link.springer.com · web viewqeipap derives from the coping koala treatment manual (barrett, dadds,...
TRANSCRIPT
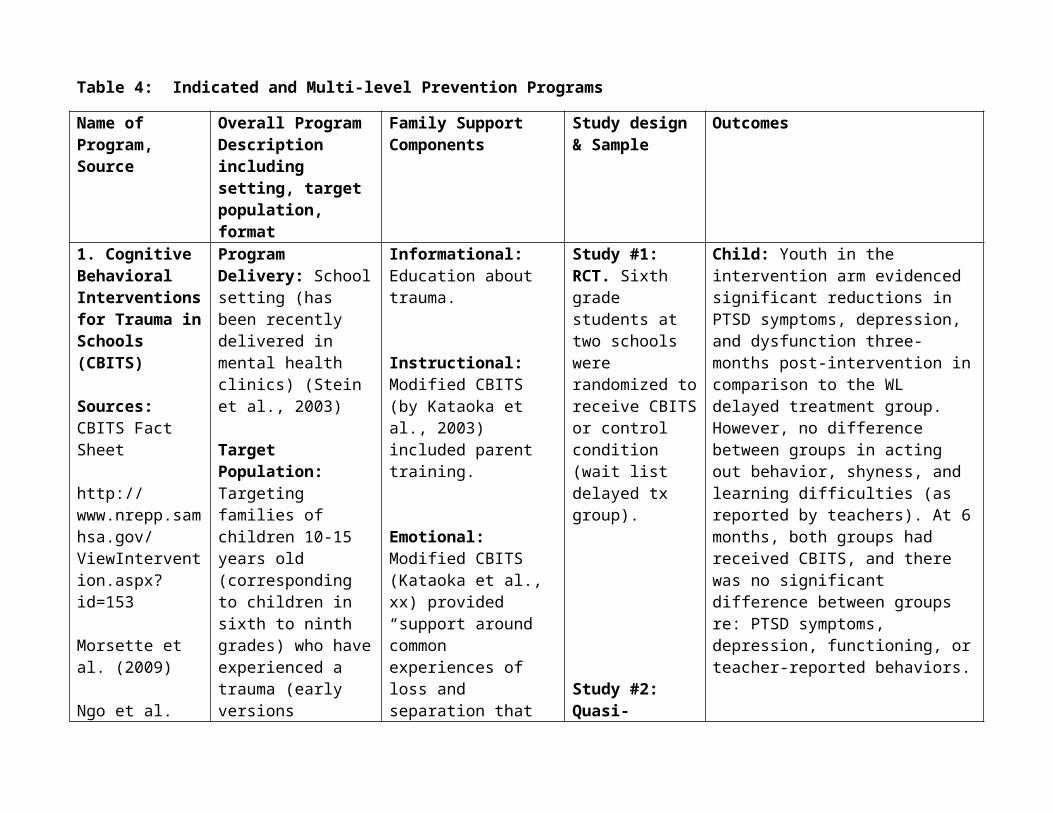
Table 4: Indicated and Multi-level Prevention Programs
Name of Program,Source
Overall Program Descriptionincluding setting, targetpopulation, format
Family SupportComponents
Study design& Sample
Outcomes
1. Cognitive Behavioral Interventions for Trauma in Schools (CBITS)
Sources: CBITS Fact Sheet
http://www.nrepp.samhsa.gov/ViewIntervention.aspx?id=153
Morsette et al. (2009)
Ngo et al. (2008)
Stein et al. (2003)
Study Sources:Study #1: Stein et al. (2003)
Study #2: Kataoka et al. (2003)
Program Delivery: School setting (has been recently delivered in mental health clinics) (Stein et al., 2003)
Target Population: Targeting families of children 10-15 years old (corresponding to children in sixth to ninth grades) who have experienced a trauma (early versions included children as young as eight).
Goals: CBITS aims to alleviate depression, anxiety, and trauma symptoms among youth exposed to a trauma and experiencing symptoms consistent with PTSD.
Program Focus: CBITS teaches children how to reduce
Informational: Education about trauma.
Instructional: Modified CBITS (by Kataoka et al., 2003) included parent training.
Emotional: Modified CBITS (Kataoka et al., xx) provided “support around common experiences of loss and separation that many experienced during the immigration process.
