laboratory findings and bone marrow cytomorphology
TRANSCRIPT
Laboratory Findings and Bone Marrow
Cytomorphology Interpretation in Multiple
Myeloma
WEBINAR JOWee 15
Multiple myeloma : Diagnosis and management
Saturday, February 6th 2021
Dr dr Agus Susanto Kosasih Sp.PK-K,MARS
Clinical Pathology Laboratory, Dharmais Cancer Hospital
National Cancer Centre
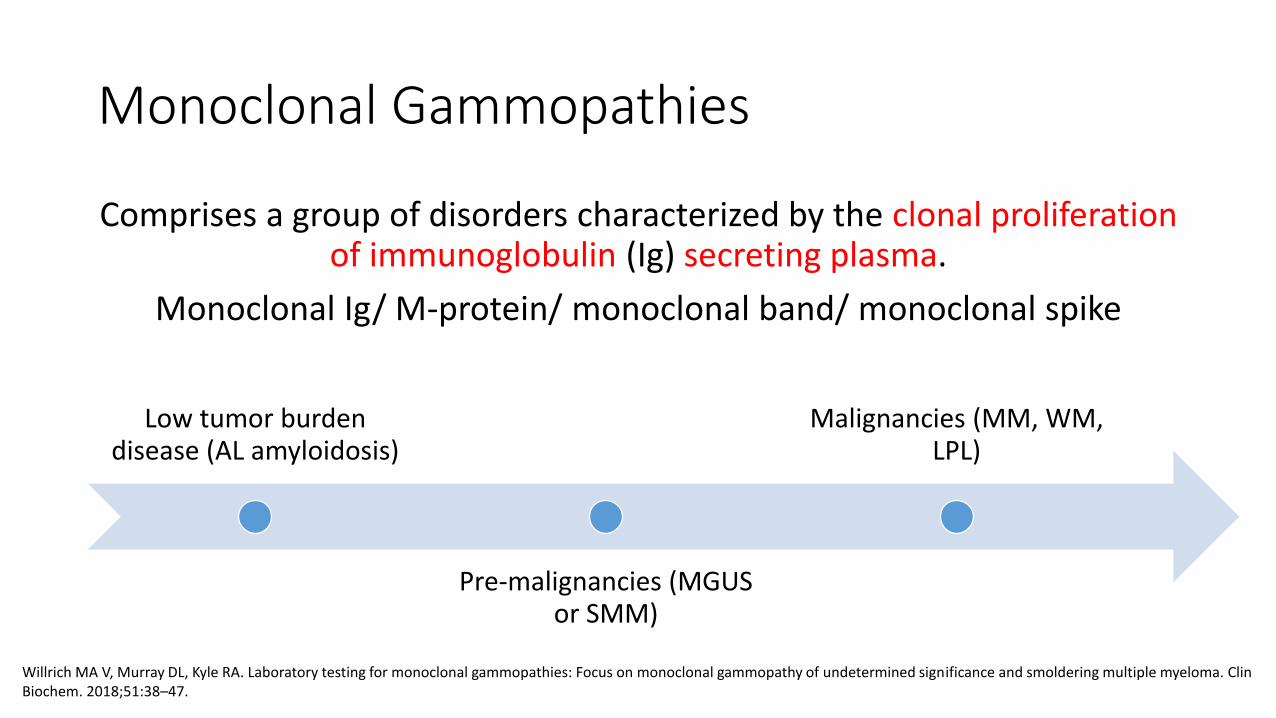
Monoclonal Gammopathies
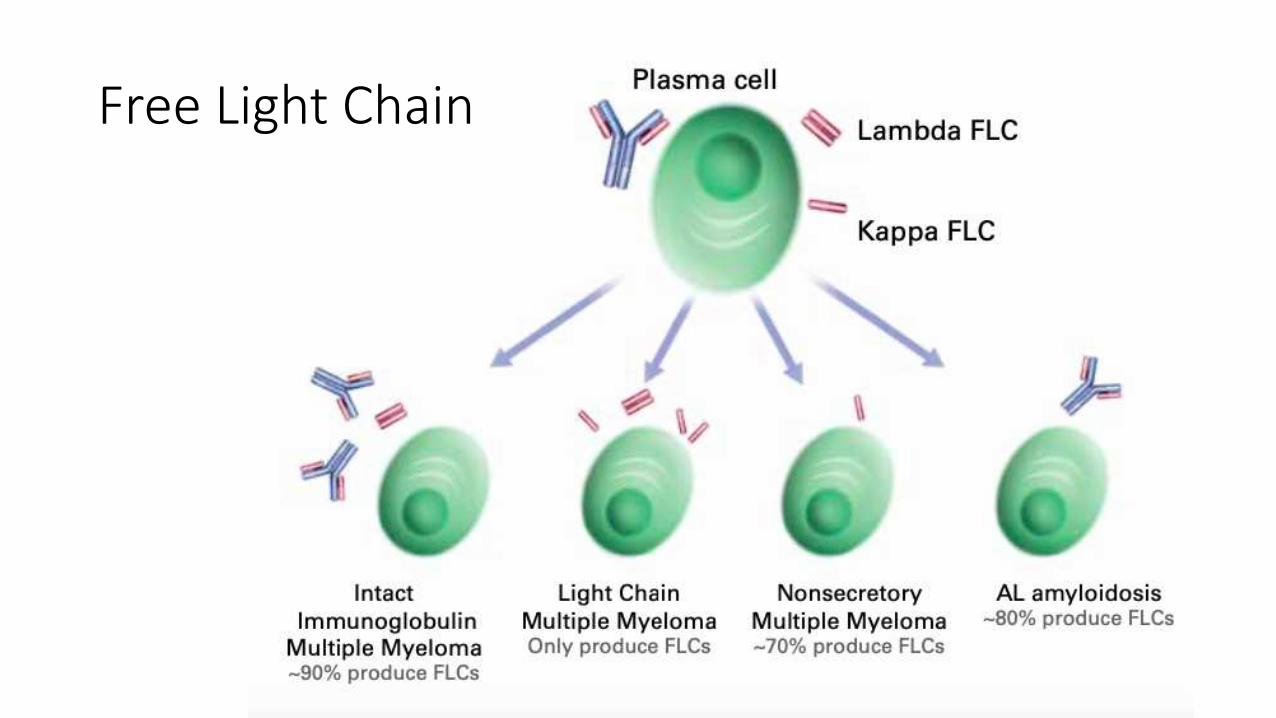
Comprises a group of disorders characterized by the clonal proliferation of immunoglobulin (Ig) secreting plasma.
Monoclonal Ig/ M-protein/ monoclonal band/ monoclonal spike
Low tumor burden disease (AL amyloidosis)
Pre-malignancies (MGUS or SMM)
Malignancies (MM, WM, LPL)
Willrich MA V, Murray DL, Kyle RA. Laboratory testing for monoclonal gammopathies: Focus on monoclonal gammopathy of undetermined significance and smoldering multiple myeloma. ClinBiochem. 2018;51:38–47.
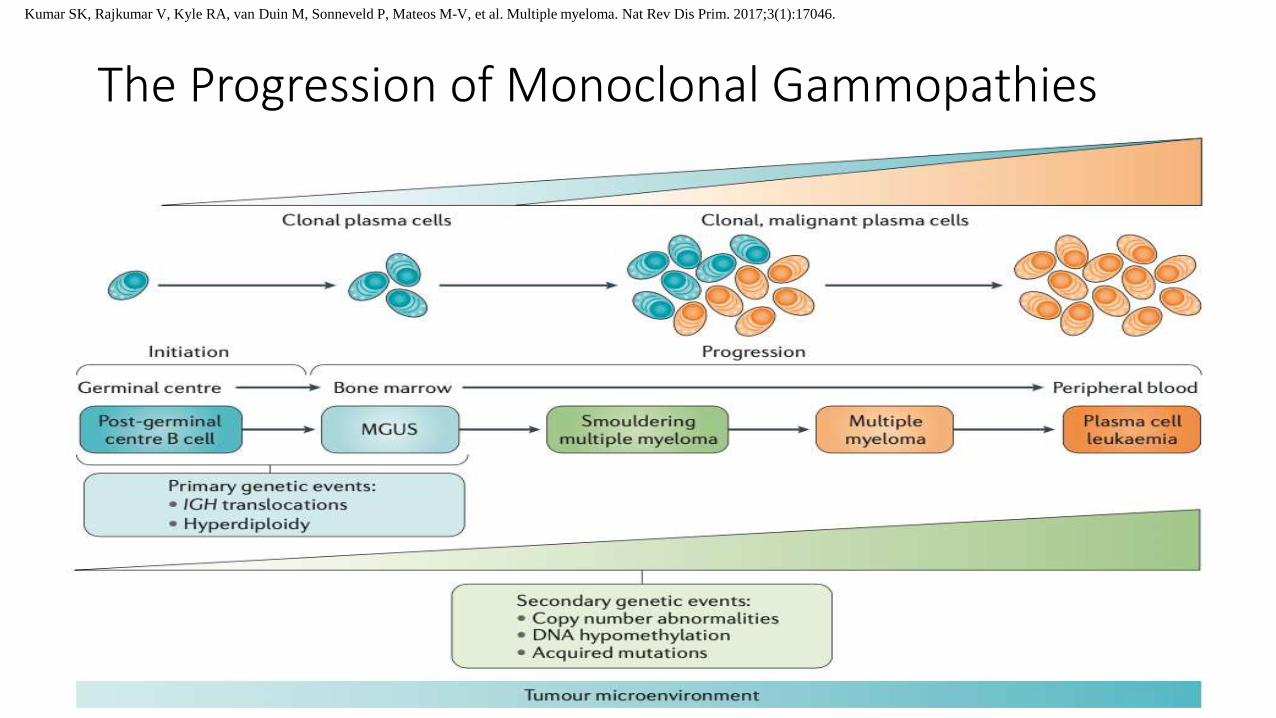
The Progression of Monoclonal Gammopathies
Kumar SK, Rajkumar V, Kyle RA, van Duin M, Sonneveld P, Mateos M-V, et al. Multiple myeloma. Nat Rev Dis Prim. 2017;3(1):17046.
Multiple Myeloma
• Definition:
• A bone marrow-based, multifocal neoplastic proliferation of plasma cells, usually associated with M protein in serum and/or urine and evidence of end organ damage related to plasma cell neoplasm
• Epidemiology:
• 1% of malignancy tumors
• 10 – 15% of hematopoietic neoplasm
• 20% death from hematological malignancies
• Incidence increases progressively with age, 90% cases aged > 50 years(median diagnosis ~ 70 years)
WHO/IARC. WHO classification of tumours of haematopoietic and lymphoid tissues. Revised 4t. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al., editors. Lyon: IARC; 2017.
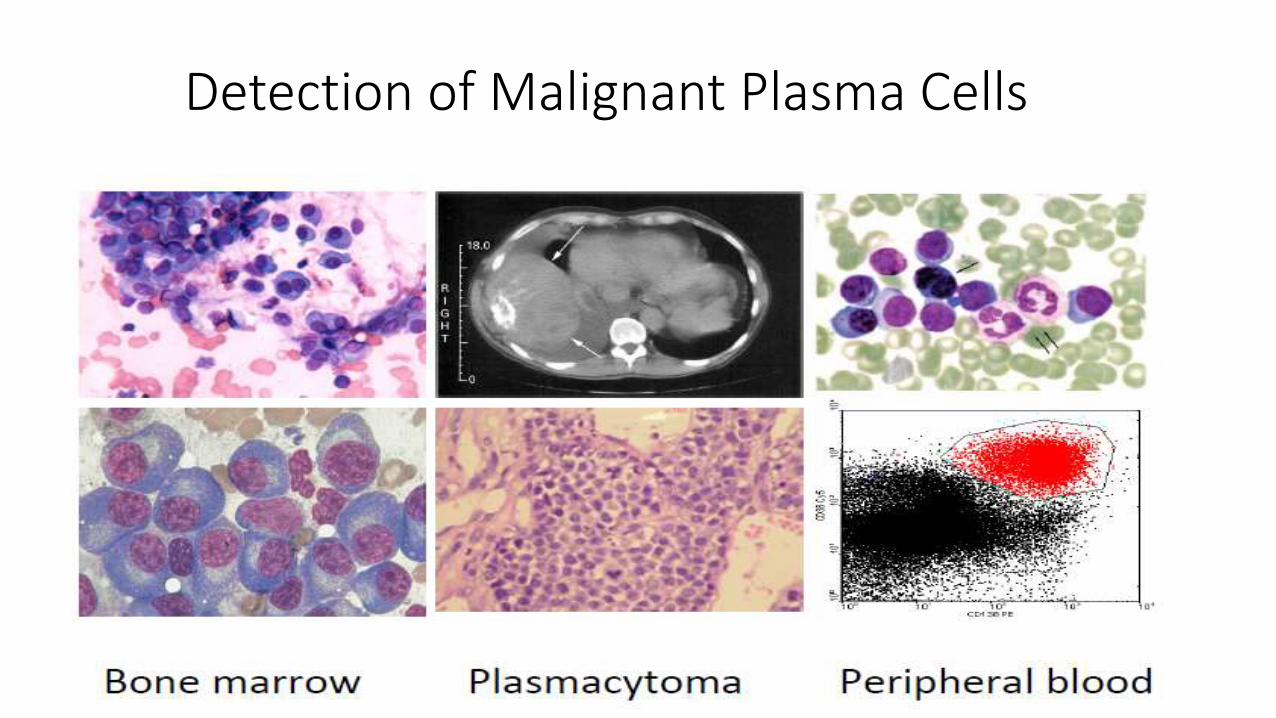
Detection of Malignant Plasma Cells
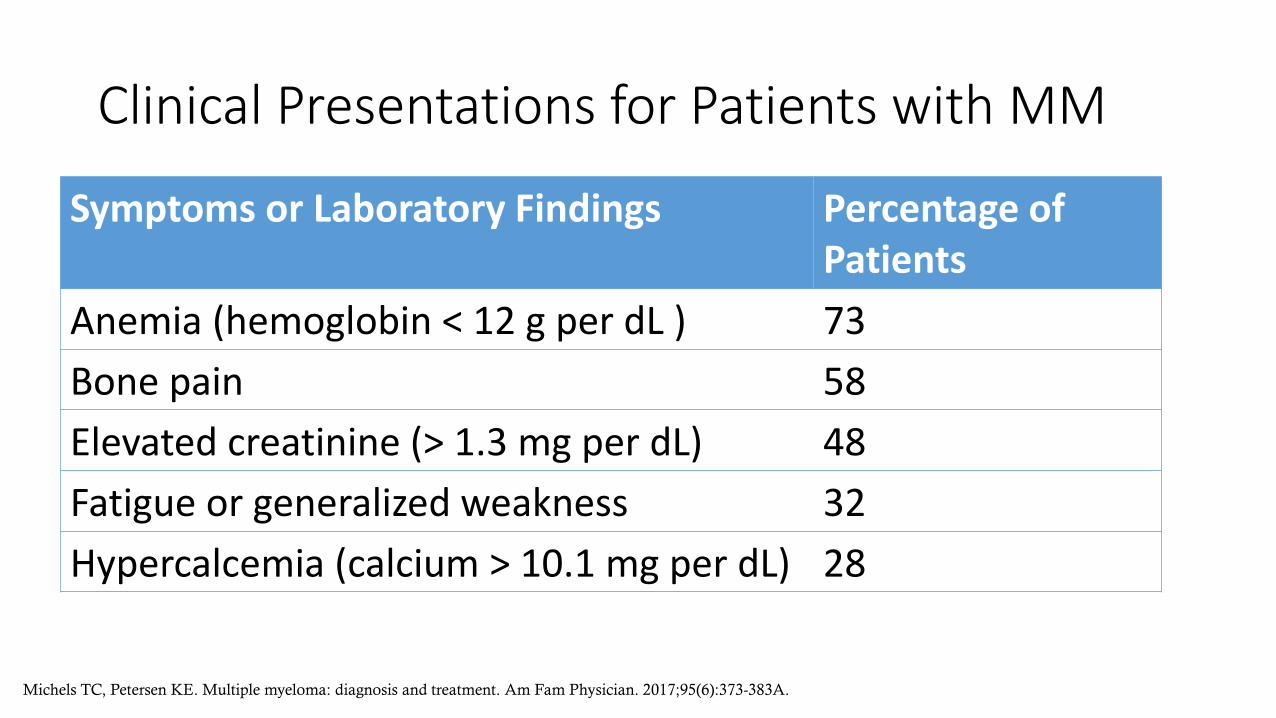
Clinical Presentations for Patients with MM
Symptoms or Laboratory Findings Percentage of Patients
Anemia (hemoglobin < 12 g per dL ) 73
Bone pain 58
Elevated creatinine (> 1.3 mg per dL) 48
Fatigue or generalized weakness 32
Hypercalcemia (calcium > 10.1 mg per dL) 28
Michels TC, Petersen KE. Multiple myeloma: diagnosis and treatment. Am Fam Physician. 2017;95(6):373-383A.

