kinerja expansion: health system strengthening …
TRANSCRIPT

i
KINERJA EXPANSION: HEALTH SYSTEM STRENGTHENING AND
BASIC EDUCATION IN PAPUA FINAL REPORT
March 2012 — March 2017
[REDACTED]

Kinerja Expansion: Health System Strengthening and Basic Education in
Papua Final Report
Cooperative Agreement No: AID-497-A-10-00003 March 15, 2012, through March 29, 2017
Prepared for Office of Democratic Governance
USAID/Indonesia Jl.Budi Kemuliaan I/1
Jakarta 10110
Prepared by RTI International1
3040 Cornwallis Road Post Office Box 12194
Research Triangle Park, NC 27709-2194 DISCLAIMER The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government.
1 RTI International is a trade name for Research Triangle Institute.
iii
List of Figures ....................................................................................................................... v
List of Tables ........................................................................................................................ v
Terms and Abbreviations ...................................................................................................... vi
Executive Summary .............................................................................................................. 1
Program Achievements ..................................................................................................... 3
Lessons Learned and Recommendations .......................................................................... 7
Introduction ........................................................................................................................... 9
Program Overview ............................................................................................................. 9
Kinerja Approach ............................................................................................................. 12
Cost Share ...................................................................................................................... 16
Health ................................................................................................................................. 18
Strengthening Management and Leadership for Health Service Delivery ........................ 18
Provincial and District Engagement ................................................................................. 21
Puskesmas Management ................................................................................................ 22
Combating Gender-Based Violence ................................................................................ 23
Health Workers’ Absenteeism Study ............................................................................... 25
Education ............................................................................................................................ 27
Good Governance ............................................................................................................... 32
[REDACTED] ................................................................................................................... 32
Media .............................................................................................................................. 32
Minimum Service Standards ............................................................................................ 34
Multi-Stakeholder Forums................................................................................................ 37
Replication .......................................................................................................................... 40
District- and Provincial-Level Replication ......................................................................... 40
National-Level Replication Efforts .................................................................................... 48
Sustainability ....................................................................................................................... 56
Monitoring & Evaluation ...................................................................................................... 60
October 2012 – June 2015 .............................................................................................. 60
October 2015 – December 2016...................................................................................... 70
Lessons Learned and Recommendations ........................................................................... 77
Table of Contents

iv
Program Design .............................................................................................................. 77
Program Management ..................................................................................................... 79
Program Content and Implementation ............................................................................. 79
Annex 1: Kinerja Papua Partner Districts ............................................................................ 82
Annex 2: Intermediary Organizations .................................................................................. 83
Annex 3: Learning Materials................................................................................................ 85
v
Figure 1: The Public Service Delivery Cycle ............................................................... 15
Table 1: Kinerja-Supported Puskesmas ..................................................................... 19
Table 2: Kinerja-Supported Schools ........................................................................ 279
Table 3: Puskesmas-Level Replication of Kinerja’s Health Interventions ................... 43
Table 4: OCA Baseline and Endline Scores ............................................................... 64
Table 5: CSS Baseline and Endline Scores ............................................................... 67
Table 6: Kinerja Papua Indicator Achievements (October 2012–June 2015) ............. 69
Table 7: Kinerja Papua Indicator Achievements (October 2015–December 2016) ..... 76
List of Figures
List of Tables

vi
adat Traditional/Indigenous AIDS Acquired Immune Deficiency Syndrome ATM AIDS, Tuberculosis, and Malaria Badan Diklat Papua’s Education and Training Agency (Badan Pendidikan dan
Latihan) BaKTI Eastern Indonesia Knowledge Exchange or BaKTI Foundation (Yayasan
BaKTI) Balatkes Provincial Health Training Agency (Balai Pelatihan Kesehatan) Bappeda Local Government Agency for Regional Development Planning (Badan
Perencanaan Pembangunan Daerah) Bappenas National Development Planning Agency (Badan Perencanaan dan
Pembangunan Nasional) BEE Business Enabling Environment BOS School Operational Assistance (Bantuan Operasional Sekolah) BOSP Educational Unit Operational Cost Analysis (Biaya Operasional Satuan
Pendidikan) BP3AKB Women’s Empowerment, Child Protection and Family Planning Agency
(Badan Pemberdayaan Perempuan, Perlindungan Anak dan Keluarga Berencana)
Bupati District Head CSS Customer Satisfaction Survey CSO Civil Society Organization CSR Corporate Social Responsibility DEO District Education Office DHO District Health Office DPRD Local Legislative Council at either the provincial, district or municipal
level (Dewan Perwakilan Rakyat Daerah) EBP Evidence-Based Planning EDS School Self-Evaluation (Evaluasi Diri Sekolah) FGD Focus Group Discussion FY Fiscal Year GBV Gender-Based Violence GHI Global Health Indicator GJD Governing Justly and Democratically GOI Government of Indonesia HDI Human Development Index HIV Human Immunodeficiency Virus HSS Health System Strengthening IDR Indonesian Rupiah IMP Integrated Micro-Planning IPP Integrated Puskesmas Planning IPPM Institute for Community Development and Empowerment (Institut
Pengembangan dan Pemberdayaan Masyarakat) IR Intermediate Result ISO International Organization for Standardization ITAT Integrated Technical Assistance Team
Terms and Abbreviations

vii
Kabupaten District Kecamatan Subdistrict KemenPAN-RB Ministry for State Administrative and Bureaucratic Reform (Kementrian
Pendayagunaan Aparatur Negara dan Reformasi Birokrasi) KIPRa Independent Consultancy Foundation for People’s Empowerment
(Yayasan Konsultansi Independen Pemberdayaan Rakyat) KOPEL Legislative Monitoring Committee (Komite Pemantau Legislatif) Kota Municipality LAN State Administrative Bureau (Lembaga Administrasi Negara) LG Local Government LPMAK Community Empowerment Agency (Lembaga Pemberdayaan
Masyarakat Amungme dan Komoro) LPSS Local Public Service Specialist LSPPA Women and Children’s Development and Study Agency (Lembaga Studi
dan Pengembangan Perempuan dan Anak) M&E Monitoring and Evaluation MCH Maternal and Child Health MDGs Millennium Development Goals MOEC Ministry of Education and Culture MOH Ministry of Health MOHA Ministry of Home Affairs MOU Memorandum of Understanding MRP Papuan People’s Assembly (Majelis Rakyat Papua) MSF Multi-Stakeholder Forum MSS Minimum Service Standards NGO Nongovernmental Organization OCA Organizational Capacity Assessment Otsus Special Autonomy (Otonomi Khusus) OSS One-Stop Shop Pemekaran Proliferation of districts PEFT Provincial Education Facilitation Team PEO Provincial Education Office PHC Primary Health Care PHFT Provincial Health Facilitation Team PHMC Public Health Malaria Control PHO Provincial Health Office PKMK UGM Center for Health Management and Policy (Pusat Kebijakan dan
Manajemen Kesehatan) at Gadjah Mada University PMC Project Management Committee PMEP Performance Management and Evaluation Plan PML Performance Management and Leadership PPMN Indonesia Association for Media Development (Perhimpunan
Pengembangan Media Nusantara) P2TP2A Integrated Services Center for the Protection of Women and Children
(Pusat Pelayanan Terpadu Pemberdayaan Perempuan dan Anak) PSD Public Service Delivery PSS Public Service Standards Puskesmas Community Health Center (Pusat Kesehatan Masyarakat) RAD KtPA Regional Action Plan for the Prevention and Management of Violence
against Women and Children (Rencana Aksi Daerah Pencegahan dan Penanganan Kekerasan terhadap Perempuan dan Anak)
RKAS School Work Plan and Budget (Rencana Kerja Anggaran Sekolah) RTI Research Triangle Institute International SBM School-Based Management SD Elementary School (Sekolah Dasar)

viii
SDGs Sustainable Development Goals SDU Service Delivery Unit Sekda Regional Secretary (Sekretaris Daerah) SI Social Impact SKPD District Technical Working Unit (Satuan Kerja Perangkat Daerah) SMERU SMERU Research Institute SOP Standard Operating Procedure SUM Scaling Up for Most-at-Risk Populations TAF The Asia Foundation TB Tuberculosis TBA Traditional Birth Attendant TOT Training of Trainers TRIMS Tools of Reporting and Information Management by Schools UGM Gadjah Mada University (Yogyakarta) UNICEF United Nations Children’s Fund UP2KP Special Unit for the Acceleration of Health Development in Papua (Unit
Percepatan Pembangunan Kesehatan Papua) URD Proposed Definitive Plans (Usulan Rencana Definitif) USAID United States Agency for International Development USG United States Government Walikota Municipality Head/Mayor WLT Women’s Leadership Training WHO World Health Organization YAPEDA The AIDS Care Foundation (Yayasan Peduli AIDS) YHI Mothers’ Hope Foundation (Yayasan Harapan Ibu) YKP The Women’s Health Foundation (Yayasan Kesehatan Perempuan) YPK The Foundation for Christian Education (Yayasan Pendidikan Kristen) YUKEMDI Foundation for the Economic Welfare of Indonesia’s Rural Communities
(Yayasan Usaha Kesejahteraan Ekonomi Masyarakat Desa Indonesia)
Definitions: Districts: In this document, the term “districts” refers to both kabupaten (districts) and kota (municipalities) for purposes of simplicity. The term “target districts” refers to the geographical areas that received technical assistance.
HIV/AIDS: Recognizing that there exists a variety of debate and terminology within the public health sector, the term “HIV/AIDS” is used within this document to reflect USAID terminology used in Indonesia.

1
The US Agency for International Development (USAID)/Indonesia Local Governance Service Improvement (Kinerja) program, led by RTI International, focused on improving the delivery of public services in three sectors, health, education, and business-enabling environment (BEE), in four provinces in Indonesia (Aceh, East Java, South Sulawesi, and West Kalimantan), starting in September 2010. In March 2012, USAID expanded Kinerja’s mandate with an [REDACTED] award to focus specifically on governance in health system strengthening (HSS) in four target districts (Jayapura, Jayawijaya, Kota Jayapura, and Mimika) in the country’s easternmost province of Papua. Shortly before the closure of Kinerja’s core program in 2015, USAID provided the program with a further [REDACTED] million to extend the Papua program for 18 months. During this period, the program consolidated its health-sector achievements (with a greater focus on district and provincial engagement) and added a new component in Papua’s education sector, with the implementation of its public service-oriented school-based management (SBM) package at elementary schools in three target districts (Jayapura, Jayawijaya, and Kota Jayapura).2
2 Kinerja did not select Mimika for SBM, as the district already received substantial support at the elementary-school level from a local organization, the Amungme and Komoro Community Empowerment Agency (Lembaga Pemberdayaan Masyarakat Amungme dan Komoro).
Executive Summary
Students at Amai elementary school dance to welcome the USAID Indonesia Mission Director.

2
At the time of the Papua program’s launch in 2012, USAID had invested heavily in Papua’s health sector through a range of projects and partners. Although gains were made at the technical level, Papua’s health sector continued to be poorly governed. Through the expansion of the Kinerja program to Papua, the aim was to address this governance deficiency by identifying and targeting the key blockages to health service delivery in the province. Kinerja also sought to improve local government (LG) ability to provide quality services to those communities most at risk from human immunodeficiency virus/ acquired immune deficiency syndrome (HIV/AIDS) and tuberculosis (TB), and to strengthen maternal and child health (MCH) services.
When USAID further expanded the Papua program in 2015 to include SBM, it did so to address similar challenges in Papua’s education sector, which was characterized by weak educational management, high teacher and student absenteeism, and low levels of community involvement and participation. Drawing on its experience of implementing SBM in its core districts, Kinerja introduced the package in Papua to promote access to high-quality basic education and to improve school management, as well as to enhance the capacity of LGs to plan, manage, and budget for education services.
In order to strengthen health systems and enhance health and education outcomes in Papua, Kinerja drew on its core-program approach, which comprised the following three-element strategy:
1. Incentives: Strengthen demand-side entities for better services
2. Innovations: Build on existing innovative practices and support LGs to test and adopt promising service delivery approaches
3. Replication: Expand successful innovations nationally and support Indonesian intermediary organizations to deliver and disseminate improved services to LGs3
Kinerja’s efforts in Papua were aligned with its governance principles (accountability, transparency, participation, and responsiveness) and built upon the experience gained from its health and education interventions in the core program. Within the specific context of Papua, 3 In contrast to Kinerja’s work in its four core provinces, replication in Papua was defined as scaling up to new service delivery units within its target districts. This changed with the launch of Kinerja’s Papua cost extension in October 2015, when the program expanded its scope to strengthen its engagement with health- and education-sector stakeholders from the provincial government.
Box 1: Top 10 program achievements ▪ 38 community health centers (puskesmas)—12 partner and 26 non-
partner puskesmas—implemented Kinerja Papua health interventions. ▪ 771 promises (160 in health, 611 in education) were made by
puskesmas and schools via service charters. Of these, 100% of the puskesmas promises were fulfilled, while 20 of Kinerja’s 30 partner schools fulfilled more than 70% of their promises.
▪ 18 newly expanded school committees successfully advocated for village funding to help them improve their facilities and education services.
▪ All 3 target districts for school-based management (SBM) made formal commitments (via circular letters) to implement SBM at all remaining elementary and junior high schools in their districts.
▪ [REDACTED] allocated by the provincial education office to replicate SBM at schools across 15 of Papua’s least-developed districts.
▪ 90 citizen journalists plus 3 citizen journalist collectives remained active after the withdrawal of direct program support in 2015.
▪ 2 five-year action plans issued, with local government support, to combat violence against women and children in Kota Jayapura and Mimika. Integrated services teams also established in both districts to handle such cases.
▪ 7 district integrated technical assistance teams —4 for health, 3 for education—established, and 2 provincial facilitation teams (health & education) formed and/or strengthened to lead on replication efforts.
▪ 5 Kinerja policy recommendations adopted by technical ministries for nationwide application.
▪ 14 civil society organizations involved in the program.
3
Kinerja sought to tailor its technical assistance to be responsive to local conditions, urban and rural nuances, and distinctive characteristics in each of its target districts.
The program’s implementation methodology consisted of three interrelated components. The first of these was to base its interventions on existing policies and programs. To this end, Kinerja developed its district- and service delivery unit (SDU)-level interventions to reflect national-level priorities and programs. With its demand-oriented program design, Kinerja also consulted with LG and civil society stakeholders in each of its target districts to identify local needs and priority areas and then, as far as possible, tailor its support to meet those needs.
One key factor in Kinerja’s governance approach was the way in which the program introduced its health and education packages to a limited number of SDUs first (three health centers and a maximum of 12 schools per district) to pilot the interventions while at the same time improving LG knowledge and capacity. In this way, government partners could see firsthand how the innovations were applied in practice, enabling them to take the lead in expanding the interventions and implementing them at additional schools and health centers in their districts.
The second component in Kinerja’s approach was to support both the end users and providers of public services. Through raising awareness and building capacity within local communities, Kinerja supported the formation of multi-stakeholder forums (MSFs) at district and subdistrict levels, and trained and mentored citizen journalists, to stimulate local demand for better services, oversee the provision and implementation of services, and actively engage with their LG/SDU counterparts to work together to improve those services.
Finally, Kinerja sought to improve the chances of long-term sustainability by implementing each of its program interventions via local intermediary organizations. During the course of the program, Kinerja worked with a total of 14 intermediary organizations to implement its innovation packages in health and education, and to support demand-side stakeholders in the program’s cross-cutting areas of media and MSFs. Apart from three institutions that Kinerja identified and included in its initial proposal for the Papua program, the remaining 11 civil society organizations (CSOs), including four Papua-based organizations, were selected either through sole-source applications or limited competition.
Program Achievements
Health Kinerja’s health program focused on strengthening existing health systems and, through a range of governance interventions, building the capacity of LGs to improve health outcomes in their respective areas of focus: HIV/AIDS and TB (Jayapura and Jayawijaya) and MCH (Kota Jayapura and Mimika). Kinerja provided technical assistance to both community health centers (puskesmas) and district health offices (DHOs). In January 2016, the program withdrew direct support to puskesmas in order to further strengthen the capacity of DHO partners in Jayapura, Jayawijaya and Kota Jayapura, and to engage more fully with provincial-level authorities to promote wider replication.
• Between 2013 and 2015, Kinerja trained a total of 318 officials (73% women) from DHOs and puskesmas to improve their management and leadership skills. Collectively, they produced a total of 310 short-, medium-, and long-term action plans to improve services directed at HIV/AIDS, TB, and MCH. Of this total, 69 were implemented by DHOs, while a further 206 were implemented by Kinerja’s 12 partner puskesmas.
• Kinerja’s Organizational Capacity Assessment (OCA) found a significant improvement in how puskesmas managers incorporated governance principles into their work between

4
2013 and 2015. Transparency scores increased by 20% on average, accountability by 16%, communication participation by 27%, and responsiveness by 29%.
• Kinerja assisted its DHO partners to establish integrated technical assistance teams (ITATs), which are responsible for supervising puskesmas, providing targeted mentoring and leading replication efforts. During 2016, ITATs conducted a series of monitoring visits to 20 puskesmas using newly developed guidelines and checklists. ITATs have reported faster follow-ups from DHO heads based on the new system, with improvements implemented more quickly. DHOs have indicated they will allocate further funding for these teams in 2017.
• Two of Kinerja’s partner puskesmas in Jayapura, Puskesmas Dosay and Depapre, were voted the district’s best performing puskesmas in 2015. Dosay also went on to become one of the first puskesmas in Papua to receive government accreditation in 2016, a proud moment for the Jayapura DHO.
• Supported puskesmas now have strong complaint-handling mechanisms in place. They have implemented complaint surveys, developed and fulfilled service charters, and improved their complaint management processes in general, such as through including the community in handling complaints. Most puskesmas also now have complaint-handling teams.
Education In line with its cost extension work plan, Kinerja launched an education-sector intervention in November 2015 to address some of the key challenges in Papua’s education sector. Drawing on one of the national government’s priorities—to improve performance in the management of schools across the country—Kinerja implemented its public service-oriented SBM package at 30 elementary schools in three target districts (Jayapura, Jayawijaya, and Kota Jayapura). As with its efforts in health, the program also strengthened the capacity of district and provincial education stakeholders to improve the delivery of education services both within partner districts and across the province.
• Kinerja successfully revitalized school committees, in line with its “expanded committee” model, at its partner schools. This model encourages the inclusion of key local leaders, such as religious and traditional leaders, in school committee. As a result, 18 newly expanded school committees advocated for and received village funding to improve school facilities and services.
• Around 40% of Kinerja’s partner schools have either published or made available to the public midterm and annual work plans and/or financial reports. Previously, such information was generally unavailable, and parents were unable to access these documents to see how their children’s schools were performing.
• All partner schools conducted their first-ever complaint surveys to gather feedback on education services. A total of 3,237 respondents participated in the surveys, which became known locally as kantong noken, the Papuan term for commonly-used woven bags.
• The complaint surveys produced 334 technical recommendations, concerning issues beyond the capacity and/or authority of schools to resolve on their own, which were submitted to district education offices (DEOs) for follow-up.
• Reflecting Kinerja’s approach in the health sector, district ITATs were also established in conjunction with the program’s DEO partners. Equipped with new guidelines and

5
checklists, the ITATs conducted monitoring visits to schools and developed additional technical recommendations for follow-up by schools and/or DEOs.
Good Governance Kinerja complemented its efforts to improve the provision of services in health and education by supporting initiatives that cut across the two sectors with the aim of improving governance in public service delivery (PSD). To this end, the program sought to engage the participation of civil society and media to promote and oversee the issue of public service-related governance, and supported the application and integration of minimum service standards (MSS) to promote reforms in health and education.
Kinerja’s media program focused on building relationships with mainstream media to improve coverage of PSD issues, and training and mentoring citizen journalists. Using both mainstream and alternative media to communicate key messages, the program sought to enhance people’s understanding of their health and education rights, as well as to stimulate demand for public service reforms among local communities and promote their involvement in efforts to improve service quality. During the cost extension, Kinerja focused on strengthening links between citizen journalists and mainstream media outlets to provide access to broader audiences and to raise public-service issues that might otherwise have gone unreported in both the health and education sectors.
• Forum Lenteng established the Halaman Papua website in 2013 to showcase the work produced by Kinerja citizen journalists, whose articles focused on social justice and public-service issues in Papua. The website, which is actively updated, is one of only a handful of Papua-dedicated online resources.
• In 2016, Kinerja facilitated a series of media tours to partner schools and puskesmas. These tours allowed both mainstream media journalists and citizen journalists to learn firsthand about key education and health issues, and help raise awareness. As a result, two newspapers (Salam Papua and Harian Papua) that had not previously been involved with Kinerja began to request citizen journalist articles for publication.
• One new feature of Kinerja’s media intervention was the Youth Journalist (Jurnalis Cilik) program, which was delivered at five partner schools. This program aimed to encourage the next generation of citizen journalists, as well as to spark children’s interest in improving education services. The program proved popular at all the schools, and a short booklet was produced and distributed to interested teachers, nongovernmental organizations (NGOs), and media outlets to assist them in implementing their own Youth Journalist activities.
With regard to MSS, Kinerja provided technical assistance to LG stakeholders to improve the application of service standards in the planning and budgeting of health and education services. The program also aimed to improve the governance of these services based on nationally mandated indicators and targets, whose application is governed by Government Regulation No. 65/2005 on the Preparation and Implementation of MSS.
• In 2014, for the first time, DHOs in Jayapura, Kota Jayapura, and Mimika established MSS costing teams (comprising DHO staff and MSF members), completed all the necessary stages to apply MSS costing to midterm and annual planning and budgeting, and successfully evaluated their MSS achievements.
• DHO allocations for achieving MSS targets were increased in three of Kinerja’s partner districts. In 2014, LGs in Jayapura, Kota Jayapura, and Jayawijaya allocated [REDACTED], respectively, toward MSS fulfillment.

6
• Kinerja also supported puskesmas to produce MSS-based activity plans. In 2016, the program repeated this process using a new Integrated Puskesmas Planning (IPP) mechanism, co-developed with the United Nations Children’s Fund (UNICEF), which aligned health center planning with DHO planning and budgeting. Moreover, the IPP process allowed for community feedback to ensure the health center plans were appropriate to local needs. Public consultations also led in some cases to new funding from villages for puskesmas activities. In Jayapura, for example, Puskesmas Depapre’s public consultation resulted in village heads agreeing to cover the operational costs of safe delivery houses, which provide medical services to expectant mothers.
One of the Kinerja program’s most distinctive features was its focus on demand-side stakeholders —namely the end-users of public services—as well as to LGs providing the services. The program promoted civil society engagement by establishing or revitalizing local community-based MSFs at both the district level and at puskesmas and schools (school committees) to monitor service delivery and advocate for service improvements.
• By the end of the Kinerja Papua program, LGs had issued 13 health MSFs with governing decrees, giving them legal status and access to funding. Subsequently, MSFs garnered increased appreciation and recognition from their local DHOs, which began to recognize the important role they play in helping to improve public services.
• Some MSFs achieved success in advocating for service improvements. The district MSF in Jayapura, for example, obtained village funding to recruit additional health volunteers to assist puskesmas by monitoring and supporting TB patients. Also, the MSF at Puskesmas Musatfak successfully advocated to the Jayawijaya DHO for the construction of a new puskesmas building, and the renovation of the former puskesmas to become a safe delivery house for expectant mothers.
• As part of its commitment to mainstream gender in all areas of its work, Kinerja developed and conducted a three-stage Women’s Leadership Training in 2016 for 35 women members of health MSFs. By the end of the training, which included a number of practice sessions and role plays, 94% of participants said they felt either “very ready” or “ready” to take up gender inequality issues with cultural leaders in their areas (up from 23% prior to the final stage).
Replication Replication was a fundamental aspect of Kinerja Papua’s overall strategy, which aimed to build ownership and commitment among LGs to improve PSD beyond the program’s initial SDUs in partner districts and, during the cost extension, beyond partner districts. Kinerja’s basic design supported replication in two ways: first, by basing its interventions on existing good practices and national programs, and second, by implementing its sectoral interventions through intermediary organizations. The program’s replication strategy consisted of documenting and disseminating good practices, encouraging exchange between partner districts, and promoting the adoption of interventions at the provincial level.
• Prior to the cost extension, 30 Kinerja good practices were replicated at 17 additional puskesmas in the four partner districts. This number increased by 9 to 26 puskesmas by the end of the program (in addition to the original 12 partner puskesmas). Costs involved in replication were jointly covered by LGs, puskesmas, and Kinerja.
• Five subdistrict head decrees were issued to formalize new MSFs at replication puskesmas in Kota Jayapura in 2016. These decrees provide the MSFs with legal status
7
and allow them to request government and village funding for their activities in supporting PSD oversight.
• In implementing its new IPP mechanism, Kinerja supported five non-partner puskesmas (in addition to nine partner puskesmas) to develop proposed activity plans for 2017. In Kota Jayapura, these plans were incorporated into the DHO’s planning documents. The DHO head was so enthusiastic about the new mechanism that he instructed the remaining eight puskesmas in the district to immediately develop similar plans for integration. Meanwhile in Jayapura, the head of the DHO allocated funds to replicate the IPP process at all 19 puskesmas in the district in 2017.
• Partner DEOs issued circular letters in 2016 instructing all elementary and junior high schools to implement Kinerja’s SBM program. The letters specifically instruct the schools to implement key features in SBM, including developing annual and four-year midterm work plans and budgets, based on MSS analysis relevant to each school, and the results of school self-evaluations. Replication has already begun in Jayapura, where with program support, the district education council assisted two non-partner schools to conduct their first-ever complaint surveys in November 2016.
• At the provincial level, Kinerja supported the Provincial Education Office (PEO) to establish a special team to oversee the replication of public service-oriented SBM at new elementary and junior high schools in underdeveloped districts across Papua. The PEO allocated [REDACTED] to cover the costs of its expansion plan for 2017.
• Kinerja assisted both the Provincial Health Office (PHO) and PEO to develop Special Autonomy (Otonomi Khusus or Otsus) guidelines, to improve the management and oversight of special autonomy funding in the health and education sectors. Despite the limited time available for implementation, both sets of guidelines were produced and disseminated to all 29 DHOs and DEOs across Papua, for use in 2017.
In addition to its replication efforts at district and provincial levels, Kinerja also disseminated its good practices among national-level stakeholders and achieved good buy-in for the wider replication of its interventions.
• In 2016, Kinerja re-engaged with Indonesia’s State Administrative Bureau (Lembaga Administrasi Nasional [LAN]), which sought to amend its training curriculum by incorporating Kinerja’s more practical approach in order to enable LG staff to improve public services. With the announcement of Kinerja’s CE, LAN agreed to designate Papua as the pilot province for the first trainings using the newly revised material. Two training modules (one for frontline staff and one for policy makers) were produced, and the first Public Service Training was conducted for subdistrict frontline staff from schools and puskesmas. Funding has been allocated and further trainings are planned for subdistrict and district government staff in 2017.
• Kinerja produced three policy papers based on its interventions in the health sector, and one policy paper drawing on the program’s implementation of SBM in Papua, which were discussed with senior officials from the Ministry of Health (MOH) and the Ministry of Education and Culture (MOEC). Following several meetings, the ministries adopted a total of five recommendations based on Kinerja’s experience in Papua.
Lessons Learned and Recommendations Kinerja staff learned a great deal through the successes achieved and challenges faced during the course of the program. These are described at relevant points in the following chapters, but
8
they helped to produce many valuable lessons that, it is hoped, will be of benefit to program donors, designers, managers and implementers in the future. This section only lists the recommendations; each of the lessons behind these recommendations is examined in full in the Lessons Learned and Recommendations chapter at the end of this report.
Program Design 1. Governance programs would have a greater likelihood of increased impact if implemented
over a longer period of time.
2. Program timelines should align with LG funding cycles.
3. Gender equity considerations must be systematically incorporated into both program design and implementation.
4. Knowledge management should be a key part of program design.
5. Improved stakeholder mapping prior to program implementation would enable better identification of potential partners.
6. SDU and district government remain the most appropriate levels for improving governance in PSD, and a flexible approach to assistance is the best way to work with them.
7. Monitoring and evaluation (M&E) should consist of a balance between quantitative and qualitative indicators.
Program Management 1. Sharing program costs is an effective method of increasing ownership among government
partners.
2. Programs should invest in intermediary organization capacity building, both prior to and during implementation.
Program Content and Implementation 1. Governance should be integrated into sectoral programming.
2. Service standards, including MSS, are useful in measuring public service quality and targeting improvement.
3. ITATs at the provincial and local government levels can strongly support sustainability and replication.
4. Programs should work with all levels of government simultaneously.
5. Involvement of traditional and religious leaders is critical for development in Papua.
6. Complaint handling represents a simple but effective entry point for introducing governance into PSD.

