ken lim consultant gynaecological oncology surgeon welsh
TRANSCRIPT

Ken LimConsultant Gynaecological Oncology
SurgeonWelsh Regional Centre for Gynaecological Oncology
Llandough Hospital


Patient Journey – Endometrial cancer
• Mrs REM is a 67 year old retired solicitor on HRT presented with heavy PV bleeding to the GP.
• She is overweight and a non insulin dependent diabetic.

• Rapid access referral to local gynaecologist, who then performed pipellebiopsy of the endometrium and a transvaginal scan. This demonstrated –
1. Complex atypical hyperplasia on histology
2. 20mm endometrial thickness
A Hysteroscopy is therefore warranted

Hysteroscopy
This confirms an adenocarcinoma

TAH and BSO +/- LN
Difficulties with large patient and comorbity
Risk of complications
Role of lymphadenectomy still unsure –ASTEC trial
(Total Abdominal Hysterectomy and bilateral
salpingoopherectomy and possibly lymph node dissection)

Histology of TAH
• More than 50%
invasion of
myometrium (Stage
1C) with Negative
Lymph Nodes
• Will require adjuvant
treatment

Patient Journey – Ovarian
cancer

• Mrs JW is 70 and was visiting her son in Canada
• She developed abdominal distension and bloating was diagnosed with irritable bowel syndrome. A week after her return to the UK she developed a swollen left leg and was diagnosed with a DVT.
• On further vaginal examination she was found to have a mass in the pelvis

• An abdominal ultrasound scan demonstrated –– “12cm x 14cm multiloculated mass in the right iliac fossaand extending into the Pouch of Douglas, there is also a moderate amount of ascites”
– Ca 125 came back as 970iu/l.
• The consultant gynaecological oncologist came to see her the next day to brief her on the management plan.

Laparotomy and debulking

• Main aim to debulk to 0cm disease
• Attempt to remove ovaries and uterus and
omentum
• Also to clinically stage disease
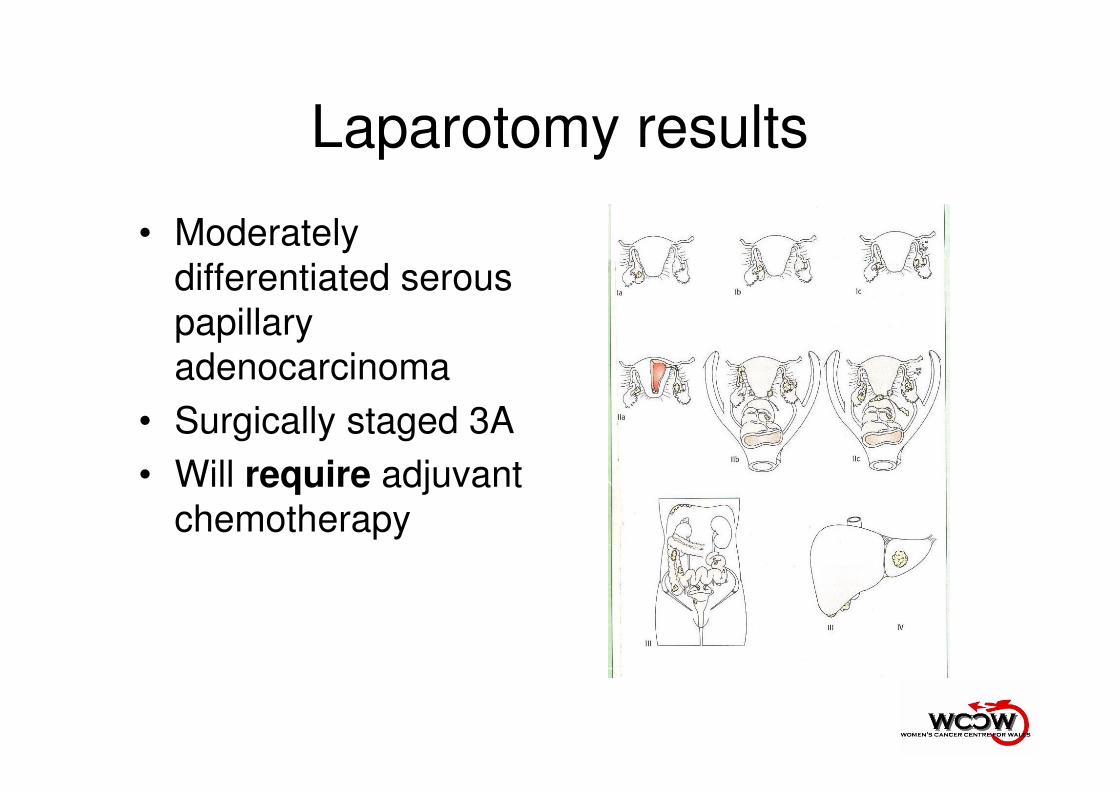
Laparotomy results
• Moderately
differentiated serous
papillary
adenocarcinoma
• Surgically staged 3A
• Will require adjuvant
chemotherapy

