la bronchiolite : come riconoscerla per meglio curarla le ... corsi di formazione... · rsv...
TRANSCRIPT

La bronchiolite : come riconoscerla per meglio curarla
LE EVIDENZE SCIENTIFICHE PER LA TERAPIA LOCALE
Maurizio Poloni U.O. Pediatria - RIMINI

RSV INFECTION- BRONCHIOLITIS
• Leading cause of hospitalization in infants - Up to 3% of all children in first year of life are hospitalized
with bronchiolitis (18% of all hospitalizations in US) – 10-12% need intensive care
• Virtually all children have been infected with RSV by the age of 2 years
• Previous infection does not transmit persistent immunity and reinfection is common and can recur in the same RSV season
• Of RSV infected infants 40% will develop a LRTI
Wright Ped Pulmonol 2011 Glezen Am J Dis Child 1986

BURDEN OF RSV INFECTION IN ARGENTINA
Ferolla AJRCCM 2013
2011 season
Prospective study in 56,560 children < 2 years. 60% of respiratory infections in hospitalized children (n=1293) were due to RSV. Annual mortality rate for RSV was 7% . Life-threatening RSV infections are a heavy burden on infants in the developing world.



DIAGNOSIS OF BRONCHIOLITIS UK, Australia USA (EU)EU (age < 12m) (age < 2 yrs)
Bronchiolitis Bronchiolitis
inspiratory crackles wheezing + wheezing
Early onset Asthma ??? Everard CurrOp 2006

Hig risk for RSV bronchiolitis in Late preterms and select infants affected by rare disorders; a dilemma of specific prevenction
• Prematurity and BPD
• Age less than 12 weeks
• Congenital cardiac illness
• Immunodeficiency
• Congenital pulmonary anomalies
• Chronic pulmonary Disease (CF, PCD…)
• Neuromuscolar Disease
• Down Syndrome
Pediatrics 2006;118;1774-1793
Manzoni – Early Human Dev 2012

Withholding therapy is much more difficult than giving it !
NEJM 2007;357:402-4


Impact of a bronchiolitis guideline on E.D. resource use and cost: a segmented time-series analysis
Akenroye AT, Baskin MN, Samnaliev M, Stack AM Pediatrics. 2014 Jan
Novembre 2007 - Aprile 2013 2929 Bambini (1 – 12 mm)
CONFRONTO CON IL PERIODO PRECEDENTE
RX: - 23%Test per RSV: - 11%Salbutamolo: - 7%
RISPARMIO TOTALE DOPO 2 AA : 196.409 dollari

Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis.
(children from 1 through 23 months of age)
Pediatrics 2014 Nov


Clinical Questions
Efficacy of pharmaceutical therapies for treatment of bronchiolitis
Role of prophylaxis in prevention of bronchiolitis

Efficacy of pharmaceutical therapies for treatment of bronchiolitis
Management of Bronchiolitis
When supplemental O2 is indicated?

Supplemental O2 is indicated when SatO2 falls persistently < 90%
Infants with O2 saturation levels < 92% should receive supplemental oxygen by nasal cannulae or facemask

Supplemental O2 is indicated when SatO2 falls < 90% or < 92%
Impact on the number of hospitalization!!!
The routine measurement of O2 saturation may be responsible for the increased admission rates of the last years
Smyth Lancet 2006
Supplemental O2 HOW TO OBTAIN A GOOD MEASUREMENT OF O2 SATURATION ?
• proper probe and appropriate placement
• avoid movement
• stability of readings pulse amplitude
• vasoconstriction and hypothermia
• ???

Suctioning of the nares should be performed before to measure O2 saturation
HOW TO OBTAIN A GOOD MEASUREMENT OF O2 SATURATION?

O2 SATURATION IN INFANT S WITH BRONCHIOLITISBEFORE AND AFTER SUCTIONING OF THE NARES
88
92
100
PRE-NARES SUCTIONING
POST-NARES SUCTIONING
▪ n = 30
▪ Sat O2 < 96%
▪ Measurement : pre and post 10 min.

