limbs applied anatomy 2015
TRANSCRIPT
The Applied Anatomy of the
Limbs
Presenter: Dr. D B Mwale
Moderator: Dr Munthali

Content
o Embryological Development
o Lower Limb
o Gross Anatomy
o Applied Anatomy
o Upper Limb
o Gross Anatomy
o Applied Anatomy
Frolich, Human Anatomy,UpprLimb
What is a limb? Ventral somatic outgrowth of outer tube
Bones (with bone, cartilage, marrow, NAV, etc.) Joints Muscle Nerves Vascular supply
No viscera--all innervation is somatic (motor or sensory) from ventral ramus of spinal nerve (except autonomics to blood vessels)
From paraxial mesoderm (i.e. somites): Dermatome gives rise to connective tissue of the dermis
Myotome gives rise to limb muscles
From lateral plate mesoderm: Bones of arm, forearm, hand, thigh, leg and foot
Blood vessels
Connective tissue (except for that of the dermis)
Peripheral nerve elements,are derived from neural crest
EMBRYOLOGY
initial growth and patterning of the limbs occurs during weeks 4 – 8.
Limb buds appear at about 4 weeks and much of the basic structures of the limbs (bones and muscle groups) are established by 8 weeks. After 8 weeks, the limb elements then just increase in size.
Disruption of growth and/or patterning can result in many possible defects:
Amelia: absence of an entire limb (e.g. early loss of Fgf signaling)
Meromelia: absence of part of a limb (e.g. later or partial loss of Fgfsignaling)
Phocomelia: short, poorly formed limb (e.g. partial loss of Fgf;
Adactyly: absence of digits (e.g. even later loss of Fgf)
Ectrodactyly: “Lobster-Claw” deformity (variant of adactyly –middle digit is lost)
Polydactyly: extra digits
Syndactyly: fusion of digits
Frolich, Human Anatomy,UpprLimb
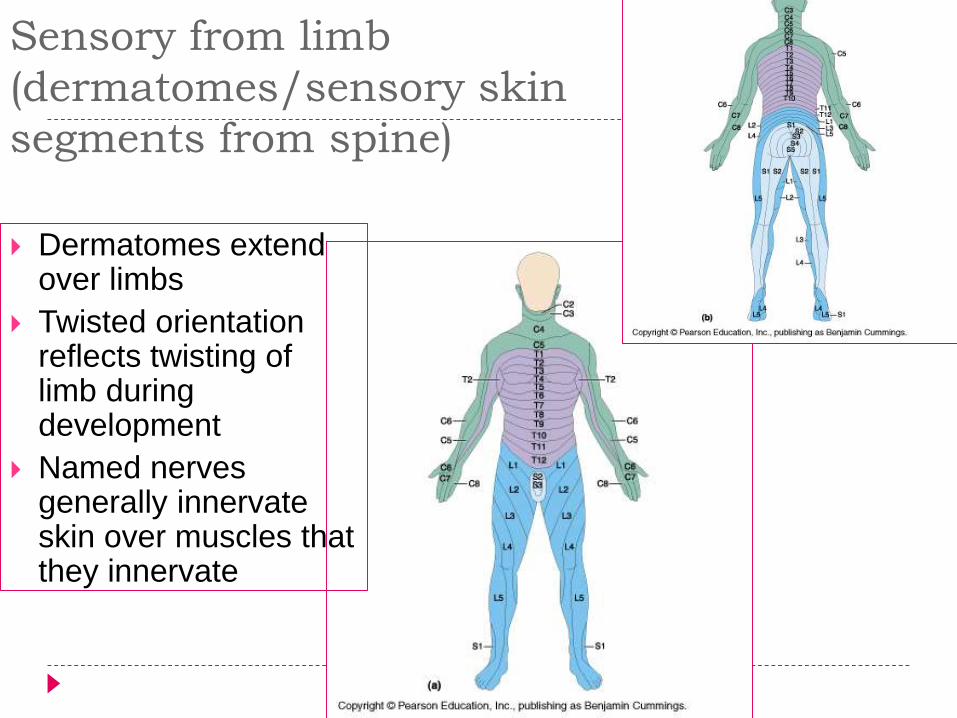
Sensory from limb
(dermatomes/sensory skin
segments from spine)
Dermatomes extend over limbs
Twisted orientation reflects twisting of limb during development
Named nerves generally innervate skin over muscles that they innervate
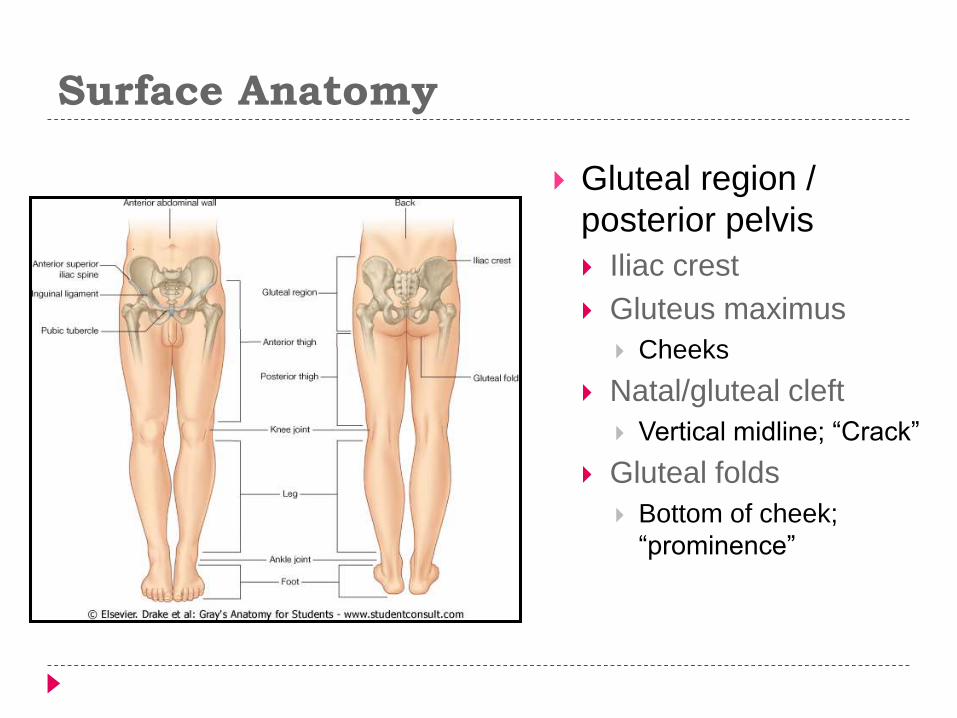
Surface Anatomy
Gluteal region /
posterior pelvis
Iliac crest
Gluteus maximus
Cheeks
Natal/gluteal cleft
Vertical midline; “Crack”
Gluteal folds
Bottom of cheek;
“prominence”
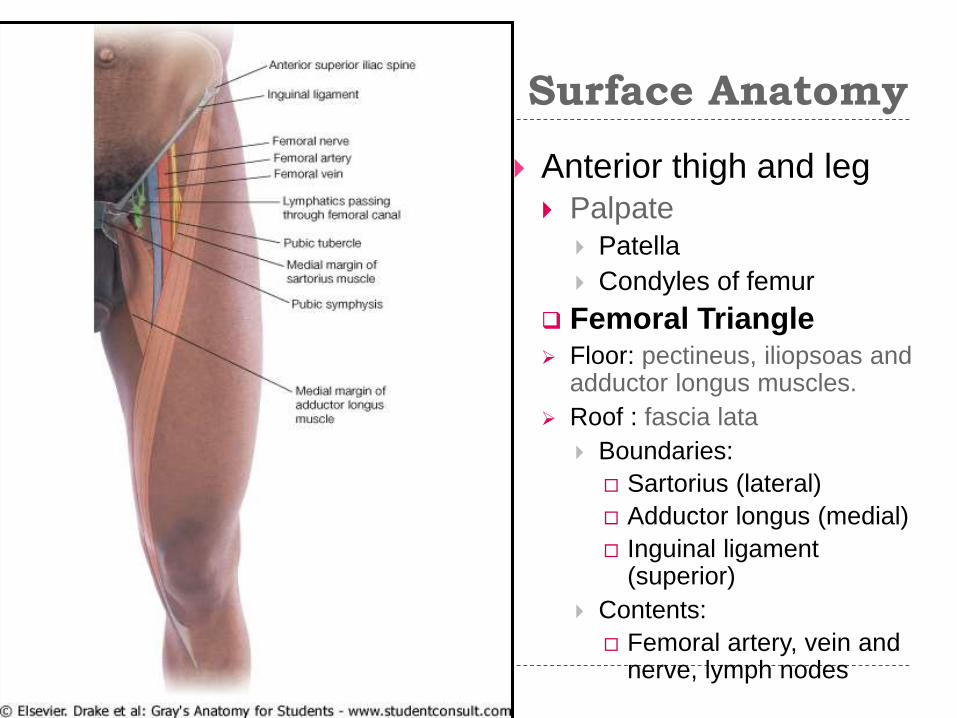
Surface Anatomy
Anterior thigh and leg Palpate
Patella
Condyles of femur
Femoral Triangle Floor: pectineus, iliopsoas and
adductor longus muscles.
Roof : fascia lata
Boundaries:
Sartorius (lateral)
Adductor longus (medial)
Inguinal ligament (superior)
Contents:
Femoral artery, vein and nerve, lymph nodes
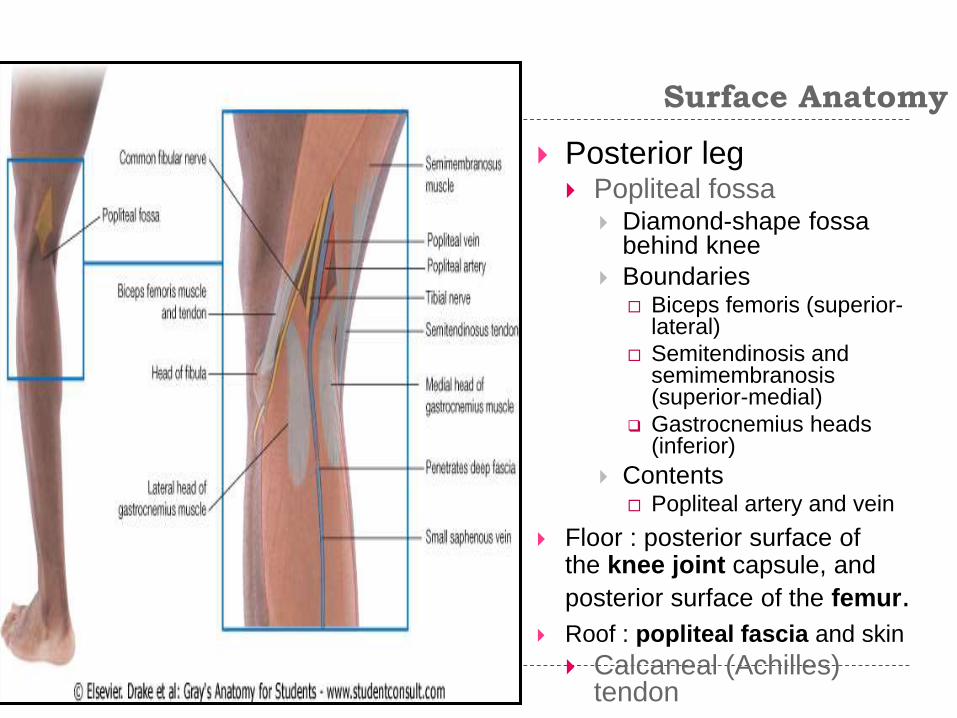
Surface Anatomy
Posterior leg Popliteal fossa
Diamond-shape fossabehind knee
Boundaries Biceps femoris (superior-
lateral)
Semitendinosis and semimembranosis(superior-medial)
Gastrocnemius heads (inferior)
Contents Popliteal artery and vein
Floor : posterior surface of the knee joint capsule, and
posterior surface of the femur. Roof : popliteal fascia and skin
Calcaneal (Achilles) tendon
Skeletal Composition

Bones of the Lower Limb
Function: Locomotion
Carry weight of entire erect body
Support
Points for muscular attachments
Components: Thigh
Femur
Knee Patella
Leg Tibia (medial)
Fibula (lateral)
Foot Tarsals (7)
Metatarsals (5)
Phalanges (14)

Thigh
Femur Largest, longest,
strongest bone in the body!!
Receives a lot of stress
Courses medially More in women!
Articulates with acetabulumproximally
Articulates with tibia and patella distally
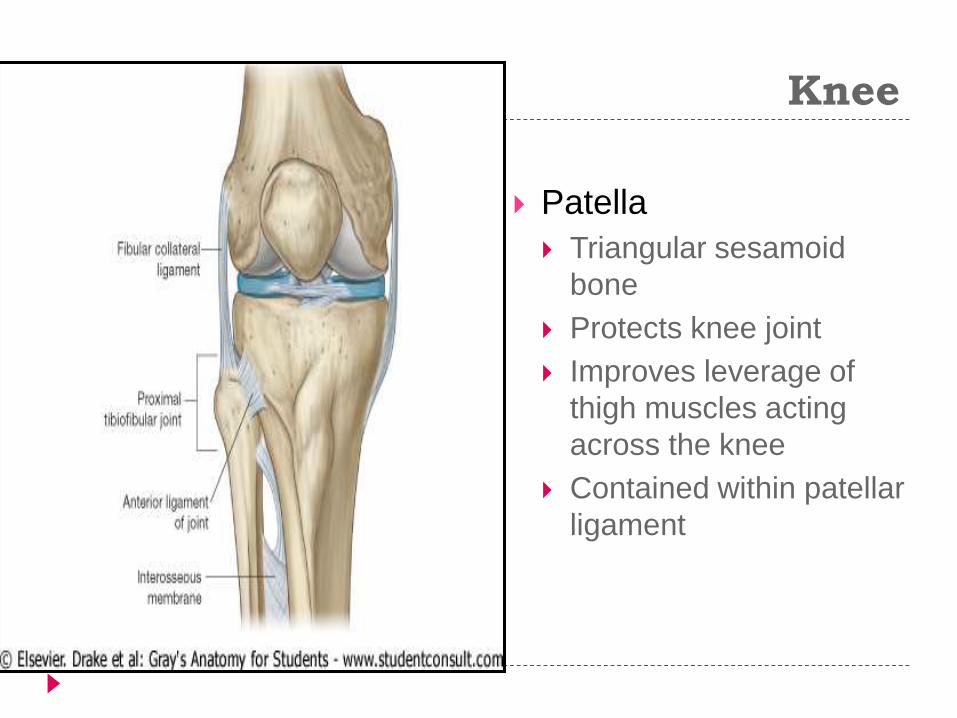
Knee
Patella
Triangular sesamoid
bone
Protects knee joint
Improves leverage of
thigh muscles acting
across the knee
Contained within patellar
ligament
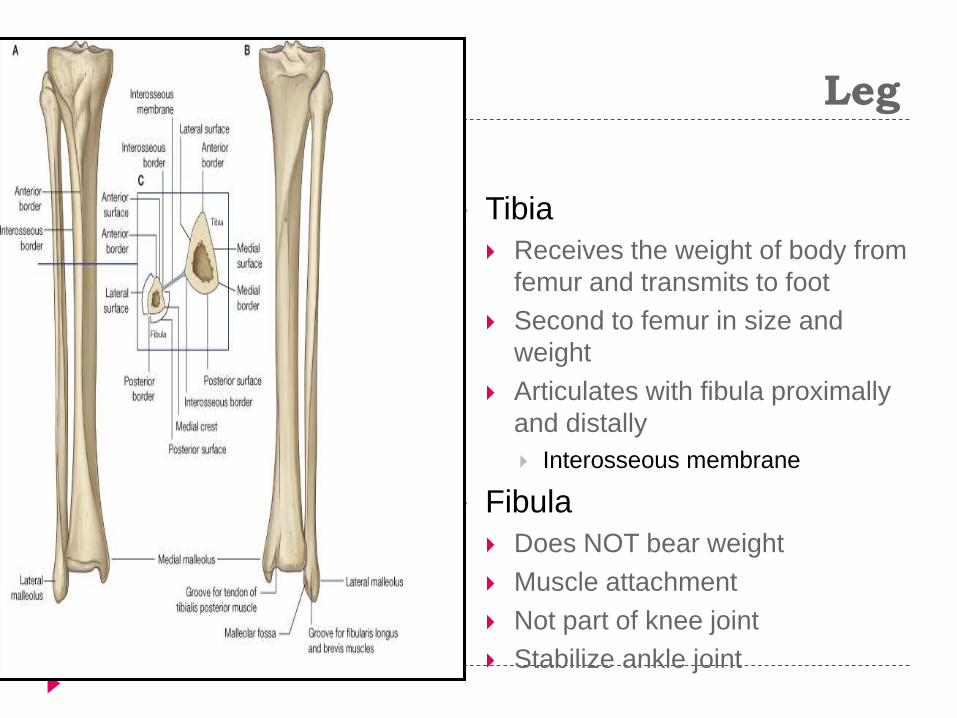
Leg
Tibia
Receives the weight of body from
femur and transmits to foot
Second to femur in size and
weight
Articulates with fibula proximally
and distally
Interosseous membrane
Fibula
Does NOT bear weight
Muscle attachment
Not part of knee joint
Stabilize ankle joint