Patient Journey – Cervical
Cancer

Colposcopy
• Mrs RW is 28, nulliparous and a young professional
• She had a smear when she was 21 and since then has persistently defaulted from her smear
• She had persistent post coital bleeding for 4 months before presenting to her GP
• At examination the cervix appeared abnormal and she was then referred on to the local colposcopy unit
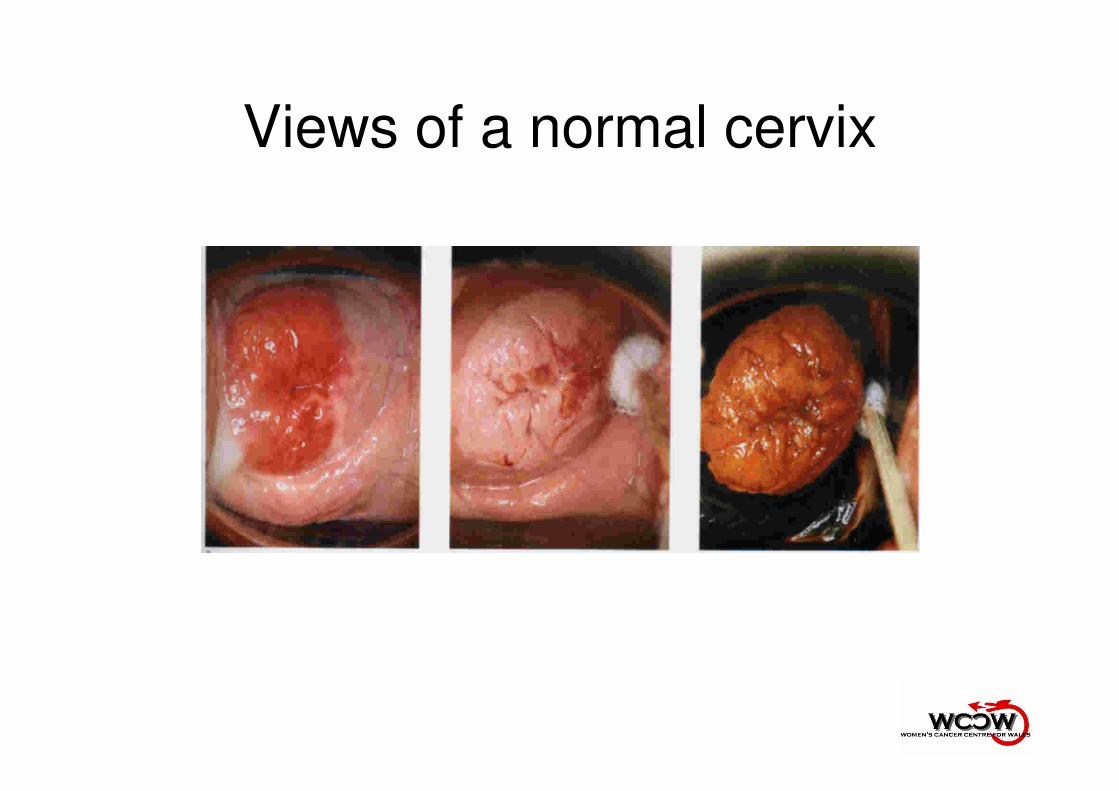
Views of a normal cervix

