juan carles contel, department of health, chronic care program, catalonia
DESCRIPTION
The Journey from a Chronic Care Program toward an Integrated Health and Social Care ModelTRANSCRIPT
The journey from a Chronic
Care Program towards a
model of Integrate health and
social care
Session structure
• A new Health Plan and the introduction of a new STORY
• Chronicity Prevention and Care
Program: the “journey” toward Integrated Care
• Towards a new evaluation framework:
The first results • A new journey toward a new Integrated
health and social care model
• Promoting self-care of the patient and citizen: Catalonian Expert Patient Program. Towards new Virtual care model
Catalan Healthcare System: some basic features
• Area: 32,106 km2
• Population: 7,611,711 inhabitants. 17% over 65 y.
(expected 32% in 2050)
• 1780 € expenditure per capita and 1150 € public expenditure
per capita in 2012
• Life expectancy: 82.27 years
• Gross Mortality rate (2010):8/1,000 inh.
• Infant mortality (2010): 2.6 /1,000 live births
• 369 Primary Health Centres (PHC) ranging from 20-45,000
inh)
• 69 “acute hospitals” (no far from 50 Km. from every home)
• 96 health-social centres (residential homes: long-stay,
convalescence, pal.liative care)
• 41 Mental Health Centres
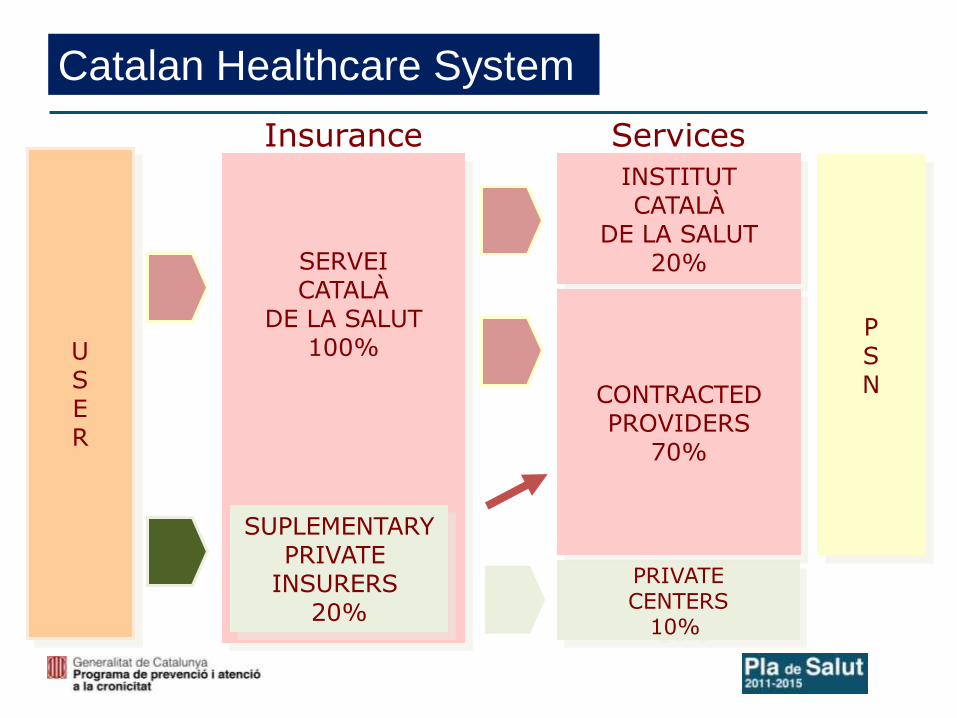
Catalan Healthcare System
U S E R
SERVEI CATALÀ
DE LA SALUT 100%
SUPLEMENTARY PRIVATE
INSURERS 20%
INSTITUT CATALÀ
DE LA SALUT 20%
PRIVATE CENTERS
10%
P S N CONTRACTED
PROVIDERS 70%
Insurance Services
Source: Catalan Health Plan 2011-2015.
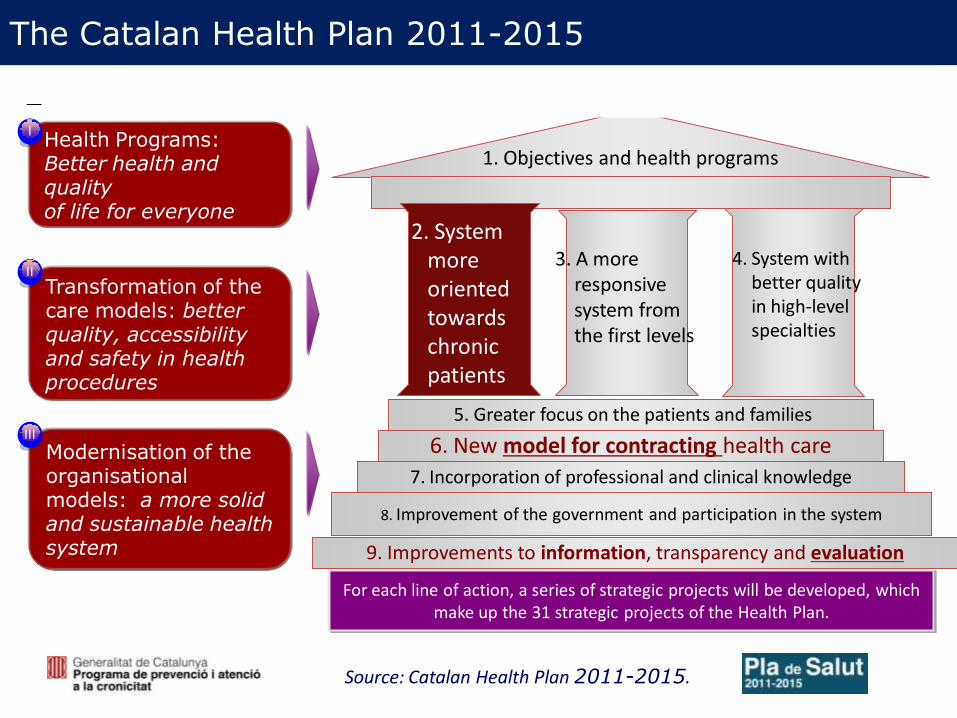
The Catalan Health Plan 2011-2015
Health Programs: Better health and quality of life for everyone
Transformation of the care models: better quality, accessibility and safety in health procedures
Modernisation of the organisational models: a more solid and sustainable health system
I
II
III
For each line of action, a series of strategic projects will be developed, which make up the 31 strategic projects of the Health Plan.
9. Improvements to information, transparency and evaluation
1. Objectives and health programs
7. Incorporation of professional and clinical knowledge
6. New model for contracting health care
5. Greater focus on the patients and families
8. Improvement of the government and participation in the system
2. System more oriented towards chronic patients
3. A more responsive system from the first levels
4. System with better quality in high-level specialties
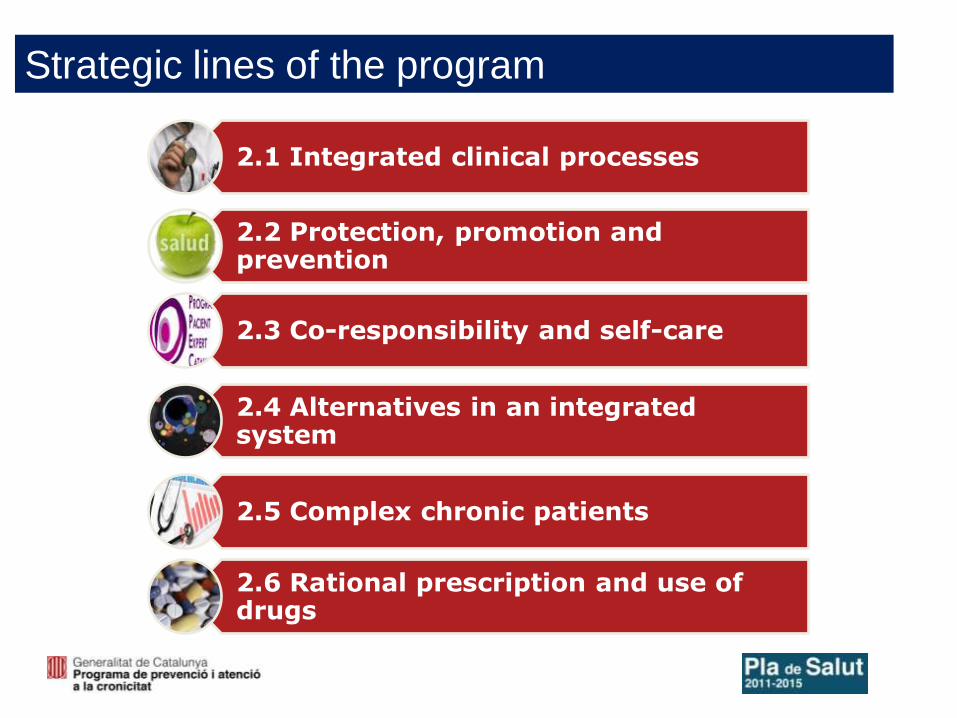
2.1 Integrated clinical processes
2.2 Protection, promotion and prevention
2.3 Co-responsibility and self-care
2.4 Alternatives in an integrated system
2.5 Complex chronic patients
2.6 Rational prescription and use of drugs
