lecture 1 pbl int-gak sempet
DESCRIPTION
pbl -ubTRANSCRIPT
CHEMICAL AGENTS THAT AFFECTS YOUR BODY
DEPARTMENT OF PHARMACOLOGY MEDICAL FACULTY
BRAWIJAYA UNIVERSITY 2007
THIS PRESENTATION CONSIST OF
1. LECTURE NOTE 2. MODULE
AFTER ATTENDING THE LECTURE THE STUDENT WILL BE ABLE TO UNDERTSTAND THE “PORT D'ENTRY”AND THE EFFECTS OF CHEMICAL AND FOREIGN SUBTANCEENTERING THE BODY
THE QUESTION , TASKS, EXERCISE AND ASSAY IN THE MODULE HAVE TO BE DONE BY STUDENT IN 7 DAYSAFTER THE LECTURES
Paracelsus (1493-1541) noted: "All substances are poisons; there is none which is not a poison. The right dose differentiates a poison and a remedy."
Chemical Forms of Drugs That Produce Toxicity. The "parent" drug administered to the patient often is the chemical form producing the desired therapeutic effect; the parent drug also may produce the toxic effects of drug. However, both therapeutic and toxic effects also can be due to metabolites of the drug produced by enzymes, light, or reactive oxygen species. In considering the toxicity of drugs and chemicals, it is important to understand their metabolism, activation, or decomposition
