knowledge translation in bc physiotherapy alison m. hoens physical therapy knowledge translation...
TRANSCRIPT

Knowledge Translation in BC Physiotherapy
Alison M. HoensPhysical Therapy Knowledge Translation Broker
UBC Dept of PT, FOM; Physiotherapy Association of BC; BC RSRNet (VCH, PHC, BCC&W)
Clinical Associate Professor, UBC Dept of PTClinical Coordinator, Physiotherapy, PHC

Objectives
To define & understand knowledge translation
To appreciate why KT is important To provide a framework for knowledge
translation in physical therapy in PT End of grant KT Integrated KT
To outline the role of the KT Broker To identify possibilities for your involvement

What is KT?
Lab ClinicalResearch
Translational
Research (KT1)
Knowledge Translation (KT2)
CIHR; Hulley et al, 2007
HealthCare

Many terms, same basic idea …
Applied health researchDiffusionDissemination Getting knowledge into practiceImpactImplementation Knowledge communicationKnowledge cycleKnowledge exchange Knowledge managementKnowledge translation
Knowledge to actionKnowledge mobilization Knowledge transfer Linkage and exchangeParticipatory researchResearch into practiceResearch transferResearch translation Transmission Utilization

Knowledge TranslationKnowledge Translation
CIHR definition Knowledge translation is the exchange,
synthesis and ethically-sound application of researcher findings within a complex system of relationships among researchers and
knowledge users. CIHRCIHR

KT “closing the know-do gap”
Know Do

But, fails to account for …
Ask Answer

KT key concepts
Ask Answer
Do Know

Knowledge translation is about ensuring that: ‘users’ are aware of and use research
evidence to inform their decision making Research is informed by current available
evidence and the experiences and information needs of ‘end users’
Researchers Users

WHY IS KT IMPORTANT IN PT?
Mikhail et al, 2005: Physical Therapists’ use of interventions with high evidence of effectiveness in the management of a hypothetical typical patient with acute LBP
68% of PTs used interventions with strong or mod evidence of effectiveness
90% used interventions with limited evidence
96% used interventions with absence of evidence of effectiveness

WHY IS KT IMPORTANT IN PT?
Stevenson, T et al. (2005). Influences on Treatment Choices in Stroke Rehabilitation: Survey of Canadian Physiotherapists. Physiotherapy Canada.
Ranking of importance of factors influencing current practice:
Experience Continuing education (practical) Colleague Influence Continuing Education (theory) Professional Literature * secondary sources Entry Level Training
Most impt infuence
Least impt infuence
BARRIERS
I had considerable freedom of clinical choice of therapy: my trouble was that I did not know which to use and when. I would gladly have sacrificed my freedom for a little knowledge.
Sir Archie Cochrane. Effectiveness and Efficiency: Random Reflections on Health Services

There seems to be little relation between the quality of the evidence and its diffusion into practice (Fitzgerald et al 2002)

BARRIERS Lack of time, computing resources, not enough
evidence, lack of access; lack of skills for searching, appraising, and interpreting; lack of incentives (Bennett S. et al, 2003. Australian OT Journal, 50, 13-22.)
Relevant literature not compiled all in one place (Closs & Lewin, 1998. Br J of Therapy & Rehab, 5, 151-155).
Publication bias, indexing issues, language issues, assessing internal validity, access to electronic databases, access to full text, assessing applicability, drawing conclusions (Maher. C. et al. Phys Ther, 84: 645-654).

BARRIERS
Information overload Rich with diversity yet highly chaotic Need tools/processes that can reliably
and sensibly address the info • Agency for Healthcare Research & Quality
http://www.ahrq.gov/research/physprac.htm
xx

Structural (e.g. financial disincentives)
Organisational (e.g. inappropriate skill mix, lack of facilities or equipment)
Peer group (e.g. local standards of care not in line with desired practice)
Individual (e.g. knowledge, attitudes, skills)
Professional - patient interaction (e.g. problems with information processing)
BARRIERS

KT framework
‘Knowledge to Action’ Cycle
Ian Graham, VP, KT, CIHR
MonitorKnowledge
Use
SustainKnowledge
Use
EvaluateOutcomes
AdaptKnowledge
to Local Context
AssessBarriers to
Knowledge Use
Select, Tailor,Implement
Interventions
Identify Problem
Identify, Review,Select Knowledge
Products/Tools
Synthesis
Knowledge Inquiry
Tailo
ring
Kno
wle
dge
KNOWLEDGE CREATION
Graham et al., 2006
Knowledge-to-Action Cycle

