laporan pagi 14 agustus 2013
DESCRIPTION
Laporan Pagi Penyakit DalamTRANSCRIPT

MORNING REPORTPULMONOLOGY DIVISION, 14 AUGUST 2013

PATIENT’S DATA
Identitiy
Name : Ms. Muslimah
Gender : Female
Age : 21 years old
Marriage Status : Unmarriage
Address : Sungai Danau, Tanah Bumbu
Religion : Mosleem
Tribe : Banjar
Occupation : -
Date of Enter : 14/08/2013 00.15 a.m

AnamnesisMajor complaint :
Shortness of breath
History of present illness:
Patient complained shortness of breath since one week before entering the hospital. Shortness of breath happened in sudden onset, and get worsed. shortness of breath accompanied by productive cough and coughing up blood for more than 3 weeks. Patient complaints fever and sweating in the night without physical activity. Decreased appetite (+). weight loss as much as 5 kg. No history of allergy. Patient admitted that her mother who passed away had the same complaint.
Past Medical History : asthma(-), HT(-), DM (-)
Family Medical History : mother had same complaint

Physical Examinationgeneral state : Good
Awareness : Compos Mentis.
Circumstances Nutrition : Less, W = 37 kg, H = 150 cm, BMI = 17.18 kg/m2
Vital Signs : BP: 100/60 mmHg right arm lying position with aneroid sphygmomanometer
P: 120x/mnt, regular, strong;
RR: 32 x / mnt torako-abdominal;
T: 36.5 ° C right axilla, digital thermometer.
SaO2: 95% without O2
Skin: good turgor. Nodules (-), petechiae (-), jaundice (-).
Head: Deformity (-).
Hair: Color black, is not easily removed, spread evenly.
Eyes: lid edema (-) / (-). Anemic conjunctiva (-) / (-). Sclera jaundice (-) / (-).

Physical ExaminationEar: defect (-). Cerumen (-). Secretions (-).
Nose: septal deviation (-). Secretions (-), bleeding (-).
Mouth and Teeth: moist lips and oral mucosa, dental caries (-), ulcers (-)
Throat: The pharynx hyperemia (-), not enlarged tonsils.
Neck: Trachea in the middle, enlargement KGB (-), enlargement of the thyroid gland (-), JVP does not increase

• Pulmonology physical examination• Inspection:
• Chest Wall Structure
• Symmetry
• Hyperinflation (-), Retraction of ICS (-)
• Sternal deformity: Pectus Carinatum(-), Pectus Excavatum (-)
• Spinal deformity: Kyphosis (-), Gibbus (-), Lordosis (-), Scoliosis (-)
• Use of accessory of respiratory muscles (-)
• Clubbing (-)
• Skin – cyanosis (-), rashes (-)

• PALPATION
• Adenopathy (-)
• Tracheal position –in the midline
• Thyroid gland – At the base of the neck
• Fremitus vocal:
↑ normal
↑ normal
↑ normal
PERCUSSION
dull normal
dull normal
dull normal
AUSCULTATION
R V
R V
R V

Support examinationExamination Result Reference Unit
HEMATOLOGI
Hemoglobin 11,2 13,00 – 17,0 g/dl
Lekosit 4,8 4,0 – 10,5 ribu/ul
Eritrosit 4,3 4,5 – 6,00 juta/ul
Hematokrit 34,3 42 – 52 vol%
Trombosit 316 150 – 450 ribu/ul
RDW-CV 14 11,5 – 14,7 %
MCV, MCH, MCHC
MCV 79,9 80,0 – 97 Fl
MCH 26,0 27,0 – 32,0 Pg
MCHC 32 32,0 – 38,0 %
KIMIA
HATI
SGOT 104 0-46 U/I
SGPT 74 0-45 U/I
GINJAL
Ureum 17 10 – 50 mg/dl
Creatinin 0,6 0,7 – 1,4 mg/dl

Support ExaminationChest X-Ray (13/08/2013)

