le strategie per migliorare l’aderenza alla terapia · mario polverino polo pneumologico ......
TRANSCRIPT

Le strategie per migliorare l’aderenza alla terapia
Mario Polverino
Polo Pneumologico Provinciale
Centro Regionale Ad Alta Specializzazione
PO «M. Scarlato», SCAFATI (SA)Scuole di Specializzazione in Pneumologia, Farmacologia

OSMED 2015 report In Italy
Patients with aderence to therapy for pulmonary obstruction
13,6%

C.E. Koop
«The drugs do not work in patients who do not
take them»
Osterberg L et al. N Engl J Med 2005

Cause mancata aderenza
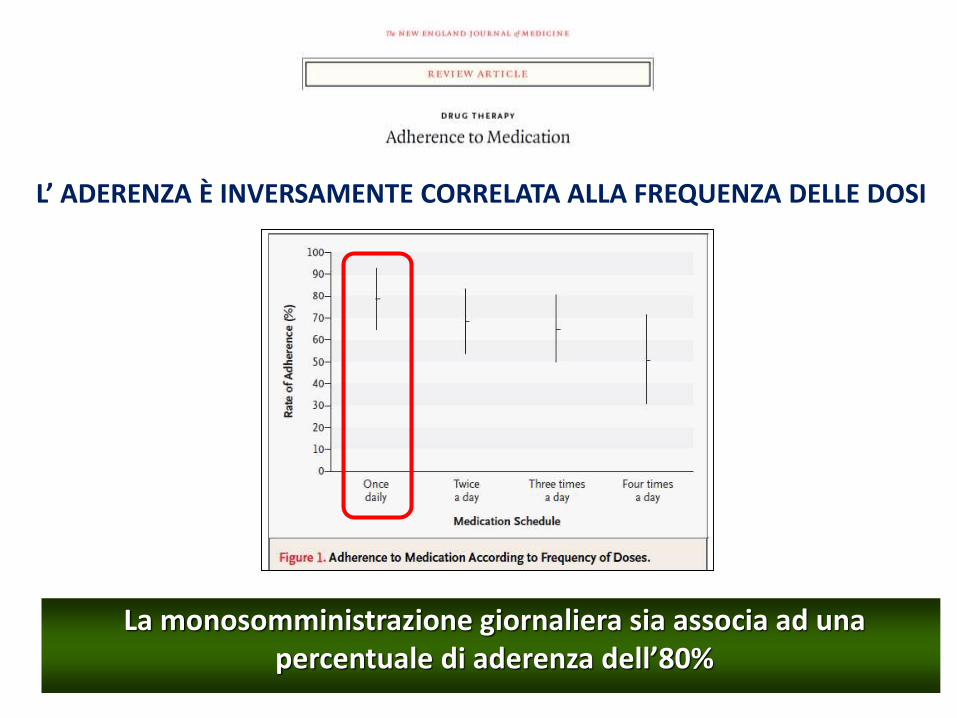
L’ ADERENZA È INVERSAMENTE CORRELATA ALLA FREQUENZA DELLE DOSI
La monosomministrazione giornaliera sia associa ad unapercentuale di aderenza dell’80%
17/11/2016 6
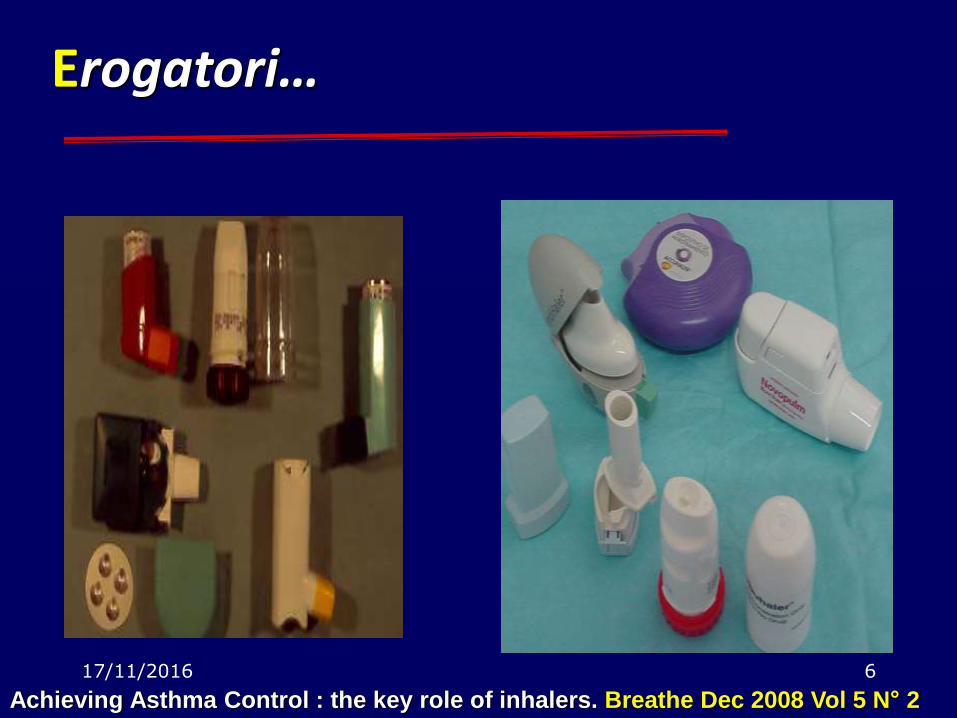
Achieving Asthma Control : the key role of inhalers. Breathe Dec 2008 Vol 5 N° 2
Erogatori…

