December 1984 through Resolution 39/46 of the General Assembly of the United Nations. It entered into force on 26 June 1987. 38 See Article 16 of CAT.
38
• Must be committed by a public official or with the consent or acquiescence of a public official or person acting in an official capacity:
o Includes the state’s failure to act. • It does not include pain or suffering arising from lawful sanctions
o For example when force is used in lawful state operations.
Persons vulnerable to torture in South Africa In the past in South Africa, torture was associated with political oppression. Today, certain groups of people in South Africa are particularly vulnerable to torture including: prisoners; persons in police custody; persons in immigration detention; patients in psychiatric hospitals; children in care facilities and persons in military detention.39
10.2 States have an obligation to protect groups that are especially vulnerable to torture40
The international legal framework -‐ The right to be free from torture As set out in the Introduction above, South Africa is a party to the UNCAT and is thus bound by its provisions. UNCAT requires states amongst other things to take measures to prevent acts of torture41; to repress all acts of torture42 and to guarantee domestic remedies for appeal and reparation to victims of torture43. In addition, the right to be free from torture has the status of a peremptory norm under international law known as jus cogens. This means that it has a higher status than treaty law or customary law.44 Thus, unlike other treaties that allow state parties to suspend some of the rights under the treaty in question; the right to be free from torture is absolute. The right to be free from torture is also contained in the Universal Declaration of Human Rights45. The International Covenant on Civil and Political Rights (ICCPR) to which South Africa is a party46 also prohibits torture47 as does the African Charter on Human and Peoples’ Rights (ACHPR).48 There are also other treaties that a legal practitioner can have regard to when enforcing the rights of victims of torture – such as the Convention on the Rights of the Child.49
39 Muntingh L, Guide to the UN Convention Against Torture in South Africa, (2011) at 13 to 15 available at http://cspri.org.za/publications/legal-‐guides/Guide%20to%20UN%20Convention%20Against%20Torture%20in%20South%20Africa.pdf. 40 Committee Against Torture, Draft General Comment 2, implementation of Article 2 by State Parties, 38th Session, paragraph 21, available at http://daccess-‐dds-‐ny.un.org/doc/UNDOC/GEN/G08/402/62/PDF/G0840262.pdf?OpenElement . 41 See Article 2.1 of CAT. 42 See article 4 of CAT which requires acts of torture to be made offences under criminal law. 43 See articles 13 and 14 of CAT. 44 Dugard J ‘International Law: a South African perspective’ Third Edition (2009) at 43. Other examples of premptory norms are the prohibition against slavery; genocide; racial discrimination including apartheid and the denial of self-‐determination. 45 See Article 5. 46 South Africa ratified the ICCPR on 10 December 1998. 47 See Article 7 of the ICCPR. 48 See Article 5 of the ACHPR. South Africa ratified the ACHPR on 9 July 2006.
39
Non-‐binding instruments A legal practitioner should be familiar with non-‐binding instruments or ‘soft law’ when dealing with victims of torture. The Manual on Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment50; which is commonly known as the Istanbul Protocol is a set of international guidelines for documenting torture and its consequences and is of use to legal practitioners.
10.3 South Africa’s domestic obligations The right to be free from torture and inhuman or degrading treatment or punishment is enshrined in the South African Constitution (the Constitution).51 Section 12 of the Constitution provides that everyone has the right to freedom and security of the person, which right includes amongst other things, the right not to be tortured in any way and the right not to be treated or punished in a cruel, inhuman or degrading way. Sections 28 and 35 of the Constitution are also of relevance. They deal with the rights of children as well as the rights of detained persons. Children have the right to be protected from maltreatment; neglect; abuse or degradation.52 Persons who are arrested for allegedly committing an offence have the right to conditions of detention that are consistent with human dignity.53 The Correctional Services Act54 in Section 2 (b) requires that prisoners in safe custody are treated with human dignity. In addition, the South African Police Services (SAPS) has developed a policy on the prevention of torture in SAPS.55 The Refugees Act56 is also of relevance when dealing with victims of torture. Section 2 of the Refugees Act contains the principle of non-‐refoulement; which is also contained in Article 3 of the UNCAT. The essence of this principle is that no person may be returned to a country where he or she would face persecution or a threat to physical safety or freedom. South Africa however does not at present have legislation dealing specifically with torture. We have a bill known as the Combating of Torture Bill. This is not yet in force.57 As South Africa does not have the crime of torture defined in legislation, acts of torture are prosecuted under other common law offences such as murder; attempted murder; assault or assault with the intent to do grievous bodily harm.
