kdigo gn guideline update – evidence summary …...1 kdigo gn guideline update – evidence...
TRANSCRIPT

1
KDIGO GN Guideline update – Evidence summary
Idiopathic focal segmental glomerulosclerosis (FSGS) in adults
Immunosuppressive therapy FSGS PICO question In patients with biopsy-proven FSGS in adults what immunosuppressive agents compared to no treatment/placebo or other immunosuppressive therapy improves efficacy outcomes (all-cause mortality, end-stage kidney disease, ≥50% loss of GFR, annual loss of GFR, complete remission) and reduces adverse effects (infection, and malignancy)? Search strategy and selection Keywords for idiopathic focal segmental glomerulosclerosis (FSGS), and immunosuppressive therapy were used to search the Cochrane Kidney and Transplant Specialized Registry of studies for all randomised controlled trials (RCTs) published up to May 2018. Studies contained in the register are identified through search strategies for CENTRAL, MEDLINE, and EMBASE. Search results The 2018 Cochrane review search update identified 45 relevant reports from the Cochrane Kidney and Transplant Specialized Registry of studies. Twelve of these reports were excluded because they were not RCTs, were the wrong population or because were the wrong intervention. There were four primary studies (33 reports) and three reports of a previously included study identified. Combined with the 2008 Cochrane review, there was 11 studies (51 reports) included with 360 participants. Eleven comparisons were identified:
1. Cyclosporin versus mycophenolate mofetil plus dexamethasone (1 study, 138 participants) 2. Cyclosporin plus low dose prednisone versus prednisone alone (1 study, 49 participants) 3. Cyclosporin plus prednisolone versus methylprednisolone (1 study, 23 participants) 4. Cyclosporin plus prednisone versus chlorambucil plus prednisone ( 1 study, 57 participants) 5. Prednisolone plus chlorambucil versus no treatment (1 study, 15 participants) 6. Cyclosporin versus supportive therapy (1 study, 19 participants) 7. Mycophenolate mofetil versus prednisone (1 study, 33 participants) 8. Dexamethasone 2 weekly versus dexamethasone 4 weekly (1 study, 8 participants) 9. Fresolimumab versus placebo (1 study, 36 participants) 10. Adalimumab versus rosiglitazone (1 study, 21 participants)* 11. Adalimumab versus galactose or conservative therapy (1 study, 21 participants)
* Data from the FONT I 2009 study could not be meta-analysed as different outcomes were reported for the different treatment arms.
FONT I 2009 Study - Joy MS, et al. Phase I trial of rosiglitazone in FSGS: I. Report of the FONT Study Group. Clinical Journal of the American Society of Nephrology: CJASN 2009;4(1):39-47.

2
Summary of the main findings Immunosuppressive therapy versus no treatment
• We are uncertain whether prednisolone plus chlorambucil compared with no treatment ( 1 study, 15 participants) increases or decreases complete remission or doubling of serum creatinine due to study limitations and very serious imprecision in the effect estimate. Other critical and important outcomes were not reported in the RCT.
• Cyclosporin compared to no treatment may have little or no effect on doubling of serum creatinine (RR 0.60, 95%CI 0.25 to 1.46), based on data from 19 patients in one RCT. The effects on other critical and important outcomes are uncertain because of very low certainty of the evidence or they were not reported in the RCT.
Cyclosporin compared with other immunosuppressive therapy
• Cyclosporin compared with MMF plus dexamethasone (1 study, 138 participants) may have little or no effect on the following: all-cause mortality (RR 0.18, 95%CI 0.01 to 3.75), end stage kidney disease (RR 2.29, 95%CI 0.46 to 11.41), ≥ 50% GFR loss (RR 4.58, 95%CI 0.55 to 11.41), infection (RR 1.09, 95%CI 0.61 to 1.93), infection requiring hospitalization (RR 0.65, 95%CI 0.22 to 1.96), total hospitalization (RR 0.79, 95%CI 0.39 to 1.57), and complete remission (RR 2.41, 95%CI 0.87 to 6.71).
• Cyclosporin plus low dose prednisone compared with prednisone alone (1 study, 49 participants) may decrease end stage kidney disease (RR 0.35, 95%CI 0.12 to 0.98) and may increase partial remission (RR 7.96, 95%CI 1.09 to 58.15). There was too few who experienced complete remission to determine an effect. Compared with prednisone alone, cyclosporin plus low dose prednisone may have little or no effect on doubling of serum creatinine (RR 1.18, 95%CI 0.72 to 1.94), and other critical and important outcomes were not reported in the RCT.
• It is uncertain if complete remission is increased by cyclosporin plus prednisolone compared with treatment methylprednisolone, due to very serious imprecision (wide confidence intervals that cross the null with appreciable benefit and harm) and serious risk of bias. Other critical and important outcomes were not reported in the RCT (1 study, 25 participants).
• Cyclosporin plus prednisone compared with chlorambucil plus prednisone was examined in one small RCT (58 participants). It is uncertain if this increases or decreases complete remission or end-stage kidney disease, due to very serious risk of bias and very serious imprecision. Other critical and important outcomes were not reported in the RCT.
Mycophenolate mofetil versus prednisone
• Mycophenolate mofetil compared with prednisone may have little or no effect on complete remission (RR 1.05, 95%CI 0.58 to1.88), based on data from 33 patients in one RCT. The effects on infection or GFR (ml/min) are uncertain, due to serious risk of bias and very serious imprecision. Other critical and important outcomes were not reported in the RCT.
Dexamethasone 2 weekly vs. Dexamethasone 4 weekly (
• We are uncertain whether dexamethasone two-weekly compared to four-weekly increases or decreases partial remission or GFR (ml/min), due to serious risk of bias and very serious imprecision (1 study, 7 participants). Other critical and important outcomes were not reported in the RCT.
Biologic therapy
• There were too few partial remission events, to determine whether there is difference between fresolimumab (1mg and 4mg) compared to placebo. Other critical and important outcomes were not reported in the small RCT (36 participants).

