lecture 10 adult asthma dahri signs and symptoms ... · sx occur after taking asas or beta-blockers...
TRANSCRIPT

Lecture 10 Adult Asthma Dahri
SIGNS AND SYMPTOMS:
Episodic breathlessness
Wheezing
Cough with or without sputum
Chest tightness
Sx worse at night and early morning
Sx occur in response to exercise, exposure to allergens or cold air
Sx occur after taking ASAS or beta-blockers
QUESTIONS TO CONSIDER IN THE DIAGNOSIS OF ASTHMA:
Has the pt had an attack or recurrent attacks of wheezing?
Does the pt have a troublesome cough at night?
Does the pt wheeze or cough after exercise?
Does the pt experience wheezing, chest tightness or cough after exposure to airborne allergens or pollutants?
Does the pts’ cold “go to the chest” or take more than 10 days to clear up?
Are symptoms improved by appropriate asthma treatment?
GOALS OF THERAPY:
Achieve and maintain control of sx
Maintain normal activity levels, including exercise
Maintain pulmonary fxn as close to normal levels as possible
Prevent asthma exacerbations
Avoid AEs from asthma medications
Prevent asthma related mortality
ASSESSMENT OF ASTHMA: 1. Asthma control:
a. Assess sx control over last 4 weeks Well-
controlled Partly controlled
Un-controlled
Daytime asthma sx > 2 times/wk
None of these
1-2 of these
3-4 of these
Night time waking
Reliever use > 2 times/wk *
Activity limitation?
* excludes use before exercise
b. Assess risk factors for poor outcomes: Risk factors for …
Exacerbations Fixed airflow limitation Medication SEs
Ever intubated for asthma
Uncontrolled asthma sx
≥ 1 exacerbation in last 12 mo
Low FEV1*
Incorrect inhaler technique and/or poor adherence
Smoking, obesity, pregnancy, blood eosinophilia
No ICS treatment
Smoking
Occupational exposure
Mucus hypersecretion
Blood eosinophilia
Frequent oral steroids
High dose/ potent ICS
P450 inhibitors
* measure FEV1 at start of txt, after 3-6 mo for personal best, then periodically
2. Treatment issues a. Check inhaler technique & adherence
Factors Involved in Non-Adherence
Medication Usage Non-medication factors
Difficulties associated with inhalers
Complicated regimens
Fears about, or actual SEs
Cost
Distance to pharmacies
Misunderstanding/lack of info
Fears about SEs
Inappropriate expectations
Underestimation of severity
Attitudes toward ill health
Cultural factors
Poor communication
b. Ask about SEs c. Written asthma action plan? d. Attitudes and goals for asthma?
3. Comorbidities – may contribute to sx and poor QOL
Conditions Drugs
Rhinosinusitis
GERD
Obesity
Obstructive sleep apnea
Depression/anxiety
Smoking
Beta-blockers
NSAIDs
NON-PHARMACOLOGICAL MANAGEMENT:
Identify & avoid precipitating factors (environmental allergens & occupational irritants)
Smoking cessation
Some evidence to encase bedding in impermeable covers for house dust mite allergens in children
TREATMENT GUIDELINES:
Lecture 10 Adult Asthma Dahri
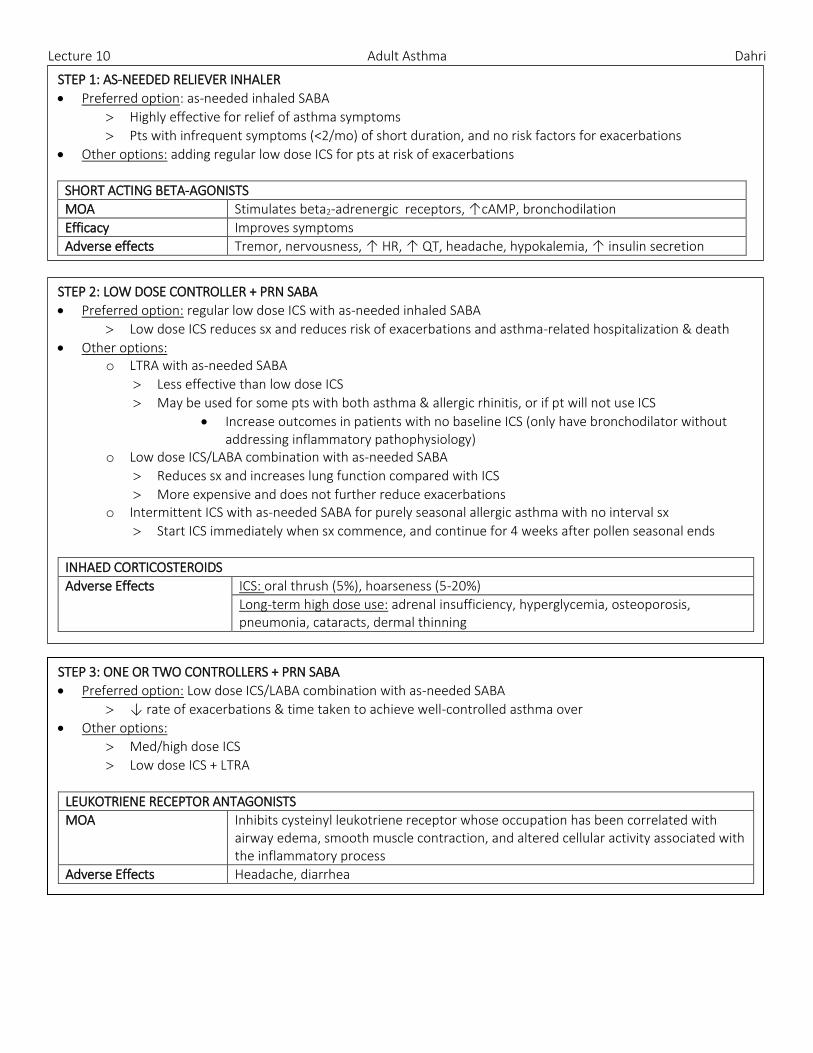
STEP 1: AS-NEEDED RELIEVER INHALER
Preferred option: as-needed inhaled SABA
Highly effective for relief of asthma symptoms
Pts with infrequent symptoms (<2/mo) of short duration, and no risk factors for exacerbations
Other options: adding regular low dose ICS for pts at risk of exacerbations
SHORT ACTING BETA-AGONISTS
MOA Stimulates beta2-adrenergic receptors, ↑cAMP, bronchodilation
Efficacy Improves symptoms
Adverse effects Tremor, nervousness, ↑ HR, ↑ QT, headache, hypokalemia, ↑ insulin secretion
STEP 2: LOW DOSE CONTROLLER + PRN SABA
Preferred option: regular low dose ICS with as-needed inhaled SABA
