kirby therapeutic treatment for benign prostatic hyperplasia 1841846015
TRANSCRIPT


Therapeutic Treatment for
Benign ProstaticH y p e r p l a s i a
Prelims new 13/5/05 2:37 pm Page i

Prelims new 13/5/05 2:37 pm Page ii

LONDON AND NEW YORK
Therapeutic Treatment for
Benign ProstaticH y p e r p l a s i a
Edited by
Roger S Kirby MA MD FRCS (Urol) FEBUVisiting Professor of Urology
St. George’s Hospital, London, UK
John D McConnell MDProfessor of Urology
University of Texas Southwestern Medical Center, Dallas, Texas, USA
John M Fitzpatrick MCh FRCSI FC Urol (SA) FRCSGlas FRCSConsultant Urologist and Professor of Surgery
Mater Misericordiae Hospital, and University College Dublin, Dublin, Ireland
Claus G Roehrborn MDProfessor of Urology
University of Texas Southwestern Medical Center, Dallas, Texas, USA
Michael G Wyllie BSc PhDManaging Director
Urodoc Limited, Herne Bay, UK
Peter Boyle PhDDirector
Division of Epidemiology and Biostatistics, European Institute of Oncology, Milan, Italy
Prelims new 13/5/05 2:37 pm Page iii

© 2005 Taylor & Francis, an imprint of the Taylor & Francis Group
First published in the United Kingdom in 2005by Taylor & Francis,an imprint of the Taylor & Francis Group, 2 Park Square, Milton ParkAbingdon, Oxon OX14 4RN, UK
Tel.: +44 (0) 20 7017 6000Fax.: +44 (0) 20 7017 6699Website: www.tandf.co.uk
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any formor by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior permission of thepublisher or in accordance with the provisions of the Copyright, Designs and Patents Act 1988 or under the terms of anylicence permitting limited copying issued by the Copyright Licensing Agency, 90 Tottenham Court Road, London W1P0LP.
Although every effort has been made to ensure that all owners of copyright material have been acknowledged in thispublication, we would be glad to acknowledge in subsequent reprints or editions any omissions brought to our attention.
British Library Cataloguing in Publication Data
Data available on application
Library of Congress Cataloging-in-Publication Data
Data available on application
ISBN 1-84184-601-5
Distributed in North and South America by
Taylor & Francis2000 NW Corporate BlvdBoca Raton, FL 33431, USA
Within Continental USATel.: 800 272 7737; Fax.: 800 374 3401Outside Continental USATel.: 561 994 0555; Fax.: 561 361 6018E-mail: [email protected]
Distributed in the rest of the world byThomson Publishing ServicesCheriton HouseNorth WayAndover, Hampshire SP10 5BE, UKTel.: +44 (0) 1264 332424E-mail: [email protected]
Composition by Parthenon PublishingPrinted and bound by T. G. Hostench S.A., Spain
Prelims new 13/5/05 2:37 pm Page iv

v
Contents
List of Contributors vii
1. Medical management – watchful waiting 1P Hegarty, J M Fitzpatrick, R C Bruskewitz
2. The placebo effect in the treatment of benign prostatic hyperplasia 11C G Roehrborn
3. Dutasteride in the treatment of the BPH patient 41J D McConnell, C G Roehrborn
4. Finasteride in the treatment of benign prostatic hyperplasia 53J D McConnell
5. Combination therapy in the treatment of BPH 67C G Roehrborn
6. The differential effects of adrenoceptor antagonists on prostate tissue growth 83N Kyprianou
7. Terazosin in the treatment of obstruction of the lower urinary tract 91M K Brawer, J M Fitzpatrick
8. Doxazosin in the treatment of benign prostatic hyperplasia 103R S Kirby
9. Alfuzosin 119A Jardin
10. Tamsulosin 139C R Chapple
11. Phytotherapeutic agents in the treatment of LUTS and BPH 167K Dreikorn, J M Fitzpatrick
12. Uroselectivity revisited 185K-E Andersson, M G Wyllie
Index 197
Prelims new 13/5/05 2:37 pm Page v

Prelims new 13/5/05 2:37 pm Page vi

vii
Karl-Erik AnderssonDepartment of Clinical PharmacologyLund University Hospital221 85 Lund, Sweden
Peter BoyleDirector, Division of Epidemiology and
BiostatisticsEuropean Institute of Oncologyvia Ripamonte 43520141 Milan, Italy
Michael K Brawer MDDirector of Northwest Prostate InstituteNorthwest HospitalSeattle, WA 98133, USA
Reginald C Bruskewitz MDProfessor of Surgery, Department of SurgeryDivision of UrologyClinical Science Center600 Highland AvenueMadison, WI 53792, USA
Christopher R Chapple MD FRCS(Urol) FEBUConsultant Urological SurgeonDepartment of UrologyRoyal Hallamshire HospitalGlossop RoadSheffield S10 2JF, UK
Kurt DreikornUrology ClinicSt. Jurgen Str.28205 Bremen, Germany
John M Fitzpatrick MCh FRCSI FC Urol (SA)FRCSGlas FRCS
Consultant Urologist and Professor of SurgeryMater Misericordiae Hospital and University
College Dublin47 Eccles StreetDublin 7, Ireland
Paul HegartyUniversity College HospitalGalway, Ireland
Alain Jardin MDChef du Service D’UrologieUniversité Paris SudCentre Hospitalier de BicêtreSecteur P. Broca78 rue Général Leclerc94275 Le Kremlin-Bicêtre, Cedex, France
Roger S Kirby MA MD FRCS (Urol) FEBUProfessor of Urology145 Harley StreetLondon W1G 6BJ, UK
List of Contributors
Prelims new 13/5/05 2:37 pm Page vii

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIAviii
Natasha Kyprianou MD PhDProfessor, Division of UrologyDepartment of SurgeryUniversity of Kentucky Medical Center800 Rose StreetLexington, KY 40536, USA
John D McConnell MDProfessor of Urology, Department of UrologyUniversity of Texas Southwestern Medical Center5323 Harry Hines Boulevard, B11.300Dallas, TX 75390-9131, USA
Claus G Roehrborn MDProfessor and Chairman, Department of UrologyThe University of Texas Southwestern Medical
Center5323 Harry Hines Boulevard, J8.142Dallas, TX 75390-9110, USA
Michael G Wyllie BSc, PhDManaging DirectorUrodoc LimitedHerne Bay, UK
Prelims new 13/5/05 2:37 pm Page viii

Medical management – watchful waitingP Hegarty J M Fitzpatrick R C Bruskewitz
1
1
INTRODUCTION
The spectrum of treatment options for benignprostatic hyperplasia (BPH) is matched by thespectrum of disease severity. New medicationsand minimally invasive modalities offer a greaterrange of choices to the urologist and the patient.This does not make treatment planning anyeasier. Despite these innovations the naturalhistory of the condition with or withoutintervention is still unclear and can only beinferred from a number of studies. As BPH israrely life-threatening, management is focused onquality of life. Provided it is safe to avoid surgery,watchful waiting (WW) can be offered to patientswho are not bothered much by their symptoms.
WW is an active process of patientmonitoring, which allows for change to medicalor surgical intervention as required. The patientmust understand that it is not a passive processand that compliance with follow-upappointments is essential. This chapter describesWW as an active treatment option.
The natural history of BPH appears to be oneof waxing and waning. Only through knowingthe natural history of the disease can we ascribenet benefit to any treatment. While the incidenceof symptomatic BPH increases with age, it doesnot follow that the disease is not progressive inany one individual. Cohorts of untreated BPHare useful in describing the heterogeneity of thedisease. As the studies have been carried out asthe classification of the disease has evolved, it isdifficult to compare results. Much of the work to
date has compared WW to transurethralresection of the prostate (TURP), however theadvent of novel medical and minimally invasivetherapies has offered a ‘middle ground’, whichmust now be explored. Not only may thesetreatments improve symptoms, but there is alsoevidence that they may retard diseaseprogression. The rate of TURP has droppedsignificantly with the introduction of α-adrenergic antagonists and finasteride. This mayreflect the lack of strong indications for TURP inthe majority of patients, or indeed that theseagents are in some way disease modifying.Although current guidelines recommend WWfor patients with mild symptoms,1 or patientswith more severe symptoms who are notbothered by them, medical management is alsoreducing the number of patients being assigned toWW, even for mildly symptomatic BPH.2 Large,randomized, controlled prospective trials usingthe American Urological Association (AUA)symptom score, urinary flow rates, and postvoidresidual are necessary to allow valid comparisonbetween the many treatments, including WW.Based on the available evidence, the indicationsfor and logistics of WW are outlined.
BALTIMORE LONGITUDINAL STUDY OFAGING
A large epidemiological study by Arrighi et al.was published in 1991.3 A cohort of 1371volunteers was followed from 1958 with physical
Ch 01 13/5/05 2:42 pm Page 1

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA2
examination, digital rectal examination (DRE),and a self-administered questionnaire. Thosewith a history of prostate cancer or prostatectomywere excluded, leaving 1057 in the final analysis.The risk of prostatectomy increased with age. Aman aged between 50 and 59 years had a 24%probability of undergoing prostatectomy in thesubsequent 20 years. This risk increased to 39%for men over 60 years. Change in prostate size(determined on DRE) and obstructive symptomsincreased the chance of prostatectomy.
The increase in prostatectomy rates with agein this cohort may not reflect progression of thedisease as historical comparison is skewed byprevailing attitudes of practicing urologists.Transrectal ultrasonography would improve thesensitivity of measuring changes in prostate size.
PROSPECTIVE STUDY OF PATIENTS WITHVOIDING SYMPTOMS
Craigen et al. prospectively followed 251 patientswith lower urinary tract symptoms (LUTS) for4–6 years.4 Initially 39 patients had prostatecancer, 89 were in acute urinary retention, and123 had prostatism. Of these 123 patients, 6.5%developed urinary retention and 39% requiredprostate surgery. Of the 67 patients who did notrequire surgery, 48% became symptom free.There was no difference in baseline symptoms,general health or age in those who did or did notrequire surgery.
This study was limited by its nonspecificurinary symptoms and patient selection.However, it illustrates that of patients who do notrequire surgery, symptoms resolve in 48% ofcases. In a more recent study, of 50 patients withan International Prostate Symptom Score (I-PSS)score of less than 7, 81.2% were clinically stable ata mean follow-up of 17 months.5
NATURAL HISTORY OF UNTREATED‘PROSTATISM’ OVER 5 YEARS
Ball et al. described the 5-year follow-up of acohort of 107 symptomatic patients for whomsurgery was not indicated.6 Ten patients requiredsurgery in the interim, two for acute retentionand eight for worsening symptoms. Of the 97untreated, 31 were subjectively improved, 50unchanged, and 16 felt worse. This studyincluded detailed urodynamic testing. Theannual decrease in maximal flow rates of 1.2 ml/swas the same as that due to aging in the generalpopulation. Voiding pressure could safely remainabove 70 cmH2O, though it tended to fall over the5-year period. On average, the ten patients whorequired surgery had lower initial flow rates andincreased prostatic length of profilometry. All tenwere classified as obstructed on pressure–flowstudies. On review of the initial assessmentparameters, it was not possible to predict thosewho would subsequently require surgery. Thesimplest and least invasive test, the urinary flowrate, was as good a screening parameter as anyother. This study demonstrated the safety of WWover a 5-year period.
In an examination of the urodynamics ofpatients with bladder outlet obstruction (BOO)who underwent WW, it was possible to predictfailure rate on the basis of obstruction grade,however.7 Treatment failure was defined aspatients who did not wish to continue WW.Pressure–flow studies were conducted at baselineand again after 1 and 4 years. After 1 year, I-PSShad fallen at unchanged Qmax and postvoidresidual (PVR), and this did not change at 4 years.LUTS severity and failure rate increased overtime in patients with severe BOO. The resultsindicate that prediction of failure is possible,which may allow a more precise prognosis for
Ch 01 13/5/05 2:42 pm Page 2

MEDICAL MANAGEMENT – WATCHFUL WAITING 3
individual patients who prefer WW. Theselection of patients for TURP, minimallyinvasive therapy, or WW on the basis ofpressure–flow studies has also been shown toyield good symptomatic effects in terms of Qmax,PVR, and I-PSS with less risk of complications.8
TURP WAITING LIST
Barham et al. reported in 1993 a study evaluating118 patients on a waiting list for TURP.9 Surgerywas indicated for symptoms of BPH incombination with an enlarged prostate on DRE.Patient mean age was 70 years (55–89 years), witha mean time on the waiting list of 3 years. Elevenof the original 118 patients were excluded becausethey had died, refused surgery, or had theprocedure elsewhere, 107 patients wereevaluated. Of these, 65% said symptoms wereunchanged, 12% improved, and 22%deteriorated. Twenty-nine patients (27%) werekept on the waiting list for severe symptoms anda peak flow rate of less than 6 ml/s. Theremaining 78 were re-evaluated. Of these, 51(65%) were discharged from the waiting list dueto mild symptoms, nine patients (12%) were keptunder review for mild symptoms with objectiveevidence of severe obstruction (flow rate between6 and 15 ml/s and residual volumes greater than150 ml) and 18 (23%) stayed on the waiting listdue to bothersome symptoms.
In summary, of the original 107 patientsevaluated, 47 (44%) were kept on the waiting list,nine (8%) remained under review, and 51 (48%)were discharged. This study demonstrated thefluctuations in BPH symptoms. The authorsconcluded that patients will opt to avoid surgeryif reassured of the natural history of BPH. Likeother studies, this study is limited by its definitionof symptoms and indications for surgery.
PROSPECTIVE TRIAL OF TURP VERSUSCONSERVATIVE MANAGEMENT
Kadow et al reported a randomized prospectivetrial of 38 patients with LUTS in 1988.10 Twenty-one patients were randomized to undergo TURP,and 17 WW. Patients were assessed byurodynamics and symptoms at baseline and 6months after treatment.
Of the WW group, 56% of patients wereeither symptom free or improved, compared to71% following TURP. Irritative symptomsdecreased in both groups, with 79% of the TURPgroup and 50% of the WW group demonstratingimprovement in detrusor instability onurodynamics. Peak flow increased from 8.5 to19.0 ml/s in the TURP group, with little changein the WW group (9.8–11.2 ml/s). Thisdemonstrates that, in a nonstratified group ofpatients, TURP is superior to WW in itsurodynamic outcome and that with conservativemanagement about half the patients improveover 6 months.
DEPARTMENT OF VETERANS’ AFFAIRSCOOPERATIVE STUDY
The Department of Veterans’ Affairs (DVA)Cooperative Study compared TURP with WWin 556 men with moderate symptoms of BPH.11
Symptoms were assessed using the Madsensymptom score and bother to patients wasmeasured by a qualify of life score. Exclusioncriteria were age less than 55, previous prostatesurgery, bladder or prostate cancer, residualvolume greater than 350 ml, or evidence of aneurogenic bladder; 280 patients wererandomized to TURP and 276 to WW. Medianage was 65, and there was no difference in thegroups in their findings on examination, peak
Ch 01 13/5/05 2:42 pm Page 3

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA4
flow, residual volume, serum creatinine, orurinalysis at baseline. The follow-up period was 3years. Flow rates and residual volumes weremeasured every 6 months, whereas symptomscores and quality of life scores were repeatedannually. All patients were advised aboutaggravating factors such as medication, coffee,and alcohol. Treatment failure was defined as anyof the following: death, urinary retention,residual urine more than 350 ml, development ofa bladder calculus, new-onset persistentincontinence, or a Madsen symptom score ofmore than 24, or more than 21 on two consecutivevisits.
The values at baseline and after 3 years’follow-up are listed in Table 1.1. The objectivemeasurement of flow rate improved with TURPand was unchanged in the WW group. Postvoidresidual volumes decreased to a greater extent inthe TURP group over the WW cohort. Botherwas ameliorated in both arms, however to agreater degree following TURP. General healthand sexual performance remained stable in bothgroups. The treatment failures were greater inthe WW group (17%) than in the TURP group
(8%). Successful outcome with WW was morelikely in those with high urinary flow rate, a lowpostvoid residual volume, and low bother score,whereas the only identifiable predictor of successin the TURP group was a high baseline botherscore.
This study demonstrates that TURP achievesbetter objective and subjective outcomes thanWW in patients with moderate symptoms ofBPH. However, patients with minimal bothercan be managed safely by WW, as 82% do notexperience treatment failure.
WATCHFUL WAITING VERSUS MEDICALTHERAPY
The studies discussed so far have comparedTURP to WW. A clinically more relevantquestion is the difference between medicalmanagement and WW. Direct comparison ofoutcomes of α-adrenergic blockade, finasteride,or WW showed improvement in symptoms andpeak flow rates for all three approaches.12
However the actual degree of symptom
TABLE 1.1 Baseline and 3-year follow-up values for patients in the DVA Cooperative Study.
*Changes on transurethral resection of the prostate (TURP) significantly different (p < 0.01) from changes on watchfulwaiting (WW). †Scale ranges from 0 (most impaired) to 100 (least impaired). (Adapted from ref. 4 with permission.)
WW TURP
Parameter Baseline 3-year follow-up Baseline 3-year follow-up
Peak urinary flow rate (ml/s)* 12.3 12.7 11.6 17.8
Residual urine volume (ml)* 113 72 110 51
Symptom score (points)* 14.6 9.1 14.5 4.9
Bother from urinary difficulties (points†)* 48.0 57.6 46.4 75.7
Sexual performance (points†) 38.6 35.6 40.0 36.0
General well-being (points†) 71.3 71.4 73.2 76.2
Ch 01 13/5/05 2:42 pm Page 4

MEDICAL MANAGEMENT – WATCHFUL WAITING 5
improvement was greatest for the α-blockadegroup. In the Veterans’ Affairs CooperativeStudies published by Lepor et al. in 1996, thedegree of improvement in AUA symptom scoreand peak flow rates was greatest among those onan α-adrenergic antagonist.13
In an examination of the effect of a variety ofBPH treatments on sexual function, finasteride,α-blockers, and TURP were associated withlevels of improvement and deterioration in sexualfunction similar to WW.14 Although surgicalintervention has been more closely associatedwith negative sexual effects in the past, thesefindings suggest that other factors, such as age,may be more influential.14,15
CURRENT TREATMENT PATTERNS GLOBALLY
The variation between countries on patterns oftreatment was the subject of six articles in aEuropean Urology supplement in 1999.1,16–20 Thedifferent approaches to treating patients are quitestriking. In particular, phytotherapeuticscommand 40% of the market share in France andGermany.17,18 This is despite the lack of evidenceof their efficacy over placebo.21 These papers alsodescribe the widening range of physicians caringfor men with BPH. This has occurred with theadvent of medical management and the fall-off inthe TURP rate occurring in most countries(except the UK).20 The prescribing of α-adrenergic antagonists in combination withfinasteride is still prevalent, and may increasefollowing recent positive findings regarding thecombination of doxazosin and finasteride;22
however, there is also evidence showing nobenefit over α-adrenergic antagonist alone.13 In atelephone survey of 502 American urologists, 20%said they favored medical management over WWin patients with only mild LUTS.23 Thus it is
evident that in recent years medical managementhas reduced both the TURP and WW rates.
TREATMENT PREFERENCES
The influence of urologist preference is welldescribed in a paper published in 1999 byStoevelaar et al.24 The preferences of 39 urologistswere evaluated in treating 670 consecutivepatients, in 13 Dutch hospitals. The majority ofpatients (67.8%) belonged to the gray area forwhich, according to the study guidelines,management should be based on patient choiceand urologist preference. Patients with highurinary flow rate, low residual volume, or mildirritative symptoms were more likely to undergoWW. Controling for patient characteristics, theurologist’s preference could more than double thelikelihood of surgery. The number of years’experience also influenced treatment choice, inthat younger urologists were less likely torecommend WW.
Patient preference should predominate indeciding treatment.25,26 However,27,28 since theadvent of medical and minimally invasivetherapies, this decision has become more difficult.When patients were shown an educational videoprogram, those who had previously chosen aninvasive therapy changed to a less invasiveoption.29 Based on AUA symptom scores, 35% ofpatients with severe symptoms preferred WW tomedical or surgical intervention.12 This indicatesthat factors other than disease severity areimportant in the decision-making process.
INDICATIONS
When TURP was introduced over 70 years ago,the mortality and morbidity were high.30 The
Ch 01 13/5/05 2:42 pm Page 5

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA6
procedure was reserved for life-threateningconditions such as hemorrhage, uremia andsepsis. With the gradual reduction in mortality,the indications for TURP have greatlyexpanded.31 The availability of medical andminimally invasive therapies has also alteredindications for treatment.32–36
STRONG INDICATIONS FOR TREATMENTOR WATCHFUL WAITING
The absolute indications for intervention are easyto define. Surgery is recommended for (1)refractory urinary retention, patients who have atleast one trial without catheter with or without α-adrenergic blockade, (2) recurrent urinary tractinfection caused by bacterial prostatitis, refractoryto medical treatment, (3) bladder calculi, (4) renalinsufficiency due to BOO, (5) severe hematuriafrom BPH. Other indications for TURP arerelative. There is no strong indication for WW,however a strategy of WW is recommended forpatients with mild symptoms of BPH.1
MODERATE INDICATIONS FOR TREATMENTOR WATCHFUL WAITING
Management of patients with moderatesymptoms of BPH is controversial. Such patientsneed to be informed of the current evidenceregarding the available treatments, so thatpotential side-effects can be weighed against thenatural history of the disease. Many patients,however, seek the opinion of a specialist, in whichcase it is appropriate to select the optimaltreatment. This is based on clinical findings and anumber of tests. For WW these include (1) thepatient’s bother from urinary symptoms, (2)postvoid residual volume, and (3) uroflowmetry.
Bother
Two patients with the same AUA symptom scoremight be bothered by their symptoms to differentdegrees. Bother is ameliorated to a greater extentby TURP than by WW.11 The interference by thedisease in the day-to-day activities of patients canbe measured using the BPH impact index.37
Postvoid residual
Patients with higher residual volumes fare lesswell with a WW strategy than with TURP.10
There is no strict cut-off volume at whichintervention is recommended.
Uroflowmetry
Objective evidence of obstruction is gained withuroflowmetry, with the maximal flow rate beingthe best predictor of surgical outcome.38–40
Patients with a flow rate greater than 15 ml/sdemonstrate poorer outcomes following TURPthan those with maximal flow rates less than15 ml/s.40,41
Conclusions
Low bother score, high urinary flow rates, andlow postvoid residual volumes favormanagement by WW, but the decision should notbe based on these factors alone. The indicationsfor WW versus other intervention are listed inTable 1.2.5
STRATEGY
Patients being followed in a strategy of WW mustunderstand that this is an active program. Thepatient’s symptoms and clinical course aremonitored, usually on an annual basis. More (orless) frequent review periods have yet to be
Ch 01 13/5/05 2:42 pm Page 6

MEDICAL MANAGEMENT – WATCHFUL WAITING 7
defined by research. Patients should receiveadvice with regard to aggravating factors such asdiuretic dose scheduling and coffee and alcoholconsumption. On review, the patient should beasked about his satisfaction with this approach.Symptoms should be reassessed, along withphysical examination and routine laboratorytesting (serum creatinine, urinalysis). Repeat ofuroflowmetry and residual urine measurementshould be considered. Medical or surgicaltreatment can be offered to those who deteriorateor those substantially bothered by a lack ofimprovement. The WW program can bedelivered in a shared care setting, provided thesystem is based on good information and mutualconfidence.42
CONCLUSIONS
Urologists tend to measure outcome by means ofsymptom score and urinary flow rates. This isbalanced against the side-effect profile of anytreatment. A minor risk of even a serious side-effect such as incontinence is considered
acceptable if the chance of success (as measuredby symptom score or urinary flow) is high. Fromthe patient’s aspect, the prime factor is whetherthe degree of bother is worth risking themorbidity of undergoing treatment. The risk ofharm may outweigh the anticipatedimprovement.
Guidelines recently issued by the AUArecommend that patients with mild symptoms(AUA score ≤ 7), or moderate to severe symptomswho are not significantly bothered by them, be‘treated’ with WW.
From the evidence in this chapter, it isappropriate to recommend WW for patients withmild symptoms. Patients with moderate or severesymptoms can be considered for WW, if theirsymptoms do not interfere with their activities ofdaily living. Large, prospective, randomizedcontrolled studies of WW versus medical andsurgical treatments are necessary to developclearer indications for each modality. Furtherresearch is necessary to outline precise follow-upschedules, the need for repeated renal functiontests, and how much postvoid residual isexcessive. Allowing patients with BPH to
TABLE 1.2 Indications for therapeutic intervention vs watchful waiting in BPH.
Strength of Strategy
indication Watchful waiting Therapeutic intervention
Strong Mild symptoms (AUA score ≤ 7) Recurrent urinary retention (more than a single episode)Recurrent urinary tract infectionsRecurrent gross hematuriaBladder stonesRenal insufficiency due to BPH
Moderate Moderate symptoms (AUA score ≥8 Moderate to severe symptoms (AUA score ≥8) andand ≤ 19) but not bothersome bothersome (high BPH Impact Score)(low BPH Impact Score)Higher peak urinary flow rate High post-voiding residual and low peak urinary flow rate (rate not specified) (volume and rate not specified)Low post-void urinary residual(volume not specified)
Ch 01 13/5/05 2:42 pm Page 7

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA8
participate in the decision process makes forbetter compliance and optimal care.
REFERENCES
1. de la Rosette J J, Alivizatos G, Madersbacher S etal. European Association of Urology. EAUGuidelines on benign prostatic hyperplasia (BPH).Eur Urol 2001; 40: 256–263; discussion 264
2. Bruskewitz R C. Management of symptomaticBPH in the US: who is treated and how? Eur Urol1999; 36 (Suppl 3): 7–13
3. Arrighi H M, Metler E J, Guess H A et al. Naturalhistory of benign prostatic hyperplasia and risk ofprostatectomy. Urology 1991; 38: 4–8
4. Craigen A A, Hickling J B, Saunders C R et al.Natural history of prostatic obstruction. J R CollGen Pract 1969; 18: 226–232
5. Netto N R Jr, Lima M L, Netto M R, D’Ancona CA L. Evaluation of patients with bladder outletobstruction and mild international prostatesymptom score followed up by watchful waiting.Urology 1999; 53: 314–316
6. Ball A J, Feneley R C L, Abrahams P H. Thenatural history of untreated ‘prostatism’. Br J Urol1981; 53: 613–616
7. Knutson T, Schafer W, Fall M et al. Canurodynamic assessment of outflow obstructionpredict outcome from watchful waiting?—a four-year follow-up study. Scand J Urol Nephrol 2001;35: 463–469
8. Knutson T, Pettersson S, Dahlstrand C.Pressure–flow studies for patient selection in thetreatment of symptomatic BPH—a one-yearfollow-up study. Scand J Urol Nephrol 2001; 35:470–475
9. Barham C P, Pocock R D, Jamed E D. Who needsa prostatectomy? Review of a waiting list. Br J Urol1993; 72: 314–317
10. Kadow C, Feneley R C L, Abrahms P H.Prostatectomy or conservative management in thetreatment of benign prostatic hypertrophy? Br JUrol 1988; 61: 432–434
11. Wasson J H, Reda D J, Bruskewitz R C et al.Comparison of transurethral surgery withwatchful waiting for moderate symptoms of benignprostatic hyperplasia. N Engl J Med 1995; 332:75–79
12. McConnell J D, Barry M J, Bruskewitz R C et al.Benign prostatic hyperplasia diagnosis andtreatment. Clinical practice guideline No 8AHCPR publication No 94-0582. Rockville:Agency for Health Care Policy and Research,Public Health Service, US Department of Healthand Human Services, 1994
13. Lepor H, Williford W O, Barry M L et al. Theimpact of medical therapy on bother due tosymptoms, quality of life and global outcome, andfactors predicting response. Veterans AffairsCooperative Studies Benign Prostatic HyperplasiaStudy Group. J Urol 1998; 160: 1358–1367
14. Leliefeld H H, Stoevelaar H J, McDonnell J.Sexual function before and after various treatmentsfor symptomatic benign prostatic hyperplasia. BJUInt 2002; 89: 208–213
15. Kassabian V S. Sexual function in patients treatedfor benign prostatic hyperplasia. Lancet 2003; 361:60–62
16. Speakman M J. Who should be treated and how?Evidence based medicine in symptomatic BPH.Eur Urol 1999; 36 (Suppl 3): 40–51
17. Lukacs B. Management of symptomatic BPH inFrance: who is treated and how? Eur Urol 1999; 36(Suppl 3): 14–20
18. Berges R R, Pientka L. Management ofsymptomatic BPH in Germany: who is treated andhow? Eur Urol 1999; 36 (Suppl 3): 21–27
19. Tubaro A, Montanari E. Management ofsymptomatic BPH in Italy: who is treated andhow? Eur Urol 1999; 36 (Suppl 3): 28–32
20. McNicholas T. Management of symptomatic BPHin the UK: who is treated and how? Eur Urol 1999;36 (Suppl 3): 33–39
21. Fitzpatrick J M, Lynch T H. Phytotherapeuticagents in the management of symptomatic benignprostatic hyperplasia. Urol Clin North Am 1996;22: 407–412
Ch 01 13/5/05 2:42 pm Page 8

MEDICAL MANAGEMENT – WATCHFUL WAITING 9
22. McConnell J D and the MTOPS SteeringCommittee. The impact of medical therapy on theclinical progression of BPH: results of the MTOPStrial. J Urol 2002; 167 (Suppl 4): abstract 1042(updated)
23. Gee W F, Holgrewe H L, Albertsen P C et al. 1997American Urological Association Gallup Survey:changes in diagnosis and management of prostatecancer and benign prostatic hyperplasia, and otherpractice trends from 1994–1997. J Urol 1998; 160:1804–1807
24. Stoevelaar H J, Van De Beek C, Casparie A F et al.Treatment choice for benign prostatic hyperplasia:a matter of urologist preference? J Urol 1999; 161:133–138
25. Barry M J, Mulley A G Jr, Fowler F J et al.Watchful waiting vs immediate transurethralresection for symptomatic prostatism: theimportance of patient preferences. J Am Med Assoc1988; 259: 3010–3017
26. Kaplan S A, Golubluff E T, Olsson C A et al. Effectof demographic factors, urinary peak flow rates,and Boyarsky symptom scores on patient treatmentchoice in benign prostatic hyperplasia. Urology1995; 45: 398–405
27. Speakman M J. Initial choices and final outcomesin lower urinary tract symptoms. Eur Urol 2001; 40(Suppl 4): 21–30
28. Teillac P. Benign prostatic hyperplasia: patients’perception of medical treatment and theirexpectations. Results of a French survey involvingpatients treated with finasteride [in French].Therapie 2002; 57: 473–483
29. Kasper J F, Mulley A G Jr, Wennberg J E.Developing shared decision-making programs toimprove the quality of health care. Qual Rev Bull1992; 18: 183–190
30. Perrin P, Barnes R, Hedley H et al. Forty years oftransurethral resections. J Urol 1976; 16: 757–758
31. Mebust W K, Holtgrewe H L, Cockett A T K et al.Immediate and postoperative complications. A
cooperative study of 13 participating institutionsevaluating 3,885 patients. J Urol 1989; 141: 243–247
32. Fitzpatrick J M. Current management and futuretrends in benign prostatic hyperplasia (BPH). IrMed J 1997; 90: 256–258
33. Debruyne F M, Witjes W P, Fitzpatrick J M et al.The international terazosin trial: a multicentrestudy of the long-term efficacy and safety ofterazosin in the treatment of benign prostatichyperplasia. The ITT group. Eur Urol 1996; 30:369–376
34. Fitzpatrick J M. Alternative instrumentaltreatments in BPH. Introduction. Eur Urol 1999;35: 117–118
35. Hegarty N J, Fitzpatrick J M. High intensityfocused ultrasound in benign prostatic hyperplasia.Eur J Ultrasound 1999; 9: 55–60
36. Ramon J, Lynch T H, Eardley I et al. Transurethralablation of the prostate for the treatment of benignprostatic hyperplasia: a collaborative multicentrestudy. Br J Urol 1997; 80: 128–134
37. Barry M J, Fowler F J, O’Leary M P et al.Measuring disease-specific health status in menwith benign prostatic hyperplasia. Med Care 1995;33: AS145–AS155
38. Jensen K M E, Bruskewitz R C, Iversen P et al.Spontaneous uroflowmetry in prostatism. Urology1984; 24: 403–409
39. Jensen K M E, Jorgensen J B, Morgensen P.Urodynamics in prostatism I. Prognostic value ofuroflowmetry. Scand J Urol Nephrol 1988; 22:109–117
40. Abrahms P H. Prostatism and prostatectomy: thevalue of urine flow rate measurement in thepreoperative assessment for operation. J Urol 1977;117: 70–71
Ch 01 13/5/05 2:42 pm Page 9

Ch 01 13/5/05 2:42 pm Page 10

The placebo effect in the treatment ofbenign prostatic hyperplasia
C G Roehrborn2
11
‘The principal quality of a physician, as wellas of a poet (for Apollo is the God of physicsand poetry), is that of fine lying, or flatteringthe patient ... And it is doubtless as well forthe patient to be cured by the working of hisimagination, or a reliance upon the promiseof his doctor, as by repeated doses of physics.’1
‘Is it ethical to use a placebo? The answer tothis question will depend, I suggest, uponwhether there is already available an ortho-dox treatment of proven or accepted value. Ifthere is such an orthodox treatment the ques-tion will hardly arise, for the doctor will wishto know whether a new treatment is more, orless, effective than the old, not that it is moreeffective than nothing.’2
PLACEBO AND PLACEBO EFFECT:DEFINITIONS AND THEORETICALCONSIDERATIONS
It has long been recognized by practicing physi-cians that procedures that offer patients reassur-ance or the expectation of help may lead tomarked improvement in their clinical status,3 andmany doctors believe that placebo interventionhas an ethically acceptable place in clinical prac-tice.4 The Latin-derived term ‘placebo’ originallyappears in the Bible (placebo domino in regionevivorum, Psalm 116, Verse 9), where it may be lit-erally translated as ‘I shall please’. This originalmeaning of please is still found in the first med-ical definition of the term in Hooper’s medical
dictionary in the early nineteenth century: ‘quali-ty ascribed to any drug prescribed to please thepatient rather than being useful’. The first articlededicated to the placebo effect did not appearuntil 1945: ‘A note on placebo’ by Pepper.5 Thepotency of belief and expectation in affectinghealth is also underscored by such dramaticharmful effects as voodoo death, which in con-trast can be referred to as a ‘nocebo’ (‘I shallharm’) effect.6
In clinical context, placebo has come to denotea deceptive practice, a view that originates fromthe practice of singing vespers for pay. This nega-tive connotation of placebo has come to dominatecontemporary thinking due to the emergence ofdouble-blind, placebo-controlled drug studies, inwhich the differentiation of effects due to thepharmacologic action of a compound from otherunspecified effects is a primary consideration.Placebo effects are so omnipresent that if they arenot controlled for in therapeutic studies, the find-ings are considered unreliable. Conditions inwhich placebo effects have been described includecough, mood changes, angina pectoris, headache,anxiety, hypertension, asthma, depression,lymphosarcoma, gastric motility, dermatitis, andpain from a variety of sources.7
A prevalent view of placebo is that its use ismandatory in clinical trials, but unethical in clin-ical practice, a view that may be challenged onboth accounts.7
One of the most influential writers in the fieldof placebo research is Arthur K. Shapiro whooffers the following definition:
Ch 02 13/5/05 2:45 pm Page 11

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA12
‘A placebo is defined as any therapy or com-ponent of therapy that is deliberately used forits nonspecific, psychological, or psychophys-iological effect, or that is used for its pre-sumed specific effect, but is without specificactivity for the conditions being treated. Aplacebo effect is defined as the psychologicalor psychophysiological effect produced byplacebos.’8
Others have suggested definitions differentfrom the one quoted above,9 or further deliberat-ed on Shapiro’s theory. Grünbaum developed adiagram to illustrate his definition of placebo(Figure 2.1).10 If a therapeutic theory recom-mends a therapy ‘t’ for a condition, this treatmentusually consists of a spectrum of factors, namelycharacteristic factors ‘F’ and incidental treatmentfactors ‘C’. These incidental treatment factorsmay be known or unknown. The patient’s lifeactivities and functions are subdivided into twoparts: the target disorder ‘D’, e.g. BPH, and otheraspects of the patient’s life functions or health.The arrows in Figure 2.1 illustrate the possiblecausations (effects). The characteristic factors ‘F’may have a positive or a negative effect on thetarget disorder (or it may have no effect whatso-ever). Similarly, the factors ‘F’ may have similarinfluences, good or bad, on other aspects of the
patient’s life, which are known as side-effects.The incidental treatment factors ‘C’ may haveside-effects, but they may also affect the targetdisorder, in which case it is referred to as a place-bo effect.
For example, let the target disorder be BPHand the therapeutic theory the administration ofα-blocking drugs by a physician who evaluatesthe patient at regular intervals. The relaxation ofthe smooth muscle in the bladder neck andprostate positively affects the symptoms of BPH(nonplacebo effect), but it also causes side-effects,namely a lowering of the blood pressure (positive)and asthenia (negative). An incidental treatmentfactor is the dispensation of the drug by the physi-cian. If he expresses his confidence in the medica-tion it may result in a positive placebo effect, if heis neutral or makes a comment like: ‘We mighttry this for a while before we have to do some-thing more serious’, it may result in a negativeplacebo effect. Obviously, the frequent visits tothe physician’s office have an impact on thepatient’s life functions as well by forcing him tomake time for the visits, etc. (negative side-effectof incidental treatment factors).
Recent research has suggested that thedopaminergic reward mechanisms of the brain
Therapy t Patient's life processes
Characteristic factors
F
Incidental treatment
factors
C
Other aspects of patient's
life functions or
health
Target disorder
D
Spectrum
of factors
nonplacebo effect
side-effects
placebo effect
side-effects
FIGURE 2.1 Illustration of a therapeutic theory used to clarify the definition of ‘placebo’. For further explanation seetext. (Adapted from reference 10.)
Ch 02 13/5/05 2:47 pm Page 12

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 13
are responsible for mediating the placebo effect.11
Brody listed three possibilities to explain why apatient improves after a certain therapy is insti-tuted:12
• The patient got better due to the natural his-tory of the condition in an organism withintact healing and recuperative powers.
• The patient got better due to the symboliceffect of the treatment, that is its impact on hisor her imagination, beliefs, and/or emotions.
• The patient got better due to some specific orcharacteristic feature of the treatment that canbe studied, isolated, and predicted within thecontext of contemporary medical theory.
A positive placebo effect (the second of the abovelist) is most likely to occur when three factors arepresent:12
• The meaning of the illness experience for thepatient is altered in a positive manner, giventhe patient’s belief system and world view.
• The patient is supported by a caring group.• The patient’s sense of mastery or control over
the illness is restored or enhanced.
This theory, emphasizing the importance of thepatient’s belief system and his or her expectations,highlights the cultural dimension of the placebophenomenon and the importance of cross-cultur-al studies in placebo research.
White et al.7 pointed out that there is no singleplacebo effect with a single mechanism and effi-cacy, but rather a multiplicity of effects with dif-ferential efficacy and mechanisms, and they pro-vide a list of placebogenic variables or determi-nants of a placebo response (Table 2.1). Turner etal.,13 in a review of the importance of the placeboeffect in pain treatment and research, listed simi-lar factors influencing the placebo response.Among the patients’ factors contributing to a
TABLE 2.1 Biopsychosocial determinants of placeboresponse. (Reproduced with permission from White etal.7)
Cultural contextBelief systemFaith
Environmental milieu
Instruction
Suggestion
Preparation characteristics
Doctor–patient relationship
Patient’s expectations and beliefs
Patient’s personality
Psychological state
Symptom severity
Discomfort severity
Anxiety and stressCentral evaluative processesCognitive processes
Cognitive schema
Self-schema
Self-control
Expectancy
Outcome expectancy
Efficacy expectations
Operant behavior
Symbolic processes
Imagination
Covert rehearsal
Emotions
Central nervous system influences upon physiologyImmune systemStress mechanismEndogenous opiates
Classical conditioning
Spontaneous remissions
Ch 02 13/5/05 2:47 pm Page 13

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA14
high placebo response rate were anticipation andexpectations, a positive attitude toward providerand treatment, anxiousness and compliance withthe prescribed treatment. As an example for thelatter, a randomized trial to evaluate the efficacyof a lipid-lowering drug in the therapy of coro-nary heart disease may be mentioned. Patients inthe placebo arm were stratified by whether theytook more or less than 80% of the placebotablets.14 Even after controling for 40 known orsuspected risk factors, the noncompliers had a57% higher 5-year mortality rate than the compli-ant patients. Either the placebo lowered mortali-ty, or patients’ compliance related to other char-acteristics associated with mortality, which wasnot assessed in this study. Among the providers’factors they listed warmth, friendliness, interest,sympathy, empathy, prestige, and, again, a posi-tive attitude towards the patient and the treat-ment.
These considerations all address the issue of a‘placebo treatment’ and the ‘placebo effect’ in theusually understood sense of a medical treatmentwith a drug. Placebo effects, however, are equallyimportant to consider when the treatment con-sists of a procedure or surgical therapy. Instead ofusing an inactive preparation, a procedure or sur-gery is performed which is similar in all respectsto the active procedure or surgery, but different inthat the key aspect of the procedure, which isbelieved to convey the main therapeutic benefit, isomitted. Such procedures are referred to as ‘shamtreatment’ and the incidental causes or effects as‘sham effects’. Throughout this chapter, the term‘placebo/sham’ will be used to indicate the perti-nence of the observation to both medical (drug)treatments and procedural (surgical) interven-tions.
RATIONALE FOR PLACEBO/SHAMCONTROLLED TRIALS
The value of controlled clinical trials in the deter-mination of the safety and effectiveness of a newintervention is largely undisputed. The US Foodand Drug Administration (FDA) recognizes fourtypes of comparative trials:
• No treatment, which involves a comparison ofthe results in comparable concurrent groupsof treated and untreated patients. This type ofcontrol is utilized when objective measure-ments of effectiveness are available and place-bo effect or spontaneous improvement of thecondition is negligible.
• Placebo control, which involves a comparisonof the results of a particular therapy with aninactive preparation or a sham procedure.
• Active treatment control, which involves acomparison of the results from the new inter-vention with those from a treatment known tobe effective.
• Historical control, which involves comparisonof the results from a new intervention withprior experience obtained in a comparablegroup of patients receiving no therapy or aknown effective regimen.
The caveat listed in the first paragraph is of greatrelevance in BPH treatment trials. While betterobjective outcome measures are being developedand utilized, there is certainly a placebo effect andthe natural history of the disease is such thatspontaneous remissions are quite common. Thus,in clinical BPH research the only alternatives areplacebo/sham-controlled trials, or active treat-ment-controlled trials. Active control trials mightsubstitute for placebo-controlled trials (1) whenthere is reasonable certainty that a new treatmentwill be more effective than other agents known to
Ch 02 13/5/05 2:47 pm Page 14

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 15
be effective; (2) when the effectiveness of the newtreatment is self-evident; or (3) where the natureof the therapy or procedure is such that it is notpossible to blind the patients or the observers.15
While the first two arguments rarely are true inBPH treatment trials, the third argumentdemands a closer look. Experience has shownthat it is feasible to blind both patients andobservers responsible for outcome assessmentregarding the randomization in a trial comparingballoon dilatation of the prostate with a shamprocedure (cystoscopy).16 As will be discussedbelow, blinding is also possible in treatment trialsusing microwave-induced heat and other mini-mally invasive treatments. Whether or not trueblinding could be achieved in a trial comparingtransurethral resection of the prostate (TURP)with a sham procedure is more questionablebecause of the need for catheterization, the bleed-ing, and the irrigation necessary following theTURP. Despite the absence of any such trial,TURP is currently considered the gold standardof BPH treatments, and, in fact, it serves occa-sionally as an active-treatment control for otherinvasive treatment modalities.
Despite the general acceptance ofplacebo/sham controls in medical research,17 oth-ers have warned against the ‘continuing unethicaluse of placebo controls’,18 stating that in manycases the use of placebo control groups is in directviolation of the Declaration of Helsinki. TheDeclaration states that:
‘The benefits, risks, burdens and effectivenessof a new method should be tested against those ofthe best current prophylactic, diagnostic, andtherapeutic methods. This does not exclude theuse of placebo, or no treatment, in studies whereno proven prophylactic, diagnostic or therapeuticmethod exists.’19
Thus, Rothman and Michels argue that theuse of a placebo is unethical whenever there is aproven therapy available according to theDeclaration of Helsinki.18 The two ethical count-er arguments which can be made are the notionthat withholding of active treatment may not leadto any harm on the part of the patient dependingon the underlying condition, and second, thatpatients in fact give their informed consent, afterbeing fully informed, to participate in a place-bo/sham controlled trial.
In the field of clinical BPH research, theAmerican Urological Association (AUA), the USFDA, and the World Health Organization(WHO) advocate rather strictly the use of placebocontrols.
The AUA BPH Clinical Trials Subcommitteeis currently preparing a blueprint for the designand reporting of clinical trials in BPH. It is notedthat BPH is a disease characterized by a some-what unpredictable natural history. A significantminority of patients experience stabilization ofsymptoms or actual improvement. Moreover,improvements in symptoms and uroflow are seenin patients treated with placebo. This makes arandomized, placebo- (or sham-) controlleddesign mandatory. New surgical technologiesshould be compared to standard surgical treat-ments, such as TURP or transurethral incision ofprostate (TUIP), utilizing a randomized design.For BPH medical therapies and minimally inva-sive technologies, efficacy relative to placebo orsham must be established (J. D. McConnell, per-sonal communication). The document further-more stipulates that patients have to be blindedtowards the assigned treatment, and that prefer-entially the treating physician should also beblinded (double-blind).
The FDA circulated a draft guidance for theclinical investigation of hyperthermia devices
Ch 02 13/5/05 2:47 pm Page 15
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA16
used for the treatment of BPH. This documentstipulates that the study protocol should include arandomized active control which best can beaccomplished by a blinded, sham-treated control.The FDA specifically discusses the use of awatchful waiting control or historical controls,and expresses concern regarding both these sug-gestions. The watchful waiting control does notassess the placebo effect of repeated catheteriza-tion which is part of the heat treatment, and thehistorical TURP control group might not be wellmatched due to different selection criteria andevaluation methodologies. However, the use of anactive, randomized, concurrent TURP controlgroup is recommended to further enhance theevaluation of hyperthermia therapy. This draftguidance document has not yet been finalized,but it is widely used in the design of trials forhyperthermia devices or other minimally invasivetreatment modalities (thermotherapy,transurethral needle ablation of the prostate(TUNA), high-intensity focused ultrasound(HIFU), etc.).
The International Consultation on BPH haspublished under the patronage of the WHO fiveconsensus documents which address the stan-dardization of the evaluation of treatment modal-ities. Similar recommendations were made in theproceedings from the 1991, 1993, 1995, and 1997meetings.20 The 2000 consensus recommenda-tions state that all new drugs and devices intend-ed for the use in LUTS and BPH should under-go rigorous testing in phase III trials of at least 12months’ duration in which they are comparedwith either standard treatments or placebo/shamtreatments to document their efficacy.21
Despite the ethical concerns voiced by some,in regards to BPH treatment trials there appearsto be unanimity between physicians, industry, thegovernment (FDA), and the WHO regarding the
mandatory use of placebo/sham control groups, atleast in those trials considered pivotal for a newtreatment.
In November 2000 the National Center forComplementary and Alternative Medicine andthe National Institute of Diabetes and Digestiveand Kidney Diseases (NIDDK) convened a con-sensus conference in Bethesda, MD (USA) on theNIH campus regarding ‘The science of the place-bo: towards an interdisciplinary research agenda’.The tremendous response and participation ofresearchers and clinicians from a wide variety ofbackgrounds highlighted the urgent need toimprove our understanding of the placebo effectand its role in biomedical research.
PLACEBO EFFECTS IN OTHER FIELDS OFMEDICINE
Blackwell et al. chose the setting of a medicalschool class to demonstrate the range of possibleplacebo effects.22 Fifty-six second-year medicalstudent volunteers were conditioned to expecteither stimulative or sedative effects, but in factall received placebo in either one or two blue orpink capsules, without knowing that in fact thenumber and color of the dispensed capsules dif-fered between the volunteers. Following theingestion of the study medication, 30% of partici-pants reported drug-associated changes, whichwere severe in one or two of the participants. Twocapsules produced more changes than one, andblue capsules were associated with more sedativeeffects than the pink capsules.
Physicians are powerful therapeutic agents,and their (placebo) influence can be felt to agreater or lesser degree at every consultation. Inan unusual study, 200 patients with nonspecificsymptoms but no definite diagnosis were selected
Ch 02 13/5/05 2:47 pm Page 16

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 17
for one of four consultations: a positive consulta-tion with therapy (thiamine hydrochloride 3 mgtablets) or without treatment, or a negative con-sultation with or without treatment.23 In a posi-tive consultation the patient was given a firmdiagnosis and told that he would be better in afew days. If no treatment was given, he was toldhe needed none. If treatment was given, he wastold that the treatment would make him betterwith certainty. In a negative consultation the doc-tor stated that he could not be sure about thediagnosis, and that therefore no treatment wasgiven (no treatment group), or that a treatmentwould be tried without assuring that it wouldhelp (treatment group). During the follow-upvisit, 64% of patients in the positive consultationgroup got better versus 39% in the negative con-sultation group (p = 0.001). However, there wasno significant difference between the treated(53%) and the not treated (50%) patients (p = 0.5).In this example the physician-related placeboeffect was clearly stronger than the effect con-veyed by the medication given.
The largest body of literature regardingplacebo effects exists in the area of pain treat-ment. Turner et al.13 identified over 150 articlesdescribing placebo effects in pain treatment andresearch. They found that placebo response ratesvary greatly. Frequently they were found to behigher than the widely accepted one-third place-bo response rate based on the classic article byBeecher.24 Placebos have time–effect curves, andpeak, cumulative, and carry-over effects similarto those of active medications. A certain placebo-responder personality could not be identified, andthe role of anxiety, expectations, and learningwere emphasized. The authors concluded thatplacebo effects plus natural history and regressionto the mean25 may result in high rates of goodoutcomes in pain treatment, which may be misat-
tributed to specific treatment effects. The impor-tant role of the physician as administrator of thetreatment for pain, be it active or placebo, wasemphasized by Gracely et al.26 Dental patientswere told that they would receive either a place-bo, a narcotic analgesic, or a narcotic antagonist,and that this treatment might increase, decrease,or have no effect on their pain. The physiciansadministering the drugs knew, however, that onegroup of patients would receive either placebo orthe narcotic antagonist but not the narcotic anal-gesic (group A), while another group wouldreceive any one of the three agents (group B).Thus, the two groups of placebo-treated patientsin groups A and B did only differ in the clinician’sknowledge of the range of possible double-blindtreatments, including the knowledge thatpatients in the group A had no chance of receiv-ing active pain medication. Nonetheless, theplacebo-treated patients in group B had signifi-cantly less pain than those in group A. Thisexperiment shows clearly that analgesia does notonly depend on the action of the administeredtreatment, but also on the expectations of thepatient and, most surprisingly, on those of thephysician, who may influence the patient’sresponsiveness by a subtle behavioral change.This phenomenon of expectation and anticipa-tion of analgesia must be taken into account whendesigning a cross-over study, as the patient’s pastexperience of pain relief (i.e. during phase I of across-over trial) may influence his/her subsequent(i.e. during phase II of a cross-over trial) responseto treatment.27
Surgical procedures may also have a verystrong placebo effect as described earlier byBeecher.28 A most striking and classic example isthe history of internal mammary artery ligationfor the treatment of angina pectoris, which waspopular in the first half of the twentieth century
Ch 02 13/5/05 2:47 pm Page 17

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA18
as a means to increase blood flow to the coronarycirculation. Beecher analyzed the early experi-ence and divided the reports into those written by‘enthusiasts’ versus ‘sceptics’. The former groupfound complete relief of chest pain in 71/213patients (38%) while the latter in only 6/56(10%).28 Cobb et al.29 and Diamond et al.30 per-formed a double-blinded study (the cardiologistwas blinded as to the procedure performed by thecardiac surgeon) of internal mammary artery lig-ation versus a sham procedure, namely skin inci-sion only, and published remarkably similarresults. Cobb et al. reported a 63% significantimprovement and 34% decrease in the use ofnitroglycerine in the ligation group versus a 56%improvement and 42% decrease in nitroglycerineuse in the sham group. Diamond et al. reported a100% improvement in both groups regardingexercise tolerance, nitroglycerine use, and anginapain. During the year after surgery, 69% ofpatients reported over 50% improvement in painin the ligation group versus 100% who experi-enced greater than 50% improvement in the shamgroup. In a review, Johnson31 discussed the possi-ble placebo effect of extracorporeal shock wavelithotripsy (ESWL) for gallstones. In a random-ized trial comparing ESWL with open cholecys-tectomy the symptomatic response was similar inboth groups but, surprisingly, the symptomaticresponse in the ESWL group was identicalwhether or not the stones had actually beencleared. Thus, the symptomatic response might atleast partially be triggered by a placebo effect.
Comparatively little is known about the place-bo effects on healthy volunteers in clinical phar-macology trials. Rosenzweig et al.27 reviewedadverse events reported during placebo adminis-tration in 109 double-blind, placebo-controlledstudies involving 1228 volunteers. The overallincidence of adverse events was 19%, and com-
plaints were more frequent after repeated dosing(28%) and in elderly subjects (26%). The most fre-quent adverse events were headache (7%),drowsiness (5%), and asthenia (4%). The overallincidence and distribution of adverse events alsoappeared to depend on the nature of the activeinvestigational drug in the young volunteers insingle-dose studies. The highest incidence for alladverse events was noted when the active drughad a central nervous system effect (16.7%). Theincidence was lower when the active drug hadmiscellaneous effects (16.2%) or a cardiovascularsystem effect (6.1%).
NATURAL HISTORY, WATCHFUL WAITING,VERSUS PLACEBO EFFECT
The importance of placebo/sham-controlled trialsin BPH research is emphasized by the highlyvariable natural history of the disease, and thetendency towards spontaneous improvement andregression documented in several watchful wait-ing studies, and, to a lesser degree in longitudinalstudies of the natural history of the disease. Whilenatural history studies refer to the longitudinalstudy of a cohort of men with signs and symp-toms of BPH over time without any kind of treat-ment intervention, the watchful waiting studiesusually entail at least a yearly follow-up visit witha ‘treating’ physician. According to the discussionabove, this consultation may have a profoundimpact on the ‘natural history’ of the diseaseprocess depending on the attitude and behavior ofthe physician. It is probably reasonable to expectthat at the end of each visit the physician wouldtell the patient that ‘he is doing well and does notneed any [additional or active] treatment’, a state-ment that carries with it a considerable placeboeffect. Even in a natural history study the mem-
Ch 02 13/5/05 2:47 pm Page 18

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 19
bers of the study population have to be seen,interviewed, and examined at regular intervals,thus providing for the possibility of a placeboeffect. Longitudinal natural history studies mayprovide nonetheless the best information aboutthe ‘background activity’ of the disease process.Watchful waiting studies add at least one knownand powerful placebo effect, and they carry withthem the possibility of ‘treatment failure’ andconversion to a presumably more active treat-ment. Lastly, placebo/sham control groups addadditional nonspecific effects and, thus, their out-comes theoretically should be superior to watch-ful waiting and natural history studies.
Regression to the mean
Placebo control arms differ in at least one othervery important characteristic from natural histo-ry studies. In general, patients are selected to par-ticipate in studies based on inclusion/exclusioncriteria, usually eliminating patients perceived tobe less symptomatic, i.e. those with lower symp-tom scores and higher peak flow rates. By theprinciple of trial conduct, patients then repeat thesymptom and flow rate assessment during andafter therapy in both active and placebo groups.However, the same inclusion/exclusion criteriaare not applied to those measurements. To deter-mine the effect that the stringency of pretrialscreening has on the outcome of placebo treat-ment, a cohort of 145 volunteers were invited tofill in the I-PSS score and perform a flow raterecording twice within a month without receiv-ing any therapy or instructions whatsoever.32
Although many patients experienced either anincrease or a decrease in both parameters, themean values did not change significantly (I-PSS12.1 vs 11.7 points, peak flow rate 17.7 vs17.4 ml/s; not significant). However, when typicalBPH trial conditions were applied and only those
patients considered for analyses who had an I-PSS score above (>7, >10, >15) and a flow ratebelow a certain threshold (<15, <12, <10 ml/s), aunilateral regression to the mean took place, bywhich the ‘more’ symptomatic volunteers (i.e.patients) experienced still considerable naturalvariability on the occasion of the second assess-ment, but the net effect was towards ‘improve-ment’, i.e. lower scores and higher flow rates. Forexample, when only considering patients with I-PSS scores >10 points, the mean differencebetween first and second assessment was between19.9 and 18.9 points or –1.1 (p < 0.05). Similarly,when only patients with a peak flow rate< 12 ml/s were considered, the mean differencebetween the first and second assessments was 9.3vs 10.9 ml/s or +1.6 ml/s (p < 0.01) (Tables 2.2 and2.3). This experiment clearly illustrates that a uni-lateral regression to the mean induced and con-trolled by the stringency of the inclusion criteriacan result in a significant ‘improvement’ in anyparameter for which a threshold is set at the base-line screening. Such purely mathematical effect isprobably at work in many if not all studies wherethe outcome parameters are measured using anumerical scale of some sort, and where baselinescreening criteria are applied.
This effect, however, is by definition not atwork in a longitudinal natural history studywhere no baseline inclusion criteria are applied,but rather all patients independent of the numer-ical value of the measured parameter are fol-lowed.
Natural history of BPH
The most informative natural history study todate is the Olmsted County study of urinarysymptoms and health status among men, whichhas given us much information about prevalenceand severity of urinary symptoms, bother, worry,
Ch 02 13/5/05 2:47 pm Page 19

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA20
and embarrassment, quality of life due to symp-toms, and the relationship between symptomsand other parameters such as flow rates, prostatevolume, and prostate-specific antigen (PSA).33–41
With continued follow-up of this cohort, datahave emerged regarding the longitudinal changesin symptoms and flow rate over time in this pop-ulation-based study. Of 904 men reporting noneto mild symptoms (AUASI 0–7 points) at base-
line, 118 reported moderate to severe symptoms(AUASI > 7 points) at 18 months’, and 196 at 42months’ follow-up.42 However, 47 men who haddeveloped moderate to severe symptoms at 18months, had none to mild symptoms at 42months. At 42 months of follow-up an averageincrease in the I-PSS of 0.18 (95% confidenceinterval 0.13 to 0.24) points per year of follow-upwas recorded. The average annual symptom
TABLE 2.2 Mean ± SD and range for AUA symptom index for tests 1 and 2, mean difference between the two tests andthe 95% confidence interval (CI) for the difference, for all subjects, and for subjects censored based on test 1 > 7 points,> 10 points, and > 15 points. Statistical comparison between tests 1 and 2 by t-test. Note the reduction in the number ofpatients available for follow-up due to censoring which affects the power of the statistical test.
*p < 0.05.
Selection Mean ± SD Range Mean difference 95% CI t-Test n
All subjects 1 12.1 ± 8.8 0–32 –0.392 11.7 ± 9.0 0–32 –1.1 to 0.29 0.133 145
> 7 at 1 1 17.8 ± 6.5 9–32 –0.972 16.8 ± 7.7 0–32 –2.0 to 0.08 0.035* 88
> 10 at 1 1 19.9 ± 5.6 11–32 –1.12 18.9 ± 6.9 0–32 –2.2 to 0.1 0.036* 70
> 15 at 1 1 22.0 ± 4.6 16–32 –1.42 20.6 ± 6.6 0–32 –2.8 to 0.01 0.026* 54
TABLE 2.3 Mean ± SD and range for peak flow rate for tests 1 and 2, mean difference between the two tests and the95% confidence interval (CI) for the difference, for all subjects, and for subjects censored based on test 1 <15 ml/s,<12 ml/s, and <10 ml/s. Statistical comparison between tests 1 and 2 by t-test. Note the reduction in the number of patientsavailable for follow-up due to censoring which affects the power of the statistical test.
*p < 0.05.
Selection Mean ± SD Range Mean difference 95% CI t-Test n
All subjects 1 17.7 ± 8.2 5.1–47.5 –0.182 17.4 ± 8.4 4.7–61.0 –1.2 to 0.82 0.36 145
< 15 at 1 1 10.7 ± 2.5 5.1–14.6 1.52 12.2 ± 4.6 4.7–25.5 0.47 to 2.6 0.002* 65
< 12 at 1 1 9.3 ± 2.1 5.1–11.8 1.6 2 10.9 ± 4.8 4.7–25.5 0.06 to 3.1 0.021* 40
< 10 at 1 1 7.3 ± 1.6 5.1–9.9 1.72 9.0 ± 3.7 4.7–17.4 0.4 to 3.8 0.05* 17
Ch 02 13/5/05 2:47 pm Page 20

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 21
score slope and variability in slope increased withpatient age at baseline from a mean of 0.05 ± 1.06(standard deviation) per year among men in theirforties to 0.44 ± 1.35 per year for men in their six-ties, and decreased to 0.14 ± 1.42 per year for menin their seventies.43 More recently, 92 months’data showed an annual change of 0.34 points/year,with 31% of all men reporting at least a 3-pointincrease. The greatest annualized increase wasobserved in men in their sixties with 0.6points/year.44
In addition, 6-year follow-up data on peakflow rate measurements in a subset of about 500men showed a median peak urinary flow rateslope decrease of –2.1% per year (25th centile–4.0, 75th centile –0.6). Peak urinary flow ratedeclined more rapidly with decreasing baselinerate, and increasing baseline age, prostate vol-ume, and symptom severity (all p = 0.001). Whenthe variables were simultaneously adjusted foreach other, a rapid decline (negative slope 4.5% orgreater per year) was more likely in men 70 yearsold or older and in those with a rate less than10 ml/s at baseline compared to those 40 to 49years old and those with a rate of 15 ml/s orgreater, respectively. Prostate volume and symp-tom severity were not statistically significant pre-dictors of a rapid decline in peak urinary flowrate when variables were considered simultane-ously.45
Based on transrectal ultrasonography(TRUS), the growth of the prostate in the menaged 40–79 years was estimated to be about 0.6 mlper year or 6 ml per decade of life. However,prostate growth followed an exponential growthpattern, with a slope estimate of 0.4 ml per yearfor men aged 40–59 years at baseline and of 1.2 mlper year for those aged 60–79 years at baseline.46
An updated analysis revealed a median growthrate of about 1.9%/year independent of age and
symptoms. However, a higher baseline serumPSA and larger prostate volume predictedgreater annualized volume increases (Figure2.2).47
Diokno et al.48 provided estimates of theprevalence, incidence, and remission of lower uri-nary tract symptoms in 803 community-dwellingmen aged 60 years or older. The annual incidenceof prostate surgery was 2.6% and 3.3% duringyears 1 and 2 of follow-up. The prevalence of atleast one symptom was 35%, with annual inci-dence rates during years 1 and 2 of follow-upbeing 16.4% and 16.1%. Remission was also notedin that 22.9% of those having severe symptoms atbaseline were asymptomatic at follow-up. Table2.4 details the changes in symptom severity fromone survey to the next. The tendency for fluctua-tion and spontaneous remission of symptoms aswell as the regression to the mean become evidentfrom an analysis of these data.
Watchful waiting studies
In the absence of other longitudinal natural his-tory studies, several watchful waiting studies areavailable for review. Most of these studies havesignificant shortcomings. Inclusion and exclusioncriteria are poorly defined, follow-up is loose,assessment instruments are either not defined orinsufficient, and patient accounting is incomplete.
Five such studies, reported between 1919 and1988 and totaling 456 patients with follow-upranging from 3 to 6 years,49–53 were analyzed forthe AHCPR BPH Guidelines.54 A change insymptom status was reported for all 456 patients,while none of the studies utilized a quantitativesymptom severity scale. Data on urinary flow rateand residual urine were available for 223 and 197patients, respectively. The peak urinary flow ratedeteriorated in 66% and improved in 20%.Residual urine increased (35%), decreased (37%),
Ch 02 13/5/05 2:47 pm Page 21

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA22
and remained unchanged (28%) in about thesame number of all patients. The mean change inpeak flow rate (in those patients for whom dataare available) was 2.2 (from a mean of 9.0 to11.2) ml/s or 24%, while the mean change inresidual urine was +37 (from a mean of 115 to152) ml or 32%. The data on symptom improve-ment were dichotomized (improved versus notimproved). The probability for symptomimprovement was then calculated using the con-
fidence profile method (CPM) described byDavid Eddy55 (Figure 2.3). The mean probabilityfor improvement in symptom severity was esti-mated to be 42.5% (90% CI 30.8 to 54.8), surpris-ingly similar to the probability for improvementnoted in the placebo arms, and in a carefullydesigned, prospective study to be discussed below.It must, however, be recognized that, because oflimitations of the dataset, the magnitude of theimprovement cannot be estimated. In updated
PSA (ng/ml)
An
nu
al %
in
cre
ase
Baseline prostate volume (ml)
An
nu
al %
in
cre
ase
4.5
4
3.5
3
2.5
2
1.5
1
0
–0.5
0 1 2 3 4 5 6 7 8 9 10
4.5
4
3.5
3
2.5
2
1.5
1
0
–0.5
0 10 20 30 40 50 60 70 80 90 100
(a)
(b)
Spearman r = 0.59, p < 0.0001
Spearman r = 0.34, p < 0.0001
FIGURE 2.2 Per cent annual increase in prostate volume by baseline prostate volume (a) and baseline serum PSA (b) inparticipants of Olmsted County study of urinary symptoms in men. (Adapted from reference 47.)
Ch 02 13/5/05 2:48 pm Page 22

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 23
guidelines for the management of BPH,published by the AUA,56 watchful waiting is rec-ommended for patients with mild symptoms(AUA symptom score ≤ 7) or moderate to severeBPH in patients who are not bothered by theirsymptoms. Watchful waiting is therefore anappropriate early treatment strategy for mostmen with BPH.
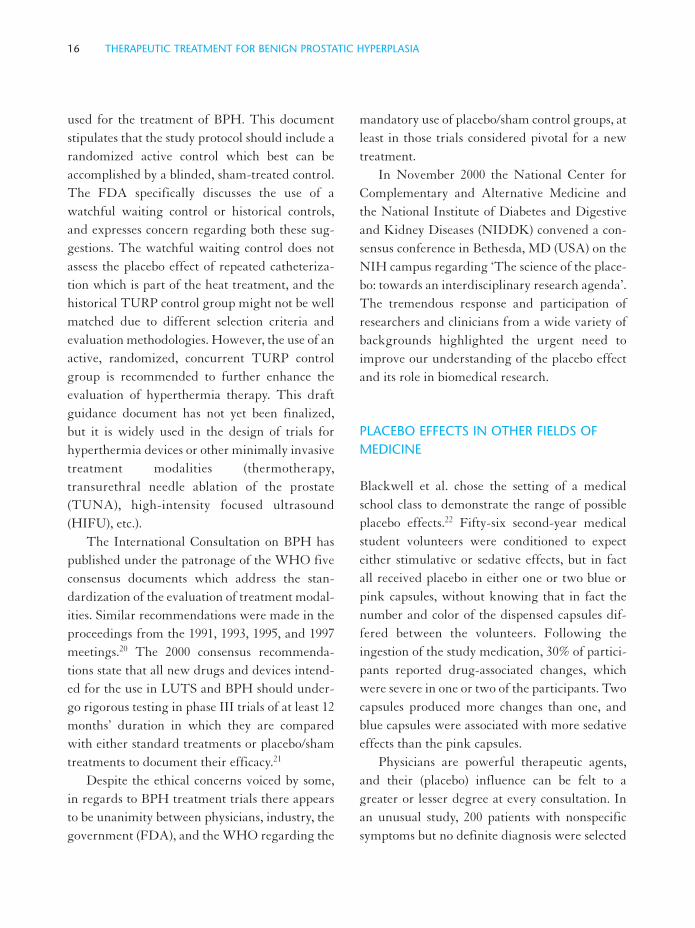
A randomized study with a 3-year follow-upwas reported comparing watchful waiting withTURP in 556 men with symptoms of BPH57.Inclusion criteria included a Madsen–Iversensymptom score between 10 and 20 points (0–27point scale), thus limiting the informational valueof the watchful waiting arm of the study topatients with moderate lower urinary tract symp-toms. There were 47 treatment failures (definedas death, recurrent infection, residual urine vol-ume over 350 ml, development of bladder calcu-lus, incontinence, a symptom score of 24 or high-er, or a doubling of serum creatinine from base-line) in the watchful waiting arm (n = 276) versus23 in the surgery arm (n = 280) over 3 years of fol-low-up (relative risk 0.48; 95% CI 0.3–0.77).Sixty-five (24%) men assigned to watchful wait-ing underwent surgery during follow-up, 20 ofthem for treatment failure. The majority of thesemen were classified as more bothered at baseline(Figure 2.4). It should be noted that about 40% ofpatients in this category experienced improve-ment in the degree of bother from urinary diffi-culties (Figure 2.4). The changes from baselinefor the watchful waiting patients are shown in
TABLE 2.4 Changes in status of obstruction severity from one survey to the next (adapted from reference 48). Patientswho underwent prostatectomy in the preceding year were excluded from the next survey.
Severity in following year (%)
Severity Year No None Mild Moderate Severe
None Baseline 293 83.6 12.3 2.7 1.4
Year 1 223 83.9 9.0 2.2 4.9
Mild Baseline 88 18.2 55.7 11.4 14.8
Year 1 84 33.3 52.4 8.3 6.0
Moderate Baseline 38 7.9 31.6 26.3 34.2
Year 1 27 3.7 33.3 22.2 40.7
Severe Baseline 35 22.9 17.1 11.4 48.6
Year 1 31 9.7 22.6 12.9 54.8
45.2%42.5%
74.1%
56.6%
80.2%
88.1%
98.4%100
90
80
70
60
50
40
30
20
10
0
Placebo Dilatation Open surgeryWatchful waiting TUIP
α-Blocker TURP
Pro
ba
bili
ty o
f im
pro
ve
me
nt
(%)
FIGURE 2.3 Probability of achieving symptom improve-ment following various treatment interventions. Meanprobability and 90% confidence interval calculated withthe confidence profile method55 using hierarchical Bayes’.
Ch 02 13/5/05 2:49 pm Page 23
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA24
Table 2.5. It should be noted that the meanchanges represented in almost all categories animprovement for those men who were followedin the assigned treatment arm (watchful waiting)over 3 years. The magnitude of the improvement,however, was less than that realized by surgery inalmost all categories (p values in Table 2.5).Furthermore, this analysis obviously excludesthose men who were categorized as treatmentfailures, underwent surgery (cross-over), or werelost to follow-up.
Placebo arms of controlled medical treatmenttrials for BPH
For the AHCPR BPH guidelines, data on 1417patients treated in 45 placebo arms of placebo-controlled trials were analyzed.54 Table 2.6 andFigure 2.3 allow a direct comparison between thewatchful waiting and the placebo studies. A sig-nificant difference between the two treatmentmodalities cannot be identified for any of the
100
75
50
25
0
Pe
rce
nta
ge
of
pa
tie
nts
Surgery SurgeryWatchful
waiting
Watchful
waiting
More bothered
at baseline
Less bothered
at baseline
FIGURE 2.4 Degree of bother from urinary difficultiesafter 3 years of follow-up among men with LUTS andBPH managed with TURP or watchful waiting stratifiedby more or less bother at baseline.57 , Improved; ,worse or no change; , cross-over to surgery.
TABLE 2.5 Changes from baseline for men followed over 3 years in a watchful-waiting protocol. (Adapted from refer-ence 57.)
*n = 276; **only patients who were followed over 3 years excluding cross-overs, failures etc.; †for difference betweentreatment groups (surgery versus watchful waiting); ‡on a scale from 0 (greatest impairment) to 100 (least impairment).
Outcome Baseline* Follow-up** Mean change ± SD p Value†
Symptom Score (0–27) 14.6 9.1 –5.5 ± 5.2 < 0.001
Residual urine (ml) 113 72 –41 ± 90 0.015
Peak flow rate (ml/s) 12.5 12.7 0.4 ± 9.2 < 0.001
Bother from urinary difficulties‡ 46.3 57.6 9.6 ± 29.7 < 0.001
Sexual performance‡ 42.5 35.6 –3.2 ± 26.6 0.92
Activities of daily living‡ 69.0 75.6 6.4 ± 30.3 < 0.001
General well-being‡ 71.2 71.4 0.1 ± 28.3 0.217
Social activities‡ 74.2 73.1 –1.7 ± 23.5 0.945
Ch 02 13/5/05 2:52 pm Page 24

