leadership and management
TRANSCRIPT

Nursing Leadership & Management
Peter Eustaquio Capistrano, PT, RN, Theo
1Peter Eustaquio Capistrano

Introducing Nursing Management
• Today all nurses are managers (but not all can be leaders)
• Nurses must learn how to work effectively & efficiently with:
staff other nurses UAP 2Peter Eustaquio Capistrano

• Nurses must understand the health care system and how the organization functions.
• You need to know what external forces affect your work.
• Be able to collaborate with others as a leader, as a follower, a team member
3Peter Eustaquio Capistrano

• You need to know what motivates people, &
• How you can help create an
environment that inspire and sustain the individuals who work with you.
4Peter Eustaquio Capistrano

Forces Changing Health Care
+ Proliferation of managed care + greater emphasis on the
business of health care (financial & marketing aspects)
+ shift from acute care to community & outpatient settings
+ shift to costumer-focus + technology advancement
5Peter Eustaquio Capistrano

Forces Changing Health Care
+ emerging new threats such as terrorism, biological warfare, global pandemics
+ addressing the ever-increasing international nursing shortage
+ high turnover rates of staff + new legislations of minimum
staffing ratios6Peter Eustaquio Capistrano
Forces Changing Health Care
Concerns (for employers, HCW, public & policy makers):• Costly live-saving medicines• Robotics• Remote care• Innovations in imaging
technologies• Non-invasive treatments &
surgical procedures
7Peter Eustaquio Capistrano

Health Care Networks• Integrated Care Networks
Due to the struggle to find ways in today’s cost-conscious health society
• Common characteristics:Deliver a whole continuum of careProvide coverage for the buyers of
health care services; and,8Peter Eustaquio Capistrano

Health Care Networks
• Accept the risk inherited in taking a fixed payment in return for providing health care for all persons.
Variety of arrangements and affiliations have occurred
9Peter Eustaquio Capistrano

The focal point for care: -- primary care rather than
hospital
goal of care: -- keep patients healthy by
treating them in the setting that incurs the lowest cost & thereby reducing expensive hospital txs.
10Peter Eustaquio Capistrano

• It is now the GOAL of the health care
industry to keep patients out of the hospitals!!!
11Peter Eustaquio Capistrano

Demands to reduce errors
Peter Eustaquio Capistrano 12

Demand to ↓ Errors 4 Systems Used to ↓ medical errors
I. Control of Medical errors:- US reported in 1999 – 98,000
death occurred each year from preventable medical mistakes in hospitals
- Medical injuries found to ↑ length of stay, patient’s costs & mortality
13Peter Eustaquio Capistrano

Demand to ↓ ErrorsA. Computerization system for
pharmacy that will alert staff for possible:
drug interactions, or adverse reactionsB. Computerized medication
administration recordsC. Patient ID band w/ bar codes
14Peter Eustaquio Capistrano

Demand to ↓ ErrorsD. Beginning fiscal year 2008,
CMS-US would no longer reimburse hospitals for the cost related to hospital-acquired infections or medical errors.
CDC-US, approx: 2m people suffer from nosocomial infections w/c costs $27.5b
(CDC, 2007)15Peter Eustaquio Capistrano

Demand to ↓ Errors
II. Leapfrog Group- A consortium of public &
private purchasers - Provides benefits to more than
37m Americans in all 50 states. - Rewards health care
organizations that demonstrate quality outcome measures
16Peter Eustaquio Capistrano

Demand to ↓ Errors
• 3 quality indicators:
1. ↑ computer-physician order entry system
2. Using evidence-based hospital referrals
3. Using ICU physician intensivists staff
17Peter Eustaquio Capistrano

Demand to ↓ ErrorsMost significant impact on
preventing medical errors:• ≥ 65,000 lives could be saved
• ≥ $41b could be saved
• ≥ 900,000 medical errors could be avoided
18Peter Eustaquio Capistrano

Demand to ↓ Errors
III. Quality management Preventive approach to address
problems before they become crises
Began in post-WW II Japan
19Peter Eustaquio Capistrano

Demand to ↓ Errors
• To improve the quality of manufactured products
• Consumers’ needs should be the focus of management
• Employees should be empowered to evaluate and improve quality
20Peter Eustaquio Capistrano

Demand to ↓ Errors• TQM build tools for continuous
improvement of product & services thru constant evaluation of how well the consumers’ needs are met devise plans to perfect the process
Done thru patient satisfaction surveys
21Peter Eustaquio Capistrano