INDICAZIONI AL RICOVERO- Sat O2 persistentemente < 90- 92 %
- Entità del Distress respiratorio
- Presenza di Apnea (5-10 % RSV, HRV)
- Disidratazione (introduzione di liquidi nelle 24 ore precedenti < al 50 % dell’abituale)
- Presistenti fattori di rischio (prematurità, BPD, CHD,
immunodeficienza, malformazione delle vie aeree, severo
deficit neurologico, Fibrosi Cistica)


INDICAZIONI AL RICOVERO
-Presistenti fattori di rischio (prematurità, BPD, CHD,
immunodeficienza, malformazione delle vie aeree, severo
deficit neurologico, Fibrosi Cistica)
DA PRENDERE IN CONSIDERAZIONE
• Fattori sociali (distanza dall'ospedale, accesso ai mezzi di trasporto o di comunicazione, collaborazione dei genitori)
• Fattori ambientali (esposizione al fumo di sigaretta, dimora umida o fredda, abitazione affollata)



TERAPIA DI SUPPORTO
NOT EFFECTIVE

N
OT E
FFEC
TIVE
TERAPIA FARMACOLOGICA
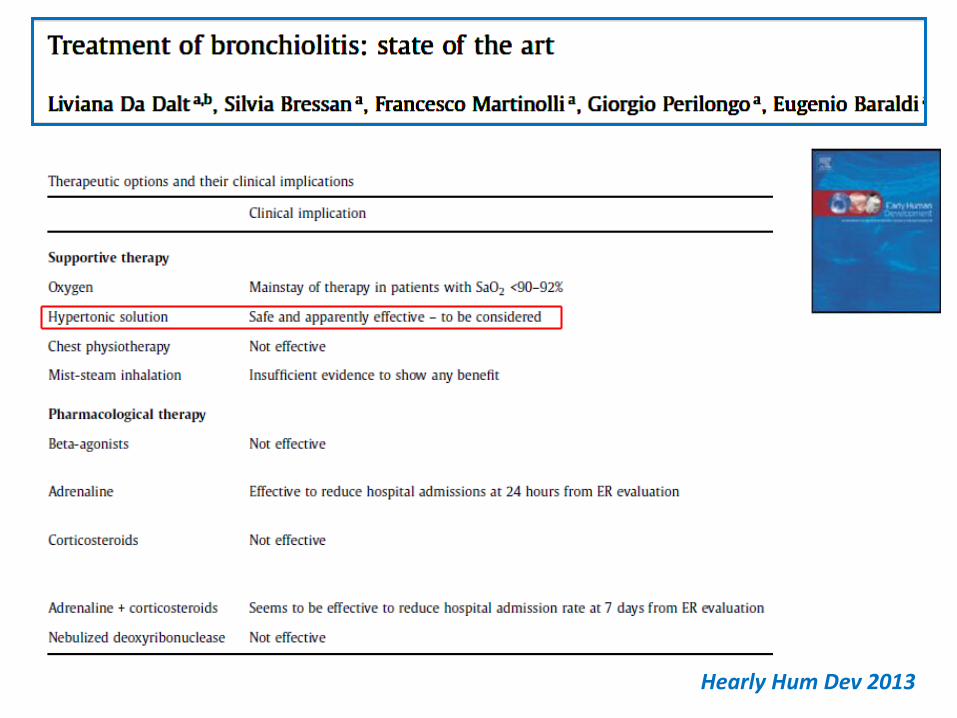
Hearly Hum Dev 2013

RCT n=96
4 mL of 3% hypertonic saline vs 0.9% every 6 hrs (+ albuterol or epinephrine as needed)
26% reduction in the length of hospitalization ($150 million annually)
No adverse effects were observed
Kuzik J Pediatrics 2007

Le soluzioni Saline
Soluzione Fisiologica NaCl 0,9% (NS)
Soluzione Ipertonica NaCl (HS)
1,5 %3%6-7%

Le soluzioni saline e l’apparato respiratorio
Modalità di Somministrazione L’aerosol è una sospensione di particelle solide o liquide
I vari tipi di device inalatori si differenziano tra loro per ildiametro che imprimono alle particelle nebulizzate (DAMM:Diametro Aerodinamico Mediano di Massa)
per le vie aeree superiori (device endonasali)
DAMM > 10 micron
vie aeree inferiori (device rino-orobuccali)
DAMM < 5 micron

L’apparato respiratorio

L’epitelio dell’apparato respiratorio

L’epitelio dell’apparato respiratorio
Legenda:ML = strato mucoso ; PCL = liquido periciliare; ASL = liquido di superficie delle vie aeree; MCC = clearance mucociliare; ENaC = canale epiteliale del sodio;CaCC = canali del calcio; CFTR = Cistic Fibrosis Transmembrane Regulator
Mandelberg A, Pediatric Pulmonol 2009
SOLUZIONE SALINA IPERTONICA
PATOLOGIE COME FIBROSI CISTICA E BRONCHIOLITE
PRESENTANO IL MEDESIMO APPROCCIO TERAPEUTICO….
???