Foot
Function: Supports the weight of the
body
Act as a lever to propel the body forward
Parts: Tarsals
Talus = ankle
Between tibia and fibula
Articulates with both
Calcaneus = heel
Attachment for Calcanealtendon
Carries talus
Navicular
Cuboid
Medial, lateral and intermediate cuneiforms
Metatarsals

Foot
3 arches Medial
Lateral
Transverse
Has tendons that run inferior to foot bones
Help support arches of foot
Function Recoil after stepping
Longitudinal
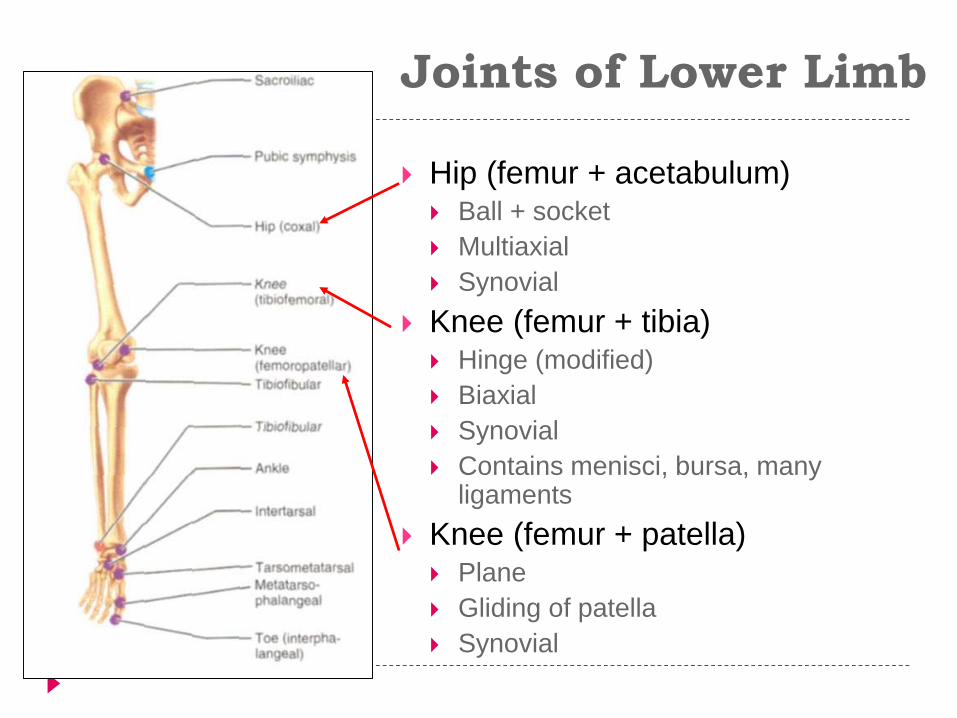
Joints of Lower Limb
Hip (femur + acetabulum) Ball + socket
Multiaxial
Synovial
Knee (femur + tibia) Hinge (modified)
Biaxial
Synovial
Contains menisci, bursa, many ligaments
Knee (femur + patella) Plane
Gliding of patella
Synovial
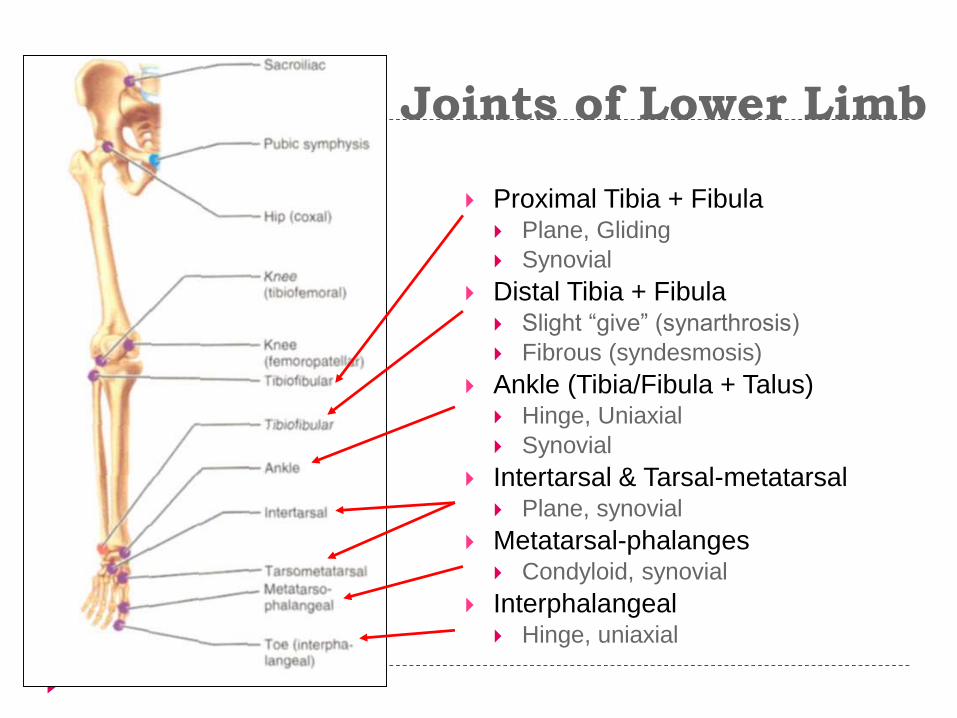
Joints of Lower Limb
Proximal Tibia + Fibula Plane, Gliding
Synovial
Distal Tibia + Fibula Slight “give” (synarthrosis)
Fibrous (syndesmosis)
Ankle (Tibia/Fibula + Talus) Hinge, Uniaxial
Synovial
Intertarsal & Tarsal-metatarsal Plane, synovial
Metatarsal-phalanges Condyloid, synovial
Interphalangeal Hinge, uniaxial
Muscles

Muscles of Thigh
& Hip Gluteals
Posterior pelvis
Extend thigh
Rotate thigh
Abducts thigh
Anterior Compartment Thigh Flexes thigh at hip
Extends leg at knee
Medial/Adductor Compartment Adducts thigh
Medially rotates thigh
Posterior Compartment Thigh Extends thigh
Flexes leg
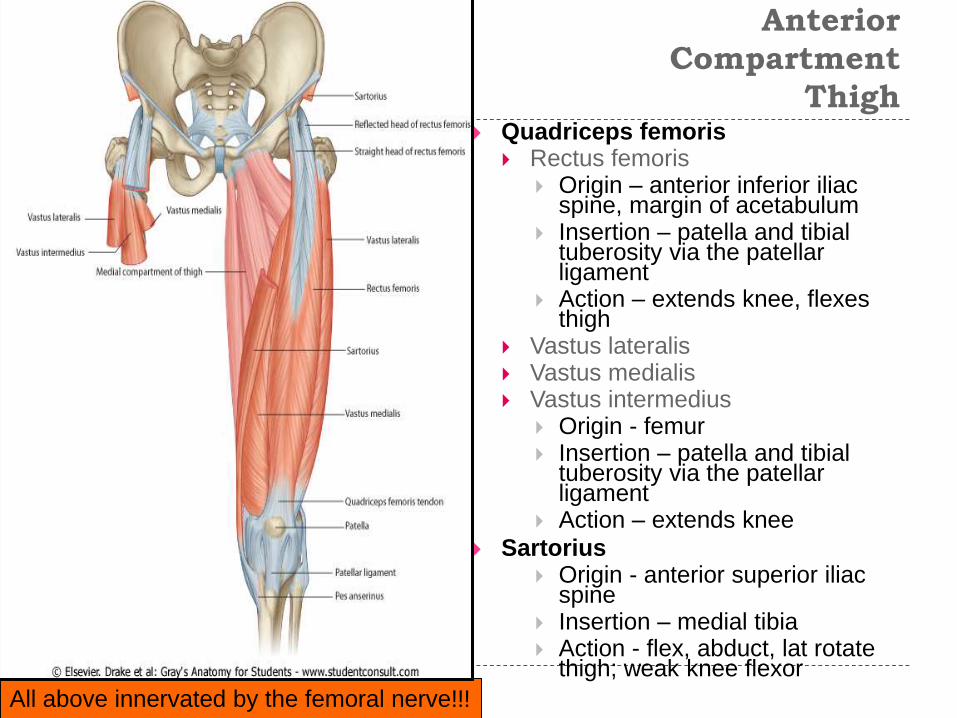
Anterior
Compartment
Thigh Quadriceps femoris
Rectus femoris Origin – anterior inferior iliac
spine, margin of acetabulum Insertion – patella and tibial
tuberosity via the patellar ligament
Action – extends knee, flexes thigh
Vastus lateralis Vastus medialis Vastus intermedius
Origin - femur Insertion – patella and tibial
tuberosity via the patellar ligament
Action – extends knee
Sartorius Origin - anterior superior iliac
spine Insertion – medial tibia Action - flex, abduct, lat rotate
thigh; weak knee flexor
All above innervated by the femoral nerve!!!
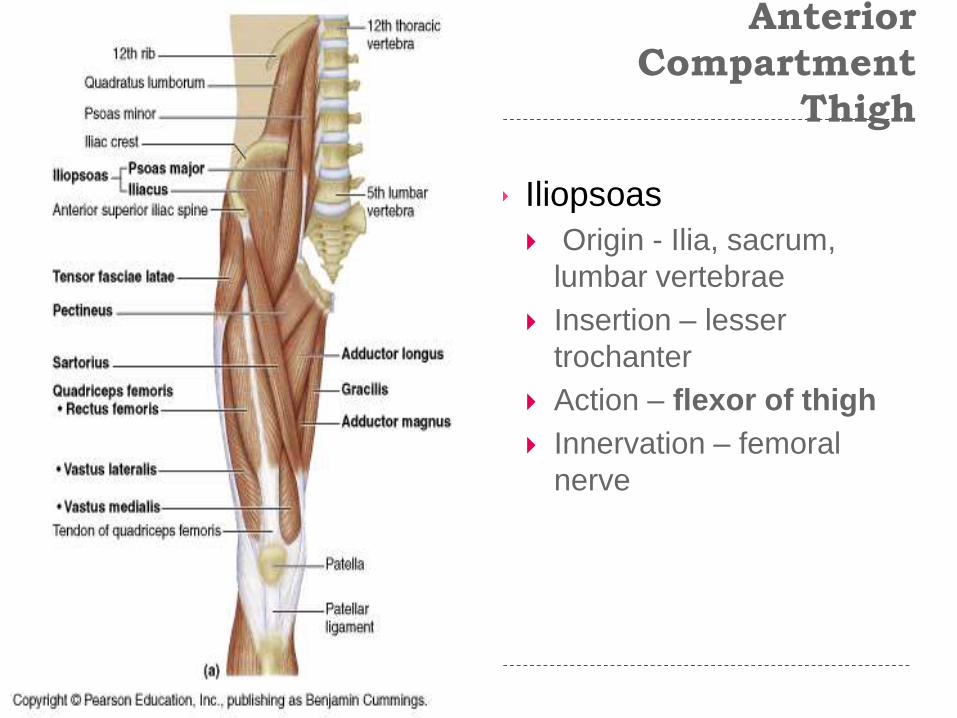
Anterior
Compartment
Thigh
Iliopsoas
Origin - Ilia, sacrum,
lumbar vertebrae
Insertion – lesser
trochanter
Action – flexor of thigh
Innervation – femoral
nerve

AdductorsMEDIAL COMPARTMENT
Adductor longus Adductor brevis Adductor magnus
Origin – inferior pelvis Insertion - femur Action – adducts and medial rotates Innervation – Obturator nerve
Pectineus Origin - pubis Insertion – lesser trochanter Action – adducts, medial rotates Innervation – femoral, sometimes obturator
Gracilis Origin - pubis Insertion – medial tibia Action – adducts thigh, flex, medial, rotates
leg Innervation – Obturator nerve
innervated by the obturator nerve
Arterial supply is via the obturator artery.