Types of KT
End of grant Traditional approach Knowledge creation by
researchers disseminated by publication & presentation
Improvements:• Targeted messages to
key stakeholders• More interactive
strategies Eg. interactive
material; e-classroom Opinion leader
Integrated KT Clinician involved in
research process from it’s inception
• Collaboration through research question, study & dissemination

How effective are variousimplementation strategies?
Intervention Number of CRCTs
Range Median effect size
Educational materials
4 +3.6%, +17.0% +8.1%
Audit and feedback
5 +1.3%, +16.0% +7.0%
Reminders 14 –1.0%, +34.0% +14.1%
Single interventions
Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay C, Vale L et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol Assess 2004.

What is effective?
Little to no effect Educational materials Didactic sessions
Sometimes effective Audit & feedback Local opinion leaders Local consensus project Patient mediated interventions
Consistently effective Reminders Interactive education (with discussion of practice) Social marketing
(Bero et al., 1998, Grimshaw et al., 2001)

An example: Inspiratory Muscle Training & COPD
Knowledge to Action Cycle
• Identify a problem that needs addressingHighly effective but greatly underutilized
• Identify, review, and select knowledge relevant to the problemDemonstrate value
• Adapt this knowledge to the local contextPT vs Nrsg vs RT led respiratory rehab programs
• Assess the barriers to using the knowledgeKnowledge of how to do it? Accessibility to equipment? Time?

An example: Inspiratory Muscle Training & COPD
Knowledge to Action Cycle
• Design transfer strategies to promote the use of this knowledge
• Monitor how the knowledge diffuses throughout the user group
• Evaluate the impact of the users’ application of the knowledge
• Sustain the ongoing use of knowledge by users

THE ROLE OF THE KT BROKER

THE ROLE OF THE KT BROKER
Knowledge Broker Definitions of ‘Broker”
• Business person who buys and sells for another in exchange for a commission
• A party who mediates between buyer & seller• An agent involved in the exchange of messages or
transactions
Definitions of ‘Knowledge Broker”:• An intermediary who connects individuals to knowledge
providers• Core function is connecting people to share & exchange
knowledge
Dr. David Yetman - Knowledge Mobilization Manager, Harris Center

THE ROLE OF THE KT BROKER
Engage stakeholders; promote interaction Involve partners in knowledge generation & dissemination Identify champions Build awareness Build relationships Strategic communication Facilitate capacity for ‘evidence-informed’
decision making Incorporate evaluation to ensure accountability
Dobbins et al (2009). Implementation ScienceDr. David Yetman - Knowledge Mobilization Manager, Harris Center

THE ROLE OF THE KT BROKER
1. Needs evaluation Identify knowledge gaps Identify opportunities
• Inventory of resources (current studies, areas of expertise, areas of interest); contact list of researchers & clinicians for specific areas of practice
2. Acquire Strategies to acquire ‘best’ knowledge
• Tools to enhance acquiring knowledge (summary of adv/disadv of search engines, databases and key skills to enhance retrieval)
• E-alerts of publications• *In conjunction with existing infrastructure eg. PABC librarian,
UBC Rehab Sciences librarian
Dobbins et al. (2009). A description of a KTB role implemented as part of a RCT evaluating 3 KT strategies

THE ROLE OF THE KT BROKER
3. Appraise Strategies to enhance ability to critically appraise quality of
evidence• Tools for appraisal of RCTs, systematic reviews, Meta-analyses
4. Apply Strategies to enhance application of clinically relevant
evidence• Development of Clinical Practice Guidelines• Development of on-line learning (pre-test, instructional video,
e-classroom, post-test)• Inclusion into policy (CPTBC)• Developing targeted resources• *Evidence-informed decision-making!
Dobbins et al. (2009). A description of a KTB role implemented as part of a RCT evaluating 3 KT strategies

PT KTB Deliverables
1. Establish a web presence 2. Facilitate PT clinician / researcher
partnerships 3. Enhance access to evidence-based
learning resources & knowledge products 4. Identify & facilitate 1 KT initiative for each
funding partner 5. 1 joint PT & OT KB activity and share
outcomes from all PT KB & OT KB activities 6. Provide progress reports & year-end
report

