lessons learned fromjiki clinical trialregist2.virology-education.com/2016/10interest/08... ·...
TRANSCRIPT

Lessons learned fromJIKI ClinicalTrial
(Inserm C1463 - EU H2020 666092)
Dr Daouda Sissoko on behalf of JIKI group
1
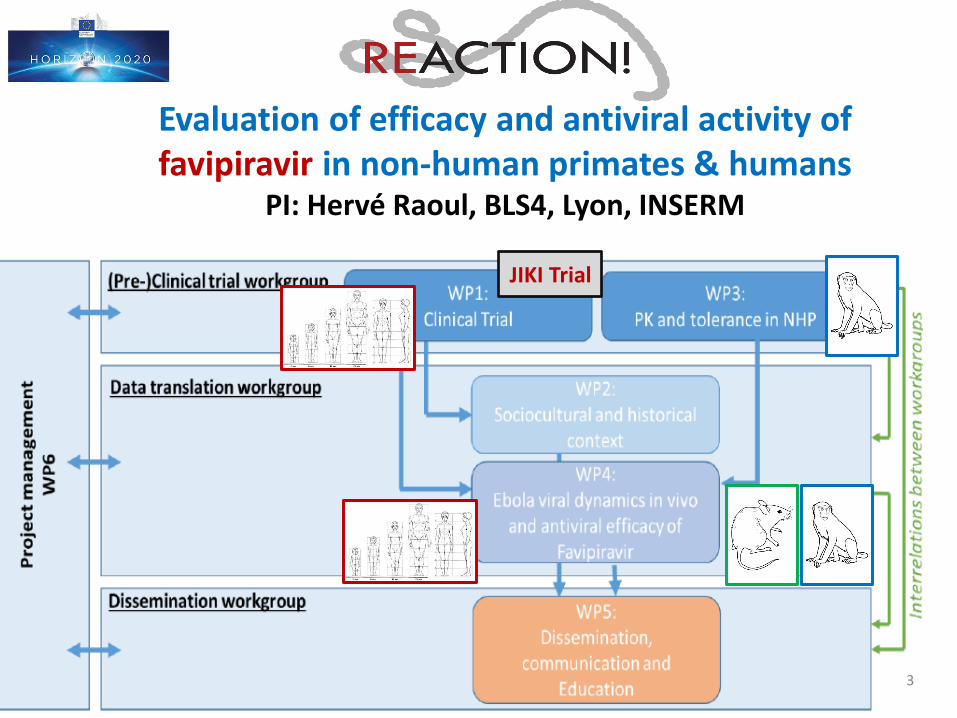
Evaluation of efficacy and antiviral activity of favipiravir in non-human primates & humans
PI: Hervé Raoul, BLS4, Lyon, INSERM
JIKI Trial
3

The Challenges of Design in Guinea, September 2014
1. Randomization, while providing the best level of evidence, not always possible
• RCTs were problematic for the community
– High number of patients from same village/ family arriving simultaneously
– Patients terrified by the expanding epidemic and high mortality rate
– Rumors and distrust in Ebola Treatment Units: RCT might lead patient to refuse to seek care
2. There was an urgent need for early and rapid triage of treatments
• Risk/benefit ratio
– Ebola mortality in Guinea was 60% in adults
– Favipiravir had an excellent reported safety profile