10.4 Providing legal services to victims of torture in South Africa Consulting with your client Legal practitioners who deal with victims of torture need to be sensitive to the client’s needs and avoid re-‐traumatising the client in the process of taking a statement. When consulting with a client who is a victim of torture: 49 See Article 37 of the Convention on the Rights of the Child (CRC). The CRC entered into force in 1990. 50 The Correctional Services Act 111 of 1998. 51 The Constitution of the Republic of South Africa Act 108 of 1996. 52 See Section 28 (d) of the Constitution. 53 See Section 35 (e) of the Constitution. 54 The Correctional Services Act 111 of 1998. 55 See http://www.saps.gov.za/docs_publs/legislation/policies/torture.htm. 56 The Refugees Act 130 of 1998. 57 For comments on the Combating of Torture Bill see http://www.peopletoparliament.org.za/focus-‐areas/prisoners-‐and-‐detained-‐persons/resources/Comments2008.pdf .
40
• Make sure that the consultation takes place in private; • Be sensitive to the client; • Be aware of appropriate referral resources – for example medical doctors and psychological
counselors; • Consult with the client as soon as possible after the torture has occurred; • Ensure that a detailed statement is taken from the client regarding the torture. This includes
the time and location of the torture; the details of who was present during the torture; the role of each person who was present; details of any threats or psychological torture; details of any physical evidence of the torture as well as details of any witnesses to the torture.58
10.5 Legal recourse for victims of torture Legal practitioners can assist clients:
• to ensure that criminal proceedings are instituted against the perpetrator of the torture • in defending a victim of torture in a criminal trial where a confession has been obtained
through torture59 • to institute a damages claim on behalf of the victim of torture. The law of delict provides
a basis for instituting such damages claim. Alternative mechanisms that legal practitioners can use to assist clients include:
• assisting clients to lay complaints against the police with the Independent Police Investigative Directorate60 (IPID) (formerly the Independent Complaints Directorate)
• lodging a complaint with the South African Human Rights Commission.61
The table summarises types of legal remedies for a victim of torture. CRIMINAL LAW
CIVIL LAW
ALTERNATIVE COMPLAINTS MECHANISMS
-‐ Ensure that perpetrator
of torture is prosecuted; -‐ Assist client in criminal
defense if client is charged with an offence and was tortured while in police custody.
-‐ Bring a damages claim
against the perpetrator; -‐ Be aware of prescription
of claim; -‐ Claim based on delict.
-‐ Submit a complaint to the
IPID; -‐ Submit a complaint to the
SAHRC.
10.6 The role of the legal practitioner beyond client representation The role of a legal practitioner in preventing torture and assisting clients in cases of torture goes beyond litigation on behalf of clients.62 There are many other ways in which the expertise of legal practitioners can assist in the prevention of torture in South Africa:
58 For further best practices on consulting with victims of torture see ‘Combating Torture: A manual for Judges and Prosecutors’ by C Foley available at http://www.essex.ac.uk/combatingtorturehandbook/manual/4_content.htm#6 59 Article 15 of CAT and Section 35 (5) of the Constitution prohibit the use of statements made as a result of torture in criminal proceedings. 60 See the IPID website at http://www.ipid.gov.za. 61 The SAHRC does not deal with complaints that fall under the mandate of the IPID. Complaint forms can be accessed on the SAHRC website at www.sahrc.org.za. 62 Association for the Prevention of Torture, The Role of Lawyers in Preventing Torture (2008), available at http://www.apt.ch/index.php?option=com_docman&task=cat_view&gid=115&Itemid=260&lang=en.
41
• Advocacy efforts around the Combating of Torture Bill to ensure that the Bill complies with the UNCAT;
• The provision of pro bono legal services at places of deprivation of liberty to ensure that detainees are aware of their rights63;
• Monitoring places of detention64; • Lobbying for the ratification of the Optional Protocol to the Convention Against
Torture65; • Assisting in compiling civil society ‘shadow reports’ to the Committee Against Torture66.
11 SOME RESOURCES FOR LEGAL PRACTITIONERS WORKING WITH VICTIMS OF TORTURE
The Civil Society Prison Reform Initiative (CSPRI) http://cspri.org.za The South African Human Rights Commission (SAHRC): http://www.sahrc.org.za/home Judicial Inspectorate for Correctional Services: http://judicialinsp.pwv.gov.za/Default.asp . Johannesburg Family Court Physical Address: 15 Market Street, Johannesburg Tel: 011 241 6831 Service: Adjudicates on family law matters. Lawyers for Human Rights (LHR) Physical Address: Heerengracht Building 87 De Korte Street Braamfontein Tel: 011 339 1960/2 Fax: 011 339 2665 Service: Provides legal assistance regarding unlawful arrests, detention and
deportation. Also provides advice and assistance with asylum application procedures, appeals and reviews in case of rejected asylum applications.