CCC
Smith IJ, et al. J Aerosol Med Pulm Drug Deliv. 2010; 23(Suppl 2):S25–37
Competence The ability to use a device correctly
• Simpler devices may enable more patients to use them correctly
• MDIs are not simple devices to use
Contrivance Knowing what to do but doing something else
• e.g.: the patient who shows good technique with a spacer and MDI in the clinic, but then does not use the spacer when at home
Compliance Taking medication as recommended
• Patients need to understand
‒ the rationale behind the medication
‒ the consequences of not taking the medication as intended
‒ the consequences of poor inhaler technique
‒ the long-term benefits of taking the medication
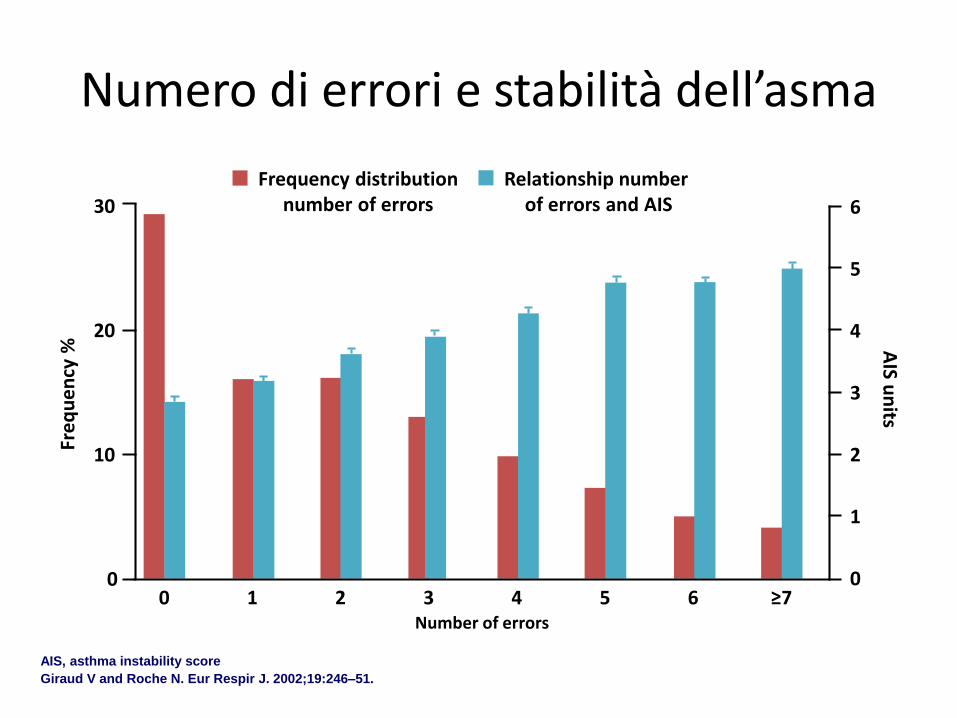
Frequency distributionnumber of errors
Relationship number of errors and AIS
Number of errors
0 1 2 3 4 5 6 ≥7
Fre
qu
en
cy %
0
10
20
30
0
1
2
3
4
5
6
AIS u
nits
Numero di errori e stabilità dell’asma
AIS, asthma instability score
Giraud V and Roche N. Eur Respir J. 2002;19:246–51.

DEVICES

Strangely… …any sponsored study concludes that its device is the best

Every mother likes her own beetle

No significant differences between inhaler devices with regards to efficacy and safety, 12
Every mother likes his beetle

Brocklebank et al. Health Technol Assess 2001;5(26)

Brocklebank et al. Health Technol Assess 2001;5(26)

Brocklebank et al. Health Technol Assess 2001;5(26)

Brocklebank et al. Health Technol Assess 2001;5(26)

Brocklebank et al. Health Technol Assess 2001;5(26)
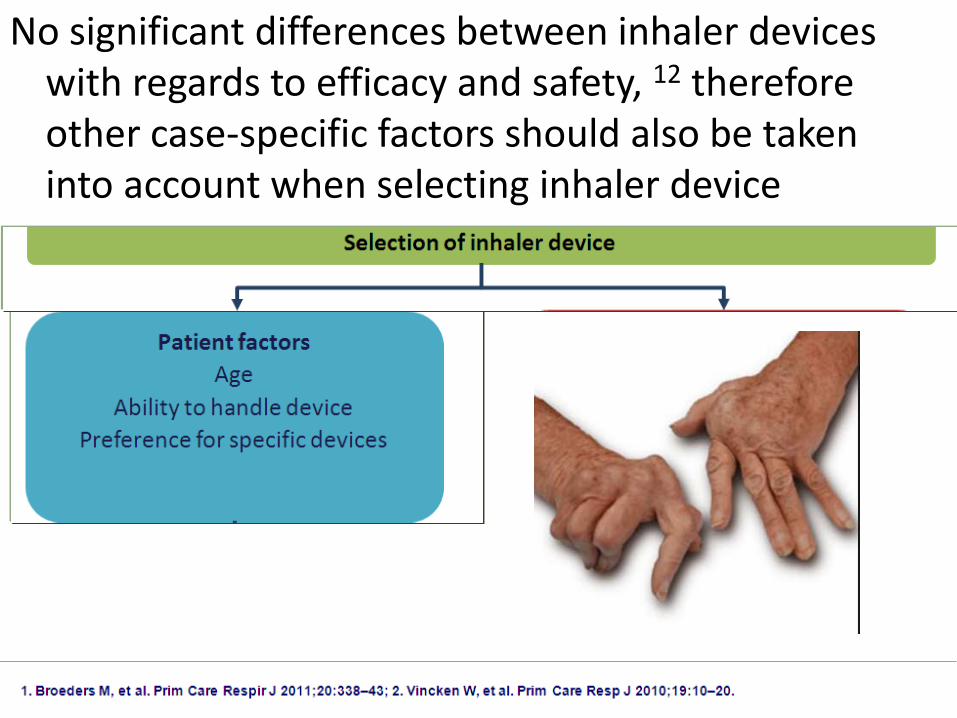
No significant differences between inhaler devices with regards to efficacy and safety, 12 therefore other case-specific factors should also be taken into account when selecting inhaler device
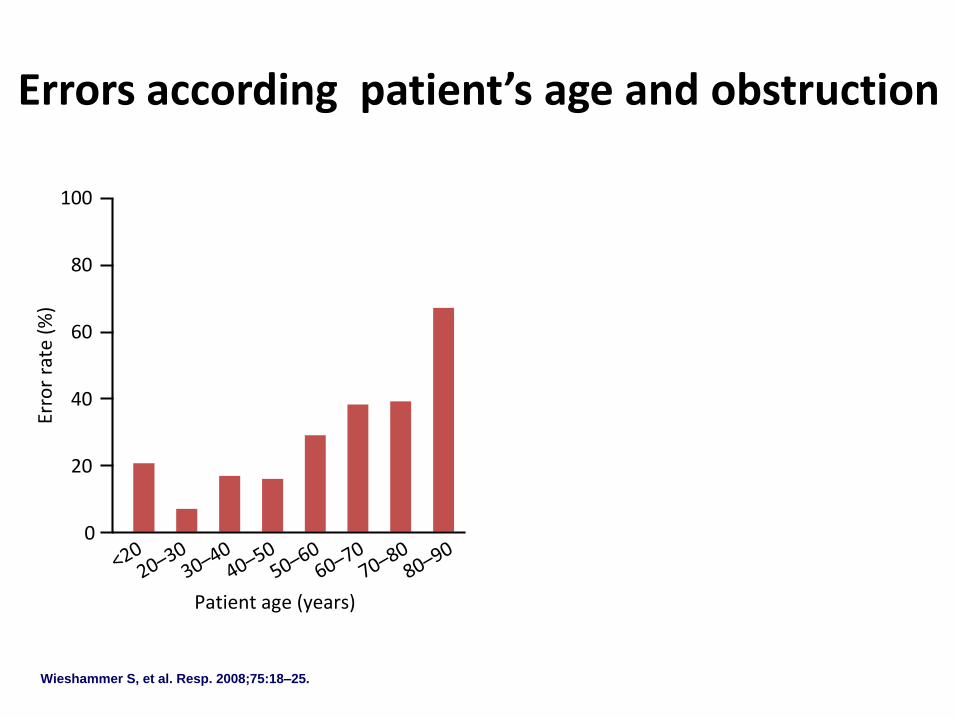
Wieshammer S, et al. Resp. 2008;75:18–25.
Patient age (years)
Erro
r ra
te (
%)
0
20
60
100
40
80
Severity of airway obstruction
No obstruction
Mild Moderate Severe
Erro
r ra
te (
%)
0
20
60
100
40
80
Errors according patient’s age and obstruction