Demand to ↓ Errors
IV. Benchmarking• Compares an organization w/
similar organizations (in contrast w/ TQM)
• Outcome indicators are identified to be used to compare performances across disciplines
22Peter Eustaquio Capistrano

Benchmarking
• Used for standard development & performance improvement
• Once the results are known, weaknesses can be addressed & enhance areas of strength
Peter Eustaquio Capistrano 23

Benchmarking
Questions to be asked in benchmarking:
+ “How did they do it?” + “What tools did they
use/” + “What were their lessons
learned?”
Peter Eustaquio Capistrano 24

• Populations & Cultural Diversity
• Generational Diversity• Aging Patients & Aging
Nurses
Peter Eustaquio Capistrano 25

Immigrant Populations & Cultural Diversity
• US Census Bureau minority population = 100m in 2007
• Hispanics – 44m (largest group)• African origin – 40 m fastest growing minority• Asians – 14m 2nd fastest growing minority
26Peter Eustaquio Capistrano

Immigrant Populations & Cultural Diversity
• The challenge for health care policy makers & the public:
to find ways to provide universal access to care regardless of care, ethnic origin, or socioeconomic status.
27Peter Eustaquio Capistrano

Immigrant Populations & Cultural Diversity
• Current trend: assume trans-cultural focus
They consider: - values - beliefs - lifestyle of the diverse cultures
28Peter Eustaquio Capistrano

Immigrant Populations & Cultural Diversity
• Trans-cultural diversity affects nursing:
- 81.8% of US nurses caucasians (2004 survey)
- 18.2% - from minority population
- only 5.4 nurses are male (2000 survey)
29Peter Eustaquio Capistrano

Generational Diversity
• Seeing four generations working together side by side in today’s workplace is common:
traditionalsBaby boomers have different
Generation X values &
millenials expectations in the workplace
30Peter Eustaquio Capistrano

Generational Diversity
• Baby boomers:
+ value professional & personal growth
+ expect that their work will make a difference
Peter Eustaquio Capistrano 31

Generational Diversity
• Traditionals:
+ value loyalty + respect authority + follows bureaucracy
policies
Peter Eustaquio Capistrano 32

Generational Diversity
• Generation X – desire a (+) work environment
• Want their work to have worth• Want independence, fun • Value independence• Tend to focus on outcomes
rather than processes
33Peter Eustaquio Capistrano

Generational Diversity
• To have balance between work & other important areas of their lives:
- personal relationships - child rearing - pleasurable pursuits
34Peter Eustaquio Capistrano

Generational Diversity
• Millenials (a.k.a. Generation Y)
• Technically savvy• Responsible• Competent• Expert in connecting online• Prepares to participate in
collaborative structures
35Peter Eustaquio Capistrano

Generational Diversity• Challenge for managers: - avoid stereotyping within the
generations - value unique contribution of
each generation - encourage mutual respect for
differences - leverage differences to enhance
teamwork36Peter Eustaquio Capistrano

Generational Diversity• Challenge for managers:
- changes in the workplace also add to conflicts due to the generations’ different expectations
37Peter Eustaquio Capistrano

Aging Patients, Aging Nurses
• Older generation 65 y/o & ↑ 37m in 2006 (12% in US
population) approximately 1 in every 10
Americans by 2030 – more than 71m older
adults
38Peter Eustaquio Capistrano

Aging Patients, Aging Nurses
• Reasons for continuation of demand for health care for aging patients:
- people are living longer - advancement in technology are
enabling people to survive previously fatal diseases & conditions
- older x often require on-going care for chronic / acute illnesses
39Peter Eustaquio Capistrano

Aging Patients, Aging Nurses
↑ older people are due to:• Increase in life expectancy • older workers retiring later• good health practices (exercise,
healthy eating, screenings)
These people will require episodic & chronic care
40Peter Eustaquio Capistrano

Aging Patients, Aging Nurses
• Nurses are growing older
• Ave. age : 46.8 (US, 2007) compared to 44.3 in 1996
• % of nurses over 54 y/o increased to 25.2% in 2004.
41Peter Eustaquio Capistrano

Aging Patients, Aging Nurses
• Means that the current need for nurses will continue and grow as more & more aging nurses will retire from work
• US Dept of Labor predicts (2014) that RN will be the second largest occupation second to retail salesperson)
42Peter Eustaquio Capistrano

• Changes for future nurses
Peter Eustaquio Capistrano 43

More Change on the Way
• Evidence-based practice applying the best scientific
evidence to a px’s unique diagnosis, condition & situation to make clinical decisions
44Peter Eustaquio Capistrano

