leadless cardiac pacemakers - jacc: journal of the ... · leadless cardiac pacemakers ... (in...
TRANSCRIPT
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 6 , N O . 1 0 , 2 0 1 5
ª 2 0 1 5 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N DA T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 5 . 0 6 . 1 0 8 1
REVIEW TOPIC OF THE WEEK
Leadless Cardiac Pacemakers
Back to the FutureMarc A. Miller, MD,* Petr Neuzil, MD,y Srinivas R. Dukkipati, MD,* Vivek Y. Reddy, MD*
ABSTRACT
Fro
Pra
Mi
Na
pa
Ju
(m
con
Lis
Ma
Despite significant advances in battery longevity, lead performance, and programming features since the first implanted
permanent pacemaker was developed, the basic design of cardiac pacemakers has remained relatively unchanged
over the past 50 years. Because of inherent limitations in their design, conventional (transvenous) pacemakers are prone
to multiple potential short- and long-term complications. Accordingly, there has been intense interest in a system able
to provide the symptomatic and potentially lifesaving therapies of cardiac pacemakers while mitigating many of the
risks associated with their weakest link—the transvenous lead. Leadless cardiac pacing represents the future of cardiac
pacing systems, similar to the transition that occurred from the use of epicardial pacing systems to the familiar trans-
venous systems of today. This review summarizes the current evidence and potential benefits of leadless pacing systems,
which are either commercially available (in Europe) or under clinical investigation. (J Am Coll Cardiol 2015;66:1179–89)
© 2015 by the American College of Cardiology Foundation.
S ince the first completely endocardial transve-nous permanent pacemaker was implantedmore than 50 years ago, significant advances
have been made in battery longevity, lead perfor-mance, and device programming (1–3). Nevertheless,the basic design of cardiac pacemakers has remainedrelatively unchanged: a (most commonly) pectoralpulse generator connected to 1 or more transvenousleads. Although highly reliable, conventional cardiacpacemakers have several limitations. The subcutane-ous pocket has a potential for local complications,such as skin erosion and pocket hematomas, whichcan be associated with a 15-fold higher risk for subse-quent infection if early reintervention is required(4–6). The insertion of transvenous leads can resultin acute complications, such as pneumothorax or up-per extremity deep vein thrombosis, and the presence
m the *Helmsley Electrophysiology Center, Icahn School of Medicine,
gue, Czech Republic. Dr. Reddy is a consultant for and has received spea
cra leadless pacemaker); has received grant support and speaking hon
nostim leadless cardiac pacemaker); and has received grant support fro
cing system). Dr. Neuzil has received grant support fromMedtronic; has rec
de Medical (manufacturer of the Nanostim leadless cardiac pacemaker);
anufacturer of the WiCS cardiac pacing system). All other authors have rep
tents of this paper to disclose.
ten to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Vale
nuscript received April 12, 2015; accepted June 10, 2015.
of chronic transvenous leads can lead to central veinobstruction, tricuspid valve insufficiency, and infec-tion (7,8). Even for single-chamber transvenous sys-tems (which are associated with a lower risk thandual-chamber system implants), more than 1 in every40 implants will result in a complication requiringsurgical intervention within the first 3 months, ofwhich more than one-half are lead related (9,10). Inthe long term, lead failures are associated with signif-icant morbidity (7).
Early recognition that transvenous leads are theweakest link of conventional pacing systems led in-vestigators more than 40 years ago to consider thepossibility of leadless cardiac pacing (1). A pre-clinicalreport in 1970 demonstrated the feasibility of a totallyself-contained intracardiac pacemaker. In that study,a canine with an iatrogenic heart block was paced for
New York, New York; and the yHomolka Hospital,
king honoraria from Medtronic (manufacturer of the
oraria from St. Jude Medical (manufacturer of the
m EBR Systems (manufacturer of the WiCS cardiac
eived grant support and speaking honoraria from St.
and has received grant support from EBR Systems
orted that they have no relationships relevant to the
ntin Fuster.
ABBR EV I A T I ON S
AND ACRONYMS
CRT = cardiac
resynchronization therapy
LCP = leadless cardiac
pacemaker
TPS = transcatheter pacing
system
Miller et al. J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5
Leadless Cardiac Pacing S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9
1180
more than 2 months. The delivery catheterwas inserted through the jugular vein, theleadless pacemaker was passed into the rightventricle under fluoroscopy, and radiallydirected spiral barbs attached the cylindricaldevice to the ventricular myocardium. Ap-proximately 2 decades later, additional pre-clinical testing again demonstrated the
potential feasibility of this approach (11). Althoughthe field of leadless cardiac pacing remained stagnantfor almost 20 years, this has changed with the adventof advancements in several areas, including catheter-based delivery systems, miniaturized high-densityenergy sources, low-power electronics, novel pack-aging capabilities, and novel communication tech-nologies. In this review, we strive to summarize thecurrent state of the 2 basic designs of leadless cardiacpacemakers (LCPs). One design uses 2 separate com-ponents, an endocardial pacing electrode and a sub-cutaneous energy transmitter, whereas the seconddesign is a completely self-contained device in whichthe pulse generator and pacing electrode are a singlecomponent.
