kindergarten new student registration checklist - 39. plainfield community ... student is true,...
TRANSCRIPT

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Kindergarten New Student Registration ChecklistThe following items are required for Kindergarten Registration:
1. Completed registration packet
2. Certified birth certificate• Please provide the Official Certified Birth Certificate with raised seal issued by the county/country in
which the student was born. We do not accept any decorative hospital issued certificates.
3. Photo identification (or Passport) of person enrolling the student
4. Any existing legal custody, divorce decree, or guardianship documents• If there are any legal documents pertaining to the custody of the student, you must provide a copy.
5. Current health requirements• Dental examination must be in before May 15, 2019.• Eye examination must be turned in before October 15, 2018.
6. Physical must be dated on or after August 16, 2017.• If physical is from out of state or country, the physical must meet State of Illinois requirements.
7. Current immunizations must be noted on the physical. (see health letter)• Students without a physical examination who have a list of currently required immnunizations will not be
allowed to start on the first day of school.
8. Most recent individualized education plan (IEP), if applicable.
9. Payment of Fees• Either payment in full at time of registration or confirmation of payment plan through District 202.
10. 3 Current Proofs of Residency (see next page and enrollment form)
NOTE:•
•
Documents that must be turned in are listed on the next page in the column named Registration Forms to be Turned In.
Documents that are for your information or are optional dependent on living situations are listed on the next page in the column named Registration Paperwork for Reference.

Plainfield Community Consolidated School District 202Residency Requirements Checklist
Proofs must be in the Parent/Guardian name with an address that is within School District 202 Boundaries.3 proofs are required, with at least one document from category A and one document from category B.
Category A – Current ResidencyRecent real estate tax billLease (signed showing date of occupancy with landlord’s name and phone number)Settlement statement (signed and within 30 days)Truth in lending statement (signed and within 30 days)Warranty deed (within 30 days)Mortgage statement / Payment book (within 30 days)Bill of Sale (within 30 days)Military housing letterResidency affidavit (Completed and Notarized)
Category B – Current ResidencyMUST BE ISSUED WITHIN THE LAST3 MONTHS (6 months for driver's license)
Auto registrationHomeowners or renters insuranceDriver’s license or state identificationPhoto identification from foreign consulate
MUST BE ISSUED WITHIN THE LAST30 DAYS
Cable billUtility bill – gas, electric, waterLetter from government agencyBank statement
Registration Forms to be Turned InPage(s)
Enrollment formStudent registration contact informationMilitary personnel questionnaireReport card language preference formRace and ethnicity formHome language surveyAcceptable use of technology formHealth history formPhysical form with current immunizationsDental examination form (due by 5/15/19)Eye examination form (due by 10/15/18)
Registration Paperwork for ReferencePage(s)
Are you ready for Kindergarten?School supply listSchool contact information and timesDistrict 202 school calendarHealth letterRace and ethnicity information letterOptional – Transportation Sitter FormOptional – Medication AuthorizationOptional – Guardianship AffidavitOptional – Residency Affidavit
Fee statement and information will be sent in summer
** Note: If you do not own or rent the home in which you are residing, please obtain the student residency affidavit along with the proofs listed above. **
1 - 3
4 - 6
7
8
9
10
11
12
13
14
15 - 16
17 - 18
19 - 21
22 - 23
24
25
26
27 - 28
29 - 31
32 - 37
38 - 39

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Enrollment FormStudent Residency Requirements
Directions: Carefully read and complete each of the following sections. You are required to provide both proof of residency documents and custodial information.
Residency of Person with Legal Custody of the StudentAs initial proof of residency, the person with legal custody of the student and with whom the student lives within School District 202 boundaries must provide at least one document from Category A and at least one documents from Category B.(A total of three documents is required).
In order to enroll without established residency, proof of future residency as described in Category C along with a $350.00 non-refundable fee per family is required.
Category A and B documents must be submitted when actual occupancy occurs. If the registering adult claims the student is homeless, Category D applies.
NOTE: If you do not own or rent the home in which you are residing, you are required to submit the residency affidavit along with the proofs of residency and may require additional paperwork. Proof of residency must be provided every year if the student is enrolled based upon a third party or lease.
Identifying Information: (To be completed by the person with legal custody of the student. Please print.)
Your namePhone number(s) Home: Cell: Work:Current address Address:
City:State: Zip Code:
Subdivision:Future Address(if under contract)
Address:City:
State: Zip Code:Subdivision:
Student’s name Grade Entering Re-enrollment? Yes NoRelation to student Mother Father Step-Mother Step-Father Aunt Uncle Guardian Other:School
Page 1

Plainfield Community Consolidated School District 202Enrollment Form - Residency Requirements Checklist
To Prove CURRENT Residency in School District 202:Proofs must be in the Parent/Guardian name with an address that is within School District 202 Boundaries.3 proofs are required, with at least one document from category A and one document from category B.
Category A – Current ResidencyRecent real estate tax billLease (signed showing date of occupancy with landlord’s name and phone number)Settlement statement (signed and within 30 days)Truth in lending statement (signed and within 30 days)Warranty deed (within 30 days)Mortgage statement / Payment book (within 30 days)Bill of Sale (within 30 days)Military housing letterResidency affidavit (Completed and Notarized)
Category B – Current ResidencyMUST BE ISSUED WITHIN THE LAST3 MONTHS (6 months for driver's license)
Auto registrationHomeowners or renters insuranceDriver’s license or state identificationPhoto identification from foreign consulate
MUST BE ISSUED WITHIN THE LAST30 DAYS
Cable billUtility bill – gas, electric, waterLetter from government agencyBank statement
To prove FUTURE residency in School District 202: One proof is required as described below
Category C - All non-residents must move into the Plainfield School District boundaries within 120 calendar days, provide proof of residency within 2 weeks after moving into the District and pay a $350.00 non-refundable fee per
family.A fully executed purchase agreement stating an approximate closing dateA fully executed sales contract, showing no unsatisfied contingenciesA fully signed lease with occupancy beginning the 1st day of student attendance
To enroll student as "Homeless" in School District 202: Mark below.Category D - Homeless
None of the documents in Categories A, B, or C above are applicable because the student is homeless and eligible for enrollment under the Illinois Education for Homeless Children Act. Please notify your student's school to speak with the Homeless Liaison.
Page 2

Enrollment Form - Proof of Custody
To Prove CUSTODY in School District 202: You must check one of the following descriptions in either, Grounds for Legal Custody OR Exceptions. Additional paperwork may be required.
Grounds for Legal CustodyCheck one of the following as applicable.If none is applicable, you must check one of the "Exceptions" noted below.
Custody is exercised by a natural or an adoptive parent with whom the student resides.Custody has been granted by court order to a person with whom the student resides for reasons other than to have access to the educational programs of this District. (Attach copy of court order)Custody is exercised under a court approved short-term guardianship. (Attach copy of court order)Custody is exercised by a caretaker adult relative who is receiving aid under the Illinois Public Aid Code for the student who resides with that caretaker for the purposes other than to have access to the educational programs of this District. (Attach copy of Public Aid documents)Custody is exercised by an adult who demonstrates that, in fact, he or she has assumed and exercises legal responsibility for the student and provides the student with a regular fixed nighttime dwelling for purposes other than to have access to the educational programs of this District. (Attach completed & notarized guardianship affidavit - MUST be approved by school administration)
Additional Informationor Explanation:
ExceptionsIf none of the above "Grounds for Legal Custody" apply, you must check one of the "Exceptions" noted below.
The student is homeless.The student is a foreign exchange student.The student has been placed with a foster parent or child care facility by the Department of Children and Family Services outside this District, but DCFS has determined it to be in the best interests of the student to maintain attendance in this District! (Attach copy of DCFS determination)The student is at least 18 years old and lives in this District on a full and indefinite length of time basis.The student is under 18, but has been emancipated by court order or marriage and lives in this District on a full and indefinite length of time basis. (Attach copy of court order or marriage license)
Warnings and AffirmationGenerally, Illinois law permits only students who are residents of School District 202 to enroll and attend on a tuition-free basis. Under the law, the residence of a student is deemed to be the residence of the person who has legal custody of the student. "If a pupil is determined to be a nonresident of the District for whom tuition is required to be charged pursuant to this section, the School Board shall refuse to permit the pupil to continue attending the schools of the District unless the required tuition is paid for the pupil." "A person who knowingly or willfully presents to any School District any false information regarding the residency of a pupil for the purpose of enabling that pupil to attend any school in that District without the payment of a non-resident tuition charge shall be guilty of a Class C Misdemeanor." (l05 ILCS 5/10-20.12b) Illinois law has made it a crime, punishable by imprisonment and fine, to knowingly or willfully present any false information regarding the residency of a student for purposes of enabling that student to attend on a tuition-free basis or to knowingly enroll or attempt to enroll a student on a tuition-free basis when the student is known to be a non-resident of the District. The School District will seek prosecution to the full extent of the law of any person who the district believes has committed any residency-related crime. Additionally, a civil lawsuit may be initiated by the School District. I affirm that I am a resident of this District and that the information presented in this Affidavit or in connection with any investigation of my residency or the residency of the student is true, complete, and accurate.
I also give approval for the release of information to District 202 to obtain any documents or information to verify my residency. This release remains valid with no exception.
Signature of Person with Legal Custody of the Student Date
Page 3

