lec 9 nutrition in developing countries
TRANSCRIPT

Dr Siham Gritly 1
Community and Public Health Nutrition 10-Nutrition in Developing Countries
Prepared by;
Dr. Siham M.O. Gritly

Dr Siham Gritly 2
Glossary
• Poverty; The state of being extremely poor. The state of being inferior in quality or insufficient in amount or the state or condition of having little or no money, goods, or means of support; condition of being poor.
• hunger; a craving or urgent need for food or a specific nutrient or an uneasy sensation occasioned by the lack of food
• Or hunger: consequence of food insecurity that, because of prolonged, involuntary lack of food, results in discomfort, illness, weakness, or pain that goes beyond the usual uneasy sensation

Dr Siham Gritly 3
• food poverty: hunger resulting from inadequate access to available food for various reasons, including inadequate resources, political obstacles, social disruptions, poor weather conditions, and lack of transportation
• famine: widespread and extreme scarcity of food in an area that causes starvation and death in a large portion of the population.
• oral rehydration therapy (ORT): the administration of a simple solution of sugar, salt, and water, taken by mouth, to treat dehydration caused by diarrhea. A simple
• ORT recipe:• • ½ L boiling water• • 4 tsp sugar• • ½ tsp salt
Dr Siham Gritly 4
• Sustainable development is the development that "meets the needs of the present without compromising the ability of future generations to meet their own needs."
• food security: access to enough food to sustain a healthy and active life.
• food insecurity: limited or uncertain access to foods of sufficient quality or quantity to sustain a healthy and active life.
• food insufficiency: an inadequate amount of food due to a lack of resources.
Dr Siham Gritly 5
Developed vs. developing countries
• Developed countries mainly depend on industries while Developing countries should struggle for integrated rural development with the sustainable agricultural development and the promotion of economic activities.
• sustainable agriculture: ability to produce food indefinitely, with little or no harm to the environment.

Dr Siham Gritly 6
• Kramer, (2003) pointed out that disparities between developed and developing countries highlighted by;
• maternal mortality,• infant mortality, • stillbirth • and low birth weight

Dr Siham Gritly 7
The double burden of diseases in the developing world
• WHO indicated that;• Hunger and malnutrition remain among the most
devastating problems facing the majority of the world’s poor and needy people
• The root causes of malnutrition include;• poverty and inequity.
• Eliminating these causes requires political and social action

Dr Siham Gritly 8
Poverty is main characteristic of developing countries
What is poverty• Poverty refers to the condition of not having
the means to afford basic human needs such as• Clean water• Balance nutrition (quantity and quality)• Health care• clothing and shelter.
Dr Siham Gritly 9
poverty is derived in collective terms at three dimensions:
• incidence of poverty (percent of individuals out of the total sample whose incomes are insufficient to attain the minimum energy level),
• depth (intensity) of poverty (meaning how far is the poor group from reaching the minimum energy level),
• and the severity of poverty (energy inequality within the poor group).

Dr Siham Gritly 10
• Each of these dimensions might require a different policy action
• the most widely used poverty measure is poverty incidence; also known as headcount ratio.

Dr Siham Gritly 11
Poverty line
• Poverty line is defined as expenditure required for daily Calorie intake of 2.400 per person in rural areas and 2000 Calories in urban areas
• Poverty is the main cause of;• Low expectancy• Low birth weight• High maternal mortality

Dr Siham Gritly 12
• Under five years of age mortality• Handicap and disability• Stress and mental illness• Suicide• Family disintegration • Drug use and crime

Dr Siham Gritly 13
Human Development Index (HPI).
• HDI Defined as; a composite (complex) index combining indicators representing three dimensions;
• 1-longevity (the expectancy at birth) long life• 2-knowledge (adult literacy rate and mean year of
schooling) knowledgeable• 3-income (real GDP Gross Domestic Product per
capita in purchasing power parity in US dollars) high standard of life
• GDP is gross income generated within the country excluded net income received from abroad