Posterior Compartment –
Hamstring
Biceps femoris (2 heads)
Origin – ischial tuberosity, distal femur
Insertion - lateral tibia, head fibula
Action - thigh extension, knee flexion, lateral rotation
Semitendinosus
Semimembranosus
Origin - ischial tuberosity
Insertion - medial tibia
Action - thigh extension, knee flexion, medial rotation
Sciatic nerve innervates all of the above muscles!!!
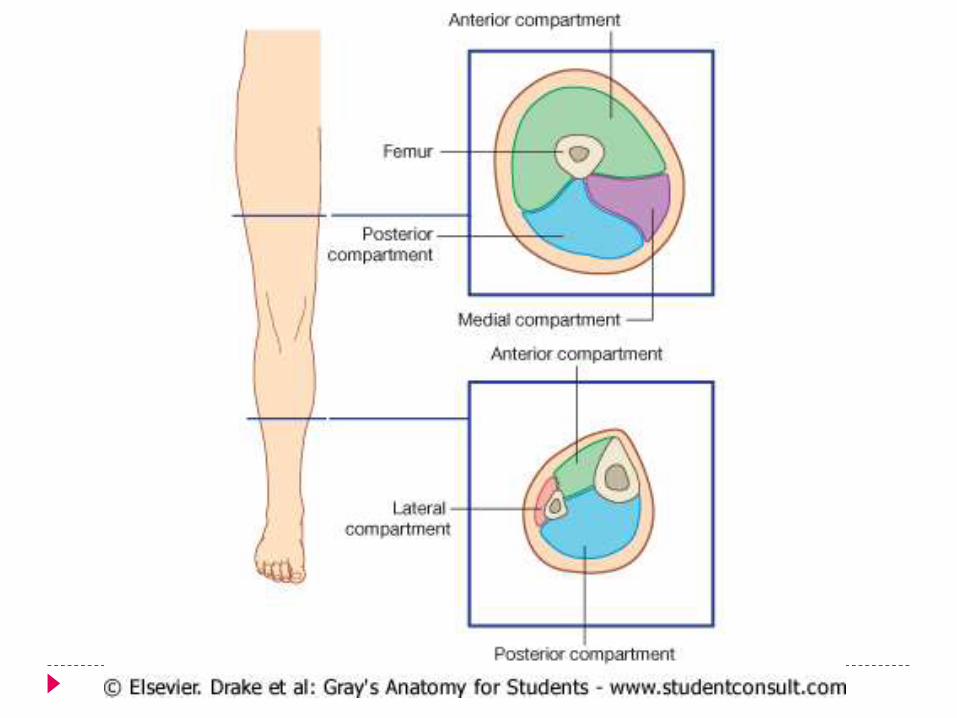
Muscles of the Leg
o Anterior Compartmento Dorsiflex ankle, invert foot, extend
toeso Innervation: Deep fibular nerve
o Lateral Compartmento Plantarflex, evert footo Innervation: Superficial Fibular
nerve
o Posterior Compartment o Superficial and deep layerso Plantarflex foot, flex toeso Innervation: Tibial nerve
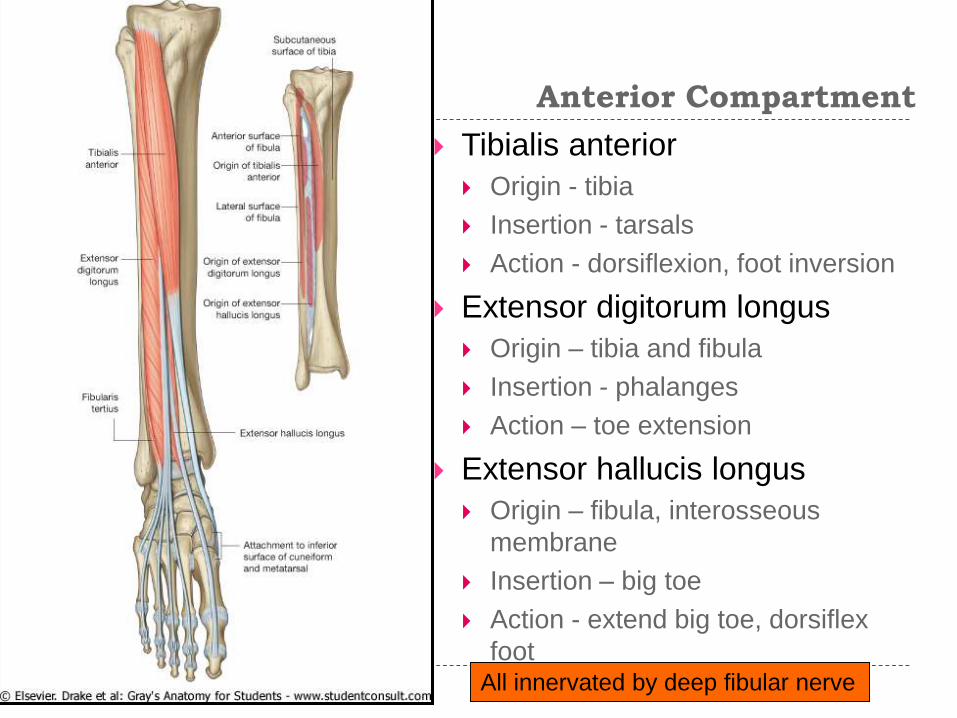
Anterior Compartment
Tibialis anterior
Origin - tibia
Insertion - tarsals
Action - dorsiflexion, foot inversion
Extensor digitorum longus
Origin – tibia and fibula
Insertion - phalanges
Action – toe extension
Extensor hallucis longus
Origin – fibula, interosseous
membrane
Insertion – big toe
Action - extend big toe, dorsiflex
foot All innervated by deep fibular nerve
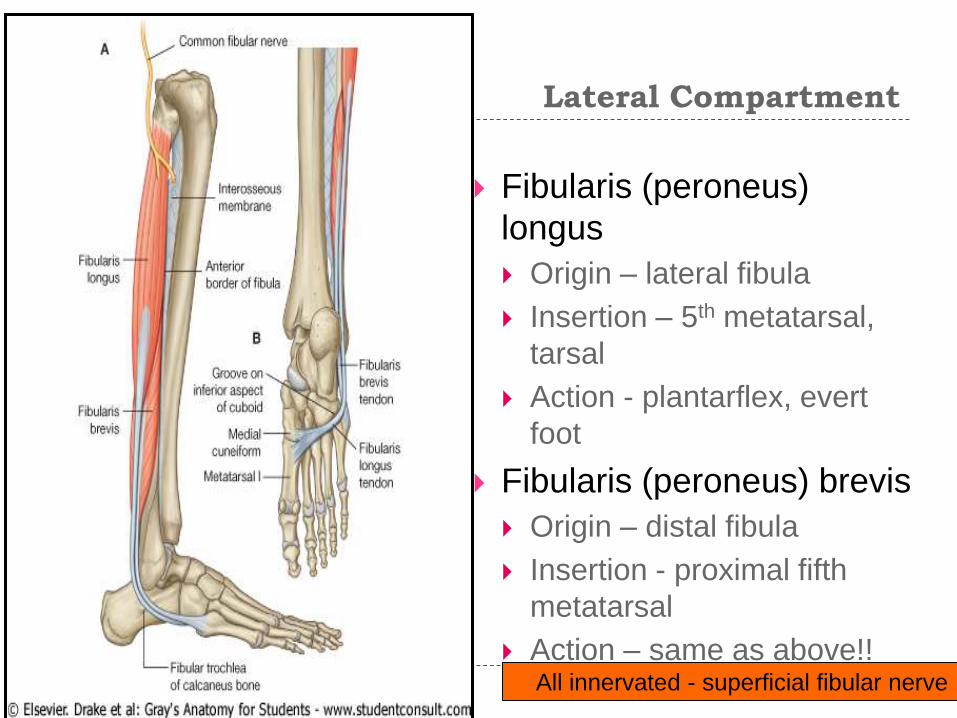
Lateral Compartment
Fibularis (peroneus)
longus
Origin – lateral fibula
Insertion – 5th metatarsal,
tarsal
Action - plantarflex, evert
foot
Fibularis (peroneus) brevis
Origin – distal fibula
Insertion - proximal fifth
metatarsal
Action – same as above!!All innervated - superficial fibular nerve

Superficial Posterior
Compartment
Triceps surae
Gastrocnemius (2 heads)
Origin - medial and lateral condyles
of femur
Insertion - posterior calcaneus via
Achilles tendon
Soleus
Origin – tibia and fibula
Insertion – same as above
Action of both – plantarflex foot
Plantaris (variable)
Origin – posterior femur
Insertion – same as above!
Action – plantarflex foot, week knee
flexion
All innervated by the tibial nerve
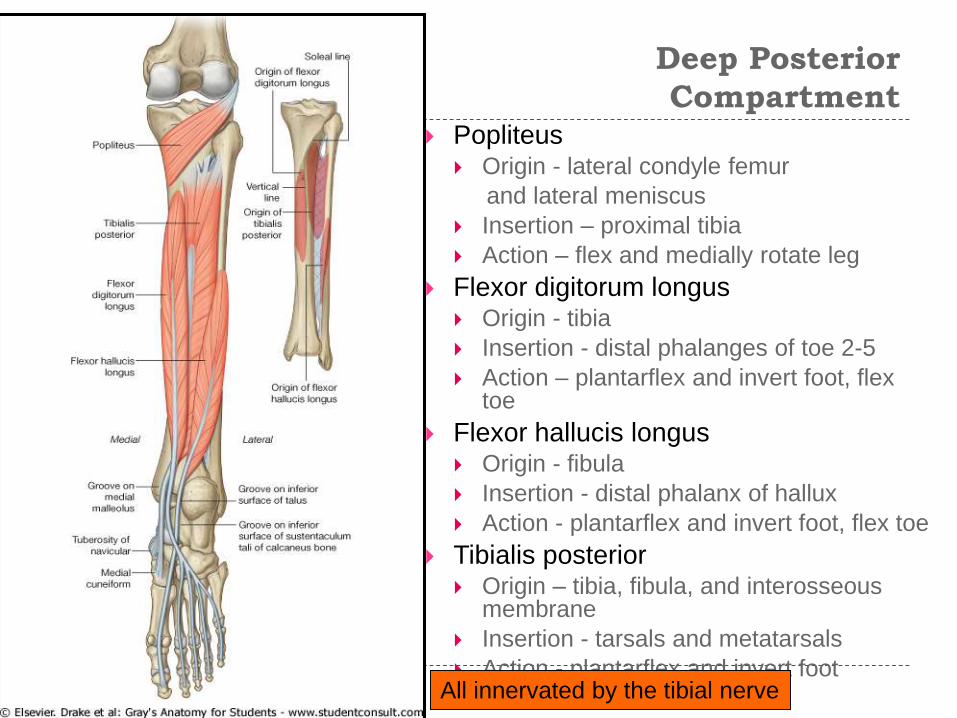
Deep Posterior
Compartment Popliteus
Origin - lateral condyle femur
and lateral meniscus
Insertion – proximal tibia
Action – flex and medially rotate leg
Flexor digitorum longus Origin - tibia
Insertion - distal phalanges of toe 2-5
Action – plantarflex and invert foot, flex toe
Flexor hallucis longus Origin - fibula
Insertion - distal phalanx of hallux
Action - plantarflex and invert foot, flex toe
Tibialis posterior Origin – tibia, fibula, and interosseous
membrane
Insertion - tarsals and metatarsals
Action - plantarflex and invert footAll innervated by the tibial nerve
Innervation
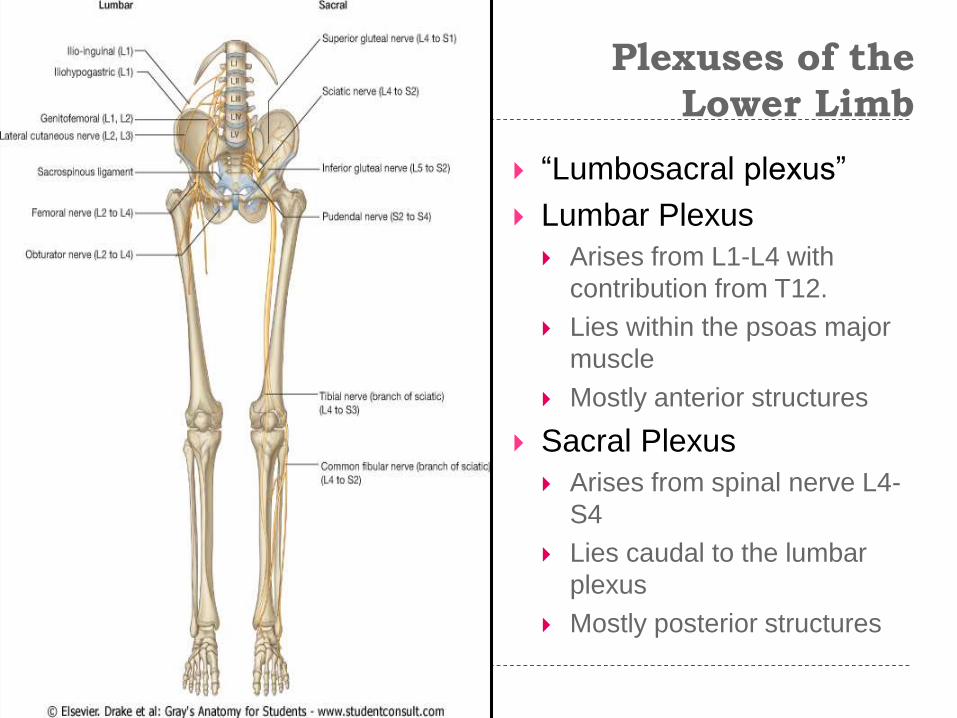
Plexuses of the
Lower Limb
“Lumbosacral plexus”
Lumbar Plexus
Arises from L1-L4 with
contribution from T12.
Lies within the psoas major
muscle
Mostly anterior structures
Sacral Plexus
Arises from spinal nerve L4-
S4
Lies caudal to the lumbar
plexus
Mostly posterior structures
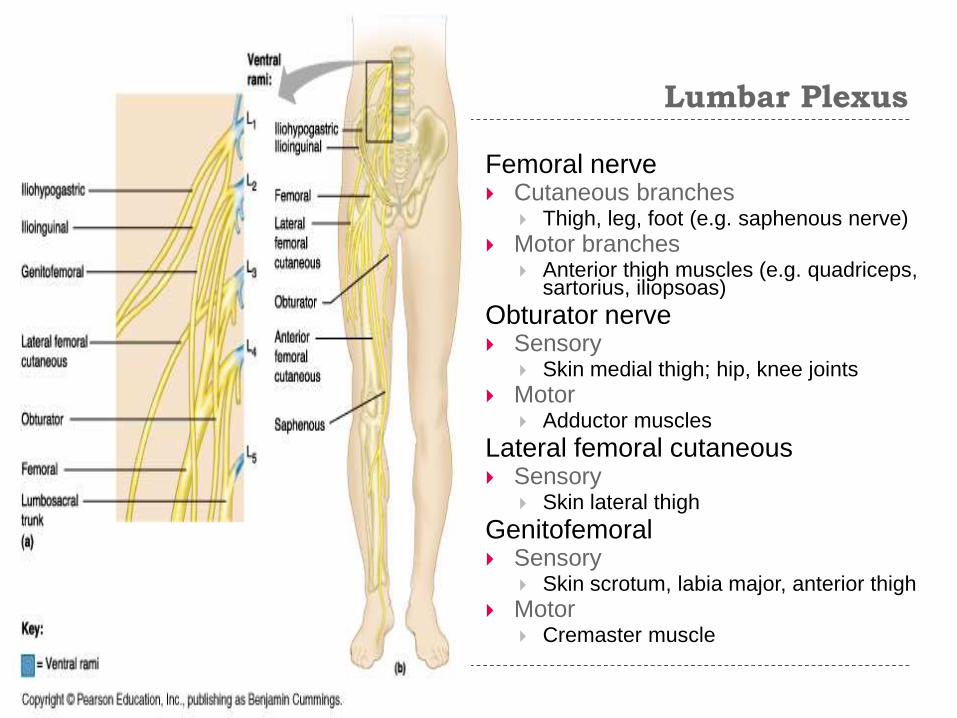
Lumbar Plexus
Femoral nerve Cutaneous branches
Thigh, leg, foot (e.g. saphenous nerve)
Motor branches Anterior thigh muscles (e.g. quadriceps,
sartorius, iliopsoas)
Obturator nerve Sensory
Skin medial thigh; hip, knee joints
Motor Adductor muscles
Lateral femoral cutaneous Sensory
Skin lateral thigh
Genitofemoral Sensory
Skin scrotum, labia major, anterior thigh
Motor Cremaster muscle
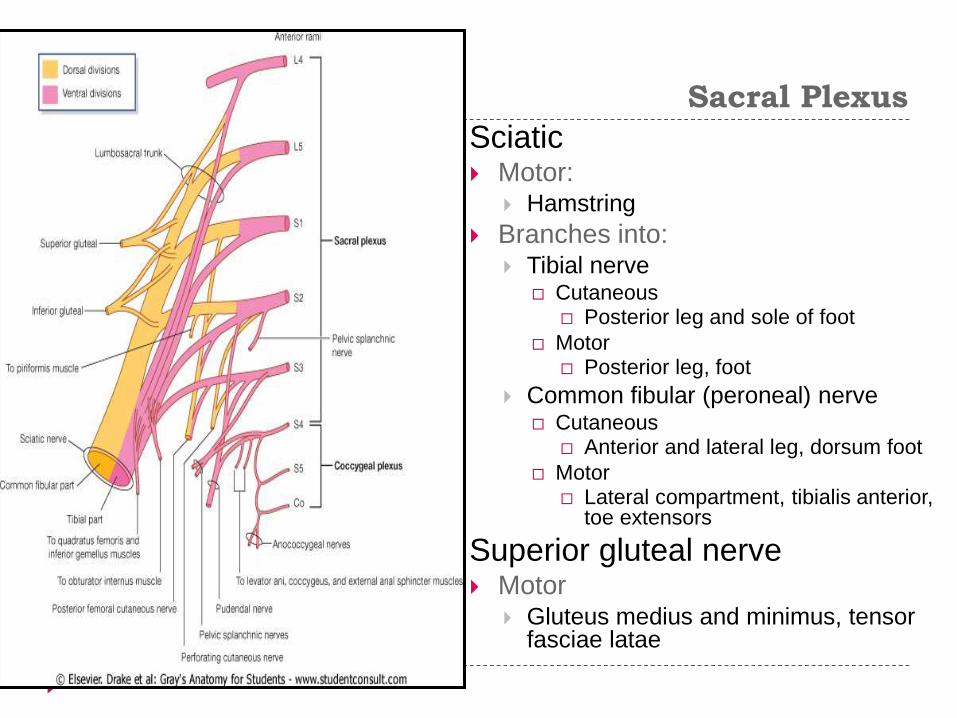
Sacral Plexus
Sciatic Motor:
Hamstring
Branches into: Tibial nerve
Cutaneous Posterior leg and sole of foot
Motor Posterior leg, foot
Common fibular (peroneal) nerve Cutaneous
Anterior and lateral leg, dorsum foot
Motor Lateral compartment, tibialis anterior,
toe extensors
Superior gluteal nerve Motor
Gluteus medius and minimus, tensor fasciae latae
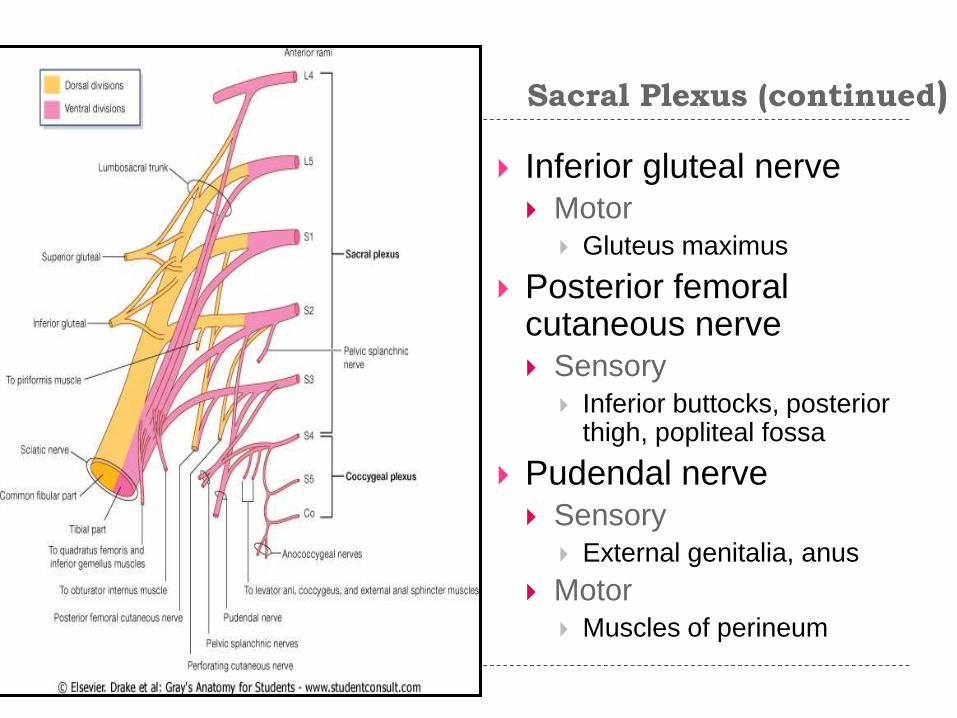
Sacral Plexus (continued)
Inferior gluteal nerve Motor
Gluteus maximus
Posterior femoral cutaneous nerve Sensory
Inferior buttocks, posterior thigh, popliteal fossa
Pudendal nerve
Sensory
External genitalia, anus
Motor
Muscles of perineum
Vasculature

