left atrial remodeling and function in advanced heart...
TRANSCRIPT

Left Atrial Remodeling and Function in Advanced Heart Failure With
Preserved or Reduced Ejection Fraction
Melenovsky et al: LA Dysfunction in HF
Vojtech Melenovsky, MD, PhD1,2; Seok-Jae Hwang, MD, PhD1;
Margaret M. Redfield1, MD; Rosita Zakeri, MBChB1; Grace Lin, MD1;
Barry A. Borlaug, MD1
1Division of Cardiovascular Diseases, Mayo Clinic, Rochester, MN
2 Department of Cardiology, Institute of Clinical and Experimental Medicine - IKEM, Prague,
Czech Republic
Correspondence to Vojtech Melenovsky, MD, PhD Department of Cardiology, IKEM Videnska 1958/9, Prague 4, 140 28, Czech Republic E-mail:[email protected] Fax: 420-261-362-486 Phone: 420-732-816-242
DOI: 10.1161/CIRCHEARTFAILURE.114.001667
Journal Subject codes: Heart failure:[110] Congestive, Hypertension:[18] Pulmonary circulation and disease, Heart failure:[11] Other heart failure
ttttalalalalalalal MMMMMMMedededededededicicicicicicicininininininineeeeeee -- IKIKKKKKK
yi
4 140 28 C h R bli
y, MD, PhD ioiollogy,,,,, IKIKIKIKIKEMEMEMEMEM
444 111404040 222888 CCC hhh RRR bbblilili
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on A
pril 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on A
pril 30, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
2
Abstract
Background—Left atrial (LA) structure and function are altered in most heart failure (HF)
patients, but there may be fundamental differences in LA properties between HF with preserved
(HFpEF) and reduced ejection fraction (HFrEF).
Methods and Results—198 HF patients (51% HFpEF, NYHA 3.1±0.7) and 40 HF-free controls
underwent catheterization, echocardiography and follow-up. Compared to controls, HF patients
had larger and more dysfunctional left atria. At identical mean LA pressure (20 vs 20 mmHg,
p=0.9), HFrEF patients had larger LA volumes (LAVI 50 vs 41 ml.m-2 p<0.001), while HFpEF
patients had higher LA peak pressures, lower LA minimal pressures, higher LA stiffness (0.79 vs
0.48 mmHg.ml-1, p<0.001), greater LA pulsatility (19 vs 13 mmHg, p<0.001) and higher wall
stress variations. Despite smaller LA volumes, better function and less mitral regurgitation,
HFpEF patients had more atrial fibrillation (AF: 42 vs 26%, p=0.02). LA dysfunction was
associated with increased pulmonary vascular resistance and right ventricular dysfunction in both
HF phenotypes. After a median follow-up of 350 days, 31 HFpEF and 28 HFrEF patients died.
LA function (total LA EF) was associated with lower mortality in HFpEF (HR 0.43, 95% CI 0.2-
0.9, p<0.05), but not in HFrEF.
Conclusions—HFrEF is characterized by greater eccentric LA remodeling, while HFpEF by
increased LA stiffness, which might contribute to greater AF burden. LA function is associated
with pulmonary vascular disease and right heart failure in both HF phenotypes, but is associated
with outcome more closely in HFpEF, supporting efforts to improve LA function in this cohort.
Key Words: heart failure; heart failure with preserved EF; left atrial function; atrial fibrillation;
pulmonary hypertension; right ventricle
ures, higher LAAAAAAA
mHgHgHggggg,,,,,,, p<p<p<pppp 0.0.00000 000000000000001111)1)11
D r
d
e y
Deeseee pppipp te ssssmamamamamallll ererererer LLLLLA A A A A vovovovovolulululuumememememes,s bbbeettttttererererer fffffunununununctctctc ioooioion nnnn ananannand dd dd leelelel ssssssssss mimmmm tr
d mmmmmororororo e eeee atatatttriririiialalalll fffffibii riririririlllllllll atatataatiooooonnn nn (A(A(A(A(AF:FF:FF 4444222 22 vsvsvsvsvs 222226%6%6%6%6%, p=p=p===0.0000 0202020202).)))) LLLLA AAAA
eaeaeaseseseddd pupupulmlmlmonononararary y y vavavascscsculululararar rrreeesisisistststananancecece aaandndnd rrrigigigghththt vvvenenentrtrtriiicucuculalalarrr dydydy
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

3
The left atrium modulates left ventricular (LV) filling by acting as an elastic reservoir, passive
conduit and active booster.1 Left atrial (LA) dysfunction and remodeling are commonly observed
in patients with heart failure (HF). Growing evidence suggests that LA dysfunction is an active
contributor to symptoms2-5 and to disease progression.3, 6, 7 HF-related LA remodeling is poorly
understood and it is not known if there are fundamental differences between HF patients with
preserved (HFpEF) or reduced LV ejection fraction (HFrEF), though prior studies suggest
greater adverse effects from loss of LA function in HFpEF compared to HFrEF.8
The LA also serves as a watershed between the LV and the pulmonary circulation,
buffering pressure and flow oscillations due to the cyclic nature of cardiac work. Impaired LA
function can thus impose greater hemodynamic stress on the pulmonary vasculature, promoting
remodeling and worsening pulmonary hypertension (PH), as observed in patients with mitral
stenosis.9,10 Increased pulmonary vascular resistance and stiffness may elevate right ventricular
(RV) afterload,11 driving further the progression to RV failure.12-15
We hypothesized that LA function is abnormal in patients with HF, that LA remodeling
differs between patients with HFrEF and similarly advanced HFpEF and that LA dysfunction is
associated with abnormal pulmonary vascular properties and RV dysfunction. To test this
hypothesis, we examined HFrEF and HFpEF patients undergoing invasive and noninvasive
hemodynamic assessment and compared them to HF-free controls to address the differences in
LA structure, function and to assess the impact of LA dysfunction on pulmonary vasculature,
right heart and clinical outcomes.
e of cardiac wowowwwww
ulmonononononononararararararary y yy y y y vavavavavavavascscscscscscscuuluu
i
e
i
rrrrrsesesesesening pppppululululu momomomomonananananaryryryryy hhhhhypypypypyperee tetetetetensn iooonn (P(P(P(P(PH)HHHH ,, asasasa ooooobserererererveveveveved ddd ininininin pppppataaa i
edddd pppppuluuluulmomomommonananann ryryryryry vvvvvasaa cucucucuculalalalaarrr r rererereresisisisisistststststananananancecececece ananananand dddd stststststifififififfnfnfnfnfnesesssssss mamamamamay yyyy eleelee evevevee atatatata eeeee
iiivivivingngng fffurururthththererer ttthehehe pppprororogrgrgrgg esesessisisiononon tttooo RVRVRV fffaiaiailululurerere.121212-22 15
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

4
Methods
Study subjects
Consecutive patients referred to Mayo Clinic (Rochester, MN) undergoing right heart
catheterization and echocardiography within a 48-hour window with sufficient raw data available
for detailed assessment (pressure waveforms and echocardiographic images) were identified. HF
was defined by cardiologist-adjudicated HF diagnosis (Framingham criteria) of >6 month
duration and elevated pulmonary artery wedge pressure (PAWP 15 mmHg at rest or 25 mmHg
at exercise). HFpEF and HFrEF were defined by LV EF 50% and <50%, respectively. Patients
with congenital heart disease, endocarditis, carcinoid, amyloid, constrictive, restrictive or
hypertrophic cardiomyopathy, intracardiac shunt (other than patent foramen ovale), high output
HF, non-Group II PH, mitral valve replacement, organic valvular disease, acute coronary
syndrome or hemodynamic instability were excluded.
Subjects with no cardiovascular disease other than Stage 1 arterial hypertension were
identified from patients undergoing preoperative evaluation, percutaneous closure of patent
foramen ovale, or evaluation for dyspnea with no identifiable cardiovascular cause. Past medical
history, medication use and contemporaneous laboratory data (±1 week) were abstracted from
the medical records. Significant CAD was defined as one or more 70% epicardial artery
stenosis or previous revascularization (angiography available in 28% controls, 82% of HFpEF
and 100% of HFrEF). For time-to-event analysis, patient vital status was determined using
outpatient records and the Social Security Death Index. Patients who underwent heart
transplantation or ventricular assist device insertion were censored as alive at the day of surgery.
The study was approved by Mayo Clinic institutional review board.
oid, constrictttttttiviviviivii
tentt fffffforororororororamamamamamammenenenenenenen ooooooov
,
y
y
PPPPPHHH,HH mititititi rararararal lll vavavavavalvlvlvlvlve e e e rerererereplplplplplacacaca emememememennntt, orororororgagagagaganininininicccc vavavavavalvulululululararararar dddddisisisisseaeaeaeaeasessss ,
ynananananamimmimimiccccc inininii stsstss abababababilillllitititi y wewewewewerrrerr eeeeexcxcxcxcxclululuuludededeededd.ddd
h hh nonono cccararardididiovovovasasascucuculalalarrr dididiseseseasasaseee otototheheherrr thththananan SSStatatagegegeg 111 aaartrtrterereriaiaialll hyhyhy
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
5
Assessment of Hemodynamics and Cardiac function
Right heart catheterization was performed in the supine position via the jugular or femoral vein
using a balloon-tipped catheter as previously described.16 Right atrial (RA), RV, pulmonary
artery (PA) pressures and PA wedge pressure (PAWP) were determined at end-expiration. All
atrial waveforms were visually inspected by an experienced cardiologist blinded to clinical data
and group allocation to determine minimal, maximal, v wave and a wave pressures within one
cardiac cycle (Figure 1). Transpulmonary gradient (TPG) was calculated as PA mean-PAWP
pressure, pulmonary vascular resistance (PVR) was calculated as TPG/cardiac output and PA
compliance was calculated as stroke volume/PA pulse pressure.
