key question # 4: what other tools are needed to support
TRANSCRIPT

Analysis. Answers. Action. www.aphl.org
Key Question # 4: What other tools are needed to support same-day diagnosis and treatment of current HCV infection?
Moderator John Ward, Task Force for Global Health
Presenter Ray Chung, Mass General Hospital
Panelists Marc Ghany, NIDDKJorge Mera, Cherokee Nation HS Benjamin Pinsky, Stanford Health

Analysis. Answers. Action. www.aphl.org
Disclosures
• John Ward –• Ray Chung – Abbvie, Gilead, Merck, BMS, Janssen,
Boehringer, Roche (research grants to institution)• Jorge Mera – institution receives grant funding from
Abbvie• Marc Ghany – nothing to disclose• Benjamin Pinsky - nothing to disclose
Analysis. Answers. Action. www.aphl.org
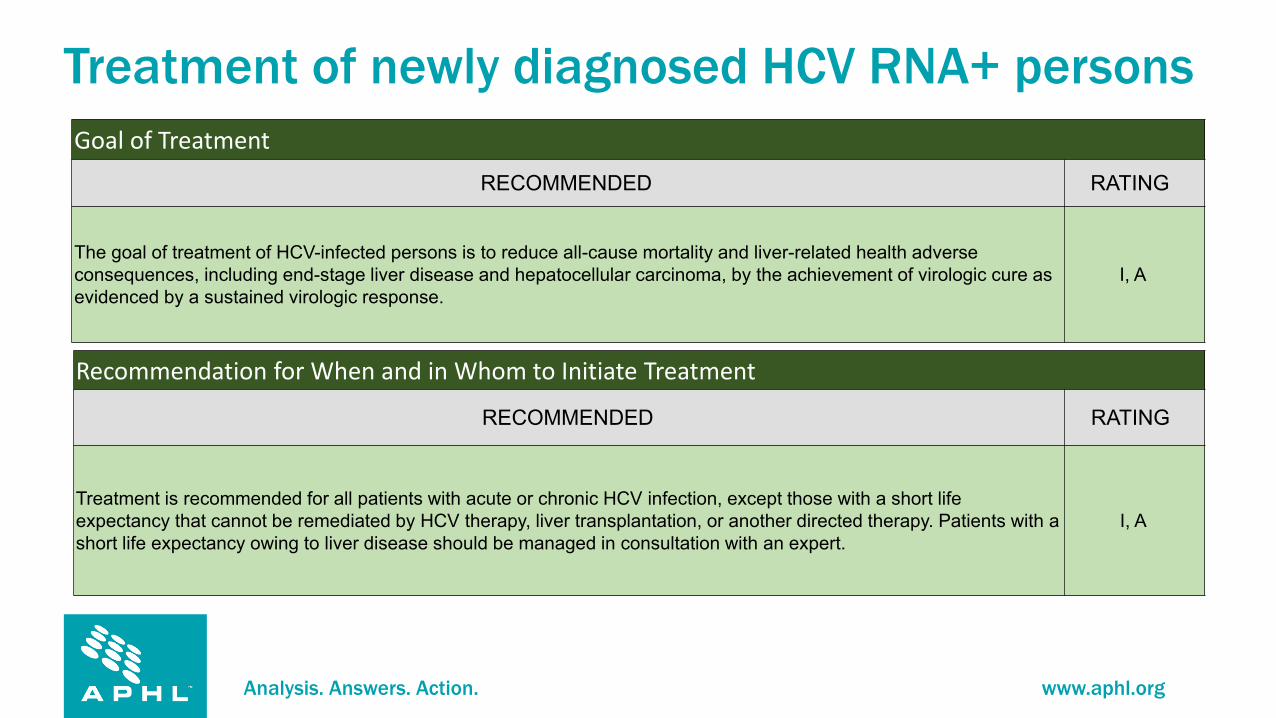
Treatment of newly diagnosed HCV RNA+ personsGoal of Treatment
RECOMMENDED RATING
The goal of treatment of HCV-infected persons is to reduce all-cause mortality and liver-related health adverse consequences, including end-stage liver disease and hepatocellular carcinoma, by the achievement of virologic cure as evidenced by a sustained virologic response.
I, A
Recommendation for When and in Whom to Initiate Treatment
RECOMMENDED RATING
Treatment is recommended for all patients with acute or chronic HCV infection, except those with a short life expectancy that cannot be remediated by HCV therapy, liver transplantation, or another directed therapy. Patients with a short life expectancy owing to liver disease should be managed in consultation with an expert.
