lastingreduction of spasticity after ending chronic
TRANSCRIPT
16ournal of Neurology, Neurosurgery, and Psychiatry 1996;60:168-173
Lasting reduction of severe spasticity after endingchronic treatment with intrathecal baclofen
Jurgen Dressnandt, Bastian Conrad
AbstractObjective-To investigate whether thedose ofintrathecal baclofen necessary for asufficient reduction of muscle tone andspasms changes during treatment ofsevere spasticity.Methods-A group of 27 patients receivedintrathecal baclofen for 61 (SD 18)months.Results-Spasticity remained absent orstrongly reduced after stopping theintrathecal baclofen infusion in sevenpatients. The dose of baclofen could bereduced to 40% of that dose which wasoriginally necessary in 10 patients. Thedose remained the same or increasedslightly in 10 patients. Possible reasons forthe continuing reduction of spasticity afterterminating long term intrathecal baclofeninfusion in some patients could be: lastingmorphological changes in spinal cord neu-rons by second messenger controlled mod-ulation of gene expression, a toxic effect ofbaclofen on spinal neurons, muscularatrophy, inflammation due to the catheter,or progression ofmultiple sclerosis.Conclusions-A higher initial daily dose ofintrathecal baclofen might lead to a faster,lasting suppression of spasticity and thedevelopment of spastic symptoms mighteven be prevented by pre-emptive treat-ment with baclofen in patientswith newly acquired lesions of the spinalcord.
(7 Neurol Neurosurg Psychiatry 1996;60:168-173)
Keywords: intrathecal baclofen; spasticity
Neurologische Klinik,Klinikum rechts derIsar, TechnischeUniversitat Munchen,Mohlstrasse 28,D-81675 Munich,GermanyJ DressnandtB ConradCorrespondence to:Dr J Dressnandt.
Received 8 November 1994and in final revised form4 September 1995Accepted 12 September 1995
For a decade severe forms of spasticity havebeen successfully treated with intrathecal infu-sion of baclofen. 4 Many authors havereported the necessity of increasing the dailydose of baclofen within the first year of treat-ment3 5 6; this stabilises thereafter. After a bolusof baclofen the increased muscle tone disap-pears within 40-90 minutes and reappearsafter four to six hours.' A reappearance ofspasticity has also been described after inter-ruption of long term treatment with intrathe-cal baclofen.7 We found that some patientstreated for several years did not requireintrathecal baclofen treatment any more andin other patients the dose necessary for suffi-cient suppression of spastic symptoms couldbe reduced appreciably. These patients are
described and hypothetical mechanisms arediscussed. Some of this data has been pre-sented previously.8
Patients and methodsPatients with severe forms of paraspasticity ortetraspasticity have been treated with continu-ous intrathecal baclofen at the Department ofNeurology of the Technical University ofMunich since 1986. The antispastic drugbaclofen (racemic solution from Ciba-Geigy)is given into the intrathecal space through asubcutaneous catheter by an implanted pro-grammable pump (Medtronic Synchromed861 1H). The catheter's tip is positioned atthe level of the 10th thoracic vertebra. Theinfusion rate is continuous. During visits torefill the pump, a neurological examinationtakes place, assessing the muscular tone withthe Ashworth scale9 1' and the elicitability ofspasms with a spasm scale.: The dose ofbaclofen is score adjusted (see results section)in accord with a clinical examination and com-plaints of the patient.From the patients who had received a pump
implant in our department, 27 were followedup for more than two years in our outpatientclinic. In 1991 we found that stopping infu-sion of intrathecal baclofen did not lead to areappearance of increased muscle tone in twopatients (1 and 2). Thereafter we tried toreduce the dose of intrathecal baclofengradually in those patients who came regularlyto have the pump refilled. From the 27patients, a trial of reduction of the intrathecalbaclofen dose has been carried out in 23. Thereduction was done in small steps in the out-patient clinic and in bigger steps if the patientswere staying in hospital. We did not try toreduce intrathecal baclofen in patients withtetraspasticity and with a large increase inmuscle tone in the upper limbs or in thosepatients who received a higher dose to reducecentral pain.Up to now intrathecal baclofen infusion has
been discontinued in six patients because ofdead batteries. In another patient the catheterwas prophylactically removed because adecubital ulcer had developed in the route ofthe catheter.
