lecture 12 somatosensory system and nociception
TRANSCRIPT
Somatosensory System: Touch, Proprioception, and Pain
Farzana Z Ali
HBY 554 – Principles of Neuroscience
Spring 2013

Learning Objectives for Part I
Part I: Touch and Proprioception
•Classify somatic sensory afferents based on their distinct functional properties
•Characterize mechanoreceptors specialized for tactile information and proprioception
•Understand the central pathways conveying tactile and proprioceptive information from body and face
• Learn about cortical maps and plasticity

Basic Senses
Somatic sensation
Vision
Audition
Vestibular sensation
Chemical senses
Energy from mechanical
forces
Afferent sensory signals
Central neurons
(qualitative + quantitative +
location)

Somatic Sensory System
Somatic - “of the body”
•Relating to body
•Pertaining to body wall in contrast to viscera
•Distinguished from germplasm or psyche
•Touch, pressure, vibration, limb position, heat, cold and pain

Subsystems
Tactile•Cutaneous mechanoreceptors •Fine touch, vibration, and pressure
Proprioceptive•Muscles, tendons, and joints •Position of limbs and other body parts in space
Nociceptive•Painful stimuli, changes in temperature and
coarse touch

Somatic Sensory Afferents
Action potentials: Somatic sensory afferent fibers Cell bodies inDorsal root ganglia ( pseudo-unipolar),Cranial nerve ganglia

Sensory Transduction
Energy of stimulus Electric signal
• Δ Permeability of cation channels • Depolarizing current• Threshold to generate AP

Dermatomes • Dorsal root gangilon
associated spinal nerve• Overlap substantially
(injury)• Pain sensation more
precise

Axon Diameter
• IA: Largest diameter sensory afferents (muscles)
•Aβ: Slightly smaller diameter fibers (touch)
•Aδ, C: Smaller diameter fibers (pain and temperature)

Receptive field
• Sig. Δ in rate of AP• Smaller receptive fields Smaller branching Dense innervation
Two-point discrimination• ↑ receptive fields• Somatic acuity

Temporal Dynamics, Channels and Filters
Channels in sensory afferents• Quality of stimulation• Filter properties of
encapsulating receptors
Stimulus movement, clothes
Spatial attributes of the stimulus: size and shape

Mechanoreceptors for Tactile Information
slow, form + texture, fingertips
spatial resolution
rapid, dense, ↑ sensitive, ↑ fields, grip
rapid, filter ν, ↓threshold, ↑ fields, vibrations
slow, stretching, internal, position/conformation
details
coarse
APs

Mechanoreceptors for Proprioception
Muscle spindles: lengthGroup IA:Velocity + directionGroup II:Sustained, static position
Golgi tendons: tensionGroup Ib:Branched in collagen fibers to form tendons
Joint receptors: finger position

Central Pathways
Cerebral cortex
Third order neurons in thalamus
Second-order neurons in brainstem nuclei
First order neurons in dorsal root and cranial nerve ganglia

Do
rsal
Co
lum
n-M
edia
l Lem
nis
calS
yste
m
Tact
ile In
form
atio
n f
rom
th
e B
od
y

Trigeminothalamic System
Trigeminal nerve trigeminal brainstem complex: i) principal, ii) spinal, iii) mesencephalicLow threshold mechanoreceptors principle nucleus cross midlinetrigeminal lemniscus /trigeminothalamic tract VPM SI and SII

Proprioceptive Pathways for Body• Upper: dorsal columns medulla nuclei cross the midline medial lemniscus VPL
• Lower: medulla outside gracilis decussate and join medial lemniscus VPL

Proprioceptive Pathway for Face
• Cell bodies in mesencephalic trigeminal nucleus• Peripheral processes innervating muscle spindles
+ Golgi tendon organs • Facial musculature + central processes• Brainstem nuclei for reflex control• Thalamus somatosensory cortex• Exact pathway not known