Wieshammer S, et al. Resp. 2008;75:18–25.
Patient age (years)
Erro
r ra
te (
%)
0
20
60
100
40
80
Severity of airway obstruction
No obstruction
Mild Moderate Severe
Erro
r ra
te (
%)
0
20
60
100
40
80
Errors according patient’s age and obstruction

No significant differences between inhaler devices with regards to efficacy and safety, 12 therefore other case-specific factors should also be taken into account when selecting inhaler device

Ideal device• Patients want an inhaler device that:
– they like, prefer, and are satisfied with1,2
– is easy to use correctly3,4
– is more forgiving of variations in technique3,4
– compensates for any comorbidities that may reduce ability to use devices5,6
– has fewer preparatory steps7
– has an intuitive technique that can be easily picked up with very little or no instructions7
– has positive feedback (such as ‘lactose taste’)8
• Once chosen, it is important that patients receive adequate training on how to use their particular device3,9,10
1. Small M, et al. Importance of inhaler-device satisfaction in asthma treatment: real-world observations of physician-observed compliance and clinical/patient-reported outcomes. Adv Ther 2011;28:202-212.2. Lavorini F, Fontana GA. Inhaler technique and patient's preference for dry powder inhaler devices. Expert Opin Drug Deliv 2014;11:1-3.3. Smith IJ, et al. Inhaler Devices: What Remains to be Done? J Aerosol Med Pulm Drug Deliv 2010;23(Suppl 2):S25-37.4. Papi A, et al. Inhaler devices for asthma: a call for action in a neglected field. Eur Respir J 2011;37:982-985.5. Press VG, et al. Misuse of respiratory inhalers in hospitalized patients with asthma or COPD. Journal of General Internal Medicine 2011:26;635-642.6. Yawn BP, et al. Practical aspects of inhaler use in the management of chronic obstructive pulmonary disease in the primary care setting. Int J Chron Obstruct Pulmon Dis 2012;7:495-502. 7. Svedsater H, et al. Qualitative assessment of attributes and ease of use of the ELLIPTA™ dry powder inhaler for delivery of maintenance therapy for asthma and COPD. BMC Pulm Med 13;13:72.8. Baldrick P and Bamford DG. A toxicological review of lactose to support clinical administration by inhalation. Food Chem Toxicol 1997;35:719-733.9. Press VG, et al. Teaching the use of respiratory inhalers to hospitalized patients with asthma or COPD: a randomized trial. J Gen Intern Med 2012;27:1317-1325.10. Giraud V, et al. Inhaler technique and asthma: feasability and acceptability of training by pharmacists. Respir Med 2011;105:1815-182

• Only feedback that dose has been taken is a sweet taste, which may simply indicate high oropharyngeal deposition
• Too many manoeuvres
• Blisters frequently changed and the device cleaned before refill
• If high resistance, it may be difficult to generate high enough inspiratory flow to disaggregate particles sufficiently
• Device must be kept upright until loaded
• Base must be turned fully in both directions
• Patient must shake before use, and drug may escape if the patient exhales into the device2
1. Lavorini F, et al. Respir Med. 2008;102:593–604; 2. O’Connor BJ. Respir Med 2004;98(Suppl 1):S10–6
Features "unfriendly" to the correct use


