key terms* - coursewareobjects.com terms* advance beneficiary notice (abn) approved charges...
TRANSCRIPT
K E Y T E R M S *
Advance Beneficiary Notice (ABN)approved chargesassignmentbenefit periodCenters for Medicare and
Medicaid Services (CMS)Correct Coding Initiative (CCI)crossover claimdiagnostic cost groups (DCGs)disabledend-stage renal disease (ESRD)fiscal intermediary (FI)formularyhospicehospital insuranceintermediate care facilities (ICFs)limiting chargemedical necessity
MedicareMedicare administrative
contractor (MAC)Medicare Part AMedicare Part BMedicare Part CMedicare Part DMedicare/Medicaid (Medi-Medi)Medicare Secondary Payer (MSP)Medicare summary notice (MSN)Medigap (MG)national alphanumeric codesnonparticipating physician
(nonpar)nursing facility (NF)participating physician (par)Physician Quality Reporting
Initiative (PQRI)
premiumprospective payment system (PPS)Quality Improvement
Organization (QIO)qui tam actionreasonable feerelative value unit (RVU)remittance advice (RA)resource-based relative value
scale (RBRVS)respite careSupplemental Security
Income (SSI)supplementary medical
insurance (SMI)volume performance
standard (VPS)whistleblowers
ABNCAPCLIACMSCCICOBRADCDCGsDDSDEFRADMEDODPMEGHPEOBERAESRD
FIGPCIHCPCSHMOICFsICULCDLGHPLMRPMAACMACMCOMDMedi-MediMGMMAMSA
MSNMSPNCDsNEMBNFnonpar physicianNPIOASDIOBRAOCNAOIGORpar physicianPAYRIDPFFS planPINPOS plan
PPOPQRIPROPPSPSOQIORARBRVSRFBSRVUSOFSSISMITEFRAUPINVAVPS
K E Y A B B R E V I AT I O N S *
*Definitions for the key terms and key abbreviations are located near the back of this textbook in the Glossary section.
X3666-Ch12 8/27/07 4:55 PM Page 432

C H A P T E R
12Medicare
● Explain eligibility criteria for Medicare.
● Name important information to abstract from apatient’s Medicare card.
● Identify the benefits and nonbenefits of Medicare.
● List the federal laws adopted to increase healthbenefits for employed workers and the elderly.
● Name the conditions when an HMO-Medicarepatient can be seen by a nonmember HMOphysician.
● Differentiate between an HMO risk plan and anHMO cost plan.
● Name the federal laws that relate to costcontainment of health services and to reduction offraud and abuse issues.
● Explain when to obtain a patient’s signature on anAdvance Beneficiary Notice or waiver of liabilityagreement.
● Define a Medicare-mandated prepayment screen.
● State the benefits for a participating versusnonparticipating physician.
● Calculate a payment for a procedure using thecurrent conversion factor.
● List situations for using an annual beneficiary claimauthorization and information release document.
● Determine the time limit requirements fortransmitting a Medicare claim.
● Explain claims submission for individuals who haveMedicare with other insurance.
● List CMS-1500 (08-05) block numbers thatrequire Medigap information when transmitting aMedicare/Medigap claim.
● Post information on the patient’s financialaccounting record after a Medicare payment hasbeen received.
O B J E C T I V E S
After reading this chapter, you should be able to:
The Insurance Handbook Evolve Site
The Insurance Handbook Student Workbook
The Insurance Handbook Workbook CD
Performance objectives, testing and review material, and hands-on practical exercises for this chapter are available in these resources
433
X3666-Ch12 8/27/07 4:56 PM Page 433

BACKGROUNDAlthough Social Security is one of the United States’most important domestic programs, this system is by nomeans the first. There were a number of social insuranceprograms throughout Europe and Latin America beforethe Social Security Act was signed into law in 1935.Before the United States had Social Security, 20 othernations already had similar systems in operation. Another30 countries had different social insurance programs inplace, such as workers’ compensation.
POLICIES AND REGULATIONSMedicare is administered by the Centers for Medicareand Medicaid Services (CMS), formerly known as theHealth Care Financing Administration (HCFA). CMS is subdivided into three divisions with the followingresponsibilities:
1. The Center for Medicare Management oversees tradi-tional fee-for-service Medicare, including developmentof payment policy and management of fee-for-servicecontractors.
2. The Center for Beneficiary Choices provides benefici-aries with information on Medicare, Medicare Select,and Medicare Plus (+) Choice programs and Medigapoptions. It also manages the Medicare + Choice plans,consumer research, and grievance and appeals functions.
3. The Center for Medicaid and State Operationsfocuses on federal–state programs, such as Medicaid, theState Children’s Health Insurance Program, insuranceregulations, and the Clinical Laboratory ImprovementsAct (CLIA).
4. CMS also enforces the insurance portability andtransaction and code set requirements of the HealthInsurance Portability and Accountability Act.
Eligibility RequirementsThe Social Security Administration (SSA) offices takeapplications for Social Security, control the eligibilityprocess, and provide information about the Medicare
program. If an individual already receives Social Securityor Railroad Retirement benefits, he or she is automaticallyenrolled in Medicare Parts A and B starting the first day ofthe month that the individual turns 65 years of age. In theyear 2000, the retirement age gradually increased forpeople born in the year 1938 or later. By 2027, full-timeretirement age will be 67 for people born after 1959.Benefits may increase if retirement is delayed beyondfull-retirement age. As of this edition, Medicare still maybegin at age 65. Those who apply for Social Security early(at age 62 years) do not receive Medicare but receivemonthly reduced Social Security benefits. If an individualis younger than 65 years of age and disabled, he or shewill automatically get Medicare Parts A and B after get-ting Social Security disability or Railroad Retirementbenefits for 24 months. An individual does not have to beretired to receive Medicare benefits.
Medicare is a federal health insurance program for thefollowing categories of people:
1. People 65 years of age or older who are on SocialSecurity
2. People 65 years of age or older who are retired fromthe railroad or Civil Service
3. Disabled individuals who are eligible for SocialSecurity disability benefits* and who are in the followingcategories:a. Disabled workers of any ageb. Disabled widows of workers who are fully or cur-
rently insured through the federal government, CivilService, SSA, Supplemental Security Income(SSI), or the Railroad Retirement Act and whosehusbands qualified for benefits under one of theseprograms
c. Adults disabled before age 18 years whose parentsare eligible for or retired on Social Security benefits
4. Children and adults who have chronic kidney diseaserequiring dialysis or end-stage renal disease (ESRD)requiring a kidney transplant
5. Kidney donors (all expenses related to the kidney trans-plantation are covered)
All persons who meet one of the previously stated eli-gibility requirements determined by SSA are eligible forMedicare Part A (hospital coverage) at no charge.Those who qualify for full Medicare benefits may alsoelect to take Medicare Part B (outpatient coverage).Medicare Part B recipients pay annually increasing basicpremiums to the SSA, and some pay a Medicare surtax onfederal income tax payments. This premium may be
434 U N I T 3 HEALTH CARE PAYERS▼
Service to Patients
Remind the patient to bring in his or her insurance identification card or cards. Give assistance to patientswho may be visually impaired or have hearing impairment and need to complete registration forms forfiling insurance claims. Work closely with caregivers andbe aware of each patient’s limitations, caring for each onewith dignity.
Answer the patient’s questions about Medicare SummaryNotice documents because these can be confusing toelderly patients and can lead to misunderstandings about payments for services rendered.
*In the disabled categories, a person must be disabled for not lessthan 12 months to apply for disability benefits. A disabled beneficiarymust receive disability benefits for 24 months before Medicare benefits begin. See Chapter 16 for further information on this topic.
X3666-Ch12 8/27/07 4:56 PM Page 434
deducted automatically from the patient’s monthly SocialSecurity check if he or she wishes. Those individuals noteligible for Medicare Part A (hospital insurance) at 65years of age may purchase Part B from the SSA.
Aliens
An alien (may be referred to as an immigrant when a per-son from another country comes to settle) is an individualwho is not a citizen or national of the United States butbelongs to another country or people. In the Medicareprogram, an alien may be eligible for Part A or B coverage.To be eligible, the applicant must have lived in the UnitedStates as a permanent resident for 5 consecutive years. It isusually not necessary to state on the CMS-1500 (08-05)form that the patient is an alien when billing Medicare.
Health Insurance CardThe patient should present his or her Medicare healthinsurance card. It indicates the patient’s name and insur-ance claim number (Figures 12–1 and 12–2) that must beabstracted from the card and used when transmitting aclaim. The claim number is the Social Security numberof the wage earner with an alpha suffix. The card indi-cates hospital and medical coverage, effective date, andpatient status. Verify effective date because Part A andPart B may have different effective dates. If a beneficiaryapplies after his or her eligibility date, Part B could havea future date shown on the card. When a husband andwife both have Medicare, they receive separate cards andclaim numbers. However, a spouse’s card might have thehusband’s claim number if she has never worked and hasno SSA work credits. Medicare cards are red, white, andblue, and cards issued after 1990 are plastic. In addition,
ask to see the patient’s Part D card for prescription coverage. If it shows a health maintenance organization(e.g., Kaiser or Secure Horizons), then you know that thepatient signed up and is covered by a managed care planand not the Medicare standard program. The physicianmay or may not have a contract with that plan so cover-age for services would be in question. Then ask to see theinsurance card for the managed care plan.
The letters after the Medicare number on the patient’sidentification card indicate the patient’s status as follows(this is only a partial listing):
A = wage earner (shown in Figure 12–1)B = husband’s number (wife 62 years or older)D = widowHAD = disabled adult
C H A P T E R 12 Medicare 435▼
This is the patient’s health insurance claim number. It must be shown on all Medicare claims exactly as it is shown on the card — including the letter at the end.
NAME OF BENEFICIARY
JANE DOE
Jane Doe
MEDICARE CLAIM NUMBER
123-XX-6789ASEX
FEMALE
SOCIAL SECURITY ACT
EFFECTIVE DATE
01/01/20XX01/01/20XX
IS ENTITLED TO
SIGNHERE
HOSPITAL INSURANCE (PART A)MEDICAL INSURANCE (PART B)
Special code indicating patient status
The date the insurancestarts is shown here.
This shows hospital insurance coverage.
This shows medical insurance coverage.
DEPA
RTM
EN
T O
F HEALTH & HUM
AN
SE
RV
ICES
USA • •
MEDICARE HEALTH INSURANCEThe name must be shownexactly as it appears onthe card when transmittinga claim.
F I G U R E 12 – 1 Medicare health insurance identification card.
F I G U R E 12 – 2 Insurance billing specialist obtainingthe identification card from a disabled Medicare patient.
X3666-Ch12 8/27/07 4:56 PM Page 435

C = disabled childJ, Kl, or Jl = special monthly benefits, never worked
under Social SecurityM = Part B benefits onlyT = uninsured and entitled only to health insurance
benefits
A patient whose Medicare card claim number ends in“A” has the same Social Security and claim numbers. A patient whose Medicare card claim number ends in “B”or “D” has different Social Security and claim numbers. A quick check between Social Security and card claimnumbers may identify a submission error and forestall aclaims rejection.
The letters preceding the Medicare number on thepatient’s identification card indicate railroad retirees:
A = retired railroad employeeExamples: A 000000 (6 digits); A 000-00-0000 (9 digits)MA = spouse of a retired railroad employeeWA/WD = widow or widower of deceased employee (age
or disability)Examples: WA000000 (6 digits); WA000-00-0000 (9 digits)CA = child or studentWCA/WCD = widow of retiree with child in her care or
disabled child of deceased employeePA/PD = parent of deceased employee (male or female)H = Railroad Retirement Board pensioner before 1937MH = wife of Railroad Retirement Board pensioner
before 1937WH = widowed wife of Railroad Retirement Board pen-
sioner before 1937WCH = widow of Railroad Retirement Board pensioner
with child in her carePH = parent of Railroad Retirement Board pensioner
before 1937JA = widow receiving a joint and survivor annuityX = divorced spouse’s annuity, for use on forms AA-3 and
AA-7 onlyExample: CA 123-45-6789C
Enrollment StatusUnder Medicare Part B, if an individual receiving SocialSecurity or Railroad Retirement benefits did not sign upfor Medicare at the time of eligibility, then an individualis eligible to enroll in Medicare 3 months before his orher 65th birthday. The enrollment period ends 3 monthsafter the month in which the person turns 65. If theenrollment period is missed, the individual must waituntil the next general enrollment period, January 1 throughMarch 31, of the following year.
A telephone hotline or, in some states, a modem con-nection is available to verify the enrollment status. This is
useful because patients can switch coverage to a seniormanaged care plan on a month-to-month basis. Mostcarriers also allow information on deductible status. Thepatient’s numeric information (Medicare number anddate of birth) is entered into the telephone system, andthe digital response indicates how much of thedeductible has been satisfied. Contact the local Medicareadministrative contractor (MAC) for information aboutthis service.
Benefits and NonbenefitsMedicare Part A: hospital benefits
Part A of Medicare is hospital insurance benefits forpeople 65 years of age or older, for people younger thanage 65 with certain disabilities, or for people with end-stagerenal disease. Funds for this health service come fromspecial contributions from employees and self-employedpersons, with employers matching contributions. Thesecontributions are collected along with regular SocialSecurity contributions from wages and self-employmentincome earned during a person’s working years.
A benefit period begins the day a patient enters ahospital and ends when the patient has not been a bedpatient in any hospital or nursing facility (NF) (for-merly called skilled nursing facility) for 60 consecutivedays. It also ends if a patient has been in a nursing facil-ity but has not received skilled nursing care for 60 con-secutive days. A nursing facility offers nursing orrehabilitation services that are medically necessary to apatient’s recovery. Services provided are not custodial.Custodial services are those that assist the patient withpersonal needs (e.g., dressing, eating, bathing, and get-ting in and out of bed). Hospital insurance protection isrenewed every time the patient begins a new benefitperiod. There is no limit to the number of benefit peri-ods a patient can have for hospital or nursing facilitycare. However, special limited benefit periods apply tohospice care.
Medicare Part A provides benefits to applicants in anyof the following situations:
1. A bed patient in a hospital (up to 90 hospital days foreach benefit period)
2. A bed patient in a nursing facility receiving skillednursing care (up to 100 extended-care days for eachbenefit period)
3. A patient receiving home health care services4. A patient who needs care in a psychiatric hospital (up
to 190 days in a lifetime)5. A terminally ill patient diagnosed as having 6 months
or less to live who needs hospice care. A hospice is apublic agency or private organization that is primarily
436 U N I T 3 HEALTH CARE PAYERS▼
X3666-Ch12 8/27/07 4:56 PM Page 436

