laurie fouser, md pediatric nephrology swedish pediatric
TRANSCRIPT

Hematuria and Proteinuria in the Pediatric Patient
Laurie Fouser, MD Pediatric Nephrology
Swedish Pediatric Specialty Care

Hematuria in the Child
• Definition • ³ 1+ on dipstick on three urines over three weeks • 5 RBCs/hpf on three fresh urines over three weeks
• Prevalence • 4-6% for microscopic hematuria on a single
specimen in school age children • 0.3-0.5% on repeated specimens

Sources of Hematuria
• Glomerular or “Upper Tract” – Dysmorphic RBCs and RBC casts – Tea or cola colored urine – Proteinuria, WBC casts, renal tubular cells
• Non-Glomerular or “Lower Tract” – RBCs have normal morphology – Clots/ Bright red or pink urine
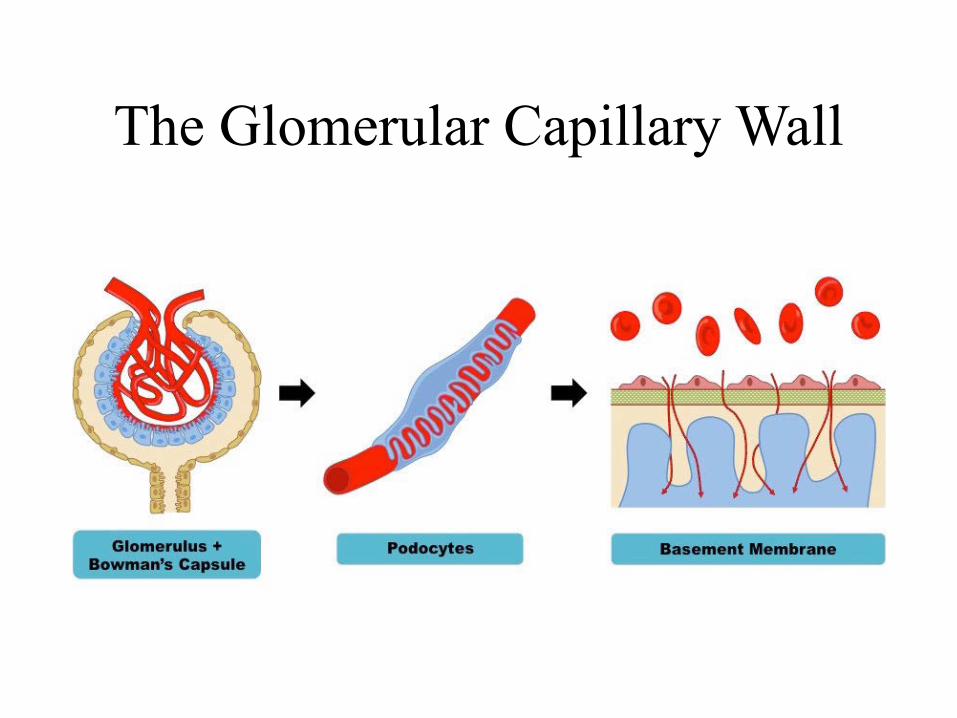
The Glomerular Capillary Wall

The Glomerular Capillary Wall

Glomerular Causes of Hematuria
• Benign or self-limiting – Benign Familial Hematuria – Exercise-Induced Hematuria – Fever-Induced Hematuria

Glomerular Causes of Hematuria
• Acute Glomerular Disease – Poststreptococcal/ Postinfectious – Henoch-Schönlein Purpura – Sickle Cell Disease – Hemolytic Uremic Syndrome

Glomerular Causes of Hematuria
• Chronic Glomerular Disease – IgA Nephropathy – Henoch-Schönlein Purpura or other Vasculitis – Alport Syndrome – SLE or other Collagen Vascular Disease – Proliferative Glomerulonephritis

Non-Glomerular Hematuria
• Extra-Renal • UTI • Benign urethralgia +/- meatal stenosis • Calculus • Vesicoureteral Reflux, Hydronephrosis • Foreign body • Rhabdomyosarcoma • AVM • Coagulation disorder

Non-Glomerular Hematuria
• Intra-Renal • Hypercalciuria • Polycystic Kidney Disease • Reflux Nephropathy with Renal Dysplasia • Sickle Cell Crisis • Renal Vein Thrombosis • Renal Hemangioma • Tumor or Leukemia • Nutcracker syndrome/Loin Pain Hematuria

Evaluation – Phase I
• Complete History – Duration, color, discrete clots vs diffuse? – In males, change during stream? – Pain or painless (dysuria, abdominal, flank) – Recent or current infection? – Rashes, joint, or GI symptoms?
Evaluation – Phase I
• Complete Physical – Blood pressure – Volume status (“dry or wet”, rales, gallop) – Edema (periorbital, pretibial, ascites) – Rash

Urinalysis with Microscopy

Evaluation - Phase I
• Complete H&P • Urinalysis with microscopy • Urine culture • Urine calcium: urine creatinine ratio • CBC with platelets (+/-Sickle prep), BUN,
Creatinine, albumin, C3 • Ultrasound of kidneys and bladder • Urine dipsticks on parents and siblings

Evaluation - Phase II
• C3, C4, ANA, Hepatitis B & C • Streptozyme • BUN, creatinine, electrolytes, albumin,
calcium, phosphorus • Hearing evaluation • VCUG or CT