Hemispatial Neglect
Parton A, Malhotra P, and Husain M. Hemispatial neglect. Journal of neurology, neurosurgery, and psychiatry 75: 13-21, 2004.
• Unilateral brain damage• Cerebral infarction or
hemorrhage• Fail to be aware of or
acknowledge items• Right inferior parietal lobe
or nearby temporo-parietal junction

Somatic Sensory Portion of Thalamus
• Ascending: spinal cord and brain stemVentral Posterior Complex of thalamus
• VPL medial lemniscusfrom posterior head + body
• VPM trigeminal lemniscusfrom face
• Muscle spindle/ Golgi tendons

Somatotopic Map
• Homunculus - “Little man”• Face and hands
> torso and proximal limbs• Manipulation,
facial expression and speech
• Cervical spinal cord• Receptor density

Cortical Plasticity
• Reorganization of cortical circuits• Peripheral lesions • Unresponsive responsive to stimulation of
neighboring regions of skin• Central representation of remaining digits• Functional remapping• Thalamus and brainstem

Learning Objectives for Part II
Part II: Pain
• Learn about nociceptive receptors and signal transduction
• Distinguish pain pathways from mechanosensory pathways
• Understand the pathway for visceral pain
• Characterize peripheral and central sensitization
• Gain insight into different aspects of the modulation of pain perception
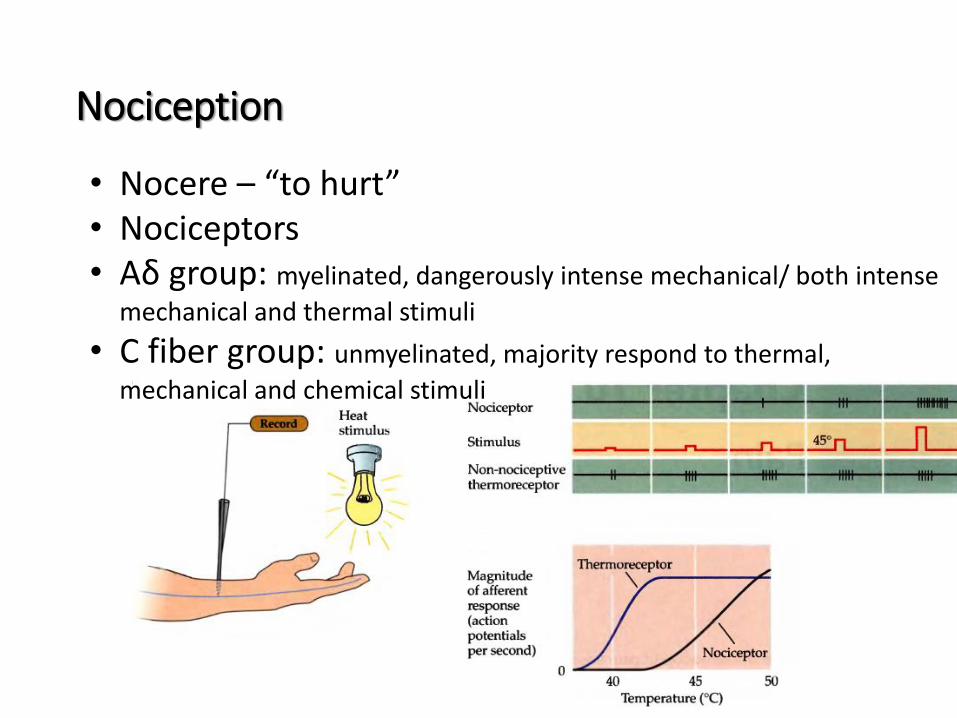
Nociception
• Nocere – “to hurt”• Nociceptors• Aδ group: myelinated, dangerously intense mechanical/ both intense
mechanical and thermal stimuli
• C fiber group: unmyelinated, majority respond to thermal,
mechanical and chemical stimuli