Strategic lines of the program
7
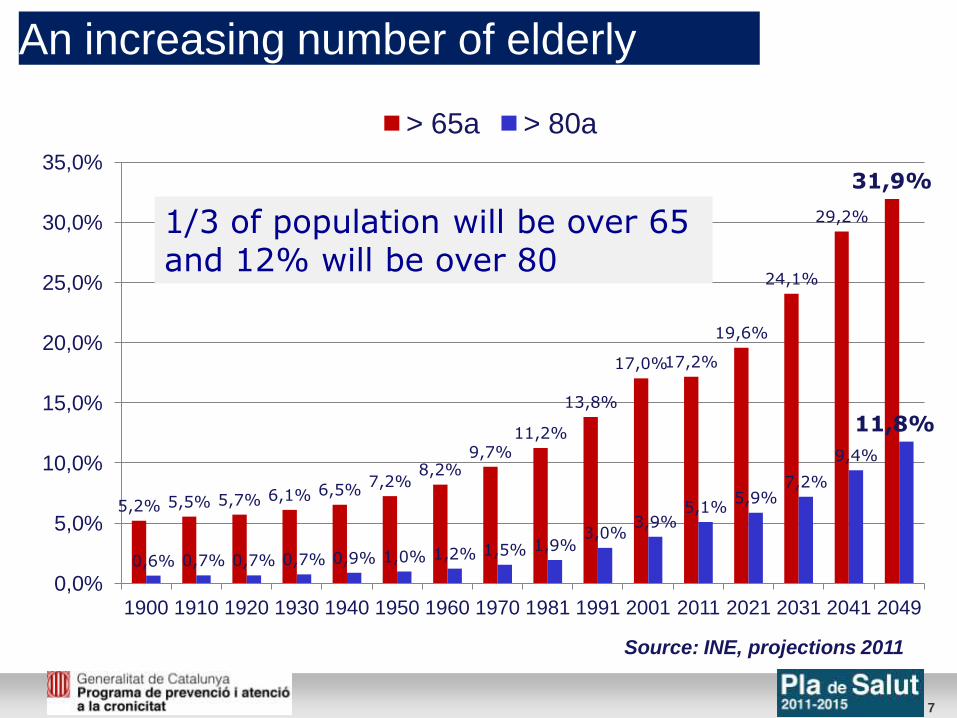
An increasing number of elderly
5,2% 5,5% 5,7% 6,1% 6,5% 7,2%
8,2% 9,7%
11,2%
13,8%
17,0% 17,2%
19,6%
24,1%
29,2%
31,9%
0,6% 0,7% 0,7% 0,7% 0,9% 1,0% 1,2% 1,5% 1,9% 3,0%
3,9% 5,1%
5,9% 7,2%
9,4%
11,8%
0,0%
5,0%
10,0%
15,0%
20,0%
25,0%
30,0%
35,0%
1900 1910 1920 1930 1940 1950 1960 1970 1981 1991 2001 2011 2021 2031 2041 2049
> 65a > 80a
Source: INE, projections 2011
1/3 of population will be over 65 and 12% will be over 80
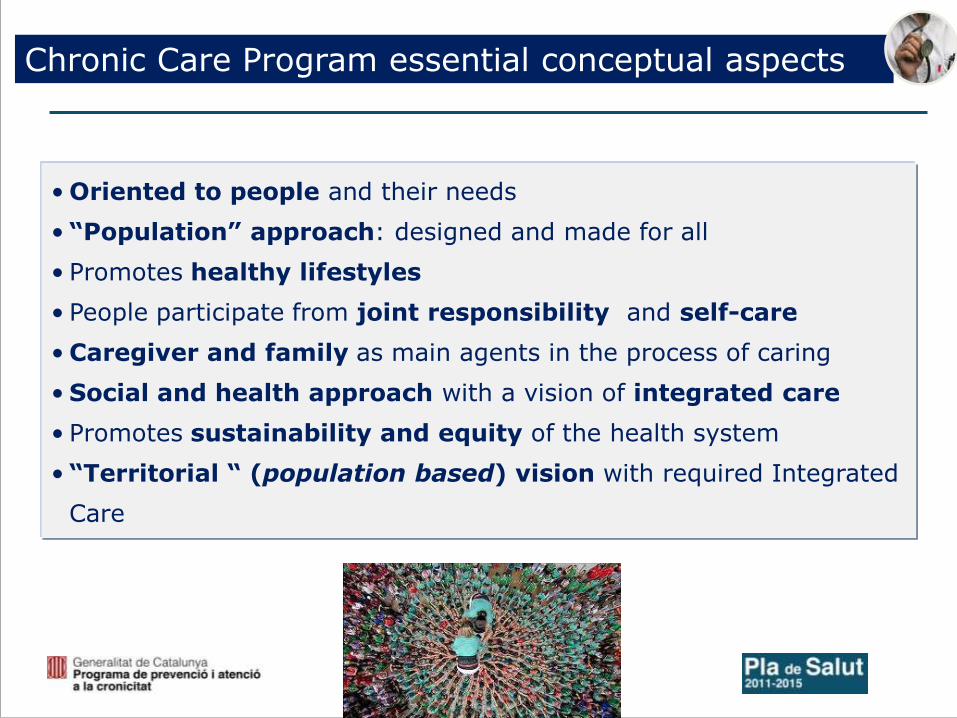
Chronic Care Program essential conceptual aspects
• Oriented to people and their needs
• “Population” approach: designed and made for all
• Promotes healthy lifestyles
• People participate from joint responsibility and self-care
• Caregiver and family as main agents in the process of caring
• Social and health approach with a vision of integrated care
• Promotes sustainability and equity of the health system
• “Territorial “ (population based) vision with required Integrated
Care
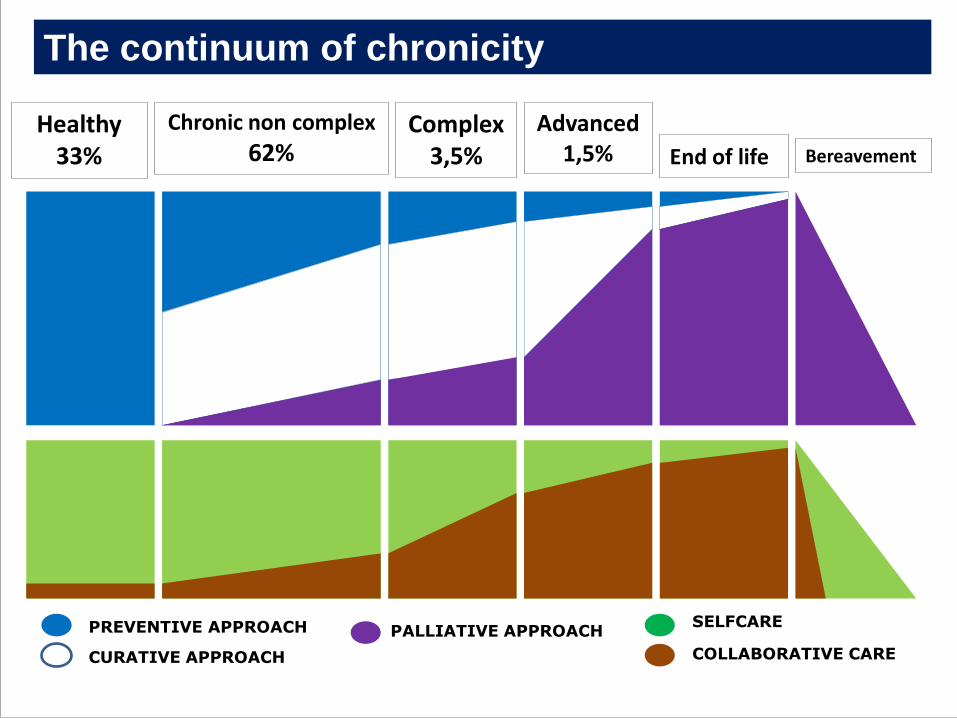
Healthy 33%
Chronic non complex
62% Complex
3,5%
Advanced 1,5% End of life Bereavement
PREVENTIVE APPROACH
CURATIVE APPROACH
PALLIATIVE APPROACH SELFCARE
COLLABORATIVE CARE
The continuum of chronicity
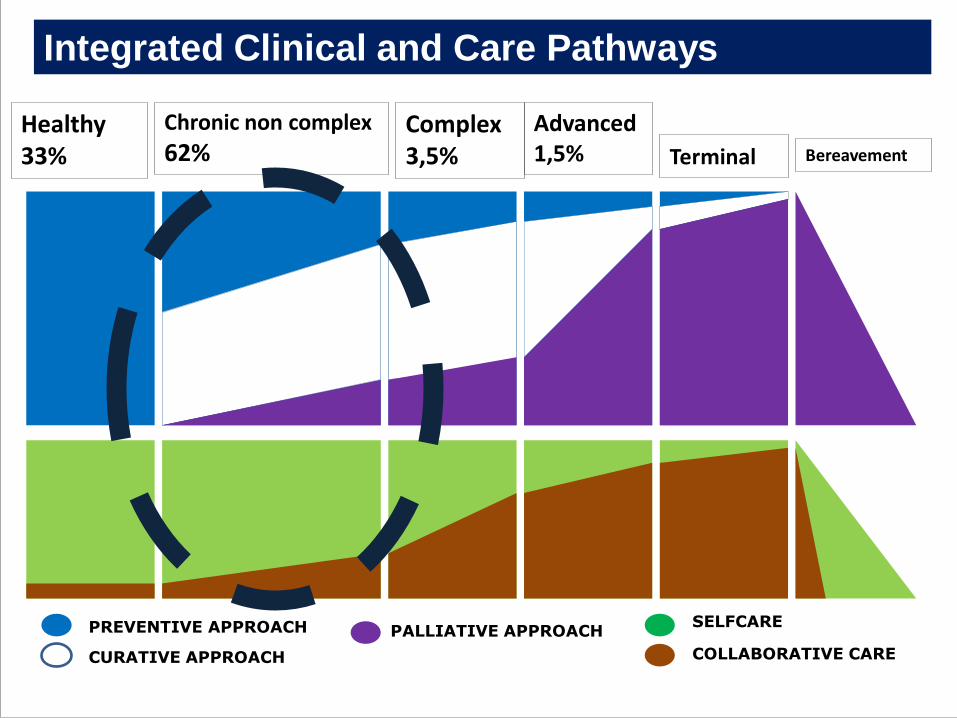
Healthy 33%
Chronic non complex
62% Complex 3,5%
Advanced 1,5% Terminal Bereavement
PREVENTIVE APPROACH
CURATIVE APPROACH
PALLIATIVE APPROACH SELFCARE
COLLABORATIVE CARE
Integrated Clinical and Care Pathways
• Integrated Care Pathways as a formal agreement among
professional clinical leaders at local level
• Based on reference clinical guidelines
• How to implement best evidence practice
• Critical key points identification
• Critical variables uploaded at Shared Clinical record
• 80% of territories implemented 3 of 4 chronic
conditions: COPD, depression, heart failure and DM2. Now
Complex Cronic Care Pathways work
• Other 6 conditions to be included in the future
11
Integrated Care Pathways
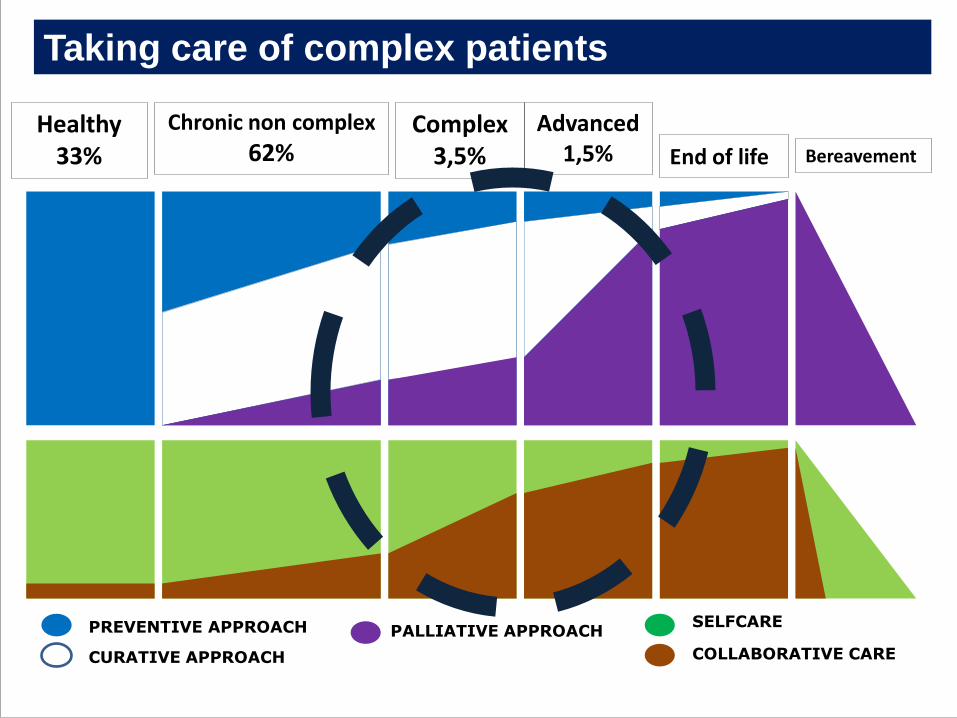
Healthy 33%
Chronic non complex
62% Complex
3,5%
Advanced 1,5% End of life Bereavement
PREVENTIVE APPROACH
CURATIVE APPROACH
PALLIATIVE APPROACH SELFCARE
COLLABORATIVE CARE
Taking care of complex patients
Taking care of complex patients
▪ Stratification model /predictive model
▪ Model of care for patients with complexity
▪ Palliative care-oriented model in persons with advanced chronic disease
▪ Collaborative model between health services and social services: integrated health and social care
14
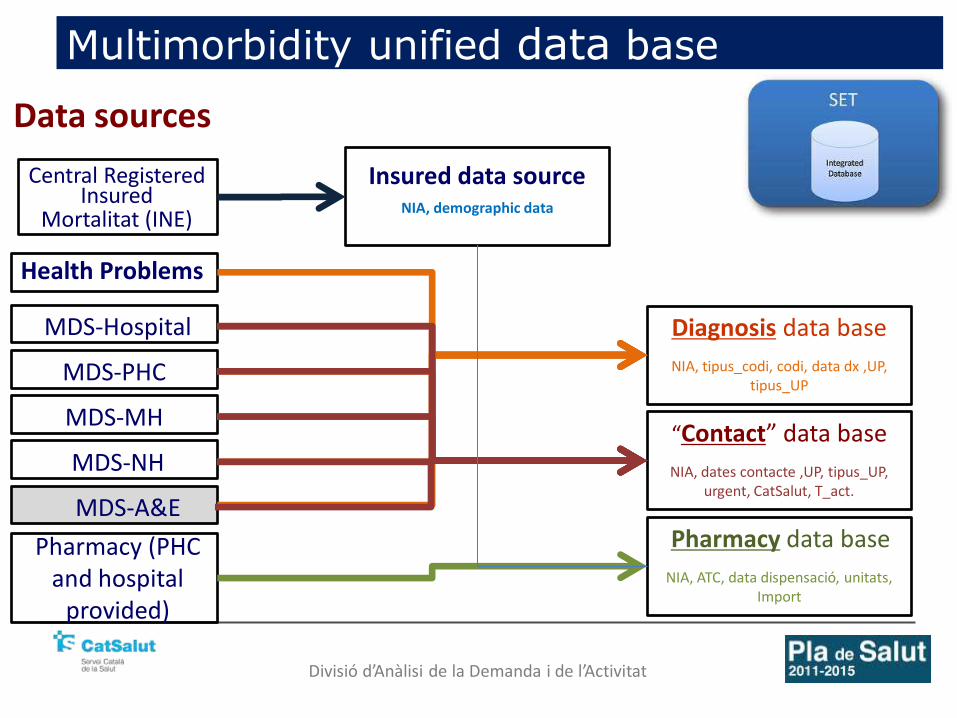
Multimorbidity unified data base
Insured data source NIA, demographic data
Diagnosis data base
NIA, tipus_codi, codi, data dx ,UP, tipus_UP
“Contact” data base
