keto-5,8-pregnane-18-al, -...
TRANSCRIPT

Journal of Clinical InvestigationVol. 41, No. 8, 1962
THE METABOLISMOF ALDOSTERONEIN NORMALSUBJECTSAND IN PATIENTS WITH HEPATIC CIRRHOSIS *
By W. S. COPPAGE,JR., D. P. ISLAND, A. E. COONERAND GRANTW. LIDDLE
(From the Department of Medicine, Vanderbilt University School of Medicine,Nashville, Tenn.)
(Submitted for publication February 12, 1962; accepted May 3, 1962)
The importance of the liver in the metabolismof cortisol has been amply demonstrated (1-3).There is comparatively little published informa-tion, however, on the role of the liver in the metab-olism of aldosterone, the most important mineralo-corticoid secreted by the adrenal cortex. Chart,Gordon, Helmer and LeSher (4) have demon-strated rapid inactivation of aldosterone by liverslices and impairment of this process under ana-erobic conditions. Yates, Urquhart and Herbst(5) demonstrated impairment of enzymatic inac-tivation of aldosterone by the passively congestedrat liver. Ayers, Davis, Liebermann and Car-penter (6) demonstrated that the disappearanceof tritiated aldosterone from the plasma was de-layed in dogs with passively congested livers.After hepatectomy the disappearance of aldos-terone from the circulation was delayed still more.
An investigation of aldosterone metabolism nec-essarily entails the identification and quantitationof the metabolic end products which are excretedin the urine. Very little aldosterone appears inthe urine in unaltered form. The major portionof what is commonly called "urinary aldosterone"is actually a water-soluble, biologically inactivemetabolite which can be reconverted to aldosteroneby acidification of the urine to pH 1. This acid-hydrolyzable metabolite is frequently referred toas a "3-oxo-conjugate" of aldosterone, althoughits exact chemical identity is not yet known. Anumber of studies have shown that patients withhepatic cirrhosis and ascites have abnormally largequantities of the 3-oxo-conjugate of aldosteronein their urine (7, 8). This is generally consideredto be a reflection of the increased secretion of al-dosterone in this disorder. The major urinarymetabolite of aldosterone is the ring-A reductionproduct identified as 3a,11,/,21-trihydroxy-20-
* These studies were supported in part by grants-in-aidfrom the United States Public Health Service (A-1748,2A-5092, and OG-2).
keto-5,8-pregnane-18-al, or tetrahydroaldosterone,by Ulick, Kusch and August (9). Earlier workhad suggested a somewhat different tentativestructure for which the term tetrahydroaldosteronewas less applicable (10). Tetrahydroaldosteroneis biologically inactive. It is apparently excretedas a glucuronic acid conjugate, inasmuch as it can-not be extracted from the urine with organic sol-vents until incubated with f-glucuronidase. It isusually excreted in increased quantities by pa-tients with cirrhosis and ascites (11). Becauseit is derived solely from aldosterone, it has beenutilized in a procedure for the indirect determina-tion of aldosterone secretion rate. Secretion ratesas determined by this method have been found tobe elevated in patients with cirrhosis and ascites(11). There is a considerable body of evidence,therefore, indicating that the secretion of aldos-terone and the excretion of aldosterone metabo-lites are elevated in patients with cirrhosis andascites. In addition, Hurter and Nabarro (12)have recently called attention to a possible altera-tion in the ratio of 3-oxo-conjugate to tetrahydro-aldosterone in the urine of such patients.
The quantitative role of the human liver in themetabolism of aldosterone has not, however, re-ceived adequate study. The availability of tritiatedd-aldosterone (the natural isomer) of high specificactivity has made it possible to carry out studiesof aldosterone metabolism in man with advantagesin identification, isolation, and quantitation af-forded by the radioactive label. The present studywas undertaken to elucidate the role of the nor-mal and diseased liver in aldosterone metabolismin man. The metabolism of aldosterone adminis-tered orally was compared with that administeredintravenously. Plasma aldosterone disappearancecurves, patterns of urinary aldosterone metabo-lites, and aldosterone secretion rates were deter-mined in normal subjects and in patients withhepatic cirrhosis.
1672

ALDOSTERONEMETABOLISMIN NORMALSUBJECTSAND PATIENTS WITH CIRRHOSIS 1673
MATERIALS AND METHODS
Sixteen normal subjects and 9 patients with cirrhosiswere studied. The normal subjects were young, healthyvolunteers from the medical or technical staffs of Van-derbilt University Hospital. All of the patients withcirrhosis had gross clinical evidence of hepatic decom-pensation, and most of them had ascites. Derangementof hepatocellular function was confirmed in all by theusual liver function tests (sulfobromophthalein retention,serum bilirubin, cephalin flocculation, thymol turbidity,serum alkaline phosphatase, and serum proteins). Infive patients histological confirmation of the diagnosis was
obtained. Most of the studies were carried out on a
metabolic ward, but occasionally patients were studied on
the general medical wards. Complete 24-hour urine col-lections were made in refrigerated containers without ad-ditional preservative and were checked for completenessby urinary creatinine determinations.