Laboratory Finding
• High ESR • Anaemia, thrombocytopenia/
pancytopenia• Rouleaux formation in peripheral
blood smears• Hyperglobulinemia• Hypercalcemia• Proteinuria• Marrow plasmacytosis
clonal > 10 %
Rouleaux Formation
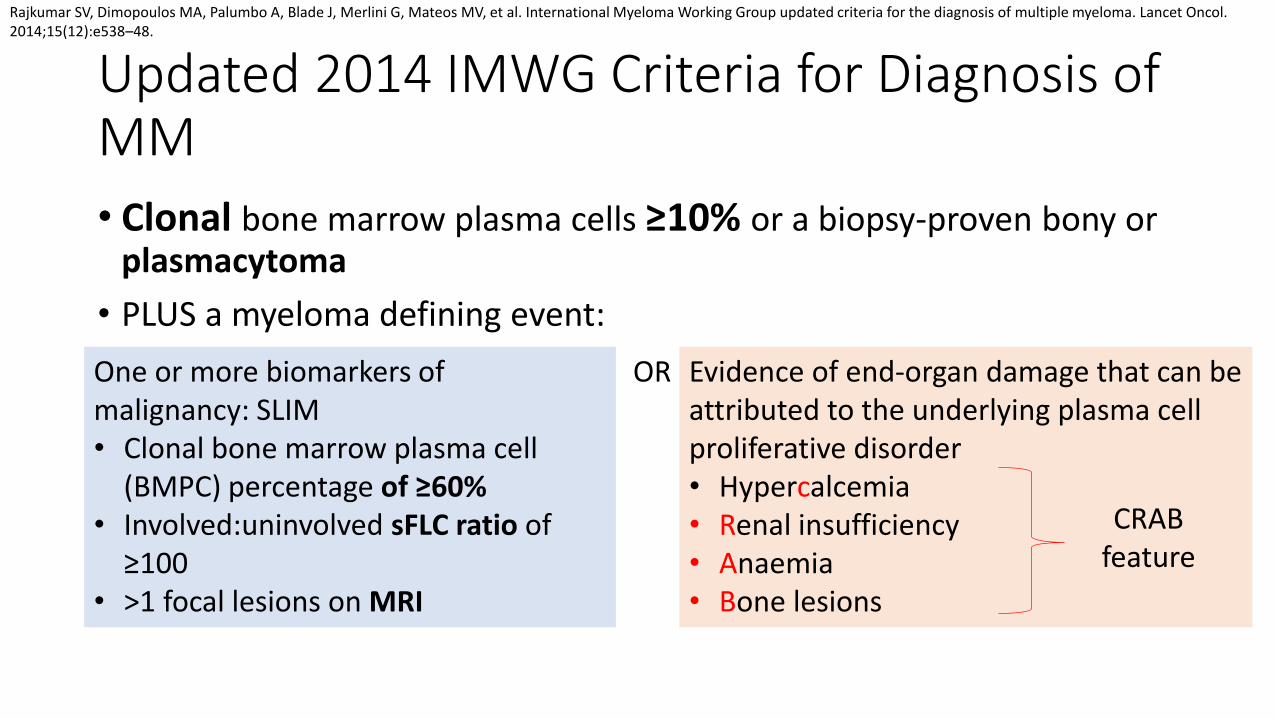
Updated 2014 IMWG Criteria for Diagnosis of MM
• Clonal bone marrow plasma cells ≥10% or a biopsy-proven bony or plasmacytoma
• PLUS a myeloma defining event:
One or more biomarkers of malignancy: SLIM• Clonal bone marrow plasma cell
(BMPC) percentage of ≥60% • Involved:uninvolved sFLC ratio of
≥100 • >1 focal lesions on MRI
Evidence of end-organ damage that can be attributed to the underlying plasma cell proliferative disorder• Hypercalcemia• Renal insufficiency• Anaemia• Bone lesions
OR
CRAB feature
Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos MV, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538–48.
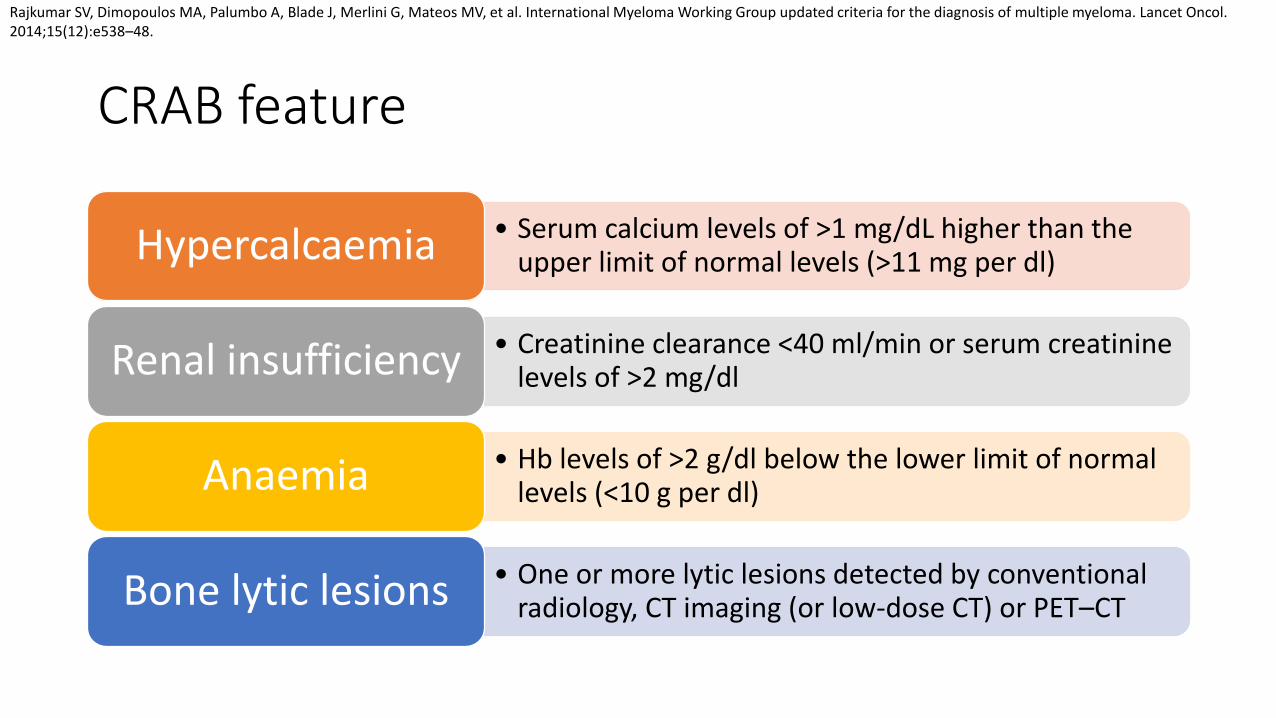
CRAB feature
• Serum calcium levels of >1 mg/dL higher than the upper limit of normal levels (>11 mg per dl) Hypercalcaemia
• Creatinine clearance <40 ml/min or serum creatinine levels of >2 mg/dl Renal insufficiency
• Hb levels of >2 g/dl below the lower limit of normal levels (<10 g per dl) Anaemia
• One or more lytic lesions detected by conventional radiology, CT imaging (or low-dose CT) or PET–CT Bone lytic lesions
Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos MV, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538–48.
Initial Diagnostic Workup of Multiple Myeloma
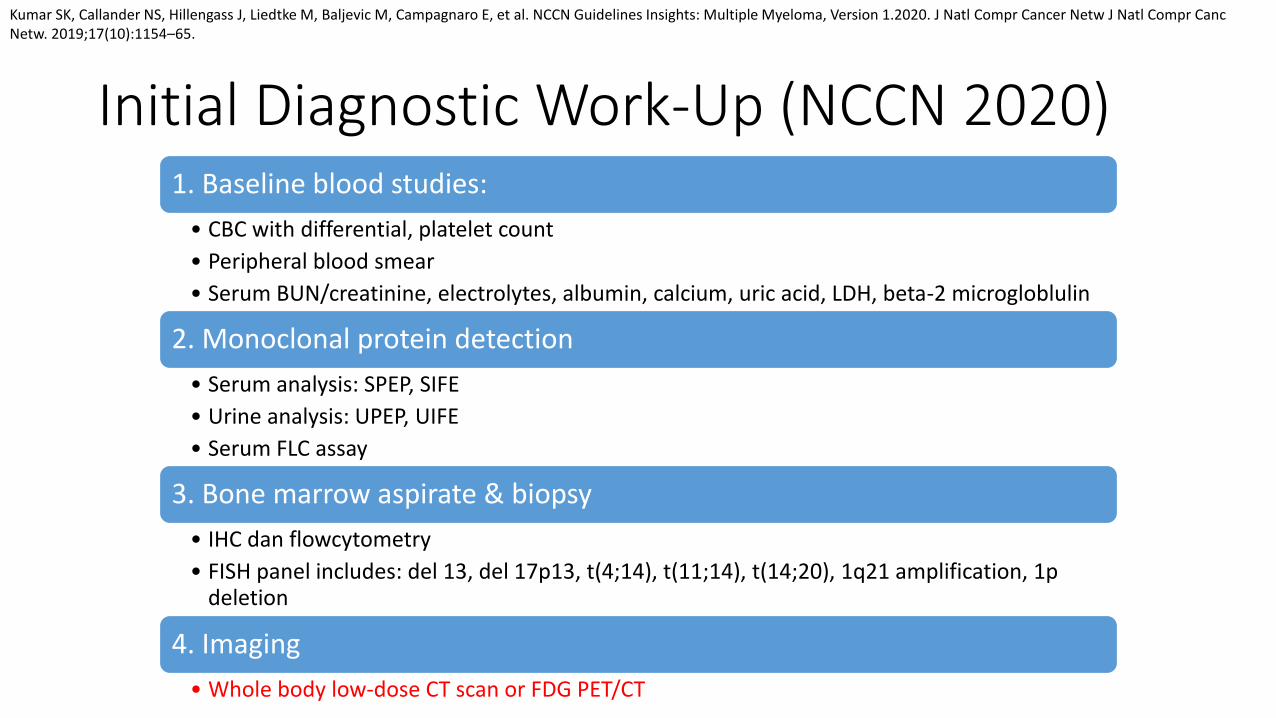
Initial Diagnostic Work-Up (NCCN 2020)1. Baseline blood studies:
• CBC with differential, platelet count
• Peripheral blood smear
• Serum BUN/creatinine, electrolytes, albumin, calcium, uric acid, LDH, beta-2 microgloblulin
2. Monoclonal protein detection
• Serum analysis: SPEP, SIFE
• Urine analysis: UPEP, UIFE
• Serum FLC assay
3. Bone marrow aspirate & biopsy
• IHC dan flowcytometry
• FISH panel includes: del 13, del 17p13, t(4;14), t(11;14), t(14;20), 1q21 amplification, 1p deletion
4. Imaging
• Whole body low-dose CT scan or FDG PET/CT
Kumar SK, Callander NS, Hillengass J, Liedtke M, Baljevic M, Campagnaro E, et al. NCCN Guidelines Insights: Multiple Myeloma, Version 1.2020. J Natl Compr Cancer Netw J Natl Compr CancNetw. 2019;17(10):1154–65.