Study #1: RCT. Sixth grade students at two schools were randomized to receive CBITS or control condition (wait list delayed tx group).
Study #2: Quasi-experimental; 198 eighth-grade students assigned to intervention or waitlist (combination of randomized and non-randomized students) Three month follow-up.
Child: Youth in the intervention arm evidenced significant reductions in PTSD symptoms, depression, and dysfunction three-months post-intervention in comparison to the WL delayed treatment group. However, no difference between groups in acting out behavior, shyness, and learning difficulties (as reported by teachers). At 6 months, both groups had received CBITS, and there was no significant difference between groups re: PTSD symptoms, depression, functioning, or teacher-reported behaviors.
Child: Youth in the intervention group exhibited decreased depression and PTSD symptoms compared to the wait list group. Intervention group had lower depression scores at follow-up compared to WL group. Greater decrease in PTSD and depression scores among intervention group youth who evidenced clinically significant levels of PTSD or depression at baseline.

Study #3: Morsette et al. (2009)
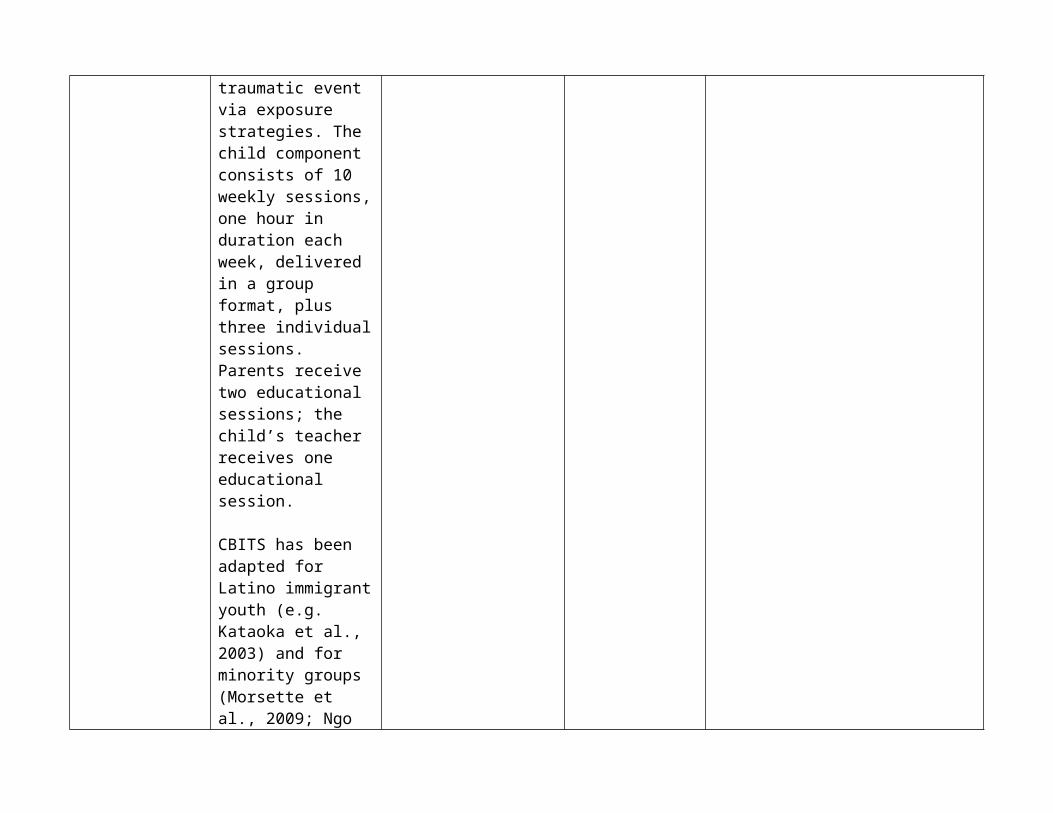
symptoms through skills development (e.g. relaxation, problem solving, managing and processing traumatic event via exposure strategies. The child component consists of 10 weekly sessions, one hour in duration each week, delivered in a group format, plus three individual sessions. Parents receive two educational sessions; the child’s teacher receives one educational session.
CBITS has been adapted for Latino immigrant youth (e.g. Kataoka et al., 2003) and for minority groups (Morsette et al., 2009; Ngo et al., xx).
