latent tb infection in the who european region · latent tb infection in the who european region...
TRANSCRIPT

Latent TB Infection in the WHO European Region
and recommendations on LTBI’s M&E framework
18th Wolfheze workshops / 15th NTP managers meeting,
31 May – 02 June 2017
Dr Andrei DADU
Technical officer,
Joint TB, HIV/AIDS and Hepatitis Programme

Why Do We Have Drug Resistance on raise?• Inadequate treatment
– Incorrect regimen (lack of drugs or knowledge)
– Poor adherence
Treatment failure / relapse with drug resistant TB
Transmission of drug resistant TB
• It is far easier to prevent TB in those infected without disease than to treat a full blown case of drug resistant TB

Dye C et al., Prospects for Tuberculosis Elimination. Ann Rev Public Health 2013. 34:271-86
Scale-up of programmatic management of LTBI is critical in order to end
the global TB epidemic as stated in the WHO’s End TB Strategy.
LTBI management contributes to the End
TB Strategy targets
• Mitigation of risk e.g. HIV prevention/ART
or prevention of infection by vaccine or
infection control have limited impact on the
trajectory of drop in TB incidence
• and so is the case with treatment of active
TB alone
• However identification and treatment of
latent infection in combination with active
TB treatment can potentially accelerates
reduction in TB incidence and achieve the
End TB Strategy target
Incidence of TB, projections to 2050

GLOBAL TB PROGRAMME
WHO LTBI Guidelines
Guidelines for intensified tuberculosis case-finding and isoniazid preventive
therapy for people living with HIV in resource-constrained settings
WHO guidelines 2011 (to be updated 2015)
Recommendations for investigating contacts of persons with infectious
tuberculosis in low- and middle-income countries
WHO guidelines 2012
Guidelines on the management of latent tuberculosis infection (high and upper
middle-income countries with TB incidence <100/100, 000)
WHO guidelines 2014
http://whqlibdoc.who.int/publications/2011/9789241500708_eng.pdf
http://apps.who.int/iris/bitstream/10665/77741/1/9789241504492_eng.pdf
http://apps.who.int/iris/bitstream/10665/136471/1/9789241548908_eng.pdf

Revised LTBI estimates
Published: October 25, 2016
1 MDR is found in each 4 TB in Europe
L MDR-TB I *:
All ages = 31 millions
0-14 years = 610 thousands
0-4 years = 260 thousands
* Provisional estimates / unpublished

120,000Estimated of all new RR/MDR-TB emerging
74,000Estimated RR/MDR in all notified TB
47,000Detected RR/MDR cases among all TB notified cases
MDR-TB and their contacts
260,000
Contacts of 0-4 years oldRR/MDR-TB
148,000
94,000Modified from JA Seddon et al, Lancet 2012

TB Incidence>=100 or lower/lower-middle income
TB incidence<100 and upper/upper-middle income
TB >=100 or lower/lower-middle income
TB <100 and upper/upper-middle income
TB Incidence>=100 or lower/lower-middle income
TB incidence<100 and upper/upper-middle income
Target countries for LTBI packages

A snapshot of the WHO’s key recommendations

E. LTBI PROGRAMMATIC MANAGEMENT AND VACCINATION AGAINST TB
PILAR 1> INTEGRATED, PATIENT CENTRED CARE AND PREVENTION

LTBI in the TB Action Plan in EUR 2016-2020)TB Action Plan in EUR 2016-2020):
• MS to adopt and adapt their national policies to align with the most up-to-date WHO recommendations
on diagnosis and treatment of latent TB infection for high-risk populations.
• MS to ensure that WHO policy recommendations on BCG vaccination for infants are implemented and
BCG revaccination is discontinued.
• MS to ensure that people accessing harm-reduction services for drug misuse will be provided the option
of TB preventive therapy.

LTBI treatment enrollment rate among PLHIV (%)
in 2015: 36% IPT coverage
among those newly enrolled into
HIV care
vs.
in 2011 4.8% as a baseline
70%
50%
40% 39%
33%
19%14%
10% 9%
3%0%
36% 36%
90%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%