engaged in providing pain relief, symptom manage-ment, and supportive services to terminally ill peopleand their families.
6. A terminally ill patient who needs respite care. Respitecare is a short-term inpatient stay that may be neces-sary for the terminally ill patient to give temporaryrelief to the person who regularly assists with homecare. Inpatient respite care is limited to stays of nomore than 5 consecutive days for each respite period.
Figure 12–3 contains information on five major classifi-cations of inpatient hospital cost-sharing benefits forMedicare Part A. Miscellaneous hospital services and sup-plies might consist of intensive care unit (ICU) costs, bloodtransfusions, drugs, x-ray and laboratory tests, medical sup-plies (casts, surgical dressings, splints), use of wheelchair,operating room (OR) and recovery room costs, and therapy(physical, occupational, and speech language). There are nobenefits for personal convenience items (television, radio,and telephone), private duty nurses, or a private roomunless the private room is determined medically necessary.Similar benefits also relate to nursing facilities.
Benefits for hospice and respite care consist of nursingand physicians’ services, drugs, therapy (physical, occu-pational, and speech-language pathology), home healthaide, homemaker services, medical social services, medicalsupplies and appliances, short-term inpatient care, andcounseling.
Medicare Part B: medical and preventive care benefits
Part B of Medicare is supplementary medical insur-ance (SMI) benefits for the aged and disabled. Fundsfor this program come equally from those who sign upfor it and the federal government. A medical insurancepremium is automatically deducted from monthlychecks for those who receive Social Security benefits,Railroad Retirement benefits, or a Civil Service annu-ity. Others pay the premium directly to the SSA. Insome states, when a person is eligible for Medicare PartB and Medicaid, Medicaid pays for the monthly Part Bpremiums.
C H A P T E R 12 Medicare 437▼
91st to 150th day1
MEDICARE (PART A): HOSPITAL INSURANCE–COVERED SERVICES FOR 2007
HOSPITALIZATIONSemiprivate room and board, general nursing andmiscellaneous hospital services and supplies.(Medicare payments based on benefit periods.)
First 60 days All but $992 $992 deductible
All but $248 a day
All but $124 a day Up to $124 a day
$248 a day
All but $496 a day $496 a day
All costs
All costs
Nothing
Nothing
Nothing
61st to 90th day
First 20 days 100% of approved amount
100% of approved amount; 80% of
approved amount fordurable medical
equipment.
Nothing for services; 20% of approved amount
for durablemedical equipment.
Limited cost sharing for
outpatient drugsand inpatientrespite care.
21st to 100th day
Beyond 100 days
Unlimited as long asMedicare conditionsare met and services
are declared “medically necessary.”
If patient elects thehospice option andas long as doctor
certifies need.
Unlimited if medically necessary.
All but first 3 pintsper calendar year.
For first 3 pints.3
All but limited costsfor outpatient drugs andinpatient respite care.
60-reserve-daysbenefit
Beyond 150 days
NURSING FACILITY CAREPatient must have been in a hospital for at least3 days and enter a Medicare-approved facilitygenerally within 30 days after hospital discharge.2(Medicare payments based on benefit periods.)
HOME HEALTH CAREPart-time or intermittent skilled care, home health aide services, durable medical equipment and supplies, and other services.
HOSPICE CAREPain relief, symptom management, and support services for the terminally ill.
BLOOD
1 This 60-reserve-days benefit may be used only once in a lifetime.2 Neither Medicare nor private Medigap insurance will pay for most long-term nursing home care.3 To the extent the blood deductible is met under Part B of Medicare during the calendar year, it does not have to be met under Part A.
Services Benefit Medicare Pays Patient Pays
F I G U R E 12 – 3 Five major classifications of Medicare Part A benefits. (Updated fromMedicare and You 2007, U.S. Government Printing Office.)
X3666-Ch12 8/27/07 4:56 PM Page 437
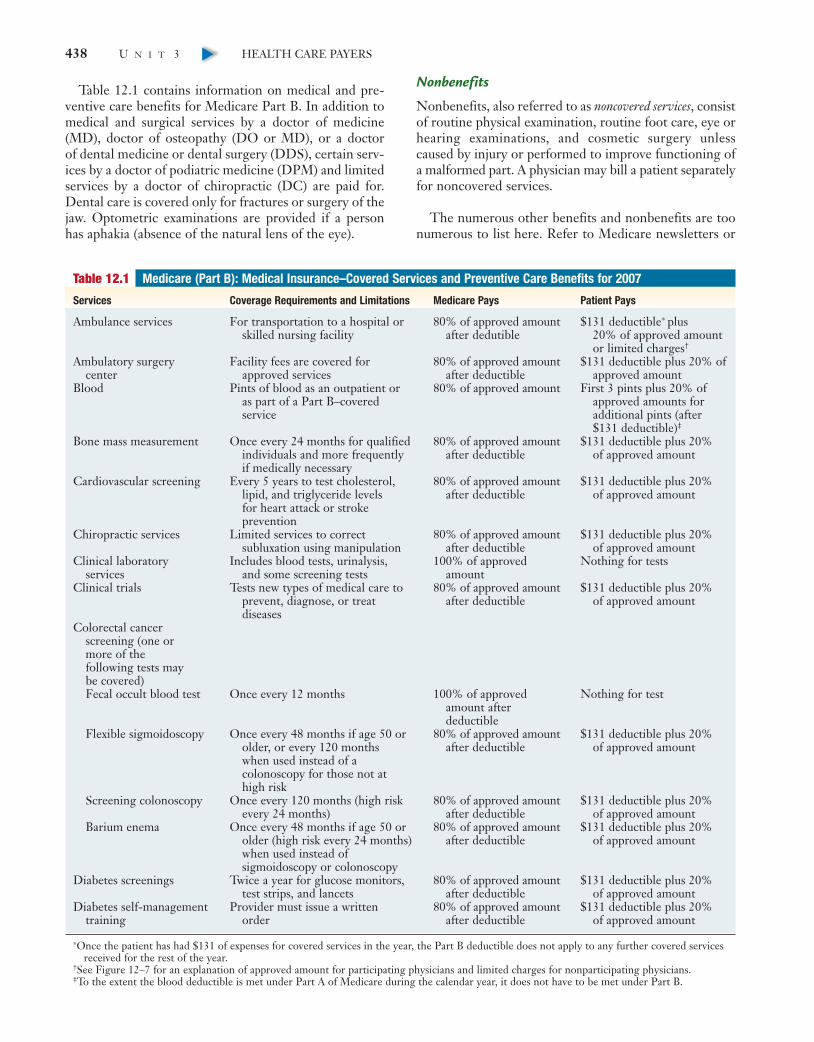
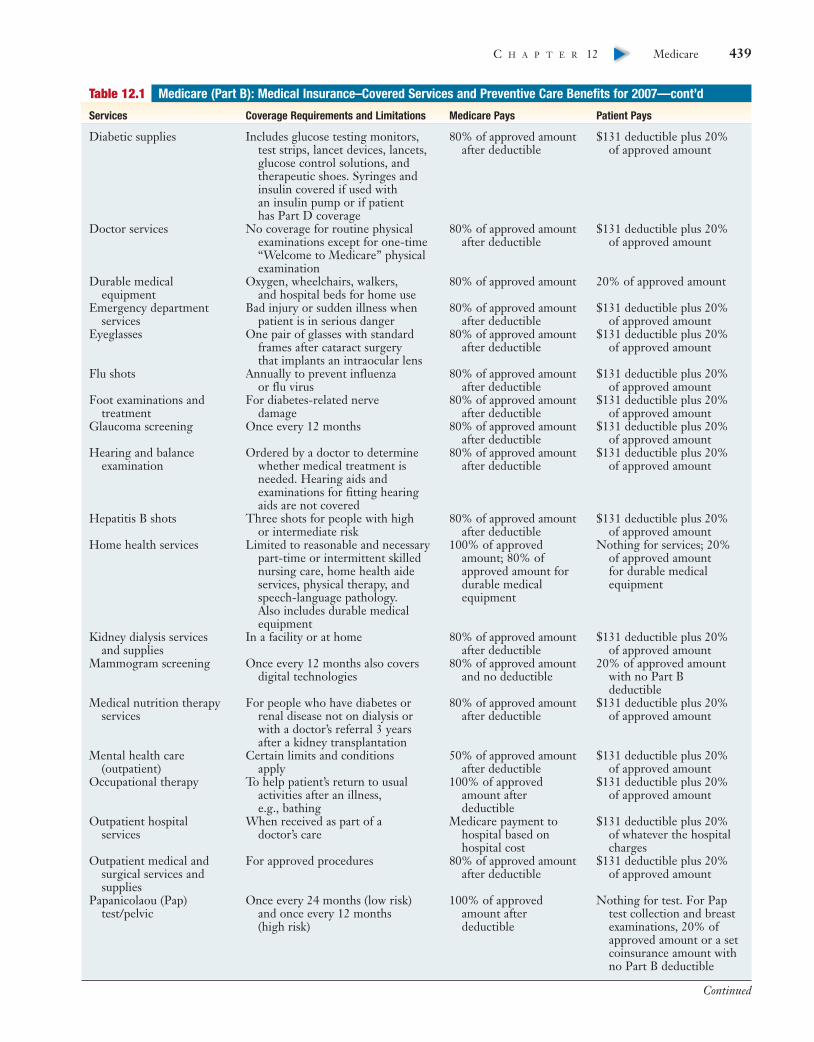
Table 12.1 contains information on medical and pre-ventive care benefits for Medicare Part B. In addition tomedical and surgical services by a doctor of medicine(MD), doctor of osteopathy (DO or MD), or a doctor of dental medicine or dental surgery (DDS), certain serv-ices by a doctor of podiatric medicine (DPM) and limitedservices by a doctor of chiropractic (DC) are paid for.Dental care is covered only for fractures or surgery of thejaw. Optometric examinations are provided if a personhas aphakia (absence of the natural lens of the eye).
Nonbenefits
Nonbenefits, also referred to as noncovered services, consistof routine physical examination, routine foot care, eye orhearing examinations, and cosmetic surgery unlesscaused by injury or performed to improve functioning ofa malformed part. A physician may bill a patient separatelyfor noncovered services.
The numerous other benefits and nonbenefits are toonumerous to list here. Refer to Medicare newsletters or
438 U N I T 3 HEALTH CARE PAYERS▼
Table 12.1 Medicare (Part B): Medical Insurance–Covered Services and Preventive Care Benefits for 2007
Services Coverage Requirements and Limitations Medicare Pays Patient Pays
Ambulance services For transportation to a hospital or 80% of approved amount $131 deductible∗ plus skilled nursing facility after dedutible 20% of approved amount
or limited charges†
Ambulatory surgery Facility fees are covered for 80% of approved amount $131 deductible plus 20% ofcenter approved services after deductible approved amount
Blood Pints of blood as an outpatient or 80% of approved amount First 3 pints plus 20% of as part of a Part B–covered approved amounts forservice additional pints (after
$131 deductible)‡
Bone mass measurement Once every 24 months for qualified 80% of approved amount $131 deductible plus 20% individuals and more frequently after deductible of approved amountif medically necessary
Cardiovascular screening Every 5 years to test cholesterol, 80% of approved amount $131 deductible plus 20%lipid, and triglyceride levels after deductible of approved amount for heart attack or stroke prevention
Chiropractic services Limited services to correct 80% of approved amount $131 deductible plus 20%subluxation using manipulation after deductible of approved amount
Clinical laboratory Includes blood tests, urinalysis, 100% of approved Nothing for testsservices and some screening tests amount
Clinical trials Tests new types of medical care to 80% of approved amount $131 deductible plus 20%prevent, diagnose, or treat after deductible of approved amountdiseases
Colorectal cancer screening (one or more of the following tests maybe covered)Fecal occult blood test Once every 12 months 100% of approved Nothing for test
amount after deductible
Flexible sigmoidoscopy Once every 48 months if age 50 or 80% of approved amount $131 deductible plus 20%older, or every 120 months after deductible of approved amountwhen used instead of a colonoscopy for those not athigh risk
Screening colonoscopy Once every 120 months (high risk 80% of approved amount $131 deductible plus 20%every 24 months) after deductible of approved amount
Barium enema Once every 48 months if age 50 or 80% of approved amount $131 deductible plus 20%older (high risk every 24 months) after deductible of approved amountwhen used instead of sigmoidoscopy or colonoscopy
Diabetes screenings Twice a year for glucose monitors, 80% of approved amount $131 deductible plus 20%test strips, and lancets after deductible of approved amount
Diabetes self-management Provider must issue a written 80% of approved amount $131 deductible plus 20%training order after deductible of approved amount
∗Once the patient has had $131 of expenses for covered services in the year, the Part B deductible does not apply to any further covered servicesreceived for the rest of the year.
†See Figure 12–7 for an explanation of approved amount for participating physicians and limited charges for nonparticipating physicians.‡To the extent the blood deductible is met under Part A of Medicare during the calendar year, it does not have to be met under Part B.
X3666-Ch12 8/27/07 4:56 PM Page 438
C H A P T E R 12 Medicare 439▼
Table 12.1 Medicare (Part B): Medical Insurance–Covered Services and Preventive Care Benefits for 2007—cont’d
Services Coverage Requirements and Limitations Medicare Pays Patient Pays
Diabetic supplies Includes glucose testing monitors, 80% of approved amount $131 deductible plus 20%test strips, lancet devices, lancets, after deductible of approved amountglucose control solutions, and therapeutic shoes. Syringes and insulin covered if used with an insulin pump or if patient has Part D coverage
Doctor services No coverage for routine physical 80% of approved amount $131 deductible plus 20%examinations except for one-time after deductible of approved amount“Welcome to Medicare” physical examination
Durable medical Oxygen, wheelchairs, walkers, 80% of approved amount 20% of approved amountequipment and hospital beds for home use
Emergency department Bad injury or sudden illness when 80% of approved amount $131 deductible plus 20%services patient is in serious danger after deductible of approved amount
Eyeglasses One pair of glasses with standard 80% of approved amount $131 deductible plus 20%frames after cataract surgery after deductible of approved amountthat implants an intraocular lens
Flu shots Annually to prevent influenza 80% of approved amount $131 deductible plus 20%or flu virus after deductible of approved amount
Foot examinations and For diabetes-related nerve 80% of approved amount $131 deductible plus 20%treatment damage after deductible of approved amount
Glaucoma screening Once every 12 months 80% of approved amount $131 deductible plus 20%after deductible of approved amount
Hearing and balance Ordered by a doctor to determine 80% of approved amount $131 deductible plus 20% examination whether medical treatment is after deductible of approved amount
needed. Hearing aids and examinations for fitting hearing aids are not covered
Hepatitis B shots Three shots for people with high 80% of approved amount $131 deductible plus 20% or intermediate risk after deductible of approved amount
Home health services Limited to reasonable and necessary 100% of approved Nothing for services; 20% part-time or intermittent skilled amount; 80% of of approved amount nursing care, home health aide approved amount for for durable medical services, physical therapy, and durable medical equipmentspeech-language pathology. equipmentAlso includes durable medical equipment
Kidney dialysis services In a facility or at home 80% of approved amount $131 deductible plus 20% and supplies after deductible of approved amount
Mammogram screening Once every 12 months also covers 80% of approved amount 20% of approved amount digital technologies and no deductible with no Part B
deductibleMedical nutrition therapy For people who have diabetes or 80% of approved amount $131 deductible plus 20%
services renal disease not on dialysis or after deductible of approved amountwith a doctor’s referral 3 years after a kidney transplantation
Mental health care Certain limits and conditions 50% of approved amount $131 deductible plus 20% (outpatient) apply after deductible of approved amount
Occupational therapy To help patient’s return to usual 100% of approved $131 deductible plus 20% activities after an illness, amount after of approved amounte.g., bathing deductible
Outpatient hospital When received as part of a Medicare payment to $131 deductible plus 20%services doctor’s care hospital based on of whatever the hospital
hospital cost chargesOutpatient medical and For approved procedures 80% of approved amount $131 deductible plus 20%
surgical services and after deductible of approved amountsupplies
Papanicolaou (Pap) Once every 24 months (low risk) 100% of approved Nothing for test. For Pap test/pelvic and once every 12 months amount after test collection and breast
(high risk) deductible examinations, 20% of approved amount or a set coinsurance amount with no Part B deductible
Continued
X3666-Ch12 8/27/07 4:56 PM Page 439

440 U N I T 3 HEALTH CARE PAYERS▼
Table 12.1 Medicare (Part B): Medical Insurance–Covered Services and Preventive Care Benefits for 2007—cont’d
Services Coverage Requirements and Limitations Medicare Pays Patient Pays
Physical examination One-time “Welcome to Medicare” 80% of approved amount $131 deductible plus 20%physical examination within after deductible of approved amountfirst 6 months patient is on Part B
Physical therapy Heat, light, exercise, and massage 100% of approved $131 deductible plus 20% treatment of injuries and disease amount after of approved amount
deductiblePneumococcal pneumonia Once in a lifetime 100% of approved Nothing for flu and PPV
vaccine (PPV) amount after if doctor accepts deductible assignment
Practitioner services Clinical social worker, physician 80% of approved amount $131 deductible plus 20% assistant, and nurse practitioner after deductible of approved amount
Prescription drugs Certain injectable cancer drugs. 80% of approved amount $131 deductible plus 20% Drug coverage for patients who after deductible of approved amounthave Part D
Prostate cancer Prostate-specific antigen (PSA) 80% of approved amount $131 deductible plus 20% screening test and digital rectal examination after deductible of approved amount.
once every 12 months No coinsurance and no Part B deductible for PSA test.
Prosthetic/orthotic items Arm, leg, back and neck braces; 80% of approved amount $131 deductible plus 20% artificial eyes; artificial limbs after deductible of approved amountand replacement parts; breast prostheses after mastectomy; prosthetic devices to replace an internal body part or function (includes ostomy supplies and parenteral and enteral nutrition therapy)
Second surgical opinions Covered in some cases and some 80% of approved amount $131 deductible plus 20% third surgical opinions are after deductible of approved amountcovered for surgery that is not an emergency
Smoking cessation Eight face-to-face visits during a 80% of approved amount $131 deductible plus 20% of 12-month period if diagnosed after deductible approved amountwith a smoking-related illness or if taking medicine that is affected by tobacco
Speech-language To regain and strengthen speech 100% of approved $131 deductible plus 20% pathology services skills amount after of approved amount
deductibleSurgical dressings For surgical or surgically treated 80% of approved amount $131 deductible plus 20%
wound after deductible of approved amountTelemedicine For some rural areas in a 80% of approved amount $131 deductible plus 20%
practitioner’s office, hospital, or after deductible of approved amountfederally qualified health center
Tests X-rays, magnetic resonance imaging, 80% of approved amount $131 deductible plus 20% computed tomography scans, after deductible of approved amountelectrocardiograms, and some other diagnostic tests
Transplant services Heart, Lung, kidney, pancreas, 80% of approved amount $131 deductible plus 20%intestine, and liver transplants; after deductible of approved amountbone marrow and cornea transplants; immunosuppressive drugs
Travel Services in United States, District 80% of approved amount $131 deductible plus 20% of Columbia, Puerto Rico, after deductible of approved amountVirgin Islands, Guam, Northern Mariana Islands, American Samoa, and Canada or on board a ship within U.S. territorial waters
X3666-Ch12 8/27/07 4:56 PM Page 440

contact the Medicare carrier to find out whether a partic-ular procedure qualifies for payment.
Medicare Part C: Medicare advantage plan
The Balanced Budget Act of 1997 created MedicarePart C, commonly referred to as Medicare AdvantagePlan, formerly called Medicare + Choice. This programwas formed to increase the number of health care optionsin addition to those that are available under Part A andPart B. Medicare Advantage Plans receive a fixed amountof money from Medicare to spend on their Medicaremembers. Some plans may require members to pay a pre-mium similar to the Medicare Part B premium. The pro-gram was introduced in 2004 and by 2006 replacedMedicare + Choice.
Plans available under this program may include thefollowing: health maintenance organization (HMO), point-of-service (POS) plan, preferred provider organization(PPO), private fee-for-service (PFFS) plan, provider-sponsored organization (PSO), religious fraternal benefitsociety (RFBS), and a pilot program, Medicare medicalsavings account (MSA). In an MSA plan, the patient choosesan insurance policy approved by Medicare that has a highannual deductible. Medicare pays the premiums for thispolicy and deposits the dollar amount difference betweenwhat it pays for the average beneficiary in the patient’sarea and the cost of the premium into the patient’s MSA.The patient uses the MSA money to pay medicalexpenses until the high deductible is reached. If the MSAmoney becomes depleted, the patient pays out of pocketuntil the deductible is reached. Unused funds roll overfor use the next year.
Medicare Part D
The Medicare Prescription Drug Improvement andModernization Act (MMA) became effective in 2003 butdrug benefits began January 1, 2006. This legislationknown as Medicare Part D provides seniors and peopleliving with disabilities with a prescription drug benefit. Itcovers prescription drugs used for conditions not alreadycovered by Parts A and B. It is a stand-alone prescriptiondrug plan offered by insurance companies and other pri-vate companies providing drug coverage that meet stan-dards established by Medicare. Other names for theseplans are Part D private prescription drug plans (PDPs), andMedicare Advantage prescription drug plans (MA-PDs).
There are two ways to get Medicare prescription drugcoverage:
1. Join a Medicare prescription drug plan that adds drugcoverage to the original Medicare plan, some Medicare
cost plans, some Medicare private fee-for-serviceplans, and Medicare medical savings account plans.
2. Join a Medicare Advantage plan such as an HMO orPPO that includes prescription drug coverage as partof the plan.
Individuals who enroll pay a monthly premium. Thosewho decide not to enroll in a Medicare drug plan whenthey are first eligible, may pay a penalty if they decide tojoin at a later time. Beginning in 2007, enrollees pay anannual deductible of $265 with an estimated premium of$35 a month (varies depending on plan) and a copaymentof drug costs up to $2400 in a year. After that, enrolleespay all drug costs until they have spent $3850 out ofpocket ($3,051.25 while in the coverage gap—sometimesreferred to as the doughnut hole—not including the drugplan’s premium). At that point, the coverage gap ends andthe enrollees pay a small coinsurance (5%) or a smallcopayment ($2.15 or $5.35) for each prescription untilthe end of the year.
People eligible for Medicaid and Medicare will payno premium or deductible and have no gap in coverage.They pay $1 per prescription for generics and $3 forbrand names. Copays are waived for those in nursinghomes. In addition, there are several programs thathelp people who have limited income and resources,and the programs, qualifications, and copayments varyby areas.
Prescription drug plans refer to the drugs in their for-mularies by tier numbers. A formulary is a list of thedrugs that a plan covers. Tier one represents generic drugsand has a low copayment associated with it. Tier two cov-ers preferred brand drugs and has a copayment, buthigher than tier one. Tier three drugs are the nonpre-ferred drugs and could have either a copayment or a per-centage of full drug cost associated with it. The fourthclassification is identified as “S,” which represents spe-cialty drugs, and requires a percentage of total cost of thedrug. Following are several classes of drugs excluded fromcoverage:
● Barbiturates● Benzodiazepines● Drugs for cosmetic purposes● Drugs for symptomatic relief of cough and colds● Drugs for weight loss or gain● Erectile dysfunction drugs● Fertility drugs● Prescription vitamins or minerals except prenatal
A provider who prescribes a drug that can be coveredby either Part B or Part D must clarify the condition andpart coverage on the prescription form (Example 12.1).
C H A P T E R 12 Medicare 441▼
X3666-Ch12 8/27/07 4:56 PM Page 441