9
[REDACTED]
The United States Agency for International Development (USAID) awarded [REDACTED] to the Local Governance Service Improvement (Kinerja) program under Cooperative Agreement No: AID-497-A-10-00003 to RTI International and its consortium of five core partners4 in September 2010. The original period of implementation was September 30, 2010, through February 28, 2015. A no-cost extension was granted on October 30, 2014, to amend the program’s end date to September 29, 2015. During the period of performance of its core program, Kinerja focused on supporting local governments (LGs) and service delivery units (SDUs) to improve the delivery of public services in education, health and the business-enabling environment (BEE) in four provinces in Indonesia (Aceh, East Java, South Sulawesi, and West Kalimantan).
In March 2012, USAID expanded Kinerja’s mandate with an [REDACTED] award to focus specifically on governance in health system strengthening (HSS)5 in four target districts (Jayapura, Jayawijaya, Kota Jayapura, and Mimika) in the country’s easternmost province of Papua. In July 2015, shortly before the closure of its core program, USAID provided Kinerja with a further [REDACTED] to continue its work in Papua, for an additional 18 months, with the aim of improving public services by strengthening systems and governance in both health and education sectors.
This final report documents the key achievements and lessons learned during the Kinerja Papua program, which ran from March 15, 2012, through March 29, 2017.6
Program Overview
Context Indonesia witnessed a largely successful democratic transition during the decade leading up to the launch of Kinerja’s original core program in 2010. However, the country continued to face a number of issues that posed a threat to its reverting to more autocratic forms of governance, such as weak rule of law, low levels of transparency and accountability, inadequate representation and persistent corruption. While district governments were significantly strengthened during the same
4 The Asia Foundation, Social Impact, SMERU Research Institute, the University of Gadjah Mada, and Partnership for Governance Reform (Kemitraan). 5 A health system is where different components, such as health facilities, service users and various health-care services, exist and interact with one another. According to the World Health Organization, health systems should improve community members’ health conditions, provide services that are equitable and responsive, provide services with fair funding mechanisms, and use resources effectively and efficiently. 6 Similar information pertaining to Kinerja’s core program is compiled in a separate completion report, Kinerja – Improving Public Service Delivery, Final Report October 2010–September 2015, which was submitted to USAID in May 2016 and approved in August 2016.
Introduction
Kinerja stakeholders talk about improving public service delivery on air at 101.1 Rock FM Jayapura.

10
period, there remained some critical gaps in LG capacity, most notably in a lack of attention to and performance in local service delivery. The challenges that these issues presented to the program elsewhere in Indonesia were magnified in Papua, which to this day remains one of Indonesia’s least-developed provinces.7
Kinerja also faced other issues unique to Papua, which influenced the program’s planning and implementation.
1) Papua’s Special Autonomy status was conferred on the province by the national government in 2001. Special autonomy is an historically controversial issue in Papua and the source of widespread discontent among the indigenous population. Demonstrations are a regular occurrence and political tensions on occasion run high, especially whenever local elections are held.8 Kinerja navigated the politics surrounding special autonomy by coordinating effectively with both the national and provincial government and staying focused on program objectives.
2) Demographics: According to a Ministry of Health (MOH) estimate in 2014, Papua’s population at the time was around 3.5 million. With a population growth rate of more than 5% per year, Papua has one of the fastest growing populations in Indonesia due to high fertility (3.5 children per married woman of reproductive age) and migration from other parts of Indonesia. These population growth trends exert pressure on the province’s already limited capacity to provide basic services in terms of volume, diversity, and quality. In addition, geographical challenges and inadequate infrastructure continue to constrain efforts to improve access to and the quality of basic services, both from cost and logistical perspectives.
3) Socio-cultural context: Papua’s rich cultural diversity offers both a tremendous asset and a significant challenge to the effective and efficient delivery of health and education services. Papua’s linguistic diversity presents a direct challenge in terms of communication, but also an indirect challenge related to narrow definitions of being perceived an “outsider,” even among native Papuans. Moreover, cultural tensions and divisions, both between indigenous Papuan and non-indigenous communities as well as between indigenous Papuan communities themselves, continue to hamper development efforts.
Taken together, each of these issues created a challenging operational environment, which Kinerja dealt with by aligning its approach to fit the local context in each of its four target districts.
Objectives The overall objective of Kinerja’s Papua program at the time of its launch in 2012 was to develop the capacity of LGs to deliver effective, safe, and high-quality personal and non-personal health services, with a minimum waste of resources, while promoting the following:
• Provincial and district policy-enabling environments
• Good governance to produce relevant, responsive basic services
• Substantive civil society engagement.
Program activities were directed at HSS to improve government ability to provide quality services to those communities most at risk from infectious diseases, including human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) and tuberculosis (TB), and to strengthen maternal and child health (MCH) services.
7 Data from Indonesia’s Central Statistics Agency (Badan Pusat Statistik) shows that in 2015, Papua remained at the bottom of the Human Development Index out of the country’s 34 provinces. 8 With security a constant concern, Kinerja developed security protocols and an emergency plan for all staff based in Papua and National Office staff travelling to Papua.

11
USAID made a considerable investment in the health sector in Papua, with a specific focus on HIV/AIDS, MCH and TB, through a range of projects and partners.9 Although these projects made significant inroads at the technical level, Papua’s health sector continued to be poorly governed and was characterized by poor definitions of roles and responsibilities, low attendance rates among health workers in health facilities, insufficiently stocked health centers and other facilities, and a lack of outreach services.
Through the expansion of the Kinerja program to Papua, USAID intended that Kinerja should address this critical governance deficiency by identifying and targeting the key blockages to health service delivery in the province.
When USAID expanded Kinerja’s Papua program in 2015, to include an educational component in the form of school-based management (SBM) at elementary schools, it did so to address similar challenges in Papua’s education sector. These included limited access for children to schools, weak educational management, low teacher competency, high teacher and student absenteeism, and little community involvement and participation. Collectively, these conditions had resulted in low attainment of basic skills, indicated by many students’ lack of ability in reading, writing, and math.
In line with USAID Indonesia’s Country Development Cooperation Strategy 2014–2018, Kinerja aimed to promote access to high-quality basic education, as well as to enhance the capacity of district and provincial governments to plan, manage, and budget for education services and to improve school management.
Kinerja drew on its core program approach to strengthen health systems and enhance health and education outcomes in Papua. This approach employed three types of interventions:
1. Incentives —Strengthen demand-side entities for better services
2. Innovations—Build on existing innovative practices and support LGs to test and adopt promising service delivery approaches
3. Replication—Expand successful innovations nationally and support Indonesian intermediary organizations to deliver and disseminate improved services to LGs
It should be noted, however, that in contrast to Kinerja’s work in its four core provinces, replication in Papua during 2012–2015 was defined as scaling up to other SDUs within the same district, as opposed to replication to other districts through work at the provincial level.10 This changed with the launch of Kinerja’s Papua cost extension in October 2015, when alongside its continuing support of district partners, the program expanded its scope to the provincial level and more formally engaged with health- and education-sector stakeholders from the provincial government.
Implementation Districts In contrast to the randomized selection of treatment districts in Kinerja’s core program, the four target districts in Papua (Jayapura, Jayawijaya, Kota Jayapura, and Mimika) were chosen by USAID, in line with the agency’s plan that Kinerja’s governance approach should complement existing USAID projects operating in those areas.
In April 2012, Kinerja conducted a joint visit with USAID to introduce the program’s expansion plans to key LG and civil society stakeholders in each of the four districts. The visit also allowed 9 These included Scaling Up for Most-at-Risk Populations (SUM) I and II; TB CARE; the United Nations Children’s Fund’s (UNICEF) The Pathways to Achieving Millennium Development Goals 4 and 5 (ACHIEVE) and Malaria in Pregnancy programs; and Engaging Citizens in Peace (SERASI). 10 Many Kinerja Papua activities, such as training on minimum service standards cost analysis and standard operating procedures, focused on district-level stakeholders due to their potential for replication to other SDUs within each district.

12
Kinerja and USAID to undertake limited needs assessments, discuss potential activities and fine-tune the Papua program design. The assessments revealed considerable diversity between each of the districts, both in terms of LG commitment and health-system development, as well as local cultural norms in relation to access to health-care services.11
The following month, Kinerja held three focus group discussions (FGDs) with national-level stakeholders in Jakarta to identify health priorities and key health system-related challenges in the implementation of MCH, HIV/AIDS, and TB programs in Papua. Stakeholders included officials from MOH and the National AIDS Commission, academics from the University of Indonesia, international development partners including World Vision Indonesia, Family Health International 360, SUM II, the Clinton Foundation’s Health Access Initiative, and UNICEF, and individual health experts.
The discussions highlighted the fact that despite various efforts to halt the spread of HIV in Papua, the weak health system in the province, which was marked by high levels of staff turnover within DHOs and community health centers (pusat kesehatan masyarakat or puskesmas), low attendance among health workers, and poor management of the health sector, continued to be a major challenge in accomplishing that goal. The participants agreed, however, that Kinerja’s plan to foster integrated services to meet current demand, by focusing, for instance, on co-infection of HIV and TB and integrating HIV care into MCH services, could provide an entry point to further strengthen Papua’s health systems.
In 2015, when Kinerja expanded its work in Papua to include education, the decision was made to implement SBM in just three of the four districts—Jayapura, Jayawijaya, and Kota Jayapura. The reason for this was twofold: first, the results of a needs assessment that Kinerja staff conducted in Mimika in July 2015 revealed a lack of commitment to the program’s aims and objectives by the head of DEO, and second, Mimika already received substantial support at the elementary-school level from a local CSO, the Amungme and Komoro Community Empowerment Agency (Lembaga Pemberdayaan Masyarakat Amungme dan Komoro [LPMAK]).
Kinerja Approach Kinerja’s governance approach comprised the following three main elements: (1) strengthen and enhance existing national- and district-level policies and programs (as opposed to introducing new programs); (2) support demand-side as well as supply-side stakeholders, to strengthen accountability mechanisms and enable LGs to better respond to people’s needs; and (3) implement program activities through local intermediary organizations to build their capacity and encourage sustainable partnerships with LGs.
Program Interventions Kinerja’s approach in Papua was aligned with its governance principles (accountability, transparency, participation, and responsiveness) and built upon the experience gained from its health and education interventions in the core program. Within the specific context of Papua, where local traditions, norms, and beliefs are the fundamental drivers of development, and religious and indigenous traditional (adat) leaders are influential figures in daily life and decision-making processes, Kinerja sought to tailor its technical assistance to be responsive to local conditions, urban and rural nuances, and distinctive characteristics in each of its target districts.
11 The assessments found that health systems in Jayapura, Kota Jayapura, and Mimika were at a more advanced stage than in Jayawijaya, where the leadership, commitment and capacity of the DHO were not as strong as in the other three districts.

13
To this end, Kinerja staff undertook an extensive consultative process with LG and civil society stakeholders in each of its four target districts to identify local needs and priority areas, as well as to discuss potential governance interventions within the program’s broader objective to strengthen health systems and enhance health outcomes with a focus on HIV/AIDS, TB, and MCH.
In Jayapura and Jayawijaya, local stakeholders identified the importance of strengthening their respective health systems by providing integrated services to combat cases of HIV-TB co-infection, due to a sharp rise in the incidence of TB in both districts as a result of the spread of HIV in Papua as a whole. Participants at the consultations also cited some of the key challenges in trying to control TB, which in addition to the increase in the number of HIV cases included the difficulty of conducting adequate monitoring of TB sufferers to administer treatment. In addressing these needs, Kinerja focused its efforts on supporting health-sector stakeholders in Jayapura and Jayawijaya to develop and/or strengthen patient referral services, data systems to record information about patients receiving treatment for HIV and TB, outreach and mobile services related to TB detection, the procurement and supply of drugs and other health commodities, regulations to ensure community mobilization on TB, and services to support and treat HIV sufferers.
In Papua’s provincial capital, Kota Jayapura, LG and community stakeholders pointed to a rise in the number of pediatric HIV cases in the district. Therefore, they stressed the need to integrate HIV-focused health-care services with maternal and neonatal services in order to prevent the transmission of the disease from HIV-positive expectant mothers to their children.12 In response, Kinerja focused on building the capacity of DHO and puskesmas staff to enable them to provide key integrated services supported by clear standard operating procedures (SOPs) for antenatal care visits, HIV testing, and referral mechanisms between puskesmas and hospitals. Kinerja’s intervention also addressed the availability of suitably-trained health staff, and better planning and budgeting for puskesmas outreach services.
In Mimika, local stakeholders identified MCH services as a priority in the district, with a particular focus on ensuring equal access to antenatal and postnatal care, and safe delivery by fostering partnerships between midwives and traditional birth attendants (TBAs). Specifically, they highlighted the need to provide MCH services to communities in more remote areas of the district whose residents rarely visited puskesmas due to a combination of the distances involved to reach their closest health centers, a lack of public transportation, and in many cases, a lack of awareness about the importance of accessing health services. Kinerja’s assistance to DHO and puskesmas personnel therefore included the development of SOPs on inpatient and outpatient MCH services, strengthening planning and budgeting for MCH outreach and mobile services, and stimulating local demand for health care through the revitalization of integrated services posts (pos pelayanan terpadu or posyandu).
Kinerja initially worked at three puskesmas in each of the four target districts to set up intervention trials, while at the same time supporting LGs to build their capacity and knowledge about the interventions they had selected. This approach allowed LGs to see how governance-related innovations could be practically applied before assuming ownership and scaling up the interventions at additional health centers in their districts.
During the 15-month implementation of Kinerja’s cost extension, the program focused on consolidating health-sector achievements by continuing to build LG capacity in three of the target
12 The prevention of mother-to-child transmission comprises four principal elements: primary prevention, preventing unintended pregnancy among HIV-positive women, preventing HIV transmission from HIV-positive pregnant women to children, and psycho-social support for women living with HIV and their children/families.
14
districts (Jayapura, Jayawijaya, and Kota Jayapura)13 and enhancing its engagement with the PHO in order to reinforce the sustainability of its interventions.
In addition, as mentioned above, Kinerja launched an education intervention in the form of SBM at 30 elementary schools (9 each in Jayapura and Jayawijaya, and 12 in Kota Jayapura), for which the program drew heavily upon the approach and tools that had proved successful when implementing SBM in three of its core districts in West Kalimantan.14
When designing the shape of its interventions, Kinerja took into account national legislation that was interpreted and applied at the district level, as well as the links between district-level health and education initiatives and major national government programs introduced by MOH and the Ministry of Education and Culture (MOEC), respectively. Therefore, Kinerja developed its district-level interventions to intersect with these national programs and build on existing innovations and training packages, and tailor its support to assist LGs and communities to make the most effective use of resources, to target services well, and to monitor and improve the quality of services.
By focusing on MCH, HIV/AIDS, and TB in the health sector, and basic education in the education sector, Kinerja’s efforts also reflected major priorities for both national and district governments in meeting the Millennium Development Goals (MDGs) and fulfilling health- and education-related MSS, as stipulated by the Government of Indonesia (GOI).
Strengthening Demand-Side Stakeholders Kinerja understood that in order to achieve the best and most sustainable outcomes in terms of improving public services, it was necessary to stimulate local demand for better service delivery among the end users of those services as well as strengthen the links between that demand and improved LG response. Stimulating demand without a subsequent LG response or, alternatively, providing services that remain unused by the public are both equally ineffective.
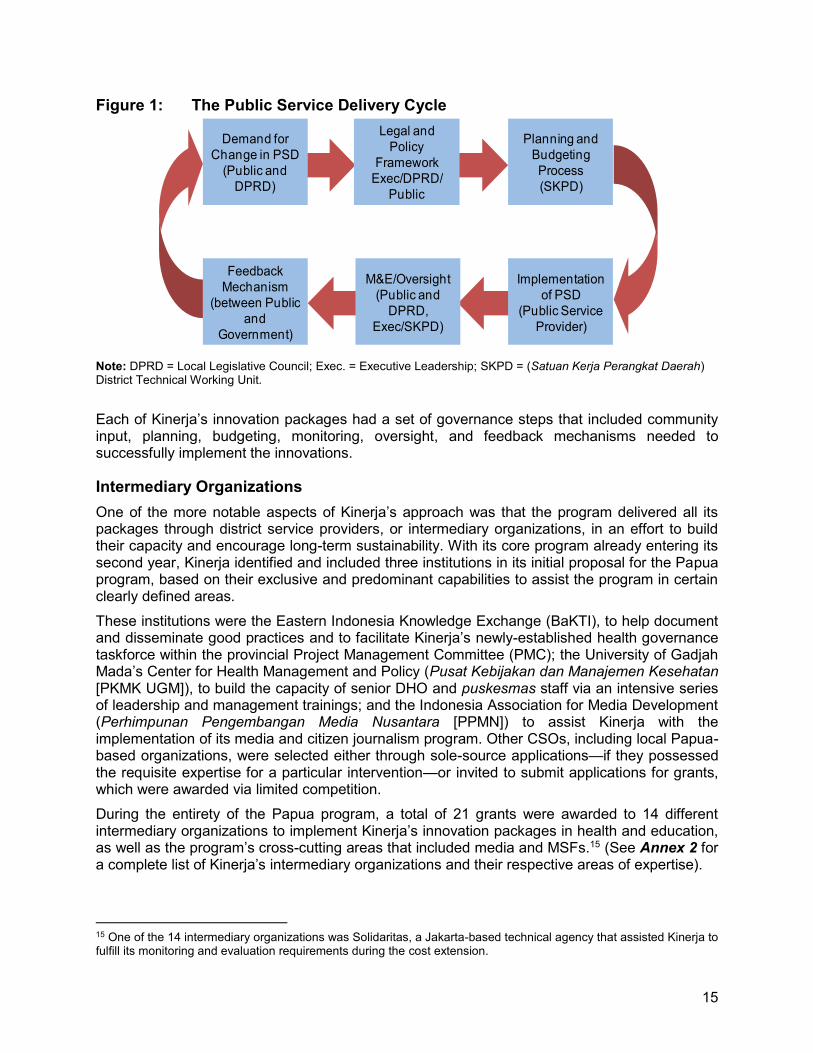
Therefore, the program encouraged active civil society engagement by supporting the formation of MSFs at both district and subdistrict levels, and training and mentoring citizen journalists, to ensure strong community-LG partnerships. The role and responsibilities of MSFs and citizen journalists, as well as some of their key achievements during Kinerja’s Papua program, are covered in greater detail in the Good Governance chapter of this report, but the diagram below illustrates how Kinerja’s incentive (demand stimulation, community empowerment), innovation (tools directed at district governments), and replication (facilitation of LG adoption of good practices) packages fit into the PSD development cycle (Figure 1).
13 Due to low commitment from the LG in Mimika, Kinerja provided only limited support to the DHO during the cost extension in response to specific requests. The program’s interventions with demand-side stakeholders, however, continued in all four districts until district-level programmatic activities ended in November 2016. 14 Although the cost extension allowed for the completion of one full implementation cycle of the package’s key components, it did not provide sufficient time to consolidate and scale up SBM within target districts. However, Kinerja established positive working relations with the PEO, which provided an avenue for sustainability and future replication (see the Replication chapter in this report for details).
15
Figure 1: The Public Service Delivery Cycle
Note: DPRD = Local Legislative Council; Exec. = Executive Leadership; SKPD = (Satuan Kerja Perangkat Daerah) District Technical Working Unit.
Each of Kinerja’s innovation packages had a set of governance steps that included community input, planning, budgeting, monitoring, oversight, and feedback mechanisms needed to successfully implement the innovations.
Intermediary Organizations One of the more notable aspects of Kinerja’s approach was that the program delivered all its packages through district service providers, or intermediary organizations, in an effort to build their capacity and encourage long-term sustainability. With its core program already entering its second year, Kinerja identified and included three institutions in its initial proposal for the Papua program, based on their exclusive and predominant capabilities to assist the program in certain clearly defined areas.
These institutions were the Eastern Indonesia Knowledge Exchange (BaKTI), to help document and disseminate good practices and to facilitate Kinerja’s newly-established health governance taskforce within the provincial Project Management Committee (PMC); the University of Gadjah Mada’s Center for Health Management and Policy (Pusat Kebijakan dan Manajemen Kesehatan [PKMK UGM]), to build the capacity of senior DHO and puskesmas staff via an intensive series of leadership and management trainings; and the Indonesia Association for Media Development (Perhimpunan Pengembangan Media Nusantara [PPMN]) to assist Kinerja with the implementation of its media and citizen journalism program. Other CSOs, including local Papua-based organizations, were selected either through sole-source applications—if they possessed the requisite expertise for a particular intervention—or invited to submit applications for grants, which were awarded via limited competition.
During the entirety of the Papua program, a total of 21 grants were awarded to 14 different intermediary organizations to implement Kinerja’s innovation packages in health and education, as well as the program’s cross-cutting areas that included media and MSFs.15 (See Annex 2 for a complete list of Kinerja’s intermediary organizations and their respective areas of expertise).
15 One of the 14 intermediary organizations was Solidaritas, a Jakarta-based technical agency that assisted Kinerja to fulfill its monitoring and evaluation requirements during the cost extension.
Implementation of PSD
(Public Service Provider)
Planning and Budgeting Process (SKPD)
Demand for Change in PSD
(Public and DPRD)
Legal and Policy
Framework Exec/DPRD/
Public
M&E/Oversight (Public and
DPRD, Exec/SKPD)
Feedback Mechanism
(between Public and
Government)

16
Working through intermediary organizations presented Kinerja with a number of challenges, however, which made it hard on occasion to guarantee the quality of the programs delivered. The generally low levels of capacity among Indonesian CSOs required Kinerja to expend a great deal of effort to address skills gaps in technical, governance, financial and/or administrative areas. In order to address this issue in its core program, Kinerja established a Capacity Development Task Force (CDTF), which was organized through the program’s East Java Provincial Office. Through until its closure in June 2015, the CDTF delivered a series of workshops for Kinerja’s intermediary organizations and CSO partners offering in-depth technical and administrative/financial briefings and trainings.
The lack of capacity was all the more apparent among CSOs in Papua, but given the logistical challenges involved (not least the distance between Papua and East Java), Kinerja was unable to facilitate CDTF trainings for its Papua-based intermediary organizations. Instead, the program’s technical staff provided additional support and oversight to assist them in carrying out their technical and governance-related activities. Kinerja also provided a grant to CIRCLE Indonesia, a Yogyakarta-based organization with consulting experience in Papua, to work alongside and strengthen the capacity of three local intermediary organizations (The AIDS Care Foundation [Yayasan Peduli AIDS (YAPEDA)], Mothers’ Hope Foundation [Yayasan Harapan Ibu (YHI)], and Foundation for the Economic Welfare of Indonesia’s Rural Communities [Yayasan Usaha Kesejahteraan Ekonomi Masyarakat Desa Indonesia (YUKEMDI)]) that were tasked with implementing Kinerja’s demand-side interventions with MSFs.
The issue of intermediary organization capacity was an ongoing challenge for the program and one that ideally should have been addressed before implementation began. A suggested approach could be to conduct capacity-building trainings during a program’s first year, and mentoring during the second, with ongoing technical support and “on-the-job training” provided as needed thereafter. (Please see the Lessons Learned and Recommendations chapter at the end of this report, where this issue and others pertaining to program design, management, content, and implementation, are explained more fully).
Cost Share Kinerja’s cost share commitment for the Papua add-on, when the program was launched in 2012, amounted to [REDACTED]. RTI’s plan was structured to tap into the following cost share resources, similar to those in Kinerja’s core program:
• Government budget inputs for time and travel for participating government staff, data collection, and analysis to strengthen LG ownership and leadership of program interventions
• Mobilization of LG health budgets related to Kinerja interventions in HIV/AIDS, TB, and MCH programming that provided the base for Kinerja Papua’s supplementary budget and human resource development support
• Kinerja activities building on LG budget allocations for specific health interventions, which were an integral part of cost-sharing arrangements. These arrangements were also included in district cooperative agreements/memorandums of understanding (MOUs)
• Media resources provided by media organizations and non-US federal actors such as campaign materials and airtime
• Encouragement of other organizations to implement activities related to the project objectives
17
• Intellectual capital produced by non-US federal government-funded agencies, including tools, manuals, or seminar presentations that were not in the public domain
• Joint activities and events between Kinerja and non-US federal donors
• Utilization of free office, training, and meeting venues provided by counterparts and partners.
In order to fulfill the program’s cost-share obligation, RTI prepared a separate cost-share plan to identify potential partners in the private sector, as well as raise cost share from LGs (to achieve government ownership of programs), grantees, and via voluntary contributions.
Taking into account some of the sensitivities of private enterprise partnerships in Papua, RTI explored potential opportunities to mobilize corporate social responsibility (CSR) funds through responsible private-sector organizations to help support Kinerja Papua’s implementation. However, Kinerja’s efforts to reach out to the private sector proved even more difficult in Papua than in its core program areas.
One international company with operations in Papua is the US-based Freeport-McMoRan, which runs the Grasberg copper and gold mine in Mimika via its affiliate PT Freeport Indonesia. Kinerja approached Freeport in the hope of raising cost share through the latter’s CSR program, but Freeport already had a local NGO partner, LPMAK, to which the company allocated CSR funds to implement health- and education-sector initiatives in the district.
Kinerja therefore decided to focus its efforts on raising cost share via the direct implementation of its program interventions. This was extremely challenging during the program’s first year of implementation. Experience from Kinerja’s core program had shown that in the initial years, LG confidence must be generated based on evidence from successful program-supported interventions—only then would LGs be prepared to allocate funding. In Papua, however, there were additional challenges; first, local partners were unaccustomed to the practice, and second, an increasing number of development partners operating in Papua paid LG staff to participate in their project activities.
At the same time, Kinerja’s core program had reached a very mature stage, whereby LGs realized the benefit of working with the program and were readily allocating funds towards district-wide replication. For this reason, in February 2014, Kinerja reallocated [REDACTED] of its Papua cost share obligations to the Kinerja core program, leaving [REDACTED] to be raised by Kinerja Papua. An adjustment for cost share obligations for core and Papua components, requested by RTI, was approved by USAID with Modification 14 issued in July 2015.
Total Kinerja Papua cost share raised through to the end of the program and reported to USAID was [REDACTED], which was slightly above the planned amount, exceeding it by 2%.

18
[REDACTED]
Kinerja’s health program in Papua focused on strengthening existing health systems in its four target districts and, through a range of governance interventions, building the capacity of LGs to improve health outcomes in their respective areas of focus: HIV/AIDS and TB in Jayapura and Jayawijaya, and MCH in Kota Jayapura and Mimika.
Kinerja provided intensive technical assistance to targeted staff from both puskesmas and DHOs in all four districts. In January 2016, the program withdrew direct support to puskesmas in order to engage more fully with provincial-level authorities and to further strengthen the capacity of DHO partners in Jayapura, Jayawijaya, and Kota Jayapura, to enable them to fulfill their primary responsibility of monitoring and supervising the provision of health care at puskesmas as well as providing technical support to SDUs as needed. Due to lack of commitment from the LG, Kinerja withdrew from working in the supply side in Mimika for the cost extension.
Together with its DHO partners, Kinerja selected three puskesmas per district as the pilot centers for the program’s health interventions ahead of scaling up efforts by LGs (Table 1).
Table 1: Kinerja-Supported Puskesmas
Jayapura Jayawijaya Kota Jayapura Mimika Depapre Hom-Hom Abepantai Limau Asri
Dosay Hubikosi Koya Barat Mapurujaya
Sentani Musatfak Tanjung Ria Timika Kota
Strengthening Management and Leadership for Health Service Delivery Kinerja’s priority throughout the Papua program was to build and strengthen the capacity of district health officials and puskesmas managers in accordance with competency standards laid out in MOH Regulation No. 971/2009. These standards include basic competencies (such as integrity, leadership, planning, budgeting, institutional management, partnership and responsiveness) and technical competencies (service and quality orientation, analytical thinking, conceptual thinking, technical/managerial/ professional expertise, and innovation).
Kinerja’s implementing partner for this capacity-building intervention was PKMK UGM, which had previously developed, in conjunction with MOH, a nationally recognized curriculum to train DHO personnel. Using information gathered during a baseline assessment in all four Kinerja districts,
Health
A mother and her baby obtain medication at the pharmacy of a partner health center.