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Student Registration - Contact InformationPlease print clearlyStudent Information
School: Student ID#: (for office use only)
Student's Legal Name: (as listed on birth certificate-First, Middle, Last)
First: Middle: Last:
Name Student Goes By:
Date of Birth: Gender: Male Female Grade:
Birthplace: City: State/Country:
Street Address:
City: State: Zip Code:
Subdivision: Home Phone #:
Student Resides With (at address above): Contact #1Relationship to Student:
Mother Father Step-Mother Step-FatherAunt Uncle Guardian Other:
Legal Custody: Yes No
Contact's Legal Name: (Legal First, Middle Initial, Last)
First: Middle: Last:
Home Phone Number: Cell Phone Number:
Employer Name:
Work Phone Number: Education Level: High School & Up
Less than High SchoolUnknownE-mail Address:
Preferred Language for School Written & Electronic Communication: English Spanish Other:
Student Resides With (at address above): Contact #2Relationship to Student:
Mother Father Step-Mother Step-FatherAunt Uncle Guardian Other:
Legal Custody: Yes No
Contact's Legal Name: (Legal First, Middle Initial, Last)
First: Middle: Last:
Home Phone Number: Cell Phone Number:
Employer Name:
Work Phone Number: Education Level: High School & Up
Less than High SchoolUnknownE-mail Address:
Preferred Language for School Written & Electronic Communication: English Spanish Other:
Page 4

Other Custodial Parent – Student Does Not Reside WithRelationship to Student:
Mother Father Step-Mother Step-FatherAunt Uncle Guardian Other:
Legal Custody: Yes No
Contact's Legal Name: (Legal First, Middle Initial, Last)
First: Middle: Last:
Street Address:
City: State: Zip Code:
Home Phone Number: Cell Phone Number:
Employer Name:
Work Phone Number: Education Level: High School & Up
Less than High SchoolUnknownE-mail Address:
Preferred Language for School Written & Electronic Communication: English Spanish Other:
Emergency Contact #1Contact's Legal Name: (Legal First, Middle Initial, Last)
First: Middle: Last:
Relationship to Student:
Aunt Uncle Neighbor Friend Childcare ProviderOther:
Street Address:
City: State: Zip Code:
Home Phone Number: Cell Phone Number:
Emergency Contact #2Contact's Legal Name: (Legal First, Middle Initial, Last)
First: Middle: Last:
Relationship to Student:
Aunt Uncle Neighbor Friend Childcare ProviderOther:
Street Address:
City: State: Zip Code:
Home Phone Number: Cell Phone Number:
Emergency Contact #3Contact's Legal Name: (Legal First, Middle Initial, Last)
First: Middle: Last:
Relationship to Student:
Aunt Uncle Neighbor Friend Childcare ProviderOther:
Street Address:
City: State: Zip Code:
Home Phone Number: Cell Phone Number:
Page 5

Medical InformationWears Glasses: Yes No Wears Contact Lenses: Yes NoMedical Information: Please list any medical conditions we need to know about.
Previous Schooling InformationPrevious School Student Attended:
Did your student receive special services and/or programs at their previous school?
SpeechELL - English Language LearnerESL - English as a Second LanguageIEP - Individualized Education ProgramSection 504 PlanGifted/AcceleratedTitle IRTI - Reading InterventionRTI - Math InterventionSocial Worker/CounselorDirect ServicesFree / Reduced Waiver
Yes NoYes NoYes NoYes NoYes NoYes NoYes NoYes NoYes NoYes NoYes NoYes No
Other:Has the student ever attended Plainfield Schools in the past? If so, please provide school name.
Yes NoSchool:
Has your student previously attended USA schools? Yes No
Siblings that are currently attending Plainfield School District 202Student Name Current School Grade Date of Birth
It is imperative that all items on this registration form are complete.As parent/guardian of the above named student, I affirm that I have completed this form in its entirety and to the best of my knowledge.**NOTE: All information must be complete for a contact or emergency contact to be valid. **
Print Name:
Signature: Date:RECORDED MESSAGE DISCLAIMER FOR ALL REGISTRATION PACKETSPlease Note: District 202 uses a message system incorporating recorded telephone calls, emails and text messages to communicate a wide range of emergency and non-emergency information with families.
This system operates through traditional land lines (telephone messages), computers (emails) and personal smart phones (telephone messages, text messages, apps, etc.).
District 202 will use all contact information provided on this form for automated telephone and text messages. You may contact your school directly to modify how you receive automated telephone and text messages, or to 'opt out' of such communications altogether.
Any modifications to how you receive automated telephone and text messages will not affect your school’s ability to reach you through other communications, and will not affect your school’s ability to use automated telephone and text messages for emergencies.
Page 6

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Military PersonnelIllinois State Board of Education
Children of U.S. Military Personnel System
Plainfield Community Consolidated School District 202 is required by the Illinois School Board of Education to provide parents/guardians the opportunity to respond to the Children of U.S. Military Personnel data
"At the time of annual enrollment or at any time during the school year, a school district or a recognized non-public school, except for sectarian non-public schools, serving any of grades kindergarten through 12 shall provide, either on its standard enrollment form or on a separate form, the opportunity for the individual enrolling the student to voluntarily state whether the student has a parent or guardian who is a member of a branch of the armed forces of the United States and who is either deployed to active duty or expects to be deployed to active duty during the school year. Each school district and recognized non-public school shall report this
For the 2018-2019 School Year Date:
Student that are currently attending Plainfield School District 202Student Name Current School Grade Date of Birth
Parent/Guardian is a member of a branch of the United States armed forces: Yes No
If yes, are you currently deployed to active duty or expect to be deployed to active duty during the 2018-2019 school year: Yes No
Parent/Guardian signature:
Parent/Guardian name:Please print clearly
Page 7

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Grade Report Card Language Preference
Student name: ID #
School:
Grade report cards are available in English and Spanish and will be made available in the language indicated on the home language survey. Please indicate which language you wish to receive your child’s grade report card.
Note: By choosing to receive my child’s grade report card only in English, I waive my right to receive the grade report card in (the language indicated on the home language survey).
I wish to receive my child’s grade report card in:
English
Home Language indicated above
Both
Signed:Parent or legal guardian Date
GRADE REPORT CARDS: In order to keep you and your child informed about your child’s progress in school, you will receive your individual student’s grade report. The grade report card includes information about the content being taught in school and the academic performance of your child. Grade report cards are sent according to the following schedule:
Kindergarten: end of each quarter
Grade 1-5: end of each quarter
Grade 6-8: end of each quarter
Grade 9-12: end of each semester
Page 8
Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Dear Parent or Guardian,
Enclosed is the form that parents or guardians need to complete to identify race and ethnicity for their children.
Please complete one form per child, and be sure to answer both parts of the two-part question. Remember
that school district staff is required to provide any missing information by observer identification. Return the
completed form to your child’s school with registration.
In fall 2007, the U.S. Department of Education issued new guidance on the collection and reporting of race and
ethnicity data for public school students and staff. The guidance implements new federal race and ethnicity
categories that were developed to obtain a more accurate picture of the nation’s diversity. The new data
collection process requires respondents to answer a two-part question, indicating ethnicity and then one or more
of five races. In the past, individuals were allowed to choose only one race or ethnicity category.
The Illinois State Board of Education (ISBE) will use the new categories starting with data to be reported for
the 2010-11 school year. This requires school districts to re-identify race and ethnicity for all students - and the
identification is to be done by parents or guardians. If a student’s parents or guardians decline to indicate race
and/or ethnicity, observer identification by school district staff is required.
The new race and ethnicity data will be used in the same manner as previously collected data, e.g., in reporting
and analyzing test results by race and ethnicity. The information will not be used to check immigration status,
and the confidentiality of individual student information will be protected.
Thank you for your cooperation in providing the needed data. Please direct any questions you may have to the
administration at your child’s school.
Page 9