Evaluation - Phase III
• Other laboratory
• Renal biopsy
• Cystoscopy

When to Refer • Family history of kidney disease • Gross hematuria or clots • RBC casts • Proteinuria ³ 1+ • Elevated creatinine or BUN • Hypertension • Imaging abnormalities • Parental anxiety

Proteinuria in the Child

Proteinuria
• Definition – 1+ or more on dipstick – Urine protein:creatinine
• >0.2 mg/mg if over 2 yrs • >0.6 mg/mg ages 6 months-
2yrs • Nephrotic range is >2 mg/mg
– Timed urine protein excretion
• >96 mg/m2/24 hrs • >150 mg/1.73m2/24hrs • Nephrotic range is >3
gm/1.73m2/24 hrs

Causes of Proteinuria
• Physiologic or Intermittent • Postural or Orthostatic • Pathologic
– Glomerular – Tubular
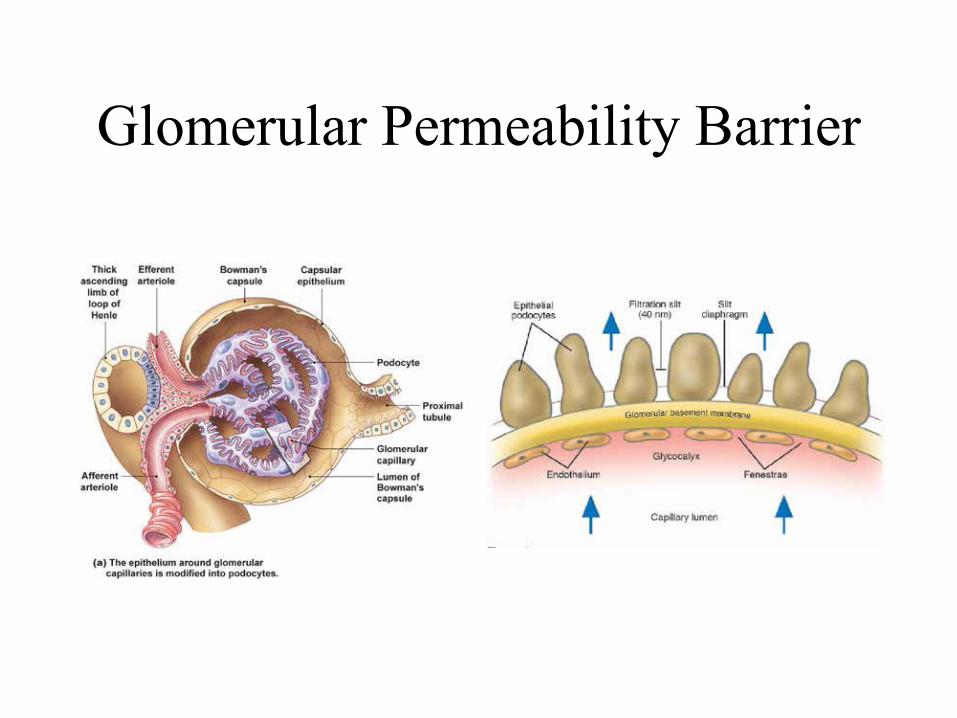
Glomerular Permeability Barrier

Physiologic or Intermittent Proteinuria
• Mechanism is change in glomerular capillary wall permeability – Increased luminal
hydrostatic pressure – Increased blood
flow
• Causes – Acute elevations in BP
or intraglomerular volume
– Catecholamines/stress – Metabolism

Physiologic or Intermittent Proteinuria
• Clinical Settings – Fever – Physical stress (march
proteinuria) – Pregnancy – Immediately post op
unilateral nephrectomy – Acute hypertension or
CHF
• Duration – Transient (hours-
days) – Self-remitting – No need for referral

Postural or Orthostatic Proteinuria
• Two patterns – Fixed, reproducible (15-20%) – Transient (75-80%)
• Accounts for 60% of children and 75% of adolescents with proteinuria
• Incidence – 2-5% of adolescents • MUST DISTINGUISH FROM PATHOLOGIC
PROTEINURIA WITH A POSTURAL COMPONENT
Postural or Orthostatic Proteinuria
• Evaluation:
– Blood pressure, edema should not be present, UA/UC
– First am void for urine protein:creatinine (patient must be sure to go to bed with empty bladder)
• If <0.2 mg/mg, likely orthostatic – Normal renal function panel and renal
ultrasound

Postural or Orthostatic Proteinuria
• Protein in 24 hr fractional urine collection – Supine: <50-75 mg for 8-12 hrs – Upright: 200-1000 mg
• Etiology – Variant of normal permeability or renal vein
kink/entrapment • Long term follow-up
– 10-20 years: resolution or benign outcome

Pathologic Proteinuria
Pathologic Proteinuria
• Fixed proteinuria >150-300 mg/24hrs or
• First am void has urine protein:creatinine >0.2 or
• Edema
– PE (edema, rash, volume), Ht, Wt, BP
– UA (?hematuria), 24 hr urine protein &creatinine
– BUN, creatinine, albumin, lytes, calcium, phosphorus, lipids, C3, C4
– CBC

Causes of Pathologic Proteinuria
• Nephrotic syndrome – Minimal change, FSGS, membranous
• Glomerulonephritis – Henoch-Schonlein purpura, IgA nephropathy,
Alport nephritis • Tubular Proteinuria
– Dent’s disease, Fanconi syndrome

When to Refer
• Parental anxiety or confirmation of orthostatic proteinuria
• Any pathologic proteinuria • ASAP for edema/anasarca,
hypoalbuminemia, hypertension, associated hematuria, elevated creatinine