laparoscopic ureterolysis and omental wrapping in patients with retroperitoneal fibrosis and...
TRANSCRIPT

Laparoscopic Ureterolysis and Omental Wrappingin Patients with Retroperitoneal Fibrosis
and Obstructive Uropathy:A Single-Center Experience
Nand Kishore Arvind, MS, MCh, DipNB,1 Onkar Singh, MS,1 Qutub Ali, MS, MCh,1 Janak Singh, MS,1
Shilpi Singh Gupta, MS,1 and Surbhi Sahay, MD2
Abstract
Objectives: To analyze the outcomes with mid- to long-term follow-up of laparoscopic ureterolysis (LU) andomental wrapping in retroperitoneal fibrosis (RPF) with obstructive uropathy.Patients and Methods: Records of 9 patients with RPF who had obstructive uropathy at presentation and hadundergone LU and omental wrapping at our center during January 2004 to June 2012 were collected andanalyzed.Results: Six females and three males underwent LU for RPF. Underlying causes of RPF could not be found in 8(89%) cases. Two patients underwent bilateral LU. Mean operative time and estimated blood loss were 213minutes (range, 180–280 minutes) and 119 mL (range, 70–200 mL), respectively. No case required conversionto open surgery. The only significant intraoperative complication (1/9 [11%]) was ureteral injury, which waseasily repaired intraoperatively. The postoperative complication rate was 44% (4/9). Most complications (75%[3/4]) were minor and did not need specific treatment. The mean follow-up period was 46 months (range, 4–72months). The success rate at last follow-up was 89%.Conclusions: Treatment of RPF is still controversial. Any future prospective randomized comparative trialsseem unlikely in view of the low incidence of RPF. LU and omental wrapping in the setting of obstructiveuropathy are safe and an effective alternative with a high success rate at mid- to long-term follow-up.
Introduction
Retroperitoneal fibrosis (RPF) is an obscure clinicalentity that has a complex etiopathogenesis. An intense
fibro-inflammatory reaction develops in the retroperitoneumand may result in compression of adjacent structures. Theestimated incidence is 1–2 in 1 million annually.1–3 In abouttwo-thirds (70%) of cases the cause of RPF cannot be ascer-tained (idiopathic); the remainder occur in association withinflammatory disorders, malignancies, or medications.4
Ureteral involvement occurs in 80%–100% cases.1,2,4,5 Often,patients are referred to the urology department after the startof medical treatment when ureteral obstruction with or with-out renal failure develops. By this time many patients havealready acquired irreversible damage to one of their kidneys.6
Because of paucity of the cases, no standard treatmenthas been established.1,7,8 Surgical ureterolysis has beenconsidered the definitive treatment for ureteral obstruction in
RPF.2,9,10 This has been classically performed by theopen approach, which has a high success rate (90%).2,11,12
However, the open approach has complications like ileus,wound infection, chylous ascites, urinary leaks, and intestinalobstruction.11,13 Laparoscopic ureterolysis (LU) and in-traperitonealization of ureters with or without omental wrap-ping have been used to reduce significant morbidity related tothe open approach. So far, no prospective study has reported onthe treatment outcomes specifically in patients having RPFwith obstructive uropathy. Herein, we present our single-center, single-surgeon’s 8 years of experience of LU andomental wrapping to treat obstructive uropathy due to RPF.
Patients and Methods
We retrospectively analyzed the records of patients whounderwent LU for newly diagnosed RPF at our center duringthe period of February 2004–June 2012. Records of all
Departments of 1Urology and 2Anaesthesiology, Bhopal Memorial Hospital & Research Centre, Bhopal, India.