7-H3-d-aldosterone, 20 ,uc per ,g, was obtained from theEndocrinology Study Section, National Institutes ofHealth, and repurified by chromatography before use. Astandard sterile stock solution, 2 tic per ml, in absoluteethanol was maintained at - 100 C for up to 4 weekswithout significant degradation.
Determination of plasma disappearance rates. Plasmadisappearance of 7-H3-d-aldosterone was determined atthe beginning of the metabolic day (8 a.m.) with patientsin the fasting state. One to 4 usc of the stock solution ofthe labeled hormone was injected through the rubbertubing of a 100-ml infusion of 5 per cent dextrose in waterinto an antecubital vein. Blood samples were obtainedfrom the opposite arm at frequent intervals for 2 hoursafter the injection. The total amount of blood removedfrom any subject did not exceed 80 ml. Plasma was
separated by centrifugation and frozen at -100 C untilit was to be analyzed for 7-H3-aldosterone. The plasmawas then thawed and 45 ,g of unlabeled d-aldosteronewas added to each sample to provide a basis for calcula-tion of losses of steroid during the purification process.
The plasma was extracted with dichloromethane (10vol), and the extract was washed once with 5 per centsodium carbonate (1/10 vol), twice with distilled water(1/10 vol), and taken to dryness under a stream of air.The residue was taken up in ethanol and applied to What-man no. 2 paper and chromatographed in a system ofligroin: methanol: water (4: 3: 1) and again in benzene:methanol: water (4: 2: 1). Aldosterone was located byultraviolet scanning and eluted with methanol. One-tenthof the eluate was used for the quantitation of aldosteroneby means of the alkaline blue tetrazolium reaction; thefigure obtained was used to calculate the recovery cor-
rection. The remainder of the eluate was counted in a
Packard Tri-Carb liquid scintillation spectrometer fortritium. The tritium recovered from this procedure was
considered to represent specifically 7-H3-d-aldosterone,and the concentration was used in plotting the plasmadisappearance curve.
Determination of urinary tetrahydroaldosterone andaldosterone secretion rate. One to 3 ,uc of 7-HW-d-aldos-
terone, 20 IAc per Ag, in ethanol was injected into an ante-cubital vein at the beginning of the metabolic day (8 a.m.).Urine was then collected on ice for the ensuing 24 hours.An aliquot of the urine representing 1/10 to 1/6 total vol-ume was extracted with dichloromethane and hydrolyzedat pH 6.2, 400 C with 75 U per ml of bacterial 8-glucu-ronidase (Sigma) for 12 hours. Fresh enzyme was addedand hydrolysis continued for another 12 hours. Theurine was then extracted with 10 vol ethyl acetate, the ex-tract was washed twice with 1/15 vol 0.1 N NaOH, oncewith 1/10 vol distilled water, once with 1/10 vol 0.1 percent acetic acid, and was then taken to dryness underreduced pressure. The residue was applied to Whatmanno. 2 paper and chromatographed in the Zaffaroni forma-mide: ethylene chloride system at 300 C for 22 to 30 hours.A known quantity of 4-C'4-cortisol was also processed inidentical fashion in order to provide a basis for calculatingsteroid losses during purification. The area correspond-ing to tetrahydroaldosterone (Rcort i so = 0.78) was elutedwith methanol. The methanol and formamide were evapo-rated under reduced pressure at 400 C and the residuedried over calcium chloride in vacuo overnight. Acetyla-tion was then carried out with 0.15 ml acetic anhydridein 0.30 ml pyridine at 300 C for 24 hours. The acetylationwas stopped with ethanol-toluene, the solvents evaporatedunder reduced pressure, and then the residue was appliedto Whatman no. 1 paper together with known quantitiesof desoxycorticosterone acetate (DCA). Chromatographywas then carried out in the system heptane: methanol:water (4: 3: 1) at 300 C for 7 to 9 hours. The area cor-responding to the triacetate of tetrahydroaldosterone(RDCA = 1.07) was eluted. The recovery of DCA indi-cator was used to correct for losses. Aliquots were thentaken for tritium counting in a well-type liquid scintillationcounter and for quantitation by alkaline blue tetrazoliumreaction with DCAas standard. Secretion rate was cal-culated by dividing radioactivity injected by the specificactivity of the tetrahydroaldosterone (11). Because indi-cators were used for correction of losses in each step, thetotal urinary tetrahydroaldosterone could be calculated.