Evidence-based practice
• The process of EBP: - identify the clinical question - find the evidence to answer the
question - evaluate the evidence - apply the evidence - evaluate the outcome
45Peter Eustaquio Capistrano

Evidence-based practice
• ΣθΤ International (honor society for nurse)
EBP: The integration of best evidence available,
nursing expertise, and the values & preference of the individuals, families & communities who are served. EBP will be successful when nurses & health care decision makers have access to a synthesis of the latest research, a consensus of expert opinion and then exercise their judgment as they plan & provide care that takes into account cultural & personal values & preferences. (2004)
46Peter Eustaquio Capistrano

Strategies for new Nurses to promote EBP:
+ keep abreast: subscribe to journals & read widely
+ encourage use of multiple sources of evidence + find established sources in your specialty + question & challenge nursing traditions,
promote spirit of risk-taking + dispel myths & traditions not supported by
evidence + Collaborate with others nurses locally &
globally + interact with other disciplines to bring nursing
evidence to the table47Peter Eustaquio Capistrano
Electronic Health Records
• Integrates health info from all sources and cane be accessed from multiple locations from authorized providers.
48Peter Eustaquio Capistrano

Electronic Health Records
• Electronic records: - ↓ redundancies - improve efficiency - ↓ medical errors - lower health care costs
49Peter Eustaquio Capistrano

Electronic Health Records
• Patient’s personal health record:
- online system allowing patients to track medications, record medical interventions, update their own medical information as needed.
50Peter Eustaquio Capistrano

Robotics & Remote Care
• Use of robots to transfer supplies and to deliver remote care
• Systems & supplies can be ordered now electronically & filled by laser-guided robots
• Robots deliver the requested supplies to nursing units
51Peter Eustaquio Capistrano

Robotics & Remote Care• Physicians in remote locations
can access pxs using wireless video connections in robots at the bedside
• Some robots offer electronic stethoscopes & other diagnostic devices
• Can follow-up lab results between cases instead of after the day’s procedures
52Peter Eustaquio Capistrano

Terrorism & Disaster Preparedness
• Extensive staff training is required
• Assess nurses’ concerns & provide accessible info, support & opportunities for debriefing
Natural disaster, attack of terrorism, epidemic are examples
53Peter Eustaquio Capistrano

Challenges Facing Nurses
Nurse mangers are challenged to: manage with decrease resourcesTo supervise teams of
professionals & non-professionals from a variety of cultures
Must a coach, teacher & facilitator because they are responsible for others’ work
54Peter Eustaquio Capistrano

• Must be a leader to motivate & inspire
• Must address the interests of both admin & employees
• Works thru others to meet the goals of individuals, the unit, & of the organization
55Peter Eustaquio Capistrano

• Organizations And
organizational theories
Peter Eustaquio Capistrano 56

Organizational Theories
• Organization – a collection of people working together
under a defined structure to achieve pre-determined
outcomes using financial, human and material
resources.
57Peter Eustaquio Capistrano

Organizational Theories
• Types: + classical Theory + Humanistic Theory + Systems Theory + Contingency Theory + Chaos Theory + Complexity Theort\y
58Peter Eustaquio Capistrano

Organization
• The lifecycle of the org is dependent on its adaptability & response to changes in its environment
• When org tends to grow, it tends to stabilize & develop more formal standards.
59Peter Eustaquio Capistrano

Organization
• When the org becomes large, it tends to lose its adaptability & its responsiveness to its environment.
60Peter Eustaquio Capistrano

Classical Theory
Focuses solely on the structure of the formal organization
main premise: efficiency thru design
people are operating within a rational & well-defined task
61Peter Eustaquio Capistrano

4 elements of Classical Theory
• Division & Specialization of Labor
• Chain of Command• Organizational Structure• Span of Control
62Peter Eustaquio Capistrano

Division & Specialization of Labor
• Division of work reduces the tasks that each employee must carry out ↑ efficiency proficiency & specialization
• Managers can standardize the work to be done 63Peter Eustaquio Capistrano

Chain of Command
hierarchy of authority & responsibility w/n the organization
Authority – as the right or power to direct activity
Responsibility – as obligation to attain objectives or perform certain functions
64Peter Eustaquio Capistrano

