know the messenger, history and basics: compliance rules
TRANSCRIPT

8/28/2020
1
History and Basics: Compliance Rules, Audits and
Requirements
Yvette Noel, CPCODirector of Education
KMC University
Know the Messenger, Hear the Message
Professional:• Director of Education for KMC University• Certified Professional Compliance Officer (CPCO)
• American Academy of Professional Coders (AAPC)• Currently Enrolled in Certified Practice Biller (CPB)
Certification• Served the Chiropractic Profession for 11 years• Served the Medical Community for 30 years• Public Speaker for different platforms
Personal:• Married to Stephen for 29 years• Proud Mother of 3 married children• Grandma to Norah• Dog mom to 2 rescues and 1 family dog• Piano player for 43 years, singer and songwriter
What is your name?What City is your
office located in?
What is the best
profession on the
planet that we are all
here for today?
The Common Ground
What We Will Cover!• Discuss History & Basics of
Compliance• Define and delineate between
Medically Necessary and Clinically Appropriate Care
• Learn the Medicare PART Process• Discovery the Components of
Documentation for Initial Assessment
• Understanding Payer Contracts regarding Compliance and policy
Let's be clear…• Compliance has been around for decades…not
new• Compliance got it start in 1992 when the General Accounting
Office (GAO) identified Medicare claims to be at high risk for fraud and abuse. So in 1996, the Office of Inspector General (OIG) initiated and audit of the Health Care Finance Administration (later named Centers for Medicare and Medicaid services (CMS) Medicare claims payment system. This resulted in an estimated finding of over $23 billion in improper payments.
•Made mandatory with Affordable Care Act•OIG•HIPAA
• The difference now, is auditors, insurance companies and the government are bothering to look!
6
1 2
3 4
5 6

8/28/2020
2
Why Does Compliance Matter?
•Every business has compliance-related activities
•We are scrutinized in healthcare more than in other industries
Types of Compliance
•OIG Compliance: Fraud, Waste and Abuse
•HIPAA Compliance
•OSHA Compliance
•Financial Compliance
•PCI Compliance
•CLIA Compliance• Multidisciplinary and certain tests
A Common Denominator
•All Compliance Includes
• Written Office policy
• Documented Procedures (SOP)
What is the Difference?•Policies
• Are general in nature• Identify company rules• Explain why they exist• Tell when the rule applies• Describe who it covers• Show how the rule is
enforced• Describe the
consequences• Are normally described
using simple sentences and paragraphs
•Procedures
• Identify specific actions
• Explain when to take actions
• Describe alternatives
• Show emergency procedures
• Include warnings and cautions
• Give examples
• Show how to complete forms
• Are normally written using an outline format
OIG Compliance
11
HIPAA Compliance
• Contains policies and procedures that relate to • The protection of the privacy of
Protected Health Information (PHI) • The security of the storage and
transmission of Electronic Protected Health Information
• Primarily concerns the privacy and security of the patient’s PHI
• Covers both paper and electronic forms of patient data
• Overseen by the Office of Civil Rights • Overseen by the Office of Inspector General
• Contains policies and procedures that relate to • The detection and prevention of fraud,
waste, and abuse within your office
• Primarily concerns documentation, coding, patient financial matters and billing
• Includes all federal, state and third-party payer regulations
12
• Under the guidance of the Department of Health and Human Services
• Policies and procedures must be customized to your practice
• Staff must be trained on the policies and procedures
• Policies and procedures must be reviewed annually to ensure they are still relevant and effective
• Staff must receive refresher training annually
7 8
9 10
11 12

8/28/2020
3
Your Passion is Also a Regulated Business
14
Who Is It?
Who is the OIG?
The Office of Inspector General's (OIG) mission is to protect the integrity of the Department of Health & Human Services (HHS) programs as well as the health and welfare of program beneficiaries.
16
The 8 Requirements of OIG Compliance
1. Policy and Procedure Install and Management
2. Choose Your Compliance Officer (CO)
3. Comprehensive Education and Training
4. Establish Disciplinary Guidelines
5. Internal Auditing and Monitoring
6. Respond Swiftly to Detected Offenses
7. Develop Open Lines of Communication
8. Avoiding Excluded Individuals
OIG Compliance Not Optional
•On October 5, 2000 the Compliance program was implemented for Individual and Small Group Physician Practices.
OCTOBER 2016
$359
The Collection Coach
million
13 14
15 16
17 18

8/28/2020
4
19
THE OUTLIERS ARE AUDITED AND MADE EXAMPLE
The Collection Coach
2013 2014 2015 2015
“Establish adequate policies and procedures
to ensure that chiropractic services billed to
Medicare are medically necessary, correctly
coded and adequately documented.”
AUGUST 2016
The Collection Coach
“Establish adequate policies and procedures
to ensure that chiropractic services billed to
Medicare are medically necessary, correctly
coded and adequately documented.”
92% error rate … Refund $339,625 The Collection Coach
DECEMBER 2017
The Collection Coach The Collection Coach
JANUARY 2018
19 20
21 22
23 24
8/28/2020
5
The Collection Coach
Who Told Them?
The Collection Coach
The Collection Coach
NO MORE WORK PLANS
Portfolios
25 26
27 28
29 30