Determination of unaltered ("free") urinary aldosteroneand the 3-ozo-conjugate. Unaltered (free) aldosteronewas determined on a dichloromethane extract of urinewhich had been adjusted to pH 6.0. Aldosterone re-leased from the 3-oxo-conjugate was determined on adichloromethane extract of urine which had been ad-justed to pH 1.0 for 24 hours before extraction by amethod derived from that of Kliman and Peterson (13).
After washing twice with a 1/15 vol of sodium carbo-nate, then once with a 1/10 vol of distilled water, andfinally with a 1/10 vol of 0.1 per cent acetic acid, thedichloromethane was removed under reduced pressure andthe residue applied to Whatman no. 2 paper. Chromatog-raphy was carried out in the system benzene: methanol:water (4: 2: 1) at 300 C for 7 to 9 hours. 4-C14-cortisolwas used an an indicator to determine recovery. Thearea corresponding to aldosterone was eluted (Rcorti.oi =1.4). The eluate was dried and the residue stored overcalcium chloride in vacuo overnight. Acetylation wascarried out using 0.15 ml acetic anhydride in 0.30 ml py-

W. S. COPPAGE, JR., D. P. ISLAND, A. E. COONERAND GRANTW. LIDDLE
1e L ['o!L4DOg
, J NjiRMAL
I
ME(I 24 1H°
L1-..~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~..........,.1.sK43< _ I,~~~~~~~~~.
MEO/24 H '.'--.. ............ ...
h~~~~~~~~~~~~~~nt~--- --i--
2 z 10 14 16
FIG. 1. COMPARISONOF EFFECTS OF ORAL AND INTRA-
MUSCULARADMINISTRATION OF d-ALDOSTERONEIN A NOR-
MAL SUBJECT. d-Aldosterone, 4,000 ,ag, given orally tothis subject on constant metabolic diet failed to modifyurinary electrolyte excretion, whereas 400 /ig intramus-cularly caused a significant decrease in urinary sodiumand increase in urinary potassium.
ridine at 300 C for 24 hours. The acetylation was stoppedwith ethanol-toluene. Aldosterone-C14-diacetate, equiva-lent to approximately 2,000 cpm, was added for the de-termination of recovery in the remainder of the procedure.The ethanol-toluene was removed under reduced pressureand the residue applied to paper. Chromatography was
carried out in the system cyclohexane: benezene: metha-nol: water (4: 2: 4: 1) for 10 hours (aldosterone diacetateRadrenosterone = 1.0) and iso-octane: tertiary butanol:methanol: water (12: 5: 3: 2) for 28 hours (aldosteronediacetate R11-de.oxycortisol = 0.98). The aldosterone diace-tate was eluted and dried. Oxidation was carried outwith 0.2 ml 0.25 per cent chromic trioxide in glacial aceticacid for 5 to 6 minutes. The reaction was stopped with15 per cent ethanol and the resulting solution was ex-
tracted with dichloromethane. The extract was dried un-
der a stream of air and applied to paper. Chromatographywas carried out in the system cyclohexane: benzene:methanol: water (4: 2: 4: 1) for 12 hours at 300 C. Thearea corresponding to the monoacetate of the oxidationproduct (R1i-keto-17a-hydroxyprogefsterone = 0.98) was eluted,dried, and counted for tritium and C14 in a Tri-Carb liquidscintillation spectrometer. The recovery of 4-C14-cortisolin the first chromatography and the recovery of aldos-terone-C14-diacetate in subsequent steps were used tocorrect for losses. Unlabeled aldosterone present in theunaltered (free) and 3-oxo-conjugate fraction was thencalculated from percentage of tritium recovered in eachfraction and the previously determined 24-hour aldos-terone secretion rate.
Urinary sodium and potassium were determined byflame photometry. Urinary creatinine was determinedby the method of Folin as described by Hawk, Oser andSummerson (14).
RESULTS
Comparison of oral versus parenteral administra-tion of d-aldosterone
In order to assess the quantitative role of thehuman liver in the metabolism of aldosterone, the
steroid was administered orally to several sub-jects and both the metabolic effectiveness and themetabolic fate of the steroid were studied. Whenadministered orally in dosage up to 4,000 fg, al-dosterone had no effect upon electrolyte excretionin a subject with normal liver function. Whenad-ministered intramuscularly, however, the steroidhad an obvious sodium-retaining and potassium-losing effect when given in dosage of only 400 jigper day (Figure 1).