OTHERS THAN FOOD AND NUTRITION A CHEMICAL SUBSTANCE / FOREIGN SUBSTANCE / XENOBIOTICS SUCHAS:
CHEMICAL FROM WATER AND AIR POLUTION TOXIC SUBSTANCES OF HEAVY METALS
TOXIN FROM ANIMAL AND MARINE TOXIN FROM PLANT CHEMICALS FROM PESTICIDES,INSECTICIDESMEDICINE AND DRUGS FOOD ADDITIVE COLOURING. ETC
AFFECTS PHYSIOLOGY AND PATHOLOGY OF MOLECULES, CELLS, TISSUE, ORGAN AND ORGANISMRANGE FROM STRUCTURAL AND FUNCTIONAL CHANGES TO NECROSIS OR APOPTOSIS OF THE CELL AND FOLLOW BY A KIND OF DISEASE ANDDEATH
HOW CHEMICAL SUBSTANCE ENTER THE BODY
1. SKIN PENETRATION
2. ABSORBTION THROUGH LUNG'S EPITHELIUM
3. ABSORBTION THROUGH GASTROINTESTINAL MUCOUS MEMBRANE
AFTER PENETRATION OR ABSORBTION THEY ENTER THE CIRCULATION AND CIRCULATE IN THE BLOOD AND THEN AFFECT THE TARGETED CELL
Routes of entry of chemicals
● Oral● Parental● Topical
– buccal– vaginal– anal– dermal– ocular– nasal
First pass metabolism
Cemical substances Distribution
• molecular size
• lipophilicity
• plasma binding