8/28/2020
6
The Collection Coach
Chiropractic ServicesWhat does Medicare Part B cover?Medicare Part B covers medical and other health care services, including chiropractic services
How much does Medicare pay yearly for chiropractic services?
Since 2010, Medicare has paid more than $450 million per year for chiropractic services
What are the coverage rules for chiropractic services?Medicare covers reasonable and necessary chiropractic services provided by a qualified chiropractor to correct spinal subluxation by means of manual manipulation of the spine. Medicare does not cover chiropractic maintenance therapy. To receive payment from Medicare, a chiropractor must have documentation to support the services provided.
Is there a limit to the number of covered chiropractic services that a beneficiary may receive?Medicare does not limit the number of covered chiropractic services that a beneficiary may receive per month or per year. Many private insurance companies impose coverage limits
31 32
33 34
35 36

8/28/2020
7
Medicare Said It…
The Collection Coach
The More
You Do
the Higher
the Risk
UNDER THE MAGNIFYING GLASS
39
UNDER THE MAGNIFYING GLASS
40
UNDER THE MAGNIFYING GLASS
41 42
37 38
39 40
41 42

8/28/2020
8
False Claims Act Violations
•Establishes liability when any person or entity improperly receives from or avoids payment to the Feds•Prohibits “knowingly presenting or causing to be presented, a false claim for payment or approval
False Claims Act Violations
• Prohibits “knowingly presenting or causing to be presented, a false claim for payment or approval”• Examples:
•Waiving deductibles or co-payments and not reporting to carriers• Up-coding for higher
reimbursements• Down-coding based on
payer type
Know the Rules that
Govern Healthcare
Follow them to reduce
risk!!
Why Mandatory?
Integrate policies and procedures that are necessary to promote adherence to federal and state laws, statutes, and regulations applicable to the delivery of healthcare services into the physician’s practice
47
Policies and Procedures Address THESE Risks
43 44
45 46
47 48

8/28/2020
9
Avoid Dual Fee Schedules
What is and isn’t a dual fee schedule? Get the facts straight• Misrepresents charges to
carriers • False Claims Act violation• May violate provider
agreements
Compliant Time of Service DiscountsDiscount is based on viable bookkeeping savings•May or may not be
defined•Often not defensible
or unreasonable•May not be
permissible on Federally insured patients•Must be paid in full at
time of service
Other Types of Discounts
•ChiroHealth USA
•Hardship Policies
•Professional Courtesy
•Billing for Family Members
Inducement Violations•Per the OIG: “incentives that are only nominal in value are NOT prohibited by [inducement law]
•No more than $15 per item or $75 in the aggregate annually• Even one free
examination, x-ray, or therapy is a risk
52
Anti-Kickback ViolationsA person who offers or transfers to a Medicare or Medicaid beneficiary any remuneration that the
person knows or should know is likely to influence the beneficiary’s selection of a particular provider,
practitioner, or supplier of Medicare or Medicaid payable items or services may be liable for civil money penalties (CMPs) of up to $10,000 for each wrongful act. The statute defines “remuneration” to include,
without limitation, waivers of copayments and deductible amounts (or parts thereof) and transfers of items or services for free or for other than fair market
value.
Do You Own It Too? Stark Law
Imaging and Physical Therapy are DHS
49 50
51 52
53 54

8/28/2020
10
State and Federal Policy
•Not always specific guidance
•State policy usually superseded by Federal…maybe
•Opinions vs. written rules
•Set policy and procedure based on the best information you have
57
What are you trying to say?
Compliance Programs must be properly installed and
operating within your office and must be constantly
monitored and updated, regardless of the size of your
practice.
Who’s Else is Watching?
I’ve Got My Eye On You
The Third Party Payer
55 56
57 58
59 60

8/28/2020
11
Payer’s Right to Monitor
In Black & White How to Look Up a Medical Policy
1. Determine 3rd party to look up
2. Are you in network directly or through a managed care entity?
3. Go to the 3rd party website and search for policy that fits the code or services best
4. If not available on website do an internet search for the service and the 3rd party Example: “Aetna Chiropractic Policy”
5. Contact provider relations of the 3rd
party if all else fails
Aetna’s Chiropractic Policy
Aet
na’
s C
hir
op
ract
ic P
olic
y
61 62
63 64
65 66

8/28/2020
12
Always Investigate First•When you add a new service, don’t assume it’s covered or billable
•Review third-party payor guidelines
•Ask state organizations-boards
• Item product manufacturers and related research
•Don’t rely on manufacturer’s coding recommendations
Important Facts to Know
•Determine which procedures you may perform that could be deemed experimental, unproven, or investigational
•Know what your board says
•Know what your carriers say
•Have proper informed consent
•Document, code, and bill these procedures correctly
What Are These Procedures?
Experimental, Investigational and Unproven procedures are defined as:
Use of technology, drug, device, treatment, or procedure that has not been recognized as having proven benefit in clinical medicine for any condition, illness, disease or injury being treated
Compliance with Rules is Critical
• Proper disclosure to patients• Can be harmful to
patient/provider reputation• Patients like to do their own
“research” and may not understand findings of “unproven” procedures
• Compliance with state guideline• Unproven procedures are often
reported to state boards for investigation by patients or patient family members
67 68
69 70
71 72