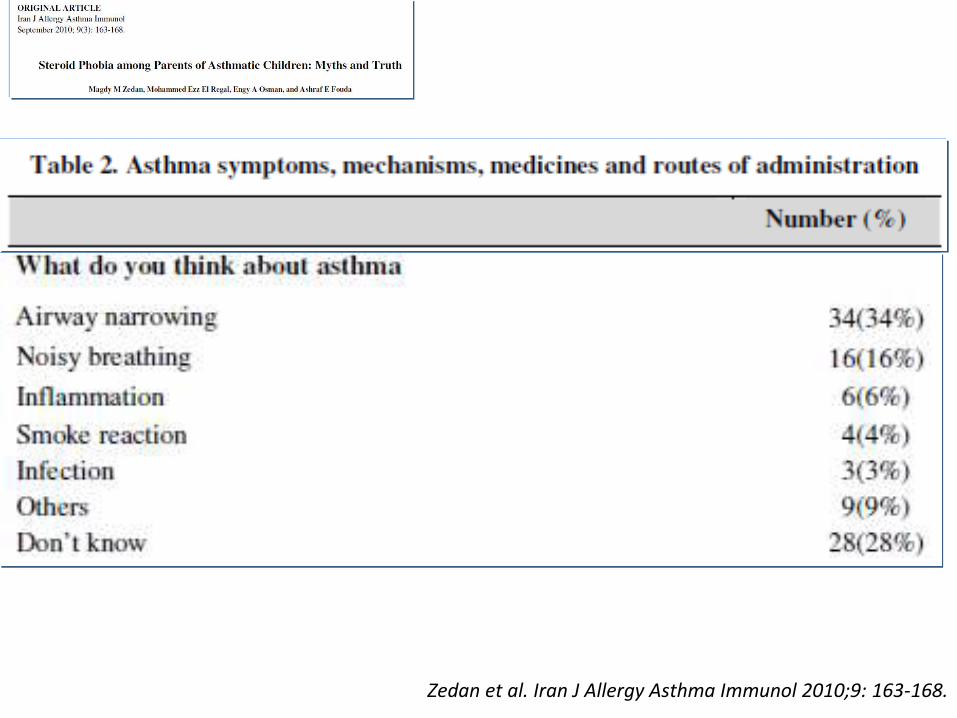
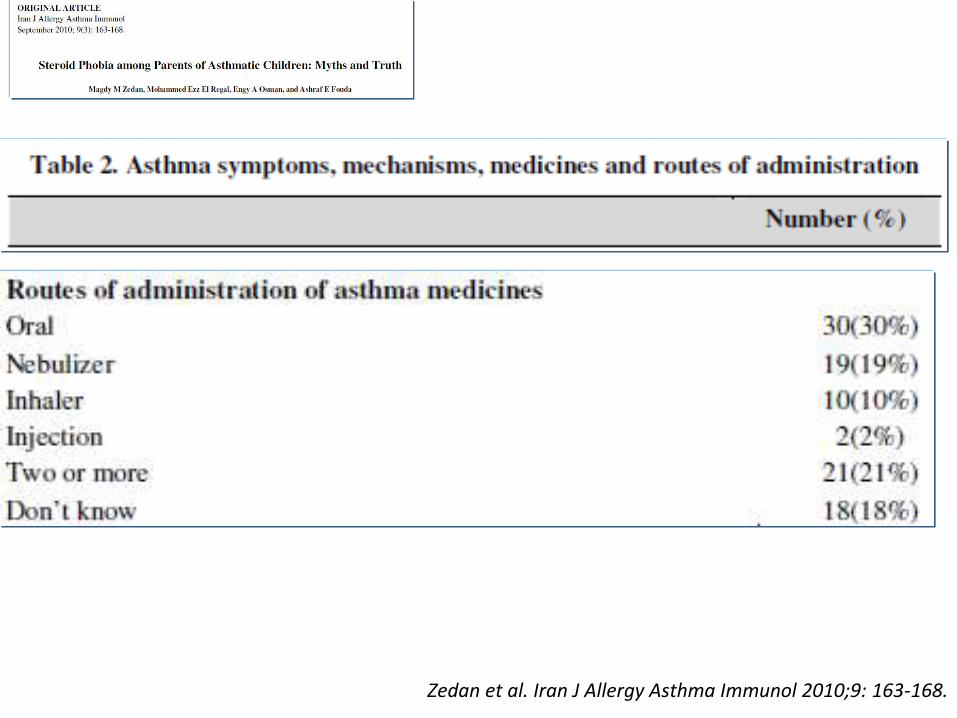
Corticophobia


Zedan et al. Iran J Allergy Asthma Immunol 2010;9: 163-168.
Zedan et al. Iran J Allergy Asthma Immunol 2010;9: 163-168.

Zedan et al. Iran J Allergy Asthma Immunol 2010;9: 163-168.
Zedan et al. Iran J Allergy Asthma Immunol 2010;9: 163-168.

Zedan et al. Iran J Allergy Asthma Immunol 2010;9: 163-168.

Zedan et al. Iran J Allergy Asthma Immunol 2010;9: 163-168.