19
PKMK adapted the curriculum16 to create a new Performance Management and Leadership (PML) training course, tailor-made to meet the needs of both DHO and puskesmas stakeholders in each district with regard to their respective focus areas.
Also feeding into the design of the new training were the results of a health barriers assessment that Kinerja and PKMK conducted in the program’s partner districts to identify specific obstacles to both the delivery of and access to quality health-care services.17
Key findings of the assessment (which were based on information gathered through FGDs and in-depth interviews with district health officials, subdistrict service providers, and members of local communities living within catchment areas of Kinerja’s partner puskesmas) included the unreliability and inaccessibility of puskesmas services; perceptions of sub-standard service quality; and perceived low capacity among health-care providers. On the supply side, respondents pointed to various contributory factors including a lack of supervision and oversight by puskesmas managers and DHO staff, a lack of discipline and work ethic among health-care staff, and limited functionality in terms of DHO leadership and stewardship (especially in Jayawijaya and Mimika).
Through the two-year PML training course, which consisted of online instruction, in-person workshops, follow-up mentoring, and refresher trainings, Kinerja assisted its partners to analyze challenges and barriers to quality health care in their regions and to develop and implement short- (3–4 months), medium- (6–12 months), and long-term (more than 12 months) action plans to address the challenges and improve health-care services (see Box 2 above).
What began with bridging workshops to raise participants’ awareness and improve their knowledge and skills about MSS
16 The curriculum was based on the following six building blocks contained in the WHO’s 2007 Framework for Action: service delivery, health workforce, information, equipment (medical products, vaccines and technology), financing, and leadership/governance. Although the Performance Management and Leadership training addressed all six areas, there was a heavy focus—especially during the first year of implementation—on SDU service delivery and health workforce, and DHO leadership/governance. 17 The results from this assessment also provided the foundation for the Health Barriers and Good Practice Seminar, which took place in May 2013. Information about the seminar is presented in the Replication chapter.
Box 2: Puskesmas/DHO action plans to address HIV/AIDS, TB, & MCH
Short-term plans:
Jayapura: Mentoring of laboratory technicians with error rates >5% for TB testing; health education campaigns on co-infection of HIV/TB at the community and village level
Jayawijaya: Development of DHO strategic planning encompassing multi-year planning for HIV, TB, and MCH; health education campaigns on co-infection of HIV/TB at community and village level in collaboration with religious leaders
Kota Jayapura: Development of SMS Gateway mechanism to support a health information system on antenatal and delivery services; optimizing Mayoral Decree No. 12/2013 on district technical working units (SKPD) responsible for integrated services posts (posyandu); development of a mayoral decree on a reproductive health center
Mimika: Establishing TBA-midwife partnerships at puskesmas level; mapping availability of TBAs at subdistrict level; development of a 24-hour on-call midwife service at puskesmas
Medium- and long-term plans:
Jayapura: Health campaigns on TB to local communities and relatives of TB patients; recruitment of laboratory technicians at puskesmas
Jayawijaya: Establishing multi-sector mobile clinic with religious and indigenous leaders, puskesmas staff; home visits for TB and HIV
Kota Jayapura: Increase capacity of puskesmas laboratory technicians on sexually transmitted infection, HIV, and TB testing; provide seminar for posyandu volunteers; train HIV program managers at puskesmas and DHO; on-the-job training for laboratory technicians at puskesmas and hospitals on TB services
Mimika: Development of Regional Health System; TBA-midwife partnerships; health promotion and educational activities on safe delivery through health facility campaigns
20
and SOPs, culminated in the next year with additional trainings in each district in response to specific requests by local stakeholders. These trainings focused on topics such as communication techniques, health information systems, and International Organization for Standardization (ISO) management systems for puskesmas.
Key Achievements • Between 2013 and 2015, Kinerja and PKMK trained a total of 318 officials (of whom 231,
or 73%, were women) from DHOs and puskesmas across all four districts.
• Collectively, they produced a total of 310 short-, medium-, and long-term action plans to improve services directed at HIV/AIDS, TB, and MCH, far exceeding the original target of 96.18 Of this total, 69 (24 short-, 25 medium-, and 20 long-term) action plans were implemented by DHOs in Kinerja’s partner districts, while a further 206 (71 short-, 72 medium-, and 62 long-term) action plans were implemented by Kinerja’s 12 partner puskesmas.
• Recognizing the value of the PML training course, Papua’s provincial health-sector training center, Balatkes (Balai Latihan Tenaga Kesehatan), signed an MOU with PKMK in 2015, with a view to replicating similar trainings to additional puskesmas and DHOs within its own curriculum.
• Elements of the PML trainings pertained to governance principles such as transparency, accountability, responsiveness, and community participation. Kinerja’s Organizational Capacity Assessment (OCA) found a significant improvement in how puskesmas management incorporated these principles into their work, with all the program’s partner puskesmas increasing their OCA scores between the baseline (April 2013) and endline (March 2015). Transparency scores increased by 20% on average, accountability by 16%, communication participation by 27%, and responsiveness by 29%. The greatest changes in scores occurred at puskesmas in Mimika and Jayawijaya.
• The PML trainings also gave puskesmas staff the opportunity to come together and share their experiences and knowledge with one another. Puskesmas staff told Kinerja that this was the first time they were able to do so, as inter-puskesmas interaction is rarely arranged by the DHOs, with most trainings focusing more on DHO staff.
• Shortly before its grant ended in March 2015, PKMK provided trainings of trainers (TOTs) for DHO officials and puskesmas staff in all four districts to strengthen their understanding of their respective roles and functions, and increase their technical knowledge and skills, as a foundation for the establishment, in April 2015, of district-level ITATs. Team members consisted of mid-level DHO staff and senior policy makers, to provide ongoing support and technical assistance to puskesmas in addition to their normal monitoring and supervisory functions.
• In 2016, at the request of the PHO, Kinerja amended the PML training module in collaboration with former PHO and DHO heads, to incorporate additional practical elements and role plays, with the specific aim to train DHO heads. Once the revisions were complete, Kinerja submitted the module to the PHO and Badan Diklat to launch trainings in 2017.
18 The target did not include long-term action plans, as Kinerja believed their implementation would be beyond the scope of the program’s original time frame. Nevertheless, the 192 short- and medium-term action plans produced by DHOs and SDUs still well-exceeded the target.

21
Provincial and District Engagement Underpinning Kinerja’s efforts to improve health systems and health outcomes in Papua was an emphasis on establishing and fostering strong relationships with key provincial- and district-level institutions and personnel. Kinerja established two forums (provincial and district) that, in addition to supporting the program’s objectives and securing the best possible environment for success, intended to: (1) respond to government needs to address challenges related to the improvement of health services; (2) ensure the program remained on track and that its activities contributed to mutually beneficial outcomes; and (3) explore and utilize opportunities for the sustainability of good practices in the health sector and to promote the scaling up of these good practices to non-partner health centers.
At the provincial level, Kinerja established a health governance taskforce within Papua’s existing PMC, which, under the auspices of the Local Government Agency for Regional Development Planning (Bappeda), was a mechanism for provincial stakeholders to coordinate various development partners operating in Papua.19 Membership of Kinerja’s new provincial taskforce was limited to the heads of the provincial Bappeda office and the PHO together with the heads of district Bappeda offices and DHOs from the program’s four target districts. Kinerja facilitated three meetings of the PMC taskforce per year through its intermediary organization, BaKTI, a South Sulawesi-based CSO that had previously collaborated with the Australia-Indonesia Partnership for Decentralization on the PMC.
BaKTI also assumed the role of facilitator for district-level technical teams that Kinerja helped to establish in its four target districts. Like their provincial PMC counterparts, the district teams (which comprised representatives from each of the district’s DHO and Bappeda offices and met on a quarterly basis) became platforms for sharing knowledge and updates on program implementation.
Within the framework of Papua’s Special Autonomy, Kinerja also actively engaged with Local Legislative Council (DPRD) members in district, and the provincial-level Papuan People’s Assembly (Majelis Rakyat Papua [MRP])20 to ensure MSS integration into LG planning and budgeting. In partnership with two intermediary organizations, the Legislative Monitoring Committee (Komite Pemantau Legislatif [KOPEL]) and the Independent Consultancy Foundation for People’s Empowerment (Yayasan Konsultansi Independen Pemberdayaan Rakyat [KIPRa]), Kinerja provided DPRD legislators with training and mentoring to improve their understanding of their budgetary and financial oversight roles, and sought to build the capacity of MRP members on health MSS.
19 The PMC was established by Bappeda and the Australia-Indonesia Partnership for Decentralization (AIPD), and contained representatives from a number of different provincial technical offices in addition to Bappeda and the PHO. Due to its extensive scope, Bappeda accepted Kinerja’s proposal to create a more manageable taskforce within it. 20 In accordance with Papua’s Special Autonomy Law 21/2001, the MRP represents indigenous communities throughout the province. Assembly members are mandated to create special local regulations on indigenous peoples’ rights and to advocate to the provincial government to determine health service standards. The MRP plays a strategic role in promoting the formulation of locally applied MSS, based on national service standards, to reflect the Papua context and to meet the needs of its indigenous population.
“We hope that this new way of thinking [on governance] will be continued by all. The direction is clear, and the system has been well-established. Now it’s up to us to move services forward and become more effective in the health sector.”
[REDACTED]

22
After the Papua program’s cost extension was launched in October 2016, Kinerja’s involvement with the PMC and the district technical teams was replaced by a closer working relationship with the PHO and Provincial Health Facilitation Team (PHFT)21, and their work to strengthen the capacity of the recently-established DHO ITATs.
Key Achievements • Kinerja worked with DHOs in Jayapura, Kota Jayapura, and Jayawijaya to establish a
health ITAT in each partner district. The key role of the ITATs was to undertake integrated supervision and mentoring to puskesmas by bringing together multiple sections of local DHOs rather than each section working independently as they had traditionally done. Each ITAT is made up of around 14 DHO staff members. The ITATs visit puskesmas, provide on-the-spot mentoring, and develop technical recommendations for DHO heads based on their findings to help overcome challenges identified. ITATs have reported faster follow-ups from DHO heads based on the new system, with improvements implemented more quickly. All three DHOs have indicated they will allocate further funding in 2017 to conduct similar visits to other puskesmas in their districts.
• Following ITAT assessments at the district level, Kinerja presented the results to the PHO, highlighting that each ITAT had different levels of capabilities and skills. The PHO agreed to standardize the ITATs, and worked with Kinerja to develop technical supervision guidelines, complete with monitoring checklists for ITAT use. The guidelines were finalized by the end of 2016 and were already being used in supervisory visits in the same year.
• KOPEL’s Local Health Budget Study assessed health budgets in Kinerja’s partner districts for the five years prior to 2014. The assessment confirmed that low budget allocations for health lead to poor health outcomes. The results were presented to the DPRD Secretariat in each district, highlighting the importance of MSS for accurate, needs-responsive budgeting.
Puskesmas Management Kinerja’s district consultations showed that in most cases, puskesmas in Papua were unable to provide adequate health services to local communities living in their catchment areas. This situation was caused by various factors, including difficulty for some in accessing health centers, limited number of available personnel, and a limited number of programs that could be considered innovative enough to be implemented in challenging environments. The quality of health-care services was also generally below standard, and personnel were not equipped to handle privacy issues correctly. In addition, community members faced their own obstacles such as difficult terrain, lack of transportation, high cost of transportation, lack of knowledge, and an unsupportive local culture for getting the health support they needed.
Kinerja provided technical assistance on four interventions related to puskesmas management. Two of these interventions—the development of service charters and technical recommendations following the completion of complaint surveys—are described in greater detail in the MSF section of the Good Governance chapter.
The remaining two interventions were as follows:
1. Development and implementation of service SOPs. Developing standardized practices in the provision of public services was a major challenge for many district administrations in
21 The PHO established the PHFT with support from UNICEF, to provide technical assistance to puskesmas and, to a lesser extent, DHOs. The team consisted of PHO officials, Cenderawasih University lecturers, and Balatkes staff.

23
Papua. The lack of SOPs not only reduced efficiency in the provision of services at puskesmas across the province, but also led to uncertainty among patients as to what to expect in terms of waiting times and treatment quality. Kinerja’s puskesmas partners chose to develop SOPs on a number of topics, including how to process samples for TB testing, the diagnosis of TB and HIV/AIDS, treatment monitoring plans, the prevention of mother-to-child transmission, and the proper maintenance of laboratory equipment. In addition to these technical SOPs, Kinerja also stressed the importance of service SOPs; that is, SOPs that do not outline medical procedures but rather the services to be provided. Kinerja focused on service SOPs relating to service flows (that is, procedures for registration, services, payment, medication, and referral) and antenatal care. All service SOPs developed with Kinerja’s support were created in a transparent and consultative manner, involving all puskesmas staff, and once finalized, were displayed on the puskesmas walls in order to ensure compliance from staff and to build awareness of health rights among patients.
2. Development and implementation of complaint-handling mechanisms. In addition to supporting the running of complaint surveys, Kinerja provided technical assistance to partner puskesmas on establishing complaint-handling mechanisms or improving existing ones. In general, support was focused on complaint surveys and complaint boxes, as well as SMS feedback systems in Jayapura and Kota Jayapura.
Key Achievements • Two of Kinerja’s partner puskesmas in Jayapura, Puskesmas Dosay and Depapre, were
assessed by the DHO as the district’s best performing puskesmas in 2015 and received awards from the District Head. Dosay also went on to be one of the first puskesmas in Papua Province to receive government accreditation in 2016, a proud moment for the Jayapura DHO.
• Kinerja’s partner puskesmas were able to close long-standing gaps in SOPs, developing tens of new SOPs per puskesmas on both technical and service topics. These SOPs have led to improved service delivery, with patients commenting that service flows are much clearer, HIV/AIDS statuses have become more confidential, and patients are now served on a first-come, first-served basis.
• All 12 of Kinerja’s partner puskesmas now have strong complaint-handling mechanisms in place. Although many previously had mechanisms such as complaint boxes, most were poorly managed, lacked transparency, and complaints were only sometimes followed up. With Kinerja’s support, the puskesmas have all implemented complaint surveys and fulfilled service charters and have improved their complaint management processes in general, such as through including the community (via the MSF) in handling complaints. Most puskesmas also now have complaint-handling teams. In Jayapura, all 19 puskesmas were asked by the DHO to implement complaint-handling mechanisms and display complaint-handling SOPs in the waiting rooms, while in Mimika, funds have been allocated to replicate complaint-handling mechanisms at three other puskesmas.
Combating Gender-Based Violence While gender was not included as a specific indicator in Kinerja’s Performance Monitoring and Evaluation Plan (PMEP), the program was committed to incorporating gender into its HSS work by raising awareness and building the technical capacity of LGs and communities to combat gender-based violence (GBV), which remains a critical issue in Papua and one that significantly

24
affects the lives of women and children. Speaking in 2016, the Minister for Women’s Empowerment and Child Protection, Yohana Yembise, stated that Papua had the highest incidence of violence against women in Indonesia, with domestic violence accounting for the majority of such cases (56%).
Although the central government has established MSS for integrated services for women and children affected by violence, awareness of these standards at the local level, let alone their implementation, remains low. Kinerja also observed that local budget allocations for addressing GBV were limited, leading to challenges for district-level Women’s Empowerment and Child Protection Offices in lobbying other sectors to cooperate in the establishment of integrated service centers.
Kinerja’s GBV strategy consisted of three elements: (1) assist LGs in providing integrated services based on MSS for women and children affected by violence; (2) build the capacity of health workers on the provision of specialized GBV-related health care; and (3) work with local communities to raise awareness about GBV, including working with young people on adolescent reproductive health and healthy relationships (a modification of the model that Kinerja used to address underage marriage in Bondowoso, one of its core treatment districts in East Java). The GBV program concentrated its efforts in two districts whose focus area was MCH—Kota Jayapura and Mimika—due to the direct impact of GBV on neonatal and maternal health outcomes.
When seeking intermediary organizations, Kinerja found that the number of local Papuan organizations working in this area was limited, as was their organizational capacity and understanding of related MSS. Therefore, Kinerja selected the Yogyakarta-based Institute for the Study of Women and Children’s Development (Lembaga Studi Pengembangan Perempuan dan Anak [LSPPA]) as its implementing intermediary organization, while for the modified reproductive health component, the program appointed the Jakarta-based Women’s Health Foundation (Yayasan Kesehatan Perempuan [YKP]), which led Kinerja’s reproductive health program in Bondowoso.
Key Achievements • Integrated Service Centers for the Protection of Women and Children (Pusat Pelayanan
Terpadu Perlindungan Perempuan dan Anak [P2TP2A]) were established in Kota Jayapura and Mimika, and both were formally recognized through the issuance of LG regulations. The two teams were strengthened by the development of referral mechanisms among government service providers, including social workers, police, counselors, and primary healthcare providers. Cases are now more comprehensively dealt with and followed up. For example, between January and August 2016, 44 cases of domestic violence were handled by P2TP2A in Mimika, 30 of which were successfully resolved through mediation, with the remainder being reported to the local police for investigation or entering the court system.
• Three of Kinerja’s partner puskesmas (Puskesmas Tanjung Ria in Kota Jayapura and Puskesmas Mapurujaya and Timika Kota in Mimika) received intense training on documenting, treating, and managing cases of violence against women and children. All staff, including janitorial staff and receptionists, at the three puskesmas were trained in how to identify and handle potential survivors of violence.
• Kinerja assisted staff from each district’s Women’s Empowerment, Child Protection and Family Planning Agency (Badan Pemberdayaan Perempuan, Perlindungan Anak dan Keluarga Berencana [BP3AKB]) to develop five-year Regional Action Plans for the Prevention and Management of Violence against Women and Children (Rencana Aksi Daerah Pencegahan dan Penanganan Kekerasan terhadap Perempuan dan Anak [RAD

25
KtPA]). The mayor of Kota Jayapura issued a decree in December 2015 to provide a firm legal base and LG funding for the district’s RAD KtPA, and although an equivalent district head decree in Mimika remained unsigned as of the end of Kinerja’s Papua program, the head of Bappeda signed the district’s action plan in June 2015 and provided funding of [REDACTED] from its 2016 budget. This funding allowed the BP3AKB to enhance the capacity of the local P2TP2A team as well as to establish a safe house in the district’s capital, Timika.
• In 2016, Kinerja began broadening its GBV work to include more focus on the role of the media. The program contributed to a TVRI Mimika talk show on GBV in August 2016, and three weeks later, led a media tour with citizen journalists and mainstream media journalists to P2TP2A Mimika and Puskesmas Timika Kota to learn about both GBV and the services available. In November 2016, Kinerja, the Ministry of Women’s Empowerment and Child Protection, and Alex Junaidi from The Jakarta Post held a two-day workshop for media editors and writers to encourage them to become more gender-sensitive in news reporting, particularly when covering cases of violence against women and children.
Health Workers’ Absenteeism Study As a result of its work with district and subdistrict service providers in Papua, Kinerja identified health worker absenteeism at community health centers as one of the main contributing factors to the low quality of health services and poor sustainability of programs and donor investments in HIV, TB, and MCH services in the province. In order to address the issue, Kinerja commissioned a study to explore the magnitude and dimensions (social, cultural, structural, geographical, and demographic) of absenteeism in the program’s four partner districts. The study also aimed to explore the policy roots of the problem, as distinguished from operational- , local- , and national-level causes.
Yogyakarta-based CSO SurveyMETER led the study, comprising quantitative and qualitative data. Between April and July 2014, SurveyMETER surveyed 346 doctors, nurses, and midwives working at puskesmas in Kinerja’s four districts and conducted 29 in-depth interviews with health workers and policy makers and 30 FGDs with local communities and staff at 53 puskesmas.
Healthcare workers provided a variety of reasons for their absence, including illness (of self or family member), approved personal leave; attending pre-approved trainings, events, or lectures; competing professional commitments (such as private medical practice); family commitments; natural disasters; security issues; and transportation difficulties.
The study revealed an overall level of 35.4% absenteeism across the four districts, based on the following levels of absenteeism per district: Jayapura, 52%; Mimika, 40%; Jayawijaya, 33%; and Kota Jayapura, 21%.
Kinerja convened an Operational Policy Barriers Analysis Workshop in October 2014 to present the results of the study to senior district and provincial stakeholders and to identify a list of interventions that could be implemented to reduce absenteeism at the puskesmas level. As a result of the workshop, LG representatives selected four priority policies each to address absenteeism in their respective areas, with Kinerja to provide support where possible to help them realize their aims.
Key Achievements • The Jayapura DHO issued and implemented three of its four recommended policies, on
(1) the provision of attendance- and performance-based incentives for doctors, nurses and midwives in accordance with where they are based in the district; (2) the conducting

26
of regular mini workshops and inter-sectoral meetings at all puskesmas in the district; and (3) the formation of a DHO ITAT to monitor and supervise the delivery of health-care services at puskesmas.
• In addition to the DHO’s commitment to addressing absenteeism, Kinerja’s follow-up assessment in May 2016 revealed that the district MSF in Jayapura was the most active of all the district forums in advocating for new policies to combat the issue, including with regard to ensuring that health workers are available at subdistrict and village levels across the entire district. These efforts prompted the DHO to conduct a study to map the availability and distribution of health workers at all 19 puskesmas in the district plus village health posts in order to identify and address existing gaps.
• The LG in Jayawijaya followed up on two of its four priorities, by: (1) implementing a merit-based fit and proper test mechanism in December 2014 to select puskesmas heads; and (2) establishing a local agreement in May 2015 to impose customary-based sanctions on anyone found guilty of harassing or threatening the safety of health workers. The successful introduction of the fit and proper tests was reinforced in May 2016 with the issuance of a District Head decree governing the new selection mechanism.
• In Kota Jayapura, the DHO followed up on one of its priorities, by promising to impose sanctions on puskesmas staff who were frequently late for work or absent, in line with prevailing district legislation.
• Results of the absenteeism study, its method, and its subsequent policies were shared by Kinerja in a number of formats. Kinerja and RTI staff presented the study at the International Family Planning Conference in Bali, in January 2016, and the Fourth Global Symposium on Health System Research in Vancouver, Canada, in November 2016. A case study based on the Vancouver presentation will be included in a forthcoming book to be published by the Asian Development Bank entitled Management for Development Results: Inclusive Development.

27
[REDACTED]
A key element during the Papua program’s cost extension was the launch in November 2015 of an education-sector intervention in the form of Kinerja’s public service-oriented SBM package, which was implemented at elementary schools in three target districts (Jayapura, Jayawijaya and Kota Jayapura). In conjunction with its education intermediary organization, the Institute for Community Development and Empowerment (Institut Pengembangan dan Pemberdayaan Masyarakat [IPPM]) and senior DEO officials, Kinerja selected a total of 30 elementary schools,22 located in urban, rural, and coastal areas, as pilot schools for the intervention (see Table 2).
SBM is a reform that seeks to increase autonomy for schools in making decisions about their management, including the use of funds, materials and human resources. Under the national government’s School Operational Assistance (Bantuan Operasional Sekolah [BOS]) program,23 school committees were established at schools nationwide to run SBM programs, with authority over non-salary operational expenditures. By channeling funds directly to schools, education stakeholders such as parents, principals, and school committees were empowered to choose the best way to allocate funding to address the challenges they faced.
Table 2: Kinerja-Supported Schools No Jayapura Jayawijaya Kota Jayapura
1 SD Inpres Komba SD Inpres Mulele SD Inpres Megapura
2 SD Inpres Abeale 1 SD Negeri Wamena SD Inpres Pasir Dua
3 SD YPK Ayapo SD YPPK Hone Lama SD Inpres Yoka Pantai
4 SD YPK Waibron SD Inpres Wesaput SD Negeri Koya Koso
5 SD Inpres Sabron Yaru SD Inpres Minimo SD Inpres Nafri
6 SD Inpres Kanda SD YPPK Wouma SD Negeri Holtekam
7 SD Inpres Depapre SD YPPK Musatfak SD Inpres Skow Sae
8 SD YPK Amai SD YPPK Holima SD YPK Skow Mabo
22 In line with its cost extension work plan, Kinerja originally selected 27 schools (9 per district), but due to lower than expected baseline scores at the schools in Kota Jayapura, Kinerja and the DEO chose an additional 3 schools in the district (nos. 10–12 in Table 2) to better reflect educational standards in what is Papua’s most-developed district. 23 Through its BOS program, which was established in 2005, the national government provides financial assistance to support elementary and junior high schools nationwide to meet their operational costs. BOS payments for elementary schools amount to [REDACTED] per student per year.
Education
Parents of students at Komba Elementary School fill out a community complaint survey.

28
9 SD YPK Yepase SD YPPK Asologaima SD Inpres Koya Tengah
10 SD Negeri Bertingkat Waena
11 SDN Inpres 6.88 Yabansai
12 SD Negeri 1 Hamadi Note: SD (sekolah dasar)=elementary school; YPK (Yayasan Pendidikan Kristen) = Foundation for Christian Education;
The results of Kinerja’s baseline study showed that the majority of its new partner schools in Papua not only failed to implement their plans and budgets (which was the case at many of Kinerja’s core program schools when they first began to implement SBM), but also had some way to go to achieve full accountability and transparency by producing and publishing financial reports. With regard to school committees, the study revealed that only four schools (elementary school [sekolah dasar (SD)] Abeale 1, Ayapo, Komba, and 6.88 Yabansai) had sufficiently strong committees in place, in terms of functionality and sustainability. The remaining 26 schools, however, had underperforming committees, due to limited membership and/or a lack of requisite legal regulations governing their roles and responsibilities.24
Drawing on its experience of implementing SBM at elementary schools in its core provinces (especially in more remote regions in West Kalimantan), Kinerja applied a more holistic approach to assist all school stakeholders, including school committees and members of local communities, to establish better governance through an institutionalized and integrated planning and budgeting process that would help identify each school’s respective needs and priorities.
In contrast to SBM implementation in the core program, however, Kinerja applied a new model when revitalizing the school committees at its partner schools in Papua. In most parts of Indonesia, school committees consist primarily of parents, but in order to reflect Papua’s unique cultural traditions, Kinerja expanded the membership of school committees to also include religious and indigenous leaders, as well as more women, young people, and representatives from village administrations.
24 In January 2017, Kinerja and its cost extension M&E partner, Solidaritas, conducted an endline study to reassess the schools’ respective performance levels following the program’s intervention. The results of this study are provided in the M&E chapter.

29
Kinerja’s SBM package comprised the following six stages: (1) the introduction of education service standards; (2) a community complaint index and school self-evaluation; (3) the participatory preparation of school plans and budgets involving school principals, teachers, school committees and community leaders; (4) the transparent and accountable application of these school plans and budgets; (5) the strengthening of school committees to oversee the implementation of the school plans; and (6) the strengthening of school committees to conduct advocacy if service charter implementation is lacking.
In addition to these efforts at the school level, an inherent part of Kinerja’s implementation strategy was to strengthen district-level service providers, to enable them to provide sufficient support to schools beyond the life of the program. To this end, Kinerja worked alongside its DEO partners to implement the program’s activities, as well as assisting them to establish education ITATs whose members included school supervisors and senior DEO policy makers. Like their DHO counterparts, which Kinerja helped to establish in 2015, the education ITATs were created to provide technical assistance to schools to ensure that SBM is implemented fully and to a uniformly high standard, and to advocate for policies and budget funds to replicate Kinerja’s SBM package to new schools in their districts.
Kinerja also built good working relations with officials at the PEO. The program provided technical assistance in a number of different areas, but one major achievement of the collaboration was the establishment of a provincial education facilitation team (PEFT), which will take the lead in overseeing SBM replication at schools in new districts across Papua.
Box 3: Kinerja-supported schools launch first service charters
All 30 of Kinerja’s partner schools, in Jayapura, Jayawijaya, and Kota Jayapura, launched their newly developed service charters and technical recommendations at public signing ceremonies in August and September 2016.
More than 150 people attended the ceremonies, including school principals, district education council (DEC) members, committee heads, senior officials from the PEO, each district’s DEO and Bappeda, as well as legislators, district heads ,and village heads.
Both ceremonies were a great success, with the service charters and recommendations signed by school principals, and the heads of the DEOs, school committees and villages. The service charters were then returned to their respective schools, while the technical recommendations were submitted to the DEOs. All three DEO heads offered their appreciation to Kinerja and IPPM for initiating efforts to improve education services at schools in their respective districts.
Jayawijaya’s district secretary, in his welcome address, said he very much appreciated the support for schools with the involvement of local community members, and he expressed his commitment to follow up on the technical recommendations produced by all nine schools in his district.
The head of the DEO in Kota Jayapura said: “Today’s event is something that we [the government] never expected. USAID-Kinerja has managed to create a new ecosystem in education management, where all partners are equally committed to improving education in Papua. [The attendance of] schools, school committees, village heads, and government representatives shows that there is a collective commitment to work together.”
The heads of the Jayapura and Kota Jayapura DEOs also confirmed their commitment to scaling up the implementation of SBM to all remaining elementary schools in their districts, plus junior and senior high schools. The PEO offered similar praise for the complaint-survey process, which culminated in the service charters and technical recommendations, saying that this was just the start in what would become the PEO’s efforts to improve educational standards across Papua.
“Despite my own doubts at the start about how much could be achieved with SBM during such a short period of time, I am happy to see tangible signs of positive change—at both schools and DEOs—as a result of Kinerja’s support during the past year.”
[REDACTED]

30
Further details about the PEFT and the PEO’s replication plans are provided in the Replication chapter.
Key Achievements • Following the results of the baseline survey, Kinerja successfully revitalized school
committees, in line with its “expanded committee” model, at 26 of its 30 partner schools.25 The program also adopted this innovative model as the subject of a policy paper, which was warmly received by MOEC in February 2017. (See the Replication chapter for further details);
• The coordinator of a local organization, the Foundation for Christian Education (Yayasan Pendidikan Kristen [YPK]), was so enthusiastic about Kinerja’s SBM package and expanded school committees that he plans to use one of the program’s partner schools, SD Amai in Jayapura, as a benchmark to replicate the package at the 200 or so schools that YPK runs in Papua and West Papua.
• Despite being a relatively novel concept in Indonesia, all 30 Kinerja-supported schools conducted public complaint surveys to gather feedback on education services. The schools then developed and issued service charters based on the survey results (see Box 3 above).26
• A total of 3,237 respondents provided feedback during the complaint surveys (which became known locally as kantong noken), highlighting the degree of local buy-in to the process.
• In addition to the 30 service charters, the complaint surveys also produced 334 technical recommendations (127 in Jayapura, 117 in Kota Jayapura and 90 in Jayawijaya), concerning issues beyond the capacity and/or authority of schools to resolve on their own, which were submitted to the DEOs for follow-up.
• All 30 schools produced MSS-based work plans and budgets by the end of December 2016. Stakeholders at SD Inpres Nafri (Jayapura) and SD Negeri Koya Koso (Kota Jayapura) adopted a novel approach by incorporating their service charters into their school plans and budgets in order to accelerate the fulfillment of the promises contained within them.
• With program support, members of newly-revitalized school committees successfully advocated to village administrations for financial assistance to help improve conditions at their schools. As a result of their efforts, 13 village heads in Jayapura and Kota Jayapura provided village funds to Kinerja schools in their areas.27 The amounts ranged from [REDACTED] for SD Kanda in Jayapura, to build a perimeter fence and contribute to teachers’ subsidies, to [REDACTED] for SD Skow Sae in Kota Jayapura, to purchase new desks and chairs, repaint the school, create a sports field and lay a paved walkway.
• Since September 2016, 40% of Kinerja’s partner schools have either published or made available to the public midterm and annual work plans and/or financial reports. Previously,
25 The baseline survey team found that the committees at four of the schools (SD Abeale 1, Ayapo, Komba, and Yabansai) contained a sufficient number of members and, most importantly, already incorporated a good mixture of different stakeholders. 26 Further information about complaint surveys and some of the issues raised in the service charters is provided in the MSF section of the Good Governance chapter. 27 Five village heads in Jayawijaya also signaled their support for Kinerja schools by issuing similar decrees, but without specifying funding amounts. These will be confirmed, and funds disbursed, in 2017.