8/28/2020
13
Procedures Which are Unproven and Require Informed Consent
Obtain Informed ConsentExperimental/Investigational
•What to Include in Your Informed Consent?
•What language is required by your state?
•What is the definition of experimental, investigational and unproven procedures?
Let’s Take a Poll!Do you have current copies of the Medical Review Policies for All of the Payers you submit to?
Who’s Else is Watching?
Now Who?
Nebraska Chiropractic Board Just Some of the Board Rules
73 74
75 76
77 78

8/28/2020
14
Going to Use Your Staff?
172 NAC 29-002 An
d A
no
the
r
Board
OIG
Board
HIPAA
Are You In Compliance or Not? Medicare?
79 80
81 82
83 84

8/28/2020
15
1. Provider Must Be Enrolled….Period!
Medicare’s Statement Regarding Mandatory Enrollment for Chiropractors: • https://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/Downloads/bp102c15.pdfo The opt out law does not define
“physician” to include chiropractors; therefore, they may not opt out of Medicare and provide services under private contract. Physical therapists in independent practice and occupational therapists in independent practice cannot opt out because they are not within the opt out law’s definition of either a “physician” or “practitioner”.
• Tells story of who rendered the service• No substitutions for providers listed
employees• Each DC must register with Medicare
• Can cause enrolled physician to deactivate• Locum Tenens (Fee for Service Compensation
Hidden Dangers of Box 24J
Common Billing Errors
85 86
87 88
89 90

8/28/2020
16
91
Do Not Take This Lightly!
Or This! KMC’s “Either/Or” PrincipleEither covered service or statutorily excluded serviceEither Medicare responsible or patient responsible
Either active treatment or maintenance careEither mandatory ABN or voluntary ABN
Either E/M style or SOAP styleCMT is either AT or GA
AT vs. GA Modifier
•Has to be a Doctor Decision
•Needs to be clarified in the Assessment
•Patient needs to understand the difference
•Definitely Gray Areas
96
Mandatory Submission
VoluntarySubmission
91 92
93 94
95 96

8/28/2020
17
Test Your KnowledgeWhat Modifier Do You Need? MN: Chiropractic Per CMS
Acute and Chronic Subluxation
The patient must have a significant health problem in the form of a neuromusculoskeletal condition necessitating treatment, and the manipulative services rendered must have a direct therapeutic relationship to the patient’s condition and provide reasonable expectation of recovery or improvement of function.
The patient must have a subluxation of the spine as demonstrated by x-ray or physical examination (PART)
If above not met or exceeded = Not Medically Necessary! GET AN ABN!
98
Analyze the ABN Forms for…
• Are all the “D” categories filled in properly?
• What fees are included on the ABN?
• Was the appropriate option selected with the appropriate outcome? Billing?
• Does it include services excluded by Medicare?
• New ABN Form Deadline Extended to 1/1/2021 (EXP 6/2023)•You will need two
• QMB Requirements
GA Modifier
Go look at YOUR ABNs…
You Must Decide!
• It is up to the office, not the patient, to determine whether the visit is medically necessary or not
• It’s a clinical decision
• It’s not a money decision
97 98
99 100
101 102

8/28/2020
18
Conduct Internal AuditsCMS Guidelines on Self-Auditing
CMS Rule Again!Conduct Regular Documentation Audits
Review EOBs Monthly
• Set “Random EOB Review” monthly
• Randomly select a handful of payments and EOBs from the prior month, or since the last time you reviewed them
• Review for patterns that could expose you to an audit
103 104
105 106
107 108

8/28/2020
19
Are You an Outlier?
• Improper documentation coding of full-spine treatment can cause you to look like an outlier
•Hence, subject to more scrutiny, red flags, and even an audit
Conduct Regular Coding Audits - CMT
Evaluation and Management-NP Evaluation and Management-Established Pt.Missing Money Anyone? 2-3X
368 NP Visits x 3 EP Re-exams=110499212 -$65.92
$65.92 x 1104 = $72,775.6899213 - $95.62
$95.62 x 1104 = $105,564.48
Modalities and Procedures
What Might Be the Trigger?
• Overutilization
• Unspecified codes
• Unusual errors
• Billing errors, like lack of Box 14 changing
• Patient complaints
• Your number came up
109 110
111 112
113 114

8/28/2020
20
CMT Codes
•There are 3 spinal CMT codes defining the number of regions treated:
• 98940: 1-2 regions• 98941: 3-4 regions• 98942: 5 regions
• 98943: Extremity – Billed 1x per visit
Philosophically Driven
•Whether you are subluxation-based chiropractor or simply believe that every patient requires a full-spine adjustment, you need clarity
•Proper documentation, coding and case management for these technique-specific and philosophically driven conundrums need to be defined by you for your office
Chiropractic Adjustments
• Look at your CMT coding ratios to evaluate code usage
• Is it realistic that your diagnosis warrants 98941 or 98942 so frequently?
• 98943
– Are you over or under utilizing?
– Are you doing but not billing?
117
S P I N E
Clinically Appropriate – Dr. Thinking
57% 40% 3%
Primary vs Compensatory
Railroad Medicare – Comparative Billing Report
115 116
117 118
119 120