Additional Diagnostic Tests (NCCN 2020)
• Whole body MRI IF whole-body CT/ FDG PET/CT negative• Tissue biopsy to confirm suspected plasmacytomas• Plasma cell proliferation• Serum viscosity• HLA typing for transplantation• Echocardiogram• Evaluation for light chain amyloidosis• SNP array and/or NGS panel on bone marrow • Assess circulating plasma cells on bone marrow as indicated
Kumar SK, Callander NS, Hillengass J, Liedtke M, Baljevic M, Campagnaro E, et al. NCCN Guidelines Insights: Multiple Myeloma, Version 1.2020. J Natl Compr Cancer Netw J Natl Compr CancNetw. 2019;17(10):1154–65.
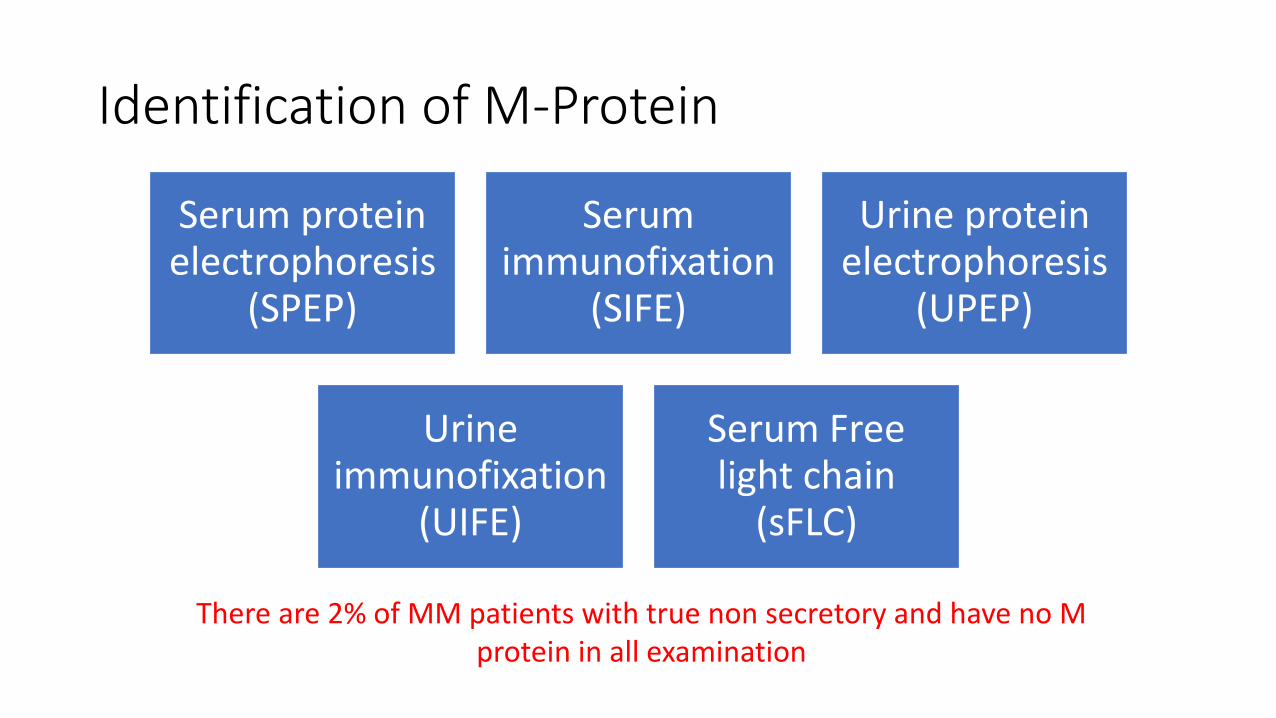
Identification of M-Protein
Serum protein electrophoresis
(SPEP)
Serum immunofixation
(SIFE)
Urine protein electrophoresis
(UPEP)
Urine immunofixation
(UIFE)
Serum Free light chain
(sFLC)
There are 2% of MM patients with true non secretory and have no M protein in all examination
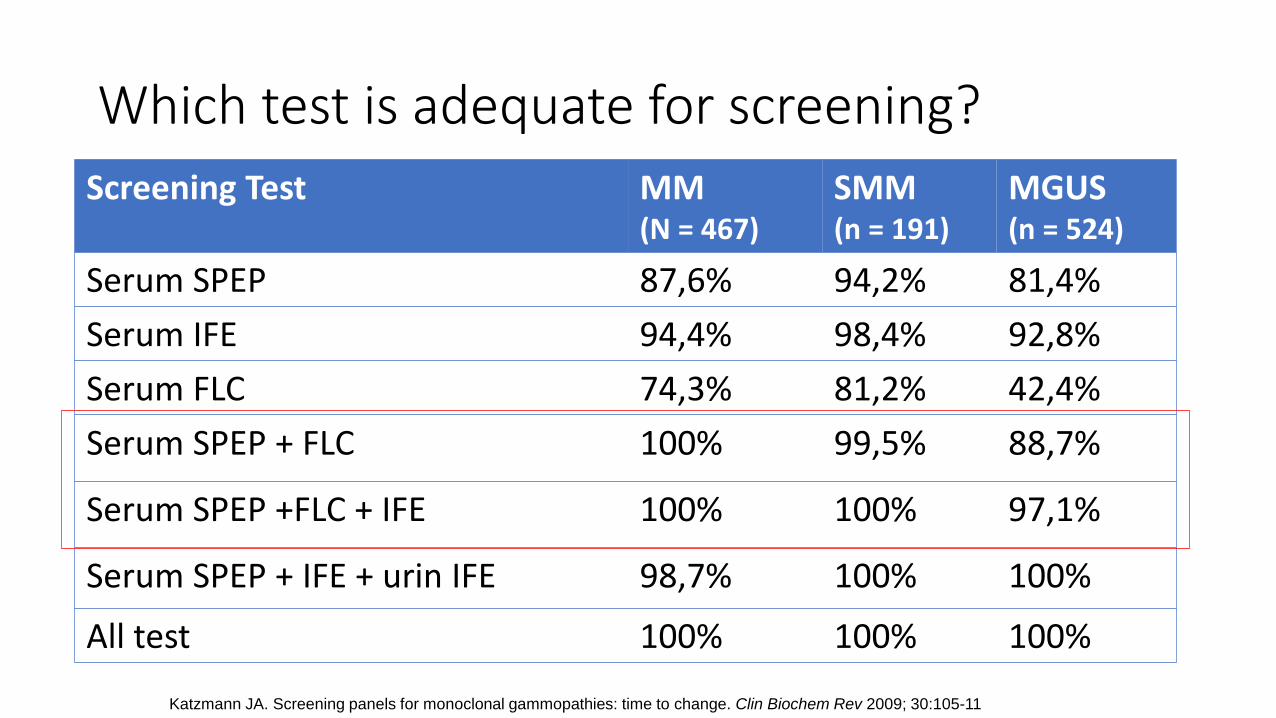
Which test is adequate for screening?
Screening Test MM(N = 467)
SMM(n = 191)
MGUS(n = 524)
Serum SPEP 87,6% 94,2% 81,4%
Serum IFE 94,4% 98,4% 92,8%
Serum FLC 74,3% 81,2% 42,4%
Serum SPEP + FLC 100% 99,5% 88,7%
Serum SPEP +FLC + IFE 100% 100% 97,1%
Serum SPEP + IFE + urin IFE 98,7% 100% 100%
All test 100% 100% 100%
Katzmann JA. Screening panels for monoclonal gammopathies: time to change. Clin Biochem Rev 2009; 30:105-11
Serum Protein Electrophoresis (SPEP)
• The most common examination to detect MM
• Divide protein in 5 major fraction• Albumin, alpha-1, alpha-2, beta and gamma
• Limitation: • Cannot distinguish isotype
• 18 – 20% patient with LCMM negative result
• Can be normal in oligo-secretory (~15-20%) or NSMM (~1-3%)
• Patient with protein M migration to beta region
• IgD myeloma very small protein M
1. Morrison T, Booth RA, Hauff K, Berardi P, Visram A. Chapter One - Laboratory assessment of multiple myeloma. In: Makowski GSBT-A in CC, editor. Elsevier; 2019. p. 1–58. 2. Leung N. Chapter 8: Clinical Tests for Monoclonal Proteins. In: Onco-Nephrology Curriculum. American Society of Nephrology; 2016. 3. Willrich MA V, Murray DL, Kyle RA. Laboratory testing for monoclonal gammopathies: Focus on monoclonal gammopathy of undetermined significance and smoldering multiple myeloma. Clin
Biochem. 2018;51:38–47.
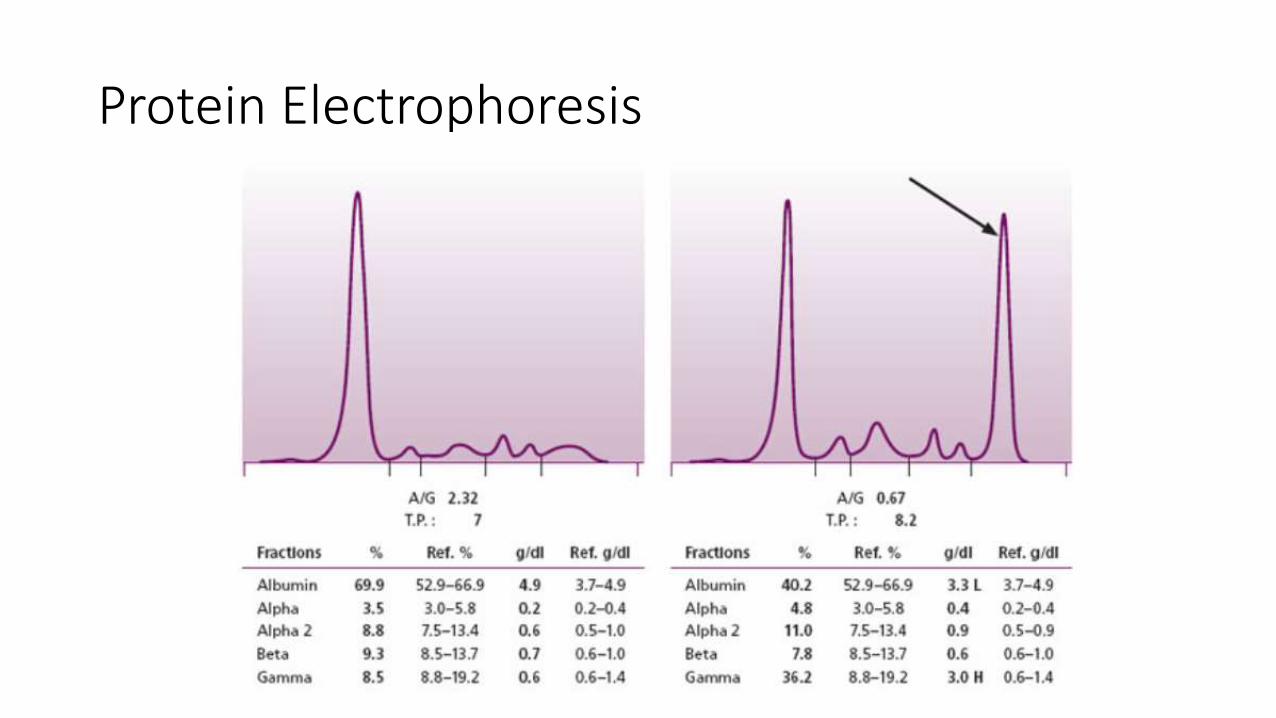
Protein Electrophoresis
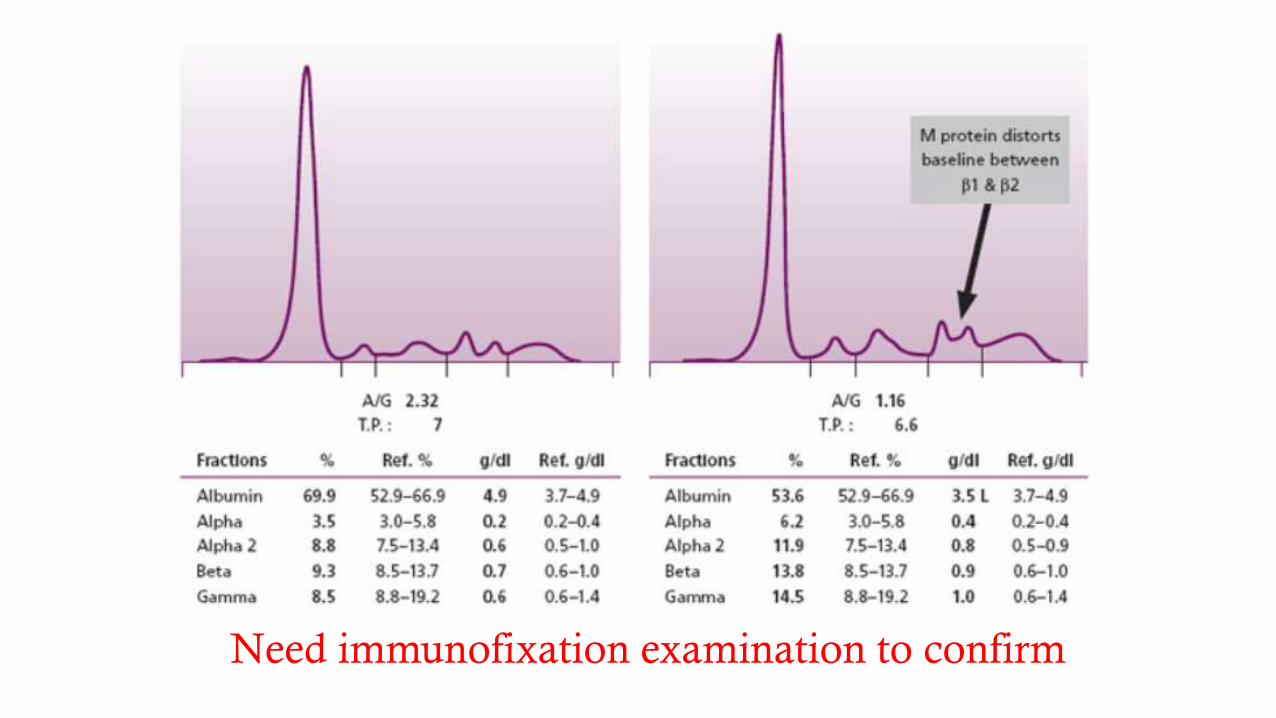
Need immunofixation examination to confirm
Immunofixation Electrophoresis (IFE)
• IFE more sensitive than SPEP for detection of M protein • Sensitivity λ100 mg/L - κ150 mg/L (10x more sensitive than SPEP)
• Characterization of M protein• Heavy chain class: IgG, IgA, IgM, IgD, IgE (rare)
• Light chain: κ and λ
• Limitation• Does not provide quantification of M-protein
• Patient with oligosecretory or NSMM
1. Morrison T, Booth RA, Hauff K, Berardi P, Visram A. Chapter One - Laboratory assessment of multiple myeloma. In: Makowski GSBT-A in CC, editor. Elsevier; 2019. p. 1–58. 2. Leung N. Chapter 8: Clinical Tests for Monoclonal Proteins. In: Onco-Nephrology Curriculum. American Society of Nephrology; 2016. 3. Willrich MA V, Murray DL, Kyle RA. Laboratory testing for monoclonal gammopathies: Focus on monoclonal gammopathy of undetermined significance and smoldering multiple myeloma. Clin Biochem.