I, A
Analysis. Answers. Action. www.aphl.org
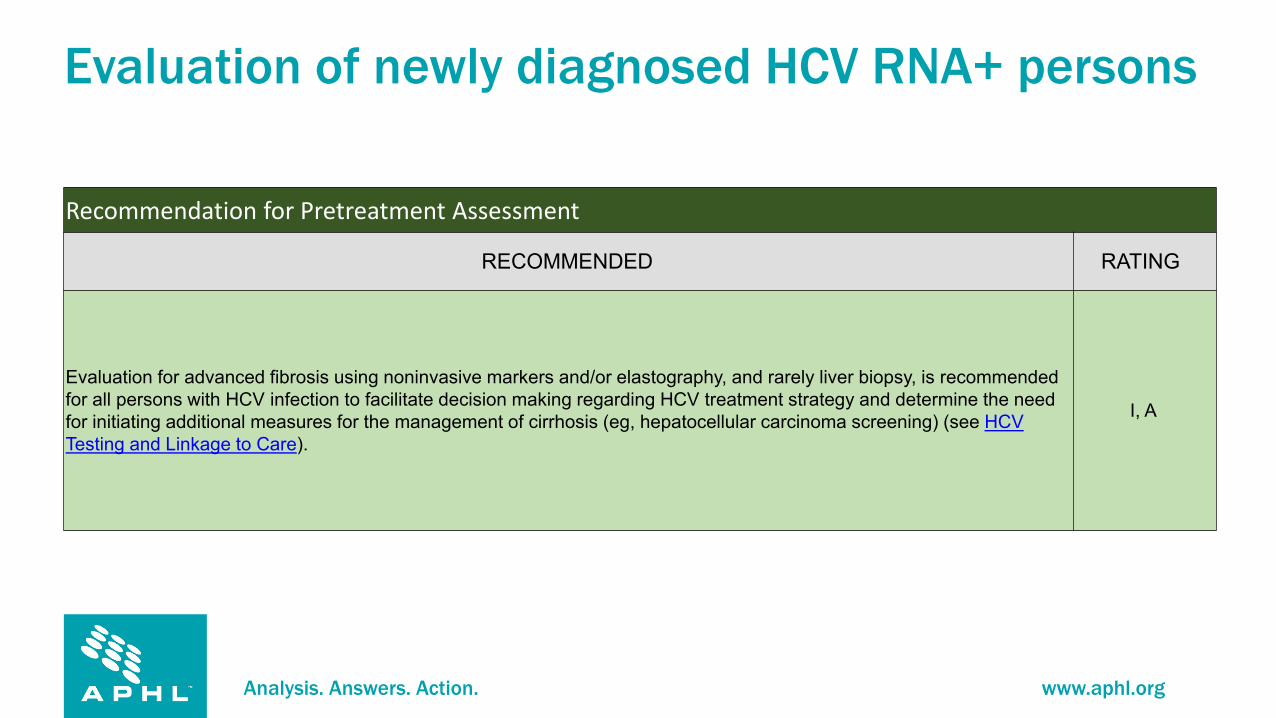
Evaluation of newly diagnosed HCV RNA+ persons
Recommendation for Pretreatment Assessment
RECOMMENDED RATING
Evaluation for advanced fibrosis using noninvasive markers and/or elastography, and rarely liver biopsy, is recommended for all persons with HCV infection to facilitate decision making regarding HCV treatment strategy and determine the need for initiating additional measures for the management of cirrhosis (eg, hepatocellular carcinoma screening) (see HCV Testing and Linkage to Care).