Dr Siham Gritly 14
• The human development index provides a more comprehensive picture of human life than income does
• The HDI ranges between 0-1• The HDI value for a countries shows the
distance that it has already travelled to words maximum possible value to 1 and allows comparisons

Dr Siham Gritly 15
• To construct the index, maximum and minimum values have been established for each of the indicators
• 1-life expectancy at birth- 25 and 85 years• 2- adult literacy rate- 0 percent and 100
percent• 3-GDP per capita; $ 100 and $ 40.000

Dr Siham Gritly 16
Human Poverty Index (HPI).
• 1997 another term Human Poverty Index was introduced • The HPI assesses levels and progress using a concept of
development much broader than that allowed by income alone (Human Development Report 2010).
• The human Poverty Index measures deprivation in human development needs (health, education and income)
• 1-longevity• 2-knowledge• 3-income

Dr Siham Gritly 17
Nutrition in developing countries
• UNFPA reported that there are some factors contributing to the poor health status among African population.
• These factors include • malnutrition, • lack of sanitation especially drinking water, and
absence of health care during pregnancy, • uncontrolled fertility, • illegal abortion • and low education.

Dr Siham Gritly 18
Food production and food security
• Food production can influenced by factors such as;
• pests, • Climatic variations,• prices, • availability of agricultural inputs and farmers'
ability to obtain them, • political stability and• peace

Dr Siham Gritly 19
• Most food in the world comes from;
• cereals.
• The second largest amount of food comes from root crops,
• followed by legumes or pulses.

Dr Siham Gritly 20
Food availability; the role of agriculture sector in developing countries
• The main objectives of agricultural sectors is to;
• provide balance and adequate diet for all the member of the community Expanding agricultural efforts to increase and improve food production
• to have to understand the needs of human and how to overcome the problems of malnutrition,
• job opportunities for huge number of the society, increase the income of rural families through greater production of cash crops so agriculture is very related to human nutrition.

Dr Siham Gritly 21
To improve nutrition, agricultural planners should aim to;
• expand the production of staple cereals and legumes
• should promote consumption of fruits, vegetables, oilseeds and
• livestock products or those of small animal husbandry.

Dr Siham Gritly 22
Access to food (food demand)
• Access to food, or food demand, is influenced by;
• economic issue,• physical infrastructure and• consumer preferences.

Dr Siham Gritly 23
food security
• Food security defined as; "access by all people at all times to enough food (quality and quantity) required for an active and healthy life"
• the under nutrition in developing countries is due to inadequate intake of both protein and energy and that it is often associated with infectious diseases.

Dr Siham Gritly 24
• Achieving food security includes ensuring:• a nutritionally adequate and safe food
supply at both the national and household levels;
• stability in the supply of food during the year and in all years;
• access by each household to sufficient food to meet the needs of all

Dr Siham Gritly 25
Food security categories:
• High food security: no indications of food access problems or limitations
• Marginal food security: one or two indications of food-access problems but with little or no change in food intake

Dr Siham Gritly 26
Food insecurity categories:
• Low food security: reduced quality of life with little or no indication of reduced food intake; formerly known as food insecurity without hunger
• Very low food security: multiple indications of disrupted eating patterns and reduced food intake; formerly known as food insecurity with hunger

Dr Siham Gritly 27
Social and cultural factors
• Social factors and cultural practices in most countries have a very great influence on;
• what people eat, • how they prepare food, • their feeding practices and • the foods they prefer
Dr Siham Gritly 28
• many practices are specifically designed;• to protect and promote health; • providing women with rich, energy-dense
foods during the first months of pregnancy• Some researcher suggested that traditional
food practices and taboos constitute an important cause of malnutrition in some areas of Africa

Dr Siham Gritly 29
• Nutritionists need to have a knowledge of the food habits and practices of the communities in which they work so that they can help to support the positive habits

Dr Siham Gritly 30
Food habits
• habit is an accustomed way of doing things. Habits accumulated through generations emerge as customs, and customs in turn create habits.
• All people have their likes and dislikes and their beliefs about food,
• They tend to like what their mothers cooked for them when they were young,
• the foods that are served on festive occasions or those eaten with friends and family away from home during their childhood.