LTBI in Global TB data collection form (EUR section only)
Country X, 2015 dataTotal pop. = 3 mln0-4 years pop. = 200 000Contacts, estimates = 4 000Actually screened = unkLTBI eligible = unkIPT enrolment = unk
National policy is available but rarely implemented and not reported
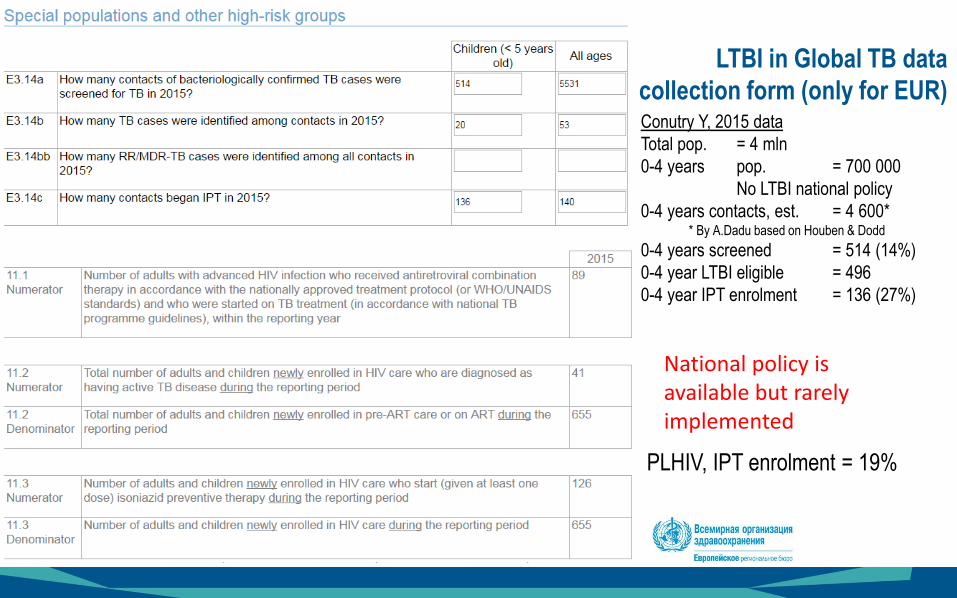
LTBI in Global TB data
collection form (only for EUR)Conutry Y, 2015 data
Total pop. = 4 mln
0-4 years pop. = 700 000
No LTBI national policy
0-4 years contacts, est. = 4 600** By A.Dadu based on Houben & Dodd
0-4 years screened = 514 (14%)
0-4 year LTBI eligible = 496
0-4 year IPT enrolment = 136 (27%)
PLHIV, IPT enrolment = 19%
National policy is available but rarely implemented
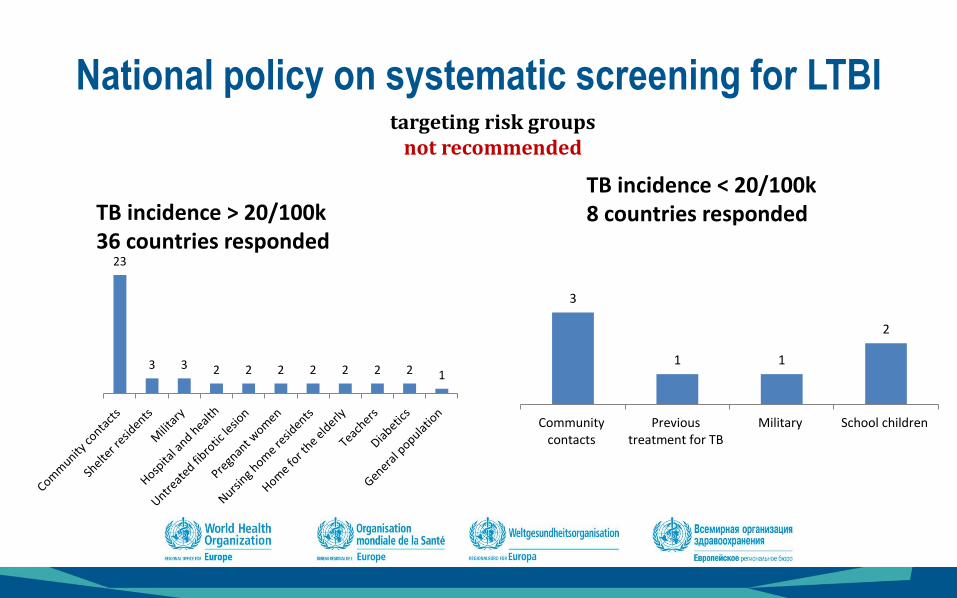
targeting risk groups not recommended
23
3 3 2 2 2 2 2 2 2 1
National policy on systematic screening for LTBI
3
1 1
2
Communitycontacts
Previoustreatment for TB
Military School children
TB incidence > 20/100k 36 countries responded
TB incidence < 20/100k 8 countries responded

Challenges: policy implementation and practices
• Weak LTBI [surveillance] and [response monitoring] in
countries and therefore poor data at regional level;
• Poor cascade analysis understanding contacts children
(weak cascade analysis)
• Estimates/Projections modelling and Drugs forecasting
• HCW commitment/engagement due to high overload on
tasks and responsibilities
• Country health system that prevent the LTBI rolleout
• Challenges in LTBI resources mobilization
• Low enrolment rate in to the LTBI treatment
among PLHIV (the beginning of the
countrywide implementation)
• LTBI management miss-practices at country
level (screening/detection);
• High RR/MDR prevalence among TB cases in
the EECA countries: 9 out of top 10 global high
MDR-TB burden countries;
• Refugees and other categories of migrants
influx across the boarders;

TAG 2017 recommendations
LTBI management
• Adapt and disseminate criteria for prioritization of at-risk population among those for whom systematic LTBI testing and treatment is recommended, in agreement with the 2014 WHO policy document;
• Create an implementation guide for contact tracing, screening and management of contacts. Evaluate the opportunity for recommending active search of the contacts (children to be prioritized);
• Analyse bottlenecks in implementation of LTBI testing and treatment among PLHIV and children under the age of 5 who are household contacts, and propose solutions;
• Develop a framework for recording and reporting of LTBI data that allows measurements of contact and LTBI indicators, using WHO guidance document on LTBI M&E with reference to both global and national core indicators;
• Develop a regional position paper/expert opinion document on the use of Interferon Gamma Release Assays (IGRA) in LTBI detection;
• Develop a regional position paper/expert opinion document on rifapentine-containing regimens and assist Member States and partners facilitate the registration of the drug with European Medicine Agency and/or country drug regulatory authorities ;
• Promote research and assessment on LTBI.