Two-dimensional and Doppler echocardiography was performed according to ASE
guidelines17 by experienced sonographers and cardiologists. Cardiac output was derived from
heart rate, LV outflow tract diameter and pulsed Doppler time-velocity integral. LV mass was
calculated using the Devereux formula5. Diastolic function was assessed by measurements of
transmitral flow velocities (E and A), E-wave deceleration, mitral annulus tissue velocities in
early and late diastole (E´ and A´, average of septal and lateral) using pulsed Doppler
echocardiography. Diastolic dysfunction was graded as described previously18. Valve
regurgitations were quantified according established guidelines19. LV EF was determined by the
modified Quinones formula that corrects for endocardial echo dropouts and image
foreshortening.20
Apical 4-chamber views were reviewed off-line to measure maximal LA volume (frame
prior to mitral valve opening), diastasis LA volume (frame prior to LA contraction) and minimal
LA volume using area-length method. Global and reservoir LA function was characterized by
total LA EF7, LA conduit function was characterized by passive LA EF and contractile function
perfrfrfrfrfrfrfororororororormememememememed d ddddd acacaaaaa c
w
a
e m
eeeeeriririririenced dddd sososososonononononogrgrgrgrgraaaaaphphphphphererererers ssss ananana d d d dd cac rdrrdiooooololololologigigigig stststststs...a CaCaCaCaCarddddiaiaiaiaiac cc cc ouououououtptptptptpututututut w
owwwww tttttrarararar ctctctctct dddddiiamamamamameteteteeter aaaandndndndnd pppppulululululsesesesesed dddd DoDoDoDoDopppppppppplelelelelerrr rr titititt mememememe-v-vvvvelololololocicicicicitytytytyty iintntntnn egegegegegrarr
eee DDDevevevererereueueuxxx fofoformrmrmulululaaa55555. DiDiDiasasastototolililiccc fufufuncncnctititiononon wwwasasas aaasssssseeessssssededed bbbyyy mmm
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

6
was characterized by active LA EF (Figure 1).21 Atrial function was also assessed by LA
function index (LAFI), which normalizes function to stroke volume and is rhythm-independent.3
Operant LA diastolic stiffness was approximated as the slope of linear regression of minimal and
maximal LA pressure-volume coordinates (Figure 1).22, 23 Meridional LA wall stress was
calculated from maximal to minimal LA volume and pressure using established formulas24,
assuming atrial wall thickness of 0.2 cm.25 RV function was assessed as previously26 by tracing
the RV endocardium in the apical 4-chamber view in systole and diastole to obtain fractional
area change (RV FAC %). The right atrial endocardium was tracked in the frame prior to
tricuspid valve opening in order to obtain maximal RA volume using the area-length method.27
Statistical Methods
Data were analyzed using JMP10 (SAS Institute Inc., Cary, NC). Distributions of continuous
variables were visually assessed for normality and summary data in the tables are reported as
mean (standard deviation) or median (25th-75th interquartile range). Between-group differences
were compared by ANOVA with Tukey post-hoc test, 2x2 ANOVA or 2 tests as appropriate.
Univariate and multivariate Cox proportional hazard model were used to examine the impact of
LA function on outcome. To allow comparisons, parameters describing LA function were z-
standardized in individual subgroups. Graphs represent mean±SE.
Results
Clinical characteristics of controls (n=40) and both HF groups (HFpEF: n=101, HFrEF: n=97)
are summarized in Table 1. Both HF groups were highly symptomatic (74% NYHA III-IV) with
80% of chronic diuretic use. Similar to prior studies28, HFpEF patients were slightly older,
sing gggggg the areaa-l-l-l-lllleneeeeee
d n
ally assessed for normality and summary data in the table
d uusisisisisingngngngn JJJJMPMPMPMPMP10101000 (((SAAAAASSSS Innnnnstststststitititititutututututee e InInInInnc.cccc , CaCaCaCaCaryryryryry, NCNCNCNCNC).)) DDDDDisisisisi trtrrrribibbbbututututioioiooon
aaallllllyyy asasasseseses ssssssededed fffororor nnnororormamamalililitytytyyy aaandndnd sssumumummmmamamaryryryyy dddatatata a a ininin ttthehehe tttababablelele
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

7
more likely to be women, more obese and more often in atrial fibrillation (AF). Prevalence of
CAD, diabetes and renal dysfunction was similar. HFpEF patients had higher systemic blood
pressure, cardiac output, LV EF and transmitral flow velocities, but smaller LV size, LV mass
and mitral regurgitation grade compared to HFrEF (Table 2).
LA structure and function in HFpEF vs HFrEF
Compared to controls, patients with HFrEF and HFpEF displayed LA dilatation, coupled with
reduced LA active contractile, reservoir and conduit functions (Table 2 and Figure 2). Patients
with HFpEF displayed greater LA stiffness while HFrEF patients displayed more eccentric LA
remodeling (Figure 2). At similar mean LA pressure (Table 2), patients with HFrEF had larger
LA volumes and more depressed LA systolic function than HFpEF. In contrast, patients with
HFpEF were characterized by higher maximal LA pressure (v-wave), lower minimal LA
pressures and increased LA stiffness (Table 2), with a steeper, leftward-shifted LA diastolic
pressure-volume relationship (Figure 2). Differences in LA volume and stiffness between HFpEF
and HFrEF persisted after adjustments to gender, age, body size and mass, AF or mitral
regurgitation grade (adjusted p-values <0.02).
Left atrial pulsatility (LA max-min pressure) and wall stress variation was higher in
HFpEF compared to HFrEF (Table 2). LA function curves (preload-stroke volume plots) were
shallower in both HFpEF and HFrEF compared to controls, indicating LA contractile
dysfunction regardless of LA geometry (Figure 3). LA functional index (LAFI) and A’ mitral
annular velocities were also more reduced in HFrEF than in HFpEF or controls (Table 2).
The presence of AF was associated with more severe LA dilatation, lower total LA EF
and higher LA stiffness, particularly in HFpEF group (Supplemental Figure). Both atrial rhythm
nts displayed mmmmmmmo
patitiiiiiienenenenenenentstststststts wiwiwiwiwiwiwiththththththth HH
m a
a w
f
morororororee eee deprrrresesesesessesesesesed d dd d LALALALALA sssssysysysysystototototolilll c cccc fffunncctiooooon n n nn ththtththanananaan HHHHHFpFFFF EFEFEFEFEF.... InInInInIn cccccononononontrttt aff
acttttterererererizizizii ededededed bbbbbyy yyy hihihihihighghghghherereree mmmmmaxaxaxaxaximimimimimalalalaa LALALALALA ppppprererereressssssssssurururuu eeeee (v(vvv(v-w-w-w-w-wavaaaa e)ee)ee , lololololowww
aaaseseseddd LALALA ssstititiffffffnenenessssss (((((TaTaTablblbleee 2)2)2), wiwiwiththth aaa sssteteteepepeppererer, leleleftftftwawawardrdrd-s-s-shihihifff
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

8
and HF phenotype impacted LA structure and function as shown by factorial analysis. LA
volume and stiffness increased, while total LA EF decreased with worsening NYHA class
(Figure 4). Mitral regurgitation had greater effects in HFpEF than HFrEF, with higher peak LA
pressure (LA v-wave) and greater LA wall stress variation with increasing mitral regurgitation in
HFpEF compared to HFrEF (Figure 3).
The Left Atrium and Pulmonary Artery-Right Heart Function
Pulmonary hypertension was common in HF patients (82% HFpEF, 79% HFpEF), due to
combination of elevated PAWP and increased transpulmonary gradient (Table 3). Mean PA
pressure, transpulmonary gradient, pulmonary vascular resistance (PVR) and pulmonary arterial
compliance (PAC) were similarly increased in both HF groups (Table 3), while PA pulse
pressure was higher in HFpEF. Global left atrial function (total LA EF) correlated inversely with
PVR and positively with PAC in both HF groups, but not in controls, and the slope the
relationship was similar between HFpEF and HFrEF (Figure 5). Similarly, LA stiffness
correlated with PAC in HFpEF and HFrEF (r=-0.35 and r=-0.41, both p<0.001), but only weakly
with PVR in HFpEF (r=0.23, p=0.03) and was unrelated to PVR in HFrEF (r=0.12, p=0.3). LA
volume was unrelated to PVR or PAC in both HF phenotypes.
Both HFpEF and HFrEF patients displayed RV dilation, but RV systolic function was
somewhat lower in HFrEF. Global LA function (total LA EF) positively correlated with RV
function in HFpEF and HFrEF with similar slope (Figure 5).
y gradient (TTabababaabaa
ce (P(PPPPPPVRVRVRVRVRVRVR) ) )) ) )) ananananananand d d d d d d pupppp
e
y n
wwwwweeree e siiiiimimimimm lalll rlrlrlrlrly y yy y ininininincrcrcrcrcreaeaeaeaeasesesess d ddd ininin bbbooth hh h h HFHFHFHFHF ggggroroorooupuuuu s s s s (T(T(TT(Tababababablelelelele 33333),))))
innnnn HHHHHFpFppFpFpEFEFEFEFEF. GlGlGlGlGloboboboobalalalall lllllefefefeffttt t atatatatatriririririalalalalal fffunununununctctctcttioioiooion nnnn (t(t(t(t(totototototalalalalal LLLLLAAAAA EEEEEF)F)F)F)F) ccorororororrerereerelalaaaatett
yyy wwwititithhh PAPAPACCC ininin bbbototothhh HFHFHF gggrororoupupuppsss,, bububuttt nononottt ininin cccononontrtrtrolololsss, aaannn
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
9
Impact of LA dysfunction on prognosis
Over a median follow-up duration of 350 days (IQR: 82-870) there were 59 deaths (HFpEF=28,
HFrEF=31). Outcome was ascertained in 100% of HF subjects. In univariate Cox analysis,
reduced global and active LA function (total LA EF and active LA EF), increased LA volume
and AF were all associated with an increased risk of death in HFpEF, but not in HFrEF (Figure
6). In multivariate Cox model that included age and gender, known predictors of mortality in
HFpEF29, either total LA EF or active LA EF remained a significant predictor of death in HFpEF
(p=0.03 and p=0.05), while LAVI was no longer predictive (p=0.16). NT-pro-BNP levels were
not predictive of mortality in either HF group.