People Opposing Women Abuse (POWA) Physical Address: Confidential Tel: 011 642 4345/6 Fax: 011 484 3195 Services: Telephonic and individual counselling for women, legal advice and
court preparation, and shelters for abused women
63 The UN Committee Against Torture in its response to South Africa’s initial report, called upon South Africa to strengthen legal aid provision to victims of torture in South Africa. See paragraph 29 of the of the Committee’s 2006 report. 64 The Association for the Prevention of Torture has produced a Practical Guide for Monitoring places of detention available at http://www.apt.ch/index.php?option=com_docman&Itemid=259&lang=en. 65 The Optional Protocol to the Convention Against Torture and other Cruel, Inhuman or Degrading Treatment or Punishment (OPCAT) has been signed by South Africa in 2006 but not yet ratified. The aim of OPCAT is to establish a system of regular visits to places of deprivation of liberty, by both independent international and national bodies. The purpose of such visits is to prevent torture and cruel, inhuman and degrading treatment. 66 The Committee Against Torture is a treaty monitoring body that is established under the CAT.

42
Fees: R1 – R5 on a sliding scale depending on income. Tswaranang Legal Advocacy Centre to End Violence Against Women Physical Address: 26 Jorrisen Street, 8th Floor, Braamfontein Centre. Tel: 011 403 4267 Fax: 011 403 4275 Services: Legal counselling regarding domestic violence, rape, maintenance,
custody access. University of Witwatersrand Law Clinic Physical Address: 1 Jan Smuts Ave, Braamfontein, Johannesburg Tel: 011 717 8562 Fax: 011 339 2640 Services: Provides advice and assistance with asylum procedures, appeals and
reviews in case of rejected asylum applications and other general legal advice.
ProBono.Org (Refugee Legal Clinic) Physical Address: 1st Floor West Wing, Women’s Jail, Constitution Hill 1 Kotze Street, Braamfontein Johannesburg Tel: 011 339 6080 Fax: 011 339 6077 Website: www.probono-‐org.org Services: Pro Bono provides the following services for both South African
citizens and non-‐nationals: • Appeals • Application for temporary residence permits • Application for joining files in the case of marriage • Opening of bank accounts • Obtaining health care when it has been refused • Where schools refuse to enroll children • Approaching courts where discrimination occurs as a result
of their status • Return to their country of origin where possible • Family reunification with a family member who has acquired