Goals & DeliverablesGoals & Deliverables
Establish a web presence UBC Dept of Physical Therapy –
Knowledge Broker, under ‘Research’ PABC – members portion of website Links to other partners

Goals & DeliverablesGoals & Deliverables
Facilitate PT clinician / researcher partnerships Identify clinicians for potential
partnerships Link clinicians & researchers for
integrated KT and end-of-grant KT collaboration opportunities

Goals & DeliverablesGoals & Deliverables
Enhance access to evidence-based learning resources & knowledge products Identify existing & develop new learning Identify existing & develop new learning
resources & online guides to assist clinicians resources & online guides to assist clinicians in acquiring, appraising, synthesizing & in acquiring, appraising, synthesizing & applying knowledge into practiceapplying knowledge into practice
Provide on-line access to the learning Provide on-line access to the learning resources, guides & other knowledge resources, guides & other knowledge productsproducts

Goals & DeliverablesGoals & Deliverables
Identify & facilitate 1 KT initiative for each funding partner Best practice for arthroplasty patients
• Use of outcome measurement Best practice for skin & wound
management Guidelines on when it is safe to mobilize
the acute medical or post-surgical client


CLINICIAN NEEDS
01020304050607080
On-lin
e re
sour
ces
Writ
ten
reso
urce
s
Article
aler
ts-pr
actic
e ar
ea
Direct
ory-
curre
nt re
sear
ch
Direct
ory-
rese
arch
ers
RESOURCES
PE
RC
EN
TA
GE
OF
R
ES
PO
ND
EN
TS
Not at all interested
Mildly interested
Moderately interested
Very interested

RESEARCHER NEEDS
010203040506070
Dir
ect
ory
-cl
inic
ian
colla
bo
rato
rs
Dir
ect
ory
-a
dm
inis
tativ
eco
llab
ora
tors
KT
tem
pla
tefo
r g
ran
ts
Inve
nto
ry -
curr
en
tp
roje
cts
Dir
ect
ory
-re
sea
rch
ers
& a
rea
RESOURCES
PE
RC
EN
TA
GE
OF
R
ES
PO
ND
EN
TS
Not at all interested
Mildly interested
Moderately interested
Very interested

ADMINISTRATORS NEEDS
01020304050607080
Inve
ntor
y -
curr
ent
proj
ects
Dire
ctor
y -
rese
arch
er &
area
s
Dire
ctor
y -
clin
icia
nco
llabo
rato
rsRESOURCES
PE
RC
EN
TA
GE
OF
R
ES
PO
ND
EN
TS
Not at all interested
Mildly interested
Moderately interested
Very interested

Best Practice for Joint Best Practice for Joint ArthroplastyArthroplasty
Baseline: VCHRI Program Evaluation Course Regional Orthopaedic Working Group PRAG Outcome Measures SubCommittee MSc: evaluation PABC
Practice Guideline Advisors Group Communications Director
UBC Faculty sponsor: Dr. Elizabeth Dean CADTH? - Canadian Agency for Drugs and
Technologies in Health (CADTH) CESEI? – Center for Excellence in Simulated
Education and Innovation

Best Practice in Skin &Best Practice in Skin &Wound CareWound Care
VCH/PHC Skin & Wound Care PT Committee VCH/PHC OT Pressure Ulcer Guidelines – in
conjunction with OT KB VCH/PHC Interdisciplinary Skin & Wound Care
Committee PABC
Practice Guideline Advisors Group Communications Director
UBC Faculty sponsor – Alison Hoens CADTH? - Canadian Agency for Drugs and
Technologies in Health (CADTH) CESEI? – Center for Excellence in Simulated
Education and Innovation

Best Practice in Skin &Best Practice in Skin &Wound CareWound Care
1. To increase the awareness of the role of PTs in prevention & management of skin & wound issues
2. To increase the number of PTs who undertake a basic risk assessment & utilize basic interventions
3. To increase the number of PTs who know where to find guidance & information on more advanced assessment & interventions

When is it safe to mobilize the acute medical / post surgical pt? PABC
Practice Guideline Advisors Group Communications Director
UBC Faculty sponsor: Dr. Darlene Reid CADTH? - Canadian Agency for Drugs
and Technologies in Health (CADTH) CESEI? – Center for Excellence in
Simulated Education and Innovation