3
• Compared to galactose or conservative therapy, we are unable to determine the effect of adalimumab on critical and important outcomes, either because there were two few events, study limitations and very serious imprecision in the effect estimates or they were not reported in the small RCT (21 participants)
Effect modifiers The following effect modifiers were considered:
• Kidney function (GFR, proteinuria, presence of albuminuria) • Relapse or resistance disease • Gender • Etiology, in particular adaptive FSGS vs. genetic or “idiopathic”
There was insufficient data to allow for the assessment of effect modifiers.
Studies from the 2012 KDIGO GN guideline evidence tables not included in 2018 evidence review.
No studies were found in the 2012 guideline that were not included in the 2018 review.

21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.1) Population: Patients with focal segmental glomerulosclerosis Intervention: Prednisolone plus chlorambucil Comparator: No treatment
Outcome Timeframe
Study results and measurements
Absolute effect estimates Certainty in effect estimates
(Quality of evidence) Plain text summary No treatment
Prednisolone plus
chlorambucil
All-cause mortality
(CI 95% - )
No studies were found that looked at all-cause
mortality Difference: fewer
End-stage kidney disease
(CI 95% - )
No studies were found
that looked at end-stage kidney disease Difference: fewer
≥50% loss of GFR
(CI 95% - )
No studies were found that looked at ≥50%
loss of GFR Difference: fewer
Malignancy
(CI 95% - )
No studies were found
that looked at malignancy Difference: fewer
Infection
(CI 95% - )
No studies were found that looked at infection
Difference: fewer
Complete remission
Relative risk: 1.75 (CI 95% 0.2 - 15.41)
Based on data from 15 patients in 1 studies1 Follow up 6 months
143 per 1000
250 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision2
We are uncertain whether prednisolone
plus chlorambucil compared with no
treatment increases or decreases complete
remission
Difference: 107 more per 1000 (CI 95% 114 fewer - 2061 more)
Doubling of serum creatinine
Relative risk: 0.3 (CI 95% 0.01 - 6.29)
Based on data from 15 patients in 1 studies3 Follow up 6 months
143 per 1000
43 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision4
We are uncertain whether prednisolone
plus chlorambucil compared with no
treatment increases or decreases doubling
serum creatinine
Difference: 100 fewer per 1000 (CI 95% 142 fewer - 756 more)
Annual GFR loss 3 years
Measured by: Scale: - Lower better
No studies were found that looked at annual
GFR loss Difference: null lower
1. Primary study Imbasciati 1980 Baseline/comparator: Control arm of reference used for intervention . 2. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very
Serious. Wide confidence intervals, Only data from one study, Low number of patients; 3. Primary study Imbasciati 1980 Baseline/comparator: Control arm of reference used for intervention .

4. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;