Historically controlled, single-arm, proof-of-concept trial – triangular test
– pre-trial mortality recorded in same ETC4

5
Mentré et al., Dose regimen of favipiravir for Ebola virus disease, Lancet Infect Dis (2015)Frange et al., Favipiravir for Children with Ebola, Lancet (2015)
Dose of favipiravir for EVDSimulation studies: 50% higher than for influenza

6
0
20
40
60
80
100
120
140
Oct Nov Dec Fev MarSept Jan Apr May
TOTAL JIKI
NZEREKORE/ALIMA
GUECKEDOU/MSF
CTS/SSA
MACENTA/Red cross
ETHICS
Discussions
with NGOs
PROTOCOL
Negociation with pharm. firm
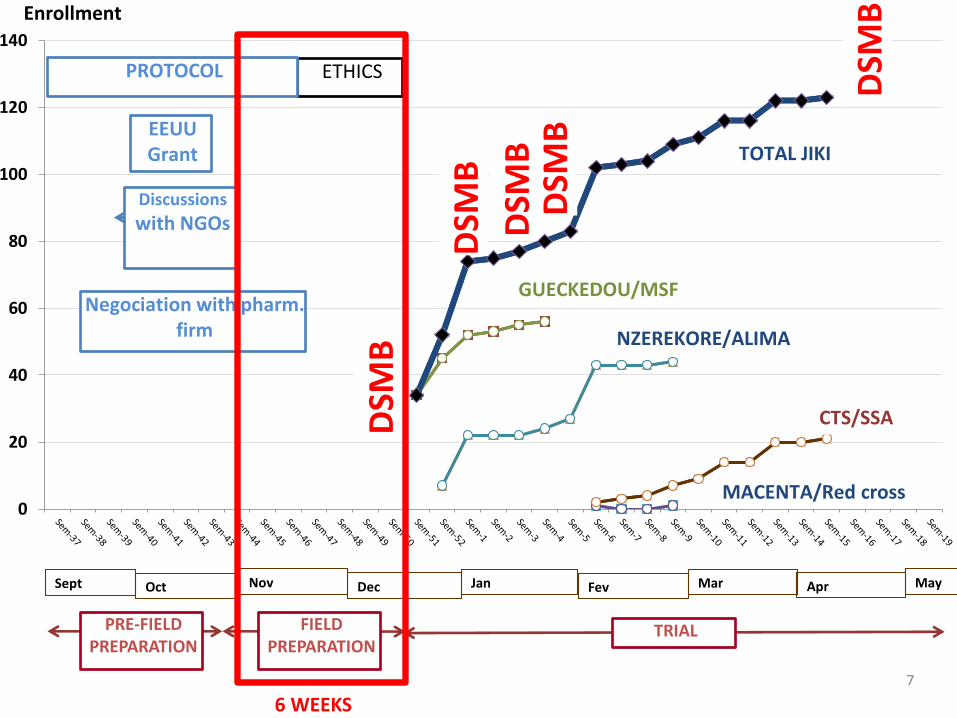
Enrollment
EEUUGrant
DSM
B
DSM
B
DSM
B
DSM
B
TRIAL
DSM
B
FIELD PREPARATION
PRE-FIELD PREPARATION
7 WEEKS
7
0
20
40
60
80
100
120
140
Oct Nov Dec Fev MarSept Jan Apr May
TOTAL JIKI
NZEREKORE/ALIMA
GUECKEDOU/MSF
CTS/SSA
MACENTA/Red cross
ETHICS
Discussions
with NGOs
PROTOCOL
Negociation with pharm. firm
Enrollment
EEUUGrant
DSM
B
DSM
B
DSM
B
DSM
B
TRIAL
DSM
B
FIELD PREPARATION
PRE-FIELD PREPARATION
6 WEEKS

8
0
20
40
60
80
100