JOURNAL OF LAPAROENDOSCOPIC & ADVANCED SURGICAL TECHNIQUESVolume 24, Number 3, 2014ª Mary Ann Liebert, Inc.DOI: 10.1089/lap.2013.0242
159

patients who presented with ureteral obstruction (either bi-lateral or unilateral in the case of a unilateral functioningkidney) and obstructive uropathy (raised serum creatininelevel) and were subjected to LU were included in the anal-ysis. Patients without obstructive uropathy, already takingmedical therapy, those with RPF secondary to malignancy,and those who underwent open ureterolysis were excludedfrom the study. Six females and 3 males fulfilled the inclusioncriteria. Workup included magnetic resonance urography orcomputerized tomography scan, radionuclide scan, and ret-rograde pyelography. With the working diagnosis of RPFwith obstructive uropathy, ureteral obstruction was relievedpreoperatively (double-J stent or percutaneous nephrostomy[PCN]) in all patients. After baseline nadir serum creatininelevels were attained, all patients underwent LU and omentalwrapping as definitive treatment. Postoperatively, medicaltherapy comprising prednisone (0.75 mg/kg/day for 3 months,0.5 mg/kg/day for the next 3 months, followed by 0.25 mg/kg/day for the next 6 months) and tamoxifen (10 mg/day) wasstarted at the time of discharge. In the case of tubercular RPF,antitubercular therapy and prednisone were given.
All patients were followed up every month for the first 3months, after every 3 months until 1 year, and then every 6months. Clinical examination and serum creatinine wereobtained at each visit. Ultrasonography was done every 3months for the first year and thereafter every 6 months.Imaging (computerized tomography scan, magnetic reso-nance urography, or radionuclide scan) was done every 6months or earlier, if indicated. We analyzed demographic andclinical data including preoperative and postoperative serumcreatinine levels, preoperative intervention, intraoperativefindings, operative time, estimated blood loss, complications,duration of hospital stay, and serum creatinine at the time oflast follow-up. Success was defined as absence of symptoms,stent-free status, improved or stable preoperative nadir serumcreatinine levels, and radiologically documented relief ofureteral obstruction.
Technique
In patients with a PCN tube in situ (i.e., those who couldnot be stented preoperatively because of tight narrowing ofthe ureter), RGP was performed just before the start of LU.Surgery was then performed. On completion of LU, a double-J stent was inserted. This was possible in all such cases.Patients with a double-J stent already in situ straightawayunderwent surgery, and the same stent was kept after com-pletion of LU.
LU was done by the transperitoneal approach in the 45�flank position in all cases. First, a 12-mm port (camera port)was placed by the open technique at the level of the umbilicusabout two fingers width toward the side to be operated on. Theperitoneal cavity was inspected with a 30� telescope followedby placement of two other ports: a 10-mm port in the mid-clavicular line in the iliac fossa (on the side to be operated on)and a 5-mm port between the xiphoid and the umbilicus(Fig. 1). In cases of bilateral ureteral obstruction (2 cases), the12-mm and 5-mm ports were common for both sides; onlythe 10-mm port was inserted separately on both sides.
As severe fibrotic encasement makes identification of theureter difficult, the ureter was identified in its proximal anddistal segment, which was relatively less encased by fibrotic
plaque. Distally, the ureter was identified at the level of itscrossing over the iliac vessels. Proximally, the right ureterwas identified on the right lateral border of the inferior venacava and medial to the lower pole of the right kidney, and theleft ureter was identified near the left gonadal vein and medialto the lower pole of the left kidney. Vascular loops were thenpassed around the proximal and distal unencased ureteralsegments. An additional 5-mm port was inserted in the an-terior axillary line at the level of the umbilicus, and usingvascular loops as slings the ureter was lifted proximally anddistally by the assistant. This provided countertraction forgentle blunt and sharp dissection to easily free the uretercompletely. We took multiple biopsy specimens from thefibrous tissue. If the ureter was accidentally opened, it wasclosed using polyglactin 910 (Vicryl�; Ethicon, Somerville,NJ) 4-0 sutures. Finally, the omentum was wrapped aroundthe whole of the dissected segment of the ureter and fixedwith Vicryl 4-0 sutures, taking two or three bites (Fig. 2). Wedid not make or prepare the omental wrap. A portion of theomentum that could be easily pulled and wrapped cir-cumferentially around the involved abdominal segment ofthe ureter was used. For bilateral cases, the patient was turnedto the opposite side for surgery.