MULTICOMPONENT (NOT SELF-CONTAINED)
LEADLESS PACING
ULTRASOUND-MEDIATED ENERGY TRANSFER.
Recently, the results of WiSE-CRT (Wireless Stimula-tion Endocardially for CRT), a prospective observa-tional feasibility study of leadless ultrasound-basedendocardial left ventricular pacing in patients withguideline-directed indication for cardiac resynchro-nization therapy (CRT) were reported (12). TheWiSE-CRT study used a system intended for chronicuse with 2 components: a subcutaneous pulse ge-nerator and a small receiver electrode. The subcu-taneous pulse generator was surgically implanted inthe left lateral thorax (subcutaneous) and generatedultrasonic acoustic energy; the small receiver elec-trode was implanted directly onto the left ven-tricular endocardium (using a retrograde aorticapproach) and converted the acoustic energy toelectric pacing pulses (13). All patients in WiSE-CRThad existing implantable cardiac devices (pace-makers or defibrillators) and were consideredeligible for enrollment if they: 1) had undergoneprior failed coronary sinus lead implantation; 2) hadundergone previously successful placement of acoronary sinus lead but were clinical nonresponders;or 3) required an upgrade to a CRT system (12,14).From an efficacy perspective, the results of WiSE-CRT were promising: left ventricular functionimproved at 6 months (mean pre-implantation left
ventricular ejection fraction of 25 � 4.0% vs. mean6-month post-implantation ejection fraction of 31 �7.0%; p < 0.01). However, the study was terminatedprematurely for safety reasons. Of the 17 patientsenrolled (of an intended 100 patients), the devicecould be successfully implanted in only approxi-mately three-quarters (n ¼ 13 [76%]). Most impor-tant, 3 patients (18%) developed serious procedure-related pericardial effusions due to either deliverysheath or guidewire manipulation; 1 of these resul-ted in a patient’s death. Additionally, 2 patients(11%) required revision of the transmitter positionbecause of loss of biventricular pacing, and in 1patient, there was unexpected depletion of thebattery.
After WiSE-CRT was terminated because of safetyconcerns, the delivery system was redesigned topermit atraumatic implantation of the receiver elec-trode onto the left ventricular endocardial surface.Similar to that studied in WiSE-CRT, the redesignedleadless system is also composed of an implantedbattery-powered ultrasonic transmitter and a leadlesspacing electrode implanted directly onto the leftventricular endocardium (Figure 1). Again, the systemdetects a right ventricular pacing pulse from a coim-planted pacemaker or defibrillator and delivers ul-trasonic energy to the electrode, which transducesthe energy to an electric pacing pulse to stimulate theleft ventricle synchronously with the right ventricle.The initial evaluation of this redesigned system in theSELECT-LV (Safety and Performance of ElectrodesImplanted in the Left Ventricle) study revealed: 1)adequate acoustic windows to permit implantation inthe majority of patients (12 of 14 [86%]); 2) significantcardiac resynchronization in all 12 implanted pa-tients, with QRS shortening by 60 � 24 ms (vs. rightventricular pacing); and, importantly, 3) no instancesof intraprocedural adverse events (15). The SELECT-LV trial continues to enroll patients at multiplecenters in Europe.
Although the initial SELECT-LV data suggest thatthe delivery system modifications have largely ad-dressed the major procedural complication observedin WiSE-CRT, there remain several technology-specific concerns that require consideration. First,although the left ventricular receiver component ofthis system is indeed leadless, the system doesrequire the use of conventional transvenous leads,because all patients required concomitant conven-tional implantable right ventricular pacing devices.Second, it is theoretically possible that long-termultrasound energy exposure to subcutaneous ormyocardial tissue in humans may have unintendedadverse consequences. Third, there may be untoward

FIGURE 1 The Leadless Endocardial Left Ventricular Pacing System
Anteroposterior (AP) (A) and lateral (LAT) (B) chest radiograph views of the implanted system, including battery, transmitter, and receiver/
pacing electrode (inset).
J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5 Miller et al.S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9 Leadless Cardiac Pacing
1181
effects of external (environmental) interference andchanges in the acoustic window on the system’ssensing or pacing performance. In some patients, theavailability of an adequate acoustic window maylimit the response to resynchronization therapy,because of either the location of the endocardialreceiver electrode (anterolateral or lateral-apical) orthe target location of the transmitter (intercostalspace, because acoustic energy is refracted by bone).Fourth, compared with conventional power sources,energy transfer of current ultrasound-mediatedpacing systems is inefficient and might result in acomparatively short battery life (16,17). In fact, inWiSE-CRT, at the 6-month post-implantation follow-up visit, the remaining battery life projection was amean of 18 months (range: 9 to 42 months). Finally,the endoluminal left ventricular positioning of thereceiver electrode could predispose to thromboem-bolic complications. Indeed, in SELECT-LV, 1 patientwith atrial fibrillation in whom oral anticoagulationwas interrupted for the procedure sustained a stroke.In subsequent cases, oral anticoagulation was notinterrupted (at operator discretion) for the procedure,and no subsequent strokes were observed; however,the safety of this strategy needs to be validated in alarger cohort of patients. However, it should be notedthat in a study that used a different approach to leftventricular endocardial pacing (using a transseptalapproach), 14% patients (7 of 51) experienced throm-boembolic events (stroke or transient ischemicattack) during follow-up (18). However, most of these
patients had subtherapeutic anticoagulation at thetime of the event (the goal international normalizedratio was 3.5 to 4.5), and this risk would certainly beexpected to be less with the smaller volume leadlesselectrodes associated with the multicomponent sys-tems. However, this potential for thromboemboliccomplications remains important to test in largeclinical trials.