Discussion
This study examined LA structure and function in HF by combining invasive pressure and
noninvasive volume data while contrasting LA parameters in the two HF phenotypes. Compared
to controls, both HF types displayed abnormal LA size and function. The HFrEF group was
characterized by greater eccentric LA remodeling, while the HFpEF group was characterized by
increased LA stiffening and greater LA pressure pulsatility, indicating that higher wall stress
variations may contribute to greater burden of AF observed in HFpEF. In both groups, LA
function was associated with pulmonary vascular disease and right heart failure. While global
LA function was less impaired in HFpEF than HFrEF, LA dysfunction was more strongly
associated with mortality in this cohort, suggesting greater vulnerability to loss of LA function in
HFpEF. These data highlight the importance of atrial dysfunction in HF and suggest that
strategies to optimize LA function and/or to prevent its deterioration may mitigate progression of
e i
e data while contrasting LA parameters in the two HF pheno
DiDiDiDD scccccusu siononn
ed ddd LALALALALA ssssstrrrucucucucuctututuuurerererre aaaaandndndndn ffunununununctctctctctioioiooion nn inininini HHHHHFFFFF bybybybyby cccccomommmmbibibibibinininininingngnnn iiiiinvnvnvnvnvasasaasa i
e dddatatataaa whwhwhililileee cococontntntrararastststinining g g g LALALA ppparararamamametetetererersss ininin ttthehehe tttwowowo HHHFFF phphphenenenooo
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

10
pulmonary vascular and right heart dysfunction while improving outcomes in HF patients and
particularly in HFpEF.
Few studies have compared LA structure/function in HFpEF and HFrEF, and none of
have reported associations between LA function and outcome.6, 30 31 In an echocardiographic
study, Triposkiadis et al compared LA remodeling in HFpEF and HFrEF and found more
eccentric LA remodeling in HFrEF group, similarly to the current data.31 In a smaller sample,
Kurt et al reported that HFpEF patients had LA enlargement, reduced LA function and increased
LA stiffness compared to controls, but in contrast to the current study, LA stiffness was not as
high in HFpEF as in HFrEF.30 However, the Kurt study measured only mean PAWP rather than
peak and minimal LA pressures, and the authors estimated LA stiffness simply as the ratio of
mean PAWP to LA systolic strain, in contrast to the more robust methods used in the current
study incorporating maximal and minimal LA pressure-volume coordinates. The current
observation of smaller and stiffer left atrium in HFpEF as compared to HFrEF is congruent with
known structure-function differences noted at the left ventricular level, supporting the notions
that HFpEF and HFrEF represent two distinct pathophysiological entities32 and that the systemic
processes favoring stiffening in all cardiac chambers, such as microvascular inflammation or
impaired nitric oxide availability, may contribute to the pathophysiology of HFpEF.33
Two overarching mechanisms are thought to drive the development of atrial dysfunction
in HF - chronic changes in loading (increased atrial preload and afterload) and the loss of normal
atrial electrical activity.10, 34 Experimental and limited human studies22, 35 have illustrated that
with increased preload, LA contractility initially rises22, 35, 36 but later declines, coinciding with
adverse changes in remodeling, apoptosis, myosin isoform expression, collagen matrix turnover
and reduced intrinsic contractility.36-38 As shown in the current data at the macro level, this
ed only meann PPPPPPPd
A stiiffffffffffffffnenenenenenenesssssssssssss sssssssimimimimimimimppplpp
A
g t
l i
A syyyyystoliccccc ssssstrtrtrtrtraiaiaiaiain,n,n,n,n, iiiiin n n n cococococontntntntntrararaststststst tot ttheheeee mmmmmorororororee eee rororoobubububb stt mmmmmetetetetethohohoohodsdsdsdsds uuuuus
g mamamamamaxixixiiximamamamamal llll ananananandd ddd mimimimiminininininimamamamamal llll LALALALALA prrprrresesesesssususususurerererere-v-v-vv-volooloo umumumumumeeeee cococcc ororororordidididinananananat
lllererer aaandndnd ssstititiffffffererer lllefefefttt atatatriririumumum iiinnn HFHFHFpEpEpEp FFF asasas cccomomompapaparerereddd tototo HHHFrFrFrEFEFEF iii
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
11
translates to an increase in atrial wall stiffness reflected by the steeper and upward-shifted
pressure-volume relationship, predominantly in HFpEF and by a shift to the larger LA volumes,
predominantly in HFrEF. Despite the difference in LA volumes, we noted that LA function
curves (preload-stroke volume relations) were similarly flattened in HFrEF and HFpEF,
indicating presence of intrinsic LA dysfunction. In HFpEF, the increase of LA stroke volume by
preload recruitment (Frank-Starling mechanism) can be blunted by increased LA stiffness, as
recently suggested.39
As shown in the current study, loss of normal atrial electrical activity in HF patients with
AF is associated with more pronounced LA dilatation, systolic dysfunction and passive stiffening
(Supplemental Figure). However, HF patients in sinus rhythm also demonstrated LA systolic
impairment (active LA EF reduced by 37% in HFpEF and 54% in HFrEF), confirming that atrial
mechanical dysfunction in HF is not restricted to patients with AF.40-42 At similar mean LA
pressures, HFpEF patients demonstrated larger LA pressure pulsatility43 and greater LA wall
stress variation. We speculate that this may contribute to the higher prevalence of AF noted in
HFpEF compared to HFrEF, despite smaller LA volumes, similar LA pressures, and similar HF
severity and mortality risk.44
The differences in LA structure-function also appear to influence how the LA copes with
mitral regurgitation. With increasing regurgitation, LA pressure and wall stress increases much
more steeply in HFpEF than in HFrEF, which may promote stretch-mediated atrial ectopy that
plays a role in initiation of AF.34 While LA function was less impaired in HFpEF than HFrEF, its
association with outcome was more pronounced, congruent with previous reports regarding the
differential impact of AF on outcomes in HFpEF or HFrEF.8 The current data provide insight
into the mechanisms by which this HF phenotype-specific difference may originate.
ysfunction andndddddd p
m alsso o o o o o o dedededededed momomomomomomonsnsnsnsnsnsnstrtra
L f
c s
p
LLLLLA AAAA EF redededededucuuuu ededededed bbbbby y y y y 3737373737%%%%% ininnin HHHHHFpEppEF ananananand dddd 5454545454%%%%% ininiii HHHHHFrFrFrFrFrEFEFEFEFEF),),),)) ccccconononoonf
ctiononononon iiin nnnn HFHFHFHFHF iiisssss nonnn t tttt rereeerestssss riiiiictctctctctededededed tttooooo papapapapatititititienenenenentststststs wwwwwitiitii hh hhh AFAFAFAFAF.40-40404040 422 AAAAAtt s
pppatatatieieientntntsss dededemomomonsnsnstrtrtratatatededed lllararargegegeg rrr LALALA ppprereressssssururureee pupupulslslsatatatilililititityyyy43 aaandndnd
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

12
Previous studies have suggested a potential association between atrial dysfunction and
pulmonary hemodynamics, but these non-invasive studies were not able to discriminate between
the impact of intrinsic LA properties from passive LA pressure elevation due to volume
overload.9, 30, 45 We observed that impaired LA global systolic function (quantified by total LA
EF)7 correlated with increased PVR and reduced PAC measured directly by cardiac
catheterization. Impaired diastolic LA function (LA stiffness) was associated with reduced PAC,
a measure of oscillatory PA load. The relations between LA functional properties and pulmonary
vasculature were similar between HFpEF and HFrEF. The current data strongly implicate that
LA dysfunction belongs among the mediators of pulmonary vascular disease in HF.11 By having
impact in PA hemodynamics, LA dysfunction can also indirectly influence RV function and
contribute to progression towards biventricular failure with poor prognosis.26, 46
These data suggest that maintenance or restoration of normal LA function may help to
“protect” the pulmonary vasculature, and in doing so, to prevent deterioration of the right heart.
Further studies are required to assess whether this approach is beneficial. Conversely, these data
also indicate that LA interventions that might increase stiffness or impair systolic function might
have unintended adverse consequences on the pulmonary vasculature. Left atrial wall scarring
and volume reductions after repeated radiofrequency AF ablations have recently been associated
with development of pulmonary hypertension,47 and removal of LA appendage, the most
contractile and compliant part of the left atrium, increases atrial stiffness and reduces atrial
performance.37 As LA interventions such as device closure and ablation become more widely
utilized in HF patients, the potential for deleterious effects on pulmonary vascular-right heart
function should be considered and evaluated in future trials.
cular disease ininininininin
ctlyyy iiiiiinfnfnfnfnfnfnfllllllueueueueueueuencncncncncncnce e eeeee R
s
s
n o
ssssssioioioioion towawawawaardrdrdrr s s s s bibibibibivevveveventntntntntririririricucucucuculalaalar rrrr fafafailuruure wiwiwiwiwiththththth pppppoooooooor r r r r prpppp ogogogogognononononosiisisis.s.s.s.s.26, 46
suggggggegegegegeststststt ttttthahahahahatt mamamamamainiii tetetetetenanaanaannncnn e eeee orororoor rrrreseesee tttttorororrratatatatatioioioioionnn nn ofofofofof nnnnnororooro mamamamamal llll LALALALALA fffunununununccc
nnnarararyyy vavavascscsculululatatatururure,e,e, aaandndnd iiinnn dododoininingggg sososo, tototo pppprerereveveventntnt dddeeeteteteriririorororatatatioioionnn ooo
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

13
Limitations
This study is retrospective, observational and is influenced by referral bias. All subjects
underwent cardiac catheterization, so this sample is generally limited to patients with more
advanced HF and may not be applicable to the entire HF population. The use of PAWP for
inclusion into HF group assured that the patients studied truly had HF, but because patients with
less advanced HF may have normal PAWP at rest, these results may not apply to HF patients
with earlier stage disease. The primary cause of ventricular dysfunction in HF patients could not
be assessed in this retrospective study. The control group was drawn from consecutive patients
referred for invasive assessment, so by virtue of being referred for cardiac catheterization, this is
not representative of completely healthy comparator group. However, this invasive study would
not be feasible in healthy volunteers. Hemodynamic and echocardiographic data were not
acquired simultaneously, but both occurred within a 48 hour time frame. The relations between
HF phenotype and atrial characteristics were studied cross-sectionally so all inferences about
causality are hypothesis-generating. Despite age-adjusted comparisons, differences in age
between groups may confound the conclusions. Data on quality of life were not systematically
recorded and all measures were performed at rest and in the supine position, so we were unable
to address the relation of our findings to exertional symptoms or quality of life.