I, A
Analysis. Answers. Action. www.aphl.org
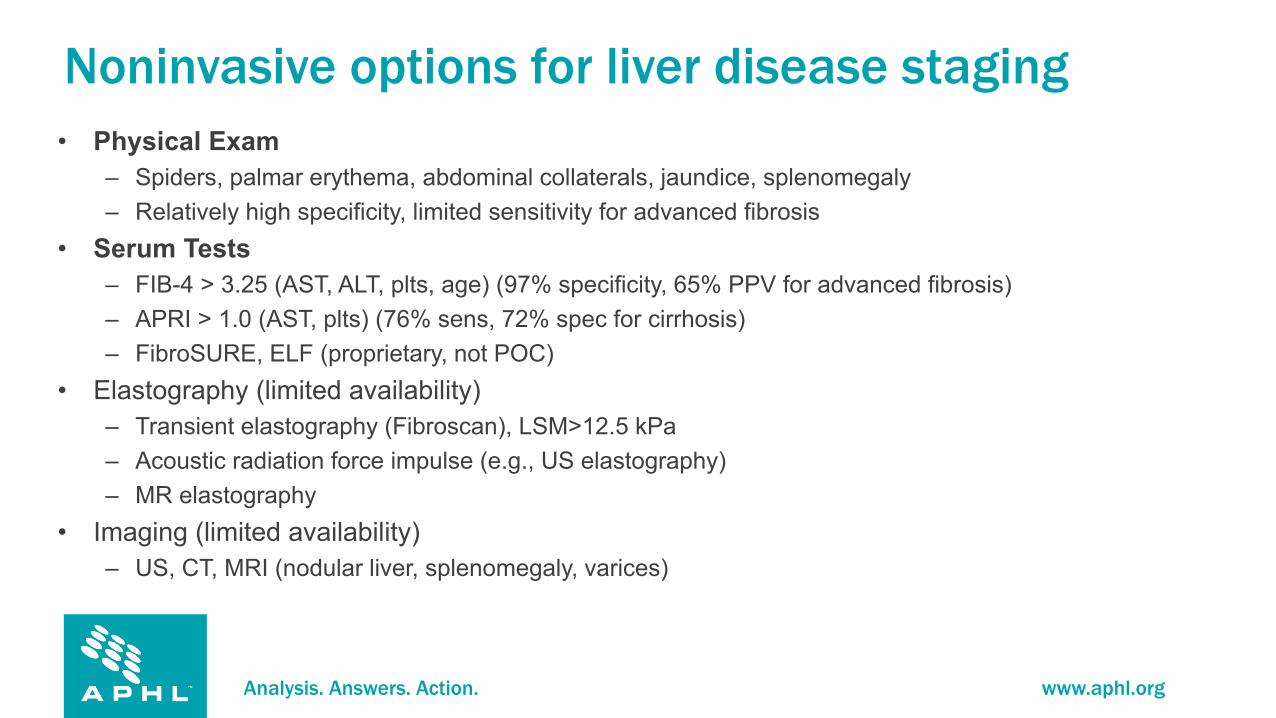
Noninvasive options for liver disease staging• Physical Exam
– Spiders, palmar erythema, abdominal collaterals, jaundice, splenomegaly – Relatively high specificity, limited sensitivity for advanced fibrosis
• Serum Tests– FIB-4 > 3.25 (AST, ALT, plts, age) (97% specificity, 65% PPV for advanced fibrosis) – APRI > 1.0 (AST, plts) (76% sens, 72% spec for cirrhosis)– FibroSURE, ELF (proprietary, not POC)
• Elastography (limited availability)– Transient elastography (Fibroscan), LSM>12.5 kPa– Acoustic radiation force impulse (e.g., US elastography)– MR elastography
• Imaging (limited availability)– US, CT, MRI (nodular liver, splenomegaly, varices)

Analysis. Answers. Action. www.aphl.org
Implications for identification of cirrhosis• Need for linkage to care – distinction between infection and
disease • No meaningful impact on selection or duration of regimen
(assuming pangenotypic regimen available)– Gt 3 cirrhosis RAS testing for SOF/VEL
• Screening for portal hypertension– Endoscopy for varices
• Screening for HCC– Imaging semiannually

Analysis. Answers. Action. www.aphl.org
Additional Pre-treatment Assessments (AASLD-IDSA HCV Guidance)• Assessment of potential drug-drug interactions (AASLD-IDSA HCV Guidance)• Pregnancy status• HCV RNA• Hepatic function panel (i.e., serum albumin, total and direct bilirubin, alanine aminotransferase
[ALT], aspartate aminotransferase [AST], and alkaline phosphatase levels)• eGFR• All patients initiating DAA therapy should be assessed for active hepatitis B virus (HBV) coinfection
with HBV surface antigen (HBsAg) testing, and for evidence of prior infection with HBV core antibody (anti-HBc) and HBV surface antibody (anti-HBs) testing.
