join the centerwatch community centerwatch...join the centerwatch community centerwatch ... watch
TRANSCRIPT

Volume 24, Issue 03. © 2020 CenterWatch. All rights reserved.
Join the CenterWatch Community!
see Focus on Supply Chain on page 6 »
see Ask the Experts on page 6 »
January 20, 2020
Industry Briefs…2
Up and Coming…4
Drug & Device Pipeline News…8Twenty-three drugs and devices have entered a new trial phase this week.
JobWatch…9
CenterWatchWeekly
This monthly feature presents a variety of questions from clinical trial profes-sionals with answers from WCG Clini-
cal’s expert staff. This issue features advice from WCG PFS Clinical’s Alexandra Opitz, lead clinical research analyst, and Amanda Miller, lead clinical research analyst/training program manager.
Question: How do we get monitoring fees in the
budget? It is hard to get sponsors to pay for monitoring. How do you charge for remote monitoring? Charging per page could be overwhelming.
Answer: We like to include monitor fees in every
initial round of budget negotiations. If the sponsor removes it in the first round of ne-
gotiations, then we almost always push back and provide a detailed explanation of why the sponsor should pay for the monitoring visit. Additionally, cost documentation can be provided.
We typically charge an hourly rate for remote monitoring because per page is over-whelming and difficult to track. Many sponsors will not agree to an open-ended hourly rate, so we will put a cap on the number of hours. For example, $40 per hour up to three hours.
Question:What parameters should we take into
account to develop a more realistic and ac-curate budget?
Answer:There are several parameters to consider.
Ask the Experts: Making the Most of Your Budget
By Brandon May
A s clinical trial executives continue to look at ways of speeding startup, one item that bears looking at is
how clinical supply management is handled.The ideal time for a clinical supply man-
ager to enter a study is six months or more before the first subject’s enrollment or be-fore the protocol has even been developed, says Reid Tonik, director of clinical supply chain and project management at Catalent.
Sites that do not employ an early supply-chain strategy before protocol development often put unnecessary risk or delay into the trial.
A product’s shelf life is probably the most substantial supply chain factor that needs to be assessed at the outset of a study, Tonik said.
“A short shelf life, or one that will be updated and extended several times throughout the study, can dictate the entire supply strategy,” he added. Some products may have shelf lives shorter than that of the trial’s planned dura-tion, which would affect how products will be shipped and stored during the study.
Additionally, expiry date requirements often vary from country to country. An optimal supply management strategy, said Tonik, is aware of and works with expiry labeling requirements of each country to reduce the risk of running into problems during the trial.
Supplies with extreme temperature requirements, such as deep-frozen storage, will often need early and novel solutions to
Focus on Supply Chain Management to Speed Trial Startups
NEW WHITE PAPERS AVAILABLE
Understanding theRTF LetterPractical guidance on what theFDA is looking for, and howto avoid receiving one.
From YourEncore
LEARN MORE
centerwatch.com/whitepapers
Understanding the RTF LetterPractical guidance on what the FDA is looking for, and how to avoid receiving one
Written by Hugh Donovan, Managing Expert, YourEncore Clinical Center of Excellence
| White Paper
NEW WHITE PAPERS AVAILABLE
Effectively Addressing the Challenges of Pediatric Clinical Trials with Patient-Centric Best PracticesFrom Firma Clinical Research
LEARN MORE
centerwatch.com/whitepapers
Effectively Addressing the Challenges of Pediatric Clinical Trials with Patient- Centric Best Practices
WHITE PAPER
Mike Keens
Firma Clinical Research
Ursula SakowiczAssociate Director, Remote Visit Services Firma Clinical Research
Learn about best practicesto effectively manage andexecute clinical trials withResearch Practitioner.
» Earn ANCC contact hours»» Subscriptions at $197
SUBSCRIBE TODAY
Caution for NIH's single IRB policy for multi-site researchBy Sue Coons, MA
A tions had to comply with the National Institutes of Health’s (NIH’s) Final
NIH Policy on the Use of a Single Institutional Review Board for Multi-Site Researchpolicy established the expectation that a single institutional review board (sIRB) of record would be used in the ethical review of non-exempt human subjects research protocols funded by NIH that are carried out at more than one site in the United States.
It does not apply to career development, research training, or fellowship awards.
However, some institutions continue to be concerned about their ability to adhere to the policy and the cost of doing so. IRB executives say it is wise to be cautious. Some institutions could spend millions of dollars to upgrade their IRB infrastructure, while some IRBs already have many of the policy requirements in place. In addition, one IRB executive worries that past NIH actions
show that the agency could revise its policy
Emerging trends in clinical research: The need for changeBy John W. Mitchell, MS
T by emerging trends in the clinical trial research sector, consider insight from
a business author and a businessman/politi-cian. In his groundbreaking book, Good to Great: Why Some Companies Make the Leap…And Others Don’t,” Jim Collins wrote:
“Good is the enemy of great. And that is one of the key reasons why we have so little that becomes great. We don’t have great schools, principally because we have good schools. We don’t have great government, principally because we have good govern-ment.”