Chain of Command
• The line of authority – higher levels of management delegate work to those below them in the organization.
• Line of authority – linear hierarchy
• Staff authority – advisory relationship; recommends & advices
65Peter Eustaquio Capistrano
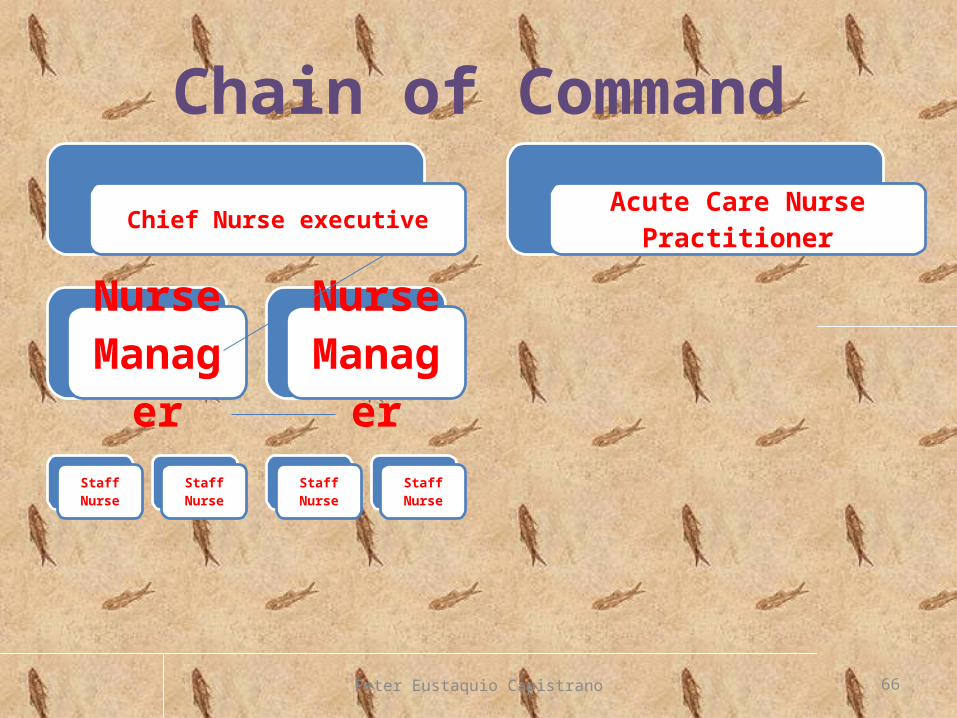
Chain of Command
Chief Nurse executive
Nurse Manager
Staff Nurse
Staff Nurse
Nurse Manager
Staff Nurse
Staff Nurse
Acute Care Nurse Practitioner
66Peter Eustaquio Capistrano

Organizational Structure
• describes the arrangement of the interrelated work group
• The design of the organization is intended to foster the organization’s survival & success
67Peter Eustaquio Capistrano

Span of Control
• Addresses the pragmatic concern of how many employees a manager can handle effectively
68Peter Eustaquio Capistrano

Span of Control
• Complex organizations – have numerous departments that are highly specialized & differentiated
• Authority is centralized
• a.k.a tall organizational structure
69Peter Eustaquio Capistrano
Span of Control
• Less Complex organizations – flat structure
• Authority is decentralized• With several managers
supervising large work groups
70Peter Eustaquio Capistrano

• Organizational theories
Peter Eustaquio Capistrano 71
Humanistic Theory
• Criticism of the Classical Theory led to the development of the Humanistic Theory in the 1930s.
• Major assumption: People desire social
relationships, respond to group pressures, & search for personal fulfilment.
72Peter Eustaquio Capistrano

Humanistic Theory
• Hawthorne effect – if special attention is given to workers
they will work better resulting to increased productivity.
73Peter Eustaquio Capistrano

Systems Theory
• Defined as a set of interrelated parts arranged in a unified whole;
• Productivity is the result of interplay among structure, people, technology & environment
74Peter Eustaquio Capistrano

Types of Systems
• Closed System – self-contained & usually can be found in the physical sciences
• Open System – interacts both internally & & with its environment (a living organism)
75Peter Eustaquio Capistrano
• Organizations are complex, social, open system
• Framework are interrelated by part of the system and their functions can be studied
• Health care org’zn requires human, financial & material resources
76Peter Eustaquio Capistrano

Health Care System as Open System
INPUT• MATERIALS • MONEY• EMPLOYEES• PATIENTS• EQUIPMENTS
THROUGHPUT
• HEALTH CARE DELIVERY
• EDUCATION
OUTPUT
• RESTORED HEALTH• REHABILITATION• DISEASE
PROTECTION• DEATH W/ DIGNITY• RESEARCH
77Peter Eustaquio Capistrano