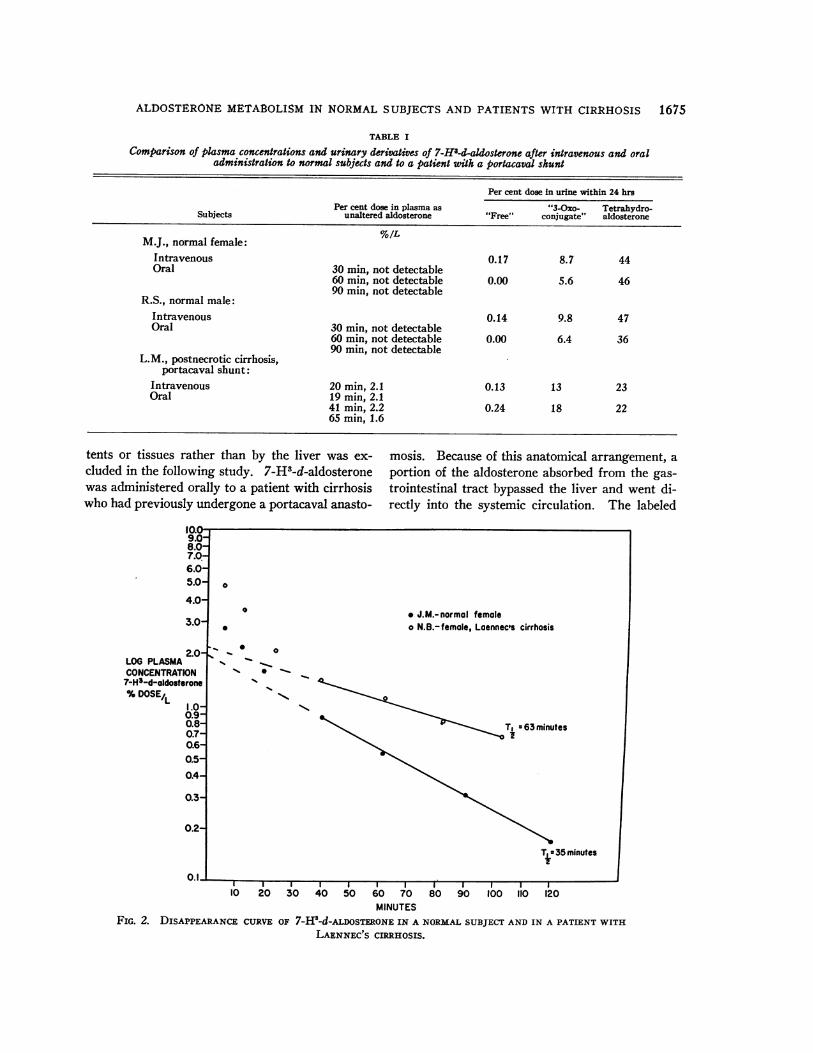
Theoretically, the ineffectiveness of orally ad-ministered aldosterone could be due either to poorabsorption from the gastrointestinal tract or tovirtually complete inactivation of the hormone dur-ing its initial passage through the liver. A seriesof studies was, therefore, performed in which7-H3-d-aldosterone was administered orally. Ab-sorption from the gastrointestinal tract was rapidand complete, as indicated by the appearance oftritium-labeled tetrahydroaldosterone and 3-oxo-conjugate in the urine in quantities comparable tothose observed after the intravenous administrationof 7-H3-d-aldosterone (Table I). After oral ad-ministration of 7-H3-d-aldosterone to a normalsubject, M.J., 46 per cent of the labeled steroid ap-peared in the urine within 24 hours as tetrahydro-aldosterone, whereas after intravenous administra-tion, 44 per cent of the labeled steroid was excretedin this form. After oral administration of the la-beled hormone, 6 per cent appeared in the urineas 3-oxo-conjugate, whereas after intravenous ad-ministration, 9 per cent of the label was excretedin this form. After oral administration of 23 uc of7-H3-d-aldosterone, none of the radioactivity couldbe detected in the blood at 30, 60, or 90 minutes,nor in the urine as unaltered aldosterone. Afterintravenous administration, even though only one-tenth the dosage was used, the unaltered labeledhormone could be measured in the blood for 2hours after the injection and 0.17 per cent of theadministered radioactivity was recovered from theurine as unaltered aldosterone. Similar observa-tions were made in a second normal subject, R.S.It would appear, therefore, that in subjects withnormal liver function virtually no aldosteronereaches the general circulation after oral adminis-tration without having undergone metabolic alter-ation.