Problem List
• Susp Pulmonary Tb
• Anemia microcytic normochromic

Cue & Clue2 ProblList Idx PDx PTx Pmo
Anamnesis:
Dyspnea (+). productive cough (+), hemoptisis (+ )more than 3 weeks. Fever (+),sweating in the night without physical activity (+). Decreased appetite (+). weight loss (+)Physical examination:Percussion:dull sonor
dull sonor
dull sonor
Auscultation: R V
V V
V V
-Susp pulmonaryTb-Anemiamicrocytic normochromic
1. Susp Pulmonary Tb
2. Chronic Bronchitis
3. Pneumonia
-Laboratorium:-LED-Sputum (3 times)-Sputum culture
•Non-Pharmacologic - high protein high calorie diet•Pharmacology - Infus NS: D5 (1:1) 20 tpm - inj. Tranexamat acid amp 3x1 - ambroxol 30 mg tab 3x1 - anti-tuberculosis drugs: Category 1 : 2(HRZE)/4(HR)3.
•Subjective complaints, vital sign, hematologi, CXR•Education Plan : Inform the patient and family about the illness and therapy that have been given

TERIMA KASIH




• Proliva: membantu menjaga kesehatan fungsi hati
• Mengandung: Selenium 200 mcg, milk thistle 300 mg, citrus bioflavonoids 120 mg, bilberry 100 mg, alfa lipoic acid 100 mg, quercetin 95% 50 mg, turmeric 40 mg, licorice 40 mg, dandelion 35 mg
• Kemasan: tablet salut selaput
• Dosis: 1 tablet sehari
• Dikonsumsi bersama dengan makanan










Click icon to add picture

MORNING REPORTPulmonology Division
14 August 2013
Pulmonology Division14 August 2013

DATA PASIENIdentitas
Nama : Nn. Noraini
Jenis Kelamin : Perempuan
Umur : 16 th
Status : Belum Menikah
Alamat : Kembang Halang Rantau
Agama : Islam
Suku Bangsa : Jawa
Pekerjaan : Pelajar
Masuk RSUD Ulin : 21/07/2013 Pukul 18.15 WITA

AnamnesisKeluhan Utama :
Nyeri perut
Riwayat Penyakit Sekarang :
Pasien mengeluhkan nyeri di ulu hati seperti ditusuk-tusuk sejak 1 hari SMRS. Keluhan dirasakan muncul mendadak, hilang timbul dan berlangsung sekitar 15-45 menit. Nyeri perut muncul saat perut kosong. Keluhan disertai perasaan kembung, mual dan apabila makan terasa cepat kenyang dan muntah. Nyeri perut berkurang apabila pasien meminum antasida sirup yang dibeli sendiri. Tidak ada keluhan sulit menelan, rasa pahit di mulut, penurunan berat badan yang drastis dalam 3 bulan terakhir, batuk, dan kulit kuning. Pasien juga mengeluhkan nyeri di suprapubik sehabis kencing sejak 3 hari SMRS. Nyeri dirasakan seperti terbakar. Tidak ada nyeri pinggang atau demam. Tidak ada keputihan yang berlebih. Siklus menstruasi normal dan tidak ada nyeri perut saat haid. Sebelum masuk RSUD Ulin Pasien pernah dirawat di RS Rantau dengan keluhan nyeri perut sekitar 1 bulan yang lalu.
Riwayat Penyakit Dahulu : HT(-), DM (-)
Riwayat Penyakit Keluarga: HT(-), DM (-)

Pemeriksaan Fisik
Keadaan Umum : Baik
Kesadaran : Compos Mentis.
Keadaan Gizi : Cukup, BB= 51 kg, TB=158 cm, IMT= 20,43 kg/m2
Tanda Vital : TD: 100/70 mmHg lengan kanan posisi berbaring dengan sfigmomanometer aneroid
N: 87x/mnt,reguler,kuat;
RR: 22 x/mnt abdomino-torakal;
T: 36,5 oC aksilla kanan, termometer digital.
Kulit : Turgor baik. Petechiae (-),Ikterus (-).
Kepala : Deformitas (-).
Rambut : Warna hitam, tidak mudah dicabut,
tersebar merata.
Mata : Edema palpebra (-/(-). Konjungtiva anemis
(-)/(-). Sklera ikterik (-)/(-).

