knowledge, attitudes and practices (kap) on micronutrient deficiency among adolescent girls,...
TRANSCRIPT
Knowledge, Attitudes and Practices (KAP) on Micronutrient
Deficiency Among Adolescent Girls, Pregnant and Lactating
Women in Selected Areas in the Kyrgyz
Republic
Presentation on the Survey ResultsFebruary 24th, 2015

Outline of the presentation
1. Background 2. Survey objectives3. Methodology4. Partnership5. Survey results6. Summary of findings7. Recommendations
Widespread micronutrient deficiencies among women age 15-49- Iron-deficient anemia (35%, DHS 2012)- Iodine deficiency goiter (1,140 people out of 100,000, MOH 2012) Anemia caused by iron deficiency leads to- Higher risk of complications during pregnancy (pregnant women)- Development of various diseases- Reduced productivity (adults)- Delay in cognitive and physical development (children)
1. Background of the surveyWidespread micronutrient deficiencies

Iodine deficiency leads to- Impaired physical and cognitive development (children) - Congenital anomalies (children) - Increased infant mortality (children)- Diseases such as endemic goiter and hypothyroidism (adults)- Female infertility and reproductive disorders (women)- Miscarriage during childbirth (women)
1. Background of the surveyWidespread micronutrient deficiencies (continued)
The overall objective of the survey is to understand the knowledge, attitudes and practices (KAP) on micronutrient deficiencies among adolescent girls, and pregnant and lactating women through exploratory investigation methods. The information from the study will inform related policy/programme responses such as awareness raising.
The specific objectives of the survey were: 1.To understand the current level of knowledge related to micronutrients among the targeted group and how this knowledge is translated into practice2.To provide recommendations for the design of an action plan to improve nutrition-related practices.
2. Objectives of the survey*Investigation of knowledge, attitude and practice regarding micronutrient deficiencies
*This survey is not intended to provide a cost intensive nationwide survey result but rather complement the existing knowledge base on nutrition, such as the DHS and MICS, and help locate areas where information and education efforts could be further strengthened.

Design: Questionnaire-based survey and focus group discussions (FGDs) for investigation of knowledge, attitudes and practices
Data collection period:Conducted in September-October 2014 during the post-harvest period
Target population: Adolescent girls aged 15 to <18 years, pregnant and lactating women in selected areas
Target areas: Urban and rural areas of 4 Oblasts with high levels of iron-deficiency anemia among adolescent girls, pregnant women and lactating women in Issyk-kul, Talas, Chuy, Osh (including Bishkek and Osh cities)
3. Methodology (1)Questionnaire-based survey for exploratory investigation of knowledge, attitude and practice
Interviewing an adolescent girl
Sampling: Aimed at obtaining insights on KAP among targeted groups in the selected 4 Oblasts (NOT nationwide)
Methodological limitations: The survey does not define prevalence of certain phenomena or incidents, as the survey is designed for an investigation of KAP. As the objective is an investigation of KAP, the survey results are presented only at aggregated level – i.e. 4 provinces combined (n=600), urban and rural areas of selected provinces. Any results disaggregated by population group or oblast should be considered as indicative.Other potential causes of micronutrient deficiency such as medical conditions, wealth levels and livelihoods were not investigated in the survey.
3. Methodology (2)

Ministry of HealthUnited Nations World Food Programme (WFP)United Nations Population Fund (UNFPA)Deutsche Gesellschaft für Internationale (GIZ)Embassy of Switzerland
4. Partnership
6. Survey results
6.1 Actual number of responses
6.2 Knowledge of iron-deficiency anemia
6.3 Attitudes and practices regarding iron-deficiency anemia
6.4 Knowledge of iodine deficiency
6.5 Attitudes and practices regarding iodine deficiency

6.1 Knowledge of anemia (1)Respondents ‘heard’ about anemia, but its causes were not widely understood by respondents
% of respondents who had at least heard about anemia
Causes of anemia mentioned by respondents (%)