The possibility that aldosterone might be metab-olized to a major extent by gastrointestinal con-
1674
1%, [.I'...%; ", "I ") .,.,
p -)
ALDOSTERONEMETABOLISMIN NORMALSUBJECTSAND PATIENTS WITH CIRRHOSIS 1675
TABLE I
Comparison of plasma concentrations and urinary derivatives of 7-H8-d-aldosterone after intravenous and oraladministration to normal subjects and to a patient with a portacaval shunt
Per cent dose in urine within 24 hrs
Per cent dose in plasma as "3-Oxo- Tetrahydro-Subjects unaltered aldosterone "Free" conjugate" aldosterone
M.J., normal female: %/LIntravenous 0.17 8.7 44Oral 30 min, not detectable
60 min, not detectable 0.00 5.6 4690 min, not detectable
R.S., normal male:Intravenous 0.14 9.8 47Oral 30 min, not detectable
60 min, not detectable 0.00 6.4 3690 min, not detectable
L.M., postnecrotic cirrhosis,portacaval shunt:
Intravenous 20 min, 2.1 0.13 13 23Oral 19 min, 2.1
41 min, 2.2 0.24 18 2265 min, 1.6
tents or tissues rather than by the liver was ex-cluded in the following study. 7-H3-d-aldosteronewas administered orally to a patient with cirrhosiswho had previously undergone a portacaval anasto-
mosis. Because of this anatomical arrangement, aportion of the aldosterone absorbed from the gas-trointestinal tract bypassed the liver and went di-rectly into the systemic circulation. The labeled
9.0-8.0-7.0-6.0-5.0-
4.0-
3.0
2.0LOG PLASMACONCENTRATION
7-H3-d-oldosterone%DOSE/L 1.0
0.9-0.8-0.7-0.6-0.5-0.4-
0.3-
0.2-
nA
0
0
* J.M.- normal femaleo N.B.-female, Laennec's cirrhosis
1 0
N-,
T, t63c minutes
T - 35 minutes
I I I I I I I I I I I I10 20 30 40 50 60 70 80 90 100 110 120
MINUTESFIG. 2. DISAPPEARANCECURVE OF 7-HW-d-ALDoSTRoNE IN A NORMALSUBJECTANDIN A PATIENT WITH
LAENNEC'S CIRRHOSIS.
AL

W. S. COPPAGE,JR., D. P. ISLAND, A. E. COONERANDGRANTW. LIDDLE
0oloE~tn%00% 0%%apooOCV)OOOOOCV'1)
N
--- n4-I'4- C' -
CV0%CV0%0%0C'0O0 0%CV) +'00%')tbu.oot'O -0 00o
0 \OW\O+OOMOO-OU4000 0ui 6 d4 4e6 6 v: 06 4 C4C 4
'0 CC4 0 ,I
l 11- W)1) eX-00 m m1 00V-4 C- 4 "- -
*01)1. .*
V*
-%6 us i -u r ; V-
m mUl)'t 10 +
C4 V-4 C0IC 0%0)V~~V 00 ui)c%C'4 " -4 C'- -o -
U)0
1(3
fall0
0
toe
4 '0 '0oooo IC V4oo00 I)oui c0%0000000l1)000%06(:, c oc3
oo01)oo _ 0%0%0% 6s od
0 eq 11)0 -4 I-. 0 - ON~4dSO11) 1) qt 4eV-1 t4 M C4' U..
000 C4)4-006Rm41
cui e-i vi 4o6 c-ieoi 00
r-cC t- ON CInl -4
0%00000N00 IdUId4t 00
C'1 -" W-4 - - C.4 V- CC'4 W-4
\0 1 ) \ 0 .-1'00 1- -
o -o li --o1o0o-oo o
o
o66 6 C 0666 6666666
'00o-4eCV)0% 000% ero sW) + '00o 0%- C4...... CC4 -"
4-4.
'0
0
Ui)
3-
V
U)
CU
CU
¢U)^
U)3 .
0o:X3:~3X
4JC
ocn
-4
0
0
.0
.,
U)
Cd
0
0
'O00 00o It I
NOC14 C1 0 4CV1M) CV)11 11
I.c* o Itm)N m
o40't- 0oI0 0 C9Mo 4 to ~om
ot u ~ c0 4QU t q" kcl 1; -
IC 00
"0 t-. Uro om
C)
u
._
bo o W:E E CrU &4 cU
0
CU
CO~i: 2
u
0~
0
CU
CU
U)
1676
iCUIC
*_ .)4i
Cd
- CI
boo,:
O 0-
-, V
0 '-
Z)-! 25
_ tD
I-,
I-
C,
o
.t .-
C.,
1',o
U;
:10
.V.U)
U)t
4-0
10Cd4NO
0
Q'0la
U)VW*C)
U)4

ALDOSTERONEMETABOLISMIN NORMALSUBJECTSAND PATIENTS WITH CIRRHOSIS 1677
hormone was readily detectable in unaltered formin peripheral venous blood 19, 41, and 65 minutesafter oral administration; 0.24 per cent of the ad-ministered dose also appeared in the urine asunaltered 7-H3-d-aldosterone (Table I). Oral ad-ministration of aldosterone to this patient, there-fore, simulated intravenous injection of the hor-mone.
One may reasonably conclude from these resultsthat there is virtually complete metabolism of al-dosterone to biologically inactive products duringa single passage through the normal liver.