31
such information was generally unavailable, and parents were unable to access these documents to see how their children’s schools were performing.
• The heads of all three target districts demonstrated their commitment to the newly established DEO ITATs by issuing governing decrees. In addition to offering legal recognition, the decrees also guarantee the provision of district funding to cover the teams’ operational costs.
• With program support, and using new technical guidelines and checklists that Kinerja developed in conjunction with the DEOs and PEO, each of the ITATs conducted a full round of monitoring visits to Kinerja-supported schools in September 2016 (and, in Jayapura and Kota Jayapura, a second round in December 2016). The visits produced a number of additional technical recommendations, which were submitted to the DEOs for follow-up.
• A total of nine good practices, based on various aspects of the program’s work in Papua’s education sector, were documented and disseminated during the cost extension.28
• In collaboration with multimedia company Impro, Kinerja produced a new 12-minute film in January 2017, showcasing the program’s SBM implementation in Papua and highlighting some of the progress made at partner schools. The film features testimonials from key education stakeholders as well as parents, teachers, and members of school committees.
28 Details of these 9 education good practices, plus 17 health sector-related good practices that were documented during the Papua program’s lifetime, are provided in the Replication chapter.

32
[REDACTED]
Media
Due to geographical isolation, ethnic diversity and a lack of basic services, non-urban communities in Papua have very little access to information about public service issues and poor knowledge of their rights to basic health care and education. Varied cultural values and beliefs towards modern health care also forced the development of a very conscious and nuanced approach when Kinerja launched its media program in May 2013. The program applied a combined approach to enhance people’s understanding of their health rights, by using mainstream media (particularly radio) in conjunction with alternative media (based on local wisdom and cultural norms) to communicate key messages in an effort to stimulate demand for public service reforms among local communities and promote their involvement in efforts to improve service quality.
Through its two intermediary organization partners, the Indonesia Association for Media Development (Perhimpunan Pengembangan Media Nusantara [PPMN]) and Forum Lenteng, Kinerja’s media program trained and mentored community members in its partner districts to engage with PSD issues through citizen journalism; produced radio and TV programs (including interactive talk shows, and features) in collaboration with local media partners (including Suluh Papua, Radar Timika, Cenderawasih Pos, and Harian JUBI newspapers, RRI Wamena and Rock FM radio stations, and TVRI Papua); wrote features for local print media; and provided in-house trainings to build the capacity of several local radio and TV stations. In more remote areas, in Jayawijaya, Mimika, and some parts of Jayapura, Kinerja identified other ways to disseminate information on public services, such as information sessions after church sermons or religious activities, cultural events, festivals, or audiovisual presentation at the community level, and also off-air radio activities.
Articles produced by citizen journalists, whether online, in mainstream, or social media, as well as their appearances on radio talk shows led to their being regarded as public-service watchdogs by the wider public. With results such as health clinics providing cleaner and more comfortable spaces for patients and ensuring adequate supplies of medicines, to schools becoming more transparent and accountable and DEOs being persuaded to tackle the issue of unequal teacher distribution, efforts undertaken by citizen journalists had a significant impact in helping to improve healthcare and education services in Kinerja’s target districts.
Good Governance
A ‘youth journalist’ reads her article about school services in front of her class.

33
During the cost extension, Kinerja’s media strategy built upon the program’s past achievements by adopting a multi-stakeholder approach that focused on strengthening links between supply- and demand-side stakeholders (through interactive talk shows) as well as between citizen journalists and mainstream media outlets (through media tours to Kinerja-supported puskesmas and schools), to provide access to broader audiences and to raise public-service issues that might otherwise have gone unreported in both the health and education sectors. This strategy ensured that Kinerja’s interventions in health and education attracted broad media support and reinforced the program’s overall objective to improve basic services and standards in the two sectors.
Key Achievements • In total, 90 people who were trained by Kinerja’s intermediary organizations actively worked as citizen journalists up until June 2015, when Kinerja ceased recording citizen journalist activity. Many of these citizen journalists, as well as new citizen journalists trained by PPMN during the program’s cost extension, remain active. Between May 2013 and June 2015, citizen journalists and 34 Kinerja-affiliated media outlets produced a total of 874 media products (including written articles, radio talk shows, and documentary videos) on health sector issues.
• Kinerja helped to garner greater exposure for its Papua citizen journalists. Forum Lenteng showcased citizen journalist work on the Halaman Papua website, established in December 2013, and through film screenings, hard copy compilations of citizen journalist articles, and DVDs of their videos. Kinerja also
supported Papua citizen journalists to attend events around the country, including the Citizen Journalism Festival in Surabaya, East Java, and a national workshop co-hosted by Kinerja and the US Embassy’s cultural center, @america, in Jakarta, both held in October 2014.
• During its final year of programming, Kinerja implemented a series of media tours to partner schools and puskesmas. These tours invited both mainstream media journalists and citizen journalists to get a close-up look at public service delivery issues and help raise awareness. The tours also resulted in stronger relationships between mainstream media and citizen journalists, leading to two newspapers (Salam Papua and Harian Papua) that had not previously been involved with the Kinerja program requesting articles
Box 4: US Ambassador stresses the importance of community input
US Ambassador to Indonesia Robert Blake visited one of Kinerja’s newly selected partner schools, SD Inpres Komba in Jayapura, on January 22, 2016, to mark the launch of the program’s SBM intervention in Papua. Kinerja organized a radio talk show for the ambassador’s visit entitled “The Importance of Community Complaints to Improve the Quality of Education Services.”
The talk show, which featured SD Komba’s Head Teacher, school committee coordinator, a local village representative, and Kinerja’s Public Services Oversight Specialist, addressed some of the key issues and challenges in elementary education in the locality. The show was also broadcast live via three local radio stations (Radio Republik Indonesia Jayapura, Rock FM Jayapura, and Radio Suara Kasih Papua Sentani).
One listener who participated in the phone-in expressed his appreciation for the improved cooperation between SD Komba’s staff and committee members with members of the local community. Ambassador Blake said he was impressed with what he had seen and, during a question and answer session with local media, stressed the importance of all stakeholders working together to improve education services: “The involvement of the community and parents is what makes a difference.”
Ambassador Blake also offered encouragement to all current and aspiring citizen journalists by answering a question put to him by one of them in attendance: “Citizen journalists like you are very valuable, especially in offering input on public services at the community level. I would strongly encourage the use of as many mechanisms [such as MSFs and citizen journalists] as possible to increase community participation.”
34
written by citizen journalists for publication. This was both in recognition of citizen journalists’ skills and the desire to expand coverage of local issues.
• Kinerja-trained citizen journalists from Kota Jayapura and Mimika were invited to provide content for a book published in 2015 by the LSPPA. Entitled Integrated Service Mentoring Program for Women and Child Victims of Violence Based on Public Service Standards, the book provided information about the services available in the two districts for women and children affected by domestic violence.
• As part of Kinerja’s sustainability strategy, Forum Lenteng established three community-based citizen journalist/filmmaking collectives (Komunitas Hiloi in Jayapura, Riyana in Kota Jayapura, and Yoikatra in Mimika) in 2014 to promote citizen journalism through alternative media channels. Due to the quality of their work, all three groups soon attracted non-program support for their continued activities, and each received critical acclaim—both at home and abroad—for feature-length documentaries on health-related issues that they produced in 2015. Yoikatra proceeded to achieve great success in 2016, when it won a prestigious Eagle Institute scholarship to produce a new film, Mama Amamapare, which went on to win Best Documentary Film at the Indonesian Film Festival in November 2016. (Further details about Yoikatra’s award-winning film are provided in the Sustainability chapter of this report.)
• One innovative feature during the cost extension period was the introduction of the Youth Journalist (Jurnalis Cilik) program at five of Kinerja’s partner schools. This program aimed to encourage what may be the next generation of citizen journalists, as well as to spark children’s interest in being a part of improving education services. The program proved popular with both students and teachers; the principal at SD Wamena, Jayawijaya, even promised to award extra credit to any of her teaching staff who published articles in the media or highlighted topics that were taken up by local radio stations for further coverage.
Minimum Service Standards Kinerja’s support for the application and integration of MSS underpinned its efforts to promote governance reforms in the delivery of public services. The quality of public services in health and education is measured against nationally mandated MSS indicators and targets (see Box 5 below), whose application is governed by Government Regulation No. 65/2005 on the Preparation and Implementation of MSS. Through activities such as comparative studies, workshops, and targeted mentoring, Kinerja increased stakeholders’ awareness and understanding of the importance of using service standards to improve both the quality and delivery of healthcare services and assisted them in developing strategies and action plans to implement service standards.
“We [Yoikatra] want to see improvements in public healthcare in Papua. We also want to show how documentary films can be braver, both in terms of themes and how those themes are presented; young filmmakers must become braver. If you really want to criticize the government, just do it. Films can change reality.”
[REDACTED]

35
When Kinerja launched its MSS intervention in May 2013, the primary aim was to improve the capacity of LGs, particularly DHOs, in the program’s four supported districts, to apply MSS to health service management, especially to planning, budgeting, implementation, and M&E at district and SDU levels. LGs compiled MSS data on health and, with program support, verified the data and analyzed the gaps between their targets and existing conditions. Plans to fill these gaps (so-called “costing” plans) were then developed and incorporated into their annual plans and budgets. Kinerja also supported SDUs to improve their annual planning and budgeting by conducting needs analyses and integrating MSS, and assisted LGs and SDUs to monitor and evaluate their MSS achievements.
The program also worked to increase the participation of demand-side stakeholders (including MSFs, citizen journalists, and mainstream media) in promoting and overseeing the issue of improved governance of health and education services based on national standards. Service standards remained a core focus during the program’s cost extension, feeding into virtually all aspects of Kinerja’s work at provincial, district, and SDU levels. In the health sector, Kinerja re-engaged with its DHO partners in Jayapura and Kota Jayapura29 to review MSS achievements in each district before assisting them to update their former MSS costing calculations using a new combined module (developed in collaboration with UNICEF, PKMK, and the PHO) that merged Kinerja’s MSS costing tools with UNICEF’s evidence-based planning (EBP) tools.30 In order to ensure that the interests of puskesmas were also met and SDU-level MSS fulfilled, the program (again, together with UNICEF and the PHO) developed and tested a new Integrated Puskesmas Planning (IPP) framework to align and synchronize health center planning with DHO planning and budgeting.31 As a result of these efforts, Kinerja’s partner DHOs and puskesmas are
29 In Jayawijaya during 2014–2015, the former DHO head chose to apply MSS at the puskesmas level as opposed to the district level. Given the limited implementation time frame during the cost extension, the new acting DHO head decided to maintain the focus solely on MSS achievement at the SDU level. 30 By adding the EBP component, problems or gaps in planning and/or budgeting can be analyzed more distinctly through bottleneck analysis, resulting in the chance to accelerate the achievement of MSS based on performance. 31 Taking MOH’s existing puskesmas planning protocol as a foundation, the new 12-stage IPP process, which incorporates UNICEF’s Integrated Micro-Planning tools and provides for substantial community input when finalizing puskesmas activity plans, culminates with the integration of priority activities into DHO work plans and budgets. As a result, SDU-level planning and budgeting reflect district-level goals and priorities, while district-level planning and budgeting support each SDU’s needs.
Box 5: National standards for health and basic education
Health:
Prior to November 2016, there were 18 MSS indicators for the health sector, as laid out in MOH Regulation 741/2008 on MSS in Health. These 18 indicators addressed four main areas: primary healthcare (incorporating MCH), healthcare referrals, epidemiology and prevention, and health promotion.
A new law, MOH Regulation 43/2016 on MSS in Health, was released in November 2016, with 12 new indicators replacing the previous 18.
Basic Education:
MOEC Regulation No. 23/2013 on Amendments to MOEC Regulation 15/2010 on MSS in Basic Education contains 27 MSS indicators.
Of these, indicators 1–14 are district-level MSS (such as the equitable distribution of qualified teachers and principals, and ensuring regular monthly visits by school supervisors to all schools), which are the responsibility of DEOs to fulfill.
Indicators 15–27 are school-related MSS (such as the availability of text books/teaching supplies and teachers’ working hours) ,which are incorporated into school plans and budgets.

36
now working more closely together, particularly with regard to planning and budgeting based on MSS achievements and targets.
Faced with similar challenges of low capacity on MSS when launching the education intervention, Kinerja provided a series of workshops for school and LG partners to increase their knowledge
about MSS. This included information on MSS indicators in basic education, how to integrate the indicators into school and district planning documents, and how to cost MSS. As with health, there was a particular focus on evidence-based planning and budgeting. The program also engaged with the provincial government to encourage it to
apply MSS in the health and education sectors.
Key Achievements • In 2014, for the first time, DHOs in Jayapura, Kota Jayapura, and Mimika established MSS
costing teams (comprising DHO staff and MSF members) and completed all the stages involved in applying MSS costing to midterm and annual planning and budgeting, including costing, incorporating costing results into planning documents, preparing budgets based on priority activities and/or MSS costing, and successfully evaluating their MSS achievements.
• DHO allocations for achieving MSS targets increased in three of Kinerja’s partner districts. In 2014, in response to advocacy efforts from the MSS costing teams, LGs in Jayapura, Kota Jayapura, and Jayawijaya allocated [REDACTED] respectively, toward MSS fulfillment. The Jayapura DHO also received [REDACTED] in Otsus funding to meet its MSS targets in health.
• DHOs in Jayapura and Kota Jayapura also successfully revised their MSS costing calculations using the program’s new combined EBP-MSS module in 2016 for the 2017 financial year. Costings were fully integrated into respective planning and budgeting documents.
• Kinerja successfully supported 14 puskesmas (including 5 non-partner puskesmas) in three districts to produce activity plans. In two of the three districts (Jayapura and Kota Jayapura), priority activities from each of the nine completed puskesmas activity plans were integrated through the IPP framework into their respective DHOs’ plans and budgets for 2017.
• A key feature of the IPP process was the inclusion of public consultations of puskesmas activity plans, which allowed for public feedback from local communities and key figures such as village heads and other leaders. These consultations often opened up new avenues of funding for puskesmas activities and needs, such as from the local villages. For example, all the village heads present at the public consultation for Puskesmas Depapre’s activity plan agreed to provide funding to help cover operational costs at safe delivery houses, while one village head contributed funds for medicine, patient transportation fees, additional food for malnourished babies and the elderly, and the renovation of auxiliary health clinics (pustu).
“The integration of DHO and puskesmas planning and budgeting is extremely valuable. So, too, are the public consultations of health center activity plans with local communities and village authorities, which have helped to improve puskesmas-level planning overall.”
[REDACTED]

37
• All of Kinerja’s 30 partner schools completed self-evaluations with the program’s support in order to move towards national accreditation. As part of this, schools developed MSS achievement maps based on eight existing national service standards (Standar Nasional Pendidikan). The results of the evaluations and MSS maps, together with the results of complaint surveys, were incorporated into annual school planning and budgeting for 2017.
• Despite challenges with data gaps, low capacity, and the short cost extension timeframe, Kinerja successfully assisted DEOs in the program’s three partner districts to complete the MSS costing process and to incorporate costing results into their 2017 work plans. All three work plans were signed and issued by the end of December 2016.
• In close cooperation with the PEO and Bappeda, Kinerja developed technical guidelines to accelerate the application and achievement of education MSS in districts across Papua. The guidelines were signed in late 2016 and are intended to be a valuable resource for the PEFT in speeding up MSS achievement at both schools and the district level.32 Signaling their strong commitment to meeting MSS targets, the PEO independently started to map levels of MSS achievement in the 15 under-served districts where it intends to replicate Kinerja’s public service-oriented SBM program in 2017. (Please see the Replication chapter for details.)
Multi-Stakeholder Forums
What set Kinerja apart from other development programs was its focus on demand-side stakeholders—namely, local communities—to encourage citizens to become actively involved in productive dialogue with their LGs and public service providers. Kinerja supported efforts to increase people’s awareness of their rights to access basic services and to articulate demands for better services. The key part of this process was the establishment or revitalization of strong community forums (MSFs) to provide input to LGs, mediate problems, and conduct oversight of SDUs.
A total of 48 MSFs were established in Kinerja’s four target districts, at both SDU and district levels.33 They played an active role in conducting complaint surveys, supporting the drafting of service charters, monitoring their implementation, and making technical recommendations to LG technical offices.
32 Kinerja originally intended to develop similar guidelines with the PHO. However, the PHO was loath to undertake efforts to assist districts to accelerate MSS achievement, as the national government was due to introduce new health-related MSS indicators, as explained in Box 5 above. 33 These MSFs comprised 16 health-sector MSFs (12 SDU- and 4 district-level MSFs in Kinerja’s original target districts), 30 school committees at Kinerja’s partner schools in its three target districts for education, and two revitalized district education councils in Jayapura and Kota Jayapura. (Despite Kinerja’s best efforts, the existing council in Jayawijaya was not receptive to the program’s aims, and opposed the addition of new members to better reflect Papua’s local context).

38
Service charters were the end product of complaint surveys, during which hundreds of service users provided feedback on the SDU’s services and facilities.34 Complaints generally covered infrastructure, management, and service provision issues. Each service charter, which was essentially a series of “promises” developed in coordination between a given school or puskesmas and the local community, outlined improvements that were to be made. Once signed,
the service charters were printed and displayed, either in puskesmas waiting rooms or on school notice boards, to support transparency. Problems identified during complaint surveys that could not be solved internally by the puskesmas or school itself were listed as a series of technical recommendations. District-level MSFs/district education councils would then discuss the recommendations with their local DHO/DEO for follow-up, and monitor their implementation.
Over time, as an increasing number of LGs began to recognize the value of MSFs and the contribution they made to their own efforts to improve health and education services, many forums were granted legal status by government decrees, which not only allowed them access to government funds to support their oversight and monitoring activities but also provided a significant boost to their future sustainability.
Key Achievements • A total of 42 service charters (12 for health and 30 for education) were developed by
Kinerja’s partner schools and puskesmas in coordination with service users and MSFs/school committees. A combined total of 771 promises (160 in health and 611 in education) were made by the SDUs. In August 2016, 100% of the health promises were determined by the MSFs to have been fulfilled, while in education, 20 of the 30 partner
34 Kinerja’s complaint-handling process, which included public complaint surveys and service charters, was developed from the findings of a Complaint-Handling Study, which was conducted by the German Society for International Development as part of its Support for Good Governance project.
Box 6: Kinerja provides MSFs with Women’s Leadership Training
As part of its commitment to mainstream gender in all areas of its work, Kinerja developed and conducted the three-stage Women’s Leadership Training (WLT) between March and October 2016 for 35 women members of health MSFs from all four target districts.
The first part of the training provided an introduction to topics such as gender and sex; gender equality and equity; how gender interacts with culture, tradition and religion, and women’s rights. The second training focused on introducing the participants to social analysis, enabling them to analyze social problems from a gender perspective. The issues analyzed included maternal mortality, domestic violence, early marriage, polygamy, and HIV/AIDS. The training also explored what it means to be a woman leader who is also gender sensitive.
The final stage of the WLT focused on improving women’s practical advocacy skills. Many of the women are already active advocates for change in their areas, but are sometimes hesitant to take up issues because of a lack of skills and knowledge, as well as feeling unable to talk to key community and government figures. This training aimed to tackle these challenges by providing interactive instruction on public speaking, lobbying, networking, taking a leadership role, and community organizing.
The program also provided follow-up mentoring for the MSF members between each of the training stages, to review the topics covered during the previous training session and to see how the women were using what they had learned in their respective communities.
By the end of the training, which included a number of practice sessions and role plays, 93% of participants said they felt either “very ready” or “ready” to take up gender inequality issues with cultural leaders in their areas. Only 7% of participants said they did not feel capable of bridging communication between community leaders about gender inequality, compared to 20% at the start of the training.
As a conclusion to the WLT, Kinerja supported the women in developing advocacy action plans for 2017, in response to local puskesmas needs in each district.

39
schools achieved over 70% of promises within just four months of issuing their service charters.
• Several MSFs garnered increased appreciation and recognition from their local DHOs, who over time came to recognize the important role they can play in helping to improve public services. For example, in Kota Jayapura, the DHO issued a decree guaranteeing the involvement of MSFs in the ITAT supervisory visits to puskesmas, and specifically tasked the MSFs with monitoring the level of community participation and complaint-handling mechanisms.
• Kinerja’s MSFs also achieved some success in advocating for service improvements. For example, the district MSF in Jayapura successfully advocated for village funding, which allowed for the recruitment of additional health volunteers to assist puskesmas by monitoring the incidence of TB in the district and, where possible, ensuring that people diagnosed with TB completed their course of treatment. In another example, the MSF at Puskesmas Musatfak successfully advocated to the DHO for the construction of a new puskesmas building, and the renovation of the former puskesmas to become a safe delivery house for expectant mothers.
• Kinerja had long-advocated for MSFs to be granted formal legal status, as such institutionalization would not only provide them with operational budget funding but would also offer them legitimacy as recognized civil society representatives, in a position to offer valuable input toward the development of public service policy. By the end of the Kinerja Papua program, LGs had issued governing decrees for 44 MSFs (all 4 district health MSFs; 9 subdistrict health MSFs in Jayapura, Jayawijaya, and Kota Jayapura; 30 school committees; and the district education council in Jayapura)—around 90% of the total 48 MSFs.
“I had never thought about women’s empowerment before [the WLT] and I didn’t see that many things could be improved. However, this training has given me the strength to do something about it.”
[REDACTED]

40
[REDACTED]
Although not mandated as with Kinerja’s core program, replication was a fundamental aspect of Kinerja Papua’s overall strategy. Kinerja aimed to do this by building ownership and commitment among governments and district heads in order to improve PSD beyond the program’s initial SDUs in partner districts, and beyond partner districts during the cost extension.
Kinerja’s basic design supported replication in two ways: first, by basing its interventions on existing good practices and national programs, such as SBM, and second, by implementing its sectoral interventions through intermediary organizations, which could continue to provide services beyond the life of the Kinerja program. The program’s replication strategy consisted of documenting and disseminating good practices, encouraging exchange between SDUs in all four partner districts, and, during the cost extension, promoting the adoption of interventions at the provincial level.
Replication in Papua primarily focused on Kinerja support to LGs in its partner districts to further expand innovations to new SDUs. During the cost extension, Kinerja also provided technical assistance to the provincial education and health offices to initiate replication in non-partner districts across the province.35
District- and Provincial-Level Replication Based on its replication strategy, Kinerja was keen to encourage LG partners in Papua to share their good practices and innovations among one another to improve PSD and encourage broader implementation.
The first step in this process was the Health Barriers and Good Practice Seminar, which was organized by Kinerja intermediary organization BaKTI and held in May 2013. Senior officials from LGs in all four partner districts and the PHO attended the seminar, during which they were presented with examples of innovations from across Eastern Indonesia. Many LGs had never encountered PSD-related good practices before, and this stimulated significant interest and a commitment to develop their own Papua-based good practices. By the end of the two-day seminar, each of the four LGs identified the following key good practices for immediate follow-up and implementation: integrated handling of AIDS, TB, and malaria (ATM) through the establishment of a district-level ATM center and ATM posts at subdistrict and village levels (Jayapura); a safe delivery house for expectant mothers (Jayawijaya); a mobile/SMS-based data collection system, known as “m-Health,” to gather and store health-related statistics (Kota Jayapura); and a safe delivery house for expectant mothers in remote areas, as well as a safe house for women subjected to domestic violence (Mimika).
35 Budgetary allocations were made by the end of the Kinerja program, with replication due to begin in 2017.
Replication
Community members and health center staff discuss services at an outdoor talk show in Jayawijaya.

41
In September 2015, Kinerja facilitated a second good practice seminar (Papua Sehat or “Healthy Papua” seminar), also facilitated by BaKTI. Attended by around 200 people, including provincial government representatives, LG officials, partner puskesmas staff, and MSF members, the seminar provided the opportunity to share information on Kinerja’s good practices and how they were being implemented at both SDU and district levels. Examples included the provision of village funds for health volunteers to combat TB in Jayapura as a result of MSF advocacy, and the beneficial impact of complaint surveys to improve health services, drawing on the experience of Puskesmas Koya Barat in Kota Jayapura, which, as a result of the complaint survey, now has an ambulance to respond to medical emergencies.
In addition to these seminars, and particularly during the cost extension, Kinerja Papua put strong emphasis on producing useful knowledge management material that met stakeholders’ needs and interests. These products included three good practice books (covering 19 good practices—10 in health, 9 in education), six program infographics, a series of three illustrated handbooks for education stakeholders, guidelines for teachers interested in implementing the Youth Journalist program, six stories of change, and two promotional films.36 All these materials were printed and shared among supply and demand stakeholders, as well as uploaded onto Kinerja's website, which was also revamped and relaunched at the beginning in May 2016 to make it more user-friendly and provide a greater focus on Kinerja’s work in Papua.
Health Kinerja’s health program was scaled up in all four partner districts, and included replication of MSFs, complaint-handling mechanisms, MSS-based action plans, IPP, SOPs, handling of GBV cases, and MSS costing (Table 3).
Table 3: Puskesmas-Level Replication of Kinerja’s Health Interventions
MSFs Complaint Handling
Action Plans IPP SOPs GBV
MSS costing
Kota Jayapura
Kotaraja X X X X Waena X X X Abepura X X X Imbi X X X Jayapura Utara X X X X Skow Mabo X X X Hamadi X X X Yoka X X X Elly Uyo X X X Twano X X X Jayapura Kanda X Harapan X X X X Mimika Wania X X X X
36 A complete list of these good practices, stories of change and films, as well as other publications produced during the Papua program is provided in Annex 3.