Needs AssessmentNeeds Assessment
Clinician Needs
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%
On-
line
trai
ning
for
EB
P
Writ
ten
dire
ctio
nsfo
r E
BP
Pra
ctic
esp
ecifi
cjo
urna
l ale
rts
Dire
ctor
y of
curr
ent
rese
arch
Dire
ctoy
of
rese
arch
ers
Resources
Per
cen
tag
e o
f R
esp
on
den
ts
Not at all interested
Mildly interested
Moderately interested
Very interested

Needs AssessmentNeeds Assessment
Researcher Needs
0102030405060
Dire
ctor
y of
clin
icia
nco
llabo
rato
rs
Dire
ctor
y of
adm
inis
trat
ive
colla
bora
tors
KT
tem
plat
efo
r gr
ants
Dire
ctor
y of
curr
ent
rese
arch
Dire
ctoy
of
rese
arch
ers
Resources
Per
cen
tag
e o
f re
spo
nd
ents
Not at all interested
Mildly interested
Moderately interested
Very interested
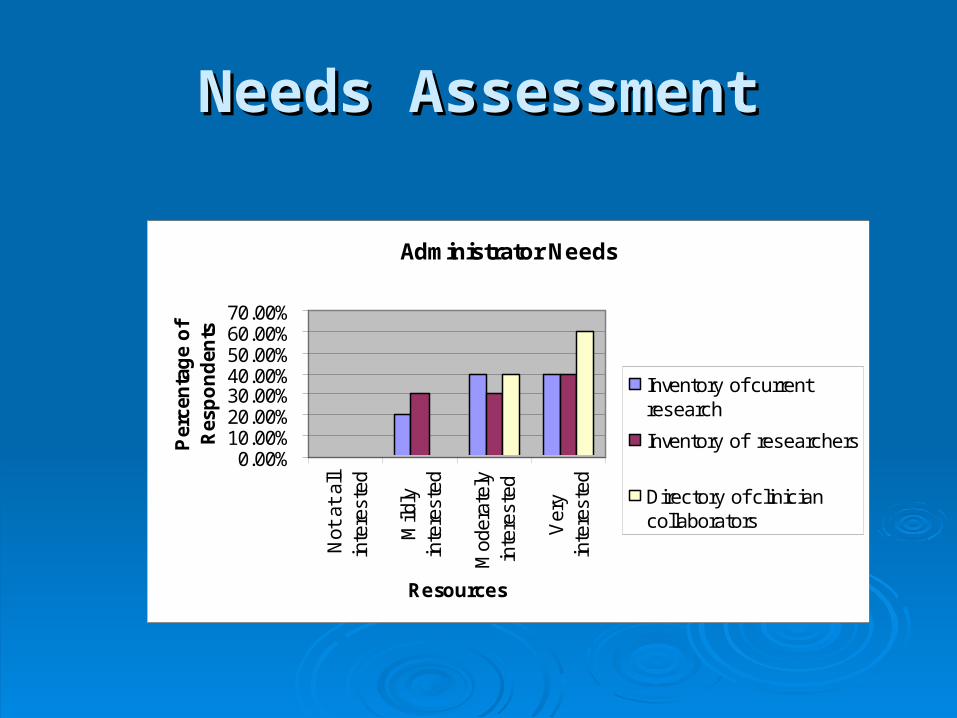
Needs AssessmentNeeds Assessment
Administrator Needs
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%
Not
at
all
inte
rest
ed
Mild
lyin
tere
sted
Mod
erat
ely
inte
rest
ed
Ver
yin
tere
sted
Resources
Per
cen
tag
e o
f R
esp
on
den
ts
Inventory of currentresearch
Inventory of researchers
Directory of cliniciancollaborators

Acknowledgements
The content of the preceding slides was derived from:
Dr. David Johnson “Developing a KT Plan in Grant Applications”
www.ahfmr.ab.ca/download.php/1ad4799af7bd4c0810fcaf2d571272f
CIHR website • http://www.cihr-irsc.gc.ca/e/39128.html• http://ktclearinghouse.ca/
CEBM website • www.cebm.net
McMaster KT+ website• http://plus.mcmaster.ca/KT/Default.aspx
Dr. DP Ryan, Director of Education & Knowledge Translation, Toronto
• rgps.on.ca/slides/knowledgetopracticeprocess.pdf