Abnormalities of aldosterone metabolism in pa-tients wtith hepatic cirrhosis
Disappearance of 7-H3-d-aldosterone fromplasma. The intravenous administration of 7-H3-d-aldosterone to normal subjects immediately pro-duced a peak concentration of the labeled hor-mone in the plasma. During the ensuing 30-min-ute period the plasma concentration fell rapidly.Then, from 30 to 120 minutes after the injection,the labeled hormone disappeared more slowlyfrom the plasma at such a rate that the logarithmof the concentration was a rectilinear function oftime (Figure 2). The slope of the latter line wasemployed to define the rate of disappearance of thesteroid from plasma, expressed as the half-time(tj) of circulating aldosterone. In seven normalsubjects the t4 of circulating aldosterone so de-termined ranged from 26 to 39 minutes with amean t4 of 34 minutes (Table II).
In contrast, when 7-H3-d-aldosterone was ad-ministered to six patients with hepatic cirrhosis,the plasma t, of the labeled steroid was prolonged,ranging from 43 to 81 minutes with a mean of 63minutes (Figure 2, Table II). There was nooverlap between the values obtained in normalsubjects and those obtained in patients withcirrhosis.
In the interpretation of the aldosterone disap-pearance curve in patients with fluid accumula-tion, one must consider the possibility that the la-beled hormone might have been sequestered inthe ascitic fluid during mixing, and might thenhave re-entered the plasma at a rate sufficient tocause an apparent delay in plasma disappearance.That such was not the case, however, is indicatedby the fact that the two patients with cirrhosis
but without detectable ascites, Patients L.M. andN.B., also had prolonged aldosterone disappear-ance times. It would appear, therefore, that theprolonged half-time of circulating aldosterone incirrhotic patients is due to liver disease per se andnot to fluid retention.
Urinary excretion of 7-H3-d-aldosterone metab-olites. Three urinary excretion products of aldos-terone were isolated: 1) the free fraction or unal-tered aldosterone, 2) the so-called 3-oxo-conju-gate, and 3) tetrahydroaldosterone.
After the intravenous administration of 7-H13-d-aldosterone, only a minute fraction of the labeledsteroid was found as unaltered aldosterone in theurine of normal or cirrhotic subjects (Table II).In two normal subjects on liberal sodium intake,0.14 and 0.17 per cent of the dose was recoveredas unaltered hormone. One normal subject onlow sodium diet excreted 0.14 per cent in this form.The unaltered fraction in seven patients with cir-rhosis was slightly higher and ranged from 0.08to 0.8 per cent of the injected dose with a meanof 0.25 per cent.
There was a clear difference between normalsubjects and patients with hepatic cirrhosis in theamount of the labeled steroid excreted as the 3-oxo-conjugate and as tetrahydroaldosterone (Figure3). Whereas 16 normal subjects excreted, on theaverage, 8.9 per cent of the administered dose asthe 3-oxo-conjugate, the 9 cirrhotic patients ex-creted 15.8 per cent of the labeled hormone in thisform. On the other hand, the normal subjectsexcreted, on the average, 41 per cent of the doseas tetrahydroaldosterone, whereas the patients withcirrhosis excreted only 29 per cent in this form.
The rate of aldosterone secretion. The rate ofsecretion of aldosterone, as calculated from thespecific activity of urinary tetrahydroaldosterone,was determined for normal subjects on a liberalsodium intake, for normal subjects on restrictedsodium diets, and for patients with hepatic cir-rhosis (Table II). In 15 normal subjects on anunrestricted diet, aldosterone secretion rate rangedfrom 95 to 249 jug per day. In 4 normal subjectson a low sodium diet, the aldosterone secretion rateranged from 284 to 528 pg per day. Ten deter-minations of aldosterone secretion rate in 9 cir-rhotic patients yielded values ranging from 248 to2,080 ug per 24 hours. The high rate of aldoster-

W. S. COPPAGE,JR., D. P. ISLAND, A. E. COONERAND GRANTW. LIDDLE
50
% INJECTED 40
7- H3- D-ALDOSTERONE
RECOVEREDIN
URINE
24HRS.
30-
20'
LEGEND:* NORMAL,LIBERAL No+o NORMAL, LOWNotx CIRRHOSIS- MEAN
10'
NORMAL C
FIG. 3. COMPARISONOF THE PER CENT TRACER DOSE OF
AS TETRAHYDROALDOSTERONEIN THE URINE IN 24 HOURS
CIRRHOSIS.
;IRRHOSIS NORMAL CIRRHOSIS7-H3-d-ALDOSTERONE RECOVEREDAS 3-OXO-CONJUGATEAND
IN NORMALSUBJECTS AND IN PATIENTS WITH HEPATIC
one secretion in the cirrhotic patients probably didnot represent the effect of liver damage alone, sincemost of these patients were on low sodium dietsat the time of study.
