kiwanis care centre - bcpsqc – quality forum 2014
TRANSCRIPT
Kiwanis Care Centre (‘KCC’)
Francoise Laity, KCC Resident Care Coordinator [email protected]
Sara Gilbert, KCC Manager [email protected]
Designing and Implementing an
Effective Behavioral
Support Unit -
Special Care Unit (SCU) Plus

Kiwanis Care Centre
Background
2009:
“Vancouver Community Project: Model of Care Framework for Vancouver Coastal Health’s SCU’s”.
Pilot:
Fairhaven (Vancouver): Chronic Behavior Residential Unit (CBRU)
2010:
Need identified for North Vancouver and other Coastal regions.
What is the SCU Plus?
Purpose: To serve individuals with moderate to severe cognitive impairment and who face behavioral challenges
What is different?
Environment
Staffing
Approach
Project Overview
Project Initiation - November 2010
Planning/monitoring:
Research/Lit Review
Communication
Construction / equipment
Human Resources (Staff Changes)
Staff Education
Admission process/criteria
Resident Transition
Project Implementation –
March 31, 2011 (1st admission)
Education
Entire Facility
Lunch and Learn Dementia: what is it and what does it mean to me?
Personhood: Look at Me
Communication
Making a Difference:
Safe Work Practices when working with Individuals with dementia
2 Day Dementia Series
Non Violence Crisis Intervention Training
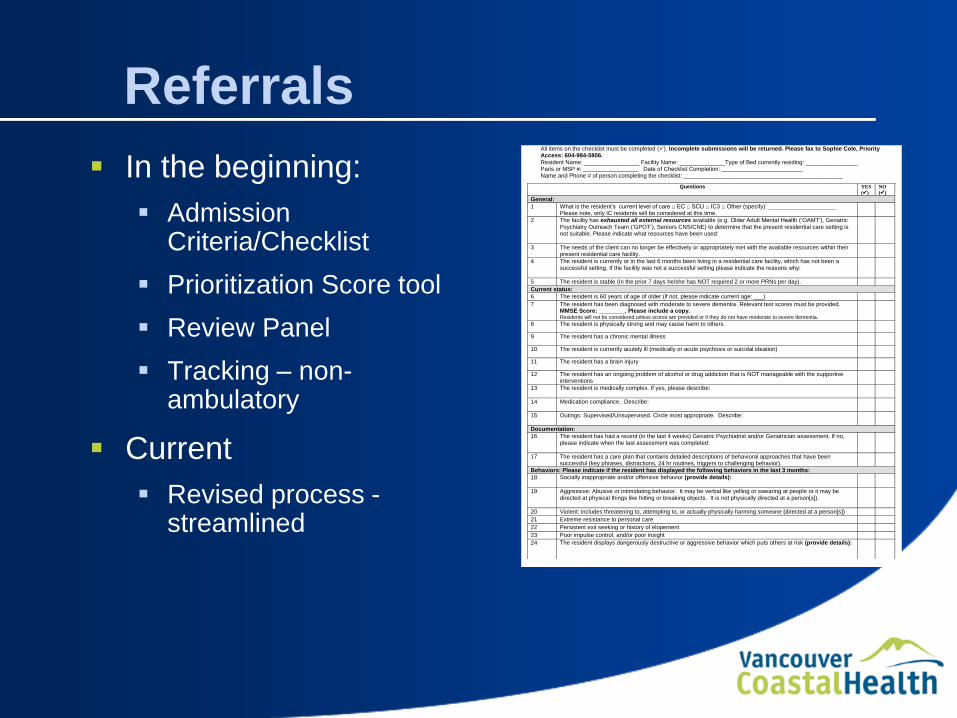
Referrals
In the beginning:
Admission Criteria/Checklist
Prioritization Score tool
Review Panel
Tracking – non-ambulatory
Current
Revised process - streamlined
Kiwanis Care Centre SCU Plus Admission Checklist All items on the checklist must be completed (). Incomplete submissions will be returned. Please fax to Sophie Cole, Priority Access: 604-984-5806.
Resident Name: _________________ Facility Name: ______________Type of Bed currently residing: ________________ Paris or MSP #: _________________ Date of Checklist Completion: _________________________ Name and Phone # of person completing the checklist: _________________________________________________
Questions YES
()
NO
()
General:
1 What is the resident’s current level of care □ EC □ SCU □ IC3 □ Other (specify): _____________________ Please note, only IC residents will be considered at this time.
2 The facility has exhausted all external resources available (e.g. Older Adult Mental Health (‘OAMT’), Geriatric Psychiatry Outreach Team (‘GPOT’), Seniors CNS/CNE) to determine that the present residential care setting is not suitable. Please indicate what resources have been used:
3 The needs of the client can no longer be effectively or appropriately met with the available resources within their present residential care facility.
4 The resident is currently or in the last 6 months been living in a residential care facility, which has not been a successful setting. If the facility was not a successful setting please indicate the reasons why:
5 The resident is stable (In the prior 7 days he/she has NOT required 2 or more PRNs per day). Current status:
6 The resident is 60 years of age of older (if not, please indicate current age: ___)
7 The resident has been diagnosed with moderate to severe dementia. Relevant test scores must be provided. MMSE Score: ________. Please include a copy. Residents will not be considered unless scores are provided or if they do not have moderate to severe dementia.
8 The resident is physically strong and may cause harm to others.
9 The resident has a chronic mental illness
10 The resident is currently acutely ill (medically or acute psychosis or suicidal ideation)
11 The resident has a brain injury
12 The resident has an ongoing problem of alcohol or drug addiction that is NOT manageable with the supportive interventions
13 The resident is medically complex. If yes, please describe:
14 Medication compliance. Describe:
15 Outings: Supervised/Unsupervised. Circle most appropriate. Describe:
Documentation:
16 The resident has had a recent (in the last 4 weeks) Geriatric Psychiatrist and/or Geriatrician assessment. If no, please indicate when the last assessment was completed:
17 The resident has a care plan that contains detailed descriptions of behavioral approaches that have been successful (key phrases, distractions, 24 hr routines, triggers to challenging behavior).
Behaviors: Please indicate if the resident has displayed the following behaviors in the last 3 months:
18 Socially inappropriate and/or offensive behavior (provide details):
19 Aggressive: Abusive or intimidating behavior. It may be verbal like yelling or swearing at people or it may be directed at physical things like hitting or breaking objects. It is not physically directed at a person[s]).
20 Violent: includes threatening to, attempting to, or actually physically harming someone (directed at a person[s])
21 Extreme resistance to personal care
22 Persistent exit seeking or history of elopement
23 Poor impulse control, and/or poor insight
24 The resident displays dangerously destructive or aggressive behavior which puts others at risk (provide details):
Environment/Care Planning
Social Worker/Resident Care Coordinator admission triage
RCC Visit
Care plan development
Partnerships:
Geripsychiatrist, OAMH, CNS, Priority Access, LGH (acute)
Medication review
Outcomes
Since initiation, only 1 hospital admit due to responsive behavior
Flow at KCC
Length of Stay
Affect on SCU (regular) wait time
Accreditation recognition (2011):
Kiwanis Care Centre staff and the seniors' team are commended for implementing a comprehensive new program including a secure yet home like environment for residents and extensive education and training for staff.
Lessons Learned
Project lessons
Communication, communication, communication
Staff implementation
Unit lessons:
Review panel
Staffing
Medication organization
Questions