refugee status in another country • Legal advice to HIV positive people
Legal Aid Board (LAB-‐Head office) Physical Address: 29 De Beer street Braamfontein Tel: 011 660 2335 Services: The LAB provides free legal services to people who cannot afford private
legal assistance in South Africa through its office in every region.
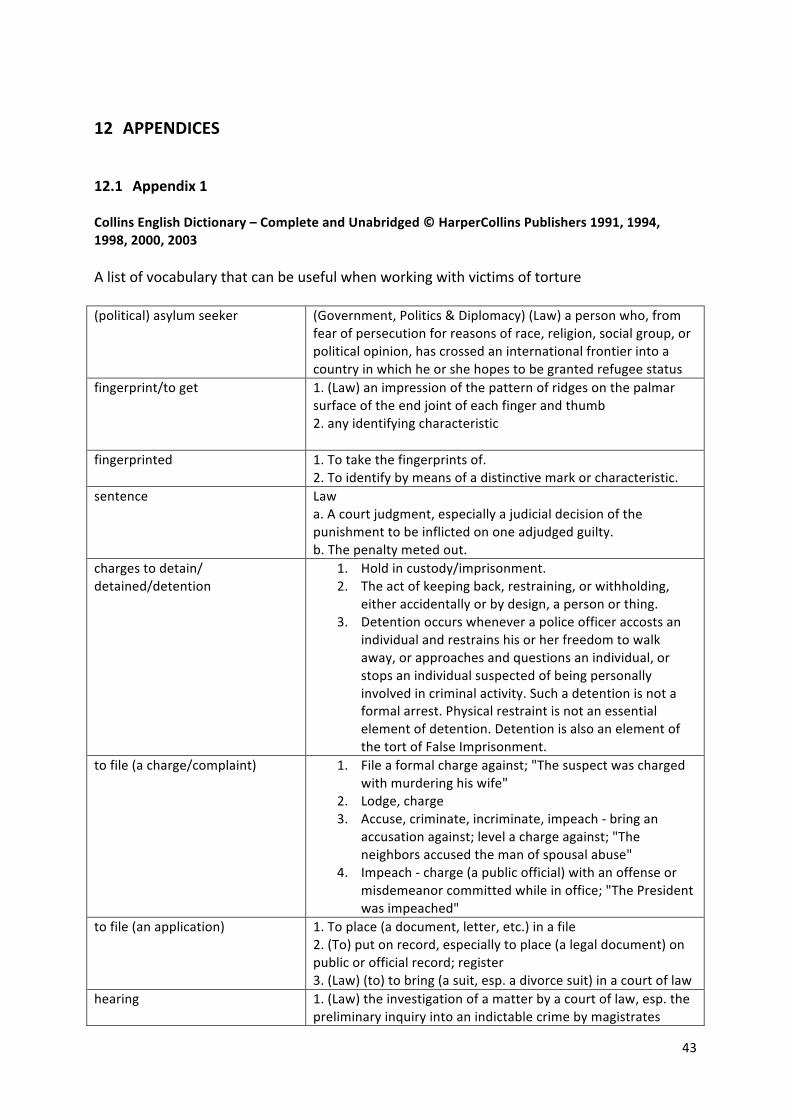
43
12 APPENDICES
12.1 Appendix 1 Collins English Dictionary – Complete and Unabridged © HarperCollins Publishers 1991, 1994, 1998, 2000, 2003 A list of vocabulary that can be useful when working with victims of torture (political) asylum seeker
(Government, Politics & Diplomacy) (Law) a person who, from fear of persecution for reasons of race, religion, social group, or political opinion, has crossed an international frontier into a country in which he or she hopes to be granted refugee status
fingerprint/to get
1. (Law) an impression of the pattern of ridges on the palmar surface of the end joint of each finger and thumb 2. any identifying characteristic
fingerprinted
1. To take the fingerprints of. 2. To identify by means of a distinctive mark or characteristic.
sentence
Law a. A court judgment, especially a judicial decision of the punishment to be inflicted on one adjudged guilty. b. The penalty meted out.
charges to detain/ detained/detention
1. Hold in custody/imprisonment. 2. The act of keeping back, restraining, or withholding,
either accidentally or by design, a person or thing. 3. Detention occurs whenever a police officer accosts an
individual and restrains his or her freedom to walk away, or approaches and questions an individual, or stops an individual suspected of being personally involved in criminal activity. Such a detention is not a formal arrest. Physical restraint is not an essential element of detention. Detention is also an element of the tort of False Imprisonment.
to file (a charge/complaint)
1. File a formal charge against; "The suspect was charged with murdering his wife"
2. Lodge, charge 3. Accuse, criminate, incriminate, impeach -‐ bring an
accusation against; level a charge against; "The neighbors accused the man of spousal abuse"
4. Impeach -‐ charge (a public official) with an offense or misdemeanor committed while in office; "The President was impeached"
to file (an application) 1. To place (a document, letter, etc.) in a file 2. (To) put on record, especially to place (a legal document) on public or official record; register 3. (Law) (to) to bring (a suit, esp. a divorce suit) in a court of law