NIA, dates contacte ,UP, tipus_UP, urgent, CatSalut, T_act.
MDS-Hospital
MDS-PHC
MDS-MH
MDS-NH
MDS-A&E
Central Registered Insured
Health Problems
Pharmacy (PHC and hospital
provided)
Pharmacy data base
NIA, ATC, data dispensació, unitats, Import
Mortalitat (INE)
Data sources
Divisió d’Anàlisi de la Demanda i de l’Activitat
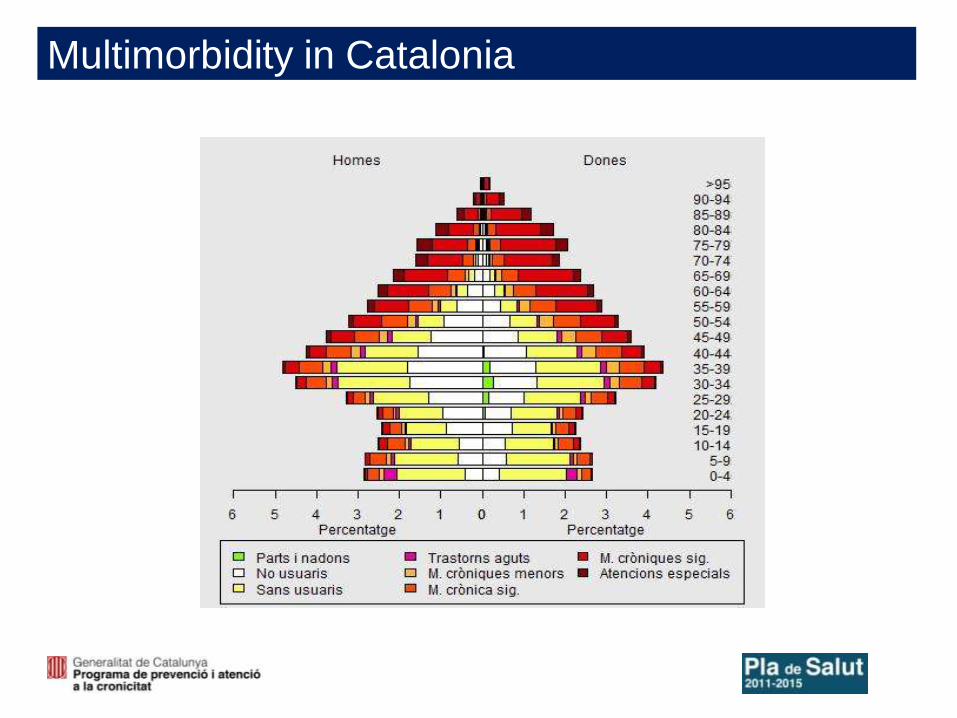
Multimorbidity in Catalonia
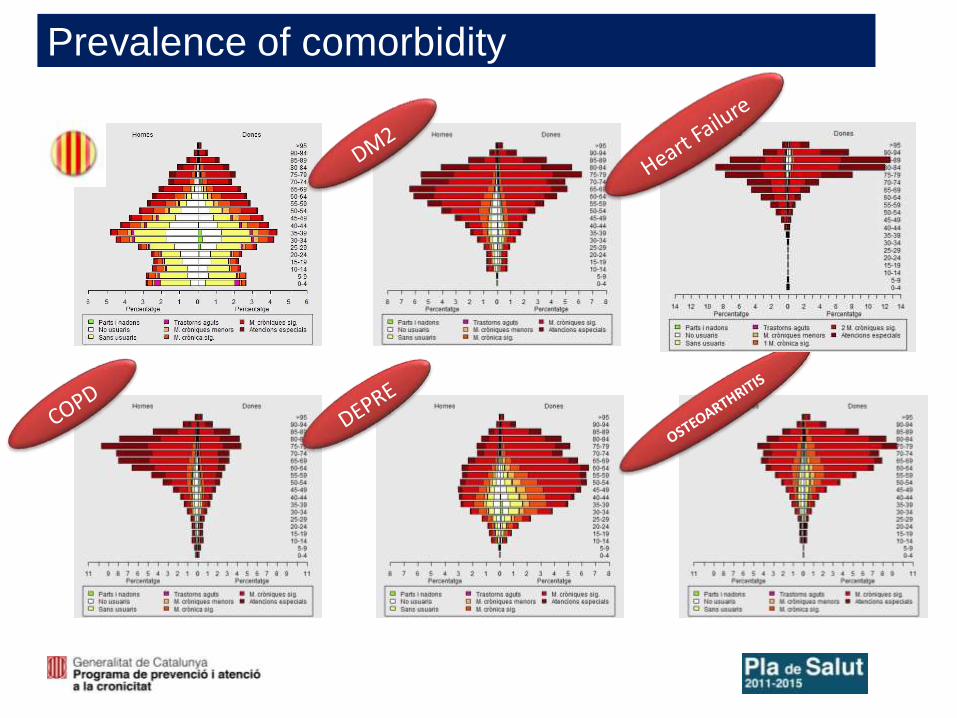
Prevalence of comorbidity
17
PCC Multimorbidity
Severe unique disease Advanced frailty
MACA Limited live prognosis Palliative approach,
Advance care planning
Two profiles of complexity
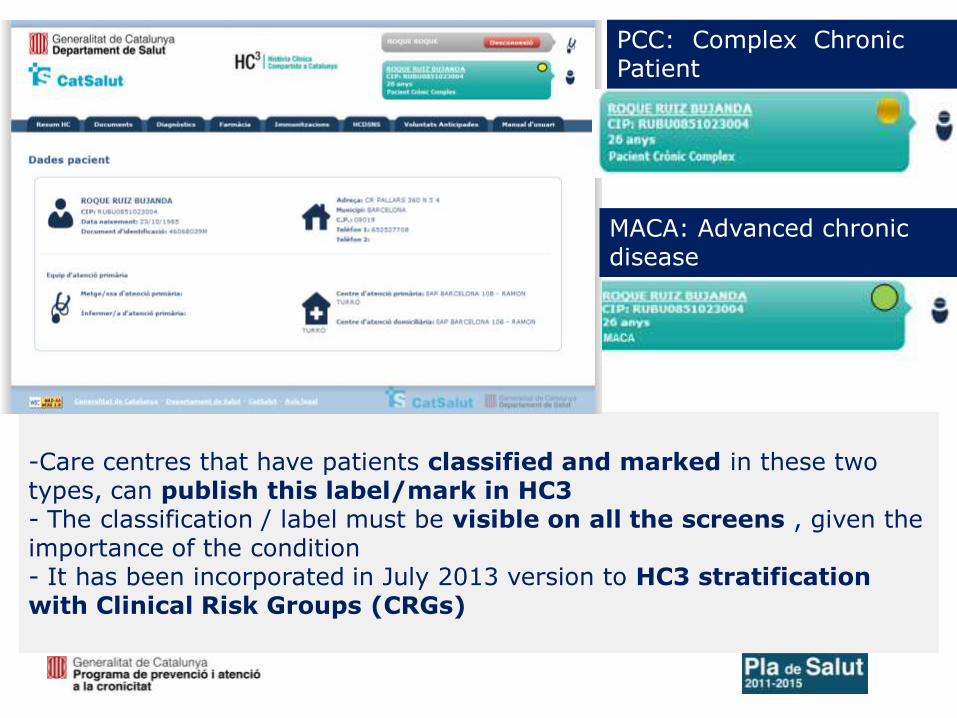
-Care centres that have patients classified and marked in these two types, can publish this label/mark in HC3 - The classification / label must be visible on all the screens , given the importance of the condition - It has been incorporated in July 2013 version to HC3 stratification with Clinical Risk Groups (CRGs)
PCC: Complex Chronic Patient
MACA: Advanced chronic disease
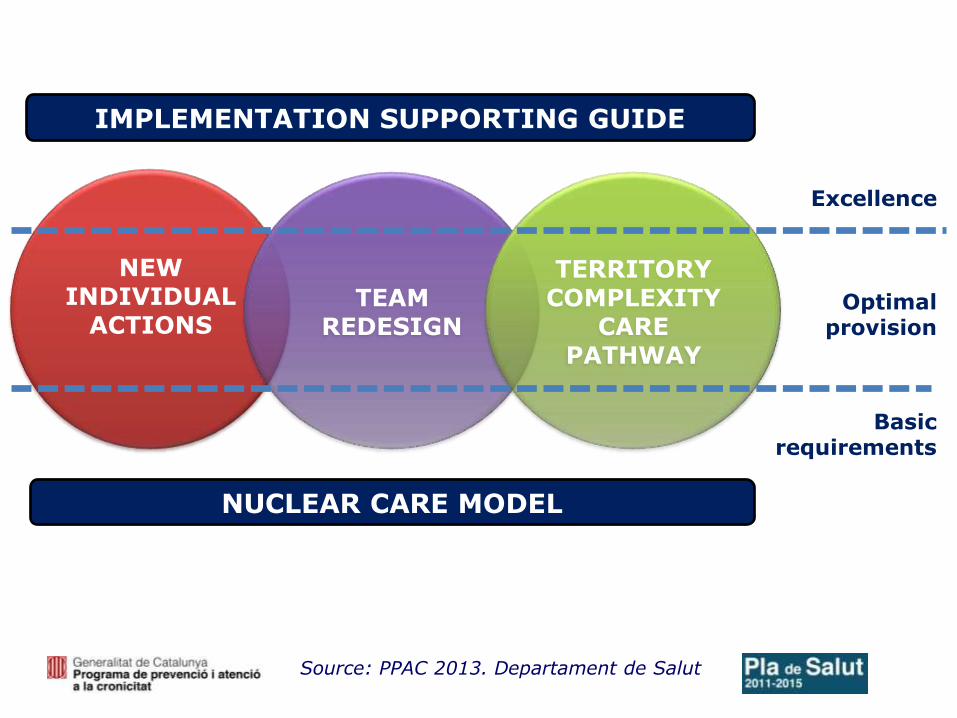
NUCLEAR CARE MODEL
IMPLEMENTATION SUPPORTING GUIDE
Source: PPAC 2013. Departament de Salut
NEW INDIVIDUAL
ACTIONS
TEAM REDESIGN
TERRITORY COMPLEXITY
CARE PATHWAY
Basic requirements
Optimal provision
Excellence
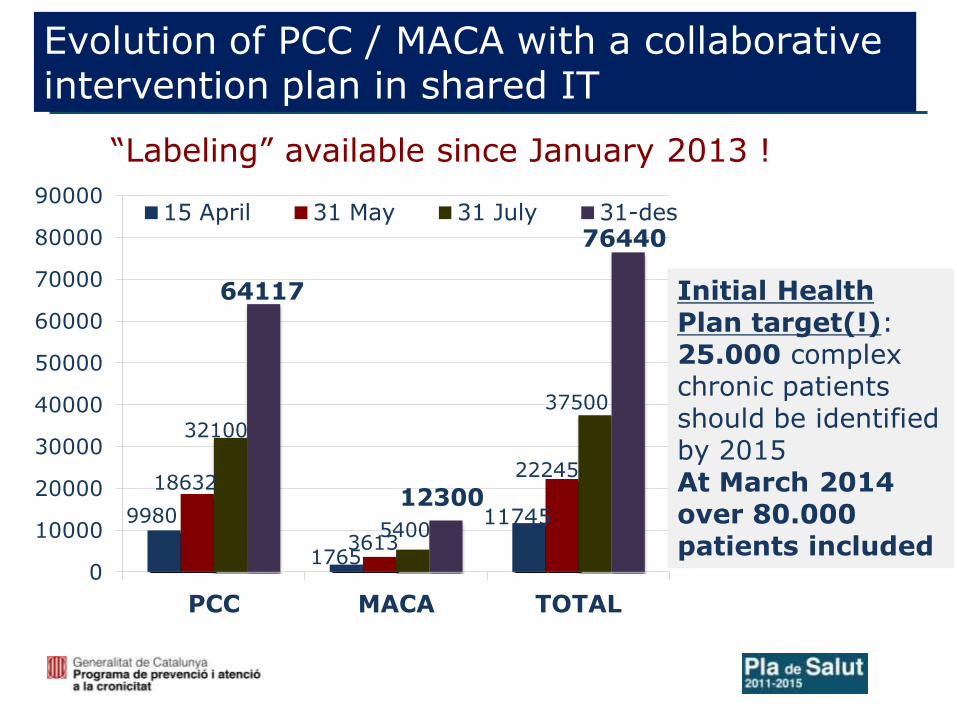
9980
1765
11745
18632
3613
22245
32100
5400
37500
64117
12300
76440
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
PCC MACA TOTAL
15 April 31 May 31 July 31-des
Initial Health Plan target(!): 25.000 complex chronic patients should be identified by 2015 At March 2014 over 80.000 patients included
Evolution of PCC / MACA with a collaborative intervention plan in shared IT
“Labeling” available since January 2013 !
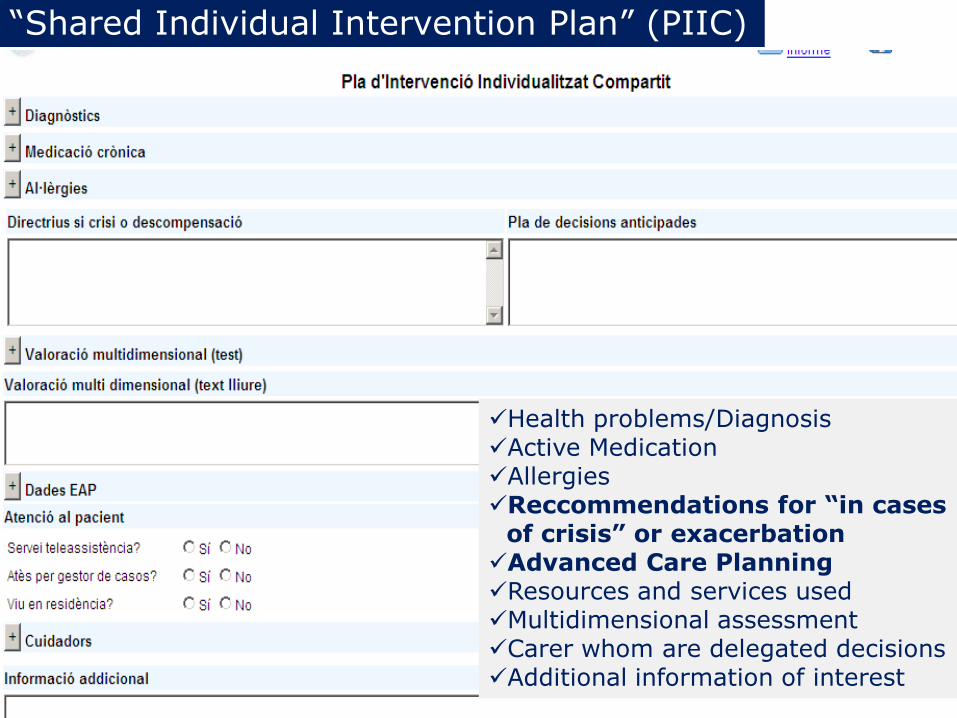
“Shared Individual Intervention Plan” (PIIC)
Health problems/Diagnosis Active Medication Allergies Reccommendations for “in cases
of crisis” or exacerbation Advanced Care Planning Resources and services used Multidimensional assessment Carer whom are delegated decisions Additional information of interest
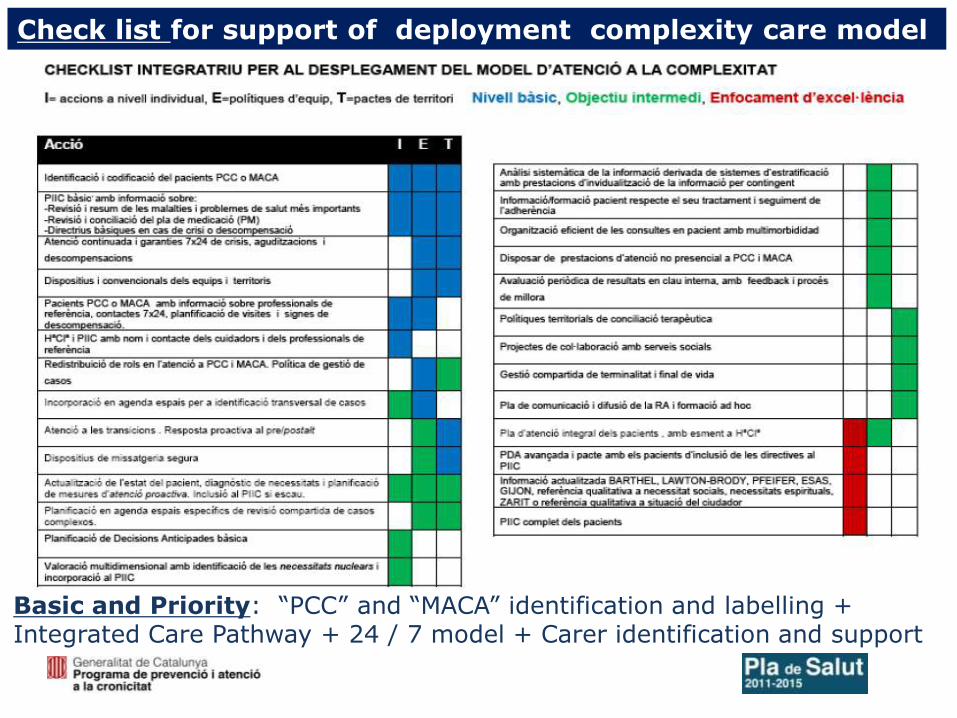
Check list for support of deployment complexity care model
Basic and Priority: “PCC” and “MACA” identification and labelling + Integrated Care Pathway + 24 / 7 model + Carer identification and support
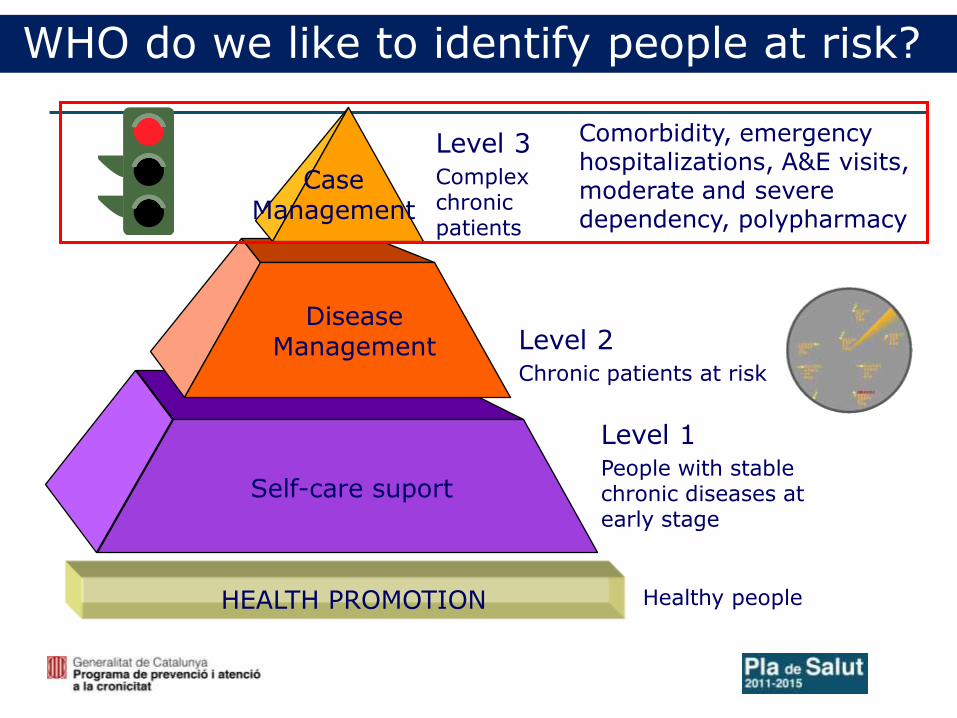
Level 2 Chronic patients at risk
Case Management
Disease Management
Self-care suport
Level 1 People with stable chronic diseases at early stage
Level 3 Complex chronic patients
Comorbidity, emergency hospitalizations, A&E visits, moderate and severe dependency, polypharmacy
HEALTH PROMOTION Healthy people
WHO do we like to identify people at risk?