Results
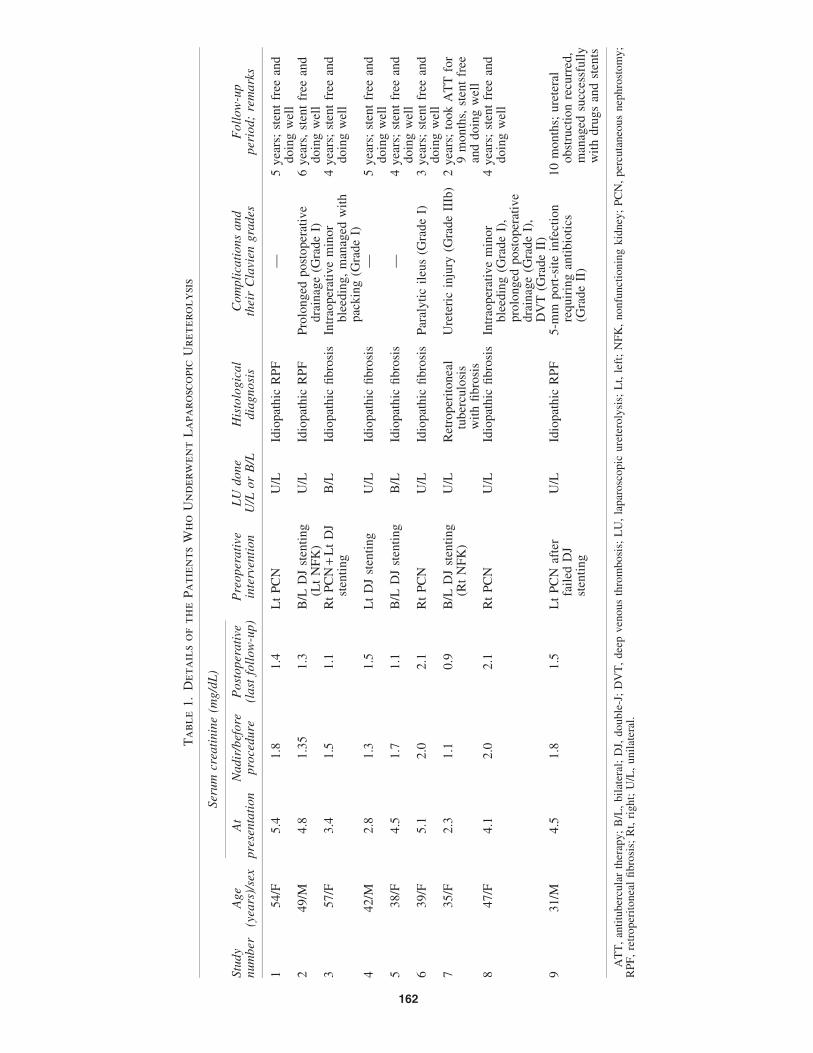
The data regarding demographic characteristics, clinicalparameters, preoperative intervention, intraoperative find-ings, complications, and follow-up are shown in Table 1. Thepatients included 6 females and 3 males. Mean age was 43.5years (range, 35–57 years), and mean body mass indexwas 27.5 kg/m2 (range, 20–37 kg/m2). Mean serum creatininelevel at presentation was 4.1 mg/dL (range, 2.3–5.4 mg/dL).Mean nadir serum creatinine level before LU was 1.6 mg/dL(range, 1.1–2.0 mg/dL). The most frequent clinical presen-tation was flank pain with uremic symptoms. One patientpresented with anuria for the last 24 hours (Case 7, withprimary tubercular RPF). A possible etiology of RPF couldbe identified only in 1 (11%) case (Table 1).
Preoperative intervention was in the form of either PCN in5 cases or double-J stenting in 6 cases. In total, all 11 cases (9patients) underwent LU and omental wrapping (Table 1).None of the cases required conversion to open surgery. Mean
FIG. 1. Port placement for right-sided laparoscopic ur-eterolysis with the patient in the 45� flank position.