When a patient has coverage under a Part D plan,obtain a photocopy of either the patient’s Medicare sup-plement or the patient’s Medicare Advantage plan card.Then check whether the drug that the patient needs iscovered by the plan, which generic drugs are available,and whether a drug needs prior authorization. Eithertelephone the number listed on the card or use a freesoftware program—Epocrates—that is available toproviders to help with these needs. Refer to the InternetResources at the end of this chapter. To learn moreabout Epocrates, go to the Evolve website and click onthe link for Epocrates.
Railroad retirement benefits
Railroad Retirement Board offices maintain eligibilityrecords for Medicare and provide information about theprogram for railroad workers and their beneficiaries.Medical insurance premiums are automatically deductedfrom the monthly checks of people who receive RailroadRetirement benefits. Those who do not receive amonthly check pay their premiums directly or, in somecases, have premiums paid on their behalf under a stateassistance program. If the allowed fees differ from thoseallowed by the regular Medicare carrier, write or fax theMedicare railroad retiree carrier, asking that fees bebased on fee data from the local carrier.
Railroad Retirement beneficiaries generally are entitledto benefits for covered services received from a qualifiedAmerican facility. However, under certain circumstances,a Medicare beneficiary may receive care in Canada orMexico. Benefits and deductibles under Parts A and B arethe same as for other Medicare recipients.
Some railroad retirees are members of a railroad hospi-tal association or a prepayment plan. These members payregular premiums to the plan and then can receive healthservices that the plan provides without additional charges.In some plans, small charges are made for certain services,such as drugs or home visits. Many prepayment plansmake arrangements with Medicare to receive direct pay-ments for services they furnish that are covered underMedicare Part B. Some prepayment plans have contractswith Medicare as HMOs or competitive medical plans
and can receive direct payment for services covered byeither hospital or medical insurance. After a claim istransmitted to the Medicare railroad retiree carrier,which is usually to a different regional Medicare admin-istrative contractor (MAC), a remittance advice (RA)document is generated explaining the decision made onthe claim and what services Medicare paid for.
Employed elderly benefits
To understand various types of scenarios that may beencountered when transmitting claims for elderly indi-viduals, one must know about several federal laws thatregulate health care coverage of those age 65 and olderwho are employed. Such individuals may have groupinsurance or a Medigap (MG) policy and may fall underbilling categories of Medicare first payer or Medicaresecondary payer (all are presented in detail later in thischapter). The federal laws that affect employed elderlyindividuals are shown in Table 12.2.
ADDITIONAL INSURANCE PROGRAMSMany Medicare recipients have Medicare in combinationwith other insurance plans. This section explains variouscoverage combinations. Guidelines for processing claimsfor these plans are presented later in this chapter.
Medicare/MedicaidPatients designated as Medicare/Medicaid (Medi-Medi) are on both Medicare and Medicaid simultane-ously. These patients qualify for Old Age, Survivors, andDisability Insurance (OASDI) assistance benefits (olderthan age 65), are severely disabled, or are blind.
Medicare/MedigapA specialized insurance policy devised for the Medicarebeneficiary is called Medigap or Medifill. This type ofpolicy is designed to supplement coverage under a fee-for-service Medicare plan. It may cover prescription costsand the deductible and copayment (e.g., 20% of theMedicare allowed amount) that are typically the patient’sresponsibility under Medicare. These plans are offeredby private third-party payers to Medicare beneficiarieswho pay the monthly premiums for this supplementalinsurance.
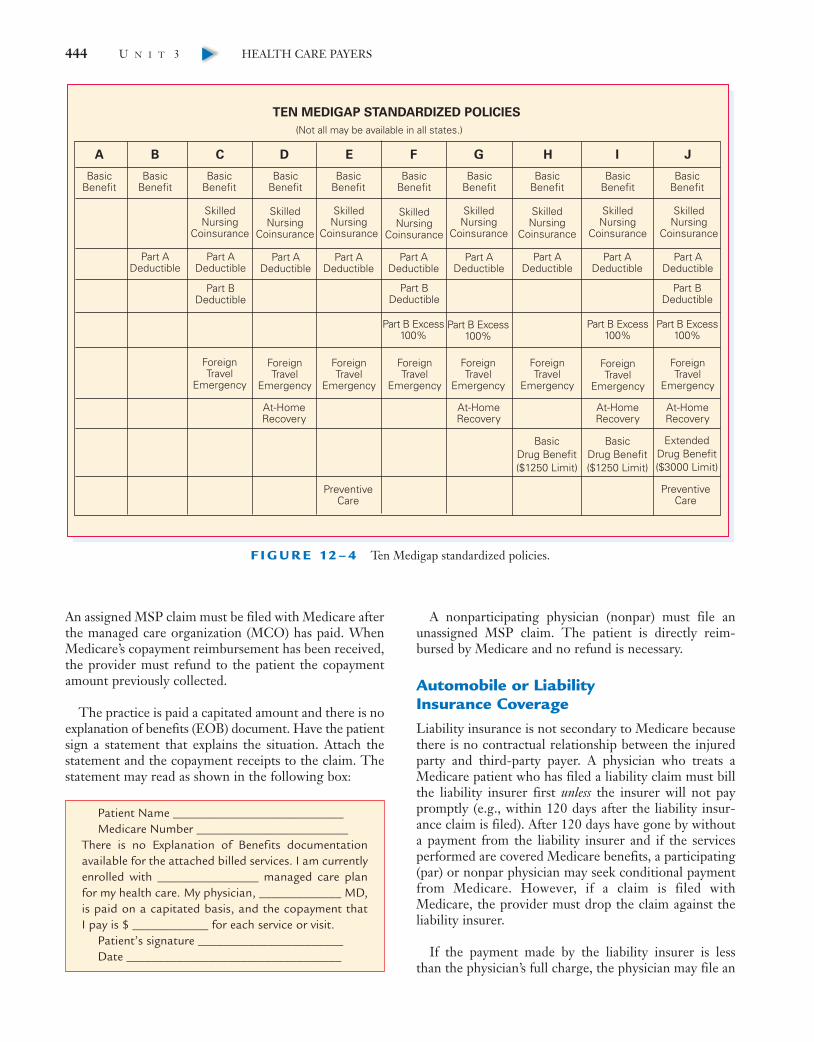
The federal government in conjunction with the insur-ance industry established predefined minimum benefitsfor 10 Medigap policies categorized by alpha letters Athrough J (Figure 12–4). Basic benefits are found in policyA. Each subsequent letter represents basic benefits plusother coverage, with the most comprehensive benefits inpolicy J. Sale of all policies are not available in all states, soindividuals in some states have fewer options than others.
Example 12.1 Prescription Note Clarifying MedicalUse of Drug and CoverageDetermination
Patient with psoriasis (autoimmune disorder) is prescribedmethotrexate. Generally, this immunosuppressive drugis prescribed for transplant patients and is covered underPart B.Added prescription note should read: “Psoriasis forPart D.”
442 U N I T 3 HEALTH CARE PAYERS▼
X3666-Ch12 8/27/07 4:56 PM Page 442

A slightly different variation of a Medigap policy isMedicare Select. This policy has the same coverage as reg-ular Medigap policies, but there is a restriction in that thebeneficiary must obtain medical care from a list of speci-fied network doctors and providers.
Medicare Secondary PayerIn some instances, Medicare is considered secondary andclassifies the situation as Medicare Secondary Payer(MSP). MSP may involve aged or disabled patients withthe following qualities:
● Aged workers under group health plans with morethan 20 covered employees
● Disabled individuals age 64 and younger who are cov-ered under a group health plan with more than 100covered employees or covered under a family mem-ber’s current employment
● Medicare beneficiaries under an employer-sponsoredgroup health plan that have end-stage renal diseaseduring the first 18 months of the patient’s eligibilityfor Medicare
● Cases of workers’ compensation when the injury orillness occurs at work
● Individuals either currently or formerly employedwith black lung disease who fall under the FederalBlack Lung Program
● Individuals receiving benefits under the Departmentof Veterans Affairs and Medicare
● Individuals covered under a Federal Research GrantProgram
● Automobile accident cases, such as medical no-faultcases and third-party liability insurance cases
Follow the suggested steps in the procedure at the endof the chapter to identify whether Medicare is primary orsecondary and to determine what additional benefits thepatient might have.
Managed care and medicare
When a patient’s primary insurance is a managed careplan that requires fixed copayments, it is possible toobtain reimbursement from Medicare for those amounts.
C H A P T E R 12 Medicare 443▼
Table 12.2 Federal Laws Affecting Employed Elderly Individuals
OMNIBUS BUDGET RECONCILIATION ACT
The Omnibus Budget Reconciliation Act (OBRA) of 1981 required that, in the case of a current or former employee ordependent younger than age 65 years and eligible for Medicare solely because of ESRD, the employer’s group coverage isprimary for up to 30 months. The Balanced Budget Act of 1997 mandated this change in the length of the coordination period.OBRA applies to all employers regardless of the number of employees. OBRA of 1986, effective in 1987, required that, if anemployee or dependent younger than age 65 years has Medicare coverage because of a disability other than ESRD, the groupcoverage is primary and Medicare is secondary. This act applies only to large group health plans having at least 100 full- or part-time employees.
TAX EQUITY AND FISCAL RESPONSIBILITY ACT
The Tax Equity and Fiscal Responsibility Act (TEFRA) of 1982 established that an employee or spouse age 65 to 69 years isentitled to the same health insurance benefits offered under the same conditions to younger employees and their spouses. The group insurance is primary and Medicare is secondary. TEFRA applies to employers with at least 20 full- or part-timeemployees.
DEFICIT REDUCTION ACT
The Deficit Reduction Act (DEFRA) of 1984, effective 1985, was an amendment to TEFRA and stated that a spouse age 65 to69 years or an employee of any age is entitled to the same group health plan offered to younger employees and their spouses.The group’s coverage is primary and Medicare is secondary. DEFRA applies to employers with at least 20 full- or part-timeemployees.
CONSOLIDATED OMNIBUS BUDGET RECONCILIATION ACT
The Consolidated Omnibus Budget Reconciliation Act (COBRA) of 1985, effective 1986, is another amendment to TEFRAeliminating the age ceiling of 69 years. An employee or spouse age 65 or older is entitled to the same group health plan offeredto younger employees and their spouses. COBRA requires that third-party payers reimburse for certain care rendered ingovernment-run veteran and military hospitals. The group’s coverage is primary and Medicare is secondary. COBRA applies toemployers with at least 20 full- or part-time employees.
TAX REFORM ACT
The Tax Reform Act was passed in 1986; it clarified certain aspects of COBRA. A spouse and dependents may elect to receivecontinued coverage even if the employee does not wish insurance coverage and terminates the plan. However, the spouse anddependents must have been covered under the plan before the covered employee terminates it. Spouses who are widowed ordivorced while receiving continued coverage must report such changes to the benefit plan administrator within 60 days of theemployee’s death to determine how many additional months of coverage are available.
X3666-Ch12 8/27/07 4:56 PM Page 443
An assigned MSP claim must be filed with Medicare afterthe managed care organization (MCO) has paid. WhenMedicare’s copayment reimbursement has been received,the provider must refund to the patient the copaymentamount previously collected.
The practice is paid a capitated amount and there is noexplanation of benefits (EOB) document. Have the patientsign a statement that explains the situation. Attach thestatement and the copayment receipts to the claim. Thestatement may read as shown in the following box:
A nonparticipating physician (nonpar) must file anunassigned MSP claim. The patient is directly reim-bursed by Medicare and no refund is necessary.
Automobile or Liability Insurance CoverageLiability insurance is not secondary to Medicare becausethere is no contractual relationship between the injuredparty and third-party payer. A physician who treats aMedicare patient who has filed a liability claim must billthe liability insurer first unless the insurer will not paypromptly (e.g., within 120 days after the liability insur-ance claim is filed). After 120 days have gone by withouta payment from the liability insurer and if the servicesperformed are covered Medicare benefits, a participating(par) or nonpar physician may seek conditional paymentfrom Medicare. However, if a claim is filed withMedicare, the provider must drop the claim against theliability insurer.
If the payment made by the liability insurer is less than the physician’s full charge, the physician may file an
Patient Name ___________________________Medicare Number ________________________
There is no Explanation of Benefits documentationavailable for the attached billed services. I am currentlyenrolled with ________________ managed care planfor my health care. My physician, _____________ MD,is paid on a capitated basis, and the copayment that I pay is $ ____________ for each service or visit.
Patient’s signature _______________________Date __________________________________
444 U N I T 3 HEALTH CARE PAYERS▼
A B C D E F G H I J
TEN MEDIGAP STANDARDIZED POLICIES
BasicBenefit
BasicBenefit
Part ADeductible
Part ADeductible
Part BDeductible
ForeignTravel
Emergency
ForeignTravel
Emergency
At-HomeRecovery
At-HomeRecovery
At-HomeRecovery
At-HomeRecovery
ForeignTravel
Emergency
ForeignTravel
Emergency
ForeignTravel
Emergency
ForeignTravel
Emergency
ForeignTravel
Emergency
ForeignTravel
Emergency
Part BDeductible
Part B Excess100%
Part B Excess100%
Part B Excess100%
Part B Excess100%
Part BDeductible
Part ADeductible
Part ADeductible
Part ADeductible
Part ADeductible
Part ADeductible
Part ADeductible
Part ADeductible
BasicBenefit
SkilledNursing
Coinsurance
SkilledNursing
Coinsurance
SkilledNursing
Coinsurance
SkilledNursing
Coinsurance
SkilledNursing
Coinsurance
SkilledNursing
Coinsurance
SkilledNursing
Coinsurance
SkilledNursing
Coinsurance
BasicBenefit
BasicBenefit
BasicBenefit
BasicBenefit
BasicBenefit
BasicBenefit
BasicBenefit
ExtendedDrug Benefit($3000 Limit)
PreventiveCare
PreventiveCare
BasicDrug Benefit($1250 Limit)
BasicDrug Benefit($1250 Limit)
(Not all may be available in all states.)
F I G U R E 12 – 4 Ten Medigap standardized policies.
X3666-Ch12 8/27/07 4:56 PM Page 444