21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.2) Population: Patients with focal segmental glomerulosclerosis Intervention: Cyclosporin Comparator: No treatment
Outcome Timeframe
Study results and measurements
Absolute effect estimates Certainty in effect estimates
(Quality of evidence) Plain text summary No treatment Cyclosporin
All-cause mortality
(CI 95% - )
No studies were found that looked at all-cause
mortality Difference: fewer
End-stage kidney disease
Relative risk: 0.33 (CI 95% 0.02 - 7.39)
Based on data from 22 patients in 1 studies Follow up Median 18
months for cyclosporin group and 24 months for the no treatment group
91 per 1000
30 per 1000
Very Low Due to serious risk of bias, Due to
very serious imprecision1
We are uncertain whether cyclosporin compared with no
treatment increases or decreases end-stage
kidney disease Difference: 61 fewer per 1000
(CI 95% 89 fewer - 581 more)
≥50% loss of GFR
Relative risk: 0.33 (CI 95% 0.04 - 2.73)
Based on data from 22 patients in 1 studies2 Follow up Median 18
months for cyclosporin group and 24 months for the no treatment group
273 per 1000
90 per 1000
Very Low Due to serious risk of bias, Due to
very serious imprecision3
We are uncertain whether cyclosporin compared with no
treatment increases or decreases ≥50% loss of
GFR Difference: 183 fewer per 1000
(CI 95% 262 fewer - 472 more)
Infection
Relative risk: 0.9 (CI 95% 0.24 - 3.38)
Based on data from 19 patients in 1 studies4 Follow up Median 18
months for cyclosporin group and 24 months for the no treatment group
333 per 1000
300 per 1000
Very Low Due to serious risk of bias, Due to
very serious imprecision5
We are uncertain whether cyclosporin compared with no
treatment increases or decreases infection
Difference: 33 fewer per 1000 (CI 95% 253 fewer - 793 more)
Malignancy
(CI 95% - )
No studies were found that looked at all-cause
mortality Difference: fewer
Complete remission
Relative risk: 4.55 (CI 95% 0.25 - 83.7)
Based on data from 19 patients in 1 studies6 Follow up Median 18
months for cyclosporin group and 24 months for the no treatment group
0 per 1000
0 per 1000
Very Low Due to serious risk of bias, Due to
very serious imprecision7
There were too few who experienced the
complete remission, to determine whether
cyclosporin compared to no treatmetn made a
difference
Difference: 0 fewer per 1000 (CI 95% 0 fewer - 0 fewer)
Doubling of serum creatinine
Relative risk: 0.6 (CI 95% 0.25 - 1.46)
Based on data from 19 patients in 1 studies8 Follow up Median 18
months for cyclosporin group and 24 months for the no treatment group
667 per 1000
400 per 1000
Low Due to serious risk of bias, Due to
serious imprecision9
Cyclosporin compared to no treatment may
have little or no difference on doubling
of serum creatinine Difference: 267 fewer per 1000
(CI 95% 500 fewer - 307 more)
Annual GFR loss 3 years
Measured by: Scale: - Lower better
No studies were found that looked at annual

Difference: null lower
GFR loss
1. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;
2. Primary study Ponticelli 1993a Baseline/comparator: Control arm of reference used for intervention . 3. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very
Serious. Wide confidence intervals, Only data from one study, Low number of patients; 4. Primary study Ponticelli 1993a Baseline/comparator: Control arm of reference used for intervention . 5. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very
Serious. Wide confidence intervals, Only data from one study, Low number of patients; 6. Primary study Ponticelli 1993a Baseline/comparator: Control arm of reference used for intervention . 7. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very
Serious. Wide confidence intervals, Only data from one study, Low number of patients; 8. Primary study Ponticelli 1993a Baseline/comparator: Control arm of reference used for intervention . 9. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision:
Serious. Only data from one study, Low number of patients;