Pemeriksaan FisikTelinga : Defek (-). Serumen (-) . Sekret (-).
Hidung : Deviasi septum (-). Sekret (-), Perdarahan (-).
Mulut dan Gigi : bibir dan mukosa mulut lembab, karies dentis (-), ulkus (-)
Tenggorokan : Faring hiperemis (-), tonsil tidak membesar.
Leher : Trakea di tengah, pembesaran KGB (-), pembesaran kelenjar tiroid (-), JVP tidak meningkat
ThorakInspeksi: Simetris. Tdk ada yg tertinggal. Palpasi : Fremitus ka : ki normal. Nyeri tekan (-), krepitasi (-).Perkusi : sonor pada semua lapang paru. Batas paru hati pada ICS 6 , batas paru lambung
pada ICS 7 linea aksilaris anteriorAuskultasi : suara napas vesikular, Rh (-), Wh (-).

Pemeriksaan FisikCor
Inspeksi : Ictus Cordis tidak terlihat, sikatrik (-), sianosis (-)
Palpasi : Ictus Cordis teraba pada sela iga 5 MCL kiri, thrill (-).
Perkusi : Batas jantung kanan pada garis parasternal kanan. Batas jantung kiri 2 jari medial garis midclavicula kiri.
Auskultasi : Bunyi jantung I - II (N). Murmur (-). Gallop (-).
Abdomen
Inspeksi : Perut datar . Venektasi (-).
Palpasi : Nyeri Tekan (+) pada regio epigastrium dan suprapubic. Hati/Lien/Massa tidak teraba.
Perkusi : Timpani. Shifting Dullness (-).
Auskultasi : Bising usus (+) normal.
Anggota Gerak : Akral hgt. Edema (-)
Px ketok ginjal (-) kiri dan kanan

Pem. PenunjangPemeriksaan Lab
Hb : 14,1 gr/dl
Leukosit : 7,8 ribu/ul
Eritrosit : 4,91 juta
Hematokrit : 41,6 volume%
Trombosit : 153 ribu/ul
RDW-CV : 12,5%
MCV : 84,9 ft
MCH : 28,7 pg
MCHC : 33,8%
Gran % : 79,1 (50,0-70,0 %)
Limfosit % : 15,0 (25,0-40,0 %)
MID% : 5,9%
Limfosit # :1,2 (1,25-4,0 ribu/ul)
GDS: 103 mg/dl
SGOT: 25 u/l
SGPT: 14 u/l
Ureum: 29 mg/dl
Creatinin: 0,6 mg/dl

Resume data dasar
Nyeri di ulu hati (+) sejak 1 hari SMRS, muncul mendadak, hilang timbul, berlangsung sekitar 15-45 menit, muncul saat perut kosong. Kembung (+), mual (+), cepat kenyang (+) muntah (+). sulit menelan (+), nyeri suprapubik sehabis kencing (+) nyeri pinggang (-), demam, keputihan (-). Nyeri tekan pada epigastrium dan supra pubik (+)

Daftar Masalah
1. Sindroma Dispepsia
2. Susp Cystitis

Cue & Clue2 ProblList Idx PDx PTx Pmo
Anamnesis:Pasien mengeluhkan nyeri ulu hati seperti ditusuk-tusuk sejak 1 hari SMRS. Keluhan dirasakan muncul mendadak, hilang timbul dan berlangsung sekitar 15-45 menit. Nyeri perut muncul saat perut kosong. Keluhan disertai perasaan kembung, mual dan apabila makan terasa cepat kenyang dan muntah. Nyeri perut berkurang apabila pasien meminum antasida sirup yang dibeli sendiri. Tidak ada keluhan sulit menelan, rasa pahit di mulut, penurunan berat badan yang drastis dalam 3 bulan terakhir, batuk, dan kulit kuning. Sebelum masuk RSUD Ulin Pasien pernah dirawat di RS Rantau dengan keluhan nyeri perut sekitar 1 bulan yang lalu.Pemeriksaan Fisik:Nyeri tekan abdomen di regio epigastrium
-Nyeri Ulu Hati-- Mual-- Muntah
1. Sindromdispepsia
2. Susp Ulkus gaster
3. Susp Gastritis e.c infeksi H. pylori
- Non invasif H.pylori Test -Barium meal (OMD)- Upper GI endoscopy
- Lifestyle-Inj ranitidin 2x1 -Inj metoclopramide-Antasid syr 3x1 C a.c
•Keadaan umum dan tanda vital