Punch
biopsy
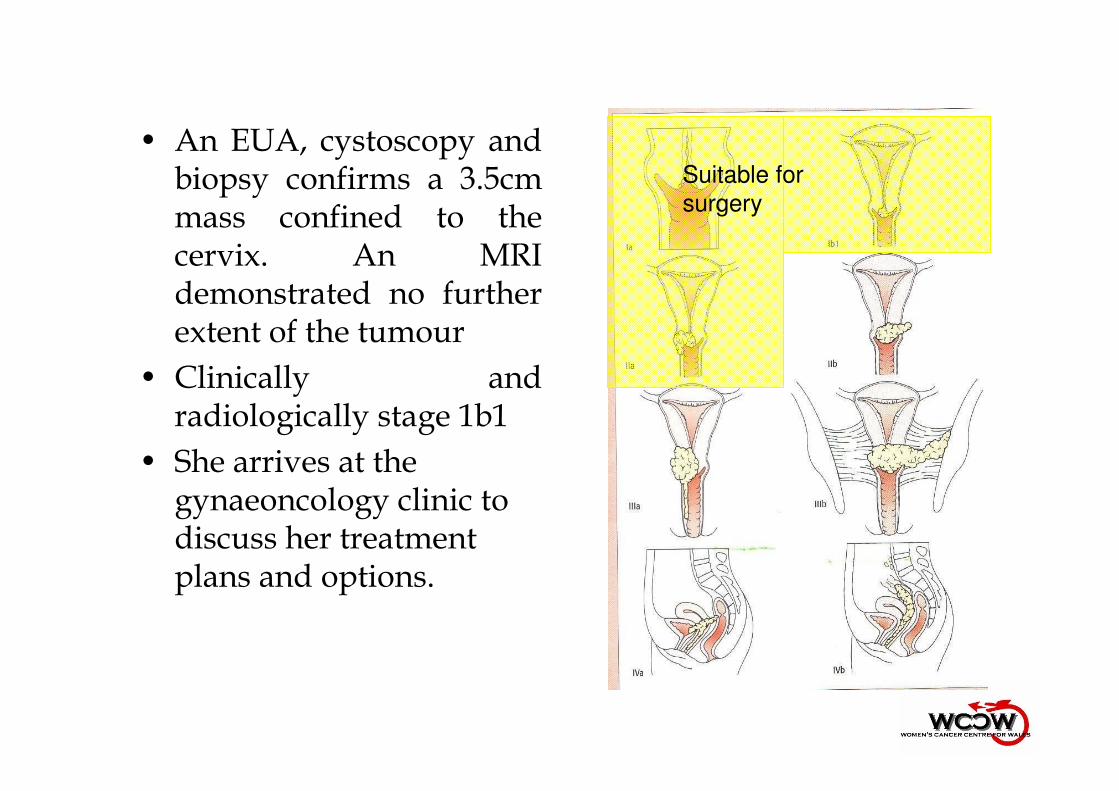
• An EUA, cystoscopy and biopsy confirms a 3.5cm mass confined to the cervix. An MRI demonstrated no further extent of the tumour
• Clinically and radiologically stage 1b1
• She arrives at the gynaeoncology clinic to discuss her treatment plans and options.
Suitable for
surgery