Secretary Donald Rumsfeld noted that one of the biggest threats to security was driven by factors that fell under the category of “we
don’t know what we don’t know.” In recent issues, Research Practitioner has
explored individual key emerging trends in clinical research, including patient centricity, eMobile advances, and precision medicine. As stand-alone trends, these innovations hold great promise and excitement.
But what insight is gained when all emerg-ing trends are considered in totality? What
clinical research? As Rumsfeld alluded, what might we not know that we don’t know? Are current advancements in clinical research, as Collins asserted, relevant enough to power (great) the sector beyond the status quo (good), given the rapidly evolving medical
ligence (AI), and the expectation of patients?
results on the use of electronic-sourced data, Hugo Stephenson, executive chairman of DrugDev and a physician investigator, observed: “I’m surprised and disappointed there hasn’t been much improvement in the entire clinical trial process, including the
© 2018 CenterWatch. Duplication or sharing of this publication is strictly prohibited. Volume 19, Number 3
Learning Objectives/Outcomes:1. Explain the need for change in clinical research.
2. List key drivers of transformation in clinical trials.
3. Describe examples of clinical trial research trends in action.
4. Discuss why the clinical trial sector will make the jump from trends to practice.
Learning Objectives/Outcomes:1. List the details that local IRBs may know about their
study populations as opposed to a single IRB.2. Describe NIH’s reasoning for going to a single IRB
policy for multi-site research.3. Discuss the impact of using a single IRB on a study’s
direct costs.4. Explain the concern about NIH’s history of choosing
the lowest-cost provider.
42 CE program information
43 Issues in research management
52 SMART IRB
55 CE post-test
May–June 2018
see Emerging trends on page 44
see Single IRB on page 49
ruary 2017 CenterWatch article about survey
s of Jan. 25, 2018, research institu-
200+ GCP questionsyou never thought to ask
and their answers
ORDER TODAY
Get answers to GCP questions clinical research professionals ask of OGCP.
GCP Questions, FDA AnswersGCP Questions, FDA Answers
2019 Edition

© 2020 CenterWatch CWW2403
CenterWatch Weekly (ISSN 1528-5731)
Beth Belton Editorial DirectorStephanie Akers ProductionRussell Titsch Business Development Director
© 2020 CenterWatch. All rights reserved. No part of this publication may be distributed or reproduced in any form or by any means without the express written consent of the publisher.
CenterWatch Main and Editorial Offices 300 N. Washington St., Suite 200, Falls Church, VA 22046 [email protected] / [email protected]
Permission requests can be emailed to [email protected].
Advertising packages and reprints are available:Email [email protected] or call 703.538.7651.
continues on next page »
WCG | CWWeekly January 20, 2020 2 of 9
Industry Briefs
Weigh Expedited Approval Benefits Against Health Risks, Researchers RecommendThe expedited approval pathways imple-mented by the FDA in the past 30 years have shortened many drugs’ road to mar-ket, but a new study from Harvard Universi-ty researchers questions whether the time saved outweighs the risks of approving new drugs without putting them through the traditional clinical trial process.
Of all drugs approved by the FDA in 2018, 81 percent followed at least one of the expedited pathways, according to the study published on the Journal of the American Medical Association online infor-mation service, JAMA Network.
Two of the programs in particular have relaxed the agency’s usual rigorous stan-dards of evidence. The Fast-Track designa-tion allows sponsors to submit new drug applications without data from phase 3 efficacy trials, the study’s authors say, and the Accelerated Approval pathway allows the use of surrogate measures that may be “only reasonably likely to predict clinical benefit” as substitutes for tradi-tional endpoints.
The result of this regulatory flexibility, the study’s authors say, is that the number of approvals based on data from at least two pivotal trials has decreased dramati-cally in the past 25 years. In the period from 1995 to 1997, 80 percent of approved drugs had undergone the traditional trial process. By 2015, that number had de-creased to 52.8 percent.
The Breakthrough Therapy designation has been increasingly popular with spon-sors because it encourages alternative clini-cal trial designs that may be smaller and faster to complete. Under this program, av-erage development times have decreased from 8 years to 4.8 years. But the research-ers argue that because this program’s name implies “a large magnitude of benefit,” its approved drugs have been misinterpreted
as having “higher levels of efficacy than has necessarily been demonstrated.”
And although sponsors qualifying for the Accelerated Approval pathway are required to conduct postapproval studies to verify their drugs’ clinical benefit, the researchers say the rate of completion has been inadequate, pointing out that by 2015 only 54 percent of studies required of sponsors in 2009 and 2010 had been completed and 20 percent had not even been started.
The researchers call for Congress, the research community or both to periodically reevaluate the balance between approv-ing drugs more quickly with less clinical evidence and the risk of rushing potentially unsafe products to market.
To read the article, click here: https://bit.ly/38l92z3.