ResultsIt was possible to stop treatment withintrathecal baclofen without the reappearanceof spastic symptoms in seven patients outof 27 and to reduce the dose appreciably
168
on January 13, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.2.168 on 1 February 1996. D
ownloaded from
Lasting reduction of severe spasticity after ending chronic treatment with intrathecal baclofen
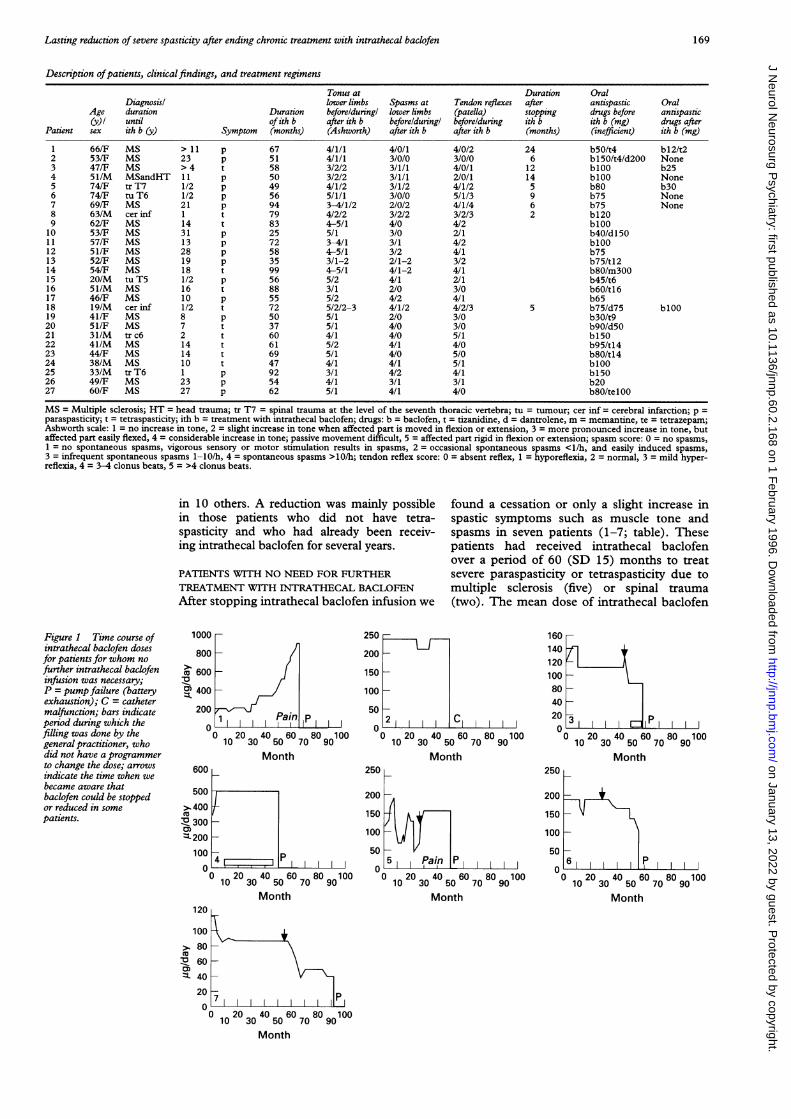
Description ofpatients, clinicalfindings, and treatment regimens
Tonus at Duration OralDiagnosisl lower limbs Spasms at Tendon reflexes after antispastic Oral
Age duration Duration beforelduringl lower limbs (patella) stopping drugs before antispastic(y)/ until of ith b after ith b beforelduringl beforelduring ith b ith b (mg) drugs after
Patient sex ith b (y) Symptom (months) (Ashworth) after ith b after ith b (months) (inefficient) ith b (mg)
1 66/F MS > 11 p 67 4/1/1 4/0/1 4/0/2 24 b50/t4 bl2/t22 53/F MS 23 p 51 4/1/1 3/0/0 3/0/0 6 b150/t4/d200 None3 47/F MS > 4 t 58 3/2/2 3/1/1 4/0/1 12 blOO b254 51/M MSandHT 11 p 50 3/2/2 3/1/1 2/0/1 14 blOO None5 74/F tr T7 1/2 p 49 4/1/2 3/1/2 4/1/2 5 b80 b306 74/F tu T6 1/2 p 56 5/1/1 3/0/0 5/1/3 9 b75 None7 69/F MS 21 p 94 3-4/1/2 2/0/2 4/1/4 6 b75 None8 63/M cer inf 1 t 79 4/2/2 3/2/2 3/2/3 2 b1209 62/F MS 14 t 83 4-5/1 4/0 4/2 blOO10 53/F MS 31 p 25 5/1 3/0 2/1 b40/d1501 1 57/F MS 13 p 72 3-4/1 3/1 4/2 blOO12 51/F MS 28 p 58 4-5/1 3/2 4/1 b7513 52/F MS 19 p 35 3/1-2 2/1-2 3/2 b75/tl214 54/F MS 18 t 99 4-5/1 4/1-2 4/1 b80/m30015 20/M tu T5 1/2 p 56 5/2 4/1 2/1 b45/t616 51/M MS 16 t 88 3/1 2/0 3/0 b60/t1617 46/F MS 10 p 55 5/2 4/2 4/1 b6518 19/M cer inf 1/2 t 72 5/2/2-3 4/1/2 4/2/3 5 b75/d75 blOO19 41/F MS 8 p 50 5/1 2/0 3/0 b30/t920 51/F MS 7 t 37 5/1 4/0 3/0 b90/d5O21 31/M tr c6 2 t 60 4/1 4/0 5/1 bl5022 41/M MS 14 t 61 5/2 4/1 4/0 b95/t1423 44/F MS 14 t 69 5/1 4/0 5/0 b80/tl424 38/M MS 10 t 47 4/1 4/1 5/1 blOO25 33/M tr T6 1 p 92 3/1 4/2 4/1 bl5026 49/F MS 23 p 54 4/1 3/1 3/1 b2027 60/F MS 27 p 62 5/1 4/1 4/0 b80/telOO
MS = Multiple sclerosis; HT = head trauma; tr T7 = spinal trauma at the level of the seventh thoracic vertebra; tu = tumour; cer inf = cerebral infarction; p =paraspasticity; t = tetraspasticity; ith b = treatment with intrathecal baclofen; drugs: b = baclofen, t = tizanidine, d = dantrolene, m = memantine, te = tetrazepam;Ashworth scale: 1 = no increase in tone, 2 = slight increase in tone when affected part is moved in flexion or extension, 3 = more pronounced increase in tone, butaffected part easily flexed, 4 = considerable increase in tone; passive movement difficult, 5 = affected part rigid in flexion or extension; spasm score: 0 = no spasms,1 = no spontaneous spasms, vigorous sensory or motor stimulation results in spasms, 2 = occasional spontaneous spasms <1/h, and easily induced spasms,3 = infrequent spontaneous spasms 1-10/h, 4 = spontaneous spasms >10/h; tendon reflex score: 0 = absent reflex, 1 = hyporeflexia, 2 = normal, 3 = mild hyper-reflexia, 4 = 3-4 clonus beats, 5 = >4 clonus beats.