Early stage cervical cancer
Simple hysterectomy
Radical
hysterectomy
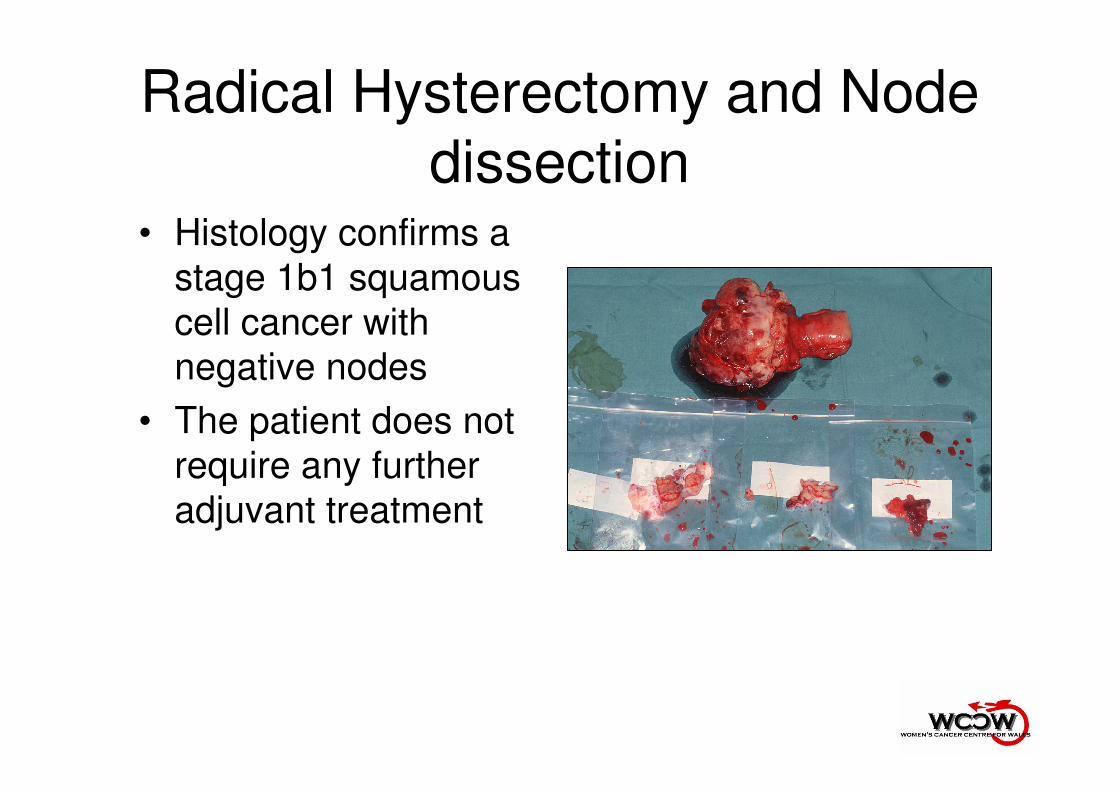
Radical Hysterectomy and Node
dissection• Histology confirms a
stage 1b1 squamous
cell cancer with
negative nodes
• The patient does not
require any further
adjuvant treatment
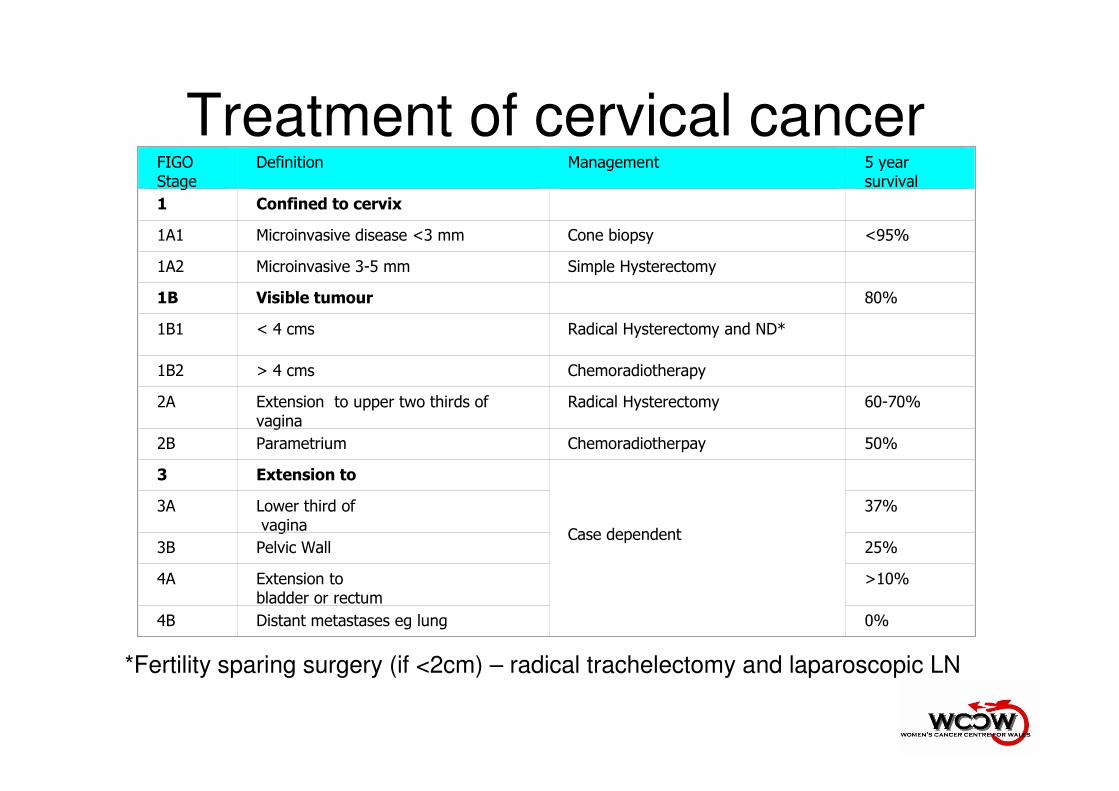
Treatment of cervical cancerFIGO Stage
Definition Management 5 yearsurvival
1 Confined to cervix
1A1 Microinvasive disease <3 mm Cone biopsy <95%
1A2 Microinvasive 3-5 mm Simple Hysterectomy
1B Visible tumour 80%
1B1 < 4 cms Radical Hysterectomy and ND*
1B2 > 4 cms Chemoradiotherapy
2A Extension to upper two thirds of vagina
Radical Hysterectomy 60-70%
2B Parametrium Chemoradiotherpay 50%
3 Extension to
Case dependent
3A Lower third ofvagina
37%
3B Pelvic Wall 25%
4A Extension tobladder or rectum
>10%
4B Distant metastases eg lung 0%
*Fertility sparing surgery (if <2cm) – radical trachelectomy and laparoscopic LN