Biogen to Buy Potential Alzheimer’s, Parkinson’s Drug from PfizerBiogen has agreed to purchase Pfizer’s early-stage neurological disease drug and initiate a phase 1b clinical study of the experimental drug in the fourth quarter of 2020.
The company plans to develop the CK1 inhibitor, PF-05251749, for treating sundowning in Alzheimer’s patients and irregular sleep-wake rhythm disorder in Parkinson’s patients.
Biogen will pay Pfizer $75 million plus royalties and up to $635 million in future payments.
Biogen and Japanese partner Eisai took a hit last March when they halted two global phase 3 trials for aducanumab, a drug that aims to slow progression of Alzheimer’s disease. But Biogen announced in October that it had changed course on the investigational drug following further data analysis and would seek the FDA’s approval after all (CenterWatch Weekly, October 28, 2019).
AstraZeneca Halts Fish Oil Drug TrialAstraZeneca has discontinued its large phase 3 clinical trial of Epanova, a fish oil-derived heart drug.
Hoping to imitate the successful results seen with Amarin’s Vascepa, AstraZeneca initiated the STRENGTH trial to dem-onstrate that Epanova was a beneficial add-on to statins for mixed dyslipidemia. The AstraZeneca trial had enrolled 13,086 patients at 675 sites across 22 countries.
With the closing of the STRENGTH trial, AstraZeneca will take a $100 million writedown on all inventories and will re-evaluate the drug’s current value of $533 million as an intangible asset.
FDA Places Partial Hold on Innate’s Lymphoma Trial After CMO IssuesThe FDA has placed Innate Pharma’s phase 2 trial studying anti-KIR3DL2 antibody lacutamab on partial clinical hold after learning that its contract manufacturing
© 2020 CenterWatch CWW2403
WCG | CWWeekly January 20, 2020 3 of 9
Industry Briefs (continued from page 2)
organization (CMO) stopped production and filed for bankruptcy.
The partial clinical hold will allow investigators to continue treating existing patients in the U.S. But patient enrollment has been suspended until the company finds a new CMO, which is expected to hap-pen before the second half of 2020.
UPMC Sets Aside $1 Billion to Develop New Diverse Treatment PortfolioUniversity of Pittsburgh Medical Center’s (UPMC) venture capital arm has announced that it is setting aside $1 billion to develop new drugs and devices to treat cancer, respira-tory disease, autoimmune disease and neuro-inflammation, among other conditions.
The initial focus of UPMC was on the de-velopment of immunotherapies for cancer, aging and transplantation, but the aim of the unit its capital arm is funding has now expanded its aim to reach other diseases where unmet clinical needs exist. UPMC recently invested in Werewolf Therapeutics, a biotech startup studying new immuno-therapies for cancer, contributing to a $56 million Series A funding deal that included other investors.
Virtual Trials Appear Promising, But Industry Reservations PersistMore than half of site startups have not considered running a completely virtual trial, according to a survey by Industry Standard Research.
In its survey, Industry Standard Research, a market research firm, queried site startup experts on their stance on implementing virtual clinical trials. Approximately 54% of surveyed sites reported that they have not considered running virtual trials, compared with 20% of sites that are currently in the process of evaluating the potential of using virtual trials in the future. Only 3% of sites are currently running virtual trials.
UK Online Map Helps Thames Valley Residents Find Nearby Clinical TrialsResidents of the Thames Valley region in the UK can now search an online, inter-active map for sites near them that are conducting clinical trials in the National Health Service.
Thames Valley Research map, spon-sored by the National Institute for Health Research Clinical Research Network Thames
Valley and South Midlands, offers users the ability to browse for nearby studies by medical specialty, keyword, postcode and study name.
Axsome Licenses Pfizer Trial Data for Narcolepsy Treatment Axsome Therapeutics has entered into a new agreement with Pfizer that will give it exclusive license to Pfizer’s clinical and non-clinical data as well as intellectual property rights for reboxetine, an active drug product being tested as a treatment for narcolepsy.
The data includes Pfizer’s relevant non-clinical studies, short-term trials and long-term trials that include over 5,000 patients. Axsome will also gain exclusive rights to engineer and market Pfizer’s late-stage esreboxetine (AXS-14), a U.S. product can-didate for fibromyalgia treatment. Licensed data will include results of a positive phase 3 trial and positive phase 2 trial of AXS-14 in patients with fibromyalgia.
Recently, Axsome released positive results of a phase 2 trial for AXS-12, its version of narcolepsy treatment rebox-etine, and the company is now initiating phase 3 trials.
By John W Mitchell
Frustration about clinical trial start-up costs is not unlike Sisyphus’ dilemma. A host of long-standing expense and
such uphill headwinds for the clinical trial sector. According to some sources, such problems even threaten the viability of the sector. Sites complain they incur more over-head costs driven by regulatory documen-tation, antiquated data collection and the demands of precision medicine to name a few — all without increased compensation from sponsors and CROs. A recent study supports this concern. Researchers at the
-opment found that the study start-up phase
remained unchanged for the past decade. -
ing investments in technology are getting trials done faster. None of this bodes well for smaller, independent players.