2018;51:38–47.
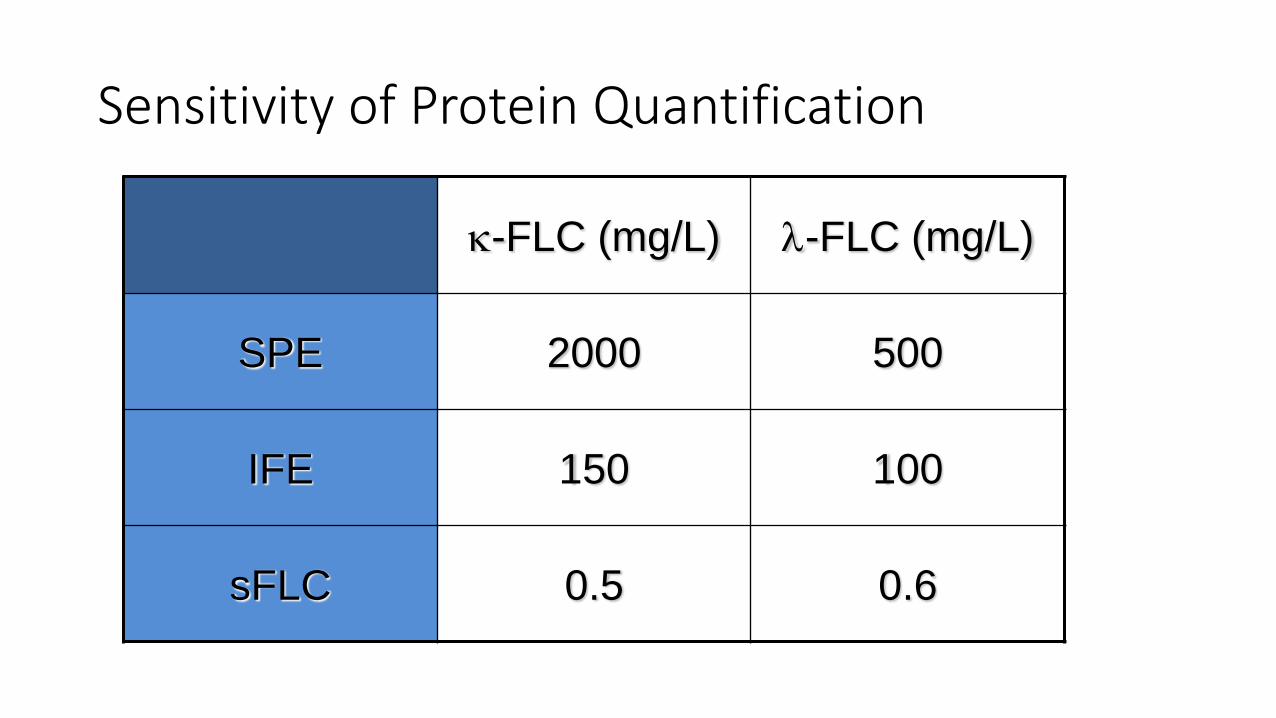
Sensitivity of Protein Quantification
k-FLC (mg/L) l-FLC (mg/L)
SPE 2000 500
IFE 150 100
sFLC 0.5 0.6
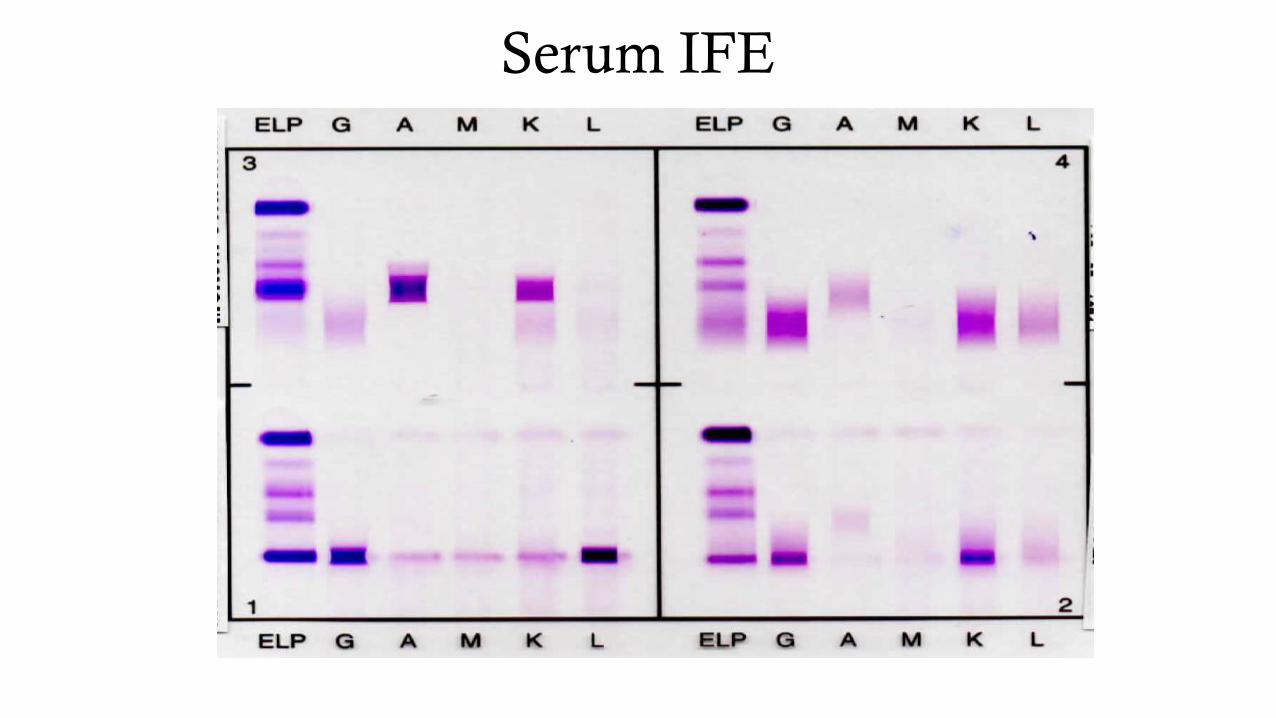
Serum IFE
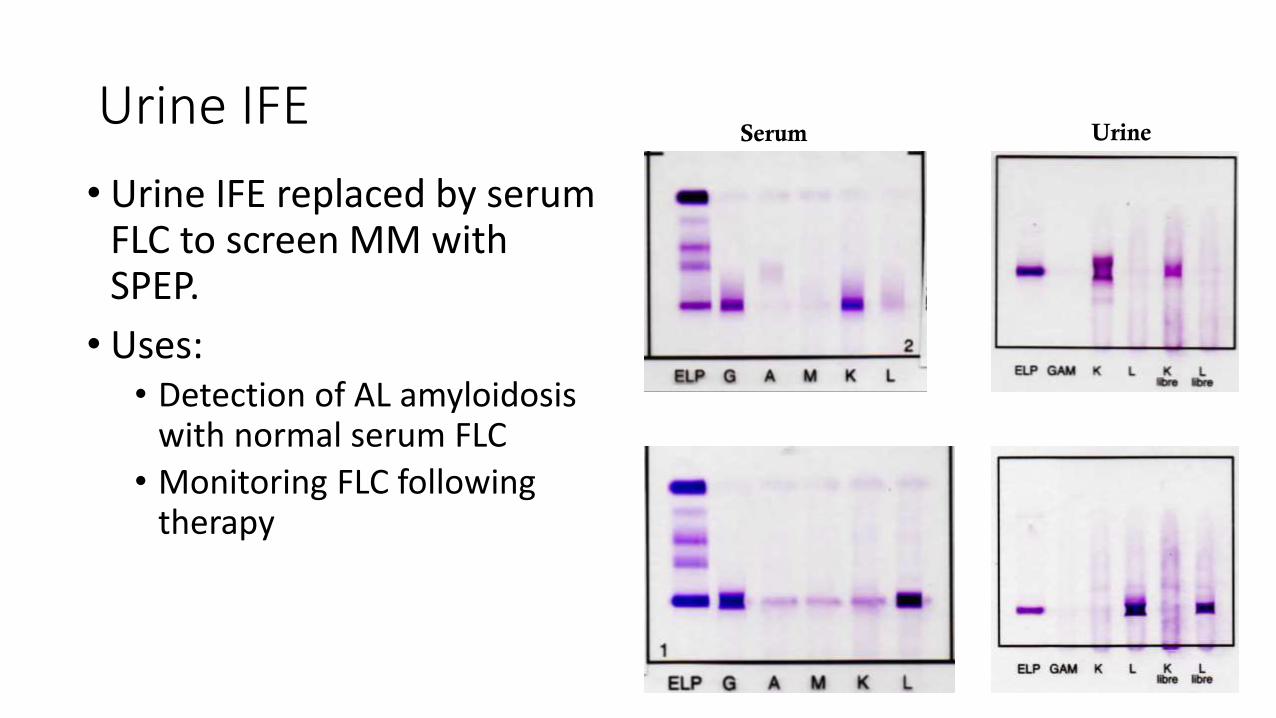
Urine IFE
• Urine IFE replaced by serum FLC to screen MM with SPEP.
• Uses:• Detection of AL amyloidosis
with normal serum FLC
• Monitoring FLC following therapy
Serum Urine
Free Light Chain
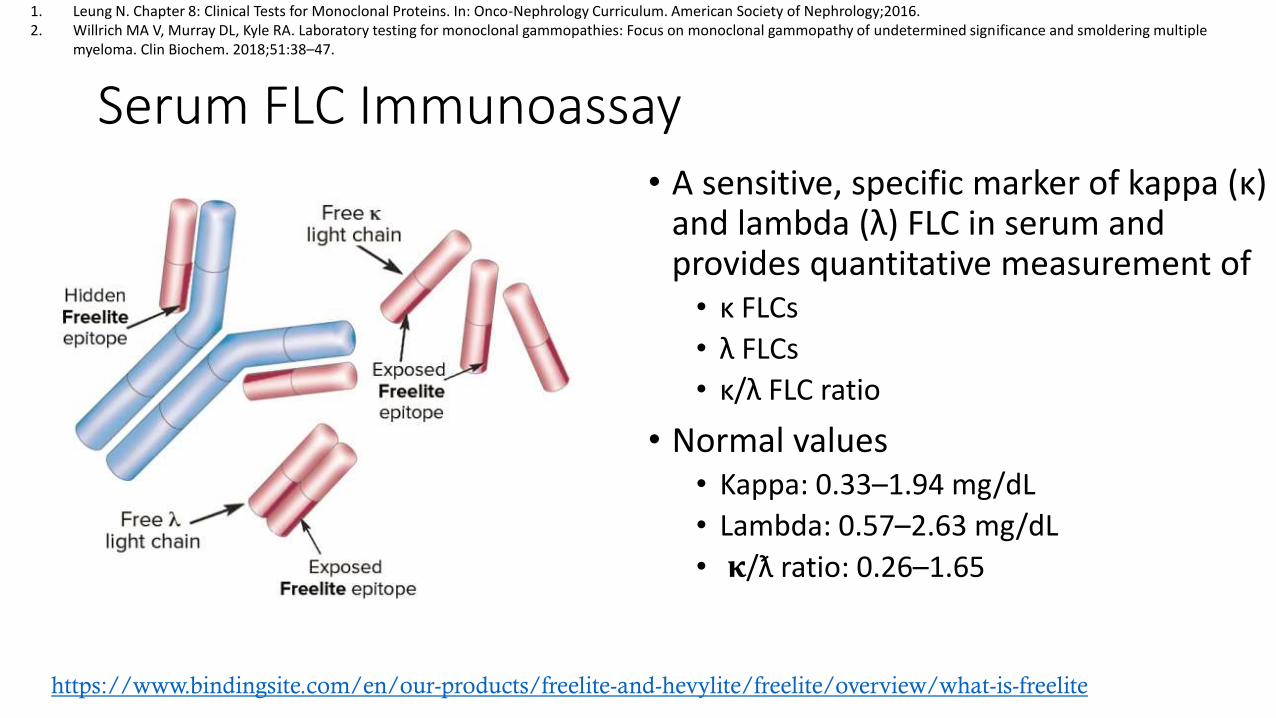
Serum FLC Immunoassay• A sensitive, specific marker of kappa (κ)
and lambda (λ) FLC in serum and provides quantitative measurement of • κ FLCs
• λ FLCs
• κ/λ FLC ratio
• Normal values• Kappa: 0.33–1.94 mg/dL
• Lambda: 0.57–2.63 mg/dL
• 𝛋/ƛ ratio: 0.26–1.65
https://www.bindingsite.com/en/our-products/freelite-and-hevylite/freelite/overview/what-is-freelite
1. Leung N. Chapter 8: Clinical Tests for Monoclonal Proteins. In: Onco-Nephrology Curriculum. American Society of Nephrology;2016.2. Willrich MA V, Murray DL, Kyle RA. Laboratory testing for monoclonal gammopathies: Focus on monoclonal gammopathy of undetermined significance and smoldering multiple
myeloma. Clin Biochem. 2018;51:38–47.