hearing
1. (Law) the investigation of a matter by a court of law, esp. the preliminary inquiry into an indictable crime by magistrates
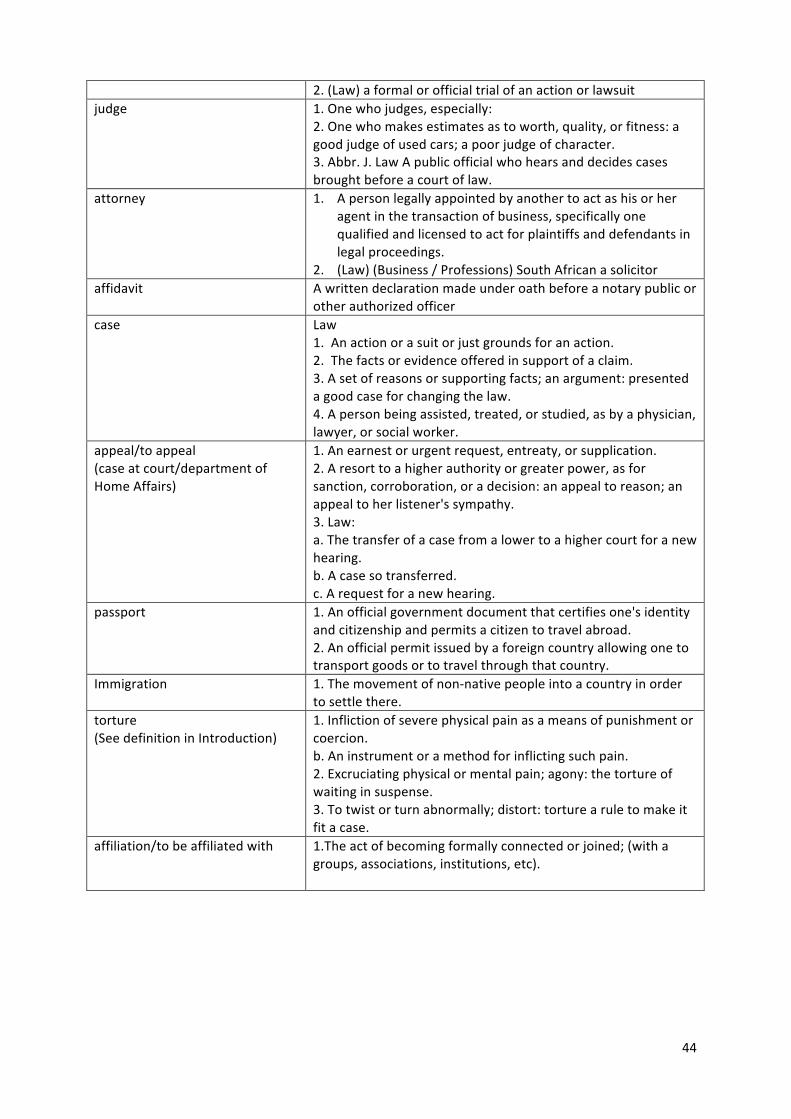
44
2. (Law) a formal or official trial of an action or lawsuit judge
1. One who judges, especially: 2. One who makes estimates as to worth, quality, or fitness: a good judge of used cars; a poor judge of character. 3. Abbr. J. Law A public official who hears and decides cases brought before a court of law.
attorney
1. A person legally appointed by another to act as his or her agent in the transaction of business, specifically one qualified and licensed to act for plaintiffs and defendants in legal proceedings.
2. (Law) (Business / Professions) South African a solicitor affidavit A written declaration made under oath before a notary public or
other authorized officer case Law
1. An action or a suit or just grounds for an action. 2. The facts or evidence offered in support of a claim. 3. A set of reasons or supporting facts; an argument: presented a good case for changing the law. 4. A person being assisted, treated, or studied, as by a physician, lawyer, or social worker.
appeal/to appeal (case at court/department of Home Affairs)
1. An earnest or urgent request, entreaty, or supplication. 2. A resort to a higher authority or greater power, as for sanction, corroboration, or a decision: an appeal to reason; an appeal to her listener's sympathy. 3. Law: a. The transfer of a case from a lower to a higher court for a new hearing. b. A case so transferred. c. A request for a new hearing.
passport 1. An official government document that certifies one's identity and citizenship and permits a citizen to travel abroad. 2. An official permit issued by a foreign country allowing one to transport goods or to travel through that country.
Immigration 1. The movement of non-‐native people into a country in order to settle there.
torture (See definition in Introduction)
1. Infliction of severe physical pain as a means of punishment or coercion. b. An instrument or a method for inflicting such pain. 2. Excruciating physical or mental pain; agony: the torture of waiting in suspense. 3. To twist or turn abnormally; distort: torture a rule to make it fit a case.
affiliation/to be affiliated with 1.The act of becoming formally connected or joined; (with a groups, associations, institutions, etc).