6.1 Knowledge of anemia (2)Adolescent girls are likely poorly informed about anemia.
% of respondents who at least heard about anemia
Causes of anemia mentioned by respondents (%) *
* The results disaggregated by adolescent girls, pregnant women and lactating women are indicative and subject to further investigation

6.1 Knowledge of anemia (3)Awareness of iron-rich foods was generally low. Majority of respondents knew about negative effects of tea consumption during the meal.
What food items do you think are rich in iron?(Percentage, multiple response)
Proportion of respondents who knew of the negative effects of tea consumption
during a meal
* Factors that inhibit non haem iron absorption are phytates, polyphenols including tannins
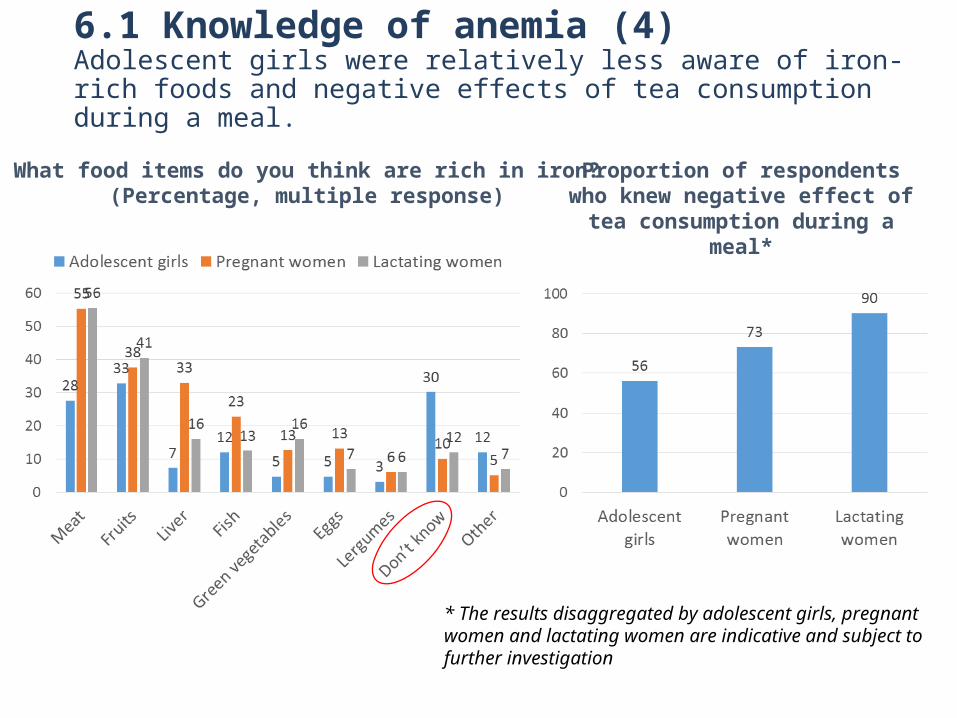
6.1 Knowledge of anemia (4)Adolescent girls were relatively less aware of iron-rich foods and negative effects of tea consumption during a meal.
What food items do you think are rich in iron?(Percentage, multiple response)
Proportion of respondents who knew negative effect of tea consumption
during a meal*
* The results disaggregated by adolescent girls, pregnant women and lactating women are indicative and subject to further investigation

6.1 Knowledge of anemia (5)Local medical personnel is the main source of information, followed to a lesser extent by family members. Media and schools were low. Difference between urban and rural was insignificant.
Where did you learn about anemia? (Percentage, multiple response)