21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.3) Population: Patients with focal segmental glomerulosclerosis Intervention: Cyclosporin Comparator: Mycophenolate mofetil plus dexamethasone
Outcome Timeframe
Study results and measurements
Absolute effect estimates
Certainty in effect estimates (Quality of evidence) Plain text summary Mycophenolat
e mofetil plus dexamethason
e Cyclosporin
All-cause mortality
12 months
Relative risk: 0.18 (CI 95% 0.01 - 3.75)
Based on data from 138 patients in 1 studies
Follow up 19.5 months
30 per 1000
5 per 1000 Low
Due to very serious imprecision1
Cyclosporin compared with MMF plus
dexamethasone may have little or no
difference on all-cause mortality
Difference: 25 fewer per 1000 (CI 95% 30 fewer - 83 more)
End-stage kidney disease
Relative risk: 2.29 (CI 95% 0.46 - 11.41)
Based on data from 138 patients in 1 studies
Follow up 19.5 months
15 per 1000
34 per 1000 Low
Due to very serious imprecision2
Cyclosporin compared with MMF plus
dexamethasone may have little or no
difference on end-stage kidney disease
Difference: 19 more per 1000 (CI 95% 8 fewer - 156 more)
≥50% loss of GFR
Relative risk: 4.58 (CI 95% 0.55 - 38.22)
Based on data from 138 patients in 1 studies
Follow up 19.5 months
30 per 1000
137 per 1000 Low
Due to very serious imprecision3
Cyclosporin compared with MMF plus
dexamethasone may have little or no
difference on ≥50% loss of GFR
Difference: 107 more per 1000 (CI 95% 13 fewer - 1117 more)
Infection
Relative risk: 1.09 (CI 95% 0.61 - 1.93)
Based on data from 138 patients in 1 studies
Follow up 19.5 months
242 per 1000
264 per 1000 Low
Due to very serious imprecision4
Cyclosporin compared with MMF plus
dexamethasone may have little or no
difference on infection Difference: 22 more per 1000
(CI 95% 94 fewer - 225 more)
Infection - requiring
hospitalization5
Relative risk: 0.65 (CI 95% 0.22 - 1.96)
Based on data from 138 patients in 1 studies
Follow up 19.5 months
106 per 1000
69 per 1000
Low Due to very serious imprecision6
Cyclosporin compared with MMF plus
dexamethasone may have little or no
difference on serious infection requiring hospitalizations
Difference: 37 fewer per 1000 (CI 95% 83 fewer - 102 more)
Malignancy
(CI 95% - )
No studies were found
that looked at malignancy Difference: fewer
Complete remission 12 months
Relative risk: 2.41 (CI 95% 0.87 - 6.71)
Based on data from 138 patients in 1 studies
Follow up 19.5 months
91 per 1000
219 per 1000 Low
Due to very serious imprecision7
Cyclosporin compared with MMF plus
dexamethasone may have little or no
difference on complete remission
Difference: 128 more per 1000 (CI 95% 12 fewer - 520 more)
Total hospitalizations
Relative risk: 0.79 (CI 95% 0.39 - 1.57)
Based on data from 138 patients in 1 studies
Follow up 19.5 months
212 per 1000
167 per 1000 Low
Due to very serious imprecision8
Cyclosporin compared with MMF plus
dexamethasone may have little or no
difference on total hospitalizations
Difference: 45 fewer per 1000 (CI 95% 129 fewer - 121 more)
Annual GFR loss 3 years
Measured by: Scale: - High better
No studies were found that looked at annual

Difference: null lower
GFR loss
1. Imprecision: Very Serious. 2. Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients; 3. Imprecision: Very Serious. Wide confidence intervals, Low number of patients, Only data from one study; 4. Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients; 5. Serious infections requiring hospitalization 6. Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients; 7. Imprecision: Very Serious. Only data from one study, Low number of patients, Wide confidence intervals; 8. Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;

21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.4) Population: Patients with focal segmental glomerulosclerosis Intervention: Cyclosporin plus low dose prednisone Comparator: Prednisone
Outcome Timeframe
Study results and measurements
Absolute effect estimates Certainty in effect estimates
(Quality of evidence) Plain text summary Prednisone
Cyclosporin plus low dose
prednisone
All-cause mortality
(CI 95% - )
No studies were found that looked at all-cause
mortality Difference: fewer
End-stage kidney disease
Relative risk: 0.35 (CI 95% 0.13 - 0.98)
Based on data from 49 patients in 1 studies Follow up 50 months
435 per 1000
152 per 1000 Low
Due to serious risk of bias, Due to serious imprecision1
Cyclosporin plus low dose prednisone compared with
prednisione alone may decrease end-stage
kidney disease Difference: 283 fewer per 1000
(CI 95% 378 fewer - 9 fewer)
Infection
(CI 95% - )
No studies were found that looked at infection
Difference: fewer
Malignancy
(CI 95% - )
No studies were found
that looked at malignancy Difference: fewer
≥50% loss of GFR
(CI 95% - )
No studies were found that looked at ≥50%
loss of GFR Difference: fewer
Complete remission
Relative risk: 2.67 (CI 95% 0.11 - 62.42)
Based on data from 49 patients in 1 studies Follow up 50 months
0 per 1000
0 per 1000
Very Low Due to serious risk of bias, Due to
very serious imprecision2
There were too few who experienced the
complete remission, to determine whether
cyclosporin plus low dose prednisone compared with
prednisione alone made a difference
Difference: 0 fewer per 1000 (CI 95% 0 fewer - 0 fewer)
Partial remission
Relative risk: 7.96 (CI 95% 1.09 - 58.15)
Based on data from 49 patients in 1 studies Follow up 50 months
43 per 1000
342 per 1000 Moderate
Due to serious risk of bias, Due to serious imprecision,Upgraded due
to Large magnitude of effect3
Cyclosporin plus low dose prednisone compared with
prednisione alone probably increase partial remission
Difference: 299 more per 1000 (CI 95% 4 more - 2457 more)
Doubling serum creatinine
Relative risk: 1.18 (CI 95% 0.72 - 1.94)
Based on data from 49 patients in 1 studies Follow up 50 months
522 per 1000
616 per 1000 Low
Due to serious risk of bias, Due to serious imprecision4
Cyclosporin plus low dose prednisone compared with
prednisone alone may have little or no
difference on doubling serum creatinine
Difference: 94 more per 1000 (CI 95% 146 fewer - 491 more)