• blood flow to different organs
• lean:fat body weight

TO UNDERSTAND HOW CHEMICAL AFFECT THE CELL
• Pharmacodynamics = the effects of the drug OR CHEMICALS on the body
• TO UNDERTAND HOW THE BODY HANDLE THE CHEMICALS
• Pharmacokinetics = the way the body affects the drug OR CHEMICALS with time
– absorption– distribution– biotransformation / metabolism– excretion of drugs

Pharmacodynamics
Mechanisms of drug action
– Non-specific drug action
general anaesthetics, osmotic diuretics, antacids
– Alter transport systemsCa antagonists, local anaesthetics, cardiac glycosides
– Alter enzyme functionCOX inhibitors, MAO inhibitors, AChE inhibitors
– Act on receptorsSynaptic transmitter substances, hormones
Receptors
Cell membranes
Intracellular
4 main types:• Agonist gated transmembrane channels• G-protein coupled • Nuclear receptors that regulate gene transcription• Linked directly to tyrosine kinase
Proteins
Transport Systems• Lipid cell membrane
– barrier to hydrophyllic molecules– transport in /out cell
• Ion channels– voltage gated – ligand gated
• Active transport processes– Na+ pump– Noradrenaline transport

Ion channelsIon channels
• Voltage and transmitter gatedCa2+ channels in heart
• Voltage gatedNa+, K+, Ca2+ - same basic structure
Subtypes of each exist
Examples:calcium antagonists Ca2+ in VSM & heartlocal anaesthetics Na+ in nervesanticonvulsants Na+
antiarhythmics Na+
Transport systems
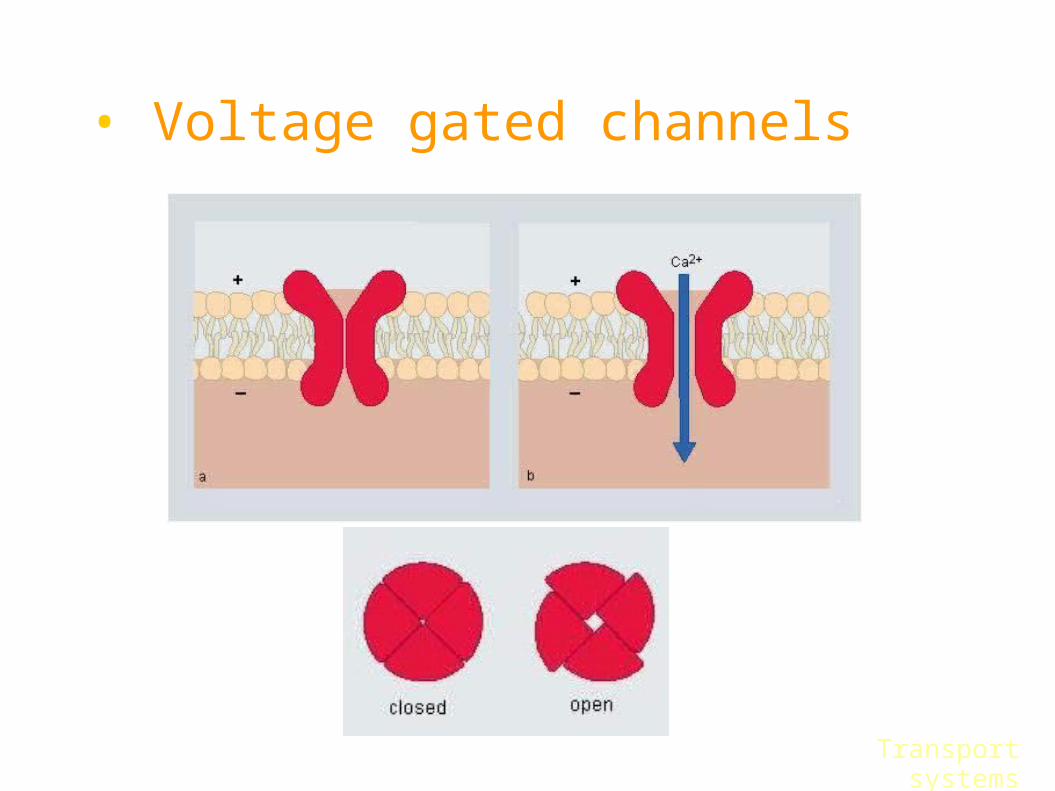
• Voltage gated channels
Transport systems

Site of drug actionMetabolism
liver, GIT, lung
Excretionurine, feaces, expelled air
Storage fat, cytoplasm, bone
Plasma CompartmentBound Free drug drug
Drug Administrationparental, oral, topical
Active transport processesActive transport processes– transport substances against concentration
gradient– special carrier molecules– require metabolic energy
• Sodium Pump– expel Na+ ions– Na+/K+ ATPase
cardiac glycosidessome diuretics
• Noradrenaline transporttricyclic antidepressants block reuptake
Transport systems
Enzymes
– Catalytic proteins that increase the rate of chemical reactions
