life-threatening weakness: strengthen your diagnostic skills
TRANSCRIPT
Life-Threatening Weakness: Strengthen Your Diagnostic Skills
Andrew D. Perron, MD, FACEPResidency Program Director & Professor
Dept. of Emergency MedicineMaine Medical Center
Portland, ME
Life-Threatening Weakness
An exhaustive talk on “weakness” would take a week (pun intended) and bore you to tears…this ain’t that. None of these are “occult UTI” or “general debilitation”
These are 4 “weakness” emergencies that you won’t see every day…but you need to recognize and treat when they come along.
Challenge yourself to establish a differential as we work through the case.
Case 1: “I’m too weak to walk”
HPI: 26-year-old female brought to the ED for “weakness”. She had been well during the day, but had felt “like I was getting sick” in the afternoon. She ate dinner at 6pm, and had gone to bed early. She awoke having to urinate at midnight, but was “unable to physically get out of the bed”. She denies headache, trauma, or new medications. No street drugs. Recent diarrheal illnesses, now resolved
PMHX: Unremarkable.

Case 1: “I’m too weak to walk”PE: Gen: Laying in bed, in no acute distress. VS: 36.7 118/72 78 14 HEENT: NC/AT PERRL EOMI Nl phonation Neck: Supple Chest: CTA Neuro: Awake and alert, with normal mental status.
Speech is clear and fluent, but quiet. CNs intact, but notable for global mild weakness with examination. Muscle strength 4- out of 5 x 4 extremities. Normal sensory examination. DTRs absent throughout.

Case 1: Key Features
Weakness… “unable to physically get out of bed”.
Recent illness. Global weakness on exam (4- out of 5) Normal sensory exam. DTR’s absent
What & Where is the lesion?
Global neurologic process Unlikely brain (symmetric & bilateral),
brainstem. Motor involved, Sensory sparing
Not global spinal cord (? Anterior cord) DTRs absent
Peripheral nerve or motor end-plate DDx: LGBS, Botulism, Myesthenia, Tick paralysis.

Imaging & studies ?
CT? MRI? Blood? LP?
Diagnosis: Landry-Guillain-Barre-Strohl Syndrome
1859 “Landry’s Ascending Paralysis”1916 G, B & S Publish disease description…it gets ignored.1924 Disease referenced in a lecture by Barre…Strohl’s name dropped from
both lecture and reference.
Diagnosis: Guillain-Barre syndrome
Acute ascending progressive demyelinating poly-neuropathy due to autoimmune response to myelin sheath

Diagnosis: Guillain-Barre syndrome: History
Ascending, progressive SYMMETRICAL weakness. If weakness is asymmetric, consider another dx. Progresses over hours to days
Usually starts in legs (but not always) Sometimes presents with pain in muscle groups Can involve CN’s 2/3 have preceding viral illness 2-4 weeks prior 40% Camphylobacter jejuni + Pregnancy & surgery also known triggers
Diagnosis: Guillain-Barre syndrome: Physical Examination
Absent DTRs nearly universal. If there is weakness with intact DTRs, STRONGLY consider another dx.
Labile VS due to dysautonomia. Tachy / Brady
Respiratory involvement (due to musculature) 30-35% need mechanical ventilation at some point
in the disease course.

Diagnosis: Guillain-Barre syndrome: Respiratory Issues
Respiratory involvement 30-35% will need mechanical ventilation Negative Inspiratory Flow (NIF)
> 30 cm/H2O is good, less than 20cm/H2O is bad Forced Vital Capacity (FVC)
< 15 ml/kg is bad Max Expiratory Pressure (MEP)
< 40 cm / H2O is bad
Guillain-Barre Syndrome: Diagnosis
Labs not really helpful (? MRI – stand-by) Diagnosis made on clinical grounds.
Classic finding is elevated CSF protein (> 400 mg/L) with no elevation in CSF cell counts Caveats: 1. Protein remains normal in 10% 2. Rise in CSF protein may not be seen for 1-
2 weeks after disease onset.

Guillain-Barre Syndrome: Diagnosis MRI in GBS
There are some case reports and case series indicating that there may be a role for MRI in the diagnostic process for GBS. Reports show that GBS patients demonstrate marked gadolinium
enhancement of the nerve roots and conus on MR imaging
Stand-byFor more data !

Guillain-Barre Syndrome: Treatment
Usual treatment concerns…resp failure & pulmonary toilet. In modern era, however, pulmonary issues don’t usually kill the patient, dysautonomia does (mortality 5-10%).