– HBsAg at POC could suffice– Importance of preventing HBV reactivation in HBV-HCV coinfected persons (shared routes of transmission)
• All patients should be assessed for HIV coinfection prior to initiating DAA therapy (linkage to care, initiation of ART)

Analysis. Answers. Action. www.aphl.org
HCV POC assays
• Only one FDA cleared, CLIA-waived HCV Ab test (venipuncture, fingerstick)
• No HCV NAT or Ag POC
Analysis. Answers. Action. www.aphl.org
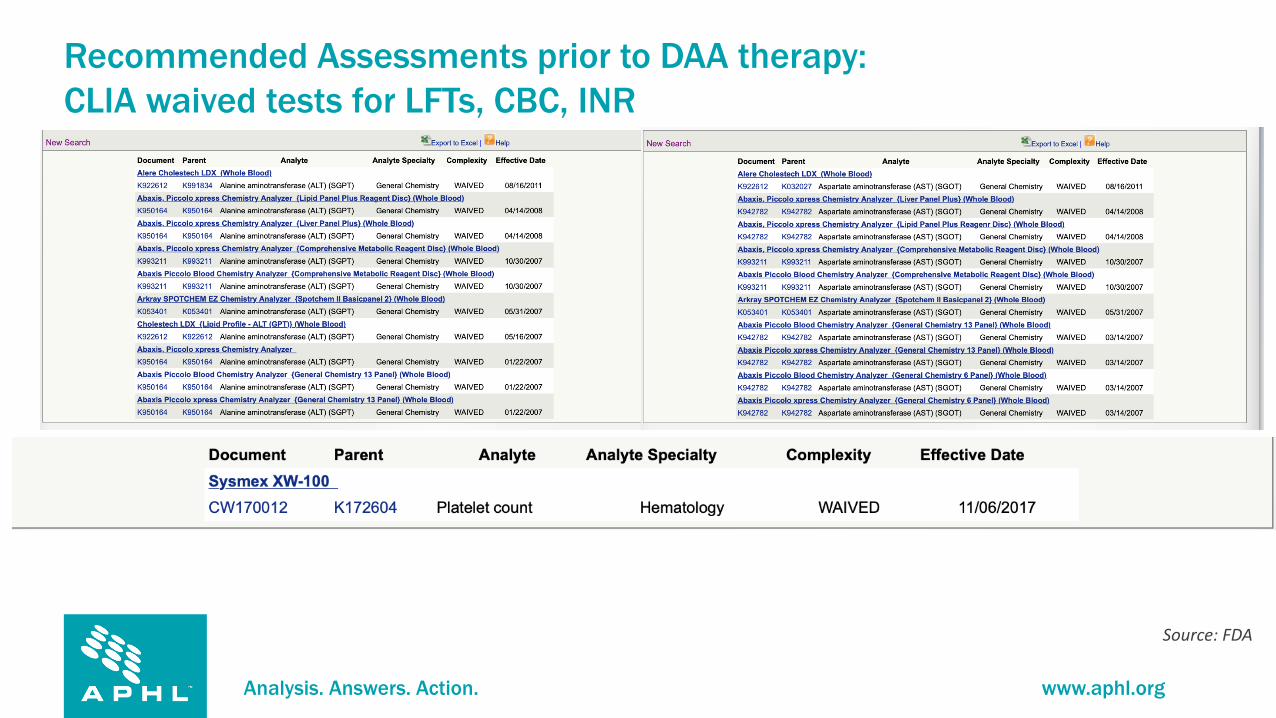
Recommended Assessments prior to DAA therapy:CLIA waived tests for LFTs, CBC, INR
Source: FDA
Analysis. Answers. Action. www.aphl.org
Recommended Assessments prior to DAA therapy• HBsAg POC
– Determine(TM) HBsAg 2 test (Abbott) is PoC, 15 min test, serum/plasma/WB
– CE mark obtained– Submitted for WHO prequalification– 2 other assays meet WHO prequalification (VIKIA HBsAg, SD Bioline)– Not yet FDA cleared
• HIV POC tests – Chembio, Clearview, Orgenics, bioLytical, OraSure (fingerstick, venous, or
oral)
Analysis. Answers. Action. www.aphl.org
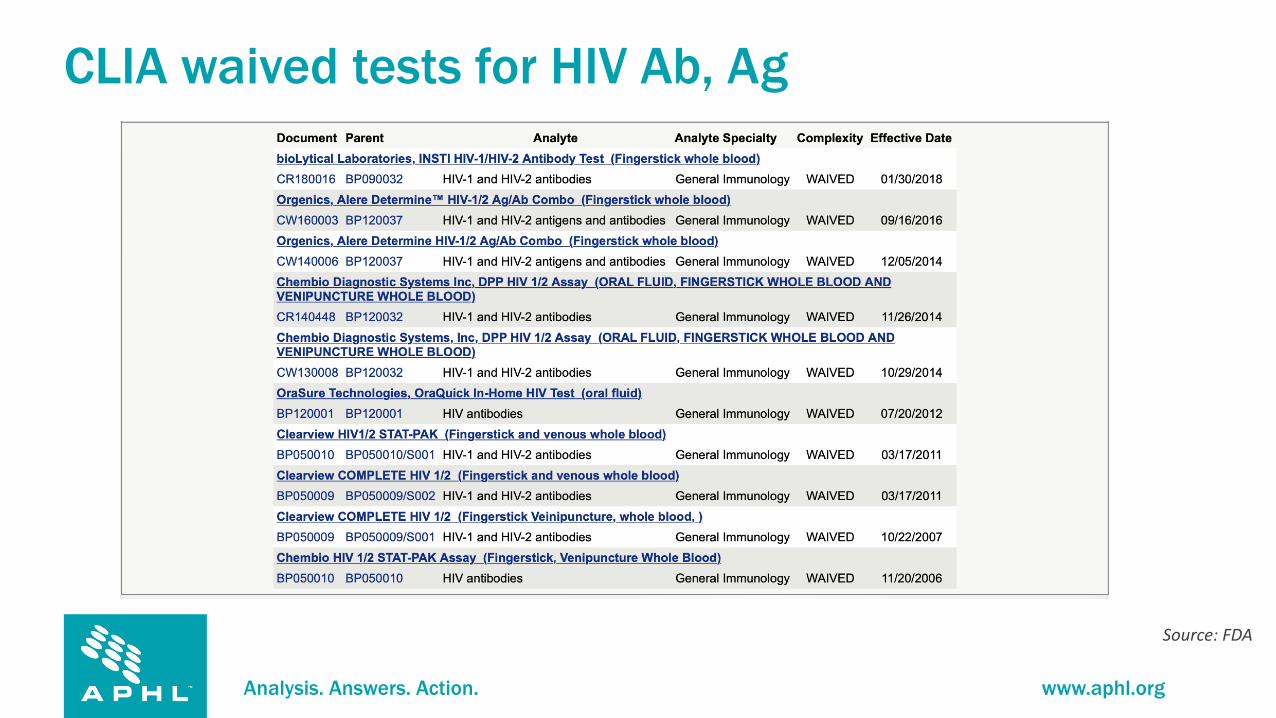
CLIA waived tests for HIV Ab, Ag
Source: FDA

Analysis. Answers. Action. www.aphl.org
Other considerations
• Acute HCV– Usually marked elevations of ALT, AST, +/- Tbili– Alters ability to interpret serum markers of fibrosis,
elastography– Some data for briefer regimens of DAAs, but current
recommendation remains identical to chronic HCV

Analysis. Answers. Action. www.aphl.org
Obstacles to same day treatment• Payer requirement for prior approval
– Cost of pangenotypic regimens (WAC $26,000 for 8-week course but variable negotiated rates)
– Often requirement for additional information (e.g., genotype, disease stage)
– Medicaid: subspecialist (18 states) or sobriety (13 states) requirement• Needed – preapproved regimens
– Take-homes at high incidence or remote sites
Stateofhepc.org, NVHR
Analysis. Answers. Action. www.aphl.org
Settings for implementation• SUD treatment facilities• Correctional facilities• Syringe service programs• Mobile treatment facilities• Primary care settings encountering high risk behaviors• Inpatient settings or EDs – consequences of IDU
– Order sets with available DAAs• Obstetrics wards (defer therapy for now)• Opportunity for contact tracing with POC HCV NAT• Brief window of opportunity!