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 25
examined parameters. However, several pointsdeserve discussion. As opposed to the long-termfollow-up in the watchful waiting studies, theplacebo studies are part of short- to mid-termmedical treatment trials ranging from 3 days to52 weeks in duration (mean 13 weeks). In allthese studies the patients are blinded as to thetreatment arm, and thus have in most cases atleast a 50 : 50 (or better in case of 2 : 1 or 3 : 1 ran-domization) chance of receiving active drug.Dropping out of such studies because of failuredoes not have the same ramification as it does inwatchful waiting studies where the patients will-ingly assume a conservative treatment approach
knowing that it might fail (i.e. they might fail andgo on to active treatments). In contrast, in someplacebo-controlled studies a promise—either tacitor openly—is made stating that following theconclusion of the trial the patient would be eligi-ble for either ‘free’ active treatment or he wouldbe ‘moved up’ on the surgical waiting list (thisphenomenon is unique to those studies conductedin the UK). The inactive preparation givenshould theoretically add to the placebo effect and,thus, improve the outcome above those noted forwatchful waiting studies. The probability for apatient to experience improvement, however, isestimated to be about 40% in the uncontrolled
TABLE 2.6 Comparison of outcomes following watchful waiting and placebo treatment. (Adapted from reference 54.)
* Calculated by confidence profile method using hierarchical Bayes’.55
Outcomes Watchful waiting Placebo
Total number of patients in database 456 1417
Peak flow rateProbability for flow rate increase 19.7% 35.8%Probability for no change in flow rate 14.2% 41.1%Probability for flow rate decrease 66.1% 23.1%Mean pretreatment flow rate (ml/s) 9.0 9.1Mean posttreatment flow rate (ml/s) 11.2 9.7Difference (ml/s) +2.2 +0.6Per cent change in peak flow rate +24.4% +6.6%
Residual urineProbability for decrease in residual urine 35.0% 38.0%Probability for residual urine to remain unchanged 28.0% 26.1%Probability for increase in residual urine 37.0% 35.9%Mean pretreatment residual urine (ml) 115 87Mean posttreatment residual urine (ml) 152 76Difference (ml) +37 –11Per cent change in residual urine +32.2% –12.6%
Symptom improvementProbability for symptom improvement 41.7% 41.7%Probability for symptoms to remain unchanged 25.8% 53.5%Probability for symptom worsening 32.4% 4.7%Mean probability for symptom improvement* 41.7% 41.7%90% Confidence interval for symptom improvement* 30.8 to 54.8% 26.3 to 65.1%
Ch 02 13/5/05 2:52 pm Page 25

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA26
watchful waiting studies, the randomized watch-ful waiting versus TURP study, and the com-bined placebo arms. The changes in peak flowrate and residual urine are similar, and similarlysmall, for these three groups as well (see Tables2.5 and 2.6). Figure 2.5 shows a comparison of thepercentage changes in peak flow rate and residualurine as well as the percentage of patients experi-encing symptom improvement between varioustreatment modalities. It becomes evident that a40% rate of patients reporting improvement andthe minimal fluctuation of peak flow rate andresidual urine represent the ‘placebo effect’ back-ground against which the more substantialchanges in these parameters achieved by activetreatment modalities must be seen.
With the advent of symptom severity assess-ment tools or symptom scores it is possible toquantitatively describe the response of patients
treated by a variety of treatment interventionsincluding placebo and watchful waiting (seeChapter 1). Unfortunately, the different symp-tom-scoring instruments differ regarding theirfoot points (0 or different from 0), their scale, andoccasionally even their direction (increasing ordecreasing severity of symptoms with increasingscore). While currently the AUASI orInternational Prostate Symptom Score(I–PSS),58–63 with its scale from 0 to 35 points, isthe most widely utilized instrument, thus facili-tating direct comparisons between studies, in theyears past different scores with different scaleswere used. The only way to compare symptomimprovement in different trials quantitatively insuch cases is to rescale the individual scales to a100% scale, and to express the changes as the dropin percentage symptom score from before to aftertreatment. Using this technique, seven placebo-
1 2 3 4 5 6 7
200
150
100
50
0
–50
–100
100
70
40
10
Pe
rce
nta
ge
ch
an
ge
s in
pe
ak f
low
ra
te
an
d r
esid
ua
l u
rin
e
Pe
rce
nta
ge
of p
atie
nts
re
po
rtin
g im
pro
ve
me
nt
in s
ym
pto
ms
FIGURE 2.5 Percentage changes in peak flow rate and residual urine (left y-axis), and percentage of patientsreporting improvement in symptoms (right y-axis) following various treatment interventions. (Adapted from reference54.)
Ch 02 13/5/05 2:53 pm Page 26

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 27
controlled trials were reanalyzed and comparedto the most significant watchful waiting study57
(Figure 2.6). These seven trials enrolled between11 and 267 subjects per arm, lasted from 4 to 24weeks, and utilized an injectable steroid hormone(norprogesterone),64 a prolactin inhibitor(bromocriptine),65 an H2 blocker (cimetidine),66
an α-blocker (alfuzosin),67 or candicin68–70 as the‘active’ drug. Each study is represented by itsactive and the placebo arm side by side. Severalpoints are noteworthy. The pretreatment symp-tom severity score expressed as percentage ofachievable score on a 100% scale ranges from 35%to almost 60%, and the drop in symptom severityfrom 7% to 33% for the placebo arms. Moreover,the pre- to posttreatment symptom score rangedoes not even overlap between some of the trialslisted, indicating that vastly different patient pop-
ulations were treated. Specifically addressing thethree placebo-controlled, double-blinded trialsusing candicin as the active drug, the drops insymptom score were 9, 15, and 33% (placebo), and6, 26, and 22% (candicin). With the exception ofthe bromocriptine trial, the baseline symptomseverity was reasonably similar between theplacebo and the active treatment arm, and in allsuch cases the placebo response closely matchedthe active drug response.
These observations allow several conclusions:
• There is a strong placebo response noted in
medical treatment trials for BPH when quan-
titative symptom severity scores are used.
• The placebo response in medical treatment
trials for BPH depends largely on the pre-
treatment characteristics of the treated cohort.
Treatment
Sym
pto
m s
co
re (
0–
10
0%
sca
le)
Wat
chfu
l waitin
g
Place
bo
α-Block
er
Place
bo
Nor
prog
este
rone
Place
bo
Bro
moc
riptin
e
Place
bo
Cim
etidine
Place
bo
Can
dicin
Place
bo
Can
dicin
Place
bo
Can
dicin
70
60
50
40
30
20
10
20%
11% 15%
27% 23%
8%
17%
7% 8%
9% 6%
15%
26%
33%
22%
FIGURE 2.6 Improvements noted using a quantitative symptom score in seven placebo-controlled trials and a watchfulwaiting study. Due to the different scales used, all scores were rescaled to a 100% scale and the reported changes expressedas mean pretreatment and mean posttreatment per cent symptom score. The number above the vertical bar indicates thechange noted following treatment (expressed as per cent).
Ch 02 13/5/05 2:54 pm Page 27

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA28
• Even when the baseline symptom severity issimilar between two trials (A and B), theresponse of the placebo group in trial Amatches more closely its actively treatedcohort than the placebo group in trial B.
• The latter fact indicates that factors other thanthe active drug or placebo are most responsi-ble for the placebo effect.
These factors may include patient selection crite-ria (solicitation, advertising), design and durationof study, incentives offered to patients (financialor otherwise), conduct and attitude of treatingphysician or research coordinator (sympatheticversus unsympathetic, friendly versus unfriendly,positive versus negative), and other unrecognizedfactors. In fact, given the parallel changes in bothtreatment groups in most trials, the latter factors,which are provider factors, are more likely to beresponsible than the previously mentionedpatient factors.
It could be reasoned that placebo-treatedpatients enrolled with similar inclusion andexclusion criteria into clinical trials using thesame class of active drugs might have a similarplacebo response. A comparison of three α1-receptor-blocker trials allows this hypothesis to betested. Eighty-two patients were treated withdoxazosin versus placebo over 16 weeks,71 2064patients with terazosin versus placebo over 52weeks,72 and 296 patients with tamsulosin versusplacebo over 12 weeks.73 In all three trials a dif-ferent symptom score was used. In the doxazosintrial, the scale ranged from 0 to 30 points, in theterazosin trials from 0 to 35 points (AUASI), andin the tamsulosin trial from 0 to 27 (Boyarskyscore). In Figure 2.7 all scores are rescaled to a100% scale and the pre- and posttreatment meanscores are expressed as a percentage of the 100%scale. Although the pretreatment symptom sever-ity is different in the three trials, the placebo
70
60
50
40
30
20
10
Doxazosin Placebo Terazosin Placebo Tamsulosin Placebo
Treatment
Sym
pto
m s
co
re (
0–
10
0%
sca
le)
19.0% 8.3% 21.7% 10.6% 13.0% 8.1%
47.3
28.3
43.7
52.0
35.7
46.9
57.4
35.2
22.2
26.3
34.4
57.4
FIGURE 2.7 Pre- and posttreatment mean symptom scores (upper and lower tickmark of vertical bar, respectively)rescaled to 100% for active-drug- and placebo-treated cohorts in three randomized α-blocker trials (for details see text).The number at the bottom of the graph represents the per cent improvement achieved.
Ch 02 13/5/05 2:55 pm Page 28

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 29
responses are very similar, ranging from 8.1 to10.6% on the 100% scale, roughly half of theactive drug cohort in each trial.
Improvements in peak urinary flow rates arealso similar between these three drug trials, rang-ing from 0.4 to 0.8 ml/s in the three placebogroups, despite the fact that the baseline meanpeak flow rates are rather different (Figure 2.8).It should be noted that this improvement in peakflow rate is very similar to the mean changesnoted in the combined placebo arm analysis of theAHCPR guidelines (0.6 ml/s) and the watchfulwaiting study (0.4 ml/s) by Wasson et al.57 Thepercentage improvement calculated for the com-bined placebo arms (6.6%) falls also in the rangeof improvements seen in these three α-blockertrials (3.8 to 8.3%).
Sham arms of controlled-device treatmenttrials for BPH
In recent years a multitude of minimally invasivedevice treatments for BPH have been developedand tested in randomized, sham-controlled, open,single-, or even double-blinded trials. While themajority of these trials compare various types ofheat treatments (transrectal or transurethralhyperthermia or thermotherapy) with a shamtreatment, one investigator compared balloondilatation with ‘sham’ cystoscopy alone in a ran-domized, double-blinded trial involving 33 menwith BPH.74 Blinding of the patients was effec-tive in that an equal number of patients in eacharm thought they had undergone balloon dilata-tion. After 3 months, 40% of balloon dilatedpatients noted marked improvement, while 27%noted no change. After cystoscopy, 63% hadmarked improvement and 12% no change. Thechanges in symptom score were significant at 3months in both groups, while the peak urinaryflow rate changes were not significant from base-
line in either group (Table 2.7). Most importantly,there was no difference in the symptom score orpeak flow rate data at 3 months between the‘active’ and the ‘sham’ treatment. This study iswidely used to support the notion that balloondilatation has no role in the treatment of BPH,and is not better than placebo/sham treatment.
Figures 2.9 and 2.10 analyze the outcomes ofthe balloon dilatation versus cystoscopy trial, onemulticenter trial using transrectal ortransurethral hyperthermia in comparison with asham control,75 and five transurethral microwavethermotherapy (TUMT) trials and their respec-tive sham-control arms.76–79 The following obser-vations can be made. The baseline or pretreat-ment mean symptom severity expressed as a per-centage of total achievable severity (rescaled to100%) is different from trial to trial. The meanimprovements in symptom severity in the shamgroups ranged from 5.2 to 15.6% (on a 100%scale), while the active thermotherapy-treatedpatients had improvements ranging from 27.0 to37.8%, or in most cases twice the improvementcompared to the sham control. The multicenterhyperthermia trial represents the exception, inthat the actively treated cohort has an improve-ment similar to the sham control, which is wellwithin the range of the other sham control trials.The changes in peak urinary flow rate follow asimilar pattern (Figure 2.10). With the exceptionof TUMT trials 2 and 4, the changes in peak flowrate are either very modest improvements ordeteriorations (0.5, 0.6, –0.2, –1.0 ml/s), while theactive-treatment arms report substantialimprovements, with the exception of the hyper-thermia trial. The changes noted in the shamarms (and the largely ineffective hyperthermiatreatment arm) are very similar to those observedafter α-blocker therapy (see Figures 2.7 and 2.8).Both thermotherapy trial 5 and the terazosin trial
Ch 02 13/5/05 2:55 pm Page 29
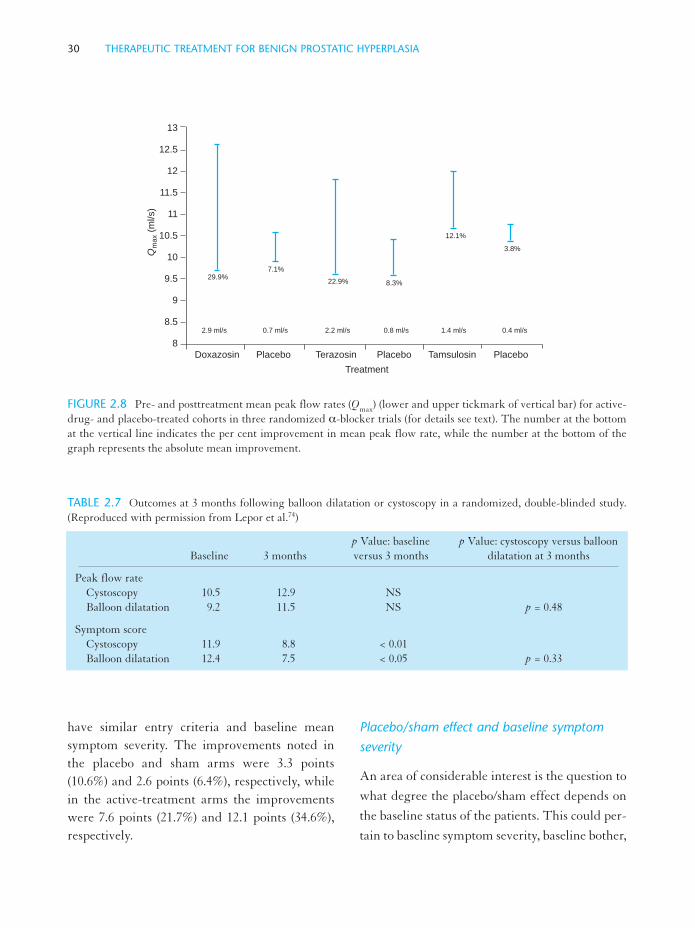
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA30
have similar entry criteria and baseline meansymptom severity. The improvements noted inthe placebo and sham arms were 3.3 points(10.6%) and 2.6 points (6.4%), respectively, whilein the active-treatment arms the improvementswere 7.6 points (21.7%) and 12.1 points (34.6%),respectively.
Placebo/sham effect and baseline symptomseverity
An area of considerable interest is the question to
what degree the placebo/sham effect depends on
the baseline status of the patients. This could per-
tain to baseline symptom severity, baseline bother,
TABLE 2.7 Outcomes at 3 months following balloon dilatation or cystoscopy in a randomized, double-blinded study.(Reproduced with permission from Lepor et al.74)
p Value: baseline p Value: cystoscopy versus balloonBaseline 3 months versus 3 months dilatation at 3 months
Peak flow rateCystoscopy 10.5 12.9 NSBalloon dilatation 9.2 11.5 NS p = 0.48
Symptom scoreCystoscopy 11.9 8.8 < 0.01Balloon dilatation 12.4 7.5 < 0.05 p = 0.33
13
12.5
12
11.5
11
10.5
10
9.5
9
8.5
8
Doxazosin Placebo Terazosin Placebo Tamsulosin Placebo
Treatment
Qm
ax (
ml/s)
2.9 ml/s 0.7 ml/s 2.2 ml/s 0.8 ml/s 1.4 ml/s 0.4 ml/s
29.9%7.1%
22.9% 8.3%
12.1%
3.8%
FIGURE 2.8 Pre- and posttreatment mean peak flow rates (Qmax) (lower and upper tickmark of vertical bar) for active-drug- and placebo-treated cohorts in three randomized α-blocker trials (for details see text). The number at the bottomat the vertical line indicates the per cent improvement in mean peak flow rate, while the number at the bottom of thegraph represents the absolute mean improvement.
Ch 02 13/5/05 2:56 pm Page 30

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 31
quality of life, baseline flow rate, and all otherimaginable parameters. Although very few inves-tigators have thus far reported data stratified bybaseline parameters, results from a multicenter,placebo-controlled, 12-month α-blocker trial(terazosin) can be analyzed.80 Figure 2.11 showsthe absolute and percentage improvement inAUA symptom score for the placebo- and drug-treated patients stratified in six strata by symptomseverity. While the active drug-treated cohort hasalmost twice the improvement within each stra-tum, the placebo-treated patients had improve-ments ranging from 1.4 points (4.6%) to 7.5 points(21.4%). The placebo improvements for theentire placebo cohort were 3.3 points (10.6%).
A similar increase in the placebo effect withincreasing baseline symptom severity has been
reported for patients treated with finasteride inthe phase III trials.81 It might be speculated thatthe baseline symptom severity may also affect thesham effect seen in device trials. This phenome-non might be due to increased expectations inpatients with more severe baseline symptoms, orsimply due to a regression to the mean.
Natural history of disease progression in long-term placebo arms
The distinction between placebo response in con-trolled studies versus the natural history of thedisease itself observed in population-based studiesbecomes blurred when the placebo control is car-ried out over a period of time long enough toallow natural history changes to take place and
60
50
40
30
20
10
Sym
pto
m s
co
re (
0–
10
0%
sca
le)
TreatmentHyp
erth
erm
ia
Sha
m
TUM
T-1
Sha
m-1
TUM
T-2
Sha
m-2
TUM
T-3
Sha
m-3
TUM
T-4
Sha
m-4
TUM
T-5
Sha
m-5
Balloon
Cys
tosc
opy
15.9%
13.0%
28.1%
15.6%
27.0%
14.4%
37.8%5.2%
28.1%
15.6% 34.6%7.4%
18.1%
11.5%
FIGURE 2.9 Pre- and posttreatment (3 months) mean symptom scores (upper and lower tickmark of vertical bar)rescaled to 100% for active-treated and sham-treated patients in a multicenter hyperthermia trial, five transurethralmicrowave thermotherapy (TUMT) trials, and a balloon dilatation versus cystoscopy trial. The improvement in per centis noted above the horizontal tickmark.
Ch 02 13/5/05 2:57 pm Page 31

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA32
confound the situation. The Proscar Long TermEfficacy and Safety Study (PLESS) followed acohort of over 3000 men with moderate symp-toms and enlarged prostate glands randomized totreatment with finasteride 5 mg daily versusplacebo over 4 years.82,83 While in most placeboarms of controlled trials lasting 12 months or lessthe combined placebo effect is maintained for theentire duration of the study, in this trial, both themean symptom score and peak flow rate slowlydrifted back to baseline after a typical initialplacebo response, without quite reaching baselinelevels, however.83
The almost 1500 men in the placebo arm ofthis trial allowed for a detailed analysis of theplacebo response and the subsequent natural his-tory stratified by baseline parameters. By far the
most powerful of these parameters proved to beunexpectedly the baseline serum PSA level.When stratifying the population by serum PSAinto tertiles or thirds of patients with PSA levelsfrom 0–1.3, 1.4–3.2, and 3.3–10 ng/ml, three dis-tinctly different patterns emerged (Figure 2.12).82
While the initial placebo response in the lowestPSA tertile for both symptom and flow rate wasmaintained over the entire 4 years of follow-up,the middle tertile experienced a slow deteriora-tion of symptoms back to baseline and in essencethe natural history and progression of diseaseeliminated any flow rate gains. In the highestPSA tertile the symptom score increased steadilyover time following an initial placebo response by–1.5 points. Over the subsequent years, the scoreincreased by 0.5 points/year, bringing it at the end
15
14
13
12
11
10
9
8
7
6
5
Qm
ax (
ml/s)
TreatmentHyp
erth
erm
ia
Sha
m
TUM
T-1
Sha
m-1
TUM
T-2
Sha
m-2
TUM
T-3
Sha
m-3
TUM
T-4
Sha
m-4
TUM
T-5
Sha
m-5
Balloon
Cys
tosc
opy
4.0%
4.0%
4.0%
4.0%
4.0%
4.0%
4.0%
4.0%
4.0%
4.0%
4.0%
4.0%
4.0%
4.0%
0.4 0.5 4.2 2.1 3.4 –0.2 4.5 0.6 4.5 2.1 2.3 –1.0 2.3 2.4
FIGURE 2.10 Pre- and posttreatment (3 months) mean peak urinary flow rates (lower and upper tickmark of verticalbar) for active-treated and sham-treated patients in a multicenter hyperthermia trial, five transurethral microwave ther-motherapy (TUMT) trials, and a balloon dilatation versus cystoscopy trial. The changes in per cent are noted below thehorizontal tickmark and the absolute improvement (deterioration) at the bottom of the graph.
Ch 02 13/5/05 2:57 pm Page 32

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 33
of the study back to the original baseline level.The initial response in terms of flow rateimprovement was completely negated by the pro-gression/natural history after 2 years, and at theend of the study, this group of patients registereda net worsening of the flow rate by a mean of–1.0 ml/s (Figure 2.12b).
For the first time, the PLESS study and itsplacebo control group allowed the study of natu-ral history and disease progression in a cohortselected for moderate symptoms and other evi-dence of disease (in contrast to a population-basedstudy) on the background of the initial combinedplacebo responses.
Relationship between placebo/sham effect andperception of improvement
Barry et al. reported an important observation byassessing the relationship between changes in the
AUASI and patients’ global rating of improve-ment in over 1200 men treated in a medical treat-ment trial for BPH.84 They noted that a meandecrease in AUASI of 3.1 points was associatedwith a slight improvement; however, this rela-tionship was strictly dependent on the baselineAUASI (Figure 2.13). For patients to perceive aslight, moderate, or marked improvement,increasing drops in AUASI were required withincreasing baseline symptom severity. In Figure2.13 this relationship is illustrated graphically forslight, moderate, and marked improvement. Thesymbols indicate the improvement in AUASInoted in the already-mentioned α-blocker trialactive-drug and placebo arms.72 It is evident, thatfor every symptom severity stratum, the improve-ment in the placebo arm fell roughly on the‘slight’ improvement line, which is the minimumimprovement noticeable to patients. Thus, for
35
30
25
20
15
10
5
AU
AS
I (0
–3
5 p
oin
ts)
Baseline symptom score
13–15P 13–15T 16–19P 16–19T 20–23P 20–23T 24–27P 24–27T 28–31P 28–31T 32–35P 32–35T
4.6% 13.7%
6.9% 17.4%
11.7% 25.1%
20.0% 30.0%
19.4% 31.4%
21.4% 36.9%
1.6 4.8 2.4 6.1 4.1 8.8 7.0 10.5 6.8 11.0 7.5 12.9
FIGURE 2.11 Improvements in symptom score expressed recorded in a placebo-controlled, 12-month α-blocker treat-ment trial for patients stratified in six baseline symptom severity strata (along x-axis labeled as P = placebo- and T = ter-azosin-treated). The per cent improvement (100% scale) and the absolute changes (at bottom of graph) are shown.
Ch 02 13/5/05 2:58 pm Page 33

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA34
each baseline symptom severity level, patientstreated with placebo would have a noticeablesymptom improvement. However, the patientstreated with active drug experienced in all strataanalyzed at least a ‘moderate’ improvement.
SUMMARY AND CONCLUSIONS
The data discussed demonstrate rather convinc-ingly that in both medical and minimally inva-sive-device treatment trials for BPH, a
placebo/sham effect must be expected, in additionto a regression to the mean effect, the magnitudeof which depends on the chosen thresholds forinclusion and exclusion (i.e. the more restrictive,the greater the effect). The combined regressionto the mean and placebo/sham effect is surpris-ingly stable across different trials and differenttreatment modalities. About 40% of patientsexperience some unspecified degree of improve-ment, albeit marginal, in watchful waiting andplacebo/sham control cohorts. Improvements insymptom severity scores range from 5 to 15%
0 4 8 12 16 20 24 28 32 36 40 44 48
0
–0.5
–1
–1.5
–2
–2.5
–3
<1.2
1.3–3.2
>3.2
(a)
Months
I-P
SS
-1.5
-1
-0.5
0
0.5
1
1.5
0 - 1.2
1.2 - 3.2
3.2 - 10
0 4 8 12 16 20 24 28 32 36 40 44 48
1.5
1
0.5
0
–0.5
–1
–1.5
0–1.2
1.2–3.2
3.2–10
(b)
Pe
ak flo
w r
ate
FIGURE 2.12 Mean ± 95% CI for symptom (a) and peak flow rate (b) in placebo-treated patients in PLESS study strat-ified by baseline serum PSA levels.
Ch 02 13/5/05 2:59 pm Page 34

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 35
(about 2 to 5 points using the AUASI ranging
from 0 to 35 points) for placebo/sham-treated
cohorts, while changes in peak urinary flow rate
are in general more modest, ranging from actual
deterioration to improvements of 1.0 ml/s with
few exceptions. The magnitude of this effect is
similar to that seen in watchful waiting studies.
Of great importance is the observation that the
magnitude of the improvement correlates direct-
ly with the baseline symptom severity. Patients’
perception of improvement also correlates with
baseline symptom severity and, in general, a larg-
er drop in symptom score is associated with a
global rating of a slight, moderate, or marked
improvement with increasing baseline symptom
score. In the limited datasets available the placebo
effect for each symptom severity stratum is of a
magnitude associated with a global perception ofslight improvement.
The statement that treatment for BPH is asso-ciated with a ‘40% placebo/sham effect’ is clearlyan inadequate oversimplification. More detailedand sophisticated analyses of responses in place-bo/sham-treated cohorts of men with BPH areneeded to further our understanding of the com-plex relationship between patients’ expectations,baseline symptom severity, bother, quality of life,nature and invasiveness of the active treatmentarm, and the responses noted in regards to symp-tom, bother, quality of life, and indirect outcomessuch as urinary flow rates. Only once a matrix ofthese responses and their predictors has beenestablished will we be able to judge newly devel-oped treatments for BPH against the backdrop oftheir associated placebo/sham effects.
5
0
–5
–10
–15
–20
0 5 10 15 20 25 30 35
AUA symptom score
slight
moderate
marked
AU
A s
ym
pto
m s
co
re im
pro
ve
me
nt
FIGURE 2.13 Relationship between baseline (x-axis) symptom score and absolute changes in scores for subjects ratingglobal improvement as slight, moderate, or marked (adapted from reference 85). The symbols indicate the absolute dropsin symptom scores from baseline for patients treated in a placebo-controlled, 12-month α-blocker treatment trial strati-fied in six strata by baseline symptom severity (placebo = triangle; α-blocker = circle).
Ch 02 13/5/05 2:59 pm Page 35
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA36
REFERENCES
1. Shaw P. The reflector: representing human affairs,as they are; and may be improved. 1750. Cited in:Drugs and Human Behavior. London: 1970
2. Hill A B. Medical ethics and controlled trials. BMed J 1963; 1: 1043–1049
3. Macedo A, Farre M, Banos J E. Placebo effect andplacebos: what are we talking about? Some concep-tual and historical considerations. Eur J ClinPharmacol 2003; 59: 337–342
4. Hrobjartsson A, Norup M. The use of placebointerventions in medical practice—a national ques-tionnaire survey of Danish clinicians. Eval HealthProf 2003; 26: 153–165
5. Pepper O H P. A note on placebo. Ann J Pharmacol1945; 117: 409–412
6. Kennedy W P. The nocebo reaction. Med Word1961; 344: 203–205
7. White L, Tursky B, Schwartz G E. Placebo in per-spective. In: White L, Tursky B, Schwartz G E(eds). Placebo. Theory, research, and mechanism.New York: The Guilford Press, 1985: 3–6
8. Shapiro A K, Morris L A. The placebo effect inmedical and psychological therapies. In: Garfield SL, Bergin A E (eds). Handbook of psychotherapyand behavior change. New York: Wiley, 1978: 371
9. Brody H. Placebos and the philosophy of medicine.Chicago: University of Chicago Press, 1977
10. Grünbaum A. Explication and implications of theplacebo concept. In: White L, Tursky B, SchwartzGE (eds). Placebo. Theory, research, and mecha-nisms. New York: The Guilford Press, 1985: 9–36
11. de la Fuente-Fernandez R, Schulzer M, Stoessl A J.The placebo effect in neurological disorders.Lancet Neurol 2002; 1: 85–91
12. Brody H. Placebo effect: an examination ofGrünbaum's definition. In: White L, Tursky B,Schwartz G E (eds). Placebo. Theory, research, andmechanisms. New York: The Guilford Press, 1985:37–58
13. Turner J A, Deyo R A, Loeser J D et al. The impor-tance of placebo effects in pain treatment andresearch. J Am Med Assoc 1994; 271: 1609–1614
14. Coronary Drug Project Research Group. Influenceof adherence to treatment and response of choles-terol on mortality in the coronary drug project. NEngl J Med 1980; 303: 1038–1041
15. Finkel M J. Placebo controls are not always neces-sary. In: White L, Tursky B, Schwartz G E (eds).Placebo. Theory, research, and mechanisms. NewYork: The Guilford Press, 1985: 419–428
16. Lepor H, Sypherd D, Machi G et al. Randomizeddouble-blind study comparing the effectiveness ofballoon dilation of the prostate and cystoscopy forthe treatment of symptomatic benign prostatichyperplasia. J Urol 1992; 147: 639–42; discussion642–644
17. Moyad MA. The placebo effect and randomizedtrials: analysis of conventional medicine. Urol ClinNorth Am 2002; 29: 125–33, ix-x
18. Rothman KJ, Michels KB. The continuing unethi-cal use of placebo controls. N Engl J Med 1994; 331:394–398
19. Zion D, Gillam L, Loff B. The Declaration ofHelsinki, CIOMS and the ethics of research on vul-nerable populations. Nat Med 2000; 6: 615–617
20. Denis L, McConnell J D, Yoshida O et al.Recommendations of the International ScientificCommittee: the evaluation and treatment of lowerurinary tract symptoms (LUTS) suggestive ofbenign prostatic obstruction. In: Denis L, GriffithsK, Khoury S et al. (eds). 4th international consulta-tion on benign prostatic hyerplasia (BPH).Plymouth: Health Publication, 1997: 669–684
21. Recommendations of the International ScientificCommittee. Evaluation and treatment of LUTS inolder men. In: Chatelain C, Denis L, Foo K T et al.(eds). 5th International Consultation on BenignProstatic Hyperplasia (BPH). Plymouth, UK:Health Publication, 2001: 519–534
22. Blackwell B, Bloomfield S S, Buncher C R.Demonstration to medical students of placeboresponses and non-drug factors. Lancet 1972; 294:1279–1282
23. Thomas K B. General practice consultations: isthere any point in being positive? Br Med J 1987;294: 1200–1202
Ch 02 13/5/05 2:59 pm Page 36

THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 37
24. Beecher H K. The powerful placebo. J Am MedAssoc 1955; 159: 1602–1606
25. Whitney C W, Von Korff M. Regression to themean in treated versus untreated chronic pain. Pain1992; 50: 281–285
26. Gracely R H, Dubner R, Deeter W R et al.Clinicians’ expectations influence placebo analge-sia. Lancet 1985; 294: 43
27. Rosenzweig P, Brohier S, Zipfel A. The placeboeffect in healthy volunteers: influence of experi-mental conditions on the adverse events profileduring phase I studies. Clin Pharmacol Therapeut1993; 54: 578–583
28. Beecher HK. Surgery as placebo. J Am Med Assoc1961; 176: 1102–1107
29. Cobb LA, Thomas GI, Dillard DH et al. An eval-uation of internal-mammary-artery-ligation by adouble-blind technic. N Engl J Med 1959; 260:115–118
30. Diamond E G, Kittle C F, Crockett J E.Comparison of internal mammary ligation andsham operation for angina pectoris. Am J Cardiol1960; 5: 483–486
31. Johnson A G. Surgery as placebo. Lancet 1994; 344:1140–1142
32. Sech S M, Montoya J D, Bernier P A et al. The so-called ‘placebo effect’ in benign prostatic hyperpla-sia treatment trials represents partially a condition-al regression to the mean induced by censoring.Urology 1998; 51: 242–250
33. Oesterling J E, Jacobsen S J, Chute C G et al.Serum prostate-specific antigen in a community-based population of healthy men. Establishment ofage-specific reference ranges [see comments]. J AmMed Assoc 1993; 270: 860–864
34. Guess H A, Chute C G, Garraway W M et al.Similar levels of urological symptoms have similarimpact on Scottish and American men—althoughScots report less symptoms. J Urol 1993; 150:1701–1705
35. Jacobsen S J, Girman C J, Guess H A et al. Naturalhistory of prostatism: factors associated with dis-cordance between frequency and bother of urinarysymptoms. Urology 1993; 42: 663–671
36. Oesterling J E, Girman C J, Panser L A et al.Correlation between urinary flow rate, voided vol-ume, and patient age in a community-based popu-lation. Prog Clin Biol Res 1994; 386: 125–139
37. Girman C J, Epstein R S, Jacobsen S J et al. Naturalhistory of prostatism: impact of urinary symptomson quality of life in 2115 randomly selected com-munity men. Urology 1994; 44: 825–831
38. Sarma A V, Wei J T, Jacobson D J et al. OlmstedCounty Study of Urinary Symptoms and HealthStatus; Flint Men's Health Study. Comparison oflower urinary tract symptom severity and associat-ed bother between community-dwelling black andwhite men: the Olmsted County Study of UrinarySymptoms and Health Status and the Flint Men'sHealth Study. Urology 2003; 61: 1086–1091
39. Sarma A V, Jacobsen S J, Girman C J et al.Concomitant longitudinal changes in frequency ofand bother from lower urinary tract symptoms incommunity dwelling men. J Urol 2002; 168:1446–1452
40. Roberts R O, Jacobson D J, Girman C J et al.Prevalence of prostatitis-like symptoms in a com-munity based cohort of older men. J Urol 2002; 168:2467–2471
41. Roberts RO, Jacobsen SJ, Rhodes T et al. Cigarettesmoking and prostatism: a biphasic association?Urology 1994; 43: 797–801
42. Jacobsen S J, Girman C J, Guess H A et al. Naturalhistory of prostatism: four-year change in urinarysymptom frequency and bother. J Urol 1995; 153:300A
43. Jacobsen S J, Girman C J, Guess H A et al. Naturalhistory of prostatism: longitudinal changes in void-ing symptoms in community dwelling men. J Urol1996; 155: 595–600
44. Rhodes T, Girman C, Jacobson D et al.Longitudinal prostate volume in a community-based sample: 7-year followup in the OlmstedCounty Study of Urinary Symptoms and HealthStatus among Men. J Urol 2000; 163: 249
45. Roberts R O, Jacobsen S J, Jacobson D J et al.Longitudinal changes in peak urinary flow rates ina community based cohort. J Urol 2000; 163:107–113
Ch 02 13/5/05 2:59 pm Page 37

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA38
46. Rhodes T, Girman C J, Jacobsen S J et al.Longitudinal measures of prostate volume in acommunity-based sample: 3.5 year followup in theOlmsted County study of health status and urinarysymptoms among men. J Urol 1995; 153: 301A
47. Rhodes T, Girman C J, Jacobsen S J et al.Longitudinal prostate growth rates during 5 yearsin randomly selected community men 40 to 79years old. J Urol 1999; 161: 1174–1179
48. Diokno A C, Brown M B, Goldstein N et al.Epidemiology of bladder emptying symptoms inelderly men. J Urol 1992; 148: 1817–1821
49. Clarke R. The prostate and the endocrines. 1919:254–271
50. Craigen A A, Hickling J B, Saunders C R et al.Natural history of prostatic obstruction. J R CollGen Pract 1969; 18: 226–232
51. Birkhoff J D, Wiederhorn A R, Hamilton M L etal. Natural history of benign prostatic hypertrophyand acute urinary retention. Urology 1976; 7: 48–52
52. Ball A J, Feneley R C, Abrams P H. The naturalhistory of untreated ‘prostatism’. Br J Urol 1981; 53:613–616
53. Kadow C, Feneley R C, Abrams P H.Prostatectomy or conservative management in thetreatment of benign prostatic hypertrophy? Br JUrol 1988; 61: 432–434
54. McConnell J D, Barry M J, Bruskewitz R C et al.Benign prostatic hyperplasia: diagnosis and treat-ment. Clinical practice guideline, number 8.Rockville, MD: Agency for Health Care Policy andResearch, Public Health Service, US Departmentof Health and Human Services, 1994
55. Eddy D M, Hasselblad V. FAST*PRO. Softwarefor meta-analysis by the confidence profile method.Boston: Academic Press, 1992
56. AUA BPH Guideline Update Panel. The manage-ment of BPH, 2003. https://shop.auanet.org/timss-net/products/guidelines/bph_management.cfm
57. Wasson J H, Reda D J, Bruskewitz R C et al. Acomparison of transurethral surgery with watchfulwaiting for moderate symptoms of benign prostat-ic hyperplasia. The Veterans’ Affairs CooperativeStudy Group on Transurethral Resection of theProstate. N Engl J Med 1995; 332: 75–79
58. O'Leary M P, Barry M J, Fowler F J Jr. Hard meas-ures of subjective outcomes: validating symptomindexes in urology. J Urol 1992; 148: 1546–1548;discussion 1564
59. Barry M J, Fowler F J Jr, O'Leary M P et al. TheAmerican Urological Association symptom indexfor benign prostatic hyperplasia. The MeasurementCommittee of the American UrologicalAssociation. J Urol 1992; 148: 1549–1557; discussion1564
60. Barry M J, Fowler F J Jr, O'Leary M P et al.Correlation of the American UrologicalAssociation symptom index with self-administeredversions of the Madsen–Iversen, Boyarsky andMaine Medical Assessment Program symptomindexes. Measurement Committee of the AmericanUrological Association. J Urol 1992; 148:1558–1563; discussion 1564
61. Schneider H, Ludwig M, Weidner W, Brahler E.Experience with different questionnaires in themanagement of patients with CP/CPPS: GPSS,IPSS and NIH-CPSI. World J Urol 2003; 21:116–118
62. Kok E T, McDonnell J, Stolk E A et al.; TriumphResearch Group; Pan-European Expert Panel. Thevaluation of the International Prostate SymptomScore (IPSS) for use in economic evaluations. EurUrol 2002; 42: 491–497
63. Porru D, Jallous H, Cavalli V et al. Prognosticvalue of a combination of IPSS, flow rate and resid-ual urine volume compared to pressure–flow stud-ies in the preoperative evaluation of symptomaticBPH. Eur Urol 2002; 41: 246–249
64. Aubrey D A, Khosla T. The effect of 17-a-hydroxy-19-norprogesterone caproate (SH582) onbenign prostatic hypertrophy. Br J Surg 1971; 58:648–652
65. Van Poppel H, Boeckx G, Westelinck K J et al. Theefficacy of bromocriptine in benign prostatic hyper-trophy. A double-blind study. Br J Urol 1987; 60:150–152
66. Lindner A, Ramon J, Brooks M E. Controlledstudy of cimetidine in the treatment of benign pro-static hypertrophy. Br J Urol 1990; 66: 55–57
67. Jardin A, Bensadoun H, Delauche-Cavallier M Cet al. Alfuzosin for treatment of benign prostatic
Ch 02 13/5/05 2:59 pm Page 38
THE PLACEBO EFFECT IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 39
hypertrophy. The BPH-ALF Group [see com-ments]. Lancet 1991; 337: 1457–1461
68. Abrams P H. A double-blind trial of the effects ofcandicidin on patients with benign prostatic hyper-trophy. Br J Urol 1977; 49: 67–71
69. Jensen KM, Madsen PO. Candicidin treatment ofprostatism: a prospective double-blind placebo-controlled study. Urol Res 1983; 11: 7–10
70. Madsen P O, Dorflinger T, Frimodt-Moeller P C etal. Candicidin in treatment of benign prostatichypertrophy. J Urol 1984; 132: 1235–1238
71. Gillenwater J Y, Conn R L, Chrysant S G et al.Doxazosin for the treatment of benign prostatichyperplasia in patients with mild to moderateessential hypertension: a double-blind, placebo-controlled, dose-response multicenter study. J Urol1995; 154: 110–115
72. Roehrborn C G, Oesterling J E, Auerbach S et al.The Hytrin Community Assessment Trial study: aone-year study of terazosin versus placebo in thetreatment of men with symptomatic benign prosta-tic hyperplasia. HYCAT Investigator Group.Urology 1996; 47: 159–168
73. Abrams P, Schulman C C, Vaage S. Tamsulosin, aselective alpha 1c-adrenoceptor antagonist: a ran-domized, controlled trial in patients with benignprostatic ‘obstruction’ (symptomatic BPH). TheEuropean Tamsulosin Study Group. Br J Urol1995; 76: 325–336
74. Lepor H, Sypherd D, Machi G et al. Randomizeddouble-blind study comparing the effectiveness ofballoon dilation of the prostate and cystoscopy forthe treatment of symptomatic benign prostatichyperplasia. J Urol 1992; 147: 639–642.
75. Abbou C C, Colombel M, Payan C et al. The effi-cacy of microwave induced hyperthermia in thetreatment of BPH: The Paris Public Hospitals’experience. In: Kurth K H, Newling D W W (eds).Benign prostatic hyperplasia. Recent progress inclinical research and practice. New York: Wiley-Liss, 1994: 449–454
76. Ogden C W, Reddy P, Johnson H et al. Sham ver-sus transurethral microwave thermotherapy inpatients with symptoms of benign prostatic bladderoutflow obstruction. Lancet 1993; 341: 14–17
77. Blute M L, Tomera K M, Hellerstein D K et al.Transurethral microwave thermotherapy for man-agement of benign prostatic hyperplasia: results ofthe United States Prostatron Cooperative Study[see comments]. J Urol 1993; 150: 1591–1596
78. de la Rosette J J, de Wildt M J, Alivizatos G et al.Transurethral microwave thermotherapy (TUMT)in benign prostatic hyperplasia: placebo versusTUMT. Urology 1994; 44: 58–63
79. Bdesha A S, Bunce C J, Snell M E et al. A shamcontrolled trial of transurethral microwave therapywith subsequent treatment of the control group. JUrol 1994; 152: 453–458
80. Roehrborn CG, Oesterling JE, Auerbach S et al.Effectiveness and safety of terazosin versus placeboin the treatment of men with symptomatic benignprostatic hyperplasia in the HYCAT study.Urology 1996; 47: 159–168
81. Gormley G J, Stoner E, Bruskewitz R C et al. Theeffect of finasteride in men with benign prostatichyperplasia. The Finasteride Study Group. N EnglJ Med 1992; 327: 1185–1191
82. Roehrborn C G, Boyle P, Bergner D et al. Serumprostate-specific antigen and prostate volume pre-dict long-term changes in symptoms and flow rate:results of a four-year, randomized trial comparingfinasteride versus placebo. PLESS Study Group.Urology 1999; 54: 662–669
83. McConnell J D, Bruskewitz R, Walsh P et al. Theeffect of finasteride on the risk of acute urinaryretention and the need for surgical treatmentamong men with benign prostatic hyperplasia.Finasteride Long-Term Efficacy and Safety StudyGroup. N Engl J Med 1998; 338 :557–563
84. Barry M J, Williford W O, Chang Y et al. Benignprostatic hyperplasia specific health status meas-ures in clinical research: how much change in theAmerican Urological Association symptom indexand the benign prostatic hyperplasia impact indexis perceptible to patients? [see comments]. J Urol1995; 154: 1770–1774
85. Barry M J, Williford W O, Chang Y C et al. BPH-specific health status measures in clinical research:how much change in AUA symptom index and theBPH impact index is perceptible to patients? J Urol1995; 154: 1770–1774
Ch 02 13/5/05 2:59 pm Page 39

Ch 02 13/5/05 2:59 pm Page 40
Dutasteride in the treatmentof the BPH patient
J D McConnell C G Roehrborn3
41
INTRODUCTION
Benign prostatic hyperplasia (BPH) and thelower urinary tract symptoms (LUTS) associatedwith the condition are becoming increasinglyprevalent as the Western male population agesand healthcare provision worldwide improves.The need for new and improved treatments forthe condition is therefore ongoing and likely toincrease.
BPH develops due to a combination of testic-ular androgens and aging. The main androgenpresent in the prostate is dihydrotestosterone(DHT). The role of DHT and the enzymeresponsible for its reduction, 5α-reductase, in thedevelopment of BPH has long been established,and the clinical potential of inhibitors of theenzyme has been proven.
Limitations of inhibitors with a selectiveaction on one of the isoforms of 5α-reductasehave been described, however. Inhibition of both5α-reductase isozymes has therefore been sug-gested as a means of increasing clinical responsein terms of reducing prostate volume and therebyimproving urinary symptoms and limiting risk ofacute urinary retention (AUR) and BPH-relatedsurgery.
The selective 5α-reductase type II inhibitorfinasteride has been available for the treatment ofBPH for over 10 years, and this is testament to itsefficacy in reducing symptoms of the condition inpatients over an extended period of time.However, dual inhibition of 5α-reductase hasbeen predicted to expand and enhance response
in both finasteride responders and nonrespon-ders.
DEVELOPMENT OF BPH AND ROLE OF DHT
The prevalence of BPH increases in a linear fash-ion alongside age. At the age of 40, approximate-ly 23% of men suffer from BPH, while 88% ofmen in their nineties are thought to have the con-dition.1
Androgen stimulation is necessary for the ini-tial growth and development of the prostate andfor the maintenance of its integrity, as well as thedevelopment of the obstructive urinary symp-toms associated with BPH.2 Although the mech-anisms underlying the development of BPH havenot been fully established, testicular androgens,particularly DHT, are recognized as integral tothe process. The influence of DHT in initial pro-static development has been determined, with thehormone found to be responsible for the embry-onic differentiation of the prostate and the forma-tion of external genitalia in the male.3 Fetal cas-tration results in inhibited formation of thegland,4 and the continued role of testicular andro-gens in later life is evidenced by the lack of BPHdevelopment among men who have undergonecastration prior to puberty.5
DHT, which is reduced by 5α-reductase fromtestosterone (Figure 3.1), has been identified asthe predominant androgen contained in theprostate,2 and its permissive if not causative role
Ch 03 13/5/05 3:02 pm Page 41

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA42
in hyperplastic prostatic growth has been out-lined in several studies.6,7
DHT binds to androgen receptors containedwithin the epithelium of the prostate.6,7 Thesereceptors are upregulated during puberty, leadingto increased androgen sensitivity and, althoughthe receptors may also bind testosterone, DHThas much greater affinity, indicating that thishormone is the main driver of subsequent genet-ic modulation in the prostate.8 Although down-regulation of many androgen receptors occursafter puberty at other sites, this does not occur inthe prostatic epithelium. Coupled with the factthat DHT levels remain constant after puberty,when testosterone levels fall, this explains thecontinued growth-promoting influence of DHTand the DHT–receptor complex in the prostate.
The formation of this complex stimulates theexpression of a range of growth factor promoters,such as epidermal growth factor (EGF), basicfibroblast growth factor, keratinocyte growth fac-tor (KGF), and insulin-like growth factor (IGF),leading to cellular proliferation,9,10 and inhibitors,such as transforming growth factor-β (TGF-β),which increases levels of apoptosis.11–13
Homeostasis is therefore achieved by the normal-ly functioning prostate. Increased stimulation byDHT leads to increased expression of growth fac-
tor promoters and hyperplastic growth. Removalof the stimulus, through surgical or chemicalmeans, leads to the opposite scenario, with a gen-eral move towards increased expression of cellgrowth inhibitors, such as TGF-β.
A lack of DHT, due to deficiency of theenzyme responsible for its formation from testos-terone, i.e. 5α-reductase, has been identified inmen with pseudohermaphroditism.14,15 The clin-ical and pathologic sequelae observed in theseindividuals provide further evidence of the role ofandrogens, specifically DHT, in the prostate.Men affected by 5α-reductase deficiency experi-ence normal or partial virilization at puberty, dueto the action of testosterone; however, the prostateitself remains underdeveloped, small, and unpal-pable on digital rectal examination.
The normal development of the prostate, andits hyperplastic growth during BPH, are there-fore predominantly attributed to the reduction oftestosterone to DHT by 5α-reductase.
5α-REDUCTASE
The increased cell proliferation that takes placeduring hyperplastic prostatic growth mainlyoccurs in the stroma of the prostate and a strong
OH
O
OH
O
H
Testosterone Dihydrotestosterone
e
type 1 and typeType 1 and type 2
5α-reductase
NADPH NADP+
FIGURE 3.1 Reduction of testosterone to dihydrotestosterone by 5α-reductase.
Ch 03 13/5/05 3:03 pm Page 42

DUTASTERIDE IN THE TREATMENT OF THE BPH PATIENT 43
positive association of 5α-reductase activity withstroma and a negative correlation with epitheli-um has been recently identified.16
Two isozymes of the highly lipophilic enzyme5α-reductase have been identified to date. Theseproteins are encoded by different genes, that fortype I being located on chromosome 5 and thatfor type II on chromosome 2.17 The distributionof the 5α-reductase isozymes differs significantly,with type I predominating in the liver, scalp, andskin, with low levels found in the prostate, whiletype II mainly occurs in the prostate and othergenital tissues and is found to a lesser extent else-where.2
The 5α-reductase deficiency observed inpseudohermaphroditic men involves type II 5α-reductase alone; type I 5α-reductase deficiencyhas not been identified to date in humans. In 5α-reductase deficient men, virilization at puberty isaccompanied by increased expression of 5α-reductase type I in the skin,18 suggesting thatDHT has paracrine effects, and that dual inhibi-tion is necessary for complete control of the hor-mone. It may also explain why finasteride, whichinhibits the action of type II 5α-reductase alone,only succeeds in reducing prostatic DHT by85–90% and often fails to significantly reduce theurinary symptoms of BPH.19,20
THE NEED FOR A DUAL 5α-REDUCTASEINHIBITOR
The efficacy of the type II 5α-reductase inhibitor,finasteride, has been described in several short-and long-term clinical trials.21–25 Mainly througha reduction in prostate volume, the drug has beenshown to significantly reduce risk of AUR andBPH-related surgery and improve urinary symp-toms and peak urinary flow (Qmax) in both
younger and older men, with positive conse-quences for quality of life scores. Since its launchin 1992, the drug has been used to treat millionsof men worldwide, with good reported success inresponders.
Stratification of the results of clinical trials hassuggested that men with larger prostates aremore likely to respond to finasteride therapy thanthose with smaller glands.26 A meta-analysis ofsix clinical trials indicated that significantlygreater improvements in Qmax and symptom scorewere experienced by men with prostates largerthan 60 ml compared to those with prostates of20 ml or smaller. The authors concluded thatfinasteride was most appropriate for men withprostates of 40 ml or greater. Severity of symp-toms does not necessarily correlate with prostatevolume, however,27 and the effects of a greaterreduction in prostate volume than that seen withfinasteride have yet to be determined.
It has been suggested that finasteride fallsshort of initial expectations due to the simultane-ous occurrence of BPH with symptoms unrelatedto prostatic growth,28 heterogeneity of the dis-ease,29 and the effect of the increase in levels oftestosterone8 as well as the influence of the DHTthat continues to circulate despite 5α-reductasetype II inhibition, i.e. that originating from type Ireduction. Between 20 and 40% of baseline DHTremains in men treated with finasteride.30–32
The exact role of DHT reduced by type I 5α-reductase is not known and the level of entry ofthis protein to the prostate has not been estab-lished. Therefore, even though finasteride suc-cessfully reduces levels of DHT in the prostate, itcan be postulated that systemic DHT maintainslevels high enough to allow continued cell prolif-eration or negate the normal ongoing apoptosis ofprostatic cells. On this basis, obstructive urinarysymptoms may therefore persist, particularly in
Ch 03 13/5/05 3:03 pm Page 43

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA44
men with smaller prostates. A dual inhibitor ofboth 5α-reductase isoforms, producing greaterreductions in prostatic and circulating DHT,would reduce this possibility.
Over the last decade, the principle of 5α-reductase inhibition in terms of reducing prostatevolume and thereby alleviating symptoms hasbeen shown to have considerable clinical benefit;however, selective inhibition of one isozyme alonemay limit the magnitude of the clinical response.
PRECLINICAL DEVELOPMENT OFDUTASTERIDE
The assumption that inhibition of both type I andtype II 5α-reductase could improve the urinarysymptoms of BPH over and above mono-inhibi-tion with finasteride led to the development ofthe 6-azasteroid molecule 17β-N-(2,5-bis(trifluoro-methyl) phenylcarbamoyl)-4-aza-5α-androst-1-en-3one (dutasteride, Figure 3.2).
A range of dual 5α-reductase inhibitors wasdeveloped simultaneously;33 however, dutasteridewas found to have a particularly high affinity forboth 5α-reductase isozymes. In vitro, the com-pound was 60 times more powerful at inhibiting
type I 5α-reductase and 10 times more powerfulat inhibiting type II 5α-reductase than finas-teride.34 Trials of the drug in humans revealedtype I inhibition to be 100-fold higher and type IIinhibition 3-fold higher than finasteride.35
Investigation of dutasteride’s mechanism ofinhibition in rats revealed that the drug affectstype I 5α-reductase differently to type II.36 Thedrug inhibits type I 5α-reductase in a classicallycompetitive manner, forming a dissociable com-plex with this isozyme. In contrast, the inhibitionof type II 5α-reductase is time-dependent. In thisanalysis, which compared the actions of finas-teride and dutasteride in rats, the latter was foundto be 20 times as powerful an inhibitor as finas-teride of 5α-reductase type I, and 10 times aspowerful with type II.
Previous studies in rats have indicated thatfinasteride acts as a dual inhibitor of 5α-reductasein these animals, so the beneficial effects of thedrug may in fact be overestimated.37 However,this model allows the direct comparison of finas-teride and dutasteride in terms of overall potency.
An additional animal study of dutasterideindicated that its half-life is considerably longerthan that of finasteride. Examination of the phar-macokinetic and pharmacodynamic properties ofdutasteride revealed a greater terminal half-lifecompared to finasteride, at 14 hours versus 1 hourin the rat, and 65 hours versus 4 hours in the dog.Total body clearance in the dog was found to be0.5 mg/min per kg and volume of distributionwas high, at 3 liters/kg. In man, a single dose wasfound to have a terminal half-life of around 240hours. Levels of DHT were found to be reducedto a significantly greater level after a 10 mg doseof dutasteride compared to a 5 mg dose of finas-teride.38
The extended half-life of dutasteride, in addi-tion to its dual-inhibitor nature and decreased
O
O
H
H
H
H
N
N
F
F F
F F
F
FIGURE 3.2 Structure of dutasteride.
Ch 03 13/5/05 3:03 pm Page 44

DUTASTERIDE IN THE TREATMENT OF THE BPH PATIENT 45
total body clearance, is considered to underpinthe greater inherent potency of this drug com-pared to selective 5α-reductase inhibitors.38
CLINICAL EXPERIENCE WITH DUTASTERIDE
Clinical experience involving dutasteride is rela-tively limited due to its recent availability on themarket, and comparison studies are lacking.What evidence there is, however, indicates thatthe drug consistently reduces prostate volume,improves urinary symptoms and Qmax, andreduces risk of AUR and BPH-related surgery.39
The pooled analysis of three phase III ran-domized, placebo-controlled studies of dutas-teride, each lasting 24 months, has substantiatedthe potential of the drug in the treatment ofLUTS in BPH patients.
A total of 4325 men aged over 50 with moder-ate to severe symptoms of BPH (AmericanUrological Association symptom index(AUASI) ≥ 12, Qmax ≤ 15 ml/s, prostate volume≥ 30 ml, as measured using transurethral ultra-
sound) took part in the trials, which took place at400 sites in 19 countries. After a 1-month placeborun-in period, participants were randomized toreceive 0.5 mg dutasteride or placebo.Assessment, involving AUASI, Qmax, and PSAmeasurement, took place at 1, 3, 6, 12, 18, and 24months and testosterone and DHT levels weremeasured at 12 and 24 months. Total prostate vol-ume was assessed at regular intervals and transi-tion zone volume was determined in two of thetrials.
In total, 68% (2951) of participants completedthe 24-month study period, with discontinuationrates similar between the active and placebogroups (n = 657 and n = 717, respectively). DHTlevels fell by a mean of 90.2% in the active groupcompared to a mean increase of 9.6% in theplacebo group (Figure 3.3).
Prostate volume fell significantly compared toplacebo after just 1 month and this differenceincreased over the course of the study period.
Total prostate volume fell by a mean of 25.7%and transition zone volume by 20.4% from base-line in the active groups; AUASI fell by 4.5 points
�������������� �
����
���
�
��
����
����
����
����
�������������������
��������������
������
����� ���
�����������������
������!�
�������
FIGURE 3.3 Changes in efficacy parameters at 24 months (expressed as a percentage change of baseline measurements,all changes for dutasteride are statistically significant (p < 0.001) versus placebo).
Ch 03 13/5/05 3:03 pm Page 45

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA46
compared to 2.3 points with placebo, reachingsignificance in the pooled results after 6 months;Qmax increased by 2.2 ml/s compared to 0.6 ml/swith placebo, with a significant differencebetween active and placebo arms after 3 months;PSA increased by 15.8% in the placebo group anddecreased by 52.4% with dutasteride.
AUR occurred in less than half the number ofdutasteride-treated patients compared to placebo(39 versus 90), representing a reduction in risk of57% (p = 0.001). BPH-related surgery was per-formed in 47 and 89 patients, respectively, indi-cating a reduction in risk of 48% (p = 0.001) withdutasteride.
Adverse event rates were similar betweengroups, at 77% for dutasteride-treated patientsand 75% in those receiving placebo. Drug-relatedadverse event rates were 14% and 19%, respec-tively, with sexual dysfunction being the mostcommonly reported in both groups (Figure 3.4).Prostate cancer was identified in 1.9% and 1.1%of the groups, respectively.
The results indicate that impressive clinicalbenefits are associated with dual 5α-reductase
inhibition. Comparison of these results with thosereported for other types of medical therapy forBPH indicates that the improvement in symptomscore for dutasteride described here comparesfavorably with that reported for finasteride andmany α-blockers.20,40 A review of the differentmedical treatments available for the managementof BPH revealed symptom improvements com-pared to placebo of 9–40% for alfuzosin, 2–34%for terazosin, 3–19% for doxazosin, and 2–20%for tamsulosin.41 In the study described above, animprovement of 13% over placebo was observed,indicating similar results compared to these alter-native therapies.
The decrease in risk of AUR and BPH-relat-ed surgery adds an additional dimension to thebenefits of dutasteride; 23% of men surviving to80 years are likely to suffer AUR and BPH-relat-ed surgery is needed in 29% of all men.42,43 Thereduction in risk observed here is thereforeextremely significant. Similar results have beenshown for finasteride,22 indicating the influenceof 5α-reductase inhibitors on this aspect of BPH.
�������������� �
��������� "������� �� #$���������� %&��������$������
�
'
(
)
*
��
����
����
���+���������
FIGURE 3.4 Sexual dysfunction adverse events: incidence (percentage of patients) over the entire study (2 years).Statistically significant for all disorders (p < 0.001), dutasteride versus placebo.
Ch 03 13/5/05 3:03 pm Page 46

DUTASTERIDE IN THE TREATMENT OF THE BPH PATIENT 47
Direct clinical comparisons of dutasteridewith finasteride are lacking, due to the recentrelease of the former drug. However, a phase IIclinical trial, involving 399 BPH patients (meanage 62.6–65.6 across treatment group, meanprostate volume 41.9–47.3 ml) did compare avariety of doses of dutasteride (0.01, 0.05, 0.5, 2.5,and 5.0 mg) to 5 mg finasteride or placebo over aperiod of 24 weeks.44 A clear dose–response rela-tionship was observed with dutasteride, with98.4 ± 1.2% DHT reduction observed with thehighest dose compared to a mean decrease of70.8 ± 18.3% with 5.0 mg finasteride (Figure 3.5).Significantly greater decreases in DHT wereobserved at dutasteride doses of 0.5, 2.5 and5.0 mg compared to both placebo (p = 0.001) andfinasteride (p = 0.001). If, as thought, the reduc-tion in DHT is the mechanism responsible for theimprovement in symptoms seen with finasteride,it may be expected that a greater fall in DHTwould be accompanied by greater improvementsin symptomatology.
OTHER CONSIDERATIONS
Prostate-specific antigen
The reductions in prostate-specific antigen (PSA)levels observed with finasteride therapy havebeen mirrored in clinical trials of dutasteride,39
and it has been suggested that this may haveimplications for prostate cancer screening.However, in vivo studies have shown that com-plexed-to-total and free-to-total ratios remainconstant with finasteride treatment, indicatingthat proportional reduction in all molecularforms of PSA occurs with 5α-reductase inhibi-tion.45–47 If similar results are found for dutas-teride, measurement of these PSA forms couldpotentially be used to screen for prostate cancerand the use of PSA in cancer screening would notbe compromised.
In addition, investigation of PSA levels inmen included in phase III trials of dutasteriderevealed reductions in PSA of around 50%.Multiplication of these scores by 2 showed levels
,����������������������� �
�������!� ������������������-���
-��
�
��
����
����
����
����
FIGURE 3.5 Comparative changes in serum DHT and testosterone following 24 weeks’ treatment with dutasteride(0.5 mg), finasteride (5 mg), or placebo (serum DHT suppression significant for dutasteride versus finasteride, p < 0.001).
Ch 03 13/5/05 3:03 pm Page 47

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA48
of PSA that were superimposable on curvesobserved at baseline, suggesting that this simplemethod could allow continued screening usingtotal PSA levels. Again, free-to-total ratio did notchange in these patients.
Hematuria
Finasteride and other anti-androgens have beenshown to have potential clinical applications inthe prevention of hematuria,48–50 possibly due todecreased expression of vascular endothelialgrowth factor (VEGF), which lowers microvesseldensity in the prostatic suburethra.51,52 It may bepostulated that the decrease in VEGF will begreater following dutasteride treatment, indicat-ing an even greater anti-hematuric effect; how-ever, such aspects remain to be investigated.
Combination therapy
The combination of 5α-reductase inhibitors andα-blockers has recently been investigated,53 andthe addition of doxazosin to 5α-reductase thera-py was found to result in significantly greaterbenefits in terms of disease progression andsymptom score than either treatment alone. Thegreater efficacy of dutasteride in terms of DHTreduction suggests that the combination of an α-blocker with this drug may hold even morepromise. However, long-term, randomized,placebo-controlled trials are needed to investigatethis theory.
CONCLUSIONS
The results of pharmacokinetic, pharmacody-namic, and clinical studies have indicated thatdutasteride is the most powerful suppressor ofDHT on the market. The drug effectively
inhibits type II 5α-reductase activity to a greaterextent than finasteride, with the additional bene-fit of completely inhibiting type I 5α-reductase.The net effect is a reduction in prostatic and cir-culating DHT to virtually zero. Greater reduc-tions in prostate volume may therefore be expect-ed with dual 5α-reductase inhibition than withselective inhibition, with positive clinical conse-quences with respect to urinary symptoms, AUR,BPH-related surgery risk and quality of life.
Dutasteride therefore builds on the well-documented long-term safety and tolerance of5α-reductase inhibitors, but potentially couldprovide additional clinical benefit to thatobserved with finasteride due to more effectiveDHT suppression.
However, a direct comparison of finasterideand dutasteride is now needed to determine therelative clinical benefits of selective and dualisozyme inhibitors as monotherapy or in combi-nation with other classes of drug.
REFERENCES
1. Berry S J, Coffey D S, Walsh P C, Ewing L L. Thedevelopment of human benign prostatic hyperpla-sia with age. J Urol 1984; 132: 474–479
2. Lee C, Kozlowski J M, Grayhack J T. Aetiology ofbenign prostatic hyperplasia. Urol Clin N Am1995; 22: 237–246
3. Wilson J D. Androgens. In: Hardman J G,Limbird L E (eds). Goodman & Gilman’s Thepharmacological basis of therapeutics, 10th edn.New York: McGraw-Hill, 2001: 1441–1458
4. Cunha G R, Donjacour A M, Cooke P S et al. Theendocrinology and developmental biology of theprostate. Endocr Rev 1987; 8: 338–362
5. Wu C P, Gu F L. The prostate in eunuchs. EORTCGenitourinary Group Monograph 10. Urologiconcology: reconstructive surgery, organ preservation
Ch 03 13/5/05 3:03 pm Page 48

DUTASTERIDE IN THE TREATMENT OF THE BPH PATIENT 49
and restoration of function. New York: Wiley-Liss,1992; 249–255
6. Walsh P C, Hutchins G M, Ewing L L. Tissue con-tent of dihydrotestosterone in human prostatichyperplasia is not supranormal. J Clin Invest 1983;72: 1772–1777
7. Traish A M, Wotiz H H. Prostatic epidermalgrowth factor receptors and their regulation byandrogens. Endocrinology 1987; 121: 1461–1467
8. Grino P B, Griffin J E, Wilson J D. Testosterone athigh concentrations interacts with the humanandrogen receptor similarly to dihydrotestosterone.Endocrinology 1990; 126: 1165–1172
9. Saez C, Gonzalez-Baena A C, Japon M A et al.Expression of basic fibroblast growth factor and itsreceptors FGFR1 and FGFR2 in human benignprostatic hyperplasia treated with finasteride.Prostate 1999; 40: 83–88
10. Crescioli C, Villari D, Forti G et al. Des (1–3) IGF-I-stimulated growth of human stromal BPH cells isinhibited by a vitamin D(3) analogue. Mol CellEndocrinol 2002; 198: 69–75
11. Farnsworth W E. Prostate stroma: physiology.Prostate 1999; 38: 60–72
12. Niu Y, Xy Y, Zhang J et al. Proliferation and dif-ferentiation of prostatic stromal cells. BJU Int 2001;87: 386–393
13. Kim I Y, Zelner D J, Sensibar J A et al. Modulationof sensitivity to transforming growth factor-beta 1and the level of type II TGF-β receptor in LNCaPcells by dihydrotestosterone. Exp Cell Res 1996;222: 103–110
14. Walsh P C, Madden J D, Harrod M J et al. Familialincomplete male pseudohermaphroditism, type 2:decreased dihydrotestosterone formation inpseudovaginal perineoscrotal hypospadias. N EnglJ Med 1974; 291: 944–949
15. Imperato-McGinley J, Guerrero L, Gautier T,Peterson R E. Steroid 5α-reductase deficiency inman: an inherited form of male pseudohermaphro-ditism. Science 1974; 186: 1213–1215
16. Sherwood J B, McConnell J D, Vazquez D J et al.Heterogeneity of 5 alpha-reductase gene expression
in benign prostatic hyperplasia. J Urol 2003; 169:575–579
17. Russell D W, Wilson J D. Steroid 5α-reductase:two genes/two enzymes. Annu Rev Biochem 1994;63: 25–61
18. Thipen A E, Silver R I, Guileyardo J M et al. Tissuedistribution and ontogeny of steroid 5α-reductaseisozyme expression. J Clin Invest 1993; 92: 903–910
19. Bartsch G, Rittmaster R S, Klocker H. Dihydro-testosterone and the concept of 5 alpha-reductaseinhibitors in human benign prostatic hyperplasia.Eur Urol 2000; 37: 367–380
20. Lepor H, Williford W O, Barry M J et al. for TheVeterans’ Affairs Cooperative Studies BenignProstatic Hyperplasia Study Group. The efficacy ofterazosin, finasteride or both in benign prostatichyperplasia. N Engl J Med 1996; 335: 533–540
21. McConnell J D, Bruskewitz R, Walsh P et al. forthe Finasteride Long-term Efficacy and SafetyStudy Group. The effect of finasteride on the riskof acute urinary retention and the need for surgicaltreatment among men with benign prostatic hyper-plasia. N Engl J Med 1998; 338: 557–563
22. Roehrborn C G, Bruskewitz R, Nickel G C et al.Urinary retention in patients with finasteride orplacebo over 4 years. Characterization of patientswith ultimate outcomes. The PLESS Study Group.Eur Urol 2000; 37: 528–536
23. Vaughan D, Imperato-McGinley J, McConnell J etal. Long-term (7 to 8-year) experience with finas-teride in men with benign prostatic hyperplasia.Urology 2002; 60: 1040–1044
24. Ekman P and the Scandinavian Finasteride StudyGroup. Maximum efficacy of finasteride isobtained within 6 months and maintained over 6years: follow-up of the Scandinavian Open-Extension Study. Eur Urol 1998; 33: 312–317
25. Lam J S, Romas N A, Lowe F C. Long-term treat-ment with finasteride in men with symptomaticbenign prostatic hyperplasia: 10-year follow-up.Urology 2003; 61: 354–358
26. Boyle P, Gould A L, Roehrborn C G. Prostate vol-ume predicts outcome of treatment of benign pro-static hyperplasia with finasteride: meta-analysis of
Ch 03 13/5/05 3:03 pm Page 49

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA50
randomized clinical trials. Urology 1996; 48:398–405
27. Christensen M M, Bniskewitz R C. Clinical mani-festations of benign prostatic hyperplasia and indi-cations for therapeutic intervention. Urol ClinNorth Am 1990; 17: 509–516
28. Barry M J, Cockett A T K, Holtgrewe H L et al.Relationship of symptoms of prostatism to com-monly used physiological and anatomical measureof the severity of benign prostatic hyperplasia. JUrol 1993; 150: 351–358
29. Shapiro E, Becich M G, Hartanto V, Lepor H. Therelative proportion of stromal and epithelial hyper-plasia is related to the development of symptomaticbenign prostatic hyperplasia. J Urol 1992; 147:1293–1297
30. Gormley G L, Stoner E, Rittmaster R S et al.Effects of finasteride (MK-906), a 5α-reductaseinhibitor, on circulating androgens in male volun-teers. J Clin Endocrinol Metab 1990; 70: 1136–1141
31. Ohtawa M, Morikawa H, Shimazaki J.Pharmacokinetics and biochemical efficacy aftersingle and multiple oral administration of N-(2-methyl-2-propyl)-3-oxo-4-aza-5-alpha-androst-1-ene-17-beta-carboxamide, a new type of specificcompetitive inhibitor of testosterone 5 alpha-reduc-tase, in volunteers. Eur J Drug MetabPharmacokinet 1991; 16: 15–21
32. De Schepper P J, Imperato-McGinley J, VanHecken A et al. Hormonal effects, tolerability, andpreliminary kinetics in men of MK-906, a 5 alpha-reductase inhibitor. Steroids 1991; 56: 469–471
33. Frye S V. Inhibitors of 5 alpha-reductase. CurrPharm Design 1996; 2: 59–84
34. Tian G, Mook R A, Moss M L, Frye S V.Mechanism of time-dependent inhibition of 5alpha-reductases by ∆1 4-azasteroids: towards per-fection of rates of time-dependent inhibition byusing ligand-binding energies. Biochemistry 1995;34: 13453–13459
35. Clark R V, Hermann D J, Gabriel H et al. Effectivesuppression of dihydrotestosterone (DHT) in menby GI198745: a novel dual 5 alpha-reductaseinhibitor. Abstract S1737. J Urol 1999; 164 (Suppl4): 268
36. Stuart J D, Lee F W, Noel D S et al.Pharmacokinetic parameters and mechanisms ofinhibition of rat type 1 and 2 steroid 5 alpha-reduc-tases: determinants for different in vivo activities ofGI198745 and finasteride in the rat. BiochemPharmacol 2001; 62: 933–942
37. Levine A C, Wang J P, Ren M et al. Immuno-histochemical localization of steroid 5α-reductasein human male fetal reproductive tract and adultprostate. J Clin Endocrinol Metab 1996; 81:384–389
38. Bramson H N, Hermann D, Batchelor K W et al.Unique preclinical characteristics of GG745, apotent dual inhibitor of 5AR. J Pharmacol ExpTher 1997; 282: 1496–1502
39. Roehrborn C G, Boyle P, Nickel J C et al. on behalfof the ARIA3001, ARIA3002 and ARIA3003 StudyInvestigators. Efficacy and safety of a dual inhibitorof 5 alpha-reductase types 1 and 2 (dutasteride) inmen with benign prostatic hyperplasia. Urology2002; 60: 434–441
40. Kirby R, Boyle P, Roehrborn C. Results of PRE-DICT (Prospective Randomized EuropeanDoxazosin and Combination) study of medicaltherapy for BPH (abstract). Br J Urol 1999; 83: 83
41. Clifford F, Farmer R. Medical therapy for benignprostatic hyperplasia: a review of the literature. EurUrol 2000; 38: 2–19
42. Boyle P. Some remarks on the epidemiology ofacute urinary retention. Arch Ital Urol NefrolAndrol 1998; 70: 77–82
43. Glynn R J, Campion E W, Bouchard G R et al. Thedevelopment of benign prostatic hyperplasiaamong volunteers in the Normative Aging Study.Am J Epidemiol 1985; 121: 78–90
44. Clark R, Hermann D, Gabriel H et al. Effectivesuppression of dihydrotestosterone (DHT) byGI198745, a novel, dual 5 alpha-reductase inhibitor.J Urol 1999; 161: 1037
45. Espana F, Martinez M, Royo M et al. Changes inmolecular forms of prostate-specific antigen duringtreatment with finasteride. Br J Urol Int 2002; 90:672–677
Ch 03 13/5/05 3:03 pm Page 50