Pediatric Pulmonol 2010


Schematic representation of theantimicrobial, immunomodulatoryand mucolytic properties of HS.
1.HS draws water into the dehydratedCF periciliary layer and improvesmucus rheology and enhancesmucociliary clearance.
2.IL-37, an antimicrobial protein isreleased by HS via disruption of theelectrostatic interaction between IL-37 and anionic glycosaminoglycans(GAGs).
3. HS liberates IL-8 from anionic matrices (GAGs) rendering the chemokinesusceptible to proteolytic degradation by neutrophil elastase, therebydecreasing inflammation.

Conclusion:
The positive effect of nebulised HS on mucociliaryclearance is based on restoring the liquid layer lining theairways.
Studies are now revealing that HS can also function byreleasing essential antimicrobial and immune moleculesfrom complexation with ionic matrices thus improvingboth antimicrobial efficiency and resolution ofinflammation.
These observations suggest that HS has beneficialtherapeutic effects other than simply increasingmucociliary clearance and thus further investigations ofthe potential mechanisms of this currently available



Wheezing prescolare
Randomized, controlled, double-blind study
41 children (mean age 31.9 6 17.4 months, range 1–6years) presented with wheezing to the emergencydepartment
Randomized after 1 albuterol inhalation to receive either4 mL of hypertonic saline 5% (HS) (n = 16) or 4 mL ofnormal saline (NS) (n = 25), both with 0.5 mL albuterol,twice every 20 minutes in the Emergency Departmentand 4 times a day thereafter if hospitalized

Wheezing prescolare

INDUCE BRONCOSPASMO?


CONCLUSIONI
4 moderati eventi avversi (1%) - 3 tosse catarraledurante la nebulizzazione
- 1 broncospasmo
L’USO DI HS 3% E’ SICURO ANCHE SENZA SALBUTAMOLO
Ralston Pediatrics 2010

Nebulized hypertonic saline (HS) solution for bronchiolitis in infants
11 trials involving 1090 infants with mild to moderate acute viral bronchiolitis 4 trials
Current evidence suggests nebulised 3% saline:
- reduces the length of hospital stay among infants hospitalised with non-severe acute viral bronchiolitis
- improves the clinical severity score in both outpatient and inpatient populations.
Zhang - Cochrane 2013 Jul
Nebulized hypertonic saline (HS) solution for bronchiolitis in infants
11 trials involving 1090 infants with mild to moderate acute viral bronchiolitis 4 trials
Current evidence suggests nebulised 3% saline:
- reduces the length of hospital stay among infants hospitalised with non-severe acute viral bronchiolitis
- improves the clinical severity score in both outpatient and inpatient populations.
Zhang - Cochrane 2013 Jul

EDITORIALE
“….Dalla nostra lettura della revisione Cochrane, che ora dovrà
essere aggiornata, e quella degli studi di Florin e Wu, pensiamo comunque che non sia il caso di introdurre l’uso routinario nei reparti di emergenza della soluzione salina ipertonica, la quale potrebbe comunque
giocare un ruolo importante nei bambini ricoverati per bronchiolite....”
Jama Pediatr. Published online May 26, 2014

The effect of 3% and 6% HS in Viral Bronchiolitis : a RCTTeunissen, ERJ Ottobre 2014
“….Except for a possible effect of nebulised hypertonic saline, no evidence-based therapy is available. …..efficacy of nebulised 3% and 6% hypertonic saline compared with 0.9% hypertonic saline in children hospitalised with viral bronchiolitis…..”Salbutamol was added to counteract possible bronchial constriction
PRIMARY ENDPOINT :length of hospital stay
Secondary outcomes : need for supplemental oxygen and tube feeding
N = 292 (median age 3.4 months / moderate-to-severe viral bronchiolitis)
RESULTS
The median length of hospital stay did not differ between the groups
The need for supplemental oxygen or tube feeding did not differ significantly
Adverse effects were similar in the three groups.