8/28/2020
21
Today’s Plan: What Not to Do!
• Documentation of an initial visit of an episode that looks like every other visit
• Initial visits of new episodes of care where the patient has no idea why they have pain... did you say “insidious onset”?
• Visits that are spaced at exactly a month apart, being billed as “AT” without proper justification-lack of case management
• Routine visit documentation that doesn’t reflect the presence of a subluxation in each region treated
Lack of Medical Necessity
-Incorrect Coding
-Insufficient Documentation
What Got Us Here Again? Today is About Solutions!
Medicare Likes to be Told a Story
• Medicare’s auditors do not want PART of the story… They want a complete non-fiction story!
• A good story includes: • Background (History)• A relatable/interesting character (Patient with a
medical problem that is examined)• Conflict to overcome (Functional deficit)• Over coming the conflict (Improvement of the
functional deficit)• Realistic events (Appropriate TX for the functional
deficit)• Character’s struggle (Effectiveness of Tx and Tx Plan)• Happy ending (Discharge from MN care)
Medicare & Other Payers Want to Help You Write Better
They have lots of resources to let chiropractors know what is expected in documentation:
• Records request checklists
• Article guidelines (Old LCD)
• Online Training Resources
• Provider representatives
• Medical Review Policies
121 122
123 124
125 126
8/28/2020
22
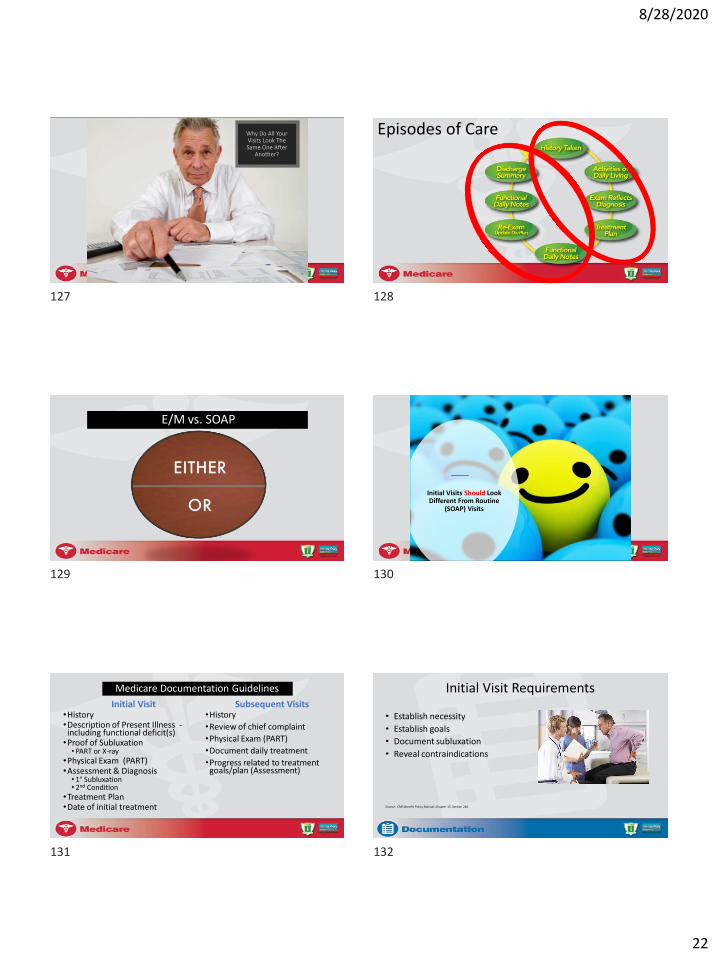
Why Do All Your Visits Look The Same One After
Another?
Episodes of Care
E/M vs. SOAP
Initial Visits Should Look Different From Routine
(SOAP) Visits
Medicare Documentation Guidelines
Initial Visit•History•Description of Present Illness -including functional deficit(s)•Proof of Subluxation• PART or X-ray
•Physical Exam (PART)•Assessment & Diagnosis • 1° Subluxation• 2nd Condition
•Treatment Plan•Date of initial treatment
Subsequent Visits•History
•Review of chief complaint
•Physical Exam (PART)
•Document daily treatment
•Progress related to treatment goals/plan (Assessment)
Initial Visit Requirements
• Establish necessity
• Establish goals
• Document subluxation
• Reveal contraindications
Source: CMS Benefit Policy Manual, Chapter 15, Section 240
127 128
129 130
131 132

8/28/2020
23
The Foundation of Medical Necessity is Found in the History
How Is It That Every One of Your Patient
Conditions is of Insidious Onset?
(Gradual)
History 101 Building a Strong Foundation•Thorough Intake Process•Train staff to look for missed entries in intake paperwork/online portal
•Outcome Assessment Tools•Write better treatment plans to prove treatment effectiveness•Have measurable and objective goals
133 134
135 136
137 138