in 10 others. A reduction was mainly possiblein those patients who did not have tetra-spasticity and who had already been receiv-ing intrathecal baclofen for several years.
PATIENTS WITH NO NEED FOR FURTHERTREATMENT WITH INTRATHECAL BACLOFENAfter stopping intrathecal baclofen infusion we
found a cessation or only a slight increase inspastic symptoms such as muscle tone andspasms in seven patients (1-7; table). Thesepatients had received intrathecal baclofenover a period of 60 (SD 15) months to treatsevere paraspasticity or tetraspasticity due tomultiple sclerosis (five) or spinal trauma(two). The mean dose of intrathecal baclofen
Figure 1 Time course ofintrathecal baclofen dosesfor patients for whom nofurther intrathecal baclofeninfusion was necessary;P = pump failure (batteryexhaustion); C = cathetermalfunction; bars indicateperiod during which thefilling was done by thegeneral practitioner, whodid not have a programmerto change the dose; arrowsindicate the time when webecame aware thatbaclofen could be stoppedor reduced in somepatients.
1000
800
600
U400
200IPain IP
0 20 340 5060 7080 90100Month
250
200
150
100 _50
2
0 20 40 60 809
10010 30 50 70 90
Month250
200
150
J0 20 40 60 80 10010 30 50 70 90
Month Month
160140120100 _80-40-203-2013 E: IP-
0 0 20 3040 5060 7080 9010010 30 50 70 90Month
250
200
150
100
50
06 P
_200 40 60__80 10C
10 30 50 70 90Month
1020 3040 5060 7080 901001030°507090nt
Month
V0)
169
0
on January 13, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.2.168 on 1 February 1996. D
ownloaded from
Dressnandt, Conrad
was 189 fug/day at the end of the first year oftreatment. These patients were followed up for11 (SD 6) months after stopping the infusion.Figure 1 shows the doses for individualpatients.
Patient 1 complained of a burning painwhich did not respond to carbamazepine oramitriptyline and therefore we tried, unsuc-cessfully, to reduce the pain by increasing theintrathecal baclofen dose. This was also thefirst patient in whom we noted a continuingsuppression of muscle tone and spasms afterthe pump had stopped. In one patient (3),who was tetraspastic, a moderate increase inmuscle tone reappeared in the arms and asmall increase in the legs after failure of thepump. The increased muscle tone with flexorspasms in the lower limbs, which had initiallyprompted intrathecal baclofen treatment, didnot reappear. In patient 5 the increase in thedose after 17 and 29 months was givenbecause the patient reported pain which didnot respond to other analgesics, and itresponded only poorly to the increased dose ofbaclofen. Patient 6, who became bedriddenafter the removal of a spinal meningeoma,could walk again three months after intrathe-cal baclofen infusion was started. A reductionof the dose after 18 months of treatment led toan increase in muscle tone and a worsening ofthe ambulatory capability and thus the dosewas increased again. Three years after begin-ning treatment with intrathecal baclofen agradual reduction to 60% of the initial dosewas initiated, after which the pump stoppedbecause of a dead battery. After eight months
without intrathecal baclofen and without anyother antispastic drugs the gait was as good asduring intrathecal baclofen treatment. Therewas no increase in muscle tone, merely thereappearance of a Babinski's sign.Two other patients (8, 18) are also dis-
cussed here. Although they are not specificallymembers of this group, they are of relevance toit. These patients, both with tetraspasticity,showed no appreciable increase in spasticity (2on the Ashworth scale) in the lower limbs afterstopping the infusion because of batteryexhaustion. In patient 8 treatment withintrathecal baclofen was started again toreduce the increased muscle tone in the upperlimbs, which had increased to 5 on theAshworth scale after intrathecal baclofen infu-sion was interrupted; it was reduced to 3 afterthe infusion was started again. The dose givenafter restarting treatment was lower thanbefore the treatment was stopped.