Dr Siham Gritly 31
Nutritional advantages of traditional food habits
• The traditional diets of most societies in developing countries are good.
• Eating certain protein-rich foods such as insects, snakes, baboons, mongooses, dogs, cats, unusual seafoods and snails is beneficial.
• Another habit that is good nutritionally is the consumption of animal blood.
• Blood is a rich food, and mixed with milk it is highly nutritious.

Dr Siham Gritly 32
Food taboos
• *Food taboos defined as a set of rules about which foods or combinations of foods may not be eaten
• The origin of these prohibitions is varied. In some cases, these taboos are a result of health considerations or other practical reasons.
• A taboo may be followed by a whole national group or tribe, by part of a tribe or by certain groups in the society.
• Within the society, different food customs may be practiced only by women or children, or by pregnant women or female children

Dr Siham Gritly 33
• There are two main types of food prohibitions; permanent and transitory.
• *permanent; maintained by specific cultural and religious groups. Consumption of these foods is part of what distinguishes each culture from other.
• *transitory, is applied to individuals within a cultural setting due to specific phase states, such as illness, pregnancy, postpartum, lactation and so on.
Dr Siham Gritly 34
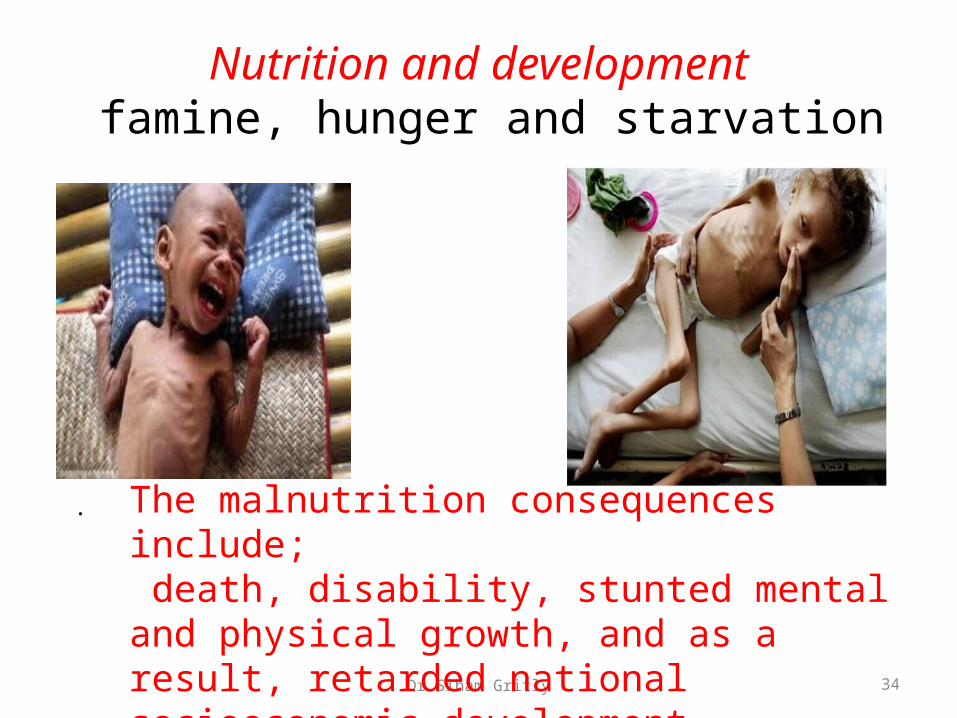
Nutrition and development famine, hunger and starvation
. The malnutrition consequences include; death, disability, stunted mental and physical growth, and as a result, retarded national socioeconomic development.