However, there are compelling data indicating apotentially significant clinical benefit to leadless leftventricular endocardial pacing. Endocardial left ven-tricular pacing is more physiological (endocardial-to-epicardial transmural activation sequence), mayenhance left ventricular diastolic and systolic perfor-mance, has the potential to be less proarrhythmic(reduced dispersion of ventricular repolarization), andlikely requires lower pacing energy outputs comparedwith optimally placed coronary sinus leads (19,20).Furthermore, because it is not limited to those coro-nary sinus branches able to accommodate a trans-venous lead, endocardial pacing offers a larger choiceof optimal left ventricular stimulation sites; there isalso the added benefit of no phrenic nerve stimulation.Leadless left ventricular endocardial pacing mightmitigate these limitations and expand our ability toprovide optimal CRT. However, there are other vari-ables, such as endocardial scar and adjacent struc-tures, including the papillary muscles, that may affectthe ability to pace at the optimal endocardial location(21). Finally, and most important, 2 independent ran-domized controlled trials, TARGET (Targeted Left

FIGURE 2 The Single-Component (Fully Self-Contained)Leadless Pacemakers
The Micra Transcatheter Pacing System (left) and Nanostim
leadless cardiac pacemaker (right) are shown next to a ruler.
Miller et al. J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5
Leadless Cardiac Pacing S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9
1182
Ventricular Lead Placement to Guide CardiacResynchronization Therapy) and STARTER (SpeckleTracking Assisted Resynchronization Therapy forElectrode Region), demonstrated that better targetingof the left ventricular pacing site (at the site of latestcontraction or ventricular activation) leads to im-provements in clinical response, including freedomfrom heart failure hospitalization or mortality (22,23).Indeed, because of these various potential advantagesto left ventricular endocardial pacing, several in-vestigators have attempted left ventricular endocar-dial pacing with standard transvenous leads (placedtransseptally across the mitral valve directly into theleft ventricle) for nonresponders or those with inac-cessible coronary sinus anatomy. Although technicallyfeasible, its widespread adoption has been limitedby the complexity of the procedure, the need foraggressive chronic oral anticoagulation (with a rec-ommended target international normalized ratio of3.5 to 4.5), and potential adverse consequences, suchas the long-term effect on the mitral valve (24).Leadless left ventricular endocardial pacing mightmitigate these risks and expand our ability to provideoptimal CRT.
INDUCTION TECHNOLOGY. Leadless pacing usinginduction (electromagnetic) technology also consistsof at least 2 components: a subcutaneous (or sub-muscular) transmitter unit located just above theheart and a receiver unit implanted into the ventric-ular endocardium (25). Briefly, the transmitter gen-erates an alternating magnetic field, of which afraction is converted to stimulatory voltage pulsesby the receiver unit. Although leadless pacing usinginduction may be feasible, it has been tested onlyin animal models (porcine and goat), and furtherwork is needed to determine the effects of align-ment, distance, and external interferences on thistechnology (26).
SINGLE-COMPONENT
(FULLY SELF-CONTAINED) LEADLESS PACING
With single-component LCPs, the pulse generator andsensing/pacing electrodes are fully contained withina single unit, thereby eliminating the leads, pectoralsurgical pockets, and intrasystem connections. Thedevice is delivered to the right ventricle with a cath-eter through the femoral vein. At present, 2 types ofsingle-unit leadless pacemakers have been implantedin humans: the Nanostim LCP (St. Jude Medical, Inc.,St. Paul, Minnesota) and, more recently, the MicraTranscatheter Pacing System (TPS) (Medtronic, Inc.,Minneapolis, Minnesota).
The LCP has CE Mark approval for European usebut remains investigational in the United States,whereas the TPS is investigational in both Europeand the United States. Comparatively, the TPS (25.9 �6.7 mm) is shorter but wider than the LCP (42 �5.99 mm); accordingly, the outer diameter of the de-livery sheath for the TPS is larger (24-F) than that forthe LCP (18-F). Of course, both devices are signifi-cantly smaller than conventional single-chambertransvenous pacemakers (approximately one-tenththe volume); this size discrepancy is further accen-tuated by the fact that the volume displacedby the pacing lead is typically not factored intothese comparisons. Examples of both devices areshown in Figure 2, and the 2 devices are comparedin Table 1.