– Drug examples
• Anticholinesterases
• Carbonic anhydrase inhibitors
• Monoamine oxidase inhibitors
• Cyclo-oxygenase inhibitors
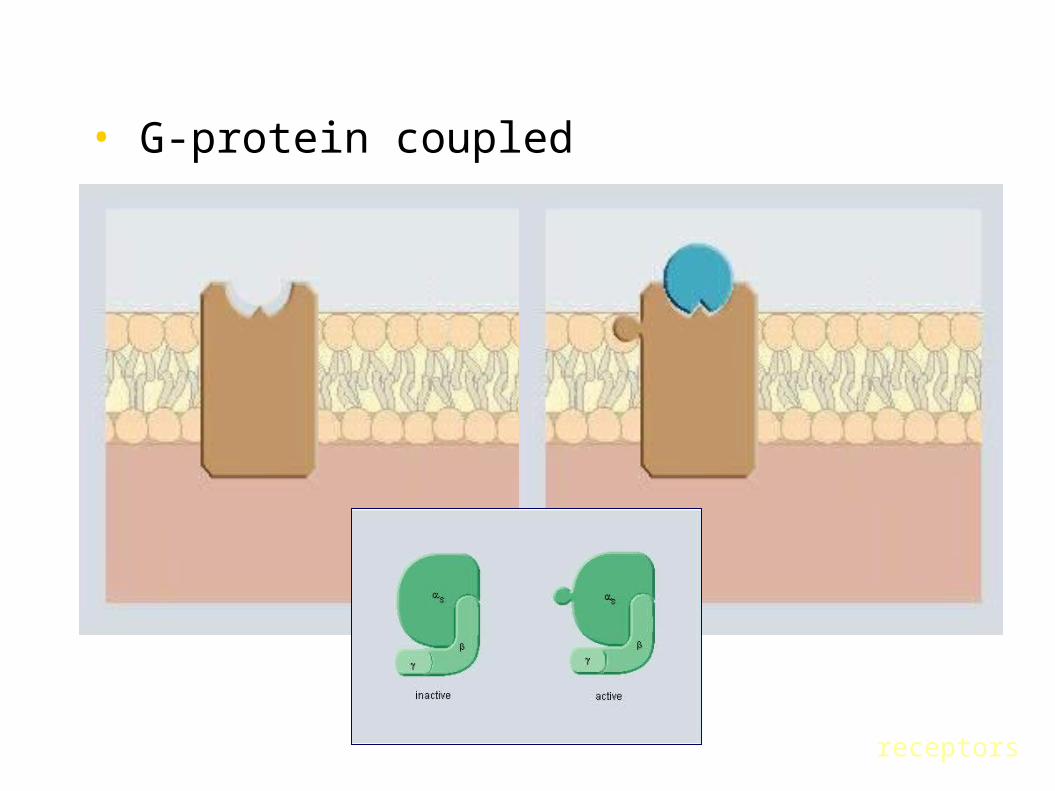
• G-protein coupled
receptors
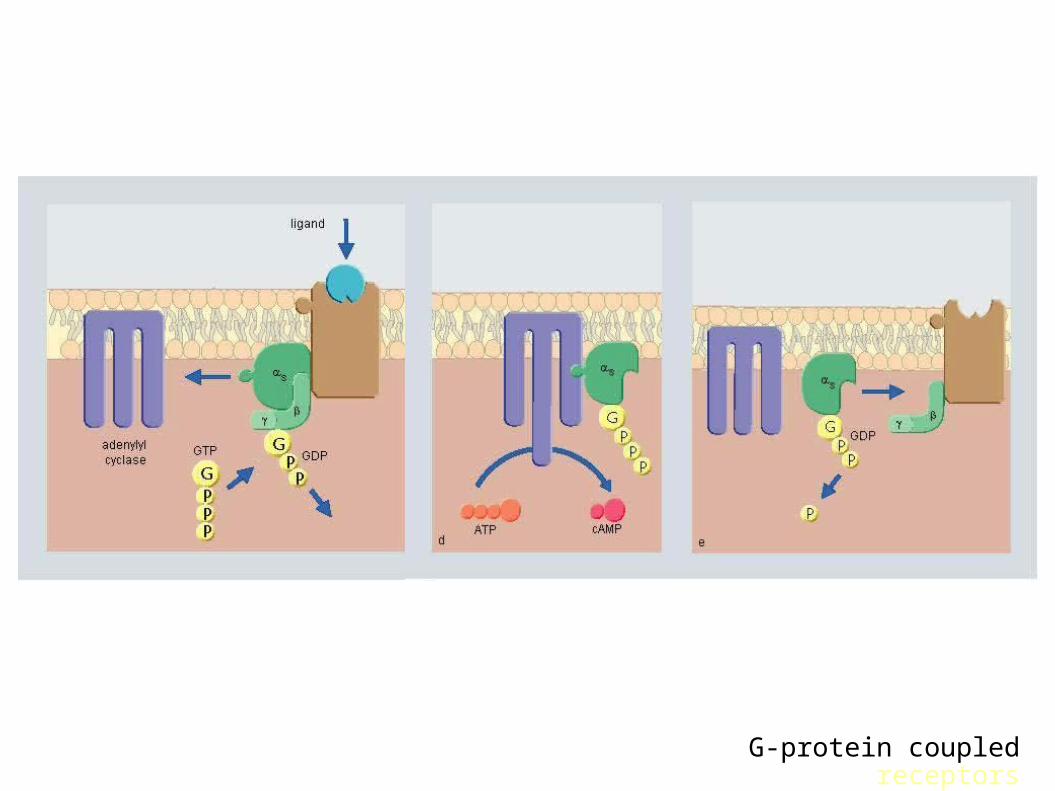
G-protein coupled receptors
receptors
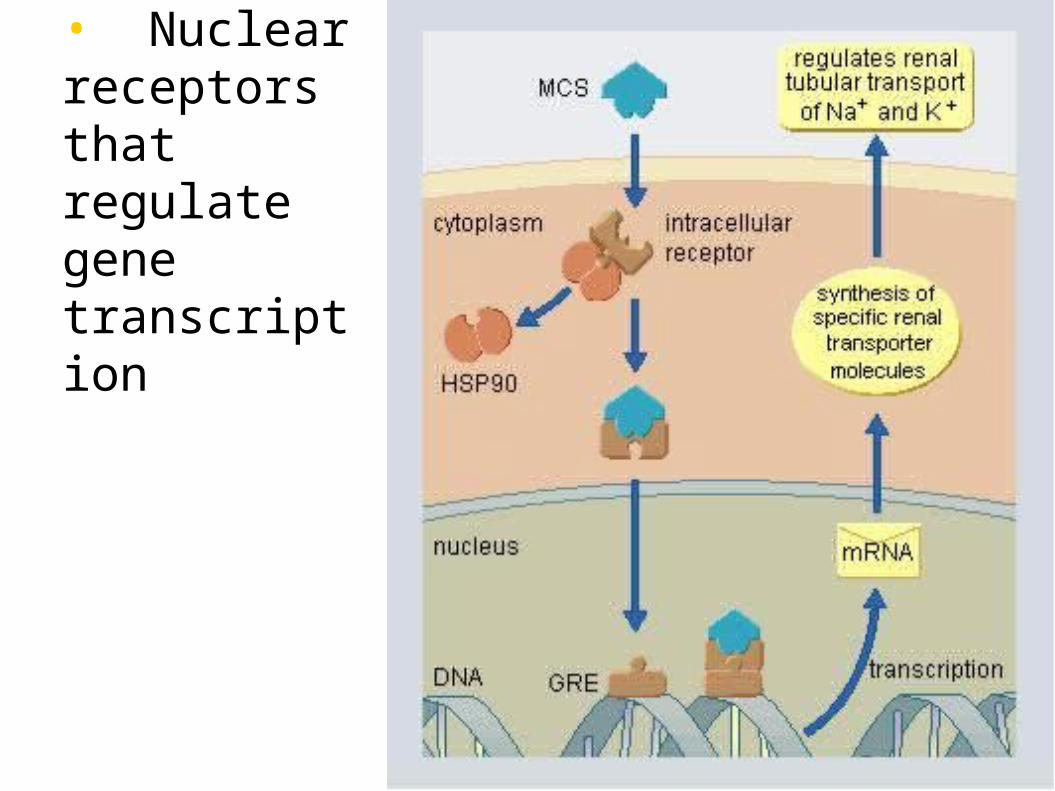
• Nuclear receptors that regulate gene transcription
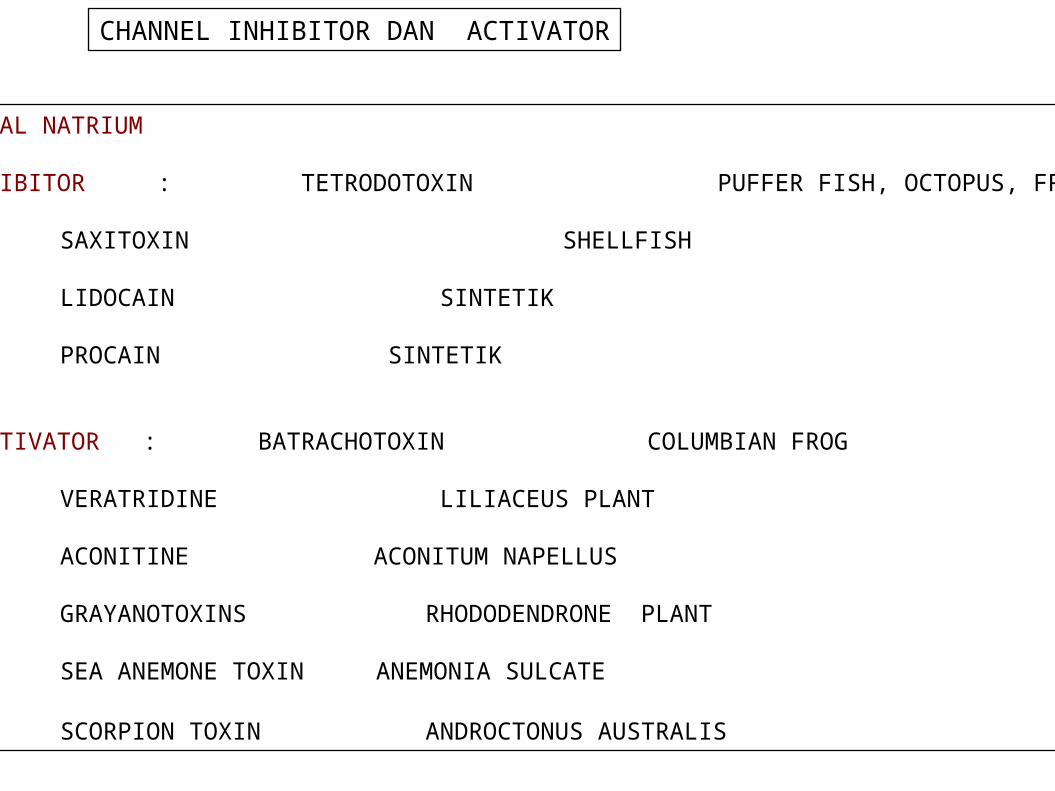
CHANNEL INHIBITOR DAN ACTIVATOR
KANAL NATRIUM
INHIBITOR : TETRODOTOXIN PUFFER FISH, OCTOPUS, FROG
SAXITOXIN SHELLFISH
LIDOCAIN SINTETIK
PROCAIN SINTETIK
ACTIVATOR : BATRACHOTOXIN COLUMBIAN FROG
VERATRIDINE LILIACEUS PLANT
ACONITINE ACONITUM NAPELLUS
GRAYANOTOXINS RHODODENDRONE PLANT
SEA ANEMONE TOXIN ANEMONIA SULCATE
SCORPION TOXIN ANDROCTONUS AUSTRALIS
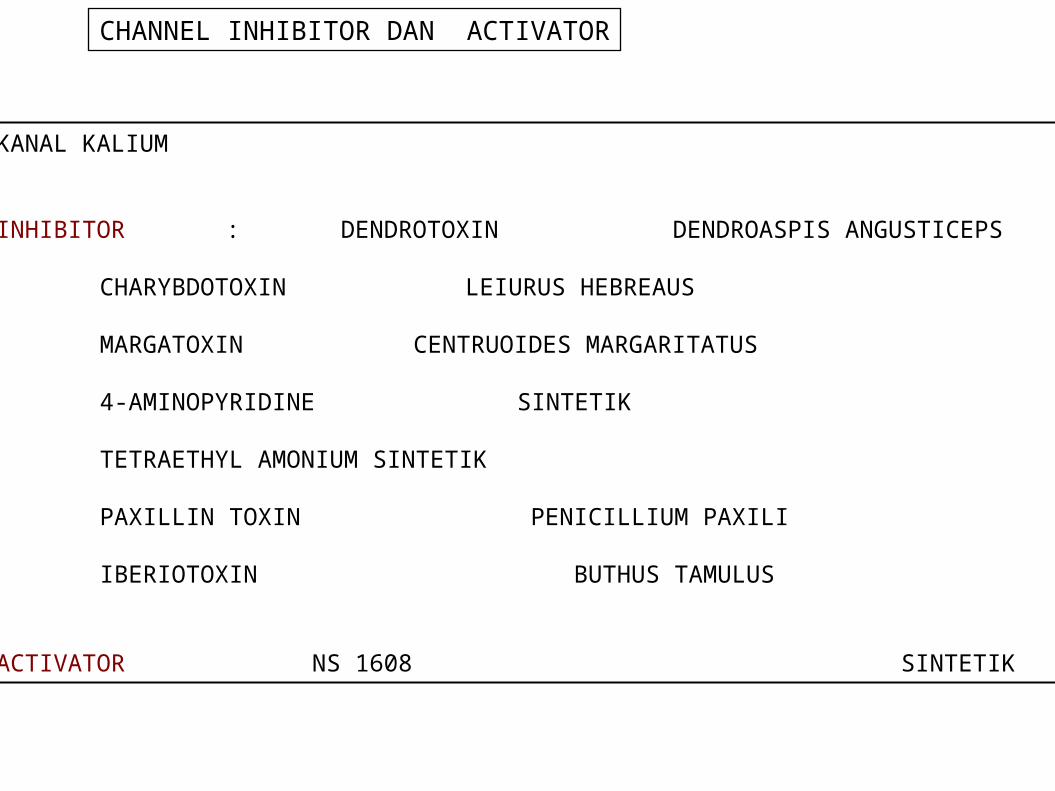
CHANNEL INHIBITOR DAN ACTIVATOR
KANAL KALIUM
INHIBITOR : DENDROTOXIN DENDROASPIS ANGUSTICEPS
CHARYBDOTOXIN LEIURUS HEBREAUS
MARGATOXIN CENTRUOIDES MARGARITATUS
4-AMINOPYRIDINE SINTETIK
TETRAETHYL AMONIUM SINTETIK
PAXILLIN TOXIN PENICILLIUM PAXILI