8/28/2020
24
Start with Chief ComplaintWhy is the patient coming in to see you?
– It may be a somatic complaint from the patient
• (e.g., “headache” or “Low back pain”)
– It may be the purpose for the visit
Most forgotten part of history!Provider Didn’t Ask Enough
Questions
Not A Good One!
Provider Did a Better Job! – Real Time
Next… HPI, ROS, and PFSH= History
•Don’t think of this as “subjective”
•Patients tend to be poor historians
•First, be a good doctor as you inquire
•Clarify and quantify over and over
HPI Explains More - Often known as “OPQRST”
Timing • When did it start? A month ago, a year ago, a day ago?• Q: How longs has this been going on?
Provocation or Palliation• Modifying Factors (ibuprofen use decreases
symptoms) • Q: Does anything make it better? What makes it
worse? What provokes your pain?
Onset / Duration• Ground level information for the Chief Complaint
• Q: What were you doing when it started? When did the pain start?
Quality • Type of symptom – dull, sharp, tingling, etcetera • Q: Can you describe it to me? Is it sharp, dull, constant,
intermittent?
Region and Radiation• Location of symptom(s)• Q: Does the pain extend anywhere else?• Q: Where exactly does it hurt? Point to where it hurts the
most.
Severity • Scale of 1-10/10 or mild, moderate, severe• Q: On a scale of 1-10, ow much does it hurt?
139 140
141 142
143 144

8/28/2020
25
Past, Family, and Social History (PFSH)
• The PFSH consists of a review of three areas:–Past History
–Family History
–Social History
Past, Family and Social History (PFSH) – Real TimeBuilding a Strong Case
Next …Review of Systems (ROS) OR 99201
• Constitutional
• Cardiovascular
• Respiratory
• Gastrointestinal
• Genitourinary
• Integumentary (skin and/or breast)
• Musculoskeletal
• Neurological
• Psychiatric
• Endocrine
• Lymphatic
Update on Re-Exam
State Board/Payers May Require
145 146
147 148
149 150
8/28/2020
26
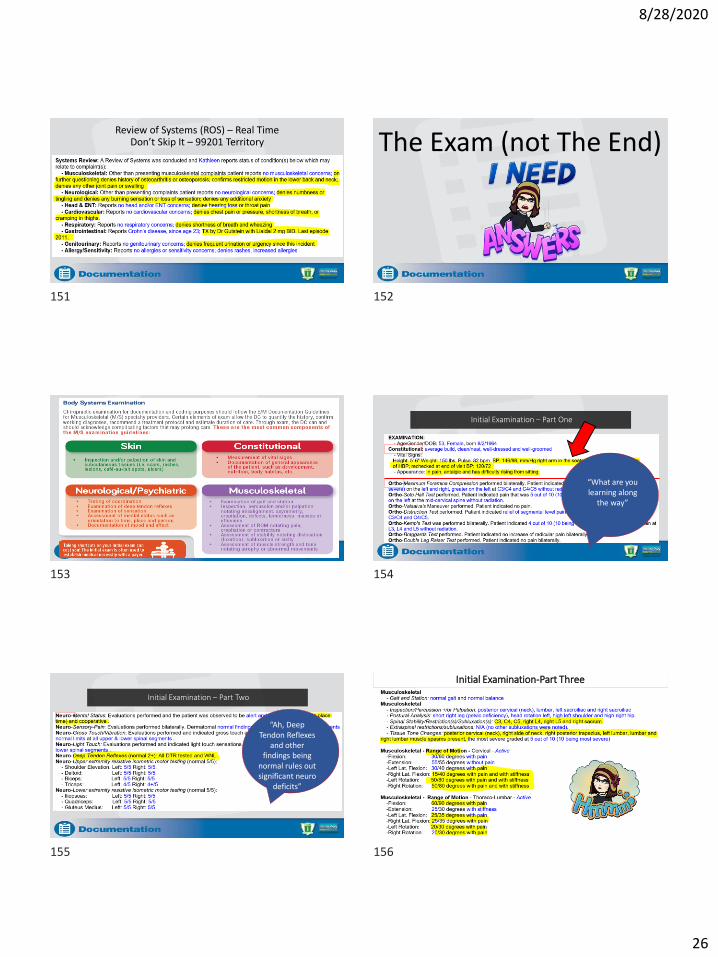
Review of Systems (ROS) – Real TimeDon’t Skip It – 99201 Territory The Exam (not The End)
Initial Examination – Part One
“What are you learning along
the way”
Initial Examination – Part Two
“Ah, DeepTendon Reflexes
and other findings being
normal rules out significant neuro
deficits”
“May be a good
candidate for active care
rehab!”
Initial Examination-Part Three
151 152
153 154
155 156

8/28/2020
27
P.A.R.T PART without X-Ray
•P – Pain (expand from subjective•A – Asymmetry (Subluxation)•R – Range of Motion Abnormality•T – Tone/Tonicity
Do I Need X-Rays? Initial Examination-X-Ray Report/Rationale
=A - Assessment
S - SUBJECTIVE• What you learned in the subjective
+O - OBJECTIVE
• What you learned in the objective
ASSESSMENT IN THE NOTE
• Often the most overlooked
section of the initial note
• More than just a diagnosis
• Doctors expect everyone know
what findings mean
157 158
159 160
161 162