“Sites are doing more work for [fewer] patients. We used to enroll about eight pa-
-sley, CEO at IACT Health. His company
-ger, and there are more procedures per pa-tient per day. So, you’re doing loads more work, but you’re only paid when you put
themselves — you put fewer patients in tri-als today.”
According to Kingsley, the only way to -
pate in three times as many concurrent tri-
from an overhead standpoint to have one trial that places eight patients, rather than three trials that place eight patients.
Also, at a time when technology is con-
technology is compounding problems in the clinical trial sector. In each of the three studies he cites above, it’s likely that three
sponsors. When each sponsor uses their own networks and devices for patient-re-ported outcomes, it adds to site workload and time.
“We have no ability to standardize tech-nology,” Kingsley says “We have to do so many trials with so many sponsors, and they have their own decision-making…
-bia (standardization between sponsors and sites).”
As an example, he cites the advantages of sites adopting electronic platforms such as eSource. Using such a platform could save billions compared to the aggregate cost of
documents. Clinically, an electronic plat-form also prevents errors such as entering a blood pressure incorrectly or performing a patient procedure out of order from the test protocol.
“We’re trying to convince the industry
Start-up Costs Can Be an Uphill Slog in Need of Change
Status Quo is Not a Viable Option: A Host of Challenges Strain Clinical Trial Site Viability
September 2018 A CenterWatch Publication Volume 25, Issue 09
By John W Mitchell
C roblem
gish payments, contract viability, preferred site status, interconnectivity and something less tangible — a lack of consideration in the
-ry care sites in Canada.
see Start-up Costs on page 6
In this issue3-4 In Review
Regulatory Update
5 Action Items
Part 4: How to Identify Candidate Fraudulence Early in The Recruitment CycleBy Angela Roberts
Top Considerations for Using Digital Health Devices in Clinical TrialsBy Vicki Gashwiler
Risk-based Quality Management: The New NormalBy Brion Regan
10-11 Pipeline NewsFDA Actions
The CenterWatch MonthlyISSN 1556-3367
Editorial DirectorProduction
© 2018 CenterWatch, LLC. All rights reserved.No part of this publication may be distributed orreproduced in any form or by any means without the express written consent of the publisher. Permission requests can be obtained via fax at (617) 948-5101 or emailed at [email protected]. Single-user annual subscriptions start at $399.
For inquiries on multi-reader and corporate
InReview
Rare, Adrenal Gland Tumors
drug Azedra for rare cancers of the adre-
therapy OK’d for these tumors. -
apy drug that attacks tumors with a high,
with inoperable locally advanced or metas-tic cancers called phenochromocytoma and paraganglioma.
Pheochromocytoma forms inside and paraganglioma grows outside the adrenal gland(s).
Both tumor types release hormones that can cause symptoms including high blood pressure, rapid heartbeat and anxiety.
University of Pennsylvania research-
percent who received at least one dose and
license is held by Progenics Pharmaceuticals.
Japan Greenlights Parkinson’s Trial
scientists have won approval from Japanese regulators to test adult stem cells as a possible treatment for Parkinson’s disease.
Induced pluriopotent stem cells (iPS) are derived from skin or blood cells and induced back into an embryonic-like plu-ripotent state that can divide into more stem cells or become any type of cell in the body, leading to a potentially unlimited source of any type of human cell needed
-ered promising for regenerative research
-man cells and, also, avoid controversy sur-rounding stem cells from human embryos.
Researchers plan to transplant iPS cells into the brains of Parkinson’s patients in the hope they will help repair or replace
Regulatory Update
Unique content, critical analysis & expert market research Subscribe to the industry’s leading global news source.
Subscribe Today! www.centerwatch.com/cwmonthly
www.centerwatch.com CONTACT SALES: [email protected] | 617.948.5100
» In-depth analytical reports on key trends» Key regulatory updates» Subscriptions start at $399
© 2020 CenterWatch CWW2403
This feature highlights changes in clinical trial organizations’ personnel.
AbbVieAfter its recent $63 billion acquisition of Allergan, AbbVie has announced a new executive team of the company. Richard Gonzalez, CEO of AbbVie, will head the merged company, and Michael Severino will continue as president and will oversee research and development (R&D). Other executive team members will include Carlos Alban as chief commercial officer, Henry Gosebruch as strategy officer, Robert Mi-chael as financial officer, and Azita Saleki-Gerhardt as president of operations. Carrie Strom, Allergan’s senior vice president of the U.S. medical aesthetics division, will lead Allergan Aesthetics, a new global business unit in AbbVie.
ADC TherapeuticsJoseph Camardo has been named ADC Therapeutics’ new head of medical affairs. Most recently, Camardo was the senior vice president of Celgene Global Health.