42
Kwamki Lama X X X
Timika Jaya X X X
Ayuka X X Jayawijaya Wolo X X Elekma X X X Wamena Kota X X Pelebaga X X Bolakme X X Kurulu X X X Walelagama X X Asolokobal X X Asologaima X X Yallenga X X
NOTE: MSF=multi-stakeholder forum; IPP =integrated puskesmas planning; SOP=standard operating procedure; GBV=gender-based violence; MSS=minimum service standards
Key Achievements • More than 30 Kinerja good practices were replicated at 26 additional puskesmas in the
four partner districts (beyond the program’s 12 original partner puskesmas). Costs involved in replication were jointly covered by LGs, puskesmas, and Kinerja.
• Through working with health ITATs to implement the new IPP mechanism, Kinerja supported five non-partner puskesmas in three districts to develop their proposed activity plans for 2017. In Kota Jayapura, these puskesmas activity plans were incorporated into the DHO’s own planning documents. The DHO head was so enthusiastic about the new mechanism that he instructed the remaining eight puskesmas in the district to develop their own activity plans. Meanwhile in Jayapura, the head of the DHO allocated funds to replicate the IPP process at all 19 puskesmas in the district in 2017.
• Five subdistrict head decrees were issued to formalize newly established MSFs in five subdistricts in Kota Jayapura in 2016. These decrees provide the MSFs with legal status, and allow them to request government and village funding for their activities in supporting PSD oversight.
• The head of the DHO in Jayapura issued a circular letter in May 2016 providing directives to all 19 puskesmas in the district to improve healthcare services by installing one or more complaint handling mechanisms and implementing SOPs to manage complaint procedures.
• In Mimika, despite the agreement to provide only limited support on a request basis during the cost extension, the DHO allocated money for the replication of three good practices at three non-partner puskesmas in 2016. The good practices covered developing service SOPs and forming SOP teams; forming MSFs, conducting complaint surveys and developing service charters; and performing MSS costing. Kinerja and DHO staff monitored the SOPs in late 2016, and replication was assessed to be progressing well, with Puskesmas Kwamki Lama staff stating that they felt confident enough to draft new SOPs by themselves in the future.

43
• At the provincial level, Kinerja trained members of the PHFT on the new combined EBP-MSS module to enable them to use the module in MSS trainings and support for other districts across Papua. The PHO also planned to introduce the new IPP mechanism to additional districts in 2016 but was ultimately unable to do so due to national budget cuts, leading to the postponement of these replication efforts until 2017.
Education Due to the short time frame for the SBM program, Kinerja did not intend to focus on replication during the cost extension. However, stakeholders at both the district and provincial levels responded with enthusiasm to the program after recognizing the benefits that would be gained from applying public service-oriented SBM in schools.
Key Achievements • DEOs in all three partner districts issued circular letters in 2016 instructing all elementary
and junior high schools to implement Kinerja’s SBM program. The letters specifically instruct the schools to implement key features of SBM, including developing annual and four-year midterm work plans and budgets, based on MSS analysis relevant to each school, and the results of school self-evaluations.
• Scaling up has already begun in some districts. In Jayapura, with program support, the district education council assisted two non-partner schools (SD Inpres Lereh and SD YPK Onomi) to conduct their first-ever complaint surveys in November 2016. In addition, the DEO head in Jayawijaya approached Kinerja’s education intermediary organization, IPPM, to assist with the replication of SBM at the district’s schools for an initial period of one year. Jayapura and Kota Jayapura also expressed an interest in working with IPPM, but were unable to do so immediately due to local elections planned for early 2017.
• Kinerja supported the PEO to form a 28-member PEFT in April 2016, which will take the lead in overseeing SBM implementation at new schools in districts across the province. Members of the PEFT include representatives from the PEO (head, secretary, program staff, and school supervisors), Bappeda, Cenderawasih University, and the Education Quality Assurance Agency. The PEFT will provide direct technical assistance to replication schools, work closely with DEOs to fulfill their MSS targets, and produce policy recommendations to improve governance and education services at both district and school levels.
• Kinerja promoted its good practices in SBM for 65 district- and school-level stakeholders by organizing a four-day study trip in August 2016 for its 30 partner schools, district education councils, local legislators, and DEO and Bappeda staff. The tour visited Kota Probolinggo, a former Kinerja partner district in East Java, to see firsthand how SBM is being implemented. Upon returning to Papua, the group recorded 50 good practices that they felt were relevant to their needs and conditions in Papua and identified which were the most viable for implementation. Each district also developed a follow-up plan to be implemented in 2016–2017.
• The PEO allocated [REDACTED] to replicate Kinerja’s public service-oriented SBM program at elementary and junior high schools in the 15 least-developed districts that make up the Gerbangmas Hasrat region of Papua, with an aim to begin in 2017. The PEO also confirmed that it intends to use Kinerja’s 30 partner schools as model schools in SBM application to guide its replication efforts.

44
Cooperation with Development Partners During its five years in operation, Kinerja coordinated and cooperated with a number of development partners to address and promote different aspects of its overall goals in Papua. The reasoning behind these collaborations varied depending on intended outcomes, but generally Kinerja undertook specific activities with development partners to: (1) complement technical programming; (2) prevent duplication and programming overlaps; (3) support replication and achieve wider coverage; (4) maximize dissemination results; and (5) conduct joint events.
This section does not provide an exhaustive list of all such collaborative efforts; it offers an overview of the key initiatives that Kinerja undertook in conjunction with other donors.
As part of Kinerja’s efforts to support the Jayawijaya DHO’s decision to apply MSS at the SDU level rather than the district level (as mentioned in the Good Governance chapter), the program collaborated with the Clinton Foundation’s Health Access Initiative in 2013. It supported the development of MSS-based action plans at puskesmas, not only to measure gaps in MSS achievement but also to complete corresponding cost analysis. Kinerja and the Health Access initiative also cooperated in Jayawijaya to encourage the implementation of both service-oriented and technical SOPs at puskesmas across the district. As a result, the Health Access Initiative adopted service SOPs developed by Kinerja to support the integration of HIV/AIDS services in Jayawijaya, while the two entities also collaborated to develop new SOPs and work plans based on MSS achievement at each of Jayawijaya’s 13 puskesmas.
Kinera’s partner districts of Jayawijaya and Mimika were also working areas for the Scaling Up for Most-at-Risk Populations (SUM) II program, whose implementation strategy, like Kinerja’s, encouraged the establishment of district-level MSFs. Through joint coordination in 2013, Kinerja and SUM II identified an MSF in Jayawijaya that had already been established at the district level by the local AIDS Commission (Komisi Penanggulangan AIDS) as a vehicle to implement each program’s respective priorities. Although the Commission’s district forum was established to focus on HIV/AIDS issues, Kinerja and SUM II encouraged forum members to discuss broader health issues at the district level. SUM II also adopted Kinerja-supported complaint surveys as a tool to strengthen MSFs in its other work districts.
Also in 2013, Kinerja cooperated with the Amungme and Komoro Community Empowerment Agency (LPMAK)37 in Mimika, to increase the DHO’s capacity on MSS-based planning and budgeting. At the puskesmas level, LPMAK also encouraged the implementation of Kinerja’s service SOPs at health centers it supported in the district and promoted the implementation of action plans resulting from Kinerja’s PML training, conducted by PKMK.
In 2014–2015, Kinerja again joined forces with LPMAK, together with Freeport’s Public Health Malaria Control (PHMC), to collaborate on the development of a long-term action plan (designed by the DHO) to reform Mimika’s health system and create a new Regional Health System (Sistem Kesehatan Daerah). Drawing on its governance approach, Kinerja assisted LPMAK and PHMC by organizing public consultations of the draft documentation for the scheme. The program also facilitated discussions among the drafting team, Mimika DHO, LPMAK and PHMC to help move the initiative forward and decide upon the necessary steps to complete the documentation. However, the process took far longer than anticipated, and despite an initial deadline set for July 2015, the documentation was still unfinished by the time Kinerja Papua’s cost extension began in October 2015. The following month, Kinerja attended a meeting with the DHO, LPMAK, and PHMC, during which all parties agreed that Kinerja’s involvement would end, due to continuing uncertainty over when the documentation would be finalized.
37 LPMAK, which was established by PT Freeport Indonesia and is funded via the latter’s CSR subdivision, Public Health Malaria Control, implements health programs in Mimika on TB, malaria, water and sanitation, MCH, and nutrition.

45
When USAID announced in April 2015 that it intended to extend the Kinerja Papua program until 2017, Kinerja staff resumed discussions held with UNICEF in previous years to establish closer ties and cooperation in areas covered by both organizations. One key area was the work undertaken to improve the capacity of DHOs in planning and budgeting. In light of Kinerja’s cost extension plan to withdraw direct support to puskesmas and focus its work at the district level, there was a need to coordinate the two parties’ respective efforts and develop a single, more substantial approach by merging Kinerja’s MSS-costing tools with UNICEF’s evidence-based planning tools. After several months of technical meetings, held in conjunction with the PHO and PKMK, which previously helped UNICEF develop the EBP tools, Kinerja and UNICEF produced a new combined EBP-MSS module, which will be used by the PHFT to improve DHO planning and budgeting in districts across Papua.
As previously mentioned in the Good Governance chapter, Kinerja and UNICEF also developed a new 12-stage integrated puskesmas-planning (IPP) mechanism, which incorporates the latter’s integrated micro-planning (IMP) tools and provides for substantial community feedback at each stage of the process. As with the EBP-MSS module, Kinerja and UNICEF produced the new IPP mechanism in close collaboration with the PHO and members of the PHFT, who will take the lead in training DHO ITATs and puskesmas to use the mechanism in future SDU-level planning.
In September 2016, Kinerja facilitated an intensive, 11-day training in collaboration with Australia’s Department of Foreign Affairs and Trade’s KOMPAK program on puskesmas accreditation. The training, which was attended by 36 DHO technical staff from 11 districts across Papua (including ITAT members from each of Kinerja’s four original target districts) and representatives from the PHO and MOH, provided practice-based instruction, capacity-building role plays and field visits to health centers, to enable the participants to assess puskesmas applying for accreditation in accordance with the 776 elements contained within the national-level accreditation protocol. The training also provided guidance for the PHO officials in attendance to provide similar trainings themselves in the future.
In the education sector, Kinerja continued to use the World Bank’s Tools of Reporting and Information Management by Schools (TRIMS) at its 30 partner schools in Papua that had proved a great success with education stakeholders in Kinerja’s three former core program districts for SBM: Bener Meriah, Barru, and Kota Singkawang. The TRIMS, which Kinerja employed to assist schools to map general MSS conditions and their respective level of MSS achievement, promoted greater transparency in educational data and were useful in the process of developing school work plans.
In response to a request by the PEO, Kinerja collaborated with the Asian Development Bank’s Analytical and Capacity Development Partnership program in 2016 to assist PEO officials to develop a Strategic Plan (Renstra), in line with development planning documents at the provincial level in Papua as well as with performance targets and indicators at the national level, as defined by MOEC. Kinerja and the Partnership shared responsibility for implementing an eight-stage development process over the course of several months, which culminated in the completed Renstra (2013–2018) being signed and issued by the head of the PEO in June 2016.38
Improving Otsus Fund Management Papua Province was accorded Special Autonomy status in 2001. In accordance with accompanying legislation, Law No. 21/2001, the national government disburses annual funding to Papua’s provincial government, which then distributes 80% of the total revenue among the
38 The Renstra’s timeframe, five years starting from 2013, was in line with the term of the current Papua Governor, Lukas Enembe.

46
province’s 29 districts to improve the lives and welfare of indigenous Papuans.39 Otsus funding constitutes a major source of financial support for Papua. In 2016, for example, the 80% of Otsus funding that was divided among district governments totaled [REDACTED], of which 30% went to education and 15% to health. Despite these substantial funding flows, Papua remains one of
Indonesia’s least-developed provinces. According to the latest figures released by Indonesia’s Central Statistics Agency in 2015, Papua was ranked at the bottom of the Human Development Index (HDI) out of the country’s 34 provinces.40
A significant factor behind these figures is a widespread lack of fiscal management capacity among LGs in Papua in terms of planning, budgeting, monitoring, and reporting. However, the problems surrounding Otsus funding go far beyond the question of capacity, as a new RTI study on the management of Otsus funds revealed (see Box 7). During discussions on the subject with national ministries and agencies (Bappenas, MOH, MOHA, and the President’s Staff Office) in 2016, there was
acknowledgement about some of the shortcomings at the national level. These included a historic lack of oversight from the
39 The remaining 20% is earmarked for spending at the provincial level. Papua Governor Lukas Enembe revised the district-provincial split in Otsus funding from 60:40 to 80:20 after being elected in 2013. 40 With less than four points separating it from Papua, neighboring West Papua province ranked first from bottom on the HDI.
Box 7: RTI study into Otsus funding highlights challenges to reform
Following a request by the PHO, Kinerja conducted a study in April 2016 that sought to map existing control mechanisms relating to Otsus funding for health at provincial and district levels, and then identify the gaps between the practical application of these oversight and control mechanisms and prevailing legislation governing their implementation, as well as common procedures and SOPs.
Taking Jayapura as an example district, the study revealed a number of key issues that contributed to five preliminary conclusions: (1) poor performance in Papua reflects weaknesses in public financial management (PFM) nationally; (2) the PFM system is too complex considering the capacity of LGs in Papua; (3) PFM requirements are fulfilled in a superficial and mechanistic way; (4) funding allocations are made based on unclear criteria; and (5) Otsus funding tends to become the focus of special autonomy discourse, resulting in important issues for fixing the PFM system receiving less attention.
After presenting and discussing these findings with provincial and national government partners, the study team developed the following recommendations: ▪ Ministries (especially MOHA and Bappenas) should intensify their support of
Papua’s provincial government to enable it to provide leadership and guidance to district governments and other development stakeholders.
▪ The national government should provide support and incentives to the provincial government to define priority MSS for Papua.
▪ Design all new national structures in Papua that aim to coordinate and accelerate development in collaboration with Papuans, and consider the option of placing central level staff/units under the Papua Governor.
▪ A wealth fund for Papua’s future should be considered, to allow for the postponement of some Otsus fund expenditures until Papuan capacity can better absorb the funds.
▪ Attention should be paid to all other funding sources and synergized with Otsus funds.
▪ Greater attention should be paid to good governance at the village level, and the relationship between Otsus funds and other funds at this level.
▪ LGs should increase their use of third parties (contracted NGOs, churches, private sector) to improve service delivery in the health sector.
▪ Those in favor of reforming Papua’s financial management systems should form a forum to discuss whether Otsus funds should be integrated with or handled more separately from other LG funding sources.
▪ Papuan politicians should promote an Otsus Plus dialogue in Papua and West Papua, down to the grassroots level, before undertaking negotiations with the national level.
Kinerja presented the results in November and December 2016 to the head of Papua’s provincial Bappeda office, as well as national-level officials at Bappenas, MOHA, and the Office of the President’s Staff, to contribute to their respective Otsus reform agendas.

47
national government on how Otsus funds are used, and the absence of Papua-specific indicators to measure levels of achievement or quality in health-care and education services plus the extent to which they benefit the local population.
The challenges facing the national government and Papua’s provincial and district administrations in trying to address this issue are myriad and complex (not least because of the political sensitivity concerning the issue of special autonomy), and there are no quick fixes. Nevertheless, during its final year of programming, Kinerja was keen to support its provincial government partners to try and achieve some initial improvement by tackling the first stage—planning—in the fund-management process. To this end, Kinerja provided assistance to PEO, PHO, and Bappeda officials to develop two sets of technical guidelines, to improve their management and monitoring of Otsus funds allocated to the education and health sectors.
The guidelines are intended to support dedicated Otsus teams at the PHO and PEO to evaluate district-level Proposed Definitive Plans (Usulan Rencana Definitif [URD]), which comprise each district health and education office’s work plan and budget, containing all proposed Otsus-funded activities as agreed upon and finalized by district technical working units (Satuan Kerja Perangkat Daerah [SKPD]) in conjunction with their provincial-level counterparts and provincial Bappeda office.
Kinerja completed initial drafts of both guidelines by the beginning of March 2016, at which point they were reviewed by the PEO/PHO and follow-up meetings held to discuss several topics in greater detail. These included performance indicators that form the basis of planning and targets for district-level Otsus-related activities; the role of DEOs/DHOs, district Bappeda offices, and SDUs in managing Otsus funds; and finalizing the format for evaluating district URD. With the results of these discussions incorporated into the guidelines, Kinerja supported provincial officials to test the guidelines by conducting trial URD evaluations at the district level (in Jayawijaya for education and Jayapura for health) in order to gain a sound understanding of the challenges faced when applying the guidelines in each sector.41
From this point on, Kinerja continued to make steady progress with the PEO and Bappeda towards finalizing the Otsus guidelines for education through several follow-up meetings to review and discuss different aspects of the guidelines, and make amendments where necessary.42 Eventually, after a lengthy but smooth process, the Otsus guidelines for education were completed in September 2016 and signed by the head of the PEO in November 2016.
Kinerja continued to provide support to its PEO partners, even during the program’s closeout phase, by providing a refresher training in February 2017 for members of the PEFT. The two-day workshop allowed the team members to review each of the stages involved in the guidelines’ development during the previous year and to determine how best to address existing challenges in relation to using the guidelines to evaluate district URD.
In contrast to the steady progress made in producing the Otsus guidelines for education, finalizing the health guidelines proved a much greater challenge. When no progress was made between the second trial of the guidelines in July 2016 and the end of September 2016, it appeared increasingly likely that the guidelines would remain in draft form. However, as the program entered its last few weeks of programmatic activities, Kinerja staff redoubled their efforts and managed to
41 Due to low attendance by the Jayapura DHO, the trial of the health guidelines was repeated (with DHO staff from Jayapura and Kota Jayapura) but only in July 2016, after a delay of four months, due to the unavailability of key senior PHO officials and the replacement of the PHO’s head of programs and planning during the intervening period. 42 As part of this process, Kinerja presented the guidelines to DEO program heads from all four Kinerja districts plus five others (Intan Jaya, Keerom, Merauke, Puncak Jaya, and Tolikara) at a PEO-led coordination meeting in August 2016.
48
secure meetings with Bappeda and PHO staff during October and November 2016, to follow up on the second trial’s findings and work towards finalizing the guidelines.
Similar reviews and discussions were held with the provincial health officials and, as a result of the input gathered, the draft health guidelines were amended with additional material incorporated to offer step-by-step guidance on evaluating district URD, and slight amendments made to annex material—on how to develop a URD, and the URD format. After several additional meetings with relevant stakeholders, the health guidelines were formally agreed upon and finalized by mid-December 2016.
Due to the amount of time needed to complete both sets of guidelines, Kinerja was unable to fulfill its original work plan objective of monitoring their implementation at the district level while building the capacity of district stakeholders in developing URD; nor was there an opportunity to further strengthen the capacity of provincial government officials and Otsus team members in evaluating URD. However, given the limited implementation period during the program’s cost extension together with the inherent complexities concerning Otsus funding, the creation of these two innovative, practical tools is, in itself, a great achievement.
A key factor that contributed to the success of this intervention was the role played by senior officials at Bappeda, who were staunch supporters and advocates of both sets of Otsus guidelines throughout the course of their development. By the end of December 2016, Bappeda had disseminated the health and education guidelines to DHOs and DEOs across Papua with instructions to use them as a reference when preparing their respective URD. Furthermore, although there remains limited understanding among some Bappeda staff about each of the stages involved in completing URD evaluations, others within the agency have begun to use both sets of guidelines to evaluate URD at the provincial level.
Also, in February 2017, Kinerja received information confirming that both the PEO and the PHO disseminated their respective guidelines to DEO and DHO staff from across Papua at their latest technical coordination meetings (Rakornis). This is very good news, as it is a clear indication that both provincial offices are following up on the achievements of 2016, and intend that the Otsus guidelines will be used in 2017 by both district and provincial staff to improve Otsus-related planning and management.
National-Level Replication Efforts
Cooperation with LAN Kinerja first began to work with the State Administrative Bureau (Lembaga Administrasi Nasional [LAN]), which encompasses Indonesia’s national training center for government staff, in 2014 to help the bureau revise its curriculum and training guidelines. LAN was keen to alter its overall training strategy and adopt Kinerja’s more practical approach in order to better enable LG staff to improve public services. To achieve this, the plan was to incorporate case studies from Kinerja’s former treatment districts from its core program, introduce aspects of a more competency-based curriculum, and develop different training packages to meet the needs of government staff at all levels, from senior policy makers down to frontline service providers.
Before work could begin on revising LAN’s curriculum, Kinerja assisted the bureau to amend the training package’s governing legislation (PerKa LAN No. 10/2011 on Guidelines for the Implementation of Public Service Training). Although a final draft of the revised regulation, PerKa LAN No. 28/2015, was completed in March 2015, it remained unsigned until the end of September 2015, coinciding with the closure of Kinerja’s core program. This prevented program staff from following up on the curriculum and providing a TOT on the new material for LAN’s provincial- and

49
national-level Master Trainers, as originally planned. With confirmation of Kinerja Papua’s extension through to March 2017, however, LAN and the program jointly agreed to make Papua the pilot province for the first trainings.
Papua’s Bappeda office and Education and Training Agency (Badan Pendidikan dan Latihan [Badan Diklat]) welcomed the decision, maintaining that there was a great need to improve the competence of government officials, at both provincial and district levels in the province.
Following a series of meetings with LAN to discuss the shape of the new training package, it was agreed that Kinerja would revise several of its own technical modules (developed during its core program) to include topics such as MSS, service SOPs, complaint-handling mechanisms, and civil society engagement, and adapt them for the Papuan context. Both parties also agreed to develop a new module on leadership and change management.
The final draft of the new Public Service Training curriculum—comprising a seven-chapter module for policy makers and an eight-chapter module for frontline staff—was presented to the head of Badan Diklat, together with all of the agency’s division heads and Master Trainers, in June 2016. They responded enthusiastically to both the modules and after adding a few more Papua-based case studies to the module for frontline staff, Kinerja conducted a TOT in July 2016 for Badan Diklat’s Master Trainers and representatives from other provincial and district government offices, including the BP3AKB, Regional Disaster Management Agency and Village Communities Empowerment Agency.
Kinerja then assisted Badan Diklat to amend the frontline module slightly and conduct the first official Public Service Training for subdistrict heads, school principals and puskesmas heads from three of Kinerja’s target districts (Jayapura, Jayawijaya, and Kota Jayapura) in September 2016.43 The five-day training, which was also attended by representatives from village administrations and provincial and district Bappeda offices, was a great success; so much so, that within days of the training ending, the head of Badan Diklat confirmed that he would allocate [REDCATED] from the agency’s 2017 budget to train other subdistrict frontline staff from Jayapura, Jayawijaya, and Kota Jayapura plus Merauke, Mimika, and Tolikara.44
National-Level Knowledge Exchange Kinerja recognized the importance of establishing and maintaining good working relationships with stakeholders at the national level. Apart from the national-level FGDs that Kinerja organized prior to the launch of implementation (as mentioned in the Introduction chapter), which included MOH and the National AIDS Commission, Kinerja’s engagement with national ministries was limited until the cost extension began in late-2015. Thereafter, Kinerja held regular meetings with relevant technical ministries, both to provide information on the program’s interventions and achievements in Papua and to obtain input to inform and further develop these efforts. These meetings also provided an opportunity for Kinerja to obtain support from its national network for the wider dissemination of the program’s good practices to improve the chances for long-term sustainability.
Shortly after Kinerja’s cost extension began, program staff met with several ministries to provide information and progress updates on several of the program’s provincial- and district-level activities. During the course of three days in January 2016, Kinerja met with the National 43 Although the Public Service Training modules were developed with district-level staff in mind, the head of Badan Diklat decided to concentrate initially on training subdistrict staff, maintaining that there was a greater need to improve financial management and good governance at that level due to the substantial amount of funding that subdistricts and villages receive from the national government. 44 Although Badan Diklat’s focus in the short term is to conduct trainings for frontline officials, it remains committed to delivering trainings of the second module for senior government staff and policy makers in the future.

50
Development Planning Agency (Bappenas) and the Ministry of Home Affairs (MOHA) regarding the development of Otsus guidelines for health and education; with MOEC regarding the development of the PEO’s Strategic Plan (Renstra); and with representatives from Asian Development Bank’s Analytical and Capacity Development Partnership program regarding the launch of Kinerja’s work on MSS in basic education.
Later that same month, Kinerja met with Yohana Yembise, the Minister for Women’s Empowerment and Child Protection, and two deputy ministers to update them on Kinerja’s progress and achievements in addressing GBV in Papua since the previous meeting with the ministry in May 2015. Kinerja explored the possibility of creating closer working ties with the ministry, both to support the minister’s focus on GBV as well as to improve the services provided to survivors of violence in Mimika by building the capacity of the district’s recently established P2TP2A team to become a benchmark for the provision of GBV-related counseling. During the meeting, Kinerja also presented the minister with its newly documented good practice on the handling of GBV cases in Kota Jayapura.
As a result of this meeting, Kinerja hosted a visit to Mimika by one of the deputy ministers and two other ministry officials, to see firsthand some of the work being undertaken to combat GBV in the district. This in turn led to further discussions with the ministry, which provided the basis for a series of six capacity-building and awareness-raising activities that Kinerja implemented between May and November 2016 in its two target districts for GBV (Kota Jayapura and Mimika) to support the ministry’s aims and objectives.
Box 8: USAID, Bappenas, & MOHA impressed by Kinerja’s work in Papua
Kinerja welcomed to Papua USAID’s new head of the Democracy, Rights and Governance Office, David Hoffman, together with senior national government officials including Bappenas’ Director of Communications and Politics, Wariki Sutikno, and MOHA’s Sub-directorate Head for Papuan and West Papuan Special Autonomy, Tomas Umbu Pati.
Keen to learn firsthand about Kinerja’s work in health and education, the group visited SD Minimo and Puskesmas Hom-Hom in Jayawijaya, and SD Amai, SD Depapre, and Puskesmas Depapre in Jayapura.
At each of the venues, Kinerja’s partners reinforced the program’s governance approach by citing positive changes that had come about as a result of community participation in wider LG efforts to improve both the delivery and quality of public services. For instance, Alpius Lupia, a senior DEO official in Jayawijaya, highlighted how community members had helped to obtain additional land for their local school via its newly expanded school committee: “With the cooperation of local people, we can achieve a great deal.”
Jayapura District Head Mathius Awaitouw echoed this sentiment, explaining that previously the LG did not know how to properly connect with local communities but now, with Kinerja’s support, they have established a strong partnership with the district’s MSF and district education council to work together to improve services in health and education.
Pak Wariki said, as quoted in Antara Papua, that he was “happy to see the changes resulting from Kinerja’s program [in Papua]. The national government is paying close attention to development here,” he added. “This is just one small example of the government’s innovation, through our cooperation with USAID.”
Pak Tomas, meanwhile, recommended that other districts in Papua also adopt Kinerja’s approach to improve the quality of education services. “If this USAID program is beneficial for the community, we at MOHA encourage all districts […] to adopt this approach using their APBD [annual budgets],” he said, as quoted by the Cenderawasih Pos.
During their time in Papua, USAID and the ministry representatives also attended a Kinerja-run training on GBV for religious leaders from all four target districts, and met with staff from USAID’s new GBV program for Eastern Indonesia, BERSAMA, to explore how Kinerja’s work to combat GBV can be sustained in the province in the future.
51
Kinerja and USAID also held several meetings with Bappenas and MOHA during the first six months of 2016 to secure an extension to the working agreement between USAID and Bappenas in line with the Papua program’s cost extension time frame. As a result of these meetings, Kinerja hosted a field trip in September 2016 for USAID and officials from the two ministries to the program’s working sites in Jayapura and Jayawijaya (see Box 8 above). In addition, MOHA’s Director General for Regional Autonomy organized a forum in October 2016 to allow Kinerja to share its good practices, based on the program’s efforts to improve PSD in Papua’s education and health sectors, and discuss possibilities for wider replication within the frame of national programming.
The good practice workshop was attended by representatives from MOHA, MOH, MOEC, Bappenas, the Ministry for State Administrative and Bureaucratic Reform (KemenPAN-RB) and LAN, as well as other agencies responsible for the provision of public services.
For its part, Kinerja secured the attendance of the secretary of Papua’s PEO and the head of the Jayapura DHO’s programs and planning division, together with the directors of two of Kinerja Papua’s intermediary organizations, YHI and IPPM, to act as resource persons and to participate in a talk show on public service-related good governance.
One of the participants at the workshop, Bappenas’ Wariki Sutikno, who had been on the joint USAID-Bappenas-MOHA trip to Papua the previous month, referred to the signs of development that could be seen in Kinerja’s districts, albeit admitting that the pace of progress in the province was slower than in other parts of the country. There was consensus among those present, however, that government reforms were urgently needed in Papua; one of the key challenges highlighted was the number of government appointments that continue to be made based on political considerations rather than meritocracy and competence.
In terms of Kinerja’s impact on education services, PEO Secretary Protasius Lobya referred to the positive changes that had taken place at the program’s 30 partner schools and three partner DEOs, despite the limited time available for implementation. He made special mention of the newly expanded school committees and complaint-survey process which, he maintained, had galvanized local communities and village administrations to become actively involved in improving education services. Pak Lobya was equally enthusiastic about Kinerja’s assistance at the provincial level, in helping PEO officials to form the PEFT, and supporting the new team’s members to improve their management of Otsus funding, as well as increasing their knowledge and capacity in applying MSS and monitoring district-level progress towards the achievement of MSS targets.
With regard to health, the Jayapura DHO’s Eduard Sihotang confirmed that he and his health office staff had benefitted greatly from the support Kinerja had provided to them during the past four years. In his opinion, one of the greatest achievements during that time was the change in mindset among health workers and directors at puskesmas, primarily as a result of the program’s emphasis on promoting community participation via MSFs. He maintained that puskesmas staff now perceived MSFs as their partners in helping to improve healthcare services, which in turn had encouraged them to become more engaged in their work. Pak Eduard also highlighted the successful application of MSS at puskesmas, with their integration into annual and midterm plans, and the implementation of service SOPs that had helped to improve management at many health centers.
When discussing how to scale up and replicate Kinerja’s good practices, everyone agreed the need for three key elements: (1) the issuance of relevant regulations at national, provincial, and district levels; (2) the documentation of information and knowledge in the form of manuals and/or guidelines; and (3) capacity development to ensure the delivery of services that meet high standards.