Arteries
Common iliac (from
aorta) branches into:
Internal iliac
Supplies pelvic organs
External iliac
Supplies lower limb

Arteries
Internal iliac branches into: Cranial and Caudal Gluteals
(Superior and Inferior)
Gluteals
Internal Pudendal
Perineum, external genitalia
Obturator
Adductor muscles
Other branches supply rectum, bladder, uterus, vagina, male reproductive glands
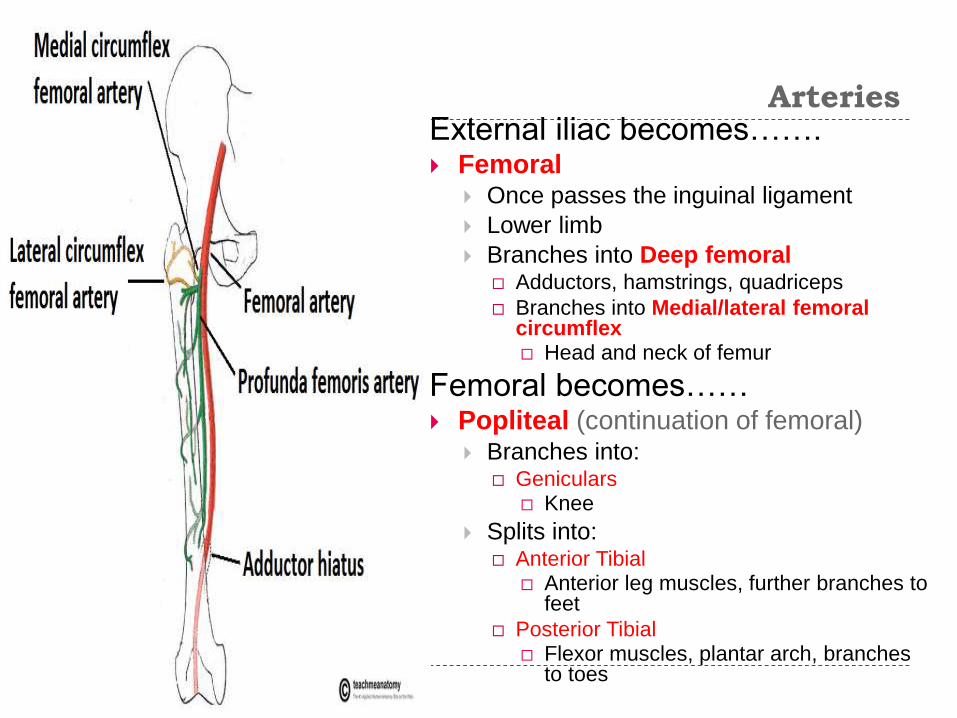
Arteries External iliac becomes…….
Femoral Once passes the inguinal ligament
Lower limb
Branches into Deep femoral Adductors, hamstrings, quadriceps
Branches into Medial/lateral femoral circumflex Head and neck of femur
Femoral becomes…… Popliteal (continuation of femoral)
Branches into: Geniculars
Knee
Splits into: Anterior Tibial
Anterior leg muscles, further branches to feet
Posterior Tibial Flexor muscles, plantar arch, branches
to toes
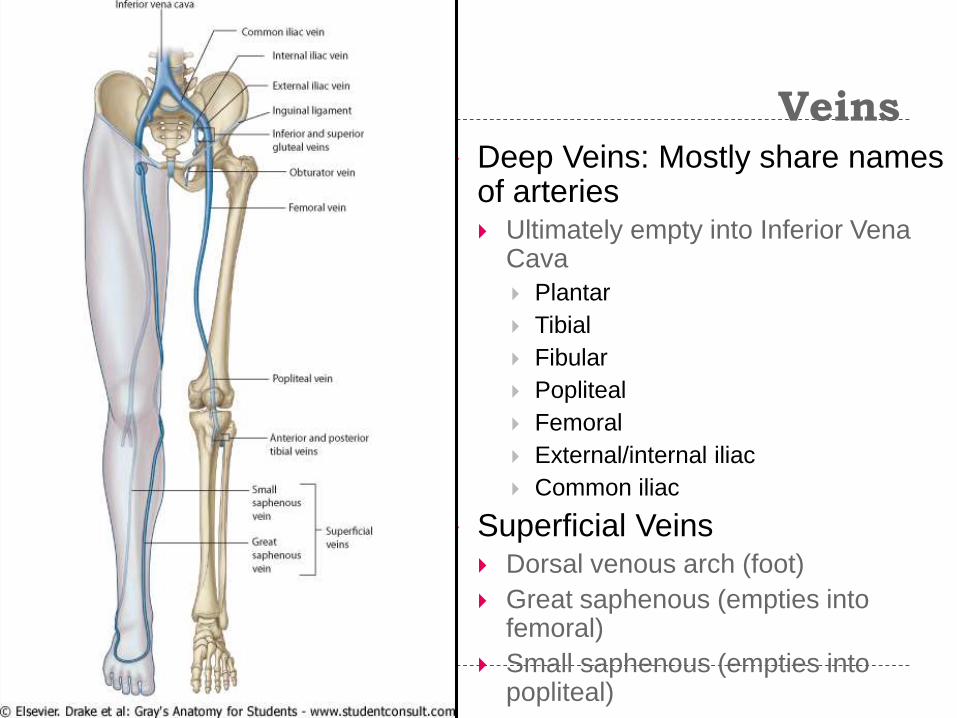
Veins Deep Veins: Mostly share names
of arteries Ultimately empty into Inferior Vena
Cava
Plantar
Tibial
Fibular
Popliteal
Femoral
External/internal iliac
Common iliac
Superficial Veins Dorsal venous arch (foot)
Great saphenous (empties into femoral)
Small saphenous (empties into popliteal)
Applying The Anatomy In The
Lower Limb
FEMUR
SURGICAL APPLICATION
Intracapsular fractures
Common in elderly
Damage medial femoral circumflex artery – avascular
necrosis of the femoral head
Femoral shaft fractures
Can damage the femoral artery and nerve
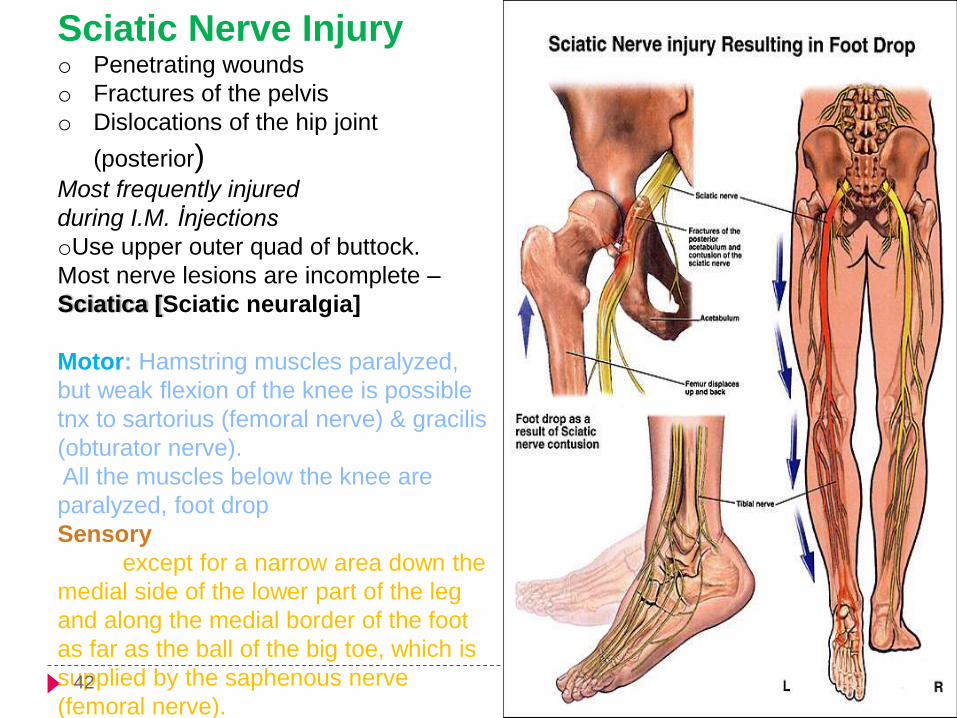
Sciatic Nerve Injuryo Penetrating wounds
o Fractures of the pelvis
o Dislocations of the hip joint
(posterior)Most frequently injured
during I.M. İnjections
oUse upper outer quad of buttock.
Most nerve lesions are incomplete –
Sciatica [Sciatic neuralgia]
Motor: Hamstring muscles paralyzed,
but weak flexion of the knee is possible
tnx to sartorius (femoral nerve) & gracilis
(obturator nerve).
All the muscles below the knee are
paralyzed, foot drop.
Sensory: Sensation is lost below the
knee, except for a narrow area down the
medial side of the lower part of the leg
and along the medial border of the foot
as far as the ball of the big toe, which is
supplied by the saphenous nerve
(femoral nerve).42
Femoral Hernia
bowel pushes into
the femoral canal,
underneath the inguinal
ligament.
It presents as a lump
situated inferolaterally
to the pubic tubercle.
common in women, due
to their wider bony
pelvis.
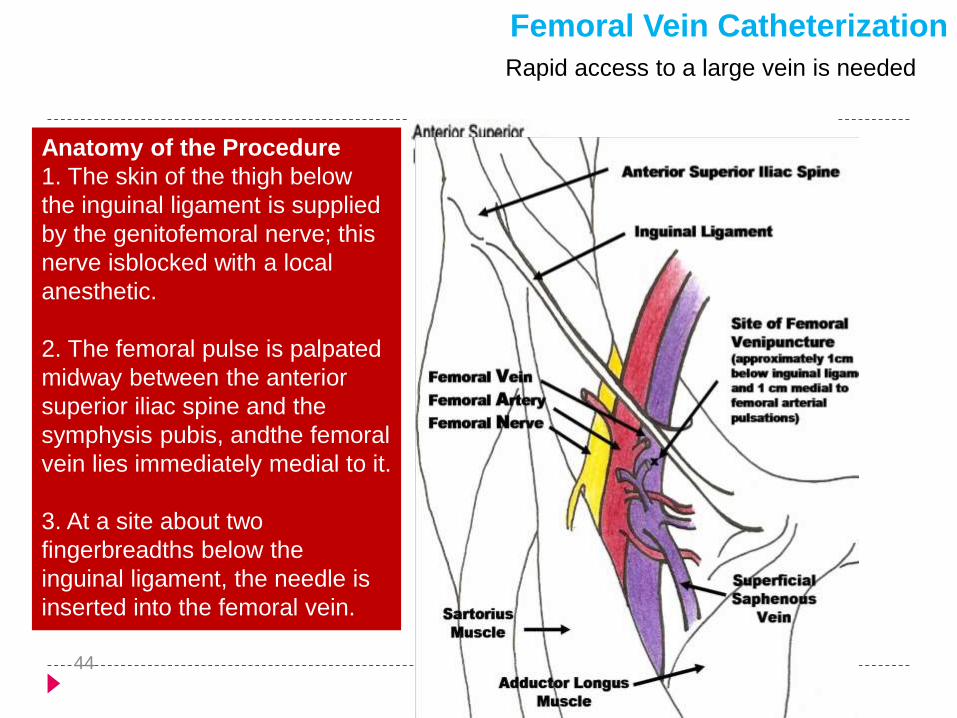
Rapid access to a large vein is needed
Femoral Vein Catheterization
Anatomy of the Procedure
1. The skin of the thigh below