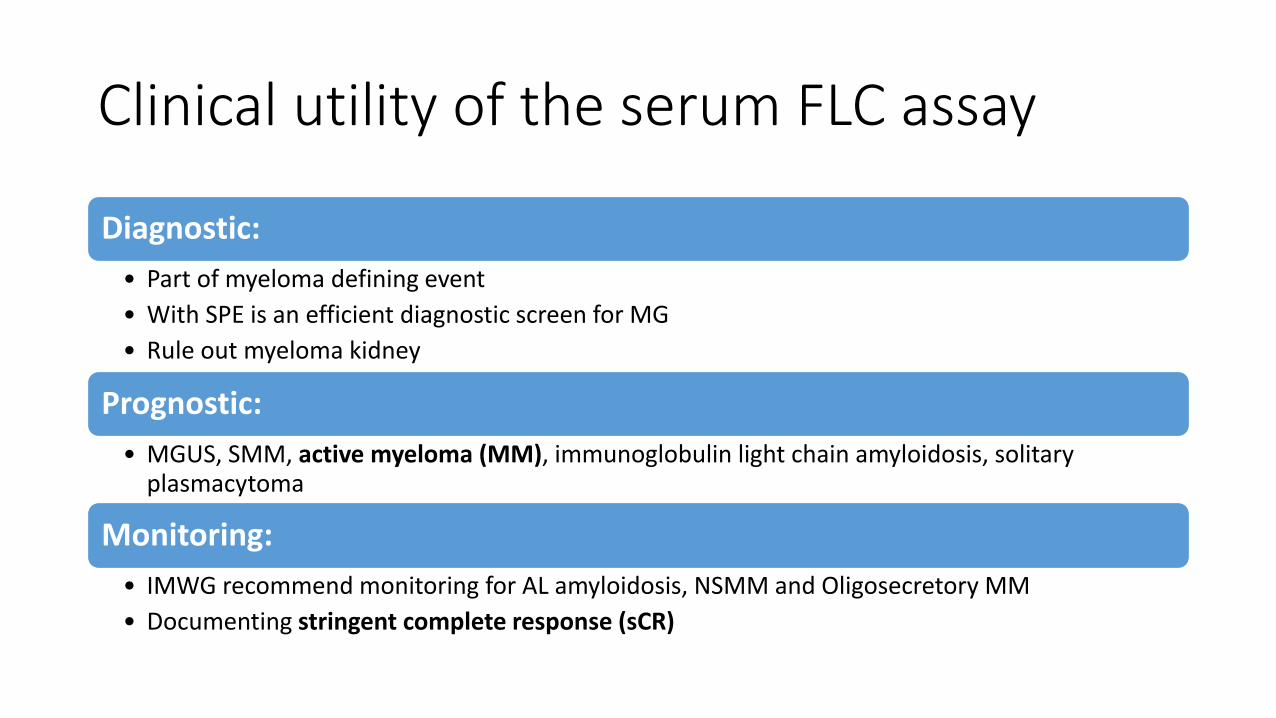
Clinical utility of the serum FLC assay
Diagnostic:
• Part of myeloma defining event
• With SPE is an efficient diagnostic screen for MG
• Rule out myeloma kidney
Prognostic:
• MGUS, SMM, active myeloma (MM), immunoglobulin light chain amyloidosis, solitary plasmacytoma
Monitoring:
• IMWG recommend monitoring for AL amyloidosis, NSMM and Oligosecretory MM
• Documenting stringent complete response (sCR)
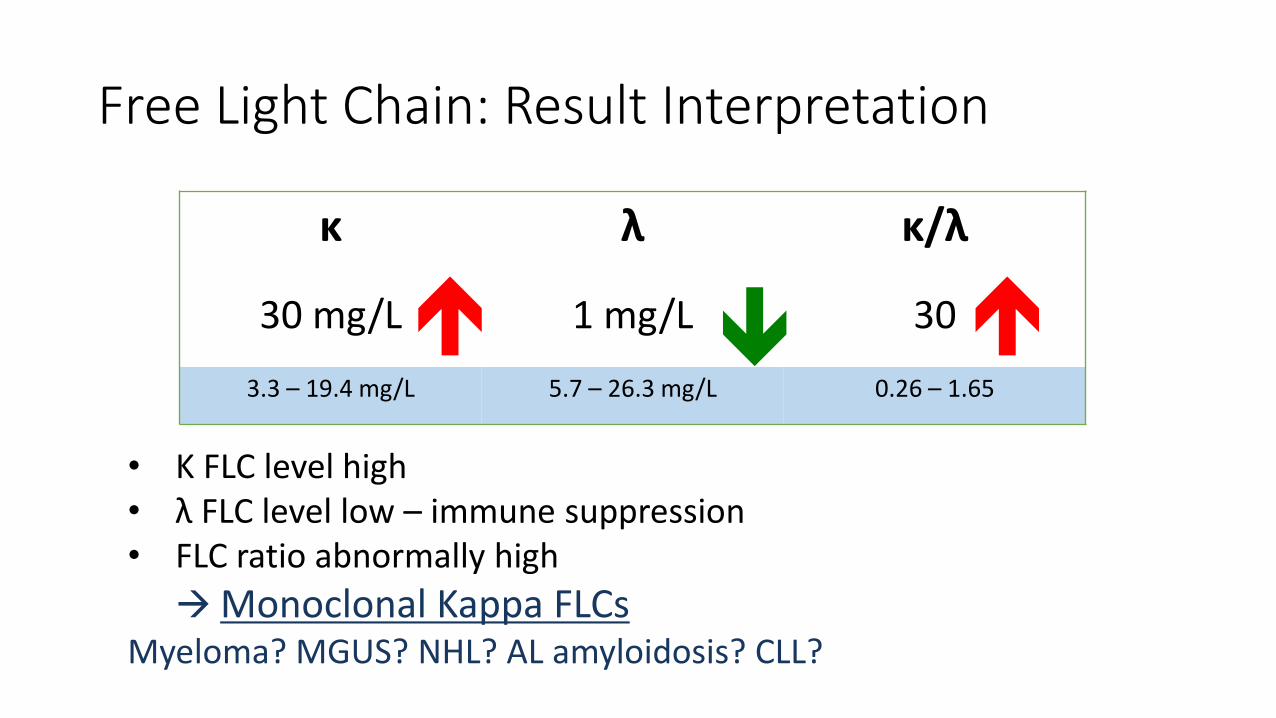
κ λ κ/λ
30 mg/L 1 mg/L 30
3.3 – 19.4 mg/L 5.7 – 26.3 mg/L 0.26 – 1.65
Free Light Chain: Result Interpretation
• Κ FLC level high• λ FLC level low – immune suppression• FLC ratio abnormally high
Monoclonal Kappa FLCsMyeloma? MGUS? NHL? AL amyloidosis? CLL?
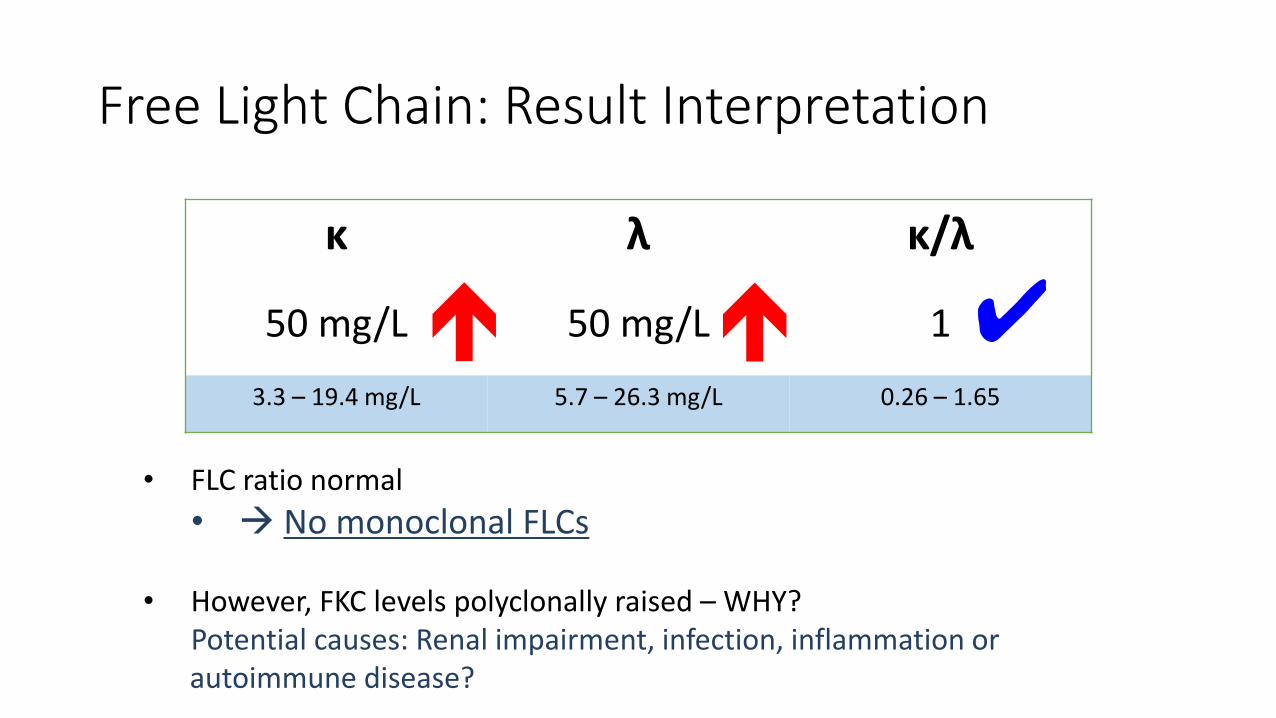
Free Light Chain: Result Interpretation
✔
• FLC ratio normal
• No monoclonal FLCs
• However, FKC levels polyclonally raised – WHY?Potential causes: Renal impairment, infection, inflammation or autoimmune disease?
κ λ κ/λ
50 mg/L 50 mg/L 1
3.3 – 19.4 mg/L 5.7 – 26.3 mg/L 0.26 – 1.65

Interpretation
• Normal samples. SPE + FLC normal MG unlikely
• Abnormal κ/λ ratios. Possible MG needs further investigation. Borderline elevated κ/λ ratios occur with renal impairment and may require appropriate renal function tests
• Low concentrations of κ, λ or both indicate bone marrow suppression
• Elevated concentrations of both κ and λ with a normal κ/λ ratio: • Renal impairment (common)• Over-production of polyclonal FLC from inflammatory conditions (common)• Biclonal gammopathies of different FLC types (rare)
• Elevated concentrations of both κ and λ with an abnormal κ/λ ratio: Possible combination of monoclonal gammopathy and renal impairment
https://www.bindingsite.com/en/our-products/freelite-and-hevylite/freelite/overview/what-is-freelite
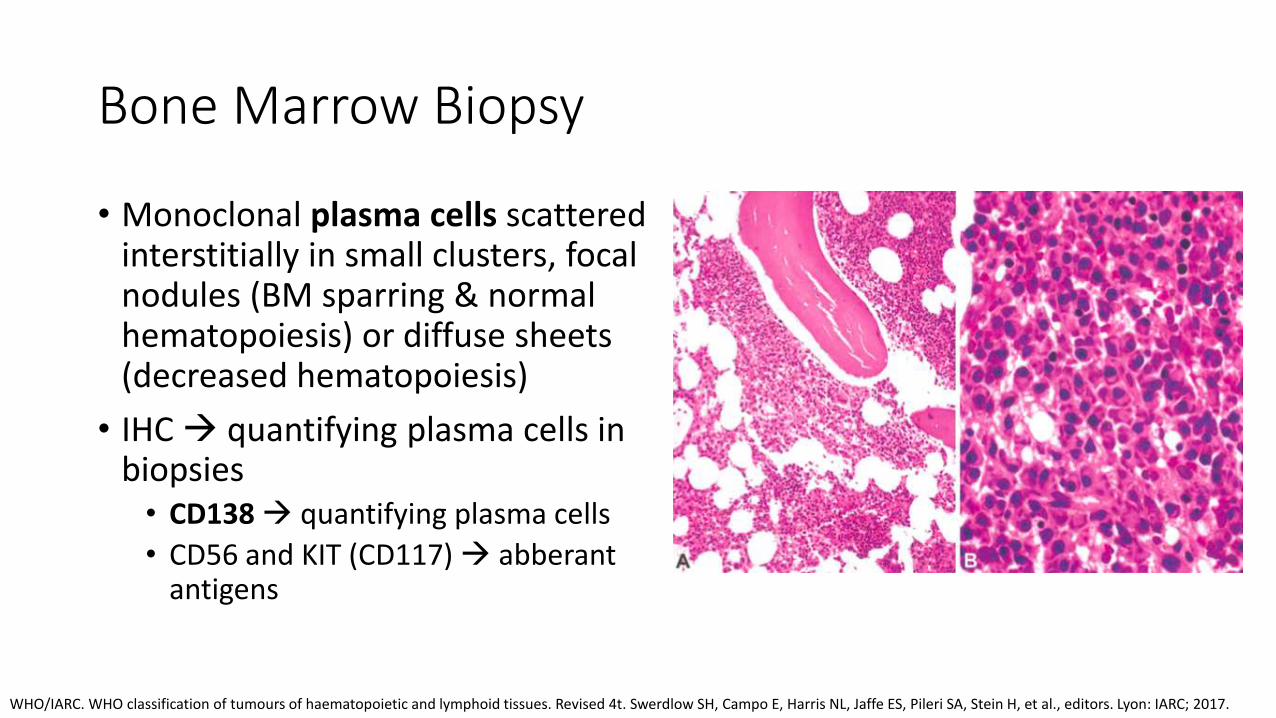
Bone Marrow Biopsy
• Monoclonal plasma cells scattered interstitially in small clusters, focal nodules (BM sparring & normal hematopoiesis) or diffuse sheets (decreased hematopoiesis)
• IHC quantifying plasma cells in biopsies• CD138 quantifying plasma cells
• CD56 and KIT (CD117) abberantantigens
WHO/IARC. WHO classification of tumours of haematopoietic and lymphoid tissues. Revised 4t. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al., editors. Lyon: IARC; 2017.