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Illinois State Board of EducationNew U.S. Department of Education Race and Ethnicity Data Standards
Note: Every student’s parents or guardians must respond to both questions (Part A and Part B). If the parents or guardians decline to respond to either question (Part A or Part B), school district staff are required to provide the missing information by observer identification.
Student name: ID #
INSTRUCTIONS: This form is to be filled out by the student’s parents or guardians, and both questions must be answered.Part A asks about the student’s race and Part B asks about the student’s ethnicity.If you decline to respond to either question, the school district is required to provide the missing information by observer identification.
Part A. Is this student Hispanic/Latino? Choose only one.(A person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin, regardless of race.)
No, not Hispanic/LatinoYes, Hispanic/Latino
The question above is about ethnicity, not race. No matter which answer you selected, continue and respond to the question below by marking one or more boxes to indicate what you consider this student’s race to be.
Part B. What is the student’s race? Choose one or more.American Indian or Alaska Native (A person having origins in any of the original peoples of North and South America, including Central America, and who maintains tribal affiliation or community attachment.)
Asian (A person having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent including, for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam.)
Black or African American (A person having origins in any of the black racial groups of Africa.)
Native Hawaiian or Other Pacific Islander (A person having origins in any of the original peoples of Hawaii, Guam, Samoa, or other Pacific Islands.)White (A person having origins in any of the original peoples of Europe, the Middle East, or North Africa.)
Parent/Guardian Signature: Date:
Note: Data collected on this form must be maintained by the school district for three years. However, when there is litigation, a claim, an audit, or another action involving this record, the original responses must be retained until the
Page 10

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Home Language Survey - Form A
The State of Illinois School Code requires that each school district shall administer a Home Language Survey to each student entering the school district for the first time. The information is used to identify the need for English language support services for your child.
Student's Name:Last First Middle
Date of Birth: Country of Birth:
School: Grade:
1. Is a language other than English spoken in your home? Yes No
If yes, which language?
2. Does your son/daughter speak a language other than English? Yes No
If yes, which language?
If the answer to question 1 or 2 is YES, the school will assess your child’s English language proficiency. As required by Illinois State law, the school will use the pre-IPT (PK only), WIDA Model, or W-APT test to measure your child’s listening, speaking, reading, and writing skills.
3. Has your son/daughter received English as a Second Language (ESL) support services in any previous school district in the USA?
Yes No
If ‘yes’, please provide state and school district
State
School District
SignatureParent or legal guardian Date
Distribution: Original/Student cumulative file Revised: 05/04/2015 FORM #247
OFFICIAL USE ONLYDistrict Enrollment Date:
ELL Program Entry Date:
Page 11

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Authorization Form:ACCEPTABLE USE OF TECHNOLOGY POLICY (AUP)
AUTHORIZATION FORM**** The following section must be completed by all employees, students, and users of District electronic resources ****
By signing below, I acknowledge that I have received, read, and understand the Acceptable Use of Technology Policy (AUP), and any implementing administrative procedures, handbooks, and guidelines. I agree to all terms of the AUP and related materials. I understand that it is my responsibility to become acquainted with the AUP and related materials, and to keep up-to-date on any changes that may be implemented from time to time. I understand that I am expected to comply by the AUP and related materials, that I may not be notified immediately by the District of changes to the AUP and related materials, and that my ignorance of the AUP and related materials is not an excuse for a violation or other misconduct. I understand that I may be disciplined (up to and including suspension and expulsion, for students, and dismissal, for employees) and/or subject to other legal action for violations of the AUP and related materials.
User’s Full Name (please print) Date of Birth
User’s Position (for Employees), Grade (for Students), or Relationship with District (for All Other Users) (please print)
User’s Signature Date
**** The following section must be completed by each student user’s parent/guardian ****As the parent/guardian of the student signing above, I acknowledge that I have received, read, and understand the Acceptable Use of Technology Policy (AUP), and any implementing administrative procedures, handbooks, and guidelines. I agree to all terms of the AUP and related materials for myself and for my student. I understand that it is my responsibility to make sure my student and I are acquainted with the AUP and related materials and keep up-to- date on any changes that may be implemented from time to time. I understand that my student is expected to comply with the AUP and related materials, that my student and I may not be notified immediately by the District of changes to the AUP and related materials, and that my or my student’s ignorance of the AUP and related materials is not an excuse for a violation or other misconduct. I understand that my student may be disciplined (up to and including suspension and expulsion) and/or subject to other legal action for violations of the AUP and related materials.
Parent/Guardian’s Full Name Date
Parent/Guardian’s Signature
Page 12

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Student Health History School Year 2018-2019Student Name: Grade: School:
Sex: Male Female Birth Date: Phone Number:
Doctor’s Name:
(if you indicate YES for any category, please explain)
# Concern Yes or No Explanation & Comments
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
Allergies
*Uses EpiPen
Asthma
*Uses Inhaler
*Uses Inhaler at School
Blood Disorders
Daily Medications
*Names of Medication(s)
School Medications REQUIREMedical Authorization Form
Diabetes
Ear / Hearing Problems
Glasses / Contacts
Eye / Vision Problems
Heart Problems
Hospitalizations
Mental Health Concerns
Neurological Problems
Physical Restrictions
Seizures
Serious Injuries
Surgery
Other
At home
At school
Last eye exam:
Age:
Age:
Age:
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Rarely Once daily More than once daily For Sports
I release this information to be shared with appropriate school and emergency personnel for health and educational purposes.
Parent / Guardian Signature Date
Page 13

Am I Ready For Kindergarten?Below is a guide to help better prepare your child for their kindergarten experience.
If your child is not "On target" for each area you have all summer to reach these goals.Sample
On Target: Your child is doing great!If your child is not "On target" no need for panic! It’s time to find some playful learning activities to help your child grow in this area.
Counting to 100On Target: Counting up to 29 or 39.
If your child gets stuck at 12, that’s a normal developmental milestone that he/she should be past before starting kindergarten. Otherwise he/she might not reach 100 before the year’s end.
Alphabet RecognitionOn Target: Names all capital letters and some lower case letters. Names half the sounds.
If your child hasn’t picked up letters and sounds yet, this is definitely something you should work on.
Name WritingOn Target: Writes first name (first letter capital).
If your child cannot write their name correctly, it’s time for daily practice.
Writing SkillsOn Target: Understands that writing is made up of letters and attempts to write some letters, draws a picture to match,
and dictates to you what they "wrote".If your child does not understand what writing looks like start a daily journal with them! They can dictate what they want to write and copy how you wrote it. They can then draw a picture to match!
Listening SkillsOn Target: Enjoys listening to a stack of picture books. Makes personal connections to stories and answers simple
questions. May be recognizing a handful of familiar words.If your child does not enjoy being read to, put more limits on screen time and make use of your library card.
Phonemic Awareness SkillsOn Target: Is able to demonstrate one to one correspondence between words in a sentence and/or can clap the correct
number of words in the sentence. Can also identify when two words rhyme.Read books that contain rhymes such as Mother Goose or Dr. Seuss and explain to your child that rhyming words sound the same at the end.
Self Help SkillsOn Target: Is comfortable wearing his or her school clothes and operating the buttons, snaps and zippers
independently.Your child needs to independently do the following: use the restroom, fasten coat, open/close car door, put papers into their folder, and zip and put on their backpack.
Fine Motor/Pencil GripOn Target: Your child holds a pencil correctly using a proper grip.
Show your child the proper grip and fix their fingers when using a pencil, crayon, or marker. This will increase their handwriting skills and supports neat handwriting.
Proper Grip →
Page 14

State of IllinoisCertificate of Child Health Examination
Student's Name
Last First Middle
Birth Date
Month/Day/Year
Sex Race/Ethnicity School/Grade Level/ID#
Address Street City ZIP Code Parent/Guardian Telephone# Home WorkIMMUNIZATIONS: To be completed by health care provider. The mo/da/yr for every dose administered is required. If a specific vaccine is medically contraindicated, a separate written statement must be attached by the health care provider responsible for completing the health examination explaining the medical reason for the contraindication.REQUIREDVaccine / Dose
DTP or DTaP
Tdap; Td orPediatric DT
Polio
Hib
Pneumococcal Conjugate
Hepatitis B
MMR
Varicella
Meningococcal conjugate (MCV4)
(Check specific type)
(Check specific type)
Haemophilus influenza type b
Measles, Mumps, RubellaComments:
(Chickenpox)
RECOMMENDED, BUT NOT REQUIRED Vaccine / Dose
Hepatitis A
HPV
Influenza
Other: Specify any immunizations administered and dates
DOSE 1Month Day Year
Tdap Td DT
IPV OPV
DOSE 2Month Day Year
Tdap Td DT
IPV OPV
DOSE 3Month Day Year
Tdap Td DT
IPV OPV
DOSE 4Month Day Year
Tdap Td DT
IPV OPV
DOSE 5Month Day Year
Tdap Td DT
IPV OPV
DOSE 6Month Day Year
Tdap Td DT
IPV OPV
Health care provider (MD, DO, APN, PA, school health professional, health official) verifying above immunization history must sign below.If adding dates to the above immunization history section, put your initials by date(s) and sign here.
Signature Title Date
Signature Title DateALTERNATIVE PROOF OF IMMUNITY1. Clinical diagnosis (measles, mumps, hepatitis B) is allowed when verified by physician and supported with lab confirmation. Attach copy of lab result.
*MEASLES (Rubeola) **MUMPS HEPATITIS B VARICELLAMonth Day Year Month Day Year Month Day Year Month Day Year
2. History of varicella (chickenpox) disease is acceptable if verified by health care provider, school health professional or health official.Person signing below verifies that the parent/guardian’s description of varicella disease history is indicative of past infection and is accepting such history as documentation of disease.Date of Disease Signature Title
3. Laboratory Evidence of Immunity (check one) Measles * Mumps ** Rubella Varicella Attach copy of lab result.*All measles cases diagnosed on or after July 1, 2002, must be confirmed by laboratory evidence.
**All mumps cases diagnosed on or after July 1, 2013, must be confirmed by laboratory evidence.
Completion of Alternatives 1 or 3 MUST be accompanied by Labs & Physician Signature:Physician Statements of Immunity MUST be submitted to IDPH for review.
Certificates of Religious Exemption to Immunizations or Physician Medical Statements of Medical Contraindication Are Reviewed and Maintained by the School Authority.
11/2015 (COMPLETE BOTH PAGES) Printed by Authority of the State of Illinois
Page 15