Cue & Clue Prob List Idx PDx PTx Pmo
Anamnesis:Pasien mengeluhkan nyeri di suprapubik sehabis kencing sejak 3 hari SMRS. Nyeri dirasakan seperti terbakar. Tidak ada nyeri pinggang atau demam. Pasien mengaku menggunakan pembersih kewanitaan secara teratur. Tidak ada keputihan yang berlebih. Siklus menstruasi normal dan tidak ada nyeri perut saat haid. Fisik:Nyeri tekan pada regio suprapubik
Nyeri kencing
Uncomplicated cystitis
-Urinalisis-Kultur urin dan tes sensitivitas
-Kaplet Forte (160 mg Trimethoprim – 800 mg Sulfamethoxazole ) 2x1 kaplet selama 3 hari
•Keadaan umum dan vital•urinalisis

TERIMA KASIH

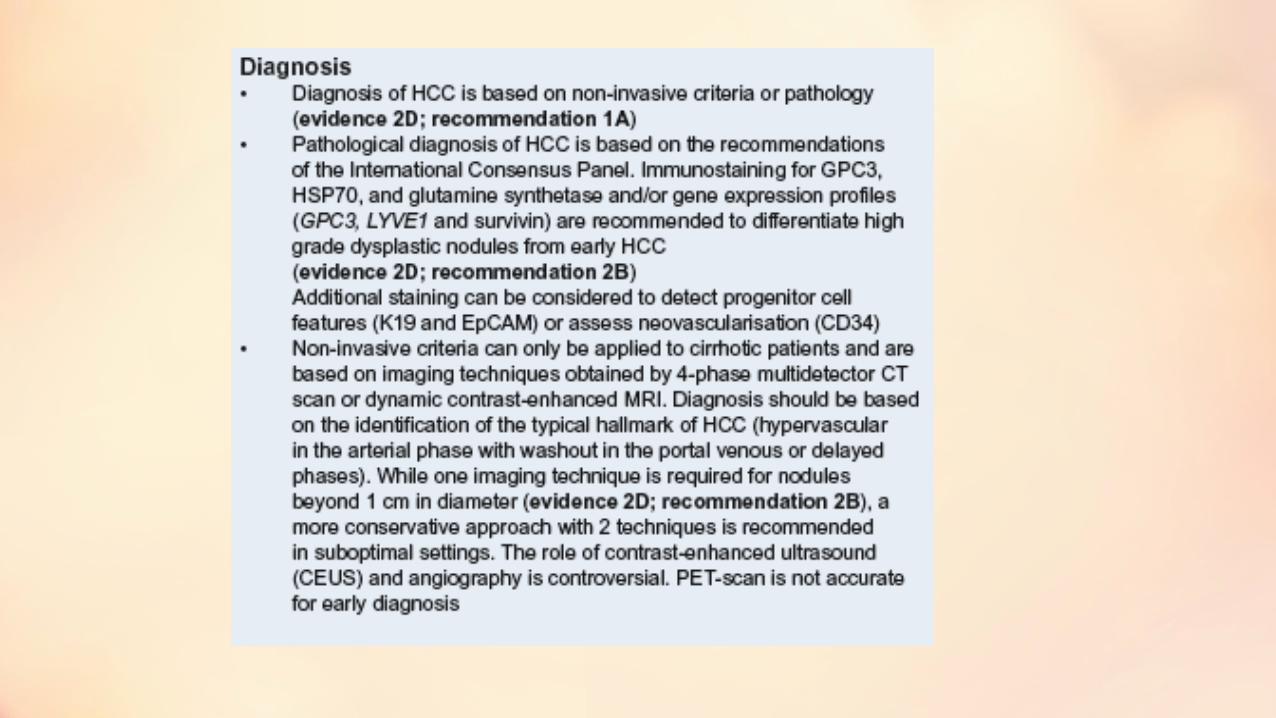
• Dyspepsia
• denotes symptoms and is not itself a disease. The guideline development group accepted the
• Rome II definition:10 Dyspepsia refers to pain or discomfort centred in the upper abdomen.
• .Centred. refers to pain or discomfort in or around the midline. Pain in the right or left
• hypochondrium is not considered to constitute dyspepsia. .Discomfort. refers to a subjective
• negative sensation that the patient does not interpret as pain, which may be characterised by or
• associated with upper abdominal fullness, early satiety, bloating, belching, nausea, retching
• and/or vomiting Patients with functional dyspepsia who identify pain as their predominant symptom may be said
• to have ulcer-like dyspepsia whereas patients with discomfort as their predominant symptom
• may be said to have dysmotility-like dyspepsia.