Nociceptor Afferents
• Aδ mechanosensitive, Aδ mechanothermal, polymodal C fibers
• Sharp first pain: Aδ activated when stimulus intensity ↑
• More delayed, diffuse, and longer-lasting second pain: small-diameter C fibers activated when simulation ↑ even farther

Signal Transduction
• Aδ and C: VR-1 or TRPV1 45°C + capsaicin+ acid• Aδ: VRL-1 or TRPV2 ↑ threshold, 52°C, not capsaicin• TRP channel family: resembles voltage gated K+ / cyclic
nucleotide gated• Influx of Na+ and Ca2+ initiates AP generation

Anterolateral System
Brainstem and thalamus in anterolateral/ventrolateral quadrant
of contralateral half of spinal cord
Cross midline
Second-order neurons in Rexed’slaminae 1 and 5
Gray matter of dorsal horn
Dorsolateral tract of Lissauer
Sensory neurons in dorsal root ganglia

Late
ral S
pin
oth
alam
icTr
act

Anterolateral vs. Dorsal Column Medial Lemniscal
• Medial lemniscus enter spinal cord, ipsilateral dorsal columnmedulla synapse on dorsal column nuclei cross midline ascend to contralateral thalamus
• Anterolateral system information crosses in spinal cord• Unilateral spinal cord lesion

Parallel Pain Pathways
Sensory discriminative: • Location, intensity, quality• VPL/ VPM
somatosensory cortex• Small receptive fields
Affective-motivational: • Unpleasant feeling,
fear and anxiety• Autonomic activation

Visceral Pain
Referred pain
Punctate

Pain from the Face
Discriminative: projections
to the contralateral ventral
posterior medial nucleus via
trigeminothalamic tract
primary and secondary
somatosensory cortex
Affective/motivational:
targets in reticular formation
and midbrain + midline
nuclei of thalamus which
supplies cingulate and
insular regions of cortex

Peripheral Sensitization
Sensitization: Neuronal sensitivityHyperalgesia: Slightly painfulSignificantly painful↑sensitivity to temperature
after a sunburnPeripheral sensitization: • “Inflammatory soup”• Vasodilation, swelling, histamine• Protect, promote healing and
guard against infection• ↑ blood flow and migration of white blood cells

Central Sensitization
Allodynia: Innocuous stimulus to the skin
• ↑ Activity in nociceptive afferents AP in dorsal horn neurons↑ pain sensitivity
Windup: ↑ Discharge rate of dorsal horn neurons from repeated ↓ ν activation of nociceptive afferents
• ∑ All slow synaptic potentials in dorsal horn neurons
sustained depolarization
• Voltage dependent L-type calcium channels
• Removing Mg block of NMDA receptor (glutamate)

Phantom Pain
Neuropathic pain:• Afferent fibers or central pathways damaged
Amputation of extremity:• Illusion that missing limb is still present• Functional reorganization of somatotopic maps
in primary somatosensory cortex• Neurons lost their original inputs from remote limb
tactile stimulation of other body parts

Placebo Effect
•Placebo - “I will please” •Physiological response following the administration
of a pharmacologically inert remedy
1. Sedative: >2/3 reportedly felt drowsy
2. Stimulant: Majority ↓ tired•1/3 headaches, dizziness, tingling extremities,
staggering gait
•Not “imagining” it•Acupuncture anesthesia, analgesia through hypnosis

Pain Modulation
• Electrical/ pharmacological stimulation midbrain
• Descending pain modulating pathways+ spinal trigeminal nucleus
• Regulated transmission of information to higher centers
• Periaqueductal gray of midbrain• Descending pathways arise from brainstem sites

Gate Theory of Pain
• Local interneurons b/w mechanoreceptiveafferent and neural circuit within dorsal horn nociceptive information to higher centers
• Rub the site of injury after stubbing a toe
• ↓ Sensational sharp pain by activating ↓ threshold mechanoreceptors