UPDATE 2014
NO nei reparti di pronto soccorso
SI in caso di ricovero ospedalieroHS


Bronchodilators for bronchiolitis
Gadomski AM, Brower MCochrane Database Syst Rev 2010
Epinephrine for bronchiolitis
Hartling L, Bialy LM, et Al.Cochrane Database Syst Rev 2011

Bronchodilators SHOULD NOT be used routinely in the management of bronchiolitis
- overall, 1 in 4 may have a transient improvement in clinical score
- no impact in the overall course of the illness: some improvement in short-term outcomes (clinical score…) no effects on admission rates and lenght of hospital stay
A carefully monitored trial of α-adrenergic or β-adrenergic is an option
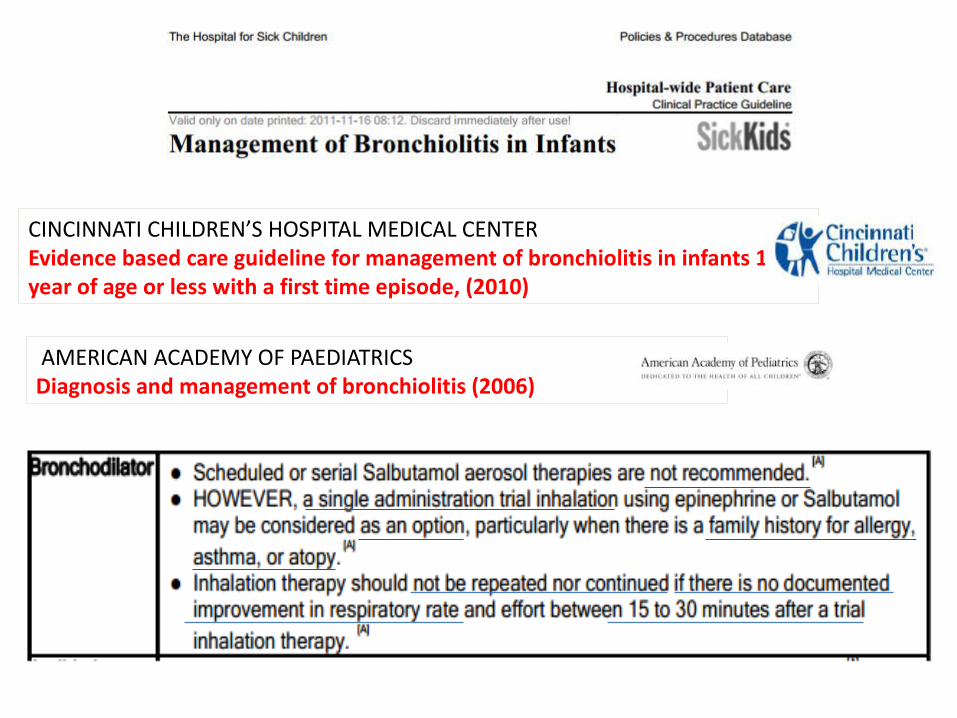
CINCINNATI CHILDREN’S HOSPITAL MEDICAL CENTER Evidence based care guideline for management of bronchiolitis in infants 1 year of age or less with a first time episode, (2010)
AMERICAN ACADEMY OF PAEDIATRICS Diagnosis and management of bronchiolitis (2006)

Update 2014
Uso di una dose di broncodilatatore non modifica il decorso della malattia
NON RACCOMANDATA

Update 2014
Uso di una dose di broncodilatatore non modifica il decorso della malattia
NON RACCOMANDATA
Which bronchodilator ?
Epinephrine may be the preferred bronchodilator for this trial in emergency department (0.25 mg/kg/dose)
Epinephrine has demonstrated slightly better clinical effect than albuterol possibily related to the α effect of the medication

EPINEPHRINE FOR BRONCHIOLITIS
Hartling L, Bialy LM, Vandermeer B, Tjosvold L, Johnson DW, Plint AC, Klassen TP, Patel H, Fernandes RM
Cochrane Database Syst Rev 2011
Riduzione della necessità di ricovero in ED
NON riduzione dei tempi di degenza nei b. ricoverati