Bone Marrow Aspirate • Plasma cells increased 10%
up to 90%
• Myeloma plasma cells: vary from immature, plasmablastic, pleomorphic to mature cells
WHO/IARC. WHO classification of tumours of haematopoietic and lymphoid tissues. Revised 4t. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al., editors. Lyon: IARC; 2017.
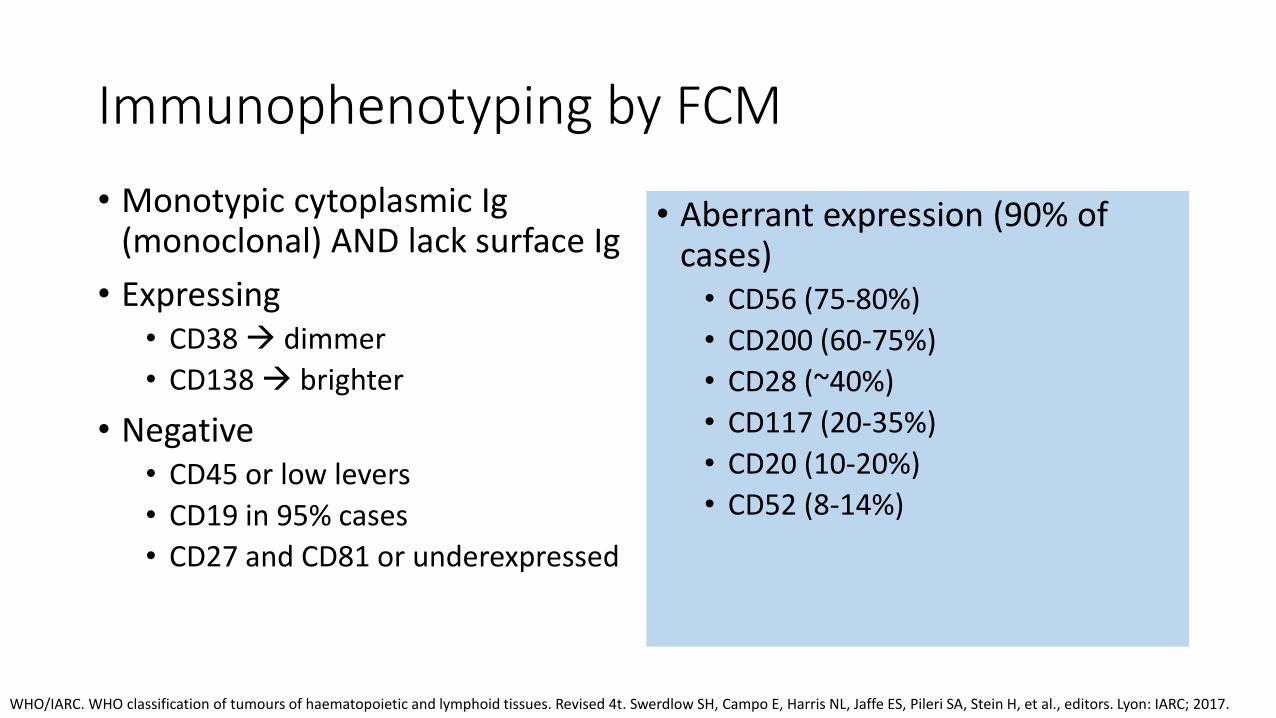
Immunophenotyping by FCM
• Monotypic cytoplasmic Ig (monoclonal) AND lack surface Ig
• Expressing• CD38 dimmer
• CD138 brighter
• Negative• CD45 or low levers
• CD19 in 95% cases
• CD27 and CD81 or underexpressed
• Aberrant expression (90% of cases)• CD56 (75-80%)
• CD200 (60-75%)
• CD28 (~40%)
• CD117 (20-35%)
• CD20 (10-20%)
• CD52 (8-14%)
WHO/IARC. WHO classification of tumours of haematopoietic and lymphoid tissues. Revised 4t. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al., editors. Lyon: IARC; 2017.
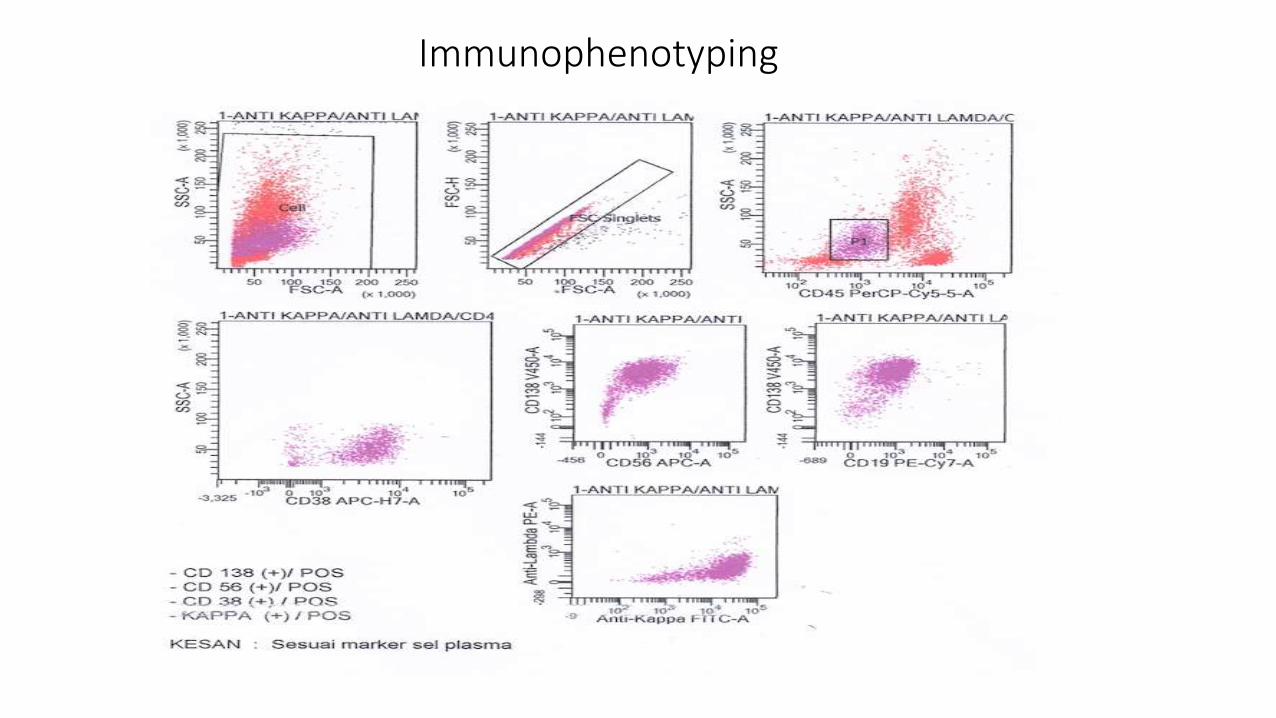
Immunophenotyping
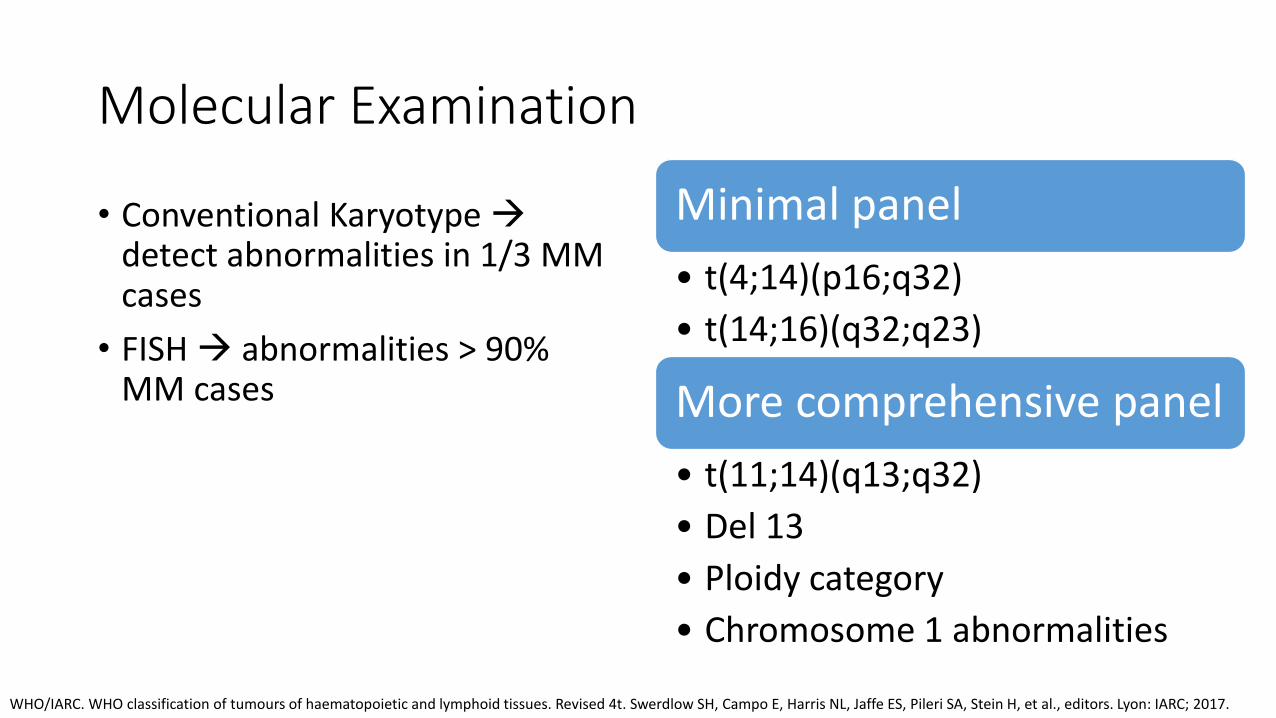
Molecular Examination
• Conventional Karyotype detect abnormalities in 1/3 MM cases
• FISH abnormalities > 90% MM cases
Minimal panel
• t(4;14)(p16;q32)
• t(14;16)(q32;q23)
More comprehensive panel
• t(11;14)(q13;q32)
• Del 13
• Ploidy category
• Chromosome 1 abnormalities
WHO/IARC. WHO classification of tumours of haematopoietic and lymphoid tissues. Revised 4t. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al., editors. Lyon: IARC; 2017.
Staging, Response Criteriaand Monitoring
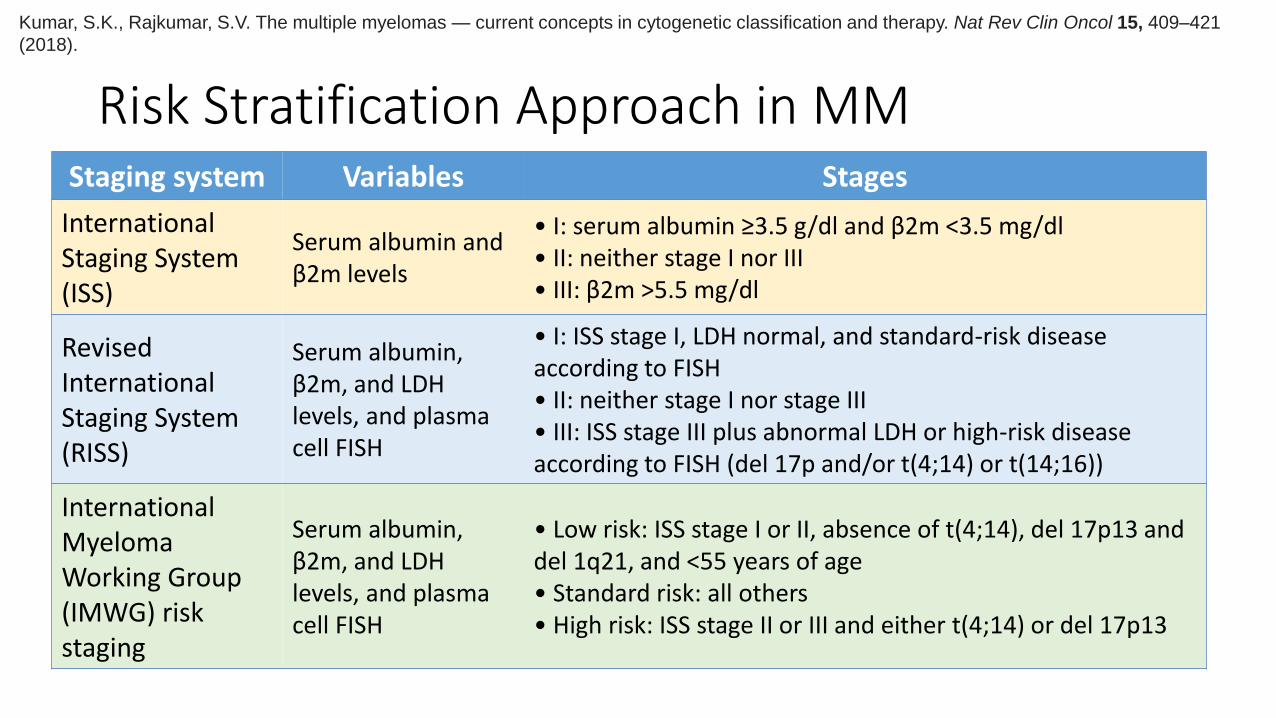
Risk Stratification Approach in MMStaging system Variables Stages
International Staging System (ISS)
Serum albumin and β2m levels
• I: serum albumin ≥3.5 g/dl and β2m <3.5 mg/dl • II: neither stage I nor III• III: β2m >5.5 mg/dl
Revised International Staging System (RISS)
Serum albumin, β2m, and LDH levels, and plasma cell FISH
• I: ISS stage I, LDH normal, and standard-risk disease according to FISH • II: neither stage I nor stage III• III: ISS stage III plus abnormal LDH or high-risk disease according to FISH (del 17p and/or t(4;14) or t(14;16))
International Myeloma Working Group (IMWG) risk staging
Serum albumin, β2m, and LDH levels, and plasma cell FISH
• Low risk: ISS stage I or II, absence of t(4;14), del 17p13 and del 1q21, and <55 years of age • Standard risk: all others• High risk: ISS stage II or III and either t(4;14) or del 17p13
Kumar, S.K., Rajkumar, S.V. The multiple myelomas — current concepts in cytogenetic classification and therapy. Nat Rev Clin Oncol 15, 409–421
(2018).