160 ARVIND ET AL.

operative time was 198 minutes (range, 180–280 minutes) forunilateral and 275 minutes (range, 270–280 minutes) for bi-lateral LU. Estimated blood loss was about 119 mL (range,70–200 mL). The longer duration of operation in bilateralcases was mainly attributed to the dissection part of theprocedure. The classical finding of a grayish-white fibroustissue plaque encasing the abdominal ureter that showed fi-broblast proliferation, lymphocytes, plasma cells, and mac-rophages on histopathologic examination was present in allexcept 1 case (Case 7, with primary tubercular RPF).
The only significant intraoperative complication (1/9[11%]) was ureteric injury that occurred during a difficultureteric dissection in 1 case of tubercular RPF. The ureteraltear was repaired using fine interrupted sutures. Minorbleeding during surgery occurred in 2 cases from multiplesmall vessels around the perifibrotic tissue in 1 case and fromsmall vessels around renal hilum in another case. Bleedingwas successfully controlled in both cases by packing andapplication of vascular clips, bipolar cautery, and Surgicel�
(Ethicon). Postoperatively, deep venous thrombosis devel-oped in 1 case and prolonged the hospital stay. Other minorpostoperative complications that were managed without needof any specific therapy included prolonged drainage fromoperative area (2 cases) and prolonged ileus (1 case). Oralfeeding was started 24–36 hours after the procedure. Themean duration of hospital stay was 5 days (range, 3–12 days).The rest of the details of patients in our series are summarizedin Table 1.
Mean follow-up was 46 months (range, 4–72 months).Mean postoperative timing of removal of stents was 6 weeks(range, 4–8 weeks). At last follow-up, 8 of the 9 patients weresymptom-free, had improved or stable preoperative nadirserum creatinine levels without stents, and had radiologicallydocumented relief of ureteral obstruction (success rate, 89%).None of the patients experienced drug treatment-related toxiceffects requiring stopping of drugs. One patient in whomureteral obstruction recurred after 4 months of LU is beingmanaged with stenting and drugs.
Discussion
RPF is an uncommon but severe disease that may result inobstructive uropathy and renal loss. Prompt diagnosis and
appropriate treatment may prevent such urologic complica-tions. Despite the possibility of severe renal functionaldamage, there is no standardized treatment of RPF. Medicalmanagement (with or without stents) consisting of cortico-steroids,14 azathioprine, cyclophosphamide,15 and tamoxi-fen16 has been used, but optimum doses and duration ofdrugs are not well established.14 Open ureterolysis or LU withor without adjuvant corticosteroids has also been reported withgood outcomes.8,17–27 However, there have been no pro-spective randomized trials comparing different approaches.
Because of varied symptoms of RPF, patients are often firstseen by medical specialities and later referred to the urologydepartment.28 Ureteral involvement with hydronephrosisoccurs in 80%–100% cases, and in about one-fourth tothree-fourths of patients at least one kidney is irreversiblydamaged.1,6,28 However, the exact incidence of obstructiveuropathy due to RPF is not clear in the literature,28 and noprospective study so far has reported on treatment outcomes(medical/surgical), particularly in patients of RPF with ob-structive uropathy. In our series 7 of the 9 patients (77.7%)lost the use of one kidney, another 2 had bilateral ureteralobstruction, and all had obstructive uropathy at presentation(Table 1). Furthermore, in spite of evolving obstructiveuropathy in RPF, renal function may initially remain normalfor a long period, and symptoms are vague, making earlydiagnosis difficult. Thus, diagnosis is usually delayed untilureteral obstruction and/or obstructive uropathy ensues.6 Inother words, the presence of obstructive uropathy with loss ofone kidney probably indicates advanced disease. Corticos-teroids are usually effective in the early stage of RPF (butmay not work in all cases); later stages are less likely to beresponsive to medical treatment.29
In RPF with obstructive uropathy there are two options fortreatment: first, relief of obstruction by stents or PCN fol-lowed by drugs (corticosteroid alone or with azathioprine,mycophenolate mofetil, or tamoxifen); and second, relief ofobstruction by surgical ureterolysis with or without adju-vant corticosteroid therapy.1,6,17,30–32 Both options have beentried with almost comparable results. Considering the firstoption, neither the type, dose, and duration of drugs nor theduration of urinary drainage (stents or PCN) is clear.32,33
Recently, Fry et al.33 reported successful treatment of 24patients with prednisone and stents only. Twenty-three of the
FIG. 2. (A and B) The omentum is being wrapped around the dissected segment of the ureter and fixed with Vicryl 4-0sutures.