52
Overall, the event was enthusiastically received and Kinerja’s holistic approach of working with both LG and civil society stakeholders attracted special mention. During a wrap-up session facilitated by MOHA’s Sub-directorate Head for Papuan and West Papuan Special Autonomy, Tomas Umbu Pati (who also joined the visit to Kinerja’s working areas in September 2016), all the participants agreed that the program had produced a number of positive changes in Papua and expressed their confidence that these improvements would be sustained and further replicated.
As for the program’s district-level work in Papua’s health and education sectors, Kinerja also ensured that it followed up with MOH and MOEC during the year, since previously meeting with both ministries prior to the closure of Kinerja’s core program in 2015.
In February 2016, Kinerja met with senior officials at MOH’s newly-formed Directorate General for Primary Health Care (PHC), which is headed up by the program’s primary contact at the ministry—the former director of MCH. The meeting was very productive and gave those present an opportunity to share updates about Kinerja’s ongoing progress in Papua and the PHC’s aims and targets in 2016. The PHC directorate and Kinerja agreed to liaise on the development of draft technical guidelines for puskesmas mentoring by DHO ITATs, while Kinerja made a commitment to assist the directorate with its puskesmas accreditation targets for 2016, as outlined by President Joko Widodo.45
During Kinerja’s last programmatic quarter, program staff developed the following three policy papers, which were submitted to MOH’s PHC directorate in early 2017:
1. Bimbingan Teknis dan Supervisi Terpadu, Indikator Penting untuk Tercapainya Pelayanan Kesehatan Prima (Integrated Technical Assistance and Supervision, As Key Indicators for the Achievement of First-Rate Health Services)
2. Perencanaan Tingkat Puskesmas Terpadu: Harmonisasi Perencanaan Kesehatan Vertikal dan Partisipatif (Integrated Puskesmas Planning: Harmonizing Vertical and Participatory Health Planning)
3. MSF/BPK sebagai Wadah Partisipasi Masyarakat untuk Peningkatan Kualitas Pelayanan Kesehatan di Daerah (MSFs/BPK as a Platform for Public Participation to Improve the Quality of Regional Health-Care Services)46
All three policy papers were welcomed by MOH officials (from the ministry’s PHC, family health, health promotion and community empowerment, and accreditation and quality divisions) and Bappenas’ deputy director for health and nutrition at a follow-up meeting in February 2017. In their feedback, ministry staff acknowledged that each of the policy papers —but particularly those on MSFs and IPP—was a tremendous contribution to the country’s puskesmas accreditation program. The meeting also allowed for initial discussions on the several recommendations contained within each policy paper, and agreement was reached that these talks would continue at Kinerja’s national workshop later in the month, with a view to MOH selecting which recommendations it would adopt for national implementation.
Kinerja also had fruitful discussions with MOEC during its final year in operation. In April 2016, Kinerja met with the head of MOEC’s Center for Policy Analysis and Synchronization, and the
45 Kinerja followed up on its commitment by facilitating the 11-day puskesmas accreditation training for DHO staff, in collaboration with KOMPAK, as previously mentioned in this chapter. 46 This latest policy paper on MSFs was an updated version of a paper Kinerja submitted to MOH in 2015, entitled MSF: Strategi Perlibatan Masyarakat untuk Meningkatkan Kualitas Pelayanan Kesehatan di Tingkat Kabupaten/Kota dan Kecematan (MSFs: Community Engagement Strategy to Improve the Quality of Health Services at Subdistrict and District Levels). The 2017 version provides greater emphasis on the structure of MSFs (ideally, ensuring as broad a cross-section of local communities as possible) and complaint-handling mechanisms.

53
ministry’s Special Staff for Regional and Central Relations (and former head of Papua’s PEO). The meeting aimed to mainstream the lessons learned and recommendations that Kinerja had compiled in a policy paper it submitted to the ministry in 2015 (Public Services in the Education Sector: Governance in PTD, BOSP & SBM) and to update MOEC on its SBM intervention in Papua.
MOEC welcomed the news about the introduction of SBM in Papua and confirmed that the ministry planned to issue a Strategic Plan and legislation to promote community participation to help improve education services across the country. Recognizing Kinerja as a leading advocate and practitioner of this approach, the program was invited to present its good practices and lessons learned, based on implementing SBM, Educational Unit Operational Cost Analysis (BOSP), and proportional teacher distribution (PTD) in its four core-program provinces, to MOEC staff later in the month.
A number of issues were discussed after the presentation, including how to address unequal teacher distribution and high levels of teacher absenteeism; calculating BOSP unit costs and managing budgets at both DEOs and schools; varying levels of fiscal capacity in different regions in relation to education budgets and educational outcomes; and how to establish good collaboration between schools and parents. In conclusion, Kinerja provided the ministry with copies of its five documented good practices in education and four technical modules (from the core program), as well as copies of the district legislation that LGs in Kinerja’s former core districts had issued to support the program’s three education packages.
As in health, Kinerja also produced a new policy paper on SBM shortly before programmatic activities ended in December 2016. Entitled Revitalisasi Komite Sekolah Kontekstual Lokal untuk Penguatan MBS Berpelayanan Publik (Revitalizing School Committees in Keeping with the Local Context to Strengthen Public Service-Oriented SBM), the paper focuses on the role played by school committees as well as providing a detailed account of how Kinerja expanded the committees at its 30 partner schools to better reflect and more fully represent local communities in the program’s three target districts.
Kinerja discussed the paper at a meeting in February 2017 with a senior advisor to MOEC and the ministry’s section head for basic education, as well as the head of MOHA’s sub-directorate on education.47 The policy paper and its recommendations were warmly received, particularly as its timing coincided with MOEC’s latest plan to overhaul Indonesia’s SBM program and revitalize school committees nationwide.48 Upon examining each of the nine recommendations put forward in the paper, the meeting participants identified five for further in-depth discussion at Kinerja’s upcoming national workshop. These five included the widespread replication of Kinerja’s SBM package; revitalizing school committees at model elementary, junior high, and senior high schools, as determined by MOEC, in all districts nationwide; encouraging village administrations to use their funding allocations to help local schools improve their facilities and education services; and a directive to protect the independence of school committees by ensuring members are selected by district education councils rather than school principals.
Kinerja conducted its national workshop on February 21–22, 2017, in Bogor, near Jakarta. Marking the formal end of the Kinerja program, the workshop, entitled National Policy Recommendations for the Expansion of Innovations to Improve Public Services in Health, 47 The meeting was also attended by the principal of SD Inpres Komba, one of Kinerja’s partner schools in Jayapura, and the directors of three of the program’s intermediary organizations for SBM – IPPM from Papua, the Indonesian Institute for Education Innovation Training and Consulting (Lembaga Pelatihan dan Konsultan Inovasi Pendidikan Indonesia – LPKIPI) from East Java, and the Center for Community and Education Research (Pusat Kajian Pendidikan dan Masyarakat – PKPM) from Aceh. 48 This plan was developed following the appointment in September 2016 of a new education minister and the issuance soon after of new legislation – MOEC Regulation No. 75/2016 on School Committees.

54
Education and BEE, provided a platform for sharing good practices and lessons learned from both Kinerja’s core and Papua programs. Attended by USAID/Indonesia’s new Mission Head [REDACTED] and Democracy, Rights and Governance Office Director [REDACTED], as well as RTI’s Vice President for Governance and Economic Development, [REDACTED], the event hosted senior national government officials and LG and civil society representatives from 11 of Kinerja’s best-performing core districts and each of the program’s four districts in Papua. Members from a number of Kinerja’s intermediary organizations, past and present, also attended and provided information on their various efforts from regions across Indonesia.
The workshop was a great success, as participants engaged in panel discussions and talk shows that addressed key issues in health and education from both a supply- and demand-side perspective. Keynote presentations were also given, by KemenPAN-RB’s Deputy Assistant for Public Service Information System Management and Policy Formulation, [REDACTED], USAID’s [REDACTED], and a member of Indonesia’s House of Representatives (Dewan Perwakilan Rakyat), [REDACTED].
As mentioned above, alongside the workshop’s activities, senior Kinerja staff held sideline discussions with officials from MOEC, MOH, and MOHA to continue talks on the program’s policy recommendations for health and education.49 At the end of the workshop, all the recommended policies (for all three sectors) were read out to the participants. After one more round of follow-up meetings with MOH and MOEC, the ministries adopted the following policies for nationwide application.
Health:
• District-level MSFs (formally known as BPKD [Local Health Consideration Forums] in national legislation) will be revitalized by expanding their membership, structure, and funding sources in order to strengthen their role in accordance with Law No. 36/2009 on Health.
• MOH will issue technical guidelines and provide capacity building in relation to integrated technical assistance and supervision that is more comprehensive, appropriate to local contexts, and meets local needs.
Education:
• Recognize the importance of MOEC Guidelines, contained in Regulation No. 75/2016 on School Committees, to ensure the application of public service-oriented SBM and to clarify the role of school committees.
• In order to accelerate school development, especially at elementary schools, the Ministry for Villages, Regional Development in Remote Areas and Transmigration and MOHA need to produce a new policy to encourage village administrations to help improve the provision of school-level education services via Village Fund Allocations (Alokasi Dana Desa).
• Both MOEC Regulation No. 44/2012 on Levies and Fee Donations and MOEC Regulation No. 75/2016 on School Committees approve and encourage schools and school committees to collect funds from parents and local communities to meet their school
49 Similar talks were held with MOHA on BEE, based on a policy paper, Penyederhanaan Jenis Izin, Pengefektifan Izin Usaha Mikro dan Kecil (IUMK) dan Perbaikan Pelayanan Terpadu Satu Pintu (License Simplification, to Improve the Effectiveness of Micro and Small Business Licenses and to Improve One Stop Shop [OSS] Services), which was developed by Kinerja’s former BEE partner, The Asia Foundation. As a result of these talks, plus a follow-up workshop with MOHA and other relevant ministries in March 2017, the national government plans to (1) compile technical guidelines on license simplification pursuant to Presidential Regulation No. 98/2014; and (2) pass authority for micro and small business licensing services from subdistrict administrations to district-level OSS.

55
development needs. However, this approval conflicts with Presidential Regulation No. 87/2016 on a Task Force to Eradicate Illegal Payments. Schools and their committees are afraid to ask for voluntary contributions or donations from students’ parents, which can affect the availability of extra-curricular activities. Therefore, it is recommended that a special policy be issued to prevent a conflict between the MOEC regulations and the presidential regulation.50
The adoption of these recommended policies by Kinerja’s national partners was a great endorsement of the program’s work since the core program was launched in 2010. By way of wrapping up its engagement with national government stakeholders, Kinerja gave a presentation to senior officials at the President’s Staff Office in March 2017, which covered the program’s key achievements in health, education, and BEE—in both core provinces and Papua. Kinerja also provided information about the policies that the technical ministries had adopted for implementation.
50 In addition to these three SBM-related policies, MOEC also confirmed the adoption of Kinerja recommendations pertaining to the program’s two other education packages, BOSP and PTD. For BOSP, the government aims to ensure that LGs use their annual budget funds to fill any existing gaps in order to meet schools’ operational needs. For PTD, MOEC will seek to introduce a stronger regulation on teacher distribution and ensure the involvement of a wide cross-section of stakeholders in implementing the program.
“The Kinerja program has produced many good practices that improve people’s welfare, which should be replicated. I, myself, have witnessed the changes that have come about as a result of Kinerja’s initiatives. This is the time for all government administrations, from the national to the local level, to adopt Kinerja’s good practices and recommendations.”
[REDACTED]

56
[REDCATED]
Kinerja placed a strong focus on sustainability since the beginning of program implementation, as it believed that supporting the development of sustainability structures was a beneficial way of encouraging long-term change and ensuring the program’s gains were not lost once the program closed.
The primary method of encouraging sustainability was to work through intermediary organizations —14 Indonesian CSOs that worked at the district or provincial level in Kinerja’s partner areas. This meant that not only was local capacity built, but the CSOs themselves developed or strengthened partnerships with local governments, leading to the potential for ongoing cooperation. Additionally, Kinerja’s staff and consultants were also primarily local residents, again meaning that governments are able to engage them as experts in the future.
One of Kinerja’s overriding goals, particularly during the program’s final year, was to reinforce existing links between LGs, intermediary organizations, and civil society, in order to provide the best chances for the sustainability of good practices and innovations.
Sustainability
MSF members meet with the Jayawijaya government to advocate for formal recognition of their forum.

57
As part of these efforts, Kinerja held six sustainability workshops during the program’s closeout phase in late 2016 and early 2017. The workshops aimed to encourage governments to consolidate and further replicate Kinerja’s interventions and to support relationship-building. The first four workshops were held at the district level in each of Kinerja’s partner districts in November 2016 and focused on highlighting local good practices and innovations for further scaling up, as well as illustrating to the LG the results of integrating governance principles into public service delivery. The fifth workshop was the Papua provincial workshop, held in November 2016 in Kota Jayapura. It was attended by government officials from across the province, including non-partner districts such as Keerom and Sarmi, who attended using their own LG budgets to learn from Kinerja’s experience. Turnout at each workshop was good, with LG representatives from village and subdistrict administrations, DHOs/DEOs, Bappeda, and DPRD in attendance, together with staff from puskesmas and schools, MSFs, district education councils, school committees, intermediary organizations, and citizen journalists.
Finally, the national sustainability workshop was held on February 21–22, 2017, in Bogor, and explored both Kinerja core and Kinerja Papua good practices. It provided a unique chance for partners and intermediary organizations from Papua, East Java, South Sulawesi, West Kalimantan, and Aceh to meet and learn from one another and featured break-out workshops on education, health, and BEE.
Kinerja also worked to develop good relationships with similar international development programs being established in Papua and across Indonesia, to ensure that Kinerja’s experiences and established structures are passed on. Kinerja’s senior management team met several times with BERSAMA, the new USAID-funded GBV program based in Papua, to encourage it to work with Kinerja’s MSFs (especially with members who participated in the
Box 9: Papua citizen journalists exemplify sustainable success with Eagle, IFF wins
As part of its sustainability strategy, Kinerja formed community groups of citizen journalists through its intermediary organization partner, Forum Lenteng, to produce and disseminate information about local people’s experiences as users of basic health services, using alternative media including documentary films. One such community group was Komunitas Yoikatra in Mimika.
With full program support during 2013–2015, Yoikatra achieved local success for several early films, but it was with Tiga Mama, Tiga Cinta (Three Women, Three Loves), a documentary highlighting the experiences of three women working in Mimika’s health sector, that Yoikatra first received international attention when the film was screened at the International Filmmakers’ Forum in South Korea in September 2015.
Direct program support ended in June 2015 when Forum Lenteng’s grant ended. Utilizing all it had learned during its collaboration with Kinerja, the citizen journalists continued to develop as a filmmaking collective. In addition to producing a series of five new documentary shorts in 2016, Yoikatra entered the prestigious Eagle Awards Documentary Competition, which provides a forum for documentary filmmakers across Indonesia to use cinematography to highlight and comment on important social issues.
With the theme of the 2016 competition entitled Healthy Indonesia, Yoikatra submitted its proposal for a new film, Mama Amamapare. In July 2016, after several rounds of voting, the Eagle Institute announced that Yoikatra was one of five winners, enabling it to receive intensive mentoring from Eagle’s senior filmmakers to turn its award-winning proposal into a polished film.
Mama Amamapare tells the story of Mama Yakoba, a traditional birth attendant from Amamapare Village in Mimika, who despite the hardships in her own life remains committed to helping women through the rigors—and sometimes dangers—of childbirth. The film highlights the important role that Mama Yakoba and others like her play in an area where the availability of more formal healthcare services is extremely limited.
In October 2016, Mama Amamapare was premiered, together with the other four Eagle award-winning films, at a gala screening in Jakarta, which was attended by Indonesia’s Health Minister, Nila Djuwita F. Moeloek. Further success followed for Yoikatra soon after, when Mama Amamapare won Best Documentary Film at the Indonesian Film Festival in November 2016.
58
Women’s Leadership Training) to fight violence against women. Many of Kinerja’s former staff are also now working with other development programs, including KOMPAK, LANDASAN, and BERSAMA, as well as directly with national government ministries as consultants.
Some good indications of the sustainability of Kinerja’s interventions are already visible in Papua. A total of 29 new regulations (18 in health and 11 in education) were issued at provincial, district, and subdistrict levels during FY 2016.51 These policies included regulations to support improved governance in PSD, improvements in service quality in both health and education, the active participation of civil society stakeholders, and the scaling up and replication of SBM. For example, as mentioned in the Replication chapter, the PEO has committed to replicating Kinerja’s SBM program to 15 underserved districts in an attempt to improve basic education in the Gerbangmas Hasrat region of the province.
Four health and three education ITATs were established in the program’s target districts and the PEO and PHO are well-placed to establish additional ITATs across the province. At the district and SDU levels, signs of sustainability are also emerging: DEOs in Jayawijaya, Kota Jayapura, and Jayapura have issued circular letters to replicate SBM to all elementary and junior high schools in the three districts, and all 30 revitalized school committees at Kinerja’s partner schools have been formally recognized by their respective DEOs. Similarly in the health sector, 14 partner MSFs have been granted governing decrees, while Mimika and Kota Jayapura have begun to replicate health MSFs to puskesmas in additional subdistricts. Meanwhile, the female members of health MSFs trained during the WLT will continue to work on their action plans during 2017, aiming to improve the quality of health services in their respective districts. LGs have also allocated funds in their 2017 annual budgets for both health and education ITATs, indicating that allocations will continue in future years.
During the cost extension period, Kinerja also worked closely with the Papua provincial government to ensure that knowledge of both good governance and Kinerja’s interventions would become part of government-led trainings. The provincial government is responsible for quality assurance and oversight as well as the capacity development of not just provincial but also district government employees, which means it plays a crucial role in passing on skills to wider audiences. This transfer of knowledge and skills is vital to the sustainability and replication of Kinerja’s interventions.
At the national level, by providing support to bodies related to civil servant training, such as LAN, Kinerja aimed to ensure that principles of good governance were well embedded in national training and learning programs. The successful implementation of LAN’s new Public Service Training for frontline officials in Papua resulted in Badan Diklat allocating budget funds to conduct further trainings for subdistrict and district government staff in 2017. The hope is that with its newly revised curriculum in place, LAN will also introduce similar trainings for frontline staff and policy makers in other parts of the country.
51 LG regulations were not recorded as part of Kinerja’s M&E plan prior to the cost extension; therefore, the exact number of policies issued to support Kinerja’s health-sector interventions during that period is unknown.

59
As Kinerja learned during its core program, working with national ministries is crucial to a program’s sustainability. Even in a decentralized environment like Indonesia, fostering strong relationships with relevant ministries is fundamental in integrating good practices into nationwide programs. Although Kinerja only intensified national-level engagement during its final year, having achieved and documented success in different areas, the program garnered a great deal of support from national partners. Subsequently, Kinerja contributed to policy development by producing four policy papers (as detailed in the Replication chapter) based on the program’s sectoral interventions in Papua, and sharing them with MOH, MOEC, and Bappenas. As a result of policy discussions, and field visits from ministry officials to Kinerja’s work locations in Papua, technical ministries adopted five of the program’s policy recommendations (two for health and three for education) for national implementation.

60
RTI International engaged two M&E partners during the course of the Kinerja Papua program. The first was Social Impact, focused on M&E activities for the Kinerja Papua program, from its launch in March 2012 through until July 2015. The second partner, Solidaritas, undertook M&E activities as one of Kinerja’s intermediary organizations during the Papua cost extension, from October 2015 until its grant ended in February 2017.
This chapter presents an overview of the key M&E findings and achievements of the Kinerja Papua program.
October 2012 – June 2015 Social Impact designed a Performance Management and Evaluation Plan (PMEP) for managing and documenting all aspects of Kinerja Papua performance management. Monitoring activities focused primarily on providing key information for managerial decision-making and oversight. Kinerja Papua Assessments, on the other hand, were geared toward identifying changes that occurred in Kinerja Papua districts and SDUs.
Monitoring & Evaluation
Staff and community members at Puskesmas Tanjung Ria open the complaints box to assess feedback.

61
The M&E strategy comprised three discrete but integrated components: 1. Assessing organizational capacity of partner health units (puskesmas and DHOs) using
primary data
2. Assessing customer satisfaction with services they obtained in partner health SDUs using primary data
3. Tracking key performance indicators related to intermediate results (IRs) within all partner units and districts for: “Building on existing innovative practices and supporting LGs to test and adopt promising service delivery approaches” (IR 1); “Strengthening local demand for better services” (IR 2); and “Expanding successful innovations and supporting Indonesian intermediary organizations to deliver and disseminate improved services to LGs” (IR 3)
Key findings and achievements for each of these components are included in this chapter. For more information on Kinerja Papua assessments, please see Assessment of USAID/Indonesia’s Kinerja Papua Program, which was completed in July 2015.
Organizational Capacity Assessment The OCA survey was conducted in the 12 puskesmas and four DHOs supported by Kinerja Papua. A custom OCA survey was structured around the specific issues Kinerja addressed with reference to the program’s four governance areas (transparency, responsiveness, community participation, and accountability) and nine subdimensions.52 Respondents from randomly selected unit departments in each public health unit were asked their perception of their organization according to the governance-related indicators. The team used a two-stage randomized cluster sampling strategy to identify respondents, first selecting work units and then individuals within the unit. Baseline data collection was conducted in April 2013 and had a total sample size of 160 respondents, with 40 from each of Kinerja’s four target districts. Endline data collection was completed in March 2015 with 160 respondents—40 respondents in each district, and 10 respondents per organization.
OCA scores increased in all but 2 of the 12 puskesmas across the four districts. The greatest changes for these scores occurred in Mimika and Jayawijaya. Scores increased in the four governance areas for all 12 SDUs. Accountability—largely the strongest area for SDUs at baseline—yielded an average 16% increase overall and transparency scores increased by 20% on average. The greatest changes observed were for community participation and responsiveness, which saw average increases of 27% and 29% respectively. Each of the districts revealed similar strengths and weaknesses in terms of capacity in the four governance areas at the baseline—low scores in both community participation and transparency. Districts improved in the dimensions in these areas, but they remained the weakest. Accountability and responsiveness continued to be areas of strength.
Jayapura Kabupaten Jayapura had the highest mean district scores at baseline. Community participation had a district-wide average increase of 21%, while responsiveness had an average score increase of 24.6%. Average accountability and transparency scores, however, decreased by 5% and 9%, respectively. Health centers had accountability as their strongest area and community participation as their weakest in both the baseline and endline. Community participation was the greatest area of improvement for two puskesmas. All puskesmas had their greatest
52 The nine sub-dimensions consisted of: consistency between standards and implementation, performance measurement, follow-up of performance measurement, complaint-handling mechanism, monitoring system, community participation, consensus-based decision-making, accessibility of information, and unit outreach.

62
subdimensional increase related to the use of complaint mechanisms. At baseline, the DHO had the highest overall OCA score; however, the number decreased over time. The DHO’s scores for accountability, responsiveness, and transparency all decreased. It had its biggest increase in the subdimension on decision-making based on consensus/input from the community.
Kota Jayapura Overall OCA scores increased from baseline to endline (Table 4). Average scores for the four governance areas all increased in the district by varying degrees. Accountability and transparency increased, respectively, by an average of 2.9% and 15.8%. Responsiveness scores increased by an average of 21.7% and community participation scores increased on average by 15.5%. Responsiveness was the strongest governance area for all four SDUs in this district at endline. Three puskesmas all experienced the greatest increases in this area. Two puskesmas had the greatest increase in the subdimension on the use of a complaint-handling mechanism. The DHO’s overall OCA score increased, with the greatest improvement recorded in the area of community participation. The DHO had its biggest increase in the subdimension on the use of a monitoring system.
Table 4: OCA Baseline and Endline Scores Partner District
Partner DHOs & Puskesmas
Baseline Score
Endline Score
Kota Jayapura DHO 2.7 2.76
Kota Jayapura Tanjung Ria 2.74 2.85
Kota Jayapura Abepantai 2.72 3.05**
Kota Jayapura Koya Barat 2.75 2.86
Jayapura DHO 3.11 2.98
Jayapura Depapre 3.04 3.06
Jayapura Dosay 2.87 2.97
Jayapura Sentani Kota 2.75 3.12*
Jayawijaya DHO 2.21 2.15
Jayawijaya Musatfak 2.27 2.80***
Jayawijaya Hom-Hom 2.25 2.69***
Jayawijaya Hubikosi 2.03 2.69***
Mimika DHO 2.87 3.06
Mimika Timika Kota 2.73 3.13*
Mimika Mapurujaya 2.78 3
Mimika Limau Asri 2.3 3.01***
Note: statistical significance is noted as follows: * p < .1, ** p < .05, *** p < .01
Jayawijaya For both baseline and endline, scores in Jayawijaya were lower than in other districts. All three puskesmas saw increases in their overall OCA scores. The transparency scores increased by 50.2% on average, and responsiveness scores increased on average by 36.7%. Accountability and community participation scores appeared to have increased by similar margins. The health centers had increased scores in all four governance areas. Two puskesmas had the lowest overall OCA scores among the SDUs at baseline and despite increased scores, they remained at the

63
lowest rank. Puskesmas Hubikosi and Musatfak experienced the greatest changes in transparency, specifically for the subdimension on availability and access to information. The DHO mostly saw decreases in governance areas, including decreases in six of the nine subdimensions.
Mimika Overall OCA scores in Mimika were low at the time of the baseline, though they were higher than those found in Jayawijaya. However, large score increases resulted in Mimika becoming the top-scoring district by the time of the endline. Each SDU increased in all governance areas from the baseline. Community participation was the weakest area at both points despite an average 44.2% increase. Three puskesmas showed changes in the related subdimension regarding whether the community can participate in management. Responsiveness was the strongest area at both points, with a 36.1% increase on average. Large changes occurred in the subdimension regarding complaint-handling mechanisms. The DHO saw a modest increase in its overall OCA score. The unit recorded its largest change in community participation, especially the subdimension regarding the use of public input and consensus in decision making.
Customer Satisfaction Survey The Customer Satisfaction Survey (CSS) was conducted in targeted health centers to understand how targeted respondents perceived the health services being provided. The survey covered the same 12 Kinerja-supported puskesmas examined in the OCA and targeted respondents who were users of the puskesmas and visited them during the data collection periods. During baseline, respondents were randomly selected using time-clustered random sampling based upon each health center’s operating hours. At endline, time-cluster random sampling was used in 7 out of 12 of the puskesmas. At the remaining 5, a convenience sample was used because of a limited number of patients, decreased service times, and a number of non-operational days. A total of 150 clients were surveyed in each unit at the baseline and endline. Baseline data collection was conducted in February 2013 with a total sample size of 1,806. Endline data collection occurred in February and March 2015 with a total sample size of 1,871.
CSS scores increased from the baseline across all districts. The overall CSS score comprised individual puskesmas scores of the 14 performance indicators included in the CSS survey.53 Eight of these indicators were identified prior to the launch of the survey, as they directly related to Kinerja’s goals. Jayapura’s CSS score was the highest among the four districts; it also saw the greatest improvement. Jayawijaya recorded the second-largest change, although it remained the district with the lowest CSS score. Kota Jayapura, similarly, experienced a score increase, but remained the district with the second-highest CSS score in the endline. Lastly, Mimika showed the smallest change in score from baseline to endline, although it ranked third-highest in terms of its endline CSS score. Of the indicators, numbers 4 (staff discipline) and 12 (adherence to operating hours) were identified as the weakest for all the puskesmas at baseline. Endline data showed improvements for both of these indicators (Table 5).
Jayapura CSS scores increased among the three puskesmas in Jayapura. Service users in this district were also more satisfied in 2015 by 7.71 points than in 2013, making it the district with the largest change and highest level of satisfaction. All the puskesmas had higher endline CSS scores than 53 The 14 indicators comprised: procedural easiness, conformity of service requirements, clarity and certainty of the serving officer, staff discipline in delivering services, staff responsibility in delivering services, staff capability in delivering services, quickness of services, fairness of getting services, staff courtesy and friendliness in providing services, reasonableness of cost for obtaining services, correspondence between fees paid and cost specified, accuracy of implementation of the services schedule, comfort at the service unit, and security of the service unit.