120
140
Oct Nov Dec Fev MarSept Jan Apr May
TOTAL JIKI
NZEREKORE/ALIMA
GUECKEDOU/MSF
CTS/SSA
MACENTA/Red cross
ETHICS
Discussions
with NGOs
PROTOCOL
Negociation with pharm. firm
Enrollment
EEUUGrant
DSM
B
DSM
B
DSM
B
DSM
B
TRIAL
DSM
B
FIELD PREPARATION
PRE-FIELD PREPARATION
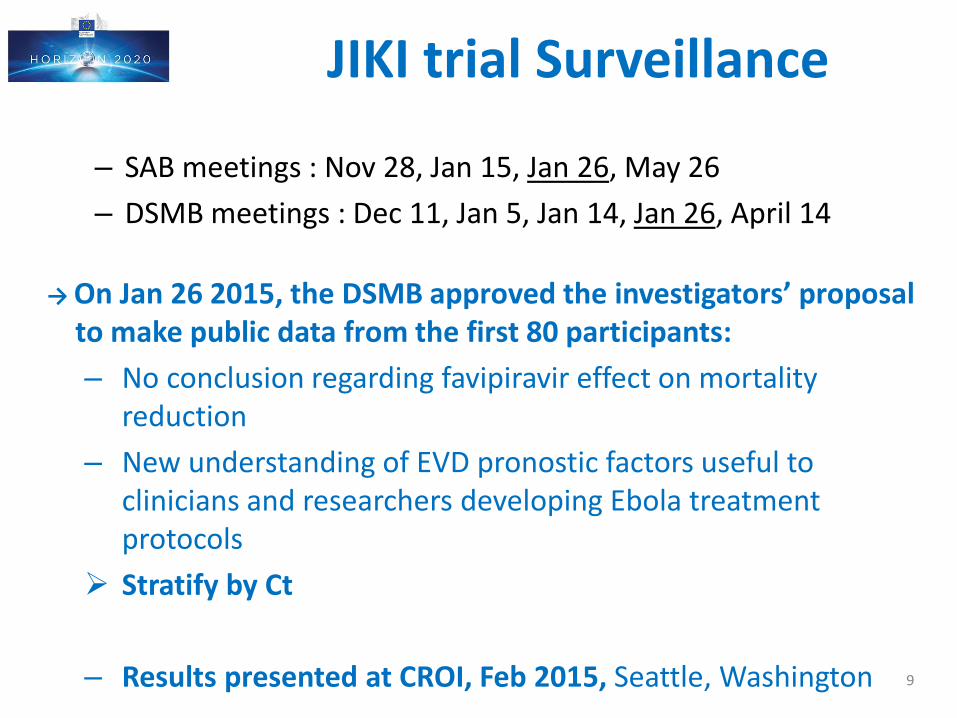
JIKI trial Surveillance
9
– SAB meetings : Nov 28, Jan 15, Jan 26, May 26
– DSMB meetings : Dec 11, Jan 5, Jan 14, Jan 26, April 14
→ On Jan 26 2015, the DSMB approved the investigators’ proposalto make public data from the first 80 participants:
– No conclusion regarding favipiravir effect on mortalityreduction
– New understanding of EVD pronostic factors useful to clinicians and researchers developing Ebola treatmentprotocols
Stratify by Ct
– Results presented at CROI, Feb 2015, Seattle, Washington
10
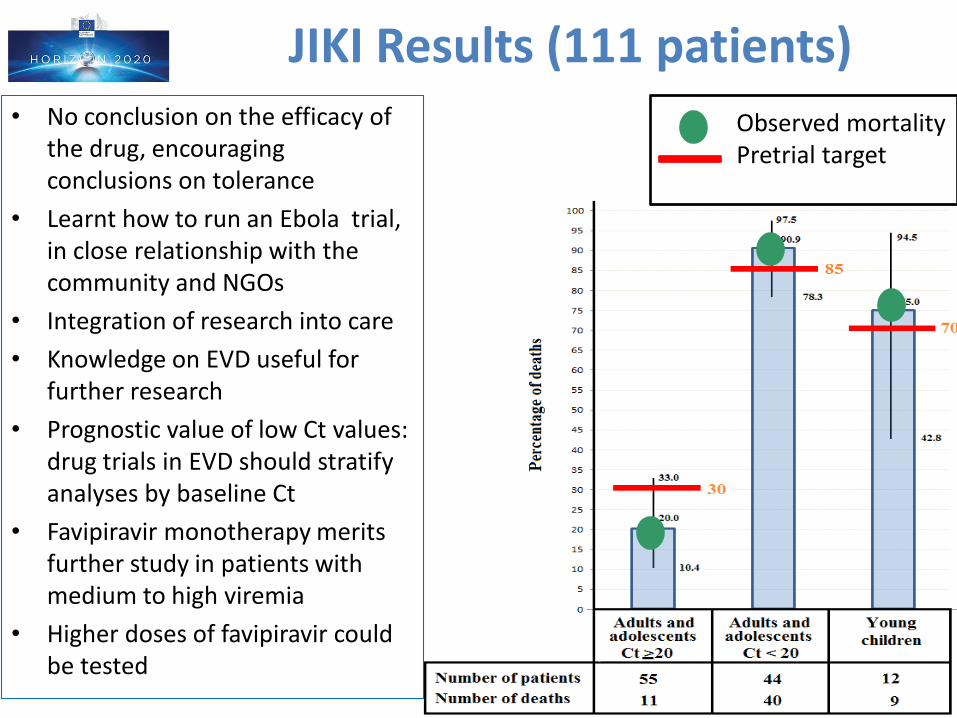
JIKI Results (111 patients)• No conclusion on the efficacy of
the drug, encouraging conclusions on tolerance
• Learnt how to run an Ebola trial, in close relationship with the community and NGOs