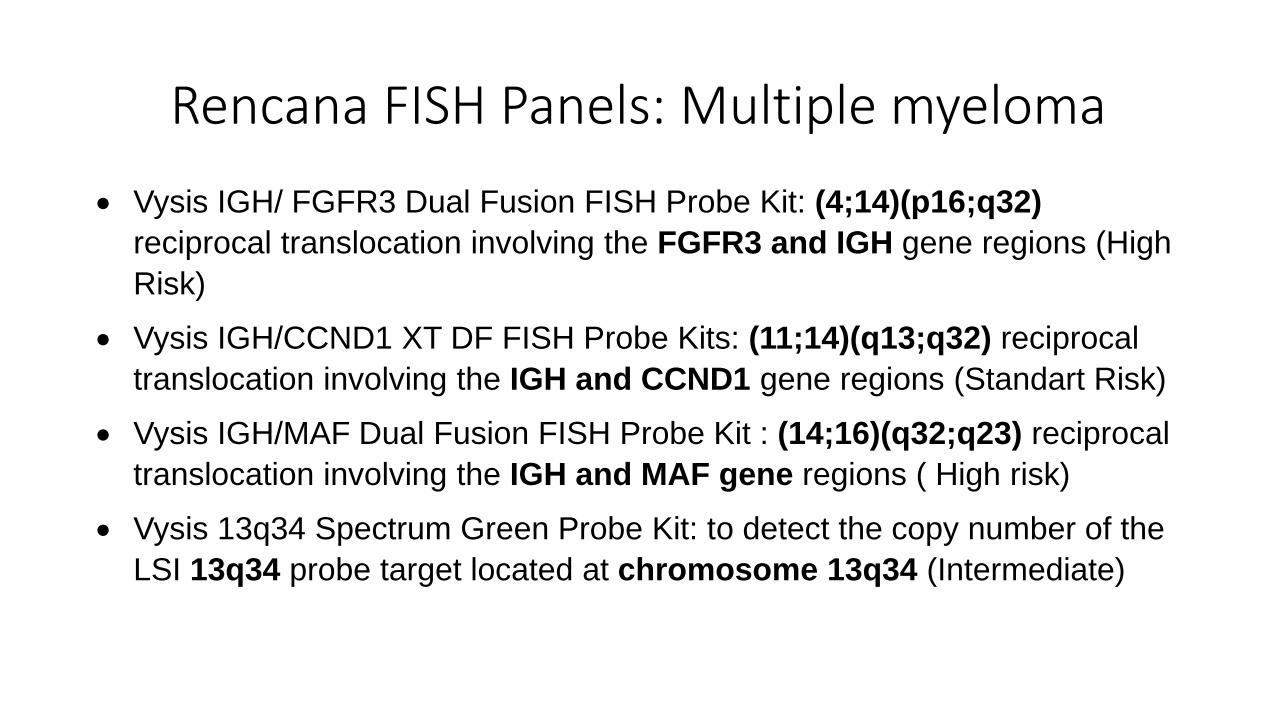
Rencana FISH Panels: Multiple myeloma
Vysis IGH/ FGFR3 Dual Fusion FISH Probe Kit: (4;14)(p16;q32)
reciprocal translocation involving the FGFR3 and IGH gene regions (High
Risk)
Vysis IGH/CCND1 XT DF FISH Probe Kits: (11;14)(q13;q32) reciprocal
translocation involving the IGH and CCND1 gene regions (Standart Risk)
Vysis IGH/MAF Dual Fusion FISH Probe Kit : (14;16)(q32;q23) reciprocal
translocation involving the IGH and MAF gene regions ( High risk)
Vysis 13q34 Spectrum Green Probe Kit: to detect the copy number of the
LSI 13q34 probe target located at chromosome 13q34 (Intermediate)
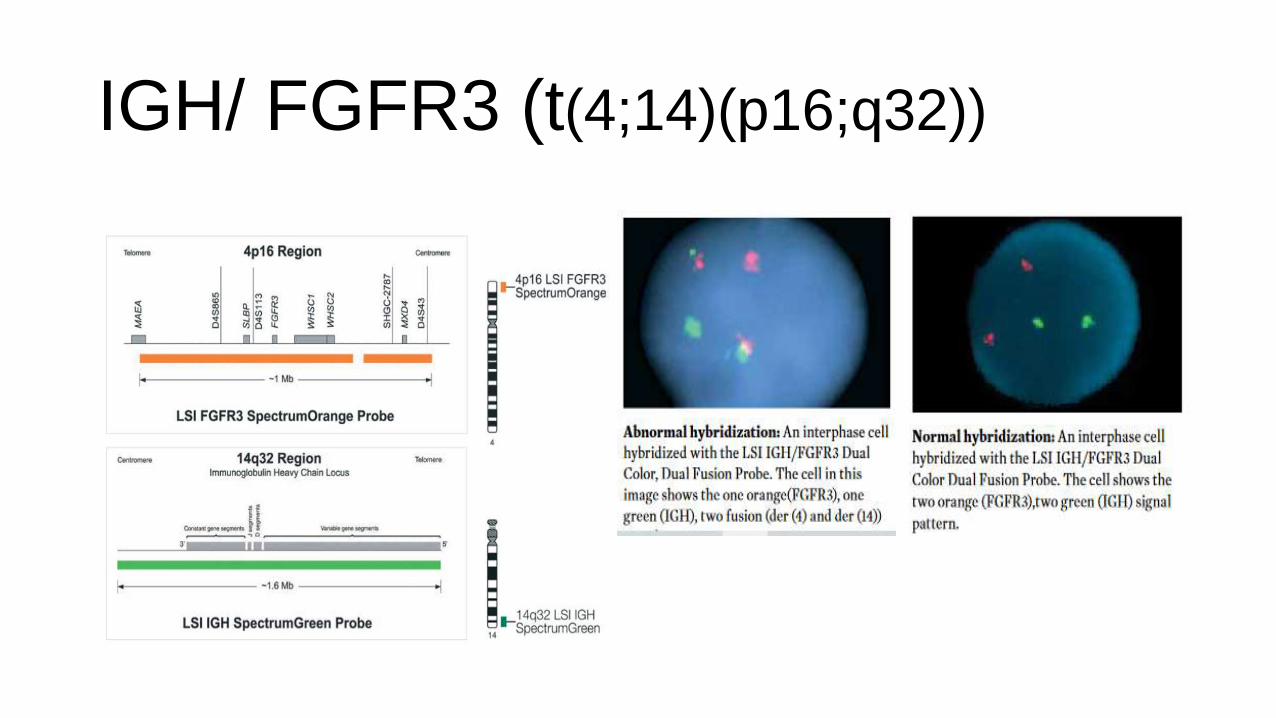
IGH/ FGFR3 (t(4;14)(p16;q32))
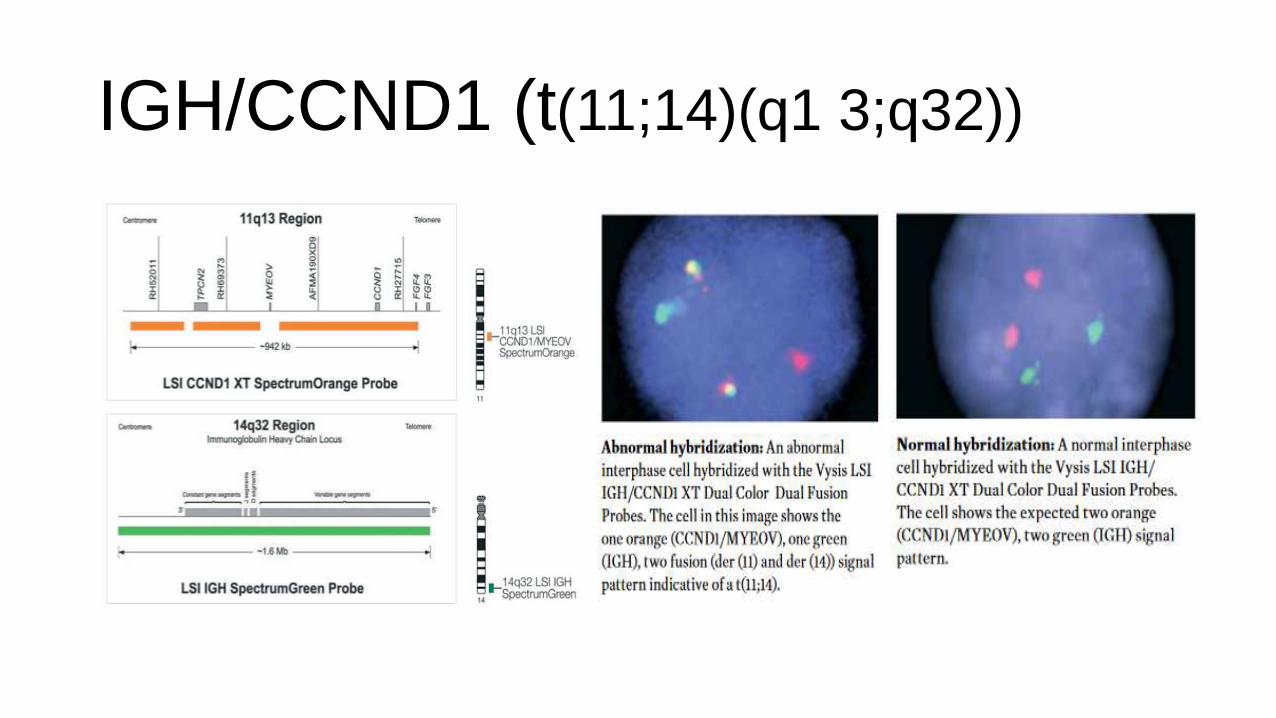
IGH/CCND1 (t(11;14)(q1 3;q32))
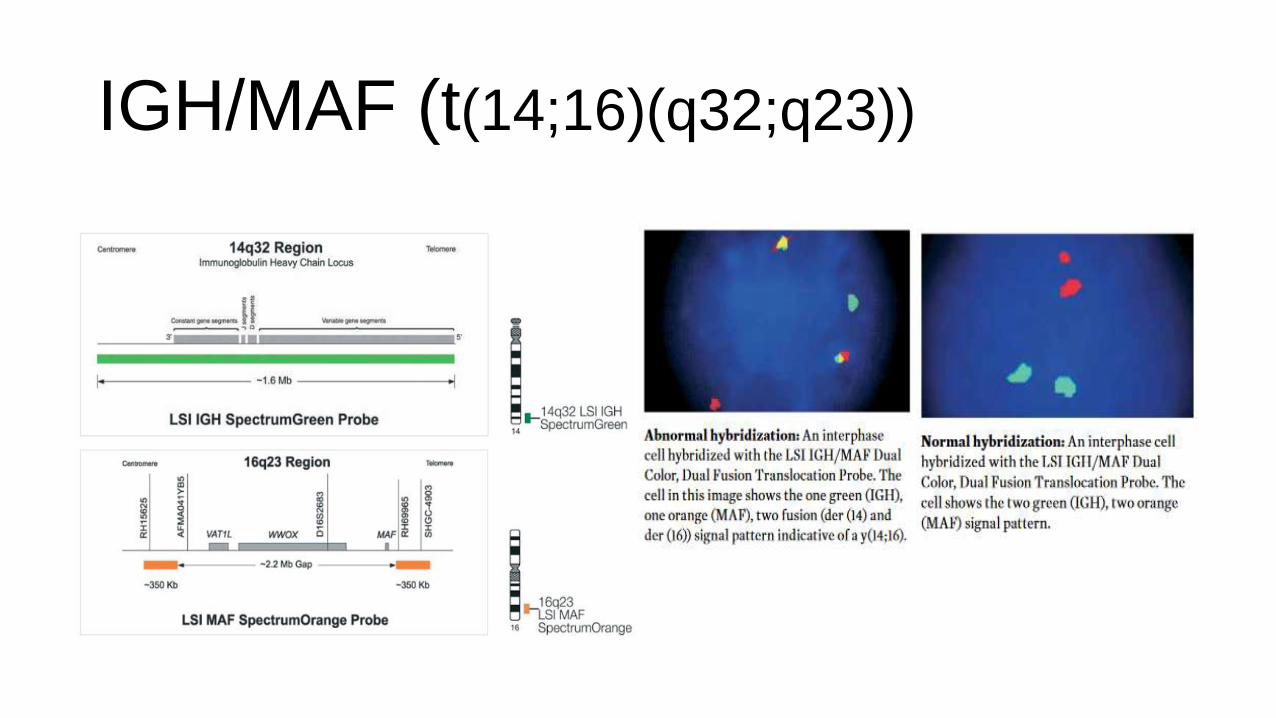
IGH/MAF (t(14;16)(q32;q23))
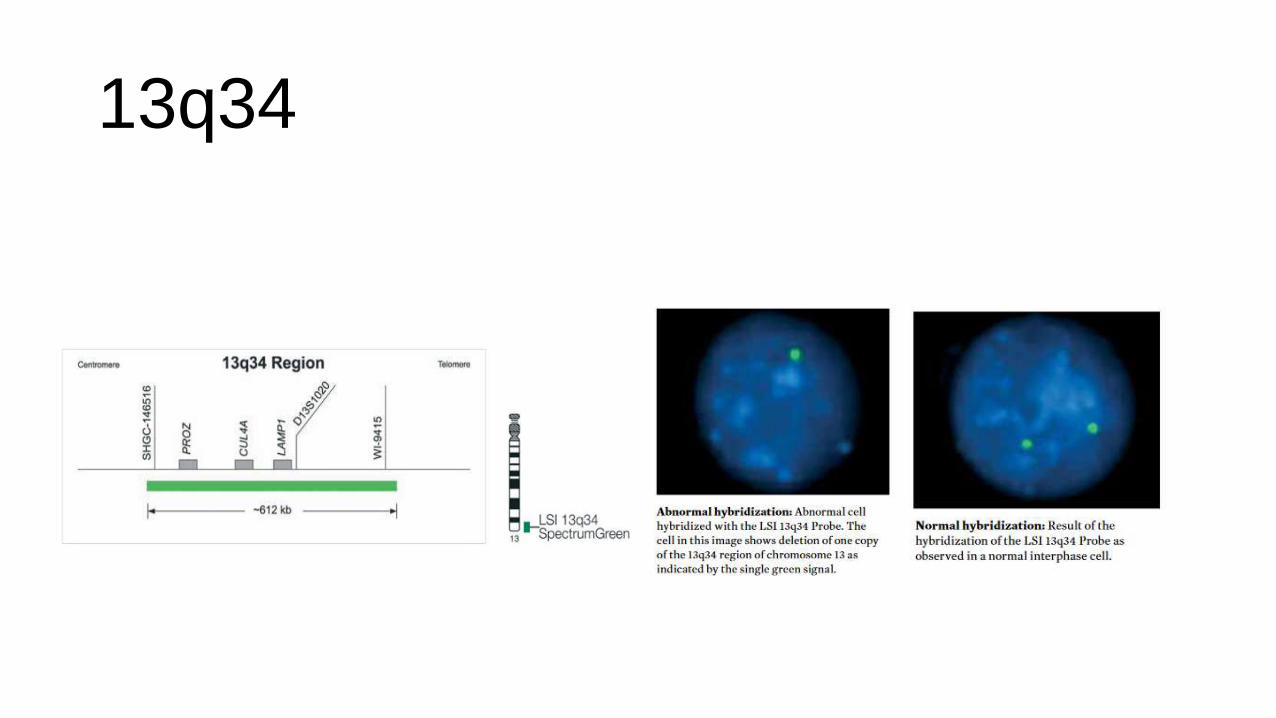
13q34
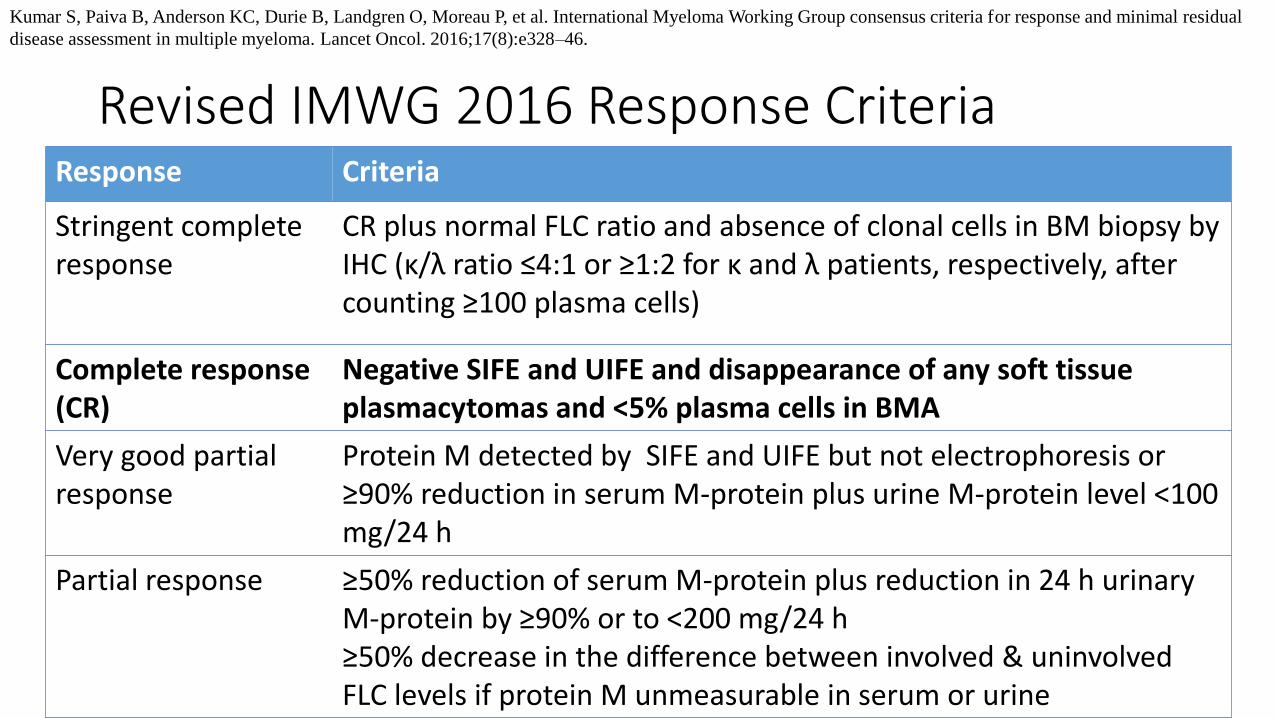
Revised IMWG 2016 Response CriteriaResponse Criteria
Stringent complete response
CR plus normal FLC ratio and absence of clonal cells in BM biopsy by IHC (κ/λ ratio ≤4:1 or ≥1:2 for κ and λ patients, respectively, after counting ≥100 plasma cells)
Complete response (CR)
Negative SIFE and UIFE and disappearance of any soft tissue plasmacytomas and <5% plasma cells in BMA
Very good partial response
Protein M detected by SIFE and UIFE but not electrophoresis or ≥90% reduction in serum M-protein plus urine M-protein level <100 mg/24 h
Partial response ≥50% reduction of serum M-protein plus reduction in 24 h urinary M-protein by ≥90% or to <200 mg/24 h≥50% decrease in the difference between involved & uninvolved FLC levels if protein M unmeasurable in serum or urine
Kumar S, Paiva B, Anderson KC, Durie B, Landgren O, Moreau P, et al. International Myeloma Working Group consensus criteria for response and minimal residual
disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328–46.
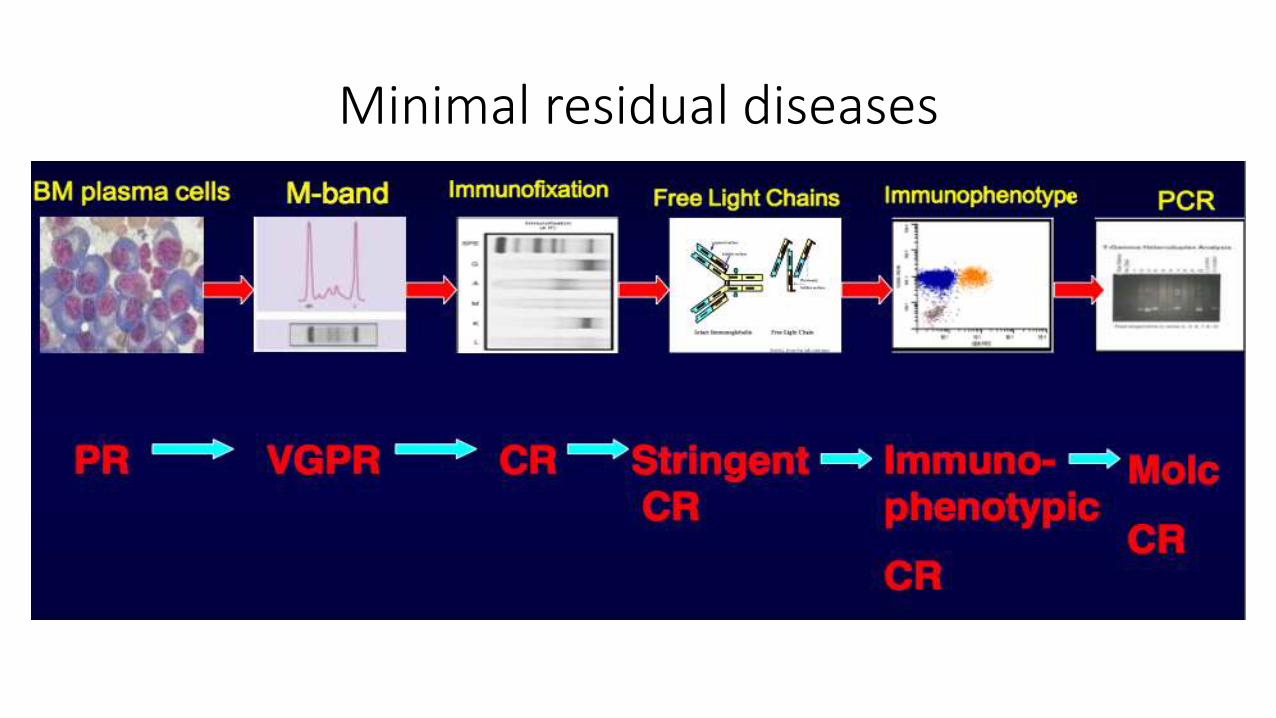
Minimal residual diseases
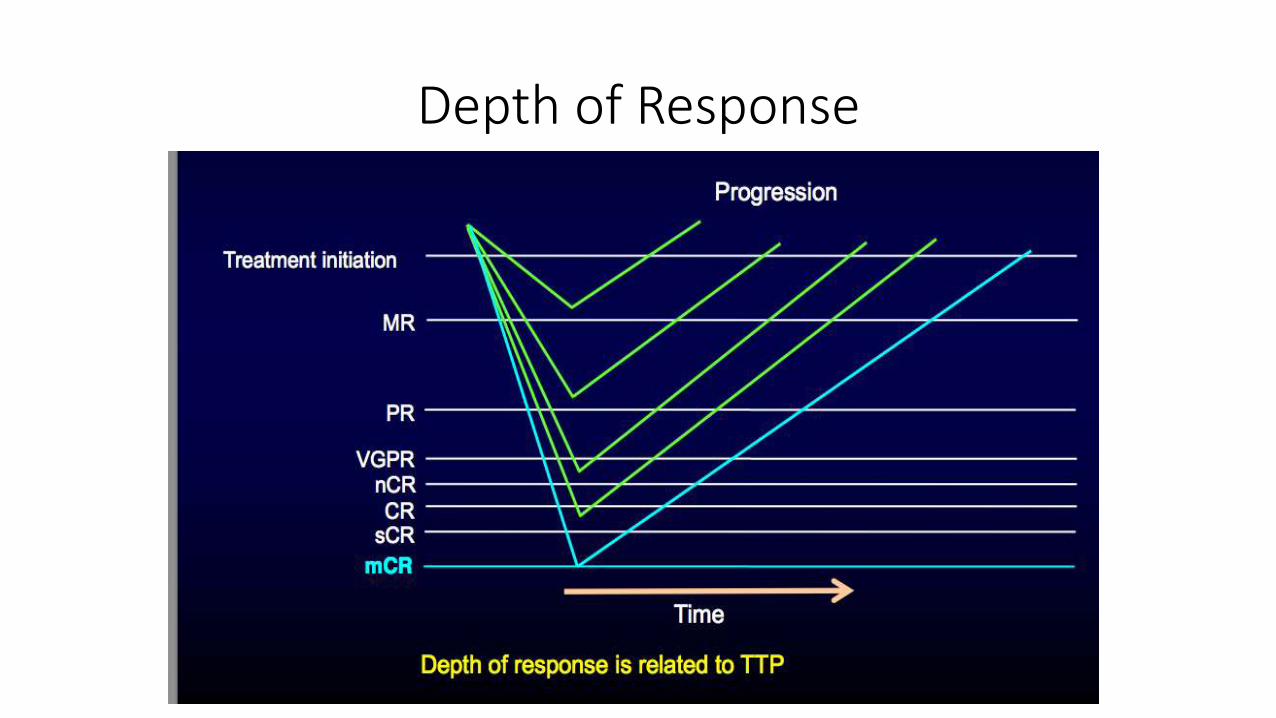
Depth of Response
FLC for Monitoring IIMM
FLC as an additional tool to monitor patients
• FLC and intact immunoglobulins are independent markers of disease