With regard to fixation mechanisms, the LCP usesan active screw-in helix and a secondary fixationmechanism consisting of 3 angled nitinol tinesperpendicular to the helix, whereas the TPS uses 4self-expanding nitinol tines to affix to the myocar-dium. Figure 3 shows an example of an implantationof an LCP that was repositioned acutely prior to beingdisconnected from the delivery catheter; it was then

TABLE 1 Characteristics of the LCP and TCP
Parameter LCP TCP
Polarity Bipolar Bipolar
Pacing modes VVI (R) VVI (R)
Rate modulation mechanism Blood temperature 3-axis accelerometer
Battery technology Lithium carbon monofluoride Lithium silver vanadiumoxide / carbon monofluoride
Programmer St. Jude Medical, model 3650 Medtronic, model 2090
Energy capacity (mAh) 248 120
Estimated longevity
ISO standard, yrs* 9.8 yrs 4.7 yrs
Alternative setting, yrs† 14.7 yrs 9.6 yrs
Size (h � w), maximumthickness, mm
42 mm � 5.99 mm 25.9 mm � 6.7 mm
Volume (cc) 1.0 0.8
Fixation mechanism Helix (screw-in) Tines
*Longevity based on fixed programming at the ISO International Organization for Standardization (ISO 14708)standard guidelines for reporting pacemaker battery duration longevity: 2.5 V, 0.4 ms, 600 U, 60 beats/min,and 100% pacing. †Longevity based on nominal settings (for the TCP): 1.5 V, 0.24 ms, 60 beats/min (with animpedance load of 500 ohms and 100% pacing).
LCP ¼ leadless cardiac pacemaker; TCP ¼ transcatheter pacing system.
J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5 Miller et al.S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9 Leadless Cardiac Pacing
1183
positioned at an alternative apical septal location toachieve stable and durable sensing and pacing pa-rameters. Figure 4 shows an example of the protectivesleeve, fixation mechanism, and bipolar sensing andpacing configuration of the TPS. Both devices usea tethering mechanism to maintain a connectionbetween the delivery catheter and the device to testpositional integrity before final deployment. Figure 5shows an example of a TPS implantation. Finally,both devices are reportedly retrievable, although onlyanimal data with the LCP exist to demonstrate thefeasibility of chronic extraction. Figure 6 shows fluo-roscopic images from a clinical case of acute retrievalof an LCP that had been inadvertently implanted inthe left ventricle (through a patent foramen ovale). Tominimize the possibility of inadvertent placement ofthe device into the left ventricle through a patentforamen ovale, left anterior oblique fluoroscopicimaging should be performed prior to device release.
The LEADLESS trial, a first-in-human, single-arm,multicenter study of the safety and clinical perfor-mance of the LCP, was recently reported (27).Briefly, patients were considered eligible if they hadindications for single-chamber, right ventricularpacing (VVI [R]). Indications included: 1) perma-nent atrial fibrillation with atrioventricular block(including atrial fibrillation with a slow ventricularresponse); 2) normal sinus rhythm with second- orthird-degree atrioventricular block with a low levelof physical activity or short expected life span; and3) sinus bradycardia with infrequent pauses or un-explained syncope with electrophysiologic findings.Exclusion criteria comprised pacemaker de-pendency, significant pulmonary hypertension, orpre-existing mechanical tricuspid valve prosthesis,pacemaker/defibrillator leads, or inferior vena cavafilter. Thirty-three patients were enrolled in theLEADLESS trial. The implantation success rate was97% (32 of 33 patients), the mean procedure durationwas 28 � 17 min, and the overall complication-freerate was 94% (31 of 33 patients). The 2 complica-tions were right ventricular perforation/cardiactamponade (the patient subsequently died of astroke) and inadvertent placement of the devicethrough a patent foramen ovale (the device wasretrieved in the same procedure, and no disabilityresulted). After 3 months of follow-up, all measuresof pacing performance (lead impedance, pacing, andsensing threshold) either improved or were stablywithin the acceptable range.
The 1-year follow-up results of the LEADLESS trialwere recently reported and demonstrated that: 1)performance measures (pacing threshold, impedance,and sensing) remained stable; 2) there were further
no complications related to the device (beyond theindex procedure); 3) there were no premature batterydepletions or under/oversensing issues; and 4)adequate rate response, defined as 80% of the pre-dicted maximal heart adjusted for age, was observedin those patients for whom it was activated (n ¼ 19 of30) (28). LEADLESS II is a large (n ¼ 600) prospective,nonrandomized, single-arm, multicenter trial thathas recently begun to assess the clinical safety andeffectiveness of the LCP. This trial is intended toprovide sufficient safety and long-term effectivenessdata to gain U.S. Food and Drug Administration reg-ulatory approval. Similarly, a single-arm, multicenterclinical trial assessing the TPS is also ongoing, andalthough no results are yet available, the in-vestigators intend to enroll up to 780 patients. Again,these data will be used to support Food and DrugAdministration approval.
The early results of the Micra Transcatheter PacingSystem Study, a prospective, multicenter, single-armtrial were recently reported. Similar to the LEADLESStrial, patients were eligible if they had a Class I or IIindication for single-chamber right ventricular pac-ing. The device was successfully implanted in allpatients (n ¼ 140 implanted patients). With regards toearly safety performance, 26 patients (18.6%) expe-rienced either a protocol-defined procedure or sys-tem-related adverse event, including 4 patients withtransient atrioventricular block, 2 with ventriculartachycardia, 1 with ventricular fibrillation and 1 withpericardial effusion without tamponade. There wereno procedure-related deaths or unanticipated serious

FIGURE 3 Implantation of the LCP
(A) The delivery catheter and leadless cardiac pacemaker (LCP) positioning in the right ventricular (RV) apex in the right anterior oblique (RAO)
view (contrast injection through the delivery sheath). (B) Positional integrity testing with traction applied to the LCP (tug test), while the device
remains tethered to the delivery catheter. After this maneuver, it was noted that the R waves declined from a baseline of 8.0 to 3.0 mV.