6.1 Knowledge of anemia (6)Adolescent girls were less informed by local medical personnel compared to pregnant and lactating women. Less than one-fifth of adolescent girls learned about anemia at school.
Where did you learn about anemia? (Percentage, multiple response)
* The results disaggregated by adolescent girls, pregnant women and lactating women are indicative and subject to further investigation
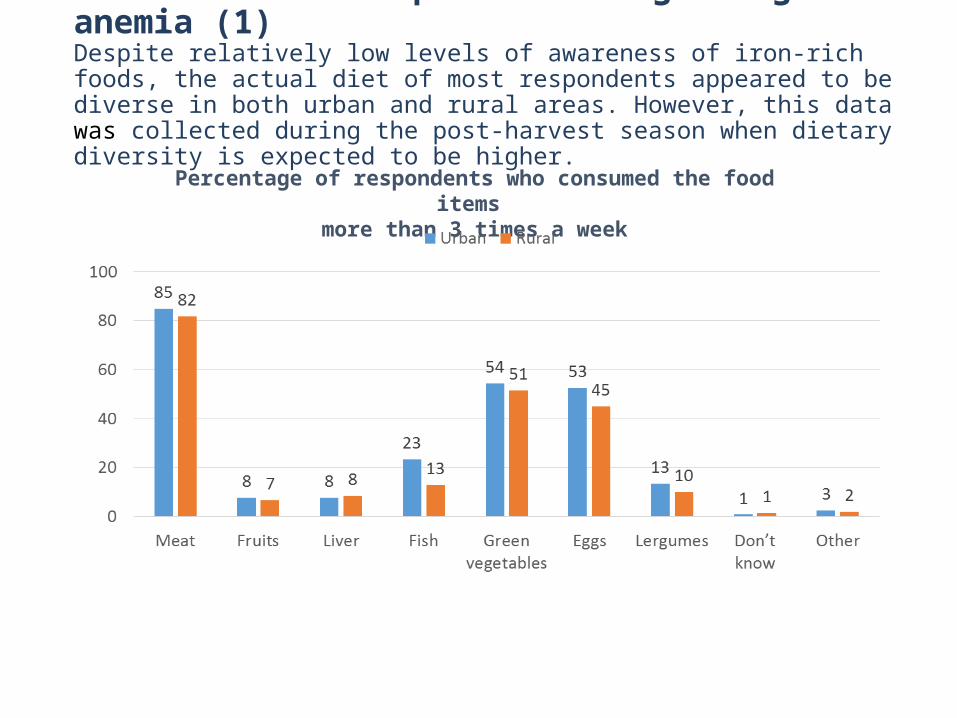
6.2 Attitude and practices regarding anemia (1)Despite relatively low levels of awareness of iron-rich foods, the actual diet of most respondents appeared to be diverse in both urban and rural areas. However, this data was collected during the post-harvest season when dietary diversity is expected to be higher.
Percentage of respondents who consumed the food items more than 3 times a week

6.2 Attitude and practices regarding food consumptionMothers were mainly involved in deciding what family members eat; however, this was not the case for one out of four respondent households.
Who usually decides what family members eat?