LA pressures were not measured directly, but assessed by PAWP, which is dampened
compared to directly measures LA pressures, leading to systematic underestimation of diastolic
LA stiffness and pulsatility, though this underestimation was uniform between HF groups and
controls. The number of enrolled subjects and deaths was moderate, which both prevented
multivariable analysis. Thus, further work is needed to confirm the univariate relationships we
observed between LA size / function and outcomes, which could be potentially cofounded by
for cardiac cathththhthhhee
weveeeeeeer,r,r,r,r,r,r, ttttttthihihihihihihis s s s s s s inininininininvavavvvvv
c
o r
hhhhheeaeee lthy vovovovovoluuuuuntntntntnteeeeeeeeeersrsrsrsrs. HeHeHeHeHemomomomomodydd nannamimimimimic cccc ananananand d d dd ececececechohh cacacacacardrdrdrdrdiooioioi grgrgrgrgrapapapapaphihhhh c
ouslslslslsly,y,yy,y, bbbbbututuutu bbbbbotototoo h hhhh ocooo cucucucucurrrrrrrredededee wwwwwititititithihihihh nnnnn aaaaa 4444488888 hohohohohoururururur tttttimimimmme ee frfrfrfrframamamamame.e TTTTThehehehh r
aaatrtrtriaiaialll chchcharararacacacteteteririristststicicicsss wewewererere ssstututudididiededed cccrororossssss-s-s-sececectititionononalalallylylyy sssooo alalallll
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
14
other intermediary factors. However, follow-up was complete in 100% of patients, enhancing
confidence in our results.
In conclusion, the current data provide insight into pathophysiology of LA dysfunction
and pulmonary hypertension in HF. The LA remodeling in HFpEF and HFrEF differs, with more
dilation and systolic dysfunction in HFrEF and with increased stiffness, pulsatility and
predilection for AF in HFpEF. Restoration of LA mechanical function may have favorable
effects on pulmonary vasculature and right heart, while processes and interventions that reduce
atrial contractility or adversely affect LA compliance may promote and exacerbate pulmonary
hypertension, leading to right heart dysfunction and increased risk of adverse outcomes,
especially in patients with HFpEF.
Sources of Funding
VM is supported by the Czech Ministry of Health (DRO institutional support IKEM 00023001;
IGA NT14050-3/2013 and NT14250-3/2013), by the Grant Agency of Czech Republic (15-
14200S), by the Czech Ministry of Education (MSMT-LK12052-KONTAKT II), by EU-funded
project CEVKOON (CZ.2.16/3.1.00/22126) and by the Fulbright Foundation.
Disclosures
None.
sed risk of aaaaaaaddddd
y the Czech Ministry of Health (DRO institutional support I
SoSoSoSoSourururururcececececessss ofo FFFununununundidddd ngnggg
yyy tthehehe CCCzezechchchhh MMMMMinininii isisisi trtrt yy ofofoff HeHHeHH alalalllththththh ((((DRDRDRDRDROOOOO inininststtitititiituttutttioioioii nanallll susupppporortt II
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

15
References
1. Braunwald E, Frahm CJ. Studies on starling's law of the heart: IV. Observations on the hemodynamic functions of the left atrium in man. Circulation. 1961;24:633-642.
2. Donal E, Raud-Raynier P, De Place C, Gervais R, Rosier A, Roulaud M, Ingels A, Carre F, Daubert JC, Denjean A. Resting echocardiographic assessments of left atrial function and filling pressure interest in the understanding of exercise capacity in patients with chronic congestive heart failure. J Am Soc of Echocardiogr. 2008;21:703-710.
3. Welles CC, Ku IA, Kwan DM, Whooley MA, Schiller NB, Turakhia MP. Left atrial function predicts heart failure hospitalization in subjects with preserved ejection fraction and coronary heart disease: Longitudinal data from the heart and soul study. J Am Coll Cardiol. 2012;59:673-680.
4. Tan YT, Wenzelburger F, Lee E, Nightingale P, Heatlie G, Leyva F, Sanderson JE. Reduced left atrial function on exercise in patients with heart failure and normal ejection fraction. Heart. 2010;96:1017-1023.
5. Melenovsky V, Borlaug BA, Rosen B, Hay I, Ferruci L, Morell CH, Lakatta EG, Najjar SS, Kass DA. Cardiovascular features of heart failure with preserved ejection fraction versus nonfailing hypertensive left ventricular hypertrophy in the urban Baltimore community: The role of atrial remodeling/dysfunction. J Am Coll Cardiol. 2007;49:198-207.
6. Gottdiener JS, Kitzman DW, Aurigemma GP, Arnold AM, Manolio TA. Left atrial volume, geometry, and function in systolic and diastolic heart failure of persons > or =65 years of age (the cardiovascular health study). Am J Cardiol. 2006;97:83-89.
7. Hoit BD. Left atrial size and function: Role in prognosis. J Am Coll Cardiol. 2014;63:493-505.
8. Olsson LG, Swedberg K, Ducharme A, Granger CB, Michelson EL, McMurray JJ, Puu M, Yusuf S, Pfeffer MA. Atrial fibrillation and risk of clinical events in chronic heart failure with and without left ventricular systolic dysfunction: Results from the candesartan in heart failure-assessment of reduction in mortality and morbidity (CHARM) program. J Am Coll Cardiol. 2006;47:1997-2004.
9. Schwammenthal E, Vered Z, Agranat O, Kaplinsky E, Rabinowitz B, Feinberg MS. Impact of atrioventricular compliance on pulmonary artery pressure in mitral stenosis: An exercise echocardiographic study. Circulation. 2000;102:2378-2384.
10. Stefanadis C, Dernellis J, Stratos C, Tsiamis E, Vlachopoulos C, Toutouzas K, Lambrou S, Pitsavos C, Toutouzas P. Effects of balloon mitral valvuloplasty on left atrial function in mitral stenosis as assessed by pressure-area relation. J Am Coll Cardiol. 1998;32:159-168.
11. Guazzi M, Borlaug BA. Pulmonary hypertension due to left heart disease. Circulation. 2012;126:975-990.
12. Butler J, Chomsky DB, Wilson JR. Pulmonary hypertension and exercise intolerance in patients with heart failure. J Am Coll Cardiol. 1999;34:1802-1806.
13. Lam CS, Roger VL, Rodeheffer RJ, Borlaug BA, Enders FT, Redfield MM. Pulmonary hypertension in heart failure with preserved ejection fraction: A community-based study. J Am Coll Cardiol. 2009;53:1119-1126.
14. Tedford RJ, Hassoun PM, Mathai SC, Girgis RE, Russell SD, Thiemann DR, Cingolani OH, Mudd JO, Borlaug BA, Redfield MM, Lederer DJ, Kass DA. Pulmonary capillary
ttrororororororophphphphphphphy y yyyyy ininininininin tttttthehehehehehehe uuAm m mmmmm CoCoCoCoCoCoCollllllllllllll CCCCCCCararararararardididididididi
J om
L m
M
JSSSSS, KiKiKiKiKitztztztztzmamamamamann nn DW, Aurigemmaaa aa GP, Arrrnonnnn lddddd AM, Manoliommmeeete ry, andd ddd fufuncncnccnctititititiononononon iinnnnn sysyy toollic aand dddd dididiidiaaastotoolilic heheeararararart fafafafafailililili ururururre oofooo(((thththththe eeee cardrdrdddiooovvascssculararararar hheeeeealalalala ththththh ssssstututudyyy)).)) AAAAAmmm mm J CaCaCaC rdrdrdiiolll.ll 20000006;6;6;6;6 997:8883
Left atrial size aaaandndndnn functctction:nn:n RoRoRoRoRolele in prpppp ognosis. J Am-505. Swedbebebebebergrgrgrgrg KKKKK,,,,, DuDuDuDuDuchchchchcharararararmememememe AAAAA,,, , GrGrGrGrGrananananangegegegeer rr rr CBCBCBCBCB,,,,, MiMiMiMiMichchchchchelelelelelsososososon nnnn EL, M
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

16
wedge pressure augments right ventricular pulsatile loading. Circulation. 2012;125:289-297.
15. Dupont M, Mullens W, Skouri HN, Abrahams Z, Wu Y, Taylor DO, Starling RC, Tang WH. Prognostic role of pulmonary arterial capacitance in advanced heart failure. Circ Heart Fail. 2012;5:778-785.
16. Borlaug BA, Nishimura RA, Sorajja P, Lam CS, Redfield MM. Exercise hemodynamics enhance diagnosis of early heart failure with preserved ejection fraction. Circ Heart Fail. 2010;3:588-595.
17. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise J, Solomon S, Spencer KT, St John Sutton M, Stewart W. Recommendations for chamber quantification. Eur J Echocardiogr. 2006;7:79-108.
18. Redfield MM, Jacobsen SJ, Burnett JC, Jr., Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: Appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194-202.
19. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A, Weissman NJ. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777-802.
20. Quinones MA, Waggoner AD, Reduto LA, Nelson JG, Young JB, Winters WL, Jr., Ribeiro LG, Miller RR. A new, simplified and accurate method for determining ejection fraction with two-dimensional echocardiography. Circulation. 1981;64:744-753.
21. Rosca M, Lancellotti P, Popescu BA, Pierard LA. Left atrial function: Pathophysiology, echocardiographic assessment, and clinical applications. Heart. 2011;97:1982-1989.
22. Dernellis JM, Stefanadis CI, Zacharoulis AA, Toutouzas PK. Left atrial mechanical adaptation to long-standing hemodynamic loads based on pressure-volume relations. Am J Cardiol. 1998;81:1138-1143.
23. Barbier P, Solomon SB, Schiller NB, Glantz SA. Left atrial relaxation and left ventricular systolic function determine left atrial reservoir function. Circulation. 1999;100:427-436.
24. St John Sutton MG, Plappert TA, Hirshfeld JW, Reichek N. Assessment of left ventricular mechanics in patients with asymptomatic aortic regurgitation: A two-dimensional echocardiographic study. Circulation. 1984;69:259-268.
25. Beinart R, Abbara S, Blum A, Ferencik M, Heist K, Ruskin J, Mansour M. Left atrial wall thickness variability measured by ct scans in patients undergoing pulmonary vein isolation. J Cardiovasc Electrophysiol. 2011;22:1232-1236.
26. Melenovsky V, Hwang SJ, Lin G, Redfield MM, Borlaug BA. Right heart dysfunction in heart failure with preserved ejection fraction. Eur Heart J. 2014; 35:3452-3462.