Analysis. Answers. Action. www.aphl.org
One shot at making a difference
• Linkage to care– SUD, harm reduction services
• Feasibility of minimal monitoring– Can we get away without on treatment monitoring? SVR12?– Smartphone adherence checks– Patient navigator (high risk groups – HERO trial)
• One and done – test and treat– LAI therapy (cf. HIV ARV LAI – Cabotegravir/rilpivirine)

Analysis. Answers. Action. www.aphl.org
Design of MINMON intervention
Solomon SS for A5360 team; CROI 2021, Abstract 135
Week 0 4 8 12 16 20 2422
1. 396 pts across 4 continents2. No pre-treatment genotyping3. All 84 tablets of SOF/VEL dispensed at entry4. No scheduled on-treatment clinic/labs5. Remote contact at Weeks 4 and 226. 95% SVR
SVR

Analysis. Answers. Action. www.aphl.org
What about a one size fits all test? FDA-cleared Multiplex NAT assays for HIV, HBV, HCV (Donor Organs)
COBAS TaqScreen MPX Test version 2.0
HBV, HCV, HIV-1, HIV-2 PCR Plasma Donor Screening: Simultaneous qualitative detection of HBV DNA, HIV-1 Group M and Group O RNA, HIV-2 RNA, and HCV RNA
Roche Molecular Systems, Inc.Pleasanton, CAUS License 1636
12/19/20149/21/2017
BL125459BL125459/22
COBAS TaqScreen MPX Test HBV, HCV, HIV-1, HIV-2 PCR Plasma/ Cadaveric plasma or serum
Donor Screening: Simultaneous qualitative detection of HBV DNA, HIV-1 Group M and Group O RNA, HIV-2 RNA, and HCV RNA.
Roche Molecular Systems, Inc.Pleasanton, CAUS License 1636
12/30/2008 BL125255
cobas MPX Test HBV, HCV, HIV-1, HIV-2 PCR Plasma/ Cadaveric plasma or serum
Donor Screening: Simultaneous qualitative detection of HBV DNA, HIV-1 Group M and Group O RNA, HIV-2 RNA, and HCV RNA.
Roche Molecular Systems, Inc.Pleasanton, CAUS License 1636
10/21/20169/21/2017
BL125576BL125576/11
Procleix Ultrio Elite Assay HBV, HCV, HIV-1, HIV-2 Nucleic Acid Test (TMA) Plasma/ Serum/ Cadaveric plasma or serum
Donor Screening: Simultaneous qualitative detection of HBV DNA, HCV RNA, HIV-1 RNA and HIV-2 RNA.
Grifols Diagnostics Solution.,San Diego, CAUS License 2032
5/03/2018 BL125652
Procleix Ultrio Assay HBV, HCV, HIV-1 Nucleic Acid Test (TMA Plasma/ Serum/ Cadaveric plasma or serum
Donor Screening: Simultaneous qualitative detection of HBV DNA, HCV RNA, and HIV-1 RNA.
Grifols Diagnostics Solution.,San Diego, CAUS License 2032
10/3/2006 BL125113
Procleix Ultrio Plus Assay HBV, HCV, HIV-1 Nucleic Acid Test (TMA) Plasma/ Serum/ Cadaveric plasma or serum
Donor Screening: Simultaneous qualitative detection of HBV DNA, HCV RNA, and HIV-1 RNA.
Grifols Diagnostics Solution.,San Diego, CAUS License 2032
5/25/2012 BL125113
UltraQual Multiplex PCR Assay HBV, HCV, HIV-1, HIV-2 Nucleic Acid Test (PCR) Plasma Source Plasma Donor Screening: Simultaneous qualitative detection of HBV DNA, HCV RNA, HIV-1 RNA and HIV-2 RNA.
National Genetics InstituteLos Angeles, CAUS License 1582
5/30/2018 BL125658
Analysis. Answers. Action. www.aphl.org
What additional tools are needed for same day diagnosis and treatment?• Cheaper screening tests (value of competition - downclassification)• POC HCV NAT (or cAg), HBsAg testing • POC multiplex HCV/HBV/HIV NAT testing• Access to elastography and other technologies• Expedited DAA approval or DAA stockpiles • Treatment navigators
Analysis. Answers. Action. www.aphl.org
What needs approval in the US?