assigned claim and must accept as full payment the greaterof either the Medicare-approved charge or sum of theliability insurance primary payment and the Medicaresecondary payment.
A nonpar physician may file an unassigned claim forMedicare secondary payment only if the payment by theliability insurer is less than the Medicare limiting charge.If the payment equals or exceeds the limiting charge, thephysician must accept the disbursement as full payment.
If Medicare payments have been made but should nothave been because the services are excluded under thisprovision, or if the payments were made on a condi-tional basis, they are subject to recovery. A copy of thenotice of payment or denial form from the other insurershould be included when sending in the CMS-1500 (08-05) claim form. Medicare is secondary even if a statelaw or a private contract of insurance states that Medicareis primary. The physician must bill the other insurerfirst. A claim for secondary benefits may be transmittedto Medicare only after payment or denial has been madeby the primary coverage. Liability insurance is not considered an MSP.
MEDICARE MANAGED CARE PLANSHealth Maintenance OrganizationsDuring the spring of 1984, the Department of Healthand Human Services published regulations givingMedicare enrollees the right to join and assign theirMedicare benefits to HMOs. HMOs had been in opera-tion for nearly 50 years when they became available as anoption for Medicare enrollees. With a Medicare HMO(also known as a senior HMO or senior plan), the patientdoes not need a Medicare supplemental insurance plan.Upon enrollment, the Medicare beneficiary is sent aninsurance card from the managed care plan (Figure12–5). However, Medicare cards are not forfeited and anelderly patient may show two cards, leading to confusionabout what the coverage is and who to bill.
Medicare makes payments directly to the HMO on amonthly basis for Medicare enrollees who use the HMOoption. Enrollees pay the HMO a monthly premium,which is an estimate of the coinsurance amounts forwhich the enrollee would be responsible plus theMedicare deductible. It appears that HMOs contractingto provide services for Medicare patients will be con-verted to a Medicare + Choice plan as their contractrenewal dates occur.
Some HMOs provide services not usually covered byMedicare, such as eyeglasses, prescription drugs, and rou-tine physical examinations. Once a person has converted
from Medicare to an HMO, he or she cannot go back toa former physician of personal choice and expectMedicare to pay the bill. The patient should receive serv-ices from a physician and hospital facility that are con-tracted with the HMO plan.
If a Medicare patient has switched over to a managedcare plan and wishes to disenroll, the patient must do thefollowing:
1. Notify the plan in writing of disenrollment.2. Complete Medicare form Medicare Managed Care
Disenrollment CMS-566, attach a copy of the disen-rollment letter, and take it to the Social Security office.
Many plans allow the patient to enroll and disenroll atany time during the year. It may take the plan 30 days fordisenrollment, and Medicare may take as long as 60 daysto reenroll a patient. Patients who disenroll may have torequalify for supplemental coverage at a higher cost.
There are two types of HMO plans that may haveMedicare Part B contracts: HMO risk plans and HMOcost plans.
Risk plan
As a condition of enrollment in an HMO risk plan, ben-eficiaries receive Medicare-covered services (exceptemergency, urgent need, and prior authorized services)only from providers who are contracted members of theHMO network. Enrollees of HMO risk plans are referredto as “restricted” beneficiaries. Usually services renderedby “out-of-plan” physicians are not covered when thesame services are available through the organization unlessa referral or prior authorization is obtained. The only
C H A P T E R 12 Medicare 445▼
I.D. NUMBER
MEMBER SINCE:
NAME:
MEDICAL
DENTAL
04865-01 LAC
04/01/95
TOWNGATE, IRENE B.
COLLEGE CLINIC(555) 486-9002
MASROUR-RAD, GUSTAVA(555) 884-4224
$20 ER
RX YES
Health America Senior
Offered by CarePlus
$3
$5BASIC
F I G U R E 12 – 5 A senior managed care plan card.
X3666-Ch12 8/27/07 4:56 PM Page 445

exception is for emergency care. Claims for HMO risk planbeneficiaries must be sent directly to the organization.
A system of Medicare reimbursement for HMOs withrisk contracts is called diagnostic cost groups (DCGs).The HMO enrollees are classified into various DCGs onthe basis of each beneficiary’s prior 12-month history ofhospitalization, and payments are adjusted accordingly.This payment system does not apply to disabled and hos-pice patients, those on renal dialysis, or those enrolledonly in Medicare Part B. Patients are reclassified eachyear according to their previous year’s use of hospitalservice. This is further discussed in Chapter 17.
Cost plan
Under an HMO cost plan, beneficiaries receive Medicare-covered services from sources in or outside of the HMOnetwork. Enrollees are referred to as “unrestricted” ben-eficiaries. Claims for cost plan beneficiaries may be sentto the HMO plan or the regular Medicare carrier.
Noncontract physician
If a noncontract physician treats a Medicare HMOpatient, the services are considered “out-of-plan” serv-ices. The claim must be submitted to the managed careplan, which determines whether it is responsible to payfor the services. Conditions that must be met follow:
1. The service was an emergency and the patient was notable to get to an HMO facility or member physician(patient was out of the HMO area).
2. The service was covered by Medicare.3. The service was medically necessary.4. The service was authorized previously or was an
approved referral.
The patient is responsible for the fee if the HMOdetermines there was no emergency and denies payment.The HMO reimburses according to the Medicare FeeSchedule Allowable Amount, so the physician cannot billthe patient for the balance. If the physician does notreceive 100% of the allowable, steps must be takenthrough the HMO’s appeals process. If this fails, contactthe Medicare Managed Care Department at the MedicareRegional CMS Operations Office. Denied services can bebilled to the patient (no more than the Medicare feeschedule or limiting charge) after the HMO EOB isreceived.
Carrier Dealing PrepaymentOrganizationA Carrier Dealing Prepayment Organization may be setup by a medical practice under contract to the government.
Such plans are considered a service contract rather thaninsurance. In the past, such plans were run by HMOs,but now practices of 12 to 15 physicians are opting to runtheir own plans. These organizations must be incorporatedand have their own Medicare provider number. Theorganization must furnish physicians’ services throughemployees and partners or under formal arrangementwith medical groups, independent practice associations,or individual physicians. Part B services must be providedthrough qualified hospitals or physicians. When operat-ing this type of organization, the physician acceptsMedicare assignment and agrees to deal with theMedicare carrier instead of CMS. Patients sign a contractagreeing to pay a monthly fee (usually $20 to $25). Thisis supposed to cover all Medicare copayments, deductibles,and nonreimbursable expenses (annual physical examina-tions and preventive care). The patient is not responsibleto pay for noncovered services.
UTILIZATION AND QUALITY CONTROLQuality Improvement OrganizationsAs explained in detail in Chapter 11, a QualityImprovement Organization (QIO) program (formerlyknown as professional or peer review organization), con-tracts with CMS to review medical necessity, reasonable-ness, appropriateness, and completeness and adequacy ofcare given in inpatient, outpatient, and emergency roomhospitals, skilled nursing facilities, home health agencies,private fee-for-service plans, and ambulatory surgical cen-ters for which additional payment is sought under the out-lier provisions of the prospective payment system (PPS).
CMS has assigned a point system for medical docu-mentation as discussed in Chapter 4. If sufficient pointsare lacking, penalties can lead to fines or forfeiture of thephysician’s license. Therefore it is extremely importantthat each patient’s care be well documented from thetreatment standpoint, as well as for justifying maximumreimbursement. A physician who receives a letter from aQIO about quality of care should consult his or her attor-ney before responding by letter or personal appeal. A photocopy of the patient’s health record can be used to substantiate the claim if there is detailed clinical documentation.
Federal False Claims Amendment ActAnother federal law to prevent overuse of services and tospot Medicare fraud is the Federal Claims AmendmentAct of 1986. This act offers financial incentives of 15% to25% of any judgment to informants (whistleblowers)who report physicians suspected of defrauding the federalgovernment. This is called a qui tam action. The laws areintended to help catch Medicare and Medicaid cheaters.
446 U N I T 3 HEALTH CARE PAYERS▼
X3666-Ch12 8/27/07 4:56 PM Page 446

The health insurance companies that process Medicareclaims have a Medicare fraud unit whose job is to catchpeople who steal from Medicare. The Office of theInspector General (OIG), Department of Health andHuman Services, is the law enforcement agency thatinvestigates and prosecutes people who steal fromMedicare. The OIG works closely with Medicare insur-ance companies, the Federal Bureau of Investigation (FBI),the Postal Inspection Service, and other federal lawenforcement agencies. If the physician is on an opticaldisk retrieval (ODR) A-1000 system, it is possible for theOIG to obtain procedure codes that show comparisonbilling with peers in the area. The Centers for Medicaidand Medicare Services alerts the OIG of offices to inves-tigate. To reduce the chances of a Medicare beneficiarycomplaining to the government, take the following actions:
● Listen to the patient’s complaint and follow up.● Publicize the provider’s hotline.● Route a beneficiary’s complaint to a compliance offi-
cer or office manager.
For information on fraud and abuse, see Boxes 2.11and 2.12. See Chapter 15 for information about fraud inthe workers’ compensation program.
Clinical Laboratory Improvement AmendmentThe CLIA of 1988 established federal standards, qualitycontrol, and safety measures for all freestanding labora-tories, including physician office laboratories (POLs).Various laboratory procedures fall within CLIA cate-gories depending on the complexity of each test. If aphysician performs only tests that pose no risk to thepatient, the laboratory may be eligible for a certificate ofwaiver that exempts it from CLIA regulations’ qualitycontrol and personnel standards; however, a registrationfee must still be paid for the waived category. The othertwo categories are moderate or high-complexity labora-tory services. Each category level requires a yearly licens-ing fee to be paid by the physician. A certificate is thenissued and must be posted in the laboratory. Various lev-els of quality control measures are necessary for eachCLIA level and must be performed in a timely manner(e.g., daily or weekly). Fines may be levied if federal stan-dards are not maintained. This has had an impact onoffice laboratories; because of the strict requirements,many physicians send patients to independent laborato-ries for tests (e.g., blood cell counts, cytology specimens,and cultures). However, some physicians prefer to drawblood from a patient, particularly if the patient has a his-tory of difficult venous access.
When claims to Medicare administrative contractorsare submitted for laboratory services performed in the
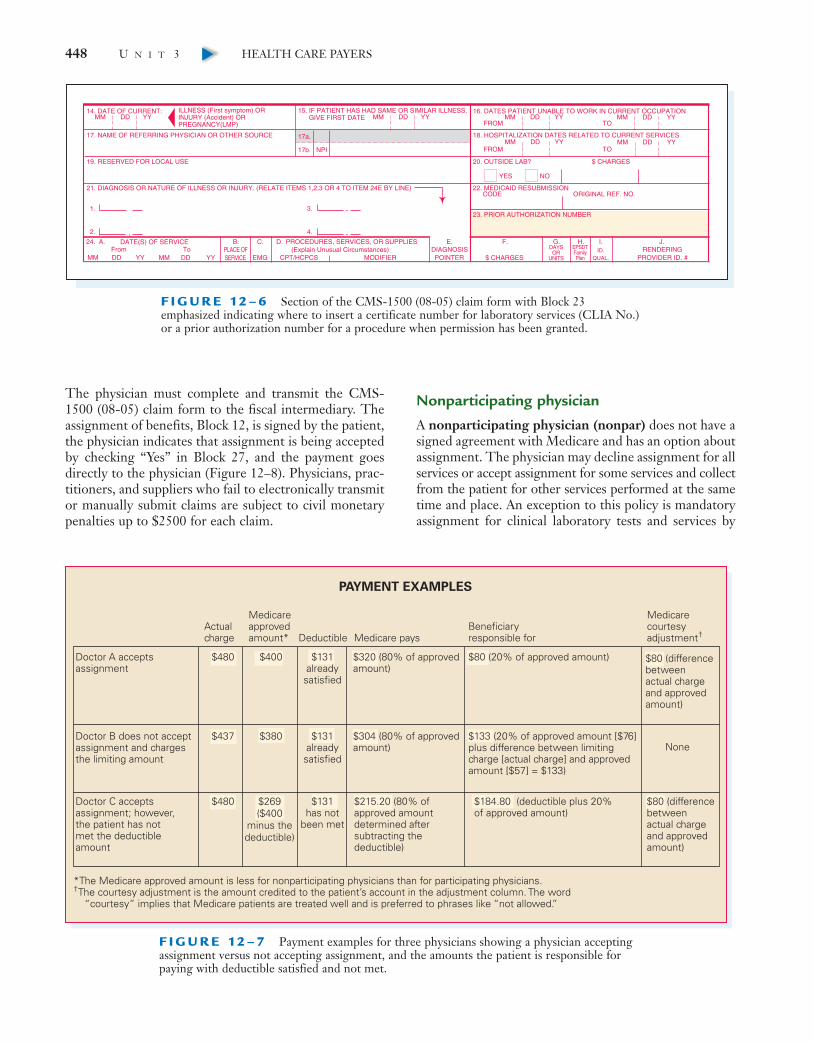
physician’s office, the 10-digit CLIA certificate numbershould be entered in Block 23 of the CMS-1500 (08-05)claim form (Figure 12–6). Physicians billing patients foroutside laboratory work are not held to these standardsbut may charge the patient only what the laboratorycharges (based on a fee schedule), plus any additionalservices the physician provides (e.g., drawing, handling,shipping, and interpretation of the blood or office visit).
PAYMENT FUNDAMENTALSProvider
Participating physician
In a participating physician (par) agreement, a physicianagrees to accept payment from Medicare (80% of theapproved charges) plus payment from the patient (20% ofapproved charge) after the $131 deductible has been met(Figure 12–7). The Medicare annual deductible is basedon the calendar year, January 1 through December 31.This agreement is referred to as accepting assignment.
C H A P T E R 12 Medicare 447▼
MEDICARE BILLINGCOMPLIANCE ISSUES
Because Medicare is a federal program, legislation setsdown the policies that must be followed. Therefore who-ever participates in the program must comply with all theregulations. Billing issues about which medical practicesshould be aware may include but are not limited to thefollowing:● Release of medical information● Reassignment of payment● Limiting charges for nonparticipating providers● Correct procedural code assignment and service
utilization● Accurate diagnostic code assignment● Medical necessity of services performed● Billing for ancillary employees (physician assistants and
nurse practitioners) called “incident-to” billing● Documentation related to selection of procedural codes
for services performed● Ancillary orders and supervision requirements● Teaching physician and resident billing● Routine waiver of copayments, deductibles, or profes-
sional courtesy discounts● Stark I and II antireferral and compensation regulations● Credit balance refunds● Correct coding initiative edits
X3666-Ch12 8/27/07 4:56 PM Page 447
The physician must complete and transmit the CMS-1500 (08-05) claim form to the fiscal intermediary. Theassignment of benefits, Block 12, is signed by the patient,the physician indicates that assignment is being acceptedby checking “Yes” in Block 27, and the payment goesdirectly to the physician (Figure 12–8). Physicians, prac-titioners, and suppliers who fail to electronically transmitor manually submit claims are subject to civil monetarypenalties up to $2500 for each claim.
Nonparticipating physician
A nonparticipating physician (nonpar) does not have asigned agreement with Medicare and has an option aboutassignment. The physician may decline assignment for allservices or accept assignment for some services and collectfrom the patient for other services performed at the sametime and place. An exception to this policy is mandatoryassignment for clinical laboratory tests and services by
448 U N I T 3 HEALTH CARE PAYERS▼
F I G U R E 12 – 7 Payment examples for three physicians showing a physician acceptingassignment versus not accepting assignment, and the amounts the patient is responsible forpaying with deductible satisfied and not met.
PAYMENT EXAMPLES
Doctor A acceptsassignment
Medicare approved amount* Deductible
$131has not
been met
$131alreadysatisfied
$131alreadysatisfied
Medicare paysBeneficiaryresponsible for
Actualcharge
$380
$269($400
minus thedeductible)
None
Medicarecourtesyadjustment†
$320 (80% of approved amount)
$80 (20% of approved amount)
$304 (80% of approved amount)
$215.20 (80% ofapproved amountdetermined aftersubtracting thedeductible)
$184.80 (deductible plus 20% of approved amount)
$80 (differencebetweenactual chargeand approvedamount)
$80 (differencebetweenactual chargeand approvedamount)
$400
$437
$480
$480
Doctor B does not acceptassignment and chargesthe limiting amount
Doctor C acceptsassignment; however,the patient has notmet the deductibleamount
$133 (20% of approved amount [$76]plus difference between limitingcharge [actual charge] and approvedamount [$57] = $133)
*The Medicare approved amount is less for nonparticipating physicians than for participating physicians.†The courtesy adjustment is the amount credited to the patient’s account in the adjustment column. The word “courtesy” implies that Medicare patients are treated well and is preferred to phrases like “not allowed.”
ILLNESS (First symptom) ORINJURY (Accident) ORPREGNANCY(LMP)
MM DD YY15. IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS.
GIVE FIRST DATE MM DD YY14. DATE OF CURRENT:
17. NAME OF REFERRING PHYSICIAN OR OTHER SOURCE
19. RESERVED FOR LOCAL USE
21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY. (RELATE ITEMS 1,2,3 OR 4 TO ITEM 24E BY LINE)
17a.
17b. NPI
OTMORF
OTMORF
MM DD YY MM DD YY
MM DD YY MM DD YY
CODE ORIGINAL REF. NO.
16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION
18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES
20. OUTSIDE LAB? $ CHARGES
22. MEDICAID RESUBMISSION
23. PRIOR AUTHORIZATION NUMBER
YES NO
1. 3.
2. 4.
FromMM DD YY
ToMM DD YY $ CHARGES
DATE(S) OF SERVICEPLACE OFSERVICE
PROCEDURES, SERVICES, OR SUPPLIES(Explain Unusual Circumstances)
CPT/HCPCS MODIFIERDIAGNOSISPOINTER
DAYSOR
UNITS
F. H. I. J.24. A. B. C. D. E.
PROVIDER ID. #EMGRENDERING
G.EPSDTFamilyPlan
ID.QUAL.
F I G U R E 12 – 6 Section of the CMS-1500 (08-05) claim form with Block 23 emphasized indicating where to insert a certificate number for laboratory services (CLIA No.)or a prior authorization number for a procedure when permission has been granted.
X3666-Ch12 8/27/07 4:56 PM Page 448