27. Peluso D, Badano LP, Muraru D, Dal Bianco L, Cucchini U, Kocabay G, Kovacs A, Casablanca S, Iliceto S. Right atrial size and function assessed with three-dimensional and speckle-tracking echocardiography in 200 healthy volunteers. Eur Heart J Cardiovasc Imaging. 2013;14:1106-14.
28. Lee DS, Gona P, Vasan RS, Larson MG, Benjamin EJ, Wang TJ, Tu JV, Levy D. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: Insights from the Framingham Heart Study of the National Heart, Lung, and Blood Institute. Circulation. 2009;119:3070-3077.
the severity ofofoooooeeeeechchchchchchchocococococococararararararardididididididiogogogogogogogrrrrararr phphphphphphph
MA, Waggoner AD, Reduto LA, Nelson JG, Young JB, We
h 4a Pr
M ao long standing hemodynamic loads based on pressure volum
MA,A,A,A,A, WWWWWagagagagaggooooonennnn r AD, Reduto LLLLLA,AAAA Nelson JG,GGGG Young JB, WMiMiMiMM ller RRRRRR.R.R.R.R. AAAAA nnnnnewewewwew,,,,, sisisisisimpmpmpmpm liiififififf edee aand dd dd acacacacaccucucucucuraraarrateteetee mmmmmetetetetethohohohohod dddd fofofofofor rr r r dededededete
h twtwtwtwtwo-dimeensn iooonnal l ll l eeece hocacaardiiioograrraphhhhhy.y.y.y.y. CCCirrccculaaatttionononnn. 19999981818188 ;;644:74ancececececellllllll otottotottititititi PPPPP, PoPoPoPPopppepp scscscsccuuu BABABABABA, PiPiPiPiPierereree ararararard ddd LALALALALA. LeLeLeLeLeftftftftft aaaatrtrttrt iaiaiaiaial llll fffffununuuu ctctctcc ioioiiion:n:n:n:n: Pfffffffraphic assessmentntntt, ,, ananananand d d dd clclcclc inininininiiicacc l ll l apapappapplplplplpliciicii ataatattioioionsnsnsnsns..... Heart. 2011;97:
MMM, StStStefefefanananadadadisisis CCCIII, ZZZacacachahaharororoulululisisis AAAAAA, ToToToutututouououzazazasss PKPKPK. LeLeLeftftft aaaoo lololongng-s-statttat ndndndddininini gg hehehehh momodydydydd nanamimimiiicc lolololl adadadss babababb seseddddd onon ppreressssurure-e-vovolululumm
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
17
29. Lam CS, Carson PE, Anand IS, Rector TS, Kuskowski M, Komajda M, McKelvie RS, McMurray JJ, Zile MR, Massie BM, Kitzman DW. Sex differences in clinical characteristics and outcomes in elderly patients with heart failure and preserved ejection fraction: The irbesartan in heart failure with preserved ejection fraction (I-PRESERVE) trial. Circ Heart Fail. 2012;5:571-578.
30. Kurt M, Wang J, Torre-Amione G, Nagueh SF. Left atrial function in diastolic heart failure. Circ Cardiovasc Imaging. 2009;2:10-15.
31. Triposkiadis F, Harbas C, Kelepeshis G, Sitafidis G, Skoularigis J, Demopoulos V, Tsilimingas N. Left atrial remodeling in patients younger than 70 years with diastolic and systolic heart failure. J Am Soc Echocardiogr. 2007;20:177-185.
32. Borlaug BA, Redfield MM. Diastolic and systolic heart failure are distinct phenotypes within the heart failure spectrum. Circulation. 2011;123:2006-2013.
33. Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013;62:263-271.
34. Aldhoon B, Melenovsky V, Peichl P, Kautzner J. New insights into mechanisms of atrial fibrillation. Phys Res. 2010;59:1-12.
35. Phan TT, Abozguia K, Shivu GN, Ahmed I, Leyva F, Patel K, Frenneaux M. Increased atrial contribution to left ventricular filling compensates for impaired early filling during exercise in heart failure with preserved ejection fraction. J Card Fail. 2009;15:890-897.
36. Kono T, Sabbah HN, Rosman H, Alam M, Stein PD, Goldstein S. Left atrial contribution to ventricular filling during the course of evolving heart failure. Circulation. 1992;86:1317-1322.
37. Hoit BD, Shao Y, Gabel M. Left atrial systolic and diastolic function accompanying chronic rapid pacing-induced atrial failure. Am J Physiol. 1998;275:H183-189.
38. Khan A, Moe GW, Nili N, Rezaei E, Eskandarian M, Butany J, Strauss BH. The cardiac atria are chambers of active remodeling and dynamic collagen turnover during evolving heart failure. J Am Coll Cardiol. 2004;43:68-76.
39. Obokata M, Negishi K, Kurosawa K, Arima H, Tateno R, Ui G, Tange S, Arai M, Kurabayashi M. Incremental diagnostic value of LA strain with leg lifts in heart failure with preserved ejection fraction. JACC. Cardiovascular imaging. 2013;6:749-58.
40. Plehn JF, Southworth J, Cornwell GG, 3rd. Brief report: Atrial systolic failure in primary amyloidosis. New Engl J Med. 1992;327:1570-1573.
41. Gupta DK, Shah AM, Giugliano RP, Ruff CT, Antman EM, Grip LT, Deenadayalu N, Hoffman E, Patel I, Shi M, Mercuri M, Mitrovic V, Braunwald E, Solomon SD. Left atrial structure and function in atrial fibrillation: ENGAGE AF-TIMI 48. Eur Heart J. 2014;35:1457-1465.
42. Santos AB, Kraigher-Krainer E, Gupta DK, Claggett B, Zile MR, Pieske B, Voors AA, Lefkowitz M, Bransford T, Shi V, Packer M, McMurray JJ, Shah AM, Solomon SD. Impaired left atrial function in heart failure with preserved ejection fraction. Eur J Heart Fail. 2014;16:1096-1103.
43. Shibata S, Hastings JL, Prasad A, Fu Q, Bhella PS, Pacini E, Krainski F, Palmer MD, Zhang R, Levine BD. Congestive heart failure with preserved ejection fraction is associated with severely impaired dynamic Starling mechanism. J Appl Physiol. 2011;110:964-971.
PPPPPPPatatatatatatatelelelelelelel KKKKKKK, , ,,,,, FrFrFrFrFrFrFrenenenenenenennenennnnn aaaaaaafor imimimimimimimpapapapapapapaiririririririrededededededed eeea
eart failure with preserved j ti f ti J C d Fail. 200dt
r i
h od 3oe GW Nili N Rezaei E Eskandarian M Butany J Strauss
eararrrrt ttt t fafafafafaililiililuruuuu e eee e with preserved ejeccccctitititition fraction. JJJJJ Card Fail. 200dbbbbbahahahahah HN,NNNN RRRRRosososososmamamamaman nnnn H,H,H,H,H, AAAAAlalalalaam m m mm M,MMMM SSSteiiiiin n n nn PDPDPDPDPD, ,, GoGoGoGooldldldll steieieieiein nn nn S.SSSS LLLLLefefefefefttttt atrrrrr fffffiliiii ling duruuringgg thee e coursesee of f evvvoolvivivivivingngngngng hheeaaart faffaillllluuruuu e. CCCCCirrrcculalaati7-1-1-1-1-132323232322.222.2. hao Y, Gabel MMMM.... LeLeLeLeLeftftftftft aaatrtrtrtrt iaiaial sysysyyystststststolololololiciccc aaaandndndndnd dddddiastolic functiod dd papapacicicingngngg-i-i-indndnducucucededed aaatrtrtriaiaialll fafafailililururureee. AAAmmm JJJ PhPhPhysysysyy ioioiolll. 1119999998;8;8;;2727275:5:5:H1H1H1838383ooee GWGWGW NiNiNiNiNililililili NNNNN RReReRR zazaeieieiii EEEEE EsEEsEE kakakakk ndndndddaariririianan MMMMM BuBBuBB ttatttanyny JJJJJ StStStS raraususss
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
18
44. Rosenberg MA, Manning WJ. Diastolic dysfunction and risk of atrial fibrillation: A mechanistic appraisal. Circulation. 2012;126:2353-2362.
45. Mehta S, Charbonneau F, Fitchett DH, Marpole DG, Patton R, Sniderman AD. The clinical consequences of a stiff left atrium. Am Heart J. 1991;122:1184-1191.
46. Ghio S, Gavazzi A, Campana C, Inserra C, Klersy C, Sebastiani R, Arbustini E, Recusani F, Tavazzi L. Independent and additive prognostic value of right ventricular systolic function and pulmonary artery pressure in patients with chronic heart failure. J Am Coll Cardiol. 2001;37:183-188.
47. Gibson DN, Di Biase L, Mohanty P, Patel JD, Bai R, Sanchez J, Burkhardt JD, Heywood JT, Johnson AD, Rubenson DS, Horton R, Gallinghouse GJ, Beheiry S, Curtis GP, Cohen DN, Lee MY, Smith MR, Gopinath D, Lewis WR, Natale A. Stiff left atrial syndrome after catheter ablation for atrial fibrillation: Clinical characterization, prevalence, and predictors. Heart Rhythm. 2011;8:1364-1371.