AffirmedAndreas Harstrick has been appointed to the position of chief medical officer at Affirmed, which will start in March 2020. Prior to this ap-pointment, Harstrick was chief medical officer at Molecular Partners.
AltasciencesPaul Sidney has been appointed to the position of senior director of compliance and regulatory affairs. Previously, Sidney served as executive director QA of mergers and acquisi-tions at Charles River Laboratories.
AMAG PharmaceuticalsAMAG Pharmaceuticals has announced that William Heiden, CEO of the organiza-tion, will step down from his position. The board of directors at AMAG is now launch-ing a search for Heiden’s replacement,
which is expected to be completed in the middle of the year.
AntengeneMark J. Alles has been named as Anten-gene’s independent director, joining the organization from his most recent 16-year tenure position as chairman and CEO of Celgene.
Arcturus TherapeuticsSteve Hughes is now serving as the chief development officer at Arcturus Therapeutics. Hughes has spent the past 20 years leading medical affairs and clinical development teams at several biopharma companies.
Carisma TherapeuticsDebora Barton was appointed to the role of chief medical officer at Carisma Therapeutics, joining the company after serving as the senior vice president of clinical and safety at Iovance Biotherapeutics.
Cellectar BiosciencesIgor Grachev has been named Cellectar Biosciences’ chief medical officer. Prior to this appointment, Grachev served as global devel-opment leader and head of innovative clinical trials initiative, R&D at TEVA Pharmaceuticals.
Clasado BioSciencesLucien Harthoorn has been appointed to the position of R&D director of Clasado BioSciences.
Dyve BiosciencesChuck Harbert has been recruited by Dyve Biosciences to be the company’s new chief scientific officer.
FibroGenFibroGen has appointed Enrique Conter-no as the company’s new CEO. Conterno was most recently a senior vice president at Eli Lilly.
Fred HutchinsonThomas Lynch, chief scientific officer at Bristol-Myers Squibb, is now president and director at Fred Hutchinson Cancer Research Center.
GlaxoSmithKlineDeborah Waterhouse, CEO of ViiV Health-care, has been appointed to the corporate executive team at GlaxoSmithKline (GSK).
GuerbetGuerbet has appointed Thomas McLaugh-lin to the position of vice president for the company’s North America division. Previously, McLaughlin served as the organization’s general manager of North American sales and service.
Immuneering Howard L. Kaufman has been appointed to the position of head of R&D at Immuneering. Prior, Kaufman was chief medical officer at Replimune Group.
Intrexon (Precigen) Helen Sabzevari will join Intrexon, now named Precigen, as the organization’s newest CEO. Sabzevari joined the subsidiary in June 2017.
IpsenIpsen has named Steven Hildemann as the biotech company’s new executive vice president and chief medical officer. Previously, Hildemann was the chief medical officer at Germany’s Merck.
Kronos BioWes Trotter has been appointed to the posi-tion of vice president of chemistry at Kronos Bio. Prior, Trotter served as director of discov-ery chemistry at Merck.
MBX BiosciencesMBX Biosciences has announced the appoint-ment of Kent Hawryluk to the position of president and CEO. Hawryluk has since served
WCG | CWWeekly January 20, 2020 4 of 9
Up and Coming
continues on next page »
© 2020 CenterWatch CWW2403
WCG | CWWeekly January 20, 2020 5 of 9
Up and Coming (continued from page 4)
as partner of Twilight Venture partners. Greg Davis has been named the vice president of product development at MBX.
Pieris PharmaceuticalsIngmar Bruns is now senior vice president and head of clinical development at Pieris Pharmaceuticals. Previously, Bruns served as the company’s vice president of clinical de-velopment. Pieris has also appointed Shane Olwill, the organization’s vice president of development and immuno-oncology, to the position of senior vice president and head of translational science.
Revitope OncologySteve Arkinstall will now serve as the CEO of Revitope Oncology, joining the company after previously serving as CEO of Elstar Therapeutics.
RhythmRhythm has announced the resignation of Keith Gottesdiener from the role of
president and CEO. A search committee has been formed by the company’s board of directors to find its new chief executive.
Rubius TherapeuticsRubius Therapeutics has announced the appointment of Laurence Turka to the position of the company’s first chief scientific officer. Prior to joining Rubius, Turka was the chief scientific officer at Rheos Medicines, where he was a co-founder.
SanionaRami Levin has been appointed to the role of CEO of Saniona after recently holding the role of president of Sobi.
The Carlyle GroupFollowing his former role as CEO and chair-man at Pfizer, Ian Read is joining The Carlyle Group as the new operating executive.
TheragnosticsAlex Jackson has been appointed to the posi-tion of head of R&D at Theragnostics. Jackson was previously responsible for the discovery phase of immune-oncology PET projects at GE Healthcare. Theragnostics has also named Ar-chie Hale as the company’s director of clinical operations. Previously, Hale was involved with drug development at Biogen, BTG and Roche, in addition to other small biotech companies.