C H A P T E R 12 Medicare 449▼
EXAMPLE ONLY
1a. INSURED’S I.D. NUMBER (For Program in Item 1)
4. INSURED’S NAME (Last Name, First Name, Middle Initial)
7. INSURED’S ADDRESS (No., Street)
ETATSYTIC
ZIP CODE TELEPHONE (INCLUDE AREA CODE)
11. INSURED’S POLICY GROUP OR FECA NUMBER
a. INSURED’S DATE OF BIRTH
b. EMPLOYER’S NAME OR SCHOOL NAME
c. INSURANCE PLAN NAME OR PROGRAM NAME
d. IS THERE ANOTHER HEALTH BENEFIT PLAN?
13. INSURED’S OR AUTHORIZED PERSON’S SIGNATURE I authorizepayment of medical benefits to the undersigned physician or supplier forservices described below.
SEX
F
HEALTH INSURANCE CLAIM FORM
OTHER1. MEDICARE MEDICAID TRICARE CHAMPVA CHAMPUS
READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM.12. PATIENT’S OR AUTHORIZED PERSON’S SIGNATURE I authorize the release of any medical or other information necessary
to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignmentbelow.
SIGNED DATE
ILLNESS (First symptom) ORINJURY (Accident) ORPREGNANCY(LMP)
MM DD YY15. IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS.
GIVE FIRST DATE MM DD YY14. DATE OF CURRENT:
17. NAME OF REFERRING PHYSICIAN OR OTHER SOURCE
19. RESERVED FOR LOCAL USE
21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY. (RELATE ITEMS 1,2,3 OR 4 TO ITEM 24E BY LINE)
17a.
17b. NPI
25. FEDERAL TAX I.D. NUMBER SSN EIN 26. PATIENT’S ACCOUNT NO. 27. ACCEPT ASSIGNMENT?(For govt. claims, see back)
31. SIGNATURE OF PHYSICIAN OR SUPPLIERINCLUDING DEGREES OR CREDENTIALS(I certify that the statements on the reverseapply to this bill and are made a part thereof.)
ETADDENGIS
32. SERVICE FACILITY LOCATION INFORMATION
SIGNED
MM DD YY
OTMORF
OTMORF
MM DD YY MM DD YY
MM DD YY MM DD YY
CODE ORIGINAL REF. NO.
28. TOTAL CHARGE 29. AMOUNT PAID 30. BALANCE DUE
$$$
33. BILLING PROVIDER INFO & PH # ( )
a. b. a. b.
PICA PICA
2. PATIENT’S NAME (Last Name, First Name, Middle Initial)
5. PATIENT’S ADDRESS (No., Street)
ETATSYTIC
ZIP CODE TELEPHONE (Include Area Code)
9. OTHER INSURED’S NAME (Last Name, First Name, Middle Initial)
a. OTHER INSURED’S POLICY OR GROUP NUMBER
b. OTHER INSURED’S DATE OF BIRTH
c. EMPLOYER’S NAME OR SCHOOL NAME
d. INSURANCE PLAN NAME OR PROGRAM NAME
YES NO
( )
If yes, return to and complete item 9 a-d.
16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION
18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES
20. OUTSIDE LAB? $ CHARGES
22. MEDICAID RESUBMISSION
23. PRIOR AUTHORIZATION NUMBER
MM DD YY
CA
RR
IER
PA
TIE
NT
AN
D IN
SU
RE
D IN
FO
RM
AT
ION
PH
YS
ICIA
N O
R S
UP
PL
IER
INF
OR
MA
TIO
N
M F
YES NO
YES NO
1. 3.
2. 4.
FM
SEXMM DD YY
YES NO
YES NO
YES NO
PLACE (State)
GROUPHEALTH PLAN
FECABLK LUNG
Single Married Other
3. PATIENT’S BIRTH DATE
6. PATIENT RELATIONSHIP TO INSURED
8. PATIENT STATUS
10. IS PATIENT’S CONDITION RELATED TO:
a. EMPLOYMENT? (CURRENT OR PREVIOUS)
b. AUTO ACCIDENT?
c. OTHER ACCIDENT?
10d. RESERVED FOR LOCAL USE
Employed Full-Time Part-Time Student Student
Self Spouse Child Other
(Medicare #) (Medicaid #) (Sponsor’s SSN) (Member ID#) (SSN or ID) (SSN) (ID)
( )
M
SEX
FromMM DD YY
ToMM DD YY
1
2
3
4
5
6
$ CHARGES
DATE(S) OF SERVICEPLACE OFSERVICE
PROCEDURES, SERVICES, OR SUPPLIES(Explain Unusual Circumstances)
CPT/HCPCS MODIFIERDIAGNOSISPOINTER
DAYSOR
UNITS
F. H. I. J.24. A. B. C. D. E.
PROVIDER ID. #EMGRENDERING
NPI
NPI
NPI
NPI
NPI
NPI
G.EPSDTFamilyPlan
ID.QUAL.
1500
APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05
NUCC Instruction Manual available at: www.nucc.org PLEASE PRINT OR TYPE APPROVED OMB-0938-0999 FORM CMS-1500 (08-05)
X
Signature on File
F I G U R E 12 – 8 Block 12 of the CMS-1500 (08-05) claim form where the patient signsauthorizing payment to be sent to the physician and Block 27 marked with an X showing thatthe physician accepts Medicare assignment of benefits.
X3666-Ch12 8/27/07 4:56 PM Page 449

physician assistants. Unassigned electronic claims thatare denied have no appeal rights.
Nonpar physicians receive only 95% of the Medicare-approved amount. Nonpar physicians may decide on acase-by-case basis whether to accept assignment. If thenonpar physician accepts assignment for a claim,Medicare pays 80% of the nonpar Medicare-approvedamount directly to the physician and the physician col-lects the remaining 20% from the patient. If the nonparphysician does not take assignment on a particular claim,he or she may “balance bill” the patient 115% of the non-par rate because Medicare will send the payment to thepatient. For example, if the nonpar rate is $100, theprovider can “balance bill” the patient for $115. However,in this case, even though the physician is required to trans-mit the claim to Medicare, the carrier pays the patientdirectly and the physician therefore must collect his orher entire fee from the patient; thus physicians must “chasethe money.” Consequently, physicians should evaluatewhether the ability to “balance bill” and collect a higherfee from the patient is worth the potential extra billing and collection costs. Furthermore, some hospitals andstates—including Minnesota, Pennsylvania, Vermont, andNew York—prohibit or limit balance billing, so physiciansmust ascertain whether or not these restrictions applybefore making a Medicare participation or nonparticipa-tion decision.
Limiting charge is a percentage limit on fees, speci-fied by legislation, that nonpar physicians may bill Medicarebeneficiaries above the allowed amount. Nonpar physi-cians may submit usual and customary fees for assignedclaims. Because of these two situations, nonpar physi-cians usually have a fee schedule that lists both usual feesand limiting charges. Some states have set limitingcharges that are more restrictive than Medicare policies.These states are Connecticut, Massachusetts, New York,Ohio, Pennsylvania, Rhode Island, and Vermont. Inquirefrom the fiscal intermediary of those states for guidelines.
Prior AuthorizationFor Medicare patients who have additional insurance,many insurance carrier group plans and MCO senior plansrequire prior authorization for surgical procedures, diag-nostic testing, and referrals to specialists. Some of theseprocedures requiring authorization are on a mandatorylist, whereas others are chosen by the regional carrier.The mandatory list is composed of procedures such as:
● Bunionectomy● Carotid endarterectomy● Cataract extractions● Cholecystectomy● Complex peripheral revascularization
● Coronary artery bypass graft surgery● Hysterectomy● Inguinal hernia repair● Joint replacements (hip, shoulder, or knee)● Transurethral prostatectomy
Carriers may have a toll-free line to call for authoriza-tion, require the completion of a preauthorization form,or require a letter only if there is a dispute over claimspayment. Check with the local carrier on its policy forpreauthorization.
The prior authorization number is used when billingthe Medicare carrier and is entered on the CMS-1500(08-05) claim form in Block 23 (see Figure 12–6). If theprocedure is not approved, the carrier sends a denial tothe physician, patient, and hospital, if applicable. If theprocedure is done as an emergency, notify the carrierwithin the time frame designated by the insurance planso an authorization can be arranged.
Waiver of Liability ProvisionLimited liability
When a patient is to receive a service from a participat-ing physician that might be denied for medical necessityor because of limitation of liability by Medicare, inform thepatient and have him or her agree to pay for the deniedservice in advance. If the Medicare guidelines or param-eters are not known for a certain procedure or service,refer to Medicare transmittals (formerly called programmemorandums) or call the Medicare carrier and ask. Somemedical practices use a computerized method to screenfor the medical necessity of a service but must have accessto national coverage determinations (NCDs) and localcoverage decisions (formerly called local medical reviewpolicies, or LMRPs) to find out if there is limited coverage.
If you expect Medicare to deny payment (entirely or inpart) instruct the patient to sign an Advance Beneficiary
450 U N I T 3 HEALTH CARE PAYERS▼
ADVANCE BENEFICIARYNOTICES
Medicare considers the appropriate use of AdvanceBeneficiary Notices (ABNs) as a compliance issue. Ask thepatient to sign an ABN document if you know the serviceis not covered or if there is a possibility that a service maybe denied for medical necessity or limitation of Medicarebenefits. A step-by-step procedure of how to complete anABN form is presented at the end of this chapter.
X3666-Ch12 8/27/07 4:56 PM Page 450
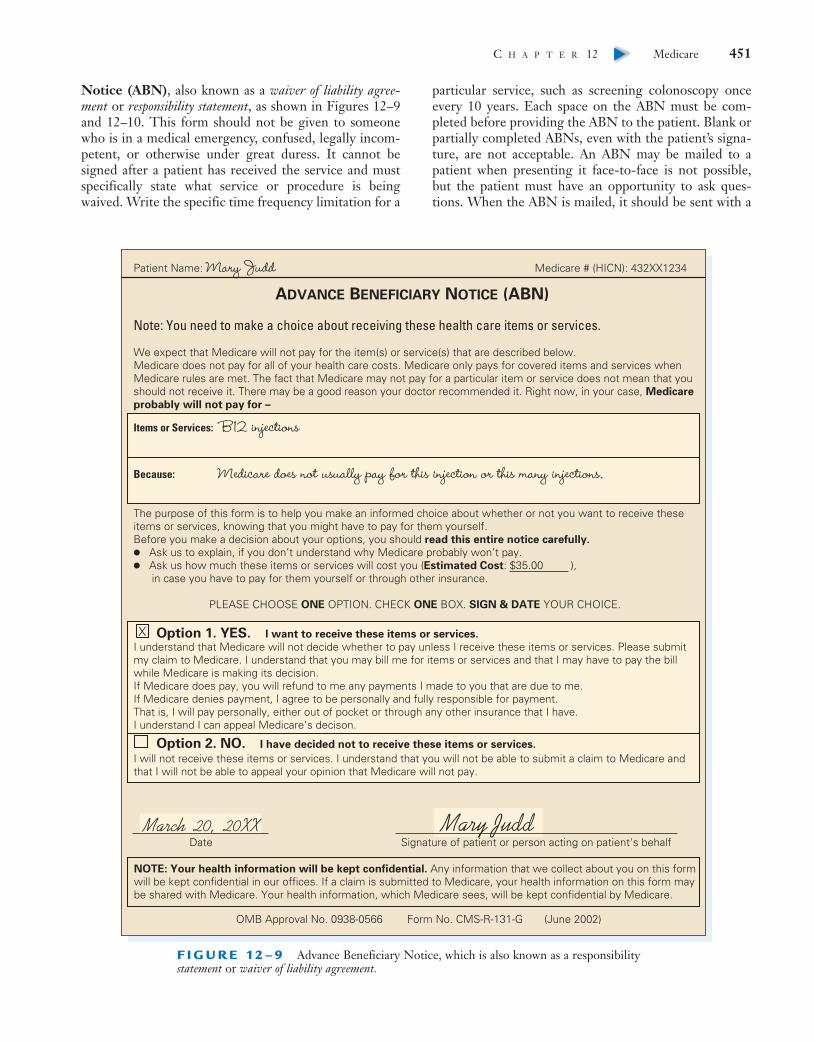
Notice (ABN), also known as a waiver of liability agree-ment or responsibility statement, as shown in Figures 12–9and 12–10. This form should not be given to someonewho is in a medical emergency, confused, legally incom-petent, or otherwise under great duress. It cannot besigned after a patient has received the service and mustspecifically state what service or procedure is beingwaived. Write the specific time frequency limitation for a
particular service, such as screening colonoscopy onceevery 10 years. Each space on the ABN must be com-pleted before providing the ABN to the patient. Blank orpartially completed ABNs, even with the patient’s signa-ture, are not acceptable. An ABN may be mailed to apatient when presenting it face-to-face is not possible,but the patient must have an opportunity to ask ques-tions. When the ABN is mailed, it should be sent with a
C H A P T E R 12 Medicare 451▼
F I G U R E 12 – 9 Advance Beneficiary Notice, which is also known as a responsibilitystatement or waiver of liability agreement.
X3666-Ch12 8/27/07 4:56 PM Page 451
cover letter explaining that the procedure will be deniedby Medicare and include contact information so the patientcan ask questions before the procedure.
To determine which services require an ABN, refer tothe National Coverage Determinations and the LocalCoverage Decisions (LCDs), formerly known as LocalMedical Review Policies (LMRPs) from the insurancecarrier. An office policy should be in place for handlingpatients who refuse to sign an ABN. When sending in aclaim, the Healthcare Common Procedure CodingSystem (HCPCS) level II modifier -GA (waiver of liabil-ity on file) must be added to pertinent codes to indicate apatient has signed the waiver. The Medicare carrier theninforms the patient that he or she is responsible for thefee. Keep this signed waiver with other patient financialdocuments and not with the patient’s health record.
If the service was not reasonable because of Medicareguidelines but the patient thought it was covered andthere is no advance notice given with signed waiver of lia-bility agreement, then:
● The provider cannot bill the patient.● The patient does not have to pay the deductible or
coinsurance.
● The patient is refunded any amount paid to theprovider on the item or service.
If assignment is accepted and the physician and patientthought the service was covered under reasonableassumptions, then:
● Medicare is billed to pay for the service.● The patient must pay the deductible and coinsurance.● Medicare will not seek a refund of money already paid
to the physician.
Nonparticipating providers must refund any amountcollected from the beneficiary when services are laterfound to be not reasonable and necessary.
Noncovered services
Do not get confused with the issue of noncoveredMedicare services because these may always be billed tothe patient. Do not give a patient an ABN when a serviceis never covered by Medicare. Instead give those patientsa different form, the Notice of Exclusions from MedicareBenefits (NEMB) (Figure 12–11). This form clearlystates that the service is never covered by Medicare andthe patient is responsible for payment. It is not a require-ment to give the patient an NEMB for a never-coveredservice in order to bill the patient but use of the formmakes it clear before the procedure is done that he or shemust pay for it. Services denied as inclusive of anotherservice (a payment already made for the other service) arenot considered a noncovered item and may not be billedto the patient. If a formal denial is necessary to bill thepatient or another insurer, a claim should be sent with aletter attached stating the need for the denial to billanother payer.
Elective Surgery EstimateEffective October 1, 1987, under the Tax Reform Act, anonparticipating physician who does not accept assign-ment for an elective surgery for which the actual chargewill be $500 or more must provide the beneficiary withthe following in writing: (1) the estimated fee for the pro-cedure, (2) the estimated Medicare-approved allowancefor the procedure, and (3) the difference in the physi-cian’s actual charge (limiting charge and the allowedamount) (Figure 12–12). The term elective surgery means asurgical procedure that can be scheduled in advance, is notan emergency, and is discretionary on the part of the physi-cian and the patient. Failure to undergo elective surgerydoes not pose a mortality threat. Give a copy of the esti-mation letter to the Medicare patient and keep the orig-inal for the files. Document the patient’s acknowledgmentby obtaining his or her signature at the bottom of the letter.
452 U N I T 3 HEALTH CARE PAYERS▼
F I G U R E 12 – 1 0 Insurance billing specialist instructing an elderly patient to sign an Advance NoticeMedicare Beneficiary Waiver of Liability Agreement for services not covered.
X3666-Ch12 8/27/07 4:56 PM Page 452
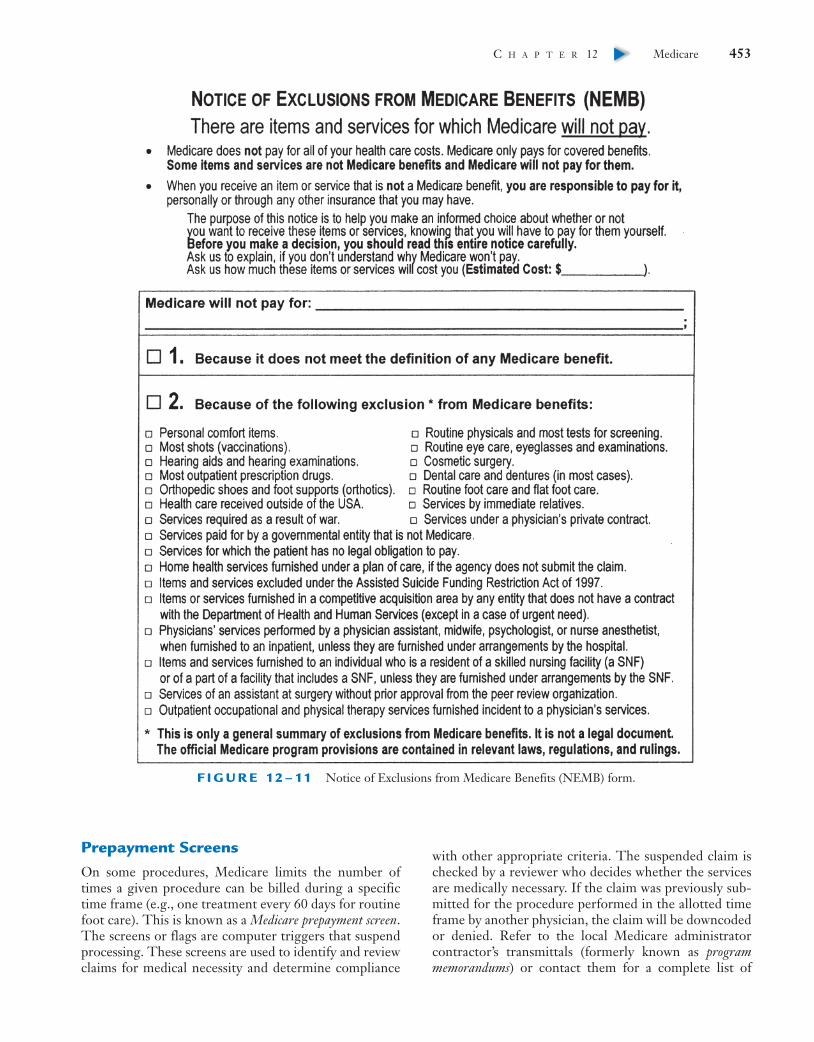
Prepayment ScreensOn some procedures, Medicare limits the number oftimes a given procedure can be billed during a specifictime frame (e.g., one treatment every 60 days for routinefoot care). This is known as a Medicare prepayment screen.The screens or flags are computer triggers that suspendprocessing. These screens are used to identify and reviewclaims for medical necessity and determine compliance
with other appropriate criteria. The suspended claim ischecked by a reviewer who decides whether the servicesare medically necessary. If the claim was previously sub-mitted for the procedure performed in the allotted timeframe by another physician, the claim will be downcodedor denied. Refer to the local Medicare administratorcontractor’s transmittals (formerly known as programmemorandums) or contact them for a complete list of
C H A P T E R 12 Medicare 453▼
F I G U R E 12 – 11 Notice of Exclusions from Medicare Benefits (NEMB) form.
X3666-Ch12 8/27/07 4:56 PM Page 453