64
at baseline. When comparing the health centers, Depapre remained the unit with the highest score in both the baseline and endline, with the highest rate of change. Puskesmas Dosay had the second-highest CSS score in the endline, followed by Puskesmas Sentani. In Jayapura, the five indicators showing the most changes were all directly related to Kinerja Papua.
Kota Jayapura Service users of the health centers in Kota Jayapura were more satisfied in 2015 than in 2013, and their level of satisfaction increased 4.51 points. Each of the units had increased endline CSS scores from the baseline. Puskesmas Koya Barat recorded the largest change from baseline to endline for customer satisfaction. In Kota Jayapura, the five indicators showing the biggest changes were all directly related to the program.
Jayawijaya Service users at the three puskesmas in Jayawijaya were also more satisfied, with their level of satisfaction increasing by 4.68 points. Although Jayawijaya remained the district with the lowest CSS score, it recorded the second-highest change between baseline and endline. Each of the SDUs had increased CSS scores in the endline. Puskesmas Hom-Hom remained the unit with the highest score in the endline as in the baseline. Puskesmas Musatfak had the second-highest CSS score in the endline, followed by Puskesmas Hubikosi. Puskesmas Hom-Hom also recorded the largest change from endline to baseline for customer satisfaction. In Jayawijaya, three of the five indicators with most change were directly related to the program.
Mimika Service users at health centers in Mimika were also more satisfied in 2015 compared to 2013, as their level of satisfaction increased by 4.46 points. Mimika recorded the smallest change in CSS score from baseline to endline, although it remained the district with the third-highest score. Each of the SDUs in Mimika had an increased endline CSS score. When comparing Kinerja’s partner puskesmas in this district, Timika Kota remained the unit with the highest score in the endline as in the baseline. Puskesmas Mapurujaya recorded the second-highest CSS score in the endline, followed by Puskesmas Limau Asri; Limau Asri also recorded the largest change from baseline to endline for customer satisfaction. In Mimika, three of the five indicators that experienced the greatest change were directly related to Kinerja Papua.

65
Table 5: CSS Baseline and Endline Scores Partner District Partner Puskesmas
Baseline Score
Endline Score
Kota Jayapura Tanjung Ria 73.47 78.19***
Kota Jayapura Abepantai 72.3 76.93***
Kota Jayapura Koya Barat 69.98 74.96***
Jayapura Sentani Kota 71.02 77.73***
Jayapura Dosay 71.66 80.33***
Jayapura Depapre 71.44 81.29***
Jayawijaya Hom-Hom 68.81 76.79***
Jayawijaya Musatfak 70.17 76.11***
Jayawijaya Hubikosi 68.63 72.22***
Mimika Mapurujaya 71.93 76.84***
Mimika Limau Asri 68.85 74.75***
Mimika Timika Kota 72.89 76.89***
Note: statistical significance is noted as follows: * p < .1, ** p < .05, *** p < .01
Qualitative Findings Regarding OCA and CSS Qualitative data collection (for both the OCA and CSS assessments) was conducted during March and April 2015 in all four Kinerja districts. Twenty-four FGDs and 10 key informant interviews were conducted with 134 respondents who were familiar with Kinerja Papua, including staff from 12 puskesmas, service users, and MSF members.
Behavior change among health unit staff SDU staff in all four districts considered the PML trainings effective in improving their knowledge and skills on management and leadership. The staff found they could easily apply their knowledge to their daily work. Education levels of the training participants influenced their receptiveness, while DHO officials in all districts more frequently mentioned scheduling issues vis-à-vis Kinerja’s trainings than puskesmas staff. Staff in all districts reported that improved understanding of MSS and SOPs motivated them to do their jobs better. The study also found that poor attitude, and particularly poor attendance, among staff reduced an individual’s motivation to improve. Even though knowledge and motivation had increased, units continued to struggle with implementing the management skills they had learned.
Community engagement in public service delivery The study found that community engagement in PSD had increased; a majority of respondents attributed this increased involvement to the establishment of MSFs. Puskesmas staff expressed their appreciation for MSFs in service delivery. However, they perceived MSFs differently across the four districts, depending on how the MSF members understood and embodied their role. For example, MSF members in Jayapura and Kota Jayapura perceived their roles as “overseers” of puskesmas, as opposed to MSF members in Jayawijaya and Mimika, who saw themselves as “helpers” of the puskesmas. Respondents’ demographic data further found that those members who were more likely to explain their role as “overseers” had prior experience with other development programs in contrast to members with less experience with other programs, who assumed their role as assistants or helpers to the health centers.

66
Customer satisfaction with health services SDU respondents noted that previously they did not care about customer satisfaction, but now, however, they noted that customer satisfaction was important and should be a goal of SDUs. Patients and MSF members noticed significant improvements in the delivery of health services. The improvements they described were based on simple demands, including improved operating hours, additional service in the afternoon, better patient waiting lounges, cleaner environments, shorter waiting times, friendlier staff, and better communication between clients and staff. The study found that almost all respondents attributed changes at the SDUs to the implementation of Kinerja-supported complaint surveys.
Conclusion The positive trends observed in the OCA—particularly among the puskesmas—suggest that partner health units increased capacity in all four governance areas. Improvement in these four areas was uneven, however. As with the OCA, the CSS found that the greatest increases generally occurred in the areas that were found to be weakest at baseline. Similarly, the greatest improvements also occurred in the districts and units found to have lower capacity at baseline. Weaker units came closer to the status of stronger units over time; however, stronger units did not see comparably sized improvements.
The CSS found higher rates of change as compared to the OCA. Low OCA scores for DHOs in each district suggest that large units and units with highly educated and busy staff are slower to improve organizational capacity. However, the nearly ubiquitous increase of OCA scores among puskesmas as well as puskesmas staff testimonials indicate that supply-side interventions supported positive changes. In addition, the public engagement mechanisms such as the MSFs and complaint surveys were identified by respondents in the qualitative study as being particularly beneficial for increasing community participation and improving responsiveness of units. These mechanisms contribute to improving customer satisfaction in certain indicators.
Despite these positive changes, however, challenges remained. Partner health unit staff appeared to have increased knowledge and skills related to policies and procedures such as MSS and SOPs as a result of Kinerja Papua, though the use of these knowledge and skills remained weak according to qualitative data. This was particularly true for the DHOs. This seemed to be associated with the busier schedules of DHO staff compared to those in the puskesmas. This may reflect an inadequate consideration of the differing needs of the various organizations. Likewise, qualitative data indicated that while the pedagogy of the trainings was well suited for many of the respondents in partner health units, it was not appropriate for all users.
Additionally, while puskesmas improved most in indicators tracking basic demands of clients (often related to infrastructure and staff discipline), these indicators are still associated with low satisfaction scores compared to other indicators.54 Furthermore, units did not improve at a similar rate in indicators related to more complex demands such as quickness of service and adherence to protocols. partner health units still have work to do in satisfying customers and adhering to government and unit-defined procedures.
Performance Indicators
Kinerja Papua activities led to progress in all three of the IRs outlined in the Kinerja Papua Program Results Framework. The program achieved 100% or more of the program target for all 22 indicators (Table 6).
54 With the exception of Indicator 12.

67
Table 6: Kinerja Papua Indicator Achievements (October 2012–June 2015)
NO. INDICATOR NAME PROGRAM TARGET
PROGRAM ACHIEVEMENT
1 GJD 2.2.3-3: Number of local mechanisms supported with US Government assistance for citizens to engage their subnational government
28 28 (100%)
2 GJD 2.2.3-4: Number of local nongovernmental and public sector associations supported with US Government assistance
19 24 (126%)
3 GJD 2.3.6: Number of individuals who received US Government-assisted training, including management skills and fiscal management, to strengthen local government
152 318 (209%)
4 GHI 1.2.2.2: Number of districts engaging civil society in health system oversight
4 4 (100%)
5 Score of Organization Capacity Assessment (OCA) 50% 81.3% (163%)
6 Number of Kinerja supported management systems that are adopted or institutionalized by local governments
8 20 (250%)
7 Average score of training test 50% 81% (162%)
8 Number of Kinerja Papua-supported action plans produced
96 310 (323%)
9 Number of Kinerja Papua-supported action plans implemented by District Health Office
12 69 (575%)
10 Number of Kinerja Papua-supported action plans implemented by puskesmas
36 206 (572%)
11 Number of Kinerja Papua-supported linkages between civil society organizations (CSOs), users, local legislative councils (DPRD), Dinas, etc., at subdistrict and district levels that are active in oversight of service delivery
20 20 (100%)
12 Number of multi-stakeholder forums (MSFs) established or strengthened by Kinerja Papua
16 16 (100%)
13 Number of service charters produced with Kinerja Papua support in puskesmas
12 12 (100%)
14 Number of promises fulfilled by puskesmas addressing complaints about services received through a Kinerja Papua-supported complaint mechanism
60 154 (257%)

68
NO. INDICATOR NAME PROGRAM TARGET
PROGRAM ACHIEVEMENT
15 Number of Kinerja Papua supported recommendation to district technical working units (SKPD)/DPRD/Bupati that have involved or are formally endorsed by other non-government actors
16 18 (113%)
16 Number of Kinerja Papua affiliated media-outlets that provide regular programing or dissemination activities related to health issues
28 34
(121%)
17 Number of Kinerja Papua-supported citizen journalists actively reporting on local government performance
40 90
(225%) 18 Number of media products produced by Kinerja Papua
affiliated media-related entities on Kinerja Papua-related issues
313 874 (279%)
19 Number of times Kinerja Papua-supported practices for health management systems are institutionalized by puskesmas not receiving direct implementation support
12 30 (250%)
20 Number of non-Kinerja Papua-supported health service units where institutionalization of Kinerja-supported practices for health management takes place
12 17 (142%)
21 Number of Kinerja Papua-supported good practices which are formalized for replication/wider use by Indonesian civil society organizations
4 6 (150%)
22 Customer satisfaction index related to health service units delivery
50% 100% (200%)
In total, 24 organizations received support from the US Government during the program (Governing Justly and Democratically [GJD] Indicator 2.2.3-4. This indicator target was overachieved (126%). Kinerja Papua also achieved its other GJD indicator, GJD 2.2.3-3, which measured the number of local mechanisms supported with US Government assistance for citizens to engage their subnational government. Kinerja also achieved its Global Health Indicator (GHI), measuring the number of districts engaging civil society in health system oversight (GHI 1.2.2.2).
On the supply side, Kinerja trained a total of 318 participants (231 women, 73%) and overachieved GJD 2.3.6 (209%). These trained individuals represented different partner health units. Of all health units, 81% of them increased their post-test score after receiving training from Kinerja’s partner, PKMK UGM (Indicator 7). The annual and program target for this indicator was 50%, meaning that the program assumed 50% of the partner health units would increase their average test scores. Kinerja met and exceeded this target.
Kinerja’s Local Public Service Specialists (LPSS) also worked closely with partner units and MSFs to advocate for the adoption of improved practices and management systems (Sub-IR 1.1), practices and systems highlighted in the trainings the units received. This progress was counted under Indicator 6, of which Kinerja achieved 250% of the program target. Technical recommendations were developed by Kinerja-supported units, as counted under Indicator 15. A

69
total of 18 technical recommendations were formed across all four Kinerja Papua districts during the program’s lifetime. Overall, Kinerja met 113% of its program target for this indicator. An example of a recommendation is the following, from Q3 FY 2015: The district of Jayawijaya signed a technical recommendation related to security issues with local indigenous populations. This recommendation was a result of advocacy conducted by various community leaders and government units, including Kinerja’s partner DHO and puskesmas.
Indicators 8, 9, and 10 document the progress made by Kinerja Papua health units in developing and completing action plans. These plans were created as a final output of the training the units received from Kinerja. A total of 310 action plans were developed in all four Kinerja districts by both partner DHOs and puskesmas. The target for Indicator 8 included short-term (3-4 months) and medium-term (6–12 months) action plans. However, long-term (more than 12 months) action plans were considered as additional achievements and reported in Q1 FY 2015. Long-term action plans were not included in the target as the implementation was thought to be beyond the scope of Kinerja Papua’s original timeline. Overall, Kinerja Papua met 323% of its program target for Indicator 8. A total of 69 action plans (24 short-term plans, 25 medium-term plans, and 20 long-term plans) were implemented by DHOs in the four partner districts. Similar to Indicator 8, long-term plans were not included in the target for Indicator 9, as the target only tracked the implementation of DHO short- and medium-term action plans. Overall, Kinerja Papua met 575% of its program target for Indicator 9. A total of 206 action plans (71 short-term plans, 72 medium-term plans, and 62 long-term plans) were implemented by puskesmas in the four districts. Overall, Kinerja Papua met 572% of its program target for Indicator 10.
Further supply-side progress was made in relation to service charters. A total of 154 promises were fulfilled by June 2015, as reported by MSF monitoring results. Promises were made to address complaints received through the complaint surveys and were subsequently documented in service charters (Indicators 13 and 14). SDU-level MSFs monitored puskesmas promises by visiting and interviewing puskesmas staff. Overall, Kinerja met 257% of its program target for Indicator 14.
Progress was also made in Kinerja’s demand-side intervention (IR 2). It saw an increase of the dissemination of information on LG responsibilities and performance (Sub-IR 2.2). These activities were conducted by local media organizations and citizen journalists managed by Kinerja’s two media intermediary organizations, PPMN and Forum Lenteng. The program supported a total of 90 active citizen journalists (225% of the program target) across all four partner districts. Additionally, through PPMN and Forum Lenteng, media products were produced (Indicator 18). Kinerja met 280% of its program target for Indicator 18. The total of 874 media products included talk shows aired by local radio stations, health features created by local TV media and print media outlets, and articles written by citizen journalists.
Kinerja also supported media outlets as a way to disseminate information, as tracked in Indicator 16. Local media organizations (including radio stations, print media outlets, and TV stations) produced Kinerja-related media products. Overall, Kinerja met 121% of its program target. Additionally, 20 linkages were formed during the program (Indicator 11) that were active in service delivery oversight, including 16 MSFs (Indicator 12). Both these indicators achieved 100% of the program target.
Apart from supply and demand interventions, the program also aimed to have Kinerja-supported good practices replicated in other puskesmas within partner districts (IR 3). A total of 30 Kinerja-supported practices for health management systems were institutionalized by 17 non-partner puskesmas (Indicators 19 and 20, respectively). Overall, Kinerja met 250% of its program target for Indicator 19 and 142% of Indicator 20.

70
October 2015 – December 2016
Kinerja’s M&E grantee for the Papua cost extension, Solidaritas, developed a new M&E plan for health and education for the 18-month period. The plan was significantly different in terms of its approach and indicators compared to the program’s M&E plan for the first three years due to the widened focus. Solidaritas and Kinerja’s M&E team utilized stories of change to assess and describe changes at the outcome level, as well as key performance indicators to monitor progress and achievements from project implementation. An evaluation of the Women’s Leadership Training (WLT) program was also conducted.
The main aim of Solidaritas’ approach was to produce information for: (1) program management and learning, and (2) the program’s accountability to stakeholders, especially USAID.
The M&E plan incorporated five aspects of performance monitoring:
1. Work plan monitoring integrated with program management
2. Collecting immediate feedback on the delivery of Kinerja’s support and technical assistance
3. Internal reflection on implementation challenges and learning
4. Performance monitoring through tracking performance indicators
5. Regularly compiling and verifying indications of outcome-level changes, including as a basis for the production and compilation of stories of change
This section presents key findings and achievements of Kinerja Papua during the cost extension.
Stories of Change Kinerja compiled stories of change in order to describe changes occurring at the outcome level. Initial indications of change were collected from field staff, and then discussed with staff at the national level to confirm that they were within Kinerja Papua’s sphere of influence. A researcher then investigated further to collect more complete information from the change makers in the field.
The six stories of changes are:
1. Meninggalkan Copy-paste Menuju Solusi (Leaving Behind Copy/Paste to Find a Solution) —integrated planning between puskesmas and the DHO with active community engagement in Jayapura
2. Masyarakat sebagai Subyek Pelayanan Kesehatan (Community Members as Subjects of Health Care) active community engagement (MSF Waniambey) in overseeing the quality of health services in Kota Jayapura;
3. Bersama-sama Menguatkan Pondasi Pendidikan di Amai (Collaborating to Strengthen the Foundations of Education at Amai)—active community engagement in improving the quality of education services at Amai Elementary School, Jayapura
4. Masyarakat Musatfak Mengawal Perbaikan Layanan (Leading the Charge for Improved Public Services)—active participation of the local community (MSF) to improve puskesmas services at Puskesmas Musatfak, Jayawijaya
5. Melek Media Cara Yoikatra (Media Literacy, the Yoikatra Way)—the Yoikatra filmmaking collective and their media literacy program leading to more active participation by civil society stakeholders in overseeing and advocating for good-quality health services in Mimika

71
6. “Iya Suster, Saya Mau Cerita…” (“Yes, Sister, I Would Like to Talk…”)—improvements in the quality of puskesmas services to address GBV at Puskesmas Timika Kota, Mimika
These stories of change reflect changes in attitude and/or behavior among DHO/DEO officials and service providers, as well as changes in community participation in conducting service oversight and policy advocacy, resulting in improved governance in basic service delivery.
The story of the Jayapura DHO integrating puskesmas activity plans into its annual work plan (Story 1) features aspects of horizontal accountability between puskesmas and the DHO. It highlights the changes in attitudes towards greater acceptance of MSF participation in puskesmas planning processes. By holding a public consultation, transparency is also promoted through this new process. Similar changes related to government acceptance of community engagement is also highlighted in the story of MSF Waniambey in Kota Jayapura (Story 2), where the DHO invited members of the MSF to participate in the district ITAT’s supervisory visits to puskesmas. Public service providers have also become more responsive to community needs, as shown in two stories of change on strengthening supply-side systems (Stories1 and 6). The first of these shows how Puskesmas Depapre in Jayapura ensures that village and community needs are addressed through its annual planning, and the second shows how Puskesmas Timika Kota in Mimika adjusted its work flow and service provision mechanisms to better cater to the needs of survivors of GBV.
Four of the stories, which showcase changes in community participation in advocacy and oversight, illustrate Kinerja’s success in promoting substantive community participation and social accountability (facility-based citizen oversight, advocacy, and community mobilization) through its support of MSF activities to improve health and education services. The MSF at Puskesmas Musatfak (Story 4) shows strong facility-based citizen oversight at the puskesmas level, in particular by monitoring the availability of healthcare services for the local community when the leadership of the puskesmas and the stewardship of the DHO are weak. The MSF in Musatfak also highlights improved community engagement in advocating for better health programs at the puskesmas (such as the availability of a safe delivery house in the subdistrict). Meanwhile, MSF Waniambey’s work in Kota Jayapura shows that the community can also be engaged in oversight at the district level, through its involvement in the DHO’s ITAT (Story 2), with funding for its involvement coming from the LG’s 2016 budget. At the same time, changes related to community mobilization by fostering discussions between school stakeholders and village authorities (Story 3) resulted in a number of village administrations allocating funds from the village budgets for infrastructural needs. Linking school stakeholders and community members, while endorsing honest and transparent relationships, had a positive effect on the mobilization of resources to support education service delivery at the village level. Story 5, about the Yoikatra Community, highlighted how Kinerja Papua promoted critical awareness among community groups and built their capacity in using media to raise public-service issues. Yoikatra has been particularly successful in utilizing media, specifically documentary films, to highlight and provide critical insight into local health-sector problems.
Overall, the stories of change documented by Kinerja Papua show how public services in Papua can be improved through community empowerment and SDU-directed governance approaches.
WLT Evaluation During the cost extension, Kinerja implemented a WLT program, which consisted of a series of training and mentoring sessions (19 capacity-building activities) for women members of health MSFs from Kinerja’s four partner districts. A limited evaluation was conducted in January 2017 to provide feedback in order to improve future WLT programs, as well as to document key changes (or the potential for future changes) resulting from the training. The main question this evaluation

72
intended to answer was: How effective was the WLT in supporting and encouraging leadership and activism among the women who participated?
Overall, the evaluation team considered the WLT to have been highly effective in increasing participants’ awareness, knowledge, and skills related to gender, analysis, and advocacy. The WLT was also effective in providing participants with the necessary motivation and inspiration to address various gender-related inequities in Papua. In terms of behavioral change, the WLT was considered limited in its effectiveness in encouraging participants to conduct advocacy related to gender-sensitive health services. However, the training was considered highly effective in enabling and encouraging participants to take more “organic” action that demonstrated one or more aspects of increased leadership capacity within their own particular environments.
The evaluation found that participation in the WLT enabled and encouraged participants to apply their new awareness, knowledge, and skills in their respective contexts.
Key to understanding these changes in participants’ behavior (including their advocacy behavior) was the authorizing environment for that behavior—the extent to which factors within the participants’ environments allowed or encouraged specific behaviors. In most cases, motivation, knowledge, skills, and incentives were not limiting factors for their behavioral change. The women were generally well motivated and have since applied their new knowledge and skills to undertake activities that are in line with the opportunities available in their everyday lives. However, many participants either do not possess such opportunities, face significant constraints in undertaking advocacy activities, or live in an environment that actively discourages or prevents them from becoming involved in pushing for change.
Another key factor in the participants’ behavioral change was the effectiveness of the WLT to “open their eyes” and enable them to see their own contexts differently. In many cases, this was primarily a critical consciousness that there was “something wrong” with “the way things are happening.” Additionally, a handful of participants—particularly those from more conducive environments—described how their participation in the WLT helped them to become more aware of the “great many ways” to promote gender equality.
In general, the evaluation team considered that it was too early to observe specific, meaningful changes resulting from the actions of WLT participants. Nonetheless, there did appear to be possibilities that “organic” behavior could contribute to larger changes across a number of domains, including domestic-level changes within the women’s families, social change in their villages, the resolution of inter-group conflict, and allocations of village and LG funding.
MSF Study Kinerja conducted a study to determine the changes that had taken place within both health and education MSFs. The study used a qualitative approach and aimed to assess the changes within the program’s 16 health MSFs at the district and puskesmas level, 30 school committees, and two district education councils. For the health MSFs, the study was conducted in November 2016, while for education, the baseline was conducted in January 201655 and the endline in January 2017.
There were limitations in the education assessment due to the fact that different researchers conducted the baseline and endline assessments, which possibly affected the interpretation and
55 As previously mentioned in the Education chapter, Kinerja and the Kota Jayapura DEO selected three additional schools in the district after the results of the baseline study were known. As a result, a similar baseline study of these three schools was conducted in April 2016.

73
analysis of qualitative data. In addition, there was a delay in baseline data collection at the three schools in Kota Jayapura.
Three dimensions were used to explore the changes of health MSFs and school committees: (1) functionality (legal status, membership, internal commitment, and communication); (2) engagement/participation (relationship with SDU/DHO/DEO in the areas of complaint handling and planning, and other external stakeholders related to advocacy); and (3) sustainability. The study found that most of the health MSFs, at both district and puskesmas level, were functioning and engaged in oversight and advocacy with SDUs or DHOs. MSF sustainability varied, with many still focusing on mobilizing resources. The four health MSFs in Mimika showed the least degree of change, both in terms of functionality and sustainability.
The study of school committees and district education councils also showed significant changes in functionality and engagement. School committees were revitalized and renewed legal status achieved. Committees at schools in Kota Jayapura and Jayawijaya showed significant changes in the dimension of functionality. All 30 school committees implemented complaint surveys and put forward technical recommendations, but due to time constraints, none had begun to monitor service charter implementation, and only one school committee was actively engaged in school planning. At the same time, it is important to note that the district education councils in Jayapura and Kota Jayapura monitored technical recommendations, but there was limited engagement in policy monitoring and advocacy. There were no observable significant changes in the dimension of sustainability.
The significant differences found between health and education MSFs in functionality, engagement, and sustainability can be attributed to the period of Kinerja’s technical assistance. Health MSFs were assisted over four years, while school committees and district education councils were only assisted for 15 months.
SBM Study The SBM study aimed to assess changes at Kinerja’s 30 partner schools following the implementation of program’s SBM package over 15 months. The endline study, which was conducted in January 2017, used a qualitative method, focusing on using rubrics to assess each school’s performance against the baseline study, which was conducted at 27 schools in January 2016, and the three additional schools in Kota Jayapura in April 2016. Limitations of this approach included the fact that different researchers conducted the baseline and endline assessments, which possibly affected the interpretation and analysis of qualitative data; plus baseline data collection at three schools (in Kota Jayapura) was conducted after the intervention had begun.
The study looked at three dimensions: (1) the availability (and quality) of schools’ annual planning/budgeting; (2) annual reporting; and (3) the availability of complaint-handling mechanisms at the schools. The study found significant changes in the two dimensions of annual planning/budgeting and complaint handling. All of Kinerja Papua’s partner schools had school work plan and budget documents (RKAS) in place, although most were prepared with very limited engagement of their respective school committees. In developing their RKAS, the schools considered the results of their School Self-Evaluations (EDS) and MSS, and to a lesser extent the results of complaint surveys. Several schools in Jayapura and Kota Jayapura also demonstrated improved transparency and accountability by publishing their work plans and budgets. In the dimension of complaint-handling mechanisms, all 30 schools conducted complaint surveys and produced post-survey service charters. Two schools also incorporated their service charter promises into their school planning documents to accelerate their fulfillment. At the time of the endline study, none of the schools had formal complaint-handling mechanisms in place.

74
Performance Indicators In line with Kinerja Papua’s Results Framework for the cost extension, performance monitoring showed that the program delivered achievements towards its three intended outcomes: (1) strengthening the enabling environment; (2) strengthening supply-side governance; and (3) achieving substantial civil society engagement.
Kinerja achieved its targets for 10 out of 13 indicators, with one of the remaining three indicators being achieved for the education sector only (Table 7).
Table 7: Kinerja Papua Indicator Achievements (October 2015–December 2016)
NO. INDICATOR NAME SECTOR PROGRAM TARGET
PROGRAM ACHIEVEMENT
1 Governing Justly and Democratically (GJD) 2.2.3-5 Number of subnational entities receiving US Government assistance that improve their performance
All 5 5 (100%)
2 GJD 2.2.3-4 Number of local nongovernmental and public sector associations supported with US Government assistance
All 5 6 (120%)
3 GJD 2.4-6 Number of US Government-supported activities designed to promote or strengthen the civic participation of women
Health 7 15 (214%)
4 Number of policies produced by local government related to Kinerja Papua support and approaches
Health 10 21 (210%)
Education 3 11 (367%)
5 Number of Kinerja good practices and innovations documented
Health 6 5 (83%)
Education 10 9 (90%)
6 Number of local governments incorporating minimum service standards (MSS) costing in their annual planning documents
Health 2 2 (100%)
Education 3 3 (100%)
7 Number of local governments incorporating MSS costing in their annual budgeting documents
Health 2 2 (100%)
8 Number of local government officials trained on management and supervision of public service delivery
District Health 30 44 (147%)
District Education
28 54 (193%)
Provincial Health
10 11 (110%)
Provincial Education
10 20 (200%)
Other 4 12 (300%)
9 Number of integrated oversight and capacity building/technical assistance held by district health and education office Integrated Technical Assistance Teams to Service Delivery Unit managers
Health 27 16 (59%)
Education 36 50 (139%)

75
NO. INDICATOR NAME SECTOR PROGRAM TARGET
PROGRAM ACHIEVEMENT
10 USAID/Indonesia PMP 1.2-1: Number of civil society organizations receiving US Government assistance engaged in advocacy interventions
All 10 9 (90%)
11 Number of policy recommendations produced by multi-stakeholder forums
Health 7 24 (343%)
Education 13 29 (223%)
12 Number of civil society representatives trained around oversight and policy advocacy
Health 26 35 (135%)
Education 81 96 (119%)
13 Number of local stakeholders using media products (and media channels) in their efforts to improve the quality of public service delivery
Media 23 95 (413%)
All five partner governments (4 district LGs and 1 province) receiving US Government assistance continued to improve their performance (Indicator 1, GJD 2.2.3-5). The improvements were tracked through the issuance of new policies at both the district and provincial level, which were related to the approaches introduced by Kinerja Papua. The target was achieved. For GJD 2.2.3-4 (Indicator 2), six local NGOs were supported with USG assistance. Kinerja met 120% of the target for this indicator.
As Kinerja promoted gender integration into its governance interventions, the WLT program consisted of 19 US Government-supported activities (series of trainings and follow-up mentoring) designed to promote or strengthen the civic participation of women (Indicator 3, GJD 2.4-6). The program achieved 271% of this target.
Kinerja Papua continued to promote the development of local policies by LGs related to Kinerja’s interventions (Indicator 4). During the cost extension, health-sector partners issued 18 new policies across all four districts. In the education sector, 11 new policies were introduced by Kinerja’s three target districts and the provincial government. The policies addressed a range of issues, including fostering community participation to improve health and education services; the replication of Kinerja’s good practices; fit and proper tests to select puskesmas heads in Jayawijaya; and a regional action plan to combat violence against women and children in Kota Jayapura. Both targets under this indicator (one for health and one for education) were overachieved, at 210% and 367%, respectively.56
Kinerja successfully documented 10 good practices based on its interventions in the health sector and 9 good practices in the education sector (Indicator 5). In so doing, the program met 167% of the target for health, but only 90% for education, due primarily to the program’s limited implementation time frame for SBM. Nevertheless, considering the constraints on Kinerja’s education staff, the production of 9 good practices was a tremendous achievement.
By December 2016, all three of Kinerja’s partner DEOs, and DHOs in Jayapura and Kota Jayapura, integrated the results of MSS costing into their respective annual work plans for 2017. This ensured that Kinerja achieved 100% of its targets for Indicator 6, in both the health and 56 The overachievement in health was due primarily to the success of long-term advocacy efforts conducted by Kinerja’s partners during the course of the program. In education, meanwhile, there was higher-than-expected buy-in for Kinerja’s SBM program from LGs and school stakeholders.