FLC have shorter half life
• More rapid indication of response
Detect light chain escape
Detect residual disease
MM in COVID-19 Era
SARS-CoV-2 Testing for MM Patients
• In countries or local communities where COVID-19 infection is widely spread, MM patients should have a PCR test of nasopharyngeal swab for SARS-CoV-2 to avoid ward spread and infections
Terpos, E., Engelhardt, M., Cook, G. et al. Management of patients with multiple myeloma in the era of COVID-19 pandemic: a consensus paper from the
European Myeloma Network (EMN). Leukemia 34, 2000–2011 (2020).
Before hospital
admission
Before starting a new
treatment line
Before cell apheresis or
ASCT

Terpos, E., Engelhardt, M., Cook, G. et al. Management of patients with multiple myeloma in the era
of COVID-19 pandemic: a consensus paper from the European Myeloma Network
(EMN). Leukemia 34, 2000–2011 (2020).

MM patients with COVID-19
• MM patients with COVID-19, but NO COVID-19 symptoms 14 days quarantine if myeloma-related events allow the delay of treatment OR the patient does not have • acute renal impairment
• extended bone disease with fractures
• severe anemia
• or other features of aggressive disease
Terpos, E., Engelhardt, M., Cook, G. et al. Management of patients with multiple myeloma in the era of COVID-19 pandemic: a consensus paper from the
European Myeloma Network (EMN). Leukemia 34, 2000–2011 (2020).
Summary
Monoclonal Gammopathy: Unregulated production of whole/ portion of immunoglobulin (M-Protein)
Electrophoresis (EP) & Immunofixation (IFE) provide excellent tools to recognize M-protein
IFE is more sensitive compared to EP to identify specific heavy chain class and light chain type and useful for follow up CR. FLC is the most sensitive and useful parameter to follow up sCR
Summary (Cont.)
FLC quantification is useful for screening and follow up monoclonal gammopathies
FLC can replace urine testing in the diagnosis of monoclonal gammopathies
FLC improves monitoring of monoclonal gammopathies:
Rapidly indicate respond to treatment
Allow detection of light chain escape
FLC ratio is an independent risk factor for MGUS/SMM progression to malignant disease