the inguinal ligament is supplied
by the genitofemoral nerve; this
nerve isblocked with a local
anesthetic.
2. The femoral pulse is palpated
midway between the anterior
superior iliac spine and the
symphysis pubis, andthe femoral
vein lies immediately medial to it.
3. At a site about two
fingerbreadths below the
inguinal ligament, the needle is
inserted into the femoral vein.
44
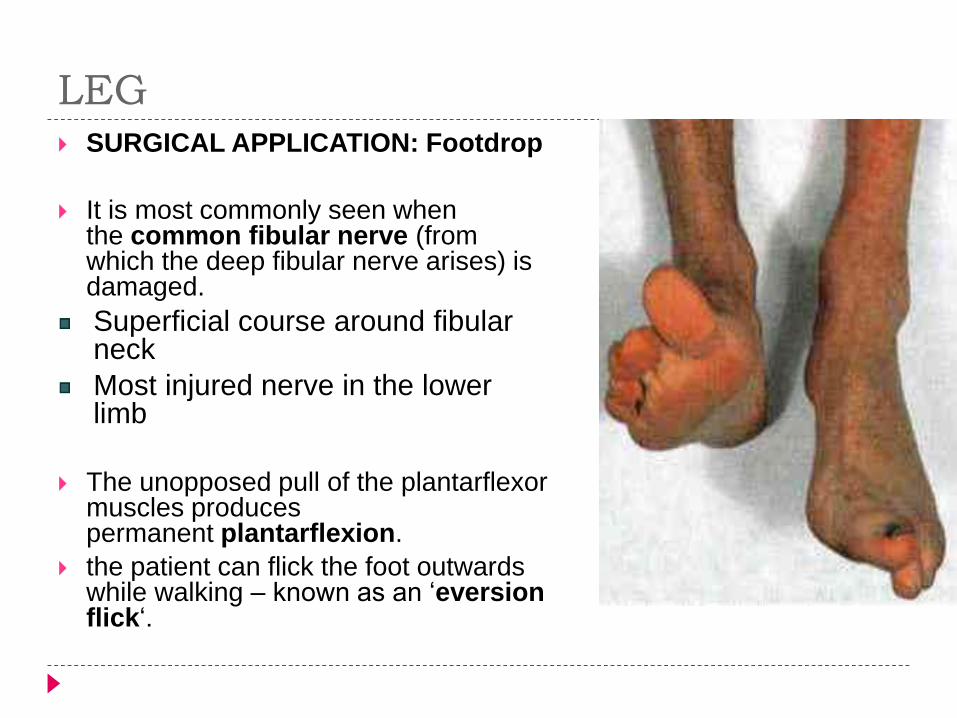
LEG SURGICAL APPLICATION: Footdrop
It is most commonly seen when the common fibular nerve (from which the deep fibular nerve arises) is damaged.
Superficial course around fibular neck
Most injured nerve in the lower limb
The unopposed pull of the plantarflexormuscles produces permanent plantarflexion.
the patient can flick the foot outwards while walking – known as an ‘eversionflick‘.
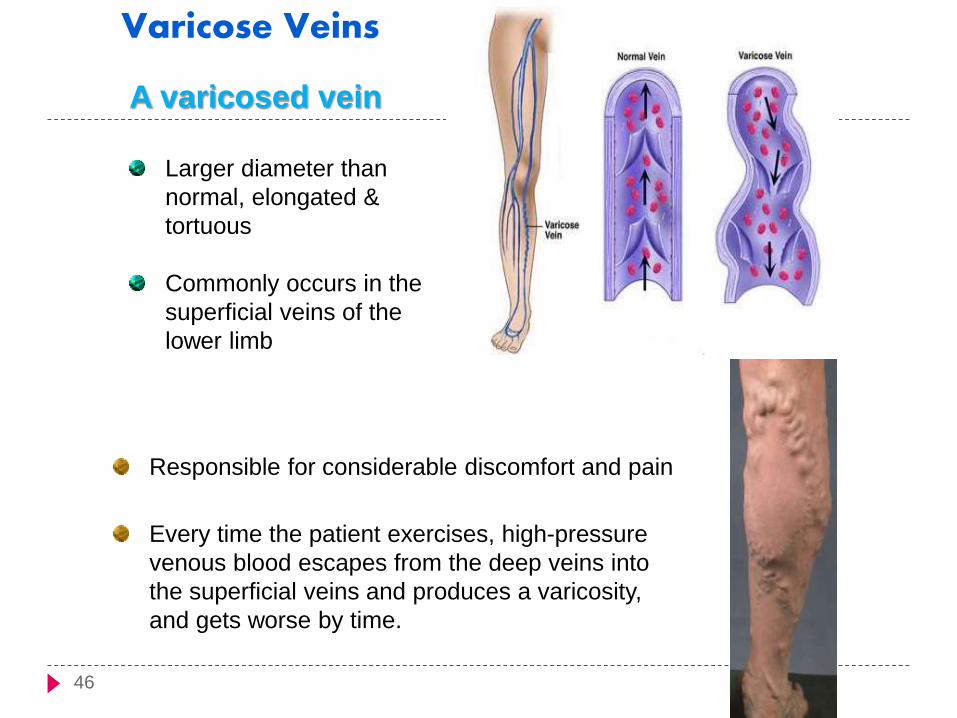
A varicosed vein
Larger diameter than
normal, elongated &
tortuous
Commonly occurs in the
superficial veins of the
lower limb
Varicose Veins
Responsible for considerable discomfort and pain
Every time the patient exercises, high-pressure
venous blood escapes from the deep veins into
the superficial veins and produces a varicosity,
and gets worse by time.
46
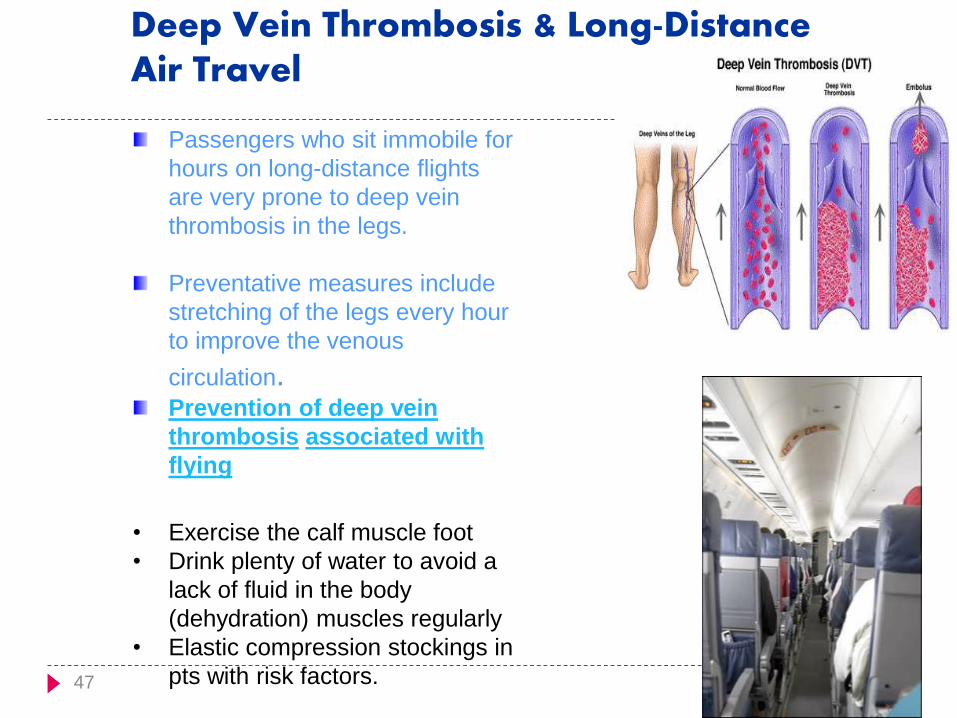
Passengers who sit immobile for
hours on long-distance flights
are very prone to deep vein
thrombosis in the legs.
Preventative measures include
stretching of the legs every hour
to improve the venous
circulation.Prevention of deep vein
thrombosis associated with
flying
• Exercise the calf muscle foot
• Drink plenty of water to avoid a
lack of fluid in the body
(dehydration) muscles regularly
• Elastic compression stockings in
pts with risk factors.
Deep Vein Thrombosis & Long-DistanceAir Travel
47
SURGICAL APPLICATION
Trendelenberg Sign - This signifies that the
abductor muscles on the standing limb are greatly
weakened or paralysed. For example, if the left leg
was raised, and pelvic drop was observed on that
side, the abductor muscles on the right leg are the
cause.
During walking, a weakness in the abductor muscles
gives rise to a characteristic gait. As the pelvis drops
on one side, the trunk lurches to the opposite side, in
an effort to maintain a steady pelvic level. This is
called the Trendelenberg gait.

UPPER LIMB
Frolich, Human Anatomy,UpprLimb
Frolich, Human Anatomy,UpprLimb
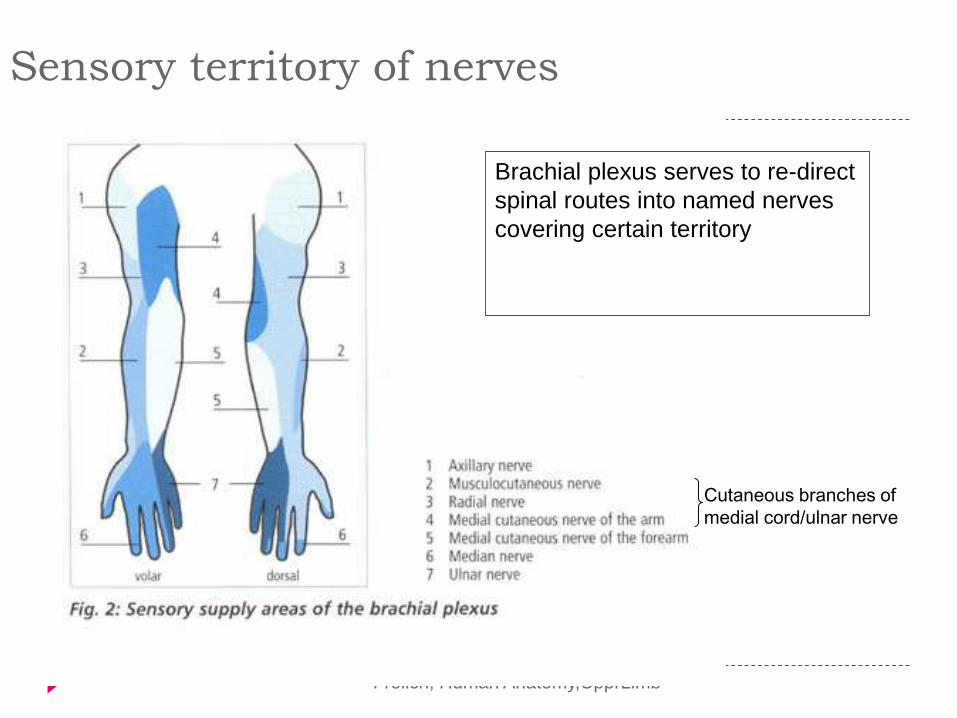
Sensory territory of nerves
Brachial plexus serves to re-direct
spinal routes into named nerves
covering certain territory
Cutaneous branches of
medial cord/ulnar nerve