the Medicare prepayment screens, which are applicablelocally.
To avoid problems, use good procedure code guide-lines discussed in Chapter 6 and adhere to the followingcriteria:
● The level of service is appropriate to documentation.● The procedure is accurate to the gender of the patient.● The frequency is appropriate.● The diagnosis and procedure match.● The provider has certification for performing services
(e.g., laboratories).● The fee is within the Medicare-approved charge.
Correct Coding InitiativeMedicare’s Correct Coding Initiative (CCI) is imple-mented by CMS in an attempt to eliminate unbundlingor other inappropriate reporting of Current ProceduralTerminology (CPT) codes. As you may recall, unbundlingis coding and billing numerous CPT codes to identifyprocedures that usually are described by a single code.Coding conflicts are picked up and claims are reviewed,suspended, or denied when conflicts occur. Software isavailable to give physicians, private insurance companies,and billing services access to the same government data-base used in auditing physicians for improper use of CPTcodes. It is currently available on the CMS website at
454 U N I T 3 HEALTH CARE PAYERS▼
A
B
F I G U R E 12 – 12 A, Worksheet. B, Sample beneficiary letter for estimatedMedicare payment for elective surgery.
X3666-Ch12 8/27/07 4:56 PM Page 454

no charge. Refer to the Internet Resources at the end ofthis chapter.
MEDICARE REIMBURSEMENTChronology of Prospective Payment SystemFor many years, Medicare payments were based on rea-sonable fees (e.g., the amounts approved by the Medicarecarrier [fiscal agents]). Medicare paid 80% of the approvedcharge. On October 1, 1983, an important development inthe Medicare Part A program, the prospective paymentsystem (PPS), became effective. Under the regulationsenacted by the Social Security Amendments of 1983, hos-pitals treating Medicare patients are reimbursed accordingto preestablished rates for each type of illness treatedbased on diagnosis. Payments to hospitals for Medicareservices are classified according to more than 500 diag-nosis-related group (DRG) numbers. Beneficiaries(patients) cannot be billed beyond the preestablishedDRG rate except for normal deductible and copaymentamounts. (See Chapter 17 for an in-depth discussion of DRGs.)
In 1984, the Deficit Reduction Act established a partic-ipating physician program that offered incentives to par-ticipating physicians and froze the fees of nonparticipatingphysicians. The 1987 Omnibus Budget Reconciliation Act(OBRA) introduced the maximum allowable actual charge(MAAC) formula, which developed the maximum fee(limiting charge) that a nonpar physician could chargeMedicare patients for each service.
Reasonable FeeReasonable fee is the amount that Medicare participat-ing providers agree to accept. It is listed on the RA, for-merly known as the EOB, as an allowed (approved) chargefor a procedure. This charge may be higher or lower thanthe fee the physician lists on the claim. When a physicianaccepts assignment, he or she may bill the patient only20% of the Medicare-allowed charge. Charging for com-pletion and submission of a claim form on an assignmentclaim violates the terms of the assignment. Interest feescannot be assessed to Medicare patients. It is permissibleto collect the deductible at the time of service if youknow how much of the deductible has already been paid;but the Medicare copayment should not be collecteduntil Medicare pays.
Mandatory assignment laws have been adopted in several states, and legislation is under consideration andpending in many more states. These state laws wouldrequire physicians to accept the approved charge for theirMedicare patients as a condition for being licensed to
practice medicine in the state. Arkansas, Florida, Illinois,Maryland, Montana, and New Hampshire have rejectedmandatory assignment proposals.
Resource-Based Relative Value ScaleAs mentioned in Chapter 6, a resource-based relativevalue scale (RBRVS) is the system Medicare uses forestablishing fees. This system takes into account work,overhead expense, and malpractice values for all CPT codesthat are published in the Federal Register each November.These are adjusted for each Medicare local carrier bygeographic practice cost indices (GPCI) by using a formulathat gives the total value for a code.
The formula for obtaining the allowed amount of agiven service or procedure is to choose an HCPCS/CPTcode and use the relative value unit (RVU) amounts listedin the Federal Register for work value, practice expense,and malpractice value and multiply each of those by theGPCI. Then to obtain the total adjusted RVU, add thethree amounts together. Finally, to discover the allowedamount for this code, multiply the annual Medicare con-version factor (CF) by the HCPCS/CPT code’s totaladjusted RVU amount. For a graphic illustration of thisformula, see Figure 6–2. To give you experience in usingthis formula, do the assignments relating to RBRVS forthis chapter in the Workbook.
To eliminate having to spend time in establishing feesand using the formula, many medical practices use a feeanalyzer for their geographic area.
Healthcare Common Procedure Coding System (HCPCS)As mentioned in Chapter 6, the federal governmentdeveloped the Healthcare Common Procedure CodingSystem (HCPCS) for the Medicare program. To obtaincorrect payment for a procedure or service, a code num-ber must be selected from level I or II of HCPCS cod-ing system. To review, the Medicare HCPCS levels ofcoding are:
● Level I: the AMA CPT codes and modifiers (nationalcodes)
● Level II: CMS-designated codes and alpha modifiers(national codes)
When transmitting a claim, be sure to use the level II HCPCS national alphanumeric codes andmodifiers rather than CPT procedure codes for certainappliances and procedures when indicated. When billingCPT modifiers, a good reference is presented in Table 6.6,as helpful hints in italics entitled “Medicare PaymentRule.”
C H A P T E R 12 Medicare 455▼
X3666-Ch12 8/27/07 4:56 PM Page 455

Physician Quality Reporting InitiativeThe Tax Relief and Health Care Act of 2006 authorizedthe Physician Quality Reporting Initiative (PQRI),which is a pay-for-reporting program for providers whobill under Medicare Part B. This financial incentive pro-gram is for eligible professionals who choose to partici-pate and successfully report on a designated set of qualitymeasures for services paid under the Medicare PhysicianFee Schedule and furnished between July 1, 2007, andDecember 31, 2007. The services must be reported usingtemporary G-codes and/or CPT category 2 codes. Thesecodes should be added to claims to reflect elements ofquality of care delivered during the encounter with thepatient. Participants may receive a bonus payment of1.5% of their charges, subject to a cap. No enrollment orregistration is required. To find additional informationabout the PQRI, such as eligible professionals, G-codes,and forms used for documenting patient encounters,refer to the Internet Resources at the end of this chapterand visit the Evolve website, which has an active link tothe Centers for Medicare and Medicaid Services.
CLAIM SUBMISSIONLocal Coverage DeterminationLocal Coverage Determination (LCD), formerly knownas Local Medical Review Policy (LMRP), is a decision bya Medicare administrative contractor whether to cover aparticular service on a contractor-wide basis in accor-dance with the Social Security Act (SSA) (i.e., a determi-nation as to whether the service is reasonable andnecessary). LCD is an educational and administrativetool to assist physicians, providers, and suppliers in trans-mitting correct claims for payment. Contractor medicaldirectors and staff develop LCDs with input from thepublic. LCDs list covered and noncovered codes for agiven Medicare policy but do not include any of the cod-ing guidance that were found in LMRPs. LCDs outlinehow contractors will review claims to determine whetherMedicare coverage requirements have been met. CMSrequires that local policies be consistent with national guid-ance. Use of LCDs helps avoid situations in which claimsare paid or denied without a full understanding of the basisfor payment and denial. LCDs may be obtained from theMedicare carrier website at www.cms.hhs.gov/mcd.
Medicare Administrative Contractorsand Fiscal IntermediariesAn organization handling claims from hospitals, NFs,intermediate care facilities (ICFs), long-term care facil-ities (LTCFs), and home health agencies is called a fiscalintermediary (FI). The National Blue Cross Association
holds the fiscal intermediary contract for Medicare Part A;in turn, it subcontracts it out to member agencies.
Organizations handling claims from physicians andother suppliers of services covered under Medicare Part Bare called Medicare administrative contractors (MAC),formerly called fiscal agents. Medicare Part B paymentsare handled by private insurance organizations undercontract with the government. Since January 1, 1992, therule for where to send a Medicare claim is to bill the car-rier who covers the area where the service occurred orwas furnished, not the carrier who services the physician’soffice.
See Internet Resources at the end of this chapter to goto the Evolve website to access the active link for thenames and addresses for claims submission in each stateand to obtain further information about this program.
Provider Identification NumbersAnother requirement of the Tax Reform Act was theestablishment of several types of identification numbersfor each physician and nonphysician practitioner provid-ing services paid by Medicare. Because there are so manynumbers, they are easily confused and end up being the source of many errors when completing blocks on the CMS-1500 (08-05) claim form. The numbers definedand shown in template examples with correct placementin Chapter 7 follow:
● Provider identification numbers (PINs), group andindividual. With the implementation of the NationalProvider Identifier on May 23, 2007, PINs are nolonger used.
● Unique physician identification numbers (UPINs).With the implementation of the National ProviderIdentifier on May 23, 2007, UPINs are no longer used.
● National provider identifier (NPI) assigned by theCenters for Medicare and Medicaid Services (CMS)was implemented on May 23, 2007.
● Durable Medical Equipment (DME) supplier number.
Patient’s Signature AuthorizationSignatures for transmitting electronic claims and accept-ance of financial responsibility must be obtained andretained in the office records because there are no hand-written signatures on electronic claims. A form created bythe medical practice may be used or a Medicare patient’ssignature may be obtained in Block 12 of the CMS-1500(08-05) claim form. This block should be signed regard-less of whether the physician is a participating or non-participating physician. The signed authorization should be kept on file in the patient’s health record for an epi-sode of care or for a designated time frame (e.g., 1 year).
456 U N I T 3 HEALTH CARE PAYERS▼
X3666-Ch12 8/27/07 4:56 PM Page 456

Claims may indicate “Signature on file” or “SOF” inBlock 12 of the claim form. Further information on thistopic may be found in Chapters 3, 7, and 8.
Signature on file situations that may occur in a medicalpractice are follow:
● Illiterate or physically handicapped. When an illiter-ate or physically handicapped enrollee signs by mark(X ), a witness should sign his or her name and addressnext to the mark. If the claim is filed for the patient byanother person, that person should enter the patient’sname and write “By,” sign his or her own name andaddress, indicate relationship to the patient, and statewhy the patient cannot sign.
● Confinement in a facility. Sometimes it is not possibleto obtain the signature of a Medicare patient becauseof confinement in a nursing facility, hospital, or home.In such cases, physicians should obtain an annual sig-nature authorization from the patient.
● Medigap claim. When transmitting a crossover claimto a Medigap carrier, annually obtain a signatureauthorization for the Medigap carrier.
● Deceased patient. Refer to Deceased Patient Claimslater in this chapter for signature requirements.
● Medicare/Medicaid (Medi-Medi) claim. These cross-over claims do not require the patient’s signature.
Time LimitThe time limit requirement for sending in claims is theend of the calendar year after the fiscal year in whichservices were furnished. The fiscal year for claims beginsOctober 1 and ends September 30 (see the following box).
On assigned claims, the provider may file withoutpenalty up to 27 months after providing service if reason-able cause for the delay is shown to the insurance carrier.Otherwise there is a 10% reduction in the reimburse-ment. On unassigned claims, the provider may be finedup to $2000 for delinquent claim submission or bedropped from Medicare. When transmitting a late claim,ask the fiscal intermediary for the guidelines that CMSconsiders reasonable cause for delay.
Paper ClaimsThe form that physicians use to submit paper claims toMedicare is the CMS-1500 (08-05). Refer to Chapter 7
for instructions on how to complete the CMS-1500 (08-05) claim form for the Medicare program. The refer-ence templates (samples of completed claim forms) forMedicare and supplemental coverage shown at the end ofthat chapter are as follows:
● Medicare, no secondary coverage: Figure 7–8● Medicare/Medicaid, crossover: Figure 7–9● Medicare/Medigap, crossover: Figure 7–10● Other insurance/Medicare MSP: Figure 7–11
Patients are not allowed to submit claims to Medicare(with four exceptions). Situations when a patient may filea claim are the following:
● Services covered by Medicare for which the patienthas other insurance that should pay first, called MSP
● Services provided by a physician who refuses to trans-mit the claim
● Services provided outside the United States● Situations in which durable medical equipment is pur-
chased from a private source
Medicare claim status is also explained in detail inChapter 7 (e.g., clean, incomplete, rejected, dirty, andother claims). To obtain the mailing address for sendingMedicare claim forms for your state or county, go to theInternet website http://www.cms.hhs.gov/contacts/incardir.asp. For further information and booklets, pamphlets, and the annual Medicare Handbook, contactthe nearest Social Security office.
Electronic ClaimsMedicare requests that all providers transmit claims elec-tronically. All electronic transmission formats are sched-uled to be standardized by the use of ANSI ASC X12N(837) Version 4010. Refer to Chapter 8 for informationon how to transmit claims electronically to the Medicarecarrier.
Medicare/Medicaid ClaimsMedi-Medi patients qualify for the benefits of Medicareand Medicaid. Use the CMS-1500 (08-05) claim formand check “Yes” for the assignment in Block 27. If thephysician does not accept assignment, then payment goesto the patient and Medicaid (in California Medi-Cal) willnot pick up the residual. The CMS-1500 (08-05) claimform will be crossed over and processed automatically byMedicaid after processing is completed by Medicare. Thefiscal intermediary may refer to this as a crossover claim,or claims transfer. It is not necessary to submit anotherform. Claims should be sent according to the time limitdesignated by the Medicaid program in the state. Generallythe Medicare payment exceeds the Medicaid fee schedule,
For services furnished on: The time limit for filing is:October 1, 2005, to December 31, 2007September 30, 2006October 1, 2006, to December 31, 2008September 30, 2007
C H A P T E R 12 Medicare 457▼
X3666-Ch12 8/27/07 4:56 PM Page 457

and little or no payment is received except when the patienthas not met his or her annual Medicare deductible.
In some states, the fiscal intermediary for a crossoverclaim may have a different address from that used for theprocessing of a patient who is on Medicare only. Write orcall the nearest Medicare fiscal intermediary for theguidelines pertinent to the state.
Medicare/Medigap ClaimsMedicare has streamlined the processing of Medicare/Medigap claims in most states. Medicare carriers transmitMedigap claims electronically for participating physicians,thus eliminating the need to file an additional claim. Thisis also called a crossover claim. Medigap payments go directlyto the participating physicians, and a Medicare SummaryNotice is sent to the patient that states “This claim has beenreferred to your supplemental carrier for any additionalbenefits.”
To assure the crossover of the Medicare/Medigap claim,complete Blocks 9 through 9d of the CMS-1500 (08-05)claim form and list the PAYRID number of the Medigapplan in Block 9d. The PAYRID for Medigap plans isreferred to as the Other Carrier Name and Address(OCNA) number, and a list of all OCNAs is published inthe Medicare newsletter.
If automatic crossover capabilities are not offered inone’s state, attach the Medicare RA to the claim form andelectronically transmit or submit a claim to the Medigapplan separately.
Refer to Figure 7–10 for submitting claims whenMedicare is primary and the patient has a Medigap (sup-plemental) policy.
Medicare/Employer SupplementalInsurance ClaimsSome individuals have supplemental coverage with com-plementary benefits by employment plans even after retire-ment. In some cases, this coverage may be paid by a formeremployer after retirement. Usually crossover relationshipsexist with many insurance carriers who insure Medicarebeneficiaries.
Medicare/Supplemental and MSP ClaimsCompleting the CMS-1500 (08-05) claim form for aMedicare patient who has supplemental insurance can beconfusing. First, decide whether the case is Medicare pri-mary or secondary payer. The procedure on determiningwhether Medicare is primary or secondary is presented at
the end of this chapter. If Medicare is primary and the secondary payer is a Medigap policy, follow Medicare/Medigap processing guidelines. After determining who isprimary, follow the directions on what should be enteredin each block of the CMS-1500 claim form, depending onthe primary payer, or follow MSP guidelines.
Templates (samples of completed claim forms) shownat the end of Chapter 7 make it easier to learn whichblocks to complete and which to ignore, depending onthe primary and secondary payer. Figure 7–11 is forbilling other insurance primary and Medicare secondary(MSP). A copy of the front and back sides of the primaryinsurance’s EOB document must be attached to the claimwhen billing Medicare.
See Chapter 7 for general instructions for completingclaims in Medicare and Medicare secondary payer cases.
Claims for Deceased PatientsThere are two ways in which to submit billing for apatient who has died:
1. Participating physician accepts assignment on the claimform. This results in the quickest payment. No signatureby a family member is needed on the CMS-1500 (08-05)claim form. Type “Patient died on (indicate date)” inBlock 12 where the patient’s signature is necessary.
2. The nonparticipating physician does not acceptassignment, bills Medicare, and submits the following:a. A CMS-1500 (08-05) claim form signed by the
estate representative who is responsible for the billb. A statement or claim for all services providedc. Name and address of the responsible partyd. Provider’s statement, signed and dated, refusing to
accept assignment
Nothing can be done about the open balance on the account until the estate is settled, and then Medicarewill pay.
Physician Substitute CoverageMany times special substitute coverage arrangements aremade between physicians (e.g., on-call, vacation, or unavail-able because of another commitment). These arrangementsare referred to as either reciprocal for on-call situations orlocum tenens for a vacation situation. Specific modifiersare used to distinguish these situations, and special billingguidelines are stated as follows:
● Reciprocal arrangement. When transmitting Medicareclaims, the regular physician must identify the serviceprovided by the substitute doctor by listing the -Q5modifier after the procedure code.
458 U N I T 3 HEALTH CARE PAYERS▼
X3666-Ch12 8/27/07 4:56 PM Page 458