6.2 Attitudes and practices regarding tea consumptionDespite high levels of awareness of the negative effects of tea consumption during the meal, around 60% of respondents ALWAYS consume tea during the meal. The proportion was higher in urban areas.
Do you drink tea during a meal? (Percentage of respondents)
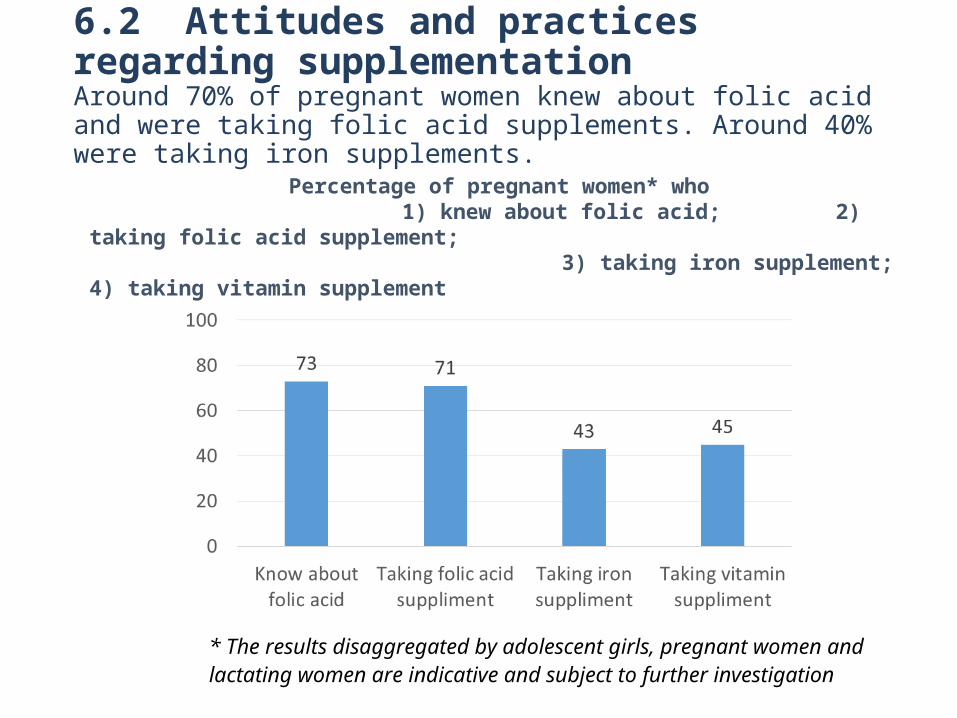
6.2 Attitudes and practices regarding supplementation
Around 70% of pregnant women knew about folic acid and were taking folic acid supplements. Around 40% were taking iron supplements.
Percentage of pregnant women* who 1) knew about folic acid; 2) taking folic acid supplement;
3) taking iron supplement; 4) taking vitamin supplement
* The results disaggregated by adolescent girls, pregnant women and lactating women are indicative and subject to further investigation