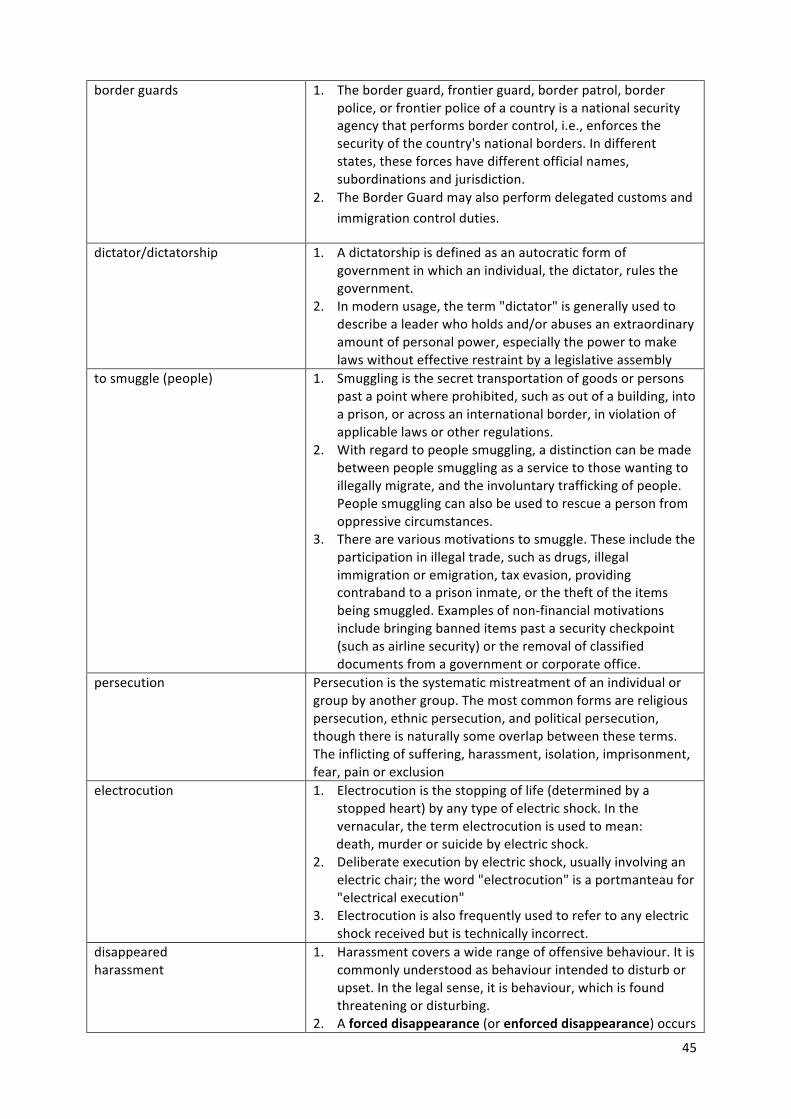
45
border guards 1. The border guard, frontier guard, border patrol, border police, or frontier police of a country is a national security agency that performs border control, i.e., enforces the security of the country's national borders. In different states, these forces have different official names, subordinations and jurisdiction.
2. The Border Guard may also perform delegated customs and immigration control duties.
dictator/dictatorship
1. A dictatorship is defined as an autocratic form of government in which an individual, the dictator, rules the government.
2. In modern usage, the term "dictator" is generally used to describe a leader who holds and/or abuses an extraordinary amount of personal power, especially the power to make laws without effective restraint by a legislative assembly
to smuggle (people)
1. Smuggling is the secret transportation of goods or persons past a point where prohibited, such as out of a building, into a prison, or across an international border, in violation of applicable laws or other regulations.
2. With regard to people smuggling, a distinction can be made between people smuggling as a service to those wanting to illegally migrate, and the involuntary trafficking of people. People smuggling can also be used to rescue a person from oppressive circumstances.
3. There are various motivations to smuggle. These include the participation in illegal trade, such as drugs, illegal immigration or emigration, tax evasion, providing contraband to a prison inmate, or the theft of the items being smuggled. Examples of non-‐financial motivations include bringing banned items past a security checkpoint (such as airline security) or the removal of classified documents from a government or corporate office.
persecution
Persecution is the systematic mistreatment of an individual or group by another group. The most common forms are religious persecution, ethnic persecution, and political persecution, though there is naturally some overlap between these terms. The inflicting of suffering, harassment, isolation, imprisonment, fear, pain or exclusion
electrocution
1. Electrocution is the stopping of life (determined by a stopped heart) by any type of electric shock. In the vernacular, the term electrocution is used to mean:
death, murder or suicide by electric shock. 2. Deliberate execution by electric shock, usually involving an
electric chair; the word "electrocution" is a portmanteau for "electrical execution"
3. Electrocution is also frequently used to refer to any electric shock received but is technically incorrect.
disappeared harassment
1. Harassment covers a wide range of offensive behaviour. It is commonly understood as behaviour intended to disturb or upset. In the legal sense, it is behaviour, which is found threatening or disturbing.
2. A forced disappearance (or enforced disappearance) occurs

46
when a person is secretly imprisoned or killed by agents of the state or by another party, such as a terrorist or criminal group. The party responsible for a disappearance does not admit to having carried out the act, thereby placing the victim outside the protection of the law.
to bribe
1. Bribery, a form of corruption, is an act implying money or gift given that alters the behavior of the recipient. Bribery constitutes a crime and is defined by Black's Law Dictionary as the offering, giving, receiving, or soliciting of any item of value to influence the actions of an official or other person in charge of a public or legal duty.