● Locum tenens arrangement. When transmitting Medicareclaims, the regular physician must identify the serviceprovided by the substitute doctor by listing the -Q6modifier after the procedure code.
AFTER CLAIM SUBMISSIONRemittance AdviceMedicare sends a payment check and a nationally stan-dardized document to participating physicians called aMedicare remittance advice (RA), formerly known asan explanation of Medicare benefits (EOMB). On the frontside of the RA are status codes that are the same nation-wide, representing the reason a claim may not have beenpaid in full or was denied, and so forth. These codes aredefined on the reverse side of the RA. If the patient hasMedigap, supplementary, or complementary crossovercoverage, the “other payer” statement will say whether theclaim has been transferred to the supplemental insurer.
Nonparticipating physicians also receive an RA withpayment information about unassigned claims. The RAwill separate payment information about assignedclaims from unassigned claims to avoid posting errorsby the practice. Check the payment against the feeschedule to determine whether the benefits are for thecorrect amount. On each claim form, note the date thepayment is posted for reference. Optional items to doc-ument are amount of payment, RA processing data, andbatch number.
Offices transmitting claims electronically receive anelectronic remittance advice (ERA) showing paymentdata, and this may be automatically uploaded into theoffice computer system. The ERA electronically postspayments, and the provider does not have to manuallypost them. Paper and electronic remittance notices havethe same format.
Medicare Summary NoticeA patient is mailed a similar document called a Medicaresummary notice (MSN). This document is designed tobe easier for the patient to understand, but because manypatients do not know what is meant by amount charged,Medicare approved, deductible, and coinsurance, it oftenbecomes necessary for the insurance billing specialist toeducate the patient. First, photocopy an RA to be used asan example, deleting the patient’s name to ensure confi-dentiality. Then use the RA to illustrate to future patientswhat various terms mean. This will increase patientunderstanding and save time.
When a claim is denied, the MSN will identify the number of the Local Coverage Decision (LCD) or
National Coverage Decision (NCD) used in denial of the claim.
BENEFICIARY REPRESENTATIVE/REPRESENTATIVE PAYEEMedicare beneficiaries may have memory impairment or may be confined to a wheelchair or bed so they have a legal right to appoint an individual to serve as their representative.
Claims assistance professionals (CAPs) act as clientrepresentatives. They have some legal standing and arerecognized by Medicare to act on the beneficiary’s behalfif the beneficiary completes a Beneficiary RepresentativeForm SSA-1696. This form is available from the SocialSecurity district office. Copies of the completed formshould be sent to the Medicare intermediary or carrierwhen appropriate.
In contrast, a representative payee is an individual ororganization chosen by the SSA to receive and adminis-ter SSA benefit funds on behalf of the beneficiary. Otherduties consist of assisting the beneficiary with check writ-ing for financial obligations, such as personal care andmaintenance, housing, medical service expenses, andinvesting any surplus monies for the beneficiary’s benefit.A representative payee is responsible for using paymentsreceived only for the benefit of the beneficiary, account-ing for the benefits received on request, and contactingSSA when anything affects eligibility for SSA benefits orprevents the representative payee’s ability to performthese responsibilities. Additional information on CAPs isfound in Chapters 1 and 18.
Posting PaymentsUsually a physician’s charge is higher than the chargeapproved by the Medicare carrier or fiscal agent. Thisdoes not mean that his or her charges are unreasonable.As mentioned, payments are established using a feeschedule based on an RBRVS, a volume performancestandard (VPS) for expenditure increases, and a limitingcharge for nonparticipating physicians. Volume perform-ance standard is the desired growth rate for spending onMedicare Part B physician services that is set each year byCongress.
Because some services may be disallowed or the pay-ments on them may be lower than those charged by thephysician, know how to post payments to the patient’sfinancial accounting record card or computerized account.Figure 12–13 illustrates how payments and contractual orcourtesy adjustments are posted. The word courtesy impliesthat Medicare patients are treated well and is preferred tophrases such as “not allowed” or “write-off.”
C H A P T E R 12 Medicare 459▼
X3666-Ch12 8/27/07 4:56 PM Page 459

Medicare does not allow for the standardized waivingof copayments. Medicare regulations require that apatient be billed for the copayment at least three timesbefore the balance is adjusted off as uncollectable.Document this as further justification if the patient is suf-fering financial hardship.
When an RA is received, it may list many patients(Figure 12–14). Do not post the entire payment made ina lump sum to the daysheet. Individually post each lineitem paid to the patient’s financial accounting record cardor computerized account and to the daysheet (Figure12–15). To prevent funds from going astray, some officesprefer to post Medicare payments to a separate daysheetand deposit each multiple reimbursement check sepa-rately. The daysheet totals will then agree with thedeposit slip totals and not get confused with othermonies collected.
Figure 12–16, A, illustrates an example of aMedicare/Medicaid case after payment by Medicare.Medicare applied the patient’s full $131 deductibleamount to the Medicare-allowed amount, reducing pay-ment to $4. The Medicaid RA (see Figure 12–16, B)shows reimbursement of the coinsurance and deductibleamounts dual-billed to Medicaid.
Calculations are shown in the following box:
Medicare Medicaid$136 Allowed amount $136 Medicare allowed −131 Deductible amount$ 5 Balance on which −32 Medicaid cutback
payment is $104 Medicaid allowed× .80 calculated$ 4 Medicare paid 80% −4 Medicare paid
$100 Medicaid payment
460 U N I T 3 HEALTH CARE PAYERS▼
F I G U R E 12 – 13 Electronically generated financial accounting record (ledgercard) illustrating how payments and contractural or courtesy adjustments should be posted.
Please Charge My:
COLLEGE CLINIC4567 Broad Avenue
Woodland Hills, XY 12345-0001Telephone: 555-486-9002
Fax: 555-487-8976JOHN SMITH100 James StreetWoodland Hills, XY 12345-0001
JOHN SMITH
The following items have been responded to by your insurance and are now due:
03/30/06 CI 99214 EST PT LEVEL 4 100.0005/04/06 CI ––––– MEDICARE CHECK 4.24�
05/04/06 CI ––––– MEDICARE COURTESY ADJUSTMENT 9.71�
05/04/06 App. to deduct: $84.9905/09/06 CI ––––– B/C #2 PMT 1.06�
Totals for 03/30/06 services: 100.00 15.01� 84.99
1-04140
COLLEGE CLINIC
GASTON INPUT, MDJOHN SMITH
05/24/06 05/09/06 84.99 84.990.00 0.00 0.001.06
Medicare - BLUE CROSS 1-04140
84.99
05/24/06
PLEASE DETACH AND RETURN THIS PORTION WITH YOUR REMITTANCE
PLEASE KEEP THIS PORTION FOR YOUR RECORDS
Billing Date Payment Due
Responsible Party
Patient
Patient:
Insurance: Account:
Date
BillingDate
LastPayment
PaidOn
Current Over60
Over90
Over120
BalanceDue
Doc Code Diag Description of Service Charge Payments Balance
Provider:
Account:
Make Checks Payable To:
Amount:
Card #:
Expiration:
Signature:
Code:
Visa/MC Amex Discover
Amount Enclosed
Please Pay
This Amount
X3666-Ch12 8/27/07 4:56 PM Page 460

C H A P T E R 12 Medicare 461▼
1. D
ate
of c
heck
and
sta
tem
ent.
12. T
his
is t
he c
heck
num
ber
on t
he
pa
ymen
t is
sued
for
the
clai
ms
in
clud
ed o
n th
is s
tate
men
t.
11. A
mou
nt o
f ch
eck.
Thi
s is
the
tot
al
am
ount
of
the
chec
k at
tach
ed a
nd
re
pres
ents
pay
men
t fo
r al
l cla
ims
in
clud
ed o
n th
is s
tate
men
t.
10. N
umbe
r of
cla
ims.
Thi
s fig
ure
re
pres
ents
the
tot
al n
umbe
r of
clai
ms
incl
uded
on
this
sta
tem
ent.
9. C
o-in
sura
nce.
Thi
s co
lum
n lis
ts t
he
20
% c
o-in
sura
nce
amou
nt fo
r cl
aim
s
incl
uded
on
this
sta
tem
ent.
8. D
educ
tible
. Thi
s co
lum
n lis
ts a
ny
de
duct
ible
app
lied
for
clai
ms
incl
uded
on t
his
stat
emen
t.
7. R
educ
tions
or
deni
als
of c
harg
es c
an
be
exp
lain
ed b
y m
atch
ing
thes
e nu
mbe
rs
to
the
num
bere
d ex
plan
atio
ns o
n
the
back
of
the
RA
.
6. P
roce
dure
cod
e-m
odifi
er. T
hese
cod
es
an
d m
odifi
ers
desc
ribe
serv
ices
ren
dere
d
as b
illed
by
you
or a
s lis
ted
in t
he
C
alifo
rnia
Sta
ndar
d N
omen
clat
ure.
5. M
edi-C
al n
umbe
r, or
spe
cial
not
atio
n,
w
hen
appl
icab
le.
4. C
laim
con
trol
num
ber.
Ref
er t
o th
is
nu
mbe
r w
hen
inqu
iring
abo
ut a
par
ticul
ar
cl
aim
.
3. N
ame
of s
uppl
ier
perf
orm
ing
serv
ices
if
no
t th
e sa
me
as t
he p
hysi
cian
/sup
plie
r
billi
ng fo
r th
e se
rvic
es.
2. P
atie
nt’s
nam
e an
d M
edic
are
num
ber.
ME
DIC
AR
E R
EM
ITTA
NC
E A
DV
ICE
Tran
sam
eric
a O
ccid
enta
l Life
Insu
ranc
e C
ompa
ny
#223
13 W
3276
FAM
PR
AC
ME
DS
EP
19,
20X
XB
EN
EFI
CIA
RY
NA
ME
M.I.
C. N
O.
PE
RFO
RM
ING
SU
PP
LIE
RS
ER
VIC
E
FRO
MM
O-D
AYTO
DAY
-YR
PLA
CE
TYP
E
PR
OC
ED
UR
EA
MO
UN
TB
ILLE
DA
MO
UN
TA
PP
RO
VE
DD
ED
UC
TIB
LE 2080
4482
6
CO
INS
UR
AN
CE
PAY
ME
NT
NO
TE
BIL
LED
AP
PR
OV
ED
DE
DU
CTI
BLE
CO
INS
UR
AN
CE
PAY
ME
NT
CLA
IMS
CO
DE
-MO
DIF
IER
SC
ON
TRO
L N
UM
BE
R
NO
TE
20
9:
CL
INIC
AL
LA
BO
RA
TOR
Y P
RO
CE
DU
RE
S W
E W
ER
E P
AID
AT
10
0%
OF
TH
E A
PP
RO
VE
D A
MO
UN
T.E
XP
LA
NA
TIO
N
A N
EW
LA
W H
AS
RE
DU
CE
D Y
OU
R M
ED
ICA
RE
PA
YM
EN
T B
y 1
% F
OR
SE
RV
ICE
S F
RO
M 0
3/0
1/8
6 T
HR
OU
GH
09
/30
/86
ON
QU
EST
ION
S R
ELA
TED
TO
TH
IS P
AYM
EN
T:T
OTA
LS
499-
XX
-t48
7-A
EX
544
458
6246
-080
-860
61.0
011
020
9005
0
** T
OTA
LS**
** T
OTA
LS**
*
9900
0
9900
0
9900
093
000
9007
0
9008
0-22
6921
0
** T
OTA
LS**
*
8100
0-X
L
8100
0-X
L71
020
J011
0A
4460
** T
OTA
LS**
*
** T
OTA
LS**
*
* *
* *
* *
* *
1 A
1 A
1 A
1 A
1 A
1 A
* *
1 B
1-E
1-E
1-E
1-E
1-E
1-D
61.0
0
28.0
028
.00
17.0
017
.00
17.0
0
17.0
0
10.0
0
10.0
0
11.0
032
5.00
61.0
026
.00
73.0
0
120.
0038
.00
46.0
0
42.0
0
43.3
056 56
**
ME
DI-
CA
L :
56
10-9
49
93
41
45
734
.29
8.66
0.00
**
ME
DI-
CA
L :
56
14
-03
75
19
50
50
20.5
95.
200.
00
2.38
0.60
0.00
40.7
88.
860.
00
154.
6737
.62
0.00
56 56 209
106 6 6 56 56 20965656 6
106
43.3
0
26.0
026
.00
3.00
3.00
3.00
3.00
5.75
5.75
10.0
019
3.85
504.
0025
2.71
60.9
40.
005
316.
20
43.3
03.
00
50.0
5
61.8
025
.00
41.3
0
42.0
0
EX
149
6260
-078
-640
EX
126
6254
-194
-800
6258
-701
-250
6254
-194
-790
EX
195
EX
126
L. W
ILS
ON
458-
07-7
080-
AM
. MIR
ELE
464-
40-3
930-
AM
. MIR
ELE
464-
40-3
930-
A
R. W
ALL
042-
16-3
112-
A
08-2
5 25
-XX
08-2
5 25
-XX
08-2
5 25
-XX
09-0
8 08
-XX
09-0
8 08
-XX
09-0
8 08
-XX
09-0
8 08
-XX
09-0
8 08
-XX
09-0
8 08
-XX
08-1
9 19
-XX
09-0
8 08
-XX
09-0
5 05
-XX
Tra
nsa
me
rica
Occ
ide
nta
l L
ife
A FIG
UR
E 1
2–
14
Med
icar
e re
mitt
ance
adv
ice
(RA
) doc
umen
t. A
,Fro
nt. I
nsur
ance
car
rier
s ar
e re
quir
ed to
use
Cen
ter
for
Med
icar
e an
d M
edic
aid
Serv
ices
mes
sage
s fo
r M
edic
are
RA
, but
eac
h ca
rrie
r ha
s its
ow
n co
de n
umbe
rs to
den
ote
the
mes
sage
s.
Con
tinue
d
X3666-Ch12 8/27/07 4:56 PM Page 461