Turnstone BiologicsTurnstone Biologics has named Saryah Azmat as the company’s new senior vice president of business development and corporate strategy. Previously, Azmat served as the global lead for Oncology Search & Evaluation at Bristol-Myers Squibb.
Waverley PharmaTheron Odlaug, CEO at Waverley Pharma, has recently announced his resignation from the company.
Sandra “SAM” Sather, MS, CCRC
The CRC’s Guide to Coordinating Clinical Research
FOURTH EDITION The guide covers key topics like specific GCP regulations, principles of informed consent, writing and training on SOPs, IRB requirements and more:
n Site feasibility studiesn Study initiation, monitoring and
closeoutn Devices and biologics research
n Documentation & data integrityn Investigational product
accountabilityn Adverse event reporting
n Interacting with sponsors, CROs and clinical trial monitors
n Study protocols and case report forms
A vital resource for both novice and experienced clinical research coordinatorsThis new edition of The CRC’s Guide is a one-volume training masterpiece that covers the roles and responsibil-ities of all key parties involved in managing clinical trials.
Order today at www.centerwatch.com/crcguide

© 2020 CenterWatch CWW2403
WCG | CWWeekly January 20, 2020 6 of 9
Features
Focus on Supply Chaincontinued from page 1
maintaining the product’s viability through-out the trial and up to the time of patient dosing. To reduce the risk of exposing products to adverse conditions that may potentially impact their potency or viability,
supply-management systems may wish to consider real-time temperature monitoring of supplies.
In addition, Tonik emphasized the importance of clearly establishing and as-signing roles and responsibilities to team members who will oversee specific steps
in the clinical supply chain at the start of the trial. A written and agreed-upon Responsible, Accountable, Consulted, and Informed (RACI) document can ensure that management tasks have a defined scope and timing, all with clear ownership and accountability.
Ask the Expertscontinued from page 1
Time and effort items are budgeted using hourly rates for the physician, nurse and/or study coordinator. Many sites pick average physician, nurse and coordinator hourly rates to use for budgeting. It is also important to make sure that items with CPT codes are accurately budgeted. These costs typically come from a Chargemaster or Medicare rates. If a rate cannot be found in the Chargemaster or through Medicare, then it is important to obtain a cost quote for the item/service.
There are several administrative fees that can be included in a budget. At a minimum, every budget should include a startup fee, an annual renewal fee and a close-out fee. These three fees cover periods of the study where there is a heavy administrative burden on the site. The amount charged for these fees will vary by site and site structure. Be able to pro-vide documentation and breakdown of how these fees were calculated. Many sponsors will request this information. If this information is not available, it is unlikely that the sponsor will pay the full amount.
Question:What suggestions do you have for renego-
tiating a portion of the budget?
Answer:In order to renegotiate the budget, it is
important to have justification of why an item should be added into the budget or a price should be increased. The justification can be as simple as a required activity tak-ing twice as long as expected and necessi-tating a budget update to more accurately reflect the cost. If justification is provided, then most sponsors are amenable to renegotiating a portion of the budget. In our renegotiation experience, the sponsor/CRO has already seen similar requests from other sites. A common area for renegotia-tion is screen fails. If the sponsor caps screen fails, we often add language into the budget stating that after the screen fail cap is reached, the site may renego-tiate the budget to include additional screen failures.
Question:We have had difficulty negotiating
reimbursement for subject-screening activity. On some studies, we can spend multiple hours each week searching through charts of patients who end up not enrolling in the study. Do you have any recommendations as to how to get this time reimbursed?
Answer:We recommend adding a pre-screening
fee or chart review fee to the budget. We include language that states the fee is to cover time spent reviewing patient charts. The fee can be a flat fee per month or it can be an hourly rate up to a certain number of hours per week or per month.
Question:How do you handle sponsors that will
not agree to pay for overhead on patient travel reimbursement?
Answer:A possible solution to this problem is to
add a travel reimbursement processing fee to the budget that will be charged each time patient travel must be reimbursed. Some sponsors may not be able to accept overhead on the actual item but may be able to accept a processing fee. Another option would be to increase the coordinator fee in the per patient budget to account for this activity.
If overhead is mandatory at your institution, then we recommend sending the sponsor the institutionwide overhead documentation. We work with several insti-tutions that have their research overhead published online, and the link can be easily provided to the sponsor/CRO.
Learn more: www.centerwatch.com/events REGISTER TODAY
Increase Compliance, Reduce Risk with Integrated Digital SolutionsPresented by Patricia Santos-Serrao, RAC, Director, Product Strategy, MasterControl
A CenterWatch Webinar Wednesday, Feb. 12, 2020 • 1:30 p.m. - 3:00 p.m. EST
FEB
12

© 2020 CenterWatch CWW2403
WCG | CWWeekly January 20, 2020 7 of 9
For more than years we have overseen more research than all other IRBs combined.