Dr Siham Gritly 35
Stages in the Development of a Nutrient Deficiency
• 1-Primary deficiency caused by inadequate diet or Secondary deficiency caused by problem inside the body------assessment methods;-Diet history and Health history
• 2-Declining nutrient stores (subclinical) and Abnormal functions inside the body assessment methods;-Laboratory tests
• 3-Physical signs and symptoms, assessment methods; -Physical examination and anthropometric measures
Dr Siham Gritly 36
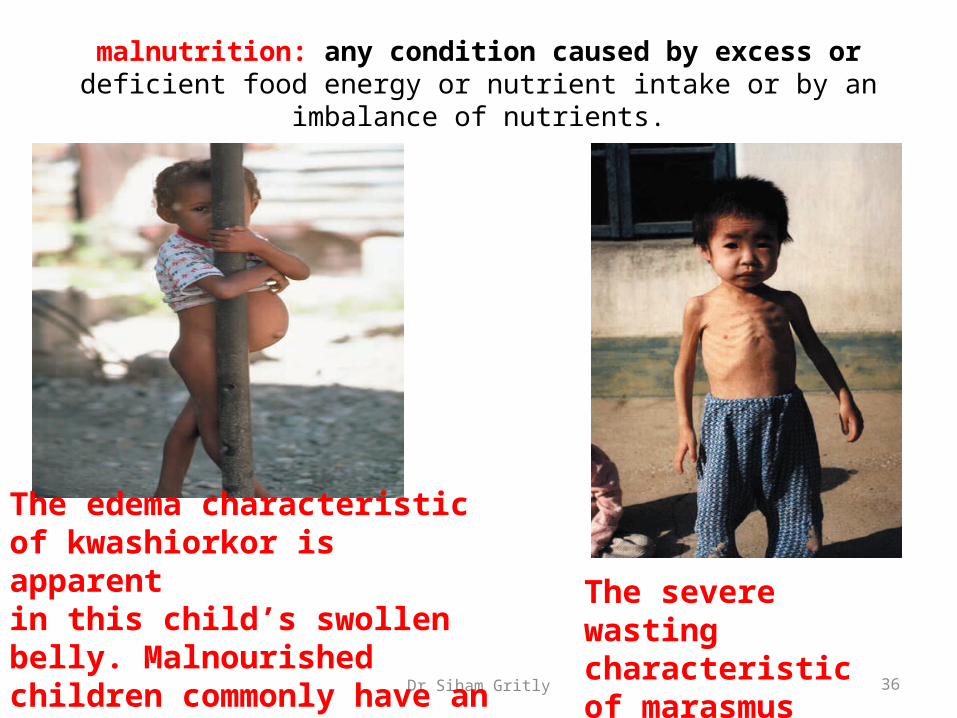
malnutrition: any condition caused by excess or deficient food energy or nutrient intake or by an imbalance of nutrients.
The severe wasting characteristic of marasmus
The edema characteristic of kwashiorkor is apparentin this child’s swollen belly. Malnourished children commonly have an enlarged abdomen from parasites as well.
Dr Siham Gritly 37
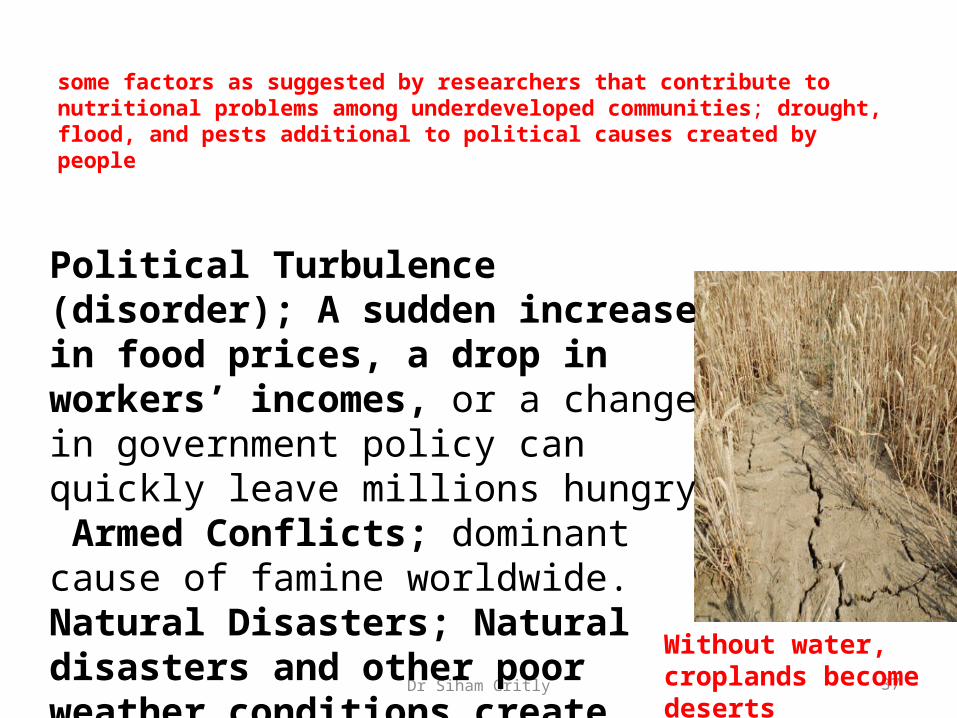
some factors as suggested by researchers that contribute to nutritional problems among underdeveloped communities; drought, flood, and pests additional to political causes created by people
Political Turbulence (disorder); A sudden increase in food prices, a drop in workers’ incomes, or a change in government policy can quickly leave millions hungry Armed Conflicts; dominant cause of famine worldwide. Natural Disasters; Natural disasters and other poor weather conditions createfood shortages
Without water, croplands become deserts