DUTASTERIDE IN THE TREATMENT OF THE BPH PATIENT 51
46. Brawer M K, Lin D W, Williford W O et al. Effectsof finasteride and/or terazosin on serum PSA:results of VA Cooperative Study #359. Prostate1999; 39: 234–239
47. Tarle M, Kraus O, Trnski D et al. Early diagnosisof prostate cancer in finasteride treated BPHpatients. Anticancer Res 2003; 23: 693–696
48. Kashif K M, Foley S J, Basketter V, Holmes S A.Haematuria associated with BPH—natural historyand a new treatment option. Prostate CancerProstatic Dis 1998; 1: 154–156
49. Perimenis P, Gyftopoulos K, Markou S, BarbaliasG. Effects of finasteride and cyproterone acetate onhematuria associated with benign prostatic hyper-plasia: a prospective, randomized, controlled study.Urology 2002; 59: 373–377
50. Kearney M C, Bingham J B, Bergland R et al.Clinical predictors in the use of finasteride for con-
trol of gross hematuria due to benign prostatichyperplasia. J Urol 2002; 167: 2489–2491
51. Pareek G, Shevchuk M, Armenakas N A et al. Theeffect of finasteride on the expression of vascularendothelial growth factor and microvessel density:a possible mechanism for decreased prostatic bleed-ing in treated patients. J Urol 2003; 169: 20–23
52. Haggstrom S, Torring N, Moller K et al. Effects offinasteride on vascular endothelial growth factor.Scand J Urol Nephrol 2002; 36: 182–187
53. McConnell JD, Roehrborn CG, Bautista OM et al.Medical Therapy of Prostatic Symptoms (MTOPS)Research Group. The long-term effect of doxa-zosin, finasteride, and combination therapy on theclinical progression of benign prostatic hyperplasia.N Engl J Med 2003; 18; 349: 2387–2398
Ch 03 13/5/05 3:03 pm Page 51

Ch 03 13/5/05 3:03 pm Page 52

Finasteride in the treatment of benign prostatic hyperplasia
J D McConnell4
53
INTRODUCTION
The androgen dependency of the prostate isresponsible both for the development of benignprostatic hyperplasia (BPH) in older men and thereduction in symptoms associated with finas-teride therapy. Dihydrotestosterone (DHT),which is converted from testosterone by two 5α-reductase isozymes, accounts for around 90% ofall intraprostatic androgens. Finasteride is aninhibitor of the type II isozyme of 5α-reductase,which effectively reduces testosterone conversionto DHT in the prostate and thereby improves theurinary symptoms associated with BPH.
The use of finasteride since its approval over adecade ago is supported by a wealth of clinicalexperience, with long-term studies indicatingthat the drug not only prevents acute urinaryretention (AUR) but may delay the need for inva-sive therapy indefinitely or negate it altogether inresponders.
It has been suggested that men with largerprostates are more likely to respond to treatmentwith finasteride than those with smaller glands.Reductions in libido and other sexual effects havealso been reported in a minority of patients, andthe reduction in prostate-specific antigen (PSA)levels may also have a bearing on the use of thedrug. The clinical relevance of these assumptionswill be examined in this chapter.
BPH affects the majority of older Westernmen and, as the age of the general populationincreases and improvements in healthcare provi-sion occur in the developing world, the preva-
lence of this disease will grow. Pharmacologictreatments with a range of mechanisms of actionare therefore desirable. Effective patient selectionand the use of finasteride as monotherapy or incombination with other preparations also ensurethe continued place of the drug in the armory ofanti-BPH agents.
DHT AND 5α-REDUCTASE
The prostate is highly dependent on testicularandrogens for its development and functionalintegrity. BPH develops in older men as a func-tion of sensitivity to these testicular androgens,specifically DHT.1 Serum and prostatic DHTlevels remain stable, unlike testosterone, whichfalls over time.
The role that androgens play in hyperplasticand normal prostatic growth is governed by thelevels of DHT that bind to androgen receptorswithin the epithelium of the prostate. This com-plex plays a critical role in stimulating androgen-mediated prostatic growth.2,3 The characteristicreduction in androgen-dependent growthobserved with aging in some other tissues doesnot occur in the prostate.4
Testosterone is reduced to DHT through theaction of 5α-reductase. Two forms of this enzymehave been identified: type I, which is found ingreater proportions in the skin and liver, and typeII, which is the predominant isozyme containedin the prostate.1
Ch 04 13/5/05 3:09 pm Page 53

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA54
The role of DHT and, by definition, the pro-tein responsible for its reduction, in the develop-ment of BPH was determined following the iden-tification of 5α-reductase deficiency in a group ofindividuals with pseudohermaphroditism5–7.Virilization occurred at puberty in these individ-uals, although their prostates remained non-palpable, and male sexuality was in evidencealongside normal muscular composition. This,plus the observation that men with castrate levelsof testosterone do not develop BPH and havevery low levels of DHT, indicated that blockadeof prostate-specific androgens could reduce thesize of the prostate, thereby relieving obstructiveurinary symptoms with limited adverse sexual orphysical implications.
THE DEVELOPMENT OF FINASTERIDE
The above observations led to the development ofsynthetic 4-azasteroid α-reductase inhibitors.These agents were designed to reduce levels oftype II 5α-reductase, the isozyme that predomi-nates in the prostate (Figure 4.1).
One compound, N-(2-methyl-2-propyl)-3-oxo-4-aza-5-α-androst-1-ene-17-β-carboxamide(finasteride), was found to reduce levels of DHT
in the canine prostate and reduce prostatic vol-ume by up to 64%.8 Further studies showed thattestosterone levels were unaffected by the drug,indicating that sexual function should bemaintained.9,10
As anticipated, intraprostatic testosterone lev-els were elevated, however, and serum and pro-static DHT were not completely inhibited, due toformation via the uninhibited type I 5α-reduc-tase.11
MODE OF ACTION
Finasteride, which reduces serum DHT byaround 70% and prostatic DHT by 85–90%(Figure 4.2),12 is thought to act predominantly onthe epithelium of the prostate, exerting its benefi-cial clinical effect by altering prostatic tissue com-position and inhibiting cell proliferation.13–16 A
O
O
NHt-BU
H H
H
H
N
FIGURE 4.1 Structure of finasteride.
T T DHT
DHTARAR
DNA
5α
T
Finasteride
FIGURE 4.2 Action of finasteride. Free testosterone (T),predominantly manufactured by the testes, enters theprostate where it binds to an androgen receptor (AR) or isconverted to dihydrotestosterone (DHT) by 5α-reductase(5α). DHT will also bind to the androgen receptor, with agreater affinity than testosterone. T or DHT then influ-ences DNA transcription.
Ch 04 13/5/05 3:09 pm Page 54

FINASTERIDE IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 55
24- to 30-month open-label extension study offinasteride in a group of 19 men whose prostateswere assessed by magnetic resonance imaging(MRI) and biopsy revealed a reduction in symp-toms, PSA, DHT, and prostate volume after 6months.14 The percentage of prostate volumeattributed to epithelium shrank significantlyfrom 19.2% to 12.5% at intermediate follow-upand to 6.4% at long-term follow-up. Changes inthe transforming growth factor beta (TGFβ) sig-naling system, in terms of upregulation of TGFβsignaling receptors and a subsequent increase inepithelial apoptosis, may be instrumental in thisprocess.
The inhibition of prostatic cell proliferationhas been demonstrated in several studies.15,16
Stromal and epithelial prostate cells from hyper-plastic and normal glands treated in vitro withfinasteride in the presence of labeled thymidinerevealed that normal stromal cells incorporatedmore thymidine than epithelial cells. Finasteridetreatment resulted in 80 ± 3% and 55 ± 10%thymidine incorporation in stromal and epithelialcells, respectively, while rates of 70 ± 4% and74 ± 4% were observed in hyperplastic tissue.
Measurement of 5α-reductase activity showedthat type II activity was reduced 100-fold whiletype I activity was reduced 5-fold, demonstratingthe selectivity of finasteride for the formerisozyme.16 The incomplete inhibition of cell pro-liferation observed indicates the action of factorsother than DHT in prostate cell proliferation,however.15
Locally produced growth factors, such as basicfibroblast growth factor (bFGF), insulin-likegrowth factor (IGF), and keratinocyte growthfactor (KGF), may also have an impact on prosta-tic enlargement,17,18 stimulating an increase inlevels of mitosis in the prostatic stroma (Figure4.3). Analysis of bFGF expression and that offibroblast growth factor receptor types 1 and 2(FGFR1, FGFR2) in finasteride-treated anduntreated BPH patients revealed strong bFGFimmunoreactivity in the stroma and weakerimmunoreactivity in the epithelium of theuntreated patients, and virtually no immunoreac-tivity in the epithelium and lower stromalimmunoreactivity in finasteride-treated patients.This suggests that finasteride treatment leads todownregulation of bFGF activity, thereby limit-
Basal
Secretory
Epithelial
compartment
Stromal
compartment
DHT
Paracrine interactions: stimulation/inhibition
bFGF
KGF
IGF
TGFβ
…
FIGURE 4.3 Locally produced growth factors influence prostatic cell proliferation and apoptosis.
Ch 04 13/5/05 3:09 pm Page 55
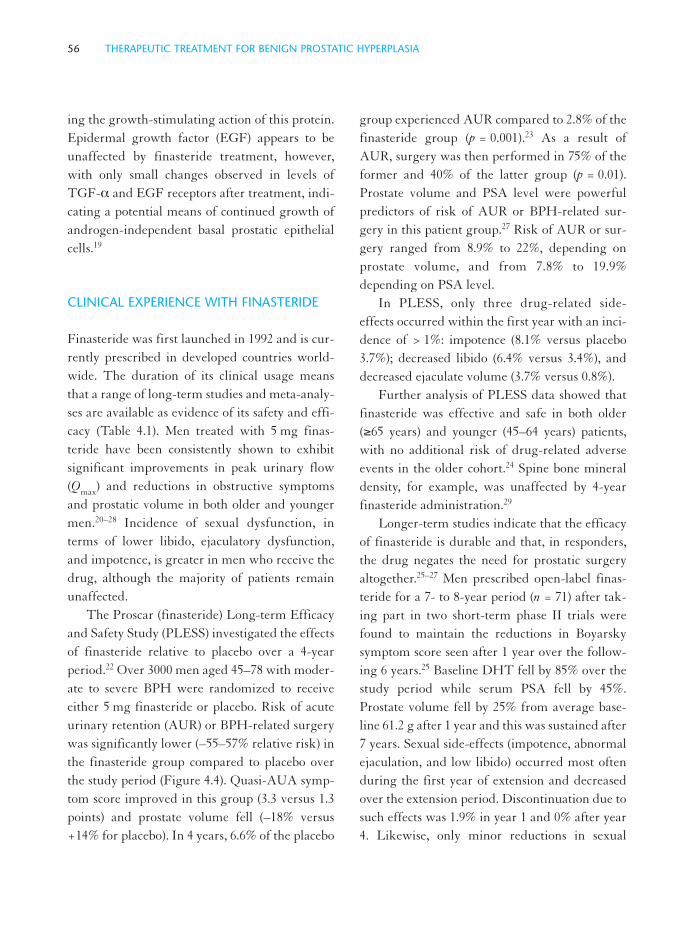
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA56
ing the growth-stimulating action of this protein.Epidermal growth factor (EGF) appears to beunaffected by finasteride treatment, however,with only small changes observed in levels ofTGF-α and EGF receptors after treatment, indi-cating a potential means of continued growth ofandrogen-independent basal prostatic epithelialcells.19
CLINICAL EXPERIENCE WITH FINASTERIDE
Finasteride was first launched in 1992 and is cur-rently prescribed in developed countries world-wide. The duration of its clinical usage meansthat a range of long-term studies and meta-analy-ses are available as evidence of its safety and effi-cacy (Table 4.1). Men treated with 5 mg finas-teride have been consistently shown to exhibitsignificant improvements in peak urinary flow(Qmax) and reductions in obstructive symptomsand prostatic volume in both older and youngermen.20–28 Incidence of sexual dysfunction, interms of lower libido, ejaculatory dysfunction,and impotence, is greater in men who receive thedrug, although the majority of patients remainunaffected.
The Proscar (finasteride) Long-term Efficacyand Safety Study (PLESS) investigated the effectsof finasteride relative to placebo over a 4-yearperiod.22 Over 3000 men aged 45–78 with moder-ate to severe BPH were randomized to receiveeither 5 mg finasteride or placebo. Risk of acuteurinary retention (AUR) or BPH-related surgerywas significantly lower (–55–57% relative risk) inthe finasteride group compared to placebo overthe study period (Figure 4.4). Quasi-AUA symp-tom score improved in this group (3.3 versus 1.3points) and prostate volume fell (–18% versus+14% for placebo). In 4 years, 6.6% of the placebo
group experienced AUR compared to 2.8% of thefinasteride group (p = 0.001).23 As a result ofAUR, surgery was then performed in 75% of theformer and 40% of the latter group (p = 0.01).Prostate volume and PSA level were powerfulpredictors of risk of AUR or BPH-related sur-gery in this patient group.27 Risk of AUR or sur-gery ranged from 8.9% to 22%, depending onprostate volume, and from 7.8% to 19.9%depending on PSA level.
In PLESS, only three drug-related side-effects occurred within the first year with an inci-dence of > 1%: impotence (8.1% versus placebo3.7%); decreased libido (6.4% versus 3.4%), anddecreased ejaculate volume (3.7% versus 0.8%).
Further analysis of PLESS data showed thatfinasteride was effective and safe in both older(≥65 years) and younger (45–64 years) patients,with no additional risk of drug-related adverseevents in the older cohort.24 Spine bone mineraldensity, for example, was unaffected by 4-yearfinasteride administration.29
Longer-term studies indicate that the efficacyof finasteride is durable and that, in responders,the drug negates the need for prostatic surgeryaltogether.25–27 Men prescribed open-label finas-teride for a 7- to 8-year period (n = 71) after tak-ing part in two short-term phase II trials werefound to maintain the reductions in Boyarskysymptom score seen after 1 year over the follow-ing 6 years.25 Baseline DHT fell by 85% over thestudy period while serum PSA fell by 45%.Prostate volume fell by 25% from average base-line 61.2 g after 1 year and this was sustained after7 years. Sexual side-effects (impotence, abnormalejaculation, and low libido) occurred most oftenduring the first year of extension and decreasedover the extension period. Discontinuation due tosuch effects was 1.9% in year 1 and 0% after year4. Likewise, only minor reductions in sexual
Ch 04 13/5/05 3:10 pm Page 56

FINASTERIDE IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 57
TABL
E 4.
1L
ong-
term
fin
aste
ride
tria
ls.
* D
epen
ding
on
pros
tate
vol
ume;
larg
er p
rost
ates
link
ed to
gre
ater
impr
ovem
ent.
ED
, ere
ctile
dys
func
tion;
FIN
, fin
aste
ride
; L L
IB, l
ower
ed li
bido
; EJD
, eja
c-ul
ator
y dy
sfun
ctio
n; S
D, s
exua
l dys
func
tion.
Red
uctio
n in
R
educ
tion
in B
PH
-P
rost
ate
Sym
ptom
St
udy
Dur
atio
nR
egim
enA
UR
ris
kre
late
d su
rger
y ri
skvo
lum
eQ
max
scor
eSi
de-e
ffec
ts
Roe
hrbo
rn e
t al.23
4 ye
ars
5m
g F
IN/d
ay
57%
55%
–18%
+1.
9m
l/s–3
.3E
D 8
.1%
or p
lace
boL
LIB
6.4
%E
JD 3
.7%
Vau
ghan
et a
l.257–
8 ye
ars
5m
g F
IN/d
ay—
—–2
5%+
20%
1-ye
ar
1st y
ear,
ED
6.4
%(o
r 10
mg
1st y
ear)
impr
ovem
ent
L L
IB 1
0.9%
mai
ntai
ned
EJD
5.8
%fe
w n
ew c
ases
ther
eaft
er
Ekm
an e
t al.26
6 ye
ars
5m
g F
IN/d
ay—
—–2
1%+
2.2
ml
30%
0.
6–1.
7% d
rop-
out
impr
ovem
ent
to S
D e
ach
year
Lam
et a
l.2710
yea
rs5
mg
FIN
/day
——
——
55.8
%
Tre
atm
ent d
urat
ion
trea
tmen
t no
t lin
ked
to s
ide-
succ
ess
effe
cts
Boy
le e
t al.43
N/A
—
——
—0.
89–1
.84
ml*
+ 1
.8–2
.8*
—m
eta-
anal
ysis
Ch 04 13/5/05 3:10 pm Page 57

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA58
function were observed in a 6-year extensionstudy of the drug.26
A 10-year follow-up study suggested thatappropriately selected patients, often with largerprostates, could be effectively treated for BPHsymptoms with finasteride over this extendedtime period.27 Of an original 43 patients whoentered phase III 12-month double-blind trials,41 completed the year and 30 continued to takethe drug for a further 4 years. Twenty-two con-tinued treatment for a further 10 years, indicatinga 48.8% overall discontinuation rate, but only26.7% between 5 and 10 years. In total, 24 (56%)were judged to be successfully treated over the10-year follow-up. The majority of withdrawalsdue to treatment failure occurred in the first 1 or2 years, suggesting continued therapeutic successin initial responders.
The adverse event profiles in the 1-year,placebo-controlled, phase III studies, the 5-yearopen extension study, and PLESS are similar.Overall, therefore, there is no evidence ofincreased side-effects with increased duration oftreatment.
Adverse treatment effects are, by and large,limited to sexual dysfunction;25,26 however, few
patients report such effects overall and superficialanalysis would appear to indicate that numbersare similar across alternative treatment options30
(Figure 4.5). A study of 670 BPH patients treatedwith a range of medical and surgical options andwatchful waiting (n = 90 (α-blocker 43, finas-teride 47), 207, and 234, respectively involvedassessment of sexual effects by questionnaire 9months after surgery or the initiation of therapy.Libido, sexual activity, potency, and penile rigidi-ty were determined. An improvement of between7 and 14% was reported for libido for all treat-ments (α-blocker 3%, finasteride 8%) and deteri-oration in libido was reported by between 7 and14% (α-blocker 14%, finasteride 8%) of all partic-ipants. Similar results were observed for sexualactivity and erectile capacity; however, completeresults for rigidity were not available for finas-teride-treated patients.
A similar degree of improvement in urinarysymptoms and quality of life has been reported insome studies of 5α-reductase inhibitors and α-blockers. For example, a randomized study oftamsulosin (0.2 mg) and finasteride (5 mg)showed both drugs to result in similar improve-ments in a group of Korean BPH patients
12
10
8
6
4
2
0
AUR (%) Surgery (%) Decrease in symptom score (points)
Finasteride
Placebo
FIGURE 4.4 Reduced risk of acute urinary retention (AUR) and BPH-related surgery with finasteride.
Ch 04 13/5/05 3:10 pm Page 58

FINASTERIDE IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 59
(n = 205) after a period of 24 weeks. I-PSS, Qmax,and quality of life improved in both groups withno significant difference between scores at end-point; however, analysis at 4 weeks showed tam-sulosin to have a swifter time to onset.31
COMBINATION STUDIES
The different mode of action of 5α-reductaseinhibitors and α-blockers has led to the assump-tion that a combination of both drug types mayincrease clinical improvement in BPH patients,due to the dual effects of inhibiting cell prolifera-tion and altering the smooth muscle tone of theprostatic stroma and detrusor.
The most comprehensive evaluation of theclinical potential of combination therapy hasbeen the Medical Therapy Of ProstaticSymptoms (MTOPS) study. This trial indicatedthat the combination of finasteride with doxa-
zosin both slows the progression of BPH andreduces risk of AUR to a greater extent thaneither type of therapy alone.32 This studyinvolved a total of 3047 BPH patients whoreceived monotherapy, placebo, or combinationtherapy for an average of 5 years. Finasteride ordoxazosin monotherapy brought about reduc-tions in risk of disease progression of 34% and39%, respectively, while combination therapy wasassociated with a 67% reduction in risk (Figure4.6). AUR risk was cut by 79% in this group com-pared to 67% in the finasteride group and 31% inthe doxazosin group. Reductions in risk of BPHsurgery were 69%, 64%, and 8% relative to place-bo in each group, respectively. No increase inside-effects was observed with combination treat-ment. The results suggest that enlargement of theprostate is slowed by finasteride while the symp-toms of BPH are reduced by doxazosin.Interestingly, the combination of the two drugsreduces the risk of clinical progression even in
0 5 10 15–20 –15 –10 –5 0
Rigidity Erection Sexual activity Libido
Deterioration (%) Improvement (%)
Watchfulwaiting
Surgery
Finasteride
* No data available
*
α-Blockers
FIGURE 4.5 Percentage of patients with improved and reduced sexual function following BPH treatment.
Ch 04 13/5/05 3:10 pm Page 59

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA60
men with only modest prostate enlargement(25–40 cc).33
Investigation of baseline characteristics andsubsequent progression of the men in theMTOPS placebo group (n = 737) indicated thateasily obtainable measures, such as PSA level,Qmax, postvoid residual urine, and prostate vol-ume, correlate significantly with disease progres-sion and the need for surgery.34 Such an approachmay allow improved patient selection to ensureoptimum clinical results.
Additional research has suggested that it maybe possible to discontinue combination therapyafter 1 year with no compromise in clinical bene-fit.35 A group of BPH patients (n = 270) were pre-scribed 2, 4, or 8 mg doxazosin alongside 5 mgfinasteride for a period of 3, 6, 9, or 12 months,after which the α-blocker was discontinued. Ofthose who discontinued doxazosin at 12 months,84% of the 2 mg group, 85% of the 4 mg group,and 87% of the 8 mg group experienced noincrease in AUA symptom score and reported nodesire to resume taking doxazosin 1 month later.
In studies of generally shorter duration andreduced patient numbers the results with combi-
nations have not been as conclusive. The additionof finasteride to terazosin in the Veterans’ AffairsCooperative Studies BPH Study Group, whichinvolved 1229 patients, conveyed no additionalbenefit compared to terazosin monotherapy after1 year.36 The relatively low average prostate vol-ume of the men involved in this study(36.2–38.4 ml) could explain the limited improve-ment observed in patients treated with finasteridealone, due to the correlation between gland sizeand clinical response observed in several stud-ies.37,38 Pharmacokinetic interactions betweenfinasteride and terazosin, but not doxazosin mayalso have a bearing on clinical response to differ-ent combination therapy regimens.39
A 6-month trial of sustained-release alfuzosin(5 mg), finasteride (5 mg), or both drugs in 1051men yielded similar findings to the VACooperative trial, with higher symptom improve-ment observed in patients who received α-block-ade or combination therapy.40 The short-termnature of this trial precludes any definitive con-clusions, however.
An additional 1-year randomized placebo-controlled study involved 1007 men who received
Finasteride Doxazosin Combination
Progression AUR Surgery
% R
educ
tion
0
–20
–40
–60
–80
–100
FIGURE 4.6 MTOPS—reductions in disease progression with combination treatment. AUR, acute urinary retention.
Ch 04 13/5/05 3:10 pm Page 60

FINASTERIDE IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 61
finasteride (5 mg) or doxazosin (1–8 mg, titrated)monotherapy, combination therapy, or placebo.Results indicated no additional benefit of finas-teride to doxazosin therapy.41 Again, meanprostate size was relatively small, at 36.3 g, whichmay explain the lack of observed efficacy of finas-teride. No stratified analysis based on prostatevolume was performed.
The role of prostate volume is illustrated by afurther trial of finasteride, alfuzosin, or a combi-nation of both in a group of 138 men with I-PSS> 13 and prostate volume of at least 60 ml.Overall, 96% of patients in the combinationgroup showed improved Qmax and I-PSS, com-pared to 84% in the α-blocker alone group and74% in the finasteride group.42
Meta-analysis of six randomized clinical trialsinvolving finasteride (Table 4.2) provides furtherevidence of the role of prostate volume inresponse to therapy, with men with largerprostates showing particularly good response totreatment with finasteride.43,44 Over 2600 individ-uals were included in this study, which includedall finasteride studies and phase III trials plus anumber of other trials including the VACooperative Study. Men with prostates smallerthan 20 g were less likely to show clinical
improvement in quasi-I-PSS symptom score andQmax compared to those with prostates larger than60 g (1.8 versus 2.8 points and 0.89 ml versus1.84 ml, respectively). Improvements werejudged to become significant in men withprostates greater than 40 ml, i.e. 50% of the entirepopulation, and the results indicate that prostatevolume is a significant predictor of response totherapy.
ADDITIONAL CONSIDERATIONS
Hematuria
Hematuria, which often emerges secondary toBPH, is associated with significant morbidity,including anemia and clot retention. Recentresearch has shown that the condition may besuccessfully treated with finasteride and otheranti-androgens.45–47 Although the exact mecha-nism is not understood, histochemical studieshave suggested that this is due to decreasedexpression of vascular endothelial growth factor(VEGF) following finasteride treatment which,as a consequence, lowers microvessel density inthe prostatic suburethra.48,49 Such mechanismscould explain the reduction in hematuria and
TABLE 4.2 Studies included in meta-analysis of finasteride.
Patients Age Prostate volume Peak flow Quasi-I-PSSStudy (n) (mean) (mean ml) (mean ml) (mean)
Gormley et al.20 567 64.1 59.9 9.6 12.1
The Finasteride Study Group60 447 65.5 48.1 8.9 11.8
Andersen et al.60 384 65.3 41.3 10.2 10.1
Lepor et al.36 601 65.7 37.5 10.4 13.4
Nickel et al.62 554 63.3 45.9 11.0 12.4
Bonilla et al.63 188 56.4 41.6 15.8 9.3
Ch 04 13/5/05 3:10 pm Page 61

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA62
intraoperative blood loss observed when patientsdue to undergo transurethral resection of theprostate (TURP) receive finasteride treatmentpreoperatively.50,51
Investigation of potential predictors of clinicalresponse to finasteride treatment in patients withgross hematuria revealed that 94% responded totreatment and that 77% suffered no furtherbleeding while taking the drug.47 Treatment waseffective in patients taking a range of anticoagu-lants. Recurrent but lower-grade bleeding andslower response time were identified in men withlarger prostates. Men with smaller prostates andthose who had undergone previous prostatecto-my had more rapid responses to treatment (2.7days in men with glands < 40 g versus 45 days inthose with glands 100–150 g and 5.5 days in menwho had undergone prostatectomy versus 18.6days in those who had not).
PSA
PSA levels have been found to fall followingapplication of finasteride to prostate cells treatedin vitro with testosterone.52 In vivo studies haveshown that plasma and serum complexed-to-totaland free-to-total ratios remain constant withfinasteride treatment, indicating that proportion-al reduction in all molecular forms of PSA occurswith finasteride treatment.53–55 Measurement ofthese PSA forms could potentially be used toscreen for prostate cancer in men receiving finas-teride, but this requires further investigation.55,56
The effect of finasteride on overall PSA levelshas implications for prostate cancer screening butmay also impact upon actual risk of prostate can-cer. A case–control study of the medication use in639 men with prostate cancer and 659 tumor-freecontrols indicated that, after adjustment for con-founders, finasteride has a protective role againstprostate cancer while nonaspirin nonsteroidal
anti-inflammatory drugs (NSAIDs) have no pro-tective influence.57
Further evidence of the potential preventativerole of finasteride has been recently highlightedin a large-scale study of the incidence of prostatecancer among men aged ≥55 years prescribedfinasteride or placebo over 7 years.58 Men whoreceived the active agent were significantly lesslikely to develop prostate cancer during the studythan those prescribed placebo (p = 0.001),although when cancer did develop in this group,it was more likely to be of a higher Gleason gradethan in the placebo group. Whether the benefitsof reduced likelihood of prostate cancer develop-ment and urinary symptoms outweigh the risksof higher-grade tumor development and sexualside-effects requires further investigation.
CONCLUSIONS
Patient perception of finasteride has been shownto be excellent. In a survey of French BPHpatients, the primary preoccupations were report-ed as a reduced risk for urological complicationsand need for surgery, with improved symptomsand quality of life of secondary importance.These expectations were easily met by finasteridein the majority of cases, and 89% of partic-ipants reported good or extremely good improve-ment of symptoms, with very few tolerabilityissues.59
The studies outlined here indicate that finas-teride is an effective long-term treatment optionfor BPH. The benefit of finasteride over placebohas been repeatedly proven in well-designedlarge-scale clinical trials and comparison studieshave shown the drug to be of similar efficacy interms of AUR prevention and necessity for BPHsurgery to α-blockers in well-chosen patientgroups. Men with larger prostates appear to ben-
Ch 04 13/5/05 3:10 pm Page 62

FINASTERIDE IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 63
efit particularly from finasteride therapy.Response to therapy has been shown to haveexceptionally long duration in responders,exceeding 10 years in many cases. The data fromthe MTOPS study indicate that the drug has fur-ther potential when used in combination with α-blockers. On this basis, future treatment algo-rithms could include both a 5α-reductaseinhibitor and α-receptor antagonist, dependingon the initial clinical presentations.
The effects of finasteride on PSA level havebeen frequently documented; however, recentfindings regarding the lack of effect of the drugon free-to-total PSA ratio may mean that sugges-tions that prostate cancer detection may be com-promised can largely be dismissed. Further inves-tigation of this aspect is required, however.
REFERENCES
1. Lee C, Kozlowski J M, Grayhack J T. Aetiology ofbenign prostatic hyperplasia. Urol Clin North Am1995; 22: 237–246
2. Walsh P C, Hutchins G M, Ewing L L. Tissue con-tent of dihydrotestosterone in human prostatichyperplasia is not supranormal. J Clin Invest 1983;72: 1772–1777
3. Traish A M, Wotiz H H. Prostatic epidermalgrowth factor receptors and their regulation byandrogens. Endocrinology 1987; 121:1461–1467
4. Wilson J D. The pathogenesis of benign prostatichyperplasia. Am J Med 1980; 68: 745–756
5. Walsh P C, Madden J D, Harrod M J et al. Familialincomplete male pseudohermaphroditism, type 2:decreased dihydrotestosterone formation inpseudovaginal perineoscrotal hypospadias. N EnglJ Med 1974; 291: 944–949
6. Imperato-McGinley J, Guerrero L, Gautier T,Peterson R E. Steroid 5a-reductase deficiency inman: an inherited form of male pseudohermaphro-ditism. Science 1974; 186: 1213–1215
7. Thigpen A E, Davis D L, Milatovich A et al.Molecular genetics of steroid 5α-reductase 2 defi-ciency. J Clin Invest 1992; 90: 799–809
8. Brooks J R, Berman C, Garnes D et al. Prostaticeffects induced in dogs by chronic or acute oraladministration of 5 alpha-reductase inhibitors.Prostate 1986; 9: 65–75
9. Rittmaster R S, Stoner E, Thompson D L et al.Effect of MK-906, a specific 5α-reductase inhibitor,on serum androgens and androgen conjugates innormal men. J Androl 1989; 10: 259–262
10. Vermeulen A, Giagulli C A, Schepper P D et al.Hormonal effects of an orally active 4-azasteroidinhibitor of 5α-reductase in humans. Prostate 1989;14: 45–53
11. Thigpen A E, Silver R I, Guileyardo J M et al.Tissue distribution and ontogeny of steroid 5alpha-reductase isozyme expression. J Clin Invest1993; 92: 903–910
12. Bartsch G, Rittmaster R S, Klocker H. Dihydro-testosterone and the concept of 5 alpha-reductaseinhibitors in human benign prostatic hyperplasia.Eur Urol 2000; 37: 367–380
13. Marks L S, Partin A W, Dorey F J et al. Long-termeffects of finasteride on prostate tissue composition.Urology 1999; 53: 574–580
14. Saez C, Gonzalez-Baena A C, Japon M A et al.Regressive changes in finasteride-treated humanhyperplastic prostates correlate with an upregula-tion of TGF-beta receptor expression. Prostate1998; 37: 84–90
15. Lobaccaro J M, Boudon C, Lechevallier E et al.Effect of finasteride (Proscar) on the proliferationof cultured epithelial and stromal cells from nor-mal and hyperplastic human prostates. Cell MolBiol (Noisy-le-grand) 1996; 42: 511–518
16. Feneley M R, Span P N, Schalken J A et al. Aprospective randomized trial evaluating tissueeffects of finasteride therapy in benign prostatichyperplasia. Prostate Cancer Prostatic Dis 1999; 2:277–281
17. Saez C, Gonzalez-Baena A C, Japon M A et al.Expression of basic fibroblast growth factor and itsreceptors FGFR1 and FGFR2 in human benign
Ch 04 13/5/05 3:10 pm Page 63

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA64
prostatic hyperplasia treated with finasteride.Prostate 1999; 40: 83–88
18. Crescioli C, Villari D, Forti G et al. Des (1–3) IGF-I-stimulated growth of human stromal BPH cells isinhibited by a vitamin D(3) analogue. Mol CellEndocrinol 2002; 198: 69–75
19. Torring N, Moller-Ernst Jensen K, Lund L et al.Possible autocrine loop of the epidermal growthfactor system in patients with benign prostatichyperplasia treated with finasteride: a placebo-con-trolled randomized study. BJU Int 2002; 89:583–590
20. Gormley G J, Stoner E, Bruskewitz R C et al. Theeffect of finasteride in men with benign prostatichyperplasia. The Finasteride Study Group. N EnglJ Med 1992; 327: 1185–1191
21. Byrnes C A, Liss C L, Tenover J L et al. Combinedanalysis of two multicenter studies of finasteride 5mg in the treatment of symptomatic benign prosta-tic hyperplasia. Prostate Cancer Prostatic Dis 1997;1: 26–31
22. McConnell J D, Bruskewitz R, Walsh P et al. forthe Finasteride Long-term Efficacy and SafetyStudy Group. The effect of finasteride on the riskof acute urinary retention and the need for surgicaltreatment among men with benign prostatic hyper-plasia. N Engl J Med 1998; 338: 557–563
23. Roehrborn C G, Bruskewitz R, Nickel G C et al.Urinary retention in patients with finasteride orplacebo over 4 years. Characterization of patientswith ultimate outcomes. The PLESS Study Group.Eur Urol 2000; 37: 528–536
24. Kaplan S A, Holtgrewe H L, Bruskewitz R et al.for the Proscar Long-Term Efficacy and SafetyStudy Group. Comparison of the efficacy and safe-ty of finasteride in older versus younger men withbenign prostatic hyperplasia. Urology 2001; 57:1073–1077
25. Vaughan D, Imperato-McGinley J, McConnell J etal. Long-term (7 to 8-year) experience with finas-teride in men with benign prostatic hyperplasia.Urology 2002; 60: 1040–1044
26. Ekman P and the Scandinavian Finasteride StudyGroup. Maximum efficacy of finasteride isobtained within 6 months and maintained over 6
years: follow-up of the Scandinavian Open-Extension Study. Eur Urol 1998; 33: 312–317
27. Lam J S, Romas N A, Lowe F C. Long-term treat-ment with finasteride in men with symptomaticbenign prostatic hyperplasia: 10-year follow-up.Urology 2003; 61: 354–358
28. Roehrborn C G, McConnell J D, Lieber M et al.Serum prostate-specific antigen concentration is apowerful predictor of acute urinary retention andneed for surgery in men with clinical benign pro-static hyperplasia. PLESS Study Group. Urology1999; 53: 473–480
29. Matsumoto A M, Tenover L, McClung M et al.Pless Study Group. The long-term effect of specif-ic type II 5alpha-reductase inhibition with finas-teride on bone mineral density in men: results of a4-year placebo controlled trial. J Urol 2002; 167:2105–2108
30. Leliefeld H H, Stoevelaar H J, McDonnell J.Sexual function before and after various treatmentsfor symptomatic benign prostatic hyperplasia. BJUInt 2002; 89: 208–213
31. Lee E. Comparison of tamsulosin and finasteridefor lower urinary tract symptoms associated withbenign prostatic hyperplasia in Korean patients. JInt Med Res 2002; 30: 584–590
32. McConnell JD, Roehrborn CG, Bautista OM et al.Medical Therapy of Prostatic Symptoms (MTOPS)Research Group. The long-term effect of doxa-zosin, finasteride, and combination therapy on theclinical progression of benign prostatic hyperplasia.N Engl J Med 2003; 349: 2387–2398
33. Kaplan S, Roehrborn C, Lee M. The superior bene-ficial effect of combination therapy with doxazosinand finasteride versus either drug alone on clinicalprogression of benign prostatic hyperplasia in theMTOPS trial was not dependent on patients hav-ing prostatic enlargement at baseline. Eur Urol2005; (Suppl) 4: 213 Abstract # 841
34. McConnell J F, Roehrborn C G, Slawin K M et al.Baseline measures predict the risk of benign pro-static hyperplasia clinical progression in placebo-treated patients. J Urol 2003; 169 (Suppl 4): abstract1287
35. Baldwin K C, Ginsberg P C, Roehrborn C G,Harkaway R C. Discontinuation of alpha-blockade
Ch 04 13/5/05 3:10 pm Page 64
FINASTERIDE IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 65
after initial treatment with finasteride and doxa-zosin in men with lower urinary tract symptomsand clinical evidence of benign prostatic hyperpla-sia. Urology 2001; 58: 203–209
36. Lepor H, Williford W O, Barry M J et al. for TheVeterans Affairs Cooperative Studies BenignProstatic Hyperplasia Study Group. The efficacy ofterazosin, finasteride or both in benign prostatichyperplasia. N Engl J Med 1996; 335: 533–540
37. Boyle P, Gould A L, Roehrborn C G. Prostate vol-ume predicts outcome of treatment of benign pro-static hyperplasia with finasteride: meta-analysis ofrandomized clinical trials. Urology 1996; 48:398–405
38. Roehrborn C G, Boyle P, Bergner D et al. for thePLESS Study Group. Serum prostate-specific anti-gen and prostate volume predict long-term changesin symptoms and flow rate: results of a four-year,randomized trial comparing finasteride versusplacebo. Urology 1999; 54: 662–669
39. Vashi V, Chung M, Hilbert J et al. Pharmacokineticinteraction between finasteride and terazosin, butnot finasteride and doxazosin. J Clin Pharmacol1998; 38: 1072–1076
40. Debruyne F M, Jardin A, Colloi D et al. Sustained-release alfuzosin, finasteride and the combinationof both in the treatment of benign prostatic hyper-plasia. European ALFIN Study Group. Eur Urol1998; 34: 169–175
41. Kirby R S, Roehrborn C G, Boyle P et al. for thePREDICT Study Investigators. Efficacy and toler-ability of doxazosin and finasteride, alone or incombination, in treatment of symptomatic benignprostatic hyperplasia: the Prospective EuropeanDoxazosin and Combination Therapy (PREDICT)trial. Urology 2003; 61: 119–126
42. Loran O B, Pushkar’ Dlu, Rasner P I. [Compara-tive evaluation of the effectiveness and safety ofcombined drug therapy of patients with benignprostatic hyperplasia with finasteride and alfu-zozine] [in Russian]. Urologiia 2002; 1: 19–22
43. Boyle P, Gould A L, Roehrborn C G. Prostate vol-ume predicts outcome of treatment of benign pro-static hyperplasia with finasteride: meta-analysis ofrandomized clinical trials. Urology 1996; 48:398–405
44. Roehrborn C G. Meta-analysis of randomized clin-ical trials of finasteride. Urology 1998; 51 (Suppl4A): 46–49
45. Kashif K M, Foley S J, Basketter V, Holmes S A.Haematuria associated with BPH—natural historyand a new treatment option. Prostate CancerProstatic Dis 1998; 1: 154–156
46. Perimenis P, Gyftopoulos K, Markou S, BarbaliasG. Effects of finasteride and cyproterone acetate onhematuria associated with benign prostatic hyper-plasia: a prospective, randomized, controlled study.Urology 2002; 59: 373–377
47. Kearney M C, Bingham J B, Bergland R et al.Clinical predictors in the use of finasteride for con-trol of gross hematuria due to benign prostatichyperplasia. J Urol 2002; 167: 2489–2491
48. Pareek G, Shevchuk M, Armenakas N A et al. Theeffect of finasteride on the expression of vascularendothelial growth factor and microvessel density:a possible mechanism for decreased prostatic bleed-ing in treated patients. J Urol 2003; 169: 20–23
49 Haggstrom S, Torring N, Moller K et al. Effects offinasteride on vascular endothelial growth factor.Scand J Urol Nephrol 2002; 36: 182–187
50. Kamalov A A, Riaboi A V, Ignashin N S et al. [Useof proscar in preoperative preparation of patientswith benign prostatic hyperplasia before transuret-eral resection] [in Russian]. Urologiia 2002; 5: 16–18
51. Sandfelt L, Bailey D M, Hahn R G. Blood loss dur-ing transurethral resection of the prostate after 3months of treatment with finasteride. Urology2001; 58: 972–976
52. Lopez Munnoz A, Larran Lopez J, Aparicio PatinoJ et al. Assessment of the effect of a 5-alpha-reduc-tase inhibitor on cultured explants of humanprostate. [in Spanish]. Actas Urol Esp 1996; 20:316–322
53. Espana F, Martinez M, Royo M et al. Changes inmolecular forms of prostate-specific antigen duringtreatment with finasteride. BJU Int 2002; 90:672–677
54. Brawer M K, Lin D W, Williford W O et al. Effectsof finasteride and/or terazosin on serum PSA:results of VA Cooperative Study #359. Prostate1999; 39: 234–239
Ch 04 13/5/05 3:10 pm Page 65
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA66
55. Tarle M, Kraus O, Trnski D et al. Early diagnosisof prostate cancer in finasteride treated BPHpatients. Anticancer Res 2003; 23: 693–696
56. Keetch D W, Andriole G L, Ratliff T L, CatalonaW J. Comparison of percent free prostate-specificantigen levels in men with benign prostatic hyper-plasia treated with finasteride, terazosin or watch-ful waiting. Urology 1997; 50: 901–905
57. Irani J, Ravery V, Pariente J L et al. Effect of nons-teroidal anti-inflammatory agents and finasterideon prostate cancer risk. J Urol 2002; 168: 1985–1988
58. Thompson I M, Goodman P J, Tangen C M et al.The influence of finasteride on the development ofprostate cancer. Published at www.nejm.org 24June, 2003 (doi: 10.1056/NEJMoa030660)
59. Teillac P. Benign prostatic hyperplasia: patients’perception of medical treatment and their expecta-tions. Results of a French survey involving patientstreated with finasteride [in French]. Therapie 2002;57: 473–483
60. The Finasteride Study Group. Finasteride (MK-906) in the treatment of benign prostatic hyperpla-sia. Prostate 1993; 22: 291–299
61. Andersen J T, Ekman P, Wolf H et al. and theScandinavian BPH Study Group. Can finasteridereverse the progress of benign prostatic hyperpla-sia? A two-year placebo-controlled study. Urology1995; 46: 631–637
62. Nickel J C, Fradet Y, Boake R C et al. Efficacy andsafety of finasteride therapy for benign prostatichyperplasia: results of a 2-year randomized con-trolled trial (the PROSPECT study). PROscarSafety Plus Efficacy Canadian Two year Study.CMAJ 1996; 155: 1251–1259
63. Bonilla J, Stoner E, Grino P et al. Intra- and inter-observer variability of MRI prostate volume meas-urements. Prostate 1997; 31: 98–102
Ch 04 13/5/05 3:10 pm Page 66

Combination therapy in thetreatment of BPH
C G Roehrborn5
67
INTRODUCTION
Treatment for benign prostatic hyperplasia(BPH) in recent years has been characterized by afall in the use of surgical procedures, mainlytransurethral resection of the prostate (TURP),and a rise in the use of minimally invasive treat-ments and, particularly, medical therapy.1–3
Up to 90% of men in their eighties are esti-mated to suffer from BPH to some extent andprevalence of the disease is growing.4
Development of the associated symptomatologyis androgen-dependent, and castration before orduring puberty prevents its occurrence. Lowerurinary tract symptoms (LUTS) secondary toBPH occur due to increased sensitivity to circu-lating androgens in the prostate. Increased cellproliferation, mainly in the transition zone of theprostate, occurs alongside a rise in the smoothmuscle tone of both the prostate and bladderneck. Symptoms of reduced urinary flow and uri-nary retention, increased urinary frequency, andnocturia are particularly common.5
Pharmacologic therapies available for thetreatment of LUTS include α-adrenoceptorantagonists (α-blockers), such as terazosin, doxa-zosin, alfuzosin, and tamsulosin, and the 5α-reductase inhibitors, finasteride and dutasteride.Other strategies, such as plant-derived medica-tion or watchful waiting, are applied to varyingextents.
Alpha-blockers act on the α-adrenoceptors ofthe prostate and bladder neck, thereby reducingthe sympathetic nervous system controlled tone of
the smooth muscle. Many placebo-controlled tri-als of α-blockers have shown them to increaseurinary flow and relieve irritative and obstructivesymptoms, often within as little as 2 weeks oftreatment.6–11
In contrast, 5α-reductase inhibitors reducethe formation of dihydrotestosterone (DHT)from testosterone in the prostate and therebyincrease rates of apoptosis and reduce rates of cellproliferation. Enlarged prostate glands thereforeshrink, causing alleviation of BPH symptoms andurinary flow in the process,12–14 as proven byplacebo-controlled trials.15–17 More recently, it hasbeen shown that the risks of acute urinary reten-tion (AUR) and BPH-related surgery are reducedin men receiving finasteride by 55% and 57%,15
respectively. However, symptom improvementmay only be observed after up to 6 months oftreatment15,16 and, indeed, it has been suggestedthat the clinical benefit is limited to men withlarger prostates.16,18
The recent development of diverse formula-tions of pharmacologic therapies, such as the dox-azosin gastrointestinal therapeutic system (GITS)and doxazosin XL, has increased patient andphysician treatment choice.10 Further alterationsin the pharmacokinetic profiles of available drugsare possible, however such avenues may be limit-ed. In real terms we may have reached the limit ofclinical benefit that can be achieved by monother-apy. Alternative pharmacologic treatment strate-gies for targeting BPH are therefore desirable.
Given the different mechanisms of action ofα-blockers and 5α-reductase inhibitors, a
Ch 05 13/5/05 3:12 pm Page 67

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA68
combination of each of the drug classes in a singledrug regimen might logically be expected to con-vey cumulative benefit to BPH patients.19 Severallarge-scale studies have been performed in recentyears to determine whether the administration ofan α-blocker in combination with a 5α-reductaseinhibitor leads to greater improvement in BPHsymptoms than either one individually andwhether the side-effects documented with eachdrug class occur with greater frequency in combi-nation.
The following represents a summary of thesalient findings from the most important combi-nation studies that have been completed.
TERAZOSIN AND FINASTERIDE
VA Cooperative Study
The first large-scale trial established to examinethe potential benefits of combining an α-blockerwith a 5α-reductase inhibitor was the Veterans’Affairs (VA) Cooperative Study.6 This multicen-ter trial compared the use of terazosin and finas-teride individually and in combination.
The double-blind, placebo-controlled trialinvolved 1229 men (87% white, 11% black, 1%Asian/Pacific Islanders, 0.5% Native Americans)aged 45–80 suffering from symptomatic BPH.Baseline measures were obtained during an initial1-month wash-out period and includedAmerican Urological Association (AUA) symp-tom score, peak urinary flow (Qmax), and volumeof postvoid residual urine (PVR). Prostate-specif-ic antigen (PSA) levels were recorded andtransurethral ultrasound examination of theprostate was also performed.
Participants had an AUA symptom score of≥8, Qmax of 4–15 ml/s, minimal voided volume of125 ml and PVR of < 300 ml. After the wash-out
period, they were randomized to receive 5 mgfinasteride, terazosin titrated to 10 mg, a combi-nation of both drugs, or placebo for a period of 1year.
Clinical evaluation, in terms of uroflowmetry,symptom score, PVR, and adverse effects, tookplace at 2, 4, 13, 26, 39, and 52 weeks. Transrectalultrasound examination took place at the half-way point and on completion of the study. PSAwas recorded at the end of the study period.
Drop-out rates were similar between groupsafter 1 year, although discontinuation due toadverse effects was less common in the placebogroup (p < 0.05). Overall, men receiving terazosineither alone or in combination were more likelyto suffer dizziness and men receiving finasteridealone or in combination were more likely to expe-rience erectile dysfunction (ED) or loweredlibido. Ejaculatory dysfunction was significantlymore common in men receiving combinationtherapy. Compliance was similar between all fourtreatment groups, however.
Examination of symptom scores revealed thatmen receiving terazosin alone or in combinationwith finasteride had improved symptoms com-pared to both the finasteride and placebo groups(p < 0.001), with respective point reductions of6.1, 6.2, 3.2, and 2.6 (Figure 5.1). Peak improve-ment levels were attained in the terazosin-exposed groups by 13 weeks and did not differsignificantly between this point and completionof the study. The improvements in symptomscore were accompanied by significant increasesin Qmax (p < 0.001 for terazosin and combinationtherapy compared to finasteride alone and place-bo), which were greatest after 4 weeks. Meanincreases in Qmax at 52 weeks were 3.2, 2.7, 1.6,and 1.4 ml/s, respectively.
Significant reductions in prostatic volumewere observed in the finasteride and combination
Ch 05 13/5/05 3:12 pm Page 68

COMBINATION THERAPY IN THE TREATMENT OF BPH 69
therapy groups (–61 ml and –70 ml, respectively)but no significant change was observed in thisvalue in the other two groups. PSA was also sig-nificantly reduced in the finasteride and combi-nation groups (p < 0.001) while increases werenoted in men who received terazosin alone orplacebo (p < 0.01).20
The results of this study confirm previouslydocumented evidence of the efficacy of tera-zosin;21,22 but, they are not in agreement withstudies indicating that finasteride reduces BPHsymptoms and improves Qmax.
23,24 The VA studysuggests that reduction in smooth muscle tone byα-blockers is more likely to reduce symptoms ofBPH than androgen suppression using 5α-reduc-tase inhibitors. The role of prostate volume wasnot assessed in this trial, however.
Despite the lack of significant additional ben-efit with the addition of finasteride to terazosintherapy described in this trial, interactionsbetween the two drugs have been document-ed.25,26 Rates of apoptosis and proliferation weredetermined from prostate samples obtained from76 men who had been treated for BPH with tera-
zosin, finasteride, or a combination of both.25
Both stromal and epithelial rates of apoptosiswere significantly higher in the combination sam-ples compared to monotherapy samples, althoughproliferation rates were similar. Upregulation oftransforming growth factor (TGF) β1 wasobserved in the terazosin and combination thera-py groups.
The cellular relationship between the twodrugs remains unclear, however. An additional,retrospective, study of cell proliferation and apop-tosis among men treated with doxazosin, tera-zosin, finasteride, or a combination of finasterideand one of the α-blockers indicated no increase inapoptotic index with addition of finasteride to theother agents.27
A molecular relationship between the twodrug classes was described in a comparison of thepharmacokinetic interactions between terazosinand finasteride and between doxazosin and finas-teride. In this trial, the maximum plasma concen-tration and area under the plasma concentra-tion–time curve from 0 to 24 hours of finasteridewere significantly greater after coadministration
Points ml/s
*p < 0.001 for comparisons with placebo or finasteride alone
Reduction in AUA symptom score Increase in Qmax
0 2 4 6 8 0 2 4 6
*
*
*
*
terazosin
terazosin + finasteride
finasteride
placebo
FIGURE 5.1 VA Cooperative Study: symptom improvement at 1 year according to treatment group. AUA, AmericanUrological Association; Qmax, peak urinary flow.
Ch 05 13/5/05 3:12 pm Page 69

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA70
with terazosin.26 The pharmacokinetic profile ofterazosin was not altered, however. Whether thisrelationship is significant in terms of drug effica-cy is as yet unknown.
ALFUZOSIN AND FINASTERIDE
ALFIN study
The α-blocker alfuzosin is a uroselective prepara-tion that targets the α1-adrenoceptors of theprostate. Animal studies have shown alfuzosin toexert its effect at doses below the threshold ofinfluence on the cardiovascular system.28–30 Itdoes not require titration to its optimum dosage.
A 6-month evaluation of the effects of com-bining 5 mg twice-daily (sustained-release alfu-zosin) with 5 mg once-daily finasteride (theALFIN study) showed similar effects to the VAstudy described above.31 Again, the α-blockerwas shown to improve symptoms of LUTS sec-ondary to BPH to a greater extent alone or incombination compared to finasteride.
The ALFIN study involved 1051 BPHpatients aged between 50 and 75 from 11European countries. Participants had anInternational Prostate Symptom Score (I-PSS)> 7 and Qmax of between 5 and 15 ml/s. Theyunderwent a 2-week wash-out period prior torandomization to alfuzosin, finasteride, or a com-bination of both.
Clinical assessment took place at baseline andthen after 1, 3, and 6 months of therapy. I-PSSwas recorded alongside uroflowmetry, bloodpressure, and heart rate during these sessions,while prostate volume, measured usingtransurethral ultrasound, and PSA level wereassessed at baseline and on completion of thestudy. Adverse events were reported throughoutthe entire trial.
All three patient groups were found to showimprovement over the study period (Figure 5.2).Mean I-PSS fell by 6.3 points in the alfuzosinalone group, 6.1 in the combination group, and5.2 in the finasteride alone group, but a signifi-cantly greater improvement in the alfuzosin and
Points ml/s
*p < 0.01 for alfuzosin vs finasteride†p < 0.03 for combination vs finasteride
Reduction in I-PSS Increase in Qmax
0 2 4 6 8 0 2 4 6
*
†
alfuzosin
alfuzosin + finasteride
finasteride
FIGURE 5.2 ALFIN Study: symptom improvement at 6 months according to treatment group. I-PPS, InternationalProstate Symptom Score; Qmax, peak urinary flow.
Ch 05 13/5/05 3:12 pm Page 70
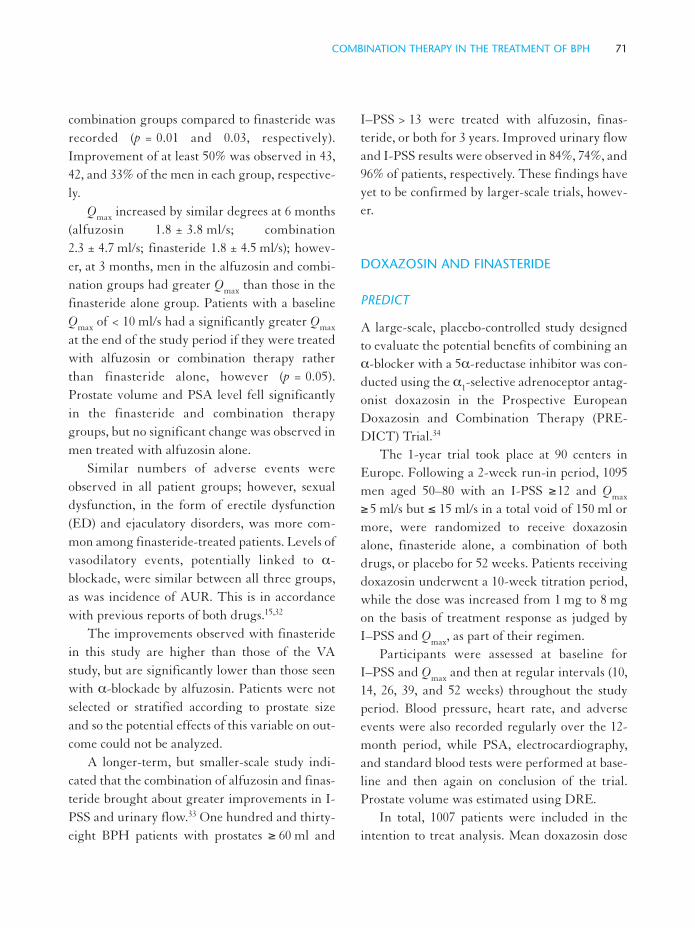
COMBINATION THERAPY IN THE TREATMENT OF BPH 71
combination groups compared to finasteride wasrecorded (p = 0.01 and 0.03, respectively).Improvement of at least 50% was observed in 43,42, and 33% of the men in each group, respective-ly.
Qmax increased by similar degrees at 6 months(alfuzosin 1.8 ± 3.8 ml/s; combination2.3 ± 4.7 ml/s; finasteride 1.8 ± 4.5 ml/s); howev-er, at 3 months, men in the alfuzosin and combi-nation groups had greater Qmax than those in thefinasteride alone group. Patients with a baselineQmax of < 10 ml/s had a significantly greater Qmax
at the end of the study period if they were treatedwith alfuzosin or combination therapy ratherthan finasteride alone, however (p = 0.05).Prostate volume and PSA level fell significantlyin the finasteride and combination therapygroups, but no significant change was observed inmen treated with alfuzosin alone.
Similar numbers of adverse events wereobserved in all patient groups; however, sexualdysfunction, in the form of erectile dysfunction(ED) and ejaculatory disorders, was more com-mon among finasteride-treated patients. Levels ofvasodilatory events, potentially linked to α-blockade, were similar between all three groups,as was incidence of AUR. This is in accordancewith previous reports of both drugs.15,32
The improvements observed with finasteridein this study are higher than those of the VAstudy, but are significantly lower than those seenwith α-blockade by alfuzosin. Patients were notselected or stratified according to prostate sizeand so the potential effects of this variable on out-come could not be analyzed.
A longer-term, but smaller-scale study indi-cated that the combination of alfuzosin and finas-teride brought about greater improvements in I-PSS and urinary flow.33 One hundred and thirty-eight BPH patients with prostates ≥ 60 ml and
I–PSS > 13 were treated with alfuzosin, finas-teride, or both for 3 years. Improved urinary flowand I-PSS results were observed in 84%, 74%, and96% of patients, respectively. These findings haveyet to be confirmed by larger-scale trials, howev-er.
DOXAZOSIN AND FINASTERIDE
PREDICT
A large-scale, placebo-controlled study designedto evaluate the potential benefits of combining anα-blocker with a 5α-reductase inhibitor was con-ducted using the α1-selective adrenoceptor antag-onist doxazosin in the Prospective EuropeanDoxazosin and Combination Therapy (PRE-DICT) Trial.34
The 1-year trial took place at 90 centers inEurope. Following a 2-week run-in period, 1095men aged 50–80 with an I-PSS ≥12 and Qmax
≥ 5 ml/s but ≤ 15 ml/s in a total void of 150 ml ormore, were randomized to receive doxazosinalone, finasteride alone, a combination of bothdrugs, or placebo for 52 weeks. Patients receivingdoxazosin underwent a 10-week titration period,while the dose was increased from 1 mg to 8 mgon the basis of treatment response as judged byI–PSS and Qmax, as part of their regimen.
Participants were assessed at baseline forI–PSS and Qmax and then at regular intervals (10,14, 26, 39, and 52 weeks) throughout the studyperiod. Blood pressure, heart rate, and adverseevents were also recorded regularly over the 12-month period, while PSA, electrocardiography,and standard blood tests were performed at base-line and then again on conclusion of the trial.Prostate volume was estimated using DRE.
In total, 1007 patients were included in theintention to treat analysis. Mean doxazosin dose
Ch 05 13/5/05 3:12 pm Page 71

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA72
was 6.4 mg/day in the monotherapy group and6.1 mg/day in the combination group.
Men who received doxazosin alone or in com-bination had significantly improved I-PSS resultscompared to those who received finasteride alone(p ≤ 0.0001) or placebo (p < 0.01), for bothobstructive and irritative symptoms (Figure 5.3).Mean I-PSS improvements were –8.3, –8.5, –6.6,and –5.7 points, respectively. No significant dif-ference was observed between the doxazosin andcombination groups or between the finasterideand placebo groups. Obstructive but not irritativesymptoms improved with finasteride comparedto placebo at endpoint (p < 0.05).
Again, for Qmax, a statistically significantimprovement was observed in the doxazosin andcombination groups (mean increases of 3.6 ml/sand 3.8 ml/s, respectively) compared to bothplacebo and finasteride alone (1.4 ml/s and1.8 ml/s, respectively, both p ≥ 0.0001). Noimprovement above placebo was observed withfinasteride treatment alone.
Discontinuation due to adverse events wassimilar between groups, however, side-effects dif-fered according to treatment regimen.
Participants treated with doxazosin alone or incombination were more likely to report asthenia,dizziness, and hypotension, while patients treatedwith finasteride and doxazosin in combinationwere more likely to suffer ED. No significant dif-ference in ED was observed between themonotherapy groups.
The PREDICT study demonstrated that, inthis patient group, doxazosin more effectivelyimproves symptoms of BPH and urinary flowthan finasteride alone or placebo. The findingsconfirm previous studies indicating the efficacy ofdoxazosin in the treatment of LUTS,35–37 and alsoreinforce the findings of the VA Study, callinginto question the value of 5α-reductase inhibitionin patients with smaller prostates.17,38,39
MTOPS
The results of all three large-scale studiesdescribed above suggest that the role of 5α-reduc-tase inhibitors as generalized monotherapy forLUTS may be somewhat limited, a finding atvariance with some of the original studies onfinasteride.15,16,23,24 An additional, longer-term
Points ml/s
*p < 0.001 for comparisons with placebo or finasteride alone
Reduction in I-PSS Increase in Qmax
0 2 4 6 8 0 2 4 6
*
*
*
*
doxazosin
doxazosin + finasteride
finasteride
placebo
FIGURE 5.3 PREDICT Study: symptom improvement at 1 year according to treatment group. I-PSS, InternationalProstate Symptom Score; Qmax, peak urinary flow.
Ch 05 13/5/05 3:12 pm Page 72

COMBINATION THERAPY IN THE TREATMENT OF BPH 73
trial, which progressed in parallel to these studies,has generated important new information onboth the clinical potential of 5α-reductaseinhibitors as monotherapy and the potential ofdrug combinations.
The Medical Therapy of Prostatic Symptoms(MTOPS) trial, a prospective, randomized, dou-ble-blind, multicenter, placebo-controlled trial,was established to determine whether medicaltherapy can prevent or delay the progression ofBPH in the long term.40 Further elucidation ofthe natural history of BPH, determining baselinefactors associated with more rapid disease pro-gression, was a secondary aim of the study.
In 18 academic centers across the US a total of3 047 patients were recruited and randomized toreceive doxazosin, finasteride, a combination ofboth, or placebo.41 Mean age of participants was62.6 years, most were white (82.6%), with 8.8%black and 7.2% Hispanic participants. The inclu-sion/exclusion criteria allowed men with allprostate sizes to be enrolled, as long as the serumPSA was less than 10 ng/ml. This resulted in awide distribution of prostate sizes and serumPSA values allowing for stratified analyses ofsubsets based on these criteria.
Disease progression was defined as a worsen-ing of BPH symptoms according to the AUAsymptom index (AUASI).42 Progression wasdeemed to have occurred in the case of one of thefollowing: a 4-point rise in AUASI, confirmed bya second visit within 4 weeks; a 50% increase increatinine relative to baseline levels; AUR; two ormore urinary tract infections (UTIs) within 1year or a single episode of urosepsis due to blad-der outlet obstruction (BOO); socially unaccept-able incontinence. The first occurrence of any ofthe above events indicated BPH progression.Progression as an endpoint represented a novelconcept at the time of the initiation of the
MTOPS study, although the PLESS study as wellas the dutasteride studies later on utilized AURand surgery as endpoints in their study design.15,17
Entirely novel was the concept of utilizing athreshold to define symptom progression. Basedon data from the VA Cooperative study, in whichmen perceived general improvement in theirsymptom status once the AUASI improved bymore than 3 points, a threshold of 4 points waschosen — to be confirmed within 4 weeks — toindicate global subjective worsening of symptomstatus.43
To assess the natural history of BPH, Qmax,prostate volume, sexual function, and quality oflife were regularly recorded with respect to BPHsymptoms. Transrectal ultrasound and DREwere used to evaluate prostate volume, the SexualFunction Inventory Questionnaire evaluated sex-uality and the Short Form-36 Health Surveyinstrument recorded quality of life scores.Prostatic biopsies were obtained at baseline and at5 years (or at primary endpoint) in 37% of studyparticipants who volunteered to take part in abiopsy substudy.
Patients were randomized to receive 5 mgfinasteride and doxazosin placebo, 5 mg finas-teride and doxazosin titrated to up to 8 mg, titrat-ed doxazosin and finasteride placebo, or twoplacebo drugs.
The results of the trial suggest that the combi-nation of doxazosin and finasteride exerts a clini-cally relevant, positive effect on rates of diseaseprogression44 (Figure 5.4). Men who receivedcombination therapy were significantly less likelyto experience BPH progression than those receiv-ing either monotherapy or placebo, with riskreduction rates of 39% for doxazosin, 34% forfinasteride, and 67% for combination therapycompared to placebo. Overall rates of BPH pro-gression events are shown in Figure 5.5.
Ch 05 13/5/05 3:12 pm Page 73

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA74
Invasive therapy and AUR risk were signifi-cantly reduced by finasteride and combinationtherapy (by 69 and 64%, and by 79 and 67%,respectively), while all treatment regimens (place-bo, doxazosin, finasteride, and combination)brought about a significant improvement inAUA symptom score (4.0, 6.0, 5.0, and 7.0, respec-tively) and Qmax (1.4, 2.5, 2.2, and 3.7 ml/s, respec-tively) at 4 years.
AUA symptom score and Qmax improved sig-nificantly more in the combination therapy groupcompared to the monotherapy groups, while
adverse events were similar to previously report-ed studies.
In addition to indicating the potential benefitsof combination therapy, MTOPS providedimportant data regarding the natural history ofuntreated BPH and the prediction of BPHpatients who will respond most effectively tomedical treatment45–47 (Figure 5.6). While thepatients receiving finasteride alone or in combi-nation experienced the expected decrease inprostate volume, patients on placebo or doxazosinalone experienced an increase in prostate volume
BPH progression Invasive therapy Acute urinary retention
Doxazosin Combination Finasteride
100
80
60
40
20
0% r
isk
redu
ctio
n co
mpa
red
to p
lace
bo
FIGURE 5.4 MTOPS Study: risk reduction of BPH clinical progression, BPH-related invasive surgery, and acute uri-nary retention in treated patients in comparison to placebo.
Renal insufficiency (0%)
UTI/urosepsis (1%)Incontinence (9%)
AUR (12%)
4 point AUA (78%)
FIGURE 5.5 MTOPS Study: distribution of BPH progression events, all groups. AUR, acute urinary retention; UTI,urinary tract infection; AUA, American Urological Association.
Ch 05 13/5/05 3:12 pm Page 74
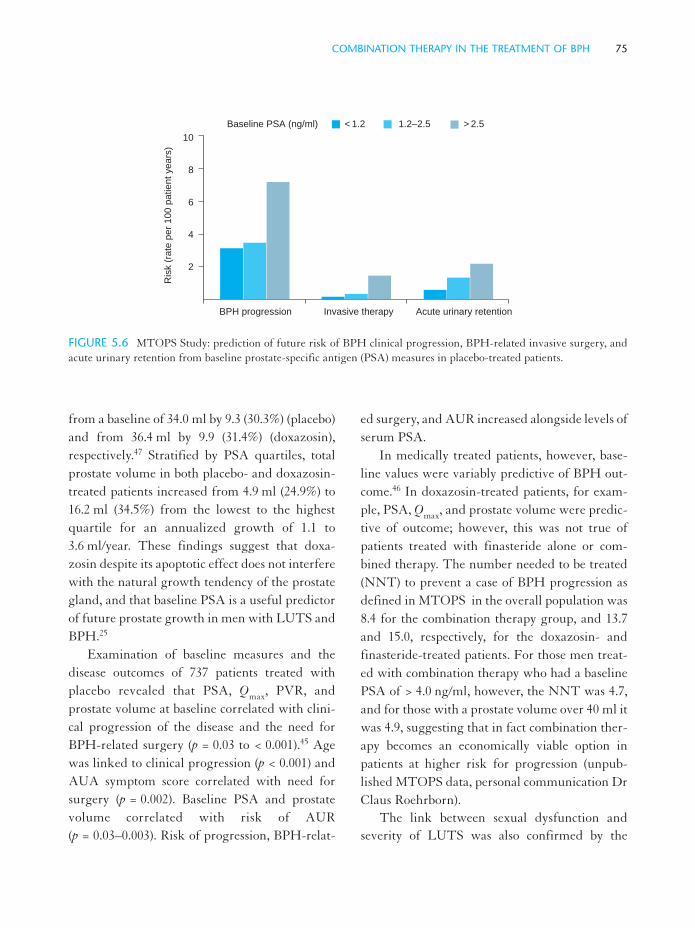
COMBINATION THERAPY IN THE TREATMENT OF BPH 75
from a baseline of 34.0 ml by 9.3 (30.3%) (placebo)and from 36.4 ml by 9.9 (31.4%) (doxazosin),respectively.47 Stratified by PSA quartiles, totalprostate volume in both placebo- and doxazosin-treated patients increased from 4.9 ml (24.9%) to16.2 ml (34.5%) from the lowest to the highestquartile for an annualized growth of 1.1 to3.6 ml/year. These findings suggest that doxa-zosin despite its apoptotic effect does not interferewith the natural growth tendency of the prostategland, and that baseline PSA is a useful predictorof future prostate growth in men with LUTS andBPH.25
Examination of baseline measures and thedisease outcomes of 737 patients treated withplacebo revealed that PSA, Qmax, PVR, andprostate volume at baseline correlated with clini-cal progression of the disease and the need forBPH-related surgery (p = 0.03 to < 0.001).45 Agewas linked to clinical progression (p < 0.001) andAUA symptom score correlated with need forsurgery (p = 0.002). Baseline PSA and prostatevolume correlated with risk of AUR(p = 0.03–0.003). Risk of progression, BPH-relat-
ed surgery, and AUR increased alongside levels ofserum PSA.
In medically treated patients, however, base-line values were variably predictive of BPH out-come.46 In doxazosin-treated patients, for exam-ple, PSA, Qmax, and prostate volume were predic-tive of outcome; however, this was not true ofpatients treated with finasteride alone or com-bined therapy. The number needed to be treated(NNT) to prevent a case of BPH progression asdefined in MTOPS in the overall population was8.4 for the combination therapy group, and 13.7and 15.0, respectively, for the doxazosin- andfinasteride-treated patients. For those men treat-ed with combination therapy who had a baselinePSA of > 4.0 ng/ml, however, the NNT was 4.7,and for those with a prostate volume over 40 ml itwas 4.9, suggesting that in fact combination ther-apy becomes an economically viable option inpatients at higher risk for progression (unpub-lished MTOPS data, personal communication DrClaus Roehrborn).
The link between sexual dysfunction andseverity of LUTS was also confirmed by the
BPH progression Invasive therapy Acute urinary retention
Baseline PSA (ng/ml) < 1.2 1.2–2.5 > 2.5
10
8
6
4
2
Ris
k (r
ate
per
100
patie
nt y
ears
)
FIGURE 5.6 MTOPS Study: prediction of future risk of BPH clinical progression, BPH-related invasive surgery, andacute urinary retention from baseline prostate-specific antigen (PSA) measures in placebo-treated patients.
Ch 05 13/5/05 3:12 pm Page 75