8/28/2020
28
INITIAL ASSESSMENT
Tell the story well……
– Patient Reporting
– Measurements
– Complications
– Co-Morbidity Factors
– Any unusual circumstances
– Diagnosis
– Can include the treatment plan
…Paint the clearest pictureThe Collection Coach
INITIAL ASSESSMENT
• What Do You Know…?
– Interpret what you learned
– Don’t add new facts
– Give your professional
opinion
– Provide judgement
– Tell what you know…
The Collection Coach
ASSESSMENT IN THE NOTE
• Often the most overlooked
section of the initial note
• More than just a diagnosis
• Doctors expect everyone know
what findings mean
INITIAL ASSESSMENT
•What do you know?
•Why is it going on?
•What is making it worse?
•What is limiting recovery?
The Collection Coach
CCGPP PROGNOSTIC FACTORS
• Older age
• History of Prior Episodes
• Severity of initial episode of injury
• Number of exacerbations
• Duration of current episode longer than 1
month
• Psycho-social factors
163 164
165 166
167 168

8/28/2020
29
CCGPP PROGNOSTIC FACTORS
• Pre-existing pathology
• Nature of employment
• Waiting more than 7 days to seek
treatment
• Congenital anomalies
• Patient compliance
The Collection Coach
• Likely people with a high school education with little to no
medical knowledge
• Many auditors doesn’t know the significance of a positive
ortho or neuro test
• Don’t know the what the diagnosis means
• Depend on Assessment for plain English
The Collection Coach
?The Collection Coach
Say What?
Disclaimer: This is documentation reviewed at KMC University. This is ICD 9 Coding.
Using Co-Morbidities In Assessment
169 170
171 172
173 174

8/28/2020
30
Using Co-Morbidities In Assessment
Complicating Factor
Assessment Gets Lost in the Sauce ASSESSMENT IN THE NOTE
• Often the most overlooked
section of the initial note
• More than just a diagnosis
• Doctors expect everyone know
what findings mean
Diagnosis for Medicare Claims
• The primary diagnosis must be subluxation Subluxation M99.0x
• Supporting musculoskeletal diagnosis Causal from subluxations, such as disc degeneration
Next – The Plan
175 176
177 178
179 180

8/28/2020
31
History Exam Clinical Decision
MakingMeet the Requirements
• Date of the plan/initial treatment
• Frequency and duration
• Treatment goals for each region/treatment to include long term goal
• An evaluation of treatment effectiveness measurement
Sample Payer MRP Date of Initial Treatment
• Relates to beginning of this treatment episode
• First date provider evaluated patient
• Submitted in Box 14 on the CMS-1500 form
• Referred to in subsequent visit documentation
Frequency and Duration
• Indicate initial part of the treatment
• It’s ok to have an end game projection
• Don’t be so specific that you appear canned or boxed into a plan
• Each section should end with an evaluation
Treatment Goals
• Treatment goals need to be functionally based.
• What functions are we restoring with our treatment plan?
• How will we measure that corrective change?
• What goals are outlined for each type of treatment?
181 182
183 184
185 186

8/28/2020
32
Evaluate the Effectiveness—Measurably!
• OATS make it easy
• Pain is difficult to track and measure
Pain decrease as a goal
9/10 to 8/10 = goal met
• Use an accepted measure that you can document simply
• Improvement in function = success!!
Initial NDI-73% Disability Initial Low Back Disability Q – 68%
Part Three: Treatment Plan
Treatment Plan (Cont.)
187 188
189 190
191 192

8/28/2020
33
Mechanic AnalogyWould you want to have your car serviced by the mechanic who says to come into his garage 3x/wk until your car gets fixed?
• Would you want to know what he would do each visit?
• Would you trust that he knows what is wrong with your car?
• Would you question when he would be done with fixing your car?
• How would you know he is done?• Does he even care about your car?• Would you regret even going into his shop?
By not DETAILING your plan of care, you are telling your patient and their third party payer that you don’t really know what is wrong with them, you are unsure what to do to treat them, and you have no idea how long it will take to get them better
Terrible Treatment Plans• 3x /wk until the patient gets better
– What is better? How will you know when they are better?
– Why 3x /wk? For how long? – What are you treating and trying to get better?– What services will the patient get and why?
• Adjust 2-3x /wk for 4 wks then next phase of care– What is the next phase of care?– What are you treating? – Why 4 weeks?– ????Do you want to be treated by this Doctor?
Patient WASN’T Treated
• Patient was advised in using ice at home
• Instructed to return for treatment
• If the patient was treated TODAY then SOAP should be added below the TX plan!!
This Visit Must Include “P” of SOAP if you Treat the same day as Exam!
Treatment is different than treatment plan. On E/M visits where you are establishing a treatment plan, if you execute
treatment the same day, don’t forget to list it.
Make it Shine!
• Home care recommendations
• Prognostic factors
• Inclusion of all possible treatment and DME options
193 194
195 196
197 198