Dr Siham Gritly 38
Nutrition, infection and national development
• the effects of nutritional status on infections and of infections on malnutrition a very important relationship.
• The majority of children in most developing countries suffer from malnutrition at some time in their first five years of life.
• control of infectious diseases and• improvements in the children's food intake and
health care. Are main factors that reduce children mortality

Dr Siham Gritly 39
• Many of the children who suffer from malnutrition and a series of infections;
• They are often;• retarded in their physical,• psychological or behavioural development, • And a shortened life expectation.
Dr Siham Gritly 40
the most common serious nutritional problems in almost all developing countries
• Protein-energy malnutrition (PEM),
• vitamin A deficiency,
• iodine deficiency disorders (IDD)
• and nutritional anaemia - mainly resulting from iron deficiency

Dr Siham Gritly 41
Principle problems of nutrition in developing countries
• Maternal malnutrition• Poor nutrition in preconception period and
pregnancy• Maternal depletion, poor pregnancy weight
gain, and depletion of nutrient stores (fat and muscle mass, iron, calcium, zinc, vitamin A, etc.)
• Maternal anemia, or protein energy malnutrition

Dr Siham Gritly 42
• Infant feeding • Exclusive breast feeding (EBF) for first 4-6
months • Those not EBF have double the infant
mortality rate as breast fed infants in developing countries
WhyWhat are the benefit of breast milk

Dr Siham Gritly 43
• Weaning• Continue breast feeding until 2 years child• energy-dense food with high-quality complete
protein, essential vitamins and minerals
What are the main weaning food used in Sudan
Dr Siham Gritly 44
• Micronutrient deficiencies• Iron deficiency– Anemia– Impaired cognitive function– Decreased physical activity– Decreased work capacity in older children and
adults– Decreased appetite– Impaired cellular immune function
•
Dr Siham Gritly 45
• Vitamin A– Irreversible blindness– Increased morbidity and mortality from
infection, especially pneumonia and diarrhea–Loss of structure and function of epithelial
linings of the body– Impaired cellular immune function