Accordingly, the LCP was redocked, and a new position was chosen (higher on the apical septum). (C) Delivery catheter and LCP positioning at
the RV apical septum (contrast injection through delivery sheath). (D) Final positioning of the LCP in the RAO view. At this location, the R waves
remained stable (>12.0 mV) at the end of the procedure and through 6 months of follow-up.
Miller et al. J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5
Leadless Cardiac Pacing S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9
1184
adverse device events. With regards to early efficacy(n ¼ 60 patients, who had been followed for 3months), as compared to baseline, the mean electricalvalues for R-wave sensing amplitude, pacing imped-ance, and pacing capture threshold were stable at3-months. The full trial results (n ¼ 720 implantedpatients) are anticipated in 2016 (29).
POTENTIAL BENEFITS OF
LEADLESS CARDIAC PACING
As its name implies, the most obvious potentialbenefit of leadless cardiac pacing is the absence of atransvenous lead. Because the majority of acute andchronic complications of conventional pacemakersare attributable to the transvenous lead, a system that
eliminates this component is desirable (30). In addi-tion to mitigating the risk of well-recognized com-plications, such as lung injury during subclavianaccess or chronic venous occlusion, there is alsothe inherent benefit of preventing intrasystemconnection errors (albeit an uncommon cause ofacute procedural complications), because the pulsegenerator pace/sense electrodes are a single unit.The single-component systems do not require a sur-gical incision/subcutaneous pocket, which mitigatesthe risk of surgical complications and may provide amore favorable cosmetic profile.
Despite their smaller size, LCPs have projectedbattery longevity that is comparable to that ofstandard single-chamber transvenous pacemakers.One of the most important determinants of battery

FIGURE 4 Fixation Mechanism of the Transcatheter Pacing System
Protective Sleeve BeingWithdrawn –Tines Extending
Tines Completely Retroflexed –Micra Still In Sheath
Sleeve Withdrawn –Micra Remains Tethered atDelivery Tool Interface
Tines
The sequence of images demonstrates the deployment of the tines as the pacemaker exits
the delivery sheath.
J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5 Miller et al.S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9 Leadless Cardiac Pacing
1185
longevity is the internal current drain. The currentdrain for the LCP is only approximately 1 mA, whichis significantly less than for a standard single-chamber transvenous pacemaker (6.24 mA) from thesame manufacturer (31–33). Additional factors ac-counting for the extended longevity of the leadlesspacemakers include the lack of “lost” energythrough the lead, the high-density lithium carbonmonofluoride battery, and, importantly, for the LCP,the use of energy-efficient conductive (vs. inductive)telemetry.
The battery life of the TCP, based on the Inter-national Organization for Standardization (ISO)standard for reporting battery longevity (2.5 V, 0.4ms, 600 U, 60 beats/min, and 100% pacing) isapproximately one-half that of the LCP (Table 1)largely because: 1) its smaller form factor also re-sults in less battery capacity (248 vs. 120 mAh); and2) instead of conductive telemetry, it employs radi-ofrequency telemetry which results in a greaterbackground current drain. However, the TCP em-ploys various energy-efficient approaches to mini-mize battery drain, such as capture management,which would increase battery longevity. As anexample, the projected battery life for the TCP at thenominal settings (1.5 V, 0.24 ms, 60 beats/min withan impedance load of 500 ohms and 100% pacing)increases to 9.6 years. In comparison, the LCP deviceat the same settings has a projected battery life of14.7 years. Finally, it should be also noted that theenergy efficiency of both the LCP and TCP are partlyrelated to the fewer enhancements (e.g., electrogram
FIGURE 5 Implantation of the Transcatheter Pacing System
(A) The delivery sheath and pacemaker positioned at the right ventricul
(C) Positional integrity testing (tug test), while maintaining the connect
storage) in these devices, as compared with con-ventional pacemakers.
The power source of the TPS device is lithium-silver vanadium oxide/carbon monofluoride, com-monly used in transvenous systems. A high-density
ar apex. (B) Tines have been exposed, and the cathode has engaged with the myocardium.
ion between the pacemaker and the delivery sheath. RAO ¼ right anterior oblique.

FIGURE 6 Retrieval of a Deployed LCP Device
The leadless cardiac pacemaker (LCP) had been inadvertently deployed within the left ventricle through a patent foramen ovale and thus required removal. (A) A trilobed
retrieval snare was advanced through the patent foramen ovale, across the mitral valve, and looped around the body of the LCP within the left ventricle. (B) The trilobed
snare was secured to the docking port on the distal end of the LCP. (C) After re-engagement of the delivery catheter to the docking port, the delivery sheath was drawn
back over the LCP. Subsequently, the LCP was unscrewed from the myocardium and removed from the left ventricle, and a new LCP was placed in the right ventricle.