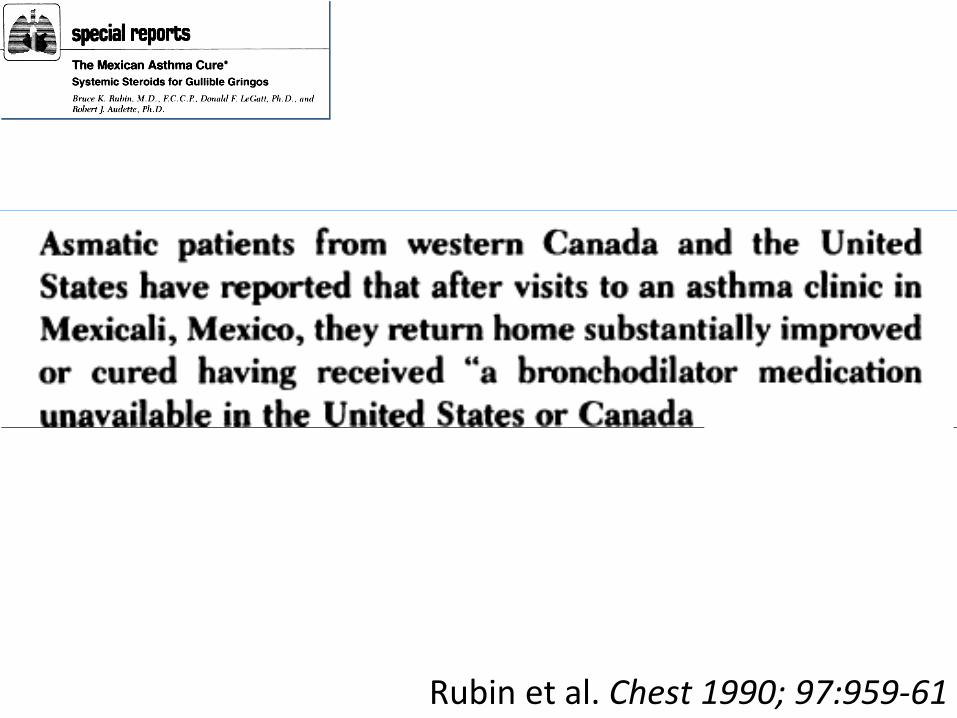
Rubin et al. Chest 1990; 97:959-61

Rubin et al. Chest 1990; 97:959-61

Rubin et al. Chest 1990; 97:959-61

Perché il paziente dovrebbe essere
aderente se…

Decisioni senza contesto clinico
Affidare la diagnosi…
• …a un questionario
• …solo all’E.O.
• …solo alla funzione
• …solo alla clinica

40
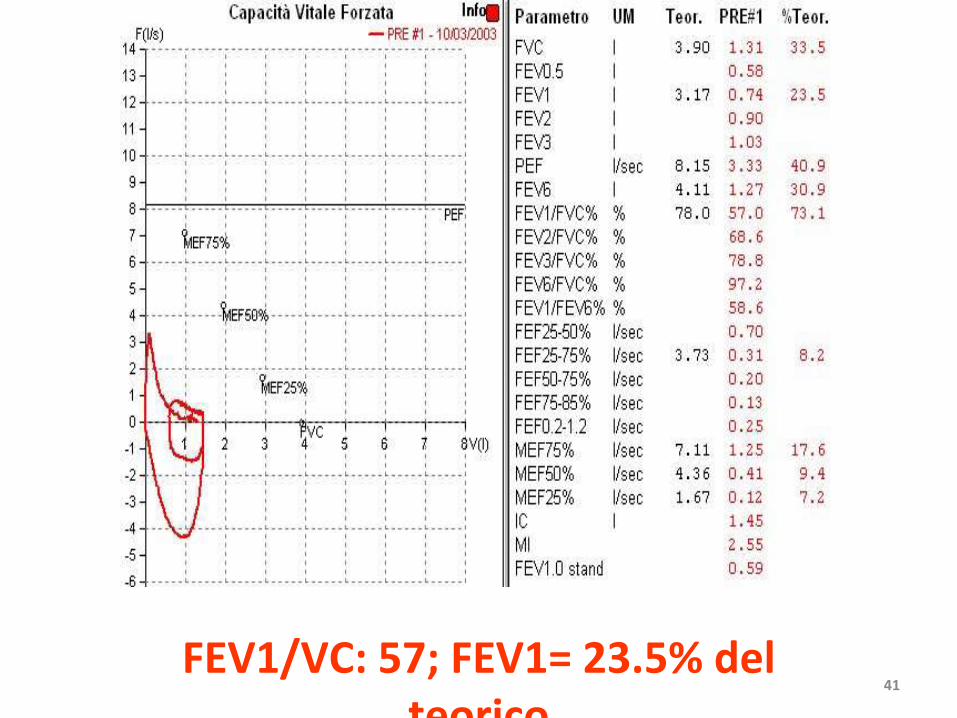
41FEV1/VC: 57; FEV1= 23.5% del
teorico

BPCO: DEFINIZIONE
La broncopneumopatia cronica ostruttiva
(BPCO) è un quadro nosologico
caratterizzato da una persistente
ostruzione al flusso aereo.
2005
COPD, a common preventable and
treatable disease, is characterized by
persistent airflow limitation that is
usually progressive and…
2014

A Review of Available National Guidelines of Treatment of COPD in Europe. Miravitlles,
Vogelmeier, Roche, Halpin, Cardoso, Chuchalin, Kankaanranta, Sandström, Śliwiński, Zatloukal, Blasi
[in press]1. Czech Republic: CZ
2. England: EN
3. Finland: FI
4. France: FR
5. Germany: GE
6. Italy: IT
7. Poland: POL
8. Portugal: POR
9. Russia: RU
10. Spain: SP
11. Sweden: SW

Diagnosis
• FEV1/FVC < 70: EN, FR, GE, FI, PO, RU
• FEV1/FVC < LLN: CZ, IT, POL, and SW

Stratification of Disease Severity
• CZ, EN, FR, GE, POL, POR and RU: GOLD (FEV1)
– IT: Stage 3 and Stage 4 in a single “severe” category.
• FI: low risk (FEV1 ≥50%) and high risk (FEV1
<50%)
• SW: GOLD (FEV1) + EX
• SP: BODE

Symptoms
• FI and SP: CAT
• CZ, POL and POR: CAT and mMRC
• FR: episodic/daily symptoms and mMRC
• RU and SW: CAT, mMRC, and Clinical COPD Questionnaire (CCQ);
• EN: mMRC, systemic symptoms, BMI, CAT, 6’WT and PaO2

Phenotypes
• CB/E: CZ, EN, POL, RU, SP and SW
• Frequent exacerbator: CZ, EN, FI, POL, POR, RU, SP and SW
– ≥2 EX: CZ and FR
– ≥2 EX or ≥1 SEVERE (hospitalization): FI, RU, POR and SP
– ≥2 EX or ≥1 SEVERE (hospitalization) + FEV1 <50%: POL
• ACOS: CZ, FI, RU, SP, FR and SW

Treatment Goals • CZ, FI, FR, POL, POR and SW: reducing
symptoms, averting the natural progression of the disease, improving QoL, enhancing PA, preventing complications and adverse consequences, and increasing life expectancy
• GE and SP: improvement of symptoms, exercise capacity, and QoL; and reduction of exacerbation frequency
• RU: short-term (symptom relief and improvement of exercise tolerance and QoL) and long-term (preventing disease progression and exacerbations and decreasing mortality
• IT: not explicitly stated:

Treatment according patient phenotype
• BC: PDE4in, mucoactive agent, and/or macrolide added to bronchodilators (CZ)
• E: theophylline (CZ)
• ACOS: ICS + LABA or ICS + LABA + LAMA (CZ, FI and SP)
• EX: regular treatment +
PDE4in
ICS
mucoactive drugs
antibiotics

Ass. %teor.
FEV1 2.78 124
FVC 3.35 118
ITFVC 83

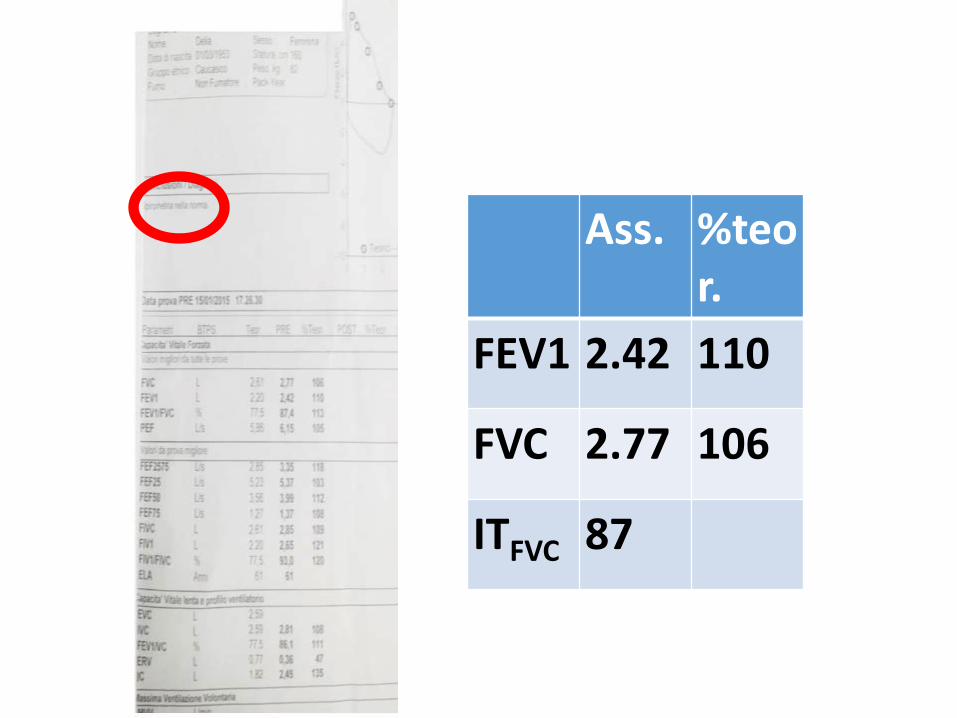
Ass. %teor.
FEV1 2.42 110
FVC 2.77 106
ITFVC 87

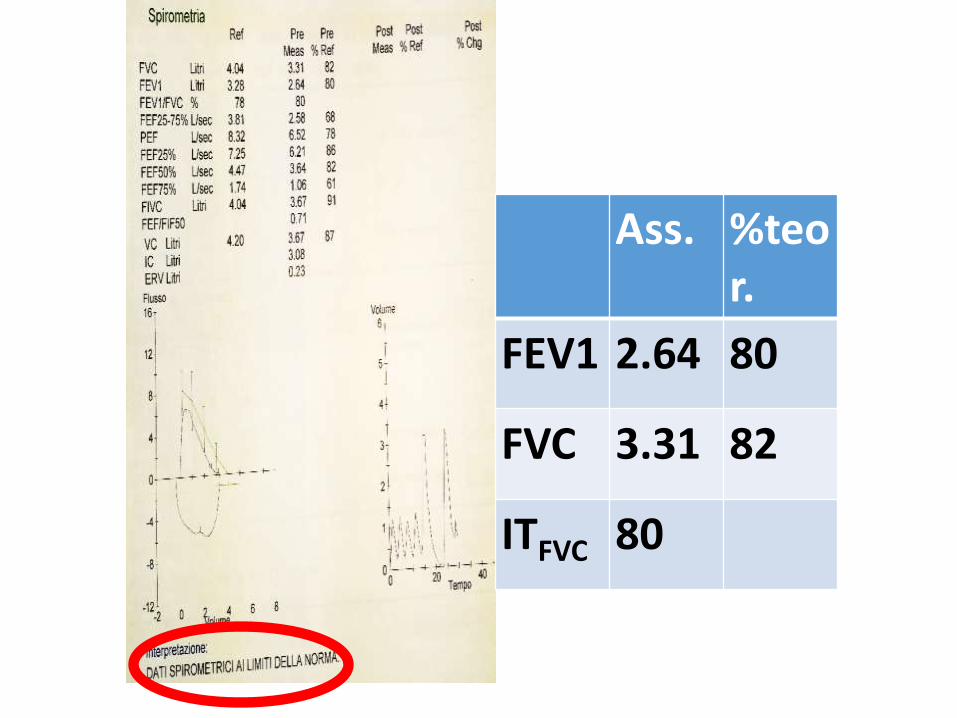
Ass. %teor.
FEV1 2.64 80
FVC 3.31 82
ITFVC 80