Dr Siham Gritly 46
• Iodine deficiency
Impaired intellectual capacity, decreased productivity,
Significant cause of poor pregnancy outcome, severely retarded infants, children, and adults

Dr Siham Gritly 47
• Others such as;• Zinc deficiency• Vitamin B12 deficiency• Folic acid• Calcium• Vitamin D

Dr Siham Gritly 48
Poverty in Sudan The UN Millennium Development Goals in Sudan
• The incidence of poverty in Northern Sudan stood at 46.5%.
• This means that almost one out of two Northern Sudanese does not have the necessary means to purchase the value of a minimum food and non-food bundle.
• Poverty levels vary greatly by state.

Dr Siham Gritly 49
• The incidence of poverty ranges from a quarter of the population in the capital to more than two thirds of the population in Northern Darfur.
• That is the percentage of individuals whose incomes are insufficient to achieve the minimum energy level ,

Dr Siham Gritly 50
the growth strategy needs to focus on two areas:
• (i) support for the agricultural sector, including livestock, forestry and fisheries, to promote growth and productivity change; and (ii) support for private sector development, with policies, institutions, incentives and infrastructural services to promote investments, innovation, productivity growth and employment creation in all sectors of the economy.
Dr Siham Gritly 51
The key roles for the government in the strategy includes
• (i) the maintenance of macroeconomic stability that reduces macroeconomic risks,
• improves the confidence of the business sector in the management of the economy,
• helps to maintain the competitiveness of Sudanese firms;
(ii) adopt policy and institutional framework that supports the strategic objectives of growth and poverty reduction;
Dr Siham Gritly 52
• (iii) pursue human development efforts that builds a skilled labor force consistent with the demands of the labor markets to foster innovation and productivity; and
(iv) economic services including infrastructure, and for agriculture, knowledge related services (research, extension and capacity building).
Dr Siham Gritly 53
• the MDGs assessments in Sudan indicate to positive and encouraging progress on;
• Goal 2 (access to education particularly at primary level),
• Goal 3 (Gender Equality and Empowerment of Women) and
• Goal 6 (HIV/AIDS).

Dr Siham Gritly 54
• Goal 1, Goal 4, Goal 5 and Goal 7 of the MDGs may not be achieved unless current efforts are scale up on all fronts (resources both human and financial) to reverse current trends.
Dr Siham Gritly 55
Discussion
• What are the main causes of poverty in Sudan

Dr Siham Gritly 56
Hunger-Relief OrganizationsRef Ellie Whitney and Sharon Rady Rolfes; Under standing Nutrition, Twelfth Edition. 2011, 2008 Wadsworth, Cengage Learning
Organization Mission Statement
Action without Borderswww.idealist.org
International organization seeking to connect people, organizations, and resources to help build a worldwhere all people can live free and dignifi ed lives.
Bread for the World www.bread.org
Non-partisan, Christian citizens’ movement seeking to influence reform in policies, programs, and conditions that allow hunger and poverty to persist globally.
Community Food Security Coalitionwww.foodsecurity.org
North American coalition of diverse people and olevels to build community food securityrganizations working from the local to the international
Congressional Hunger Centerwww.hungercenter.org.
Bipartisan organization training and inspiring leaders with the intent to end hunger, and advocatingpublic policies to create a food-secure world