• POC HCV NAT (or cAg) testing• POC HBsAg testing• POC multiplex HIV/HBV/HCV NAT testing• Long acting injectable DAAs (high risk for loss to f/u,
nonadherence)
Analysis. Answers. Action. www.aphl.org
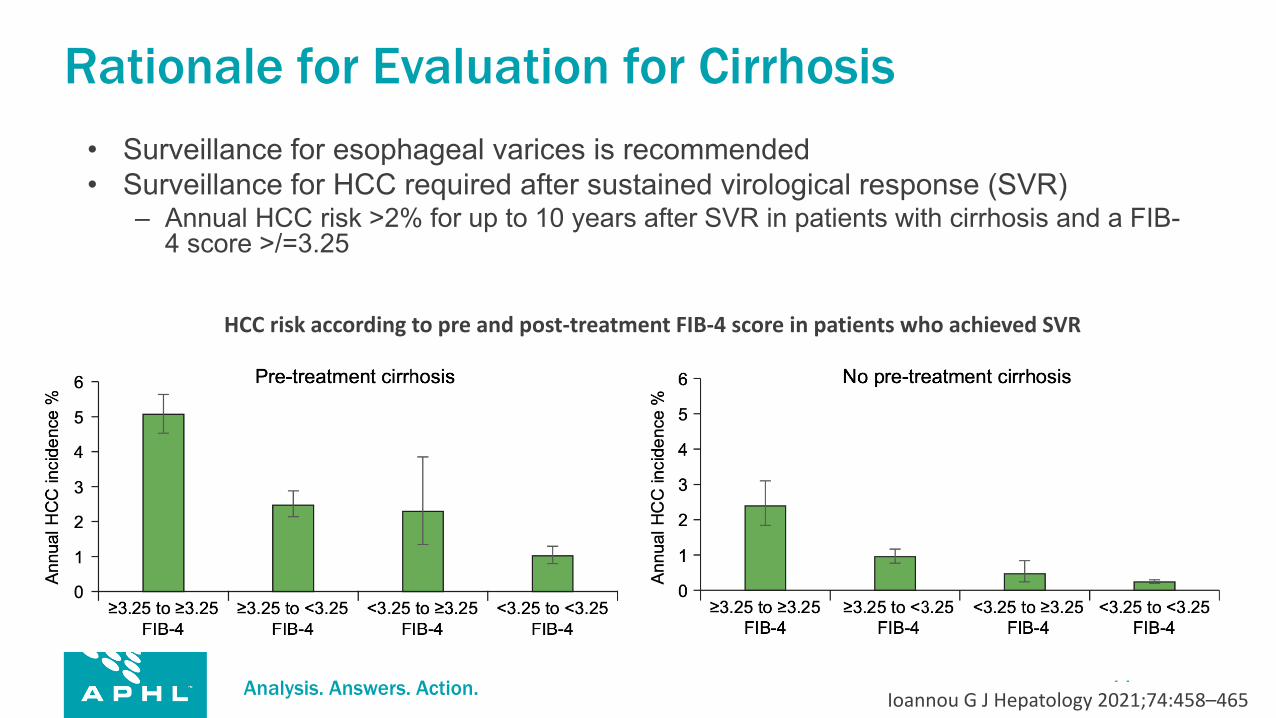
Rationale for Evaluation for Cirrhosis• Surveillance for esophageal varices is recommended• Surveillance for HCC required after sustained virological response (SVR)
– Annual HCC risk >2% for up to 10 years after SVR in patients with cirrhosis and a FIB-4 score >/=3.25
Ioannou G J Hepatology 2021;74:458–465
HCC risk according to pre and post-treatment FIB-4 score in patients who achieved SVR

Analysis. Answers. Action. www.aphl.org
Diagnose and Treat AlgorithmPOC Testing
RNA Negative RNA Positive
HBsAg+ HBsAg-
CBCHepatic panelAnti-HIVSerum pregnancy test
Repeat HCV RNA 12 weeks post treatment
Pangenotypic regimen for 8 or 12 weeksPatient navigator support if needed
Refer to specialist
No treatment indicated
Evaluate for cirrhosis
Present Absent
Treatment naiveDAA Treatment experienced

Analysis. Answers. Action. www.aphl.org
Possible Impact of Lack of POC HCV RNA in HCV Cascade of Care GAPS
Percentages for 715 hepatitis C virus (HCV) antibody-positive patients, showing cascade of care — Cherokee Nation Health Services, October 2012–July 2015
68%
57%• HCV antibody detected but
patient lost to follow-up for HCV RNA testing
• Reflex RNA not available in most rural areas
GAP 32 %
• Patients lost to follow-up
GAP 43 %Identification and Clinical Management of Persons with Chronic Hepatitis C Virus Infection — Cherokee Nation, 2012–2015. MMWR Morb Mortal Wkly Rep 2016;65:461–466.