The largest one meta-analysis on bronchiolitis 48 studies and 5000 patients
Adrenaline reduced admission on day 1 in the outpatient- emergency setting
BUT no effect for inpatients!
BMJ 2011;342:d1714

June 13, 2013
Skjerven HO, Hunderi JO, Brügmann-Pieper SK, Brun AC, Engen H, Eskedal L, Haavaldsen M, Kvenshagen B, Lunde J, Rolfsjord LB, Siva C, Vikin T, Mowinckel P, Carlsen KH, Lødrup Carlsen KC

404 infants (mean age 4.2 m.) admitted to a pediatric department inhaled adrenaline vs. saline 0,9% (on-demand vs fixed-schedule) Primary outcome: lenght of hospital stay
In the treatment of acute bronchiolitis, inhaled racemic adrenaline is NOT more effective than inhaled saline !!!
Skjerven NEJM 2013 June 13

Nebulised Adrenaline at home?
Because of the lack of studies and potential adverse effects nebulised adrenaline is NOT recommended in the home setting

Efficacy of pharmaceutical therapies for treatment of bronchiolitis
Corticosteroids are NOT recommended for the treatment of acute bronchiolitis
60% hospitalized children with brochiolitis receive corticosteroids
sistemic corticosteroids - no benefits were found in length of stay, clinical score or outcomes
(Cochrane 2010)
inhaled corticosteroids - no benefits in the course of acute disease
inhaled corticosteroids - no benefits in the prevention of post bronchiolitic wheeze (Cochrane 2011)

Immunohistochemistry of lungs on day 7 after infection RSV
Normal Neutrophils infiltration
Huck et al Respir Research 2007

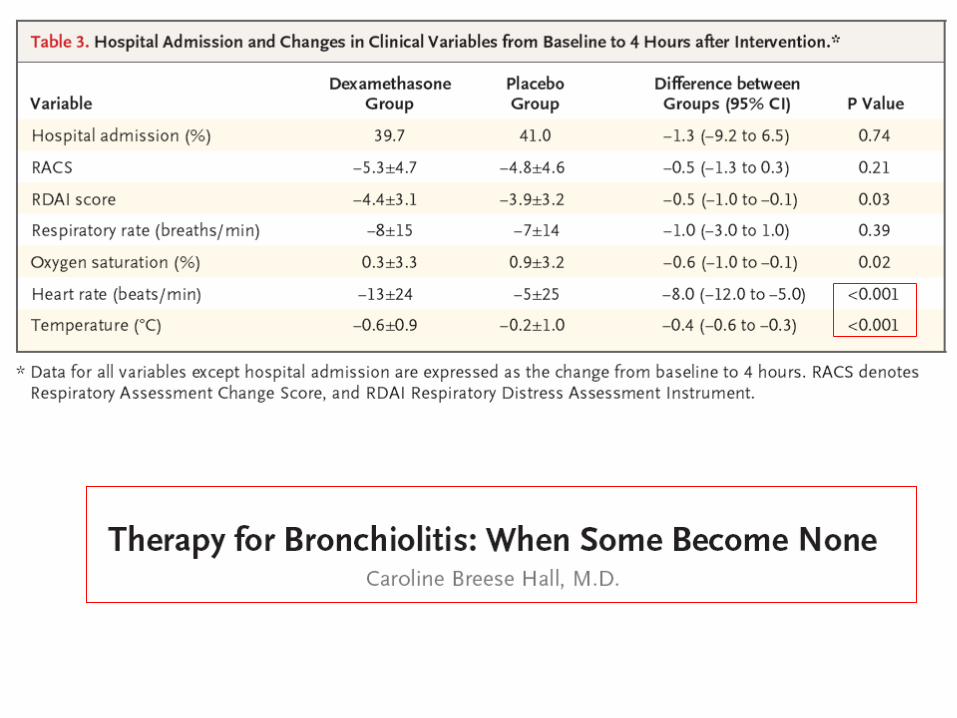
600 children (2-12 months) - first episode of bronchiolitis: 20 emergency departments Excluded children with previous wheeze episodes Dexamethasone os 1mg/kg vs placebo
Outcomes: - Hospital admission after 4 hr of observation - Clinical Score - Length of hospital stay (LOS)
Corneli et al NEJM 2007;357:331