Patient 18 had only moderate spasticity(muscle tone in the arms 3-4, legs 2, spasmsin the legs 1) for six months without intrathecalbaclofen, but after severe pneumonia therewas an increase in spasticity more pronouncedin the upper limbs (muscle tone 5) than in thelower ones (muscle tone 3, spasms 4) so thatthe treatment was restarted (for these patientssee figs 2 and 3).
PATIENTS IN WHOM APPRECIABLE REDUCTIONOF DOSE WAS POSSIBLEWe reduced the dose of intrathecal baclofen ineight patients with multiple sclerosis, one withcerebral infarction, and one with a spinal
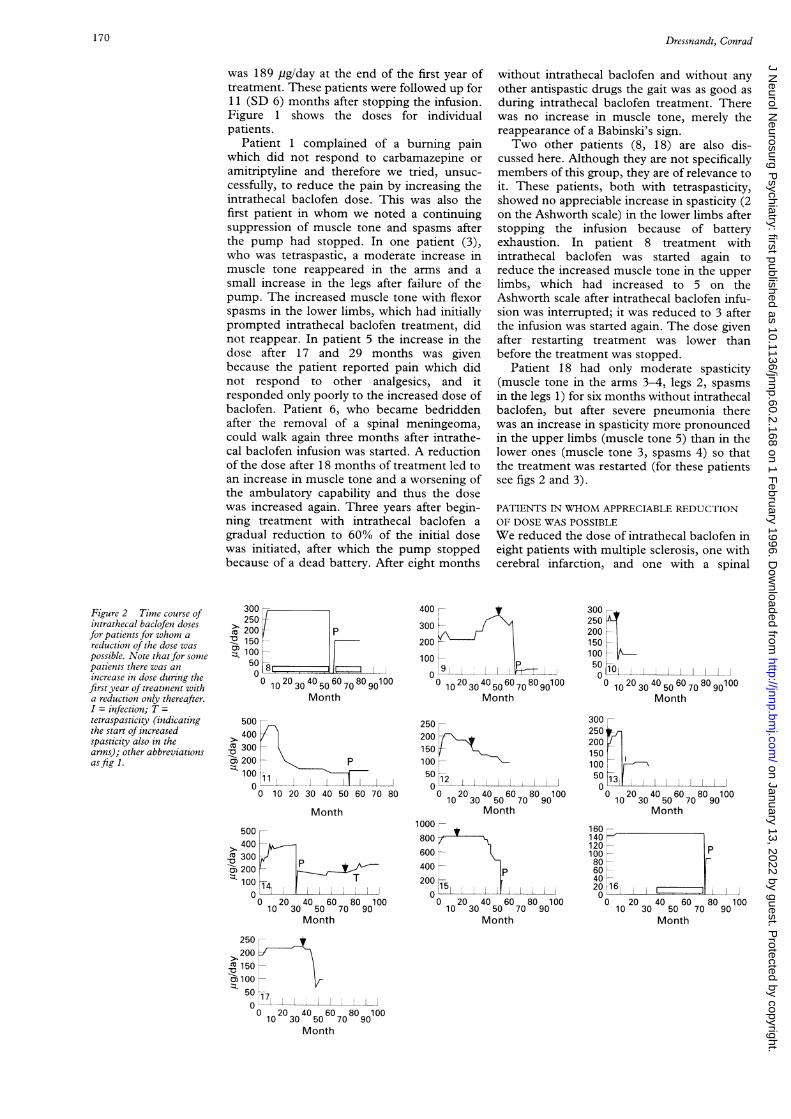
Figure 2 Time course ofintrathecal baclofen dosesfor patients for whom areduction of the dose waspossible. Note that for somepatients there was anincrease in dose during thefirst year of treatment witha reduction only thereafter.I = infection; T =tetraspasticity (indicatingthe start of increasedspasticity also in thearms); other abbreviationsasfig 1.