24
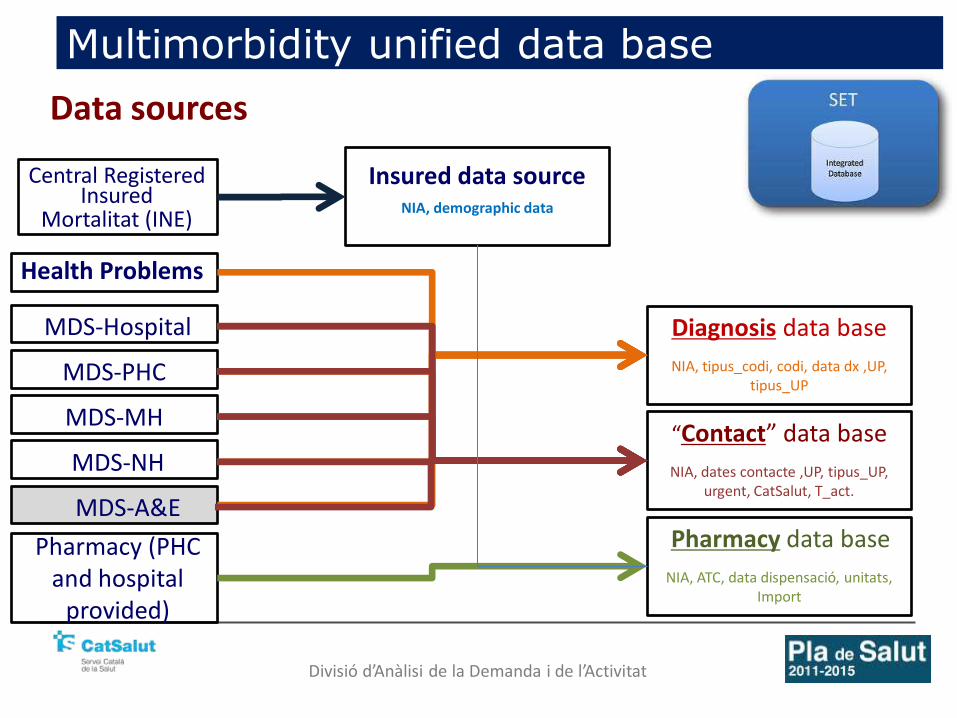
Multimorbidity unified data base
Insured data source NIA, demographic data
Diagnosis data base
NIA, tipus_codi, codi, data dx ,UP, tipus_UP
“Contact” data base
NIA, dates contacte ,UP, tipus_UP, urgent, CatSalut, T_act.
MDS-Hospital
MDS-PHC
MDS-MH
MDS-NH
MDS-A&E
Central Registered Insured
Health Problems
Pharmacy (PHC and hospital
provided)
Pharmacy data base
NIA, ATC, data dispensació, unitats, Import
Mortalitat (INE)
Data sources
Divisió d’Anàlisi de la Demanda i de l’Activitat
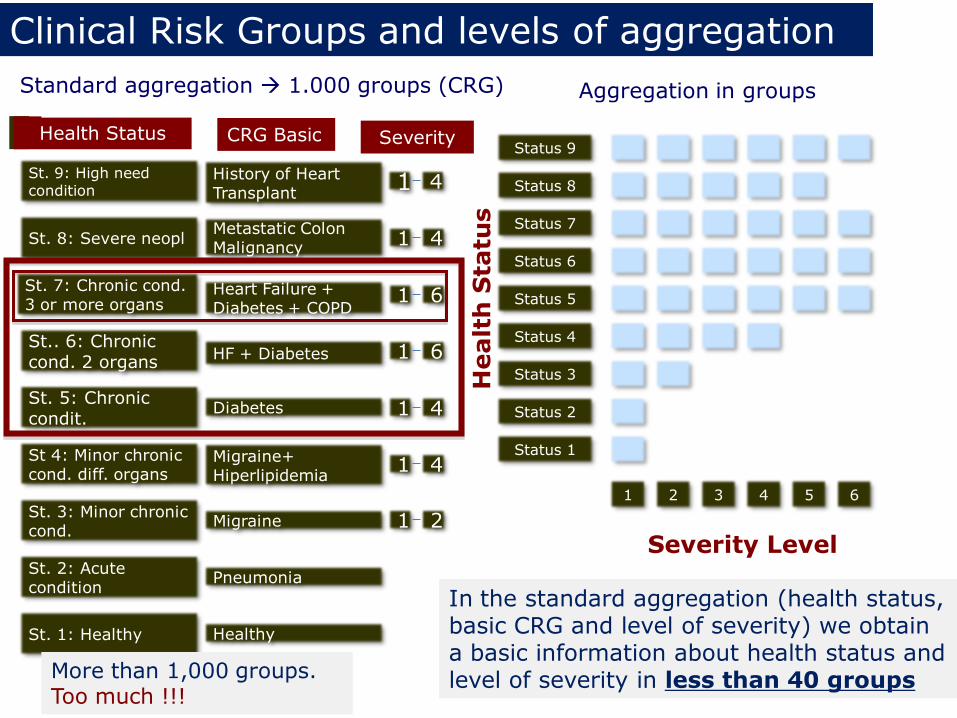
Clinical Risk Groups and levels of aggregation
Standard aggregation 1.000 groups (CRG) Aggregation in groups
St. 9: High need condition
St. 8: Severe neopl
St. 7: Chronic cond. 3 or more organs
St.. 6: Chronic cond. 2 organs
St. 5: Chronic condit.
St 4: Minor chronic cond. diff. organs
St. 3: Minor chronic cond.
St. 2: Acute condition
St. 1: Healthy
History of Heart Transplant
Metastatic Colon Malignancy
Heart Failure + Diabetes + COPD
HF + Diabetes
Diabetes
Migraine+ Hiperlipidemia
Migraine
Pneumonia
Healthy
1 4
1 4
1 6
1 6
1 4
1 4
1 2
Health Status CRG Basic Severity
In the standard aggregation (health status, basic CRG and level of severity) we obtain a basic information about health status and level of severity in less than 40 groups
Healt
h S
tatu
s
Severity Level
Status 9
Status 8
Status 7
Status 6
Status 5
Status 4
Status 3
Status 2
Status 1
1 2 3 4 5 6
More than 1,000 groups. Too much !!!
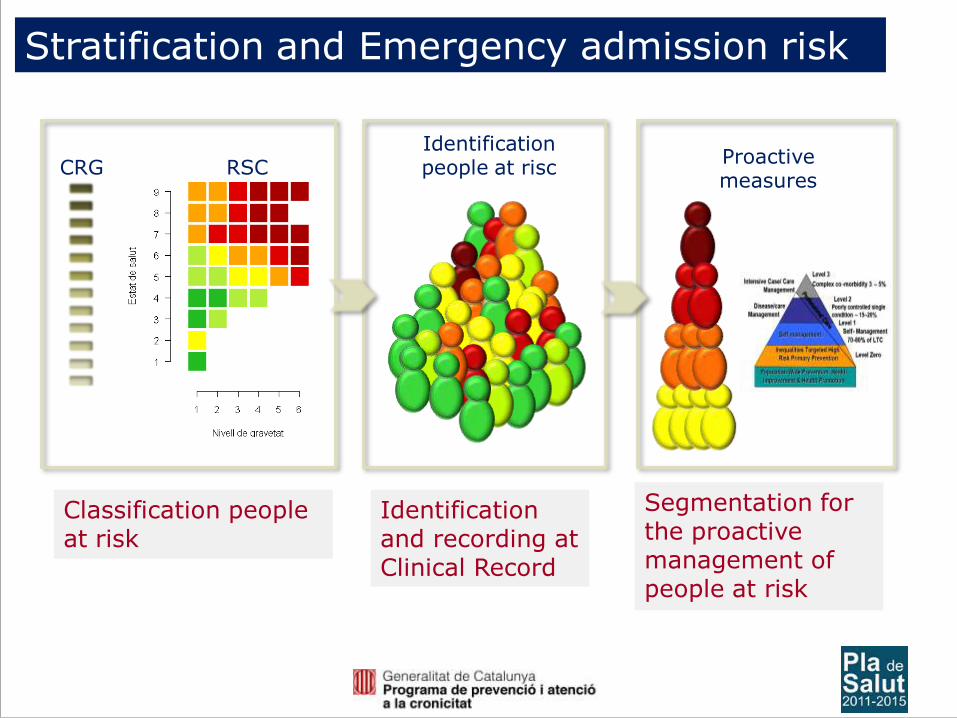
Stratification and Emergency admission risk
CRG RSC Identification people at risc
Proactive measures
Classification people at risk
Segmentation for the proactive management of people at risk
Identification and recording at Clinical Record
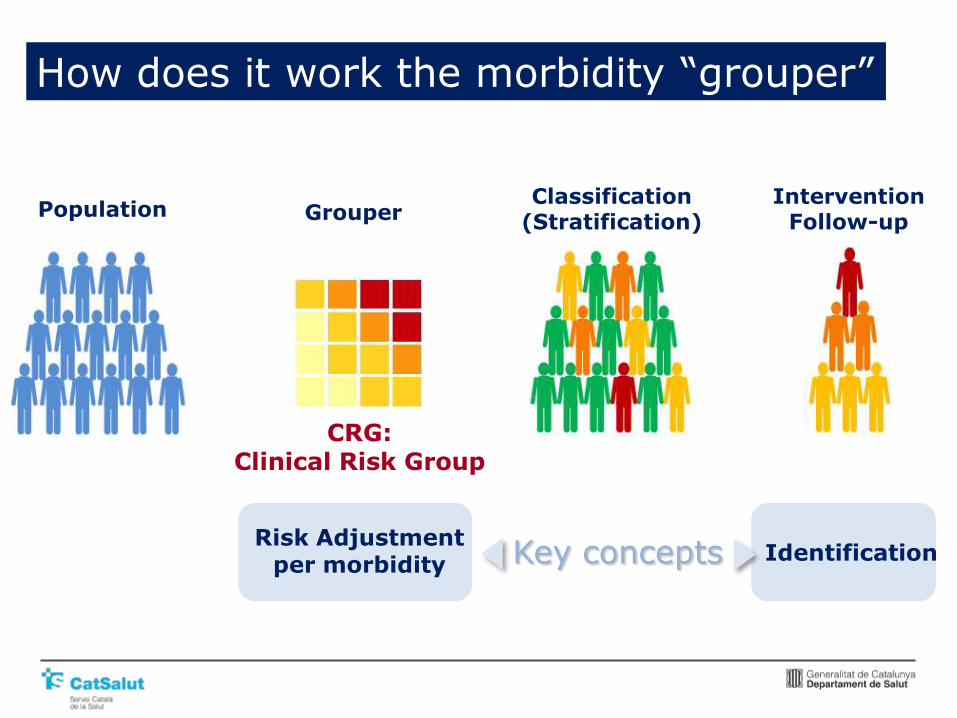
How does it work the morbidity “grouper”
Population Grouper Classification
(Stratification) Intervention
Follow-up
CRG: Clinical Risk Group
Risk Adjustment per morbidity
Identification Key concepts
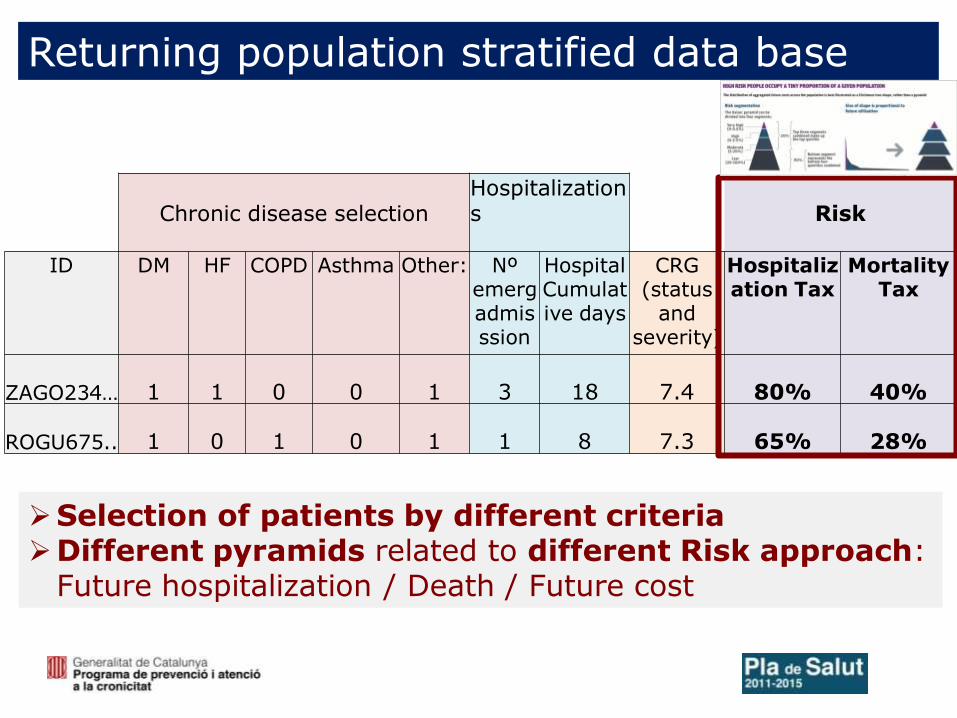
Returning population stratified data base
Chronic disease selection Hospitalizations
Risk
ID DM HF COPD Asthma Other: Nº emerg admisssion
Hospital Cumulative days
CRG (status
and severity)
Hospitalization Tax
Mortality Tax
ZAGO234… 1 1 0 0 1 3 18 7.4 80% 40%
ROGU675.. 1 0 1 0 1 1 8 7.3 65% 28%
Selection of patients by different criteria Different pyramids related to different Risk approach:
Future hospitalization / Death / Future cost
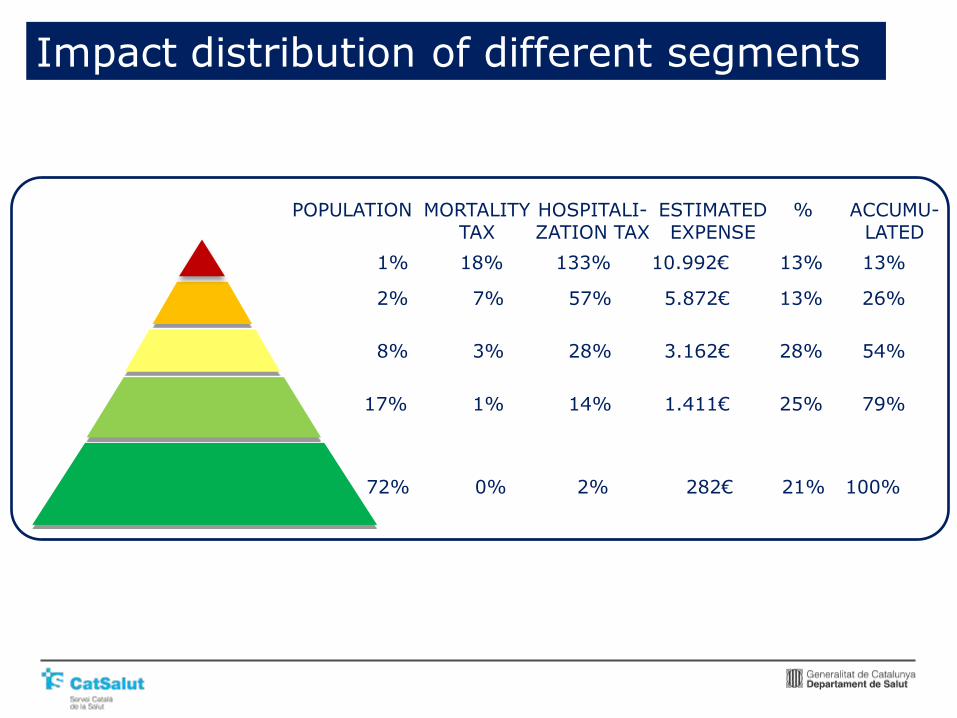
1% 18% 133% 10.992€ 13% 13%
2% 7% 57% 5.872€ 13% 26%
8% 3% 28% 3.162€ 28% 54%
17% 1% 14% 1.411€ 25% 79%
72% 0% 2% 282€ 21% 100%
POPULATION MORTALITY TAX
HOSPITALI-ZATION TAX
ESTIMATED EXPENSE
% ACCUMU-LATED
Impact distribution of different segments
Different utilization of Stratification
• To adjust models of “per capita” financing, assigning different budget related to morbidity burden in each PHC
• To identify populations and population segments with higher multimorbidity burden and more RISK of.........................: Emergency hospital admission High Cost High pharmacy consumption High mortality Higher Social Services Utilization • To assign “individual” RISK: not yet well calculated, we need more
variables to be included and should accept limitation of these tools • How to incorporate Stratification scores into Information Systems: Visualization and access to Shared Clinical Record and local clinical
record Return of data base to local providers • Validated model in American population or an own national/regional
model ?