462 U N I T 3 HEALTH CARE PAYERS▼
1 – See enclosed letter. 2 – Claim was filed after the time limit. 4 – These bills are handled by a special intermediary. 5 – This payment is for an adjustment of a previous claim. 6 – Charges over the maximum Medicare allowance are not covered. 7 – Services before Medicare entitlement are not covered. 8 – Services after Medicare entitlement ended are not covered.10 – Other charges submitted with this claim may be on a separate statement which you have received or will receive soon.12 – Routine examinations and related services are not covered.13 – Immunizations or other routine and preventative services are not covered.16 – We need an itemization of this charge. Please resubmit your claim with this information.17 – Prescription drugs are not covered.18 – Charges for this physician/supplier are not covered.19 – We need a full description of the service or supply to consider this charge. Please resubmit your claim with this information.23 – We need a written report for this service. Please resubmit your claim with this information.26 – More than $312.50 annual psychiatric expense is not covered.27 – We need from the prescribing physician the specific length of time this medical equipment is needed. Please resubmit your claim with this information.30 – This charge was previously considered.37 – Claims for these services will be made by a home health agency or hospital.39 – Equipment that is not medically necessary is not covered. (See Note 89)42 – These supplies or services are not covered.45 – Over 621/2% of psychiatric expenses is not covered.46 – Routine foot care is not covered.47 – Routine eye examinations or eye refractions are not covered.48 – Partial payment of this claim was made to the beneficiary.49 – This service cannot be considered until the hospital makes the necessary arrangement with the carrier for its processing.50 – The beneficiary is not responsible for this reduction/denial under the assignment agreement.54 – Care before and/or after surgery is included in the surgery benefit. (See Note 50)56 – This is the full charge allowed based upon the prevailing or usual and customary rate.62 – Payment has been reduced because this test is commonly part of an automated test group. (See Note 50)66 – This service is not covered when done by this laboratory.70 – There were no charges or bills with your claim form. Please resubmit your claim with this information.72 – We need a signed and dated prescription showing medical necessity and specific length of time needed. Please resubmit your claim with this information.73 – Before another month’s payment can be made, we need a new signed and dated prescription showing further necessity of the medical equipment and specific length of time needed.80 – We need to know the place of service to consider this charge. Please resubmit your claim with this information.
83 – SSA advises us that they are unable to verify the patient’s eligibility for Part B Medical Insurance Plan. For this reason, no payment can be made on this claim. 84 – The patient’s HIC number shown on this claim was incorrect. Please use the correct HIC number on all future claims. 85 – The patient’s name shown on this claim was incorrect. Please use the correct name on all future claims. 86 – Over 621/2% of the allowable charges for psychiatric services is not covered. 89 – If you did not know that Medicare does not pay for this medical service, you may request a review of this decision. See below paragraph entitled “Your right to review of a case.” 90 – This service by a chiropractor is not covered. 93 – Over $500.00 annual expense billed by a physical therapist is not covered. 95 – These specific services by this supplier are not covered. 96 – Please verify the date of this service. Resubmit your claim with this information. 99 – We need a complete diagnosis before the claim can be considered. Please resubmit your claim with this information.106 – The Medicare covered services on this claim have been forwarded for additional processing under Medi-Cal.107 – This claim was not forwarded for Medi-Cal processing. Please bill Medi-Cal directly and attach a copy of this statement.108 – The bills for these services have been transferred to Blue Shield of California Medicare Claims, Chico, CA 95976. You will hear from them.129 – Payment for services prior to July 1 is based on the previous year’s payment rate.131 – Payment for this physician service in a hospital department is reduced since this service is commonly performed in the physician’s office. (See Note 50)138 – This amount is more than Medicare pays for maintenance treatment of renal disease.147 – This charge is not covered because an allowance for purchase of the same equipment was previously made.151 – Your claim was transferred to a Health Maintenance Organization for processing.153 – These are more visits (treatments) for this diagnosis than Medicare covers unless there were unusual circumstances. (See Note 89)154 – This service is not covered for your patient’s reported condition. (See Note 89)155 – Only one visit per month to a nursing home is covered unless special need is indicated. (See Note 89)156 – This laboratory test for the reported condition and/or illness is not covered. (See Note 89)158 – Procedures whose effectiveness has not been proven are not covered. (See Note 89)161 – The frequency of services for this condition are not covered. (See Note 89)162 – More than one visit per day for this condition are not covered. (See Note 89)172 – This type of services billed by a psychologist are not covered.179 – The amount for this service is included in the approved amount for the consultation/office/hospital visit.181 – Payment for this service is included in the major surgical fee.
187 – We need the name and address of the individual doctor who performed this service. Please resubmit your claim with this information.192 – Medicare benefits have been reduced because the patient’s employer group health plan has paid some of these expenses.198 – A claim must be sent to the patient’s employer group health plan first. After the claim has been processed by that plan, resubmit this claim with the bills and the notice the other insurance company sent you.203 – Clinical laboratory services. Blood Gas Studies and Rhythm Strips (1–3 leads) furnished in a hospital setting are reimbursed through the hospital.205 – The date of this service is after the patient’s expiration date provided to us by SSA. If service was rendered to this patient on this date, have the patient’s estate contact the local Social Security Office for assistance.206 – For payment, these services must be billed by the performing laboratory with the assignment accepted.213 – We did not send this claim to Medicaid. Please send this statement and a copy of the claim to the agency that handles Medicaid in your area.216 – This service or item cannot be processed until your application for a Medicare provider identification number is received and approved.218 – Since you are Medicare participating, we have processed this claim as assigned. Future claims must be billed on assignment. If the bill was paid in full, you must immediately refund the amount due to the beneficiary.219 – We need this charge submitted on your letterhead bill. Please resubmit your claim with this information.221 – The name and Medicare number submitted on this claim do not match. Please verify for whom these services were rendered and provide the correct name and number on the claim and resubmit.223 – We did not consider this for payment because you did not send the extra information we asked for. Payment can be requested again by sending us another claim form and all the information.226 – Medicare will pay rent for the prescribed number of months or until the equipment is no longer needed, whichever occurs first. This is the first monthly rental payment.227 – You will receive a notice each month when additional rental payments are paid.231 – Medicare will no longer pay for rental on this item since the purchase price has been paid.237 – The amount of this payment is the difference between the approved purchase allowance and the rental payments you have received.
KEY TO CODES FOR PLACE AND TYPE OF SERVICE
1. Office2. Home3. Inpatient hospital4. Skilled nursing facility5. Outpatient hospital6. Independent laboratory7. Other8. Independent kidney disease treatment center
A. Medical careB. Surgery (includes treatment of fractures)C. ConsultationD. Diagnostic X-rayE. Diagnostic laboratoryF. Radiation therapyG. AnesthesiaH. Assistance at surgeryI. Other medical serviceJ. Whole blood or packed red cells
Type of servicePlace of service
WHERE TO SEND REFUNDS
Transamerica Occidental LifeC/O Check and Payment ControlBox 54905, Terminal AnnexLos Angeles, CA 90054-0905
YOUR RIGHT TO REVIEW OF A CASE
If you have a problem or question about the way a claim was handled or about the amount paid, please write Transamerica Occidental Life, Box 54905, Terminal Annex, Los Angeles,California 90054, within 6 months of the date of this notice. We will give your request full consideration.
Your Social Security office will help you file a request for review of a claim if it is more convenient for you.
EXPLANATION OF NOTES Additional notes may be listed on the front of this form.
B
When refunding a payment you should send a checkwith a letter of explanation. The letter should includeyour Transamcrica Occidental/Medicare check number, beneficiary name and Medicare identification number (HICNo.), control number to which the payment relates,and any other information which may be pertinent to the refund. Send this information to:
F I G U R E 12 – 14 , c o n t ’ d B, Back of Medicare RA document.
X3666-Ch12 8/27/07 4:56 PM Page 462
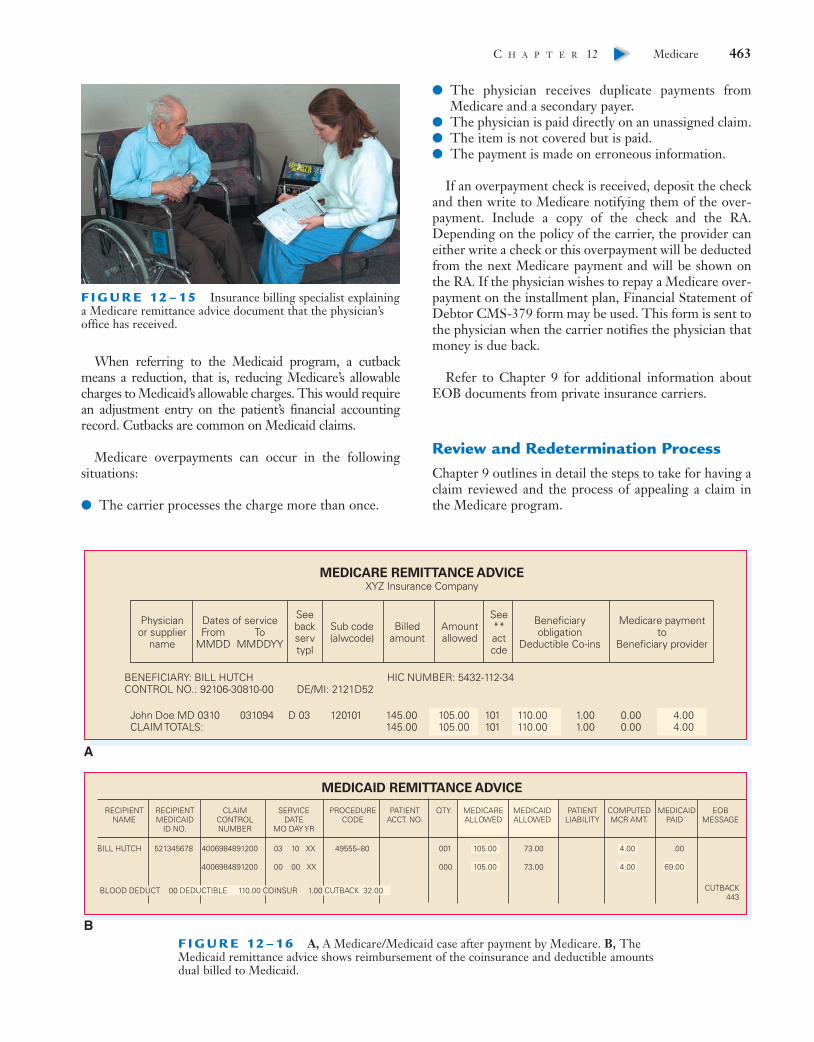
When referring to the Medicaid program, a cutbackmeans a reduction, that is, reducing Medicare’s allowablecharges to Medicaid’s allowable charges. This would requirean adjustment entry on the patient’s financial accountingrecord. Cutbacks are common on Medicaid claims.
Medicare overpayments can occur in the following situations:
● The carrier processes the charge more than once.
● The physician receives duplicate payments fromMedicare and a secondary payer.
● The physician is paid directly on an unassigned claim.● The item is not covered but is paid.● The payment is made on erroneous information.
If an overpayment check is received, deposit the checkand then write to Medicare notifying them of the over-payment. Include a copy of the check and the RA.Depending on the policy of the carrier, the provider caneither write a check or this overpayment will be deductedfrom the next Medicare payment and will be shown onthe RA. If the physician wishes to repay a Medicare over-payment on the installment plan, Financial Statement ofDebtor CMS-379 form may be used. This form is sent tothe physician when the carrier notifies the physician thatmoney is due back.
Refer to Chapter 9 for additional information aboutEOB documents from private insurance carriers.
Review and Redetermination ProcessChapter 9 outlines in detail the steps to take for having aclaim reviewed and the process of appealing a claim inthe Medicare program.
C H A P T E R 12 Medicare 463▼
F I G U R E 12 – 15 Insurance billing specialist explaininga Medicare remittance advice document that the physician’soffice has received.
MEDICARE REMITTANCE ADVICEXYZ Insurance Company
MEDICAID REMITTANCE ADVICE
Physicianor supplier
name
Dates of serviceFrom
MMDDTo
MMDDYY
Seebackservtypl
Sub code(alwcode)
Billedamount
Amountallowed
See**actcde
Beneficiaryobligation
Deductible Co-ins
Medicare paymentto
Beneficiary provider
BENEFICIARY: BILL HUTCHCONTROL NO.: 92106-30810-00 DE/MI: 2121D52
HIC NUMBER: 5432-112-34
110.00110.00
John Doe MD 0310 031094 D 03 120101 145.00145.00
105.00105.00
101101
1.001.00
0.000.00
4.004.00CLAIM TOTALS:
RECIPIENTNAME
RECIPIENTMEDICAID
ID NO.
CLAIMCONTROLNUMBER
SERVICEDATE
MO DAY YR
PROCEDURECODE
PATIENTACCT. NO.
QTY. MEDICAREALLOWED
MEDICAIDALLOWED
PATIENTLIABILITY
4006984891200
4006984891200
COMPUTEDMCR AMT.
MEDICAIDPAID
EOBMESSAGE
BILL HUTCH 521345678 03 10 XX
00 00 XX
49555–80 001
000
105.00
105.00
73.00
73.00
4.00
4.00
.00
69.00
CUTBACK443
BLOOD DEDUCT 00 DEDUCTIBLE 110.00 COINSUR 1.00 CUTBACK 32.00
A
BF I G U R E 12 – 1 6 A, A Medicare/Medicaid case after payment by Medicare. B, TheMedicaid remittance advice shows reimbursement of the coinsurance and deductible amountsdual billed to Medicaid.
X3666-Ch12 8/27/07 4:56 PM Page 463

464 U N I T 3 HEALTH CARE PAYERS▼
P R O C E D U R E 1 2 . 1
DETERMINE WHETHER MEDICARE IS PRIMARY OR SECONDARY
AND DETERMINE ADDITIONAL BENEFITS1. Inquire whether the patient is covered under one or
more of the following plans or situations:● Automobile liability insurance, no-fault insurance, and self-
insured liability insurance. An individual injured or illbecause of an automobile accident may be coveredby liability insurance or no-fault insurance.
● Disability insurance. Disability insurance coverageoffered through an employer-sponsored large grouphealth plan (LGHP).
● Employee group health plan (EGHP). Insurance policiesfor individuals 65 years of age or older who are stillemployed. Employers with 20 or more employees arerequired to offer workers and their spouses ages 65 through 69 years the same health benefits offeredto younger workers. Workers may accept or reject theemployer’s health insurance plan. If they accept it,Medicare becomes the secondary insurance carrier.
● Employer supplemental insurance. A Medicare beneficiaryhas this plan through a former employer. Some peopleare covered by employment plans even after retirement,as long as the plan allows it and the insured informsthe insurance company that he or she wishes tomaintain coverage. These are known as conversion poli-cies. Complementary benefits can vary in these supple-mental plans, and these policies are not considered“Medigap” as defined by federal law. NOTE: When anemployee retires and Medicare becomes the primarycoverage, the company’s group health plan coordi-nates benefits with Medicare.
● Federal Black Lung Act. An act was formed to coveremployees or former coal miner employees who haveillness related to black lung disorder and have accept-able diagnoses that occur on the Department ofLabor’s list.
● Veterans Affairs (VA). A Medicare beneficiary is alsoreceiving benefits from the Department of VeteransAffairs. In this situation, there must be a decision madeas to where to send the claim. Medicare is not second-ary to the VA and the VA is not secondary to Medicare.
The claim is sent where specified by the patient. Theclaim can be sent to Medicare, where, if the claim isprocessed, the patient must satisfy his or her contrac-tual requirement to pay any deductible and copaymentamounts. If the patient asks that the claim be sent tothe VA instead of Medicare, the claim is processed andany payments issued are considered as payment in full.Many veterans want the claim sent to the VA.
● Workers’ compensation. An individual suffers a diseaseor injury connected with employment.
These plans are billed as primary (first) payer andMedicare second. Payments for these types of policiesmay not necessarily go to the physician but may go to theinsured.2. Ask to see the Medicare card, as well as any other insurance
cards, and make photocopies of both sides of each card.3. Inquire of the patient whether the supplemental cover-
age was carried over (conversion policy) from his or heremployer.
4. Call both carriers if the type of plan is not clearly iden-tified.
5. Bill the correct insurance plan.For Medigap cases, nonparticipating physicians may
collect copayments and deductibles up to their limitingcharge (unless the state forbids collection of more thanthe allowed amount) from patients at the time of service.Participating physicians may not collect copayments/deductibles from patients covered by Medigap if thepatient requests the physician to submit the claim to theMedigap insurer. Collect copayments after receiving theMedicare/Medigap RA document.
For other secondary insurance, write the patient’s groupand policy (or certificate) numbers on the Medicare RA,attach it to either a new CMS-1500 (08-05) or a copy ofthe original Health Insurance Claim Form CMS-1500(08-05), and electronically transmit or submit it to thesecondary carrier. Then copy the physician’s billing state-ment that shows date of treatment, description of serv-ice(s) rendered, fees, and diagnosis.
X3666-Ch12 8/27/07 4:56 PM Page 464

This is a brief chapter review or summary of the keyissues presented. To further enhance your knowledge ofthe technical subject matter, review the key terms and keyabbreviations for this chapter by locating the meanings inthe glossary at the end of this book that appear in a sec-tion before the index.
1. Medicare is administered by the Centers forMedicare and Medicaid Services (CMS).
2. Medicare is a health insurance program for peopleage 65 or older, people younger than age 65 with cer-tain disabilities, and people of all ages with end-stagerenal disease.
3. The patient’s complete name exactly as shown on hisor her insurance card and Medicare claim numberincluding the letter at the end must appear on allMedicare claims.
4. Medicare Part A is hospital insurance benefits andPart B is supplementary medical insurance (SMI)benefits.
5. Medicare Part C is referred to as Medicare AdvantagePlan. These plans offer a number of health careoptions in addition to those available under MedicarePart A and Part B.
6. Medicare Part D Prescription Drug Plan is a stand-alone drug plan, presented by insurance and otherprivate companies that offer drug coverage thatmeets the standards established by Medicare.
7. Several federal acts regulate health care coverage ofpersons age 65 and older who are employed.
8. Medigap (MG) is a specialized Medicare supplemen-tal insurance policy whose predefined minimumbenefits are regulated by the federal government anddevised for the Medicare beneficiary.
9. Medicare Secondary Payer (MSP) is a primary insur-ance plan of a Medicare beneficiary that must pay forany medical care or services first before a Medicarefiscal intermediary is sent a claim.
10. To present overuse of services and spot fraud, theFederal Claims Amendment Act was enacted in 1986
which offers financial incentives to informants(whistleblowers).
11. The Clinical Laboratory Improvement Amendments(CLIA) is a federal act established in 1988 that regulateslaboratory certification and accreditation standards,quality control, proficiency testing, personnel stan-dards, program administration, and safety measuresfor all freestanding laboratories, including physicianoffice laboratories (POLs).
12. Because Medicare is a federal program, providersthat transmit claims to Medicare must comply withbilling and coding regulations issued by CMS.
13. Participating physicians agree to accept assignmenton all Medicare claims and may bill the patient onlyfor the Medicare deductible ($131 in 2007) and coin-surance amounts.
14. An Advance Beneficiary Notice (ABN) is an agreementgiven to the patient to read and sign before renderinga service if the participating physician thinks that itmay be denied for payment because of medical neces-sity or limitation of liability by Medicare. ABNs applyif the patient is in an original Medicare program anddo not apply for patients in private fee-for-service ormanaged care plans.
15. Correct Coding Initiative (CCI) is federal legislationthat attempts to eliminate unbundling or other inap-propriate reporting of procedural codes for servicesto Medicare patients.
16. To obtain correct payment for a procedure or serv-ice, a code number must be selected from level I orII of HCPCS coding system and transmitted to theMedicare administrative contractor.
17. The time limit for sending in Medicare claims is theend of the calendar year after the fiscal year in whichservices were furnished.
18. Medicare sends a payment check and a nationally stan-dardized document to participating physicians called aMedicare remittance advice (RA) and a similar documentto the patient called a Medicare summary notice (MSN).
C H A P T E R 12 Medicare 465▼
P R O C E D U R E 1 2 . 2
COMPLETE AN ADVANCE BENEFICIARY NOTICE (ABN) FORM
1. Complete an ABN form by inserting the patient’s nameand health insurance claim number as it appears on theMedicare card.
2. Include the service or treatment that Medicare will likelydeny in the appropriate block.
3. State the reason for anticipated denial in the appropri-ate block.
4. Insert the estimated cost for the service or procedure.However, not including an amount does not invalidatean ABN.
5. The patient must select one of the following options onthe ABN form:a. Receive the services affected by coverage limitationsb. Decline the service or procedure
6. Date the form and have the patient or the patient’s rep-resentative sign it.
K E Y P O I N T S
X3666-Ch12 8/27/07 4:56 PM Page 465
For active links to the following resources, visit the Evolve website at http://evolve.elsevier.com/fordney/handbook● Centers for Medicare and Medicaid Services Forms, Publications, Regulations,
Transmittals (formerly called Program Memorandums)
● CLIA waived tests
● CMS Manual System
● Education and training
● Epocrates freeware
● Federal Register
● Intermediary Carrier Directory
● Social Security Online
466 U N I T 3 HEALTH CARE PAYERS▼
C D A S S I G N M E N T
ST
UD
EN
T
● Do the exercises for cases 8, 9, and 10 using the Student Software Challenge to developskills and review concepts you have learned for this chapter. These cases increase indifficulty. The cases use onscreen encounter forms (superbills) from which you arerequired to abstract information. Using the AltaPoint Practice Management section ofthe software, complete Workbook assignments 12–11 through 12–13.
X3666-Ch12 8/27/07 4:56 PM Page 466
✔ Study Chapter 12.
✔ Answer the multiple choice, fill-in-the-blank, and true/false review questions in theWorkbook to reinforce the theory learned in this chapter and to help prepare you for afuture test.
✔ Complete the assignments in the Workbook to give you experience in computingMedicare in mathematical calculations, selecting HCPCS code numbers, abstractingfrom patients’ health records, preparing financial accounting record cards, and com-pleting forms pertinent to the Medicare program.
✔ Turn to the glossary at the end of this textbook for a further understanding of the keyterms and key abbreviations used in this chapter.
C H A P T E R 12 Medicare 467▼
A S S I G N M E N TS
TU
DE
NT
X3666-Ch12 8/27/07 4:56 PM Page 467