300250200C 200
O 15010050
Month
500
> 400CU 300 -
cS200 - P1001
00 10 20 30 40 50 60 70 80
Month
500
> 400 -U ~300= 200 -Z. 1001 T
00 20 40 60 80 100
10 30 50 70 90Month
250200150100 -
0
1212000 20 0 40 0 600 800 100
10 30 50 70 90Month
1000_
800600 -
400 - P200 r
00 20 40 60 80 100
10 30 50 70 90Month
300250200150100
50
10 30 50 70 90Month
160140 -
120 - P100
80 -
60 -
4020 !16100 20 40 60 80 100
10 30 50 70 90
Month
0 020 3040 5060 7080 90100
10 30 50 70 90
Month
o
170
on January 13, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.2.168 on 1 February 1996. D
ownloaded from
Lasting reduction of severe spasticity after ending chronic treatment with intrathecal baclofen
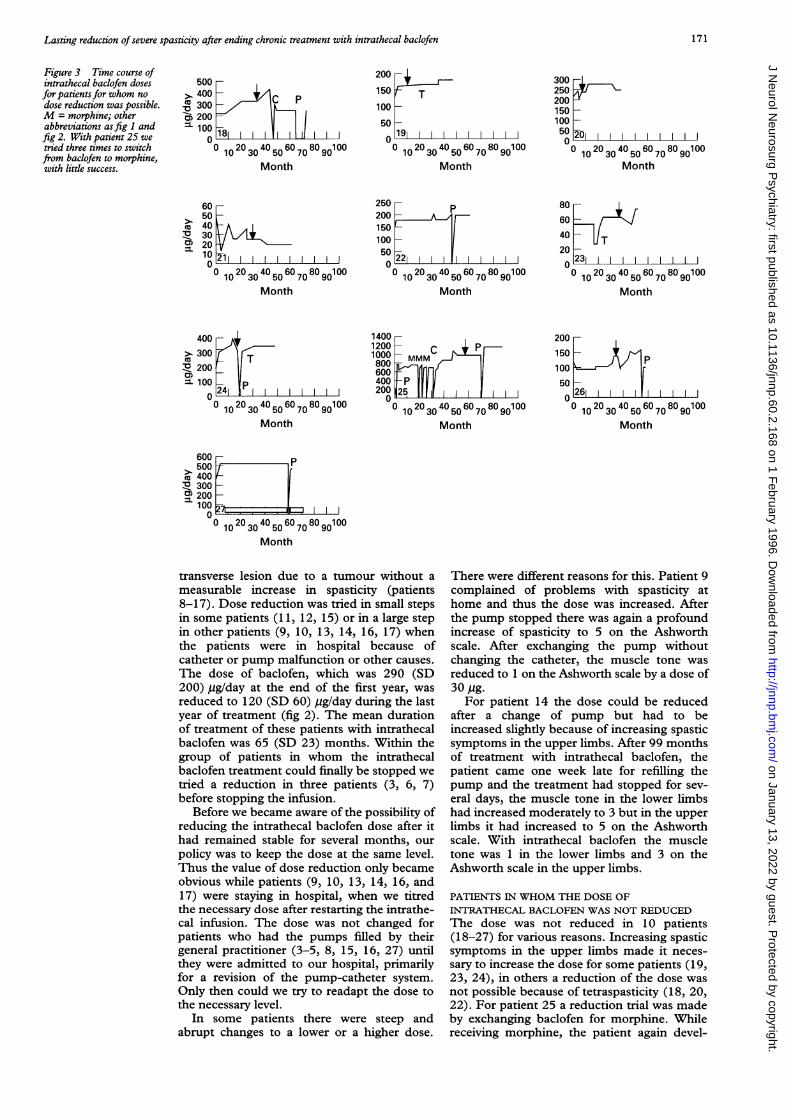
Figure 3 Time course ofintrathecal baclofen dosesfor patients for whom nodose reduction was possible.M = morphine; otherabbreviations asfig 1 andfig 2. With patient 25 wetried three times to switchfrom baclofen to morphine,with little success.
500>. 400
300cn 200=- 100
n
C P
1 i1
200
150 T10C5C
I-I r00 200 400 600 800 100
10 30 50 70 90Month
) r9i0 0 20 3040 5060 7080 9010010 30 50 70 90
Month
30025020015010050o 201 0
10 30 40 50 60 70 80 90100Month
°10 ° 30 ° 50 6 70 0 90Month
25020015010050
80604020A
Month
231
°10 ° 30 ° 50 70 90Month
400>. 300n 200CD=- 100
0
Month
14001200 C P1000800
600
400 P200 25 11
0
0 0 20 3040 5060 7080 90100°10230 5070n 90
Month
IP
10 20 30 40 50 60 70 80 90100Month
600 r>.
500
400n 300
200 -
100 -A I
0 1
° 10 230 450670890 °°
Month
transverse lesion due to a tumour without a
measurable increase in spasticity (patients8-17). Dose reduction was tried in small stepsin some patients (11, 12, 15) or in a large stepin other patients (9, 10, 13, 14, 16, 17) whenthe patients were in hospital because ofcatheter or pump malfunction or other causes.
The dose of baclofen, which was 290 (SD200) ,ug/day at the end of the first year, was
reduced to 120 (SD 60) ,g/day during the lastyear of treatment (fig 2). The mean durationof treatment of these patients with intrathecalbaclofen was 65 (SD 23) months. Within thegroup of patients in whom the intrathecalbaclofen treatment could finally be stopped wetried a reduction in three patients (3, 6, 7)before stopping the infusion.
Before we became aware of the possibility ofreducing the intrathecal baclofen dose after ithad remained stable for several months, our
policy was to keep the dose at the same level.Thus the value of dose reduction only becameobvious while patients (9, 10, 13, 14, 16, and17) were staying in hospital, when we titredthe necessary dose after restarting the intrathe-cal infusion. The dose was not changed forpatients who had the pumps filled by theirgeneral practitioner (3-5, 8, 15, 16, 27) untilthey were admitted to our hospital, primarilyfor a revision of the pump-catheter system.Only then could we try to readapt the dose tothe necessary level.