• Integration of research into care
• Knowledge on EVD useful for further research
• Prognostic value of low Ct values: drug trials in EVD should stratify analyses by baseline Ct
• Favipiravir monotherapy merits further study in patients with medium to high viremia
• Higher doses of favipiravir could be tested
Observed mortalityPretrial target
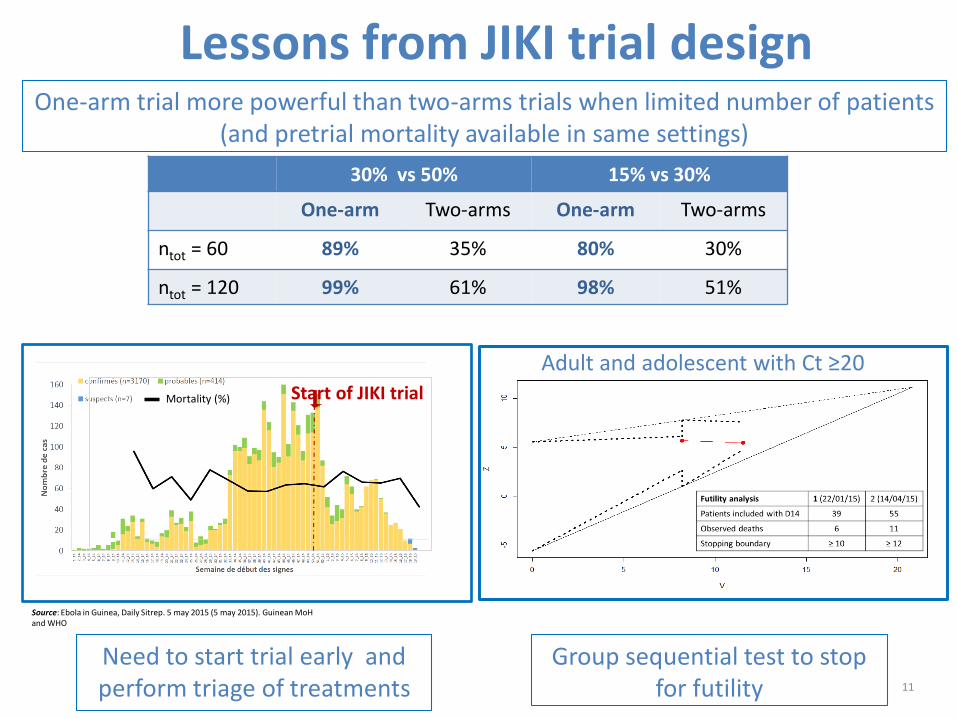
Lessons from JIKI trial design
Source: Ebola in Guinea, Daily Sitrep. 5 may 2015 (5 may 2015). Guinean MoHand WHO
Start of JIKI trialMortality (%)
11
30% vs 50% 15% vs 30%
One-arm Two-arms One-arm Two-arms
ntot = 60 89% 35% 80% 30%
ntot = 120 99% 61% 98% 51%
One-arm trial more powerful than two-arms trials when limited number of patients (and pretrial mortality available in same settings)
Need to start trial early and perform triage of treatments
Group sequential test to stop for futility
Adult and adolescent with Ct ≥20
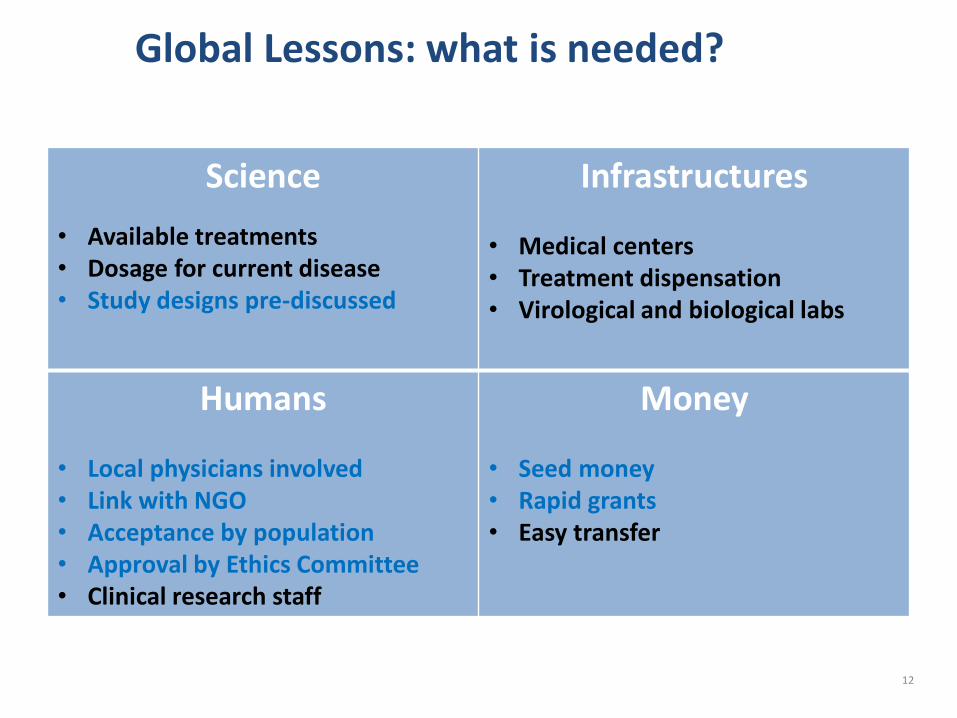
Global Lessons: what is needed?