Paz. sesso femminile, a. 70
• Fumatrice (45 pack/years), dispnea e tosse

Ass. %teor
FEV1
0.92 40
FVC 2.10 72
IT 55

SIGN?
BTS?
BBC?
ERS?
GOLD?
CNN?ATS?
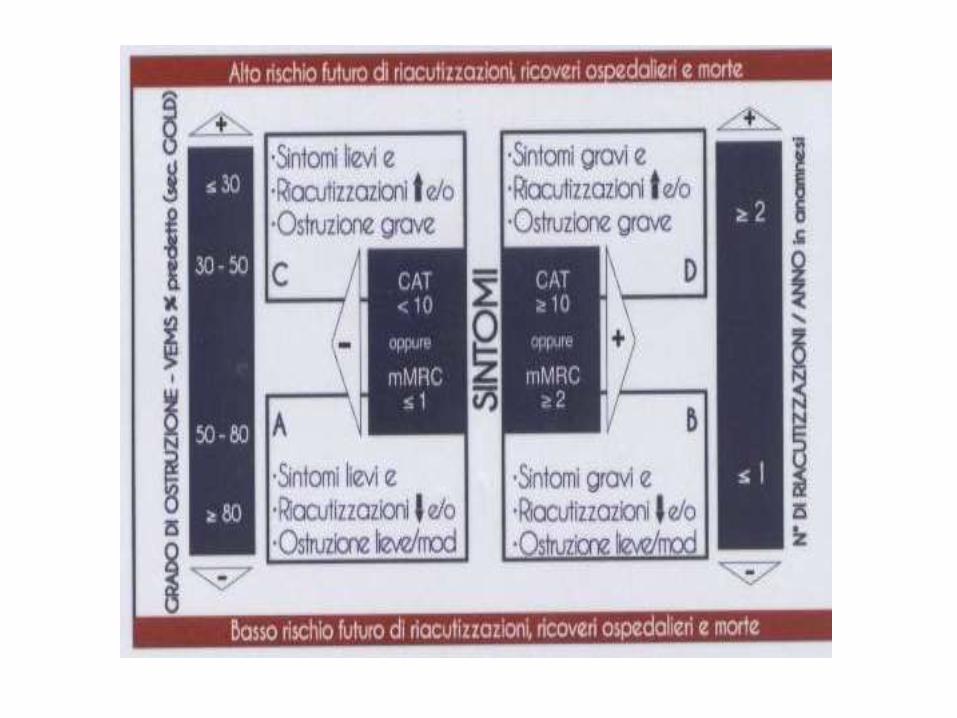
Come calibrare la terapia?


Uso CSI limitato stadi più avanzati o a pazienti con
almeno 2 R / anno
1
2
3
4
Riacutizzazioni
anno
≥ 2
< 2
MRC2 +
CAT 10 +
MRC 0 1 CAT < 10
Trattamento farmacologico
S
T
A
D
I
SABA o
SAMA2a opzione
LAMA o
LABAo
SABA +
SAMA
LAMA oLABA
2a opzione
LAMA + LABA(
A)
(B)
ICS + LAMA
o
ICS+LABA+
LAMA
ICS/LABA+
PDE4
LAMA+LABA
;
LAMA +
PDE4
ICS + LABA
o LAMA2a opzione
LAMA + LABA
(C)
(D)
GOLD 2013
I broncodilatatori sono il trattamento cardine della
BPCO e gli unici indicati negli stadi lievi/moderati (
<2 riacutiz/anno )

FARMACOTERAPIA DELLA BPCO
STABILE (17/20)
60
%
<2
>2
r
i
a
c
u
t
i
z
z
a
z
i
o
n
i
/
a
n
n
o
80% 50%
VEMS % del
predetto
LAMA o
LABA
SABA
o
SAMA
(LAMA O LABA?)
LABA o LAMA
(LABA+ ICS)
LABA + ICS
LAMA + LABA + ICS
LAMA o LABA +
roflumilast
LAMA + LABA
LABA o LAMA
sintomi
LABA +
LAMA
?20%
30%
Person
e con
BPCO
%
50%



SABA o
SAMA
LABA o
LAMA
LABA +
LAMA
LABA
+ CSI
TRIPLI
CE
LABA o
LAMA
LABA + CSI
TRIPLICE
LABA o
LAMA
LABA o
LAMA
+ CSI o
PDE4
LABA +
LAMA
+ CSI o
PDE4
LABA +
LAMA
+ CSI +
PDE4



Perché il paziente dovrebbe essere aderente se…
Perché il paziente dovrebbe essere aderente se…
…i medici non sono d’accordo fra loro?

AFT 3 e 4
DOCENTI

Verificare la diagnosi in pazienti che assumevano BD

ANAMNESI FISIOLOGICA
Età - Sesso

ANAMNESI
Esposizione a sorgenti
inquinanti - Fumo

COMORBIDITA'