In some patients there were steep andabrupt changes to a lower or a higher dose.
There were different reasons for this. Patient 9complained of problems with spasticity athome and thus the dose was increased. Afterthe pump stopped there was again a profoundincrease of spasticity to 5 on the Ashworthscale. After exchanging the pump withoutchanging the catheter, the muscle tone was
reduced to 1 on the Ashworth scale by a dose of30 pg.
For patient 14 the dose could be reducedafter a change of pump but had to beincreased slightly because of increasing spasticsymptoms in the upper limbs. After 99 monthsof treatment with intrathecal baclofen, thepatient came one week late for refilling thepump and the treatment had stopped for sev-eral days, the muscle tone in the lower limbshad increased moderately to 3 but in the upperlimbs it had increased to 5 on the Ashworthscale. With intrathecal baclofen the muscletone was 1 in the lower limbs and 3 on theAshworth scale in the upper limbs.
PATIENTS IN WHOM THE DOSE OFINTRATHECAL BACLOFEN WAS NOT REDUCEDThe dose was not reduced in 10 patients(18-27) for various reasons. Increasing spasticsymptoms in the upper limbs made it neces-sary to increase the dose for some patients (19,23, 24), in others a reduction of the dose wasnot possible because of tetraspasticity (18, 20,22). For patient 25 a reduction trial was madeby exchanging baclofen for morphine. Whilereceiving morphine, the patient again devel-
6050
c 40n 30m 20
10A
171
u v
uv
on January 13, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.2.168 on 1 February 1996. D
ownloaded from

Dressnandt, Conrad
oped severe spasms within a week so that thetreatment with baclofen was restarted. Figure3 shows that no appreciable dose reductionwas possible.
As shown in figs 1, 2, and 3 the intrathecalbaclofen dose had to be increased in manypatients during the first year of treatment butit tended to remain stable thereafter. Duringthe first two weeks after implantation of thepump the initial dose was titred individually tothat level at which there was a reduction ofmuscle tone to 1-2 on the Ashworth scale inthe lower limbs and/or the spasms werereduced to 0-1 on the spasm scale. When thepatients came to have the pump refilled itdepended on the clinical examination (muscletone, spasms, tendon reflexes) whether thedose of intrathecal baclofen remained thesame or whether it had to be increased orreduced.
DiscussionTo our knowledge, a lasting reduction of spas-ticity after ending chronic intrathecal infusionof baclofen has not been reported up to now.Obviously there is great individual variabilityin the intrathecal baclofen dose which is nec-essary for reducing spasticity at the beginningof the treatment (for example, 9, 15, 23).Usually a dose is chosen which reduces themuscle tone enough but does not completelysuppress the patellar reflex. This regime ischosen to reduce the risk of venous thrombosisdue to flaccid paresis. The great interindivid-ual variability of an intrathecal baclofen dosemakes it impossible to deduce from the patientgroup if there is a specific dose which will leadto lasting suppression of spasticity. Neither isit clear whether the infusion of higher thannecessary doses will lead to the observed effectfaster. It is important to note that the lastingreduction of spasticity or a reduced need forintrathecal baclofen to suppress spasticity wasmore pronounced in the lower than in theupper limbs in patients with tetraspasticity.
Possible mechanisms for this differentialeffect could be structural changes at the caudalspinal cord due to mechanical or reactiveinflammatory lesions caused by the intraspinalcatheter. However, some of our patients whohad only an incomplete transsection could stillmove their legs (1, 15) or even walk (6). Thusthe hypothesis that mechanical or reactiveinflammatory lesions are the primary causedoes not explain the findings in all patients.
For patients with multiple sclerosis it isassumed that new inflammatory lesions withinthe spinal cord lead to a reduction of spinalexcitatory circuits and cause spinal spasticsymptoms. However, some of those patientswho were able to stop treatment (5, 6) or whoshowed an obviously more pronounced effectin the lower limbs than in the upper limbs (8,18) did not have multiple sclerosis. Thus someother factors must be involved.
Alhough there was obviously muscle atro-phy in some patients due to inactivity this can-not be the main reason for the sustainedsuppression of spastic symptoms, because one
of the patients (6) could walk, others (1, 15)could voluntarily bend their knees, and inmost patients the tendon reflexes reappeared.