Last First Middle Birth Date Month/Day/Year Sex School Grade Level/ ID
HEALTH HISTORY TO BE COMPLETED AND SIGNED BY PARENT/GUARDIAN AND VERIFIED BY HEALTH CARE PROVIDERALLERGIES(Food, drug, insect, other)
YesNo
List:
Diagnosis of asthma? Yes NoChild wakes during night coughing? Yes No
Birth defects? Yes NoDevelopmental delay? Yes No
Blood disorders? Hemophilia,Sickle Cell, Other? Explain.
Yes No
Diabetes? Yes No
Head injury/Concussion/Passed out? Yes No
Seizures? What are they like? Yes No
Heart problem/Shortness of breath? Yes No
Heart murmur/High blood pressure? Yes No
Dizziness or chest pain with exercise? Yes No
Eye/Vision problems? No Glasses Contacts Last exam by eye doctorOther concerns? (crossed eye, drooping lids, squinting, difficulty reading)
Ear/Hearing problems? Yes No
Bone/Joint problem/injury/scoliosis? Yes No
MEDICATION(List all prescribed or taken on a regular basis.)
YesNo
List:
Loss of function of one of paired organs? (eye/ear/kidney/testicle)
Yes No
Hospitalizations?When? What for?
Yes No
Surgery? (List all.)When? What for?
Yes No
Serious injury or illness? Yes No
TB skin test positive (past/present)? * Yes No *If yes, refer to local health department.
TB disease (past or present)? * Yes No
Tobacco use (type, frequency)? Yes No
Alcohol/Drug use? Yes No
Family history of sudden death before age 50? (Cause?)
Yes No
Dental Braces Bridge Plate Other
Information may be shared with appropriate personnel for health and educational purposes.Parent/GuardianSignature Date
PHYSICAL EXAMINATION REQUIREMENTS Entire section below to be completed by MD/DO/APN/PAHEAD CIRCUMFERENCE if < 2-3 years old HEIGHT WEIGHT BMI B/PDIABETES SCREENING (NOT REQUIRED FOR DAY CARE) BMI>85%age/sex Yes No And any two of the following: Family History Yes NoEthnic Minority Yes No Signs of Insulin Resistance (hypertension, dyslipidemia, polycystic ovarian syndrome, acanthosis nigricans) Yes No At Risk Yes No
LEAD RISK QUESTIONNAIRE Required for children age 6 months through 6 years enrolled in licensed or public school operated day care, preschool, nursery school and/or kindergarten. (Blood test required if resides in Chicago or high risk zip code.)
Questionnaire Administered? Yes No Blood Test Indicated? Yes No Blood Test Date ResultTB SKIN OR BLOOD TEST Recommended only for children in high-risk groups including children immunosuppressed due to HIV infection or other conditions, frequent travel to or born in high
prevalence countries or those exposed to adults in high-risk categories. See CDC guidelines. http://www.cdc.gov/tb/publications/factsheets/testing/TB_testing.htm.No test needed Test performed
Skin Test: Date Read / / Result: Positive Negative mmBlood Test: Date Reported / / Result: Positive Negative Value
LAB TESTS (Recommended) Date Results Date ResultsHemoglobin or Hematocrit
Urinalysis
Sickle Cell (when indicated)
Developmental Screening Tool
SYSTEM REVIEW Normal Comments/Follow-up/Needs
SkinEars Screening Result:Eyes Screening Result:NoseThroatMouth/DentalCardiovascular/HTNRespiratory Diagnosis of Asthma
Normal Comments/Follow-up/Needs
EndocrineGastrointestinalGenito-Urinary LMP
NeurologicalMusculoskeletalSpinal ExamNutritional statusMental Health
Currently Prescribed Asthma Medication:Quick-relief medication (e.g. Short Acting Beta Agonist)Controller medication (e.g. inhaled corticosteroid)
Other
NEEDS/MODIFICATIONS required in the school setting DIETARY Needs/Restriction
SPECIAL INSTRUCTIONS/DEVICES e.g. safety glasses, glass eye, chest protector for arrhythmia, pacemaker, prosthetic device, dental bridge, false teeth, athletic support/cup
MENTAL HEALTH/OTHER Is there anything else the school should know about this student?If you would like to discuss this student’s health with school or school health personnel, check title: Nurse Teacher Counselor Principal
EMERGENCY ACTION needed while at school due to child’s health condition (e.g., seizures, asthma, insect sting, food, peanut allergy, bleeding problem, diabetes, heart problem)?Yes No If Yes, please describe
On the basis of the examination on this day, I approve this child’s participation in (If No or Modified please attach explanation.)PHYSICAL EDUCATION Yes No Modified INTERSCHOLASTIC SPORTS Yes No Modified
Print Name (MD,DO, APN, PA) Signature Date
Address Phone(COMPLETE BOTH PAGES)
Page 16

State of IllinoisIllinois Department of Public Health
PROOF OF SCHOOL DENTAL EXAMINATION FORM
To be completed by the parent (please print):
Student’s Name: Last First Middle Birth Date: (Month/Day/Year)
/ /
Address: Street City ZIP Code Telephone
Name of School: Grade Level: Gender:
Male Female
Parent or Guardian: Address (of parent / guardian):
Street
City Zip
To be completed by dentist:
Oral Health Status (check all that apply)
Yes No Dental Sealants Present
Yes No Caries Experience / Restoration HistoryA filling (temporary/permanent) OR a tooth that is missing because it was extracted as a result of caries OR missing permanent 1st molars.
Yes No Untreated CariesAt least 1/2 mm of tooth structure loss at the enamel surface. Brown to dark-brown coloration of the walls of the lesion. These criteria apply to pit and fissure cavitated lesions as well as those on smooth tooth surfaces. If retained root, assume that the whole tooth was destroyed by caries. Broken or chipped teeth, plus teeth with temporary fillings, are considered sound unless a cavitated lesion is also present.
Yes No Soft Tissue Pathology
Yes No Malocclusion
Treatment Needs (check all that apply)Urgent Treatmentabscess, nerve exposure, advanced disease state, signs or symptoms that include pain, infection, or swelling.
Restorative Careamalgams, composites, crowns, etc.
Preventive Caresealants, fluoride treatment, prophylaxis.
Otherperiodontal, orthodontic.Please note:
Signature of Dentist Date of Exam
AddressStreet City Zip Code
Telephone
Illinois Department of Public Health, Division of Oral Health217-785-4899 • TTY (hearing impaired use only) 800-547-0466 • www.idph.state.il.us
IOCI 0600-10 Printed by Authority of the State of Illinois
Page 17

State of IllinoisIllinois Department of Public Health
DENTAL EXAMINATION WAIVER FORMPlease print):
Student’s Name: Last First Middle Birth Date: (Month/Day/Year)
/ /
Address: Street City ZIP Code Telephone
Name of School: Grade Level: Gender:
Male Female
Parent or Guardian: Address (of parent / guardian):
Street
City Zip
I am unable to obtain the required dental examination because:
My child is enrolled in the free and reduced lunch program and is not covered by private or public dental insurance (Medicaid/All Kids).
My child is enrolled in the free and reduced lunch program and is ineligible for public insurance (Medicaid/All Kids).
My child is enrolled in Medicaid/All Kids, but we are unable to find a dentist or dental clinic in our community that is able to see my child and will accept Medicaid/All Kids.
My child does not have any type of dental insurance, and there are no low-cost dental clinics in our community that will see my child.
Signature Date
Illinois Department of Public Health, Division of Oral Health217-785-4899 • TTY (hearing impaired use only) 800-547-0466 • www.idph.state.il.us
December 2006Page 18