LAPAROSCOPIC URETEROLYSIS AND OMENTAL WRAPPING FOR RPF 161
Ta
ble
1.
Deta
ils
of
th
eP
atien
ts
Wh
oU
nd
erw
en
tL
apa
ro
sco
pic
Uretero
ly
sis
Ser
um
crea
tinin
e(m
g/d
L)
Stu
dy
num
ber
Age
(yea
rs)/
sex
At
pre
senta
tion
Nadir
/bef
ore
pro
cedure
Post
oper
ati
ve(l
ast
foll
ow
-up)
Pre
oper
ati
vein
terv
enti
on
LU
done
U/L
or
B/L
His
tolo
gic
al
dia
gnosi
sC
om
pli
cati
ons
and
thei
rC
lavi
engra
des
Foll
ow
-up
per
iod;
rem
ark
s
154/F
5.4
1.8
1.4
Lt
PC
NU
/LId
iopat
hic
RP
F—
5yea
rs;
sten
tfr
eean
ddoin
gw
ell
249/M
4.8
1.3
51.3
B/L
DJ
sten
ting
(Lt
NF
K)
U/L
Idio
pat
hic
RP
FP
rolo
nged
post
oper
ativ
edra
inag
e(G
rade
I)6
yea
rs,
sten
tfr
eean
ddoin
gw
ell
357/F
3.4
1.5
1.1
Rt
PC
N+
Lt
DJ
sten
ting
B/L
Idio
pat
hic
fibro
sis
Intr
aoper
ativ
em
inor
ble
edin
g,
man
aged
wit
hpac
kin
g(G
rade
I)
4yea
rs;
sten
tfr
eean
ddoin
gw
ell
442/M
2.8
1.3
1.5
Lt
DJ
sten
ting
U/L
Idio
pat
hic
fibro
sis
—5
yea
rs;
sten
tfr
eean
ddoin
gw
ell
538/F
4.5
1.7
1.1
B/L
DJ
sten
ting
B/L
Idio
pat
hic
fibro
sis
—4
yea
rs;
sten
tfr
eean
ddoin
gw
ell
639/F
5.1
2.0
2.1
Rt
PC
NU
/LId
iopat
hic
fibro
sis
Par
alyti
cil
eus
(Gra
de
I)3
yea
rs;
sten
tfr
eean
ddoin
gw
ell
735/F
2.3
1.1
0.9
B/L
DJ
sten
ting
(Rt
NF
K)
U/L
Ret
roper
itonea
ltu
ber
culo
sis
wit
hfi
bro
sis
Ure
teri
cin
jury
(Gra
de
IIIb
)2
yea
rs;
took
AT
Tfo
r9
month
s,st
ent
free
and
doin
gw
ell
847/F
4.1
2.0
2.1
Rt
PC
NU
/LId
iopat
hic
fibro
sis
Intr
aoper
ativ
em
inor
ble
edin
g(G
rade
I),
pro
longed
post
oper
ativ
edra
inag
e(G
rade
I),
DV
T(G
rade
II)
4yea
rs;
sten
tfr
eean
ddoin
gw
ell
931/M
4.5
1.8
1.5
Lt
PC
Naf
ter
fail
edD
Jst
enti
ng
U/L
Idio
pat
hic
RP
F5-m
mport
-sit
ein
fect
ion
requir
ing
anti
bio
tics
(Gra
de
II)
10
month
s;ure
tera
lobst
ruct
ion
recu
rred
,m
anag
edsu
cces
sfull
yw
ith
dru
gs
and
sten
ts
AT
T,
anti
tuber
cula
rth
erap
y;
B/L
,bil
ater
al;
DJ,
double
-J;
DV
T,
dee
pven
ous
thro
mbosi
s;L
U,
lapar
osc
opic
ure
tero
lysi
s;L
t,le
ft;
NF
K,
nonfu
nct
ionin
gkid
ney
;P
CN
,per
cuta
neo
us
nep
hro
stom
y;
RP
F,
retr
oper
itonea
lfi
bro
sis;
Rt,
right;
U/L
,unil
ater
al.