2. The bribe is the gift bestowed to influence the recipient's
conduct. It may be any money, good, right in action, property, preferment, privilege, emolument, object of value, advantage, or merely a promise or undertaking to induce or influence the action, vote, or influence of a person in an official or public capacity.
nightmare
A nightmare is a dream that can cause a strong negative emotional response from the sleeper, typically fear and/or horror. The dream may contain situations of danger, discomfort, psychological or physical terror. Sufferers usually awaken in a state of distress and may be unable to return to sleep for a prolonged period of time. [
stowaway
1. To hide aboard a ship or a plane to get free transportation; "The illegal immigrants stowed away on board the freighter"
2. hide out, hide -‐ be or go into hiding; keep out of sight, as for protection and safety
demonstration
1. The act of demonstrating 2. (Government, Politics & Diplomacy) a manifestation of grievances, support, or protest by public rallies, parades, etc. 3. A manifestation of emotion 4. (Military) a show of military force or preparedness
12.2 Appendix 267 The following guidelines are based on the Istanbul Protocol: Manual on the Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment. These guidelines are not intended to be a fixed prescription, but should be applied taking into account the purpose of the evaluation and after an assessment of available resources. Evaluation of physical and psychological evidence of torture and ill treatment may be conducted by one or more clinicians, depending on their qualifications. I. Case information Date of exam: Exam requested by (name/position): Case or report No.: Duration of evaluation: hours, minutes Subject’s given name: Birth date: Birth place: Subject’s family name: Gender: male/female:
67 United Nations. (2004). Istantbul Protocol Manual for the Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment. Professional Training Series, No 8/Rev.1. Geneva.
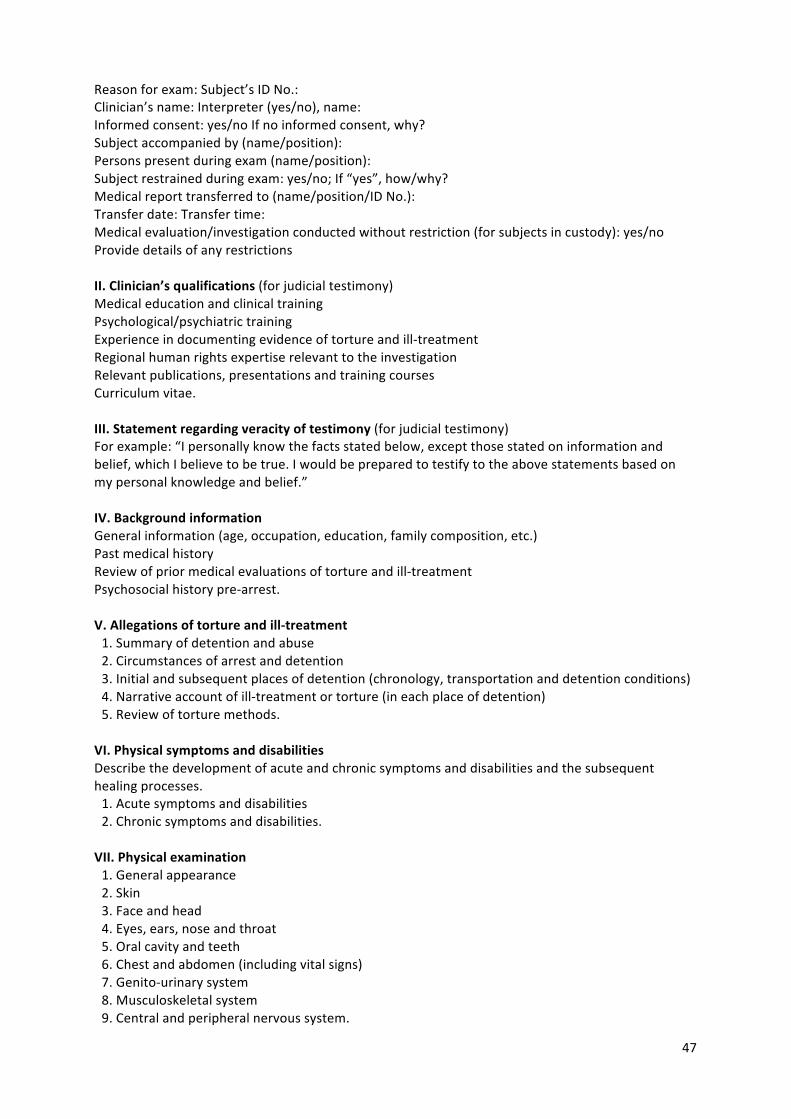
47
Reason for exam: Subject’s ID No.: Clinician’s name: Interpreter (yes/no), name: Informed consent: yes/no If no informed consent, why? Subject accompanied by (name/position): Persons present during exam (name/position): Subject restrained during exam: yes/no; If “yes”, how/why? Medical report transferred to (name/position/ID No.): Transfer date: Transfer time: Medical evaluation/investigation conducted without restriction (for subjects in custody): yes/no Provide details of any restrictions II. Clinician’s qualifications (for judicial testimony) Medical education and clinical training Psychological/psychiatric training Experience in documenting evidence of torture and ill-‐treatment Regional human rights expertise relevant to the investigation Relevant publications, presentations and training courses Curriculum vitae. III. Statement regarding veracity of testimony (for judicial testimony) For example: “I personally know the facts stated below, except those stated on information and belief, which I believe to be true. I would be prepared to testify to the above statements based on my personal knowledge and belief.” IV. Background information General information (age, occupation, education, family composition, etc.) Past medical history Review of prior medical evaluations of torture and ill-‐treatment Psychosocial history pre-‐arrest. V. Allegations of torture and ill-‐treatment 11. Summary of detention and abuse 12. Circumstances of arrest and detention 13. Initial and subsequent places of detention (chronology, transportation and detention conditions) 14. Narrative account of ill-‐treatment or torture (in each place of detention) 15. Review of torture methods. VI. Physical symptoms and disabilities Describe the development of acute and chronic symptoms and disabilities and the subsequent healing processes. 11. Acute symptoms and disabilities 12. Chronic symptoms and disabilities. VII. Physical examination 11. General appearance 12. Skin 13. Face and head 14. Eyes, ears, nose and throat 15. Oral cavity and teeth 16. Chest and abdomen (including vital signs) 17. Genito-‐urinary system 18. Musculoskeletal system 19. Central and peripheral nervous system.