State of IllinoisEye Examination Report
Illinois law requires that proof of an eye examination by an optometrist or physician (such as an ophthalmologist) who provides eye examinations be submitted to the school no later than October 15 of the year the child is first enrolled or as required by the school for other children. The examination must be completed within one year prior to the first day of the school year the child enters the Illinois school system for the first time. The parent of any child who is unable to obtain an examination must submit a waiver form to the school.
Student Name(Last) (First) (Middle Initial)
Birth Date(Month/Day/Year)
Gender Grade
Parent or Guardian(Last) (First)
Phone(Area Code)
Address(Number) (Street) (City) (ZIP Code)
Country
To Be Completed By Examining Doctor
Case History
Date of exam
Ocular history: Normal or Positive for
Medical history: Normal or Positive for
Drug allergies: NKDA or Positive for
Other information
ExaminationDistance NearRight Left Both Both
Uncorrected visual acuity 20/ 20/ 20/ 20/Best corrected visual acuity 20/ 20/ 20/ 20/
Was refraction performed with dilation? Yes No
Normal Abnormal Not Able to Assess CommentsExternal exam (lids, lashes, cornea, etc.)Internal exam (vitreous, lens, fundus, etc.)Pupillary reflex (pupils)Binocular function (stereopsis)Accommodation and vergenceColor visionGlaucoma evaluationOculomotor assessmentOtherNOTE: "Not Able to Assess" refers to the inability of the child to complete the test, not the inability of the doctor to provide the test.
DiagnosisNormal Myopia Hyperopia Astigmatism Strabismus Amblyopia
Other
Continued on next page
Page 19
State of IllinoisEye Examination Report
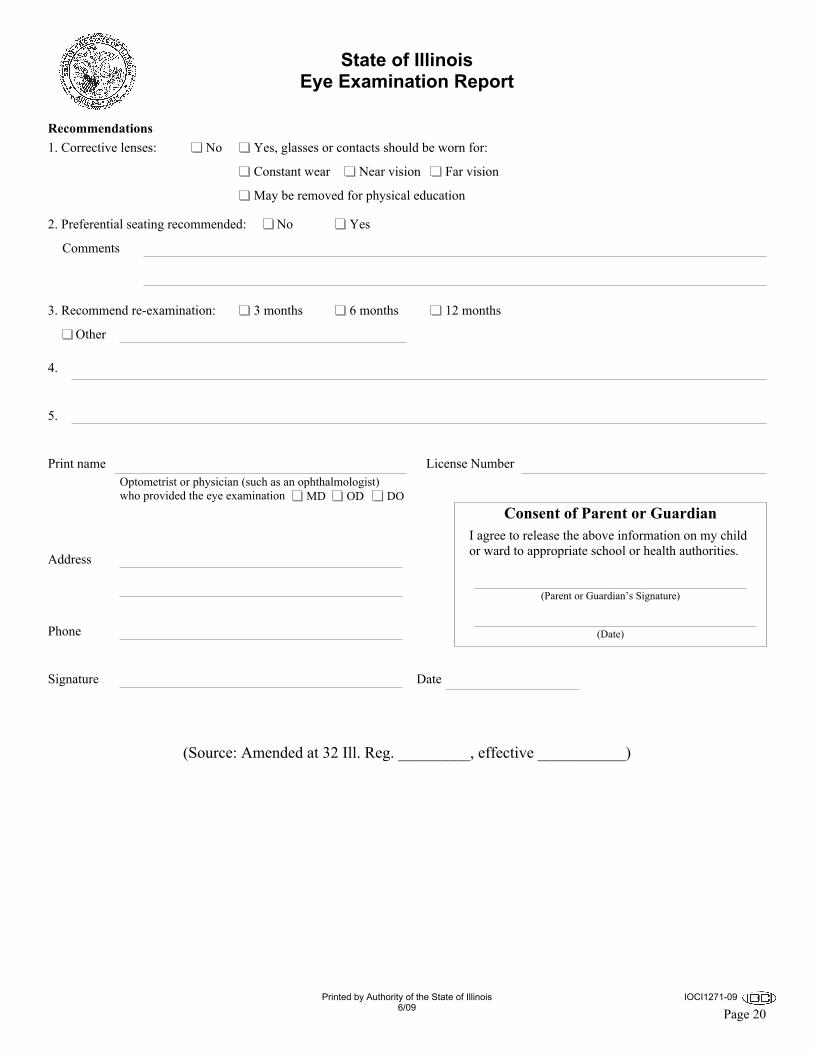
Recommendations1. Corrective lenses: No Yes, glasses or contacts should be worn for:
Constant wear Near vision Far vision
May be removed for physical education
2. Preferential seating recommended: No Yes
Comments
3. Recommend re-examination: 3 months 6 months 12 months
Other
4.
5.
Print nameOptometrist or physician (such as an ophthalmologist)who provided the eye examination MD OD DO
License Number
Address
Phone
Signature Date
(Source: Amended at 32 Ill. Reg. _________, effective ___________)
Consent of Parent or GuardianI agree to release the above information on my child or ward to appropriate school or health authorities.
(Parent or Guardian’s Signature)
(Date)
Printed by Authority of the State of Illinois6/09
IOCI1271-09
Page 20

State of IllinoisDepartment of Public Health
Eye Examination Waiver Form
Please Print
Student Name(Last) (First) (Middle Initial)
Birth Date(Month/Day/Year)
School Name Grade Level Gender Male Female
Address(Number) (Street) (City) (ZIP Code)
Phone(Area Code)
Parent or Guardian(Last) (First)
Address of Parent or Guardian(Number) (Street) (City) (ZIP Code)
I am unable to obtain the required vision examination because:
My child is enrolled in medical assistance/ALL KIDS, but we are unable to find a medical doctor who performs eye examinations or an optometrist in the community who is able to examine my child and accepts medical assistance/ALL KIDS.
My child does not have any type of medical or vision/eye care coverage, my child does not qualify for medical assistance/ALL KIDS, there are no low-cost vision/eye clinics in our community that will see my child, and I have exhausted all other means and do not have sufficient income to provide my child with an eye examination.
Other undue burden or a lack of access to an optometrist or to a physician who provides eye examinations:
Signature Date
(Source: Added at 32 Ill. Reg. _________, effective ___________)
Printed by Authority of the State of Illinois6/09
IOCI1271-09
Page 21

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
2018-2019 School Supply Lists
KindergartenKindergarten8 wide dry erase markers - black6 large glue sticks2 dozen #2 pencils (sharpened)2 boxes 24 regular crayons2 sturdy pocket folders (no fasteners), 1 red and 1 blue1 box facial tissue1 pair gym shoes for physical education days1 supply box1 box 8 classic washable markers1 spiral notebook (70-100 pages)1 highlighter1 pair 5-inch blunt tip scissors1 pair headphones or earbuds1 art shirt1 box quart or sandwich size Ziploc bags (girls)1 box gallon size Ziploc bags (boys)
First GradeFirst Grade8 dry erase markers (dark colors)8 large glue sticks2 dozen #2 pencils (sharpened)1 pink eraser2 boxes 24 regular crayons1 box 12 colored pencils8 washable, broad-tip classic color markers2 highlighters6 folders with bottom pockets / solid colors / plastic / no prongs
1 each: red, blue, yellow, orange, green, purple2 boxes facial tissue1 plastic supply box2 spiral notebooks, 70 sheets, wide rule/wide lined1 composition notebook1 3-ring binder (1 inch size)1 pair 5-inch blunt tip scissors1 art shirt1 eraser for white board1 pair headphones or earbuds1 pair gym shoes for physical education days1 box gallon-size Ziploc bags (boys)1 box quart or sandwich-size Ziploc bags (girls)
Full Day KindergartenFull Day Kindergarten8 wide dry erase markers - black6 large glue sticks2 dozen #2 pencils (sharpened)4 boxes 24 regular crayons4 sturdy pocket folders (no fasteners)1 box facial tissue1 pair gym shoes for physical education days1 supply box1 box 8 classic washable markers1 spiral notebook (70-100 pages)2 highlighters1 pair 5-inch blunt tip scissors1 pair headphones or earbuds1 art shirt1 box quart or sandwich size Ziploc bags (girls)1 box gallon size Ziploc bags (boys)
Second GradeSecond Grade6 dry erase markers (dark colors)4 large glue sticks3 dozen #2 pencils (sharpened)2 pink erasers2 boxes 24 regular crayons2 highlighters8 washable, broad-tip classic color markers
10 plain pocket folders; no clasps or prongs.2 each: red, green, blue, yellow, purple
2 boxes facial tissue1 plastic supply box (no pouches)5 spiral notebooks, 70 sheets, wide rule/wide lined2 packs 3x3-inch sticky notes1 pair 5-inch blunt tip scissors1 12 inch ruler (1/4 inch scale)1 eraser for white board1 pair headphones or earbuds1 pair gym shoes for physical education days1 art shirt1 box gallon-size Ziploc bags (boys)1 box quart or sandwich-size Ziploc bags (girls)
** Supplies "run out" during the school year. Please check with your child periodically to see if any need replacing **
Revised 1/1/0001 Page 22