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Table 1. Clinical and laboratory characteristics
Controls
n = 40
HFpEF
n=101
HFrEF
n=97
p
Age, years 63 ± 7 71 ± 10 * 61 ± 13 † < 0.0001
Female gender 53 % 58% 20% *† < 0.0001
BMI, kg.m-2 29 ± 5.8 34 ± 8.6 * 31 ± 6.9 † 0.006
BSA, m2 2.0 ± 0.3 2.0 ± 0.3 2.1 ± 0.3 * 0.02
NYHA grade 1.0 ± 0.2 3.0 ± 0.6 * 3.2 ± 0.7 *† < 0.0001
HF hospitalization, ever 0 43 % 91 % < 0.0001
HF diagnosis duration, years 0 1.0 (1.5 – 2.0) 3.0 (1.0-7.5) < 0.0001
Coronary artery disease 0 % 44 % * 46 % * < 0.0001
Hypertension 57 % 93 % * 56 % † < 0.0001
Pacemaker or ICD 0 % 12 % * 66 % *† < 0.0001
Atrial fibrillation 0 % 42 % * 26 % *† < 0.0001
Diabetes mellitus 0 % 47 % * 41 % * < 0.0001
Diuretics 23 % 83 % * 87 % * < 0.0001
Loop diuretics daily dose, mg 0 45 ± 46 * 75 ± 97 *† < 0.0001
BB/ACEi or ARB / AldoRA, % 13 / 42 / 5 67* / 59 / 16 95*† / 82*† / 38*† all < 0.0001
NT-pro-BNP, pg.ml-1 19 (14-65) 1142 (408–2914) * 2481 (1174-4757)*† < 0.0001
GFR §, ml.min.1.73 m-2 71 ± 32 47 ± 21 * 46 ± 21 * 0.01
.7 †††
%
†
1.0 00 1(1(1(1(1.5.5.555 –––– 22222.00.0.0.0))) ) 3.3333 0 0000 (1(11(1( .0000.0-77-7-7.5.5.555))))
44 %%%% * 46 % *
9393939393 %%%%% **** 5656565656 %%%%% †††††
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
20
Values a means±SD or medians (IQR). ANOVA and Tukey post-hoc test or Chi-square test. * p<0.05 vs controls, † p<0.05 vs HFpEF. NTproBNP tested after log-transformation. § GFR: glomerular filtration rate, estimated with MDRD formula. BMI: body mass index, BSA: body surface area, BB: beta-blockers, ACEi: angiotensin-converting enzyme inhibitors, ARB: angiotensin receptor blockers, AldoRA: aldosterone receptor antagonists.
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

21
Table 2. Left atrial and left ventricular function Controls
n = 40
HFpEF
n = 101
HFrEF
n = 97
p
Left atrial function
LA pressure mean, mmHg 8.1 ± 2.8 20 ± 6.1 * 20 ± 8.1 * < 0.0001
minimum, mmHg 5.5 ± 3.7 16 ± 6.1* 18 ± 7.3*† < 0.0001
A§ and V wave, mmHg 12±4 / 12±5 23±8 * / 34±13 * 24±9 */ 30±12 * < 0.0001 / < 0.0001
min-max difference, mmHg 7.9 ± 2.8 19 ± 10 * 13 ± 7.8 *† < 0.0001
LA volume max, ml 45 ± 12 85 ± 28 * 104 ± 38 *† < 0.0001
pre-A§, ml 30 ± 10 55 ± 17 * 77 ± 29 *† < 0.0001
min, ml 16 ± 6.3 54 ± 27 * 71 ± 35 *† < 0.0001
LA volume max/BSA, ml.m-2 23 ± 5 41 ± 12 * 50 ±17 *† < 0.0001
LA EF - total, % 65 ± 8.9 39 ± 17 * 35 ± 15 *† < 0.0001
- active §, % 48 ± 11 30 ± 14 * 22 ± 13 *† < 0.0001
- passive§, % 33 ± 11 26 ± 9.3 * 21 ± 10 *† < 0.0001
LA stiffness, mmHg.ml-1 0.30 ± 0.20 0.79 ± 0.75 * 0.48 ± 0.44 † < 0.0001
LA function index (LAFI) 220 ± 118 60 ± 65 * 30 ± 37 *† < 0.0001
LA wall stress max, kdynes.cm-2 80 ± 31 294 ± 120 * 281 ± 123 * < 0.0001
min, kdynes.cm-2 38 ± 25 137 ± 59 * 167 ± 74 *† < 0.0001
change, kdynes.cm-2 41 ± 18 158 ± 92 * 113 ± 74 *† < 0.0001
††
†
41 ± 12 * 50 ±17 *†
555555 ±±±±± 1717171717 ***** 77777777 77 ±±±±± 29292929 *****† †††
54 ± 22227 7 77 * 717171717 ± 35 *†
4444411111 ± ± ±±± 1212121212 ***** 55550 0 000 ±1±1±1±1±17 777 7 *†*†*†*†*†
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
22
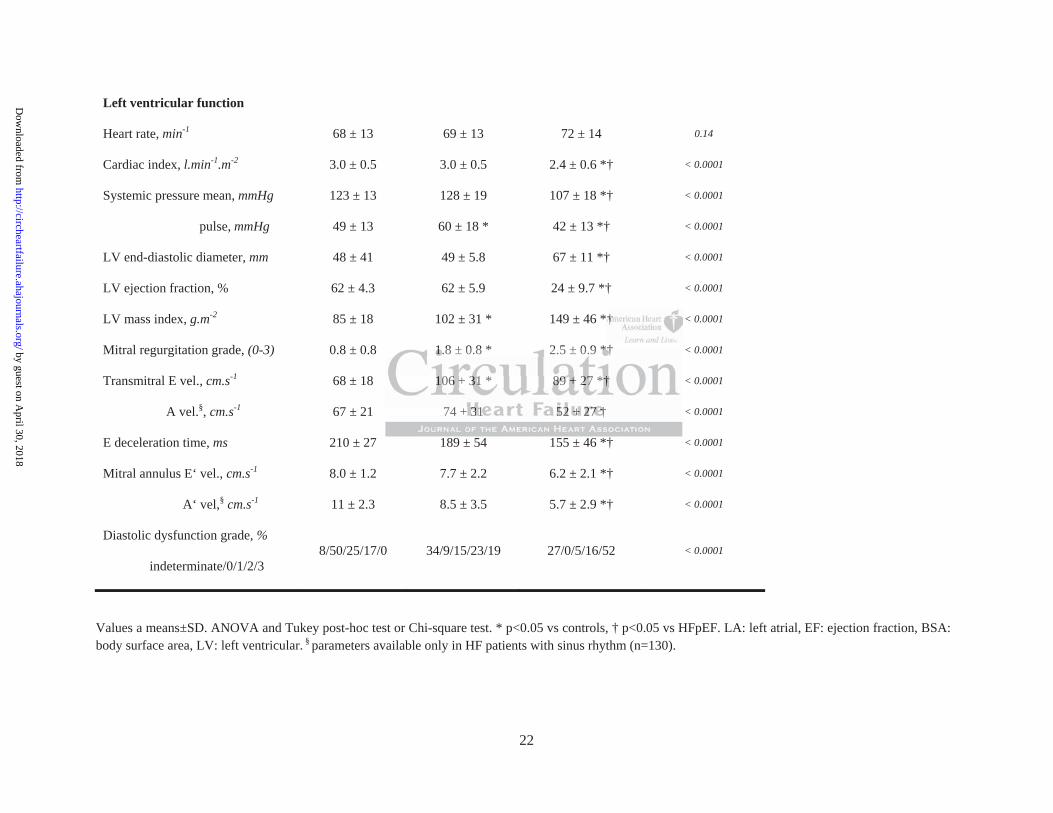
Values a means±SD. ANOVA and Tukey post-hoc test or Chi-square test. * p<0.05 vs controls, † p<0.05 vs HFpEF. LA: left atrial, EF: ejection fraction, BSA: body surface area, LV: left ventricular. § parameters available only in HF patients with sinus rhythm (n=130).
Left ventricular function
Heart rate, min-1 68 ± 13 69 ± 13 72 ± 14 0.14
Cardiac index, l.min-1.m-2 3.0 ± 0.5 3.0 ± 0.5 2.4 ± 0.6 *† < 0.0001
Systemic pressure mean, mmHg 123 ± 13 128 ± 19 107 ± 18 *† < 0.0001
pulse, mmHg 49 ± 13 60 ± 18 * 42 ± 13 *† < 0.0001
LV end-diastolic diameter, mm 48 ± 41 49 ± 5.8 67 ± 11 *† < 0.0001
LV ejection fraction, % 62 ± 4.3 62 ± 5.9 24 ± 9.7 *† < 0.0001
LV mass index, g.m-2 85 ± 18 102 ± 31 * 149 ± 46 *† < 0.0001
Mitral regurgitation grade, (0-3) 0.8 ± 0.8 1.8 ± 0.8 * 2.5 ± 0.9 *† < 0.0001
Transmitral E vel., cm.s-1 68 ± 18 106 ± 31 * 89 ± 27 *† < 0.0001
A vel.§, cm.s-1 67 ± 21 74 ± 31 52 ± 27 † < 0.0001
E deceleration time, ms 210 ± 27 189 ± 54 155 ± 46 *† < 0.0001
Mitral annulus E‘ vel., cm.s-1 8.0 ± 1.2 7.7 ± 2.2 6.2 ± 2.1 *† < 0.0001
A‘ vel,§ cm.s-1 11 ± 2.3 8.5 ± 3.5 5.7 ± 2.9 *† < 0.0001
Diastolic dysfunction grade, %
indeterminate/0/1/2/3 8/50/25/17/0 34/9/15/23/19 27/0/5/16/52 < 0.0001
†††††††
1.8 ± 0.8 * 2.5 ± 0.9 *†11111.8 ± 0.8 * 2.5 ± 0.9 *****†††††
101066 ±±± 3131313131 * 888889 9999 ±±± 27727 *† †
74 ±±± 3333311111 525252 ±±±±± 22227777 7 †††††
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

23
Table 3. Right heart and pulmonary vascular function
Controls
n = 40
HFpEF
n = 101
HFrEF
n = 97
p
ANOVA
RA mean pressure, mmHg 5.3 ± 3.0 13 ± 5.6 * 12 ± 6.6 * < 0.0001
PA pressure systolic, mmHg 28 ± 6.2 56 ± 19 * 51 ± 15 * < 0.0001
diastolic, mmHg 9.0 ± 3.8 21 ± 7.3 * 22 ± 8.1 *† < 0.0001
mean, mmHg 17 ± 4.4 35 ± 11 * 35 ± 10 * < 0.0001
pulse, mmHg 19 ± 4.0 35 ± 14 * 28 ± 10 *† < 0.0001
Transpulmonary gradient, mmHg 8.7 ± 3.1 15 ± 8.0 * 14 ± 6.6 * < 0.0001
Pulm. arterial compliance (PAC), ml.mmHg-1 4.5 ± 1.5 3.1 ± 1.4 * 3.0 ± 1.4 * 0.0004
Pulm. vascular resistance (PVR), w.u. 1.5 ± 0.6 2.6 ± 1.7 * 3.0 ± 1.7 * 0.005
RV end-diastolic area, cm2 15 ± 3.7 21 ± 6 * 22 ± 7 * < 0.0001
RV fractional area change (RV FAC) % 50 ± 7.3 40 ± 10 * 36 ± 13 *† < 0.0001
RA max volume, ml 37 ± 12 72 ± 37 * 83 ± 44 * < 0.0001
Tricuspid regurgitation grade, (0-3) 0.7 ± 0.8 2.2 ± 1.1 * 2.3 ± 1.0 * < 0.0001
Values a means±SD. ANOVA and Tukey post-hoc test. * p<0.05 vs controls, † p<0.05 vs HFpEF. RA: right atrial, RV: right ventricular, w.u.: Wood´s units.