Learn more about working with the gold standard in IRB review: www.wcgclinical.com/services/irb/
wcgclinical.com
More than 10,000 protocols
Nearly 24,000 investigators
More than 112,000 sites
Every day, WCG supports:
With Five Decades of Clinical Research Experience – We Are the “Gold Standard” in Ethical Review
Consider - WCG participates in over 90% of all FDA New Drug Approvals.
© 2020 CenterWatch CWW2403
WCG | CWWeekly January 20, 2020 8 of 9
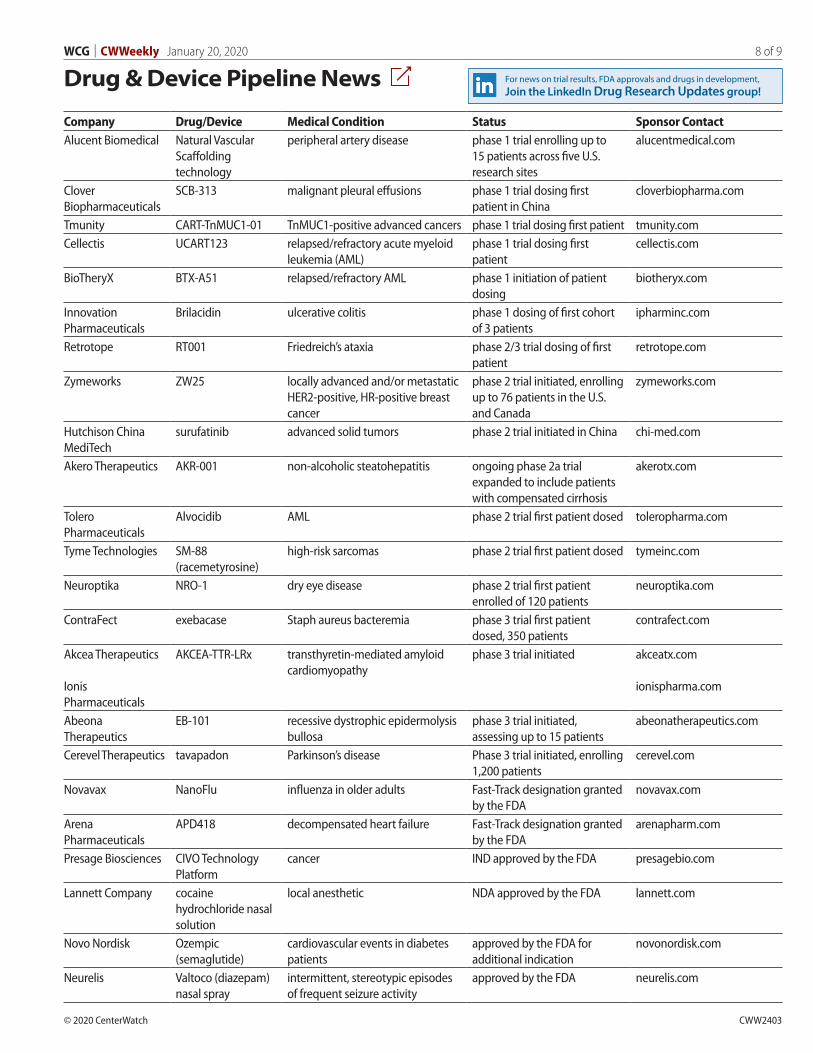
Drug & Device Pipeline News
Company Drug/Device Medical Condition Status Sponsor ContactAlucent Biomedical Natural Vascular
Scaffolding technology
peripheral artery disease phase 1 trial enrolling up to 15 patients across five U.S. research sites
alucentmedical.com
Clover Biopharmaceuticals
SCB-313 malignant pleural effusions phase 1 trial dosing first patient in China
cloverbiopharma.com
Tmunity CART-TnMUC1-01 TnMUC1-positive advanced cancers phase 1 trial dosing first patient tmunity.comCellectis UCART123 relapsed/refractory acute myeloid
leukemia (AML)phase 1 trial dosing first patient
cellectis.com
BioTheryX BTX-A51 relapsed/refractory AML phase 1 initiation of patient dosing
biotheryx.com
Innovation Pharmaceuticals
Brilacidin ulcerative colitis phase 1 dosing of first cohort of 3 patients
ipharminc.com
Retrotope RT001 Friedreich’s ataxia phase 2/3 trial dosing of first patient
retrotope.com
Zymeworks ZW25 locally advanced and/or metastatic HER2-positive, HR-positive breast cancer
phase 2 trial initiated, enrolling up to 76 patients in the U.S. and Canada
zymeworks.com
Hutchison China MediTech
surufatinib advanced solid tumors phase 2 trial initiated in China chi-med.com
Akero Therapeutics AKR-001 non-alcoholic steatohepatitis ongoing phase 2a trial expanded to include patients with compensated cirrhosis
akerotx.com
Tolero Pharmaceuticals
Alvocidib AML phase 2 trial first patient dosed toleropharma.com
Tyme Technologies SM-88 (racemetyrosine)
high-risk sarcomas phase 2 trial first patient dosed tymeinc.com
Neuroptika NRO-1 dry eye disease phase 2 trial first patient enrolled of 120 patients
neuroptika.com
ContraFect exebacase Staph aureus bacteremia phase 3 trial first patient dosed, 350 patients
contrafect.com
Akcea Therapeutics
Ionis Pharmaceuticals
AKCEA-TTR-LRx transthyretin-mediated amyloid cardiomyopathy
phase 3 trial initiated akceatx.com
ionispharma.com
Abeona Therapeutics
EB-101 recessive dystrophic epidermolysis bullosa
phase 3 trial initiated, assessing up to 15 patients
abeonatherapeutics.com
Cerevel Therapeutics tavapadon Parkinson’s disease Phase 3 trial initiated, enrolling 1,200 patients
cerevel.com
Novavax NanoFlu influenza in older adults Fast-Track designation granted by the FDA
novavax.com
Arena Pharmaceuticals
APD418 decompensated heart failure Fast-Track designation granted by the FDA
arenapharm.com
Presage Biosciences CIVO Technology Platform
cancer IND approved by the FDA presagebio.com
Lannett Company cocaine hydrochloride nasal solution
local anesthetic NDA approved by the FDA lannett.com
Novo Nordisk Ozempic (semaglutide)