2018-2019 School Supply Lists
Third GradeThird Grade8 dry erase markers (dark colors)4 large glue sticks3 dozen #2 pencils (sharpened)1 pink eraser1 box 24 regular crayons1 box 12 colored pencils (not mechanical)8 washable, broad-tip classic color markers2 highlighters (different colors)6 folders with bottom pockets / solid colors.
1 each: red, blue, yellow, orange, green, purple2 boxes facial tissue1 plastic supply box (no larger than 6" x 9")4 spiral notebooks, 70 sheets, wide rule/wide lined1 pack filler paper, wide-ruled3 packages 3x3-inch Post-It notes1 pack 100 note cards – white and lined – 3" x 5"1 pair 5-inch blunt tip scissors1 12-inch ruler (1/4 inch scale)1 eraser for white board1 pair headphones or earbuds1 pair gym shoes for physical education days1 art shirt1 box gallon-size Ziploc bags (boys)1 box quart or sandwich-size Ziploc bags (girls)
Fourth GradeFourth Grade8 dry erase markers4 large glue sticks2 dozen #2 pencils (sharpened)6 pens (3 blue, 3 red)1 pink eraser1 box 24 regular crayons1 box 12 colored pencils (not mechanical)8 washable, broad-tip classic color markers2 highlighters8 folders with bottom pockets / solid colors / pronged2 boxes facial tissue1 plastic supply box (no larger than 6" x 9")8 spiral notebooks, 70 sheets, wide rule/wide lined2 packs filler paper, wide-ruled1 package 3x3-inch Post-It notes1 pack 100 note cards – white and lined – 3" x 5"1 pair 7-inch pointed tip scissors1 12-inch ruler (1/8 inch scale)1 eraser for white board1 pair headphones or earbuds1 pair gym shoes for physical education days1 art shirt1 box gallon-size Ziploc bags (boys)1 box quart or sandwich-size Ziploc bags (girls)
** Supplies "run out" during the school year. Please check with your child periodically to see if any need replacing **
Fifth GradeFifth Grade8 dry erase markers (dark colors)4 glue sticks3 dozen #2 pencils (sharpened)5 pens (3 blue or black, 2 red)1 box colored pencils or crayons (parent's choice)8 washable, broad-tip classic color markers2 highlighters – different colors7 folders with bottom pockets - solid colors.
1 each: black, red, blue, yellow, orange, green, purple2 folders with pockets AND prongs – solid colors1 3-ring binder (1/2 inch)3 boxes facial tissue1 plastic supply box (no larger than 6" x 9")7 one subject spiral notebooks2 packs filler paper, wide-ruled2 packages 3x3-inch Post-It notes1 pack 100 note cards – white and lined – 3" x 5"1 pair 7-inch pointed tip scissors1 12-inch ruler (1/8 inch scale)1 eraser for white board1 pair headphones or earbuds1 pair gym shoes for physical education days1 art shirt1 box gallon-size Ziploc bags (boys)1 box quart or sandwich-size Ziploc bags (girls)
Elementary SchoolsElementary SchoolsCentral (815-436-9278)Charles Reed (815-254-2160)Creekside (815-577-4700)Crystal Lawns (815-436-9519)Eagle Pointe (815-577-4800)Eichelberger (815-577-3606)Freedom (815-254-4005)Grand Prairie (815-436-7000)Lakewood Falls (815-439-4560)Liberty (815-609-3037)Lincoln (815-577-4500)Meadow View (815-439-4828)Ridge (815-577-4630)River View (815-439-4840)Thomas Jefferson (815-577-2021)Walker's Grove (815-439-2885)Wesmere (815-439-3244)
Page 23

Elementary School Locations and TimesCentral
23723 Getson DrivePlainfield, IL 60544815-436-9278Fax: 815-436-8415
Charles Reed2110 Clublands ParkwayPlainfield, IL 60586815-254-2160Fax: 815-254-9385
Creekside13909 S Budler RoadPlainfield, IL 60544815-577-4700Fax: 815-372-0607
Crystal Lawns2544 Crystal DriveJoliet, IL 60435815-436-9519Fax: 815-436-8433
Eagle Pointe24562 Norwood DrivePlainfield, IL 60585815-577-4800Fax: 815-609-9403
Eichelberger12450 S Essington RoadPlainfield, IL 60585815-577-3606Fax: 815-577-6407
Freedom11600 Heritage Meadows DrivePlainfield, IL 60585815-254-4005Fax: 815-254-9706
Grand Prairie3300 Caton Farm RoadJoliet, IL 60431815-436-7000Fax: 815-436-1233
Lakewood Falls14050 S Budler RoadPlainfield, IL 60544815-439-4560Fax: 815-886-0463Full-day: 8:55 a.m. - 3:30 p.m.
Liberty1401 Essington RoadBolingbrook ,IL 60490815-609-3037Fax: 815-609-5963
Lincoln14740 Meadow LanePlainfield, IL 60544815-577-4500Fax: 815-609-5853
Meadow View2501 Mirage AvenuePlainfield, IL 60586815-439-4828Fax: 815-436-3747
Ridge1900 Caton Ridge DrivePlainfield, IL 60586815-577-4630Fax: 815-609-9387
River View2097 Bronk RoadPlainfield, IL 60586815-439-4840Fax: 815-436-4930
Thomas Jefferson1900 Oxford WayJoliet, IL 60431815-577-2021Fax: 815-254-6862
Walker's Grove24810 W 135th StreetPlainfield, IL 60544815-439-2885Fax: 815-439-2883
Wesmere2001 Wesmere ParkwayPlainfield, IL 60586815-439-3244Fax: 815-439-3413
Kindengarten does not meet on half days or five hour days. Kindergarten AM classes will not meet on late start days, but PM classes will meet at the regular time.
School Day All Schools except Lakewood Falls Lakewood Falls Elementary Star Plus
Program (Central)Full Day 9:05 AM - 3:40 PM 8:55 AM - 3:30 PM 8:55 AM - 3:30 PM5 hour To Be Determined To Be Determined To Be DeterminedEarly Release Day To Be Determined To Be Determined To Be DeterminedHalf Day 9:05 AM - 12:05 PM 8:55 AM - 11:55 AM 8:55 AM -11:55 AMLate Start 11:05 AM - 3:40 PM 10:55 AM - 3:30 PMAM 9:05 AM - 11:50 PM 8:55 AM - 11:40 PMPM 12:55 PM - 3:40 PM 12:45 PM - 3:30 PM
Bonnie McBeth Learning Center: (does not meet on half days or five hour days)Morning: 8:00 AM - 3:00 PM Special: 8:00 AM - 1:00 PMAfternoon: 12:30 PM - 3:00 PM Autism Program: 10:00 AM - 3:00 PM
Page 24


Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Kindergarten Health RequirementsDear Kindergarten Parents/Guardians,
The District 202 nursing staff welcomes you and your child as he/she begins kindergarten.
Incoming kindergarten students must have the following health examinations on file at your child's school according to the Illinois Department of Public Health and PSD 202 Board of Education policy.
⦁ A physical examination that has taken place on or after August 17, 2016. Students without a physical examination and list of current immunizations will not be allowed to start on the first day of school per District 202 Board of Education policy. The examination must be signed by the medical provider and be recorded on the Certificate of Child Health Examination form (11-15). The health history section of the examination form must be completed and signed by the parent. All students age 6 and under must have the lead screening section completed by the medical provider. In addition, the diabetes screening section must also be completed.⦁ The immunizations required for kindergarten entry are:
⦁ Four or more doses of DTP/DTaP with the last dose received on or after the 4th birthday⦁ Four or more doses of the same type of Polio vaccine, with a booster given on or after the 4th
birthday. There must be at least 6 months between the 3 dose series and the booster.⦁ Two doses each of measles, mumps and rubella (usually given as MMR) with the first dose on or
after the 1st birthday and the second dose no less than four weeks later⦁ Two doses of varicella (chicken pox) with the first dose on or after the 1st birthday and the
second dose no less than four weeks later⦁ A dental examination is to be on file at your child's school before May 15, 2018. This examination must
be recorded on the Proof of School Dental Examination form and has to have taken place on or after November 15, 2016.
⦁ An eye examination is to be on file at your child's school by October 15, 2017. The eye exam must be recorded on the Illinois Eye Exam Report and needs to have taken place on or after August 17, 2016.
Please make your doctor's appointments early. Doctor's offices are very busy during the summer months with back-to-school appointments and it will get very difficult to get an appointment as the first day of school approaches. Please make copies of all papers submitted and keep them for your records.Child Health Examination forms, Dental exam forms and Vision exam forms, as well as a list of district nurses and their phone numbers may be found at www. psd202. org > Departments and Programs > Health Services. If your child has any specific health care needs such as diabetes, allergies, asthma, seizure disorder or medication that is to be taken at school, please contact the nurse at your child's school before classes begin.
Sincerely,Jill Accardo, BSN, MBA, RN, PEL-CSN, NCSN,Nursing CoordinatorOn behalf of all PSD 202 nurses
Page 26