IBERIOTOXIN BUTHUS TAMULUS
ACTIVATOR NS 1608 SINTETIK
Passage of chemicals through body
● Administration
● Absorption
● Distribution
● Metabolism
● Excretion
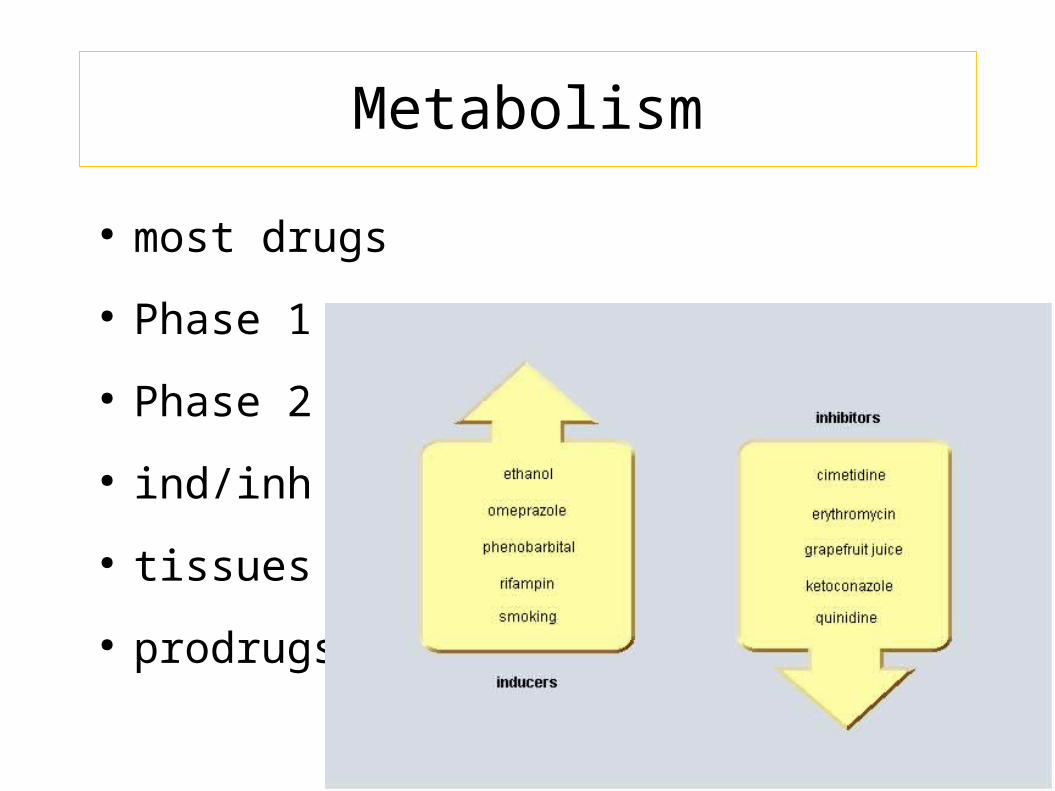
● most drugs
● Phase 1
● Phase 2
● ind/inh
● tissues
● prodrugs
Metabolism
DOSE-RESPONSE RELATIONSHIP
Evaluation of the dose-response or the dose-effect relationship is crucially important to toxicologists. There is a graded dose-response relationship in an individual and a quantal dose-response relationship in the population. Graded doses of a drug given to an individual usually result in a greater magnitude of response as the dose is increased. In a quantal dose-response relationship, the percentage of the population affected increases as the dose is raised; the relationship is quantal in that the effect is specified to be either present or absent in a given individual. This quantal dose-response phenomenon is extremely important in toxicology and is used to determine the median lethal dose (LD50) of drugs and other chemicals.