162

24 patients had obstructive uropathy at presentation, but only7 (29%) had a solitary functioning kidney. Average stentduration was 13.7 months (range, 2–50 months), and steroidtherapy was administered for a mean period of 34 months.Success rate in their series was 75%. In another series, Ilieet al.32 treated 28 patients (25 had obstructive uropathy) withstent(s) or PCN with or without steroids. The mean stentduration was 19.34 months (range, 2–60 months). Althoughthese authors reported a success rate of 86% at last follow-up,their criteria of successful treatment were symptom-free statusand stable serum creatinine level only. After a mean follow-upof 60.9 months (range, 24–110 months), 5 patients were still onstents and steroids, and 8 additional patients were on stentswithout steroids. Thus, 15 (54%) patients were stent free andoff steroids. These data indicate that the efficacy of medicalmanagement (with urinary drainage) in patients of RPF withobstructive uropathy is not well documented and that thedurations for which stent(s) or PCN are required are usuallylonger (2–60 months).14,30–33 In RPF patients who are alreadyin obstructive uropathy (many with a solitary functioningkidney), longer durations of stents or PCN along with steroidsmay place them at more risk of complications related to stentsor PCN.34–36 In view of the above data we proceeded withinitial LU in our patients of RPF with obstructive uropathy.However, we do institute adjuvant medical management(prednisone and tamoxifen) in order to further reduce the re-currence risk and to relieve systemic manifestations of RPFthat are not tackled by surgery. In our patients mean stentduration was only 6 weeks post-LU, and 89% (8/9) patientswere stent free and off drugs. In a similar series reportedrecently, Sinescu et al.37 reported results for 19 patientswith RPF (17 had obstructive uropathy) treated by ureter-olysis and omental wrapping without adjuvant steroids.Stent duration was 1 month. After at least 1 year of follow-up 17 of 19 patients were stent free, and 15 of the 17 patientswith obstructive uropathy (88%) had normal serum creati-nine levels.
Ureterolysis (open or laparoscopic) has been reported tohave a success rate as high as 100%.8,12,18,25,26 The open ap-proach for ureterolysis has approximately 9% mortalityand 60% morbidity.18 In an attempt to reduce procedure-related morbidity Kavoussi et al.19 first described LU in 1992.Since then LU has been used by several investigators (withsome modifications) only to demonstrate common advan-tages of minimal invasiveness of laparoscopy and compara-ble efficacy to the open approach.18,20–27 Elashry et al.18
compared the results of six LU procedures with seven openureterolyses (all unilateral cases) and found the laparoscopicapproach to be better in all aspects they considered exceptmean operative time (255 minutes for laparoscopic versus232 minutes for the open approach). Our mean operative timefor 7 unilateral LU cases was 196 minutes. In a large series of70 cases of RPF (idiopathic and secondary) comparing LU(36 cases) with the open approach (34 cases), no differencewas found in terms of operative time, estimated blood loss,length of hospital stay, complications, transfusion require-ments, and postoperative resolution of ureteral obstruction.But, for idiopathic RPF cases treated by LU, hospital stay andtransfusion requirement were significantly less than forpatients who underwent open ureterolysis.25 The reportedsuccess rate of LU is 83%–100% at 17–36 months of follow-up.8,18,25,26 The reported rate of intraoperative and peri-
operative complications of LU can be as high as 30%, and suchcomplications include bleeding, urinary leakage, epididymo-orchitis, port-site erythema, urinary retention, and ileus.22 Inour series, apart from minor intraoperative complications theonly significant problem was ureteric injury. One patient inwhom ureteral obstruction recurred after 4 months of LU wasnoncompliant and did not follow the postoperative drugregimen.
A debatable point is whether ureterolysis should be com-bined or not with ureteral intraperitonealization or omentalwrapping. Although there is no proven basis for these addi-tional steps, ureterolysis done as an isolated procedure isassumed to have more chance of recurrences. In our experi-ence omental wrapping adds only a few extra minutes to thetotal operative time.