cardiovascular events in diabetes patients
approved by the FDA for additional indication
novonordisk.com
Neurelis Valtoco (diazepam) nasal spray
intermittent, stereotypic episodes of frequent seizure activity
approved by the FDA neurelis.com
For news on trial results, FDA approvals and drugs in development, Join the LinkedIn Drug Research Updates group!

© 2020 CenterWatch CWW2403
WCG | CWWeekly January 20, 2020 9 of 9
Upcoming Event HighlightsThe Source for Clinical Research Jobs and Career Resources
More Jobs
[ V IE W ALL JOB L IS T INGS ]
Twice monthly, CWWeekly provides featured listings of clinical research job openings, upcoming industry conferences and educational programs from JobWatch, CenterWatch’s online recruitment website for both clinical research employers and professionals.
Jobs via Kelly Services
[ V IE W ALL KELLY SER V ICE S J OBS ]
Marketing Director - Employee Engagement & Internal CommunicationsWIRB-Copernicus Group (WCG)Princeton, NJ
Data CoderKMR GroupChicago, IL
Senior Financial Reporting AnalystWIRB-Copernicus Group (WCG)Princeton, NJ
Document Processor Western Inst. Review BoardPuyallup, WA
Assistant Director, Center for Clinical Research EducationMassachusetts General HospitalBoston, MA
Senior VP & Chief Data Officer WIRB-Copernicus Group (WCG)Princeton, NJ
Director, Service EngagementWIRB-Copernicus Group (WCG)Hamilton, NJ
Recruiting CoordinatorWIRB-Copernicus Group (WCG)Hamilton, NJ
Sr Clinical Scientist South San Francisco, CA
Senior Manager/ AD of Biostatistics South San Francisco, CA
Clinical Trials Associate Foster City, CA
Clinical Project Associate Foster City, CA
Medical Director, Hematology South San Francisco, CA
Contact Center Representative - 2nd Shift Cincinnati, OH
Clinical Support Coordinator Associate Rancho Cordova, CA
Process EngineerIndianapolis, IN
Executive Administrative Assistant Columbia, MD
Project Manager - Scientific St Charles, MO
Product Data Analyst West Chester, PA
Clinical Research Associate (CRA) San Diego, CA
Clinical Research Scientist Somerville, NJ
Clinical Research Scientist Blue Ash, OH
Conferences
SEPTEMBER 9 – SEPTEMBER 10, 2020
CLINICAL TRIAL RISK AND PERFORMANCE MANAGEMENT SUMMIT
Philadelphia, PA
[ V IE W A LL CONFER ENCES ]
Webinars
J A N UA R Y 2 3 , 2 0 2 0
REAL-WORLD EVIDENCE AND DATA: A TUFTS STUDY OF 30 PHARMA COMPANIES
1:30 p.m. - 3:00 p.m. EST
The Tufts Center for the Study of Drug Development (CSDD) investigated how the industry is using real-world data (RWD) and real-world evidence (RWE). The study of 30 biopharmaceutical companies includes current and planned used of RWD, operational issues and return on investment and performance areas impacted by RWE.
F E B R UA R Y 1 2 , 2 0 2 0
INCREASE COMPLIANCE, REDUCE RISK WITH INTEGRATED DIGITAL SOLUTIONS: CREATE A CONNECTED SYSTEM AND STREAMLINE YOUR OPERATIONS
1:30 p.m. - 3:00 p.m. EST
Win that coveted first-to-market spot. When you integrate your digital solutions you’ll streamline operations, improve quality and mitigate risk. First to market is just around the corner.
[ V IE W A LL WEB INAR S ]
JobWatch