DOSE-RESPONSE RELATIONSHIP
The LD50 of a compound is determined experimentally, usually by administration of the chemical to mice or rats (orally or intraperitoneally) at several doses (usually four or five) in the lethal range To linearize such data, the response (death) can be converted to units of deviation from the mean, or probits (probability units). The probit designates the deviation from the median; a probit of 5 corresponds to a 50% response, and because each probit equals one standard deviation, a probit of 4 equals 16% and a probit of 6 equals 84%. A plot of the percentage of the population responding, in probit units, against log dose yields a straight line The LD50 is determined by drawing a vertical line from the point on the line where the probit unit equals 5 (50% mortality). The slope of the dose-effect curve also is important. The LD50 for both compounds depicted in is the same (10 mg/kg). However, the slopes of the dose-response curves are quite different. At a dose equal to one-half the LD50 (5 mg/kg), less than 5% of the animals exposed to compound B would die, but 30% of the animals given compound A would die.
The quantal, or "all-or-none," response is not limited to lethality. As described in 1 and 5, similar dose-effect curves can be constructed for any effect produced by chemicals.
There are marked differences in the LD50 values of various chemicals. Some result in death at doses of a fraction of a microgram (LD50 for botulinum toxin equals 10 pg/kg); others may be relatively harmless in doses of several grams or more. While categories of toxicity that are of some practicality have been devised based on the amount required to produce death, often it is not easy to distinguish between toxic and nontoxic chemicals. Paracelsus (1493-1541) noted: "All substances are poisons; there is none which is not a poison. The right dose differentiates a poison and a remedy." It is simply not possible to categorize all chemicals as either safe or toxic. The real concern is the risk associated with use of the chemical. In the assessment of risk, one must consider concentration or dose as well as the harmful effects of the chemical accrued directly or indirectly through adverse effects on the environment when used in the quantity and in the manner proposed. Depending on the use and disposition of a chemical, a very toxic compound ultimately may be less harmful than a relatively nontoxic one.
Types of Toxic Reactions. Toxic effects of drugs may be classified as pharmacological, pathological, or genotoxic (alterations of DNA), and their incidence and seriousness are related, at least over some range, to the concentration of the toxic chemical in the body. An example of a pharmacological toxicity is excessive depression of the central nervous system (CNS) by barbiturates; of a pathological effect, hepatic injury produced by acetaminophen; of a genotoxic effect, a neoplasm produced by a nitrogen mustard. If the concentration of chemical in the tissues does not exceed a critical level, the effects usually will be reversible. The pharmacological effects usually disappear when the concentration of drug or chemical in the tissues is decreased by biotransformation or excretion from the body. Pathological and genotoxic effects may be repaired. If these effects are severe, death may ensue within a short time; if more subtle damage to DNA is not repaired, cancer may appear in a few months or years in laboratory animals or in a decade or more in humans.
Local versus Systemic Toxicity. Local toxicity occurs at the site of first contact between the biological system and the toxicant. Local effects can be caused by ingestion of caustic substances or inhalation of irritant materials. Systemic toxicity requires absorption and distribution of the toxicant; most substances, with the exception of highly reactive chemical species, produce systemic toxic effects. The two categories are not mutually exclusive. Tetraethyl lead, for example, injures skin at the site of contact and deleteriously affects the CNS after it is absorbed into the circulation.
Most systemic toxicants predominantly affect one or a few organs. The target organ of toxicity is not necessarily the site of accumulation of the chemical. For example, lead is concentrated in bone, but its primary toxic action is on soft tissues; DDT (chlorophenothane) is concentrated in adipose tissue but produces no known toxic effects there.