8/28/2020
34
Signature Guidelines
Subsequent Visits Medicare Said It…
Medicare Documentation Guidelines
ROS
Subsequent Visit Documentation
What is expected for subsequent visits:• History• Exam• Assessment• Treatment • Progress towards goal
199 200
201 202
203 204

8/28/2020
35
Medicare Said It…
Subsequent Visits Routine Visits: Rule 22 (Sample Colorado Rule)Read This: It isn’t Only There
Routine Visits-Rule 22 (Sample Colorado Rule)Continued
Review of Chief ComplaintWhat’s Changing?
•Step away from the OUCH forms…•Different Chief Complaint Each Day•Patient driving the bus
Most forgotten part of history!
205 206
207 208
209 210

8/28/2020
36
Subsequent Visit – Physical Exam
• Examine area(s) of spine– They want to see PART
– How has the PART changed due to treatment
• Presence or absence of subluxation (PART) – PART documentation on EVERY
visit!
Subsequent Visit -Treatment
• CMT– List spinal/vertebral areas adjusted that
are MN
– Include secondary areas of compensation that were treated
– Include technique
– Manual manipulation
– Can include handheld device with manual force
– How did patient handle the treatment
• Passive/Active therapies– Document what was done, why is was
done, and how if effected the patient
Subsequent Visit -Assessment
Documentation needs to show what the doctor is thinking:
• Treatment effectiveness
• Assessment of change since last visit
– How and Why
• What is the progress towards the functional goals?
Progress Toward Goals
• Can be unchanged
– For very short term
• Must be quantitative
• Function is the key
Documenting Ancillary ServicesVisit 2-First TX Visit
Number the Visit(s)
P.A.R.T
Primary vs Compensatory
211 212
213 214
215 216
8/28/2020
37
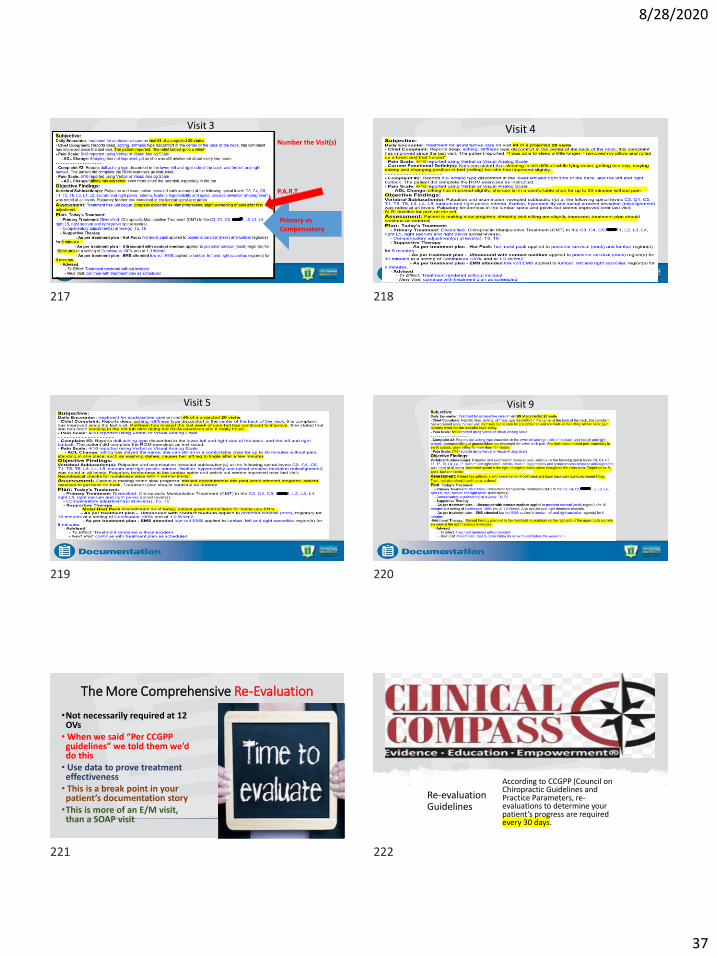
Visit 3
Number the Visit(s)
P.A.R.T
Primary vs Compensatory
Visit 4
Visit 5 Visit 9
The More Comprehensive Re-Evaluation
•Not necessarily required at 12 OVs• When we said “Per CCGPP guidelines” we told them we’d do this• Use data to prove treatment effectiveness• This is a break point in your patient’s documentation story•This is more of an E/M visit, than a SOAP visit
Re-evaluation Guidelines
According to CCGPP (Council on Chiropractic Guidelines and Practice Parameters, re-evaluations to determine your patient’s progress are required every 30 days.
217 218
219 220
221 222