• ENDOSCOPY VERSUS BARIUM MEAL FOR PATIENTS WITH ALARM FEATURES
• Endoscopy is more sensitive than barium meal at detecting early curable gastric cancer and is
• also more likely to detect gastric and duodenal erosions.30,31 Any lesions seen can also be biopsied
• immediately. A well conducted barium meal is a useful investigation which will detect most
• serious disease in the upper GI tract32 but it does involve a radiation dose (typical effective dose
• 2mSv equivalent to 11 months of background radiation).33 This is particularly relevant now that
• the European Union regulations governing the exposure of patients to medical radiation are in
• force.34
• C Upper GI endoscopy is the investigation of choice when further evaluation is warranted
• and should be widely available.
• þ Barium meal studies are appropriate where the local endoscopy services are unavailable
• or for patients who cannot tolerate endoscopy.
• A A non-invasive H. pylori test and treat strategy is as effective as endoscopy in the initial
• management of patients with uncomplicated dyspepsia who are less than 55 years old.

• BREATH TESTS
• Since their introduction, both 13C and 14C urea breath tests (CUBTs) have been used widely in
• patients both before and after H. pylori eradication therapy.55 An RCT has shown that, compared
• to an accepted gold standard, accuracy was 94.8% before antimicrobial therapy and 95.4%
• afterwards.56 False negative results may occur and CUBT should not be performed within two
• weeks of proton pump inhibitor (PPI) or within four weeks of antibiotic therapy.57

• FAECAL ANTIGEN TESTS
• Enzymatic immunoassays that detect the H. pylori antigen in stool specimens are available. A
• large number of patients have been evaluated using the stool antigen test for the initial diagnosis
• of H. pylori infection and the mean sensitivity and specificity has been calculated at 93.1% and
• 92.8% respectively.62 Caution is needed following eradication therapy as omeprazole significantly
• reduces faecal antigen values, resulting in a decreased accuracy.65,66

• B The CUBT or faecal antigen tests are recommended for the pre-treatment diagnosis of H.
• pylori infection in the community. Less accurate, hospital-based serology tests have a
• place within the non-invasive test and treat strategy.
• B CUBT is the recommended test to determine whether H. pylori has been successfully
• eradicated.
• þ The CUBT should not be performed within two weeks of proton pump inhibitor therapy
• or within four weeks of antibiotic therapy as false negative results may occur.

• A H. pylori eradication therapy should be considered in the management of functional
• dyspepsia.

• H. PYLORI ERADICATION OPTIONS
• The evidence base for H. pylori eradication options has also improved since the previous SIGN
• guidelines were published. An update of the numbers of medicines to use, the duration of
• treatment and the influence of known antimicrobial resistance are given below.
• Dual therapies eradicate H. pylori from fewer people than triple therapies114
• n Triple therapies including PPIs and two antibiotics give consistently high eradication rates
• n Metronidazole or clarithyromycin resistance established by laboratory testing is associated
• with reduced eradication of H. pylori by regimens including these antibiotics
• n Two weeks of triple therapy versus a one week regimen does not increase the eradication rate.
Title and content layout with list
• Add your first bullet point here
• Add your second bullet point here
• Add your third bullet point here









Click icon to add picture