Recurrent Cervical/endometrial
cancer• If had full radical dose
of radiotherapy and
ONLY central disease
then….
• Exenterative
procedure (Removal
of bladder +/- rectum)
Patient Journey – Vulval
cancer

• Mrs GT is a catering manager who has been suffering with quite severe pruritis vulvae for the 2 years
– No help with various creams
– A 3 cm nodule was discovered on the left labia which bled easily
– A lump was found on the right groin
• Referred to the gynaecological oncology centre

• EUA and Wide Local Excision scheduled for the following week– “a moderately differentiated
Squamous Cell Carcinoma extending to the cut margins”.
• A CT scan – 1 abnormal looking lymph
nodes in the right groin measuring 2 cm and was thought to be suspicious of a metastasis
• She was brought back to the clinic the following week for the results.

• Definitive surgery is Radical excision (hemivulvectomy/vulvectomy/WLE) and Bilateral groin node dissection
• Choice of whether unilateral or bilateral groin nodes performed is dependent on the distance from midline
• Complications include
– 50% risk of wound breakdown
– High risk of lymphoedema

Follow Up
• Very variable
• No evidence that it is useful in detecting early recurrence
• Other useful reasons to follow up– Complications
– Patient and Physician morale
– Research data
• Currently – 3 months (1st year)
– 6 months (2nd year)
– Yearly till 5 years
The Future
• Total Laparoscopic
Hysterectomy for
Endometrial cancer
• Radical
Trachelectomy for
early cervical cancer
• Sentinal Node biopsy
for vulval cancers
• Improved interface
between clinicians
and registries
• ? Direct clinician data
input
• Electronic patient
record