Annual GFR loss
Measured by: Scale: - Lower better
No studies were found that looked at annual
GFR loss Difference: null lower
1. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Serious. Only data from one study;
2. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very Serious. Only data from one study, Low number of patients, Wide confidence intervals;
3. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Serious. Wide confidence intervals, Only data from one study, Low number of patients; Upgrade: Large magnitude of effect.
4. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Serious. Only data from one study, Low number of patients;

21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.5) Population: Patients with focal segmental glomerulosclerosis Intervention: Cyclosporin plus prednisolone Comparator: Methylprednisolone
Outcome Timeframe
Study results and measurements
Absolute effect estimates Certainty in effect estimates
(Quality of evidence) Plain text summary Methylprednis
olone Cyclosporin
plus prednisolone
All-cause mortality
(CI 95% - )
No studies were found that looked at all-cause
mortality Difference: fewer
End-stage kidney disease
(CI 95% - )
No studies were found
that looked at end-stage kidney disease Difference: fewer
≥50% loss of GFR
(CI 95% - )
No studies were found that looked at ≥50%
loss of GFR Difference: fewer
Infection
(CI 95% - )
No studies were found that looked at infection
Difference: fewer
Malignancy
(CI 95% - )
No studies were found
that looked at malignancy Difference: fewer
Complete remission
Relative risk: 2.31 (CI 95% 0.55 - 9.74)
Based on data from 25 patients in 1 studies1 Follow up 3 months
167 per 1000
386 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision2
We are uncertain whether cyclosporin plus prednisolone
compared with methylprednisone
increases or decreases complete remission
Difference: 219 more per 1000 (CI 95% 75 fewer - 1460 more)
Annual GFR loss
Measured by: Scale: - Lower better
Mean
Mean
No studies were found that looked at annual
GFR loss Difference: MD null lower
1. Primary study Bhaumik 2002 Baseline/comparator: Control arm of reference used for intervention . 2. Risk of bias: Serious. Unclear sequence generation/ generation of comparable groups, resulting in potential for selection bias, unclear
concealment of allocation during randomization process, resulting in potential for selection bias, Unclear loss to follow up and selective outcome reporting; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;

21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.6) Population: Patients with focal segmental glomerulosclerosis Intervention: Cyclosporin plus prednisone Comparator: Chlorambucil plus prednisone
Outcome Timeframe
Study results and measurements
Absolute effect estimates Certainty in effect estimates
(Quality of evidence) Plain text summary Chlorambucil plus
prednisone
Cyclosporin plus
prednisone
All-cause mortality
(CI 95% - )
No studies were found that looked at all-cause
mortality Difference: fewer
End-stage kidney disease
Relative risk: 1.06 (CI 95% 0.33 - 3.35)
Based on data from 58 patients in 1 studies Follow up 4 years
167 per 1000
177 per 1000
Very Low Due to very serious risk of bias, Due to very serious imprecision1
We are uncertain whether cyclosporin
plus prednisone compared with
chlorambucil plus prednisone increases or
decreases end-stage kidney disease
Difference: 10 more per 1000 (CI 95% 112 fewer - 392 more)
≥50% loss of GFR
(CI 95% - )
No studies were found that looked at ≥50%
loss of GFR Difference: fewer
Infection
(CI 95% - )
No studies were found that looked at infection
Difference: fewer
Malignancy
(CI 95% - )
No studies were found
that looked at malignancy Difference: fewer
Complete remission
Relative risk: 1.41 (CI 95% 0.48 - 4.16)
Based on data from 58 patients in 1 studies2
Follow up 4 years
167 per 1000
235 per 1000
Very Low Due to very serious risk of bias, Due to very serious imprecision3
We are uncertain whether cyclosporin
plus prednisone compared with
chlorambucil plus prednisone increases or
decreases complete remission
Difference: 68 more per 1000 (CI 95% 87 fewer - 528 more)
Annual GFR loss 3 years
Measured by: Scale: - Lower better
No studies were found that looked at annual
GFR loss Difference: null lower
1. Risk of bias: Very Serious. Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias, Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Selective outcome reporting; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;
2. Primary study Heering 2004 Baseline/comparator: Control arm of reference used for intervention . 3. Risk of bias: Very Serious. Inadequate sequence generation/ generation of comparable groups, resulting in potential for selection bias,
Inadequate concealment of allocation during randomization process, resulting in potential for selection bias, Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Selective outcome reporting; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;