±±±±±±± 11111110 0 0 0 0 0 0 *******
8
4
19 99 99 ±± ±±± 4.4444 0 0000 35 ± 14 * 222228 ± ±±±± 10 *†
8.77.7.7.7 ± 3.1.1.1.1.1 1515151515 ±±±±± 88888 0000.0 * 11114 444 ± ±± 6.6.6.6.6 6 666 ****
4.5 ± 1.5 33333.11111 ±±±±± 1111.44444 * 3333.00000 ± 1.4 *
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
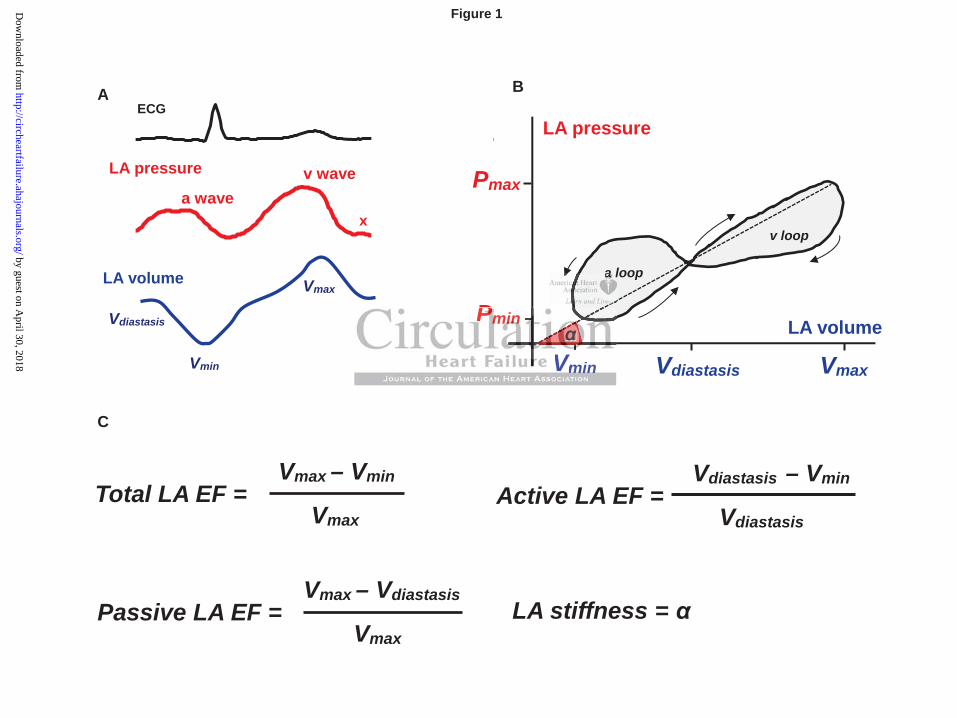
Figure Legends
Figure 1. Characteristics of left atrial (LA) function. A) Representative ECG, LA pressure
and LA volume waveforms. B) Schematic example of LA pressure-volume loop with smaller a-
loop and larger v-loop. LA stiffness is represented by slope of dashed line ( ) that connects
maximal and minimal pressure-volume points. C) Equations used for LA functional
characterization.
Figure 2. Left atrial (LA) remodeling and dysfunction in controls vs HFpEF and HFrEF.
A) increased maximal, diastasis and minimal LA volumes and B) reduced total, active and
passive LA ejection fraction in patients with HFpEF and HFrEF compared to controls. C) Slope
of P-V relationships in controls and in patients with HFpEF or HFrEF. *p< 0.05 vs controls, #p<
0.05 vs HFrEF. Thus, HFrEF patients display greater LA chamber dilation and lower
contractility, while HFpEF patients display stiffer LA chambers.
Figure 3. LA performance in HF and controls and the influence of mitral regurgitation on
the left atrium. A) Relations between LA volume prior the onset of LA contraction (LA pre-A
volume) and LA active stroke volume in controls and HF patients with sinus rhythm (n=130). B)
The impact of mitral regurgitation grade on peak LA pressure (LA v-wave, left) and min-max
LA wall stress change (right) in controls, HFrEF and HFpEF. Lines represent results of linear
regression with 95% confidence intervals and correlation coefficients. Thus, LA performance is
reduced due to impairment of the Frank-Starling mechanism in both HF groups, while the
presence of mitral regurgitation is associated with higher wall stress variations and greater v-
wave height in HFpEF.
nd B) reduceeeeed d ddddd
F compmpmpmpmpmpmparararararararededededededed tttttttooooooo coc
5
T a
H
iiiiinn nnn controrororoolslslslsls aaaaandndndndnd iiin n nn n papapapapatitititit enenenene tsssss wwithhh HFHFHFFHFpEpEpEpEpEFFFFF orororo HHHHHFrFrEFEFEFEFEF.. ... *ppppp<<<<< 0.0.0.0.0.05000r
Thuhuhuhuuss,ss,s, HHHHHFrFrFrFrFrEFEFEFEFEF pppppattieieieieientntntntntsss dididididispspspspsplalalall y yyyy grgrgrgrgreaeaeaeaeateteteteter rr LALALALALA cccchahahahahambmmbmm ererererer dddddilililii a
HHFpFpEFEF pppppatatatieientntntsss didispspsppplalay y y y stststififfeferrr LALA ccchahambmbererersss.
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
25
Figure 4. The impact of HF severity on the left atrium. The impact of HF severity (NYHA
functional class) on LA characteristics assessed by ANOVA and Tukey post-hoc test, *p<0.05 vs
controls, §p< 0.05 vs NYHA II, #p<0.05 vs NYHA III. LAVI max: body surface area-indexed
maximal LA volume. Thus, LA dysfunction is related to HF severity.
Figure 5. The left atrium and pulmonary vascular properties/right heart function. A)
Relation of global LA function (total LA EF, %) to pulmonary vascular resistance (PVR) and
pulmonary artery compliance (PAC) and right ventricular systolic function (RV fractional area
change, RV FAC %) in HFrEF (red), HFpEF (blue) controls (black). Lines represent results of
linear regression with 95% confidence intervals, r: Pearson´s correlation coefficient. Thus, LA
dysfunction is associated with greater pulmonary vascular disease and RV dysfunction in HF.
Figure 6. The impact of LA characteristics and atrial fibrillation on survival in HFpEF and
HFrEF. Univariate Cox model was used to determine the hazard ratio for death associated with
being in a group above median of a parameter (or yes/no for AF). Continuous parameters were z-
standardized within HF subgroups.*p<0.05. Thus, LA dysfunction is associated with mortality in
HFpEF but not HFrEF.