Another explanation might be a toxic effectof baclofen on the spinal cord neurons. Thiswould also explain why lasting suppression ofspastic symptoms was more pronounced in thelower limbs than in the upper limbs, reflectinga correlation with the concentration ofbaclofen. The concentration of baclofen in theCSF is four times higher at the lumbothoraciclevel than at the cervical level when it is given atthe lumbothoracic level."I -' But as some ofour patients could walk again without showingany deterioration after having receivedintrathecal baclofen for years, it is unlikely thata toxic effect alone is the reason for the sus-tained suppression of spasticity. Also, toxicitytests in animals did not show any toxic sideeffects of intrathecal baclofen."' 6
Possibly structural changes are induced bythe prolonged influence of highly concentratedbaclofen at the spinal level. These may be theresult of altered intracellular mechanisms dueto long term alterations of second messengerdependent regulators. Baclofen binds to presy-naptic and postsynaptic GABA-B receptors'7and down regulates Ca2+ influx by a protein Gcoupled change of Ca2+ channels.'8 20 Further-more it is known that protein G dependentsecond messengers and Ca2+ can regulate geneexpression within the nucleus,2' and hencelong term adaptive changes could occur. Theability of baclofen to cause long lasting adap-tive morphological and, hence, physiologicalchanges in spinal neurons has been shown.After repetitive pain stimuli early gene proteinsfos, jun, and krox24 are expressed in spinalneurons. These gene expressions can be modu-lated by morphine, baclofen, and NMDA-antagonists.22 25 When morphine or baclofenwas given before noxious stimuli, an activationof an intracellular cascade activating thenucleus and leading to the expression ofimmediate early genes could be prevented.A dose dependent effect can be deduced
from the finding that the suppression of spas-ticity was stronger and more lasting in thelower limbs than in the upper limbs of twopatients with tetraspasticity. The concentra-tion of baclofen infused at the lumbothoraciclevel decreases in a cranial direction (see ear-lier).
Patient 18 had a sustained suppression ofspastic symptoms for six months after thepump had stopped, but there was again a pro-found increase in muscle tone in the lower andupper limbs after a severe infection. Thiscould indicate that the mechanisms which areresponsible for spastic symptoms remaineddown regulated during the period when therewas no incease in spasticity after the pump hadstopped but then were upregulated again afteran infection. Thus a reversability of the longlasting suppression of spasticity after stoppingintrathecal baclofen infusion has to be consid-ered. Whether such a change will also occur inthe other seven patients who still do not needintrathecal baclofen remains to be seen.By contrast with a possible reduction after
172
on January 13, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.2.168 on 1 February 1996. D
ownloaded from

Lasting reduction of severe spasticity after ending chronic treatment with intrathecal baclofen
several years of intrathecal baclofen treatment,it is obviously necessary to increase the doseduring the first year of treatment. This findinghas also been reported by other authors.356The reason for this is not clear. After begin-ning treatment with intrathecal baclofen thereis a down regulation of GABA-B receptors inthe spinal cord at least during the first sevendays in rats.26 No studies have investigated thelong term effects at the cellular level.Electrophysiological investigations prove thatbaclofen binds at lower concentrations to thepresynaptic GABA-B receptor in the substan-tia gelatinosa than to the postsynaptic GABA-Breceptor at a-motoneurons.27 2X It can only bespeculated whether the down regulation of theGABA-B receptor in the substantia gelatinosameans that it is necessary to increase the doseof baclofen; its binding at the postsynapticGABA-B receptor on a-motoneurons is thusenhanced and the excitability of the a-motoneurons is reduced directly.25
In conclusion, from a group of 27 patientswho received intrathecal baclofen for morethan two years, seven patients had sustainedsuppression of spastic symptoms such asincreased muscle tone and spasms after dis-continuing intrathecal baclofen. The dose ofintrathecal baclofen could be reduced consid-erably in 10 other patients after a treatmentperiod of more than two years. These findingsare possibly explained by long term baclofeninduced morphological changes in spinal cordneurons. It could well be that earlier treatmentor the use of a higher daily dose of intrathecalbaclofen would yield a better and longer last-ing suppression of spasticity. Perhaps a pre-emptive, early treatment with baclofen couldalso prevent or decrease the development ofspastic symptoms such as spasms andincreased muscle tone after spinal cord lesionsor a sudden paraparesis or monoparesis due tomyelitis in an acute bout of multiple sclerosis.
Presently, we recommend trying to reducethe dose of intrathecal baclofen after a con-stant effective dose has been reached, at leastonce a year. Treatment with intrathecalbaclofen, with all its possible complications,can be terminated in at least some patients.
1 Penn RD, Kroin JS. Intrathecal baclofen alleviates spinalcord spasticity [letter]. Lancet 1984;i:1078.
2 Ochs G, Struppler A, Meyerson BA, et al. Intrathecalbaclofen for long term treatment of spasticity: a multi-centre study. J Neurol Neurosurg Psychiatry 1989;52:933-9.
3 Loubser PG, Narayan RK, Sandin KJ, Donovan WH,Russell KID. Continuous infusion of intrathecalbaclofen: long-term effects on spasticity in spinal cordinjury. Paraplegia 1991;29:48-64.
4 Penn RD. Intrathecal baclofen for spasticity of spinal ori-gin: seven years of experience. J Neurosurg 1992;77:236-40.
5 Meythaler JM, Steers WD, Tuel SM, Cross LL, HaworthCS. Continuous intrathecal baclofen in spinal cord spas-ticity. A prospective study. Am .7 Phys Med Rehabil 1992;71:321-7.