8/28/2020
38
The 30-Day Rule-CMS
If a patient exhibits no change in the outcome assessment data for a maximum period of three consecutive re-examinations or 60 days, the patient should be considered for a clinical change in treatment. May include the following:
• Modifying treatment approach
• Co-treat with an allied health provider
• Referral for a second opinion
• Determine that the patient has reached maximum improvement
• The clinical decision as to which, change in treatment, path should be followed is dependent on the individual practitioner‘s profession integration of outcome assessment data
Why Re-evaluate?
To Assess Progress:
• Changes in condition(s)• New injury, decreased or increased symptoms,
new co-morbidities…
• Effectiveness of Tx• Did the treatment so far help? How much?
• What is needed to meet therapeutic goals?• Does the patient need more care? Why? How
much more?
Why Re-evaluate?
To Improve Patient Care:– A patient is more than their
diagnosis… they want to see progress from symptoms
– By seeing where they are in their healing, we can effectively change treatment to meet their needs
– Sets clinical, professional, and financial boundaries to care provided
Various Re-evaluations
• Periodic re-evaluation to determine if further care is necessary
• New condition, new injury, new accident
• Evaluations for considering discharge
• Non-treatment related E/M services
The Frequently "Missed” Re-Exam Component?
•You must update the history
•It’s a component of E/M
•If you don’t have the patient fill something out, do it verbally and document it
•EHR systems allow for this
223 224
225 226
227 228

8/28/2020
39
A Recent IME and AuditComponents of a Periodic Re-Evaluation
The re-exam should be scheduled on a specific date in the treatment plan. At the re-exam you should:
• Update the history; consider getting hand-written update from pt.• Re-examine all positives and significant negatives from the initial
examination• Patient completes new Outcome Assessment Questionnaires; score
them and compare scores with original• Assess the effectiveness of the previous course of treatment, in your
assessment portion of the note • Modify the diagnoses if appropriate and update a new treatment plan, if
needed
PART
Most Overlooked Component of Re-Eval?
• Assessment of the effectiveness of care
• Statements as to what’s next
• Does the patient need more care?
• Why does the patient need more care?
229 230
231 232
233 234

8/28/2020
40
The Collection Coach
?
Give Them an Update
Also a Treatment Visit!?
Transitional DX
Change of diagnosis to fit the patient’s current state
– If no longer right sciatica with LBP reduce the severity to what it is now
Time to Discharge
235 236
237 238
239 240

8/28/2020
41
When to Release from Active Care
• At scheduled re-evaluations review patient’s progress towards:
• ADL goals
• Functional goals
• Symptom free goals• If possible
• Within active treatment if the results warrant
• Reschedule evaluation earlier
– Per CCGPP: When the patient arrives at Final Plateau (maximum therapeutic benefit)
– Complete or partial resolution of the condition and all reasonable treatment and diagnostic studies have been provided
– Patient is unlikely to improve further
When to Release from Active Care
Therapeutic Withdrawal
Administrative Discharge
Final Discharge
Medically Necessary Care
Discharge from Active Care
Therapeutic Withdrawal
Final/Administrative Discharge
Discharge Summary
Types of Therapeutic Withdrawal
• Gradual Withdrawal
– Where the patient’s care is tapered off
• Abrupt Withdrawal
– Patient instructed to return if the symptoms recur
– Patient is scheduled for an evaluation at a later date to determine if there is any regression
– Tends to be the typical MD approach
Times a Week # of Weeks
3 2
2 2
1 2
1 every other week 4
Total = 14 visits
241 242
243 244
245 246

8/28/2020
42
Therapeutic Withdrawal
CCGPP (Clinical Compass)
• Therapeutic Withdrawal (TW) is included as proper case management
• Without Therapeutic Withdraw
• There is no way to determine the stability of the spine
• Determine if a patient require on going care
Therapeutic Withdrawal
Maintenance – The patient is MAINTAINING THE CURRENT
STATE and not expected to improve.
Therapeutic Withdrawal– The doctor is not 100% convinced that the
patient will not relapse if active care is discontinued. WE’RE TESTING TO SEE IF STABILITY CAN BE MAINTAINED.
–(A short-term trial)
Order After Unsuccessful Therapeutic Withdrawal
Check with payer and don’t assume it is covered!
Medicare covers Chronic Care, but not open ended.
Visit 16-Begin Therapeutic Withdrawal
When to Release from Care
CCGPP Says– Arrive at Final Plateau
(maximum therapeutic benefit)
– Complete or partial resolution of the condition and all reasonable treatment and diagnostic studies have been provided
– Patient is unlikely to improve further
Clinical Discharge
• Releasing from Medically Necessary Care
– The patient doesn’t need treatment to improve function anymore
– Release them so they can fly on their own
– Be the place they can maintain safety
– Discharge puts a “pin” in this active episode
247 248
249 250
251 252

8/28/2020
43
Discharge Summary• Include:
– Conditions treated
– Initial treatment date
– Date of discharge
– # of Visits
– Services provided
– DME/orthotics RX’ed
– Recap initial exam findings
– Recap radiology and/or lab testing
– Status of patient at discharge
– Your assessment of patient’s treatment
– Recommendation for future care
Final Visit-Discharge! Final Discharge Checklist
❑ You’ve finished a course(s) of treatment
❑ The patient has met or not likely to move closer to reaching goals
❑ You have effectively attempted therapeutic withdrawal or written down why it is not indicated
❑ The patient has been given educational and self management tools about their condition
❑Written discharge is placed in chart
Take Time To Properly Train All Team Members
253 254
255 256
257 258