Low dose ICS reduces sx and reduces risk of exacerbations and asthma-related hospitalization & death
Other options: o LTRA with as-needed SABA
Less effective than low dose ICS
May be used for some pts with both asthma & allergic rhinitis, or if pt will not use ICS
Increase outcomes in patients with no baseline ICS (only have bronchodilator without addressing inflammatory pathophysiology)
o Low dose ICS/LABA combination with as-needed SABA
Reduces sx and increases lung function compared with ICS
More expensive and does not further reduce exacerbations o Intermittent ICS with as-needed SABA for purely seasonal allergic asthma with no interval sx
Start ICS immediately when sx commence, and continue for 4 weeks after pollen seasonal ends
INHAED CORTICOSTEROIDS
Adverse Effects ICS: oral thrush (5%), hoarseness (5-20%)
Long-term high dose use: adrenal insufficiency, hyperglycemia, osteoporosis, pneumonia, cataracts, dermal thinning
STEP 3: ONE OR TWO CONTROLLERS + PRN SABA
Preferred option: Low dose ICS/LABA combination with as-needed SABA
↓ rate of exacerbations & time taken to achieve well-controlled asthma over
Other options:
Med/high dose ICS
Low dose ICS + LTRA
LEUKOTRIENE RECEPTOR ANTAGONISTS
MOA Inhibits cysteinyl leukotriene receptor whose occupation has been correlated with airway edema, smooth muscle contraction, and altered cellular activity associated with the inflammatory process
Adverse Effects Headache, diarrhea

Lecture 10 Adult Asthma Dahri
STEP 4: TWO OR MORE CONTROLLERS + PRN SABA
Before considering step-up: check inhaler technique and adherence
Preferred options: o Combination low dose ICS/formoterol as maintenance and reliever regimen (SYMBICORT SMART)
o Combination medium dose ICS/LABA with PRN SABA o CHILDREN: refer for expert advice
Other options: o Add on tiotropium (LAMA) for adult patients (≥ 18 years) with a history of exacerbation o High dose ICS + LTRA (however studies show little extra benefit & increased risk of SEs) o Increase dosing frequency (for budenoside-containing inhalers) o Add-on LTRA or low dose theophylline
Symbicort: budenoside + formoterol
Maintenance: Symbicort 100 or 200 – 1 to 2 inh BID or 2 inh once daily
Reliever: Symbiort 100 or 200 – 1 additional inh PRN, repeat if no relief x 6 inh total (max 8 inh/day)
STEP 5: HIGHER LEVEL CARE AND/OR ADD-ON TREATMENT
Preferred option: referral for specialist investigation and consideration of add-on treatment
If sx uncontrolled or exacerbations persist Step 4 txt, check inhaler technique & adherence before referral
Add-on omalizumab (anti-IgE) – for pts with mod-severe allergic asthma that is uncontrolled on Step 4 txt
Other options:
Tiotropium: for adults (≥ 18 yo) with a history of exacerbations despite Step 4 txt; reduces exacerbations
Sputum-guided txt: in specialized centers; reduces exacerbations and/or corticosteroid dose
Add-on low dose oral corticosteroids (≤ 7.5 mg/day prednisone equivalent) May benefit some pts, but has significant systemic side-effects (monitor for osteoporosis)
Anti-IgEs
MOA IgE-neutralizing antibody
ADRs Injection site reactions, viral infections, URTI, headache, sinusitis, pharyngitis
ORAL STEROID ADRS
Cardiovascular (15%) Dyslipidemia, electrolyte imbalance, edema, renal/heart dysfunction, HTN
Infections (15%) Viral, bacterial, skin6
GI (10%) PUD, pancreatitis
Psychological (9%) Steroid psychosis, minor mood disturbances
Endocrine (7%) Diabetes, fat redistribution, interference with hormone secretion
Dermatologic (5%) Subcutaneous atrophy, acne, hirsutism, alopecia
MSK (4%) Osteoporosis, osteonecrosis, myopathy
Opthamologic (4%) Glaucoma, cataract