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA76
MTOPS data.48 A correlation was observedbetween LUTS and five domains of sexual dys-function (libido, sexual function, ejaculatoryfunction, the patient’s assessment of his sexualproblems, and overall satisfaction). In addition,men with larger prostates were more likely tohave low libido, low overall sexual functioning,reduced ejaculatory function, and greater sexualproblems.
ADDITIONAL COMBINATION STUDIES
Anticholinergic plus α-blocker
The anticholinergic agent tolterodine is used forthe treatment of incontinence related to detrusorinstability, while the α-blocker tamsulosin iscommonly used for the treatment of BOO.Patients may present with concomitant BOO anddetrusor instability. Investigation of the efficacyof a combination of 2 mg tolterodine twice dailyand 0.4 mg tamsulosin once daily was performedto determine whether patient quality of lifeimproved as a result.49
Fifty patients took part in the study, and allinitially received tamsulosin for 1 week. Afterthis point, the patients were randomized to con-tinue with this regimen or to receive tolterodinein addition to tamsulosin. Baseline urodynamicsand quality of life were recorded and these meas-ures were repeated after 3 months of treatment.
Quality of life scores were found to increasesignificantly in patients who received combina-tion therapy (p = 0.0003), while no increase wasobserved in patients who received tamsulosinalone. In addition, a significant difference inmaximum detrusor pressure and unstable con-traction pressure was observed in the combina-tion group. Qmax and volume at first contractionimproved significantly in both groups and noAUR was reported. The results suggest that this
combination is a safe and effective treatmentoption for this patient group.
Combined ‘natural’ products
The role of plant-derived therapy in the treat-ment of BPH has been, and still is, consideredcontroversial,50–52 and the combination of prod-ucts such as Serenoa repens, β-sitosterol, andPygeum africanum is even more debatable.
One trial comparing a combination of cer-nitin, Serenoa repens, β-sitosterol, and vitamin Eto placebo indicated potential benefits for patientsreceiving the active agents.53 In total, 127 BPHpatients with a Qmax of 5–15 ml/s took part in thestudy and were randomized to receive either thecombined therapy or placebo for 3 months.AUASI, Qmax, PSA, and PVR were assessed atbaseline and on conclusion of the trial.
Significant reductions in nocturia (p < 0.001)and daytime frequency (p < 0.04) were observedin the active arm of the study compared to theplacebo group. Average score on AUASI alsoimproved in this group compared to placebo(p < 0.014). No difference in PSA, Qmax, or PVRwas observed and no serious side-effects werereported.
The combination of phytotherapy with con-ventional pharmacotherapy has not been fullyinvestigated to date; however, a 3-month trial oftamsulosin, cernitin, or a combination of the tworevealed significant improvements in I-PSS in allthree groups, but improved Qmax and average uri-nary flow only in the tamsulosin and combinationgroups.54
DISCUSSION
Several large-scale studies have indicated that thecombination of an α-blocker with a 5α-reductaseinhibitor does not add any clinically significant
Ch 05 13/5/05 3:12 pm Page 76

COMBINATION THERAPY IN THE TREATMENT OF BPH 77
value to α-blockade alone.6,31,34 However, thelarger and longer-term MTOPS study wouldappear to be at variance with these findings44
(Table 5.1). In this trial, participants were fol-lowed up for 4.5 years on average and those whowere involved in the pilot phase were followed upfor an average of 6 years. This is considerablylonger than previous trials of combination thera-py for BPH. The VA and PREDICT studies hada duration of 1 year, while the ALFIN study last-ed just 6 months.
Although earlier trials indicated no benefitover and above α-blockade with the addition offinasteride treatment, the evidence provided byMTOPS has shown that combination therapymay be appropriate for many patients, particular-ly those with larger glands and higher baselineserum PSA values. This observation is reflectedin the recently published AUA Guidelines on theManagement of BPH state, on the basis of panelconsensus, that the combination of an α-blockerand a 5α-reductase inhibitor may be appropriatein LUTS patients with demonstrable enlarge-ment of the prostate.55
Any reduction in risk of AUR and BPH-related surgery associated with combination ther-apy described in the MTOPS study should beweighed up against cost and other factors on anindividual basis, however.55 The panel stated thatthose most likely to benefit are men at greatestrisk of disease progression, i.e. those with largerprostates and higher PSA levels. Although thebest-tested combination to date is doxazosin andfinasteride, and the safety of other combinationshas not been fully assessed, the panel assumes thatany combination of these drug classes would leadto a similar degree of clinical benefit.
Additional factors should also be consideredin the combination therapy debate. Cost issues areof primary importance, as dual therapy is obvi-
ously more expensive than monotherapy alone. Ithas been suggested that dual therapy need not becontinued indefinitely, however, which may havea bearing on associated costs.
Baldwin et al. found that BPH patients treat-ed initially with finasteride plus an α-blocker tol-erated discontinuation of combination therapyafter 1 year with no compromise in clinical bene-fit.56 A group of BPH patients (n = 270) were pre-scribed 2, 4, or 8 mg doxazosin alongside 5 mgfinasteride for a period of 3, 6, 9, or 12 months,after which doxazosin was discontinued. Of thosewho discontinued combination therapy at 12months, 84% of the 2 mg group, 85% of the 4 mggroup, and 87% of the 8 mg group experienced noincrease in AUA symptom score and reported nodesire to resume taking doxazosin 1 month later.Similarly high tolerance levels were reported inpatients with BOO and moderately enlargedprostates who discontinued combination therapyafter 9 months.57
Other factors, such as the difference in theeffects of 5α-reductase inhibitors and α-blockerson PSA levels,58 and the recently discovered rela-tionship between the use of finasteride and areduction in risk of prostate cancer,59 may alsoinfluence the use of combination therapy.
It has been suggested that prostate volumeinfluences the outcome of patients treated withfinasteride, and that men with larger prostateswill benefit more from treatment with 5α-reduc-tase inhibitors.16,17 The VA, ALFIN, and PRE-DICT studies all included BPH patients with rel-atively small prostates (36.2–38.4 ml, mean41.2 ml, and mean 36.3 g, respectively). Men withlarger glands may therefore benefit more fromcombination treatment than those with smallerglands, who might be better treated with an α-blocker alone.60 The ongoing subset stratification
Ch 05 13/5/05 3:12 pm Page 77

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA78
TABL
E 5.
1C
ompa
riso
n of
larg
e-sc
ale
com
bina
tion
stud
ies
of B
PH
trea
tmen
ts.
*Eva
luat
ion
tool
s: fo
r V
A, P
RE
DIC
T, a
nd M
TO
PS
= A
mer
ican
Uro
logi
cal A
ssoc
iatio
n sy
mpt
om sc
ore;
for
AL
FIN
= I
nter
natio
nal P
rost
ate
Sym
ptom
Sco
re.
Mea
n ag
eM
ean
base
line
Reg
imen
Sym
ptom
sco
re*
Qm
axP
rost
ate
volu
me
Dur
atio
n(y
ears
)pr
osta
te v
olum
e (m
l)n
(dai
ly d
ose)
% im
prov
emen
t%
impr
ovem
ent
% c
hang
e
VA
Coo
pera
tive
Stud
y61
year
6536
.2–3
8.4
305
Ter
azos
in (1
0m
g)38
26+
1
310
Fin
aste
ride
(5m
g)20
15–1
7
309
Com
bina
tion
3931
–19
305
Pla
cebo
1613
+1
AL
FIN
316
mon
ths
6341
.235
8A
lfuz
osin
(10
mg)
4119
–0.5
344
Fin
aste
ride
(5m
g)36
18–1
1
349
Com
bina
tion
3923
–12
PR
ED
ICT
341
year
6336
.3g
275
Dox
azos
in (<
8m
g)49
35—
264
Fin
aste
ride
(5m
g)39
18—
286
Com
bina
tion
4937
—
270
Pla
cebo
3310
—
MT
OP
S444
year
s62
31.0
756
Dox
azos
in (4
/8m
g)35
24+
18
768
Fin
aste
ride
(5m
g)30
21–1
6
786
Com
bina
tion
4135
–13
737
Pla
cebo
2413
+18
Ch 05 13/5/05 3:12 pm Page 78

COMBINATION THERAPY IN THE TREATMENT OF BPH 79
of the MTOPS data may provide further insightinto this area.
CONCLUSIONS
The reduction in frequency of TURP for thetreatment of BPH and the rise in use of medicaltherapy suggest high levels of patient and physi-cian satisfaction with pharmacologic options.However, future advances in available drugpreparations may be limited. Dual therapy,involving preparations from different drug class-es, may represent a further potential avenue formedical BPH therapy.
The efficacy of the α-blockers doxazosin, ter-azosin, alfuzosin, and tamsulosin and the 5α-reductase inhibitors finasteride and dutasteridehas been proven in many large, well-controlledclinical trials. However, the combination of thetwo drug classes has produced variable clinicalresults. Until recently, the benefits that might log-ically be expected from therapy targeting twoseparate elements of BPH pathology—namely,prostatic enlargement and an increase in smoothmuscle tone—had not been described in larger-scale studies.
The results of the MTOPS trial, however,indicate that symptomatic improvements in BPHoccur to a greater extent in men receiving doxa-zosin and finasteride in combination compared toeither agent alone. Disease progression, asassessed mainly by a four-point rise in theAUASI, was significantly less likely in patients inthe combination group, while AUR and BPHsurgery were also less common in this group.
The strength of the findings has led to theinclusion of recommendations for combinationtherapy in suitable patients in the AUA BPHmanagement guidelines. Further trials assessing
the safety and efficacy of other types of α-blockerand 5α-reductase inhibitor in combination maybe expected to follow.
The value of different types of combinationtherapy, involving plant-derived preparations orthe use of anticholinergics for example, remainsto be determined.
REFERENCES
1. Holtgrewe H L, Bay-Nielsen H, Carlsson P et al.The economics of the management of lower uri-nary tract symptoms and benign prostatic hyper-plasia. In: Denis L, Griffiths K, Khoury S et al.(eds). The fourth international consultation onbenign prostatic hyperplasia (BPH), Paris, 2–5 July,1997. Plymouth, UK: Health Publications, 1998:63–81
2. Baine W, Yu W, Summe J P, Weis K A.Epidemiologic trends in the evaluation and treat-ment of lower urinary tract symptoms in elderlymale Medicare patients from 1991 to 1995. J Urol1998; 160: 816–820
3. McVary K T. Medical therapy for benign prostatichyperplasia progression. Curr Urol Rep 2002; 3:269–275
4. Berry S J, Coffey D S, Walsh P C, Ewing L L. Thedevelopment of human benign prostatic hyperpla-sia with age. J Urol 1984; 132: 474–479
5. Madsen F A, Bruskewitz R C. Clinical manifesta-tions of benign prostatic hyperplasia. Urol ClinNorth Am 1995; 22: 291–298
6. Lepor H, Williford W O, Barry M J et al. for theVeterans’ Affairs Cooperative Studies BenignProstatic Hyperplasia Study Group. The efficacy ofterazosin, finasteride or both in benign prostatichyperplasia. N Engl J Med 1996; 335: 533–539
7. Chapple C R, Baert L, Thind P et al. and TheEuropean Tamsulosin Study Group. Tamsulosin0.4 mg once daily: tolerability in older and youngerpatients with lower urinary tract symptoms sugges-tive of benign prostatic obstruction (symptomaticBPH). Eur Urol 1997; 32: 462–470
Ch 05 13/5/05 3:12 pm Page 79

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA80
8. Roehrborn C G for the ALFUS Study Group.Efficacy and safety of once-daily alfuzosin in thetreatment of lower urinary tract symptoms andclinical benign prostatic hyperplasia: a randomised,placebo-controlled trial. Urology 2001; 58: 953–959
9. Janknegt R A, Chapple C R. Efficacy and safety ofthe alpha-1 blocker doxazosin in the treatment ofbenign prostatic hyperplasia: analysis of 5 studies.Eur Urol 1993; 24: 319–326
10. Kirby R S, Andersen M, Gratzke P et al. A com-bined analysis of double-blind trials of the efficacyand tolerability of doxazosin-gastrointestinal thera-peutic system, doxazosin standard and placebo inpatients with benign prostatic hyperplasia. BJU Int2001; 87: 192–200
11. Van Kerrebroeck P, Jardin A, van Cangh P, LavalK U. Long-term safety and efficacy of a once-dailyformulation of alfuzosin 10 mg in patients withsymptomatic benign prostatic hyperplasia: open-label study. Eur Urol 2002; 41: 54–61
12. Marks L S, Partin A W, Dorey F J et al. Long-termeffects of finasteride on prostate tissue composition.Urology 1999; 53: 574–580
13. Saez C, Gonzalez-Baena A C, Japon M A et al.Regressive changes in finasteride-treated humanhyperplastic prostates correlate with an upregula-tion of TGF-beta receptor expression. Prostate1998; 37: 84–90
14. Feneley M R, Span P N, Schalken J A et al. Aprospective randomized trial evaluating tissueeffects of finasteride therapy in benign prostatichyperplasia. Prostate Cancer Prostatic Dis 1999; 2:277–281
15. McConnell J D, Bruskewitz R, Walsh P et al. forthe Finasteride Long-term Efficacy and SafetyStudy Group. The effect of finasteride on the riskof acute urinary retention and the need for surgicaltreatment among men with benign prostatic hyper-plasia. N Engl J Med 1998; 338: 557–563
16. Roehrborn C G, Bruskewitz R, Nickel G C et al.Urinary retention in patients with finasteride orplacebo over 4 years. Characterization of patientswith ultimate outcomes. The PLESS Study Group.Eur Urol 2000; 37: 528–536
17. Roehrborn C G, Boyle P, Nickel J C et al. on behalfof the ARIA3001, ARIA3002 and ARIA3003 StudyInvestigators. Efficacy and safety of a dual inhibitorof 5 alpha-reductase types 1 and 2 (dutasteride) inmen with benign prostatic hyperplasia. Urology2002; 60: 434–441
18. Boyle P, Gould A L, Roehrborn C G. Prostate vol-ume predicts outcome of treatment of benign pro-static hyperplasia with finasteride: meta-analysis ofrandomized clinical trials. Urology 1996; 48:398–405
19. Roehrborn C G. Is there a place for combinationmedical therapy? Curr Opin Urol 2001; 11: 17–25
20. Brawer M K, Lin D W, Williford W O et al. Effectof finasteride and/or terazosin on serum PSA:results of VA Cooperative Study #359. Prostate1999; 39: 234–239
21. Lepor H, Auerbach S, Puras-Baez A et al. A ran-domized, placebo-controlled multicenter study ofthe efficacy and safety of terazosin in the treatmentof benign prostatic hyperplasia. J Urol 1992; 148:1467–1474
22. Brawer M K, Adams G, Epstein H, TerazosinBenign Prostatic Hyperplasia Study Group.Terazosin in the treatment of benign prostatichyperplasia. Arch Fam Med 1993; 2: 929–935
23. Gormley G J, Stoner E, Bruskewitz R C et al. Theeffect of finasteride in men with benign prostatichyperplasia. N Engl J Med 1992; 327: 1185–1191
24. The Finasteride Study Group. Finasteride (MK-906) in the treatment of benign prostatic hyperpla-sia. Prostate 1993; 22: 291–299
25. Glassman D T, Chon J K, Borkowski A et al.Combined effect of terazosin and finasteride onapoptosis, cell proliferation and transforminggrowth factor-beta expression in benign prostatichyperplasia. Prostate 2001; 46: 45–51
26. Vashi V, Chung M, Hilbert J et al. Pharmacokineticinteraction between finasteride and terazosin, butnot finasteride and doxazosin. J Clin Pharmacol1998; 38: 1072–1076
27. Erdogru T, Ciftcioglu M A, Emreoglu I et al.Apoptotic and proliferative index after alpha-1-adrenoceptor antagonist and/or finasteride treat-
Ch 05 13/5/05 3:12 pm Page 80

COMBINATION THERAPY IN THE TREATMENT OF BPH 81
ment in benign prostatic hyperplasia. Urol Int 2002;69: 287–292
28. Martin D, Jammes D, Angel I. Effects of alfuzosinon urethral and blood pressures in conscious malerats. Life Sci 1995; 57: 387–391
29. Rouquier L, Claustre Y, Benavides J. α1-Adrenoceptor antagonists differentially controlserotonin release in the hippocampus and striatum:a microdialysis study. Eur J Pharmacol 1994; 261:59–64
30. Martin D J, Lluel P, Guillot E et al. Comparativealpha-1 adrenoceptor subtype selectivity and func-tional uroselectivity of alpha-1 adrenoceptor antag-onists. J Pharmacol Exp Ther 1997; 282: 228–235
31. Debruyne F M, Jardin A, Colloi D et al. Sustainedrelease alfuzosin, finasteride and the combinationof both in the treatment of benign prostatic hyper-plasia. European ALFIN Study Group. Eur Urol1998; 34: 169–175
32. Jardin A, Bansadoun H, Delauche-Cavallier M C,Attali P. Alfuzosin for treatment of benign prostat-ic hyperplasia. Lancet 1991; 337: 1457–1461
33. Loran O B, Pushkar’ D I U, Rasner P I.Comparative evaluation of the effectiveness andsafety of combined drug therapy of patients withbenign prostatic hyperplasia with finasteride andalfuzozin [in Russian]. Urologiia 2002; Jan–Feb:19–22
34. Kirby R S, Roehrborn C, Boyle P et al. for thePREDICT Study Investigators. Efficacy and toler-ability of doxazosin and finasteride, alone or incombination, in treatment of symptomatic benignprostatic hyperplasia: the Prospective EuropeanDoxazosin and Combination Therapy (PREDICT)Trial. Urology 2003; 61: 119–126
35. Christensen M M, Bendix Holme J, Rasmussen P Cet al. Doxazosin treatment in patients with prostat-ic obstruction. A double-blind placebo-controlledstudy. Scand J Urol Nephrol 1993; 27: 39–44
36. Fawzy A, Braun K, Lewis G P et al. Doxazosin inthe treatment of benign prostatic hyperplasia innormotensive patients: a multicenter study. J Urol1995; 154: 105–109
37. Lepor H, Kaplan S A, Klimberg I et al. Doxazosinfor benign prostatic hyperplasia: long-term efficacyand safety in hypertensive and normotensivepatients. J Urol 1997; 157: 525–530
38. Lepor H, Williford W O, Barry M J et al. for theVeterans’ Affairs Cooperative Studies BenignProstatic Hyperplasia Study Group. The impact ofmedical therapy on bother due to symptoms, qual-ity of life and global outcome and factors predictingresponse. J Urol 1998; 160: 1358–1367
39. Roehrborn C G, Boyle P, Bergner D et al. for thePLESS Study Group. Serum prostate-specific anti-gen and prostate volume predict long-term changesin symptoms and flow rate: results of a four-year,randomized trial comparing finasteride versusplacebo. Urology 1999; 54: 662–669
40. Bautista O M, Kusek J W, Nyberg L M et al. for theMTOPS Research Group. Study design of theMedical Therapy of Prostatic Symptoms (MTOPS)trial. Control Clin Trial 2003; 24: 224–243
41. Kusek J W, Ahrens A, Burrows P K et al. for theMTOPS Research Group. Recruitment for a clini-cal trial of drug treatment for benign prostatichyperplasia. Urology 2002; 59: 63–67
42. Barry M J, Fowler F J Jr, O’Leary M P et al. and theMeasurement Committee of the AmericanUrological Association. The American UrologicalAssociation symptom index for benign prostatichyperplasia. J Urol 1992; 148: 1549–1557
43. Jacobsen S J, Guess H A, Panser L et al. A popula-tion-based study of health care-seeking behaviourfor the treatment of urinary symptoms: theOlmstead County study of urinary symptoms andhealth status among men. Arch Fam Med 1993; 2:729–735
44. McConnell J D, Roehrborn C G, Bautista O M etal. The long-term effect of doxazosin, finasteride,and combination therapy on the clinical progres-sion of benign prostatic hyperplasia. N Engl J Med2003; 349: 2387–2398
45. McConnell J D, Roehrborn C G, Slawin K M et al.Baseline measures predict the risk of benign pro-static hyperplasia clinical progression in placebo-treated patients. J Urol 2003; 169 (Suppl 4): abstract1287
Ch 05 13/5/05 3:12 pm Page 81

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA82
46. Kaplan S A, Roehrborn C G, McConnell J D et al.Baseline symptoms, uroflow and post-void residualurine as predictors of BPH clinical progression inthe medically treated arms of the MTOPS trial. JUrol 2003; 169 (Suppl 4): abstract 1289
47. Roehrborn C G, McConnell J D, Jacobs S C et al.Baseline prostate volume and serum PSA predictrate of prostate growth: analysis of the MTOPSdata. J Urol 2003; 169 (Suppl 4): abstract 1361
48. McVary K, Foley J, Bautista O, Kusek J.Association of lower urinary tract symptoms(LUTS) with sexual function in men participatingin a clinical trial of medical therapy for benign pro-static hyperplasia. J Urol 2003; 169 (Suppl 4):abstract 1252
49. Athanasopoulos A, Gyftopoulos K, Giannitsas K etal. Combination treatment with an alpha-blockerplus an anticholinergic for bladder outlet obstruc-tion: a prospective, randomized, controlled study. JUrol 2003; 169: 2253–2256
50. Gerber G S. Phytotherapy for benign prostatichyperplasia. Curr Urol Rep 2002; 3: 285–291
51. Dreikorn K. The role of phytotherapy in treatinglower urinary tract symptoms and benign prostatichyperplasia. World J Urol 2002; 19: 426–435
52. Levin R M, Das A K. A scientific basis for the ther-apeutic effects of Pygeum africanum and Serenoarepens. Urol Res 2000; 28: 201–209
53. Preuss H G, Marcusen C, Regan J et al.Randomized trial of a combination of naturalproducts (cernitin, saw palmetto, β-sitosterol, vita-min E) on symptoms of benign prostatic hyperpla-sia (BPH). Int Urol Nephrol 2001; 33: 217–225
54. T Aoki A, Naito K, Hashimoto O et al. Clinicalevaluation of the effect of tamsulosin hydrochlorideand cernitin pollen extract on urinary disturbanceassociated with benign prostatic hyperplasia in amulticentered study [In Japanese]. Hinyokika Kiyo2002; 48: 259–267
55. AUA BPH Guideline Update Panel. The manage-ment of BPH, 2003. https://shop.auanet.org/timss-net/products/guidelines/bph_management.cfm
56. Baldwin K C, Ginsberg P C, Roehrborn C G,Harkaway R C. Discontinuation of alpha-blockadeafter initial treatment with finasteride and doxa-zosin in men with lower urinary tract symptomsand clinical evidence of benign prostatic hyperpla-sia. Urology 2001; 58: 203–209
57. Baldwin K C, Ginsberg P C, Harkaway R C.Discontinuation of alpha-blockade after initialtreatment with finasteride and doxazosin for blad-der outlet obstruction. Urol Int 2001; 66: 84–88
58. Keetch D W, Andriole G L, Ratliff T L, CatalonaW J. Comparison of percent free prostate-specificantigen levels in men with benign prostatic hyper-plasia treated with finasteride, terazosin or watch-ful waiting. Urology 1997; 50: 901–905
59. Thompson I M, Goodman P J, Tangen C M et al.The influence of finasteride on the development ofprostate cancer. Published at www.nejm.org June24, 2003 (doi: 10.1056/NEJMoa030660)
60. Horninger W, Bartsch G. Drug therapy of benignprostatic hyperplasia. Is combination therapy with5 alpha-reductase inhibitors and alpha-receptorblockers effective? [in German]. Urologe A 2002;41: 442–446
Ch 05 13/5/05 3:12 pm Page 82

The differential effects of adrenoceptorantagonists on prostate tissue growth
N Kyprianou6
83
INTRODUCTION
Benign prostatic hyperplasia (BPH) is the mostfrequently diagnosed neoplastic disease in theaging male, affecting approximately 85% of allmen over 50 years of age. By the ninth decade oflife, 50% of all American men require treatmentfor symptomatic relief of the lower urinary tractsymptoms (LUTS) associated with BPH.Clinically, BPH is characterized by prostaticenlargement and the accompanying symptoms ofprogressive bladder outlet obstruction.
Histologically, BPH can present as hyperpla-sia in both the stromal and glandular componentsof the gland and arises in the periurethral andtransition zones.1 It has been hypothesized thatthis abnormal proliferation arises because of theability of the prostate stroma to retain an embry-onic growth potential that is ‘reawakened’ in theaging gland.2 Although aging and the presence ofa functional testis have become established asmajor factors causally related to the developmentof the disease,3,4 the molecular processes involvedin the pathogenesis of BPH remain poorly under-stood.
In this chapter we review some recent clinicaldata5 that may provide additional insight into thepathophysiology of BPH and facilitate the devel-opment of more effective pharmacologic therapy.
MEDICAL MANAGEMENT OF BPH: AHISTORICAL PERSPECTIVE
The development of LUTS secondary to prostat-ic enlargement is thought to be caused by static
(mechanical) and dynamic components of ure-thral restriction. The mechanical component aris-es from the physical obstruction of urinary out-flow caused by urethral constriction, induced bythe mass of the enlarged gland. The dynamiccomponent is related to the variations in smoothmuscle tone in the fibromuscular stroma, prostatecapsule, and bladder neck.6 Treatment modalitiestherefore aim either to reduce the mechanicalobstruction, or to induce relaxation of the peri-urethral prostatic smooth muscle.
A critical level of androgen is required tomaintain the benign growth pattern and andro-gen deprivation results in significant involutionof the glandular epithelial component of theprostate,7 without affecting stromal growth.Androgen ablation/deprivation undoubtedlyleads to a favorable ‘therapeutic’ response incanine BPH,4 a species where the bulk of thehyperplasia is androgen-dependent epithelialproliferation. In man, however, the maximaltherapeutic effect of androgen deprivationappears to be limited by both the substantial stro-mal component of the proliferation1,8 and byintrinsic resistance of stromal cells to androgenmodulation.8
Given that at least 40% of the cellular volumeof the enlarged prostate is composed of stromalsmooth muscle, it is not surprising that pharma-cologic intervention at this level has proved high-ly successful. In this context, α1-adrenoceptorantagonists (α-blockers) are widely used to pro-duce acute symptomatic relief. The classic beliefis that α-blockers reduce the tone of the prostatesmooth muscle and thereby inhibit the dynamiccomponent of the obstruction.9,10 The pharmacol-
Ch 06 13/5/05 3:16 pm Page 83

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA84
ogy of α-blockers is described in detail else-where.11 The following represents a summary ofthe key features.
Periurethral smooth muscle tone, and there-fore urethral resistance, varies according to thedegree of sympathetic nervous system activationof the α1-adrenoceptors in the prostate andprostate capsule.12,13 Therefore, pharmacologicblockade of the α1-adrenoceptors would reducethe actions of noradrenaline (the endogenousneurotransmitter), resulting in tissue relaxation.This provided the impetus for the developmentof several α1-blockers and has resulted in wide-spread use of this class of drugs as first-line inter-vention in BPH.
Currently, four native α1-adrenoceptor sub-types—α1A, α1B, α1D, and α1L—have been identi-fied and are known to be located in the prostate.11
The best correlation between prostate tissue con-traction and binding with any α1-adrenoceptorrecognition site is with the α1A subtype.14,15 Manyinvestigators consider this evidence to be consis-tent with a primary role of this adrenoceptor sub-type in the control of prostate tone and urethralresistance. However, when considering the treat-ment of BPH symptoms, extraprostatic actions ofα1-blockers must also be taken into account11. Inparticular, α1-adrenoceptors in the bladder andbladder neck,16,17 and spinal cord,18,19 and onefferent pathways19,20 may make an importantcontribution to the overall improvements in uro-dynamic and symptom profiles that are observedshortly after the onset of therapy.
Although the immediate and short-term ther-apeutic benefit of α-blockers is believed to arisefrom the prostatic and extraprostatic physiologicactions listed above, it has become apparent thatin the long term other factors or loci may make anequally important contribution.5
THE α-BLOCKER PARADOX
Consistent with their actions as α-blockers onperiurethral stromal smooth muscle, the acuteclinical benefit of terazosin and doxazosin inBPH is well documented22.
In the early days of use in the management ofBPH, there was a general expectation that α-blockers might serve as clinical ‘sticking plaster’in the face of ongoing glandular hyperplasia;tachyphylaxis (tolerance) to the drug action wasanticipated. Although this may undoubtedlyoccur in individual patients, the effects of doxa-zosin and terazosin in BPH have been main-tained (Figure 6.1), in some cases for up to 7years,22–24 a period over which the prostate masswould be expected to increase by up to 50%.1 Theequivalent long-term data for doxazosin similar-ly show no overall evidence of tachyphylaxis. Onthe assumption that the increase in prostate bulk(the static component of obstruction) would resultin a corresponding increase in urethra resistance,considerable diminution in benefit might beanticipated over an equivalent time period.
0
–1
–2
–3
–4
–5
–6
–7Boy
arsk
y sc
ore,
mea
n ch
ange
fr
om b
asel
ine
Months 6 12 18 24 30 36 42 48 54 60
FIGURE 6.1 Long-term terazosin efficacy data. Datawere generated in open-label uncontrolled clinical trials.From 1 month onwards all points were significantly dif-ferent from baseline and there was no evidence of tachy-phylaxis.
Ch 06 13/5/05 3:16 pm Page 84

ADRENOCEPTOR ANTAGONIST EFFECTS ON PROSTATE TISSUE GROWTH 85
Several clinical papers now offer a partialexplanation of the well-documented, but unex-pected longevity of the α-blocker response.5,23,25
These were retrospective, placebo-controlledstudies involving a total of 134 BPH patients andwere designed to determine the effects of α-blockers on apoptosis and the interrelationshipwith symptom improvement. Importantly, eachpatient acted as his own control: LUTS and his-tochemical parameters were measured at baselineand at one other time point in the study after thepatient had been assigned to either placebo or α-blocker.
In three other studies, cell proliferation andapoptosis were evaluated in BPH patients, whocomprised an untreated control group and twocohorts treated with either terazosin or doxazosinat doses designed to provide symptom relief.26–28
The treatment period varied from 1 week to 3years. Terazosin was used at 1–10 mg/day anddoxazosin at 2–8 mg/day. Proliferation and apop-tosis of the stromal and epithelial cell components
of the prostate, obtained by initial biopsy or atprostatectomy, were quantified by Ki 67immunostaining and TUNEL (terminal trans-ferase UTP-end labeling) assay, respectively.
Both terazosin and doxazosin induced epithe-lial and stromal cell apoptosis within the firstmonth of treatment (Figure 6.2) when comparedwith the untreated controls (p < 0.05). Themarked induction of stromal apoptosis was paral-leled by significant decreases in smooth muscle α-actin expression (Figure 6.3). This loss of prostatesmooth muscle cells correlated with the morpho-logic stromal regression (measured by trichromestaining) and improvement in BPH symptoms.Proliferation was relatively unaffected by bothdrugs.
The data indicate that there is a significantinduction of apoptosis in the prostate epitheliumand stroma in response to terazosin and doxa-zosin (over the normal therapeutic dose range).Compared with the untreated controls, terazosininduced epithelial and stromal cellular apoptosis
30
25
20
15
10
5
0
Apo
ptot
ic in
dex
(%)
Control < 1 1–5 6–11 12–36(n = 31) (n = 12) (n = 12) (n = 9) (n = 9)
FIGURE 6.2 Effect of terazosin on prostate apoptosis inpatients with BPH. The apoptotic index of glandularepithelial ( ) and stromal ( ) smooth muscle cells inbiopsy sections is expressed as mean percentage ofTUNEL–positive cells/total number of cells after variousperiods of terazosin therapy (1–10 mg/day). (Adaptedfrom Chon et al.23)
60
50
40
30
20
10
0Str
omal
sm
ooth
mus
cle
expr
essi
on (
%)
Control < 1 1–5 6–11 12–36(n = 31) (n = 14) (n = 20) (n = 15) (n = 12)
FIGURE 6.3 Effect of terazosin on stromal smooth mus-cle α-actin expression. The bars represent the quantitativeevaluation of smooth muscle α-actin immunoreactivity inprostate sections from BPH patients treated with tera-zosin (1–10 mg/day). (Adapted from Chon et al.23)
Ch 06 13/5/05 3:17 pm Page 85

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA86
within the first month of treatment, which corre-lated with morphologic stromal regression andthe improvement in LUTS. There was no effecton cell proliferation. The data indicate that tera-zosin induced apoptosis in the glandular epitheli-um and stroma but has no effect on the cellulardynamics of normal (i.e. nonBPH) tissue.22,23
There is an excellent correlation between thedegree of apoptosis and improvement of symp-toms (Figure 6.4). One interpretation of thesephenomena is that α-blockers can affect abnor-mal prostate growth such as that observed inBPH and potential prostate carcinoma. Thiscould reflect a direct effect on cellular dynamicsor may arise secondary to an action on cellularproliferative factors. As in the case of the vascula-ture, androgenic and estrogenic factors alter theexpression of α1-adrenoceptors in prostate tis-sue.28,29 Catecholamines have been shown to haveproliferative (promitogenic) action in several vas-cular tissues.30 Should this translate to theprostate, the observed effects could merely reflectthe drug-induced attenuation of endogenous cat-echolamines. A model of the potential interven-tion points for terazosin is shown in Figure 6.5.
The most obvious explanation of the proapoptot-ic phenomenon is that this is directly related toblockade of α1-adrenoceptor subtypes. A goodcorrelation is known to exist between activity atthe α1A subtype and prostate smooth muscle con-traction.11 However, prostate tissue contains otherα1-adrenoceptor subtypes (α1A and α1B) and it istempting to speculate that an action at one ofthese could underpin the cellular effects of the α-blockers. It is likely that an action additional toblockade of the proliferative effects of endoge-nous catecholamines, and independent of α-adrenoceptors, is involved.5,30
The clinical evidence for a proapoptotic actionof doxazosin and terazosin is supported by cellbiology and in vivo animal experiments.31,32 In amouse prostatic reconstruction model, α-blockershad a proapoptotic action and reduced oncogene-induced growth hormone without affecting nor-mal cellular growth patterns31. This proapoptoticeffect does not appear to be restricted to themouse, at least in vitro; a similar profile of activi-ty is observed in cancer cell lines33–35 at drug con-centrations similar to those found therapeutical-ly.33 The effect was apparent in both hormone-dependent and hormone-independent celllines,32,34 and as such could indicate a potentialbeneficial effect in prostate carcinoma, in addi-tion to prevention of BPH/LUTS. Intriguingly,these actions are not found with tamsulosin.34
Tamsulosin is a sulfonamide that is structurallydissimilar to the quinazoline α-adrenoceptorantagonists (Figure 6.6). This indicates that theproapoptotic actions are not a class effect, and areindependent of the α1-adrenoceptor.5,32,34
The effects of terazosin on prostatic apoptosismay also help in the interpretation of clinical datagenerated by the Veterans’ Affairs study36 and thePREDICT study37 using a combination of finas-teride with terazosin and doxazosin, respectively.
10
Sym
ptom
impr
ovem
ent
5Apoptosis induction
r = 0.79
FIGURE 6.4 Correlation between induction of apoptosisand improvement in BPH/LUTS.
Ch 06 13/5/05 3:17 pm Page 86

ADRENOCEPTOR ANTAGONIST EFFECTS ON PROSTATE TISSUE GROWTH 87
These studies showed that the combination offinasteride and an α-blocker does not provide anytherapeutic benefit within the first 2 years overterazosin alone, at least with respect to symptomimprovement. Potentially, doxazosin and tera-zosin in their own right can affect prostategrowth by inducing both epithelial and stromalapoptosis; by comparison, the anti-androgeniceffect of finasteride is likely to be restricted toinduction only of glandular epithelial apoptosis.38
Thus, it could be argued that the apoptosis-inducing profile of quinazolines provides themolecular basis for the inability of finasteride toenhance the therapeutic effect of doxazosinand/or terazosin therapy in the short to mediumterm.
However, considering the multifactorialpathogenesis, there is logic in the use of therapiesthat target different cellular components. Thecombination of a 5α-reductase inhibitor with aquinazoline-type α-blocker should potentially
combine the clinical benefit resulting from theanti-growth effects of androgen deprivation-induced apoptosis in the epithelium with theapoptosis induced by the quinazolines in the stro-ma. In the long-term MTOPS study over 7 yearssuch synergy was observed.24 At least with respect
Androgens(DHT) Androgens
(DHT)
Cell
proliferation Cell proliferation Apoptosis
Apoptosis
Prostate hyperplasia Terazosin-treated
Pro
Pro Anti
Anti
Noradrenaline
Noradrenaline
Noradrenaline Noradrenaline
Imbalanced
Balanced
+
+ +
KGFEGFIGFs
KGFEGFIGFs
TGF-β
TGF-β
– s.
– s.
Terazosin
Terazosin Terazosin
FIGURE 6.5 Representation of some of the major factors controling tissue proliferation and apoptosis. DHT, dihydro-testosterone; EGF, endothelial growth factor; IGF, insulin-like growth factor; KGF, keratinocyte growth factor; TGF-β,transforming growth factor β.
Terazosin
Tamsulosin
NH2
•HCl•2H2O
NCH3O
CH3O CH2 C
HH2NO2S
CH3O N N N C
O
O
CH3
OCH2CH3
NHCH2CH2O •HCl
FIGURE 6.6 Structures of quinazoline (terazosin) andsulfonamide (tamsulosin) α-adrenoceptor antagonists.
Ch 06 13/5/05 3:17 pm Page 87

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA88
to delaying clinical progression, the combinationwas more effective than either component.Intriguingly, doxazosin alone was found to delayprogression only over the first 3 years or so. Thusthe long-term data are consistent with the data inthe combination studies described above, of 2years’ duration.36,37
SUMMARY
There is now considerable evidence that α-block-ers have a proapoptotic effect in prostate tissue.Although such an action may not underlie theshort-term therapeutic benefit observed withthese agents, it could make an important contri-bution to the longer-term durability of theresponse. The proapoptotic effect of doxazosinand terazosin in both stromal and epithelial com-ponents could offer an explanation of the inabili-ty of finasteride (which has effects on epithelialcomponents) to augment the response of these α-blockers in clinical studies of up to 2 years’ dura-tion. The finding that tamsulosin does not havethese properties raises the possibility that theproapoptotic action is not a class effect, and maybe independent of the α1-adrenoceptor.
REFERENCES
1. Oesterling J E. Benign prostatic hyperplasia: areview of its histogenesis and natural history.Prostate Suppl 1996; 6: 67–73
2. McNeal J E. Origin and evolution of benign pro-static enlargement. Invest Urol 1978; 15: 340–345
3. Berry S J, Coffey D S, Walsh P C, Ewing L L. Thedevelopment of human benign prostatic hyperpla-sia with age. J Urol 1984; 132: 474–479
4. Issacs J T, Coffey D A. Etiology and disease processof benign prostatic hyperplasia. Prostate 1989; 2(Suppl): 33–50
5. Kyprianou N. Doxazosin and terazosin suppressprostate growth by inducing apoptosis: clinical sig-nificance. J Urol 2003; 169: 1520–1525
6. Caine M. Alpha-adrenergic mechanisms indynamics of benign prostatic hypertrophy. Urology1988; 32: 16–20
7. McConnell J D. Medical management of benignprostatic hyperplasia with androgen suppression.Prostate Suppl 1990; 3: 49–59
8. Peters C A, Walsh P C. The effect of nafarelinacetate, a luteinizing-hormone-releasing hormoneagonist on benign prostatic hyperplasia. N Engl JMed 1987; 317: 599–604
9. Caine M, Raz S, Zeigler M. Adrenergic and cholin-ergic receptors in the human prostate, prostate cap-sule and bladder neck. Br J Urol 1975; 47: 193–202
10. Lepor H. Role of long-acting selective alpha-1blockers in the treatment of benign prostatic hyper-plasia. Urol Clin North Am 1990; 17: 651–657
11. Andersson K E, Lepor H, Wyllie M G. Prostaticalpha 1-adrenoceptors and uroselectivity. Prostate1997; 30: 202–215
12. Lepor H, Tang R, Shapiro E. The alpha-adreno-ceptor subtype mediating the tension of humanprostatic smooth muscle. Prostate 1993; 22: 301–307
13. Caine M, Pfau A, Perlberg S. The use of alpha-adrenergic blockers in benign prostatic obstruction.Br J Urol 1976; 48: 255–263
14. Marshall I, Burt R P, Andersson P O et al. Humanalpha 1c-adrenoceptor, functional characterizationin the prostate. Br J Pharmacol 1992; 107: 327P
15. Lepor H, Tang R, Meretyk S, Shaprio E. Alpha 1-adrenoceptor subtypes in the human prostate. JUrol 1993; 149: 640–642
16. Perlberg S, Caine M. Adrenergic response of blad-der muscle in prostatic contraction. Urology 1982;20: 524–527
17. Yoshimura N, Sasa M, Yoshida O, Takaori S. a1-Adrenergic receptor-mediated excitation from thelocus coeruleus of the sacral parasympathetic pre-ganglionic neurone. Life Sci 1990; 47: 789–797
18. Ishizuka O, Persson K, Mattiasson A et al.Micturition in conscious rats with and without out-
Ch 06 13/5/05 3:17 pm Page 88

ADRENOCEPTOR ANTAGONIST EFFECTS ON PROSTATE TISSUE GROWTH 89
let obstruction: role of spinal α1-adrenoceptors. BrJ Pharmacol 1996; 117: 962–966
19. Ramage A G, Wyllie M G. Effects of doxazosinand terazosin on inferior mesenteric nerve activity,spontaneous bladder contraction and blood pres-sure in anaesthetized cats. Br J Pharmacol 1994;112: 526P
20. Danuser H, Thor K. Inhibition of central sympa-thetic and somatic outflow to the lower urinarytract of the cat by the α1-adrenergic receptor antag-onist prazosin. J Urol 1995; 153: 1308–1312
21. Eri L M, Tveter K J. α-Blockade in the treatmentof symptomatic benign prostatic hyperplasia. J Urol1995; 75: 265–270
22. Kyprianou K, Litvak J P, Borkowski A et al.Induction of prostate apoptosis by doxazosin inbenign prostatic hyperplasia. J Urol 1998; 159:1810–1815
23. Chon J K, Borkowski A, Partin A W et al. α1-Adrenoceptor antagonists terazosin and doxazosininduce prostatic apoptosis without affecting cellproliferation in patients with benign prostatichyperplasia. J Urol 1999; 166: 2002–2005
24. McConnell J D. For the MTOPS steering commit-tee: the long term effects of medical therapy on theprogression of BPH: results from the MTOPS trial.J Urol 2002; 167: 265, abstract 1042
25. Lepor H and the Terazosin Research Group.Long-term efficacy and safety of terazosin inpatients with benign prostatic hyperplasia. Urology1995; 45: 406–413
26. Kirby R S. Doxazosin in benign prostatic hyperpla-sia: effects on blood pressure and urinary flow innormotensive and hypertensive men. Urology1995; 46: 182–186
27. Lepor H, Kaplan S A, Klimberg I et al. Doxazosinfor benign prostatic hyperplasia; long-term efficacyand safety in hypertensive and normotensivepatients. The Multicenter Study Group. J Urol1997; 157: 525–530
28. Zhang J, Hess M, Hittmair A et al. Human prosta-tic smooth muscle cells in culture: estradiol
enhances expression of smooth muscle cell-specificmarkers. J Urol 1994; 153: 341A
29. Benaim E A, Lin V K, McConnell J D.Quantitation of alpha 1c-adrenergic receptorexpression in minute quantities of prostate tissue. JUrol 1995; 153: 343A
30. Wyllie M G. Does doxazosin affect prostaticgrowth? Prostate 1998; 35: 152–153
31. Yang G, Timme T L, Park S H et al. Transforminggrowth factor beta 1 transduced mouse prostatereconstitutions: II. Induction of apoptosis by doxa-zosin. Prostate 1997; 33: 157–163
32. Kyprianou N, Allen L F, Wyllie M G. Induction ofprostate apoptosis by doxazosin; alpha1-adrenocep-tor-dependent and -independent actions? Br JPharmacol 1997; 22: 283P
33. Kirby R S. Doxazosin in the treatment of obstruc-tion of the lower urinary tract. In: Kirby R S,McConnell J D, Fitzpatrick J M, Roehrborn C G,Boyle P (eds). Textbook of benign prostatic hyper-plasia. Oxford: Isis Medical Media 1996: 287–293
34. Benning CM, Kyprianou N. Quinazoline-derivedalpha1-adrenoceptor antagonists induce prostatecancer via an alpha1-adrenoceptor-independentaction. Cancer Res 2002; 62: 597–602
35. Kyprianou N, Benning CM. Suppression of humanprostate cancer cell growth by alpha1-adrenoceptorantagonists, doxazosin and terazosin, via inductionof apoptosis. Cancer Res 2000; 60: 4550–4555.
36. Lepor H, Williford W O, Barry M J et al. The effi-cacy of terazosin, finasteride, or both in benign pro-static hyperplasia. Veterans’ Affairs CooperativeStudies Benign Prostatic Hyperplasia Study Group[see comments]. N Engl J Med 1996; 335: 533–539
37. Kirby RS, Roehrborn C, Boyle P, et al. Efficacy andtolerability of doxazosin and finasteride, alone or incombination, in the treatment of symptomaticbenign prostatic hyperplasia: the prospectiveEuropean doxazosin and combination therapy(PREDICT) trial. Urology 2003; 61: 119–126.
38. Peters C A, Walsh P C. The effect of nafarelinacetate, a luteinizing-hormone-releasing-hormoneagonist on benign prostatic hyperplasia. N Engl JMed 1987; 317: 599
Ch 06 13/5/05 3:17 pm Page 89

Ch 06 13/5/05 3:17 pm Page 90

Terazosin in the treatment of obstructionof the lower urinary tract
M K Brawer J M Fitzpatrick7
91
INTRODUCTION
The treatment of the lower urinary tract symp-toms (LUTS) associated with benign prostatichyperplasia (BPH) with α-adrenoceptor antago-nists (blockers) has evolved considerably since thepioneering clinical work of Marco Caine1 usingphenoxybenzamine. Initially, only two types of α-adrenoceptor (α1 and α2) were identified.Phenoxybenzamine has antagonist activity atboth α1- and α2-adrenoceptors and is therefore anonselective antagonist. Subsequently, it wasfound that prostate tissue contraction relied pri-marily on activation of the α1-adrenoceptor.2
This led to the development and clinical evalua-tion of the prototype selective α1-adrenoceptorantagonist, prazosin, in an attempt to reduce theside-effects associated with phenoxybenzamine.
The proposed mechanism for the efficacy ofselective α1-blockade in BPH is via relaxation ofprostate smooth muscle. It therefore follows thatthe magnitude of the clinical response to selectiveα1-blockade in BPH should be related directly tothe proportion of the hyperplasia that is smoothmuscle. Shapiro et al.3 evaluated the relationshipbetween the percentage area density of prostatesmooth muscle and the clinical response to theselective long-acting α1-antagonist, terazosin.Before starting terazosin therapy, prostate biopsyspecimens were obtained from 26 men. The doseof terazosin was titrated to 5 mg, provided thatserious adverse events were not observed. Thepercentage area density of smooth muscle in the
biopsy specimens was quantified using doubleimmunoenzymatic staining and color-assistedcomputer image analysis. A direct relationshipbetween the increase in peak urinary flow rate(Qmax) and the percentage area density of smoothmuscle was observed. This correlation stronglysupports the hypothesis that a component of thedevelopment of bladder outlet obstruction ismediated by an increase in prostate smooth mus-cle tone. Certainly the classical belief is that α-antagonists act by reducing the tone of theprostate smooth muscle, decreasing urethralresistance, and thereby the dynamic componentof the obstruction.4,5 However, increasingly this isbeing challenged and it is probable that extrapro-static actions of α-antagonists are of considerableimportance.6
Although bladder outlet obstruction in agingmen is often mediated by prostate smooth muscleproliferation, there is increasing evidence that theseverity of urinary symptoms is not exclusivelythe result of bladder outlet obstruction. The cor-relation between symptom severity captured bythe American Urological Association (AUA)symptom index and Qmax is poor7 and, unlikeQmax, the density of prostate smooth muscle is notdirectly correlated with symptom severity.3 Theseobservations suggest that urinary symptoms inthe aging male are probably multifactorial. It isalso conceivable that symptom improvement inmen with prostatism is achieved via nonprostatesmooth muscle events mediated by the α1-adrenoceptor.
Ch 07 13/5/05 3:19 pm Page 91

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA92
Our understanding of adrenoceptor pharma-cology has increased considerably. Four nativeα1-adrenoceptor subtypes have now been identi-fied and are known to be located in the prostate:the α1A, α1B, and α1D subtypes are high-affinityreceptors for prazosin; the α1L is a low-affinityreceptor. The evolution of this nomenclature hasbeen confusing and has changed over the last fewyears, as reviewed by Bylund et al.8 The best cor-relation between prostate tissue contraction andbinding with any of the α1-adrenoceptor recogni-tion sites is with the α1A subtype (Figure 7.1).9,10
On the basis of this and other evidence, manyinvestigators consider that the α1A subtype with-in the periurethral stroma is the prime determi-nant of prostatic tone. However, the extraprostat-ic actions of α-antagonists may make importantcontributions to the overall urodynamic andsymptom score that is observed soon after thera-py is initiated.6
Considerably less is known about the role ofthe prostate α1B and α1D subtypes. However,these could be linked to the effects of terazosin on
glandular growth and apoptosis (see Chapter 10),described in more detail below.11
The α-antagonists that have been used clini-cally in the treatment of LUTS/BPH can be sub-grouped according to their selectivity for differ-ent receptor subtypes and their pharmacokinetichalf-lives. Phenoxybenzamine is a non-selectiveα-antagonist with equal affinity for α1- and α2-adrenoceptors. Drugs with selectivity for the α1-adrenoceptor, including prazosin, alfuzosin,indoramin, terazosin, doxazosin, and tamsulosin,were subsequently developed. The primaryadvantage of these selective α1-antagonists is thatthe incidence and severity of adverse events is sig-nificantly less than with the nonselective α-block-er, phenoxybenzamine. There is no evidencefrom in vitro or whole-animal experiments thatany of the established agents is selective for anyone α1-adrenoceptor subtype (Figure 7.2),6 orpossesses any degree of clinical uroselectivity asdefined by the α-blocker subcommittee of theInternational Consultation on BPH.12
6
3
2 4
2
2
3
4
7
5 2
6
1
45
3
7
6
1
5
7Pro
stat
e pA
2
pKi
6 7 8 9 10
10
9
8
7
6
a
Pro
stat
e pA
2
pKi
6 7 8 9 10
10
9
8
7
6
b
Pro
stat
e pA
2
pKi
6 7 8 9 10
10
9
8
7
6
c
FIGURE 7.1 Correlation plots of the potency of prazosin (1), terazosin (2), indoramin (3), SNAP 1069 (4), 5-methyl-urapidil (5), SKF104856 (6), and RS 17053 (7) for cloned human and animal (RS 17053) α1A- (a), α1B- (b), and α1D- (c)adrenoceptors versus their potency at inhibiting α1-mediated contraction of the human prostate in vitro. There is a goodcorrelation between functional α1-adrenoceptor affinity (pA2) on human prostate and binding affinity (pKi) for most, butnot all, α1-adrenoceptor antagonists at the cloned α1A subtype. (Adapted from references 32 and 49.)
Ch 07 13/5/05 3:19 pm Page 92

TERAZOSIN IN LOWER URINARY TRACT OBSTRUCTION 93
As a class, α1-adrenoceptor antagonists havebeen shown to be safe and effective in the treat-ment of obstruction-related LUTS.13 Obstructiveand irritative symptoms are improved, andchanges in urinary flow and residual volume areconsistent with a reduction in urethral resistance.Prazosin has been used in this context for severalyears, but its clinical use is limited by its dosingregimen and the orthostatic hypotension that fol-lows rapid absorption. Terazosin was the firstselective α1-antagonist specifically developed toovercome these shortcomings. It has similar affin-ity for the α1A-, α1B-, and α1D-adrenoceptor sub-types (Figure 7.2),14 and is therefore considered tohave a balanced profile. In addition, terazosin canbe distinguished from prazosin on the basis ofphysicochemical differences that result in a moregradual onset of action and a much longer plasmahalf-life (16 hours compared with about 3 hours).
In this chapter we review the clinical data onterazosin and discuss how the balanced action ofterazosin across the three high-affinity α1-adrenoceptor subtypes translates into potential
clinical advantages for patient, primary-carephysician, and urologist alike.
HISTORIC BACKGROUND
Terazosin is a potent quinazoline α-adrenoceptorantagonist that is extremely selective for the α1
versus the α2 subtype.2 There is little evidencefrom isolated-tissue studies or whole-animalexperiments that terazosin has higher affinity forany one of the α1-adrenoceptor subtypes.14 Theplasma half-life (16 hours) is consistent with once-daily dosing. The contribution of metabolites tothe overall profile of terazosin is unknown.
SAFETY AND EFFICACY IN THEMANAGEMENT OF BPH
Short-term efficacy
At least 11 double-blind placebo-controlled stud-ies in patients with BPH/LUTS have been com-pleted, and a rigorous meta-analysis of the find-ings has been reported.15
The data from a large (285 patients) represen-tative study16 are shown in Figure 7.3. Statisticallysignificant decreases from baseline were observedfor obstructive, irritative, and total symptomscores, for all terazosin groups; the higher dosesproduced statistically significant improvementsover placebo, with up to 70% of patients achiev-ing more than a 30% improvement in symptomscores. Changes in symptoms were mirrored bydose-related improvements in peak and meanurinary flow (Figure 7.4).
The LUTS symptoms associated with BPHwere also improved to a statistically significantextent in most of the studies included in the meta-analysis.15 Irrespective of the different symptom
7.0
7.5
8.0
8.5
9.0
9.5
Low
Affinity
High
pKi
Dox
azos
in
Tera
zosi
n
Alfu
zosi
n
Tam
sulo
sin
5-m
ethy
lura
pidi
l
FIGURE 7.2 Affinities of doxazosin, terazosin, alfu-zosin, tamsulosin, and 5-methylurapidil (5-MU) for thecloned α1A- ( ), α1B- ( ), and α1D-( ) adrenoceptor sub-types.
Ch 07 13/5/05 3:19 pm Page 93

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA94
scores used in these studies, consistently greaterresponses were recorded in patients treated withterazosin than in those receiving placebo and,when assessed, the degree of symptom bother-someness was reduced significantly. The usualeffective dose was either 2 mg or 5 mg per day,although additional benefits were observed insome patients with doses up to 10 mg per day.
The beneficial effects of terazosin on irritativeand obstructive symptoms and urinary flow areseen within the first few weeks of treatment,often before the dose of terazosin has been titrat-ed to its optimum (Figure 7.4). This has consider-able clinical implications, in that patients may bemore likely to comply with treatment if theyexperience an early improvement in symptoms.
Systematic reviews of the effectiveness of ter-azosin in the treatment of LUTS have confirmedthat the drug is superior to both placebo andfinasteride.15,17,18 In these analyses, terazosintreatment was associated with increases in peak
flow of 1.4 ml/s compared to placebo and with anaverage reduction in symptom score of 2.2 pointsbeyond that observed with placebo.
Long-term efficacy
Any treatment for LUTS/BPH must achieve adurable clinical response in order to assume ameaningful role in patient management. Thedurability of the terazosin response has beenreported in one open-label study of almost 500men over a 4-year period.19 In this study, tera-zosin was started at 1 mg per day and the dosewas titrated upwards at the investigators’ discre-tion, to a maximum of 20 mg per day. The pri-mary efficacy variables were Qmax and Boyarskysymptom score. At the follow-up visits, Qmax wassignificantly higher than baseline; a 30%improvement over the course of the follow-upwas observed in 40–59% of patients. Similarly, theirritative, obstructive, and total Boyarsky symp-tom scores were significantly lower than at base-line at all follow-up intervals (Figure 7.5); 30% or
70
60
50
40
30
20
10
0
% o
f pat
ient
s
Placebo 2 mg 5 mg 10 mgTerazosin
FIGURE 7.3 Percentage of patients experiencing greaterthan 30% improvement in total symptoms scores ( ) andpeak urinary flow ( ) in a randomized double-blindcomparison of placebo and terazosin once daily (n = 285).
3.5
3.0
2.5
2.0
1.5
1.0
0Mea
n ch
ange
pea
k flo
w r
ate
(ml/s
)
Month of treatment
1 2 3Baseline
n = 473 n = 457
FIGURE 7.4 Mean change in peak flow rate betweenbaseline and 3 months in terazosin-treated patients. The nvalues indicate the number of patients at each time inter-val. All data points were significantly different from base-line (p ≤ 0.05).
Ch 07 13/5/05 3:19 pm Page 94
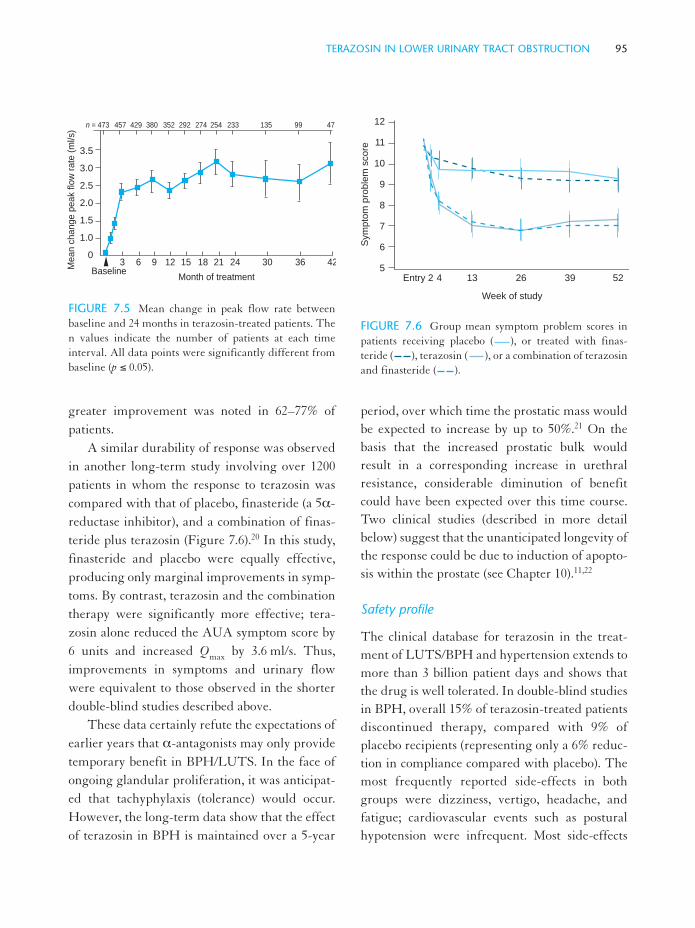
TERAZOSIN IN LOWER URINARY TRACT OBSTRUCTION 95
greater improvement was noted in 62–77% ofpatients.
A similar durability of response was observedin another long-term study involving over 1200patients in whom the response to terazosin wascompared with that of placebo, finasteride (a 5α-reductase inhibitor), and a combination of finas-teride plus terazosin (Figure 7.6).20 In this study,finasteride and placebo were equally effective,producing only marginal improvements in symp-toms. By contrast, terazosin and the combinationtherapy were significantly more effective; tera-zosin alone reduced the AUA symptom score by6 units and increased Qmax by 3.6 ml/s. Thus,improvements in symptoms and urinary flowwere equivalent to those observed in the shorterdouble-blind studies described above.
These data certainly refute the expectations ofearlier years that α-antagonists may only providetemporary benefit in BPH/LUTS. In the face ofongoing glandular proliferation, it was anticipat-ed that tachyphylaxis (tolerance) would occur.However, the long-term data show that the effectof terazosin in BPH is maintained over a 5-year
period, over which time the prostatic mass wouldbe expected to increase by up to 50%.21 On thebasis that the increased prostatic bulk wouldresult in a corresponding increase in urethralresistance, considerable diminution of benefitcould have been expected over this time course.Two clinical studies (described in more detailbelow) suggest that the unanticipated longevity ofthe response could be due to induction of apopto-sis within the prostate (see Chapter 10).11,22
Safety profile
The clinical database for terazosin in the treat-ment of LUTS/BPH and hypertension extends tomore than 3 billion patient days and shows thatthe drug is well tolerated. In double-blind studiesin BPH, overall 15% of terazosin-treated patientsdiscontinued therapy, compared with 9% ofplacebo recipients (representing only a 6% reduc-tion in compliance compared with placebo). Themost frequently reported side-effects in bothgroups were dizziness, vertigo, headache, andfatigue; cardiovascular events such as posturalhypotension were infrequent. Most side-effects
3.5
3.0
2.5
2.0
1.5
1.0
0
Mea
n ch
ange
pea
k flo
w r
ate
(ml/s
)
Month of treatmentBaseline
3 6 9 12 15 18 21 24 30 36 42
n = 473 457 429 380 352 292 274 254 233 135 99 47
FIGURE 7.5 Mean change in peak flow rate betweenbaseline and 24 months in terazosin-treated patients. Then values indicate the number of patients at each timeinterval. All data points were significantly different frombaseline (p ≤ 0.05).
12
11
10
9
8
7
6
5
Sym
pto
m p
rob
lem
sco
re
Entry 2 4 13 26 39 52
Week of study
FIGURE 7.6 Group mean symptom problem scores inpatients receiving placebo ( ), or treated with finas-teride ( ), terazosin ( ), or a combination of terazosinand finasteride ( ).
Ch 07 13/5/05 3:19 pm Page 95

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA96
were mild in severity and did not warrant treat-ment or discontinuation of therapy.
Terazosin was equally well tolerated overmuch longer periods. In the long-term studydescribed above,21 the incidence of adverse eventswas similar to that observed in the initial double-blind studies.
Overall, the side-effect profile of terazosin atdoses that are fully effective in providing relief ofLUTS/BPH appears to be characteristic of theclass.13
OVERALL CLINICAL PROFILE
Effects on blood pressure
The role of α1-adrenoceptors in the control of thehemodynamic baseline is of potential clinical con-sequence to both normotensive and hypertensiveBPH patients. Epidemiologic studies have shownthat up to 40% of men with BPH have hyperten-sion (controlled or uncontrolled).
Although (as described above) there is someconsensus that the α1A-adrenoceptor is the primedeterminant of prostate tissue contraction, muchless is known about the subtype involved in car-diovascular regulation. Perhaps not surprisingly,as blood pressure is the algebraic summation ofmany cardiac and vascular processes, the ‘bloodpressure receptor subtype’ has not been identi-fied.6 Although there may be differential distri-butions within the vasculature, all three subtypes(α1A, α1B, and α1D) are ubiquitous.8,23 On this basisit can be assumed that these three subtypes areinvolved in cardiovascular homeostasis and thateffective blood pressure control will thereforeoccur only with a balanced α1-adrenoceptorantagonist, such as terazosin. Equally, a ‘uroselec-tive’ antagonist will not provide effective blood
pressure control in the many LUTS/BPHpatients who also have hypertension.
It is well documented that the changes inblood pressure observed with α1-blockers arehighly dependent on the hemodynamic baseline.Terazosin lowers blood pressure when the sym-pathetic tone is high, for example in BPH/LUTSpatients with hypertension (Figure 7.7),17,24 buthas much less effect on resistance vessels innormotensive patients, in whom only clinicallyinsignificant changes in blood pressure areobserved (Figure 7.7).17,24,25 Terazosin has noeffect on the hemodynamic baseline, irrespectiveof whether the BPH/LUTS patients are physio-logically normotensive or are stabilized on hyper-tensive therapy.24,25
Overall, therefore, the potential antihyperten-sive effect of terazosin could be of considerableadvantage to the relatively high proportion (40%)of BPH/LUTS patients who have uncontrolledor poorly controlled hypertension. Similarly, thelong-term effects of terazosin in normotensivepatients are of little clinical concern, although thepotential to produce first-dose postural hypoten-sion must always be considered.
170
160
150
140
130
120
110
100
90
80
70
Blo
od p
ress
ure
(mm
Hg)
Terazosin Placebo Terazosin Placebo
a b
FIGURE 7.7 Effect of terazosin on blood pressure in (a)hypertensive and (b) normotensive patients. Data showblood pressure at baseline ( ) and after treatment ( ).(Adapted from reference 17.)
Ch 07 13/5/05 3:19 pm Page 96

TERAZOSIN IN LOWER URINARY TRACT OBSTRUCTION 97
Tamsulosin does not appear to lower bloodpressure consistently or markedly in hypertensivepatients.26 This profile is claimed to arise from theintrinsic ‘uroselectivity’ of the drug; however, thisclaim has been disputed,6 and the ‘uroselectivity’may simply reflect incomplete α-blockade at thedose used in clinical practice (0.4 mg).27
Cardiovascular risk factors
Most of the risk factors for hypertension are com-mon to congestive heart failure and atherosclero-sis.28 Particularly relevant are an abnormal lipidprofile and abnormal insulin resistance/glucosetolerance. The metabolic effects of terazosin andother antihypertensive agents have been reviewedby Pool.28,29 Terazosin has potentially beneficialactions on several of the risk factors (abnormallipids, fibrinolysis, platelet aggregation) thatcould have important implications in the preven-tion of hypertension, coronary heart disease(CHD), and atherosclerosis.30–32
Extensive studies of almost 17 000 hyperten-sive patients in primary care and communityfacilities suggest that the blood-pressure-lower-ing actions of terazosin, coupled with its benefi-cial effects on associated cardiovascular risk fac-tors, should significantly reduce CHD.30 On thebasis of the Framingham model,33 a reduction inthe incidence of CHD of approximately 20%would be predicted from these changes in CHDrisk factors. However, the recent results from theALLHAT study,34 and the conclusions of JNC-7,35 indicate that terazosin and other α-blockersshould not be considered as front-line monother-apy in the treatment of cardiovascular disease.However, bearing in mind that manyBPH/LUTS patients have several associated car-diovascular risk factors, these data provide sup-port for the use of terazosin in any holistic
approach to the management of the BPH/LUTSpatient as a whole.
Effects on the urogenital tract
The clinical improvement in BPH/LUTSobserved with any α-antagonist depends on avariety of actions within the urogenital tract.6,12
Although actions on prostate smooth muscleundoubtedly contribute to these effects, it isimportant to remember that there is no directcorrelation between changes in urethral resist-ance and flow rates on the one hand and symp-tom improvement on the other. Furthermore, itshould be remembered that patients usually pres-ent because of symptoms and bothersomeness,not because of reduced urinary flow. Thus, theextraprostatic actions of terazosin on the bladder,bladder neck, spinal cord, and efferent path-ways6,36 may be just as important as the changesinduced in periurethral prostate smooth muscletone.
Effects on glandular growth
Although (as described above) the immediate andshort-term therapeutic benefits of α-antagonistsundoubtedly arise from direct and indirectactions on prostate smooth muscle, it is becomingapparent that other factors are important in thelong term.
In the early days of the use of α-blockers inBPH/LUTS, tachyphylaxis (tolerance) to thedrug was expected, and, because of the continuedglandular hyperplasia, it was thought that α-antagonists might act only as clinical ‘stickingplasters’, with the effect reducing with time.Clearly, long-term studies with terazosin (Figure7.5) show a durability of response beyond theoriginal expectations.
Ch 07 13/5/05 3:19 pm Page 97

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA98
The findings of at least two recent clinicalstudies may offer some insight into this apparent-ly paradoxical longevity of response with tera-zosin.11,20,37 In one study cell proliferation andapoptosis were evaluated in BPH patients whoeither received no treatment (control group) orwere treated with terazosin at the normal clinicaldose range (1–10 mg); the treatment period wasbetween 1 week and 3 years. Compared with theuntreated controls, terazosin induced epithelialand stromal cellular apoptosis within the firstmonth of treatment (Figure 7.8), and there was aparallel increase in the expression of smooth mus-cle α-actin. The loss of prostate smooth musclecells correlated with morphologic stromal regres-sion and the improvement in LUTS. There wasno effect on cell proliferation. The data indicatethat terazosin treatment (over the normal doserange) results in a substantial induction of apop-tosis in the glandular epithelium and stroma.
However, there was no effect on the cellulardynamics of normal (i.e. nonBPH) tissue. Onepotential interpretation is that terazosin can affectabnormal prostate growth, such as that observedin BPH or prostate carcinoma. Theoretically thiscould account for the durability of the response toterazosin in long-term studies.
The effects of terazosin on prostate apoptosismay also help in the interpretation of the clinicaldata generated in the Veterans’ Affairs study(Figure 7.6).20 This study showed that the combi-nation of finasteride and terazosin did not pro-vide any therapeutic benefit over terazosin alone,at least with respect to symptom improvement.Terazosin potentially affects prostate growth byinducing apoptosis in both epithelial and stromalcomponents. Should this be the case, it is perhapsnot surprising that finasteride (which affects onlyepithelial tissue) cannot augment the response toterazosin. However, further clinical evaluation ofthis hypothesis is required. The overall profile ofterazosin and the possibility that the induction ofapoptosis is independent of the α1-adrenoceptorand is not a class effect is explored in Chapter 30.
CONCLUSIONS
Terazosin has a balanced pharmacologic actionacross the three high-affinity receptor subtypes ofthe α1-adrenoceptor, which is reflected clinicallyin the drug’s utility in the holistic approach to themanagement of the patient with BPH/LUTS. Atthe level of the prostate, the potent action of tera-zosin on the α1A-adrenoceptor subtype undoubt-edly accounts for the rapid changes seen in uri-nary flow rate and voiding pressure, secondary tochanges in urethral resistance. However, in addi-tion to these prostatic actions, the extraprostaticactions of terazosin on the bladder, bladder neck,
30
25
20
15
10
5
0
Apo
ptot
ic in
dex
(%)
Control < 1 1–5 6–11 12–36(n = 31) (n = 12) (n = 12) (n = 9) (n = 9)
Treatment period (months)
FIGURE 7.8 Effect of terazosin on prostate apoptosis inpatients with BPH. The apoptotic index of glandularepithelial ( ) and stromal ( ) smooth muscle cells inbiopsy sections is expressed as mean percentage ofTUNEL-positive cells/total number of cells after variousperiods of terazosin therapy (1–10 mg/day). (Adaptedfrom reference 11.)
Ch 07 13/5/05 3:19 pm Page 98

TERAZOSIN IN LOWER URINARY TRACT OBSTRUCTION 99
and higher centers also contribute to the signifi-cant changes in symptoms and bothersomeness.
In addition there is increasing evidence thatterazosin may have an additional action on apop-tosis within prostate tissue. Intriguingly, thisaction, which could underpin the durability of theclinical benefit seen with terazosin, may notinvolve an action at adrenoceptors and may notbe a class effect.
Terazosin produces clinically beneficialreductions in blood pressure in patients withBPH/LUTS who are also hypertensive, viaactions at all three high-affinity α1-adrenoceptorsubtypes. However, in patients who are nor-motensive or whose hypertension is controlled,only minor, clinically insignificant reductions inblood pressure are observed. Terazosin also hasbeneficial effects on several cardiovascular riskfactors (e.g. lipid profiles, glucose metabolism)which, when coupled with the blood-pressure-lowering effect seen in hypertensive BPHpatients, could translate into a reduction in CHDrisk.
In addition to the balanced pharmacologicaction across all three high-affinity α1-adrenocep-tor subtypes, the physicochemical properties ofterazosin offer considerable advantages over mostother α-antagonists. Terazosin has a long plasmahalf-life, which makes it suitable for once-dailyadministration. The relatively slow absorptionand gradual onset of action associated with thislong plasma half-life underpin the reducedpropensity for postural effects and general side-effects. Importantly, the pharmacokinetics areunchanged in the elderly or in patients with renalfailure.
Terazosin is well tolerated in both old andyoung patients. Most side-effects are mild ormoderate and do not require treatment or discon-tinuation of therapy.
Overall, therefore, terazosin has a desirableclinical profile for the treatment of BPH/LUTS.Any theoretic advantage that could be achievedwith a genuinely ‘uroselective’ agent will ulti-mately have to be weighed against the deficits ofsuch therapy with respect to the treatment of thewhole patient.
REFERENCES
1. Caine M, Pfau A, Perlberg S. The use of alphaadrenergic blockers in benign prostatic obstruction.Br J Urol 1976; 48: 255–263
2. Lepor H, Gup D I, Bauman M, Shapiro E.Laboratory assessment of terazosin and alpha1-blockade in prostatic hyperplasia. Urology 1988; 32(Suppl): 21–26
3. Shapiro H, Hartatano V, Lepor H. The response toalpha blockade in benign prostatic hyperplasia isrelated to the percent density of prostate smoothmuscle. Prostate 1992; 21: 297–307
4. Caine M, Raz S, Ziegler M. Adrenergic and cholin-ergic receptors in the human prostate, prostaticcapsule and bladder neck. Br J Urol 1975; 27:193–202
5. Lepor H. Role of long-acting selective alpha1-blockers in the treatment of benign prostatic hyper-plasia. Urol Clin North Am 1990; 17: 651–657
6. Andersson K -E, Lepor H, Wyllie M G. Prostaticalpha1-adrenoceptors and uroselectivity. Prostate1997; 30: 202–205
7. Barry M J, Cockett A T K, Holtgrewe H L et al.Relationship of symptoms of prostatism to com-monly used physiological and anatomical measuresof severity of benign prostatic hyperplasia. J Urol1993; 150: 351–358
8. Bylund B D, Eikenberg D C, Hieble J -P et al.International Union of Pharmacology nomencla-ture of adrenoceptors. Pharmacol Rev 1994; 46:121–136
Ch 07 13/5/05 3:19 pm Page 99