Frolich, Human Anatomy,UpprLimb
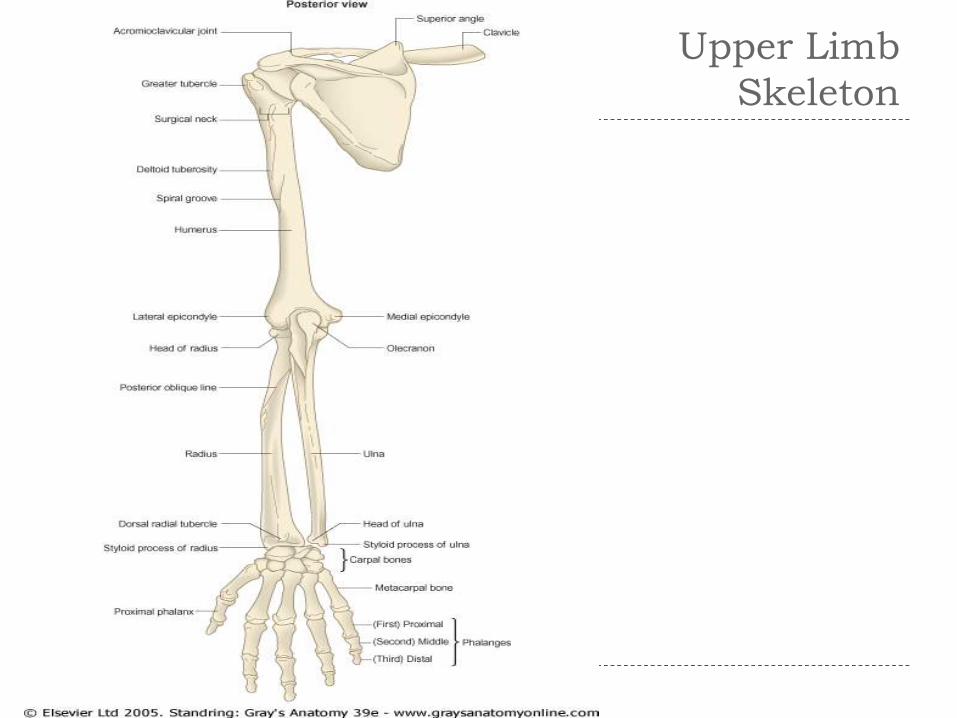
Upper Limb Skeleton
Scapula
Humerus
Radius, ulna
Carpals--proximal,
distal (x8)
Digits
Metacarpals (x5)
Phalanges (x14)
Upper Limb
Skeleton
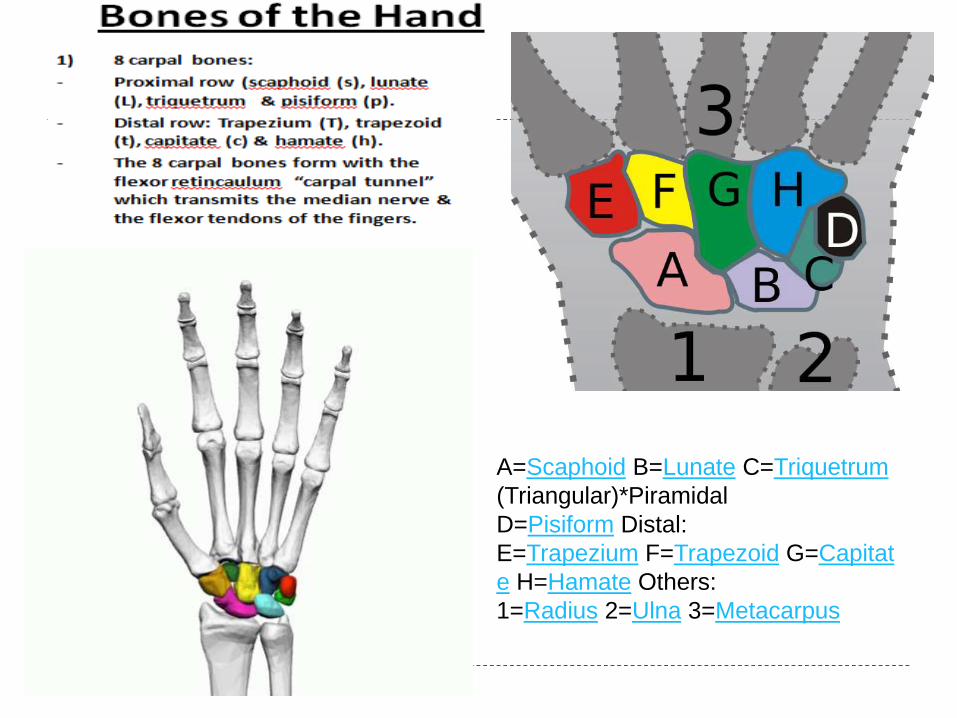
A=Scaphoid B=Lunate C=Triquetrum
(Triangular)*Piramidal
D=Pisiform Distal:
E=Trapezium F=Trapezoid G=Capitat
e H=Hamate Others:
1=Radius 2=Ulna 3=Metacarpus

Frolich, Human
Anatomy,UpprLimb
Surface Anatomy of Upper Limb
Biceps + Triceps brachii
Olecrenon Process
Medial Epicondyle
Cubital Fossa
Anterior surface elbow
Contents
Median Cubital Vein
Brachial Artery
Median Nerve
Boundaries
Medial= Pronator teres
Lateral= Brachioradialis
Superior= Line between epicondyles
pg 786 + 784
Frolich, Human
Anatomy,UpprLimb
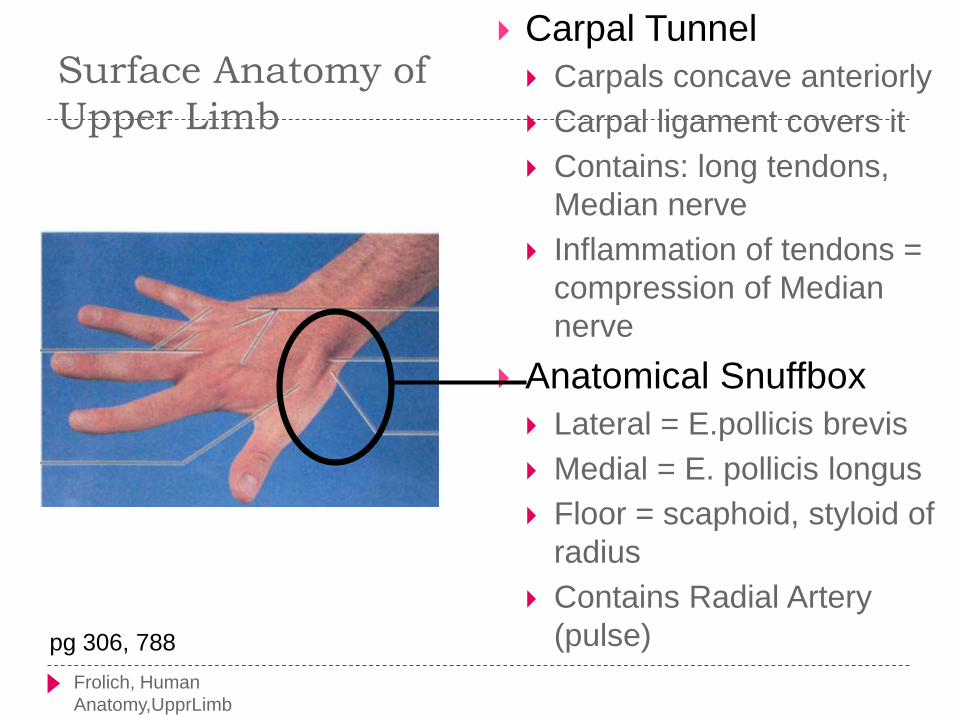
Surface Anatomy of
Upper Limb
Carpal Tunnel
Carpals concave anteriorly
Carpal ligament covers it
Contains: long tendons,
Median nerve
Inflammation of tendons =
compression of Median
nerve
Anatomical Snuffbox
Lateral = E.pollicis brevis
Medial = E. pollicis longus
Floor = scaphoid, styloid of
radius
Contains Radial Artery
(pulse)pg 306, 788
Frolich, Human Anatomy,UpprLimb
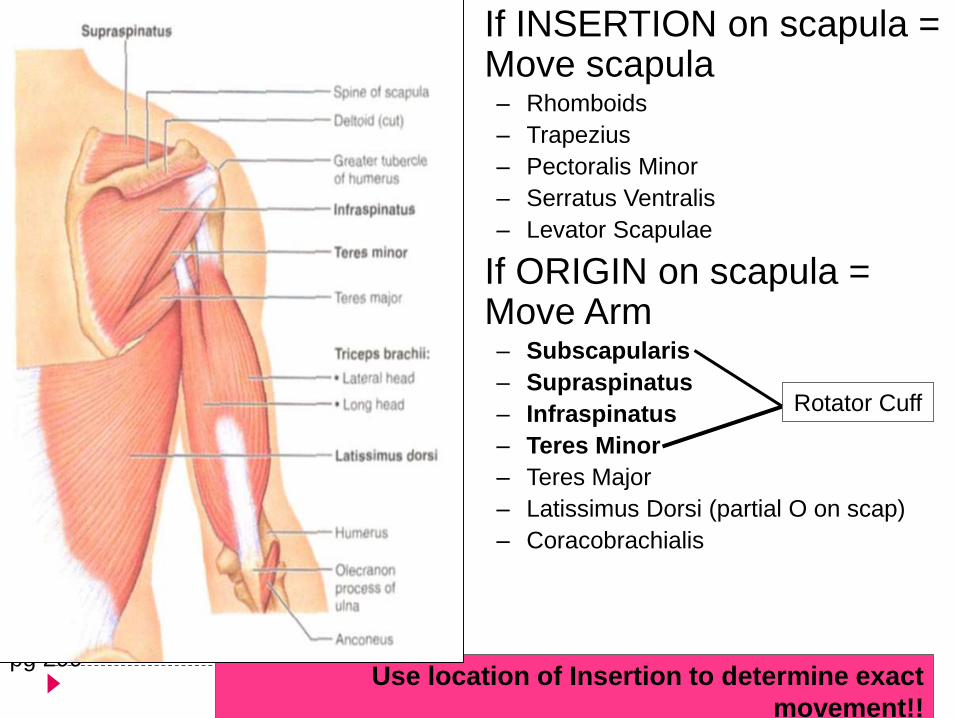
• If INSERTION on scapula = Move scapula– Rhomboids
– Trapezius
– Pectoralis Minor
– Serratus Ventralis
– Levator Scapulae
• If ORIGIN on scapula = Move Arm– Subscapularis
– Supraspinatus
– Infraspinatus
– Teres Minor
– Teres Major
– Latissimus Dorsi (partial O on scap)
– Coracobrachialis
pg 299
Rotator Cuff
Use location of Insertion to determine exact
movement!!

Frolich, Human Anatomy,UpprLimb
Axilla = Armpit
Region between arm and chest
Boundaries
Ventral - pectoral muscles
Dorsal = latissimus dorsi, teres major
subscapularis
Medial = serratus ventralis
Lateral = bicipital groove of humerus
Contents
Axillary lymph nodes, Axillary vessels n Brachial Plexus

Frolich, Human Anatomy,UpprLimb
POSTERIOR AND ANTERIOR COMPARTMENTS
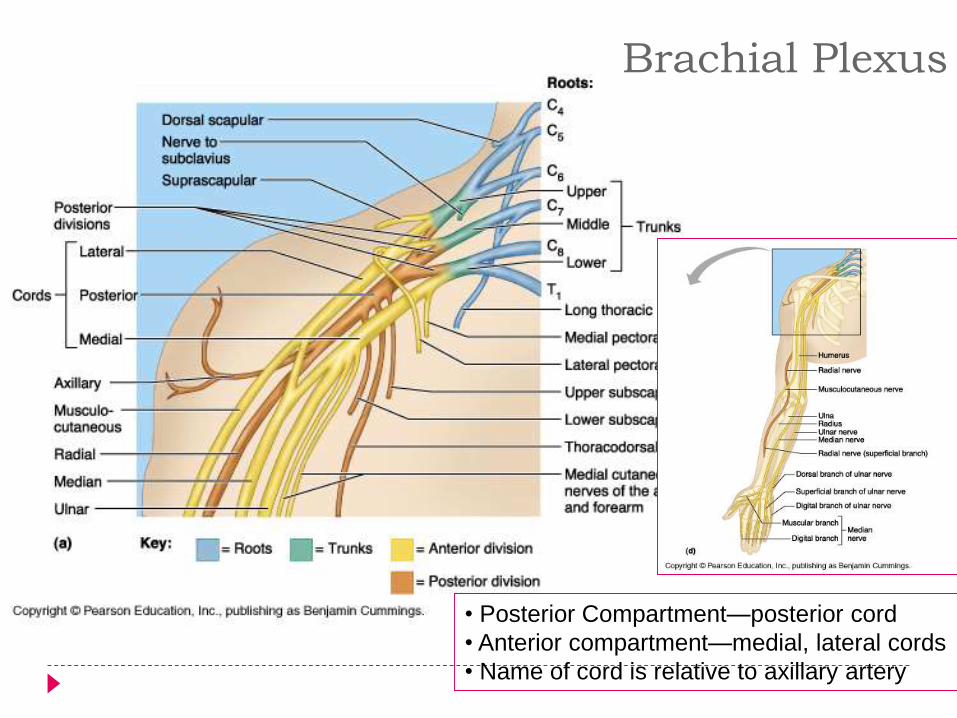
Brachial Plexus
• Posterior Compartment—posterior cord
• Anterior compartment—medial, lateral cords
• Name of cord is relative to axillary artery
Parts of Brachial Plexus
Really Tired? Drink Coffee
Buddy!
R = ROOTS (ventral rami)
T = TRUNKS
D = DIVISIONS
C = CORDS
B = BRANCHES
Frolich, Human Anatomy,UpprLimb
ANTERIOR MUSCLES
M-C
Biceps
brachialis
Median
Forearm flexors
Thumb intrinsics (1M$
nerve)
Ulnar
Flexor carpi ulnaris
Hand intrinsics
POSTERIOR MUSCLES
Muscles (radial nerve)
Triceps
Anconeus
Brachioradialis
Carpal, digit extensors
Frolich, Human Anatomy,UpprLimb
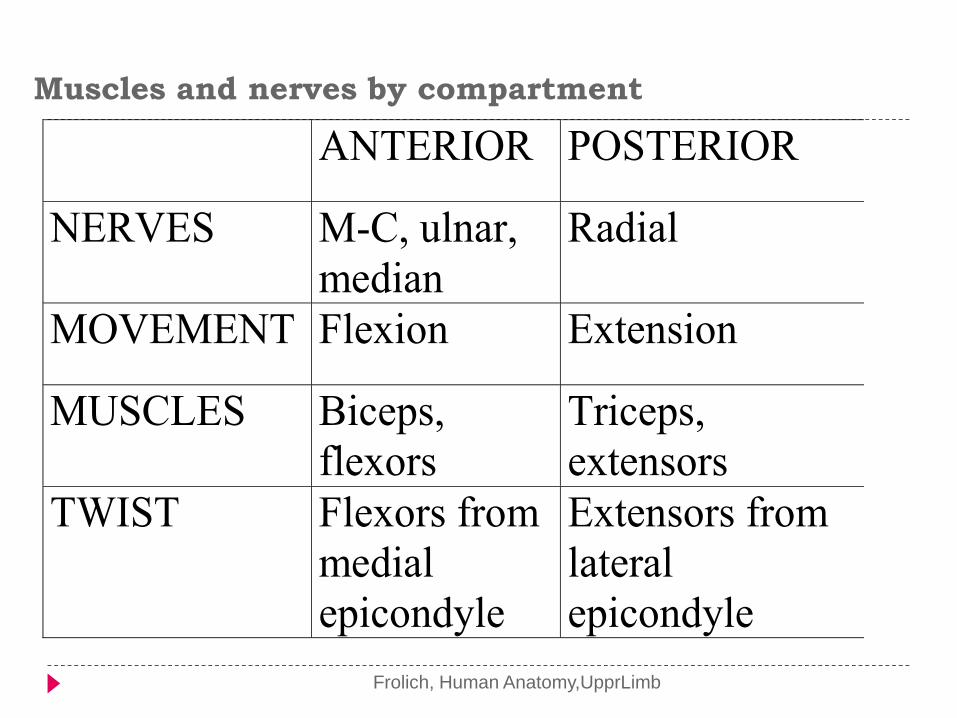
Muscles and nerves by compartment
ANTERIOR POSTERIOR
NERVES M-C, ulnar,
median
Radial
MOVEMENT Flexion Extension
MUSCLES Biceps,
flexors
Triceps,
extensors
TWIST Flexors from
medial
epicondyle
Extensors from
lateral
epicondyle