GLUCOCORTICOIDS FOR ACUTE VIRAL BRONCHIOLITIS IN INFANTS AND YOUNG CHILDREN
RCTs comparing systemic or inhaled steroids versus placebo in children with bronchiolitis under 24 months. 17 trials - 2596 participants
Current evidence does not support a clinically effect of systemic or inhaled steroids on admissions or length of hospitalisation
Cochrane Database Syst Rev. 2013 Jun


Withholding therapy is much more difficult than giving it !
NEJM 2007;357:402-4

Gupta et al. Indian Pediatr 2008
Boogaard Chest 2007
Kneyber Pediatr Pulm 2008
Bisgaard AJRCCM 2008

PEDIATRICS AAP GUIDE-LINE UPDATE 2014
• AAP : non raccomandata dose di prova con broncodilatatore (albuterolo o salbutamolo)
EBM : broncodilatatori ininfluenti sul decorso della bronchiolite (qualità evidenza: B, forte raccomandazione)
S.Ralston (American Academy of Pediatrics Subcommittee on Bronchiolitis) Commento - Bmj Ottobre 2014
…..le linee guida non ti dicono cosa fare nel caso del singolo paziente (= base condivisa evidence-based)
“La grande maggioranza dei pazienti con bronchiolite non beneficia di broncodilatatori, questo non significa che il paziente occasionale non potrebbe trarne benefici”

• Uso a breve termine di SOLUZIONE SALINA IPERTONICA non impatto clinico
EBM : una, due, o tre dosi in D.E. non incide sul rischio di
ospedalizzazione (maggioranza degli studi, numero consistente)
Ralston : Commento - Bmj Ottobre 2014
non si può ignorare la Revisione Cochrane del 2013
durata Ricovero = -1 giorno
HS utile nella bronchiolite se somministrata IN MODO
COSTANTE per un PERIODO RELATIVAMENTE PROLUNGATO
PEDIATRICS AAP GUIDE-LINE UPDATE
NBQUINDI

Some final thoughts……..
• Several aspects of bronchiolitis management are still debated
• Beta-agonists and steroids (systemic and inhaled) are not recommended for routine use
• Hypertonic saline may provide significant benefit but………….