76
education sectors. In the health sector, in addition to promoting the integration of MSS costing into annual work plans, Kinerja also promoted the integration of the costing results into annual budgets. In December 2016, both of Kinerja’s target DHOs (in Jayapura and Kota Jayapura) for Indicator 7 issued their 2017 budgets, with MSS costing incorporated in them.
Building the capacity of LG officials to improve the management and supervision of service delivery was a central tenet of Kinerja’s work with supply-side stakeholders. During the cost extension, Kinerja conducted a series of trainings on PSD management and supervision for partners at both district and provincial levels. A total of 141 service providers (86 men and 53 women) were considered to have fulfilled the criteria of “trained” participants (Indicator 8).
As a follow-up to these trainings, Kinerja supported district ITATs to conduct integrated monitoring and supervisory visits to SDUs (Indicator 9). In education, the DEO ITATs in all three of Kinerja’s target districts conducted a total of 51 visits to the program’s 30 partner schools, resulting in Kinerja meeting 142% of the education-sector target for this indicator. In the health sector, DHO ITATs conducted 16 similar visits to puskesmas in Jayapura, Jayawijaya, and Kota Jayapura, leaving the target for this indicator underachieved at 59%. This was due to several challenges, including limited DHO budget funds to cover the costs of the visits, and the longer-than-expected time taken to produce technical guidelines and monitoring checklists for use during the visits.
Five CSOs (YHI, YAPEDA, PPMN, IPPM, and CIRCLE Indonesia) and four district-level health MSFs supported by Kinerja engaged in advocacy (Indicator 10). The program’s target for Indicator 10 was 10 organizations; therefore, this indicator remained underachieved at 90%. The initial target included Kinerja's plan to support Papua’s Alliance of Independent Journalists; however, this did not materialize due to the Alliance not being receptive to Kinerja’s proposal.
The central tenet of Kinerja’s social accountability model was to support and strengthen MSFs to enable them to engage in advocacy and produce policy recommendations (Indicator 11). In the cost extension period, MSFs produced a total of 24 technical recommendations pertaining to health-sector issues and submitted them to policy makers in all four partner districts. In education, by way of follow-up to the implementation of complaint surveys at Kinerja’s partner schools, 29 technical recommendations were produced and submitted to DEO policy makers. Kinerja surpassed both its health- and education-sector targets under Indicator 11, at 343% and 223%, respectively.
Kinerja also trained civil society representatives around oversight and policy advocacy (Indicator 12). Both of the indicator’s targets, for health and education, were overachieved, with 35 health stakeholders assessed as “trained” (135%) and 95 stakeholders in education (119%).
Kinerja also saw improved use of media products and channels (radio and TV talk shows, TV and printed features) among local stakeholders in their efforts to improve the quality of public services (Indicator 12). Kinerja met 413% of this indicator’s target.

77
[REDACTED]
Kinerja staff learned many valuable lessons during the program’s lifetime. Kinerja hopes these lessons and recommendations—which cover three main areas: program design, program management, and program content and implementation—will be taken into account when designing similar programs in the future.
Program Design 1. Governance programs would have a greater likelihood of increased impact if implemented over a longer period of time. Kinerja Papua’s timeframe was too short for such an innovative program, particularly in terms of its ability to support sustainability of improvements made and encourage replication. This was especially the case with regard to the SBM intervention during the cost extension period, for which there was insufficient time to provide the optimal level of assistance and monitoring, primarily due to the lower starting point encountered in Papua (for example, lack of functioning school committees, lack of understanding of MSS). The Papuan provincial government and Kinerja’s LG partners made it clear that they wished to have more support over a longer period of time; it should be noted that this was not for financial reasons but rather for technical support and oversight. This should be considered for future programs.
2. Program timelines should align with LG funding cycles. When program timelines, such as the Kinerja cost extension period, do not align with LG funding cycles, it is difficult to quickly and sufficiently incorporate interventions into government plans and budgets. This led to a reduced sense of ownership among LG partners, as well as a lack of certainty among SDUs and MSFs as to whether support would continue in the future. During the cost extension phase, for example, Kinerja was able to push LGs to allocate budgets for the 2017 financial year but was neither able to ensure allocations nor support LGs in implementation (as the program completed its field activities in November 2016).
3. Gender must be systematically incorporated into both program design and implementation. Kinerja did not develop a Gender Mainstreaming Strategy until 2013 following new recommendations by USAID. This meant that gender was initially overlooked and not incorporated into activities, primarily due to a lack of understanding and knowledge of gender and gender mainstreaming among Kinerja’s technical and field staff. While the main focus of Kinerja’s gender work in Papua was on GBV, Kinerja incorporated additional gender elements during the cost extension phase, with the development and implementation of the WLT and the incorporation of gender sensitivity into trainings for partners and community members. Nonetheless, gender could have been better incorporated from the beginning of Kinerja’s work in Papua and not viewed as an “add on,” and staff should be sufficiently trained on gender in order to fully integrate gender into all program elements.
Lessons Learned and Recommendations
Particpiants in the Women’s Leadership Training explore the interconnected roots of social problems.

78
4. Knowledge management should be a key part of program design. Learning materials will not be well used if developed without a knowledge management strategy in place. Kinerja developed numerous learning materials and documents during its lifetime; however, many of these were not optimally shared with partners due to the lack of a clear distribution strategy. As with gender, Kinerja dealt with this issue better during the cost extension phase, but improvements could still have been made through clearer communication between technical, field, and knowledge management staff with regards to the needs of partners.
5. Improved stakeholder mapping prior to program implementation would enable better identification of potential partners. More in-depth stakeholder mapping would ensure that programs accurately assessed partners’ capacities prior to program implementation and would reduce the likelihood of working with inappropriate partners. Both formal and informal bodies and leaders should be included in stakeholder mapping; for example in Papua, both the Traditional Community Body (Lembaga Masyarakat Adat), which is the official cultural representative body, and the (unelected) heads of ethnic groups should be included. Stakeholder mapping should cover gender, culture/tradition, religion, and ethnic groups, and should include the private sector. Kinerja did undertake stakeholder mapping at the beginning of the Papua program; however, the mapping was not deep enough to fully reveal partners’ capacity and commitment.
For example, Kinerja Papua aimed to work closely with the MRP, which is a legislative assembly composed of indigenous Papuans and equal in status to the DPRD. Kinerja expected that the MRP was capable and willing to push the DPRD to approve budgets and laws relating to public service delivery. Unfortunately, the MRP was much weaker than anticipated, both in terms of skills and commitment and in terms of members not sufficiently understanding their roles or functions. If programs wish to work with the MRP in the future, Kinerja recommends training it to better understand its role, but only if enough time and resources are available.
6. SDU and district government remain the most appropriate levels for improving governance in PSD, and a flexible approach to assistance is the best way to work with them. Kinerja’s experience in Papua has confirmed the program’s hypothesis that working at SDU and district government levels, rather than at provincial government level, has the most impact on improving governance in public health and education services. Modelling an innovation at the SDU level is key to gaining the support of LG partners, as it is easier to demonstrate that a new idea is already working well on the ground. Working with the provincial government is effective in encouraging sustainability and replication, but because services are not delivered directly by the province, limited improvements can be made in services themselves if working at this level.
Interventions must also be flexible to ensure that local needs and interests are responded to, while allowing for changes and alterations to be made as needed. Programs should also be aware of the potential benefits that can be gained by fostering relations with village and subdistrict governments, particularly with regard to increasing financial support and ensuring SDUs’ needs are integrated within local planning.
7. M&E should consist of a balance between quantitative and qualitative indicators. Kinerja’s initial M&E partner, Social Impact, focused primarily on quantitative evidence to illustrate the extent of program outcomes. This approach, however, did not provide the full picture; for example, the M&E approach only recorded the number of technical recommendations submitted by MSFs to LGs, but did not allow for the documentation of the actual results from the implementation of the recommendations. During the cost extension phase under the new M&E partner, Solidaritas, a new M&E plan was developed, incorporating qualitative elements such as capturing stories of change at the SDU and community levels. Although there remains room for improvement in Kinerja’s qualitative M&E method, the stories of change nevertheless provided important information that otherwise would have gone uncaptured about the program’s
79
achievements. For future programs, Kinerja recommends that information gathered from field staff about potential indications of change should be discussed at quarterly planning meetings to allow for input, clarification, and reflection from other staff prior to beginning documentation.
Program Management 1. Sharing program costs is an effective method of increasing ownership among government partners. From the beginning, Kinerja strongly encouraged LGs to contribute financially to all activities. However, the program initially encountered difficulties due to the lack of familiarity with the idea of sharing costs, as traditionally donors would fund the entire program themselves. Complicating this was the fact that other programs/NGOs traditionally pay LG officials to attend trainings and events. Over time, as governments came to understand the concept and appreciate the program’s benefits, they were increasingly willing to play a financial role in both implementation and replication. This led to stronger partnerships, increased feelings of ownership, and higher levels of commitment.
2. Programs should invest in intermediary organization capacity building, both prior to and during implementation. As in many of Indonesia’s remote or under-developed regions, the program discovered that CSOs in Papua have lower levels of skills and knowledge than expected. This was particularly the case for Kinerja’s supply-side CSOs (that is, those working directly with the government on technical issues); demand-side CSOs working on community empowerment, after training from Kinerja and another partner CSO, were sufficiently strong and able to carry out work as required by Kinerja. For the supply-side CSOs, additional training on technical topics should be provided during future programs’ preparation phases to ensure that they are not only able to assist the government, but will also be respected by them. Extra training could be provided over the first year of a program, mentoring during the second year, and ongoing technical support and “on-the-job” training provided as needed thereafter. Improved stakeholder mapping would also ensure that CSOs’ skills are accurately understood and that inaccurate assumptions are avoided.
Program Content and Implementation 1. Governance should be integrated into sectoral programming. Incorporating good governance into technical sectors can have a significant impact on improving service quality. However, this is difficult to achieve if the underlying technical skills remain weak—for example, if midwives’ antenatal and delivery skills are low, or if teachers’ subject knowledge is minimal. Midwives can follow service SOPs and referral procedures perfectly, but if they do not possess the skills to spot a post-partum hemorrhage, maternal mortality will remain a problem. This reflects the fact that as Kinerja was solely a governance project, sectoral impact was thus only achieved indirectly—the program was unable to build the technical skills of midwives and teachers because this lay outside of its mandate. Therefore, where improvements in health and education outcomes occurred, improvements were generally more significant in areas where technical skills were already sufficient. This indicates that encouraging good governance in PSD is a worthwhile initiative, but that technical skills should be built simultaneously alongside such efforts.
2. Service standards, including MSS, are useful in measuring public service quality and targeting improvement. When SDUs, LGs, and the community are aware of standards and are able to measure services against such standards, PSD is more likely to improve. National standards can be implemented at the SDU level through service SOPs, which are particularly relevant to the health sector, where clinical SOPs have long existed without noting administrative and managerial tasks (such as how to refer patients or manage complaints).
80
At the district levels, national standards can be implemented through MSS. Although a number of programs have worked on MSS in the past, Kinerja discovered that LGs in Papua were more receptive to incorporating MSS indicators into their work plans when a smaller number of indicators based on specific program interventions were prioritized. LGs previously felt overwhelmed to address them all simultaneously, due to limited skills and finances. By using its more concentrated approach, Kinerja achieved more significant gains in fulfilling key MSS indicators, such as antenatal care and SBM, by focusing government attention on specific issues.
3. ITATs at the provincial and local government levels can strongly support sustainability and replication. Public demand for PSD improvement is high, and government funding is available for the creation and continuation of ITATs in fields such as health and basic education. Teams such as ITATs are very much needed in under-developed areas to ensure that public services are improved, and Kinerja’s experience in Papua indicates that their existence and active assistance to LGs is potentially a strong driver in sustaining and replicating public service improvements. Kinerja recommends that future programs support their LG partners to establish similar technical assistance teams for better coordination, improved efficiency, and guaranteed follow-up after the end of the program.
4. Programs should work with all levels of government simultaneously. Kinerja’s approach to working in Papua during the cost extension phase represented a shift in focus from SDUs to local and provincial governments. This increased level of focus on district and provincial government partners led to the development of key sustainability elements such as the ITATs, implementation modules on important provincial topics such as Special Autonomy Funds, and inter-district sharing events in Papua. Such developments supported higher levels of replication and peer-to-peer learning, and improved historically weak vertical communication flows between provincial and district technical offices.
Relationships with national technical ministries, even in a decentralized environment like Indonesia, are crucial and should be viewed as such from the beginning of a program. While Kinerja developed strong working relationships with public service-related ministries such as KemenPAN-RB and LAN, its relationships with technical ministries such as MOH and MOEC were limited until the cost extension period, during which Kinerja worked more closely with ministries. This change can be attributed to two key factors: (1) Kinerja had more good practices and lessons learned that could be shared with national ministries, thanks to the program’s maturity; and (2) the development of a new mindset among national ministries under the presidency of Joko Widodo (Jokowi). Jokowi’s government places a high focus on good governance, which has led to greater transparency and openness and more willingness to co-operate, with national ministries becoming pro-active in reaching out to donors and other partners for assistance. The final FGDs with MOH and MOEC, for example, were well attended and very successful, with the ministries appearing more open to sharing, learning, and adopting proven good practices.
5. Involvement of traditional and religious leaders is critical for development in Papua. Kinerja provided training for leaders on topics such as public service oversight, MSS, and gender mainstreaming to build knowledge and increase capacity. Traditional and religious leaders were offered the chance to become members of MSFs, which many took up. This was a critical development, as the voices of traditional and religious leaders are highly respected and listened to in Papua, and can have a major impact on behavior and mindset change. The involvement of traditional and religious leaders also encourages a greater proportion of “ordinary” citizens to become MSF members themselves—if respected social leaders are active in a movement, then other citizens begin to see that a certain issue is important and worthwhile. Local processes can be particularly effective in introducing complaint-handling mechanisms; Kinerja used established concepts such as para-para pinang (sitting and talking while eating betel nut) and kantong noken (traditional Papuan woven bag) to implement complaint handling.

81
6. Complaint handling represents a simple but effective entry point for introducing governance into public service delivery. Even in communities that have little to no experience with community participation in PSD, complaint-handling mechanisms such as the complaint survey can be said to be accepted, successful, and effective—only 2 out of 30 Kinerja partner schools in Papua rejected the results of the complaint survey, for example. Community members appreciate the opportunity to become involved in public service oversight, while SDUs themselves generally begin to see the local communities as their allies in advocating to meet SDU needs. This method is successful in bringing together communities and SDUs, as well as in improving service quality, because their advocacy to district technical offices becomes stronger.

82
Note: dark blue = Kinerja Papua partner districts
Annex 1: Kinerja Papua Partner Districts

83
Organization Area of Expertise Work Locations
BaKTI BaKTI primarily focuses on supporting the adoption of good practices in PSD in underdeveloped areas of eastern Indonesia.
Kinerja provided BaKTI a grant to develop cooperation between the program and provincial and local governments for effective implementation of health system strengthening programming; and to support knowledge management efforts and the replication of good practices.
All four partner districts
CIRCLE Indonesia
Since 2006, CIRCLE has worked with approximately 50 CSOs on issues such as sustainable livelihood development, health, HIV prevention, and gender mainstreaming. In Papua, CIRCLE works in the fields of economic development and GBV prevention training, conducting baseline surveys, and strategic planning.
Kinerja provided a grant to CIRCLE to strengthen the capacity of its MSF-support intermediary organizations to enable MSFs to advocate for better health-care services related to MCH, HIV and TB.
All four partner districts
Forum Lenteng The Jakarta-based organization has experience in implementing engagement strategies, organizational capacity building and program sustainability through the involvement of local communities via the web, video, radio and other alternative media.
Kinerja provided a grant to Forum Lenteng to increase the capacity of local organizations, as well as citizen journalists, to use alternative media to improve understanding of people’s rights to health services.
All four partner districts
IPPM Established in 2005 in Jayapura, IPPM builds the capacity of local communities in Papua through socio-ecoconomic and socio-cultural programs in health, education and citizenship.
Kinerja provided a grant to IPPM to assist with the implementation of SBM – with a special focus on the revitalization and expansion of school committees.
Jayapura, Jayawijaya and Kota Jayapura
KIPRa Established in 1999, KIPRa is a Jayapura-based organization that builds the capacity of CSOs, as well as conducts policy advocacy with LGs.
Kinerja provided a grant to KIPRa to strengthen the capacity of the Papuan People’s Assembly (MRP), indigenous groups and faith-based institutions to enable them to better advocate for the provision of basic health services within the framework of Special Autonomy.
All four partner districts
KOPEL KOPEL is a national legislative oversight NGO, which focuses on improving transparency and accountability among publicly elected officials.
Kinerja’s provided a grant to KOPEL to strengthen the capacity of DPRD legislators in budgeting and monitoring health services based on service standards, and assessing LG performance. The grant also aimed to engage MSFs to engage with their local DPRD.
All four partner districts
LSPPA LSPPA was established in 1991 and focuses on strengthening the rights of women and children in Indonesia. The organization’s activities have included the dissemination of information about gender inequality through discussions, seminars and books, as well as helping women in rural areas to develop and implement income-generation strategies.
Kota Jayapura and Mimika
Annex 2: Intermediary Organizations

84
Organization Area of Expertise Work Locations
Kinerja awarded a grant to LSPPA to help strengthen district-level Integrated Services for Women and Child Victims of Violence (P2TP2A) based on public service standards.
PKMK UGM PKMK was awarded a grant to develop and implement a Performance Management and Leadership (PML) training course for managers and health workers at DHOs and puskesmas in the areas of HIV/AIDS, TB and MCH. The university center also provided mentoring as a follow-up to the PML training, to support the implementation of DHO and health center action plans.
All four partner districts
PPMN PPMN was established to improve the professionalism of the media industry in Indonesia. The organization has conducted a range of different trainings across the archipelago, from in-house training of radio station staff in remote areas to journalism training.
Under the Kinerja grant, PPMN was tasked with raising people’s awareness of their health rights and available services through media campaigns, including radio and TV broadcasts. PPMN also worked to increase public participation (including through citizen journalists) to monitor the implementation and quality of health-care services.
All four partner districts
Solidaritas Solidaritas is a social enterprise that was founded in 2013 to assist planning and implementing organizations in development to find creative solutions using accurate data and information.
Kinerja awarded a grant to Solidaritas to assist in developing an M&E plan for the Papua program’s CE, as well as supporting Kinerja’s M&E team to assess the program’s impact during its final year of programming.
All four partner districts
YAPEDA YAPEDA was established in 2003 to help combat the spread of HIV in the district of Mimika.
Kinerja provided a grant to YAPEDA to build the capacity of MSFs to monitor the quality of public health services, specifically in MCH, and to advocate for reforms where needed. A significant part of its activities under the Kinerja grant involved improving community members’ understanding of their health rights.
Mimika
YHI YHI was founded in 2001 as an outreach program to improve the welfare of the people in Papua through programs in education, economics, social welfare and health. The foundation has played an active role in HIV/AIDS prevention in high-risk regions in Jayapura. YHI has also been involved in projects that have addressed reproductive health and GBV.
Kinerja provided a grant to YHI to strengthen MSFs in Jayapura and Kota Jayapura, to enable them to advocate for policy improvements on MCH and HIV prevention. The organization was also tasked with increasing people’s awareness of their health rights, and encouraging community participation to monitor the quality of local health-care services.
Jayapura and Kota Jayapura
YKP YKP was established in 2001 to address women’s reproductive health issues and the difficulties they experience due to social inequalities, gender stereotyping and discriminatory policies.
Kinerja provided a grant to YKP to provide reproductive health education (based on the Kespro model that YKP and Kinerja implemented in Bondowoso, East Java) to adolescents in Mimika in order to address GBV. YKP’s strategy included campaigning for reproductive rights and access to reproductive health services for women, and increasing public awareness on reproductive rights and promoting gender equality.
Mimika
YUKEMDI Founded in 1995, YUKEMDI focuses on empowering rural communities in Jayawijaya. The organization is particularly active in programs to prevent and control the spread of HIV/AIDS among at-risk groups, as well as economic empowerment programs for people living with HIV or AIDS.
YUKEMDI was awarded a grant by Kinerja to build the capacity of MSFs in advocating for improvements in health-care services surrounding HIV/AIDS, TB and MCH.
Jayawijaya
85
Kinerja Papua Good Practices Sector Title
Health
Video tutorial covering five topics from Kinerja’s PML Training (PKMK UGM)
Five good practice videos produced by BaKTI: - SOPs for MCH - Integrated Services for Victims of GBV - MSS Costing Integration - Complaint-handling Mechanisms - SDU-level MSFs
Program Pendampingan Layanan Terpadu untuk Korban Kekerasan terhadap Perempuan dan Anak berbasis Standar Pelayanan Publik (Integrated Service Mentoring Program for Women and Child Victims of Violence based on Public Service Standards)
Kemitraan Dinas Kesehatan dan Forum Masyarakat untuk Pelayanan Kesehatan yang Lebih Baik di Kota Jayapura (DHO-MSF Partnerships for Improved Health Services in Kota Jayapura)
Pengelolaan Pengaduan Meningkatkan Kualitas Pelayanan Kesehatan dan Manajemen Puskesmas Abepantai (Complaint Handling to Improve the Quality of Health Services and Management at Puskesmas Abepantai)
Advokasi Peningkatan Pelayanan Kesehatan melalui Jurnalisme Warga dan Talk Show Radio di Kabupaten Jayawijaya (Advocacy via Citizen Journalism and Radio Talk Shows to Improve Health Services in Jayawijaya)
Partisipasi Masyarakat dalam Perencanaan Kegiatan Pencapaian Standar Pelayanan Minimal Kesehatan di Kabupaten Jayapura (Community Participation in Planning Activities to Achieve Minimum Service Standards in Health in Jayapura)
Penanganan Terpadu Perempuan dan Anak Korban Kekerasan dengan Melibatkan Masyarakat di Kota Jayapura (Integrated Handling of Women and Child Victims of Violence with Community Involvement in Kota Jayapura)
PTP Terpadu di Puskesmas Depapre, Kabupaten Jayapura (IPP at Puskesmas Depapre, Jayapura)
Annex 3: Learning Materials

86
Sector Title SOP Layanan untuk Manajemen Puskesmas yang Lebih Baik: Praktek Baik dari Puskesmas Dosay, Kabupaten Jayapura (Service SOPs for Improved Puskesmas Management: A Good Practice from Puskesmas Dosay, Jayapura)
Health
Peningkatan Pelayanan Kesehatan dengan Bimbingan Teknis dan Supervisi Terpadu (Improving Health Services through Integrated Technical Assistance and Supervision)
Pemilihan Kepala Puskesmas melalui Tes Kepatutan dan Kelayakan di Kabupaten Jayawijaya (Selecting Heads of Puskesmas through Fit and Proper Tests in Jayawijaya)
Replikasi MSF untuk Meningkatkan Kualitas Pelayanan Kesehatan di Kota Jayapura (MSF Replication to Improve Health Services in Kota Jayapura)
Education
Perencanaan Sekolah Partisipatif Berbasis Standar Pelayanan Minimal, Evaluasi Diri Sekolah, dan Survei Pengaduan (Participatory School Planning Based on MSS, EDS, and Complaint Surveys) Peningkatan Kualitas Pelayanan Pendidikan di Sekolah Melalui “Komite Sekolah Diperluas” (Improving the Quality of Education Services at Schools through “Expanded School Committees”) Pengendalian Perencanaan Dana Otonomi Khusus dan Reviu Usulan Rencana Definitif Bidang Pendidikan (Controlling the Planning of Special Autonomy Funding and Reviewing Education-Sector Proposed Definitive Plans) Dewan Pendidikan Berkonteks Papua (District Education Boards in a Papuan Context) Integrasi SPM dalam Rencana Kerja Dinas Pendidikan (Integrating MSS into DEO Work Plans) Peran Tim Bimbingan Teknis Pendidikan dalam Supervisi Sekolah Terkait Program MBS Berorientasi Pelayanan Publik (The Supervisory Role of Education ITATs at Schools Implementing Public Service-Oriented SBM) Jurnalis Cilik Peduli Sekolah (Youth Journalists Caring about Schools) Transparansi Perencanaan dan Anggaran Sekolah Jalan Menuju Prestasi: Pembelajaran SDN 1 Hamadi, Kota Jayapura (Transparency in School Planning and Budgeting as a Road to Achievement: Lessons Learned from SDN 1 Hamadi, Kota Jayapura) Kontribusi Dana Kampung Untuk Meningkatkan Pelayanan SDN Inpres Nafri, Kota Jayapura (Village Fund Contributions to Improve Services at SDN Inpres Nafri, Kota Jayapura)

87
Infographics No. Title
1. Kinerja program overview
2. Kinerja’s health program in Papua 3. Kinerja’s education program in Papua 4. Multi-stakeholder forums 5. Minimum Service Standards
6. Complaint-handling mechanisms
Illustrated Handbooks No. Title
1. Seri Pembelajaran Masyarakat Buku 1: Masyarakat Berhak Bersuara (Community Learning Series, Book 1: Community Members Have the Right to Have their Say)
2. Seri Pembelajaran Masyarakat Buku 2: Komite Sekolah (Community Learning Series, Book 2: School Committees)
3. Seri Pembelajaran Masyarakat Buku 3: Survei Pengaduan (Community Learning Series, Book 3: Complaint Surveys)
Stories of Change No. Title
1. “Iya, Suster, saya mau cerita...” (“Yes, Sister, I would like to talk…”)
2. Mengawal Perbaikan Layanan Kesehatan (Leading the Charge for Improved Public Services)
3. Melek Media, Cara Yoikatra (Media Literacy, the Yoikatra Way)
4. Meninggalkan Copy/Paste Menuju Solusi (Leaving Behind Copy/Paste to Find a Solution)
5. Masyarakat Sebagai Subyek Pelayanan Kesehatan (Community Members as Subjects of Health Care)
6. Bersama-sama Menguatkan Pondasi Pendidikan di Amai (Collaborating to Strengthen the Foundations of Education at Amai)

88
Policy Papers No. Title
1. Bimbingan Teknis dan Supervisi Terpadu, Indikator Penting untuk Tercapainya Pelayanan Kesehatan Prima (Integrated Technical Assistance and Supervision, As Key Indicators for the Achievement of First-Rate Health Services)
2. Perencanaan Tingkat Puskesmas Terpadu: Harmonisasi Perencanaan Kesehatan Vertikal dan Partisipatif (Integrated Puskesmas Planning: Harmonizing Vertical and Participatory Health Planning)
3. MSF/BPK sebagai Wadah Partisipasi Masyarakat untuk Peningkatan Kualitas Pelayanan Kesehatan di Daerah (MSFs/BPK as a Platform for Public Participation to Improve the Quality of Regional Health-Care Services)
4. Revitalisasi Komite Sekolah Kontekstual Lokal untuk Penguatan MBS Berpelayanan Publik (Revitalizing School Committees in Keeping with the Local Context to Strengthen Public Service-Oriented SBM)
Films
No. Title 1. Kinerja Papua Health Program 2. Health System Strengthening for MCH 3. Public Service-oriented SBM in Papua
Studies & Assessments
Research Triangle Institute No. Title
1. Provincial Control Mechanisms for Improved Performance of Papua Special Autonomy Funds: An Exploratory Study in the Health Sector (2016)
KOPEL No. Title
1. Local Health Budget Study 2009-2013 (2014)
Social Impact No. Title
1. Kinerja Papua - Organizational Capacity Assessment: Baseline Report (May 2015) 2 Assessment of USAID/Indonesia’s Kinerja Papua Program (July 2015)

89
Solidaritas No. Title
1. Multi-stakeholer Forum Sustainability Mapping Study (2017)
SurveyMETER No. Title
1. Papua Health Worker Survey: Results of a Study in Four Districts (2015)

[REDACTED]
Sampoerna Strategic Square South Tower, 18th Floor
Jl. Jend. Sudirman Kav. 45 – 46, Jakarta 12930
Email: [email protected]
USAID-Kinerja
Back cover photo by Carsten ten Brink (Creative Commons); front cover photo © USAID Indonesia.