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
TRANSPORTATION OFFICE14812 S. Eastern Avenue, Plainfield, IL 60544
PHONE: (815) 436-7800 FAX: (815) 439-4830
TRANSPORTATION POLICY FOR STOP LOCATION OTHER THAN STOP ASSIGNED TO HOME ADDRESS
During the school year, students may be transported to / from one stop address other than their home bus stop; however, the stop must be for every day of the week. The stop address must also be within the student's school attendance boundaries.
The four possible choices for bus transportation are:1. Pick up at home; drop off at home.2. Pick up at home; drop off at sitter.3. Pick up at sitter; drop off at sitter.4. Pick up at sitter; drop off at home.
Students who are transported to / from a bus stop other than their assigned stop must have a parent / guardian signed transportation request form on file at the District’s Transportation Department. A copy of that form is on the next page. Additional copies are available in each school’s main office or at the District Office.
Requests received by the District Transportation Office will become effective after (3) threeschool days.
Page 27

Transportation Sitter FormStudents who are regularly transported to or from a bus stop other than the one assigned for their home address must have a signed, current request on file at the District’s Transportation Office. Sitter forms must be re-submitted annually. Requests are granted based on current seats available, time schedules, and must be within the attendance boundaries of the school your child is attending. Information is also requested if District 202 does not transport the student due to day care center/sitter or parent transportation. Transportation must be to the same address 5 days per week. The address provided for morning transportation may be different from the afternoon address.
Please return this form to: TRANSPORTATION OFFICE14812 S. Eastern AvenuePlainfield, IL 60544
Or fax it as soon as possible to: (815) 439-4830
The District Transportation Office Requires a three (3) day notice (working days) to implement busing changes during the school year and a 2 week notice prior to start up of a new school year.
If you have any questions, please call Transportation at 815-436-7800
REQUEST TO TRANSPORT STUDENT TO/FROM DIFFERENT BUS STOP
STUDENT’S NAME:(Last Name) (First Name)
SCHOOL: GRADE:
HOME ADDRESS: CITY: ZIP:
HOME PHONE NUMBER: HOME SUBDIVISION:
WORK PHONE NUMBER(S) OF PARENT/GUARDIAN(S):
DAD: MOM:
SITTER’S NAME:
SITTER’S ADDRESS: CITY: ZIP:
SITTER’S PHONE NUMBER: SITTER’S SUBDIVISION:
Select the time of day to be bused to and/or from the sitter: To school only From school only Both ways
DATE FOR BUSING TO START AT SITTER:
ADDITIONALCOMMENTS:
PARENT / GUARDIAN NAME PRINTED:
SIGNATURE: DATE:
Adult providing childcare is required to sign the statement belowI acknowledge the above named student is in my care as indicated above requiring transportation from the bus stop associated to my address. I understand I am responsible they arrive to and/or from the bus stop safely, and am responsible for their behavior at the bus stop. SITTER'S SIGNATURE: DATE:
Page 28
Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Medication Authorization Form
1. Medications, which include both PRESCRIPTION DRUGS and OVER-THE-COUNTER, to be taken during the school day will only be administered after the parent/guardian, and physician, Advanced Practice Nurse, or Physician Assistant completes the Plainfield School District 202 "Medication Authorization Form". The form is available from the building nurse or the district website. This form must be filled out at the beginning of each school year or when a new medication is to be given.
2. The first dosage of medication should not be given at school in case the student suffers an allergic or other adverse reaction.
3. Prescription Medication must be brought to school by a parent/guardian and must be in the original pharmaceutical container labeled with the student’s name, name of medication, the dosage and all pertinent instructions. Over-the-Counter medication must be brought to school by a parent/guardian in its original unopened / sealed container with the student’s name affixed to the container. If it is absolutely impossible for parents to bring the medication to school, we askthat students, upon their immediate arrival to school, turn the medication into the health office in a sealed envelope. Unused medication should be picked up by parent/guardian at the end of each school year. If the parent/guardian does not pick up the medication by the last day of school, the building nurse will dispose of and document that medications were discarded. Medications will be discarded in the presence of a witness.
4. Medication will be stored in the school in a safe place. The student must come to the school’s nurses office for his/her medicine. The school will strive to assist students to remember to come to the office to take his/her medication.
5. Students are prohibited from keeping any kind of medication in their possession while at school, except where a student is authorized to self-administer an epinephrine auto-injector (EpiPen®), diabetic care supplies or asthma medication. Students must have the Emergency Medication Hold Harmless and Indemnity Form signed by their parents/guardian and physicians to keep their inhalers, diabetic care supplies, or epinephrine auto-injectors with them in school. In case of emergency or loss of these items, we recommend that these students also keep an additional inhaler, diabetic care supplies, or epinephrine auto-injector in the health office.
6. Acknowledging that occasionally a medication must be administered during the school day, a certified school nurse or registered professional nurse, if available, shall administer the medication. If a nurse is unavailable, a building administrator or other staff member who volunteers may either:
a. Supervise the self-administration of the medication; or b. Administer the medication himself/herself.
7. Medications will generally not be administered to students during field trips or other school-sponsored activities located away from the customary site of storage of the medication. In these situations, medication will only be administered to a student if absolutely necessary for the critical health and well-being of the student as documented in a student’s individualized health care plan or Emergency Allergy Action Plan. Medication to be administered in these situations must be sent to school by a parent/guardian, in a pharmaceutical container labeled with the student’s name, name of medication, dosage and all pertinent instructions. The administration protocol will be determined by District staff.
Revised 1/13/2018 Page 29

Plainfield CCSD 202 and its employees and agents are to incur no liability, except for willful and wanton conduct, as a result of any injury arising from the administration or self-administration of medication pursuant to these procedures.
Student InformationName Birth DateSchool Grade
Parent Phone NumbersHome Phone Work Phone Emergency Phone
PARENT'S REQUEST FOR MEDICATION ADMINISTRATIONI hereby request that Plainfield School District 202 administer to my child during school hours, the drug(s) ordered byDr. Physician’s Phone REQUIRED
I have determined that the following medication(s) must be taken during school hours.Enter each medication needed in a separate box below. Use an additional form if more than 4 medications are needed.
LICENSED PRESCRIBER'S ORDER EXAMPLE ▼ Only enter one of these ▼
Drug Dosage(mg/mL) Time given
orFrequencySide effects Route
Diagnosis Start dateEnd date
Physician’s Signature
Acetaminophen (Tylenol) 325mg Enter specific time(s)Enter interval of timeUpset stomach p.o.
Headaches, pain 1/1/2018
Dr. ExampleLICENSED PRESCRIBER'S ORDER FOR MEDICATION # 1 ▼ Only enter one of these ▼
Drug Dosage(mg/mL) Time given
orFrequencySide effects Route
Diagnosis Start dateEnd date
Physician’s Signature
LICENSED PRESCRIBER'S ORDER FOR MEDICATION # 2 ▼ Only enter one of these ▼
Drug Dosage(mg/mL) Time given
orFrequencySide effects Route
Diagnosis Start dateEnd date
Physician’s Signature
LICENSED PRESCRIBER'S ORDER FOR MEDICATION # 3 ▼ Only enter one of these ▼
Drug Dosage(mg/mL) Time given
orFrequencySide effects Route
Diagnosis Start dateEnd date
Physician’s Signature
LICENSED PRESCRIBER'S ORDER FOR MEDICATION # 4 ▼ Only enter one of these ▼
Drug Dosage(mg/mL) Time given
orFrequencySide effects Route
Diagnosis Start dateEnd date
Physician’s Signature
The physician's signature is REQUIRED on each medication listed above.(All orders will expire on August 1st if no end date is specified)
Parent/Guardian Signature Received by Nurse DatePage 30

Page 31

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Guardianship AffidavitWhen the child does not live with natural or adoptive parent or court ordered guardian.
I.Answers to the following inquiries are necessary in determining residency for school attendance. This form is to be completed by the adult who demonstrates, that he or she has assumed legal responsibility over the student, and provides the student with a regular fixed nighttime dwelling. (Subject to approval by school administration)
II.IF YOU PROVIDE AN ANSWER WHICH YOU KNOW IS FALSE, YOU CAN BE CRIMINALLY PROSECUTED FOR PERJURY.
III. General Information1.
2.
3.4.
5.6.
7.
Name of studentAgeGrade in schoolAddress where student presently lives
Name of MotherWhere does Mother live?
Name of FatherWhere does Father live?
Are parents divorced?
IV.8.9.10.
Who has custody of student?What is the date of the divorce decree?A certified copy of the divorce decree, order of custody and/or joint parenting agreement and any amendments thereto must be furnished.
Page 32

Guardianship AffidavitWhen the child does not live with natural or adoptive parent or court ordered guardian.
V. IF STUDENT IS NOT LIVING WITH A PARENT:11.
12.
13.
14.
15. a.
b.
c.
d.
16.
a.
b.
c.
d.
e.
f.
g.
h.
i.
Name of person(s) with whom the Student lives.
What is your relationship to the student?
Your present address.
Your present phone number.
Does the student live with you full-time?
If part-time, state what portion of time the student lives with you and where and with whom he or she
When did the student begin living with you?
How long do you intend to have the student live with you?
Indicate below the times the student will visit his or her custodial parent at his or her present address during the upcoming year.
Approximately how many nights (including weekends)
Approximately how often at meal times (including weekends)
Approximately how often on weekends
Approximately how often on weekdays
Winter (Christmas) vacation
Spring vacation
Approximately how many school holidays
Summer vacation
Other
Page 33