Contingency Theory
Contingency Theory believe organizational performance can be enhance by matching an organization’s structure to its environment.
Environment people, objects, ideas that influence the org.
78Peter Eustaquio Capistrano

Contingency Theory
• Environment of a health care org’n:
patientsPotential
patients third-party
payers
competitors regulators suppliersPharmaceuti-
cals
Peter Eustaquio Capistrano 79

Contingency Theory• Given the variety of health care
services and different types of patients served today,
The organizations differ w/ respect to the environment they face
Levels of skills & training of their caregivers
The emotional & physical needs of patients 80Peter Eustaquio Capistrano

Chaos Theory
• The nature of relationship we have w/ each other &
with the organization does not follow a straight line.
81Peter Eustaquio Capistrano

Chaos Theory
challenges traditional thinking regarding the design of organizations.
organizations are living, self-organizing systems that are complex and ever-changing.
82Peter Eustaquio Capistrano

Chaos Theory
• Chaos theory suggests that the drive to create a
permanent organizational structure is doomed to fail.
83Peter Eustaquio Capistrano

Chaos Theory
• Organizations, to succeed, must ensure:
+ flexibility + fluidity, + speed of adaptability, & + cultural sensitivity
84Peter Eustaquio Capistrano

Chaos Theory
• The role of leadership in Chaos Theory (changing organizations) :
+ build resilience in the midst of change
+ to maintain balance between tension & order
+ promote creativity, & + prevent instability
85Peter Eustaquio Capistrano

Chaos Theory
• Challenges of Chaos Theory: to reflect on creative and
flexible formats that can be quickly adjusted and changes as organizations shift.
abandon our attachments to any particular model of design
86Peter Eustaquio Capistrano

Complexity Theory
• Organization is a mixture of all the theories that consider it as a total system.
reasons: random events interfere with
expectationsPatient’s condition change in an
instant
87Peter Eustaquio Capistrano

Complexity Theory
necessary staff are not available or is not equipped
failure of equipments to function well
tasks are sometimes contradicting with the values of the pxs, nurses & physicians
88Peter Eustaquio Capistrano

Complexity Theory
• Health care continues to focus on px care providers rather than the system as a whole.
• Using high reliability teams has been effective in preventing serious errors.
89Peter Eustaquio Capistrano

Complexity Theory
• Hierarchy is less important in complexity theory.
• Every encounter between a px & a caregiver offers information about possible solutions to problems
90Peter Eustaquio Capistrano

Complexity Theory
• Manager’s task:Encourage the flow of info
between and among all team members, leaders &
followers, whether top-down, bottom-up, or sideways.
91Peter Eustaquio Capistrano

Traditional Organizational
Structures• When structure is not aligned with organizational needs, the organizational response to environmental change:
diminishes decisions are delayed, poor,
overlooked conflicts result performance deteriorates
92Peter Eustaquio Capistrano

Traditional Organizational
Structures• Types:
+ Functional Structure + Service-line Structure + Hybrid Structure + Matrix Structure + Parallel Structure
93Peter Eustaquio Capistrano

Functional Structure
• Employees are grouped in departments by specialty with similar tasks
• Reports to the same manager
• Tends to centralize decision-making (top organization)
94Peter Eustaquio Capistrano

Functional Structure
• Weaknesses:
+ coordination across functions is poor
+ decision-making responsibilities can pile up at the top
+ overloaded senior managers
95Peter Eustaquio Capistrano

Functional Structure
+ Coordination across functions are slow
+ General management training is limited
+ top managers may be uninformed of day-to-day operations
96Peter Eustaquio Capistrano

Service-line Structure
• a.k.a. Product-line structure, service-integrated structure
• All functions needed to produce a product or service are grouped together in self-contained units
97Peter Eustaquio Capistrano

Service-line StructureCEO
Executive secretary
Cardiology
Nursing
Dietary
Pharmacy
Oncology
Nursing
Dietary
Pharmacy
Burn Unit
Nursing
Dietary
Pharmacy
98Peter Eustaquio Capistrano
Service-line Structure• Strengths: + have potential for rapid
change in an unstable environment
+ high client satisfaction due to specialization
+ coordination occurs easily + service is priority because
employees sees it as the purpose why the org exists 99Peter Eustaquio Capistrano