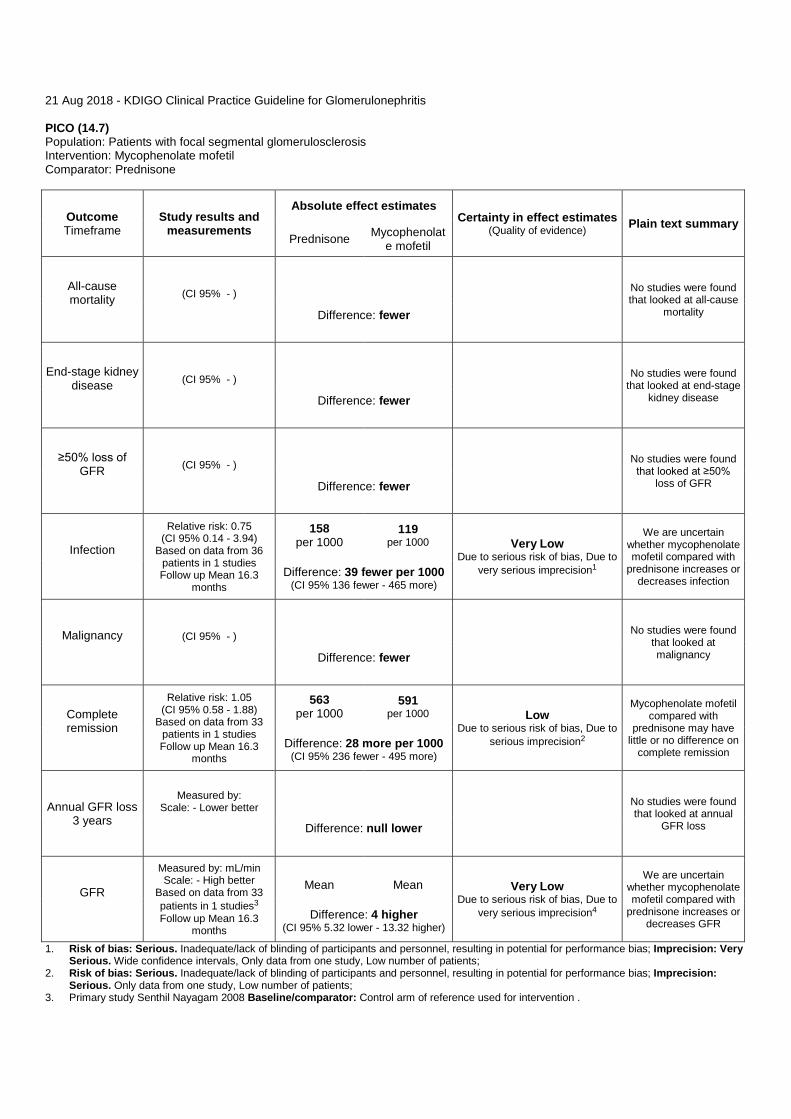
21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.7) Population: Patients with focal segmental glomerulosclerosis Intervention: Mycophenolate mofetil Comparator: Prednisone
Outcome Timeframe
Study results and measurements
Absolute effect estimates Certainty in effect estimates
(Quality of evidence) Plain text summary Prednisone Mycophenolat
e mofetil
All-cause mortality
(CI 95% - )
No studies were found that looked at all-cause
mortality Difference: fewer
End-stage kidney disease
(CI 95% - )
No studies were found
that looked at end-stage kidney disease Difference: fewer
≥50% loss of GFR
(CI 95% - )
No studies were found that looked at ≥50%
loss of GFR Difference: fewer
Infection
Relative risk: 0.75 (CI 95% 0.14 - 3.94)
Based on data from 36 patients in 1 studies Follow up Mean 16.3
months
158 per 1000
119 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision1
We are uncertain whether mycophenolate mofetil compared with
prednisone increases or decreases infection
Difference: 39 fewer per 1000 (CI 95% 136 fewer - 465 more)
Malignancy
(CI 95% - )
No studies were found
that looked at malignancy Difference: fewer
Complete remission
Relative risk: 1.05 (CI 95% 0.58 - 1.88)
Based on data from 33 patients in 1 studies Follow up Mean 16.3
months
563 per 1000
591 per 1000 Low
Due to serious risk of bias, Due to serious imprecision2
Mycophenolate mofetil compared with
prednisone may have little or no difference on
complete remission Difference: 28 more per 1000
(CI 95% 236 fewer - 495 more)
Annual GFR loss 3 years
Measured by: Scale: - Lower better
No studies were found that looked at annual
GFR loss Difference: null lower
GFR
Measured by: mL/min Scale: - High better
Based on data from 33 patients in 1 studies3 Follow up Mean 16.3
months
Mean
Mean Very Low
Due to serious risk of bias, Due to very serious imprecision4
We are uncertain whether mycophenolate mofetil compared with
prednisone increases or decreases GFR
Difference: 4 higher (CI 95% 5.32 lower - 13.32 higher)
1. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;
2. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Serious. Only data from one study, Low number of patients;
3. Primary study Senthil Nayagam 2008 Baseline/comparator: Control arm of reference used for intervention .

4. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;

21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.8) Population: Patients with focal segmental glomerulosclerosis Intervention: Dexamethasone 2 weekly Comparator: Dexamethasone 4 weekly
Outcome Timeframe
Study results and measurements
Absolute effect estimates Certainty in effect estimates
(Quality of evidence) Plain text summary Dexamethason
e 4 weekly Dexamethason
e 2 weekly
All-cause mortality
(CI 95% - )
No studies were found that looked at all-cause
mortality Difference: fewer
End-stage kidney disease
(CI 95% - )
No studies were found
that looked at end-stage kidney disease Difference: fewer
≥50% loss of GFR
(CI 95% - )
No studies were found that looked at ≥50%
loss of GFR Difference: fewer
Infection
(CI 95% - )
No studies were found that looked at infection
Difference: fewer
Malignancy
(CI 95% - )
No studies were found that looked at infection
Difference: fewer
Complete remission
(CI 95% - )
No studies were found that looked at complete
remission Difference: fewer
Partial remission
Relative risk: 0.75 (CI 95% 0.07 - 7.73)
Based on data from 7 patients in 1 studies Follow up 11 months
334 per 1000
251 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision1
We are uncertain whether
dexamethasone 2 weekly compared to 4 weekly increases or
decreases partial remission
Difference: 83 fewer per 1000 (CI 95% 311 fewer - 2248 more)
Annual GFR loss 3 years
Measured by: Scale: - Lower better
No studies were found that looked at annual
GFR loss Difference: null lower
GFR
Measured by: mL/min Scale: - High better
mL/minMean
mL/minMean
Very Low Due to serious risk of bias, Due to
We are uncertain whether

Based on data from 7 patients in 1 studies2 Follow up 11 months
Difference: 13 lower (CI 95% 40.53 lower - 14.53 higher)
very serious imprecision3 dexamethasone 2 weekly compared to 4 weekly increases or
decreases GFR 1. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very
Serious. Wide confidence intervals, Only data from one study, Low number of patients; 2. Primary study Cho 2011 Baseline/comparator: Control arm of reference used for intervention . 3. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias; Imprecision: Very
Serious. Wide confidence intervals, Only data from one study, Low number of patients;

21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.9) Population: Patients with focal segmental glomerulosclerosis Intervention: Fresolimumab Comparator: Placebo
Outcome Timeframe
Study results and measurements
Absolute effect estimates Certainty in effect estimates
(Quality of evidence) Plain text summary Placebo Fresolimumab
All-cause mortality
(CI 95% - )
No studies were found that looked at all-cause
mortality Difference: fewer
End-stage kidney disease
(CI 95% - )
No studies were found
that looked at end-stage kidney disease Difference: fewer
≥50% loss of GFR
(CI 95% - )
No studies were found that looked at ≥50%
loss of GFR Difference: fewer
Infection
(CI 95% - )
No studies were found that looked at infection
Difference: fewer
Malignancy
(CI 95% - )
No studies were found
that looked at malignancy Difference: fewer
Complete remission
(CI 95% - )
No studies were found that looked at complete
remission Difference: fewer
Partial remission - Fresolimumab 1
mg 4 months
Relative risk: 3.67 (CI 95% 0.19 - 69.01)
Based on data from 24 patients in 1 studies1 Follow up 9 months
0 per 1000
0 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision2
There were too few who experienced the partial remission, to determine whether fresolimumab (1 mg) compared to
placebo made a difference
Difference: 0 fewer per 1000 (CI 95% 0 fewer - 0 fewer)
Partial remission - Fresolimumab 4
mg 4 months
Relative risk (CI 95% - )
Based on data from 22 patients in 1 studies3 Follow up 9 months
0 per 1000
per 1000
There were too few who experienced the partial remission, to determine whether fresolimumab
(4mg) compared to placebo made a
difference
Difference: fewer per 1000
Annual GFR loss
Measured by: Scale: - Lower better
No studies were found that looked at annual

Difference: null lower
GFR loss
1. Primary study Vincenti 2017 Baseline/comparator: Control arm of reference used for intervention . 2. Risk of bias: Serious. Unclear sequence generation/ generation of comparable groups, resulting in potential for selection bias, Unclear
concealment of allocation during randomization process, resulting in potential for selection bias; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;
3. Primary study Vincenti 2017 Baseline/comparator: Control arm of reference used for intervention .