6.2 Attitudes and practices regarding health systems Local level systems to detect anemia seem to be functioning in both rural and urban areas
Proportion of respondents who were diagnosed as anemic by health
personnel over the last 3 months
Proportion of anemic respondents who were given an explanation of anemia, besides
medication
This is largely consistent with DHS (2012) which showed that 35% of women of reproductive age were anemic.
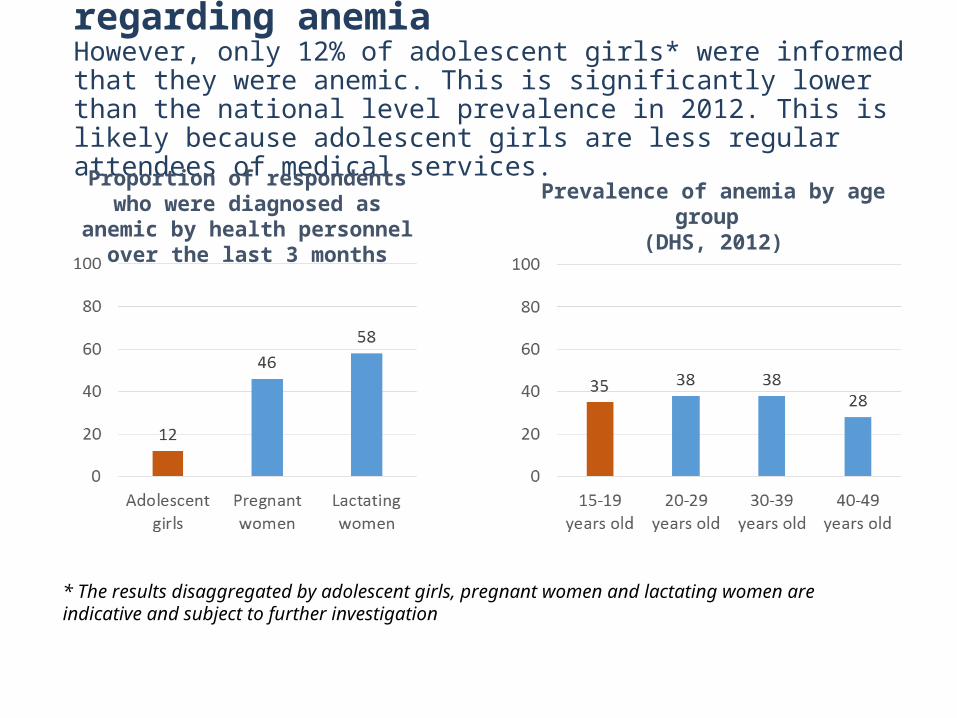
6.2 Attitudes and practices regarding anemia However, only 12% of adolescent girls* were informed that they were anemic. This is significantly lower than the national level prevalence in 2012. This is likely because adolescent girls are less regular attendees of medical services.
Proportion of respondents who were diagnosed as anemic by health
personnel over the last 3 months
Prevalence of anemia by age group (DHS, 2012)
* The results disaggregated by adolescent girls, pregnant women and lactating women are indicative and subject to further investigation
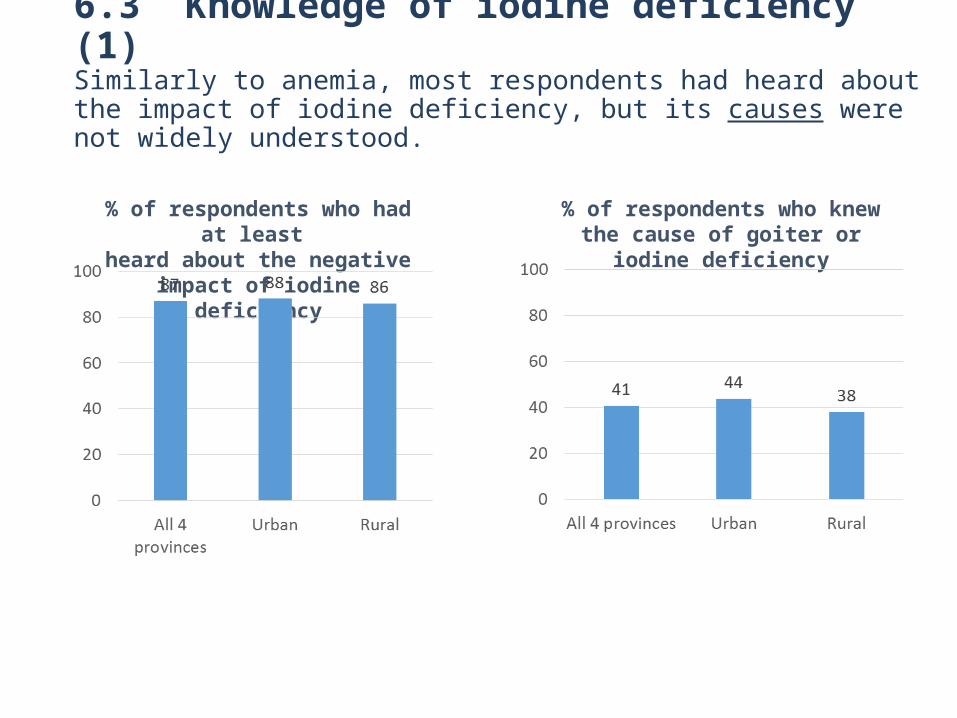
6.3 Knowledge of iodine deficiency (1)Similarly to anemia, most respondents had heard about the impact of iodine deficiency, but its causes were not widely understood.
% of respondents who had at least heard about the negative impact of
iodine deficiency
% of respondents who knew the cause of goiter or iodine deficiency

6.3 Knowledge on iodine deficiency (2)Similarly to anemia, local medical personnel were the main source of information. Media, schools and VHCs* were very low.
Where did you learn about negative impact of iodine deficiency? (Percentage, multiple response)
* VHC = Village Health Committee

6.4 Practice related to iodine deficiencyDespite relatively low levels of awareness of iodine deficiency, the majority of households had heard about iodized salt and actually used it.
Have you heard about iodized salt? % of respondents using iodized salt* at home
*MICS 2014 indicates that 92.8 percent of households had salt testing 15 parts per million or more of iodate.