Drawbacks of this series include its retrospective natureand the small number of cases. However, our results indicatethat LU with omental wrapping in patients with RPF andobstructive uropathy can be safe and effective and thus avalid option with a high success rate.
Conclusions
LU with omental wrapping in the setting of obstructiveuropathy provides all the advantages of minimal invasivenessand is a safe and effective alternative with a high success rateat mid- to long-term follow-up.
Disclosure Statement
No competing financial interests exist.
References
1. Vaglio A, Salvarai C, Buzio C. Retroperitoneal fibrosis.Lancet 2006;367:241–251.
2. Buff DD, Bogin MB, Faltz LL. Retroperitoneal fibrosis: Areport of selected cases and review of the literature. NYState J Med 1989;89:511–516.
3. Ormond JK. Bilateral uretral obstruction due to envelop-ment and compression by an inflammatory retroperitonealprocess. J Urol 1948;59:1072–1079.
4. Cronin CG, Lohan DG, Blake MA, Roche C, McCarthy P,Murphy JM. Retroperitoneal fibrosis: A review of clinicalfeatures and imaging findings. AJR Am J Roentgenol2008;191:423–431.
5. Chan SL, Johnson HW, McLoughlin MG. Idiopathic ret-roperitoneal fibrosis in children. J Urol 1979;122:103–104.
6. Moroni G, Gallelli B, Banfi G, Sandri S, Messa P, Ponti-celli C. Long-term outcome of idiopathic retroperitonealfibrosis treated with surgical and/or medical approaches.Nephrol Dial Transplant 2006;21:2485–2490.
7. Kottra JJ, Dunnick NR. Retroperitoneal fibrosis. RadiolClin North Am 1996;43:1259–1275.
8. Duchene DA, Winfield HN, Cadeddu JA, Clayman RV,Gomella LG, Kavoussi LR, et al. Multi-institutional surveyof laparoscopic ureterolysis for retroperitoneal fibrosis.Urology 2007;69:1017–1021.
9. Ormond JK. Idiopathic retroperitoneal fibrosis: An estab-lished clinical entity. JAMA 1960;19:1561–1568.
10. Streem SB, Frankee JJ, Smith JA Jr. Management of upperurinary tract obstruction. In: Walsh PC, Retik AB, VaughanED, Wein AJ (eds.). Campbell’s Urology, 8th ed. Phila-delphia: W.B. Saunders, 2002:463–512.
LAPAROSCOPIC URETEROLYSIS AND OMENTAL WRAPPING FOR RPF 163

11. Tiptaft RC, Costello AJ, Paris AM, Blandy JP. The longterm follow-up of idiopathic retroperitoneal fibrosis. Br JUrol 1982;54:620–624.
12. Lepor H, Walsh PC. Idiopathic retroperitoneal fibrosis.J Urol 1979;122:1–6.
13. Barbalias GA, Liatsikos EN. Idiopathic retroperitoneal fi-brosis revisited. Int Urol Nephrol 1999;31:423–429.
14. Kardar AH, Kattan S, Lindstedt E, Hanash Kal. Steroidtherapy for idiopathic retroperitoneal fibrosis: Dose andduration. J Urol 2002;168:550–555.
15. Marcolongo R, Tavolini IM, Laveder F, Busa M, NoventaF, Bassi P, et al. Immunosuppressive therapy for idiopathicretroperitoneal fibrosis: A retrospective analysis of 26cases. Am J Med 2004;116:194–197.
16. van Bommel EF, Hendriksz TR, Huiskes AW, Zeegers AG.Brief communication: Tamoxifen therapy for nonmalignantretroperitoneal fibrosis. Ann Intern Med 2006;144:101–106.
17. Baker LR, Mallinson WJW, Gregory MC, Menzies EA,Cattell WR, Whitfield HN, et al. Idiopathic retroperitonealfibrosis. A retrospective analysis of 60 cases. Br J Urol1988;60:497–503.
18. Elashry OM, Nakada SY, Wolf JS, Figenshau RS,McDougall EM, Clayman RV. Ureterolysis for extrinsicureteral obstruction: A comparison of laparoscopic andopen surgical techniques. J Urol 1996;156:1403–1410.