21 Aug 2018 - KDIGO Clinical Practice Guideline for Glomerulonephritis PICO (14.10) Population: Patients with focal segmental glomerulosclerosis Intervention: Adalimumab Comparator: Galactose or conservative therapy
Outcome Timeframe
Study results and measurements
Absolute effect estimates Certainty in effect estimates
(Quality of evidence) Plain text summary Galactose or conservative
therapy Adalimumab
All-cause mortality
Relative risk (CI 95% - )
Based on data from 21 patients in 1 studies1 Follow up 6 months
0 per 1000
0 per 1000
Low Due to serious risk of bias, Due to
serious imprecision2
There were too few who experienced all-cause mortality, to determine whether adalimumab compared to control
(conservative therapy or galactose) made a
difference
Difference: 0 fewer per 1000 (CI 95% 0 fewer - 0 fewer)
End-stage kidney disease
Relative risk: 2.0 (CI 95% 0.15 - 27.45)
Based on data from 21 patients in 1 studies3 Follow up 6 months
71 per 1000
142 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision4
We are uncertain whether adalimumab
increases or decreases end-stage kidney
disease Difference: 71 more per 1000
(CI 95% 60 fewer - 1878 more)
≥50% loss of GFR
(CI 95% - )
No studies were found that looked at ≥50%
loss of GFR Difference: fewer
Infection
Relative risk: 1.11 (CI 95% 0.6 - 2.04)
Based on data from 21 patients in 1 studies5 Follow up 6 months
643 per 1000
714 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision6
We are uncertain whether adalimumab
increases or decreases infection Difference: 71 more per 1000
(CI 95% 257 fewer - 669 more)
Serious adverse event -
hospitalization
Relative risk: 3.0 (CI 95% 0.64 - 14.02)
Based on data from 21 patients in 1 studies7 Follow up 6 months
143 per 1000
429 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision8
We are uncertain whether adalimumab
increases or decreases serious adverse event -
hospitalization Difference: 286 more per 1000
(CI 95% 51 fewer - 1862 more)
50% reduction in proteinuria
Relative risk: 0.17 (CI 95% 0.01 - 2.71)
Based on data from 21 patients in 1 studies9 Follow up 6 months
357 per 1000
61 per 1000 Very Low
Due to serious risk of bias, Due to very serious imprecision10
We are uncertain whether adalimumab
increases or decreases 50% reduction in
proteinuria Difference: 296 fewer per 1000
(CI 95% 353 fewer - 610 more)
Malignancy
Relative risk (CI 95% - )
Based on data from 21 patients in 1 studies Follow up 6 months
per 1000
per 1000
Low Due to serious risk of bias, Due to
serious imprecision11
There were too few who experienced
malignancy, to determine whether
adalimumab compared to control (conservative therapy or galactose)
made a difference
Difference: fewer per 1000
Complete remission
(CI 95% - )
No studies were found that looked at complete
remission Difference: fewer

Annual GFR loss 3 years
Measured by: Scale: - Lower better
Difference: null lower
1. Systematic review [19] with included studies: FONT II 2011 Baseline/comparator: Control arm of reference used for intervention . 2. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Unclear sequence
generation/ generation of comparable groups, resulting in potential for selection bias, Unclear concealment of allocation during randomization process, resulting in potential for selection bias; Imprecision: Serious. Only data from one study, Low number of patients, Wide confidence intervals, Only data from one study, Low number of patients;
3. Systematic review [19] with included studies: FONT II 2011 Baseline/comparator: Control arm of reference used for intervention . 4. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Unclear sequence
generation/ generation of comparable groups, resulting in potential for selection bias, Unclear concealment of allocation during randomization process, resulting in potential for selection bias; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;
5. Systematic review [19] with included studies: FONT II 2011 Baseline/comparator: Control arm of reference used for intervention . 6. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Unclear sequence
generation/ generation of comparable groups, resulting in potential for selection bias, Unclear concealment of allocation during randomization process, resulting in potential for selection bias; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;
7. Systematic review [19] with included studies: FONT II 2011 Baseline/comparator: Control arm of reference used for intervention . 8. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Unclear sequence
generation/ generation of comparable groups, resulting in potential for selection bias, Unclear concealment of allocation during randomization process, resulting in potential for selection bias; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;
9. Systematic review [19] with included studies: FONT II 2011 Baseline/comparator: Control arm of reference used for intervention . 10. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Unclear sequence
generation/ generation of comparable groups, resulting in potential for selection bias, Unclear concealment of allocation during randomization process, resulting in potential for selection bias; Imprecision: Very Serious. Wide confidence intervals, Only data from one study, Low number of patients;
11. Risk of bias: Serious. Inadequate/lack of blinding of participants and personnel, resulting in potential for performance bias, Unclear sequence generation/ generation of comparable groups, resulting in potential for selection bias, Unclear concealment of allocation during randomization process, resulting in potential for selection bias; Imprecision: Serious. Only data from one study, Low number of patients;
References [19] Immunosuppressive treatment for focal segmental glomerulosclerosis in adults. 2018;