7. Summary of findings: Knowledge
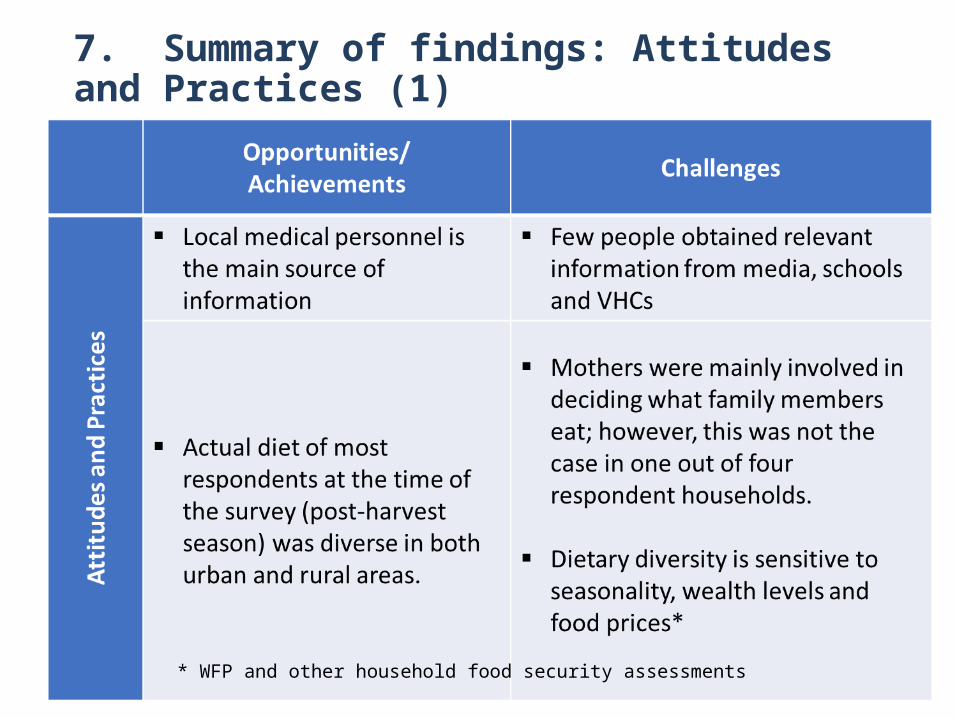
7. Summary of findings: Attitudes and Practices (1)
* WFP and other household food security assessments

7. Summary of findings: Attitudes and Practices (2)

1. Food and nutrition education should be strengthened to improve understanding of the causes and consequences of anemia and other micronutrient deficiencies, to encourage the consumption of a variety of foods during the whole year and to promote behavioral change related to tea consumption during the meal.
2. Food and nutrition education should be further promoted through non-medical services to reach:
Adolescent girls who attend less regularly medical services Mothers, with a further emphasis on the one in four mothers who are
not involved in decisions on household food consumption Elders and fathers who are also widely involved in decision making
related to food and nutritionSuch non-medical services include: School education VHCs and community events Media information campaigns Social workers and agricultural extension workers
7. Recommendations (1)

7. Recommendations (2)
4. Strengthen postgraduate education of medical personnel through introduction of training modules to enhance knowledge and skills on nutrition.
5. Further study of other potential underlying causes of iron-deficiency such as economic access to iron-rich foods, social and environmental factors and seasonality
6. Further investigation of iodine deficiency, including monitoring the status of iodine deficiencies* among vulnerable groups
3. Develop simple and effective methods/tools for food and nutrition education, which can be used by medical and non-medical personnel (e.g. school teachers), such as positive nutrition practices using available foods (iodized salt, green leafy vegetables and legumes, etc.).
A poster in a secondary school (Nookat district)
* Iodine status monitoring was discontinued in 2007