19. Kavoussi LR, Clayman RV, Brunt LM, Soper NJ. La-paroscopic ureterolysis. J Urol 1992;147:426–429.
20. Matsuda T, Arai Y, Muguruma K, Uchida J, Shichiri Y,Komatz Y. Laparoscopic ureterolysis for idiopathic retro-peritoneal fibrosis. Eur Urol 1994;26:286–290.
21. Demirci D, Gulmez I, Ekmekcioglu O, Sozuer EM, KeklikE. Intraperitonealization of the ureter during laparoscopicureterolysis: A modification of the technique. J Urol 2001;165:180–181.
22. Fugita OE, Jarrett TW, Kavoussi P, Kavoussi LR. La-paroscopic treatment of retroperitoneal fibrosis. J Endourol2002;16:571–574.
23. Wen CC, Wang DS. Laparoscopic ureterolysis for benignand malignant conditions. J Endourol 2005;19:710–714.
24. Fong BC, Porter JR. Laparoscopic ureterolysis: Technicalalternatives. J Endourol 2006;20:820–822.
25. Srinivasan AK, Richstone L, Permpongkosol S, KavoussiLR. Comparison of laparoscopic with open approach forureterolysis in patients with retroperitoneal fibrosis. J Urol2008;179:1875–1878.
26. Simone G, Leonardo C, Papalia R, Guaglianone S, GallucciM. Laparoscopic ureterolysis and omental wrapping. Ur-ology 2008;72:853–858.
27. Castilho LN, Mitre AI, Iizuka FH, Fugita OE, Colombo JRJr, Arap S. Laparoscopic treatment of retroperitoneal fi-brosis: Report of two cases and review of the literature. RevHosp Clin Fac Med Sao Paulo 2000;55:69–76.
28. Brandt AS, Kamper I, Kukuk S, Haage P, Roth S. Asso-ciated findings and complications of RPF in 204 patients.J Urol 2011;185:526–531.
29. Money S. Idiopathic retroperitoneal fibrosis: Prompt diag-nosis preserves organ function. Cleve Clin J Med 2002;69:160–166.
30. Vaglio A, Palmisano A, Alberici F, Maggiore U, Ferretti S,Cobelli R, et al. Prednisone versus tamoxifen in patientswith idiopathic retroperitoneal fibrosis: An open-labelrandomised controlled trial. Lancet 2011;378:338–346.
31. Alder S, Lodermeyer S, Gaa J, Heemann U. Successfulmycophenolate mofetil therapy in nine patients with idio-pathic retroperitoneal fibrosis. Rheumatology (Oxford)2008;47:1535–1538.
32. Ilie CP, Pemberton RJ, Tolley DA. Idiopathic retroperito-neal fibrosis: The case for nonsurgical treatment. BJU Int2006;98:137–140.
33. Fry AC, Singh S, Gunda SS, Boustead GB, Hanbury DC,McNicholas TA, et al. Successful use of steroids and ure-teric stents in 24 patients with idiopathic retroperitonealfibrosis: A retrospective study. Nephron Clin Pract 2008;108:c213–c220.
34. Dyer RB, Chen MY, Zagoria RJ, Regan JD, Hood CG,Kavanagh PV. Complications of ureteral stent placement.Radiographics 2002;22:1005–1022.
35. Richter S, Ringel A, Shalev M, Nissenkorn I. The in-dwelling ureteric stent: A ’friendly’ procedure with un-friendly high morbidity. BJU Int 2000;85:408–411.
36. Hausegger KA, Portugaller HR. Percutaneous nephrostomyand antegrade ureteral stenting: Technique—Indications—Complications. Eur Radiol 2006;16:2016–2030.
37. Sinescu I, Surcel C, Mirvald C, Chibelean C, Gıngu C,Avram D, et al. Prognostic factors in retroperitoneal fi-brosis. J Med Life 2010;3:19–25.
Address correspondence to:Onkar Singh, MS
Department of UrologyBhopal Memorial Hospital & Research Centre
Bhopal, 462038India
E-mail: [email protected]
164 ARVIND ET AL.