Miller et al. J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5
Leadless Cardiac Pacing S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9
1186
lithium carbon monofluoride battery powers the LCP.Although this is an ideal power source for miniatur-ized leadless pacemakers because of its high energycapacity, prior applications were limited by concernsfor abrupt end-of-service characteristics. However,technological developments (including a proprietary-algorithm fuel gauge to accurately predict theremaining energy capacity of the cell) have ensuredthat that the leadless pacemaker conforms to the In-ternational Organization for Standardizationrequirement that the device provide pacing functionfor at least 6 months from the recommendedreplacement time to end of service (34,35). The LCPand TPS are also believed to be safe for use withmagnetic resonance imaging (conditionally), becauseof their lack of ferrous material; however, additionalpre-clinical and clinical testing is necessary toconfirm this. Finally, because of the greater distancebetween the radiograph source and the operator(located at the femoral insertion site) during LCPimplantation, there is potentially less radiationexposure for the implanting physician. However,there are currently no comparisons in total radiationexposure between leadless pacemaker implants andconventional transvenous systems.
POTENTIAL LIMITATIONS OF
LEADLESS CARDIAC PACING
For the current generation of single-unit LCPs,the most important limitation is their ability toperform only single-chamber pacing, specifically
right ventricular pacing. Therefore, these deviceswould not be appropriate for most patients withsinus node dysfunction, who derive significantclinical benefit from dual-chamber sensing/pacing(30). Although multichamber systems (atrioventric-ular and biventricular) are in development, thereare currently no available data on the feasibility ofthese systems. Device-device communication andfixation mechanisms (in the morphologicallydistinct right atrium) are just a few of the chal-lenges that must be overcome before multicom-ponent systems can become a reality (CentralIllustration). To our knowledge, there have notbeen any chronic device embolizations with single-component systems, but this remains a potentialsource of concern. The optimal fixation mechanism,with regard to both chronic performance and theneed for future extraction, remains to be seen. Thelong-term reliability and accuracy of rate-responsivefeatures, now that the sensor has been relocatedfrom the subcutaneous pulse generator to the intra-ventricular space, is not yet known. However, theongoing LEADLESS II trial is assessing rate-responsecharacteristics (as a secondary endpoint) in a seriesof patients undergoing graded exercise testing.Furthermore, although the single-component sys-tems are, by volume, significantly smaller thanconventional cardiac pacemakers, the portion of thedevice that interacts with the endocardium has awider diameter, which has raised the possibility ofproarrhythmia. The delivery system for single-unitleadless pacemakers includes a large venous sheath
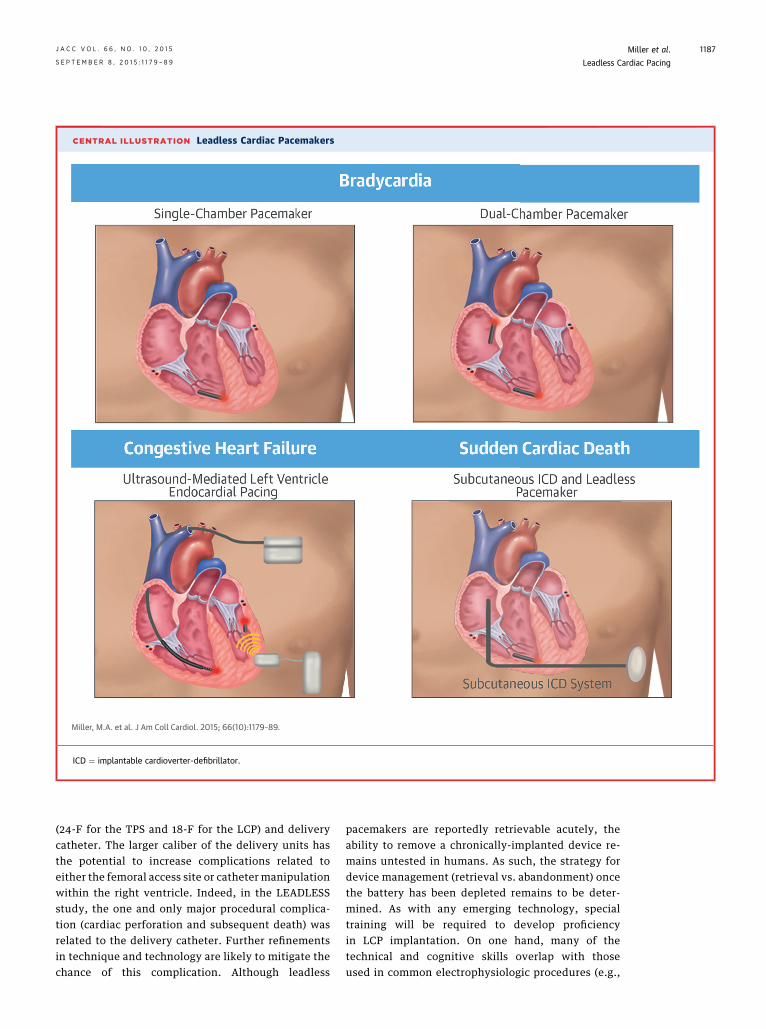
CENTRAL ILLUSTRATION Leadless Cardiac Pacemakers
Miller, M.A. et al. J Am Coll Cardiol. 2015; 66(10):1179–89.