FOREARM POSTERIOR
known as the extensor muscles.
all innervated by the radial nerve.
muscles divided into deep and superficial
compartments separated by a layer of fascia.
FOREARM POSTERIOR
Superficial muscles
Extensor Carpi Radialis Longus and Brevis,Extensor
Digitorum,Extensor Digiti Minimi and Extensor Carpi
Ulnaris
Deep Muscles
the supinator, abductor pollicis longus, extensor pollicis
brevis, extensor pollicis longus and extensor indicis.
With the exception of the supinator, these muscles act on
the thumb and the index finger
Frolich, Human Anatomy,UpprLimb
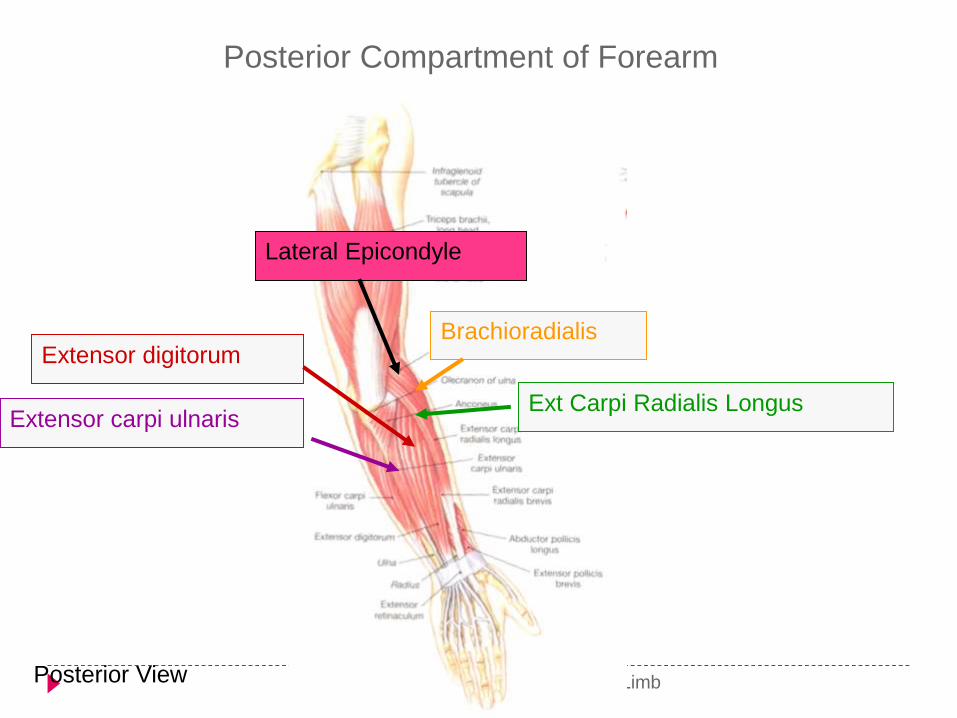
Posterior Compartment of Forearm
Extensor digitorum
Extensor carpi ulnarisExt Carpi Radialis Longus
Brachioradialis
Lateral Epicondyle
Posterior View
FOREARM- ANTERIOR Superficial Compartment
all originate from a common tendon - medial epicondyle of the humerus.
Flexor Carpi Ulnaris
attaches to the pisiform carpal bone., Flexion and adduction at the wrist, innervated by Ulnar nerve.
Palmaris Longus
attaches to the flexor retinaculum of the wrist; Flexion at the wrist; innervated by Median nerve.
Flexor Carpi Radialis
attaches to the base of metacarpals II and III; Flexion and abduction at the wrist; innervation by Median nerve.
Pronator Teres
attaches laterally to the mid-shaft of the radius; Pronation of the forearm, innervation by Median nerve.
FOREARM
Intermediate compartment
flexor digitorum superficialis
splits into four tendons and attach to the middle
phalanges of the four fingers.
Flexes the metacarpophalangeal joints and proximal
interphalangeal joints at the 4 fingers, and flexes at the
wrist.
Innervated by Median nerve.
FOREARM - ANTERIOR
Deep Compartment
Flexor Digitorum Profundus
flex the distal interphalangeal joints of the fingers, flexes
the metacarpophalangeal joints and the wrist.
Innervated by ulnar nerve (medial) and median nerve
(lateral)
Flexor Pollicis Longus
Flexes the interphalangeal joint and metacarpophalangeal
joint of the thumb; innervated by Median Nerve.
Pronator Quadratus
Pronates the forearm; Innervated by Median Nerve.
Frolich, Human Anatomy,UpprLimb
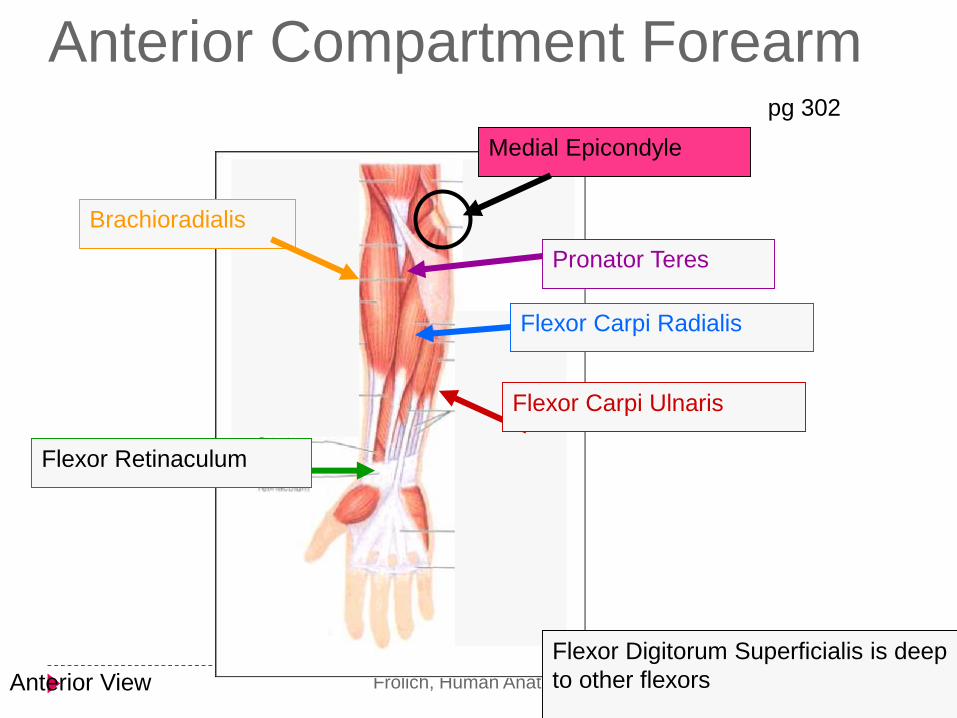
Anterior Compartment Forearm
Flexor Carpi Radialis
Flexor Retinaculum
Medial Epicondyle
Flexor Digitorum Superficialis is deep
to other flexors
pg 302
Flexor Carpi Ulnaris
Brachioradialis
Pronator Teres
Anterior View
Carpal Tunnel
Formed by the carpal bones and overlying flexor
retinaculum (attaches to the pisiform, hook of hamate,
the scaphoid and the trapezium bones).
Structures passing through:
Median nerve
Tendons of flexor digitorum superficialis/profundus
Flexor pollicis longus
Flexor carpi radialis (not in carpal tunnel)

Muscles of the Hand
Thenar muscles : abductor pollicis brevis, flexor pollicis brevis, opponens pollicis
and adductor pollicis.
All act on the thumb
Innervated by the median nerve
Hypothenar Muscles : Abductor digiti minimi, flexor digiti minimi and oppponens digiti
minimi.
Innervated by the ulnar nerve
All act on the small finger
Interosseous muscles: 8 muscles
Flex metacarpophalangeal joints and extension of interphalangeal joints
Adduction and Abduction of fingers, in relation to the middle finger
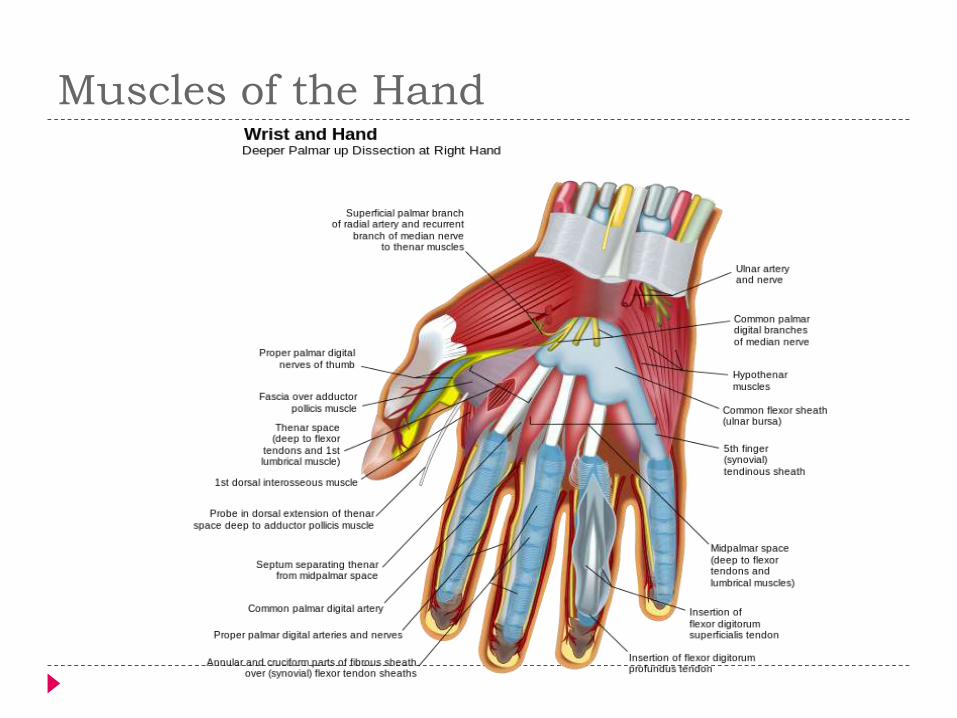
Muscles of the Hand

Frolich, Human Anatomy,UpprLimb
Routes of nerves (in human)
M-C: between biceps brachii and brachialis
Median: medial/posterior to biceps, branches into forearm flexors at elbow then to hand through carpal tunnel Recurrent median (1M$) superficial at wrist to thumb
over thenar emminence) deficit - ape’s hand
Ulnar: medial in arm, posterior to medial epicondle of humerus (funny bone) down medial forearm medial to carpal tunnel into palm
Radial: deep posterior arm around lateral epicondyle of humerus to forearm (deep and superficial branches)
Frolich, Human Anatomy,UpprLimb
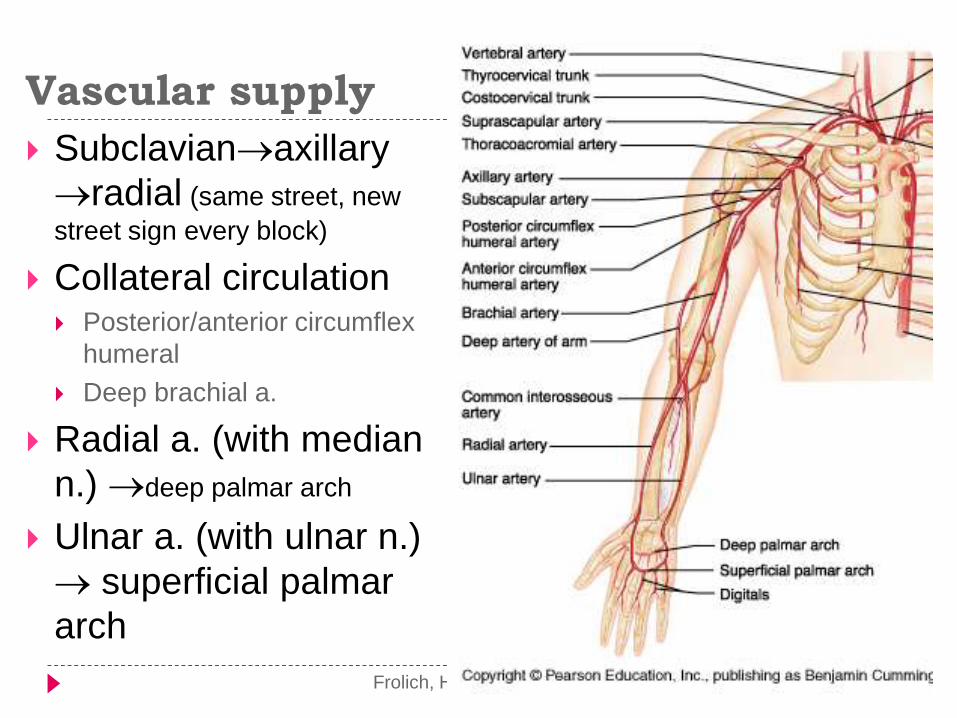
Vascular supply
Subclavianaxillary
radial (same street, new
street sign every block)
Collateral circulation Posterior/anterior circumflex
humeral
Deep brachial a.
Radial a. (with median
n.) deep palmar arch
Ulnar a. (with ulnar n.)
superficial palmar
arch
APPLIED ANATOMY OF UPPER
LIMB
SCAPULAR
articulates with humerus at the glenohumeral joint,
and with clavicle at acromioclavicular joint.
SURGICAL APPLICATION
The long thoracic nerve innervates the serratus anterior,
which originates from ribs 2-8, and attaches the costal
face of the scapula, pulling it against the ribcage. Damage
to this nerve causes winging of the scapular