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA100
9. Marshall I, Burt R P, Andersson P -O et al. Humanalpha1c-adrenoceptor, functional characterisation inthe prostate. Br J Pharmacol 1992; 107: 327P
10. Lepor H, Tang R, Shapiro E. The alpha-adreno-ceptor subtype mediating the tension of humanprostatic smooth muscle. Prostate 1993; 22: 301–307
11. Chon J K, Borkowski A, Partin A W et al. Alpha1-adrenoceptor antagonists, doxazosin and terazosininduce prostate apoptosis without affecting cellproliferation in patients with benign prostatichyperplasia. J Urol 1999; 161: 2002–2008
12. Jardin A, Andersson K -E, Bono V A et al. Alpha-blockers in the treatment of BPH. In: Denis L,Griffiths K, Khoury S et al. (eds). Proceedings ofthe fourth international consultation on benignprostatic hyperplasia (BPH). Plymouth: SCI, 1998:599–632
13. Eri L M, Tveter K J. Alpha-blockade in the treat-ment of symptomatic benign prostatic hyperplasia.J Urol 1995; 154: 923–934
14. Kenny B, Naylor A M, Carte A J et al. Effect ofalpha1-adrenoceptor antagonists on prostatic pres-sure and blood pressure in the anaesthetised dog.Urology 1994; 44: 52–57
15. Boyle P, Robertson C, Manski R et al. Meta-analy-sis of randomized trials of terazosin in the treat-ment of benign prostatic hyperplasia. Urology2001; 58: 717–722
16. Lepor H, Aurbach S, Puras-Baez A et al. A ran-domised multi-centre placebo controlled study ofthe efficacy and safety of terazosin in benign pro-static hyperplasia. J Urol 1992; 148: 1467–1474
17. Wilt T J, Howe R W, Rutks I R, MacDonald R.Terazosin for benign prostatic hyperplasia.Cochrane Database Syst Rev 2002; CD003851
18. Kaplan S A. Terazosin for treating symptomaticbenign prostatic obstruction: a systematic review ofefficacy and adverse events. J Urol 2002; 168:1657–1658
19. Lepor H. Long-term efficacy and safety of tera-zosin in patients with benign prostatic hyperplasia.Terazosin Research Group. Urology 1995; 45:406–413
20. Lepor H, Williford W O, Barry M J et al. Theimpact of medical therapy on bother due to symp-toms, quality of life and global outcome, and fac-tors predicting response. Veterans’ AffairsCooperative Studies Benign Prostatic HyperplasiaStudy Group. J Urol 1998; 160: 1358–1364
21. Oesterling J E. Benign prostatic hyperplasia: areview of its histogenesis and natural history.Prostate Suppl 1996; 6: 67–73
22. Kyprianou N, Litvak J P, Borkowski A et al.Induction of prostate apoptosis by doxazosin inbenign prostatic hyperplasia. J Urol 1998; 159:1308–1312
23. Hoffman B B, Hu Z -H. Regulation of responsesmediated by alpha1-adrenergic receptors in smoothmuscle cultures. Pharmacol Commun 1995; 6: 1–3
24. Kirby R S. Terazosin in benign prostatic hyperpla-sia: effects on blood pressure in normotensive andhypertensive men. Br J Urol 1998; 82: 373–379
25. Lowe F C, Olson P J, Padley R J. Effects of tera-zosin therapy on blood pressure in men withbenign prostatic hyperplasia concurrently treatedwith other antihypertensive medications. Urology1999; 54: 81–85
26. Chapple C R. Tamsulosin. In: Kirby R, McConnellJ D, Fitzpatrick J M et al. (eds). Textbook of benignprostatic hyperplasia, 2nd edn. London: Taylor andFrancis, 2005
27. Wyllie M G. Alpha1-adrenoceptor selectivity: theNorth American experience. Urology 1999; 36(Suppl): 59–63
28. Pool J L. Effects of doxazosin on coronary heartdisease risk factors in hypertensive patients. Br JClin Pract Symp Suppl 1994; 74: 8–12
29. Pool J L. Effects of doxazosin on serum lipids. Areview of the clinical data and the molecular basisfor altered lipid metabolism. Am Heart J 1991; 121:251–260
30. Itskovitz H D. Alpha1-blockade for the treatmentof hypertension: a megastudy of terazosin in 2214clinical practice settings. Clin Ther 1994; 16:490–504
31. Shinori H, Gotoh E, Ito T et al. Long-term thera-py with terazosin may improve glucose and lipid
Ch 07 13/5/05 3:19 pm Page 100

TERAZOSIN IN LOWER URINARY TRACT OBSTRUCTION 101
metabolism in hypertensives: a multicenterprospective study. Am J Med Sci 1994; 307 (Suppl):91–95
32. Hernandez R, Angeli-Greaves M, Carvajal A R etal. Terazosin: ex vivo platelet aggregation effects inpatients with arterial hypertension. Am JHypertens 1996; 9: 437–444
33. Levy D, Wilson P W F, Anderson K M, Castelli WP. Stratifying patients at risk from coronary heartdisease; new insights from the Framingham HeartStudy. Am Heart J 1990; 119: 712–717
34. Flack J M, Nasser S A. The antihypertensive andlipid-lowering treatment to prevent heart attacktrial (ALLHAT). Major outcomes in high-riskhypertensive patients randomized to angiotensin-
converting enzyme inhibitor or calcium channelblocker versus diuretic. Curr Hypertens Rep 2003;5: 189–191
35. JNC-7. The seventh report of the Joint NationalCommittee on Prevention, Detection, Evaluationand Treatment of High Blood Pressure. May 2003:NIH Publication No 03-5233
36. Ramage A G, Wyllie M G. A comparison of effectsof doxazosin and terazosin on the spontaneoussympathetic drive to the bladder and related organsin anaesthetised cats. Eur J Pharmacol 1996; 117:962–966
37. Kyprianou N. Doxazosin and terazosin suppressprostate growth by inducing apoptosis. Clinical sig-nificance. J Urol 2003; 169: 1520–1525
Ch 07 13/5/05 3:19 pm Page 101

Ch 07 13/5/05 3:19 pm Page 102

Doxazosin in the treatment ofbenign prostatic hyperplasia
R S Kirby8
INTRODUCTION
The treatment with α1-adrenoceptor antagonistsof the benign prostatic hyperplasia (BPH) symp-tom complex associated with obstruction of thelower urinary tract has evolved substantially fromthe original observations of Caine with phenoxy-benzamine. Initially, only two types of α-adreno-ceptor (α1 and α2) were identified. Phenoxy-benzamine, an antagonist at both α-adrenocep-tors, was classified as a nonselective α-adrenocep-tor antagonist. Subsequently, the prime determi-nant of periurethral smooth muscle tone wasfound to be the α1-adrenoceptor, which led to theclinical evaluation of the first α1-selective antago-nist, prazosin, in an attempt to improve the side-effect profile of phenoxybenzamine. Under-standing has increased further, to an extent wherethree major subtypes of the α1-adrenoceptor havebeen cloned and characterized, namely α1A, α1B,
and α1D. A fourth receptor subtype, the α1L-adrenoceptor, has also been defined pharmaco-logically, but neither fully characterized norcloned.1 The evolution of the nomenclature,which has been confusing and has undergonechange over the last few years, is described in areview by Bylund et al.2
As a class, α1-adrenoceptor antagonists arewell tolerated and effective in the treatment ofobstruction-related lower urinary tract symp-toms.3 Both obstructive and irritative symptomsare improved, and there are changes in urinaryflow and residual volume consistent with a reduc-tion in urethral resistance. Prazosin has been used
in this context for several years, but its therapeu-tic potential has been limited owing to the dosingregimen and the side-effects associated with therapidity of onset of action. Doxazosin, a selectiveα1-adrenoceptor antagonist, was developed toovercome these shortcomings. It has similar affin-ity for all α1-adrenoceptor subtypes and, there-fore, can be considered to have a balanced phar-macologic profile.4 In addition, doxazosin can bedistinguished from prazosin on the basis of phys-iochemical differences, which result in a moregradual onset of action and an extended plasmahalf-life (22 hours), consistent with utility as aonce-a-day agent (Figure 8.1).5,6 Doxazosin hashad a wide exposure in BPH and hypertensivepatients, and also in the high proportion ofpatients with concomitant disease.7
0
–10
–20
–30
–40
–500 2 4 6 8
Time (h)Cha
nge
in s
tand
ing
syst
olic
BP
(m
mH
g)
FIGURE 28.1 Onset of action of doxazosin ( ; meandose 0.95 mg i.v.) and prazosin ( ; mean dose 1 mg i.v.):effect on standing systolic blood pressure (BP). (FromElliot et al.,5 with permission.)
103
Ch 08 13/5/05 3:25 pm Page 103

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA104
This chapter reviews the available data ondoxazosin, and analyzes whether the balancedaction of doxazosin on α1-adrenoceptor subtypestranslates into clinical advantages for patient, pri-mary-care physician, and urologist, alike.
α1-ADRENOCEPTOR HETEROGENEITY
To understand the clinical profile of doxazosin itis necessary to consider briefly the pathophysio-logic roles of α1-adrenoceptor subtypes. A com-prehensive review of the literature is not withinthe scope of this chapter, but the salient featuresare summarized below. For a more detailedreview of the potential role of the different α1-adrenoceptor subtypes throughout the urogenital,cardiovascular, and central nervous system, con-sult Kirby et al.8
All three high-affinity α1-adrenoceptor sub-types α1A, α1B, and α1D are present in the prostate.The α1-receptor predominates, in both hyper-plastic and normal prostate tissue, and its pres-ence is correlated with the prostatic contractileresponse.9–11 α-Blockers were first thought torelieve the symptoms of BPH by inhibiting theα1A-adrenoceptors of the prostatic smooth mus-cle. Any associated side-effects were assumed tobe mediated via α1-adrenoceptors in the vascula-ture. However, more recent evidence suggeststhat both the efficacy and tolerability of α-block-ers in BPH may have a centrally mediated com-ponent.8 The α1D-receptor subtype, for example,is predominant in CNS structures involved withmicturition. Side-effects such as asthenia anddizziness may be due to a central rather than avascular effect. As such, although an α1-adreno-ceptor subtype probably cannot preferentially betargeted as a treatment for BPH, reducing activi-
ty at the α1B subtype may reduce cardiovascularcomplications.8
SAFETY AND EFFICACY OF DOXAZOSIN INBPH TREATMENT
Short-term efficacy
A number of double-blind, placebo-controlledclinical studies of doxazosin in patients with BPHhave been completed, and reported in the litera-ture.12–19 Patients enrolled in the studies havebeen men aged between 50 and 80 years with clin-ical evidence of BPH and maximum flow ratesbelow 15 ml/s. In general, patients receivingtreatment with other α1-adrenoceptor antago-nists, and patients with urinary tract infections orother serious illnesses, were excluded from thesestudies. A wash-out phase of at least 1 week wasfollowed by a double-blind treatment period ofbetween 1 and 6 months. Patients were random-ized either to doxazosin (at an initial dose of1 mg/day and increased sequentially according toprotocol) or to placebo. Both normotensive andhypertensive patients were included in thesestudies.
Treatment with doxazosin increased bothmaximum and average urinary flow rates inalmost all studies. The changes achieved statisti-cal significance compared with placebo in themajority of patients. Doxazosin also produced aconsistently reduced residual urine volume, albeitsmall and variable, compared with placebo.BPH-associated symptoms were also improved toa statistically significant extent in the majority ofstudies. Irrespective of the different symptomscores used in these studies, consistently greaterresponses were recorded in patients treated withdoxazosin than in those given placebo.
Ch 08 13/5/05 3:25 pm Page 104

DOXAZOSIN IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 105
In the studies reported above, the beneficialeffects of doxazosin on symptoms and uroflowwere seen within the first few weeks of treatment,often before doxazosin had been titrated to theoptimum dose (Figure 8.2). This has importantclinical implications, in that patients may beencouraged to continue to comply with treatmentif they experience an early improvement in symp-toms.
Doxazosin has a beneficial effect on symp-toms and urinary flow rates, irrespective of thebaseline severity of disease. In a pooled analysis ofthree of the double-blind, placebo-controlledstudies reported above, doxazosin was seen toproduce a significantly greater improvementcompared to placebo in peak urinary flow rate,symptom severity, and symptom bother.20
Stratification by severity of symptoms at baselinedemonstrated that the greatest improvementwith doxazosin was seen in patients with the mostsevere symptoms (p = 0.0001); age did not impacton the capacity to benefit from treatment. Thus,it can be concluded that treatment with doxa-zosin is effective in patients with mild, moderate,
and severe BPH, not just those with only mild or
moderate symptoms.
Pooled analysis also allowed a more in-depth
assessment of urodynamic changes with doxa-
zosin versus placebo.21 Doxazosin significantly
improved free urinary flow rate versus placebo,
and reduced detrusor pressure, leading to a
decreased voiding time and increased voided vol-
ume. Urethral resistance was also reduced with
doxazosin.
While the majority of studies have been con-
cluded in men between 50 and 80 years of age, the
efficacy and safety of α1-adrenoceptor antagonists
has also been investigated in men over the age of
80 years.22 In a study of doxazosin and terazosin,
both agents were seen to produce a significant
increase in peak urinary flow rate and a
significant improvement in American Urological
Association (AUA) symptom score. Importantly,
doxazosin or terazosin could be introduced for
the treatment of BPH in patients who were
already receiving antihypertensive treatment.
0 2 4 6 7 8 10 12 14
Duration of treatment (weeks)
Mea
n ch
ange
(m
l/s)
4
3
2
1
0
–1
0 2 4 6 7 8 10 12 14
Duration of treatment (weeks)
Mea
n ch
ange
(sc
ore)
0
–1
–2
–3
–4
–5
–6
* *
**
**
* *
†
*
**
**
**
a b
FIGURE 8.2 Effect of doxazosin ( ) versus placebo ( ) on (a) symptom score and (b) peak uroflow. Asterisks indi-cate significant differences from placebo (*p < 0.005); dagger indicates significant difference from baseline (†p < 0.05).(From Fawzy et al.,14 with permission.)
Ch 08 13/5/05 3:25 pm Page 105

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA106
Long-term efficacy
The longest double-blind study with doxazosinwas conducted by Holme et al.,15 with a durationof 29 weeks. This study demonstrated that effica-cy was maintained throughout the treatmentperiod. These double-blind data are supported bydata from an open-label extension study ofpatients who completed three of the double-blind, placebo-controlled studies listed above.23 Atotal of 450 men entered the long-term study, anddata are available for up to 48 months of follow-up. Results show that doxazosin, over the courseof 4 years, produces a clinically and statisticallysignificant increase in maximum and average uri-nary flow rate (Figure 8.3), as well as a clinicallyand statistically significant improvement in total,obstructive, and irritative BPH symptoms(Figure 8.4).
In a further analysis of only those patientswith concurrent hypertension and BPH, treat-ment with doxazosin over 48 months resulted in
a sustained improvement in the severity andbothersomeness of BPH symptoms, and anincrease in maximum urinary flow rate.24 Therewas also a significant and sustained reduction indiastolic blood pressure.
The efficacy and tolerability of doxazosin incombination with finasteride has also been evalu-ated in the Prospective European Doxazosin andCombination therapy (PREDICT) trial.25 In thisstudy of 1095 men, doxazosin was effective inimproving symptoms and flow and was moreeffective that finasteride or placebo. Addition offinasteride did not provide further benefit to thatobserved with doxazosin alone. Therefore, over-all the results were similar to combination studiesinvolving other α-blockers.26
The PREDICT study and the MedicalTherapy of Prostatic Symptoms (MTOPS)27
study have also provided further evidence of thedurability of the response to doxazosin with littleevidence of tachyphylaxis.
2.5
2.0
1.5
1.0
0.5
0
0 < 60 3 6 9 12 15–18 21–24 27–30 33–36 39–42
Months
Qm
ax m
ea
n c
ha
ng
es v
s b
ase
line
(m
l/s)
**
**
** *
*
*
*
n = 449 438 402 372 352 321 297 257 131 59
days
FIGURE 8.3 Maximum urinary flow rates (Qmax) during the 4-year open-label extension study with doxazosin.Decreased patient numbers at successive time points are not because patients withdrew from the study, but primarilybecause patients were enrolled as they completed each double-blind study, which spanned many months. Asterisks indi-cate p < 0.0001 versus baseline. (From Lepor et al.,23 with permission.)
Ch 08 13/5/05 3:25 pm Page 106

DOXAZOSIN IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 107
Safety profile
The clinical database for doxazosin in the treat-ment of hypertension extends to more than 3 bil-lion patient days. Data from studies of doxazosinin BPH have shown consistently that the com-pound is equally well tolerated in patients withthis condition and, intriguingly, perhaps is evenbetter tolerated in normotensive than in hyper-tensive patients.
In a pooled analysis of seven double-blind,placebo-controlled studies, doxazosin was welltolerated in normotensive and hypertensivepatients with BPH.28 In general, older patients(≥65 years) treated with doxazosin experiencedfewer adverse events than younger patients (42%versus 47%), although the difference was not sta-tistically significant. A similar incidence ofadverse events was seen in the placebo group(38% compared with 44%). The most commonly
reported adverse events in all groups were dizzi-ness, headache, fatigue, and dyspnea. The major-ity of adverse events were mild and did notrequire discontinuation of treatment.
The good tolerability profile of doxazosin hasalso been seen with long-term treatment.23 In the4-year, long-term extension study, almost 90% ofadverse events were mild or moderate in severity.The tolerability profile of doxazosin was verysimilar to that seen in short-term studies, themost frequently reported adverse events beingdizziness, headache, and fatigue. Doxazosin wassimilarly well tolerated by normotensive andhypertensive patients with BPH. The incidenceof adverse events with doxazosin did not increaseover time. In fact, a reverse Kaplan–Meier plot ofpatient withdrawals from therapy during long-term treatment illustrates a leveling-off of discon-tinuations after the first few months.Approximately half of those patients who discon-
0
–1
–2
–3
–4
–5
–6
–7
0 < 60 3 6 9 12 15–18 21–24 27–30 33–36 39–42
n = 407 416 373 365 347 316 290 252 124 57
Months
Me
an
ch
an
ge
fro
m b
ase
line *
*
* * * * * * * *
*
***
****
**
*
*
**
* *
**
*
*
days
FIGURE 8.4 Effect of doxazosin on obstructive ( ), irritative ( ), and Boyarsky total ( ) symptom bothersome-ness score during the 4-year open-label extension study with doxazosin. Decreased patient numbers at successive timepoints are not because patients withdrew from the study, but primarily because patients were enrolled as they completedeach double-blind study, which spanned many months. Asterisks indicate p < 0.0001 versus baseline. (From Lepor et al.,23
with permission.)
Ch 08 13/5/05 3:25 pm Page 107

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA108
tinued therapy with doxazosin due to adverseevents did so within the first 9 months of therapy(Figure 8.5).
TREATMENT OF THE WHOLE PATIENT
Effects on blood pressure control
The involvement of α1-adrenoceptor subtypes incardiovascular control is of prime importance innormotensive and hypertensive patients. Not sur-prisingly, as blood pressure regulation is the alge-braic sum of many cardiac and vascular processes,the ‘blood pressure subtype’ of the α1-adrenocep-tor has not been identified. Although there maybe differential distributions within the vascula-ture, and distribution may be species and vesseldependent, all subtypes appear to play a role inthe contractile response of vascular tissue.8,9,30
The human α1A-adrenoceptor appears to be thepredominant α-adrenoceptor subtype in arterialsmooth muscle, but this does not mean that it nec-essarily controls systemic blood pressure andorthostasis. It is more reasonable to assume that
cardiovascular homeostasis depends on all sub-types, and effective blood pressure control will beachieved only with a balanced α1-adrenoceptorantagonist. Equally, a prostate-selective antago-nist may be incapable of providing effective bloodpressure control in BPH patients with associatedhypertension.
It is well documented that the blood pressure-lowering effects of α1-adrenoceptor antagonistsare highly dependent on the hemodynamic base-line. Doxazosin lowers blood pressure when sym-pathetic drive is high, for example in hyperten-sion. In contrast, doxazosin has less effect onresistance vessel tone in normotensive patients,and clinically insignificant changes in blood pres-sure are observed (Figure 8.6).31,32 Interestingly,there is no effect on the hemodynamic baseline,irrespective of whether BPH patients are physio-logically normotensive or are stabilized on anti-hypertensive therapy.31
Hypertension and BPH are often encounteredconcomitantly in primary care practice. It isimportant, therefore, that an agent used to treatBPH can be used effectively and safely in patients
100
80
60
40
20
0
< 60 3 6 9 12 15 18 21 24 27 30 33 36 39 42
Duration of treatment (months)
Cu
mu
lative
dis
co
ntin
ua
tio
n (
%)
days
FIGURE 8.5 Reverse Kaplan–Meier plot of discontinuations from long-term doxazosin therapy because of adverseevents (upper curve) or inadequate clinical response (lower curve). (From Lepor et al.,23 with permission.)
Ch 08 13/5/05 3:25 pm Page 108

DOXAZOSIN IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 109
receiving additional antihypertensive treatment.The Hypertension and BPH Intervention Study(HABIT) evaluated the efficacy and safety ofdoxazosin in patients with concomitant hyperten-sion and BPH, in a community-based setting.33
There were four groups in the study: patientstreated with antihypertensives who were wellcontrolled; patients treated and poorly controlled;untreated, hypertensive patients; and untreatednormotensive patients. Treatment with doxa-zosin was effective in all groups of patients; therewas significant improvement in symptom scoresas well as BPH-specific indices of health status(p < 0.0001). A clinically important and beneficialreduction in blood pressure was seen only inpatients who had an elevated blood pressure atbaseline, and was evident in both younger (45–64
years) and older (≥65 years) patients. The inci-dence of treatment-related adverse events wassimilar across all groups, ranging from 30 to 37%.The majority were mild or moderate in severity,the most frequent being dizziness, fatigue, som-nolence, and headache.
Cardiovascular risk factors
Many of the risk factors for hypertension arecommon to congenital heart failure and athero-sclerosis.34 Particularly relevant are an aberrantlipid profile and insulin resistance/glucose intol-erance. The effects of doxazosin compared withother quinazolines and other antihypertensiveagents have been extensively reviewed byPool.34,35 Clearly, doxazosin offers a number ofbenefits in this respect. In the Treatment of MildHypertension Study (TOMHS),36 doxazosin, incontrast to other antihypertensive agents, pro-duced sustained reductions over a 48-month peri-od in total and low-density lipoprotein (LDL)cholesterol and triglycerides, and increases inhigh-density lipoprotein (HDL) cholesterol andHDL: total cholesterol ratios.
Although understanding of the effect of α-blockers on serum lipid profile is incomplete,Pool34,35 has identified several in vitro loci thatcould account for the clinical observations.Increases in LDL-receptor activity and lipopro-tein lipase activity, and decreases in intracellularLDL synthesis and cholesterol absorption, havebeen observed in the presence of these drugs. Asingle α1-adrenoceptor subtype has not beenlinked to these effects. Indeed, studies of doxa-zosin metabolites indicate that a component ofthe drug’s actions may arise from a direct actionon signal transduction, independent of the α1-adrenoceptor.37
In the context of cardiovascular risk factors,catecholamines are involved in smooth muscle
170
160
150
140
130
120
110
100
90
80
70
Hypertensive Normotensive
Blo
od
pre
ssu
re (
mm
Hg
)
FIGURE 8.6 Effect of doxazosin ( ) on the blood pres-sure of hypertensive and normotensive BPH patients ( ,baseline). (From Kirby32 with permission.)
Ch 08 13/5/05 3:26 pm Page 109

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA110
proliferation in the vasculature via an α1-adreno-ceptor mechanism.38,39 α1-Adrenoceptor-antago-nist attenuation of a proliferative vascularresponse could have important implications in theprevention of hypertension, coronary heart dis-ease (CHD), and atherosclerosis. Doxazosin hasalso been shown to have a favorable effect onother cardiovascular risk factors, includingincreased fibrinolysis, inhibition of platelet aggre-gation, attenuation of the adverse hemodynamicand hemostatic effects of smoking, and regressionof left ventricular hypertrophy.34,35
Extensive studies of almost 5000 hypertensivepatients in general practice show a beneficialeffect of doxazosin in significantly reducingCHD.40 On the basis of the Framingham Studyequation,41 an approximate 20% reduction inCHD incidence would be predicted to resultfrom these changes in CHD risk factors. In theHypertension and Lipid Trial (HALT), a studyenrolling over 800 patients with hypertension in aclinical practice setting, treatment with doxazosinproduced a significant reduction in mean totalcholesterol levels, LDL cholesterol, and triglyc-erides; levels of HDL cholesterol were essentiallyunchanged. In previously untreated patients,these doxazosin-induced changes in serum lipidprofile, together with a significant reduction inblood pressure, resulted in a reduction in mean 5-year coronary disease risk of 15%.42 The effects ofdoxazosin on predicted coronary disease risk arein contrast to other antihypertensive agents, e.g.β-blockers. In a 5-year comparison of doxazosinand the β-blocker atenolol, doxazosin significant-ly reduced the predicted 10-year risk of CHD byapproximately 12%, whereas atenolol had essen-tially no effect (0.2% increase). While both agentswere effective antihypertensives, and both werewell tolerated, only doxazosin had favorableeffects on the serum lipid profile.43
More recently, the Antihypertensive Lipid-Lowering Treatment to Prevent Heart AttackTrial (ALLHAT) was completed.44 Although theinterpretation of data has created considerabledebate, careful analysis confirms that it does notaffect the management of BPH patients withdoxazosin.45
Thus, the beneficial effects of doxazosin oncardiovascular risk further support the use of abalanced agent in the treatment of the BPHpatient as a whole.
Sexual function
For several years there has been indirect evidencethat doxazosin has a positive effect in males witherectile dysfunction (ED). In the 4-year TOMHSstudy,36,46 a much reduced incidence of ED wasreported in the doxazosin group compared withplacebo (Figure 8.7). In contrast, other antihyper-tensive agents (e.g. diuretics) appeared to increasethe incidence. Throughout the duration of thestudy, erection problems disappeared in 88% ofmen randomized to doxazosin, compared with55% of men in all other groups combined.
More recently, in an Italian multicenter studyin BPH patients, doxazosin was found to improveerectile function, independent of any improve-ment in LUTS.47 The positive effect is consistentwith the well-documented role of α1-adrenocep-tors in the control of corpus cavernosal tone48 andthe clinical benefit observed with intracavernosalinjection of α1-adrenoceptor antagonists.
Although doxazosin may not necessarily rep-resent effective monotherapy for ED per se, thereis some suggestion that it could form part of acombination strategy in the management of EDrefractory to other agents. In one study of menwith moderate to severe ED, oral doxazosinimproved the response to intracavernosalalprostadil injection. There was an 18% improve-
Ch 08 13/5/05 3:26 pm Page 110

DOXAZOSIN IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 111
ment in International Index of Erectile Function(IIEF) with alprostadil alone, compared with a52% improvement over 12 weeks with the addi-tion of doxazosin (p < 0.0149). More recently, evi-dence of synergy with sildenafil has also beenreported.50
Overall, given the high degree of co-morbidED in LUTS,51 the impact of therapy (negative orpositive) should be an important component ofthe decision-making process.
Other contributing factors to the clinical profileof BPH
When considering the urogenital tract it isimportant to remember the potential contribu-tion from extraprostatic actions to the overallclinical profile of BPH.48 There is no direct corre-lation between flow rates and urethral resistanceand the observed improvement in symptoms.Furthermore, it should be remembered thatpatients generally present because of symptomsand bothersomeness, not because of a reduced
urinary flow. Thus, the extraprostatic actions thathave been observed with doxazosin on the blad-der,48 spinal cord,52 and efferent pathways53 maybe just as important as changes induced in peri-urethral stromal tone.
Several studies have shown that certain α1-adrenoceptor antagonists may regulate prostategrowth by inducing apoptosis in the epithelialand stromal cells.54 Over the clinical dose range,within the first month of treatment both doxa-zosin and terazosin produced a significant induc-tion of apoptosis in prostate biopsies compared tountreated controls. This was paralleled by a lossof prostatic smooth muscle and an improvementin BPH symptomatology.55 This effect, not foundwith tamsulosin,54,56 is considered to be confinedto quinazoline-derived α1-antagonists and mayindeed be independent of an action on the α1-adrenoceptor.54
Potentially such an action could account forthe long-term clinical durability of the responseto doxazosin in BPH patients.
100
25
20
15
10
5
0
Doxazosin Enalapril Placebo Amilodipine Acebutolol Chlorthalidone
(n = 71) (n = 61) (n = 118) (n = 59) (n = 72) (n = 70)
Treatment group
Pe
rce
nta
ge
of
pa
tie
nts
FIGURE 8.7 Treatment of Mild Hypertension Study: incidence of men reporting inability to maintain an erection.(From Neaton et al.,36 with permission.)
Ch 08 13/5/05 3:26 pm Page 111

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA112
DOXAZOSIN: THE NEW GITSFORMULATION
A new formulation of doxazosin, the doxazosingastrointestinal therapeutic system (GITS), hasbeen developed to enhance the pharmacokineticprofile of the drug. It employs controlled-releasetechnology to allow more gradual drug deliverywith the first dose, and precise, sustained serumlevels with long-term, once-daily administration.It is as effective and well tolerated as the standardformulation. For example, in a study of patientswith mild hypertension, both doxazosin standardand doxazosin GITS produced significant reduc-tions in blood pressure compared to placebo(p < 0.001). The most commonly reported side-effects were headaches, dizziness, and asthenia.57
The GITS formulation appears to eliminate theneed for doxazosin dose titration in most patients.In a combined analysis of two randomized, dou-ble-blind studies in hypertension, approximately60% of patients achieved goal blood pressureresponse at the 4 mg starting dose.58 The simpli-
fied dosing regimen is likely to result in feweroffice visits for patients.
Studies with doxazosin GITS have also beencarried out in patients with BPH.18,19,59 Resultshave shown that doxazosin GITS provides effec-tive relief from the signs and symptoms of BPH,with an efficacy comparable to that of the stan-dard formulation. In a combined analysis of twodouble-blind, placebo-controlled studies, a simi-lar increase in urinary flow rate and a similarimprovement in symptoms were seen with doxa-zosin GITS and doxazosin standard (Figure 8.8).Fewer titration steps were needed with doxazosinGITS, and almost 50% of patients achievedsymptom relief at the starting dose of 4 mg/day.Tolerability was also enhanced with doxazosinGITS. In the same combined analysis, the overallincidence of adverse events was similar in doxa-zosin GITS and placebo groups, and lower thanthat with standard doxazosin treatment (Table8.1)
Intriguingly, in a ‘gold standard’ double-blindstudy, the doxazosin GITS (4 mg, 8 mg) was
20
18
16
14
12
10
8
00 1 2 3 4 5 6 7 8 9 10 11 12 13
Week
Mea
n to
tal I
-PS
S
a14
13
12
11
10
9
8
00 1 2 3 4 5 6 7 8 9 10 11 12 13
Week
Mea
n Q
max
(m
l/s)
b
*
*
*
*†
*†
*†
*†§
*†§ *† *†
*†
*†*‡
****
*†
*†
FIGURE 8.8 Effect of doxazosin gastrointestinal therapeutic system (GITS) ( ), doxazosin standard ( ), and placebo( ) on (a) total International Prostate Symptom Score (I-PSS) and (b) maximum urinary flow rate. (From Kirby et al.,59
with permission.)
Ch 08 13/5/05 3:26 pm Page 112

DOXAZOSIN IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 113
found to be more effective than tamsulosin(0.4 mg, 0.8 mg) in improving LUTS symp-toms.60 This could represent the first evidencefrom a carefully controlled study that α-blockersmay have different effects.
CONCLUSIONS
Doxazosin has a balanced pharmacologic actionat all subtypes of the α1-adrenoceptor, which isreflected clinically in a beneficial effect on thewhole patient. It improves both symptoms andmeasures of urinary flow in the patient withBPH, as well as producing clinically importantblood pressure reductions in BPH patients withhypertension. It is likely that an action on alladrenoceptor subtypes is required to produce thisprofile. In subjects with physiologic or drug-con-trolled normotension, only minor, clinicallyinsignificant changes in blood pressure areobserved.
Doxazosin appears to have a beneficial effecton several risk factors (e.g. lipid profile, glucosemetabolism) associated with hypertension, CHD,and atherosclerosis. The α1-adrenoceptor subtypeinvolved has not been identified, and there maybe a contribution from receptor-independentevents.
In addition to these pharmacologic actions,the physiochemical properties of the drug offerconsiderable advantages. In particular, doxazosin,compared with other α1-adrenoceptor antago-nists, has a long plasma half-life consistent withonce-daily dosing. The associated gradual onsetof action also underpins the reduced propensityfor side-effects. Importantly, the pharmacokinet-ics are unchanged in the elderly and in renal fail-ure. The new GITS formulation extends theestablished benefits of standard doxazosin thera-py. Doxazosin GITS has an efficacy and tolerabil-ity profile similar to that of the standard formula-tion, with the additional advantages of anenhanced pharmacokinetic profile and simplifieddosing regimen.
Doxazosin is very well tolerated in both oldand young patients. Most adverse events are mildor moderate in severity and do not require dis-continuation of therapy. There is no suggestion ofa deleterious impact on sexual function—in fact,there is evidence of a positive effect of doxazosinon erectile dysfunction.
Overall, the balanced action of doxazosin onα1-adrenoceptor subtypes is associated with ahighly desirable clinical profile for the BPHpatient. Any advantages arising from a genuinelyprostate-selective antagonist will ultimately have
TABLE 8.1 Incidence of adverse events in patients with BPH treated with doxazosin GITS, doxazosin standard, andplacebo. (Adapted from Kirby et al.59)
GITS, gastrointestinal therapeutic system.
Doxazosin GITS (%) Doxazosin standard (%) Placebo (%)(n = 666) (n = 651) (n = 156)
All adverse events 41.1 53.6 39.1
Treatment-related adverse events 16.1 25.3 7.7
Discontinuations due to 3.3 4.8 0.6treatment-related adverse events
Ch 08 13/5/05 3:26 pm Page 113

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA114
to be weighed against the deficits of such therapyin the treatment of the whole patient.61
REFERENCES
1. Kenny B A, Miller A M, Williamson I J et al.Evaluation of the pharmacological selectivity pro-file of α1 adrenoceptor antagonists at prostatic α1adrenoceptors: binding, functional and in vivostudies. Br J Pharmacol 1996; 118: 871–878
2. Bylund B D, Eikenberg D C, Hieble J P et al.International Union of Pharmacologic nomencla-ture of adrenoceptors. Pharmacol Rev 1994; 46:121–136
3. Eri L M, Tveter K L. Alpha-blockade in the treat-ment of symptomatic benign prostatic hyperplasia.J Urol 1995; 154: 923–934
4. Kenny B A, Naylor A M, Carter A J et al. Effect ofalpha1 adrenoceptor antagonists on prostatic pres-sure and blood pressure in the anesthetized dog.Urology 1994; 44: 52–57
5. Elliot H L, Meredith P A, Sumner D J et al. Apharmacodynamic and pharmacokinetic assess-ment of a new alpha-adrenoceptor antagonist, dox-azosin (UK-33274) in normotensive subjects. Br JClin Pharmacol 1982; 13: 699–703
6. Young R A, Brogden R N. Doxazosin: a review ofits pharmacodynamic and pharmacokinetic prop-erties and therapeutic efficacy in mild to moderatehypertension. Drugs 1988; 35: 535–541
7. Boyle P, Napalkov P. The epidemiology of benignprostatic hyperplasia and observations on concomi-tant hypertension. Scand J Urol Nephrol 1995; 168:7–12
8. Kirby R, Andersson K E, Lepor H et al. Alpha-1adrenoceptor selectivity and the treatment ofbenign prostatic hyperplasia and lower urinarytract symptoms. Prostate Cancer Prostatic Dis2000; 3: 76–83
9. Forray C, Chiu G, Wetzel J M et al. Effects of novelalpha1-C adrenergic receptor antagonists on thecontraction of human prostate smooth muscle. JUrol 1994; 151: 267A (abstract 159)
10. Goetz A S, Lutz M W, Rimele T J et al.Characterization of alpha1 adrenoceptor subtypesin human and canine prostate membranes. JPharmacol Exp Ther 1994; 271: 1228–1233
11. Ford A P, Daniels D V, Chang D J et al.Pharmacological pleiotropism of the humanrecombinant alpha1A-adrenoceptor: implicationsfor alpha1-adrenoceptor classification. Br JPharmacol 1997; 121: 1127–1135
12. Chapple C R, Carter P, Christmas T J et al. A threemonth double-blind study of doxazosin as treat-ment for benign prostatic bladder outlet obstruc-tion. Br J Urol 1994; 74: 50–56
13. Gillenwater J Y, Conn R L, Chrysant S G et al.Doxazosin for the treatment of benign prostatichyperplasia in patients with mild to moderateessential hypertension: a double-blind, placebo-controlled, dose-response multicenter study. J Urol1995; 154: 110–115
14. Fawzy A, Braun K, Lewis G P et al. Doxazosin inthe treatment of benign prostatic hyperplasia innormotensive patients: a multicenter study. J Urol1995; 154: 105–110
15. Holme J B, Christensen M M, Rasmussen P C et al.29 weeks doxazosin treatment in patients withsymptomatic benign prostatic hyperplasia. Scand JUrol Nephrol 1994; 28: 77–82
16. Christensen M M, Holme J B, Rasmussen P C et al.Doxazosin treatment in patients with prostaticobstruction. A double-blind placebo-controlledstudy. Scand J Urol Nephrol 1993; 27: 39–44
17. Mobley D F, Kaplan S, Ice K et al. Effect of doxa-zosin on the symptoms of benign prostatic hyper-plasia: results from three double-blind placebo-controlled studies. Int J Clin Pract 1997; 51:282–288
18. Andersen M, Dahlstrand C, Høye K. Double-blindtrial of the efficacy and tolerability of doxazosin inthe gastrointestinal therapeutic system, doxazosinstandard, and placebo in patients with benign pro-static hyperplasia. Eur Urol 2000; 38: 400–409
19. Gratzke P, Kirby R S. Doxazosin GITS and doxa-zosin standard in patients with benign prostatichyperplasia: double-blind trial of efficacy and toler-ability. Fortschr Med 2000; 11: 83–92
Ch 08 13/5/05 3:26 pm Page 114

DOXAZOSIN IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 115
20. Roehrborn C G, Siegel R L. Safety and efficacy ofdoxazosin in benign prostatic hyperplasia: a pooledanalysis of three, double-blind, placebo-controlledstudies. Urology 1996; 48: 406–415
21. Abrams P. Urodynamic effects of doxazosin in menwith lower urinary tract symptoms and benign pro-static obstruction. Results from three double-blindplacebo-controlled studies. Eur Urol 1997; 32:39–46
22. Kaplan S A, Ikeguchi T E E, Santarosa R P. Thetreatment of benign prostatic hyperplasia withalpha blockers in men over the age of 80 years. Br JUrol 1997; 80: 875–879
23. Lepor H, Kaplan S A, Klimberg I et al. Doxazosinfor benign prostatic hyperplasia: long-term efficacyand safety in hypertensive and normotensivepatients. J Urol 1997; 157: 525–530
24. Fawzy A, Hendry A, Cook E et al. Long-term (4year) efficacy and tolerability of doxazosin for thetreatment of concurrent benign prostatic hyperpla-sia and hypertension. Int J Urol 1999; 6: 346–354
25. Kirby R S, Roehrborn C, Boyle P et al. for thePREDICT study investigators. Efficacy and tolera-bility of doxazosin and finasteride, alone or in com-bination, in treatment of symptomatic benign pro-static hyperplasia: the Prospective EuropeanDoxazosin and Combination Therapy (PREDICT)Trial. Urology 2003; 61: 119–216
26. Lepor H, Williford W O, Barry M J et al. for theVeterans’ Affairs Cooperative Studies BenignProstatic Hyperplasia Study Group. The efficacy ofterazosin, finasteride or both in benign prostatichyperplasia. N Engl J Med 1996; 335: 533–539
27. McConnell J D, the MTOPS steering committee.The impact of medical therapy on the clinical pro-gression of BPH: results of the MTOPS trial. J Urol2002; 167 (Suppl 4): abstract 1042
28. Kaplan S A, Meade D’Alisera. Tolerability of a-blockade with doxazosin as a therapeutic option forsymptomatic benign prostatic hyperplasia in theelderly patient: a pooled analysis of seven double-blind, placebo-controlled studies. J Gerontol 1998;53A: M201–M206
29. Bylund D B, Regan J W, Faber J E et al. Vascularalpha-adrenoceptors: from the gene to the human.Can J Physiol Pharmacol 1995; 73: 533–543
30. Hoffman B B, Hu Z-H. Regulation of responsesmediated by alpha1-adrenergic receptors in smoothmuscle cultures. Pharmacol Commun 1995; 6: 1–3
31. Kaplan S A, Meade-D’Alisera P, Quinones S et al.Doxazosin in physiologically and pharmacological-ly normotensive men with benign prostatic hyper-plasia. Urology 1995; 46: 512–517
32. Kirby R. Doxazosin in benign prostatic hyperpla-sia: effects on blood pressure and urinary flow innormotensive and hypertensive men. Urology1995; 46: 182–186
33. Guthrie R M, Siegel R L for the Hypertension andBPH Intervention Trial (HABIT) MulticenterStudy Group. A multicenter, community-basedstudy of doxazosin in the treatment of concomitanthypertension and symptomatic benign prostatichyperplasia: The Hypertension and BPHIntervention Trial (HABIT). Clin Ther 1999; 21:1732–1748
34. Pool J L. Effects of doxazosin on coronary heartdisease risk factors in the hypertensive patients. BrJ Clin Pract Symp Suppl 1994; 74: 8–12
35. Pool J L. Effects of doxazosin on serum lipids. Areview of the clinical data and molecular basis foraltered lipid metabolism. Am Heart J 1991; 121:251–260
36. Neaton J D, Grimm R H, Prineas R J et al.Treatment of Mild Hypertensive Study: finalresults. J Am Med Assoc 1993; 270: 713–724
37. Chait A, Gilmore M, Kawamura M. Inhibition oflow density lipoprotein oxidation in vitro by the 6-and 7-hydroxy metabolites of doxazosin, an alpha1-adrenergic antihypertensive agent. Am JHypertens 1994; 7: 159–164
38. Jackson C L, Schwartz S M. Pharmacology ofsmooth muscle cell replication. Hypertension 1992;20: 713–736
39. Hu Z -H, Shi X -Y, Okazaki M, Hoffman B B.Angiotensin II induces transcription and expres-sion of alpha1-adrenergic receptors in vascular
Ch 08 13/5/05 3:26 pm Page 115

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA116
smooth muscle. Am J Physiol 1995; 268:H1006–1014
40. Langdon C G, Packard R S. Doxazosin in hyper-tension: results of a general practice study in 4809patients. Br J Clin Pract 1994; 48: 293–298
41. Levy D, Wilson P W F, Anderson K M, Castelli WP. Stratifying patients at risk from coronary heartdisease; new insights from the Framingham HeartStudy. Am Heart J 1990; 119: 71–77
42. Levy D, Walmsley P, Levenstein M for theHypertension and Lipid Trial Study Group.Principal results of the Hypertension and LipidTrial (HALT): a multicenter study of doxazosin inpatients with hypertension. Am Heart J 1996; 131:966–973
43. Daae L N W, Westlie L. A 5-year comparison ofdoxazosin and atenolol in patients with mild-to-moderate hypertension: effects on blood pressure,serum lipids, and coronary heart disease risk. BloodPress 1998; 7: 39–45
44. Flack J M, Nasser S A. The Antihypertensive andLipid-Lowering Treatment to Prevent HeartAttack Trial (ALLHAT). Major outcomes in high-risk hypertensive patients randomized toangiotensin-converting enzyme inhibitor or calci-um channel blocker vs diuretic. Curr HypertensRep 2003; 5: 189–191
45. Kirby R S, Pool J L. Interpretation of the ALL-HAT interim analysis and implications for thetreatment of patients with BPH. Prostate CancerProstatic Dis 2000; 3: 152–156
46. Grimm R H, Grandits G A, Prineas R J et al.Long-term effects on sexual function of five anti-hypertensive drugs and nutritional hygienic treat-ment in hypertensive men and women. Treatmentof Mild Hypertension Study (TOMHS).Hypertension 1997; 29: 8–14
47. De Rose A F, Carmignani G, Corbu C et al.Observational multicentric trial performed withdoxazosin: evaluation of sexual effects on patientswith diagnosed benign prostatic hyperplasia. UrolInt 2002; 68: 95–98
48. Andersson K -E. Pharmacology of lower urinarytract smooth muscles and penile erectile tissues.Pharmacol Rev 1993; 45: 253–308
49. Kaplan S A, Rodolfo B R, Kohn I J et al.Combination therapy using oral alpha-blockersand intracavernosal injection in men with erectiledysfunction. Urology 1998; 52: 739–743
50. De Rose A F, Giglio M, Traverso P et al. Combinedoral therapy with sildenafil and doxazosin for thetreatment of non-organic erectile dysfunctionrefractory to sildenafil monotherapy. Int J ImpotRes 2002; 14: 50–53
51. Frankel S J, Donovan J L, Peters T I et al. Sexualdysfunction in men with lower urinary tract symp-toms. J Clin Epidemiol 1998; 51: 677–685
52. Ishizuka O, Persson K, Mattiasson A et al.Micturition in conscious rats with and without out-let obstruction: role of spinal alpha1 adrenoceptors.Br J Pharmacol 1996; 117: 962–966
53. Ramage A G, Wyllie M G. Effects of doxazosinand terazosin on inferior mesenteric nerve activity,spontaneous bladder contraction and blood pres-sure in anaesthetised cats. Br J Pharmacol 1994;112: 526P
54. Kyprianou N. Doxazosin and terazosin suppressprostate growth by inducing apoptosis: clinical sig-nificance. J Urol 2003; 169: 1520–1525
55. Chon J K, Borkowski A, Partin A W et al. Alpha-1adrenoceptor antagonists terazosin and doxazosininduce prostate apoptosis without affecting cellproliferation in patients with benign prostatichyperplasia. J Urol 1999; 161: 2002–2008
56. Kyprianou N, Benning C M. Suppression ofhuman prostate cancer cell growth by alpha 1-adrenoceptor antagonists doxazosin and terazosinvia induction of apoptosis. Cancer Res 2000; 60:4550–4555
57. Os I, Stokke H P. Doxazosin GITS compared withdoxazosin standard and placebo in patients withmild hypertension. Blood Press 1999; 8: 184–191
58. Os I, Stokke H P for the Doxazosin Investigators’Study Group. Effects of doxazosin in the gastroin-testinal therapeutic system formulation versus dox-azosin standard and placebo in mild-to-moderatehypertension. J Cardiovasc Pharmacol 1999; 33:791–797
Ch 08 13/5/05 3:26 pm Page 116

DOXAZOSIN IN THE TREATMENT OF BENIGN PROSTATIC HYPERPLASIA 117
59. Kirby R S, Andersen M, Gratzke P et al. A com-bined analysis of double-blind trials of the efficacyand tolerability of doxazosin in the gastrointestinaltherapeutic system (GITS), doxazosin standard,and placebo in patients with benign prostatichyperplasia. BJU Int 2001; 87: 192–200
60. Kirby R S. A randomized, double-blind crossoverstudy of tamsulosin and controlled-release doxa-
zosin in patients with benign prostatic hyperplasia.BJU Int 2003; 91: 41–44
61. Roehrborn C G, Schwinn D A. Alpha1-adrenergicreceptors and their inhibitors in lower urinary tractsymptoms and benign prostatic hyperplasia. J Urol2004; 171: 1029–1035
Ch 08 13/5/05 3:26 pm Page 117

Ch 08 13/5/05 3:26 pm Page 118

AlfuzosinA Jardin
9
INTRODUCTION
Alfuzosin, a quinazoline derivative, acts as aselective antagonist of α1-adrenoceptor-mediatedcontraction of bladder neck, proximal urethral,and prostatic smooth muscle. Bladder outletresistance resulting from benign prostatic hyper-plasia (BPH) is consequently reduced. Alfuzosinis approved in Europe for the treatment of symp-tomatic BPH.
PHARMACOLOGIC PROFILE OF ALFUZOSINAT α1-ADRENOCEPTOR SUBTYPES
The human prostatic smooth muscle containshigh densities of α1-adrenoceptors.1,2 Several α1-adrenoceptor subtypes have been identified andtheir heterogeneity revealed both pharmacologi-cally and by molecular cloning.3,4 The three α1-adrenoceptor subtypes with high affinity for pra-zosin (grouped under the α1H heading), so faridentified, i.e. α1A-, α1B-, and α1D-adrenoceptors,have been cloned (α1a, α1b, and α1d). Anotheradrenoceptor subtype has been identified and ischaracterized by a low affinity for prazosin andfor that reason entitled α1L.5,7,8 Table 9.1 summa-rizes the affinity for the three cloned α1-adreno-ceptors of the major α1-adrenoceptor antagonistsavailable today. As shown with doxazosin, tera-zosin, and prazosin, alfuzosin has no distinctselectivity for any of the receptor subtypes.Uroselectivity has been shown to result from thepharmacodynamic properties of agents without
specificity for any particular subtype, however.9
In addition, uroselectivity does not appear to berelated to receptor subtype affinity.10
AFFINITY OF ALFUZOSIN FOR α-ADRENOCEPTORS IN THE HUMANPROSTATE
The cranial region of the human prostatic adeno-ma possesses high affinity [3H]-prazosin bindingsites.11,12 These sites display the pharmacologiccharacteristics of α1-adrenoceptors. As shown inTable 9.2, [3H]-prazosin binding is potently dis-placed by alfuzosin and phentolamine, with IC50
values in the low nanomolar range, while the α2-adrenoceptor antagonists idazoxan and yohim-bine, and the β-adrenoceptor antagonist propra-nolol, only affect [3H]-prazosin binding with IC50
values in the micromolar range. Thus, alfuzosin
TABLE 9.1 Affinity of various α1-adrenoceptor antago-nists for the human cloned α1-adrenoceptors.
Adapted from Forray C et al.6 and Kenny et al.7
AffinityCompound α1a α1b α1d
Alfuzosin 8.20 8.53 8.40
Doxazosin 8.56 8.98 8.78
Prazosin 9.70 9.60 9.50
Tamsulosin 9.70 8.90 9.80
Terazosin 8.16 8.71 8.46
5-ME-Urapidil 8.68 6.76 7.91
119
Ch 09 13/5/05 3:33 pm Page 119

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA120
shows high affinity for α1-adrenoceptors in thehuman prostate, which represents the pharmaco-logic target in BPH. In support of this view, it hasbeen reported that alfuzosin-displaceable [125I]-HEAT (iodo-4-hydroxyphenyl-ethyl-amino-methyl-tetralone) binding sites, which have thepharmacologic characteristics of α1-adrenocep-tors, are exclusively associated with muscularstroma of the prostate and are markedly elevatedin sections from prostatic adenomas as comparedwith nonhypertrophic tissue.13
As far as α1-adrenoceptor subtypes are con-cerned, Faure et al.14 have shown that the humanprostate expresses at the level of the apex, base,periurethral, and lateral lobe, mRNA transcriptscorresponding to α1a-, α1b-, and α1d-adrenocep-tors. In addition, these authors have shown that areconstituted partial sequence (349 amino acids)of the human prostatic α1α-adrenoceptor shares94% identity with the bovine brain α1a-adreno-ceptor, and that this receptor represents the pre-dominant α1-adrenoceptor subtype in this tissue.
FUNCTIONAL UROSELECTIVITY OFALFUZOSIN
Effects on elevated urethral and blood pressure
Inhibition of urethral responses to stimulation ofhypogastric sympathetic nerves in the cat is con-sidered to represent an animal model of thedynamic sympathetic constriction of urethralsmooth muscle, which is regarded as a contribu-tory factor in the obstructive disorders whichcharacterize BPH.15 On the other hand, α1-adrenoceptor antagonist reduction of blood pres-sure in spontaneous hypertensive rats is acceptedas a model to assess antihypertensive drugs actingat receptors physiologically stimulated by anincreased sympathetic tone. Thus a relationship
between the ability of alfuzosin to inhibit sympa-thetically mediated increases in urethral tone inthe cat and sympathetically mediated hyperten-sion in the spontaneously hypertensive rat can beconsidered as a relevant way to evaluate the ther-apeutic margin in BPH with respect to unwantedvascular effects (e.g. orthostatic hypotension).15
Studies conducted in the anesthetized cat andin conscious spontaneously hypertensive rats con-firm the α1-antagonist properties of alfuzosin.The compound produces a dose-related as well asa complete and prolonged inhibition of the rise inurethral pressure resulting from postganglionicstimulation of hypogastric sympathetic nerves inthe cat. As shown in Table 9.3, alfuzosin decreas-es the urethral resistance induced by hypogastricnerve stimulation in the cat at doses 11 timeslower than those which reduce blood pressure inspontaneously hypertensive rats.15
Effects on normal urethral and arterial bloodpressure
In recent years, attempts have been made to eval-uate, in the same animal, the respective effects ofα1-adrenoceptor antagonists on prostatic tissue
TABLE 9.2 Affinity of alfuzosin for α1-adrenoceptors incranial human prostatic adenoma labeled with 3H-pra-zosin.
*IC50 values represent drug concentrations producing50% inhibition of specific 3H-prazosin binding. Values aretaken from Pimoule et al.11 and Lefevre-Borg et al.12
Drug IC50* (µM)
Alfuzosin 0.035 ± 0.008
Phenoxybenzamine 0.038 ± 0.016
Idazoxan 3.5 ± 1.0
Yohimbine 6.0 ± 2.0
Propranolol 37 ± 9
Ch 09 13/5/05 3:33 pm Page 120

ALFUZOSIN 121
compared to side-effects, most particularly theeffects on blood pressure. In the most recentlydeveloped model, which allows the simultaneousmeasurement of urethral and arterial pressures inconscious male rats,16 a direct estimation of thefunctional uroselectivity of alfuzosin was per-formed. At clinically relevant doses (10–30 µg/kg,intravenous route), alfuzosin decreased urethralpressure without noticeable effects on blood pres-sure (Figure 9.1). In a comparative investigation,using the same experimental model, the function-al uroselectivity of alfuzosin has been shown to besuperior to that of other α1-adrenoceptor antago-nists.17 These results are further evidence thatfunctional uroselectivity may be achieved in theabsence of pharmacologic selectivity for one ofthe α1-adrenoceptor subtypes.
TISSUE DISTRIBUTION
The role of tissue distribution of α1-adrenoceptorantagonists and its possible effect on functionaluroselectivity has been less rigorously examined.However, a direct measurement of plasma andprostate distribution of alfuzosin, related to meas-urement of its pharmacologic activity on arterial
blood pressure and urethral pressure, has broughtnew and useful information.18 One hour follow-ing oral administration of 10 mg/kg of alfuzosin
TABLE 9.3 Effects of alfuzosin on urethral pressure (UP) in the cat and on mean arterial blood pressure (AP) in thespontaneously hypertensive rat.
The doses of each compound producing a 50% reduction in urethral pressure (UP50) in anesthetized cats and a 20% reduc-tion in blood pressure (UP20) in spontaneously hypertensive rats are shown. Values are taken from Lefevre-Borg et al.15
Dose producing a 50% reduction Dose producing a 20% reductionin urethral pressure in arterial blood pressure Uroselectivity ratio
Compound (ID50 UP) (mg/kg, id) (ID20AP) (mg/kg, po) (ID20 AP/ID50 UP)
Alfuzosin 0.36 4.0 11
Terazosin 0.12 0.42 3.5
Prazosin 0.12 0.13 1
0.001 0.010 0.100 1
0
–20
–40
–60
–80
–100
Ure
thra
l p
ressu
re (
% in
hib
itio
n)
Dose (mg/kg. i.v.)
FIGURE 9.1 Effect of alfuzosin (triangle) comparedwith vehicle control (circle) on an increase in urethralpressure in the anesthetized cat. Doses of alfuzosin corre-spond to cumulative i.v. bolus administration of the drug.Increased urethral pressure was elicited by electrical stim-ulation of sympathetic hypogastric nerves. (From ref. 5with permission.)
Ch 09 13/5/05 3:33 pm Page 121

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA122
in rats, plasma and prostate levels, respectively,reached 88.0 ng/ml and 335 ng/ml, leading to aprostate/plasma concentration ratio of 3.8. At 6hours, the plasma concentration decreased to20 ng/ml, whereas prostatic tissue concentrationwas still about nine times higher than plasmaconcentration. Moreover, in the same study, anindex of the antagonistic activity of alfuzosinagainst phenylephrine-induced urethral contrac-tions was directly correlated with prostatic tissueconcentrations. This study, by demonstrating thatalfuzosin concentrates in the prostate at levels4–9-fold above the plasma levels, may thus pro-vide a basis for its preferential activity in thelower urinary tract compared to vascular effects.High prostatic diffusion of alfuzosin has alsobeen observed in orally treated patients.19
Conclusions
In conclusion, alfuzosin is a potent selective α1-adrenoceptor antagonist which displays function-al uroselectivity in animal models. These phar-macologic properties lend support to the theorythat alfuzosin alleviates the dynamic componentof urinary obstruction attributable to sympathetictone in BPH. These pharmacologic properties arelikely to underlie the clinical profile of alfuzosin.
PHARMACOKINETIC PROPERTIES
The pharmacokinetics of alfuzosin are linear andnonsaturable. Absorption of the immediaterelease (IR) formulation of alfuzosin is relativelyrapid, with a maximum plasma concentrationoccurring after a mean of 1.5 hours. Its bioavail-ability is 64%, with a negligible effect of concomi-tant administration of food on its absorption.Alfuzosin is approximately 90% protein bound inplasma. It is extensively metabolized by the liver
and the metabolites are inactive. Its main route ofelimination is fecal. The mean plasma elimina-tion half life of IR alfuzosin is 4.8 hours. Becauseof this pharmacokinetic profile, the IR of alfu-zosin has to be administered three times daily(7.5 mg/day). The slow release (SR) formulationof alfuzosin (5 mg daily), currently available inEurope, has been developed in order to improvecompliance with the treatment by reducing thenumber of daily doses from three to two. The rel-ative bioavailability of this formulation is 15%lower than for the IR formulation of alfuzosin.The time to reach the peak is longer, approxi-mately 3 hours instead of 1.5 hours, confirmingthat the absorption is delayed as well as its appar-ent elimination half-life, which is 8 hours. Theusual recommended daily dose is 5 mg twicedaily, i.e. 10 mg/day. This higher daily dosagecompares with the usual daily dose of 7.5 mg forthe IR formulation, compensating for the relativeloss of bioavailability.
A once-daily formulation of alfuzosin is nowavailable and, although the absorption character-istics are different from the IR and SR formula-tions, the metabolism of the drug is similar.20,21
Inactive barrier layers ensure that the active ele-ment is released over 20 hours. The dissolutionrate is almost constant between 2 and 12 hoursand the area under the plasma concentration–timecurve is similar over 24 hours to that observed for2.5 mg thrice-daily and 5 mg twice-daily formu-lations. The plasma elimination half-life of theprolonged-release 10 mg formulation was 9.1hours compared to 7 hours for the IR formula-tion.19 The pharmacokinetic properties of 10 mgalfuzosin once-daily were not significantly differ-ent in patients with renal impairment or in olderadults compared to the IR formulation.22,23
The overall pharmacokinetic profile of alfu-zosin is not significantly changed in patients with
Ch 09 13/5/05 3:33 pm Page 122

ALFUZOSIN 123
renal insufficiency, in contrast to what is observedin patients with hepatic insufficiency, wheredosage modifications appear to be necessary.
PHARMACODYNAMIC EFFECTS IN HUMANS
Urodynamic effects
Intravenous alfuzosin significantly reduced highurethral pressure arising from neurologic causes.One hundred and sixty-three patients with neu-rogenic bladder disease (NBD) and a mean max-imal urethral pressure of 108 cmH2O wereincluded in a randomized, double-blind, placebo-controlled study assessing the effect of a single i.v.injection of alfuzosin (0.5, 1, or 2 mg) or placebo.Alfuzosin significantly and dose-dependentlydecreased urethral pressure, with a meandecrease of 44% for the 2 mg dose.24 A single i.v.test dose of 5 mg alfuzosin had previously beenused to determine which patients with spinal cordinjury (n = 21) were likely to benefit from alfu-zosin therapy. Response was assessed in terms ofchange in micturition, residual urine, and poste-rior urethral pressure and diameter.25
Furthermore, in a placebo-controlled study con-ducted in 66 patients with NBD, this decreasewas maintained with oral alfuzosin for 12 weeksand associated with a significant improvement ofvoiding symptoms (–45%) and residual urine vol-ume (–39%) compared with placebo.26 Theseactions appear to be correlated with the α1-adrenoceptor antagonism produced by alfuzosin.
In patients with BPH, orally administered IRalfuzosin significantly and dose-dependentlyincreased urinary flow rates from the first dose.27
At 90 minutes after a single alfuzosin dose, peakflow rate (PFR) was significantly increased by 23and 34% with 1.25 and 2.5 mg, respectively, com-pared with placebo in 93 patients with initial PFR
values of less than 15 ml/s. In patients with PFRvalues of less than 10 ml/s (n = 47), mean increas-es in PFR with 1.25 or 2.5 mg alfuzosin or place-bo were even greater: 26, 55, and 17%, respective-ly.27 Similar results were observed with SR alfu-zosin. At 180 minutes after a single SR alfuzosindose, PFR was significantly increased by 29 and36% with 3 and 5 mg doses compared with place-bo (+17%) in elderly patients (≥65 years) with ini-tial PFR values of less than 15 ml/s.28
The 30% increase in flow rates, which is therate of improvement expected with α1-blockertherapy in patients with BPH, is maintained aftermultiple-dose administration of alfuzosin.28–32
Furthermore, this is of the same order of magni-tude as that of prazosin 4 mg per day33,34 and tam-sulosin 0.4 mg per day.31 In those patients with anincrease in PFR of at least 25% (i.e. 45–50% ofpatients), the mean increase with alfuzosin isapproximately 5 ml/s.
Residual urine volume is a parameter reflect-ing not only the decrease in urinary flow resist-ance, but also the bladder contractility which mayshow wide intra-individual variability betweenserial examinations.35 Alfuzosin has been shownto decrease significantly the volume of residualurine by 38% after 6 months of treatment com-pared with 9% in placebo recipients.29
A pooled analysis of 11 double-blind, placebo-controlled trials involving 1470 LUTS patientsshowed that immediate- and sustained-releasealfuzosin effectively reduced postvoid residualurine volume.36 Significant differences wereobserved between patients treated with alfuzosinand those who received placebo. The analysisshowed that acute urinary retention (AUR) wasmore common in men with residual urine greaterthan 100 ml. Patients receiving alfuzosin wereless likely to suffer AUR than those receivingplacebo.
Ch 09 13/5/05 3:33 pm Page 123
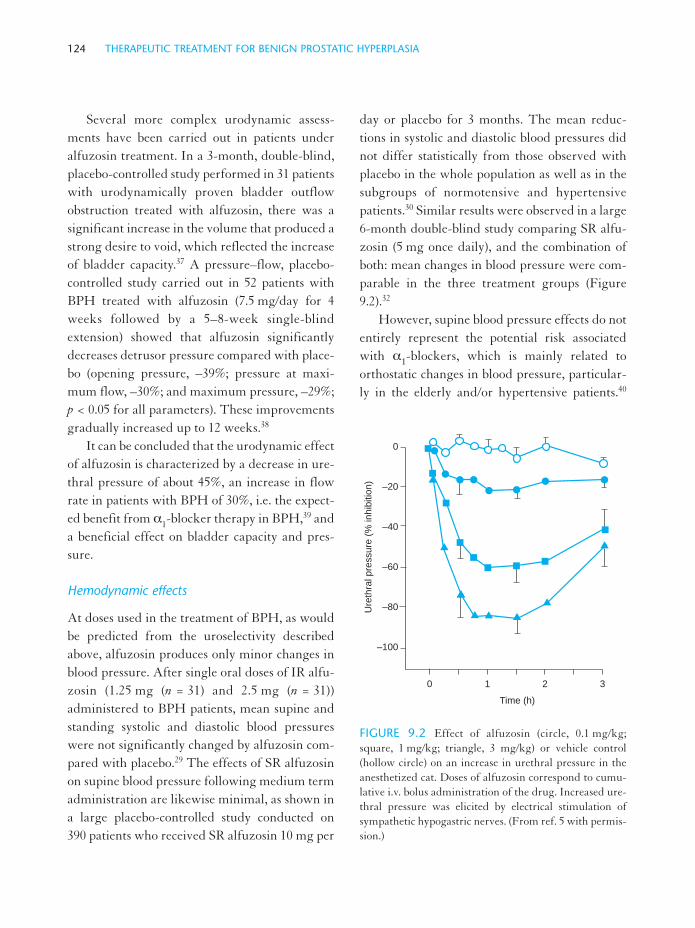
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA124
Several more complex urodynamic assess-ments have been carried out in patients underalfuzosin treatment. In a 3-month, double-blind,placebo-controlled study performed in 31 patientswith urodynamically proven bladder outflowobstruction treated with alfuzosin, there was asignificant increase in the volume that produced astrong desire to void, which reflected the increaseof bladder capacity.37 A pressure–flow, placebo-controlled study carried out in 52 patients withBPH treated with alfuzosin (7.5 mg/day for 4weeks followed by a 5–8-week single-blindextension) showed that alfuzosin significantlydecreases detrusor pressure compared with place-bo (opening pressure, –39%; pressure at maxi-mum flow, –30%; and maximum pressure, –29%;p < 0.05 for all parameters). These improvementsgradually increased up to 12 weeks.38
It can be concluded that the urodynamic effectof alfuzosin is characterized by a decrease in ure-thral pressure of about 45%, an increase in flowrate in patients with BPH of 30%, i.e. the expect-ed benefit from α1-blocker therapy in BPH,39 anda beneficial effect on bladder capacity and pres-sure.
Hemodynamic effects
At doses used in the treatment of BPH, as wouldbe predicted from the uroselectivity describedabove, alfuzosin produces only minor changes inblood pressure. After single oral doses of IR alfu-zosin (1.25 mg (n = 31) and 2.5 mg (n = 31))administered to BPH patients, mean supine andstanding systolic and diastolic blood pressureswere not significantly changed by alfuzosin com-pared with placebo.29 The effects of SR alfuzosinon supine blood pressure following medium termadministration are likewise minimal, as shown ina large placebo-controlled study conducted on390 patients who received SR alfuzosin 10 mg per
day or placebo for 3 months. The mean reduc-tions in systolic and diastolic blood pressures didnot differ statistically from those observed withplacebo in the whole population as well as in thesubgroups of normotensive and hypertensivepatients.30 Similar results were observed in a large6-month double-blind study comparing SR alfu-zosin (5 mg once daily), and the combination ofboth: mean changes in blood pressure were com-parable in the three treatment groups (Figure9.2).32
However, supine blood pressure effects do notentirely represent the potential risk associatedwith α1-blockers, which is mainly related toorthostatic changes in blood pressure, particular-ly in the elderly and/or hypertensive patients.40
0 1 2 3
0
–20
–40
–60
–80
–100
Ure
thra
l p
ressu
re (
% in
hib
itio
n)
Time (h)
FIGURE 9.2 Effect of alfuzosin (circle, 0.1 mg/kg;square, 1 mg/kg; triangle, 3 mg/kg) or vehicle control(hollow circle) on an increase in urethral pressure in theanesthetized cat. Doses of alfuzosin correspond to cumu-lative i.v. bolus administration of the drug. Increased ure-thral pressure was elicited by electrical stimulation ofsympathetic hypogastric nerves. (From ref. 5 with permis-sion.)
Ch 09 13/5/05 3:34 pm Page 124
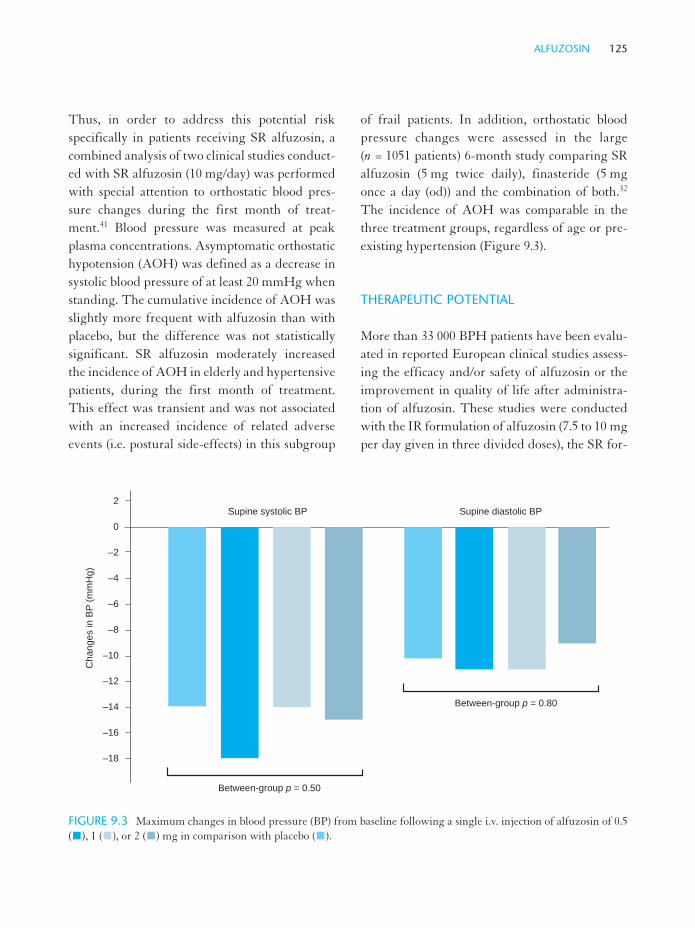
ALFUZOSIN 125
Thus, in order to address this potential riskspecifically in patients receiving SR alfuzosin, acombined analysis of two clinical studies conduct-ed with SR alfuzosin (10 mg/day) was performedwith special attention to orthostatic blood pres-sure changes during the first month of treat-ment.41 Blood pressure was measured at peakplasma concentrations. Asymptomatic orthostatichypotension (AOH) was defined as a decrease insystolic blood pressure of at least 20 mmHg whenstanding. The cumulative incidence of AOH wasslightly more frequent with alfuzosin than withplacebo, but the difference was not statisticallysignificant. SR alfuzosin moderately increasedthe incidence of AOH in elderly and hypertensivepatients, during the first month of treatment.This effect was transient and was not associatedwith an increased incidence of related adverseevents (i.e. postural side-effects) in this subgroup
of frail patients. In addition, orthostatic bloodpressure changes were assessed in the large(n = 1051 patients) 6-month study comparing SRalfuzosin (5 mg twice daily), finasteride (5 mgonce a day (od)) and the combination of both.32
The incidence of AOH was comparable in thethree treatment groups, regardless of age or pre-existing hypertension (Figure 9.3).
THERAPEUTIC POTENTIAL
More than 33 000 BPH patients have been evalu-ated in reported European clinical studies assess-ing the efficacy and/or safety of alfuzosin or theimprovement in quality of life after administra-tion of alfuzosin. These studies were conductedwith the IR formulation of alfuzosin (7.5 to 10 mgper day given in three divided doses), the SR for-
2
0
–2
–4
–6
–8
–10
–12
–14
–16
–18
Between-group p = 0.50
Between-group p = 0.80
Supine systolic BP Supine diastolic BP
Ch
an
ge
s in
BP
(m
mH
g)
FIGURE 9.3 Maximum changes in blood pressure (BP) from baseline following a single i.v. injection of alfuzosin of 0.5( ), 1 ( ), or 2 ( ) mg in comparison with placebo ( ).
Ch 09 13/5/05 3:35 pm Page 125