Visualization in Shared Clinical Record and different RISK scores
Morbidity group and RISK calculated and published twice a year
Description of different RISK segments
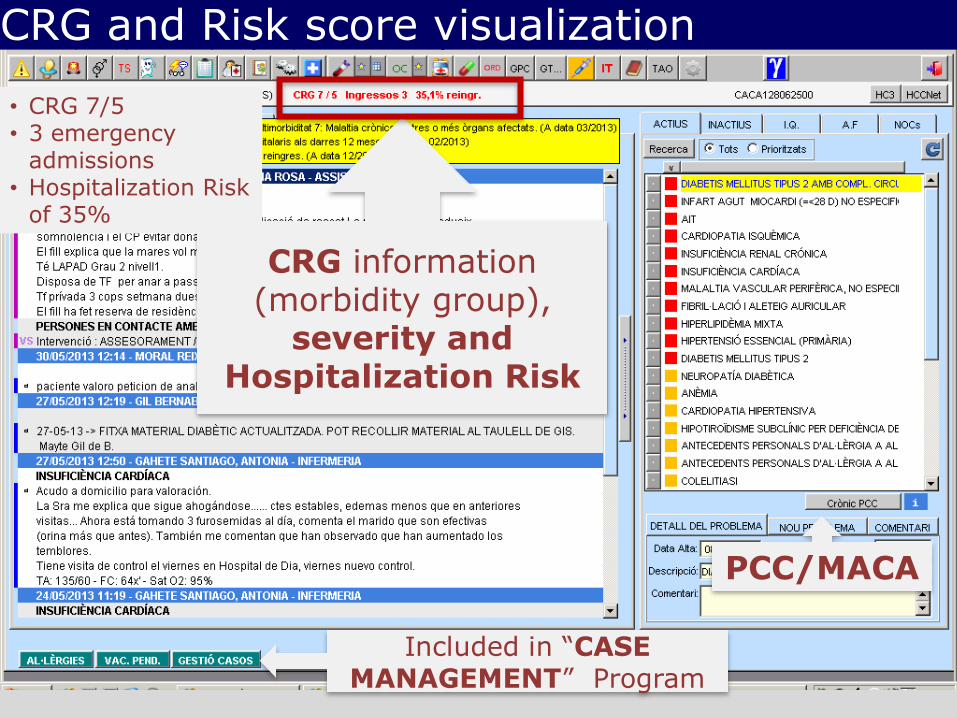
CRG information (morbidity group),
severity and Hospitalization Risk
• CRG 7/5 • 3 emergency
admissions • Hospitalization Risk
of 35%
PCC/MACA
Included in “CASE MANAGEMENT” Program
CRG and Risk score visualization
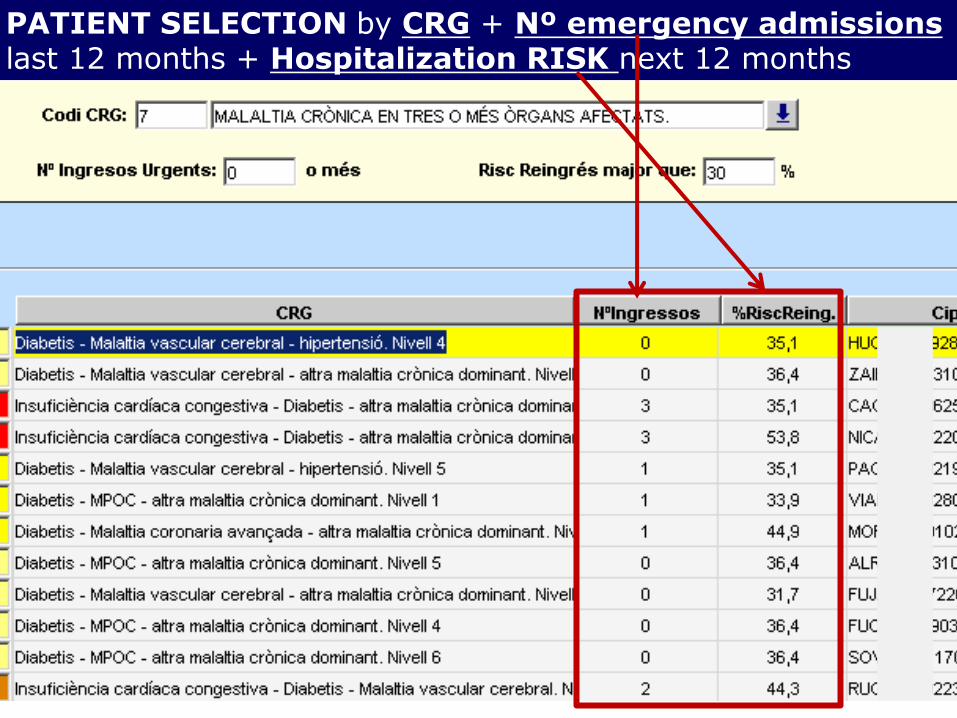
PATIENT SELECTION by CRG + Nº emergency admissions last 12 months + Hospitalization RISK next 12 months
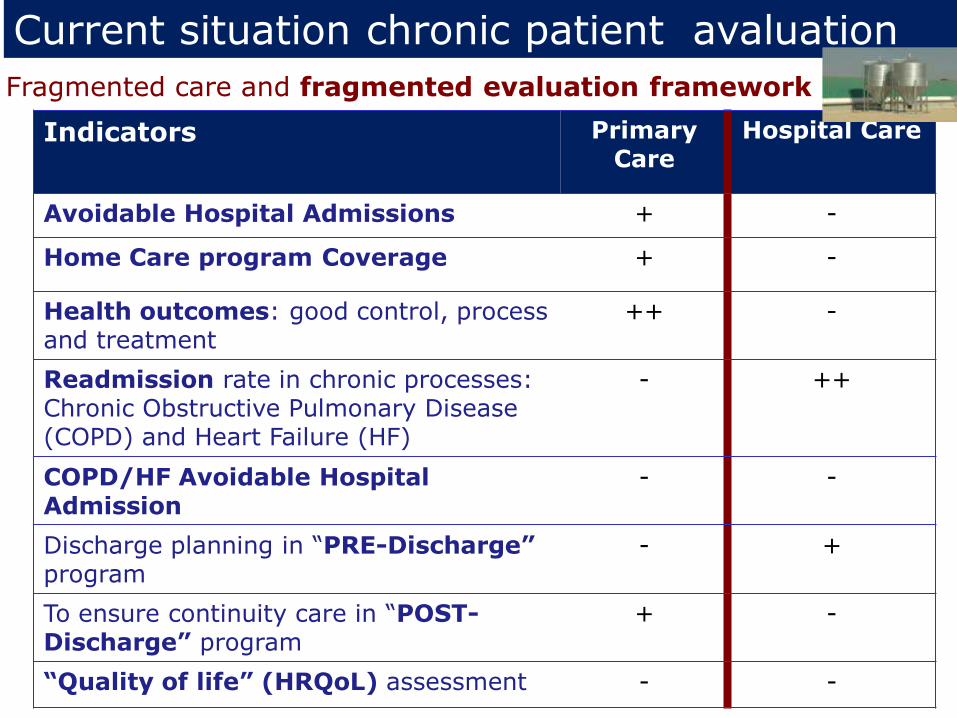
Current situation chronic patient avaluation
Indicators Primary Care
Hospital Care
Avoidable Hospital Admissions + -
Home Care program Coverage + -
Health outcomes: good control, process and treatment
++ -
Readmission rate in chronic processes: Chronic Obstructive Pulmonary Disease (COPD) and Heart Failure (HF)
- ++
COPD/HF Avoidable Hospital Admission
- -
Discharge planning in “PRE-Discharge” program
- +
To ensure continuity care in “POST-Discharge” program
+ -
“Quality of life” (HRQoL) assessment - -
Fragmented care and fragmented evaluation framework

New evaluation vision: “Triple Aim”
Population
Health
Experience
of Care
Per Capita
Cost
• Health Outcomes Indicators incorporates in evaluation Primary Health Care (PHC) (good control chronic diseases, vaccination..)
• Quality of life
• Satisfaction
• PROM
• Costs
• Service utilization: Avoidable Hospitalizations , Readmissions,…
Evaluation and commissioning of ”Integrated Care”
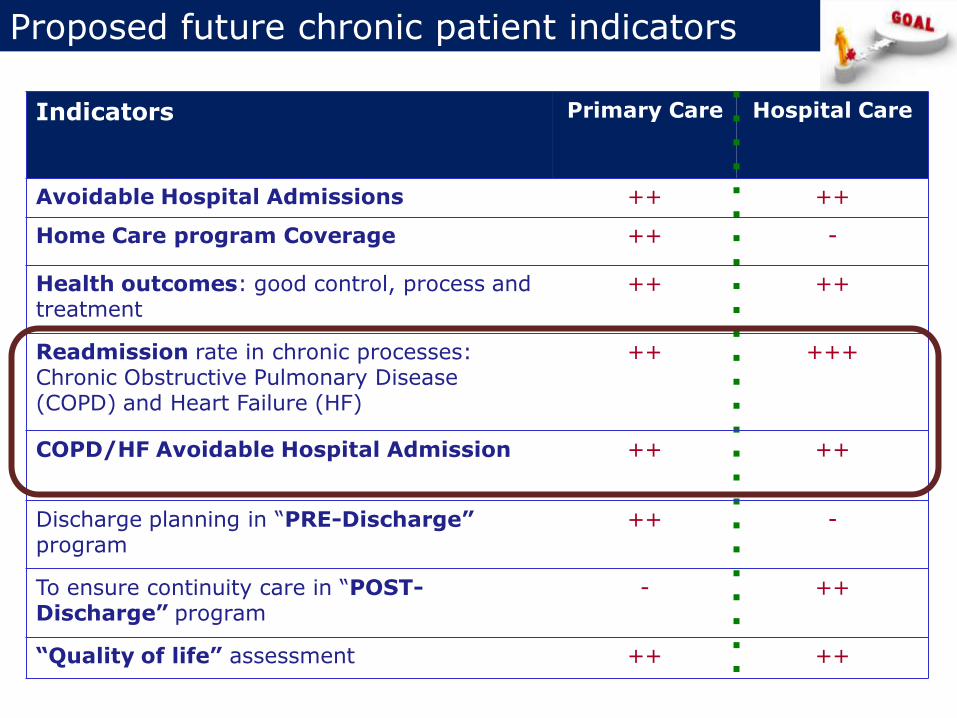
Proposed future chronic patient indicators
Indicators Primary Care Hospital Care
Avoidable Hospital Admissions ++ ++
Home Care program Coverage ++ -
Health outcomes: good control, process and treatment
++ ++
Readmission rate in chronic processes: Chronic Obstructive Pulmonary Disease (COPD) and Heart Failure (HF)
++ +++
COPD/HF Avoidable Hospital Admission ++ ++
Discharge planning in “PRE-Discharge” program
++ -
To ensure continuity care in “POST-Discharge” program
- ++
“Quality of life” assessment ++ ++
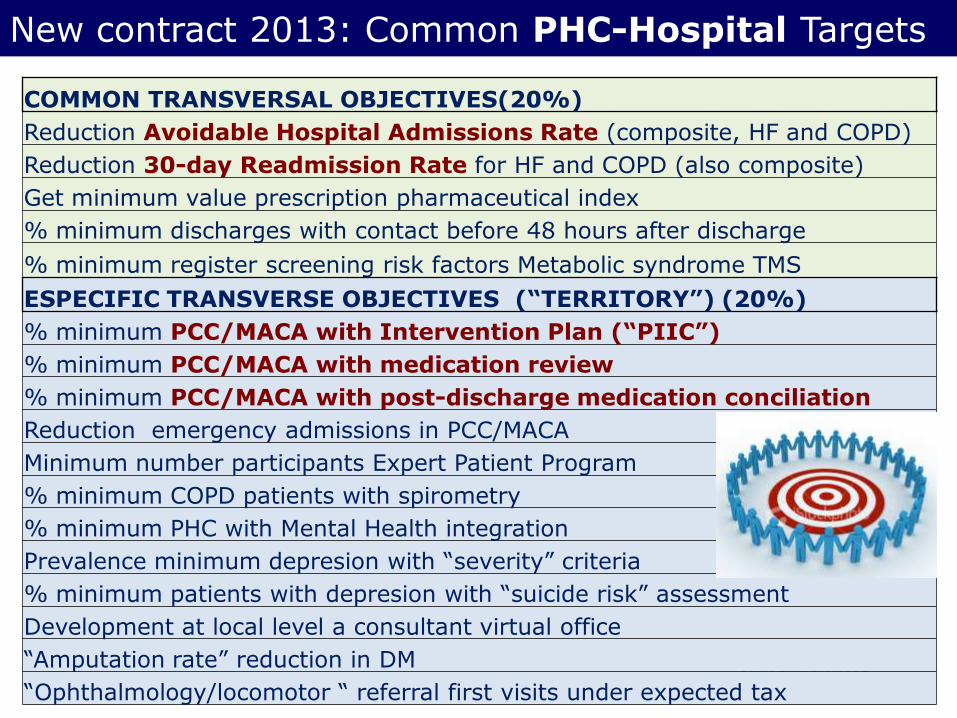
New contract 2013: Common PHC-Hospital Targets