WINGING SCAPULAR
CLAVICLE
SURGICAL APPLICATION: Fracture of the Clavicle
Common fracture point is the junction of the medial 2/3
and lateral 1/3, due to fall on shoulder or outstretched
hand.
lateral end of the clavicle is displaced inferiorly by the
weight of the arm, and medially, by the pectoralis major.
The medial end is pulled superiorly, by the
sternocleidomastoid muscle.
The suprascapular nerves may be damaged, these
innervate the lateral rotators of the shoulder –
so unopposed medial rotation of the upper limb –
the ‘waiters tip’ position.
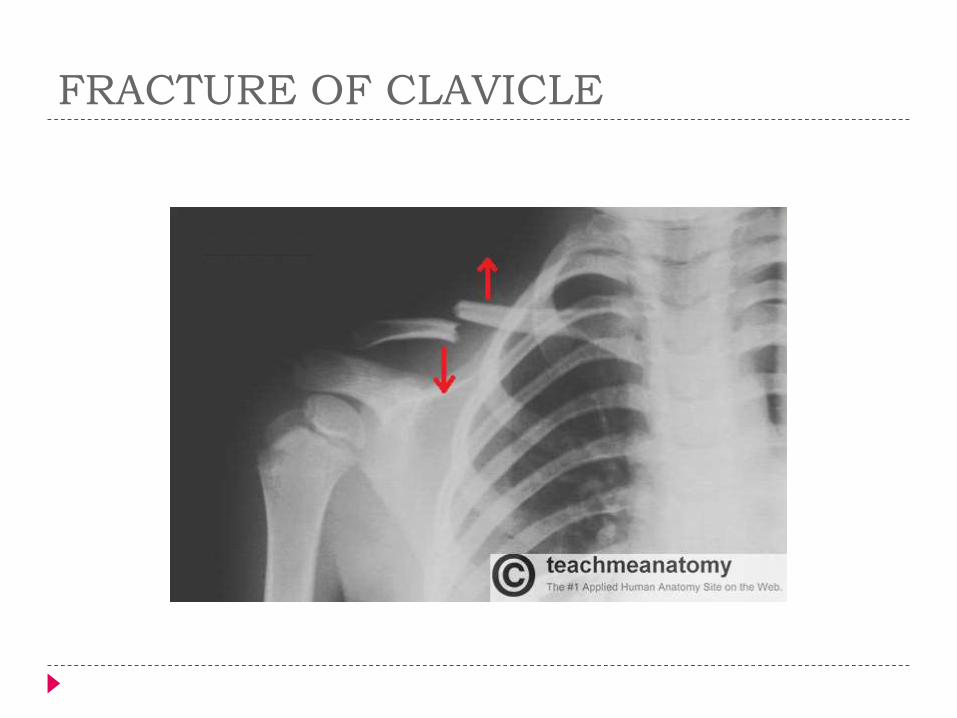
FRACTURE OF CLAVICLE
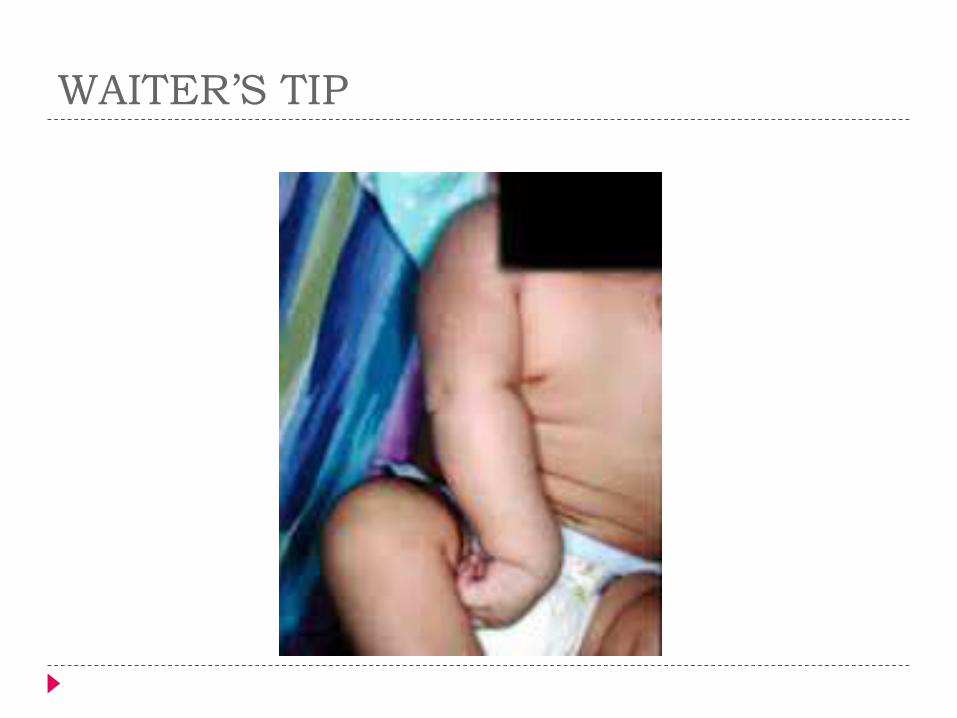
WAITER’S TIP

HUMERUS
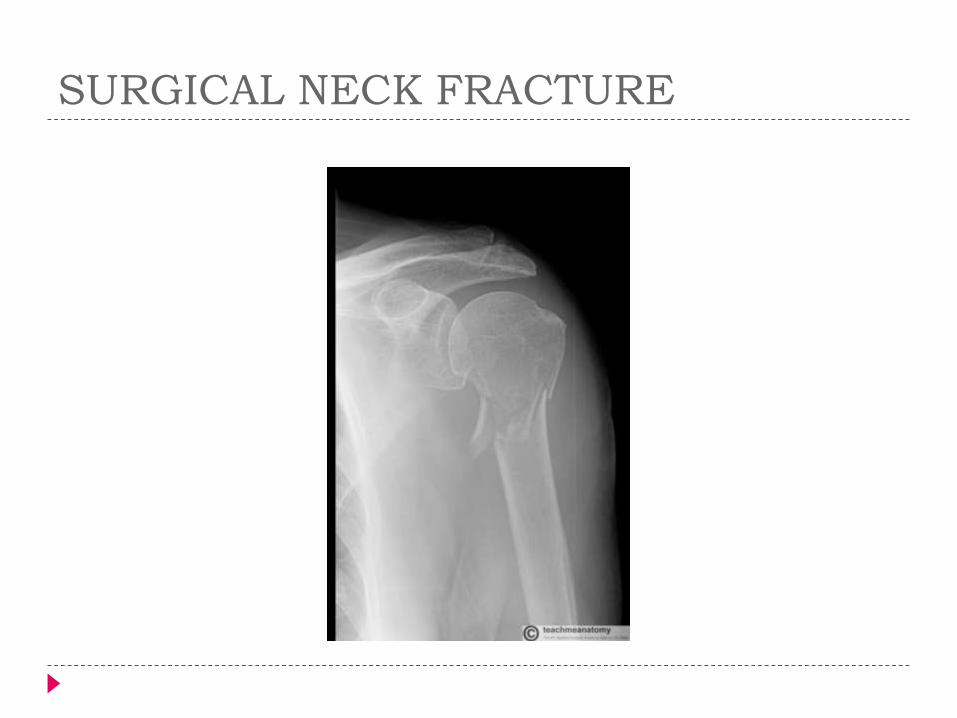
SURGICAL APPLICATION: Surgical Neck Fracture
This is a frequent site of fracture, this occurs by falling on an outstretched hand.
May result in damage to axillary nerve and posterior circumflex artery.
Damage to the axillary nerve will result in paralysis to the deltoid and and teres minor muscles; the patient will not be able to abduct their arm loss of sensation of the skin over the deltoid (regimental badge area).
SURGICAL NECK FRACTURE
HUMERUS
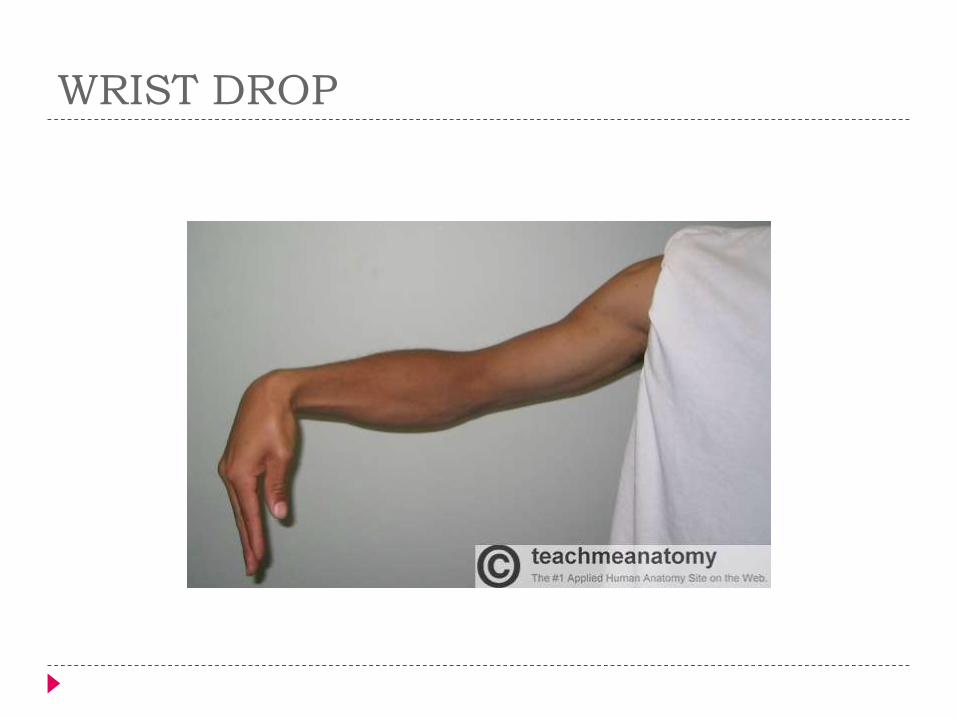
SURGICAL APPLICATION: Mid-shaft Fracture
A mid-shaft fracture could damage the radial
nerve and profunda brachii artery – in radial groove.
The radial nerve innervates the extensors of the
wrist. This results in unopposed flexion of the wrist -
‘wrist drop’.
sensory loss over the dorsal surface of the hand,
and the proximal ends of the lateral 3 and a half
fingers dorsally.
WRIST DROP
HUMERUS
SURGICAL APPLICATION: Distal Humeral Fracture
A supraepicondylar fracture - interference to the blood supply of the forearm from
the brachial artery - Volkmann’s ischaemiccontracture – uncontrolled flexion of the hand, as flexors muscles become fibrotic and short.
damage to the medial, ulnar or radial nerves.
A medial epicondyle fracture could damage the ulnar nerve - ulnar claw is the result.
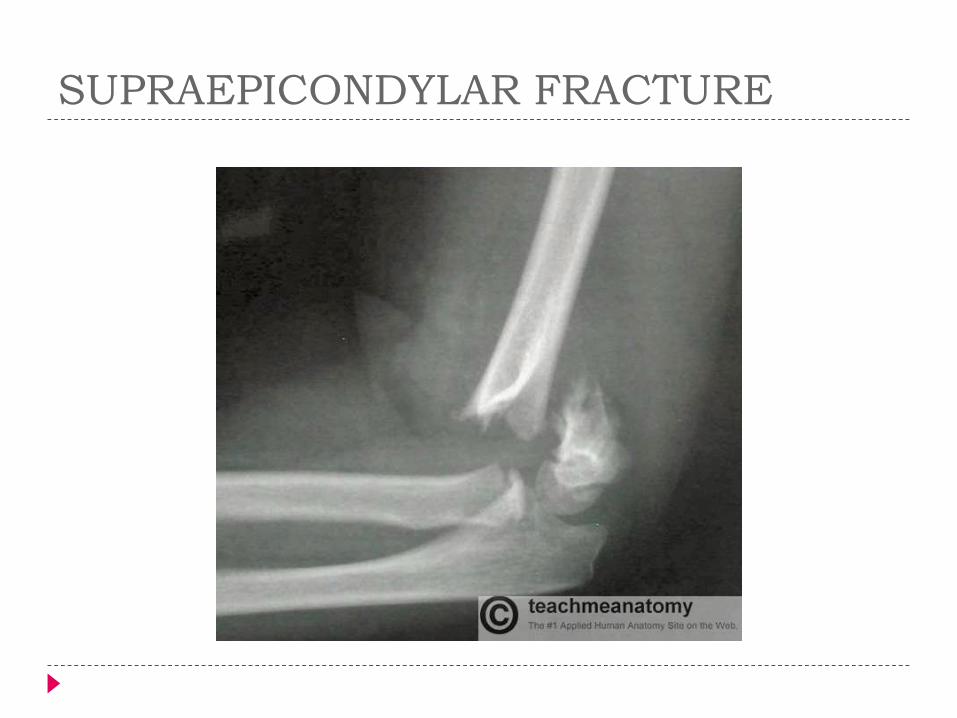
SUPRAEPICONDYLAR FRACTURE
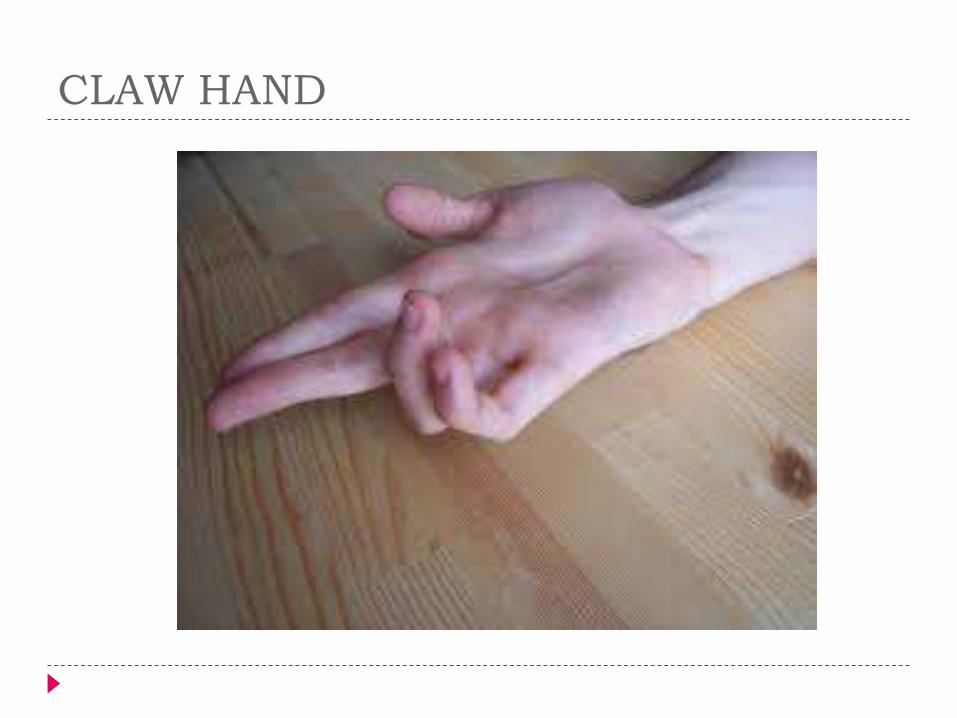
CLAW HAND
SURGICAL APPLICATION – Common
Fractures of the Ulna
The interosseous membrane transmits force from
one bone to the other, thus, fractures of both the
forearm bones are not uncommon.
There are two classical fractures:
Monteggia’s Fracture – The proximal shaft of ulna
is fractured, and the head of the radius dislocates
anteriorly at the elbow.
Galeazzi’s Fracture – A fracture to the distal radius,
with the ulna head dislocating at the distal radio-
ulnar joint.

Monteggia’s Fracture
SURGICAL APPLICATION: Common
Fractures of the Radius
Colles’ Fracture – The most common type of radial
fracture. A fall onto an outstretched hand causing a
fracture of the distal radius, with posterior
displacement of wrist - ‘dinner fork deformity’.
Smith’s Fracture – A fracture caused by falling onto
the back of the hand. It is the opposite of a Colles’
fracture, as the distal fragment is now placed
anteriorly.

COLLE’S FRACTURE

SURGICAL APPLICATION: Fractures of the
Carpal Bones
The two carpal bones that are most commonly
fractured are the scaphoid and lunate.
Scaphoid fracture
tenderness in the anatomical snuffbox
cut off the blood supply to the proximal part of the bone ,
causing avascular necrosis.
lunate fracture
occurs when falling on a outstretched hand
can be associated with some median nerve damage.
CARPAL TUNNEL
Clinical Relevance: Carpal Tunnel Syndrome
Compression of the median nerve
The typical signs of carpal tunnel syndrome are pins
and needles in the sensory distribution of the
median nerve and weakness of thenar muscles.
It can be treated by cutting into the flexor
retinaculum, relieving the pressure.