Guillain-Barre Syndrome: ED Care
Treatment rarely required for tachycardia. Usual treatment of bradycardia. Use short-acting agentsfor treatment of all dysautonomias, as they are extremely labile. May require temporary pacing for heart-block.
Definitive treatment is plasma exchange or IVIG. Both have been proven to shorten recovery time by approx 50%. Cost, difficulty, and efficacy of 2 treatments are comparable.

Guillain-Barre Syndrome: Prognosis
Full recovery expected in 50-95%(depending on series cited) Symptoms usually peak at 2 weeks, plateau for 4
weeks, then resolve in most. Usually resolved completely in 6-12 months 7-15% with persistent neurological dysfunction Mortality < 5% in “expert hands”

LGBSS: Key Points Acute, ascending, progressive neuropathy. If reflexes are intact or weakness is asymmetric,
search for another diagnosis. No ED lab or imaging test will confirm/refute the
diagnosis. Dysautonomia, not respiratory insult, most likely to
result in M&M.

Case 2: Grandma
This is also a real case
She is my partner’s grandma…No names have been changed to protect the innocent (everybody calls her “grandma”)
Tell me you can’t see yourself put in this EXACT situation
Yup, that is really grandma

Case 2: Grandma
90 y/o female, Friday 5pmPMHx: HTNSoc hx: Primary provider for husband, mostly Italian
speakingGeneralized weakness ~2-4wksNew onset slurred speech ~wkNot eating much, starts but can’t finish ~2-4wksNeck and face is “tired”Blurry visionShorter than usual phone conversation“You’re the doctor…what should she do?”
“Call your doctor” “Its Friday 5pm …do something!”
“Go to the ED” CT CT neck Carotids ECG Enzymes UA Which study came back
Positive?
None of them !!
All Negative
Next Test? MRI Neg
“Now you are past my pay grade” Consultation?
Ophthalmology? Neurology?

Ophthamologist
Dx Strabismus (when you only have a hammer…) Referred to Strabismus specialist Recommended use of a patch Vision ? improved with patch
Still speech issues Still very tired Not eating Now Very depressed

“What are you going to do??”
“She’s Freakin’ 90 years old” “Tell her to go back and see her primary
care doctor” Next steps?? Consultation
Neurologist Test done….Diagnosis made 3 days later Symptoms completely resolved with treatment
Key Points
Elderly Female Generalized weakness ~2-4wks New onset slurred speech ~ 1 wk Not eating, starts but can’t finish ~2-4 wks Neck and face is “tired” Blurry vision

“Something Gravis”
“Umm yah…that makes total sense!!” “Probably not the first time I have missed
it”

Myasthenia Gravis
Most common disorder of neuromuscular transmission Best characterized and understood as an
autoimmune disorder Relatively rare: 100-200 / million pop. Occurs at any age…but bimodal peaks
3rd decade (female predominance) 8th decade (male predominance)

What are the hallmarks of MG?
Focal extremity weakness Fluctuating / variable
Unilateral / Bilateral Ptosis Diplopia Dysarthria
Painless Reflexes preserved Only affects striated muscle

Characteristic Sequence
Eyes → Extra-ocular muscles (ptosis / diplopia)
Facial Muscles (expression / speech) Pharyngheal (mastication,
swallowing) Neck / Proximal muscles (this is rare)

Myesthenia Pearl
Myesthenia always gets worse with repetitive muscle use and gets better after rest. Corollary: The symptoms are usually the
least in the morning, and progress throughout the day.
Clinical Features
Cardinal Feature = Fluctuating skeletal muscle weakness true muscle fatigue
Worsening contractile force of the muscle Not sensation of tiredness Usually specific muscle fatigue, not general
weakness, but different muscle groups at different times
Symptom free periods diminish Fluctuation of severity continues
Classic symptoms
50% with ocular symptoms Ptosis and/or diplopia50% w/ ocular sx develop generalized
symptoms in 2yrs 15% bulbar symptoms
Dysarthia, dysphagia, fatigable chewing!! 5% with proximal limb weakness <5% neck, respiratory muscle weakness