Since the rate of aldosterone secretion was
elevated in the patients with hepatic cirrhosis, itseemed pertinent to inquire whether the rate ofaldosterone secretion would itself modify theplasma disappearance of 7-H3-d-aldosterone or
the pattern of urinary excretion of metabolites.That an increase in aldosterone secretion ratedoes not of itself result in prolongation of theplasma t4 of aldosterone becomes apparent fromexamination of Table II. In R.A., a normal sub-ject whose aldosterone secretion was elevated to528 jug per 24 hours by dietary sodium restriction,the plasma tj of 34 minutes did not differ fromthose of other normal subjects with comparativelylow aldosterone secretion rates. The proportionof labeled hormone excreted as the 3-oxo-conju-gate or as tetrahydroaldosterone was approxi-mately the same for the 4 normal subjects with
high aldosterone secretion rates owing to dietarysodium restriction as it was for the 12 normalsubjects with low aldosterone secretion rates.The delayed plasma disappearance of 7-H3-d-al-dosterone and the altered pattern of excretion ofurinary metabolites in patients with cirrhosis,therefore, is to be attributed to the presence ofhepatic disease and not to the increased rate ofsecretion of aldosterone.
DISCUSSION
In contrast to cortisol, which in trace amountshas a plasma tj of 60 to 90 minutes in normal sub-jects (15), aldosterone has a relatively short to.The average aldosterone tj of 34 minutes observedin the present study is almost identical with thatfound by Tait, Tait, Little and Laumas (16).The rate of plasma clearance of aldosterone is, likethat of cortisol, slower in the presence of hepaticcirrhosis. Peterson (3) has reported a prolongedplasma tj of tritiated aldosterone in one of twopatients with hepatic cirrhosis studied.
1678
" 3 -OXO- CONJUGATE"i TETRAHYDROALDOSTERONE
.0
0@
00
x
x
* ~~~~xX
x XX
xXXx
XX
00 ~~~~x

ALDOSTERONEMETABOLISMIN NORMALSUBJECTSAND PATIENTS WITH CIRRHOSIS 1679
The present study confirms that of Hurter andNabarro (12) in demonstrating an increase in the3-oxo-conjugate: tetrahydroaldosterone ratio in pa-tients with cirrhosis. It is possible that the re-duction of ring A is a rate-limiting step in themetabolism of aldosterone and that this process isimpaired in patients with cirrhosis. Consequently,more of the aldosterone might be metabolized tothe 3-oxo-conjugate, a process which does not re-quire ring A reduction. On the other hand, Jonesand associates (17) have demonstrated a similarincrease in the 3-oxo-conjugate: tetrahydroaldos-terone ratio in pregnancy, a condition in whichplasma aldosterone tj is not prolonged (18). Itmust be conceded, therefore, that in cirrhosis theprecise relationship between the prolongation ofplasma aldosterone t1 and the shift in metabolicfate of the hormone remains speculative.
The demonstration of the relative ineffectivenessof orally administered aldosterone is in accordwith the results of previous studies (19, 20). Theuse of the tritiated steroid in the present work,however, has demonstrated that the lack of effectis not due to poor absorption, since labeled metabo-lites quickly appear in the plasma and urine. Theappearance of free aldosterone in the plasma andurine of the patient with a portacaval shunt indi-cates that it is the liver rather than the gastro-intestinal tract which inactivates the hormone.
Both of the major metabolites of aldosteroneappear to be formed in the liver, since none of theorally administered hormone escaped unaltered inits passage through the liver and since the quan-tities of 3-oxo-conjugate and tetrahydroaldosteronewhich appeared in the urine after oral administra-tion were comparable to those observed after in-travenous administration of the labeled hormone.That aldosterone is virtually all metabolized on asingle passage through the normal liver, whereascortisol is not, offers at least a partial explanationfor the observation that the plasma half-time ofaldosterone is considerably shorter than that ofcortisol.
The high levels of urinary "aldosterone" (freeplus 3-oxo-conjugate) which have been demon-strated in hepatic cirrhosis are due to three fac-tors: increased aldosterone secretion, decreasedrate of metabolism of aldosterone, and excretion ofa greater proportion as the 3-oxo-conjugate,
which, although inactive in itself, is converted tobiologically active aldosterone by acid hydrolysis.
SUMMARY
1. The oral administration of aldosterone is in-effective in man because of rapid metabolism ofthe hormone during a single passage through theliver.
2. Both of the major urinary metabolites ofaldosterone, 3-oxo-conjugate and tetrahydroal-dosterone, are formed in the liver.