ICD ¼ implantable cardioverter-defibrillator.
J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5 Miller et al.S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9 Leadless Cardiac Pacing
1187
(24-F for the TPS and 18-F for the LCP) and deliverycatheter. The larger caliber of the delivery units hasthe potential to increase complications related toeither the femoral access site or catheter manipulationwithin the right ventricle. Indeed, in the LEADLESSstudy, the one and only major procedural complica-tion (cardiac perforation and subsequent death) wasrelated to the delivery catheter. Further refinementsin technique and technology are likely to mitigate thechance of this complication. Although leadless
pacemakers are reportedly retrievable acutely, theability to remove a chronically-implanted device re-mains untested in humans. As such, the strategy fordevice management (retrieval vs. abandonment) oncethe battery has been depleted remains to be deter-mined. As with any emerging technology, specialtraining will be required to develop proficiencyin LCP implantation. On one hand, many of thetechnical and cognitive skills overlap with thoseused in common electrophysiologic procedures (e.g.,

Miller et al. J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5
Leadless Cardiac Pacing S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9
1188
fluoroscopic imaging, manipulation and implantationof devices within the right ventricle); on the otherhand, additional skills will undoubtedly requirefurther proctoring/training (e.g., large venoussheaths, intraprocedural positional integrity testing).Future clinical competency statements will likelyaddress this matter (36).
CONCLUSIONS
As with any transformative technology, a number ofquestions remain unanswered with each of theseleadless pacing systems. Randomized clinical trialswill be necessary to definitively determine whether
the theoretical benefits of leadless systems will besuperior to those of conventional pacemakers bothfrom a safety perspective (fewer acute and chroniccomplications) and in terms of long-term pacing andsensing performance. However, it certainly seemspossible that the future of cardiac pacing will see theminimization, if not eventual extinction, of all pacingleads.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Vivek Y. Reddy, Helmsley Electrophysiology Center,Icahn School of Medicine, One Gustave L. LevyPlace, Box 1030, New York, New York 10029. E-mail:[email protected].
RE F E RENCE S
1. Lown B, Kosowsky BD. Artificial cardiac pace-makers. I. N Engl J Med 1970;283:907–16.
2. Beck H, Boden WE, Patibandla S, et al. 50thanniversary of the first successful permanentpacemaker implantation in the United States: his-torical review and future directions. Am J Cardiol2010;106:810–8.
3. Nathan DA, Center S, Wu CY, et al. Animplantable synchronous pacemaker for the longterm correction of complete heart block. Am JCardiol 1963;11:362–7.
4. Mallela VS, Ilankumaran V, Rao NS. Trends incardiac pacemaker batteries. Indian Pacing Elec-trophysiol J 2004;4:201–12.
5. van Rees JB, de Bie MK, Thijssen J, et al.Implantation-related complications of implantablecardioverter-defibrillators and cardiac resynchro-nization therapy devices: a systematic review ofrandomized clinical trials. J Am Coll Cardiol 2011;58:995–1000.
6. Klug D, Balde M, Pavin D, et al. Risk factorsrelated to infections of implanted pacemakersand cardioverter-defibrillators: results of alarge prospective study. Circulation 2007;116:1349–55.
7. Hauser RG, Hayes DL, Kallinen LM, et al.Clinical experience with pacemaker pulse gener-ators and transvenous leads: an 8-year prospec-tive multicenter study. Heart Rhythm 2007;4:154–60.
8. Korkeila P, Nyman K, Ylitalo A, et al. Venousobstruction after pacemaker implantation. PacingClin Electrophysiol 2007;30:199–206.
9. Wiegand UK, Bode F, Bonnemeier H, et al.Long-term complication rates in ventricular, singlelead VDD, and dual chamber pacing. Pacing ClinElectrophysiol 2003;26:1961–9.
10. Kirkfeldt RE, Johansen JB, Nohr EA, et al.Complications after cardiac implantable electronicdevice implantations: an analysis of a complete,nationwide cohort in Denmark. Eur Heart J 2014;35:1186–94.
11. Sutton R. The first European journal on cardiacelectrophysiology and pacing, the European
Journal of Cardiac Pacing and Electrophysiology.Europace 2011;13:1663–4.
12. Auricchio A, Delnoy PP, Butter C, et al., forthe Collaborative Study Group. Feasibility,safety, and short-term outcome of leadlessultrasound-based endocardial left ventricularresynchronization in heart failure patients: re-sults of the Wireless Stimulation Endocardiallyfor CRT (WiSE-CRT) study. Europace 2014;16:681–8.
13. Auricchio A, Delnoy PP, Regoli F, et al., for theCollaborative Study Group. First-in-man implan-tation of leadless ultrasound-based cardiac stim-ulation pacing system: novel endocardial leftventricular resynchronization therapy in heartfailure patients. Europace 2013;15:1191–7.