Reversible and Irreversible Toxic Effects. The effects of drugs on humans, whenever possible, must be reversible; otherwise, the drugs would be prohibitively toxic. If a chemical produces injury to a tissue, the capacity of the tissue to regenerate or recover largely will determine the reversibility of the effect. Injuries to a tissue such as liver, which has a high capacity to regenerate, usually are reversible; injury to the CNS is largely irreversible because the highly differentiated neurons of the brain have a more limited capacity to divide and regenerate.
Delayed Toxicity. Most toxic effects of drugs occur at a predictable (usually short) time after administration. However, such is not always the case. For example, aplastic anemia caused by chloramphenicol may appear weeks after the drug has been discontinued. Carcinogenic effects of chemicals usually have a long latency period: 20 to 30 years may pass before tumors are observed. Because such delayed effects cannot be assessed during any reasonable period of initial evaluation of a chemical, there is an urgent need for reliably predictive short-term tests for such toxicity, as well as for systematic surveillance of the long-term effects of marketed drugs and other chemicals
Chemical Carcinogens. Chemical carcinogens are classified into two major groups, genotoxic and nongenotoxic. Genotoxic carcinogens interact with DNA, whereas nongenotoxic carcinogens do not. Chemical carcinogenesis is a multistep process. Most genotoxic carcinogens are themselves unreactive (procarcinogens or proximate carcinogens) but are converted to primary or ultimate carcinogens in the body. The drug-metabolizing enzymes often convert the proximate carcinogens to reactive electron-deficient intermediates (electrophiles). These reactive intermediates can interact with electron-rich (nucleophilic) centers in DNA to produce a mutation. Such interaction of the ultimate carcinogen with DNA in a cell is thought to be the initial step in chemical carcinogenesis. The DNA may revert to normal if DNA repair mechanisms operate successfully; if not, the transformed cell may grow into a tumor that becomes apparent clinically.
At present, there is much concern about the risk from exposure to chemicals that have producedcancer in laboratory animals. For most of these chemicals, it is not known if they also producecancer in humans. Regulatory agencies take one of three approaches to potential chemicalcarcinogens. For food additives, the U.S. Food and Drug Administration (FDA) is very cautiousbecause large numbers of people are likely to be exposed to the chemicals, and they are not likely tohave beneficial effects to individuals. For drugs, the FDA weighs the relative risks and benefits ofthe drugs for patients. Thus it is unlikely that the FDA will approve the use of a drug that producesAcute versus Chronic Exposure. Effects of acute exposure to a chemical often differ from thosethat follow chronic exposure. Acute exposure occurs when a dose is delivered as a single event.Chronic exposure is likely to be to small quantities of a substance over a long period of time, whichoften results in slow accumulation of the compound in the body. Evaluation of cumulative toxiceffects is receiving increased attention because of chronic exposure to low concentrations of variousnatural and synthetic chemical substances in the environment.
Chemical Forms of Drugs That Produce Toxicity. The "parent" drug administered to the patientoften is the chemical form producing the desired therapeutic effect; the parent drug also mayproduce the toxic effects of drug. However, both therapeutic and toxic effects also can be due tometabolites of the drug produced by enzymes, light, or reactive oxygen species. In considering thetoxicity of drugs and chemicals, it is important to understand their metabolism, activation, ordecomposition.
stable and are referred to as reactive intermediates. An example of a toxic reactive intermediate isthe metabolite of acetaminophen , which is very reactive and binds to nucleophiles such asglutathione; when cellular glutathione is depleted, the metabolite binds to cellular macromolecules,the mechanism by which acetaminophen kills liver cells . Both parathion and acetaminophen aremore toxic under conditions in which CYPs are increased, such as following ethanol orphenobarbital exposure, because CYPs produce the toxic metabolites .

Reactive Oxygen Species. Paraquat is an herbicide that produces severe lung injury. Its toxicity is not due to paraquat or its metabolites but rather to reactive oxygen species formed during one-electron reduction of paraquat paired with an electron donation to oxygen
How paraquate destroy he lung function ?
question Question
1. how paraquate affect your lung function
2. Organophaosphat insectisides give spesific sign of intoxication describe
Question and assay
1.
How a carcinogen substances may develop cancer in certain patients
Smoking have many social problem as Cigarrete smoke is toxic to human health . Cigarrete factory employ thousand Of labour. Have you any idea to solve these problems?
Chronic exposure to chemical may affect homeostasis of the bodycan you give an example of chemical that alter homeostasis of Gastroitestinal function.