Dr Siham Gritly 57
Hunger-Relief Organizations
Organization Mission Statement
Food and Agriculture Organization(FAO) of the United Nationswww.fao.org
International organization leading efforts to defeat hunger by helping to develop and modernizecountries’ agriculture, forestry, and fi shery practices
Oxfamwww.oxfamamerica.org
America International relief and development organization aiming to create lasting solutions to poverty, hunger, and injustice.
Pan American Health Organizationwww.paho.org
International public health agency aiming to strengthen national and local health systems with thepurpose of improving the quality of, and lengthening, the lives of peoples in the Americas.
The Hunger Project www.thp.org
International relief organization emphasizing sustainable solutions such as rural development and selfreliance to facilitate food security
Dr Siham Gritly 58
Hunger-Relief Organizations
Organization Mission Statement
United Nations Children’s Fund (UNICEF)www.unicef.org
International organization advocating for the protection of children’s rights, to help meet their basic needs and to expand their opportunities to reach their full potentials.
World Food Programwww.wfp.org
Food aid branch of the United Nations aiming to prepare for, protect during, and provide assistance after, emergencies, as well as reducing hunger and undernutrition
World Health Organization (WHO) www.who.int
United Nations agency acting as the authority on international public health by infl uencing policy, setting research agendas, establishing standards, and providing technical support to monitor and assesshealth trends
World Hunger Year (WHY)www.whyhunger.org
Domestic organization supporting and funding community-based organizations intent on empoweringindividuals and building self-reliance to provide long-term solutions to hunger and poverty.

Dr Siham Gritly 59
references• The world health report 2002: reducing risks, promoting healthy life.
Geneva, World Health Organization, 2002.
• Diet, physical activity and health. Geneva, World Health Organization, 2002 (documents A55/16 and A55/16 Corr.1).
• . Popkin BM. The shift in stages of the nutritional transition in the developing world differs from past experiences! Public Health Nutrition, 2002, 5:205-214.
• The world health report 1998. Life in the 21st century: a vision for all. Geneva, World Health Organization, 1998
• Nutrition and development: a global assessment. Rome, Food and Agriculture Organization of the United Nations and Geneva, World Health Organization, 1992.
• Promoting appropriate diets and healthy lifestyles. In: Major issues for nutrition strategies. Rome, Food and Agriculture Organization of the United Nations and Geneva, World Health Organization, 1992:17-20.
Dr Siham Gritly 60
• Ref Ellie Whitney and Sharon Rady Rolfes; Under standing Nutrition, Twelfth Edition. 2011, 2008 Wadsworth, Cengage Learning
• Drewnowski A, Popkin BM. The nutrition transition: new trends in the global diet. Nutrition Reviews, 1997, 55:31-43.
• World agriculture: towards 2015/2030. Summary report. Rome, Food and Agriculture Organization of the United Nations, 2002.
• Bruinsma J, ed. World agriculture: towards 2015/2030. An FAO perspective. Rome, Food and Agriculture Organization of the United Nations/London, Earthscan, 2003

Dr Siham Gritly 61
Questions to Identify Food Insecurity in Household
• 1. Did you worry whether food would run out before you got money to buy more?
• 2. Did you find that the food you bought just didn’t last and you didn’t have money to buy more?
• 3. Were you unable to afford to eat balanced meals?• 4. Did you or other adults in your household ever cut the size
of your meals or skip meals because there wasn’t enough food?• 5. Did this happen in three or more months during the previous
year?• 6. Did you ever eat less than you felt you should because there
wasn’t enough money for food?

Dr Siham Gritly 62
• Were you ever hungry but didn’t eat because you couldn’t afford enough food?
• 8. Did you ever lose weight because you didn’t have enough money to buy food?
• 9. Did you or other adults in your household ever not eat for a whole day because you were running out of money to buy food?
Dr Siham Gritly 63
• 10. Did this happen in three or more months during the previous year?
• 11. Did you rely on only a few kinds of low-cost food to feed your children because you were running out of money to buy food?
• 12. Were you unable to feed your children a balanced meal because you couldn’t afford it?
• 13. Were your children not eating enough because you just couldn’t afford enough food?

Dr Siham Gritly 64
• 14. Did you ever cut the size of your children’s meals because there wasn’t enough money for food?
• 15. Were your children ever hungry but you just couldn’t afford enough food?
• 16. Did your children ever skip a meal because there wasn’t enough money for food?
• 17. Did this happen in three or more months during the previous year?
• 18. Did your children ever not eat for a whole day because there wasn’t enough money for food?