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA126
mulation (SR alfuzosin 5 mg bid), and, morerecently, the once-a-day formulation (alfuzosin10 mg od) for the treatment of symptomaticBPH.
Clinical efficacy
Jardin et al.29 reported the efficacy of alfuzosin ina large multicenter placebo-controlled study of518 patients with symptoms of BPH whoreceived either alfuzosin 7.5 or 10 mg/day orplacebo for 6 months. Patients were evaluatedusing the Boyarsky symptom scoring system, uri-nary flow rates, and postvoid residual urine vol-ume. Obstructive and irritative symptoms,assessed according to the Boyarsky scale,improved significantly in the alfuzosin group
compared with the placebo group (p = 0.004).Fewer patients in the alfuzosin group than in theplacebo group dropped out due to lack of efficacy(6.8 vs 14.6%, p = 0.0004) and the prevalence ofspontaneous acute urine retention (AUR) waslower in the alfuzosin group (0.4% vs 2.6%,p = 0.04). By 6 months, mean urinary flow rateshad increased (p < 0.05) and residual volume haddecreased (p < 0.017) in the alfuzosin group.Clinical improvement with alfuzosin could bemaintained for up to 30 months, as observed innoncomparative extensions of the original 6-month study42,43 (Figure 9.4)
In a 3-month placebo-controlled study withthe SR formulation of alfuzosin (5 mg bid) in 390men, patients reported a clinically relevant andstatistically significant improvement of their
1
0
–1
–2
–3
0
–1
–2
1
0
–1
2
1
0
–1
Systo
licS
ysto
licD
iasto
licD
iasto
lic
Ch
an
ge
s in
BP
(m
mH
g)
Length of study (days)
0 28 56 84
p = 0.18
p = 0.02
p = 0.84
p = 0.008
(a)
(b)
FIGURE 9.4 Systolic and diastolic blood pressure (BP) in a 3-month study of placebo ( ) vs. slow release (SR) alfuzosin10 mg/day ( ) in 390 patients with BPH: (a) changes from baseline in supine BP; (b) changes in upright minus supine BP.(Unpublished data.)
Ch 09 13/5/05 3:35 pm Page 126

ALFUZOSIN 127
urinary symptoms in comparison with placebo(Figure 9.5). A clinical improvement in LUTSwas observed whatever their initial severity, withan overall improvement in total I-PSS score of30% as a mean.30 The clinical efficacy wasobserved from the first month. Maximum flowrate increased significantly with SR alfuzosin(+2.4 ml/s, i.e. +29%) compared with placebo(+1.1 ml/s, i.e. +14%, p = 0.006). Residual urinewas also significantly reduced with SR alfuzosin.In those patients with baseline Qmax ≤ 12 ml/s andI-PSS score ≥13, the total I-PSS score decreasedby 6.7 points (36%) (comparison versus placebo:p = 0.002) (Table 9.4).
The efficacy of the once-daily formulation,administered at a dose of 10 mg per day without
initial titration, has been compared to that of theIR formulation (2.5 mg thrice daily) and placeboin a 3-month study which involved 436 patients:symptomatic improvement with the od formula-tion was significantly higher than placebo andsimilar to that of the IR formulation, with I-PSSimprovements of 6.9 points in the od group and6.4 points in the 2.5 mg tid group (p = 0.002 and0.02 vs placebo, respectively). The bothersome-ness of these symptoms, assessed using the quali-ty of life index, was also significantly improvedwith both formulations compared with placebo(Table 9.5) (the ALFORTI study44). Followingtreatment with alfuzosin od, Qmax (measured attrough plasma levels) also significantly increasedin comparison with placebo (mean SD values:
10
9
8
7
6
5
4
0
0 0.5 1 1.5 2 2.5
Length of study (years)
Sco
re
*
*
**
**
FIGURE 9.5 Total BPH symptom score improvement with alfuzosin: maintenance of symptomatic efficacy in the longterm. Part 1: 6-month placebo-controlled study (circle; n = 251); part 2: 1-year open extension (triangle; n = 131); part 3:1-year (additional) open extension (square; n = 50). *p < 0.05 vs baseline. (Data from refs 29, 42, and 43 with permission.)
Ch 09 13/5/05 3:35 pm Page 127

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA128
+2.3 (3.6) ml/s and +1.6 (3.2) ml/s, respectively;p = 0.03), demonstrating the therapeutic coverageover a 24-hour period.
In a 9-month, non-blinded extension of thisstudy, the long-term efficacy of 10 mg od alfu-zosin was assessed over 12 months.45 In total, 311of the original 436 patients took part in the exten-sion phase. At the start of the extension phase,mean I-PSS was 10.9 and did not change over thesubsequent 9 months, with mean I-PSS 9.3 at
endpoint. Significant improvements wereobserved in patients who had originally receivedplacebo as part of the double-blind study(p = 0.0001). Peak flow, which was 11.5 ml/s atmonth 3, remained at its improved rate at month12 (p = 0.0001 compared to baseline).
In addition, the 10 mg od formulation hasbeen compared to 15 mg od over 3 months.46 Asin the ALFORTI study, the ALFUS studyincluded a wash-out period of 1 month before
TABLE 9.5 Symptomatic improvement after 3 months of treatment with the once daily formulation of alfuzosin (10 mgod): comparison with immediate release (IR) alfuzosin and placebo.44
*Intergroup comparison; †mean (SD). Data from van Kerrebroeck et al.44
Alfuzozin AlfuzosinPlacebo 10 mg od 2.5 mg tid(n = 154) (n = 143) (n = 150) p*
I-PSS scoreBaseline† 17.7 (4.1) 17.3 (3.5) 16.8 (3.7) 0.13Change vs. baseline† –4.9 (5.9) –6.9 (4.9) –6.4 (5.6) 0.005% of patients with a 26 37 42clearance of at least 50%
Quality of life indexBaseline† 3.3 (1.0) 3.3 (1.0) 3.3 (0.9) 0.96Change vs. baseline† –0.6 (1.2) –0.1 (1.1) –1.1 (1.1) 0.002
TABLE 9.4 Lower urinary tract symptoms (LUTS) and peak urinary flow (Qmax) improvement in patients with baselineQmax ≤ 12 ml/s and I-PSS ≥13*
*Adapted from Buzelin et al.30; †intergroup comparison; ‡mean (SD). SR, slow release.
Parameter SR alfuzosin 10 mg/day Placebo p†
I-PSS score‡ n = 104 n = 110Baseline 17.8 (3.9) 18.3 (4.1)Final 11.2 (6.5) 14.4 (6.5)Change vs baseline –6.7 (–36%) –4.0 (–22%) 0.002
Qmax (ml/s)‡ n = 91 n = 91Baseline 9.3 (2.1) 8.9 (2.2)Final 12.5 (5.1) 10.1 (3.8)Change vs baseline +3.2 (+39%) +1.1 (+16%) 0.0006
% Patients with Qmax change >30% 53 26
Ch 09 13/5/05 3:35 pm Page 128

ALFUZOSIN 129
treatment with nontitrated alfuzosin or placebo.I-PSS, uroflowmetry, and quality of life wereassessed at baseline and then regularly through-out the studies. The men who took part in thetrial were aged 50 or over, had a history of LUTSsuggestive of BPH, an I-PSS of 13 or greater, apeak flow of 5–12 ml/s, a voided volume of150 ml or greater, and a PVR volume of 350 ml orless.
Patients were stratified in each study accord-ing to whether they were < 65 or ≥65 and alsoaccording to blood pressure (< 90 or ≥90 mmHg).The primary efficacy outcome was mean changein I-PSS.
The 3-month trial indicated that 15 mg odalfuzosin and 10 mg od both improved I-PSS sig-nificantly compared to placebo.46 In the ALFUSstudy, endpoint I-PSS scores improved frombaseline by 3.6 points in the 10 mg od group and3.4 points in the 15 mg od group (p = 0.001 and0.004, respectively). As in the ALFORTI study,improvements were observed in the I-PSS fillingand voiding subscores.
Peak urinary flow increased by 1.7 ml/s (17%,p = 0.0004) in the 10 mg od group and by 0.9 ml/s(10%) in the 15 mg od group.
Quality of life is now becoming accepted as animportant criterion in the evaluation of treat-ments for BPH.47 Results from a study involvingover 7000 outpatients treated with alfuzosin for 3months in general practice showed quality of lifescores to improve by 43% and to correlate signifi-cantly with symptom scores.48 These sympto-matic and quality of life improvements weremaintained in those patients who continued thetreatment for 2 years (> 4500)49 and 3 years(> 3200).50 In this population, the rate of sponta-neous AUR and of prostate surgery was low,respectively 0.3% and 3.7%,50 confirming the ben-
eficial effect of alfuzosin on the risk of AURdemonstrated in the medium term.29
In the ALFUS and ALFORTI trials,44,46 qual-ity of life scores were significantly better in theactive treatment groups compared to placebo. Inthe ALFORTI trial, the quality of life index fellby 33%, 30%, and 18% in the 10 mg od, 2.5 mgtid, and placebo groups, respectively44 (p = 0.0008and 0.005 for the active groups vs placebo, respec-tively). In the ALFUS study, quality of life indeximproved by 18% in both active groups comparedto 8% with placebo (p = 0.002 vs placebo). Theextension of the ALFORTI trial45 saw animprovement from 2.3 at month 3 to 2.1 at end-point (35% improvement from baseline).
The potential additive benefit of combiningthe α1-blocker alfuzosin and the 5α1-reductaseinhibitor finasteride was assessed in a European,randomized double-blind, multicenter trialwhich involved 1051 patients with lower urinarytract symptoms associated with BPH.26 Patients(n = 358) received SR alfuzosin 5 mg twice dailywithout dose titration, finasteride (n = 344) 5 mgonce daily, or both drugs (n = 349) for 6 months.Symptomatic improvement was significantlyhigher from the first month of treatment with SRalfuzosin, alone or in combination; mean changesin I-PSS versus baseline at endpoint were –6.3and –6.1, respectively, compared with –5.2 withfinasteride alone (SR alfuzosin vs finasteride,p = 0.01; combination vs finasteride p = 0.03).More than 40% of patients who received alfu-zosin alone or in combination with finasteridehad a 50% reduction of their urinary symptoms(Figure 9.6). In the overall population, increasesin Qmax were greater with SR alfuzosin and thecombination compared with finasteride aloneafter 1 month of therapy, but changes at endpointwere similar in the three treatment groups. Inthose 47% of patients likely to be obstructed
Ch 09 13/5/05 3:35 pm Page 129

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA130
(baseline Qmax <10 ml/s), however, mean increas-es in Qmax were significantly higher with SR alfu-zosin, alone or in combination, whatever the visit.Thus, in this 6-month trial, SR alfuzosin wasmore effective than finasteride, with no addition-al benefit in combining both groups.
As described above, in symptomatic BPHpatients, alfuzosin reduces the residual urine vol-ume and in the medium term the incidence ofAUR.29 This beneficial effect on bladder empty-ing is also confirmed by the low rate of AURobserved in long-term treatment. Moreover, alfu-zosin has also been demonstrated to be useful inthe management of AUR. Alfuzosin (5 mg bid)administered for 2 consecutive days in patients
suffering from AUR secondary to BPH signifi-cantly increased the chance of voiding afterremoval of the catheter in comparison with place-bo.51 These results were confirmed at the comple-tion of the study: 22 out of 40 (55%) of patientstreated with alfuzosin voided successfully incomparison with 12 out of 41 (29%) who receivedthe placebo.52
Overall, alfuzosin has been found to producesymptomatic improvement in patients sufferingfrom moderate BPH, i.e. a 25% improvement intwo-thirds of treated patients and a 50% improve-ment in one-third, with a favorable impact onquality of life. The increase in flow rate was 30%,and residual urine volume may be decreased by
6 weeks 3 months 6 months 6 weeks 3 months 6 months
Length of study
Pe
rce
nta
ge
of p
atie
nts
im
pro
ve
d
75
70
65
60
55
50
45
40
Alfuzosin Placebo
FIGURE 9.6 Maintenance in the long term (up to 6 months) of at least 25% improvement in BPH symptoms (circles,obstructive scores; squares, irritative scores; triangles, total scores) in patients given alfuzosin or placebo.
Ch 09 13/5/05 3:35 pm Page 130

ALFUZOSIN 131
40%. The relief is prompt, more pronounced thanwith finasteride, and can be maintained over 3years. In the medium term, alfuzosin reduced theincidence of AUR and, in long-term treatment, itis associated with a low incidence of AUR andprostate surgery.
Side-effects and tolerance
Oral IR alfuzosin (7.5–10 mg/day) is generallywell tolerated in clinical studies of up to 30months’ duration.29,42,43 The overall incidence ofside-effects with alfuzosin appears to be similar tothat seen with placebo, and the incidence of pos-tural side-effects potentially related to the phar-macodynamic properties of alfuzosin appears tobe lower than that with prazosin (up to 2 mg bid)and similar to that observed with the SR formu-lation of tamsulosin 0.4 mg od. Reported adverseeffects with alfuzosin are usually transitory: themajority occur within the first 4 weeks of treat-ment and resolve spontaneously after drug with-drawal. Furthermore, both the SR and the od for-mulations of alfuzosin are at least as well tolerat-ed as the immediate formulation.
In the 6-month placebo-controlled study,29 theoverall incidence of adverse events was similar inalfuzosin-treated patients (36%) and in the place-bo group (36%), with a similar rate of drop-outfor adverse events (10 and 9%, respectively). Inaddition, the number of patients reporting at leastone vasodilatation-related adverse effect was alsosimilar in alfuzosin and placebo groups (11 and10%, respectively). A lower incidence of impo-tence with alfuzosin (< 1%) compared with place-bo (3%) may reflect the beneficial effect of α1-adrenoceptor antagonists in this condition (Table9.6). Alfuzosin appears to be well tolerated in thelong term,42,43 which is of particular interestbecause BPH patients are likely to require long-term treatment.
In support of these data were the results of anoncomparative, nonblinded, multicenter post-marketing general practice survey, involving over13 000 evaluable BPH patients who received alfu-zosin 2.5 mg three times daily for 3 months. Thisstudy showed that the overall discontinuationrate was low (3.7%) and that two-thirds ofpatients’ withdrawals due to side-effects werecaused by vasodilatation-related adverse events:vertigo/dizziness (1.4%), malaise (0.6%), posturalhypotension (0.6%), and headache (0.4%). Most ofthese side-effects occurred during the first weekof treatment and in fewer than 0.3% of patientsafter the first dose.53 As expected, postural side-effects were more common in the elderly and inpatients receiving concomitant antihypertensivetreatment. In this survey, which was extended upto 3 years, the incidence of side-effects leading to
TABLE 9.6 Adverse effects reported by patients withbenign prostatic hyperplasia during 6 months’ treatmentwith alfuzosin 7.5–10 mg/day (n = 251) or placebo(n = 267). (Adapted from Jardin et al.29)
Adverse Alfuzosin Placeboeffect recipients (%) recipients (%)
Vasodilatoryadverse effects
Dizziness 7.2 5.2Headache 6.4 4.9Postural hypotension 1.9 1.2Drowsiness 1.6 < 1Tachycardia 1.6 < 1
Other adverse effectsSkin rash 4.4 5.2Dry mouth 4.4 2.6Diarrhea 2.8 < 1Nausea 2.4 < 1Vomiting 1.6 1.9Asthenia 2.0 3.8Chest pain 2.0 < 1Hypertension 1.6 2.3Bad taste < 1 3.4Impotence < 1 2.3
Ch 09 13/5/05 3:35 pm Page 131

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA132
drug discontinuation was 2.3% and 4.2% duringthe 1-year and 3-year survey, respectively.48–50,53
These figures confirm the good safety profile inlong-term administration. Alfuzosin was bettertolerated than prazosin in terms of posturalsymptoms in patients with BPH.33,34 The IR for-mulation of alfuzosin (2.5 mg tid) was as well tol-erated as the marketed formulation of tamsulosin(0.4 mg od) in a 12-week study conducted inBPH.31 Decreases in supine and standing bloodpressure were slightly greater in patients receiv-ing alfuzosin than with tamsulosin. However,these changes were not associated with anincreased incidence of side-effects, confirmingthat they were not clinically relevant. The num-ber of drop-outs for adverse events was twice aslow with alfuzosin than with tamsulosin (4% and8%, respectively). The incidence of posturalhypotension was low, i.e. 1% with alfuzosin and3% with tamsulosin.
The safety profile of SR alfuzosin was specifi-cally addressed in a pooled analysis of two place-bo-controlled studies involving 588 patients (292receiving SR alfuzosin 5 mg twice daily and 296 aplacebo).41 Fifty-one per cent of the patients were≥65 years of age and 43% had associated cardio-vascular disease including hypertension and/orwere receiving concomitant antihypertensivedrugs. SR alfuzosin administered without initialtitration was very well tolerated, with an overallincidence of adverse events similar to that ofplacebo (18.5% and 15.8% of patients, respective-ly) and an overall incidence of withdrawal fromtherapy for adverse events lower than that ofplacebo (3.4% and 5.7%, respectively). Adverseevents potentially related to vasodilatation wereinfrequent with SR alfuzosin (the same incidenceas with placebo, i.e. 2.7% of patients) and theseadverse events occurred mainly during the firstmonth of alfuzosin treatment.
The safety profile of SR alfuzosin was alsocompared to that of a standard dose of finasteride(5 mg od) and the combination of both drugs.32
The incidence of postural symptoms was notincreased in those patients who received alfuzosin(Table 9.7). Conversely, impotence and ejaculato-ry disorders were significantly more frequentwith finasteride, alone or in combination, thanwith alfuzosin alone. No ejaculatory disorderswere reported with alfuzosin monotherapy.
The safety profile of the od SR formulation ofalfuzosin assessed in the ALFORTI study wasalso very satisfactory. Alfuzosin od 10 mg wasadministered without dose titration. No first-dayeffect was observed. The incidence of adverseevents related to vasodilatation was low (dizzi-ness/vertigo 2.8%, headache 1.4%, malaise 1.4%,asymptomatic hypotension 0.7%). No case of syn-cope was recorded. In addition, no sexual dys-function was observed.44
An additional 3-month study showed similar-ly low rates of patient withdrawal and adverseevents.46 At least one serious adverse event wasexperienced by 4.5, 3.4, and 2.9% of the 10 mg,15 mg, and placebo groups, respectively, withpotentially drug-related negative effects reportedby 52, 43, and 43% of each group. Dizziness wasreported by 7.4% of patients in the active group.Again, clinically relevant blood-pressure orheart-rate changes did not occur. Althoughsupine systolic and diastolic blood pressure fell inthe active groups, levels did not differ significant-ly from the placebo groups (–1.1, 2.3, and2.7 mmHg and 0.8, 1.5, and 2.1 mmHg, respec-tively). Orthostatic hypotension rates were alsosimilar between active groups and placebo.Again, ejaculatory disorders did not occur.
In a 9-month extension of the 10 mg od for-mulation of alfuzosin, no specific events occurredthat were not observed during the 3-month
Ch 09 13/5/05 3:35 pm Page 132

ALFUZOSIN 133
double-blind phase.45 Discontinuation due toadverse effects occurred in 5.6% of patients;vasodilatory effects were reported by 4.4% ofpatients, but were not due to first-day or ageeffects. Hypertensive patients reported morevasodilatory-related effects. No clinically relevantchanges in systolic or diastolic blood pressureoccurred (–2.6 and –2.8 mmHg compared tobaseline, respectively). Nonclinically relevantorthostatic hypotension affected 2.8% of patientsand risk was low in patients with mild and mod-erate renal impairment. Only 0.6% of patientsreported ejaculatory disorders.
Apart from the intrinsic functional uroselec-tivity of alfuzosin, the low incidence of posturalevents observed with the new formulation ofalfuzosin could be related to its pharmacokineticproperties, i.e. delayed peak plasma concentra-tions due to both a slowing and a prolongation ofthe rate of release of the active drug. The lack of
CNS-related side-effects such as asthenia or som-nolence could also be related to its low brain bar-rier penetration. Overall, consistent with thegood tolerability of the drug, alfuzosin is not asso-ciated with impairment of sexual function.
PLACE OF ALFUZOSIN IN THERAPY
Although it is unlikely that a drug would abolishboth the static and dynamic components of BPHas effectively as surgery, pharmacologicapproaches to the symptomatic treatment of BPHhave attracted increasing interest and havebecome the mainstay of patient management. α1-Blockers such as alfuzosin54 and 5α-reductaseinhibitors55 are now considered first-line therapyfor BPH. 5α-Reductase inhibitors can reduce thesize of the prostate, but may take months to havesuch an effect and in the overall study population,
TABLE 9.7 Comparative safety profile of alfuzosin (slow release (SR) 5 mg twice daily), finasteride (5 mg once daily),and the combination of both drugs: incidence of adverse effects.
Data from Debruyne et al.32
Alfuzosin Finasteride Combination Intergroup(n = 358) (n = 344) (n = 349) p
Vasodilatory events (%)Vertigo/dizziness 1.7 1.2 2.3 NSHeadache 2.0 1.2 1.4 NSPostural hypotension/hypotension 0.6 0.9 0.6 NSMalaise 0.3 0.3 0.3 NS
Sexual disorders (%)Impotence 2.2 6.7 7.4 < 0.002Ejaculation failure 0.0 1.5 0.9 0.04Decreased libido 0.6 1.7 2.0 NS
Others (%)Somnolence 0.0 0.3 0.6 NSAsthenia/fatigue 1.1 0.6 0.0 NSMyocardial infarction 0.0 0.3 0.3 NSAcute urinary retention 0.6 0.3 0.3 NS
Ch 09 13/5/05 3:35 pm Page 133

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA134
the magnitude of benefit is relatively modest.55
The potential benefits of the combination ofalfuzosin and finasteride have yet to be demon-strated in the medium term.32
The potential clinical advantage of alfuzosinover some other α1-adrenoceptor antagonists isthat it selectively blocks contraction mediated byα1-adrenoceptors in the genitourinary tract com-pared to its action on receptors in the vasculature.Therefore, as described above, alfuzosin may beeffective in BPH at doses that produce minimaladverse effects related to vascular α1 blockade,especially postural symptoms. In addition, theincidence of CNS-related adverse events (i.e.asthenia, somnolence) is not markedly increasedwith alfuzosin compared to placebo and no dele-terious effects on sexual function have beenreported. With increased realization of theimportance of maintained sexual function inolder adults, this factor is likely to be of signifi-cant value to BPH patients. Both the SR and IRformulations of alfuzosin offer patient-friendlydaily dosings. These are convenient for the nor-mal routine of daily life, as once-a-day and twice-a-day regimens are associated with better compli-ance (73 and 70%, respectively) than are thrice-daily regimens (52%).56 There is new evidenceregarding the od formulation, indicating that it isas effective as SR and IR formulations, withfewer vasodilatory effects.44
The beneficial effect of alfuzosin as an adju-vant treatment of AUR is promising, as is thereported low incidence of AUR in patients treat-ed in the medium and long term with alfuzosin.Although the predictive criteria of those patientswith BPH who are likely to respond to α1-block-ers have not yet been identified, the α1-blockeralfuzosin is a first-line and safe agent in patientswith symptomatic BPH.
ACKNOWLEDGMENTS
The author would like to thank S. Arbilla, M. C.Delauche and D. Martin for their fruitful collab-oration in the writing of this chapter.
REFERENCES
1. Muramatsu I, Oshita M, Ohmura T et al.Pharmacological characterization of α1-adrenocep-tor subtypes in the human prostate: functional andbinding studies. Br J Urol 1994; 74: 572–578
2. Hieble J P, Caine M, Zalaznik E. In vitro charac-terization of the α-adrenoceptors in humanprostate. Eur J Pharmacol 1985; 107: 111–117
3. Michel M C, Büscher R, Kerker J et al. α-Adrenoceptor subtypes affinities of drugs for thetreatment of prostatic hypertrophy. Evidence forheterogeneity of chloroethylclonidine-resistant ratrenal α1-adrenoceptor. Naun Schmied ArchPharmacol 1993; 348: 385–395
4. Price D T, Schwinn D A, Lomasney J W et al.Identification, quantification and localization ofmRNA for three distinct alpha1 adrenergic sub-types in human prostate. J Urol 1993; 150: 546–551
5. Ford A P D W, Arredondo N F, Blue D R Jr et al.RS-17053 (N-[2-(2-cyclopropylmethoxyphenoxy)-ethyl]-5-chloro-α, α-dimethyl-1H-indole-3-ethan-amine hydrochloride), a selective α1A-adrenoceptorantagonist, displays low affinity for functional α1-adrenoceptors in human prostate: implications foradrenoceptor classification. Eur J Pharmacol 1996;49: 209–215
6. Forray C, Bard J A, Wetzel J M et al. The alpha1-adrenergic receptor that mediates smooth musclecontraction in human prostate has the pharmaco-logical properties of the cloned alpha1c subtype. MolPharmacol 1994; 45: 703–708
7. Kenny B A, Miller A M, Williamson I J R et al.Evaluation of the pharmacological selectivity pro-file of α1-adrenoceptors: binding, functional and invivo studies. Br J Pharmacol 1996; 118: 871–878
Ch 09 13/5/05 3:35 pm Page 134

ALFUZOSIN 135
8. Van Der Graaf P H, Deplanne V, Duquenne C etal. The α1A-adrenoceptor is not involved inphenylephrine-mediated contractions of rabbit iso-lated prostate. Eur Urol 1996; 30/52: 51
9. Foray C, Noble S A. Subtype selective α1-adreno-ceptor antagonists for the treatment of benign pro-static hyperplasia. Expert Opin Invest Drugs 1999;8: 2073–2094
10. Debruyne F M J. Alpha-blockers: are all createdequal? Urology 2000; 56 (Suppl 5A): 20–22
11. Pimoule C, Shoemaker H, Jardin A, Langer S Z.Identification and characterization of high affinity[3H]-prazosin binding to the α-adrenoceptor in thehuman prostatic adenoma. Fund Clin Pharmacol1988; 3: 446(abstract)
12. Lefevre-Borg F, O’Connor S E, Schoemaker H etal. Alfuzosin, a selective α1-adrenoceptor antago-nist in the lower urinary tract. Br J Pharmacol1993; 109: 1282–1289
13. Benavides J, Peny B, Scatton B. Autoradiographicdistribution of alfuzosin sensitive α1-adrenoceptorsin normal and hyperplasic human prostate. In:Proceedings of the 22nd congress of theInternational Society of Urology, Sevilla, Spain,1991: abstract 487
14. Faure C, Pimoule C, Vallencien G et al.Identification of α1-adrenoceptor subtypes presentin the human prostate. Life Sci 1994; 54: 1595–1605
15. Lefevre-Borg F, Lechaire J, O’Connor S E. In vivouroselectivity of alfuzosin compared to prazosinand terazosin. Br J Pharmacol 1992; 106: 84P
16. Martin D, Jammes D, Angel I. Effects of alfuzosinon urethral and blood pressures in conscious malerate. Life Sci 1995; 57: 387–391
17. Martin D J, Lluel P, Guillot E et al. Comparativeα1-adrenoceptor subtype selectivity and functionaluroselectivity of α1-adrenoceptor antagonists. JPharmacol Exp Ther 1997; 282: 228–235
18. Martin D J, Lluel P, Pouyet T et al. Relationshipbetween the effects of alfuzosin on rat urethral andblood pressures and its tissue concentrations. LifeSci 1998; 63: 169–176
19. Mottet N, Bressolle F, Costa P et al. Orally admin-istered alfuzosin (ALF) has a high prostatic diffu-
sion in benign prostatic hyperplasia tissue(abstract). J Urol 2000; 163 (Suppl 4): 305–306
20. Rauch C, Ahtoy P, Pinquier L et al. Bioequivalenceof a new once-a-day controlled-release alfuzosinformulation with the immediate-release alfuzosin[abstract]. Eur J Urol 2000; 37 (Suppl 2): 119
21. Rauch C, Andre F, Thenot J -P et al.Bioequivalence study of a new once-a-day con-trolled-release alfuzosin formulation with the 5 mgtwice daily formulation [abstract]. J Urol 2000; 163(Suppl): 306
22. Pinquier J L, Fuder H, Amersdorffer J et al. Safetyand pharmacokinetics of alfuzosin 10 mg oncedaily formulation comparatively to standard for-mulation (2.5 mg tid) in elderly subjects (abstract).Clin Pharmacol Ther 1999; 65: 202
23. Pinquier J L, Rauch-Desanti C, Miller R P et al.Effect of renal impairment on the pharmacokinet-ics and safety of alfuzosin 10 mg OK formulation(abstract). Clin Pharmacol Ther 2000; 67: 111
24. Perrigot M, Delauche–Cavallier M C, Amarenco Aet al. Effect of intravenous alfuzosin on urethralpressure in patients with neurogenic bladder dis-ease. Neurol Urodyn 1996; 15: 119–131
25. Cramer P, Neveux E, Regnier F et al. Bladder-neckopening test in spiral cord injury patients using anew I.V. alpha-blocking agent, alfuzosin.Paraplegia 1989; 27: 119–124
26. Delauche-Cavallier M C, Richard M, Buzelin J Met al. Alpha-blocker therapy with alfuzosin inneurogenic bladder disease. Neurol Urodyn 1993;12: 24A(abstract)
27. Teillac P, Delauche-Cavallier M C, Attali P and theDualf Group. Urinary flow assessment after a sin-gle oral administration of alfuzosin, a new alpha-blocker, in patients with benign prostatic hypertro-phy. Br J Urol 1992; 70: 58–64
28. Hansen B J, Nordling J, Mensik H J A et al. andthe Alfech study group. Alfuzosin in the treatmentof benign prostatic hyperplasia: effects on symptomscores, urinary flow-rates and residual volume. Amulticentre, double-blind placebo-controlled trial.Scand J Urol Nephrol 1994; (Suppl 157): 169–176
Ch 09 13/5/05 3:35 pm Page 135

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA136
29. Jardin A, Bensadoun H, Delauche-Cavallier M C,Attali and the BPH-ALF Group. Alfuzosin fortreatment of benign prostatic hypertrophy. Lancet1991; 337: 1457–1461
30. Buzelin J M, Roth S, Geffriaud-Ricouard C,Delauche-Cavallier M C and the ALGEBI StudyGroup. Efficacy and safety of sustained-releasealfuzosin 5 mg in patients with benign prostatichyperplasia. Eur Urol 1997; 31: 190–198
31. Buzelin J M, Fonteyne E, Kontturi M et al.Comparison of tamsulosin with alfuzosin in thetreatment of patients with lower urinary tractsymptoms suggestive of bladder outlet obstruction(symptomatic benign prostatic hyperplasia). Br JUrol 1997; 80: 597–605
32. Debruyne F M K, Jardin A, Colloi D et al. SR-alfu-zosin, finasteride and the combination of both inthe treatment of benign prostatic hyperplasia. EurUrol 1998; 34: 169–175
33. Buzelin J M, Hebert M, Blondin P and thePRAZALF Group. Alpha-blocking treatmentwith alfuzosin in symptomatic benign prostatichyperplasia: comparative study with prazosin. Br JUrol 1993; 72: 922–927
34. Stephenson T P, Jensen R D and the PRANALFGroup. A placebo-controlled study of the efficacyand tolerability of alfuzosin and prazosin, for thetreatment of benign prostatic hypertrophy (BPH).Proceedings of the 11th Congress of the EuropeanAssociation of Urology, Berlin, Germany, 1994; 25:abstract 48
35. Birsch N E, Hurst G, Doyle P T. Serial residualurine volumes in men with prostatic hypertrophy.Br J Urol 1988; 62: 571–575
36. McNeill S A, Hargreave T B, Geffriaud-RicouardC et al. Postvoid residual urine in patients withlower urinary tract symptoms suggestive of benignprostatic hyperplasia: pooled analysis of eleven con-trolled studies with alfuzosin. Urology 2001; 57:459–465
37. Ramsay J W A, Scott G I, Whitfield H N. A dou-ble-blind controlled trial of a new α1 blocking drugin the treatment of bladder outflow obstruction. BrJ Urol 1985; 57: 657–659
38. Martorana G, Gilberti C, Di Silverio F et al. Effectsof short-term treatment with α1-blocker alfuzosinon urodynamic pressure/flow parameters inpatients with benign prostatic hyperplasia. EurUrol 1997; 32: 47–53
39. Eri L M, Tveter K J. α-Blockade in the treatmentof symptomatic benign prostatic hyperplasia. J Urol1995; 154: 923–934
40. Lipsitz L A. Orthostatic hypotension in the elderly.N Engl J Med 1989; 321: 952–956
41. Buzelin J M, Delauche-Cavallier M C, Roth S et al.Clinical uroselectivity: evidence from patientstreated with SR alfuzosin for symptomatic benignprostatic obstruction. Br J Urol 1997; 79: 898–906
42. Jardin A, Bensadoun H, Delauche-Cavallier M C,Attali P and the BPH-ALF Group. Long termtreatment of benign prostatic hypertrophy withalfuzosin: a 12–18 month assessment. Br J Urol1993; 72: 615–620
43. Jardin A, Bensadoun H, Delauche-Cavallier M Cet al. and the BPHALF Group. Long term treat-ment of benign prostatic hyperplasia alfuzosin: a24–30 month survey. Br J Urol 1994; 74: 579–584
44. van Kerrebroeck P, Jardin A, Laval KU et al.Efficacy and safety of a new prolonged release for-mulation of alfuzosin 10 mg once daily versus alfu-zosin 2.5 mg thrice daily and placebo in patientswith symptomatic benign prostatic hyperplasia.ALFORTI Study Group. Eur Urol 2000; 37:306–313
45. van Kerrebroeck P, Jardin A, van Cangh P et al.Long-term safety and efficacy of a once-daily for-mulation of alfuzosin 10 mg in patients with symp-tomatic benign prostatic hyperplasia: open labelextension study. Eur Urol 2002; 41: 54–61
46. Roehrborn G C. Efficacy and safety of once dailyalfuzosin in the treatment of lower urinary tractsymptoms and clinical benign prostatic hyperpla-sia: a randomized placebo-controlled trial. ALFUSStudy Group. Urology 2001; 58: 953–959
47. Fowler F J, Barry M J. Quality of life assessmentfor evaluating benign prostatic hyperplasia treat-ments. Eur Urol 1993; 24 (Suppl 1): 24–27
Ch 09 13/5/05 3:35 pm Page 136
ALFUZOSIN 137
48. Lukacs B, Leplège A, Thibault P, Jardin A.Prospective study in men with clinical benign pro-static hyperplasia treated with alfuzosin by generalpractitioners: 1-year results. Urology 1996; 48:731–740
49. Lukacs B, Comet D, Doublet D et al. Health relat-ed quality of life in benign prostatic hyperplasiapatients treated for 2 years with alfuzosin. JEpidemiol Bio 1997; 2: 203–211
50. Lukacs B, Grange J C, Comet B, McCarthy C andthe BPH group in General Practice. Three yearprospective study of 3228 BPH patients treatedwith alfuzosin in General Practice. Prostate CancerProstatic Dis 1998; 5: 276–283
51. McNeill S A, Donat R, Pillai M K et al.Prospective, multicentre randomized, placebo con-trolled, double-blind study of the effects of alfu-zosin on the outcome of trial removal of catheterfollowing acute urinary retention. J Urol 1998; 159:abstract 980
52. McNeill S A, Daruwala P D, Mitchell I D C et al.Sustained-release alfuzosin and trial withoutcatheter after acute urinary retention: a prospec-tive, placebo-controlled trial. BJU Int 1999; 84:622–627
53. Lukacs B, Blondin P, McCarthy C et al. Safety pro-file of 3 months’ therapy with alfuzosin in 13 389patients suffering from benign prostatic hypertro-phy. Eur Urol 1996; 29: 29–35
54. Wilde M J, Fitton A, McTavish D. Alfuzosin: areview of its pharmacodynamic and pharmacoki-netic properties and therapeutic potential in benignprostatic hyperplasia. Drugs 1993; 45: 410–429
55. Gormley G J, Stonnerr E, Bruskewitz R C et al.The effect of finasteride in men with benign pro-static hyperplasia. N Engl J Med 1992; 327:1185–1191
56. Greenberg R N. Overview of patient compliancewith medication dosing: a literature review. ClinTher 1986; 6: 592–599
Ch 09 13/5/05 3:35 pm Page 137

Ch 09 13/5/05 3:35 pm Page 138

TamsulosinC R Chapple
10
INTRODUCTION
Introduction to α1-adrenoceptor antagonists
α1-Adrenoceptor antagonists were originallydeveloped for the treatment of hypertension.Blockade of postsynaptic α1-adrenoceptors in theblood vessels by these agents results in vasodilata-tion. As a consequence, the peripheral vascularresistance and blood pressure are reduced.Examples of α1-adrenoceptor antagonists thathave been developed for and/or are still used forthe treatment of hypertension are alfuzosin, dox-azosin, prazosin, and terazosin.
In 1976, Caine et al. proposed a hypothesis forthe use of α1-adrenoceptor antagonists in lowerurinary tract symptoms (LUTS) suggestive ofbenign prostatic obstruction (BPO), also referredto as symptomatic benign prostatic hyperplasia(BPH).1 By inhibiting the effect of noradrena-line—the neurotransmitter of the sympatheticnervous system—at α1-adrenoceptors in the blad-der neck, prostatic urethra, and prostate capsuleand stroma, α1-adrenoceptor antagonists reducethe dynamic component of BPH.1–3 Today, α1-adrenoceptor antagonists are one of the mostwidely used medical therapies for this condi-tion.3–5 They improve symptoms and urinaryflow quickly (within a few weeks) and have afavorable clinical response in about 70% ofpatients. Total symptom score is in generalimproved by 30–40% and maximum urinary flowrate (Qmax) is increased by 16–25%.3–4
The 5α-reductase inhibitor (5αRI) finasterideis another medical treatment option for LUTS
suggestive of BPH accepted by the 4th and 5thInternational Consultations on BPH.6,7 It reducesthe prostatic mass and therefore the mechanicalor static component of BPH. Several direct com-parative studies between α1-adrenoceptor antag-onists and finasteride have been published or pre-sented.8–10 The initial trial demonstrated superiorefficacy of α1-adrenoceptor antagonists overfinasteride in terms of improvement in BPHsymptoms and peak flows. More recently, theMTOPS study has demonstrated greater efficacyfor a combination of α1-adrenoceptor antagonist+ 5αRI, although the extrapolation of these find-ings to clinical practice still remains the subject ofdebate11. Comparison of an alternative 5αRI,dutasteride, to α1-adrenoceptor suggests thatthere are no major therapeutic differences.
There is evidence that the efficacy of α1-adrenoceptor antagonists is independent ofprostate size at baseline.12 Finasteride in contrastacross the whole spectrum of patients has modestefficacy compared with placebo and is most effec-tive in patients with an enlarged prostate(> 40 g).6,13
Finally, α1-adrenoceptor antagonists workmuch faster (within a few weeks) than finasteride(up to 6 months) and, in contrast to 5αRIs are notassociated with erectile dysfunction or loss in sex-ual interest and do not reduce prostate-specificantigen (PSA).14 These facts together will rein-force the use of α1-adrenoceptor antagonists asfirst-choice medical therapy for LUTS suggestiveof BPH. The most important drawback of theclassical α1-adrenoceptor antagonists remains,
139
Ch 10 13/5/05 3:36 pm Page 139

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA140
however, adverse events attributed to the bloodpressure-lowering potential such as dizziness,orthostatic hypotension, and syncope. In addition,in order to reduce the occurrence of the first doseeffect (i.e. excessive blood pressure reduction withsubsequent symptomatic orthostatic hypoten-sion), they are recommended to be initiated at alow, subtherapeutic dose with gradual titration tothe optimal therapeutic dose.
Introduction to tamsulosin
Tamsulosin hydrochloride (YM-617) has beenspecifically developed by the YamanouchiPharmaceutical Company for the treatment ofLUTS suggestive of BPH. The chemical struc-ture of tamsulosin, a methoxybenzenesulfon-amide, differs from that of the other clinicallyavailable short-acting (alfuzosin and prazosin)and long-acting (doxazosin and terazosin) α1-adrenoceptor antagonists which are quinazolinederivatives.15 This may have consequences fordrug–receptor interaction.
In the late 1980s and the 1990s, it became clearthat part from α1- and α2-adrenoceptors, thereexist several subtypes of the α1-adrenoceptor. TheInternational Union of Pharmacology(IUPHAR) has accepted the existence of three α1-adrenoceptor subtypes (with high affinity for pra-zosin): α1A, α1B, and α1D, (quoted in lower casewhen referring to the cloned entities).16 Anotherα1-adrenoceptor subtype has been describedpharmacologically, which is a low-affinity pra-zosin adrenoceptor, termed α1L.12 Although themolecular identify of this fourth α1-adrenoceptorsubtype is not fully established, recent evidencesuggests that the α1L subtype may represent a par-ticular conformational state of the α1-adrenocep-tor.17 It has been demonstrated that the α1A andα1L-adrenoceptor subtypes are the predominantfunctional α1-adrenoceptors in the human
prostate.17–22 Research indicates that α1-adreno-ceptors in the human detrusor are of the α1D andto a lesser extent of the α1A subtypes and it hasbeen suggested that inhibition of these subtypesleads to improvement of irritative symptoms byα1-adrenoceptor antagonists.23 It is not completeclear which subtype is involved in blood pressureregulation in humans, since receptor binding andmolecular biological techniques do not provideconsistent data on this matter.24–26 However, clin-ical pharmacology studies with doxazosin, tera-zosin, and tamsulosin suggest that α1B-adreno-ceptors are more prominently involved in vaso-constriction than α1-adrenoceptors.27,28
At present, tamsulosin is the only clinicallyavailable α1-adrenoceptor antagonist that dis-plays selectivity for α1A- and, to a slightly lesserextent, α1D, over α1B-adrenoceptors.29–31 In addi-tion, tamsulosin has 12 times greater affinity forα1-adrenoceptors in the human prostate than inthe aorta in contrast to prazosin which has simi-lar affinity for those in the prostate and aorta.32
This can be referred to as receptor pharmacolog-ic uroselectivity.33 Other available α1-adrenocep-tor antagonists (alfuzosin, doxazosin, prazosin,and terazosin) do not display selectivity for any ofthe α1-adrenoceptor subtypes.29–31
Tamsulosin hydrochloride is available world-wide as a modified-release formulation. Due tothe long half-life (about 10–13 hours in elderlysubjects), tamsulosin can be classified as a long-acting α1-adrenoceptor antagonist that can betaken once daily (after a meal). In Japan it wasintroduced by Yamanouchi in 1993 under thetradename Harnal®. In Europe it was first intro-duced in The Netherlands in 1995 and has sincebeen marketed in most countries by YamanouchiEurope (tradenames Omnic®, Omic®, Omix®,and Flomax®) and/or Boehringer Ingelheim(Alna®, Pradif®, Josir®, or Urolosin®).
Ch 10 13/5/05 3:36 pm Page 140

TAMSULOSIN 141
Tamsulosin is also available in many LatinAmerican countries (Flomax® and Secotex®) andwas approved by the FDA in the US in 1997(Flomax®).
PHYSIOLOGIC UROSELECTIVITY
Physiologically, an α1-adrenoceptor antagonistcan be considered uroselective if it inhibits to alesser extent than other α1-adrenoceptor antago-nists the α1-adrenoceptors in the vascular system.Considerable species differences for tissue distri-bution and functionality of α1-adrenoceptor sub-types exist. Therefore, α1-adrenoceptor antago-nists can only be differentiated from a physiolog-ic uroselectivity point of view based on resultsobtained in human beings.
Two such experimental studies have been per-formed with tamsulosin and a hemodynamicallyactive α1-adrenoceptor antagonist to evaluate theinhibition of phenylephrine or cold-inducedvasoconstriction.27,28 One placebo-controlled trialcompared a single dose of tamsulosin (modified-release formulation) 0.2 mg and doxazosin 1 mgin eight Japanese healthy subjects in a cross-overdesign.27 The other placebo-controlled trial com-pared equi-effective single doses of tamsulosin(modified release) 0.4 mg with terazosin 5 mg inten healthy Caucasian volunteers in a cross-oversetting.28 Figure 10.1a shows that the number ofpatients who had an increase in diastolic bloodpressure of 7.6 mmHg after phenylephrine infu-sion was reduced to a lesser extent in tamsulosin-treated than in terazosin-treated patients. Inaddition, the inhibition of phenylephrine-induced increases in diastolic blood pressure rela-tive to placebo was less with tamsulosin than ter-azosin (Figure 10.1b).
There is evidence from in vivo studies inhuman volunteers that tamsulosin causes lessinhibition of vasoconstriction and therefore haslower affinity for vascular α1-adrenoceptors thandoxazosin and terazosin.27,28
CLINICAL UROSELECTIVITY
Clinical uroselectivity has been defined as‘desired effects on obstruction and LUTS relatedto adverse events’ in patients with LUTS sugges-tive of BPH.33 This implies that the α1-adreno-ceptor antagonist should have at least comparableefficacy to other α1-adrenoceptor antagonistswith an improved side-effect profile (i.e. lowerpotential to induce excessive blood pressurereductions with subsequent dizziness, sympto-matic orthostatic hypotension, and syncope).
Japanese clinical placebo-controlled data
A randomized, double-blind, placebo-controlled,parallel-group, phase II, dose-ranging study wasperformed in 270 Japanese patients with LUTSsuggestive of BPH, using 0.1, 0.2, or 0.4 mg tam-sulosin once daily for 4 weeks, after a 2-weekplacebo run-in period.34
The Qmax for the placebo, 0.2 mg, and 0.4 mggroups improved by 1.4 ml/s (15%), 4.0 ml/s(44%), and 3.6 ml/s (35%), respectively (nonsignif-icant vs placebo; Table 10.1). With respect to aver-age urinary flow rate (Qave), there were statistical-ly significant differences between 0.2 and 0.4 mgtamsulosin once daily (increases of 26% and 41%,respectively) and placebo (decrease of 4%). Inaddition, global subjective improvement was sim-ilar in the 0.2 mg and the 0.4 mg dosing groupsand significantly better in comparison with place-bo (p < 0.01). Approximately 80% of patients
Ch 10 13/5/05 3:36 pm Page 141

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA142
reported that their condition had (slightly, mod-
erately, or markedly) improved.
Tamsulosin was very well tolerated. Neither
orthostatic hypotension nor a significant decrease
in blood pressure were observed.
In conclusion, both 0.2 and 0.4 mg tamsulosin
once daily are effective and well-tolerated
dosages in the treatment of Japanese patients with
LUTS suggestive of BPH. Tamsulosin 0.2 mg isthe recommended dose in Japan.
European clinical placebo-controlled data
A randomized, double-blind, placebo-controlled,parallel group, phase II dose-ranging study wasperformed in the UK.35 After a 3-week placeborun-in period, 126 patients with LUTS due to
����������� ��
�����������
�
��
�
��
��
���
�� � � � � �� ����
�������
���
���
��
���
���
�� ��
�!
�"
#�$�
��$
%&
��
����
���
���
�'�
�(
����
��
)) )
)) )
������������������ �������������
�
�
�
�
��
*��
���
�!�
��(�
$��
�
�� � � � � �� ����
�������
���
FIGURE 10.1 (a) Number of responders (increase diastolic blood pressure (DBP) > 7.6 mmHg) during treatment withplacebo, tamsulosin, or terazosin and (b) percentage inhibition of phenylephrine (PE)-induced increase in diastolic bloodpressure during treatment with tamsulosin or terazosin relative to placebo.28 *p < 0.05.
Ch 10 13/5/05 3:36 pm Page 142

TAMSULOSIN 143
BPH (Qmax < 15 ml/s for a voided volume> 100 ml; urethral resistance: detrusor pressure(Pdet) at Qmax (PdetQmax)/Qmax
2 ≥ 0.5) were ran-domized to placebo or tamsulosin (0.2, 0.4, or0.6 mg) once daily for 4 weeks. Efficacy was eval-uated by free-flow and pressure–flow parametersand by a modified Boyarsky symptom score(eight symptoms to be rated from 0 to 5; totalscore range 0–40).
Table 10.1 and Figure 10.2a show that boththe 0.4 and 0.6 mg dose increased mean Qmax
(2.2 ml/s or 22.6% and 1.8 ml/s or 20.2%, respec-tively) statistically significantly compared withplacebo (–0.1 ml/s or –0.9%, p < 0.05). The 0.4 mgdose produced the greatest decrease in meanPdetQmax (–26.6 cmH2O or –28.2%) comparedwith an increase of 4.9 cmH2O (+5.7%) withplacebo (Figure 10.2b). The decrease in meantotal symptom score was comparable for the 0.4(–4.1 or –28.7%) and 0.6 mg dose (–4.4 or –28.2%)and was superior to the decrease in the placebogroup (–2.9 or –17.7%: Table 10.2 and Figure10.2c). The difference versus placebo did notreach statistical significance, probably due to thesmall sample size and the relatively short dura-tion of treatment (4 weeks). The percentage ofpatients who experienced slight or muchimprovement in their condition was also greatestin the 0.4 mg group (Figure 10.2d).
It can be concluded that optimal improve-ment in all efficacy parameters was achieved withthe 0.4 mg dose of tamsulosin. This dose was alsowell tolerated and did not induce statistically sig-nificantly greater blood pressure changes duringthe first 8 hours after the first dose. Therefore, the0.4 mg dose was further evaluated in phase IIIclinical trials in Europe.
Two multinational, multicenter, double-blind, randomized, placebo-controlled phase IIIstudies were performed in Europe. The Boyarsky
symptom score was used to assess the effect onLUTS (nine symptoms, each to be rated from 0 to3; total score range 0–27).36 Both studies enrolledmore than 300 patients with mild–moderateLUTS (total Boyarsky score > 6) suggestive ofBPH (free flow Qmax 4–12 ml/s for a voided vol-ume ≥120 ml). They were randomized to 12weeks of treatment with placebo or tamsulosin0.4 mg once daily in a 1 : 2 ratio (after a 2-weekplacebo run-in period).37 As the design, assess-ments, and results (Tables 10.1. and 10.2) of bothstudies were comparable, a meta-analysis thatinvolved 193 placebo and 381 tamsulosin patientswas carried out.38
Tamsulosin increased mean peak flow Qmax by1.6 ml/s (16%). Although there was a considerableplacebo-effect (0.6 ml/s or 6%), the difference wasstatistically significant (p = 0.002: see Table 10.1).The same applied for the percentage of patientswith a clinically significant improvement in Qmax
(defined as an increase from baseline of ≥ 30%)39:32% of tamsulosin- and 20% of placebo-treatedpatients (p = 0.003). Mean total Boyarsky symp-tom score was decreased to a statistically signifi-cant extent in the tamsulosin (–3.3 or –35.1%)versus the placebo group (–2.4 or –25.5%,p = 0.002). The same applied for the decrease intotal voiding (p = 0.008) and filling (p = 0.017)scores. A decrease in total Boyarsky symptomscore from baseline ≥ 25% was considered to be aclinically significant response.40 This wasachieved in 66% of patients in the tamsulosin and49% of patients in the placebo group (p < 0.001).
Tamsulosin has a fast onset of action. Theincrease in mean Qmax was already apparent andoptimal compared with placebo at the first assess-ment after 4 weeks of treatment with tamsulosin0.4 mg (Figure 10.3a). Although improvements intotal Boyarsky symptom score were apparent andsignificant over placebo at the first assessment at
Ch 10 13/5/05 3:36 pm Page 143

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA144
TABL
E 10
.1E
ffec
t of
plac
ebo
or ta
msu
losi
n on
mea
n fr
ee f
low
Qm
axin
pla
cebo
-con
trol
led
stud
ies
in J
apan
, Eur
ope,
and
the
US.
Tam
sulo
sin
Pla
cebo
Fir
st a
utho
rD
urat
ion
(wee
ks)
Dos
e (m
g)B
asel
ine
End
-poi
ntC
hang
eC
hang
e (%
)B
asel
ine
Cha
nge
Cha
nge
(%)
pV
alue
Kaw
abe34
40.
29.
113
.14.
044
9.4
1.4
15N
S0.
410
.414
.03.
635
NS
Abr
ams35
40.
29.
610
.71.
213
10.9
–0.1
–1N
S0.
49.
812
.12.
223
0.03
0.6
9.1
10.9
1.8
20N
S
Abr
ams37
120.
410
.712
.01.
413
10.4
0.4
40.
028
Cha
pple
3812
0.4
10.2
11.8
1.6
1610
.10.
66
0.00
2
Lep
or43
130.
49.
5—
1.8
189.
80.
55
< 0
.001
0.8
9.6
—1.
819
< 0
.001
Nar
ayan
4413
0.4
——
1.5
——
0.9
—0.
064
0.8
——
1.8
—0.
007
Lep
or46
530.
49.
5—
1.7
189.
90.
44
—0.
89.
5—
2.1
22
Ch 10 13/5/05 3:36 pm Page 144

TAMSULOSIN 145
4 weeks, the symptom score continued to improvefor the last 8 weeks of the trial when the effectwas (nearly) optimal (Figure 10.3b). At 4 weeks,about 70% of the total effect seen after 12 weekswas achieved.
Tamsulosin 0.4 mg was very well tolerated. Ithad minimal effects on blood pressure. In com-parison with placebo there were no clinically sig-nificant changes in supine or standing systolic ordiastolic blood pressure at end-point. Except forthe change in standing diastolic blood pressure(–2.5 mmHg), the differences were also not statis-tically significant (Table 10.3). Approximately20% of patients were hypertensive. In both the
normotensive and hypertensive subgroups, tam-sulosin 0.4 mg did not affect blood pressure to aclinically significantly greater extent than place-bo. The decrease in standing diastolic blood pres-sure in normotensive patients was statistically sig-nificantly greater than in the placebo group butthe reduction was minimal (–0.8 mmHg;p = 0.049: Table 10.4).
In addition, tamsulosin did not induce moreadverse events than placebo, be it treatmentemergent adverse events (36% vs 32%, p = 0.290)or possibly/probably drug-related adverse eventsaccording to the investigator (13% vs 12%,p = 0.802). The same applied for the percentage
�+
�����
�����
�����
���
���
���
���
���
��
�
�
��
������� ����� �� �� �����
���
,��
��
���
��
$� �
��-
���
.�/
�
����
���
���)
���)
��
�
�
�
�
������� ����� �� �� �����
)0 � �� �����1����!��� '�����(������
���
,��
�
����
���
��
�-��
�2��
������
��+ ���
���
���
���
���
���
���
��
�������� ����� �� �� �����
���
,��
(�
���
���
$��
����
��
� �
��1�
( ��
���
��
FIGURE 10.2 Effect of placebo or tamsulosin (0.2, 0.4, or 0.6 mg) once daily on (a) mean free flow Qmax, (b) meanPdetQmax, (c) mean total modified Boyarsky symptom score, and (d) percentage of patients who had slight or muchimprovement in their condition after 4 weeks of therapy in the phase II dose-ranging study in the UK.35
�� �� 3'�� ��� ��
��
�+
�+)
��
�
��
�+
��
�
��
�
��
��
���
�$�
���
��
���
�!(
� ��
�
���
���
����
� �1
��(�
�'�$
������� ����� �� �� �����
)0 � �� �����1����!��� '�����(������
Ch 10 13/5/05 3:36 pm Page 145

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA146
TABL
E 10
.2E
ffec
t of
plac
ebo
or ta
msu
losi
n on
mea
n to
tal s
ympt
om s
core
in p
lace
bo-c
ontr
olle
d st
udie
s in
Jap
an, E
urop
e, a
nd th
e U
S.
Tam
sulo
sin
Pla
cebo
Fir
st a
utho
rD
urat
ion
(sym
ptom
sco
re)
(wee
ks)
Dos
e (m
g)B
asel
ine
End
-poi
ntC
hang
eC
hang
e (%
)B
asel
ine
Cha
nge
Cha
nge
(%)
pV
alue
Abr
ams35
40.
216
.913
.6–3
.4–2
016
.7–2
.9–1
8N
S(m
odif
ied
0.4
14.9
10.2
–4.1
–29
NS
Boy
arsk
y)0.
615
.810
.9–4
.4–2
8N
S
Abr
ams37
120.
49.
56.
0–3
.4–3
69.
3–2
.2–2
40.
002
(Boy
arsk
y)
Cha
pple
3812
0.4
9.4
6.1
–3.3
–35
9.4
–2.4
–26
0.00
2(B
oyar
ksy)
Abr
ams42
120.
417
.7—
–8.8
–50
17.4
–4.7
–27
≤0.
01(I
-PSS
)
Lep
or43
130.
419
.8—
–8.3
–42
19.6
–5.5
–28
<0.
001
(I-P
SS)
0.8
19.9
—–9
.6–4
8<
0.00
1
Nar
ayan
4413
0.4
——
–5.1
——
–3.6
—0.
01(I
-PSS
)0.
8—
—–5
.8—
0.01
Lep
or46
530.
419
.7—
–9.4
–48
19.1
–6.5
–34
—0.
820
.0—
–9.7
–49
Ch 10 13/5/05 3:36 pm Page 146

TAMSULOSIN 147
of patients that discontinued due to adverseevents (4.5% vs 3.6%). Adverse events commonlyattributed to hemodynamically active α1-adreno-ceptor antagonists such as dizziness, orthostatichypotension, and syncope occurred at a compara-ble incidence in the tamsulosin and placebogroups (Table 10.5). This also applied for otheradverse events associated with α1-adrenoceptor
antagonists (asthenia, somnolence, rhinitis/nasalcongestion). The only adverse event that wasreported by significantly more tamsulosin thanplacebo patients was abnormal ejaculation (4.5%vs 1%, p = 0.045). This adverse event was, howev-er, very well tolerated by the patients, because fewtamsulosin patients (0.8%) withdrew from thestudy for this reason.38,41 Other sexual function-
������������������ ��
�
�
�
�
+
��
���
�� �
�&�1
���4
1�1
�(
���
����
� � ��
�����5��4��
0���!��� '��(������� ��� ���(�� �
������������������ ��
��
��
��
��
���
��
�-�
��2�
�
� � ��
�����5��4��
FIGURE 10.3 Effect of placebo or tamsulosin 0.4 mg once daily on (a) mean Qmax and (b) mean total Boyarsky symptomscore over time in the meta-analysis of the two European phase III placebo-controlled studies.38
Ch 10 13/5/05 3:36 pm Page 147

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA148
related adverse events (impotence and decreasedlibido) were reported to the same extent in thetamsulosin and placebo groups (Table 10.5).41
Another randomized, double-blind, placebo-controlled phase IV, 12-week study has been per-formed with tamsulosin 0.4 mg once daily inEuropean patients with LUTS (I-PSS ≥ 13) sug-gestive of BPH (Qmax < 12 ml/s): ESPIRIT(European Standardized Pressure FlowInvestigation Trial).42 In a subset of this trial(n = 193), the effects on pressure–flow parameterswere studied in particular. Tamsulosin producedstatistically significant decreases in PdetQmax
(–7.2 cmH2O or –10%) compared with placebo(+2.0 cmH2O or + 3%; p = 0.038: Table 10.6).Effects on pressure–flow Qmax and theAbrams–Griffiths (AG) number (PdetQmax – [2 ×Qmax]) were also significantly improved in thetamsulosin-treated compared with the placebo-
TABLE 10.3 Change in mean systolic and diastolic bloodpressure (SBP/DBP) at end-point with placebo or tamsu-losin 0.4 mg in meta-analysis of two European phase IIIplacebo-controlled studies: all patients.38
*p = 0.018 vs placebo.
Placebo Tamsulosin(n = 189) (n = 373)
Supine SBP (mmHg)Baseline 144.3 143.1Change –3.5 –3.1
Supine DBP (mmHg)Baseline 85.4 85.4Change –0.9 –1.6
Standing SBP (mmHg)Baseline 142.9 141.8Change –1.7 –3.3
Standing DBP (mmHg)Baseline 86.4 86.8Change –0.4 –2.5*
TABLE 10.4 Change in mean systolic and diastolic blood pressure (SBP/DBP) at end-point with placebo or tamsulosin0.4 mg in meta-analysis of two European phase III placebo-controlled studies: normotensive and hypertensive patients.38
*p = 0.049 vs placebo.
Normotension HypertensionPlacebo Tamsulosin Placebo Tamsulosin(n = 150) (n = 294) (n = 39) (n = 79)
Supine SBP (mmHg)Baseline 139.7 137.8 162.2 162.7Change –2.5 –2.0 –7.2 –7.2
Supine DBP (mmHg)Baseline 81.4 81.1 100.9 101.6Change +1.0 +0.4 –8.3 –9.1
Standing SBP (mmHg)Baseline 138.7 137.4 159.1 157.9Change –0.6 –2.5 –5.7 –6.3
Standing DBP (mmHg)Baseline 83.0 83.1 99.3 100.5Change +1.0 –0.8* –5.6 –8.7
Ch 10 13/5/05 3:36 pm Page 148

TAMSULOSIN 149
treated patients. The AG number was reduced by10.3 (–19%) on tamsulosin and increased by 1.2(2%) on placebo (p = 0.014). Clinical improve-ment in total I-PSS occurred within 1 week withcontinuing improvement up to 12 weeks(decrease 8.8 or –50% vs –4.7 (–27%) with place-bo; p ≤ 0.01).
It can be concluded that tamsulosin 0.4 mgonce daily is the optimal dose for European
patients with LUTS suggestion of BPH. It has arapid onset of action: Qmax is maximally increasedat the first assessment after 4 weeks and totalsymptom score within 1 week. It is extremelywell tolerated, even without the need for dosetitration. It has no clinically significant effect onblood pressure in normotensive or hypertensivepatients and no increased potential to inducesymptomatic orthostatic hypotension comparedwith placebo. Abnormal ejaculation is the onlyadverse event that occurs to a greater extent thanwith placebo.
US clinical placebo-controlled data
Two randomized, double-blind, placebo-con-trolled phase III short-term (13-week) studieswere performed in the US with tamsulosin0.4 mg or 0.8 mg once daily.43,44 The AmericanUrological Association (AUA) symptom index,which is identical to the International Prostate
TABLE 10.5 Incidence of adverse events (AEs) withplacebo or tamsulosin 0.4 mg in the meta-analysis of thetwo European placebo-controlled phase III studies.38,41
Values are numbers of patients with percentages in paren-theses.
*Possibly or probably drug-related according to the inves-tigator; †p = 0.045 vs placebo.
Placebo Tamsulosin(n = 193) (n = 381)
Any AE 61 (32) 137 (36)
Any drug-related* AE 24 (12) 50 (13)
Discontinued due toadverse events 7 (3.6) 17 (4.5)
Dizziness 6 (3.1) 13 (3.4)
Headache 4 (2.1) 8 (2.1)
Tachycardia/palpitation 3 (1.6) 5 (1.3)
Postural hypotension 1 (0.5) 0 (0)
Syncope 1 (0.5) 1 (0.3)
Asthenia 2 (1.0) 4 (1.0)
Somnolence 2 (1.0) 1 (0.3)
Rhinitis (nasal congestion) 1 (0.5) 1 (0.3)
Abnormal ejaculation 2 (1.0) 17 (4.5)†
Impotence 3 (1.6) 3 (0.8)
Libido decreased 0 (0) 4 (1.0)
Discontinued due to 1 (0.5) 3 (0.8)sexual function-relatedadverse events
TABLE 10.6 Effect on pressure–flow parameters andtotal I-PSS after 12 weeks of therapy with tamsulosin0.4 mg or placebo in the European ESPRIT study.42
n = 193 instead of 160 for total I-PSS. *p = 0.038;†p = 0.020; ‡p = 0.014; **p ≤ 0.01.
Placebo Tamsulosin(n = 54) (n = 106)
PdetQmax (cmH2O)Baseline 68.0 69.2Change (%) at 12 weeks 2.0 (3%) –7.2 (–10%)*
Pressure flow Qmax (ml/s)Baseline 6.4 7.1Change (%) at 12 weeks 0.4 (6%) 1.5 (21%)†
AG numberBaseline 55.2 55.1Change 1.2 (2%) –10.3 (–19%)‡
Total I-PSS scoreBaseline 17.4 17.7Change –4.7 (–27%) –8.8 (–50%)**
Ch 10 13/5/05 3:36 pm Page 149

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA150
Symptom Score (I-PSS), was used in these studiesto assess the effect on LUTS (seven symptoms,each to be rated from 0 to 5; total score range0–35).45 In each study, approximately 750 patientswith moderate–severe LUTS (total I-PSS ≥ 13) suggestive of BPH (Qmax 4–15 ml/s)were randomized to one of the three groups after
a placebo run-in of 4 weeks. There were four pri-mary efficacy parameters in each study (at end-point): (a) mean change in total I-PSS, (b) meanchange in Qmax, (c) number of symptom scoreresponders (decrease total I-PSS ≥ 25%), and (d)number of Qmax responders (increase Qmax ≥ 30%).
������������������������� ���������
0 �$1� 0 �$1��
��
�
��
��
���
�� �
��1�
( ��
���
���
��(�
$��
��6
�
)0���!��� '��(������
))
) )
������������������������� ���������
0 �$1� 0 �$1�
�
��
�
���
��
�-�
��(�
$��
��6
�
)0���!��� '��(������
)
)) )
FIGURE 10.4 Percentage of (a) Qmax responders and (b) total symptom score responders at end-point in the placebo andtamsulosin groups of two short-term US studies: study 143 and study 2.44
Ch 10 13/5/05 3:36 pm Page 150

TAMSULOSIN 151
In both studies, tamsulosin 0.4 mg and 0.8 mgonce daily were statistically significantly superiorto placebo (see Tables 10.1 and 10.2, and Figure10.4a and b). The only parameter that did notreach but approached statistical significance overplacebo in the 0.4 mg group (p = 0.064) was meanQmax (measured at through plasma concentration)
in one of the studies.40 Tamsulosin 0.4 mg and0.8 mg had comparable efficacy in both studies,only the change in total I-PSS at end-point wasgreater in the 0.8 mg than in the 0.4 mg group(p = 0.020). However, the difference between thetwo treatment groups was already partly appar-ent after 1 week of therapy when both the
������������������������� ���������
���
���
��
��
�
��
�
���
7��
��
� �
�3#�
00
�1�
( ��
���
��
� � � � � � � � + �� �� �� ��
�����5��4��
0���!��� '��(������� ��� ���(�� �!���� ��� �$�����
������������������������� ���������
�
�
�
�
���
7��
��
��
�-�
��2�
�
� � � � � � � � + �� �� �� ��
%���������5��4��
0���!��� '��(������� ��� ���(�� �!���� ��� �$�����
FIGURE 10.5 Effect of tamsulosin (0.4 or 0.8 mg) and placebo on (a) mean Qmax and (b) mean total I-PSS score over timein one of the US short-term studies.43
Ch 10 13/5/05 3:36 pm Page 151

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA152
patients in the 0.4 and 0.8 mg groups had received0.4 mg (Figure 10.5b). This shows that the greatereffect of the 0.8 mg dose with regard to change intotal I-PSS at end-point was probably caused by adifference in response between treatment/patientgroups and not by a difference in response to tam-sulosin dose.
Tamsulosin 0.4 mg had a very fast onset ofaction in both studies. In one of the studies, Qmax
was measured 4–8 hours after intake of the firstdose.43 At that time point, Qmax was already sig-nificantly and maximally increased comparedwith placebo (Figure 10.5a). In addition, the dif-ference in improvement in total I-PSS scorebetween tamsulosin and placebo was significantat the first assessment after 1 week (Figure10.5b).43,44 The symptom score continued toimprove up to 13 weeks when the optimal effecton LUTS was achieved. At week 1, approximate-ly 50% of the total reduction was observed.
Tamsulosin 0.4 mg and 0.8 mg had no clini-cally significant effects on blood pressure, eitherin normotensive or (controlled or uncontrolled)hypertensive patients. Multiple and rigorousorthostatic stress testing was performed at everyvisit in both studies. Despite this, the number ofpatients that developed symptomatic orthostatichypotension with tamsulosin 0.4 mg or 0.8 mg inboth studies was comparable to that with placebo:1 (0.2%), 2 (0.4%), and 0 (0%), respectively. Othersymptoms of orthostatic hypotension reportedduring the multiple and rigorous orthostaticstress tests (such as dizziness, lightheadedness,and faintness/syncope) were also included in theadverse events listing (Table 10.7). The onlyadverse event that was reported consistently andsignificantly more frequently with the 0.4 mgdose in both studies was abnormal ejaculation(6% and 11%) vs <1% with placebo. The occur-rence of this adverse event was dose-dependent as
TABLE 10.7 Incidence of adverse events with placebo, tamsulosin 0.4 mg or tamsulosin 0.8 mg in the two US placebo-controlled, short-term (13-week), phase III studies.39,40 Data in parentheses are percentages.
*Significant vs placebo; †significant vs 0.4 mg.
Study 139 Study 240
Placebo Tamsulosin 0.4 mg Tamsulosin 0.8 mg Placebo Tamsulosin 0.4 mgTamsulosin 0.8 mg(n = 254) (n = 254) (n = 248) (n = 239) (n = 248) (n = 244)
Any AE 151 (59) 165 (65) 180 (73) 181 (76) 194 (78) 188 (77)
Discontinued 22 (9) 18 (7) 31 (13) 20 (8) 22 (9) 30 (12)due to adverseevents
Dizziness 13 (5) 25 (10) 28 (11)* 37 (15) 50 (20) 56 (23)*
Orthostatic 0 (0) 1 (0.4) 2 (0.8) 0 (0) 0 (0) 0 (0)hypotension
Asthenia 5 (2) 12 (5) 13 (5) 22 (9) 27 (11) 29 (12)
Headache 46 (18) 48 (19) 45 (18) 53 (22) 49 (20) 59 (24)
Rhinitis 14 (6) 31 (12)* 37 (15)* 26 (11) 35 (14) 50 (20)*
Abnormal 0 (0) 15 (6)* 44 (18)*† 1 (< 1) 27 (11)* 45 (18) *†
ejaculation
Ch 10 13/5/05 3:36 pm Page 152
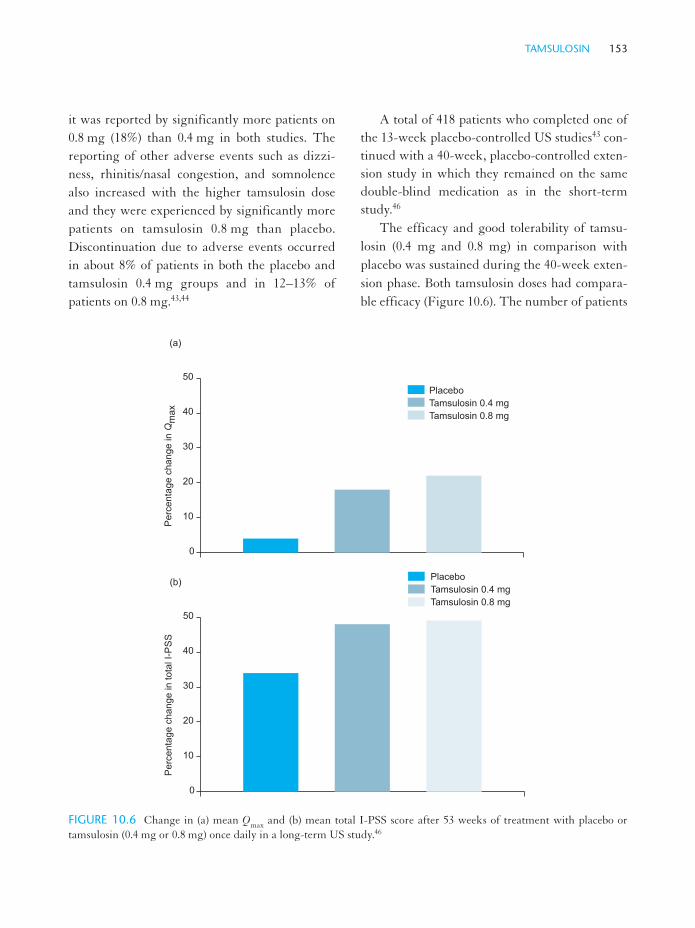
TAMSULOSIN 153
it was reported by significantly more patients on0.8 mg (18%) than 0.4 mg in both studies. Thereporting of other adverse events such as dizzi-ness, rhinitis/nasal congestion, and somnolencealso increased with the higher tamsulosin doseand they were experienced by significantly morepatients on tamsulosin 0.8 mg than placebo.Discontinuation due to adverse events occurredin about 8% of patients in both the placebo andtamsulosin 0.4 mg groups and in 12–13% ofpatients on 0.8 mg.43,44
A total of 418 patients who completed one ofthe 13-week placebo-controlled US studies43 con-tinued with a 40-week, placebo-controlled exten-sion study in which they remained on the samedouble-blind medication as in the short-termstudy.46
The efficacy and good tolerability of tamsu-losin (0.4 mg and 0.8 mg) in comparison withplacebo was sustained during the 40-week exten-sion phase. Both tamsulosin doses had compara-ble efficacy (Figure 10.6). The number of patients
������������������������� ���������
�
��
��
��
�
��
���
���
��
���
���
���
� �
�3#�
00
������������������������� ���������
�
��
��
��
�
��
���
���
��
���
���
���
��
�-
FIGURE 10.6 Change in (a) mean Qmax and (b) mean total I-PSS score after 53 weeks of treatment with placebo ortamsulosin (0.4 mg or 0.8 mg) once daily in a long-term US study.46
Ch 10 13/5/05 3:36 pm Page 153