37
COMMON TRANSVERSAL OBJECTIVES(20%)
Reduction Avoidable Hospital Admissions Rate (composite, HF and COPD)
Reduction 30-day Readmission Rate for HF and COPD (also composite)
Get minimum value prescription pharmaceutical index
% minimum discharges with contact before 48 hours after discharge
% minimum register screening risk factors Metabolic syndrome TMS
ESPECIFIC TRANSVERSE OBJECTIVES (“TERRITORY”) (20%)
% minimum PCC/MACA with Intervention Plan (“PIIC”)
% minimum PCC/MACA with medication review
% minimum PCC/MACA with post-discharge medication conciliation
Reduction emergency admissions in PCC/MACA
Minimum number participants Expert Patient Program
% minimum COPD patients with spirometry
% minimum PHC with Mental Health integration
Prevalence minimum depresion with “severity” criteria
% minimum patients with depresion with “suicide risk” assessment
Development at local level a consultant virtual office
“Amputation rate” reduction in DM
“Ophthalmology/locomotor “ referral first visits under expected tax
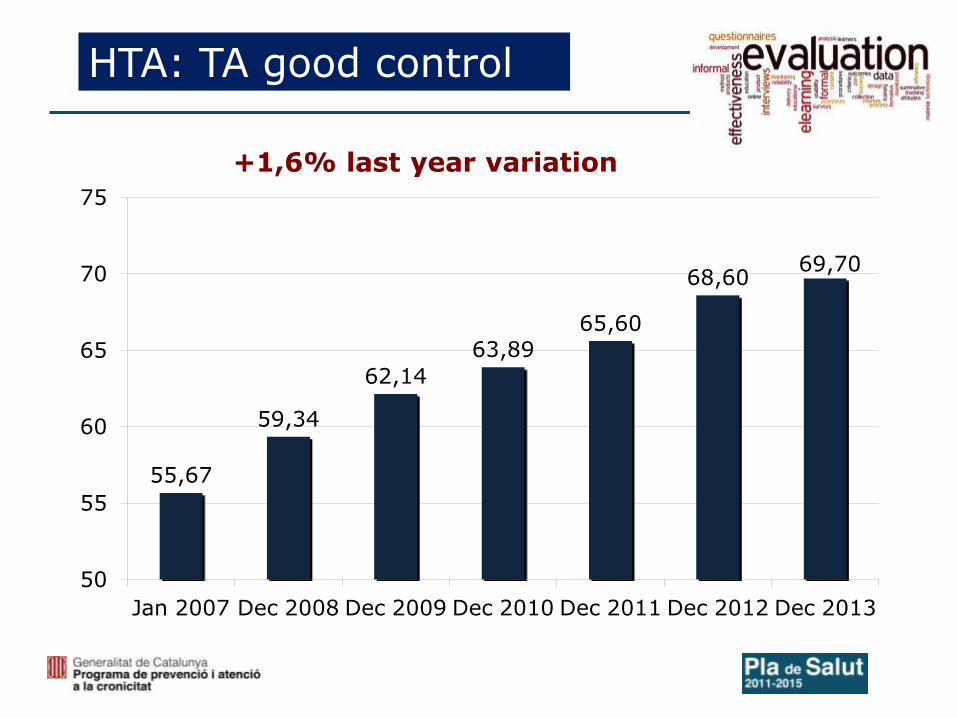
HTA: TA good control
+1,6% last year variation
55,67
59,34
62,14
63,89
65,60
68,60 69,70
50
55
60
65
70
75
Jan 2007 Dec 2008 Dec 2009 Dec 2010 Dec 2011 Dec 2012 Dec 2013
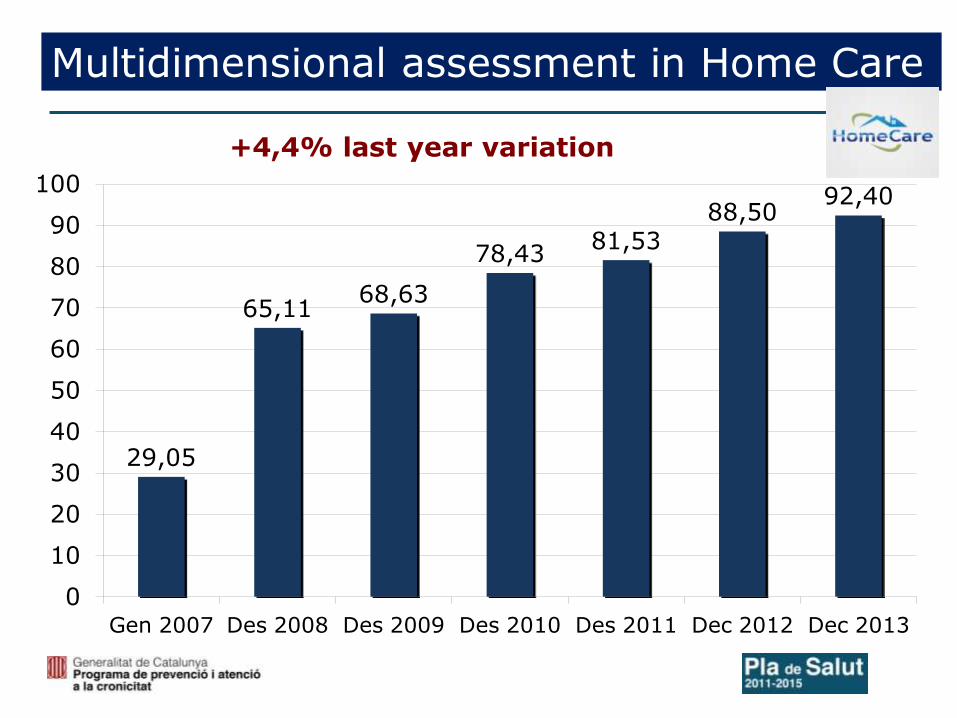
Multidimensional assessment in Home Care
+4,4% last year variation
29,05
65,11 68,63
78,43 81,53
88,50 92,40
0
10
20
30
40
50
60
70
80
90
100
Gen 2007 Des 2008 Des 2009 Des 2010 Des 2011 Dec 2012 Dec 2013
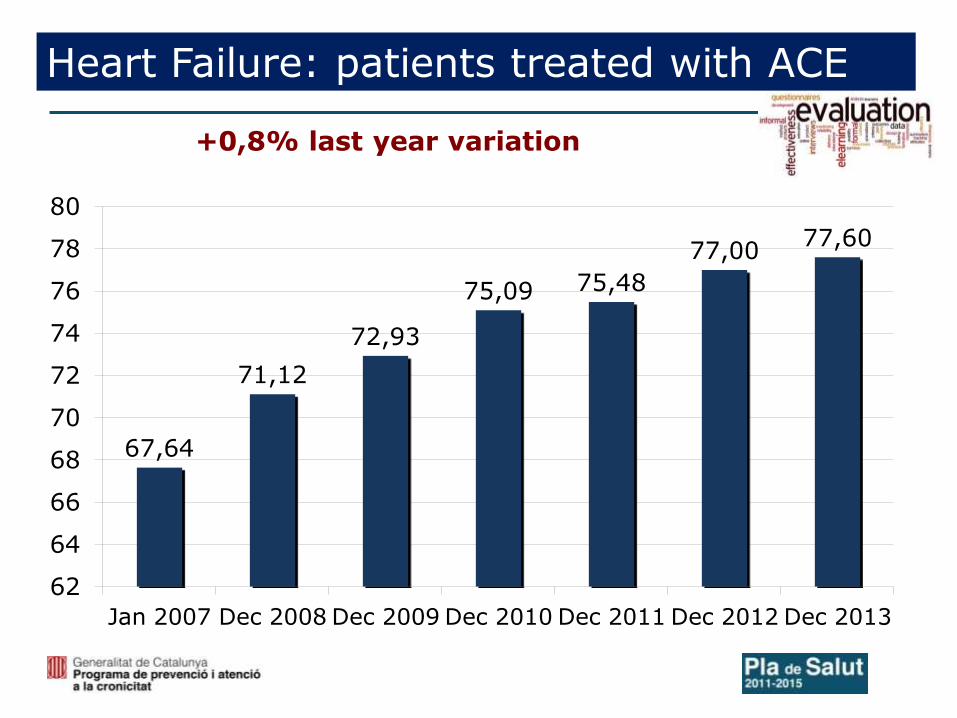
Heart Failure: patients treated with ACE
+0,8% last year variation
67,64
71,12
72,93
75,09 75,48
77,00 77,60
62
64
66
68
70
72
74
76
78
80
Jan 2007 Dec 2008 Dec 2009 Dec 2010 Dec 2011 Dec 2012 Dec 2013
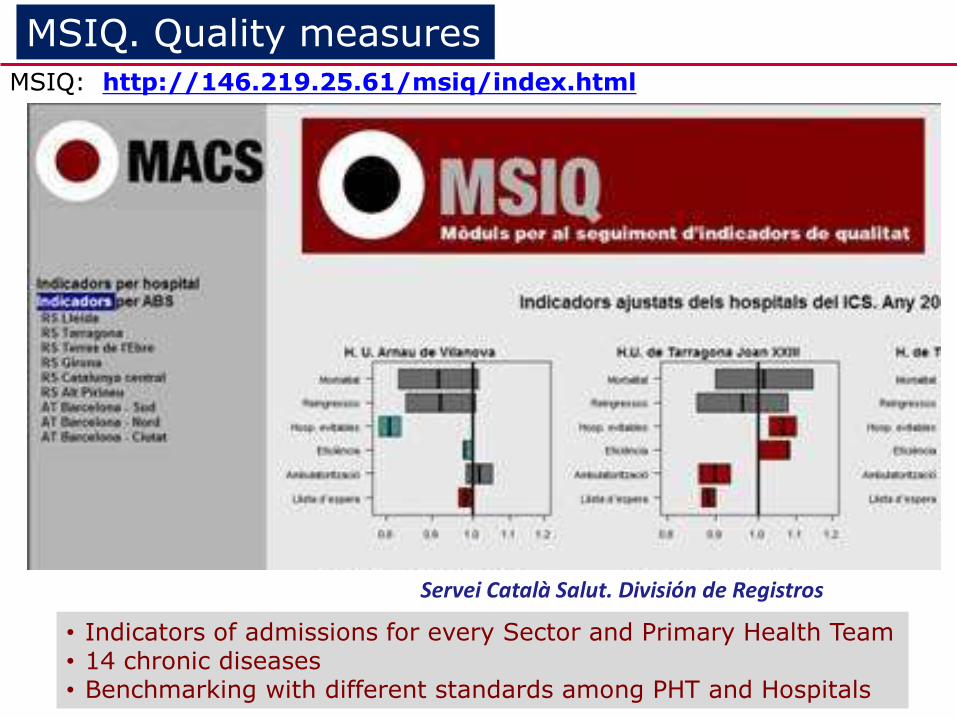
• Indicators of admissions for every Sector and Primary Health Team • 14 chronic diseases • Benchmarking with different standards among PHT and Hospitals
Servei Català Salut. División de Registros
MSIQ. Quality measures MSIQ: http://146.219.25.61/msiq/index.html
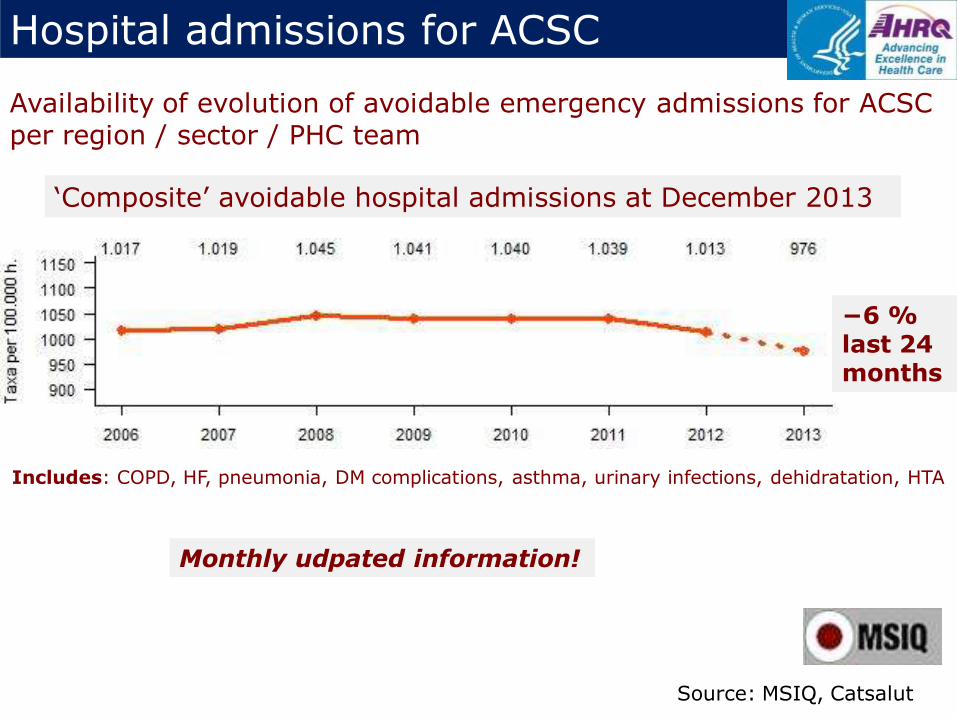
Hospital admissions for ACSC
‘Composite’ avoidable hospital admissions at December 2013
Monthly udpated information!