SINTOMISpirometria
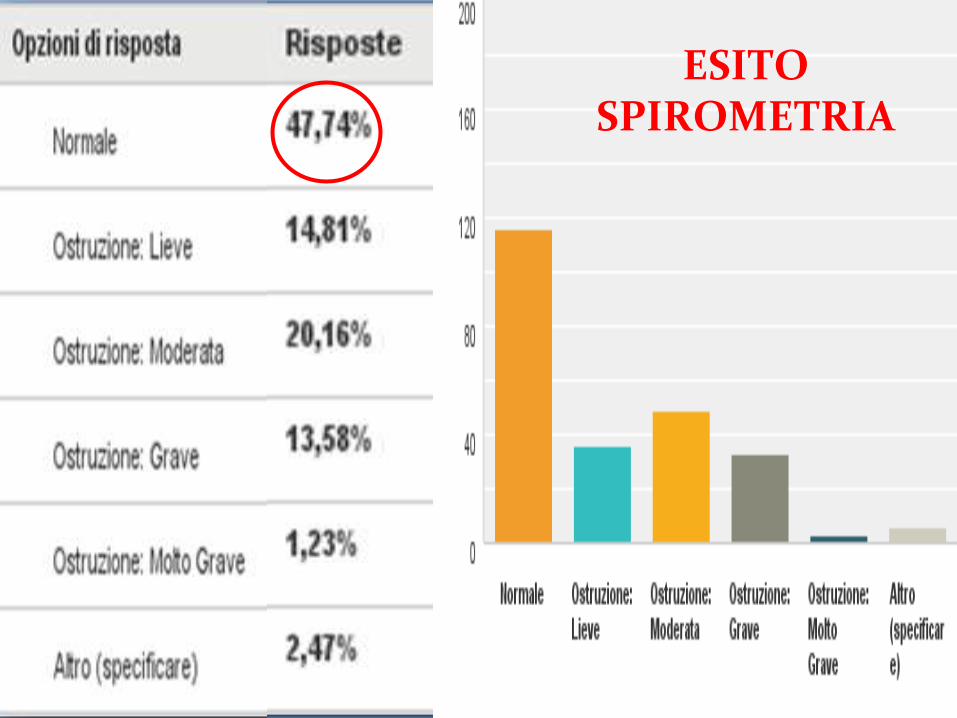
ESITO SPIROMETRIA

TERAPIA POST VALUTAZIONE
Conferma Terapia

PRE
POST
TERAPIA POST VALUTAZIONE
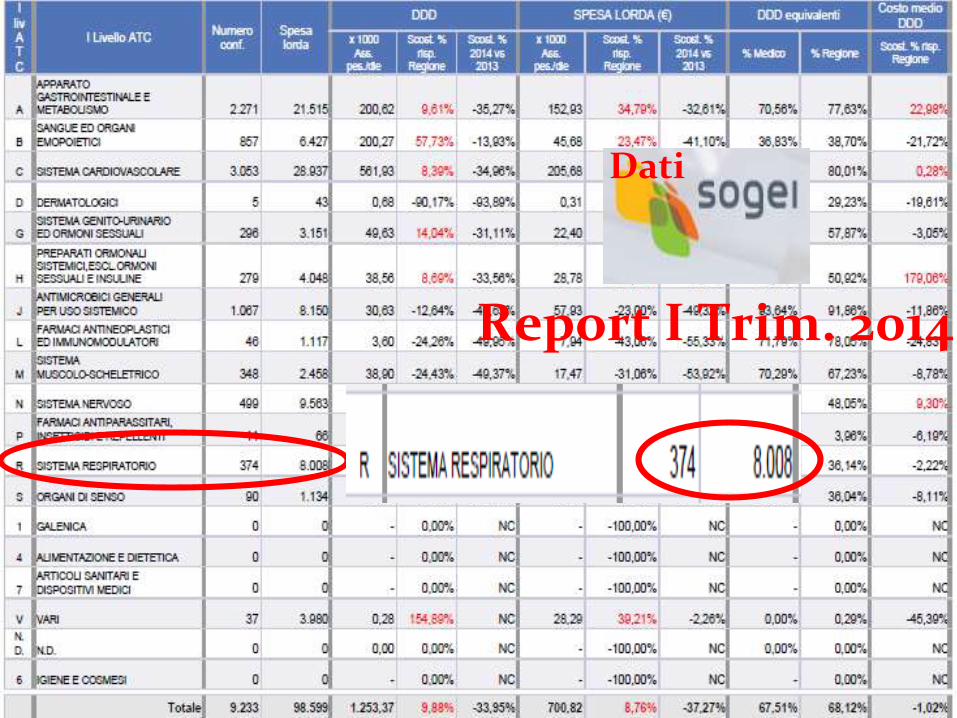
Report I Trim. 2014
Dati
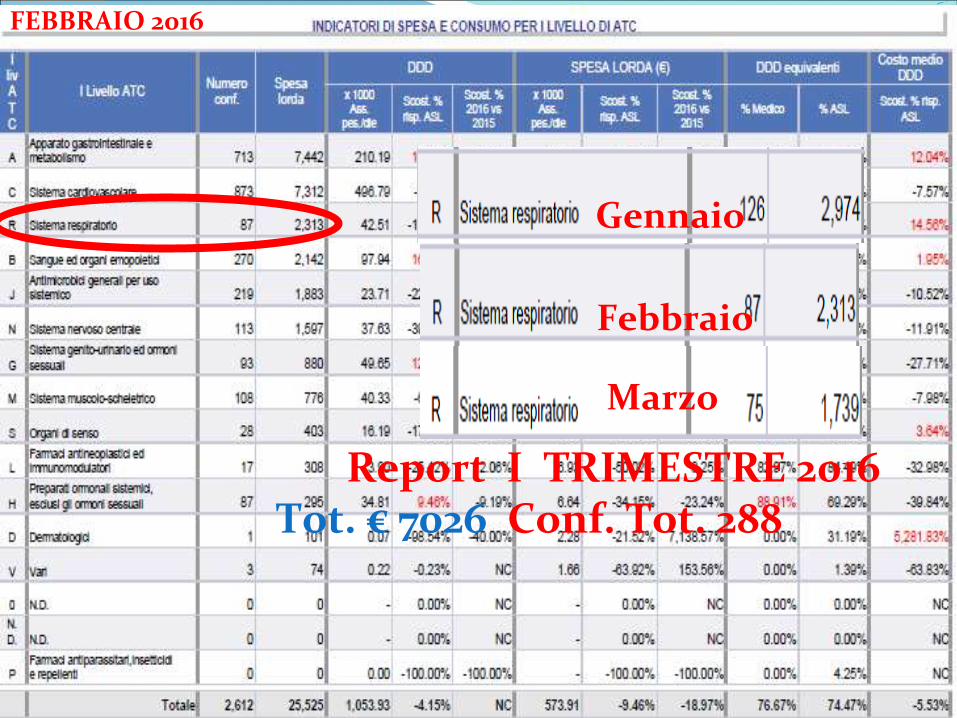
FEBBRAIO 2016
Report I TRIMESTRE 2016Tot. € 7026 Conf. Tot. 288
Gennaio
Febbraio
Marzo
OSMED 2015 report In Italy
Patients with aderence to therapy for pulmonary obstruction
13,6%
OSMED 2015 report In Italy
Patients with aderence to therapy for pulmonary obstruction
13,6%BEN il aderente

Conclusioni
1. LG uniformi, chiare, inequivocabili, facilmente intuibili e applicabili

Conclusioni
1. LG uniformi, chiare, inequivocabili, facilmente intuibili e applicabili
2. Comunicazione

Arch Bronconeumol. 2016 Apr;52(4):179-180. Epub 2016 Mar 10

Appello finale


QUESTIONARIO DELL’AMORE




Grazie
dell’attenzione
CENSURA
Il relatore a 9 mesi Il relatore oggi