14. Lee KL, Tse HF, Echt DS, et al. Temporaryleadless pacing in heart failure patients withultrasound-mediated stimulation energy and ef-fects on the acoustic window. Heart Rhythm2009;6:742–8.
15. Reddy V, Sedivy P, Mraz T, et al. Wireless LVendocardial stimulation for cardiac resynchroni-zation: initial experience from the SELECT-LVStudy (abstr). Heart Rhythm 2014;11 Suppl:S41.
16. Van Gelder BM, Bracke FA, Oto A, et al.Diagnosis and management of inadvertentlyplaced pacing and ICD leads in the left ventricle:a multicenter experience and review of theliterature. Pacing Clin Electrophysiol 2000;23:877–83.
17. Benditt DG, Goldstein M, Belalcazar A. Theleadless ultrasonic pacemaker: a sound idea? HeartRhythm 2009;6:749–51.
18. Rademakers LM, van Gelder BM, Scheffer MG,et al. Mid-term follow up of thromboemboliccomplications in left ventricular endocardial car-diac resynchronization therapy. Heart Rhythm2014;11:609–13.
19. Bordachar P, Ploux S, Lumens J. Endocardialpacing: the wave of the future? Curr Cardiol Rep2012;14:547–51.
20. Mihalcz A, Kassai I, Geller L, et al. Alternativetechniques for left ventricular pacing in cardiac
resynchronization therapy. Pacing Clin Electro-physiol 2014;37:255–61.
21. Spragg DD, Dong J, Fetics BJ, et al. Optimalleft ventricular endocardial pacing sites for cardiacresynchronization therapy in patients withischemic cardiomyopathy. J Am Coll Cardiol 2010;56:774–81.
22. Khan FZ, Virdee MS, Palmer CR, et al. Targetedleft ventricular lead placement to guide cardiacresynchronization therapy: the TARGET study: arandomized, controlled trial. J Am Coll Cardiol2012;59:1509–18.
23. Saba S, Marek J, Schwartzman D, et al. Echo-cardiography-guided left ventricular lead place-ment for cardiac resynchronization therapy:results of the Speckle Tracking Assisted Resynch-ronization Therapy for Electrode Region trial. CircHeart Fail 2013;6:427–34.
24. Whinnett Z, Bordachar P. The risks and bene-fits of transseptal endocardial pacing. Curr OpinCardiol 2012;27:19–23.
25. Wieneke H, Konorza T, Erbel R, et al. Leadlesspacing of the heart using induction technology: afeasibility study. Pacing Clin Electrophysiol 2009;32:177–83.
26. Wieneke H, Rickers S, Velleuer J, et al. Lead-less pacing using induction technology: impact ofpulse shape and geometric factors on pacing ef-ficiency. Europace 2013;15:453–9.
27. Reddy VY, Knops RE, Sperzel J, et al. Perma-nent leadless cardiac pacing: results of theLEADLESS Trial. Circulation 2014;129:1466–71.
28. Knops RE, Tjong FV, Neuzil P, et al. Chronicperformance of a leadless cardiac pacemaker:1-year follow-up of the LEADLESS trial. J Am CollCardiol 2015;65:1497–504.
29. Ritter P, Duray GZ, Steinwender C, et al. Earlyperformance of a miniaturized leadess cardiacpacemaker: the Micra Transcatheter Pacing Study.Eur Heart J 2015 [E-pub ahead of print].
30. Gillis AM, Russo AM, Ellenbogen KA, et al.HRS/ACCF expert consensus statement on pace-maker device and mode selection. J Am Coll Car-diol 2012;60:682–703.

J A C C V O L . 6 6 , N O . 1 0 , 2 0 1 5 Miller et al.S E P T E M B E R 8 , 2 0 1 5 : 1 1 7 9 – 8 9 Leadless Cardiac Pacing
1189
31. Berger T, Roithinger FX, Antretter H, et al. Theinfluence of high versus normal impedance ven-tricular leads on pacemaker generator longevity.Pacing Clin Electrophysiol 2003;26:2116–20.
32. de Voogt WG. Pacemaker leads: performanceand progress. Am J Cardiol 1999;83 Suppl:187D–91D.
33. Markewitz A, Kronski D, Kammeyer A, et al.Determinants of dual chamber pulse generatorslongevity. Pacing Clin Electrophysiol 1995;18:2116–20.
34. Mond HG, Freitag G. The cardiac implantableelectronic device power source: evolution and rev-olution.PacingClinElectrophysiol2014;37:1728–45.
35. Bock DC, Marschilok AC, Takeuchi KJ, et al.Batteries used to power implantable biomedicaldevices. Electrochim Acta 2012;84:155–64.
36. Tracy CM, Akhtar M, DiMarco JP, et al.American College of Cardiology/American HeartAssociation 2006 update of the clinical compe-tence statement on invasive electrophysiologystudies, catheter ablation, and cardioversion: a
report of the American College of Cardiology/American Heart Association/American College ofPhysicians Task Force on Clinical Competence andTraining developed in collaboration with theHeart Rhythm Society. J Am Coll Cardiol 2006;48:1503–17.
KEY WORDS brachycardia,cardiac resynchronization therapy,electrophysiology