Service-line Structure• Weaknesses: + possible duplication of
resources + lack of in-depth technical
training & specialization + services operate independently
& often compete + units (w/c is autonomous) have
duplicate staff & competes for resources 100Peter Eustaquio Capistrano

Hybrid Structure
During growth of organizations, both self-
contained units & functional units converge
101Peter Eustaquio Capistrano

Hybrid Structure• Strengths: + provides simultaneous
coordination w/n product divisions while maintaining the quality of each function
+ improves the alignment between corporate & service or product goals
+ fosters better adaptation to the environment while still maintaining efficiency 102Peter Eustaquio Capistrano

Hybrid Structure• weaknesses: + conflict between top admin &
managers + managers often recent admin’s
intrusions into what they see as their own area of responsibility
+ over time, organizations tend to accumulate large corporate staff to oversee divisions
103Peter Eustaquio Capistrano

Hybrid StructureCEO
NURS
ING
STORE
ROOM
DIETARY
ADMITTIN
G
PHARMA CY
BILLING
104Peter Eustaquio Capistrano

Matrix Structure
• Integrates both product & functional structures into one overlapping structure.
• Different managers are responsible for function & product
• (e.g. Nurse manager for oncology clinic may report to the vp for nursing as well as to the vp for outpatient services)
105Peter Eustaquio Capistrano

Matrix Structure• Weakness:
+ dual authority + excellent interpersonal
skills are needed from managers involved
+ time consuming due to frequent meetings to resolve conflicts & problems
106Peter Eustaquio Capistrano

Matrix Structure
• Weakness:
+ one side of the organization may become dominate over the other
107Peter Eustaquio Capistrano

Matrix Structure
Vice-President, Outpatient Services
Oncology Pediatrics Family medicine
Vice-President for Nursing
ServicesNurse
ManagerNurse
Manager
Nurse Manager
108Peter Eustaquio Capistrano

Parallel Structure
• Unique to health care
• Complex relationship that exists between he formal authority of the HC org and the authority of its medical staff (separate &a autonomous from its org.)
• two lines of authority: organizational dilemma
109Peter Eustaquio Capistrano

Parallel StructureCEO
Chief Nurse
executive
NM
RN
LPN
UAP
NM
NM
Hr dIRECTOR
chief financial Officer
BUDGET
BUDGET pERSON
NEL
Chief Suport
Services
HOUSEKEEPING
MAINTENANCE
MEDICAL dIRECTOR
CHIEF OF SERVICES
INTERNAL mEDICINE
SURGERY
OB
110Peter Eustaquio Capistrano

Leadership And
Management
111Peter Eustaquio Capistrano

• Nurse managers need a body of knowledge and skills distinctly different from those needed for nursing practice!!!
• Yet few nurses have the education or training necessary to be managers!!!
112Peter Eustaquio Capistrano

• Managers depend on experiences with former supervisors, who also learn supervisory techniques on the job!!!
• Often a gap exists between what managers know and what they need to know!!!
113Peter Eustaquio Capistrano

Leader • Anyone who uses
interpersonal skills to influence others to accomplish the specific goals.
• Exerts influence by using a flexible repertoire of personal behaviors & strategies.
114Peter Eustaquio Capistrano

Manager
• Latin: manu, agere, “to lead from the hand”
• An individual employed by an organization responsible & accountable for efficiently accomplishing the goals of the organization.
115Peter Eustaquio Capistrano

Leader • Often do not have
delegated authority but obtain power thru influence
• Have a variety of roles than do managers
• May or may not be a part of a formal org.
Manager • Have assigned
position w/n the formal organization
• Have a legitimate source of power due to delegated authority
• Expected to carry out specific functions, duties, responsibilities
Peter Eustaquio Capistrano 116

Leader • Focus on group
process, informal gathering, empowering people
• Emphasize interpersonal relationship
Manager • Emphasize control,
decision-making, decision analysis & results
• Manipulate the environment, people, money, time & other resources to achieve organizational goals
Peter Eustaquio Capistrano 117

Leader • Directs willing
followers
• Goals that may or may not reflect the those of the organization
Manager • Have a greater
formal responsibilities & accountability for rationality & control than leaders
• Direct willing & unwilling subordinates
Peter Eustaquio Capistrano 118

119Peter Eustaquio Capistrano

120Peter Eustaquio Capistrano

121Peter Eustaquio Capistrano

122Peter Eustaquio Capistrano

123Peter Eustaquio Capistrano

124Peter Eustaquio Capistrano

125Peter Eustaquio Capistrano