Guardianship AffidavitWhen the child does not live with natural or adoptive parent or court ordered guardian.
17.
a.
b.
c.
d.
e.
f.
g.
h.
i.
18. State the reason(s) why the student is living with you:
19. List the names and locations of each school the student has attended during the past five years and the dates of attendance.
20. a.
b.
c.
Indicate below the times the custodial parent will visit the student during the upcoming year.Approximately how many nights (including weekends)
Approximately how often at meal times (including weekends)
Approximately how often on weekends
Approximately how often on weekdays
Winter (Christmas) vacation
Spring vacation
Approximately how many school holidays
Summer vacation
Other
Do you own a residence (home)?
If so, what is the address?
Are you occupying your present place of residence as a tenant?
Page 34

Guardianship AffidavitWhen the child does not live with natural or adoptive parent or court ordered guardian.
d.
e.
21. a.
b.
c.
d.
22. a.
b.
c.
d.
23.
24.
a.
b.
c.
If so, give the name and address of your landlord or management company.
How long do you intend to reside at the place where you are presently residing?
Who provides the student’s living expenses and costs?
If living expenses and costs are shared, please indicate the arrangements for sharing such expenses.
Is the person(s) with whom the Student is staying paid any money for food, housing, or for keeping the student?
Do you pay any money for the student?
Who is responsible for the discipline and control of the student?
Does the person(s) with whom the Student is staying have authority to discipline the student?
Who is financially responsible for any damages caused by the student?
In the event of an accident or other emergency, who may direct and consent to medical treatment and sign any releases required?
Briefly state who enrolled the Student in the School District and the reasons why the Student was enrolled in the District.
Do you have court approved custody or guardianship of the student?
If yes, why was the guardianship secured?
Attach copies of any agreements, judgments, decrees or other documents awarding or giving custody of the named student to any person. If to your knowledge there are no such documents, please check below.
No such documents
If not, state the name and address of the person who does:
Page 35

Guardianship AffidavitWhen the child does not live with natural or adoptive parent or court ordered guardian.
25.
26.
27.
28.
29.
30.
31.
a.
b.
32.
33.
Where did the Student reside during the previous summer?
Who declares the Student as a dependent for income tax purpose?
Who is authorized to receive report cards?
Who would attend Parent conferences at the school?
Who would receive notifications in case of Student discipline, suspension or expulsion?
On Saturdays and Sundays, where does the Student stay?
Where does the Student take his or her meals?
From Monday through Friday?
On Saturdays and Sundays?
List the names and ages of any brothers and sisters, where they live and where they attend school.
Name Age Address School Attended
Provide any additional information which may help to establish your residency and the student’s residency or which is otherwise relevant to the question.
Page 36

Guardianship AffidavitWhen the child does not live with natural or adoptive parent or court ordered guardian.
In executing this affidavit, I acknowledge having read and understand the following:
"If a pupil is determined to be a nonresident of the District for whom tuition is required to be charged pursuant to this section, the School Board shall refuse to permit the pupil to continue attending the schools of the District unless the required tuition is paid for the pupil." "A person who knowingly or willfully presents to any School District any false information regarding the residency of a pupil for the purpose of enabling that pupil to attend any school in that District without the payment of a non-resident tuition charge shall be guilty of a Class C Misdemeanor." (105 ILCS 5/10-20.12b)
I understand that if the information provided in connection with this Affidavit is determined to be false or misleading, resulting in the child/children named above to not be legally entitled to attendance in Plainfield Community Consolidated School District 202, the School District will take legal action to recoup valid tuition charges and legal fees.
The Student’s residence within the School District has not been established solely for the purpose of attending the schools thereof. The foregoing facts are sworn to in order to induce the School District to enroll the student in the schools of the District.
I certify that I understand the residency requirements and that I know the penalty for fraudulent registration.
I HEREBY SWEAR THAT THE ANSWERS TO THE FOREGOING QUESTIONS ARE TRUE AND CORRECT AND I UNDERSTAND THAT I MAY BE SUBJECT TO CRIMINAL PROSECUTION FOR PERJURY IF I HAVE KNOWINGLY ANSWERED ANY OF THE QUESTIONS FALSELY.
Signature Date
STATE OF ILLINOIS)
SS.)
COUNTY OF WILL)
I do hereby certify that on the ____ day of __________________, 20____,
Did state on oath that the answers to the questions on the foregoing document were true and correct to the knowledge of the affiant.
Notary Public
▼ N
otar
y Se
al ▼
Page 37

Plainfield Community ConsolidatedSchool District 202We prepare learners for the future.
Administration Center15732 Howard StreetPlainfield, IL 60544
(815) 577-4000 – telephoneWeb: www.psd202.org
Residency Affidavit**must be updated in the spring of each year**
Residency Requirements when the Parent/Legal Guardian does not own or lease the residence, consists of the following:The parent/legal guardian must provide 2 proofs of residency in addition to completing the residency affidavit.AND The homeowner must provide 3 proofs of residency.
Residency Requirements Parent/Legal Guardian: 3 proofs of residency with parent/legal guardian name and current address are required. You will need a notarized residency affidavit as well as to 2 proofs from Category B.
Category AResidency Affidavit - Completed & Notarized
Category BMUST BE ISSUED WITHIN THE LAST3 MONTHS (6 months for driver's license)
Auto registrationHomeowners or renters insuranceDriver’s license or state identificationPhoto identification from foreign consulate
MUST BE ISSUED WITHIN THE LAST30 DAYS
Cable billUtility bill – gas, electric, waterLetter from government agencyBank statement
Homeowner: 3 proofs of residency in the homeowner’s name with an address within School District 202 boundaries are required, with at least one document from category C and one document from category D.
Category CRecent Real Estate Tax BillLease (signed showing date of occupancy with landlord’s name and phone number)Settlement statement (signed and within 30 days)Truth in lending statement (signed and within 30 days)Warranty deed (within 30 days)Mortgage statement / Payment book (within 30 days)Bill of Sale (within 30 days)Military housing letter
Category DMUST BE ISSUED WITHIN THE LAST3 MONTHS (6 months for driver's license)
Auto registrationHomeowners or renters insuranceDriver’s license or state identificationPhoto identification from foreign consulate
MUST BE ISSUED WITHIN THE LAST30 DAYS
Cable billUtility bill – gas, electric, waterLetter from government agencyBank statement
Page 38

Residency AffidavitPlainfield Community Consolidated School District 202
PARENTS/GUARDIAN MUST COMPLETE THIS SECTION AND FURNISH TWO (2) PROOFS OF RESIDENCY. SEE CATEGORIES A & BTHIS AGREEMENT AUTOMATICALLY TERMINATES ON THE LAST DAY OF THE 2018-2019 SCHOOL YEARI, verify that my child(ren) and I live at Apt
City Zip CodeOur residence within this district has been established because:
We intend to remain at this residence untilPrevious home phone Previous address Apt
City Zip CodeName of Child Grade District 202 School
I understand residence information may be verified by a home visit and that I must notify the school immediately in writing when I move out. Falsification of residency information on this document will be grounds for removing student(s) from the Plainfield School District and tuition fees will be assessed from the first day of student attendance. I am aware that under Illinois state law that it would be classified a Misdemeanor for Falsification of information and I could face criminal prosecution. I affirm (declare) under penalty of the law that the foregoing is true and correct.ONLY SIGN IN FRONT OF A NOTARY.
Signature of Parent/Legal Guardian Print name of Parent/ Guardian Home Phone
Subscribed and sworn to before me on this ________ day of __________________, 20____
Signature of Notary
Business Phone
▼ N
otar
y Se
al ▼
DISTRICT RESIDENT MUST COMPLETE THIS SECTION AND FURNISH THREE (3) PROOFS OR RESIDENCY. SEE CATEGORIES C & D.
I, verify thatand their child(ren)are living with me in my home at Apt
City Zip CodeUtility bills are paid by me. I understand residence information may be verified by a home visit and that I must notify the school immediately, in writing, when the above-named family moves out of my home. I understand that Under the Illinois state law that it would be classified a misdemeanor for falsification of information and I could face criminal prosecution. I affirm (declare) under penalty of the law that the foregoing is true and correct. Enrollment will be terminated immediately should it be determined that the residency requirements are not being met.ONLY SIGN IN FRONT OF A NOTARY.
Signature of District Resident Print Name of District Resident Home Phone
Subscribed and sworn to before me on this ________ day of __________________, 20____
Signature of Notary
Business Phone
▼ N
otar
y Se
al ▼
Page 39