Ocular muscles
Variable eyelid weakness throughout day May switch from eye to eye May start bilaterally then improve in one
eye May start unilateral, then become bilateral
So severe it can occlude vision Extra-ocular muscles often involved
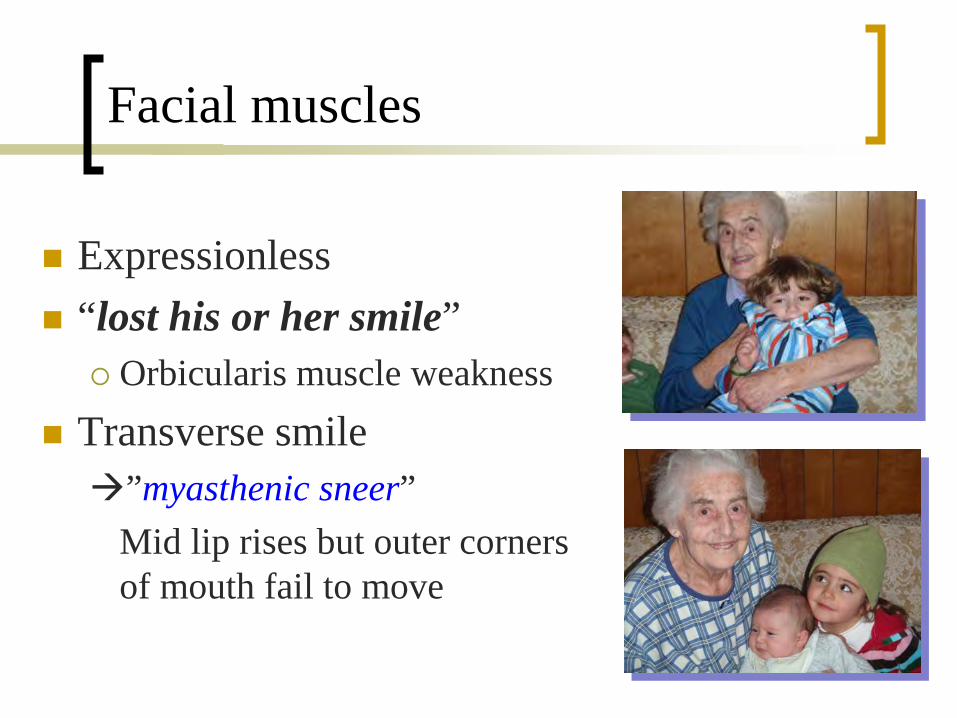
Facial muscles
Expressionless “lost his or her smile”
Orbicularis muscle weakness Transverse smile”myasthenic sneer”
Mid lip rises but outer corners of mouth fail to move

Testing: What is the peak sign?
Orbicularis oculi weakness may be indicated by a positive peek sign after gentle eyelid closure. After complete initial apposition of the lid margins, they quickly (within 30 seconds) start to separate and the sclera starts to show (ie, a positive peek sign).
The presence of a peek sign increases the likelihood of myasthenia gravis (a LOT) but absence of the peek sign does not rule it out.

Ice pack test: “the poor-man’s edrophonium”
Pt’s w/ ptosis not helpful with extra-ocular muscle weakness
Can use when Tensilon test too risky Place ice pack over eyelid for 2 minutes
Cooling improves neuromuscular transmission Re-evaluate degree of ptosis
80% sensitive

Does This Patient Have Myasthenia Gravis?Katalin Scherer, Richard S. Bedlack, David L. Simel,
h/o Speech becoming unintelligible during prolonged speech LR 4.5
Presence of Peak sign LR 30 Food remaining in mouth after swallowing and
quiver test no increase in likelihood Ice test positive LR 24 (negative LR 0.16) Tensilon test positive LR 15 (negative LR 0.11) Sleep/rest test positive LR 53 (negative LR 0.52)
JAMA, April 20, 2005—Vol 293, No. 15
Myesthenia gravis: ED Points
Consider in the patient with progressive skeletal weakness
Know the “peak test” / “ice pack” test Myesthenic and cholinergic crisis look
similar If airway becomes an issue
Can be resistant to sux (need high doses) Non-depolarizers better

Case 3 (and 3a, 3b and 3c)
Case 3,3a,3b and 3c
A family presents with diplopia, dysarthria, and dysphagia. All have nausea and vomiting. One has a sore throat, one says it is hard to keep his head up. All feel “weak”.
VS Normal CN’s show multiple defects All have normal sensation All are fully alert Diagnosis…?
Botulism
Paralytic disease (“top down”) Caused by toxins from Clostridium
botulinum Found everywhere- top layers of soil, > 1,000 fathoms
below the sea, >11k feet elevation in a glacier! Lakes, rivers, fish, animals, etc etc
Gram + anaerobic rod Rods produce spores Spores produce toxin → toxin is bad

Botulism
6 forms of botulism are seen Food-borne Wound Infant Adult intestinal Injection Inhalational
Foodborne Botulism
1,000 cases per year world-wide 112 in the U.S. (2010 CDC data) Alaska highest in the U.S. (800x the rate of the
lower 48) Mikiyak- warm fermented whale meat and blubber Tipmuk- fish cached in willow leaves
Republic of Georgia highest worldwide Multiple food sources 94% are from home processed foods