Includes: COPD, HF, pneumonia, DM complications, asthma, urinary infections, dehidratation, HTA
Availability of evolution of avoidable emergency admissions for ACSC per region / sector / PHC team
Source: MSIQ, Catsalut
−6 % last 24 months
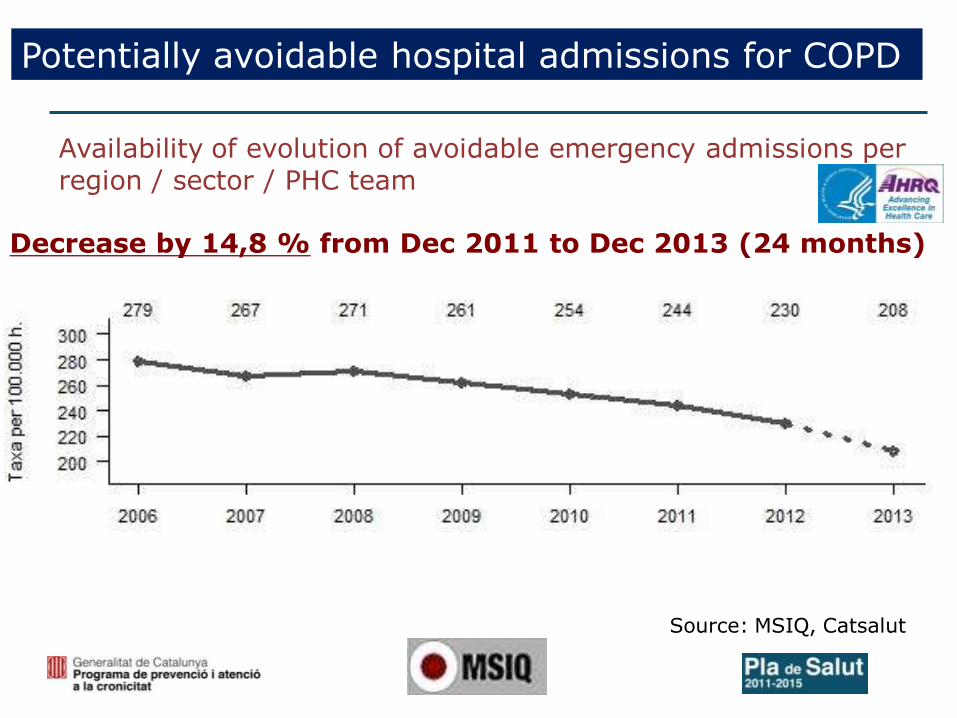
Potentially avoidable hospital admissions for COPD
Decrease by 14,8 % from Dec 2011 to Dec 2013 (24 months)
Availability of evolution of avoidable emergency admissions per region / sector / PHC team
Source: MSIQ, Catsalut
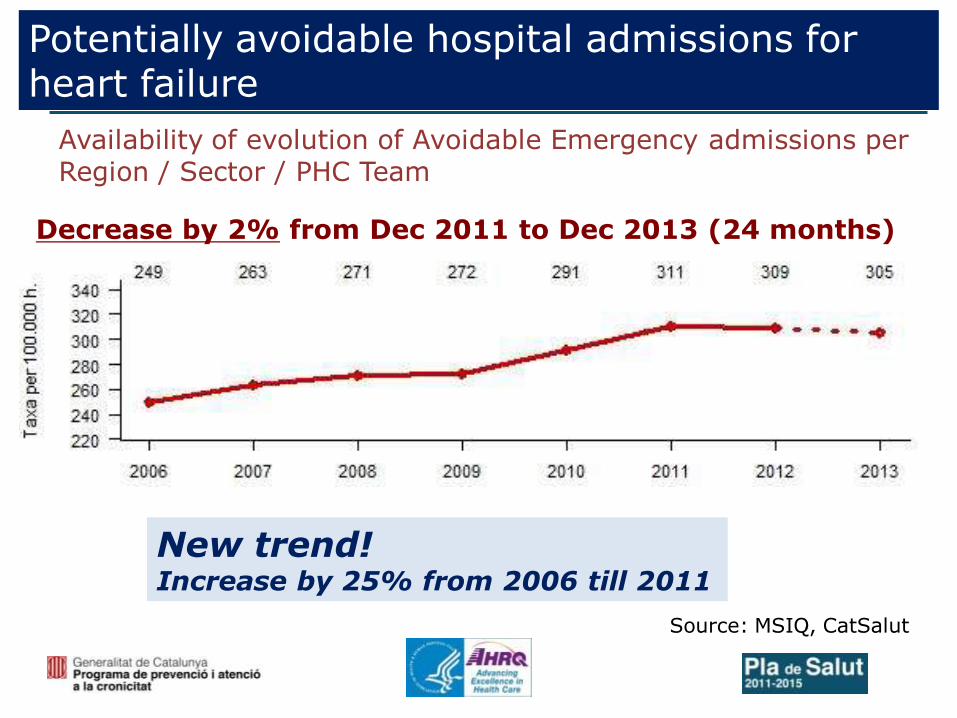
Potentially avoidable hospital admissions for heart failure
Source: MSIQ, CatSalut
Decrease by 2% from Dec 2011 to Dec 2013 (24 months)
Availability of evolution of Avoidable Emergency admissions per Region / Sector / PHC Team
New trend! Increase by 25% from 2006 till 2011
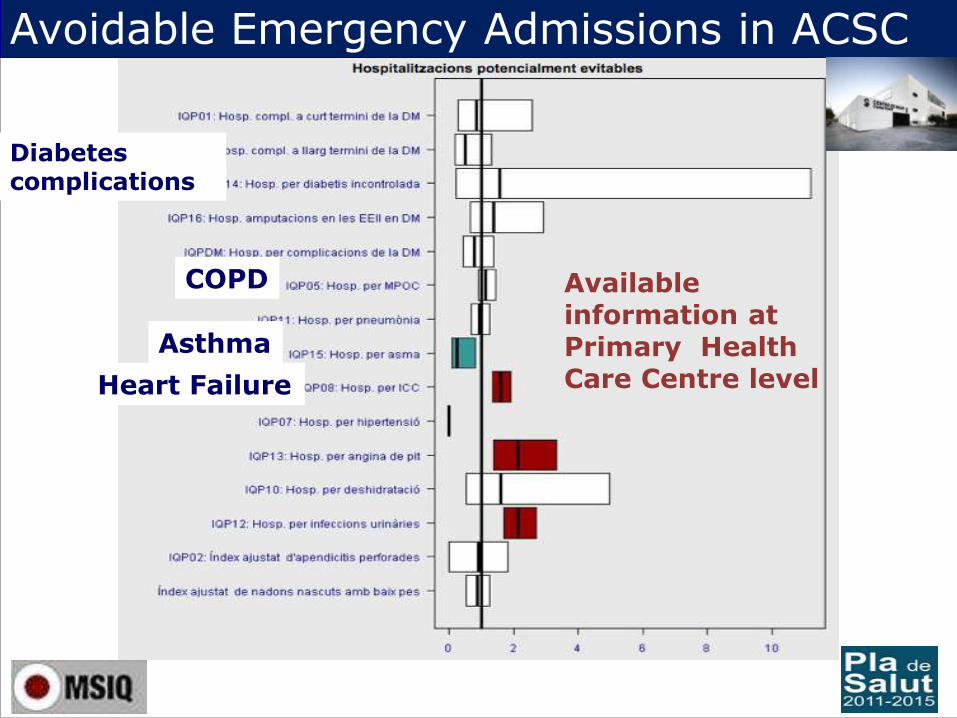
Heart Failure
COPD
Avoidable Emergency Admissions in ACSC
Available information at Primary Health Care Centre level
Diabetes complications
Asthma
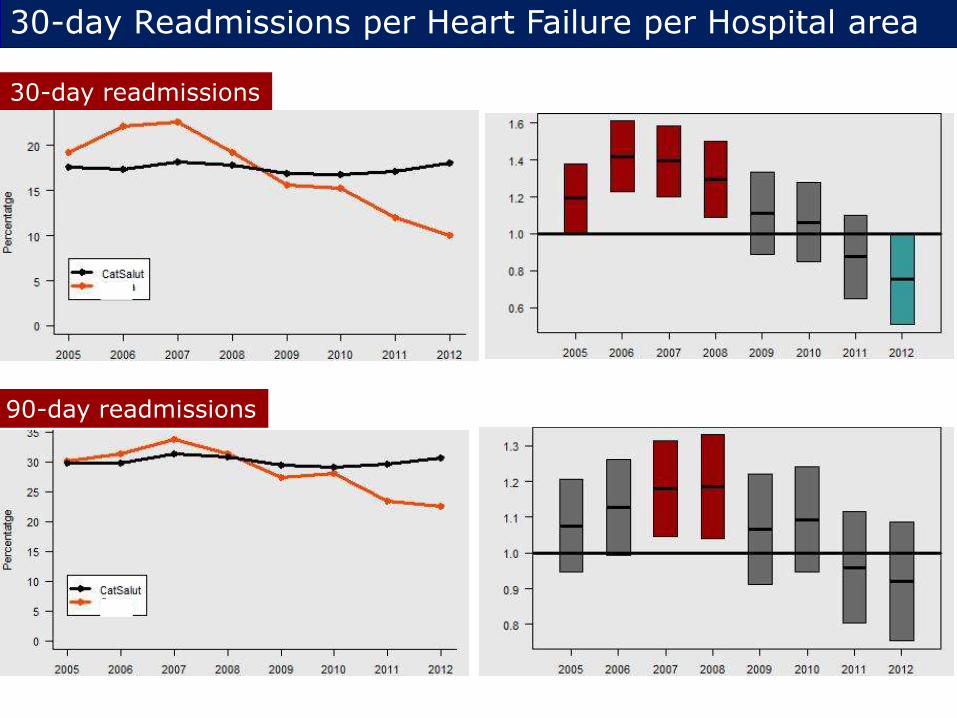
30-day readmissions
90-day readmissions
30-day Readmissions per Heart Failure per Hospital area

Expected per capita expenditure
The 1% of top consumers spend 1.701,5M €, the 23% of total cost with an average of 21.540€ per cápita cost The 5% of top consumers, spend 3.783,6M €, 51% of total cost with an average of 9.580€ per cápita cost
Average expenditure (€)
Percentiles related to expenditure

Expected per capita expenditure
Average expenditure (€)
Primary Care Pharmacy Emerg.adm. A&E Outpatient Clinics
AGE
Primary Care
Pharmacy
Emergency admissions
Outpatients clinics

Expected per capita expenditure Average expenditure (€)
Primary Care Pharm. Emerg.adm. A&E Outpatient Clinics
COPD Diabet. Dement Card. CVA Ment. Cirros. Kidney H. Fail. Neopl. VIH
Primary Care
Pharmacy
Emergency admissions
Outpatients clinics
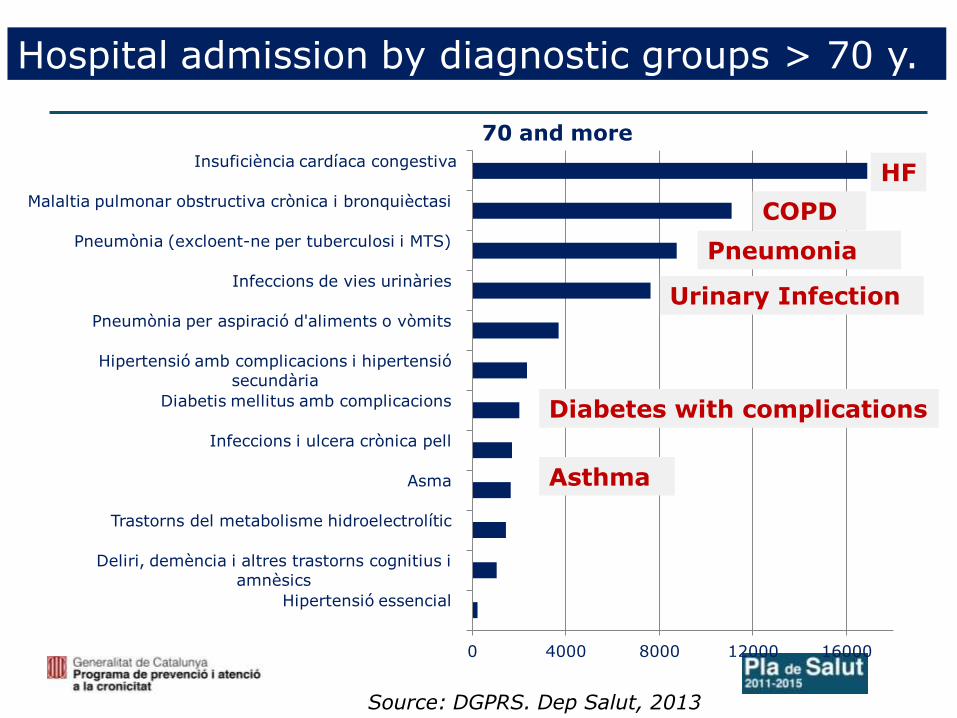
Hospital admission by diagnostic groups > 70 y.
0 4000 8000 12000 16000
Hipertensió essencial
Deliri, demència i altres trastorns cognitius i
amnèsics
Trastorns del metabolisme hidroelectrolític
Asma
Infeccions i ulcera crònica pell
Diabetis mellitus amb complicacions
Hipertensió amb complicacions i hipertensió
secundària
Pneumònia per aspiració d'aliments o vòmits
Infeccions de vies urinàries
Pneumònia (excloent-ne per tuberculosi i MTS)
Malaltia pulmonar obstructiva crònica i bronquièctasi
Insuficiència cardíaca congestiva
70 and more
Pneumonia
Source: DGPRS. Dep Salut, 2013
COPD
HF
Urinary Infection
Asthma
Diabetes with complications
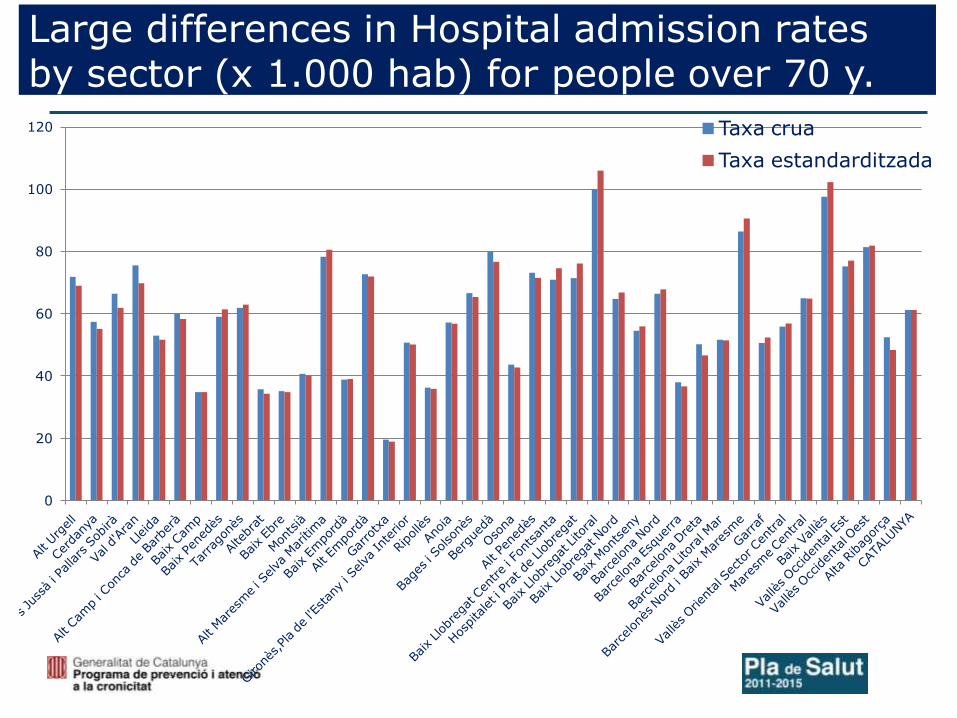
Large differences in Hospital admission rates by sector (x 1.000 hab) for people over 70 y.
0
20
40
60
80
100
120 Taxa crua
Taxa estandarditzada
2.5. Complex Chronic Patients deployment
▪ To define a stratification model that allows segmentation of the population with chronic diseases with different risk levels. Creating a predictive model that incorporates risk situation at Shared Clinical record.
▪ To design Complex Chronic Patient Care Model (PCC).
▪ To design care model for people with advanced chronic disease.