Adults (n=88) experimentally infected with wild-type RSV A nasal spray of RNA-interference (ALN-RSV01) or saline placebo was administered for 3 days after RSV inoculation.
RNA-i is a natural mechanism regulating protein expression
Acquisition of infection lower (p<0.007) in ALN-RSV01 treated
DeVincenzo PNAS 2010
Plint AC, Johnson DW, Patel H, Wiebe N, Correll R, Brant R, Mitton C, Gouin S, Bhatt M, Joubert G, Black KJ, Turner T, Whitehouse S, Klassen TP: Pediatric emergency research canada (PERC) epinephrine and dexamethasone in children with bronchiolitis.N Engl J Med 2009, 360(20):2079-2089
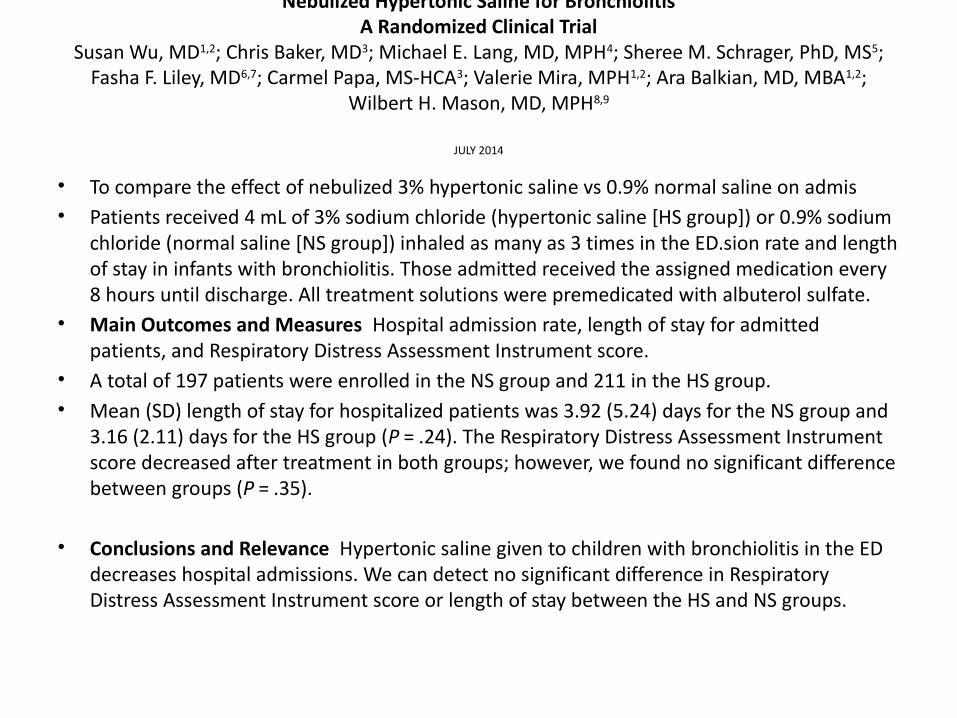
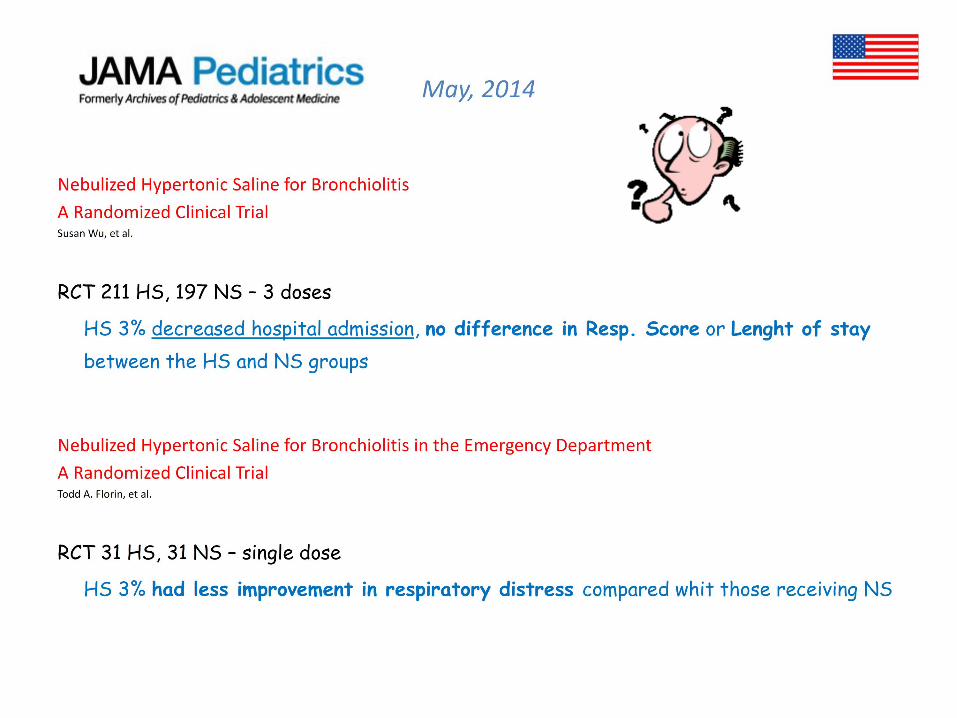
Nebulized Hypertonic Saline for BronchiolitisA Randomized Clinical Trial
Susan Wu, MD1,2; Chris Baker, MD3; Michael E. Lang, MD, MPH4; Sheree M. Schrager, PhD, MS5; Fasha F. Liley, MD6,7; Carmel Papa, MS-HCA3; Valerie Mira, MPH1,2; Ara Balkian, MD, MBA1,2;
Wilbert H. Mason, MD, MPH8,9
JULY 2014
• To compare the effect of nebulized 3% hypertonic saline vs 0.9% normal saline on admis• Patients received 4 mL of 3% sodium chloride (hypertonic saline [HS group]) or 0.9% sodium
chloride (normal saline [NS group]) inhaled as many as 3 times in the ED.sion rate and length of stay in infants with bronchiolitis. Those admitted received the assigned medication every 8 hours until discharge. All treatment solutions were premedicated with albuterol sulfate.
• Main Outcomes and Measures Hospital admission rate, length of stay for admitted patients, and Respiratory Distress Assessment Instrument score.
• A total of 197 patients were enrolled in the NS group and 211 in the HS group. • Mean (SD) length of stay for hospitalized patients was 3.92 (5.24) days for the NS group and
3.16 (2.11) days for the HS group (P = .24). The Respiratory Distress Assessment Instrument score decreased after treatment in both groups; however, we found no significant difference between groups (P = .35).
• Conclusions and Relevance Hypertonic saline given to children with bronchiolitis in the ED decreases hospital admissions. We can detect no significant difference in Respiratory Distress Assessment Instrument score or length of stay between the HS and NS groups.