48
VIII. Psychological history/examination 11. Methods of assessment 12. Current psychological complaints 13. Post-‐torture history 14. Pre-‐torture history 15. Past psychological/psychiatric history 16. Substance use and abuse history 17. Mental status examination 18. Assessment of social functioning 19. Psychological testing: (see chapter VI, sect. C.1, for indications and limitations) 10. Neuropsychological testing (see chapter VI, sect. C.4, for indications and limitations). IX. Photographs X. Diagnostic test results (see annex II for indications and limitations) XI. Consultations XII. Interpretation of findings 1. Physical evidence A. Correlate the degree of consistency between the history of acute and chronic physical symptoms and disabilities with allegations of abuse. B. Correlate the degree of consistency between physical examination findings and allegations of abuse. (Note: The absence of physical findings does not exclude the possibility that torture or ill-‐treatment was inflicted.) C. Correlate the degree of consistency between examination findings of the individual with knowledge of torture methods and their common after-‐effects used in a particular region. 2. Psychological evidence A. Correlate the degree of consistency between the psychological findings and the report of alleged torture. B. Provide an assessment of whether the psychological findings are expected or typical reactions to extreme stress within the cultural and social context of the individual. C. Indicate the status of the individual in the fluctuating course of trauma-‐related mental disorders over time, i.e. what is the time frame in relation to the torture events and where in the course of recovery is the individual? D. Identify any coexisting stressors impinging on the individual (e.g. ongoing persecution, forced migration, exile, loss of family and social role, etc.) and the impact these may have on the individual. E. Mention physical conditions that may contribute to the clinical picture, especially with regard to possible evidence of head injury sustained during torture or detention. XIII. Conclusions and recommendations 1. Statement of opinion on the consistency between all sources of evidence cited above (physical and psychological findings, historical information, photographic findings, diagnostic test results, knowledge of regional practices of torture, consultation reports, etc.) and allegations of torture and ill-‐treatment. 2. Reiterate the symptoms and disabilities from which the individual continues to suffer as a result of the alleged abuse. 3. Provide any recommendations for further evaluation and care for the individual. XIV. Statement of truthfulness (for judicial testimony) For example: “I declare under penalty of perjury, pursuant to the laws of ........ (country), that the foregoing is true and correct and that this affidavit was executed on ................. (date) at ............. (city), ............ (State or province).”
49
XV. Statement of restrictions on the medical evaluation/investigation (for subjects in custody) For example: “The undersigned clinicians personally certify that they were allowed to work freely and independently and permitted to speak with and examine (the subject) in private, without any restriction or reservation, and without any form of coercion being used by the detaining authorities”; or “The undersigned clinician(s) had to carry out his/her/their evaluation with the following restrictions: ...........” XVI. Clinician’s signature, date, place XVII. Relevant annexes A copy of the clinician’s curriculum vitae, anatomical drawings for identification of torture and ill treatment, photographs, consultations and diagnostic test results, among others.