6 Coffey JR, Cahill D, Steers W, et al. Intrathecal baclofenfor intractable spasticity of spinal origin: results of a long-term multicenter study. .7 Neurosurg 1993;78:226-32.
7 Zierski J, Muller H, Dralle D, Wurdinger T. Implantedpump systems for treatment of spasticity. Acta NeurochirSuppl (Wein) 1988;43:94-9.
8 Dressnandt J, Konstanzer A, Conrad B. Reversal of spastic-ity after longterm treatment with intrathecal baclofen. 7Neurol 1992;239S3:37
9 Ashworth B. Preliminary trial of carisoprodol in multiplesclerosis. Practitioner 1964;192:540-2.
10 Lee KC, Carson L, Kinnin E, Patterson V. The Ashworthscale: a reliable and reproducible method of measuringspasticity. Y7 Neurol Rehabil 1989;3:205-9.
11 Kroin JS, Penn RD. Implantable pumps to deliver drugsdirectly into the CNS. In: Neuwelt EA, ed. Implications ofthe blood-brain barrier and its manipulation. Vol 2. Clinicalaspects. New York: Plenum Press, 1989:601-16.
12 Sallerin-Caute B, Lazorthes Y, Monsarrat B, Cros J,Bastide R. CSF baclofen levels after intrathecal adminis-tration in severe spasticity. EurJ7 Clin Pharmacol 1991 ;40:363-5.
13 Kroin JS, Ali A, York M, Penn RD. The distribution ofmedication along the spinal canal after chronic intrathe-cal administration. Neurosurgery 1993;33:266.
14 Wilson PR, Yaksh TL. Baclofen is antinociceptive in thespinal intrathecal space of animals. Eur _7 Pharmacol1978;51:323-30.
15 Yaksh TL, Reddy R. Studies in the primate on the anal-gesic effects with the intrathecal actions of opiates, adren-ergic agonists and baclofen. Anesthesiology 1981 ;54:451-67.
16 Kroin JS, Penn RD, Bessinger RL, Arzbaecher RC.Reduced spinal reflexes following intrathecal baclofen inthe rabbit. Exp Brain Res 1984;54:191-4.
17 Bowery NG, Hill DR, Hudson AL, Doble A, MiddlemissDN, Shaw J, Turnbull M. (-)-Baclofen decreases neuro-transmitter release in the mammalian CNS by action at anovel GABA receptor. Nature 1980;283:92-4.
18 Bowery NG, Pratt GD. GABAB receptors as targets fordrug action. Arzneimittelforschung 1992;42:215-23.
19 Dolphin AC, Scott RH. Inhibition of calcium currents incultured rat dorsal root ganglion neurones by (-)-baclofen. BrJ Pharmacol 1986;88:213-20.
20 Kangrga I, Jiang M, Randic M. Actions of (-)-baclofen onrat dorsal horn neurons. Brain Res 1991;562:265-75.
21 Zimmermann H. Synaptic transmission. Cellular and molecularbasis. New York: Oxford University Press, 1993:94-104.
22 Castro-Lopes JM, Tavares I, Tolle TR, Coito A, CoimbraA. Increase in GABAergic cells and GABA levels in thespinal cord in unilateral inflammation of the hindlimb inthe rat. Eur-fNeurosci 1992;4:296-301.
23 Castro-Lopes JM, Tavares I, Tolle TR, Coimbra A.Carrageenan-induced inflammation of the hind foot pro-vokes a rise of GABA-immunoreactive cells in rat spinalcord that is prevented by peripheral neurectomy orneonatal capsaicin treatment. Pain 1994;56:193-201.
24 Tolle TR, Herdegen T, Schadrack J, Bravo R,Zimmermann M, Zieglgansberger W. Application ofmorphine prior to noxious stimulation differentially mod-ulates expression of Fos, Jun and Krox-24 proteins in ratspinal cord neurons. Neuroscience 1994;58:305-21.
25 Tolle TR, Schadrack J, Castro-Lopes JM, Conrad B,Ziegelgansberger W. Baclofen reduces immediate-earlygene expression in the rat spinal cord following noxiousthermal and inflammatory stimulation. Y Neurol 1995;242S2:45.
26 Kroin JS, Bianchi GD, Penn RD. Intrathecal baclofendown-regulates GABAB receptors in the rat substantiagelatinosa. Y Neurosurg 1993;79:544-9.
27 Allerton CA, Boden PR, Hill RG. Actions of GABAB ago-nist, (-)-baclofen, on neurones in deep dorsal horn of therat spinal cord in vitro. BrjPharmacol 1989;96,29-38.
28 Kangrga I, Jiang M, Randic M. Actions of (-)-baclofen onrat dorsal horn neurons. Brain Res 1991;562,265-75.
29 Dressnandt J, Auer C, Conrad B. Influence of baclofenupon the alpha-motoneuron in spasticity by means of F-wave analysis. Muscle Nerve 1995;18:103-7.
173
on January 13, 2022 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.2.168 on 1 February 1996. D
ownloaded from