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA154
that discontinued due to adverse events remainedlow and comparable in the placebo (6%) and tam-sulosin 0.4 mg (5%) groups. A total of 16% ofpatients on 0.8 mg discontinued due to adverseevents.
It can be concluded that tamsulosin 0.4 mg isthe optimal dose in the treatment in Americanpatients with LUTS suggestive of BPH with avery good safety profile.44 It has a fast onset ofaction with significant improvements in Qmax
within 24 hours and a symptomatic score within1 week. It does not lower blood pressure to a clin-ically significant extent, even in uncontrolledhypertensives. It has no increased potential forsymptomatic orthostatic hypotension comparedwith placebo, even when administered withoutdose titration and when exposed to multiple andrigorous orthostatic stress testing. Only abnormalejaculation occurred consistently and significant-ly more often with tamsulosin 0.4 mg than place-bo. Therefore, 0.4 mg is the recommended tam-sulosin dosage in the US. If patients fail torespond after 2–4 weeks, the dose may beincreased to 0.8 mg.
Long-term open-label extension studies
All patients (be it tamsulosin- or placebo-treated)who completed the two European placebo-con-trolled phase III studies could be enrolled in along-term extension study with open-label tam-sulosin for up to 4 years. In an interim analysis,355 patients were treated with tamsulosin for upto 3 years.47 The significant improvements inQmax, total Boyarsky symptom score, Qmax respon-ders, and symptom score responders observed inthe 12-week placebo-controlled studies were sus-tained for up to 3 years in the patients whoremained in the study. The increase in mean Qmax
from baseline ranged from 0.7 to 1.8 ml/s
(p < 0.05) and remained between 11.5 and 12 ml/sthroughout the follow-up period (Figure 10.7a).Total Boyarsky symptom score was improvedfrom baseline by 3.7 to 4.1 (or –39% to –44%:p < 0.001) (Figure 10.7b). The percentage ofpatients having a clinically significant responsewas also sustained: about 30% for Qmax andbetween 70 and 80% for symptom score respon-ders (Figure 10.8a and b). Tamsulosin alsoremained very well tolerated. A total of 27% ofpatients had possibly/probably drug-relatedadverse events over the entire 3-year period anddizziness and abnormal ejaculation were still themost common side-effects (occurring in ≤ 6% ofpatients). Similar results were seen in a meta-analysis of the extension of the placebo-controlledstudies and an alfuzosin comparative study (seelater) which involved 516 patients followed for upto 3 years.48
In the US, a total of 955 patients receivedopen-label therapy with tamsulosin for up to 2years49 with sustained efficacy and safety. Therange for improvements from baseline were 1.4 to2.5 ml/s for Qmax, –5.9 to –10.4 for total I-PSS,32–44% for Qmax responders, and 58–83% forsymptom score responders. A further long-termUS trial involved 609 BPH patients treated withtamsulosin for 6 years.50 Participants received amaintenance dose of 0.4 or 0.8 mg/day. Theimprovements in AUA symptom index and Qmax
were maintained throughout the study period,with good levels of tolerance. Orthostatichypotension was observed in only 1.3% of thegroup.
It can be concluded that the favorable effica-cy/safety ratio of tamsulosin is sustained inapproximately 1500 patients with LUTS sugges-tive of BPH receiving open-label tamsulosin forup to 3 years in Europe or the US.
Ch 10 13/5/05 3:36 pm Page 154

TAMSULOSIN 155
Direct comparative clinical studies vs other
α1-adrenoceptor antagonists
Three direct comparative clinical studies have
been performed.51–53 One was a European phase
III, double-blind, randomized, comparative
study between alfuzosin (2.5 mg twice daily for 2
weeks and 2.5 mg three times daily for 10 weeks)
and tamsulosin (0.4 mg once daily after breakfastthroughout). It involved 256 patients with LUTS(total Boyarsky score > 6) suggestive of BPH(Qmax 4–12 ml/s).51 The other single-blind, ran-domized trial compared terazosin (dose titratedfrom 1 to 5 mg once daily) and tamsulosin (0.2 mgonce daily throughout) for 8 weeks in 98 Koreanpatients with LUTS (total I-PSS ≥ 8) suggestive
�
�
�
�
+
��
���
,��
�
���
1�(
���
����
� �� � �� � �� �� � +� ��� ��� ��� � ���
�8��� � ���+� ����� ����� ����� ����� ����� �� ��
�����5��4��
�
��
��
�
���
,��
�
��-
��
�2��
� �� � �� � �� �� � +� ��� ��� ��� � ���
�8�� �� ����� ���+� ����� ��+�� ����� �� �� �����
�����5��4��
FIGURE 10.7 Effect of tamsulosin over time on (a) mean Qmax and (b) mean total Boyarsky symptom score in patientsfollowed for up to 3 years in an extension of the two European placebo-controlled studies.47
Ch 10 13/5/05 3:36 pm Page 155

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA156
of BPH (Qmax 5–15 ml/s).52 The results show that
tamsulosin had comparable efficacy to both alfu-
zosin and terazosin. They all increased Qmax by
1.6–2.1 ml/s (16–22%: Figure 10.9a) and reduced
total symptom score by 36–40% (Figure 10.9b).
Both tamsulosin and alfuzosin were very well
tolerated. The incidence of abnormal ejaculationwas also comparable in both groups (one patientwith tamsulosin and none with alfuzosin).Terazosin was, however, associated with signifi-cantly more drug-related adverse events (37% ofpatients) than tamsulosin (2% of patients;p = 0.001). In particular, dry mouth (16% vs 0%)
�
��
�
��
��
���
���
�� �
��1�
( ��
���
���
��(�
$��
��6
�
� �� � �� � �� �� � +� ��� ��� ��� � ���
�����5��4��
�
��
��
��
�
��
���
��
�-�
��(�
$��
��6
�
�� � �� � �� �� � +� ��� ��� ��� � ���
�����5��4��
FIGURE 10.8 Effect of tamsulosin over time on (a) Qmax responders and (b) total Boyarsky symptom score respondersin patients followed for up to 3 years in an extension of the two European placebo-controlled studies.47
Ch 10 13/5/05 3:36 pm Page 156

TAMSULOSIN 157
and dizziness (12% vs 0%) were reported morefrequently with terazosin. None of the patientson tamsulosin or terazosin experienced (drug-related) abnormal ejaculation. Alfuzosin and ter-azosin produces significant decreases in bloodpressure compared with baseline whereas this
was not the case with tamsulosin (Figure 10.10).In addition, the blood pressure reductions withalfuzosin were statistically significantly greaterthan those with tamsulosin, especially in elderlypatients.51
���
����� �����(��'��� � � ���1�( �������
9���$9��:�++�
&�����������:�++�
� �� �� �� � ��
��������������
�����������
����������� ��
;�!����������
��������������
�����������
����������� ��
;�!����������
9���$9��:�++�
&�����������:�++�
� �� �� ��
���
����� �����(��'��� ����-
FIGURE 10.9 Percentage improvement in (a) total symptom score and (b) Qmax in two direct comparative clinical trialsbetween tamsulosin and alfuzosin51 or tamsulosin and terazosin.52
Ch 10 13/5/05 3:37 pm Page 157

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA158
A third double-blind, randomized study com-pared the potential of tamsulosin and terazosin toinduce orthostatic hypotension during earlymorning and nocturnal orthostatic stress testingin 50 normotensive elderly subjects (more than50% had LUTS).53 Tamsulosin and terazosin
were administered for 15 days according to theirrecommended dosage regimen in daily practice:tamsulosin 0.4 mg once daily after breakfastwithout dose titration, terazosin dose titratedfrom 1 to 5 mg once daily in the evening. Theresults show that tamsulosin caused significantly
�����������������
���
���
��
���
���
��
��
�
��
�
&�
���
��
!���
���
���
� �
�$
(��
��
�.
��
0�(��0&� 0�(��%&� 0 �$��0&� 0 �$��%&�
)����!��� !����������
���
)
)
)
���������;�!�����
��
��
�
��
��
��
�
�
&�
���
��
!���
���
���
� �
�$
(��
��
�.
��
0�(��0&� 0�(��%&� 0 �$��0&� 0 �$��%&�
)����!��� '�� ��������
���
)
)
)
FIGURE 10.10 Effect on blood pressure (BP) in direct comparative clinical study between (a) tamsulosin and alfuzosin51
and (b) tamsulosin and terazosin.52 S, systolic; D, diastolic.
Ch 10 13/5/05 3:37 pm Page 158

TAMSULOSIN 159
less symptomatic orthostatic hypotension (4% ofpatients) than terazosin (36% of patients;p = 0.011: Figure 10.11). The patient with symp-tomatic orthostatic hypotension on tamsulosinhad pre-study vertigo, which was an exclusioncriterion for the study.
It can be concluded that α1-adrenoceptorantagonists have similar efficacy in the treatmentof LUTS suggestive of BPH. It is their potentialto lower blood pressure and produce cardiovascu-lar-related adverse events such as symptomaticorthostatic hypotension that differentiatesbetween α1-adrenoceptor antagonists.3,4 Tam-sulosin 0.4 mg has the lowest potential to reduceblood pressure and causes less symptomaticorthostatic hypotension than terazosin. This maybe clinically important as orthostatic hypotensionand syncope are risk factors for falling. Falls arethe sixth largest cause of death in the elderly andthe cost of fall-related fractures in the elderlyamounts to US $10 billion/year.54 Tamsulosin,furthermore, is easy to use as it does not requiredose titration and can be taken once a day.
Tolerability in elderly patients and patientswith co-morbidity or co-medication
Tamsulosin has been repeatedly shown to be welltolerated.51–53,55 A subgroup analysis of younger(< 65 years) and older (≥ 65 years) patientsenrolled in the two European phase III placebo-controlled trials38 revealed that tamsulosin 0.4 mgonce daily had comparable effects on blood pres-sure and was as well tolerated in both youngerand older patients, compared with placebo.56
In two observational surveys, in which almost20 000 German patients with LUTS suggestive ofBPH received tamsulosin 0.4 mg once daily for 4or 12 weeks, approximately 40–50% of patientshad concomitant hypertension, other cardiovas-cular (CV) diseases, or diabetes.57 It appeared thatoverall about 95% of patients rated the global tol-erability of tamsulosin as good or very good.Concomitant hypertension, other CV diseases, ordiabetes had only a minor effect on global tolera-bility, which became significant due to the largepatient numbers. It was still rated as good or very
�������������8���
����������� ����8���
���������8���
�
�
�
�
��
��
*��
���
�!(
� ��
�
5� �
�1�
( ��
� ��
�� �
�� �
���
1(�
���
�
)����!��� '�� �������
)
FIGURE 10.11 Number of patients with symptomatic orthostatic hypotension during orthostatic stress testing in directcomparative trial between tamsulosin and terazosin.53
Ch 10 13/5/05 3:37 pm Page 159

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA160
good in more than 90% and 95% of cases in thetwo surveys. A multivariate analysis showed thathypertension did not contribute to changes inglobal tolerability. Diabetes and other CV dis-eases contributed significantly. This may be due
to the reduced quality of life associated with theseconditions and the large patient numbers andmay therefore not be clinically significant for themajority of these patients. Many patients in thesetrials also took concomitant CV medication
&�
��
����
�� �
����
����
1�!
��
����
��
����� ����!(� �� �
α�#����4����8��+�<��� ���$���8����β#�� �� ������8�������1 � ����(1��8 ���
� �� �� �� � ��
��
��
��
��
��1 � ����(1���� �'��� ���=����'��(�1 � ����(1
���# ��� �$5� �>���
&�
��
����
���
!!���
�1�
! ��
����
��
����� ����!(� �� �
α�#����4����8��+�<��� ���$���8����β#�� �� ������8�������1 � ����(1��8 ���
� �� � �� �� ���
��
��
��
��
α�#&���4������� �'��� ���=����'��α�#����4���
���# ��� �$5� �>���
FIGURE 10.12 Percentage of patients that perceived (a) the global efficacy and (b) the global tolerability as better thanthat of previous treatment with β-sitosterol, other phytotherapy, finasteride, or other α1-adrenoceptor antagonists.59
Ch 10 13/5/05 3:37 pm Page 160

TAMSULOSIN 161
(diuretics, β-blockers, angiotensin-convertingenzyme (ACE) inhibitors, or calcium antago-nists). Global tolerability in these patientsremained good to very good in 95% of patientsand the CV co-medication did not contribute tochanges in global tolerability in a multivariateanalysis. Blood pressure changes in patients withco-morbidity or co-medication were minimal andcomparable to those reported for tamsulosin andplacebo in placebo-controlled trials. In patientswith co-morbidity or co-medication, additionalblood pressure reductions were not more than2 mmHg. This did not significantly contribute toblood pressure changes in a multivariate analysis.
In three clinical interaction studies, tamsu-losin was administered to the hypertensivepatients controlled with the β-blocker atenolol,the ACE inhibitor enalapril, or the calciumantagonist nifedipine. The results confirm thattamsulosin has no clinically significant additionaleffects on blood pressure or an increased potentialto produce orthostatic hypotension in hyperten-sive patients treated with antihypertensive med-ication.58
It can be concluded that in such elderlypatients and the majority of patients with cardio-vascular co-morbidity or co-medication, tamsu-losin is well tolerated and has minimal effects onblood pressure.
USE IN PATIENTS PRETREATED WITH OTHERMEDICAL THERAPY
In two large German observational surveys,patients pretreated with other medical therapies,such as phytotherapy, finasteride, or other α1-adrenoceptor antagonists, were asked to rate theglobal efficacy and tolerability of tamsulosin incomparison with their previous treatment (i.e.
worse, similar, better).59 It appeared that relativeto patients pretreated with other α1-adrenoceptorantagonists, the global efficacy of tamsulosin wasperceived better than that of previous treatmentin about 25% of phytotherapy- and 15% of finas-teride-pretreated patients (Figure 10.12a).Relative to previous treatment with phyto-therapy, the global tolerability of tamsulosin wasperceived better than that of previous treatmentin about 25% of other α1-adrenoceptor antago-nists and 13% of finasteride pretreated patients(Figure 10.12b).
META-ANALYSIS
In addition to the two meta-analyses mentionedpreviously38,41 two systematic reviews of tamsu-losin in the treatment of BPH have been per-formed in recent years.60,61 The latest of theseincluded 14 studies with a total of 4122 partici-pants, mean age 64, with moderate LUTS.Patients were treated with a range of doses oftamsulosin per day. The weighted mean differ-ence (WMD) for mean change in Boyarsky symp-tom score from baseline showed a 12% improve-ment with 0.4 mg/day and a 16% improvementwith 0.8 mg/day, relative to placebo.Improvements in Qmax were 1.1 ml/s for bothdosages. Lower doses of tamsulosin(0.2–0.4 mg/day) were found to be as effective asalternative α-antagonists.
Rates of adverse events, which were generallymild, included dizziness, rhinitis, and abnormalejaculation. These increased in a dose-dependentmanner, with discontinuations due to such effectssimilar to placebo at the 0.2 mg/day dose, butincreasing to 16% with 0.8 mg/day. Efficacyincreased only slightly with higher doses.
Ch 10 13/5/05 3:37 pm Page 161

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA162
ANCILLARY PROPERTIES
Effect on PSA
In contrast to finasteride, which reduces meanPSA plasma levels by 50%, tamsulosin (0.4 or0.8 mg once daily), in comparison with placebo,had no clinically significant effect on PSA plasmalevels, either in the phase III placebo-controlledEuropean54 (Figure 10.13) or US studies.43,44
Effect on lipids
Modest positive effects on lipid plasma levels havebeen described in hypertensive patients treatedwith hemodynamically active α1-adrenoceptorantagonists. In one of the US placebo-controlledstudies, tamsulosin also reduced serum triglyc-eride levels by 9% compared with < 1% on placebo.44
SUMMARY
α1-Adrenoceptor antagonists have superior effi-cacy over finasteride and phytotherapy (at least in
the short term), work independent of prostatesize, are not associated with erectile dysfunction,and do not affect PSA plasma levels. Therefore,they are a very good first-choice medical therapyfor patients with LUTS suggestive of BPH. Themajor disadvantages of the classical α1-adreno-ceptor antagonists that were originally developedfor hypertension (prazosin, doxazosin, terazosin,and alfuzosin) are their blood pressure-loweringpotential with subsequent risk of (first-dose)orthostatic hypotension and associated need fordose titration. The reduction of the occurrence oforthostatic hypotension is clinically importantbecause it is one of the risk factors for falling.Falls may lead to major injuries such as fracturesand are the sixth leading cause of death in the eld-erly.
Tamsulosin is an α1-adrenoceptor antagonistthat displays selectivity for α1A- and α1D-adreno-ceptors. In human volunteers, tamsulosin (modi-fied-release formulation) caused less inhibition ofexperimentally induced vasoconstriction thanhemodynamically active α1-adrenoceptor antago-nists such as doxazosin and terazosin and it was
����������������
�
��
��
��
�
��
��
��
���
��
���
�!(
� ��
�
%�������?��6
%�������?��6
%�������?��6
@� ����6�������
3������?��6
3������?��6
3������?��6
7������0;!����������
FIGURE 10.13 Percentage of patients with specific changes in PSA from baseline on placebo or tamsulosin 0.4 mg oncedaily in the meta-analysis of the two European phase III placebo-controlled studies.62
Ch 10 13/5/05 3:37 pm Page 162

TAMSULOSIN 163
therefore specifically developed to treat LUTSsuggestive of BPH. It is available in Japan, mostEuropean countries, many Latin American coun-tries, and the US. The recommended dosage forCaucasian patients is 0.4 mg once daily (after ameal). Tamsulosin 0.4 mg can be administered asits therapeutic dose from the start of therapy withno need for dose titration. As such it has superi-or efficacy to placebo and is as effective as otherα1-adrenoceptor antagonists such as alfuzosinand terazosin. It has, however, a negligible poten-tial for blood pressure lowering compared withother α1-adrenoceptor antagonists such as alfu-zosin and terazosin, and induces less sympto-matic orthostatic hypotension than terazosin. Theonly adverse event that was reported consistentlyand significantly more often with tamsulosin0.4 mg than placebo was abnormal ejaculation.There was no difference in reporting of abnormalejaculation on tamsulosin, alfuzosin, or terazosinin comparative trials. The very good tolerabilityand minimal effects on blood pressure of tamsu-losin are maintained in elderly patients and thevast majority of patients with cardiovascular co-morbidity and co-medication. The global efficacyof tamsulosin 0.4 mg was perceived better thanthat of previous treatment with finasteride orphytotherapy. The global tolerability was per-ceived better than that of previous treatment withother α1-adrenoceptor antagonists or finasteride.Tamsulosin 0.4 mg once daily is therefore a verygood first-choice medical therapy for Caucasianpatients with LUTS suggestive of BPH.
REFERENCES
1. Caine M, Pfau A, Perlberg S. The use of alpha-adrenergic blockers in benign prostatic obstruction.Br J Urol 1976; 48: 255–263
2. Chapple C R. Medical therapy and quality of life.Eur Urol 1998; 34 (Suppl 2): 10–17
3. Chapple C R. Pharmacotherapy for benign prosta-tic hyperplasia—the potential for α1-adrenoceptorsubtype-specific blockade. Br J Urol 1998; 81(Suppl 1): 34–47
4. Djavan B, Marberger M. A meta-analysis on theefficacy and tolerability of α1-adrenoceptor antago-nists in patients with lower urinary tract symptomssuggestive of benign prostatic obstruction. EurUrol 1999; 36: 1–13
5. McVary K T. Medical therapy for benign prostatichyperplasia progression. Curr Urol Rep 2002; 3:269–275
6. Denis L, McConnell J, Yoshida O et al. and TheMembers of the Committees. 4th InternationalConsultation on BPH. Recommendations of theInternational Scientific Committee: the evaluationand treatment of lower urinary tract symptoms(LUTS) suggestive of benign prostatic obstruction.In: Denis L, Griffiths K, Khoury S et al. (eds).Proceedings 4th international consultation onbenign prostatic hyperplasia (BPH). Paris, 2–5 July,1997. Plymouth: Plymbridge Distributors, 1998:669–684
7. Focus on lower urinary tract symptoms: nomencla-ture, diagnosis, and treatment options. Highlightsfrom the 5th international consultation on benignprostatic hyperplasia, June 25–27, 2000, Paris,France. Rev Urol 2001; 3: 139–145
8. Lepor H, Williford W O, Barry M J et al. The effi-cacy of terazosin, finasteride, or both in benign pro-static hyperplasia. N Engl J Med 1996; 335: 533–539
9. Debruyne F M J, Jardin A, Colloi D et al. on behalfof the European ALFIN study group. Sustained-release alfuzosin, finasteride and the combinationof both in the treatment of benign prostatic hyper-plasia. Eur Urol 1998; 34: 169–175
10. Kirby R S, Roehrborn C, Boyle P et al. for thePREDICT Study Investigators. Efficacy and toler-ability of doxazosin and finasteride, alone or incombination, in treatment of symptomatic benignprostatic hyperplasia: the Prospective EuropeanDoxazosin and Combination Therapy (PREDICT)Trial. Urology 2003; 61: 119–126
Ch 10 13/5/05 3:37 pm Page 163

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA164
11. McConnell J D, Roehrborn C G, Bautista O M etal. The long-term effect of doxazosin, finasteride,and combination therapy the clinical progression ofbenign prostatic hyperplasia. N Engl J Med 2003;349: 2387–98
12. Lepor H, Williford W O, Barry M J et al. for theVeterans Affairs Cooperative Studies BenignProstatic Hyperplasia Study Group. The impact ofmedical therapy on bother due to symptoms, qual-ity of life and global outcome, and factors predict-ing response. J Urol 1998; 160: 1358–1367
13. Boyle P, Gould A L, Roehrborn C G. Prostate vol-ume predicts outcome of treatment of benign pro-static hyperplasia with finasteride: meta-analysis ofrandomized clinical trials. Urology 1996; 48:398–405
14. Brawer M K, Lin D W, Williford W O et al. Effectsof finasteride and/or terazosin on serum PSA:results of VA Cooperative Study #359. Prostate1999; 39: 234–239
15. Wilde M I, McTavish D. Tamsulosin. A review ofits pharmacological properties and therapeuticpotential in the management of symptomaticbenign prostatic hyperplasia. Drugs 1996; 52:883–898
16. Bylund D B, Bond R A, Clarke D E et al.Adrenoceptors. In: Gidlestone (ed). The IUPHARcompendium of receptor characterization and clas-sification. London: IUPHAR Media, 1998: 58–74
17. Ford A P D W, Daniels D V, Chang D J et al.Pharmacological pleiotropism of the humanrecombinant α1A-adrenoceptor: implications forα1-adrenoceptor classification. Br J Pharmacol1997; 121: 1127–1135
18. Price D T, Schwinn D A, Lomasney J W et al.Identification, quantification, and localization ofmRNA for three distinct alpha1 adrenergic recep-tor subtypes in human prostate. J Urol 1993; 150:546–551
19. Forray C, Bard J A, Wetzel J M et al. The alpha1-adrenergic receptor that mediates smooth musclecontraction in human prostate has the pharmaco-logical properties of the cloned human alpha (1c)subtype. Mol Pharmacol 1994; 45: 703–708
20. Nasu K, Moriyama N, Kawabe K et al.Quantification and distribution of α1-adrenoceptorsubtype in RNA’s in human prostate: comparisonof benign hypertrophied and non-hypertrophiedtissue. Br J Pharmacol 1996; 119: 797–803
21. Ford A P D W, Arrendondo N F, Blue D R Jr et al.RS-17053 (N-[2-(2-cyclopropylmethoxyphenoxy)-ethyl]-5-chloro-α1-adimethyl-1H-indole-3-ethanamine hydrochloride), a selective α1A-adreno-ceptor antagonist, displays low affinity for func-tional α1-adrenoceptors in human prostate: impli-cations for receptor classification. Mol Pharmacol1996; 49: 209–215
22. Marshall I, Burt R P, Chapple C R. Noradrenalinecontractions of human prostate mediated by α1A-(α1C-) adrenoceptor subtype. Br J Pharmacol 1995;115: 781–786
23. Malloy B J, Price D T, Price R R et al. α1-Adren-ergic subtypes in human detrusor. J Urol 1998; 160:937–943
24. Hatano A, Takahashi H, Tamaki M et al.Pharmacological evidence of distinct α1-adreno-ceptor subtypes mediating the contraction ofhuman prostatic urethra and peripheral artery. Br JPharmacol 1994; 113: 723–728
25. Faure C, Goutrier C, Langer S Z, Graham D.Quantification of α1-adrenoceptor subtypes inhuman tissues by competitive RT-PCR analysis.Biochem Biophys Res Com 1995; 213: 935–943
26. Rudner X I, Booth J W, Funk B L et al. Subtypespecific regulation of human vascular α1-adrener-gic receptors by vessel bed and age. Circulation1999; 100: 2336–2343
27. Harada K, Ohmori M, Fujimura A. Comparison ofthe antagonistic activity of tamsulosin and doxa-zosin at vascular α1-adrenoceptors in humans.Naunyn Schmiedeberg’s Arch Pharmacol 1996;354: 557–561
28. Schafers R F, Fokuhl B, Wasmuth A et al.Differential vascular α1-adrenoceptor antagonismby tamsulosin and terazosin. Br J Clin Pharmacol1999; 47: 67–74
29. Foglar R, Shibata K, Horie K et al. Use of recom-binant α1-adrenoceptors to characterize subtype
Ch 10 13/5/05 3:37 pm Page 164

TAMSULOSIN 165
selectivity of drugs for the treatment of prostatichypertrophy. Eur J Pharmacol 1995; 288: 201–207
30. Michel M C, Grubbel B, Taguchi K et al. Drugs fortreatment of benign prostatic hyperplasia: affinitycomparison at cloned α1-adrenoceptor subtypesand in human prostate. J Auton Pharmacol 1996;16: 21–28
31. Richardson C D, Donatussi C F, Page S O et al.Pharmacology of tamsulosin: saturation-bindingisotherms and competition analysis using clonedα1-adrenergic receptor subtypes. Prostate 1997; 33:55–59
32. Yamada S, Suzuki M, Tanaka C et al. Comparativestudy on α1-adrenoceptor antagonist binding inhuman prostate and aorta. Clin Exp PharmacolPhysiol 1994; 21: 405–411
33. Andersson K E. Uroselectivity. In: Cockett A T,Khoury S, Aso Y et al. (eds). Proceedings of the 3rdinternational consultation on benign prostatichyperplasia (BPH). Jersey: Scientific Communic-ations International, 1996: 541–542
34. Kawabe K, Ueno A, Takimoto Y et al. and theYM617 Clinical Study Group. Use of an α1-block-er, YM617, in the treatment of benign prostatichypertrophy. J Urol 1990; 144: 908–912
35. Abrams P, Speakman M, Stott M et al. A dose-ranging study of the efficacy and safety of tamsu-losin, the first prostate-selective α1A-adrenoceptorantagonist, in patients with benign prostaticobstruction (symptomatic benign prostatic hyper-plasia). Br J Urol 1997; 80: 587–596
36. Boyarsky S, Jones G, Paulson D F, Prout G R. Anew look at bladder neck obstruction by the Foodand Drug Administration regulators: guide linesfor investigation of benign prostatic hypertrophy.Trans Am Assoc Genitourin Surg 1977; 68: 29–31
37. Abrams P, Schulman C C, Vaage S and theEuropean Tamsulosin Study Group. Tamsulosin, aselective α1C-adrenoceptor antagonist: a random-ized, controlled trial in patients with benign pro-static ‘obstruction’ (symptomatic BPH). Br J Urol1995; 76: 325–336
38. Chapple C R, Wyndaele J J, Nordling J et al. onbehalf of the European Tamsulosin Study Group.Tamsulosin, the first prostate-selective α1A-adreno-
ceptor antagonist. A meta-analysis of two random-ized, placebo-controlled, multicentre studies inpatients with benign prostatic obstruction (sympto-matic BPH). Eur Urol 1996; 29: 155–167
39. Lepor H, Auerbach S, Puras-Baez et al. A ran-domized, placebo-controlled multicenter study ofthe efficacy and safety of terazosin in the treatmentof BPH. J Urol 1992; 148: 1467–1474
40. Aso Y, Boccon-Gibod L, Da Silva F C et al.Subjective response, objective response, impact onquality of life. In: Cocket A T K, Aso Y, Denis L,Khoury S (eds). Proceedings of the internationalconsultation on benign prostatic hyperplasia(BPH), Paris, 26–27 June. SCI, 1991: 85–90
41. Hofner K for the European Tamsulosin StudyGroup. Tamsulosin: effect on sexual function inpatients with LUTS suggestive of BPO (sympto-matic BPH). Eur Urol 1998; 33 (Suppl 1): 129(abstract 515)
42. Abrams P, Tammela T L, Hellstrom P et al. for theESPIRIT Group. European pressure–flow investi-gation of tamsulosin in men with lower urinarytract symptoms (LUTS) suggestive of benign pro-static obstruction (BPO) – ESPRIT study. J Urol1998; 159 (Suppl 5): 256 (abstract 982)
43. Lepor H for the Tamsulosin Investigator Group.Phase III multicenter placebo-controlled study oftamsulosin in benign prostatic hyperplasia.Urology 1998; 51: 892–900
44. Narayan P, Tewari A and Members of UnitedStates 93–01 Study Group. A second phase III mul-ticenter placebo controlled study of 2 dosages ofmodified release tamsulosin in patients with symp-toms of benign prostatic hyperplasia. J Urol 1998;160: 1701–1706
45. Barry M J, Fowler F J, O’Leary M P et al. and theMeasurement Committee of the AmericanUrological Association. The American UrologicalAssociation symptom index for benign prostatichyperplasia. J Urol 1992; 148: 1549–1557
46. Lepor H for the Tamsulosin Investigator Group.Long-term evaluation of tamsulosin in benign pro-static hyperplasia: placebo-controlled, double-blindextension of phase III trial. Urology 1998; 51:901–906
Ch 10 13/5/05 3:37 pm Page 165

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA166
47. Schulman C C, Cortvriend J, Jonas U et al. onbehalf of the European Tamsulosin Study Group.Tamsulosin: 3-year long-term efficacy and safety inpatients with lower urinary tract symptoms sugges-tive of benign prostatic obstruction: analysis of aEuropean, multinational, multicenter, open-labeled study. Eur Urol 1999; 36: 609–620
48. Schulman C C, Buzelin J-M, Lock T M T W.Tamsulosin: 3-year follow-up of efficacy and safetyin 516 patients with LUTS suggestive of BPO. JUrol 1998; 159 (Suppl 5): 256 (abstract 983)
49. Lepor H and the Tamsulosin Investigator Group.Tamsulosin, long-term, open-label, extension studyto evaluate response and efficacy. J Urol 1997; 157(Suppl 4): 331 (abstract 293)
50. Narayan P, Evans C P, Moon T. Long-term safetyand efficacy of tamsulosin for the treatment oflower urinary tract symptoms associated withbenign prostatic hyperplasia. J Urol 2003; 170:498–502
51. Buzelin J M, Fonteyne E, Kontturi M et al. for theEuropean Tamsulosin Study Group. Comparisonof tamsulosin with alfuzosin in the treatment ofpatients with lower urinary tract symptoms sugges-tive of bladder outlet obstruction (symptomaticbenign prostatic hyperplasia). Br J Urol 1997; 80:597–605
52. Lee E, Lee C. Clinical comparison of selective andnon-selective α1A-adrenoceptor antagonists inbenign prostatic hyperplasia: studies on tamsulosinin a fixed dose and terazosin in increasing doses. BrJ Urol 1997; 80: 606–611
53. De Mey C, Michel M C, McEwen J, Moreland T. Adouble-blind comparison of terazosin and tamsu-losin on their differential effects on ambulatoryblood pressure and nocturnal orthostatic stress test-ing. Eur Urol 1998; 33: 481–488
54. Coffey D S. Controversies in the management oflower urinary tract symptoms: an overview. Br JUrol 1998; 81 (Suppl 1): 1–5
55. Michel M C, Bressel H U, Goepel M, Rubben H. A6-month large-scale study into the safety of tamsu-losin. Br J Clin Pharmacol 2001; 51: 609–614
56. Chapple C R, Baert L, Thind P et al. on behalf ofthe European Tamsulosin Study Group.Tamsulosin 0.4 mg once daily: tolerability in olderand younger patients with lower urinary tractsymptoms suggestive of benign prostatic obstruc-tion (symptomatic BPH). Eur Urol 1997; 32:462–470
57. Michel M C, Mehlburger L, Bressel H-U et al.Tamsulosin treatment of 19,365 patients with lowerurinary tract symptoms: does co-morbidity altertolerability? J Urol 1998; 160: 784–791
58. Lowe F C. Coadministration of tamsulosin andthree antihypertensive agents in patients withbenign prostatic hyperplasia: pharmacodynamiceffect. Clin Ther 1997; 19: 730–742
59. Michel M C, Bressel H -U, Mehlburger L, GoepelM. Tamsulosin: real life clinical experience in 19365 patients. Eur Urol 1998; 34 (Suppl 2): 37–45
60. Wilt T J, MacDonald R, Rutks I. Tamsulosin forbenign prostatic hyperplasia. Cochrane DatabaseSyst Rev 2003; 1: CD002081
61. Wilt T J, MacDonald R, Nelson D. Tamsulosin fortreating lower urinary tract symptoms compatiblewith benign prostatic obstruction: a systematicreview of efficacy and adverse effects. J Urol 2002;167: 177–183
62. Denis L for the European Tamsulosin StudyGroup. Tamsulosin: effect on PSA levels in 3-month placebo-controlled studies and long-termfollow-up of these studies. Eur Urol 1998; 33 (Suppl1): 130 (abstract 517)
Ch 10 13/5/05 3:37 pm Page 166

Phytotherapeutic agents in the treatmentof LUTS and BPHK Dreikorn J M Fitzpatrick
11
167
INTRODUCTION
The spectrum of synthetic pharmaceutical treat-ment options for patients presenting with lowerurinary tract symptoms (LUTS) secondary tobenign prostatic hyperplasia (BPH) has expandedconsiderably over the last decade and this hasbeen accompanied by an increase in the use ofplant-derived therapies.1,2 At the same time, aworldwide decrease in classical operative proce-dures has been reported, with rates oftransurethral resection of the prostate (TURP)and open prostatectomy falling by up to 50% insome countries.3
While there is at least some agreement con-cerning the scientific rationale and indications forthe use of α-adrenoceptor blockers and 5α-reductase inhibitors, the role of phytotherapeuticagents in the treatment of LUTS and BPH hastraditionally been less clear and has been continu-ously debated.4–22 The use of plant extracts is longestablished in France and Germany, and so prod-ucts containing extracts of Serenoa repens andPygeum africanum, among others, have a marketshare of up to 50% of all preparations used for thetreatment of symptomatic BPH. In these coun-tries, plant extracts are prescribable drugs, theircosts being totally or partly reimbursed by theheathcare system, in contrast to the UK, forexample, where they are neither approved norreimbursed.23
In the US, plant-derived medications are soldas nonreimbursable nonprescription dietary sup-plements, mostly in natural health food stores.
Some preparations which are available by pre-scription only in Europe, such as the lipido-sterolic extract of Serenoa repens (LSESr)Permixon®, are not available at all in the US.1 In2000, US sales of dietary supplements werereported to have reached $17.1 billion,24 andaround $1.5 billion are reportedly spent on theself-medication of LUTS.25
According to some US urologists, 50–90% ofnewly referred patients with LUTS secondary toBPH have already tried or are using some form ofalternative or complementary medication at thetime of their presentation.13–15,26 The suggestionthat ‘natural agents’, commonly supposed to bewithout side-effects, might be as efficacious assynthetic and chemical products, seems attractivefor patients who prefer such an approach.17,26 Weas treating physicians have to face this develop-ment. This widespread and increasing patientpreference, however, has to be balanced againstthe need for increased awareness of the impor-tance and necessity to select treatment options onevidence-based rationales.27,28
ORIGIN OF PLANT EXTRACTS
In Europe alone, more than 100 botanic prepara-tions are available for the treatment of LUTS sec-ondary to BPH.5,6,29 Although extracts from morethan 30 different plants are being used for theseproducts, the most popular phytotherapeuticagents originate from the roots, seeds, barks, orfruits of the plants listed in Table 11.1.
Ch 11 13/5/05 3:37 pm Page 167

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA168
Some preparations are produced from a singleplant, others contain extracts from two or moresources. The extraction procedures differ fromcompany to company. Therefore, the compositionand components of one individual product maybe significantly different to those of another man-ufacturer, even if the product originates from thesame plant(s). As a consequence, the results ofbasic research studies or clinical trials involving aspecific product cannot automatically be appliedto another preparation.
Several active components of plant extractshave been identified (Table 11.2). However,whether these elements represent all the mostactive and important elements of the preparationsfor the beneficial in vitro and in vivo effectsdescribed (Table 11.3) is still not known.6,8–12,29,30
The precise mechanism of action of manyproducts has also yet to be elucidated, althoughantiestrogenic and proapoptotic effects have beenreported for some preparations, alongside inhibi-tion of 5α-reductase activity.31,32
As the extraction methods of products derivedfrom the same source could lead to differing lev-els of efficacy, bioavailability, and pharmacody-namics, it has been recommended that individual
products be evaluated separately.29 In addition,both synthetic and natural products should besubjected to identical analytic, biological, andclinical evaluations.
PHYTOTHERAPEUTIC COMPOUNDS
Serenoa repens
The extracts from the berries of the Americandwarf palm (Serenoa repens, saw palmetto, Sabalserrulata) are the most popular plant-based
TABLE 11.1 Origin of phytotherapeutic agents for the treatment of LUTS secondary to BPH
Common term Element utilized Latin term
American dwarf palm, saw palmetto Fruit Serenoa repens, Sabal serrulata
South African star grass Root Hypoxis rooperi
Pine Root Pinus
Spruce Root Picea
African plum tree Bark Pygeum africanum
Stinging nettle Root Urtica dioica
Rye Pollen Secale cereale
Pumpkin Seeds Cucurbita pepo
TABLE 11.2 Proposed active constituents of plantextracts.
Phytosterols (β-sitosterol)
Phyto-estrogens
Free fatty acids (lauric and myristic acid)
Lectins
Flavonoids
Plant oils
Polysaccharides
Ch 11 13/5/05 3:37 pm Page 168

PHYTOTHERAPEUTIC AGENTS IN THE TREATMENT OF LUTS AND BPH 169
products used in the treatment of symptomaticBPH.4–6,13–16,29 In Germany alone, more than 30different products contain Serenoa repens,6,29
while numerous similar products are also avail-able in the US. Many of them contain extractsfrom other plants (Pygeum africanum, pumpkinseeds, etc.) and minerals, such as zinc. The differ-ent extracts contain mainly free and esterifiedfatty acids, phytosterols, and long-chain alcohols.More recently, free fatty acids have been proposedto be the active components of Serenoa repensextracts, primarily responsible for their beneficialeffects on the prostate. On this basis the precisecomposition could critically influence both bio-logical and clinical activity.
The most extensively investigated preparationis Permixon, an n-hexane LSESr and a complexmixture of free fatty acids, phytosterols, aliphaticalcohols, and various polyphrenic com-pounds.6,29,33 A number of potential mechanismsof action have been attributed to Permixon,including anti-androgenic and anti-inflammato-ry activity, inhibition of cell proliferation, andpromotion of apoptosis.31,33–38
The action of Permixon is now considered tobe predominantly attributable to uncompetitive5α-reductase type I and type II inhibition, result-ing in lower levels of dihydrotestosterone (DHT)formation from testosterone in the prostate.31,39
Although Rhodes et al.,40 in 1993, did not
TABLE 11.3 Proposed mode of action of plant extracts.
Mechanism of action Extract
Inhibition of 5α-reductase I and II activity Serenoa repens, Secale cereale, cactus flower
Anti-estrogenic effect Serenoa repens, Pygeum africanum
Anti-androgenic effect Serenoa repens, Cucurbita pepo
Anti-inflammatory effect Serenoa repens, β-sitosterol, Pygeum africanum,Cucurbita pepo
Induction of apoptosis β-Sitosterol, Serenoa repens
Interference with prostaglandin metabolism β-Sitosterol, Pygeum africanum
Inhibition of phospholipase A2 and 5-lipoxygenase enzymes β-Sitosterol
Suppression of prostate cell metabolism and growth Urtica dioica, Serenoa repens
Inhibition of proliferative growth factors Urtica dioica, Serenoa repens
Decrease of sex hormone-binding globulin Urtica dioica
Protection/strengthening of detrusor muscle Pygeum africanum
Alteration of cholesterol metabolism Pygeum africanum
Free radical scavengers/membrane stabilization Pygeum africanum
Inhibition of aromatase activity Cactus flower
Reduction of prostatic urethral resistance Secale cereale
Action on α-adrenergic receptors Secale cereale, Serenoa repens
Ch 11 13/5/05 3:37 pm Page 169

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA170
subscribe to this, the theory that Permixon is aneffective inhibitor of 5α-reductase type I and typeII has been substantiated by in vitro studies byBayne et al.31,39 In a specially developed clinicallyrelevant model, 5 days’ treatment of co-culturedhuman prostate cells with 10 µg/ml Permixonresulted in significant inhibition of 5α-reductasetype I and type II; the dose utilized was estimatedto correspond to the concentration reached inplasma and prostate at the recommended clinicaldose.
The hypothesis promulgated is that lauric andmyristic acid, which comprise a subfraction of thefree fatty acids contained in the preparation,modulate the cell-membrane environment in away that reduces the activity of the nuclear mem-brane-bound 5α-reductase.41 The observationthat no decrease of prostate-specific antigen(PSA) is observed in vivo42 is explained by theassumption that Permixon, in contrast to finas-teride, does not interfere with PSA productionand has little or no effect on other androgen-dependent processes which rely on the binding ofandrogens to their receptor. Subsequent studiesalso suggested that Permixon specifically decreas-es cell proliferation and increases the apoptoticindex of the prostatic stromal and epithelialcells.38 Studies involving alternative sources ofSerenoa repens have suggested that it has anti-estrogenic or anti-inflammatory effects.32,43
Lower levels of DHT and higher levels oftestosterone have been identified in the prostatesof Permixon-treated BPH patients;44 however,superficially at variance with an action as a 5α-reductase inhibitor, no significant effect on serumlevels of PSA and prostate volume has beendemonstrated in several studies.6,29,33,42 Indeed,the data on several potential mechanisms ofaction of Serenoa repens are often confusing andcontradictory and many of the effects described
have only been demonstrated in vitro, often withconsiderably higher dosages of the extract thanare recommended for clinical treatment.
The commonly recommended dose of Serenoarepens is 320 mg daily, often divided into twodoses. A dose of 160 mg Permixon twice dailyseems to be as efficacious as two capsules of160 mg once daily.45 Aside from occasional gas-trointestinal discomforts, no significant side-effects have been reported with the extract, incontrast to most other medical or surgicalapproaches.
The numerous published clinical trials involv-ing Serenoa repens extracts have been criticallyreviewed by a committee during the 4th (1997)and 5th (2000) International Consultations onBPH,6,29 and in two articles by one of the com-mittee members.15,16 These Consultations recom-mended that extracts of Serenoa repens producedby different manufacturers be evaluated separate-ly and regarded as discrete entities, due to vari-ance between products associated with differentextraction processes and other factors. They alsohighlighted the need for placebo-controlled trialsof such products, as are conducted for traditionalsynthetic pharmaceuticals.
Although it is accepted that uncontrolled tri-als and comparative trials without placebo con-trols are of only limited value in the quantifica-tion of the clinical efficacy of Serenoa repens in thetreatment of LUTS and BPH,6,29 several trialsinvolving the extract have taken place that indi-cate that significant improvements in LUTSsymptomatology occur. However, the results aredependent on the product (and presumably thecomposition).
A recent long-term trial examined the effica-cy of twice-daily Permixon (160 mg) in 130 BPHpatients over 2 years.46 Prostatic symptoms wereassessed using validated instruments such as the
Ch 11 13/5/05 3:37 pm Page 170

PHYTOTHERAPEUTIC AGENTS IN THE TREATMENT OF LUTS AND BPH 171
International Prostate Symptom Score (I-PSS)and sexual function using the Male SexualFunction (MSF-4) questionnaire. PSA, peak uri-nary flow (Qmax), and quality of life were alsoevaluated every 6 months. Significant improve-ments were observed for I-PSS, Qmax, and qualityof life, while prostate size fell by 5.9 ml by the endof the study period. MSF-4 scores rose signifi-cantly in the second year of treatment and totalPSA and hormonal levels did not change.
A further, longer-term study of Permixon inmen with mild to moderate BPH (n = 26)revealed that twice-daily administration of320 mg of the drug decreased mean I-PSS by 8.8 ± 0.18, increased Qmax by4.13 ± 0.51 ml/s on average, and improved quali-ty of life after 5 years, providing further evidenceof the long-term efficacy of the drug.47
It has been suggested that a ‘placebo effect’may contribute to the improvements observed inmen receiving some extracts of Serenoa repens. Ina study of 50 men with LUTS, who were treatedfor 6 months with a Serenoa repens preparation, asignificant improvement in I-PSS from 19.5 to12.5 was noted (p = 0.001).48 No significantchanges in PSA levels or improvement in Qmax,postvoid residual volume (PVR), bladder capaci-ty, or detrusor pressure at peak urinary flow ratewere observed, however. The authors accept thatthis subjective improvement in voiding symp-toms that occurred without demonstrable objec-tive change in any of the measure urodynamicparameters may be attributable in part to theplacebo effect and conclude that further studies,including placebo-controlled trials, are needed.48
Other studies have suggested that the benefitdoes not only arise from a placebo effect. A trialexcluding patients who had previously respondedto placebo medication revealed that, when treatedwith Permixon, these nonresponders showed sig-
nificant reductions in both daytime and nocturnalurinary frequency and improvement in Qmax.
49
Some data have proven inconclusive.6,16,29
Thus, although it was shown in the 30-day studydescribed above49 that dysuria, daytime frequen-cy, nocturia, and Qmax were all significantlyimproved in Permixon-treated patients com-pared with baseline values and placebo-treatedpatients, the study did not show any real per-ceived clinically relevant benefit of the drug overplacebo by the patients or their physicians. Whenthe patients and physicians were asked to assessthe global efficacy of the treatment at the end ofthe trial, the rates of satisfaction were 68% and47%, respectively, for the placebo group versus71% and 57%, respectively, for the Serenoa repens-treated patients. The short-term nature of thistrial limits the interpretation of the data.
In an attempt to quantify the benefit moreprecisely, double-blind randomized clinical trialshave been undertaken on some Serenoa repens-containing products. In a 6-month, double-blind,randomized comparative trial with finasteride in1098 patients, the efficacy of Permixon was foundto be equivalent to that of the 5α-reductaseinhibitor50. The decrease in I-PSS was 37% and39% and the increase in Qmax was 2.7 ml/s (25%)and 3.2 ml/s (30%) in the Serenoa repens and finas-teride groups, respectively. Greater drug-relatedside-effects, particularly in terms of loweredlibido and increased erectile dysfunction wereobserved in the finasteride group.
Unfortunately, this study did not include aplacebo group and the volumes of the prostateswere rather small (baseline volumes 43 ml and44 ml, respectively, for the two groups). As weknow today, the effect of finasteride may be lim-ited in small prostates.51 Therefore, in analogy tothe VA study,52 the comparison between Serenoarepens and finasteride in this study might simply
Ch 11 13/5/05 3:37 pm Page 171

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA172
show equivalency of both agents to placebo,although Hamdy et al. postulated that prostaticvolume does not correlate with the efficacy oftreatment using either finasteride orphytotherapy.53
Comparison of Serenoa repens to ‘convention-al’ therapy is not limited to finasteride, however.A comparison of the α-blocker tamsulosin toPermixon took place over a period of 12 monthsand involved 811 BPH patients from 11 differentcountries.54 I-PSS fell by 4.4 in each group andQmax also improved to a similar extent. A secondtrial, involving alfuzosin and Permixon, alsorevealed the latter drug to be equally effective forthe treatment of urinary symptoms. Sixty-threemen with mild to moderate BPH who did notrespond to placebo were randomized to receiveeither 320 mg Permixon daily or 2.5 mg alfuzosinthree times a day for 3 weeks.55 Symptom scoresimproved significantly from baseline with no sig-nificant difference between treatment groups.
Overall, therefore, Permixon has been shownto produce clinical efficacy equivalent to thatobserved with both α-blockers and finasteride;this would tend to indicate that the action ofPermixon does not arise from a placebo effectalone.
Phytosterols/β-sitosterol
Although β-sitosterol and various other phyto-sterols are contained in many plant extracts usedfor the treatment of symptomatic BPH, somemanufacturers presume that β-sitosterol is themajor active component and therefore classifytheir preparation by the content of this element.Most preparations available derive from thespecies Hypoxis rooperi, Pinus, or Picea.
β-Sitosterol is claimed to be both a cyclo-oxy-genase and a lipoxygenase inhibitor, interferingwith prostaglandin metabolism and thereby
exerting anti-inflammatory effects.30 A stimula-tory effect on transforming growth factor(TGFβ), which induces apoptosis, and trans-location protein kinase Cα has also been dis-cussed.6,56,57
In a German study the β-sitosterol prepara-tion Harzol® was evaluated in a 6-month, dou-ble-blind, placebo-controlled study of 200patients.56,58 While the placebo group showedonly mild improvements, statistically significantimprovements were noted for I-PSS, quality oflife, Qmax, and PVR in the β-sitosterol-treatedpatients who received 20 mg of the product, threetimes daily. The I-PSS improved by 2.3 points forplacebo and 7.4 for β-sitosterol; Qmax increased by1.1 ml/s for placebo and 5.2 ml/s for the testgroup. Follow-up observations (up to 18 months)have shown that those patients who continuedtreatment and even those who stopped the med-ication maintained their benefit, while placebo-treated patients improved with a similar responseonce started on β-sitosterol.56
Another preparation, also containing mainlyβ-sitosterol (Azuprostat®, 65 mg twice daily) wasevaluated in a 6-month, randomized, placebo-controlled trial of 177 patients.59 The magnitudeof the statistically significant improvement in thisstudy was great: the I-PSS improved by 2.8 in theplacebo group compared to 8.2 in the treatmentgroup and Qmax increased by 4.4 ml/s and8.8 ml/s, respectively. The results of both studieswith phytosterols, although exciting, await con-firmation by other groups.
African plum tree
Extracts from the bark of the African plum tree(Pygeum africanum) are widely used in Franceand the US. Almost all basic research and clinicalstudies have been performed with the productTadenan®.6,15,16 The chloroform extract contains
Ch 11 13/5/05 3:37 pm Page 172

PHYTOTHERAPEUTIC AGENTS IN THE TREATMENT OF LUTS AND BPH 173
phytosterols, short-chain (lauric and myristic)and unsaturated long-chain (oleic and linolic)fatty acids.
The extract is thought to inhibit fibroblastproliferation and to exert an anti-inflammatoryand anti-estrogenic effect.6,60,61 Eleven con-stituents have been identified in the crude extract,including high levels of myristic acid, which isthought to affect membrane fluidity directly andto reduce the contact between propagating freeradicals and unsaturated lipid substances, therebyslowing the process of hydrolysis and membranedegradation.61 Moreover, in a rabbit model, theagent is thought to protect the bladder muscula-ture from contractile dysfunction caused by outletobstruction, improving bladder ultrastructure,bladder compliance, and contractileresponses.62–67
According to Levin et al.65 and Hass et al.,61
obstruction induces ischemic muscular mem-brane damage, which might be caused by lipidperoxidation. High levels of myristic acid foundin the Pygeum extract may make the bladder cellmembranes less susceptible to lipid peroxidationand thereby exert their protective effect on thebladder. However, in the experimental studiesdemonstrating this effect, highly supraclinicaldoses were used. Therefore, the applicability ofthese findings to clinical BPH remains question-able. Although there are numerous open andshort-term placebo-controlled studies suggestingclinical efficacy,68–70 the trials do not meet theguidelines recommended by the InternationalConsultation conferences.6
Breza et al.71 reported a multicenter open-label trial involving 85 patients, treated over 2months with Tadenan, followed by 1 monthwithout treatment. Improvement in I-PSS was40%, reduction of nocturia 32%, improvement ofquality of life 31%, and increase in Qmax 19%,
without any reduction of prostate volume.Significantly, the improvements were maintainedduring the 1-month no-treatment phase. Overall,the data are not conclusive, however, and longer-term data are not available.
Stinging nettle
Extracts from the roots of the stinging nettle(Urtica dioica) are widely used in Germany. Theycontain a complex mixture of water- and alcohol-soluble compounds, including lectins, phenols,and sterols.5,6,30
Whether the suggested modes of action,which include inhibition of prostatic growth fac-tor interaction, suppression of prostatic cellmetabolism and modulation of the binding of sexhormone-binding globulin, have any relevance inclinical BPH is uncertain. Studies performedmore than 10 years ago are inconclusive becauseof small patient numbers and short trial dura-tion.72,73 In a randomized, placebo-controlled, 3-month study of 41 patients, a liquid preparationshowed superiority over placebo, but was notmarketed because its taste was not accepted bypatients.74
Extracts of stinging nettle are often combinedwith one or more alternative plant-derived thera-py, as discussed later in the chapter.
Rye grass pollen extract
A product deriving from the pollen of someselected plants growing in southern Sweden ismarketed as a registered pharmaceutical(Cernilton®) in some European countries, Japan,Korea, and Argentina. The extract consists of awater- and fat-soluble fraction combined into atablet or capsule.
In vitro studies suggest that pollen extractsexert an effect on α-adrenergic receptors, relax
Ch 11 13/5/05 3:37 pm Page 173

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA174
the sphincteric musculature, increase prostaticand serum zinc levels, and 5α-reductase activi-ty.30,75 Moreover, the growth of immortal cancercell lines was inhibited and in rats atrophy of theprostatic lobes was observed.76
In a German 3-month, multicenter, double-blind, placebo-controlled study of 103 patients,nocturia and diurnal frequency were significant-ly reduced by 69 and 66%, respectively, in thetreatment group, compared to 37% and 44% inthe placebo group.77 A 6-month, double-blind,placebo-controlled study of 60 patients reportedan overall significant symptomatic improvementof 69% in the pollen extract group compared to29% in the placebo group.78
In a comparative trial of 89 patients over 4months with a Pygeum africanum extract(Tadenan), the pollen extract showed betterresults with regard to improvement of irritativeand obstructive symptom scores, Qmax, and resid-ual urine.75 However, comparison of Cernilton totamsulosin and a combination of both revealedthe combination and tamsulosin alone to be moreeffective than Cernilton alone.79
Pumpkin seeds
Extracts from pumpkin seeds (Cucurbita pepo) areused to treat symptomatic BPH in several coun-tries, such as Germany. The seeds contain asweet-tasting, oily substance, mainly composed oflinolic acid, ∆5 and ∆7 sterols, tocopherol, seleni-um, magnesium, and carotenoid. The extract isthought to have an anti-androgenic and anti-phlogistic action.
A randomized, placebo-controlled, double-blind trial of 476 men with BPH showed a signif-icantly greater reduction in I-PSS (–6.8) com-pared to the placebo group (–5.6) over a period of12 months. The other parameters (Qmax, quality
of life, prostate volume, PVR) did not change ineither of the groups, however.80
Cactus flower extracts
Cactus flower extract, known as opuntia, isincluded in the British herbal pharmacopoeia asindicated for prostatic hypertrophy and is a com-monly used herbal remedy for BPH in Israel.
Aqueous and organic solvent extracts of driedcactus flower powder have been described as hav-ing a broad spectrum of activity, including inhibi-tion of both type I and type II 5α-reductase activ-ity and inhibition of aromatase and antioxidantactivity.81 The authors postulate that as cactusflower has simultaneous 5α-reductase and aro-matase inhibitory activity it possesses a uniquelydual advantage in the treatment of BPH; howev-er, there are no reports of any controlled clinicaltrials with cactus flower products.
COMBINATION PRODUCTS
Although there is no scientific evidence showingthat the efficacy of phytotherapeutic preparationsis enhanced by the combination of extracts fromseveral plants, many companies offer mixtures ofplant extracts, claiming that the possible effectsdemonstrated for extracts from individual plantsmay be additive in combination products.
In a 3-month, randomized, double-blindstudy of 53 patients given extracts from pumpkinseeds and Serenoa repens, urinary flow rates, mic-turition time, residual urine, frequency of mic-turition, and a subjective assessment of the treat-ment effect were all significantly improved whilethe changes in the placebo group were not.82
A combination product of Serenoa repens andstinging nettle (Prostagutt® forte) was used in arandomized, placebo-controlled study of 40
Ch 11 13/5/05 3:37 pm Page 174

PHYTOTHERAPEUTIC AGENTS IN THE TREATMENT OF LUTS AND BPH 175
patients (6-month double-blind treatment phasefollowed by 6 months of open treatment). Greaterimprovement in both I-PSS and Qmax wasobserved with treatment than with placebo: I-PSSdecreased from 18.6 to 11.1 in the treatmentgroup during the 6 months of double-blind treat-ment, compared to a decrease from 19 to 17.6(p = 0.002) with placebo. During the open-labelextension phase, the initially placebo-treatedpatients decreased in I-PSS from 17.6 to 13.3 andthe treatment group continued to improve from11.1 to 9.8. Qmax increased by 2.3 ml/s over thefirst phase in the verum group and by an addi-tional 1.15 ml/s over the open-label second 6-month phase, while an increase of only 0.45 ml/swas observed in the placebo group over the initialplacebo phase with a 2 ml/s increase during thesubsequent active treatment phase.83
The same preparation was also comparedwith finasteride in 489 patients randomized andobserved for 48 weeks.84 There was a statisticallysignificant improvement in each group, with adrop in I-PSS from 11.3 to 6.5 for the patientstreated with the plant extract, compared with adecrease from 12.6 to 6.9 in finasteride-treatedpatients. Qmax increased by 1.9 ml/s in the plantextract group and 2.7 ml/s in the finasteridegroup; however, there was no statistical signifi-cance between the treatment groups. Prostate vol-ume and PSA decreased in the finasteride grouponly. The mean baseline prostate volume was42 ml in the plant extract group versus 44 ml inthe finasteride group.
META-ANALYSES OF PHYTOTHERAPEUTICAGENTS
If adequate (gold-standard) randomized, placebo-controlled studies are lacking, confirmation of
efficacy of a drug is often sought through meta-analysis. There are some potential limitations inthis approach, however, as it has been shown thatthe agreement between meta-analyses and subse-quent large clinical trials can be discordant. Meta-analyses have a positive predictive value of 68%and a negative predictive value of 67%.85 Thismeans that up to one-third of meta-analyses maynot accurately predict subsequent clinical trialresults. Further, when the studies pooled in ameta-analysis are of poor quality, the meta-analy-sis itself can be compromised and the impact ofthe conclusions diluted. Overall, however, there isan increasingly widespread use of meta-analysesin the health-care environment.
Several meta-analyses involving plant-derivedBPH treatments have been published, four onSerenoa repens extracts,86–89 two on β-sitos-terols,90,91 one on Pygeum africanum,92 and two onrye grass pollen (Cernilton).93,94 In general, themeta-analyses support the hypothesis that phy-totherapeutic agents are beneficial in the treat-ment of LUTS in BPH patients.
In the original meta-analysis published byWilt et al.86 on Serenoa repens, 18 randomizedstudies were included, involving 2939 men withBPH. The mean weighted difference in compar-ison to placebo was an improvement in symptomscore of 1.41 points, an increase in Qmax of1.93 ml/s and a reduction in nocturia episodes of0.76 per night. A follow-up analysis conducted 4years later, with an additional three trials and atotal of 3139 patients, revealed quantitatively andqualitatively similar results.57 Overall, urinarysymptom score fell by 1.41 points (range 0–19),nocturia rates fell by 0.76/night, and Qmax
increased by 1.86 ml/s. Despite the benefit observed in these analyses,
the inclusion of products from 11 different man-ufacturers obtained by different extraction
Ch 11 13/5/05 3:37 pm Page 175

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA176
processes partially compromised the interpreta-tion of the data and thereby potential extrapola-tion to general clinical use.
On the basis of the evidence, it was thereforeconcluded that Serenoa repens improves urologicsymptoms and flow parameters, but that furtherclinical profiling is needed. In particular, the clin-ical activity of individual standardized prepara-tions should be determined.
It has been emphasized by an expert commit-tee at the ICUD BPH Consultations,6 and evenrecently by Wilt himself,18 that comparisonbetween various manufacturers’ preparations ofthe same plant extract is problematic. Data analy-sis can be hindered because of variations in theextraction processes, absence of precise analyticalinformation on composition, lack of certainty thatthe same supposedly active component(s) of theextract are included in the final product, andvariability in batch preparation. Moreover, onlyone of the 18 studies included in the first meta-analysis by Wilt et al. fulfilled the three main cri-teria of being placebo-controlled, utilizing stan-dard symptom score evaluations, and being of atleast 3 months’ duration.
In an attempt to address some of the issuesraised in previous analyses, another meta-analysison a single Serenoa repens product (Permixon) waspublished by Boyle et al.87 Eleven placebo-con-trolled randomized trials and two open-label tri-als were pooled. Eleven trials had informationregarding Qmax and nocturia. The additionalPermixon effect, beyond that observed on place-bo, on Qmax was 1.87 ml/s and the additionaleffect on nocturia was a decrease of 0.55 episodesper night. A further meta-analysis conducted bythe same team of all contemporary publisheddata available on Permixon involved a further1963 men from four randomized studies.89 Theadditional data allowed examination of the effect
of Permixon on I-PSS and revealed that, in addi-tion to improving peak flow (2.28 ± 0.29 aboveplacebo) and nocturia (1.01 ± 0.13 above placebo),the drug caused a significant fall in I-PSS(–4.7 ± 0.41). Such changes are at least as great asthose described in equivalent meta-analyses forterazosin95 and finasteride96 (Figure 11.1).
Wilt et al.90 also published a review of β-sitos-terol studies, including four double-blind trials of519 men, with a duration of 4–26 weeks. Theweighted mean difference (WMD) of β-sitosterolversus placebo was –4.9 points on the I-PSS (35%improvement versus placebo) in two studies.When a study which did not show pure β-sitos-terol-β-D-glucoside to be superior to placebo wasexcluded, the WMD for the Qmax was 5.13 ml/s(53% improvement). The authors state that β-sitosterols improve symptom scores by 35%, Qmax
by 34%, and reduced PVR by 24%. Nevertheless,the necessity of additional studies of sufficientsize and duration, with known concentrations ofβ-sitosterol, is emphasized in order to assess thelong-term efficacy of β-sitosterols and their abili-ty to prevent complications from BPH. Threedifferent preparations were used in the four stud-ies, and as it is uncertain whether the doses arecomparable, no definite conclusions can be drawnfrom this review.
MacDonald et al.93 published a review of fourold studies with the rye pollen extract Cernilton.Two placebo-controlled and two comparative tri-als involving 444 men were included. None of thestudies would have fulfilled the quality criteria ofthe recommendations of the InternationalConsultation, because of short trial duration,insufficient and incomplete outcome data, and nocontrols in two studies. The conclusion of thereview was that Cernilton is well tolerated andmodestly improves subjective urologic symptoms.Cernilton was not shown to improve urinary flow
Ch 11 13/5/05 3:37 pm Page 176
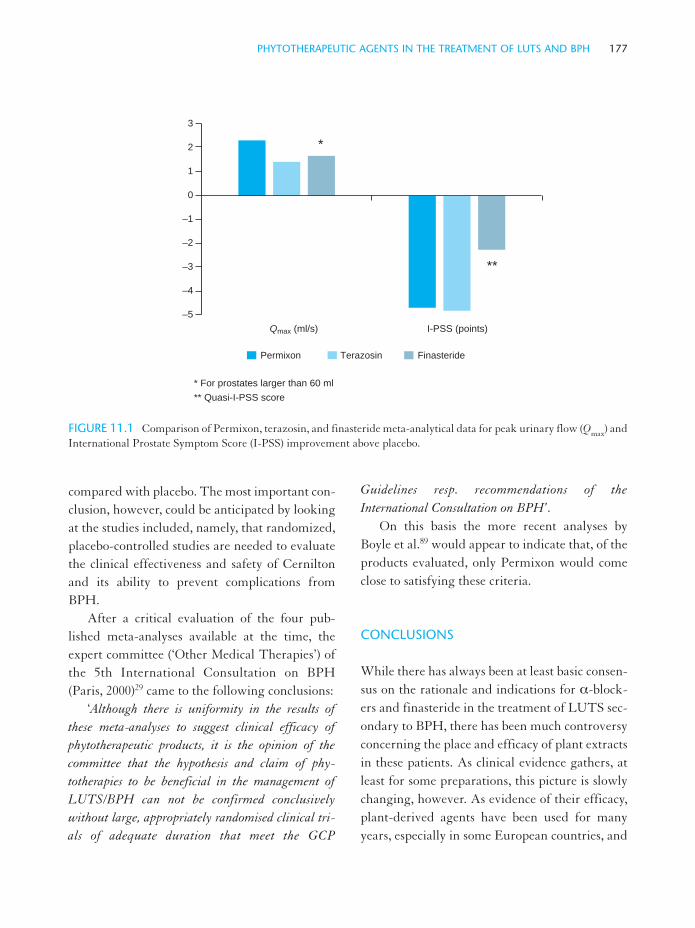
PHYTOTHERAPEUTIC AGENTS IN THE TREATMENT OF LUTS AND BPH 177
compared with placebo. The most important con-clusion, however, could be anticipated by lookingat the studies included, namely, that randomized,placebo-controlled studies are needed to evaluatethe clinical effectiveness and safety of Cerniltonand its ability to prevent complications fromBPH.
After a critical evaluation of the four pub-lished meta-analyses available at the time, theexpert committee (‘Other Medical Therapies’) ofthe 5th International Consultation on BPH(Paris, 2000)29 came to the following conclusions:
‘Although there is uniformity in the results ofthese meta-analyses to suggest clinical efficacy ofphytotherapeutic products, it is the opinion of thecommittee that the hypothesis and claim of phy-totherapies to be beneficial in the management ofLUTS/BPH can not be confirmed conclusivelywithout large, appropriately randomised clinical tri-als of adequate duration that meet the GCP
Guidelines resp. recommendations of theInternational Consultation on BPH’.
On this basis the more recent analyses byBoyle et al.89 would appear to indicate that, of theproducts evaluated, only Permixon would comeclose to satisfying these criteria.
CONCLUSIONS
While there has always been at least basic consen-sus on the rationale and indications for α-block-ers and finasteride in the treatment of LUTS sec-ondary to BPH, there has been much controversyconcerning the place and efficacy of plant extractsin these patients. As clinical evidence gathers, atleast for some preparations, this picture is slowlychanging, however. As evidence of their efficacy,plant-derived agents have been used for manyyears, especially in some European countries, and
Qmax (ml/s) I-PSS (points)
* For prostates larger than 60 ml
** Quasi-I-PSS score
3
2
1
0
–1
–2
–3
–4
–5
*
**
Permixon Terazosin Finasteride
FIGURE 11.1 Comparison of Permixon, terazosin, and finasteride meta-analytical data for peak urinary flow (Qmax) andInternational Prostate Symptom Score (I-PSS) improvement above placebo.
Ch 11 13/5/05 3:37 pm Page 177

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA178
their use is increasing in the US, where a 100%rise in the sale of botanic products has been notedsince 1994. Moreover, there is an increasing trendof patients and even physicians in many countriesto turn away from chemical and synthetic drugsto ‘natural’ preparations and paramedical formsof therapy. Additionally, an increasing number ofpatients prefer self-medication and treatment,which is supported by the marketing strategies ofcompanies producing such products.
On the other hand, the medical profession isincreasingly aware of the importance of the needto make treatment selections on the basis of goodevidence of benefit : risk from carefully con-trolled clinical trials.27,28 For novel therapies,potentially this may lead to conflicts when guide-lines are established according to the principles ofevidence-based medicine.
It is astonishing that, although a tremendousamount of literature concerning the use of phy-totherapy in LUTS and BPH exists, many impor-tant questions remain at least partially unan-swered:
• Which are the active components of thepreparations?
• How do they exert their claimed effects? • What is their bioavailability? • Is there a dose dependency? • How can the products be standardized and
compared?
The International Consultations on BPH haverepeatedly called for phytotherapeutic prepara-tions to be subjected to the same critical evalua-tions which are applied to the treatment of LUTSand BPH with drugs designed by medicinalchemists, such as α-blockers and 5α-reductaseinhibitors.6–8,11,29,97 Ony a few companies have sofar taken up this challenge. Reasons for others nothaving done this might include that the costs of
such evaluations would be difficult to recoupbecause these products are not patentable.
Overall, it can reasonably be concluded thatphytotherapeutic products are generally well tol-erated and, in some countries, less expensive thanα-blockers and 5α-reductase inhibitors.Although both objective and subjective clinicalimprovements have been shown in carefully con-trolled clinical trials, these evaluations have beenrestricted to only a few products/brands and haveyet to be mirrored with the majority of plant-based preparations.
It is pertinent to note that most plant extractsare complex mixtures and a product from onecompany is, in real terms, unique, as the extrac-tion procedures differ from producer to producerand the exact compositions of the preparationsmay vary between batches. In the majority ofcases they are also only partly chemically defined.Therefore, the products of the different compa-nies may not be comparable with regard to thecomponents contributing to the overall biologicaland clinical profile, even if the extracts originatefrom the same plant. As a consequence, meta-analyses containing extracts from different com-panies are only of limited use in evaluation of theefficacy of plant extracts, even if the productsstem from the same species.
In addition, it may be assumed that an extractfrom one type of plant has different mechanismsof action, efficacy, bioavailability, and pharmaco-dynamics, compared to an extract from anotherplant species. For this reason, meta-analyseswhich include studies with products from differ-ent companies and different plant species maycarry a substantial risk of ‘inborn errors’ if gener-al conclusions are drawn. Further, meta-analyti-cal data from one brand will not be directly trans-latable to another with a different composition.
Ch 11 13/5/05 3:37 pm Page 178