orororororororrererererererelalalalalalalatitititititiiononononononon cccccccoeoeoeoeoeoeoeffffffffffffff
iated with greater pulmonary vascular disease and RV dysfu
a a
h
iateteteteted dd d d wiwiwiwiwithtttt gggggreater pulmonary vvvvvasaaasascular diseassssseeeee and RV dysfu
acttttt ooooof fff LALALALALA ccccchahahahaharararararactctcterereree isisisisstttitt cscscscscs aaaaandndndndnd atatatatatriririririalalalalal fffffibibibibibriririririllllllllllatatatatatioioioioi n nnnn ononononon sususuurvrvrvrvr ivivivvivaaa
CCoxoxox mmmododelel wwwasasas uuusesesedd tototo ddetetetererermiminenene ththeee hahazazazardrd rrratatatioio ffororor ddeaeaeathth
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
LA volume
LA pressure
A
a wavev wave
x
LA stiffness =
Active LA EF =Vdiastasis – Vmin
Vdiastasis
Figure 1
Total LA EF =Vmax – Vmin
Vmax
Passive LA EF =Vmax – Vdiastasis
Vmax
C
Vdiastasis
Vmin
Vmax
LA pressure
LA volume
Vmin Vdiastasis Vmax
Pmax
Pmin
B
a loop
v loop
ECG
a a a a l
P
VmiminnVV
PPPPPmimimimiinnnnnP
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Figure 2
C B A
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

A B
Figure 3
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Figure 4
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
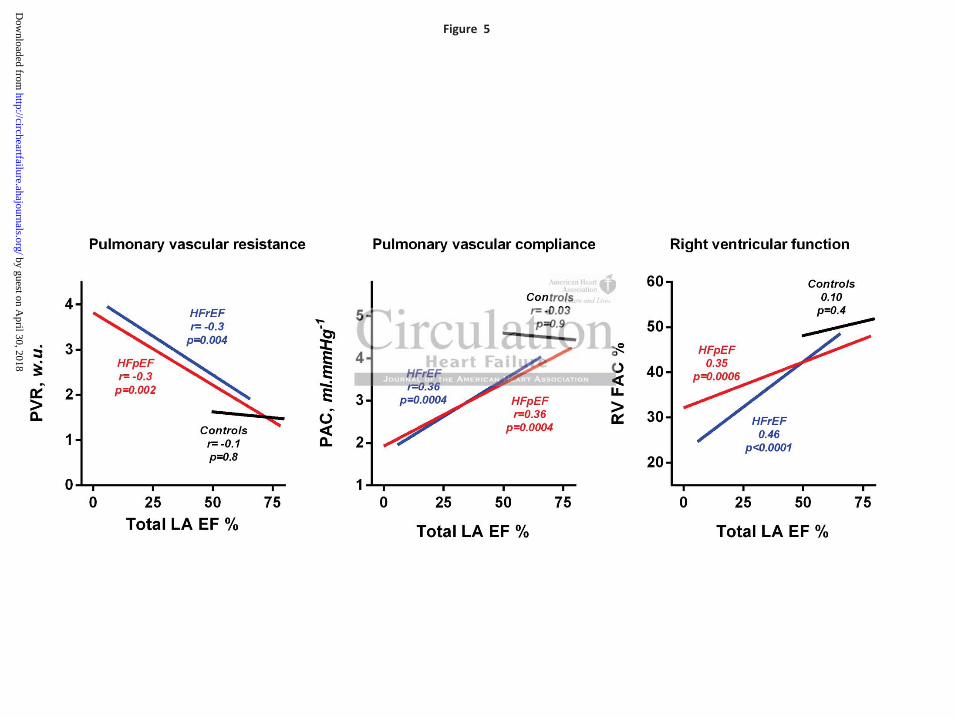
Figure 5
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
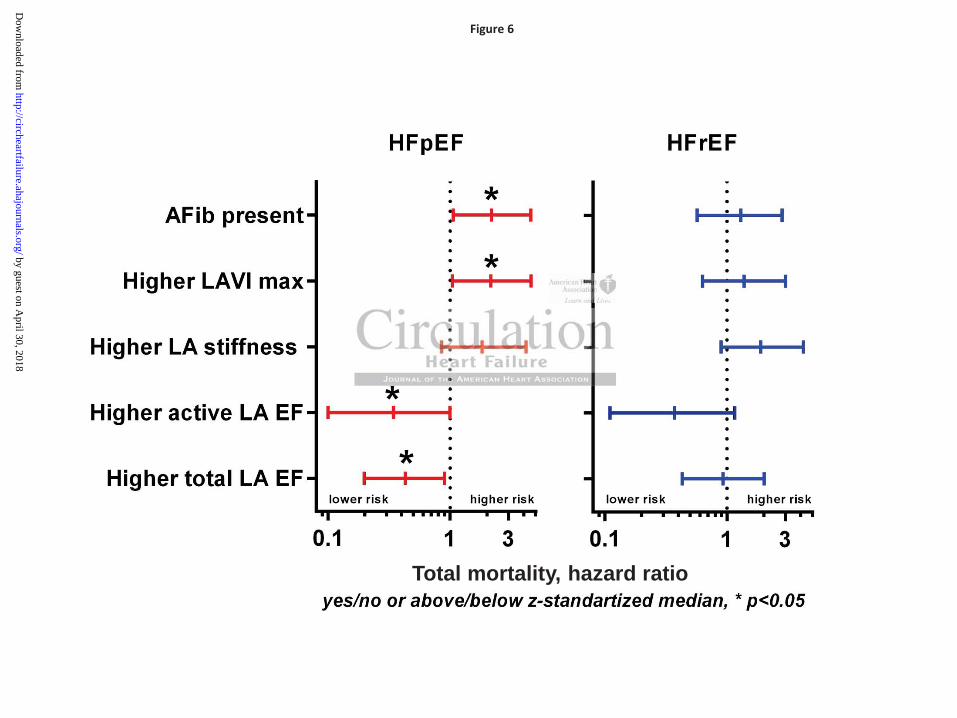
Figure 6
Total mortality, hazard ratio
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
BorlaugVojtech Melenovsky, Seok-Jae Hwang, Margaret M. Redfield, Rosita Zakeri, Grace Lin and Barry A.
Ejection FractionLeft Atrial Remodeling and Function in Advanced Heart Failure With Preserved or Reduced
Print ISSN: 1941-3289. Online ISSN: 1941-3297 Copyright © 2015 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation: Heart Failure published online January 15, 2015;Circ Heart Fail.
http://circheartfailure.ahajournals.org/content/early/2015/01/15/CIRCHEARTFAILURE.114.001667World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circheartfailure.ahajournals.org/content/suppl/2015/03/12/CIRCHEARTFAILURE.114.001667.DC2 http://circheartfailure.ahajournals.org/content/suppl/2015/01/15/CIRCHEARTFAILURE.114.001667.DC1
Data Supplement (unedited) at:
http://circheartfailure.ahajournals.org//subscriptions/
is online at: Circulation: Heart Failure Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information about thisEditorial Office. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation: Heart Failure Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on April 30, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
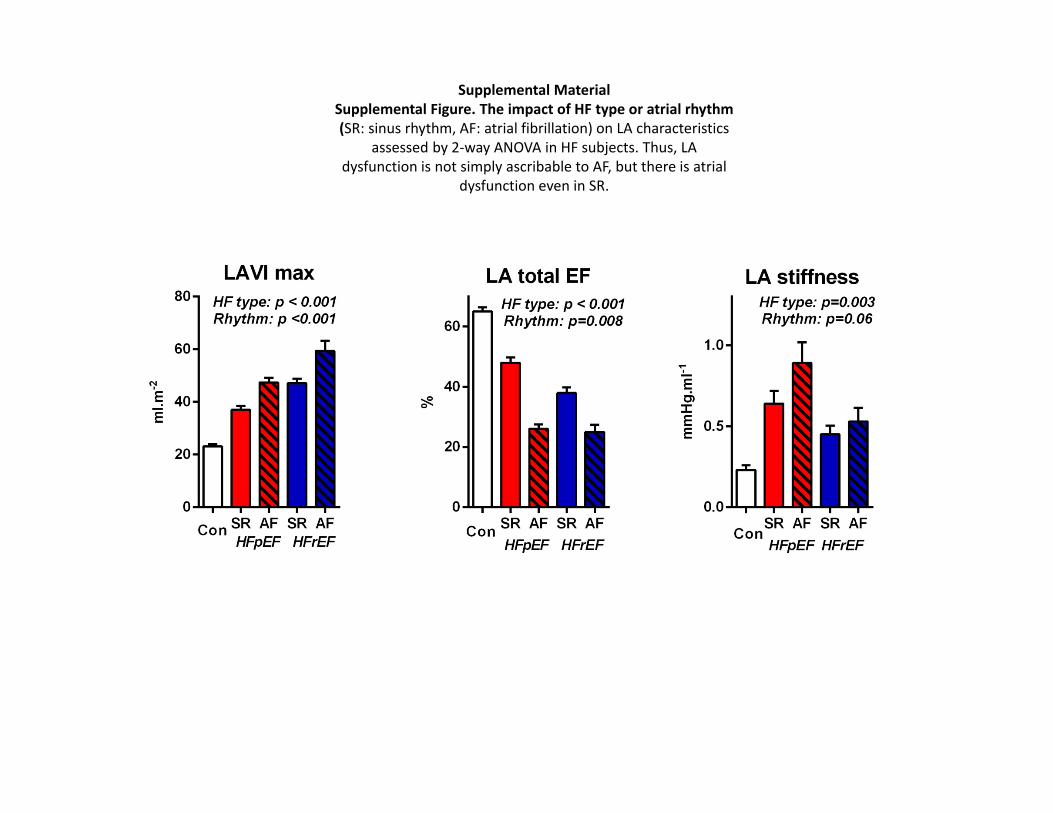
Supplemental MaterialSupplemental Figure. The impact of HF type or atrial rhythm (SR: sinus rhythm, AF: atrial fibrillation) on LA characteristics
assessed by 2‐way ANOVA in HF subjects. Thus, LA dysfunction is not simply ascribable to AF, but there is atrial
dysfunction even in SR.
Original Articles
10 Circulation: Heart Failure
구혈률저하 심부전의 좌심방은 크기가 증가하고
기능이 저하되나, 구혈률보존 심부전에서는
좌심방 경직도가 증가하여 심방세동이 증가한다
최 진 오 교수 · 삼성서울병원 순환기내과
초록
배경
대부분의 심부전 환자에서 좌심방의 구조와 기능은 변화한다.
구혈률보존 심부전(heart failure with preserved ejection
fraction)과 구혈률저하 심부전(heart failure with reduced
ejection fraction) 간에 좌심방의 변화 양상에는 근본적인
차이가 있을 수 있다.
방법 및 결과
총 198명의 심부전 환자(구혈률보존 심부전 환자 51%,
뉴욕심장학회 기능 분류 3.1±0.7)와 40명의 심부전이
없는(heart failure-free) 대조군 환자에게 심도자 및
심초음파 검사를 시행하고, 그 경과를 추적하였다. 대조군에
비하여 심부전 환자들은 좌심방이 크고, 기능이 저하되어
있었다. 심부전 환자군 간의 비교를 보면, 평균 좌심방압
(20 vs. 20mmHg; P=0.9)은 차이가 없었으나, 구혈률저하
심부전군의 좌심방은 크기가 더 증가되어 있었다(좌심방
용적지수 50 vs. 41mL/m2; P<0.001). 반면, 구혈률보존
심부전군은 좌심방 최대 압력이 더 높고 최소 압력은 더 낮아,
더 높은 좌심방 경직도를 보였고(0.79 vs. 0.48mmHg/mL;
P<0.001), 좌심방 박동성(19 vs. 13mmHg; P<0.001)과
벽장력의 변동성(wall stress variations)이 더 증가되어
있었다. 구혈률보존 심부전군은 좌심방 용적이 더 작고,
기능 은 더 좋았으며, 승모판 역류도 덜 심하였지만,
심방세동은 더 많았다(42 vs. 26%; P=0.02). 양 군 모두
좌심방의 기능부전은 폐혈관 저항의 증가 및 우심실기능
저하와 연관되어 있었다. 추적 관찰 기간(중앙값 350일)
중에 구혈률보존 심부전 환자 31명과 구혈률저하 심부전
환자 28명이 사망하였다. 좌심방기능(총 좌심방 구혈률)은
구혈 률보존 심부 전에 서는 낮은 사 망률과 연관되어
있었으나(HR 0.43; 95% CI, 0.2-0.9; P<0.05), 구혈률저하
심부전에서는 연관이 없었다.
결론
구혈률저하 심부전에서의 좌심방 리모델링은 편심성
(eccentric) 확장이 주된 양상인 반면, 구혈률보존 심부전에서
는 좌심방 경직도가 증가하는 것이 특징으로, 이는 심방세동
의 발생에 영향을 줄 수 있다. 좌심방기능은 양 군 모두에서 폐
혈관질환 및 우심부전과 관련되었으나, 구혈률보존 심부전이
보다 더 밀접하게 연관되어 있었으며, 이는 구혈률보존 심부전
환자들에서 좌심방기능을 호전시키기 위한 노력에 대한 의학
적 근거가 될 것이다.