12
Science
• Available treatments• Dosage for current disease• Study designs pre-discussed
Infrastructures
• Medical centers• Treatment dispensation• Virological and biological labs
Humans
• Local physicians involved• Link with NGO• Acceptance by population• Approval by Ethics Committee• Clinical research staff
Money
• Seed money • Rapid grants• Easy transfer

Conclusion: Challenges & Recommendations
• Three challenges1. ANTICIPATION: be ready on time and not at the end of the
outbreak
2. ANTICIPATION: collect necessary medical knowledge on diseases and drugs to define adequate intervention(s)
3. Make intervention(s) acceptable locally with the help of local opinion leaders, NGOs and anthropologists
• Three recommendations (outside outbreaks)
1. Perform in vitro, animal and phase I research for emerging infectious diseases have potential treatments and dosage available
2. Build strong links with researchers, clinicians and NGOs in Southern countries (training, academic exchanges,…)
3. Have designs and teams ready to conduct trials 13

Acknowledgements
14
Special thanks to:
• All patients who accepted to participate in the study
• Scientific Advisory Board: L Abel, G Carson, G Davies, A Diallo, P Frange, B Godard, A Kelly, F Le Marcis, N Morgensztejn,
A Ndjeyi Mbiguino, VK Nguyen, C Semaille, AM Taburet, JM Treluyer, Y Yazdanpanah
• Data Safety Monitoring Board: D Baush, B Bazin, E Bottieau, A Faye, R Garraffo, R Porcher, P Redfield
• Sponsor (Inserm): T Damerval, JF Delfraissy, Y Levy, C Levy-Marchal,
• Ethics Committees of Inserm (CEEI/IRB), MSF (MSF ERB), and Republic of Guinea (CNERS)
• Toyama Chemical Co., Ltd, for the donation of favipiravir: H Kitaguchi, K Yamada
The JIKI study group is constituted as follows:
– Guinea Ebola Task Force: S Keita
– Centre de Formation et de Recherche en Santé Rurale de Maferinyah: AH Beavogui
– MSF: I Arnould, A Antierens, N Bangoura, E Berbain, D Camara, FS Camara, S Carazo, AM Camara, L Delamou, B
Draguez, E Folkeson, MC Lamah, A Lefevre, T Leno, M Loua, K Malme, E Manfrin, A Maomou, S Ombelet, P Piguet,
M Poncin, OO Sakovogui, AY Sidiboun, A Tounkara, M Van Herp, D van Hoeydonck, I Verreckt
– ALIMA: B Abdoul, A Augier, G Baret, TS Barry, S Berrette, A Bongono, C Camara, M Conde, I Defourny, JM Dindart,
R Doumbouya, G Leduc, M Loua, R Lolamou FR Koundouno, S Harouna, V Massala, A Moumouni, P Mumbere, JP
Olele, R Palich, F Petitjean, O Peyrouset, C Provost, S Shepherd, C Sekou, A Soumah
– Croix Rouge Française: G Colin, D Dougo, P Gorovogui, E Olivier, Y Ruaux, B Simon, T Tran Minh, FT Simpogui
– Inserm: X Anglaret, M Cervantes-Gonzalez, S Eholie, X de Lamballerie, C Laouenan, D Malvy, F Mentre, R Moh, B
Murgue, C Nchot, L Nguessan, B Siloue, D Sissoko
– P4 Lyon Mérieux: S Baize, H Raoul
– EMLab: J Akoi Bore, M Carroll, S Diederich, S Duraffour, J Hinzmann, RF Koundouno, A Kraus, B Liedigk, P Maes, D
Ngabo, M Rudolf, R Thorn
– BFAST: Y Deccache, C Dumont, JF Durant JL Gala, L Irenge, B Smiths, N Toufic, S Van CauwenbergheSSA: H
Dampierre, V Foissaud, F Janvier, C Rapp, H Savini
– ADERA: O Fouassier, J Rivenc
– Solthis: A Abadie, R Benhamou, E Dortenzio, PE Martineau, L Pizarro