▪ To define collaborative model between health services and social services: design care a collaborative model, access to “Shared her” by social services and incorporation to it information of common interest, identifying common targets in contracts Department of Health and Department of Social Welfare.
PROGRAMA PREVENCIÓ I ATENCIÓ A LA CRONICITAT
Integrated Health and Social Care is high priority and policy in England
https://www.gov.uk/government/policies/making-sure-health-and-social-care-services-work-together
Direcció d’Atenció Primària Costa de Ponent
Integrated Care in Torbay
PROGRAMA PREVENCIÓ I ATENCIÓ A LA CRONICITAT

Integrated Care Model and Social Services
Mrs Smith in Torbay

Basis for a Social and Health Integrated Care
Plan for Catalonia:
PAISS

25th February 2014: New Government Agreement where is launched a new Integrated Health and Social Care Plan in Catalonia
Accountable and reporting to Department of Presidency
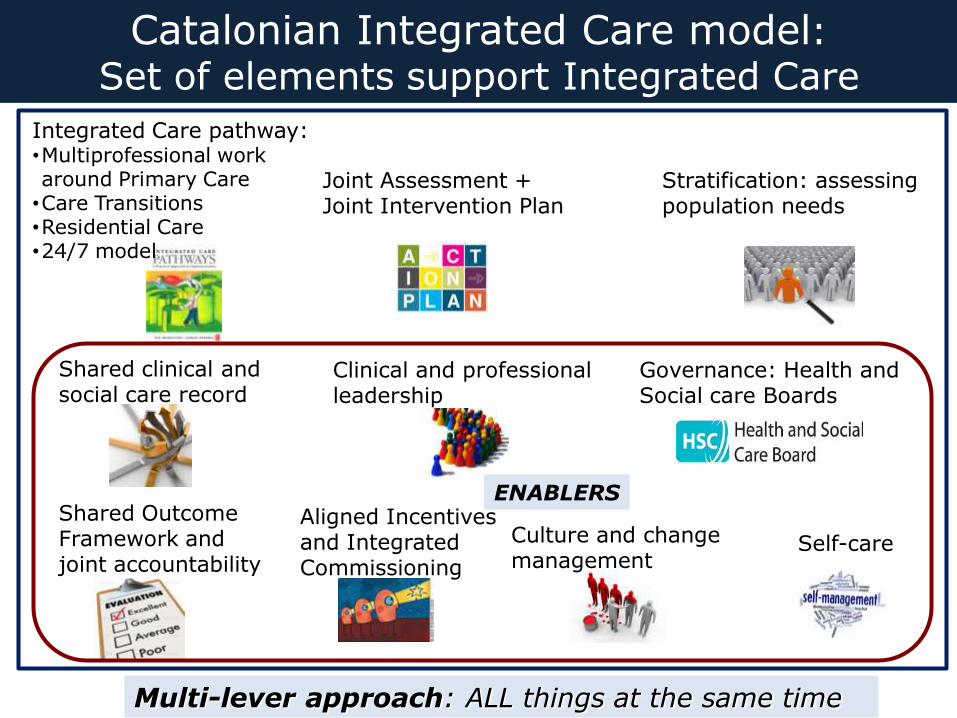
Catalonian Integrated Care model: Set of elements support Integrated Care
Multi-lever approach: ALL things at the same time
Integrated Care pathway: •Multiprofessional work around Primary Care
•Care Transitions •Residential Care •24/7 model
Joint Assessment + Joint Intervention Plan
Stratification: assessing population needs
Clinical and professional leadership
Governance: Health and Social care Boards
Shared Outcome Framework and joint accountability
Aligned Incentives and Integrated Commissioning
Shared clinical and social care record
Culture and change management
Self-care
ENABLERS
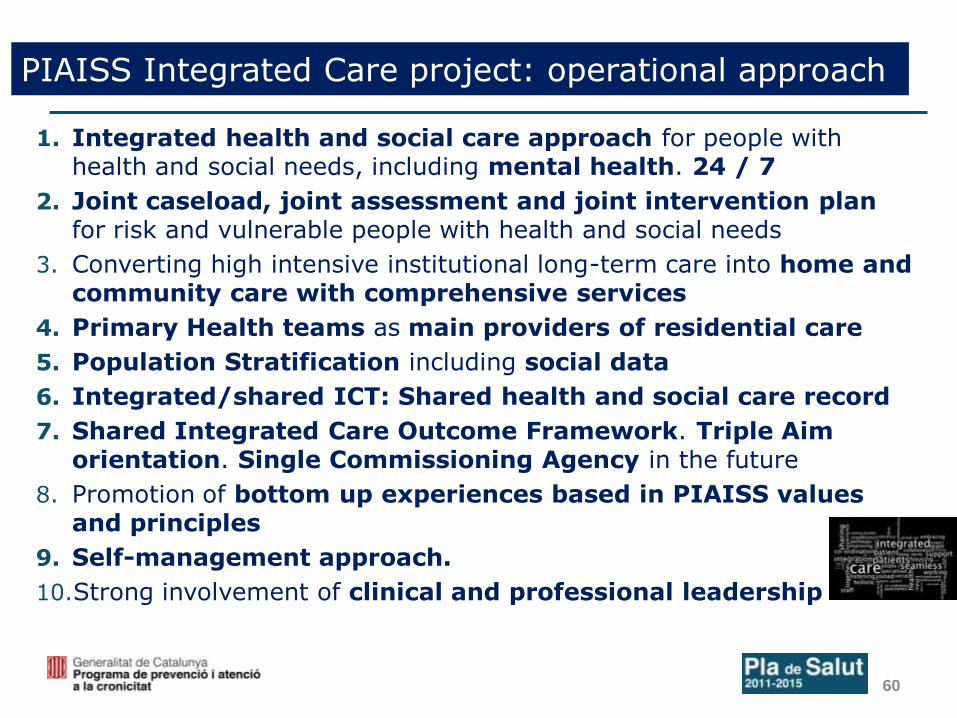
PIAISS Integrated Care project: operational approach
1. Integrated health and social care approach for people with health and social needs, including mental health. 24 / 7
2. Joint caseload, joint assessment and joint intervention plan for risk and vulnerable people with health and social needs
3. Converting high intensive institutional long-term care into home and community care with comprehensive services
4. Primary Health teams as main providers of residential care
5. Population Stratification including social data
6. Integrated/shared ICT: Shared health and social care record
7. Shared Integrated Care Outcome Framework. Triple Aim orientation. Single Commissioning Agency in the future
8. Promotion of bottom up experiences based in PIAISS values and principles
9. Self-management approach.
10.Strong involvement of clinical and professional leadership
60
How to conduct a collaborative model?
Local Operational Plan
Situation analysis (through SWOT analysis or any other methodology for analysing): starting point, barriers, facilitators, opportunities and threats. External and internal analysis.
Planning: defining an action plan, operational objectives, action lines and operationalized and calendarized actions.
Communication and implementation: risk analysis tools as well as control and monitoring tools will be used, transversal implementation considerations such as quality, communication, training will be taken into account.
Assessment: the project’s assessment and monitoring model, as well as participating agents’ responsibilities, assessment commissions and reports to be created should be defined.
61
How to conduct a collaborative model?
1. Environmental and internal analysis at local level
Minimum internal and external situation analysis / Identify critical elements enabling the building of proposals to be collected in ‘Local Operational and Functional Plan’ (LFP) / Highly operational guidance and implementability with short terms results.
2. Integrated operational care model
Operational approach promoting common space and time.
3. Define and use a “territorial governance board”
Strategic governing body / steering group / implementing group
4. Define a common porfolio for people/users
Complex Chronic care and dependence / Home nursing and home help service (SAD) / Hospital discharge planning / Institutionalized people / Mental health / Childhood at-risk / Abuse / Active aging, health promotion and disease prevention / Other
62
How to conduct a collaborative model?
5. Shared information systems: constructing a new eClinical and Social care record
• Identify the person with the CIP (Identification Number) as a common identifier.
• Prior agreement on the coding and register of social problems.
• Prepare the local social services information system for it to be ‘interoperable’ in a short-medium term and provide a minimum set of information and variables for a Shared Social and Clinical Record model.
• Access to a minimum set of information and variables of common interest on social field for the Shared Clinical Record of Catalonia (HCCC). Later stage: HCSC fed with input from both health and social parties.
1st stage: generation of a Social Intervention Plan incorporated to HCSC. 2nd stage: Shared Individual Intervention Plan.
• Communication systems to improve accessibility, messaging and virtual work between social and health areas.
• Introduce social variables gradually to available health stratification.
63
How to conduct a collaborative model?
6. Selection of people based on cross-database and lists of people from social and health areas and stratification (!!!)
7. Definition of guaranteed protected pathways in transitions (discharge planning + post discharge support) among services and in crisis situation and proactive planning.
8. Dependence assessment and recognition procedure optimized with a guaranteed maximum response time.
9. Incorporation and definition of roles and responsibilities of different professional profiles (esp. Social workers working in PHC
10. Accountable professional reference for complex cases.
64

How to conduct a collaborative model?
11. Common and transverse Shared/Single Outcome Framework with incentive alignment. Progressive process.
Triple aim vision: health results and good care, service utilization and good perception of care.
12. Definition and implementation of an integrated home care model.
13. Joint action plan for promoting autonomy, active aging, health and well being and disease prevention incorporating the role and collaboration of telecare services.
13. Accessibility solutions and joint technical assistance from a territorial perspective.
14. Incorporation of the third sector.
65

North Ireland is developing and Integrated health and social care record !!!
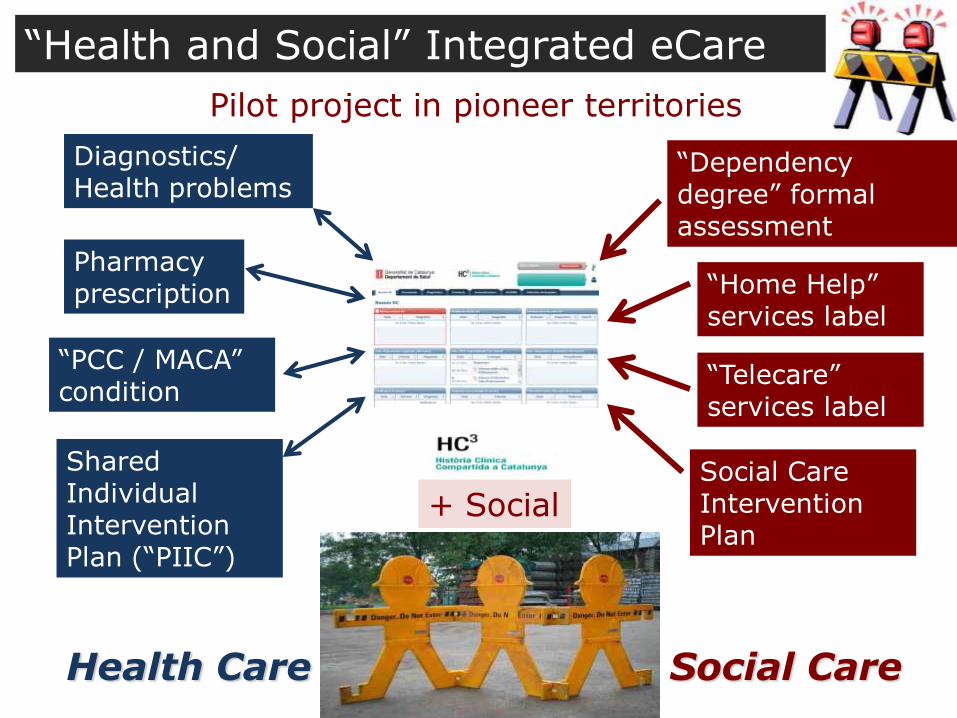
“PCC / MACA” condition
Shared Individual Intervention Plan (“PIIC”)
Diagnostics/ Health problems
“Dependency degree” formal assessment
“Home Help” services label
“Telecare” services label
Social Care Intervention Plan
Pharmacy prescription
Health Care Social Care
+ Social
“Health and Social” Integrated eCare
Pilot project in pioneer territories
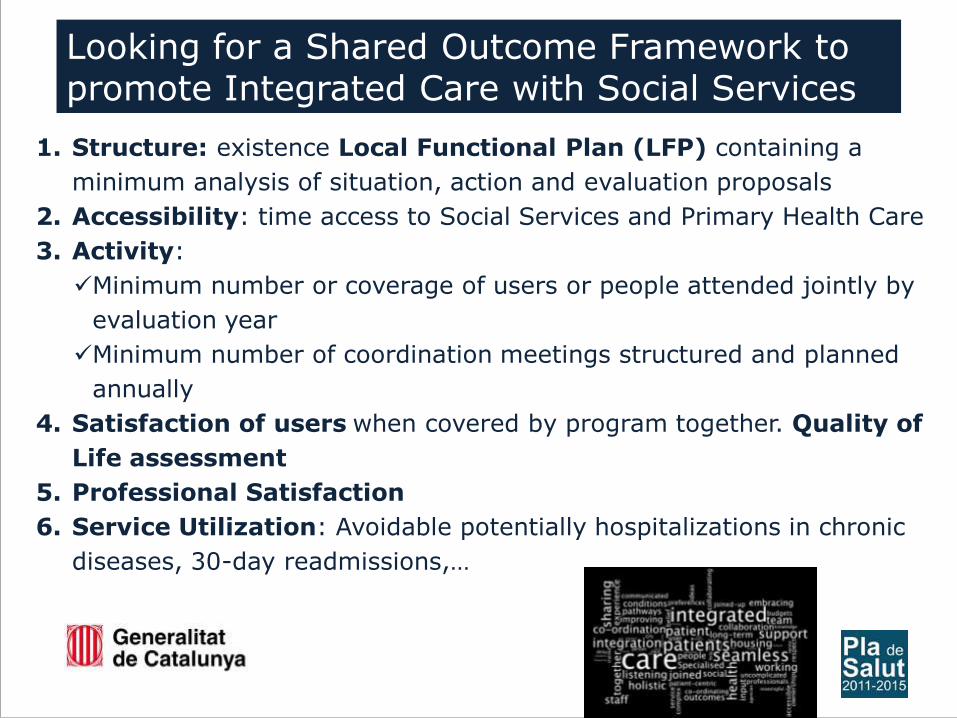
1. Structure: existence Local Functional Plan (LFP) containing a
minimum analysis of situation, action and evaluation proposals
2. Accessibility: time access to Social Services and Primary Health Care
3. Activity:
Minimum number or coverage of users or people attended jointly by
evaluation year
Minimum number of coordination meetings structured and planned
annually
4. Satisfaction of users when covered by program together. Quality of
Life assessment
5. Professional Satisfaction
6. Service Utilization: Avoidable potentially hospitalizations in chronic
diseases, 30-day readmissions,…
Looking for a Shared Outcome Framework to promote Integrated Care with Social Services

®
212 PHT
2 HOSPITAL
316 GROUPS
3191 PARTICIPANTS
233 EXPERT PATIENTS
649 PROFESSIONAL
OBSERVERS
ACTIONS 2006-2013 Source: Programa Paciente Experto Catalunya® 2013

www.gencat.cat/salut/pladesalut
70