Nebulized Hypertonic Saline for Bronchiolitis in the Emergency DepartmentA Randomized Clinical TrialTodd A. Florin, MD, MSCE1,2; Kathy N. Shaw, MD, MSCE3,4; Marlena Kittick, MPH3; Stephen Yakscoe, BA3; Joseph J. Zorc, MD, MSCE3,4
July 2014
• Objective To determine whether nebulized 3% HS compared with normal saline (NS) improves respiratory distress in infants with bronchiolitis not responding to standard treatments in the emergency department.
• Interventions Patients were randomized to receive either nebulized 3% HS (HS group) or NS (NS group).
• Main Outcomes and Measures The primary outcome was change in respiratory distress at 1 hour after the intervention, as measured by the Respiratory Assessment Change Score (a decrease indicates improvement). Secondary outcomes included vital signs, oxygen saturation, hospitalization, physician clinical impression, parental assessment, and adverse events.
• Results The 31 patients enrolled in each treatment arm had similar baseline demographic and clinical characteristics. At 1 hour after the intervention, the HS group demonstrated significantly less improvement in the median Respiratory Assessment Change Score compared with the NS group
• There were no significant differences in heart rate, oxygen saturation, hospitalization rate, or other outcomes.
• Conclusions and Relevance Infants with bronchiolitis and persistent respiratory distress after standard treatment in the emergency department had less improvement after receiving 3% HS compared with those who received NS. Based on these results and the existing evidence, administration of a single dose of 3% HS does not appear to be indicated to treat bronchiolitis in the acute care setting.

Per i pediatri in cerca di risposte sul modo migliore curare i loro pazienti nulla può essere più frustrante di due studi clinici controllati (RCT) con risultati contraddittori scrivono in un editoriale su JAMA Pediatrics due ricercatori canadesi - Sim Grewal, dell’Università dell’Alberta e Terry Klassen, dell’Università di Winnipeg - a proposito di due studi clinici di recente pubblicati. Nel primo, di Todd Florin e colleghi, 62 pazienti con bronchiolite e distress respiratorio persistente sono stati randomizzati a ricevere soluzione fisiologica o soluzione ipertonica al 3%: a un’ora dall’intervento le condizioni respiratorie del gruppo trattato con l’ipertonica erano migliorate meno rispetto ai pazienti curati con soluzione salina. Nel secondo studio, svolto da Suzan Wu e colleghi, 408 bambini con bronchiolite sono stati randomizzati a ricevere ipertonica o fisiologica in un reparto di emergenza. Gli autori hanno riscontrato un tasso di ricovero nel gruppo ipertonica inferiore al gruppo fisiologica, senza peraltro che emergessero differenze significative tra i due gruppi nella durata del ricovero o nelle condizioni respiratorie. «Valutare l'efficacia della soluzione salina ipertonica nel trattamento della bronchiolite non è facile, e una limitazioni più significative nei dati pubblicati finora è la casistica limitata» sottolineano i due autori, ricordando che l’ultima revisione sistematica sul ruolo della salina ipertonica nel trattamento della bronchiolite è la Cochrane del 2013, da cui emerge che probabilmente l’ipertonica non serve ai pazienti trattati nei reparti di emergenza ma può essere utile nel ridurre la degenza in ospedale. «I due studi appena pubblicati, apparentemente contraddittori e potenziale fonte di confusione, per svolgere appieno il loro ruolo di ricerca sull’argomento dovranno essere incorporati in una revisione sistematica aggiornata per vedere se i risultati globali cambieranno» aggiungono Grewal e Klassen. E concludono: «Dalla nostra lettura della revisione Cochrane, che ora dovrà essere aggiornata, e quella degli studi di Florin e Wu, pensiamo comunque che non sia il caso di introdurre l’uso routinario nei reparti di emergenza della soluzione salina ipertonica, la quale potrebbe comunque giocare un ruolo importante nei bambini ricoverati per bronchiolite».
Jama Pediatr. Published online May 26, 2014