3. The rate of removal of labeled aldosteronefrom the plasma is prolonged in patients with he-patic cirrhosis.
4. In hepatic cirrhosis there is an increase in theproportion of aldosterone which is metabolized tothe 3-oxo-conjugate and a decrease in the pro-portion which is converted to tetrahydroaldos-terone.
REFERENCES
1. Schneider, J. J., and Horstmann, P. M. Effects ofincubating compound E and related steroids withvarious surviving rat tissues. J. biol. Chem. 1952,196, 629.
2. Hechter, O., Frank, E., Caspi, E., and Frank, H.Corticosteroid metabolism in liver: In vivo me-tabolism of cortisone and cortisol by dog liver.Endocrinology 1957, 60, 705.
3. Peterson, R. E. Adrenocortical steroid metabolismand adrenal cortical function in liver disease. J.clin. Invest. 1960, 39, 320.
4. Chart, J. J., Gordon, E. S., Helmer, P., and LeSher,M. Metabolism of salt-retaining hormone by sur-viving liver slices. J. clin. Invest. 1956, 35, 254.
5. Yates, F. E., Urquhart, J., and Herbst, A. L. Im-pairment of the enzymatic inactivation of adrenalcortical hormones following passive venous con-gestion of the liver. Amer. J. Physiol. 1958, 194,65.
6. Ayers, C. R., Davis, J. O., Liebermann, F., and Car-penter, C. C. J. Effects of chronic hepatic venouscongestion on the disappearance of tritiated aldos-terone from plasma. Endocrine Soc. Abstr. 1960,42, 17.
7. Axelrad, B. J., Cates, J. E., Johnson, B. B., andLuetscher, J. A., Jr. Aldosterone in urine of nor-mal men and of patients with oedema. Its in-creased recovery after hydrolysis with acid andwith beta-glucuronidase. Brit. med. J. 1955, 1,196.
8. Dyrenfurth, I., Stacey, C. H., Beck, J. C., and Ven-ning, E. H. Aldosterone excretion in patients withcirrhosis of the liver. Metabolism 1957, 6, 544.
W. S. COPPAGE,JR., D. P. ISLAND, A. E. COONERANDGRANTW. LIDDLE
9. Ulick, S., Kusch, K., and August, J. T. Correctionof the structure of a urinary metabolite of aldos-terone. J. Amer. chem. Soc. 1961, 83, 4482.
10. Ulick, S., and Lieberman, S. Evidence for the oc-currence of a metabolite of aldosterone in urine.J. Amer. chem. Soc. 1957, 79, 6567.
11. Ulick, S., Laragh, J. H., and Lieberman, S. Theisolation of a urinary metabolite of aldosteroneand its use to measure the rate of secretion ofaldosterone by the adrenal cortex of man. Trans.Ass. Amer. Phycns 1958, 71, 225.
12. Hurter, R., and Nabarro, J. D. N. Aldosterone me-tabolism in liver disease. Acta endocr. (Kbh.)1960, 33, 168.
13. Kliman, B., and Peterson, R. Double isotope deriva-tive assay of aldosterone in biological extracts.J. biol. Chem. 1960, 235, 1639.
14. Hawk, P. B., Oser, B. L., and Summerson, W. H.Practical Physiological Chemistry, 12th ed. Phila-delphia, Blakiston, 1947, p. 839.
15. Peterson, R. E., Wyngaarden, J. B., Guerra, S. L.,Brodie, B. B., and Bunim, J. J. The physiologicaldisposition and metabolic fate of hydrocortisone inman. J. clin. Invest. 1955, 34, 1779.
16. Tait, J. F., Tait, S. A. S., Little, B., and Laumas,K. R. The disappearance of 7-H3-d-aldosterone inthe plasma of normal subjects. J. clin. Invest. 1961,40, 72.
17. Jones, K M., Lloyd-Jones, R., Riondel, A., Tait, J.F., Tait, S. A. S., Bulbrook, R. D., and Green-wood, F. C. Aldosterone secretion and metabolismin normal men and women and in pregnancy.Acta endocr. (Kbh.) 1959, 30, 321.
18. Layne, D. S., Little, B., Meyer, C. J., Tait, J. F., andTait, S. A. S. The turnover rate, distribution, andplasma binding of aldosterone in pregnancy. En-docr. Soc. Abstr. 1961, 43, 16.
19. Thorn, G. W., Sheppard, R. H., Morse, W. I., Reddy,W. J., Beigelman, P. M., and Renold, A. E.Comparative action of aldosterone and 9-alpha-fluorohydrocortisone in man. Ann. N. Y. Acad.Sci. 1955, 61, 609.
20. Ledingham, J. G. G., Martin, F. I. R., Moxham, A.,Hurter, R., and Nabarro, J. D. N. The metaboliceffects of aldosterone given by mouth. Lancet1961, 1, 630.
1680