PHYTOTHERAPEUTIC AGENTS IN THE TREATMENT OF LUTS AND BPH 179
In conclusion, as long as the components ofplant extracts are not chemically defined or stan-dardized for all products, separate scientific stud-ies have to be performed with each extract/mix-ture in order to assess its individual efficacy. If theprinciples of evidence-based medicine are appliedto the evaluation of the current data on phy-totherapeutic agents in the treatment of LUTSand BPH, clear-cut evidence for their efficacyuntil recently has been difficult to establish.Although there is increasing evidence of efficacyfor some products this is not true of all extracts byany means. More proof is needed for other plant-based medications, particularly if the prescriptioncosts are to be reimbursed by the public healthcare system.
If patients buy phytotherapeutic agentsbecause of their preferences for ‘natural’ productsas dietary supplements at their own expense theyshould not be discouraged because they will, atleast, enjoy a placebo effect. However, it must bestressed that a sole symptom relief may mask theprogression of a disease.
Uncontrolled studies with low patient num-bers and of short duration, not performed accord-ing to accepted standards and guidelines, are ofquestionable value. Likewise, meta-analyses areonly acceptable if the quality of the studiesincluded is assessed and shown to be appropriate.Due to the widely controversial and partly insuf-ficient ‘hard’ data about the efficacy of phytother-apy for the treatment of symptomatic BPH, theInternational Consultations on BPH were reluc-tant to recommend phytotherapy as a therapeuticoption.98 The same opinion was developed by anexpert committee which established the guide-lines for the German urologists according to theprinciples of evidence-based medicine.99 Moreevidence has become available, from gold-stan-dard clinical trials and rigorous meta-analysis,87,89
however, suggesting that a review of the role ofphytotherapy in the management of the BPH isrequired.
REFERENCES
1. Gerber G S. Phytotherapy for benign prostatichyperplasia. Curr Urol Rep 2002; 3: 285–291
2. Vallancien G, Pariente P. Treatment of lower uri-nary tract symptoms suggestive of benign prostaticobstruction in real life practice in France. ProstateCancer Prostatic Dis 2001; 4: 124–131
3. Bruskewitz R. Management of symptomatic BPHin the US: who is treated and how? Eur Urol 1999;36 (Suppl 3) 7–13
4. Dreikorn K, Richter R. Conservative nonhormon-al treatment of patients with benign prostatichyperplasia. N Develop Biosci 1989; 5: 109–121
5. Dreikorn K, Schönhöfer P S. Stellenwert vonPhytotherapeutika bei der Behandlung der benig-nen Prostatahyperlasie (BPH). Urologe A 1995; 34:119–129
6. Dreikorn K, Borkowsi A, Braeckman J et al. Othermedical therapies. In: Denis L, Griffiths K, KhouryS et al. (eds). Proceedings of the 4th internationalconsultation on benign prostatic hyperplasia (BPH)1997. Plymouth: Plymbridge Distributors, 1998:633–659
7. Fitzpatrick J M, Dreikorn K, Khoury S et al. Themedical management of BPH with agents otherthan hormones or alpha-blockers. In: Cocket A TK, Aso Y, Chatelain C et al. (eds). Proceedings ofthe 2nd international consultation on benign pro-static hyperplasia (BPH), Paris 26–27 June 1991SCI. 1991: 195–199
8. Fitzpatrick J M, Dreikorn K, Khoury S et al. Themedical management of BPH with agents otherthan hormones or alpha-blockers. In: Cocket A TK, Aso Y, Chatelain C et al. (eds). Proceedings ofthe 2nd international consultation of benign prosta-tic hyperplasia (BPH), Paris 27–30 June 1993 SCI.1993: 445–450
Ch 11 13/5/05 3:37 pm Page 179
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA180
9. Fitzpatrick J M, Lynch T H. Phytotherapeuticagents in the management of symptomatic benignprostatic hyperplasia. Urol Clin North Am 1995;22: 407–412
10. Fitzpatrick J M, Lynch T H. Phytotherapeuticagents. In: Kirby R, McConnell J D, Fitzpatrick JM et al. (eds). Textbook of benign prostatic hyper-plasia. Oxford: Isis Medical Media, 1996; 331–337
11. Fitzpatrick J M, Braeckman J, Denis L et al. Themedical management of BPH with agents otherthan hormones or alpha-blockers. In: Cockett A TK, Khoury S, Aso Y et al. (eds). Proceedings of the3rd international consultation on benign prostatichyperplasia (BPH), Monaco, 26–28 June 1995, SCI,1996: 489–494
12. Fitzpatrick J M. Phytotherapy for treatment ofbenign prostatic hyperplasia: case not proven.Urology 1998; 53: 462–464
13. Lowe F C, Ku J C. Phytotherapy in treatment ofbenign prostatic hyperplasia: a critical review.Urology 1996; 48: 12–20
14. Lowe F C, Fagelman E. Phytotherapy in treatmentof benign prostatic hyperplasia. Curr Opin Urol1998; 8: 27–29
15. Lowe F C, Fagelman E. Phytotherapy in the treat-ment of benign prostatic hyperplasia: an update.Urology 1999; 53: 671–678
16. Lowe F C, Dreikorn K, Borkowski A et al. Reviewof recent placebo-controlled trials utilizing phy-totherapeutic agents for treatment of BPH.Prostate 1998; 37: 187–193
17. Marks L S, Tyler V E. Saw palmetto extract:newest (and oldest) treatment alternative for menwith symptomatic benign prostatic hyperplasia.Urology 1999; 53: 457–461
18. Wilt T J. Phytotherapy. In: Chapple C R,McConnell J D, Tubaro A (eds). Benign prostatichyperplasia. London: Martin Dunitz, 2000: 39–63
19. Dreikorn K. The role of phytotherapy in treatinglower urinary tract symptoms and benign prostatichyperplasia. World J Urol 2002; 19: 426–435
20. Preuss H G, Marcusen C, Regan J et al.Randomized trial of a combination of naturalproducts (cernitin, Serenoa repens, β-sitosterol, vita-
min E) on symptoms of benign prostatic hyperpla-sia (BPH). Int Urol Nephrol 2001; 33: 217–225
21. Levin R M, Das A K. A scientific basis for the ther-apeutic effects of Pygeum africanum and Serenoarepens. Urol Res 2000; 28: 201–209
22. Klingler H C. New innovative therapies for benignprostatic hyperplasia: any advance? Curr OpinUrol 2003; 13: 11–15
23. Chapple C R. Introduction and concludingremarks. Eur Urol 1999; 36 (Suppl 3): 1–6
24. Statement by Joseph A Levitt, Director, Center forFood Safety and Applied Nutrition, Food andDrug Administration, before the Committee onGovernment Reform, Chairman Dan Burton, USHouse of Representatives, March 20, 2001.http://www.cfsan.fda.gov/~lrd/st010320.html
25. Kurtzweil P. An FDA guide to dietary supple-ments. US Food and Drug Administration, 1999.http://vm.cfsan.fda.gov/zdms/dfsupp.html
26. Ernst E. Harmless herbs? A review of the recentliterature. Am J Med 1998; 104: 170–178
27. Friedland D J, Go A S, Davoren J B et al.Evidence-based medicine: a frame work for clinicalpractice. Stamford: Appleton & Lange, 1998
28. Speakman M J. Who should be treated and how?Evidence based medicine in symptomatic BPH.Eur Urol 1999; 36 (Suppl 3): 40–51
29. Dreikorn K, Lowe F, Braeckman J et al. Othermedical therapies. In: Denis L, Griffiths K, KhouryS et al. (eds). Proceedings of the 5th internationalconsultation on benign prostatic hyperplasia(BPH). Plymouth: Plymbridge Distributors, 2001
30. Buck A C. Phytotherapy for the prostate. Br J Urol1996; 78: 325–336
31. Bayne C W, Donelly F, Ross M et al. Serenoa repens(permixon®): a 5-alpha-reductase types I and IIinhibitor—new evidence in a co-culture model ofBPH. Prostate 1999; 40: 232–241
32. Di Silverio F, D’Eramo G, Lubrano C et al.Evidence that Serenoa repens extract displays anantiestrogenic activity in prostatic tissue of benignprostatic hypertropy patients. Eur Urol 1992; 21:309–314
Ch 11 13/5/05 3:37 pm Page 180

PHYTOTHERAPEUTIC AGENTS IN THE TREATMENT OF LUTS AND BPH 181
33. Plosker G L, Brogden R N. Serenoa repens(Permixon®): a review of its pharmacology andtherapeutic efficacy in benign prostatic hyperplasia.Drugs Aging 1996; 9: 379–395
34. Paubert-Braquet M, Cousse H, Raynaud J P et al.Effect of the lipido-sterolic extract of Serenoa repens(Permixon®) and its major components on basicfibroblast growth factor-induced proliferation ofcultures of human prostate biopsies. Eur Urol 1998;33: 340–347
35. Délos S, Iehlé C, Carsol J L et al. Inhibition ofhuman prostatic testosterone metabolism by alipidosterol extract of Serenoa repens (Permixon®). JUrol 1996; 155 (Suppl): 572A
36. Paubert-Braquet M, Raynaud J P, Braquet G,Cousse G. Permixon® (lipid sterolic extract ofSerenoa repens) and some of its components inhibitb-FGF- and EGF-induced proliferation of humanprostate organotypic cell lines. J Urol 1997; 157(Suppl 4): 138 (abstract 541)
37. Paubert-Braquet M, Cousse H, Raynaud J P et al.Effect of the lipidosterolic extract of Serenoa repens(Permixon®) and its major components on basicfibroblast growth factor-induced proliferation ofcultures of human prostatic biopsies. Eur Urol1998; 33: 340–347
38. Vacherot F, Azzouz M, Gil-Diez-de-Medina S etal. Effect of Permixon® on apoptosis and prolifera-tion in the prostate of patients with BPH. J Urol1999; 161: 362
39. Bayne C W, Donelly F, Chapman K et al. A novelcoculture model for benign prostatic hyperplasiaexpressing both isoforms of 5-alpha-reductase. JClin Endocrinol Metab 1998; 83: 206–213
40. Rhodes L, Primka R L, Berman C et al.Comparison of finasteride (Proscar®), a 5-α reduc-tase inhibitor and various commercial plantextracts in in vitro and in vivo 5-α reductase inhi-bition. Prostate 1993; 22: 43–51
41. Habib F K, Ross M, Bayne C W et al. The localisa-tion and expression of 5-alpha-reductase types Iand II mRNAs in human hyperplastic prostate andin prostate primary cultures. J Endocrinol 1998;156: 509–517
42. Stauch G, Perles P, Vergult G et al. Comparison ofFinasteride (Proscar®) and Serenoa repens(Permixon®) in the inhibition of 5-alpha reductasein healthy male volunteers. Eur Urol 1994; 26:247–252
43. Breu W, Hagenlocher M, Redl K et al.Antiphlogistische Wirkung eines mit hyperkritis-chem Kohlendioxid gewonnenen Sabalfucht-Extraktes. In-vitro-Hemmung des Cyclo-oxygenase- und 5-Lipoxygenase-Metabolismus.Drug Res 1992; 42: 547–551
44. Di Silverio F, Monti S, Sciarra A et al. Effects oflong-term treatment with Serenoa repens(Permixon®) on the concentrations and regionaldistribution of androgens and epidermal growthfactor in benign prostatic hyperplasia. Prostate1998; 37: 77–83
45. Stepanov V N, Siniakova L A, Sarrazin B,Raynaud J P. Efficacy and tolerability of the lipi-dosterolic extract of Serenoa repens (Permixon®) inbenign prostatic hyperplasia: a double-blind com-parison of two dosage regimens. Adv Ther 1999;16: 231–241
46. Pytel Y A, Lopatkin N, Gorilovsky L et al. Long-term clinical and biological effects of the lipido-sterolic extract of Serenoa repens in patients withsymptomatic benign prostatic hyperplasia. AdvTher 2002; 19: 297–306
47. Aliaev IuG, Vinarov A Z, Lokshin K L, Spivak LG. Five-year experience in treating patients withprostatic hyperplasia with permixon (Serenoa repensPierre Fabre Medicament) [in Russian]. Urologiia2002; 1: 23–25
48. Gerber G S, Zagaja G P, Bales G T et al. Saw pal-metto (Serenoa repens) in men with lower urinarytract symptoms: effects on urodynamic parametersand voiding symptoms. Urology 1998; 51:1003–1007
49. Descotes J L, Rambeaud J J, Deschaseaux P, FaureG. Placebo-controlled evaluation of the efficacyand tolerability of Permixon® in benign prostatichyperplasia after exclusion of placebo responders.Clin Drug Invest 1996; 9: 291–297
50. Carraro J C, Raynaud J P, Koch G et al.Comparision of phytotherapy (Permixon®) with
Ch 11 13/5/05 3:37 pm Page 181

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA182
finasteride in the treatment of benign prostatichyperplasia: a randomized international study of1.089 patients. Prostate 1996; 29: 231–240
51. Boyde P, Gould A I, Roehrborn G. Prostate volumepredicts outcome of treatment of benign prostatichyperplasia with finasteride: meta-analysis of ran-domised clinical trials. Urology 1996; 48: 398–405
52. Lepor H, Williford W O, Barry M J et al. The effi-cacy of terazosin, finasteride, or both in benign pro-static hyperplasia. N Engl J Med 1996; 335: 533
53. Hamdy F C, Chopin D K, Authié D et al. Prostaticvolume does not correlate with efficacy of treat-ment for mild to moderate benign prostatic hyper-plasia using either finasteride or phytotherapy. 4thInternational consultation on BPH, Paris 1997;abstract 77
54. Debruyne F, Koch G, Boyle P et al. Comparison ofa phytotherapeutic agent (Permixon) with an α-blocker (tamsulosin) in the treatment of benignprostatic hyperplasia: a 1-year randomized interna-tional study. Eur Urol 2002; 41: 497–507
55. Grasso M, Montesano A, Buonaguidi A et al.Comparative effects of alfuzosin versus Serenoarepens in the treatment of symptomatic benign pro-static hyperplasia. Archiv Españoles Urol 1995; 48:97–103
56. Berges R R, Kassen A, Senge T. Treatment ofsymptomatic benign prostatic hyperplasia with β-sitosterol: an 18-month follow-up. BJU Int 2000;85: 842–843
57. Kassen A, Berges R, Senge T. Effect of beta-sitos-terol on transforming growth factor-beta-1 expres-sion and translocation protein kinase C alpha inhuman prostate stromal cells in vitro. Eur Urol2000; 37: 735–741
58. Berges R R, Windeler J, Trampisch H et al.Randomised, placebo-controlled, double blind clin-ical trial of beta-sitosterol in patients with benignprostatic hyperplasia. Lancet 1995; 345: 1529–1532
59. Klippel K F, Hiltl D-M, Schipp B. A multicentric,placebo-controlled, double-blind clinical trial of β-sitosterol (phytosterol) for the treatment of benignprostatic hyperplasia. Br J Urol 1997; 80: 427–432
60. Andro M C, Riffaud J P. Pygeum Africanumextract for the treatment of patients with benignprostatic hyperplasia: review of 25 years of pub-lished experience. Curr Therap Res 1995; 56:796–817
61. Hass M A, Nowak D M, Leonova E et al.Identification of components of Prunus africanaextract that inhibit lipid peroxidation. Phyto-medicine 1999; 6: 379–388
62. Levin R M, Hass M A, Bellamy F et al. Effect oforal Tadenan treatment on rabbit bladder structureand function after partial outlet obstruction. J Urol2002; 167: 2253–2259
63. Levin R M, Riffaud J P, Bellamy F et al. Effects ofTadenan® pretreatment on bladder physiology andbiochemistry following partial outlet obstruction. JUrol 1996; 56: 2084–2088
64. Levin R M et al. Protective effect of Tadenan® onbladder function secondary to partial outletobstruction. J Urol 1996; 155: 1466–1470
65. Levin R M, Buttyan R, Horan P et al. Changes incontractile response of the rabbit bladder to fieldstimulation following unilateral iscemia. Protectiveeffect of Tadenan®. J Urol 1997; 157 (Suppl 4): 172
66. Buttyan R et al. Early molecular response to rabbitbladder outlet obstruction. Neurol Urodyn 1992;11: 225–238
67. Chen M W, Levin R M, Horan P et al. Effects ofunilateral ischemia on the contractile response ofthe bladder. Protective effect of Tadenan (Pygeumafricanum extract). Mol Urol 1999; 3: 5–10
68. Barlet A, Albrecht J, Aubert A et al. Efficacy ofPygeum africanum extract in the treatment of mic-turitional disorders due to benign prostatic hyper-plasia: evaluation of objective and subjectiveparameters: a multicentre, placebo-controlled dou-ble-blind trial. Wien Klin Wochenschr 1990; 102:667–673
69. Chatelain C, Autet W, Brackmann F. Comparisonof once a twice daily dosage forms of Pygeumafricanum extract in patients with benign prostatichyperplasia: a randomised, double-blind studywith long term open label extension. Urology 1999;54: 473–478
Ch 11 13/5/05 3:37 pm Page 182
PHYTOTHERAPEUTIC AGENTS IN THE TREATMENT OF LUTS AND BPH 183
70. Yablonsky F, Riffaud J P. Pygeum africanum forthe treatment of patients with BPH: a review of 25years of published experience. Curr Therap Res1995; 56: 796–817
71. Breza J, Dziurny O, Borowka A et al. Efficacy andacceptability of Tadenan (Pygeum africanumextract) in the treatment of benign prostatic hyper-plasia (BPH): a multicentre trial in Central Europe.Curr Med Res Opin 1998; 143: 127–139
72. Dathe G, Schmid H. Phytotherapie der benignenProstatahyperplasie: Doppelblindstudie mitExtractum Radicis Urticae (ERU). Urologe [B]1987; 27: 233–236
73. Vontobel H P, Herzog R, Rutishauser G H.Ergebnisse einer Doppelblindstudie über dieWirksamkeit von ERU-Kapseln in der konserva-tiven Behandlung der benignen Prostata-hyperplasie. Urologe [A] 1985; 24: 49–51
74. Engelmann U, Boos G, Kres H. Therapie derbenignen Prostatahyperplasie mit BazotonLiquidum. Urologe [B] 1996; 36: 287–291
75. Dutkiewicz S. Usefulness of Cernilton in the treat-ment of benign prostatic hyperplasia. Int UrolNephrol 1996; 28: 49–53
76. Habib F K, Ross M, Lewenstein A et al. The iden-tification of a prostate inhibitory substance in apollen extract. Prostate 1995; 26: 133–139
77. Becker H, Ebeling L. Konservative Therapie derbenignen Prostatahyperplasie (BPH) mitCernilton. Urologe [B] 1988; 28: 301–306
78. Buck A C, Cox R, Rees R W M et al. Treatment ofoutflow tract obstructive due to benign prostatichyperplasia with the pollen extract Cernilton. Br JUrol 1990; 66: 398–404
79. Aoki A, Naito K, Hashimoto O et al. Clinical eval-uation of the effect of tamsulosin hydrochlorideand cernitin pollen extract on urinary disturbanceassociated with benign prostatic hyperplasia in amulticentered study [in Japanese]. Hinyokika Kiyo2002; 48: 259–267
80. Bach D. Phytopharmaka. In: Höfner K, Stief C G,Jonas U (eds). Benigne Prostatahyperplasie. Berlin,Heidelberg: Springer, 2000: 238–260
81. Jonas A, Rosenblut G, Krapf D et al. Cactus flowerextracts may prove beneficial in benign prostatichyperplasia due to inhibition of 5-alpha-reductaseactivity, aromatase activity and lipid peroxidation.Urol Res 1998; 26: 265–270
82. Carbin B E, Larsson B, Lindahl O. Treatment ofbenign prostatic hyperplasia with phytosterols. Br JUrol 1990; 66: 639–641
83. Metzker M, Kieser M, Hölscher U. Wirksamkeiteines Sabal-Urtica-Kombinationspräparates bei derBehandlung der benignen Prostatahyperplasie(BPH). Urologe [B] 1996; 36: 292–300
84. Sökeland J, Albrecht J. Kombination aus Sabal-und Urticaextrakt mit Finasterid bei BPH (Styad.Ibis II nach Alken). Urologe [A] 1997; 36: 327–333
85. LeLorier J, Grégoire G, Benhaddad A et al.Discrepancies between meta-analyses and subse-quent large randomised controlled trials. N Engl JMed 1997; 337: 536–542
86. Wilt T J, Ishani A, Stark G et al. Saw palmettoextracts for treatment of benign prostatic hyperpla-sia: a systematic review. J Am Med Assoc 1998; 280:1604–1609
87. Boyle P, Lowe F, Robertson C, Roehrborn C G.Meta-analysis of clinical trials of Permixon® in thetreatment of symptomatic benign prostatic hyper-plasia. Urology 2000; 55: 533–539
88. Wilt T, Ishani A, MacDonald R. Serenoa repens forbenign prostatic hyperplasia. Cochrane DatabaseSyst Rev 2002; (3): CD001423
89. Boyle P, Robertson C, Lowe F, Roehrborn C G.Meta-analysis of Permixon in treatment of sympto-matic benign prostatic hyperplasia: an update[abstract]. J Urol 2003; 169 (Suppl 4): 1297
90. Wilt T J, McDonald R, Ishani A. b-sitosterol forthe treatment of benign prostatic hyperplasia: sys-tematic review. BJU Int 1999; 83: 976–983
91. Wilt T, Ishani A, MacDonald R et al. Beta-sitos-terols for benign prostatic hyperplasia. CochraneDatabase Syst Rev 2000; (2): CD001043
92. Wilt T, Ishani A, MacDonald R et al. Pygeumafricanum for benign prostatic hyperplasia.Cochrane Database Syst Rev 2002; (1): CD001044
Ch 11 13/5/05 3:37 pm Page 183

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA184
93. MacDonald R, Ishani A, Rutks I et al. A systemat-ic review of Cernilton for the treatment of benignprostatic hyperpasia. BJU Int 2000; 85: 836–841
94. Wilt T, MacDonald R, Ishani A et al. Cernilton forbenign prostatic hyperplasia. Cochrane DatabaseSyst Rev 2000; (2): CD001042
95. Boyle P, Robertson C, Manski R et al. Meta-analy-sis of randomized trials of terazosin in the treat-ment of benign prostatic hyperplasia. Urology2001; 58: 717–722
96. Boyle P, Gould L, Roehrborn C G. Prostate volumepredicts outcome of treatment of benign prostatichyperplasia with finasteride: meta-analysis of ran-domized clinical trials. Urology 1996; 48: 398–405
97. Roehrborn C G, Boyle P, Nickel J C et al. on behalfof the ARIA3001, ARIA3002, and ARIA3003
study investigators. Efficacy and safety of a dualinhibitor of 5 alpha-reductase types 1 and 2 (dutas-teride) in men with benign prostatic hyperplasia.Urology 2002; 60: 434–441
98. Denis L, McConnell J, Yoshida O et al. 4th interna-tional consultation of BPH. Recommendations ofthe international scientific committee: the evalua-tion and treatment of lower urinary tract syn-dromes (LUTS) suggestive of benign prostaticobstruction. In: Denis L, Griffiths K, Khoury S etal. (eds). Proceedings of the 4th international con-sultation of benign prostatic hyperplasia (BPH).Plymouth: Plymbridge Distributors, 1998; 669–984
99. Altwein J, Aumüller G, Berges R et al. Leitliniender Deutschen Urologen zur Therapie des BPH-Syndromes. Urologe [A] 1999; 38: 529–536
Ch 11 13/5/05 3:37 pm Page 184

Uroselectivity revisitedK-E Andersson M G Wyllie
12
BACKGROUND
The two major components of lower urinarytract symptoms (LUTS)—voiding (obstructive)and storage (irritative) symptoms—associatedwith benign prostatic hyperplasia (BPH) havetraditionally been linked directly or indirectly topathophysiologic changes in the prostate.1
Voiding symptoms have been attributed to twofacets of prostate function: the physical mass ofthe enlarged gland (the static component) and thetone of the smooth muscle of the prostate stroma(the dynamic component).2 Storage symptoms,however, have been more closely associated withthe bladder dysfunction produced secondary tothe increased outflow resistance, arising fromprostate-dependent urethral obstruction. Theprecise interrelationship between morphologicBPH, bladder outflow obstruction, and profile of
symptoms produced is, however, unclear3 andthere are several paradoxes. In particular, bothvoiding and storage symptoms are common inwomen.3,4 Furthermore, many patients who haveundergone prostatectomy to relieve obstructionstill experience persistent storage symptoms.Several studies have also now shown that there islittle or no correlation between drug-inducedchanges in flow and symptom improvement5,6.The use of LUTS as a clinical descriptor is a neu-tral way to describe the symptoms, and makes noassumption about their link to the prostate.
On the basis of our knowledge of the controlof periurethral, stromal prostate smooth muscletone it is logical to assume that prostate α-adreno-ceptors should be responsible for at least part ofthe LUTS associated with BPH (Figure 12.1).However, the welldocumented beneficial effects
FIGURE 12.1 Sympathetic innervation of the human prostate showing the location of α1- and α2-adrenoceptors.
185
Ch 12 13/5/05 3:37 pm Page 185

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA186
of α1-adrenoceptor antagonists on the symptomsof BPH7–11 occur even in the absence of outflowobstruction. This indicates that extraprostatic α1-adrenoceptors may also be fundamentallyinvolved in the pathogenesis of LUTS.10 The lackof correlation between α-antagonist-inducedimprovements in urine flow and symptomimprovement6,12 could also be explained on thebasis of an action via extraprostatic α1-adrenocep-tors (Figure 12.1).
The extraprostatic α1-adrenoceptors may belocated in the bladder, ganglia, and nerves inner-vating the lower urinary tract and at spinal orsupraspinal levels within the central nervous sys-tem. Indeed, there is evidence for involvement ofα1-adrenoceptors in the spinal control of bothsympathetic and somatic (filling), as well as para-sympathetic (voiding), efferent activity of thelower urinary tract.10,13
In approximately 10% of patients, the use ofα1-adrenoceptor antagonists in common clinicaluse (alfuzosin, doxazosin, tamsulosin, terazosin)has been limited by side-effects, particularlydizziness, headache, asthenia, nasal congestion,and orthostatic hypotension, that may be attrib-uted to action on nonprostatic α1-adrenoceptors.It is likely that most of the common side-effectsare characteristic of a direct action on the vascula-ture. To circumvent these side-effects, the phar-maceutical industry has attempted to find α1-adrenoceptor antagonists that are selective for theprostate α1-adrenoceptors. The underlyingassumption is that these should be ‘uroselective’agents. It should be noted, however, that the def-inition of uroselectivity is ambiguous because thecriteria were not established at the outset. Notsurprisingly, therefore, the term has been used invarious contexts which are often confusing andcontradictory. In this chapter we attempt to putsome degree of definition on the criteria to be
used in the definitive designation of a drug asuroselective as it relates to management of thepatient with LUTS/BPH.
In theory, the selectivity of drugs can bedefined using a variety of parameters, includingpharmacologic or physiologic uroselectivity, ormay be defined from a clinical perspective.9,14
Ultimately, however, only clinical uroselectivity isrelevant to patient and physician.
PHARMACOLOGIC UROSELECTIVITY
α1-Adrenoceptors
Multiple α1-adrenoceptor subtypes have beenidentified,15–17 and may offer the opportunity totarget the prostate selectively. Receptor cloningand pharmacologic studies of the human prostatehave revealed the existence of both high-affinity(α1A, α1B, and α1D) and low-affinity (α1L) recep-tors for prazosin.
α1-Adrenoceptors in the prostate
Nerves that contain adrenergic, cholinergic, andnonadrenergic, noncholinergic neurotransmittersor mediator-producing enzymes supply thesmooth muscles of the prostate capsule and thetrabecular tissue around the ducts.18,19 The adren-ergic nerves are considered to be responsible forprostate smooth muscle tone by releasing nora-drenaline, which stimulates contraction via α-adrenoceptors.20 Although both α1- and α2-adrenoceptors can be identified in the humanprostate, the contractile effects of noradrenalineare mediated primarily by α1-adrenoceptors.10
All three high-affinity α1-adrenoceptor sub-types have been identified in prostate stromal tis-sue using molecular techniques. The α1a subtypepredominates, representing 60–85% of the
Ch 12 13/5/05 3:37 pm Page 186

UROSELECTIVITY REVISITED 187
α1adrenoceptor population. However, the α1-adrenoceptor subtype responsible for prostaticsmooth muscle contraction has not been estab-lished unequivocally, although it is likely to beclosely related to the α1A-adrenoceptor.
α1-Adrenoceptors in the urethra
Urodynamic studies in humans have suggestedthat up to about 50% of intraurethral pressure ismaintained by stimulation of α-adrenoceptors, asjudged from results obtained with α1-adrenocep-tor antagonists.21,22 In human male urethralsmooth muscle, functional and receptor-bindingstudies have suggested that the predominatingpostjunctional α-adrenoceptor is α1.
23,24 UsingRNase protection assays and in situ hybridiza-tion, Nasu et al.25 quantified and studied the dis-tribution of α1-adrenoceptor subtypes in thehuman proximal urethra. They found (in bothmales and females) that mRNA for the α1a sub-type was predominant; the ratio of mRNA forα1a, α1b, α1d in the male urethra was 100 : 0 : 0.Fukasawa et al.26 found that in man the α1L-adrenoreceptor subtype was more prominent inthe male urethra than in the prostate.
α1-Adrenoceptors in the bladder
In detrusor muscle from most species, includinghumans, β-adrenoceptors, which mediate relax-ation, normally dominate over α-adrenoceptors,which mediate contraction; the normal responseto noradrenaline is β-adrenoceptor-mediatedrelaxation. However, this may change in outflowobstruction. Perlberg and Caine27 assessed theresponse to noradrenaline in the hypertrophicbladder and found that, in strips taken fromhypertrophic bladders, noradrenaline caused α-adrenoceptor-mediated contraction in almostone-quarter of patients. This change was also
reflected in the symptoms: patients whose blad-ders responded to noradrenaline by contractinghad symptoms of bladder overactivity. Thisobservation suggests that a change in the responseto noradrenaline may play a role in producingboth obstructive and irritative symptoms.However, Smith and Chapple28 studied α1-adrenoceptor function in strips from obstructedbladders and found that only five of 72 stripsresponded to phenylephrine; these results are notin agreement with the view that α-adrenoceptorstimulation during storage contributes to bladdercontraction and thereby to symptoms. Most prob-ably, the balance between β- and α-adrenoceptorfunctions in the bladder changes in BPH, but it isnot known what this really means for the patho-physiology of LUTS, particularly storage symp-toms.
The predominating postjunctional α-adreno-ceptor subtype in the human lower urinary tractseems to be α1; however, the number of α1-adrenoceptors in the detrusor is very low.29 Innormal human isolated detrusor muscle, drugsthat selectively stimulate isolated α-adrenocep-tors, particularly those acting on α1-adrenocep-tors, produce a small and variable contractileeffect.23 It is not clear which α1-adrenoceptor sub-type predominates in the detrusor, trigone, andbladder base.
Walden et al.30 reported a predominance ofα1a-adrenoceptor mRNA in the human bladderdome, trigone and bladder base. This contrastswith the findings of Malloy et al.,31 who foundthat among the high-affinity receptors for pra-zosin, only α1a- and α1d-adrenoceptor mRNAwas expressed in the human bladder. The total α1-adrenoceptor expression was low(6.3 ± 1.0 femtomol/mg), but was highly repro-ducible. The relationship between the differentsubtypes was 66% α1d and 34% α1a; α1b was not
Ch 12 13/5/05 3:37 pm Page 187

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA188
expressed. This is in contrast to findings in thehuman prostate.32 The fact that drugs that actselectively on prostate α1-adrenoceptors mayhave little effect on LUTS could, in theory, beexplained if they did not block the α1-adrenocep-tors (α1D) of the bladder.33 Considering thedoubtful functional importance of the bladderα1-adrenoceptors, this mechanism seems unlike-ly, but cannot be discounted completely.
α1-Adrenoceptors in peripheral and centralnervous system structures (Figure 12.2)
In animal experiments, facilitatory α1-adrenocep-tors have been identified in ganglia and oncholinergic terminals in the bladder.34–37 Aneffect of α1-adrenoceptor antagonists at the gan-glionic and/or prejunctional level, leading to adecrease in acetylcholine release, is also possible.
Descending spinal pathways involved in mic-turition include noradrenaline-containing projec-tions from the locus coeruleus.38 From the locuscoeruleus, the noradrenergic neurones supplysympathetic and parasympathetic nuclei in thelumbosacral spinal cord. Bladder activationthrough these bulbospinal noradrenergic path-ways may well involve excitatory α1-adrenocep-tors.39 Thus, in the anesthetized cat, electricalstimulation of the locus coeruleus induced blad-der contractions that were antagonized byintrathecal administration of prazosin.39–42 Inaddition, destruction of noradrenergic cell bodiesin the locus coeruleus by microinjection of 6-hydroxydopamine produced a hypoactive blad-der, which could be partly reversed by intrathecalinjection of prazosin or phentolamine in cats,depressed the external urethral sphincter activity,and reduced reflex firing in pudendal nerve effer-ent pathways by a presumed central site ofaction.43 In the conscious cat, however, Downie etal.44 found that the intrathecal prazosin did not
alter the micturition reflex. The reasons for theseapparently conflicting results are unclear, butmost of the evidence supports a key central rolefor central α1-adrenoceptors.
Pontine micturition center
Cortex
Hypogastric nerve
Sacral micturition center (S2–S4)
Lumbar cord(T10–L2)
Bladder afferent
Pelvic nerve
Detrusor
Urethra
Pelvic floor Pudendal nerve
FIGURE 12.2 The micturition reflex. The afferentbranch of the micturition reflex runs in the spinal cord viathe dorsal root ganglia to the pontine micturition center,which is under voluntary control. The efferent branchruns from the pontine micturition center to the sacralmicturition center, from which the preganglionic nervesrun to the pelvic plexus and then to the bladder to causecontraction. At the same time, the efferent branch inhibitsthe hypogastric and pudendal nerves, leading to relax-ation of the outflow region and the pelvic floor.
Ch 12 13/5/05 3:38 pm Page 188

UROSELECTIVITY REVISITED 189
In the central nervous system, facilitatory α1-adrenoceptors, tonically active in both the sympa-thetic and somatic neural control of the lower uri-nary tract, were identified in the cat.45,46
Intrathecal doxazosin decreased micturition pres-sure, both in normal rats and in animals with pos-tobstruction bladder hypertrophy.47 The effectwas much more pronounced in the animals withhypertrophied/overactive bladders. Doxazosindid not markedly affect the frequency or ampli-tude of the unstable contractions observed in ratswith obstructed bladders. It was suggested thatdoxazosin may have an action at the level of thespinal cord and ganglia, thereby reducing activityin the parasympathetic nerves to the bladder, andthat this effect was more pronounced in rats withbladder hypertrophy than in normal rats.47
Urodynamic studies revealed that sponta-neously hypertensive rats (SHRs) have pro-nounced bladder overactivity.48 These animalsalso have an increased noradrenergic bladderinnervation and an increased voiding frequency.49
Whereas the control rats (Wistar Kyoto rats) havea regular contraction frequency during continu-ous cystometry, the SHRs show both micturitionand nonmicturition contractions. To investigatewhether the peripheral adrenergic system wasinvolved in the pathogenesis of the bladder over-activity, SHRs were treated with 6-hydroxy-dopamine in order to destroy the noradrenergicnerves chemically. Under these conditions, blad-der overactivity was maintained (as demonstratedby continuous cystometry).50 Furthermore, α1-adrenoceptor antagonists, injected intra-arteriallynear the bladder, did not abolish the bladderoveractivity. On the other hand, when givenintrathecally, the same dose of α1-adrenoceptorantagonist normalized micturition. Although therelevance of these findings to man is not known,it is probable that spinal α1-adrenoceptors may
contribute to the overall clinical improvement inLUTS seen with α1-adrenoceptor antagonists.
The neuronal localization of α1-adrenoceptorsubtypes (α1a, α1b, α1d) in the human spinal cordwas investigated.51 In situ hybridization studiesrevealed that α1-adrenoceptor mRNA was pres-ent in ventral gray matter only (ventral > dorsal;sacral > lumbar = thoracic > cervical). Signalingcell bodies were detected in anterior horn motorneurones at all levels, in the dorsal nucleus ofClark, and in intermediolateral columns in cervi-cal enlargement, in thoracic and lumbar spinalcord regions, and in the parasympathetic nucleusin the sacral spinal cord. Although all three high-affinity α1-adrenoceptor subtypes were presentthroughout the human spinal cord, α1d-adreno-ceptor mRNA predominated. Whether this hasany clinical significance in the treatment ofLUTS remains to be established. It is pertinent,however, to note that the distribution of α1-adrenoceptor mRNA subtypes in the rat spinalcord is different from that in humans;52 thisshould be borne in mind when discussing theclinical relevance of data obtained in rats.
Overall, there is good evidence in severalspecies that α1-adrenoceptors at spinal andsupraspinal levels can profoundly influence themicturition reflex. The possibility that they maycontribute to the overall clinical improvement inLUTS cannot be discounted.
α1-Adrenoceptors in the cardiovascular system
The involvement of α1-adrenoceptor subtypes invascular control is of particular relevance to anydiscussion of uroselectivity. Species- and vessel-dependent α1A-, α1B-, α1D-, and α1L-adrenocep-tors all seem to subserve the contractile responsein vascular tissue.53–57 On this basis, one couldassume that cardiovascular homeostasis dependson all of the different subtypes, albeit to varying
Ch 12 13/5/05 3:38 pm Page 189

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA190
extents. Equally, no one α1-adrenoceptor subtypecan be considered to be the ‘blood pressureadrenoceptor’.
Summary of pharmacologic uroselectivity
There is good evidence to suggest that an agentselective for the α1A-adrenoceptor subtype willinfluence periurethral smooth muscle tone, ure-thral resistance, and thereby urinary flow.However, there is some degree of uncertainty asto whether the use of α1A-adrenoceptor antago-nists would improve symptoms. Indeed, shouldan extraprostatic action on the other subtypes berequired to optimize symptom improvement, anα1A-adrenoceptor-selective antagonist may havelower efficacy than existing agents. Equally, a
selective action at α1A-adrenoceptors may notnecessarily translate into a reduction in cardiovas-cular side-effects. Thus, although several agentswith considerable pharmacologic (α1A-adreno-ceptor) ‘uroselectivity’ have been synthesized,58,59
there is no guarantee that this will translate intoclinical benefit.
PHYSIOLOGIC UROSELECTIVITY
Obviously the response in the whole animal and,indeed, in man represents an integrated responsethat is much more complicated than can be pre-dicted from analysis at the pharmacologic orreceptor level in isolation. In the whole animal,homeostatic mechanisms tend to counteract
TABLE 12.1 Binding affinities (pKI) for compounds at cloned human α1-adrenoceptors.
Affinities were determined by displacement of 0.2 nM [3H]prazosin from rat-1 fibroblasts stably expressing cloned α1-adrenoceptor subtypes by 12 concentrations of competing drug. Values represent mean ± SEM for three to five separatedeterminations. Hill slopes for displacement curves were not significantly different from unity. (Data from reference 67with permission.)
pKI
Compound α1A α1B α1D
BMY 7378 6.2 ± 0.10 6.7 ± 0.11 8.2 ± 0.10
Prazosin 9.7 ± 0.20 9.6 ± 0.14 9.5 ± 0.10
Doxazosin 8.5 ± 0.20 9.0 ± 0.20 8.4 ± 0.12
WB 4101 9.3 ± 0.10 8.2 ± 0.16 9.2 ± 0.06
5-Methylurapidil 8.5 ± 0.09 6.8 ± 0.13 7.8 ± 0.09
Tamsulosin 10.3 ± 0.21 9.5 ± 0.17 10.1 ± 0.22
Phentolamine 8.1 ± 0.09 7.1 ± 0.15 7.8 ± 0.03
SNAP 1069 7.8 ± 0.19 7.6 ± 0.18 6.8 ± 0.20
Indoramin 8.3 ± 0.03 8.0 ± 0.12 7.3 ± 0.15
Alfuzosin 8.0 ± 0.20 8.0 ± 0.13 8.5 ± 0.07
Spiperone 7.6 ± 0.12 8.5 ± 0.16 8.1 ± 0.03
Terazosin 8.6 ± 0.22 8.7 ± 0.08 8.3 ± 0.13
Ch 12 13/5/05 3:38 pm Page 190

UROSELECTIVITY REVISITED 191
many of the effects produced by any drug,particularly under normal conditions. However,in disease or in situations of abnormal pathophys-iology, homeostatic compensation may haveoccurred to the maximum extent. Thus, theresponse to the drug under these conditions maybe substantially different—either exaggerated orattenuated.
In terms of LUTS and in the context of uros-electivity, an agent that decreases outflow resist-ance without affecting the blood pressure wouldobviously be of considerable interest. Manygroups have reported that α1-adrenoceptorantagonists decrease urethral resistance in animalmodels.60–66 Indeed, such animal models are usedroutinely within the pharmaceutical industry todetermine the relative potency and selectivity ofα1-adrenoceptor antagonists for prostate functionover other parameters such as blood-pressurelowering. The rank order of potency of the effectsof various α1-adrenoceptor antagonists on ure-thral pressure has been defined in several animalmodels, and has then been related to blood pres-sure changes in the same animal.11,65 The ratio ofthese effects could therefore be considered as apotential index of uroselectivity. Although suchmodels may have some predictive value, they alsohave limitations, and the results may be bothspecies- and assay-dependent.67,68 Thus, resultsobtained in one animal species may differ fromthose obtained in another, and it has not beenestablished which animal model is the most pre-dictive of effects in humans.
Side-effects that may be dose limiting clinical-ly are not always cardiovascular (or directly relat-ed to hemodynamic changes), but may arise fromthe central nervous system, for example drowsi-ness and dizziness. Also, because such effects can-not always be studied in animals, animal modelsmay not adequately predict benefit–risk profiles
or provide a reliable index of clinical uroselectiv-ity as it would impact on patient management.The use of animal models has, however, pro-duced encouraging results. All establishedagents—alfuzosin, doxazosin, prazosin, tamsu-losin, and terazosin—affect urethral pressure inanimals over the same dose range that producesvascular effects (see Table 12.1 and Figure 12.3).The relative lack of uroselectivity seen in whole-animal studies is entirely consistent with thereceptor-binding profile of these α1-adrenoceptorantagonists (i.e. the pharmacologic ‘uroselectivi-ty’, as defined by the selectivity for the α1A-adrenoceptor subtype over the other subtypes)(Figure 12.3). Thus, none of these agents can beconsidered to demonstrate significant physiologicuroselectivity in the whole animal. Although it ispossible to carry out similar evaluations inman,69,70 ultimately we need to define clinicaluroselectivity9,71.
CLINICAL UROSELECTIVITY
A clinically relevant definition of uroselectivitycan be made only in relation to man. It is knownthat α1-adrenoceptor antagonists have more pro-nounced effects on blood pressure in hypertensivepatients than in normotensive patients. For exam-ple, it is well documented that doxazosin and ter-azosin effectively reduce blood pressure in hyper-tensive BPH patients but have only relativelymodest effects in normotensive men (Figure12.4).72,73 Assuming that this occurs at doses thataffect urinary flow, both drugs could be consid-ered to demonstrate clinical uroselectivity, at leastin normotensive BPH patients. Ironically, howev-er, using this definition neither agent would beclassified as uroselective in hypertensive BPHpatients. The blood pressure-lowering effect is of
Ch 12 13/5/05 3:38 pm Page 191

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA192
benefit in the large number of BPH patients whoare hypertensive. Thus, in theory, a drug couldaffect blood pressure in a hypertensive subjectbefore it has any noticeable effects on the urethra(i.e. the drug has no uroselectivity or indeed hasvascular selectivity). The same drug may reduceoutflow resistance in a normotensive patient butwithout having any effects on blood pressure (i.e.the drug is uroselective in this situation). The sit-uation is complicated further by the fact thatpharmacokinetic properties may contribute toapparent differences between drugs in the effectson different organ systems.
In the context of managing patients withBPH, it is therefore both obvious and essential tohave an all-encompassing but precise definitionof clinical uroselectivity. This has to take intoaccount the fact that the clinical endpoints of out-flow obstruction (as defined urodynamically) andLUTS, and adverse effects may vary independ-
ently. Thus, uroselectivity (as for any clinicaltherapeutic index) may be defined by describingthe ratio between the dose required for thedesired therapeutic action and the dose that pro-duces side-effects. Such a definition of uroselec-tivity is the one recommended in 1995 by theFourth international consultation on benign pro-static hyperplasia: ‘desired effects on obstructionand lower urinary tract symptoms related toadverse effects’.9 It should be noted that clinicaluroselectivity defined in this way is not an all-or-nothing phenomenon but is merely a qualitativedescriptor.
The clinical definition should be borne inmind when considering the profiles described forthe α1-adrenoceptor antagonists. It is obviousthat, although animal studies have greatlyincreased our understanding of the control of thelower urinary tract, they may be of relatively littlevalue in the prediction of clinical uroselectivity.
7.0
7.5
8.0
8.5
9.0
9.5
7.0
7.5
8.0
8.5
9.0
Low
Affinity
High
alpha 1A alpha 1B alpha 1D Prostate pressure Blood pressure
Dox Ter Alf Tam 5-MU Dox Ter Alf Tam 5-MU
pKi
Pse
udo
pA2
(a) (b)
FIGURE 12.3 (a) Selectivity profile of doxazosin (Dox), terazosin (Ter), alfuzosin (Alf), tamsulosin (Tam), and 5-methylurapidil (5-MU)for the cloned α1A-, α1B, and α1D-adrenoceptor subtypes. 5-MU is the only compound that showsselectivity for the cloned human α1A-adrenoceptor. (b) Selectivity profile of the same compounds in the anesthetized dog.All compounds are equi-active on prostate pressure and blood pressure, except the α1A-selective 5-MU, which is about 30-fold prostate selective.
Ch 12 13/5/05 3:38 pm Page 192

UROSELECTIVITY REVISITED 193
CONCLUSIONS
A drug may be uroselective in the sense that it hasa preference for the α-adrenoceptors in theprostate, or that in an animal model it can affectthe prostate and urethra without affecting bloodpressure, for example. There are α1-adrenocep-tors in the urethra, trigone, detrusor, spinal cord,supraspinal structures, and peripheral ganglia,the contributions of which to the symptoms ofBPH remain unknown, and whose subtypes havenot been determined. Thus, such a definition ofuroselectivity may not be meaningful from a clin-ical point of view. A clinically meaningful defini-tion of uroselectivity can be made only withrespect to findings in man, and considers desiredeffects on obstruction and LUTS relative toadverse effects. Clinical uroselectivity can be usedas a guideline for selecting drugs for the manage-ment of BPH that are cost-effective and safe, andwhich can improve the individual patient’s quali-ty of life. It is possible, however, that the pharma-ceutical industry may have exhausted both thepharmacologic and pharmacokinetic options forachieving uroselectivity74.
REFERENCES
1. Abrams P. New words for old; urinary tract symp-toms for ‘prostatism’. Br Med J 1994; 308: 929–930
2. Caine M. The present role of alpha-adrenergicblockers in the treatment of benign prostatic hyper-trophy. J Urol 1986; 136: 1–4
3. Shapiro E, Lepo H. Pathophysiology of clinicalbenign prostatic hyperplasia. Urol Clin North Am1995; 22: 285–290
4. Jollys J V, Jollys J C, Wilson J et al. Does sexualequality extend to urinary symptoms? NeurourolUrodyn 1993; 12: 391–392
5. Lepor H, Machi G. Comparison of the AUA symp-tom index in unselected males and females between55 and 79 years of age. Urology 1993; 42: 36–40
6. Barry M J, Cockett A T K, Holtgrewe H L et al.Relationship of symptoms of prostatism to com-monly used physiological measures of the severityof benign prostatic hyperplasia. J Urol 1993; 150:351–358
7. Eri L M, Tveter K J. α-Blockade in the treatmentof symptomatic benign prostatic hyperplasia. J Urol1995; 154: 923–934
8. Chapple C R. Selective α1-adrenoceptor antago-nists in benign prostatic hyperplasia: rationale andclinical experience. Eur Urol 1996; 29: 129–144
170
160
150
140
130
120
110
100
90
80
70
Baseline Treatment
Terazosin Placebo Terazosin Placebo
Hypertensive Normotensive
Blo
od p
ress
ure
(mm
Hg)
FIGURE 12.4 Effect of terazosin on blood pressure in hypertensive and normotensive patients. Data show blood pres-sure at baseline and after treatment. (Adapted from reference 70.)
Ch 12 13/5/05 3:38 pm Page 193
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA194
9. Jardin A, Andersson K -E, Bono V A et al. Alpha-blockers in the treatment of BPH. In: Denis L,Griffiths K, Khoury S et al. (eds). Proceedings ofthe fourth international consultation on benignprostatic hyperplasia (BPH). Plymouth: SCI, 1998:599–632
10. Andersson K -E, Lepor H, Wyllie M G. Prostaticα1-adrenoceptors and uroselectivity. Prostate 1997;30: 202–215
11. Djavan B, Marberger M. A meta-analysis on theefficacy and tolerability of α1-adrenoceptor antago-nists in patients with lower urinary tract symptomssuggestive of benign prostatic obstruction. EurUrol 1999; 36: 1–13
12. Gerber G S, Contreras BA, Zagaja G P et al.Doxazosin in men with lower urinary tract symp-toms: urodynamic evaluation at 15 months.Urology 1997; 50: 229–233
13. Andersson K -E. α1-Adrenoceptors and bladderfunction. Eur Urol 1999; 36 (Suppl 1): 96–102
14. Andersson K -E. The concept of uroselectivity. EurUrol 1998; 33 (Suppl 2): 7–11
15. Hieble J P, Bylund D B, Clarke D E et al.International Union of Pharmacology. Recom-mendation for nomenclature of α1-adrenoceptors:consensus update. Pharmacol Rev 1995; 47:267–270
16. Langer S Z. History and nomenclature of α1-adrenoceptors. Eur Urol 1999; 36 (Suppl 1): 2–6
17. Zhong M, Minneman K P. α1-Adrenoceptor sub-types. Eur J Pharmacol 1999; 375: 261–276
18. Dail W G. Autonomic innervation of male repro-ductive genitalia. In: Maggi C A (ed). NervousControl of Urogenital System. London: HarwoodAcademic Publishers, 1993: 69–101
19. Hedlund P, Ekström P, Larsson B et al. Heme oxy-genase and NO-synthase in the human prostate—relation to adrenergic, cholinergic and peptide-con-taining nerves. J Auton Nerv Syst 1997; 63: 115–126
20. Caine M, Raz S, Zeigler M. Adrenergic and cholin-ergic receptors in the human prostate capsule andbladder neck. Br J Urol 1975; 47: 193–202
21. Appell R A, England H R, Hussell A R, McGuireE J. The effect of epidural anesthesia on the ure-
thral closure pressure profile in patients with pro-static enlargement. J Urol 1980; 124: 410–411
22. Furuya S, Kumamoto Y, Yokoyama E et al. Alpha-adrenergic activity and urethral pressure in prosta-tic zone in benign prostatic hypertrophy. J Urol1982; 128: 836–839
23. Andersson K -E. Pharmacology of lower urinarytract smooth muscles and penile erectile tissues.Pharmacol Rev 1993; 45: 253–308
24. Hatano A, Takahashi H, Tamaki M et al.Pharmacological evidence of distinct α1-adreno-ceptor subtypes mediating the contraction ofhuman prostatic urethra and peripheral artery. Br JUrol 1994; 113: 723–728
25. Nasu K, Moriyama N, Fukasawa R et al.Quantification and distribution of alpha 1-adreno-ceptor subtype mRNAs in human proximal ure-thra. Br J Pharmacol 1998; 123: 1289–1293
26. Fukasawa R, Taniguchi N, Moriyama N et al. Thealpha1L-adrenoceptor subtype in the lower urinarytract: a comparison of human urethra and prostate.Br J Urol 1998; 82: 733–737
27. Perlberg S, Caine M. Adrenergic response of blad-der muscle in prostatic obstruction. Urology 1982;20: 524–537
28. Smith D J, Chapple C R. In vitro response ofhuman bladder smooth muscle in unstableobstructed male bladders: a study of pathophysio-logical causes. Neurourol Urodyn 1994; 13:414–415
29. Goepel M, Wittmann A, Rübben H, Michel M C.Comparison of adrenoceptor subtype expression inporcine and human bladder and prostate. Urol Res1997; 25: 199–206
30. Walden P, Durkin M, Lepor H et al. Localizationof mRNA and receptor binding sites for the α1a-adrenoceptor in the rat, monkey and human uri-nary bladder and prostate. J Urol 1997; 157:1032–1038
31. Malloy B J, Price D T, Price R R et al. Alpha1-adrenergic receptor subtypes in human detrusor. JUrol 1998; 160: 937–943
32. Nasu K, Moriyama N, Kawabe K et al.Quantification and distribution of alpha1-adreno-
Ch 12 13/5/05 3:38 pm Page 194

UROSELECTIVITY REVISITED 195
ceptor subtype mRNAs in human prostate: com-parison of benign hypertrophied tissue and non-hypertrophied tissue. Br J Pharmacol 1996; 119:797–803
33. Schwinn D A, Price R R. Molecular pharmacologyof human α1-adrenergic receptors: unique featuresof the α1a-subtype. Eur Urol 1999; 36 (Suppl 1):7–10
34. de Groat W C, Booth A M. Inhibition and facilita-tion in parasympathetic ganglia. Fed Proc 1980; 39:2290–2996
35. Akasu T, Gallagher J P, Nakamura T et al.Noradrenaline hyperpolarization and depolariza-tion in cat vesical parasympathetic neurones. JPhysiol 1985; 361: 165–184
36. Keast J R, Kawatani M, de Groat W C.Sympathetic modulation of cholinergic transmis-sion in cat vesical ganglia is mediated by α1- andα2-adrenoceptors. Am J Physiol 1990; 258:R44–R50
37. Somogyi G T, Tanowitz M, de Groat W C.Prejunctional facilitatory α1-adrenoceptors in therat urinary bladder. Br J Pharmacol 1995; 114:1710–1716
38. de Groat W C, Booth A M, Yoshimura N. Neuro-physiology of micturition and its modification inanimal models of human disease. In: Maggi C A(ed). London: Harwood Academic Publishers,1993: 227–289
39. Sasa M, Yoshimura N. Locus coeruleus noradren-ergic neurons as a micturition center. Microsc ResTech 1994; 29: 226–230
40. Yoshimura N, Sasa M, Ohno Y et al. Contraction ofurinary bladder by central norepinephrine origi-nating in the locus coeruleus. J Urol 1988; 139:423–427
41. Yoshimura N, Sasa M, Yoshida O, Takoaori S. α1-Adrenergic receptor-mediated excitation from thelocus coeruleus of the sacral parasympathetic pre-ganglionic neuron. Life Sci 1990; 47: 789–797
42. Yoshimura N, Sasa M, Yoshida O, Takaori S.Mediation of micturition reflex by central norepi-nephrine from locus coeruleus in the cat. J Urol1990; 143: 840–843
43. Gajewski J, Downie J W, Awad S A. Experimentalevidence for a central nervous system site of actionin the effect of alpha-adrenergic blockers on theexternal urinary sphincter. J Urol 1984; 132:403–409
44. Downie J W, Bialik G J, Shefchyk S J et al. Rolesfor sacral spinal alpha-adrenoceptors in mediatingor modulating bladder and sphincter activity in thecat. Neurourol Urodyn 1991; 10: 367–369
45. Danuser H, Thor K. Inhibition of central sympa-thetic and somatic outflow to the lower urinarytract of the cat by the α1-adrenergic receptor antag-onist prazosin. J Urol 1995; 153: 1308–1312
46. Ramage A G, Wyllie M G. A comparison of theeffects of doxazosin and terazosin on the sponta-neous sympathetic drive to the bladder and relatedorgans in anesthetized cats. Eur J Pharmacol 1995;294: 645–650
47. Ishizuka O, Persson K, Mattiasson A et al.Micturition in conscious rats with and without out-let obstruction: role of spinal α1-adrenoceptors. BrJ Pharmacol 1996; 117: 962–966
48. Persson K, Pandita R K, Spitsbergen J M et al.Spinal and peripheral mechanisms contributing tohyperactive voiding in spontaneously hypertensiverats. Am J Physiol 1998; 275: R1366–1373
49. Steers W D, Clemow D B, Persson K et al. Thespontaneously hypertensive rat: insight into thepathogenesis of irritative symptoms in benign pro-static hyperplasia and young anxious males. ExpPhysiol 1999; 84: 137–147
50. Pandita R K, Alm P, Steers W D et al. Hyperactivevoiding in spontaneously hypertensive rats is notaffected by chemical sympathectomy (abstract).International Bladder Symposium, WashingtonDC, 4–7 November 1999: 1005P
51. Smith M S, Schambra U B, Wilson K H et al.Alpha1-adrenergic receptors in human spinal cord:specific localized expression of mRNA encodingalpha1-adrenergic receptor subtypes at four distinctlevels. Brain Res Mol Brain Res 1999; 63: 254–261
52. Day H E, Campeau S, Watson S J Jr, Akil H.Distribution of alpha 1a-, alpha 1b- and alpha 1d-adrenergic receptor mRNA in the rat-brain andspinal cord. J Chem Neuroanat 1997; 13: 115–139
Ch 12 13/5/05 3:38 pm Page 195
THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA196
53. Hatano A, Takahashi H, Tamaki M et al.Pharmacological evidence of distinct α1-adreno-ceptor subtypes mediating the contraction ofhuman prostatic urethra and peripheral artery. Br JUrol 1994; 113: 723–728
54. Kohno Y, Saito H, Takita M et al. Heterogeneity ofα1-adrenoceptor subtypes involved in adrenergiccontractions of dog blood vessels. Br J Pharmacol1994; 112: 1167–1173
55. Kenny B A, Chalmers D H, Philpott P C, NaylorA M. Characterization of an α1D-adrenoceptormediating the contractile response of rat aorta tonoradrenaline. Br J Pharmacol 1995; 115: 981–986
56. Muramatsu I, Ohmura T, Hashimoto S, Oshita M.Functional subclassification of vascular α1-adreno-ceptors. Pharmacol Commun 1995; 6: 23–28
57. Vargas H M, Gorman A J. Vascular alpha-1 adren-ergic receptor subtypes in the regulation of arterialpressure. Life Sci 1995; 57: 2291–2308
58. Williams T J, Blue D R, Daniels D V et al. In vitroalpha 1-adrenoceptor pharmacology of Ro-70-0004and RS-100329; novel alpha 1A-adrenoceptorantagonists. Br J Pharmacol 1999; 127: 252–258
59. Lopez FJ, Arias L, Chan R et al. Synthesis, phar-macology and pharmacokinetics of 3-(4-aryl-piper-azin-1-ylalkyl)-uracils as uroselective alpha(1A)-antagonists. Bioorg Med Chem Lett 2003; 2:1873–1878
60. Imigawa J, Akima M, Saki K. In vivo experimentsfor the evaluation of α1-adrenoceptor antagonisticeffects of SGB-1534 on canine urethra. Eur JPharmacol 1989; 167: 167–172
61. Shibasaki M, Sudoh K, Inagaki O et al. Effect ofoptical isomers of YM-12617 on increased intra-urethral pressure induced by phenylephrine inanaesthetized dogs. J Autonom Pharmacol 1992;12: 263–268
62. Breslin D, Fields D W, Chow T C et al. Medicalmanagement of benign prostatic hyperplasia: acanine model comparing the in vivo efficacy ofalpha-1-adrenergic antagonists in the prostate. JUrol 1993; 149: 395–399
63. Lefevre-Borg F, O’Connor S E, Schoemaker H etal. Alfuzosin, a selective α1-adrenoceptor antago-
nist in the lower urinary tract. Br J Pharmacol1993; 109: 1282–1289
64. Kenny B A, Naylor A M, Carter A J et al. Effect ofalpha-adrenoceptor antagonists on prostatic pres-sure and blood pressure in the anaesthetized dog.Urology 1994; 44: 52–57
65. Martin D J, Lluel P, Guillot E et al. Comparativealpha-1 adrenoceptor subtype selectivity and func-tional uroselectivity of alpha-1 adrenoceptor antag-onists. J Pharmacol Exp Ther 1997; 282: 228–235
66. Akiyama K, Hora M, Tatemichi S et al. KMD-3213, a uroselective and long-acting alpha (1a)-adrenoceptor antagonist, tested in a novel ratmodel. Pharmacol Exp Ther 1999; 291: 81–91
67. Hieble J P, Kolpak D C, McCafferty G P et al.Effects of alpha1-adrenoceptor antagonists on ago-nist and tilt-induced changes in blood pressure:relationship to uroselectivity. Eur J Pharmacol1999; 373: 51–62
68. Walsh P C. Benign prostatic hyperplasia. In: WalshP C, Retik A B, Stamey T E, Vaughan E D Jr (eds).Campbell’s urology, 6th edn. Philadelphia:Saunders, 1992: 1009–1027
69. Sultana S R, Murray K, Craggs M D et al. Alpha1
adrenoceptor antagonist selectivity determined bysimultaneous blood pressure and long-term ure-thral pressure monitoring in men. Br J ClinPharmacol 1998; 45: 192
70. Wyllie M G. Alpha1-adrenoceptor selectivity: theNorth American experience. Eur Urol 1999; 36(Suppl 1): 59–63
71. Roehrborn C G. Are all alpha blockers createdequal? An update. Urology 2002; 59 (Suppl 2): 3–6
72. Kirby R S. Doxazosin in benign prostatic hyperpla-sia: effects on blood pressure and urinary flow innormotensive and hypertensive men. Urology1995; 46: 182–186
73. Lepor H and the Terazosin Research Group.Long-term efficacy and safety of terazosin inpatients with benign prostatic hyperplasia. Urology1995; 45: 406–413
74. Wyllie M G. Uroselectivity; end of the road? BJUInt 2003; 92: 141–142
Ch 12 13/5/05 3:38 pm Page 196

Index
adrenoceptors 185–91subtypes 92, 93, 103–4
adrenoceptor antagonists 91–2apoptosis induction 85–6blood pressure effects 193differential effects on prostate tissue growth
83–9physiologic uroselectivity 190–1, 192–3serum lipids 109vs watchful waiting 4–5
African plum tree (Pygeum africanum) 172–3ALFIN study 70–1, 77–8ALFORTI study, alfuzosin 128–9, 132ALFUS study, alfuzosin 129alfuzosin 119–37
acute urinary retention 123alpha-adrenoceptor affinity 119–20blood pressure 120, 122–4
vs tamsulosin 157–8clinical studies 125–31
ALFORTI 128–9, 132ALFUS 129
combination therapy, finasteride 129, 131, 133efficacy 126–34
vs placebo 27, 46formulation, comparisons 122hemodynamic effects 124–5pharmacodynamic effects 122–3pharmacokinetic properties 122pharmacologic profile 119prostate/plasma concentrations 122safety and adverse events 132, 133therapeutic applications 133–4urodynamic effects 123
urethral pressure 121vs tamsulosin 157–8
ALLHAT (Antihypertensive Lipid-LoweringTreatment to Prevent Heart Attack Trial)110
alpha-1 adrenoceptorsbinding affinities 186, 190in bladder 187–8in cardiovascular system 189–90contractile role 186and LUTS 93in peripheral and CNS structures 188–9pharmacologic uroselectivity 186–90in prostate 186–7subtypes 84in urethra 187
alpha-adrenoceptor antagonists 91–2with 5-alpha reductase inhibitor, MTOPS
trial 76–7apoptosis 85–6see also alfuzosin; doxazosin; tamsulosin:
terazocin5-alpha-reductase (5-AR) 42–3
deficiency, pseudohermaphroditism 4, 43types I and II 43type II see finasteride
5-alpha-reductase inhibitors (5-ARI)and alpha-blockers 48combination therapy 48DHT 41–2DHT reduction 47dual isoforms 43–4, 46phytotherapeutic agents 178see also dutasteride; finasteride
197
Index 13/5/05 3:38 pm Page 197

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA198
American dwarf palm (Serenoa repens) 76,168–72
American Urological Association (AUA)AUASI scale 26, 73bother score 6, 24combination therapy guidelines 77watchful waiting treatment guidelines 5–7
androgen ablation/deprivation 83angina, surgical procedures, placebo effects
17–18apoptosis, alpha-adrenoceptor antagonists 85–6
balloon dilatation vs cystoscopy, placebo/shamcontrolled trials 29–33
Baltimore longitudinal study of aging, watchfulwaiting 1–2
bladderalpha-1 adrenoceptors 187–8smooth muscle, alpha-blockers 83
bladder outlet obstruction (BOO) 185tolterodine/tamsulosin combination therapy
76watchful waiting 2
blood pressure effectsadrenoceptor antagonists 193alfuzosin 122–4, 120doxazosin 108–9tamsulosin 148
vs alfuzosin 157–8, 158vs terazosin 157–8
terazosin 96, 99BMY-7378, binding affinities 190bother score 6, 24Boyarsky symptom scores 145, 147, 154BPH (benign prostatic hyperplasia)
historical perspective 83–6natural history, placebo effects 18–34treatment preferences 5
bromocriptine, efficacy, vs placebo 27
cactus flower extracts 174candicin, efficacy, vs placebo 27cardiovascular system, alpha-1 adrenoceptors
189–90cernitin, combination therapy 76cimetidine, efficacy, vs placebo 27combination studies
ALFIN study 70–1MTOPS trial 72–6phytotherapy 76Veterans’ Affairs (VA) Cooperative Study
68–70confidence profile method (CPM), symptom
improvement 22controlled clinical trials, placebo/sham effect
14–16coronary heart disease (CHD), doxazosin 109–10Cucurbita pepo (pumpkin) 174cystoscopy vs balloon dilatation, placebo/sham
controlled trials 29–33
Declaration of Helsinki, rationale forplacebo/sham controlled trials 15
detrusor overactivity (DO),tolterodine/tamsulosin combination therapy76
DHT (dihydrotestosterone)5-alpha-reductase inhibitors (5-ARI) 47BPH development 41–2dual inhibition, dutasteride treatment 44formation 42
doxazosin 103–17affinity for adrenoceptor subtypes 93ALLHAT trial 110antihypertensive effects 108–9binding affinities 190efficacy 46with finasteride 5GITS formulation 112–13
adverse events 113
Index 13/5/05 3:38 pm Page 198
INDEX 199
HABIT 109HALT 110MTOPS 59, 72–6, 77–8, 106PREDICT 71–2, 77–8, 106prostate apoptosis effect 85–6safety and efficacy
adverse events 107–8long-term 84–5, 106safety profile 107short-term 104–5
sexual dysfunction 110–11TOMHS 109uroselectivity 192
drugs, meta-analyses 61, 161dutasteride 41–51
adverse events 46clinical experience 45–7combination studies 48preclinical development 44–5and PSA (prostate-specific antigen) 45, 47–8structure 44vs finasteride 47–8
ESPIRIT (European Standardized PressureFlow Investigation Trial) 148–9
FDA, rationale for placebo/sham controlledtrials 14–15
finasteride 53–66adverse events 58ALFIN study 70–1, 77–8clinical studies 56–9combination studies 59–61
with alfuzosin 129, 131, 133with alpha-adrenoceptors 5with doxazosin 5terazosin, interactions 60
development 54DHT and 5-alpha-reductase 53–4hematuria prevention 48, 61
meta-analysis 61mode of action 54MTOPS study 59–60, 72–6, 77–8PREDICT study 71–2, 77–8, 106PSA effects 62safety profile 133structure 54VA Cooperative Study 60vs dutasteride 47–8
France and Germany, phytotherapeutic agents 5
growth factorsDHT-receptor complex 42and finasteride 55
3H-prazosin, binding sites 120HABIT (Hypertension and BPH Intervention
study), doxazosin evaluation 109HALT (Hypertension and Lipid Trial),
doxazosin 110hematuria prevention, finasteride treatment 48,
61hermaphroditism, pseudohermaphroditism, 5-
AR deficiency 43hyperplasia, adrenoceptor antagonist differential
effects 83–7hypertension, TOMHS 109hyperthermia devices see TUMThypotension, tamsulosin 147, 149, 159, 161Hypoxis rooperi (South African star grass) 168
124I-HEAT, binding sites 120I-PSS (International Prostate Symptom Score)
26tamsulosin 149, 150–2
indoraminbinding affinities 190efficacy, and potency 92
Ki 67 immunostaining 85
Index 13/5/05 3:38 pm Page 199

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA200
lipids, alpha-blocker effects 109–10LUTS (lower urinary tract symptoms)
alpha-adrenoceptor antagonist therapy 93dutasteride treatment 45effects of alpha-1 adrenoceptors 93terazosin therapy 91–6watchful waiting prospective study 3
5-methylurapidilaffinity for adrenoceptor subtypes 93binding affinities 190uroselectivity 192
micturition reflex 188MTOPS (Medical Therapy of Prostatic
Symptoms) trial 59–60, 72–6, 77–8doxazosin 106
norprogesterone, efficacy, vs placebo 2, 27
Olmsted County Study of Urinary Symptomsand Health Status Among Men 19–21
orthostatic hypotension, tamsulosin 147, 149,159, 161
pain treatment, placebo effects 17patients
monitoring see watchful waitingtreatment preferences 5
peripheral NS, alpha-1 adrenoceptors 188–9phenoxybenzamine 103phentolamine, binding affinities 190phytotherapeutic agents 167–84
5-alpha-reductase inhibition 168–9active constituents 168combination preparations 174–5combination therapy 76France and Germany 5meta-analyses 175–7mode of action 169origin 167–8
phytosterols/beta-sitosterol 172Picea (spruce) 168Pinus (pine) 168placebo/sham effect 11–39
balloon dilatation vs cystoscopy studies 29–33biopsychosocial determinants 13controlled trials, cystoscopy vs balloon
dilatation 29–33definitions and theoretical considerations
11–13ethical considerations 15hyperthermia treatment studies 15–16, 29–32improvement perception 33–4long-term natural history of disease
progression 31–3medical treatment studies 24–9natural history studies 18–34, 31–3
regression to mean 19watchful waiting studies 21–4
Olmsted County study 19–21pain control 17phytotherapeutic agents, Serenoa repens 170quantitative symptom scores 30–3surgical procedure studies 17–18therapeutic theory 12watchful waiting studies 21–4
plants, phytotherapeutic agents 167–84PLESS (Proscar Long-term Efficacy and Safety
Study) 32–3, 56–8postvoid residual urine (PVR), treatment
indications 6prazosin
binding affinities 190efficacy, and potency 923H-prazosin, binding sites 120
PREDICT (Prospective European Doxazosinand Combination Therapy) study 71–2,77–8
finasteride 106terazosin 86–7
Index 13/5/05 3:38 pm Page 200

INDEX 201
prostate, innervation 185prostatic growth/development
cell proliferation control 86–7finasteride 54–6growth rate (40–79 y) 21
prostatic size/volumedoxazosin 111dutasteride 45, 77finasteride 56, 61, 77terazosin growth effects 97–8
prostatism, watchful waiting over 5 years 2–3PSA (prostate-specific antigen)
dutasteride treatment 45, 47–8and finasteride 62
pseudohermaphroditism, deficiency of 5-alpha-reductase 43
pumpkin (Cucurbita pepo) 174Pygeum africanum 172–3
rye (Secale cereale) 168, 173meta-analyses 175–7
Sabal serrulata (saw palmetto) see Serenoa repensSecale cereale (rye) 168, 173Serenoa repens (American dwarf palm) 168–72
cernitin, beta-sitosterol and vitamin Ecombination therapy 76
combination therapy 174–5meta-analyses 175
sexual function/dysfunctiondoxazosin 110–11dutasteride 46ejaculation abnormalities 147, 147–9MTOPS data 75–6tamsulosin 147–8
beta-sitosterolmeta-analysis 175–7phytotherapeutic agents 172Serenoa repens, cernitin and vitamin E
combination therapy 76
smooth muscle, alpha-blockers 83SNAP 1069
binding affinities 190efficacy, and potency 92
South African star grass (Hypoxis rooperi) 168spiperone, binding affinities 190spruce (Picea) 168stinging nettle (Urtica dioica) 173surgical procedures
placebo effects 17–18risk, MTOPS data 72–6
symptom improvement, confidence profilemethod (CPM) 22
tamsulosin 139–70adverse events 149affinity for adrenoceptor subtypes 93ancillary properties 162binding affinities 190blood pressure effects 148chemical structure 87clinical studies
direct comparative studies 155–9European phase II 142–3European phase III 143, 147European phase IV 148Japanese phase II 141–2, 144long-term 154–5US phase III 149–52
co-medication 159–60dosages and formulations 140–1, 158–9efficacy and tolerability 46, 146, 159–61, 160
vs placebo 28elderly patients 159–60ESPIRIT 148–9meta-analysis 161onset of action 143, 152previous treatment comparisons 161tolterodine combination therapy 76uroselectivity 192
Index 13/5/05 3:38 pm Page 201

THERAPEUTIC TREATMENT FOR BENIGN PROSTATIC HYPERPLASIA202
vs alfuzosin, blood pressure effects 157–8vs terazosin, blood pressure effects 157–8
terazosin 91–101affinity for adrenoceptor subtypes 93binding affinities 190blood pressure effects 96, 193cardiovascular risk factors 97chemical structure 87effects on urogenital tract 97efficacy 46
long-term 84–5, 93–4and potency 92short-term 93vs placebo 28
finasteride interactions 60historic background 92LUT obstruction 91–2prostate apoptosis effect 85–6prostate gland growth 97–8safety profile 95–6uroselectivity 192VA Cooperative Study 60
testosteronedutasteride treatment 47formation of DHT 42
tolterodine, tamsulosin combination therapy 76TOMHS (Treatment of Mild Hypertension
Study), doxazosin evaluation 109–11TUMT (transurethral microwave
thermotherapy)efficacy, vs sham control 29placebo/sham controlled trials 15–16, 29–32
TUNEL assay 85TURP (transurethral resection of prostate) 1
indications 4, 5–6vs conservative management 3WW, waiting list 3
urethra, alpha-1 adrenoceptors 187urethral pressure, alfuzosin 120–1urinary flow rate Qmax
and density of smooth muscle 91ESPIRIT study 148–9treatment indications 6
urinary retention, acutealfuzosin 123MTOPS data 74, 75
urinary tract symptoms see LUTSurodynamic studies, doxazosin 104–5urologists, treatment preferences 5uroselectivity 185–96
clinical, defined 191pharmacologic 186–90physiologic 190–1, 192–3summary 190
Urtica dioica (stinging nettle) 173
Veterans’ Affairs (VA) Cooperative Study 3–4baseline and 3-year follow-up 3–4terazosin 86–7terazosin vs finasteride 60, 68–70
vitamin E, beta-sitosterol, Serenoa repens andcernitin combination therapy 76
watchful waiting (WW, patient monitoring) 1–9placebo/sham effect 21–4strategy 6–7treatment indications 6vs medical therapy 6–7vs placebo, comparison of outcomes 25
WB-4101, binding affinities 190WHO, on placebo/sham control groups 16
YM-617 see tamsulosin
Index 13/5/05 3:38 pm Page 202