Foodborne Botulism
Incubation 2 hours to 8 days Dose dependant
Typical Chain of Events: Food not heated enough to kill spores
Spores can live for hours at 212 deg F (100 deg C)
Food then held at temperatures that allow germination of spores
Spores produce toxin Toxin ingested

Infantile Botulism
Spores ingested or inhaled Multiply in the intestine Less acidic environment Immature gut physiology, and flora
The ingested spores produce toxin
Infantile Botulism
Vehicles Honey
16% of samples are positive for spores Accounts for 15% of cases
Corn Syrup 28% of samples positive for spores
Food Carpet, soil/dust, dust from new
construction

Botulism: Presentation
Symmetric Descending motor paralysis Involves cranial, spinal, and peripheral
nerves. NO CNS Changes !! NO SENSORY changes !!
Botulism: Testing
Can isolate from serum, feces, gastric aspirate, food source…but can’t wait for any of that (remember irreversible binding) State Lab
Usual labs useless Clinical diagnosis

Botulism: Treatment Supportive care for all Heptavalent Antitoxin (CDC has it @ 9 regional locations)
Only works on free toxin. Once toxin binds to the nerve, it is permanent. Dose = one vial, administered IV
For wound botulism, wound is debrided and antitoxin infiltrated into area
BabyBIG (age < 1 year) Human Botulinum Immune Globulin Supply held by the California Dept of Health $45,000 for a full course

Anti-toxin
With either anti-toxin, you cannot un-do paralysis…can only prevent worsening.
Earlier treatment = less mortality (once full paralysis, it will take months for re-generation of Ach release capability)
Mortality = 10% when antitoxin within 24 hours after sx onset
Mortality = 15% when antitoxin > 24 hours after sx onset Mortality = 46% when antitoxin not given before
complete paralysis
Wound Botulism: Treatment
Antibiotics helpful in wound botulism ONLY Pen G IV
20-30 million U/kg/d IV in 6 divided doses
Chloramphenicol 50 mg/kg/d IV
Clindamycin 600 mg IV q8h
Botulism: Prevention Home Canned Foods
Sterilize with pressure cooker 250o F x 30 min
Discard bulging cans Don’t let cooked foods sit at room
temperature for long periods of time
Don’t give honey / corn syrup to infants

Botulism: Key Points
Descending paralytic disease Multiple routes of entry Think about this when faced with multiple
bilateral neuro deficits in head / face Normal mentation / sensation Early treatment greatly improves mortality

Case 4a and 4b

Case 4a and 4b
Twin 28-year-old sisters present to the ED both complaining of weakness.
One is just back from hiking the Appalachian trail, and the other is training for a marathon.
The hiker is complaining of progressive proximal muscle weakness over the past 10 days. The runner says she gets profoundly weak after she runs.

Case 4a and 4b
They both have normal VS and normal mentation. On careful inspection, the hiker has a diagnostic skin finding. Following running on a treadmill in the cardiac services lab, the runner has a diagnostic lab finding.

The Runner
K = 4.3 (pre-running) K = 1.9 (immediately
after running) K = 4.2 (post-running)

Tick Paralysis
Rare, usually Western US/Canada. All ticks implicated, but most cases = D.
Andersonii (Rocky Mtn wood tick) Tick needs to be attached / feeding for 4-7
days (minimum) Salivary toxin slows motor conduction
(probably via sodium channel interruption) Paresthesias / weakness / fatigue with
normal sensation & sensorium.

Tick Paralysis
Can be confused with LGBS (guillain-barre)
Need to look in all the nooks and crannies
Expect substantial improvement within hours of tick removal
Hypokalemic periodic paralysis
Rare (super-rare) related to a defect (usually inherited) in muscle ion-channels
Attacks triggered by vigorous exercise, stress, high-carb meals (all drive K into cells via epi, insulin, or both)
Proximal muscle weakness (legs > arms). Can have hyporeflexia.
Normal exam between attacks.
Hypokalemic periodic paralysis
Between attacks K is usually normal After trigger that drives it into cells
(stress / exercise / carbs), then avg = 2.4(with as low as 1.5 described).
Can be associated with hyperthyroidism Need to trigger it to diagnose it Can treat (and prevent) with oral K
supplementation.

Life Threatening Weakness
Lots of causes of “weakness” Think of the “big 4”
Guillan-Barre (Landry + Strohl) Myasthenia Gravis Botulism Periodic paralysis (tick / hypokalemia)
All are: Rare Have potential for “saves” Have specific “tricks” for ED identification