Delivered by mental health professionals, including school mental health personnel (recommended by developers)
Study #3: Pilot study (pre/post) with American Indian youth. Four out of 48 completed the program.
Child: Three of the four who completed evidenced decreased symptoms of PTSD or depression.
2. Coping Power Program (CPP)
Sources: www.copingpower.com
Lochman & Wells (2002)
Lochman & Wells (2003)
Lochman & Wells (2004)
Lochman et al. (2009)
Study Sources:Study #1: Lochman & Wells (2002)
Study #2: Lochman & Wells (2003)
Study #3: Lochman & Wells (2004)
Program Delivery:School setting; has been adapted for delivery in mental health settings.
Target Population: Targeting children in late elementary or early middle school with aggression/behavioral problems as they move into early adolescence, and their families.
Goals: To decrease the risk of behavioral problems during childhood and over the long term.
Program Focus: Parents and children meet in separate, concurrent groups. Child component lasts two years (meeting once or twice per month, for 40-60 minutes per session); focus on enhancing coping and problem solving skills. Parent component: 16 sessions over 15
Instructional: Parenting techniques (e.g., positive reinforcement, monitoring, supervision, communication skills), stress reduction strategies.
Study #1: RCT. 245 students randomized to CPP, a universal intervention (parent and teacher meetings), CPP + the universal intervention, or a control group.
Study #2: 473 youth in 17 classes who were identified as being the most aggressive were randomized to CPP, CPP + a classroom intervention (parent and teacher meetings), the classroom intervention, or control. One-year follow-up.
Child: All of the intervention groups evidenced lower rates of substance use and improvements in social functioning and self regulation than the control group at posttest. Based on teacher report, children in the CPP + universal component evidenced the greatest gains in problem solving and anger management, and aggressive behavior towards the teacher over time.
Parent: All three interventions were associated with improvements in parenting.
Child: Both the CPP and CPP+ classroom condition evidenced significant decreases in delinquency in comparison to the control group. CPP+ classroom condition was also associated with reduced levels of school aggression at follow-up. Treatment effects spread to other children who did not receive Coping Power but were in the same classrooms as the intervention youth, as these youth evidenced lower rates of substance use.
Child: The CPP group (particularly, the

months.
Delivered by a professional team.
Study #3: RCT: 183 boys randomly assigned to CPP (child only), CPP + parent component, or control. 1 year follow-up.
parent and child CPP) was associated with decreased delinquency and substance use at follow-up in comparison to the control group. Teacher reported behavior also improved during follow-up, which was attributed primarily to the child CPP condition.
3. Early Risers “Skills for Success”
Sources:
https://casat.unr.edu/bestpractices/view.php?program=31
http://www.nrepp.samhsa.gov/ViewIntervention.aspx?id=137
August et al. (2001)
August et al. (2002)
August et al. (2003)
Program Delivery: Setting depends on component: School based child component, school or center- based parent/family CORE component, FLEX family component delivered at home.
Target Population: Targeting families of children six to 12 years of age who are exhibiting behavioral problems.
Goals: To reduce the onset for conduct disorder and associated behavioral problems (e.g. substance abuse).
Program Focus: Early Risers consists of CORE and FLEX components. CORE:
Informational: Child development handouts, information on decreasing parents’ stress, encouraging family interactions.
Instructional: Parenting techniques
Emotional: Provision of emotional support during FLEX meetings as needed re: parents concerns about their family, child’s school and home functioning, etc…
Instrumental: Case management, meal
Advocacy: Family advocate assists parents by helping parents communicate with their child’s school.
Study #1: RCT Ten elementary schools similar demographically were randomly assigned to either the program or a control condition. Children who were high risk from both arms were eligible for inclusion; 124 youth from the control schools, 124 from the experimental schools. Two-year follow-up.
Study #2: RCT. 125 children identified as moderately or highly aggressive were assigned to either the intervention or a
Child: Children in the intervention group evidenced significant improvements in school behaviors and academic achievement in comparison to the control group.
Parent: Examined the mediating role of attendance as it impacted parenting practices.
Child: In comparison to the control group, intervention youth were rated higher on functioning (e.g. leadership, social manners), and were more likely to select peers as friends who were less aggressive. Children in the intervention group also reported greater amount of friendship and leisure activities.

August et al. (2006)
Bloomquist et al. (2009)
Klimes-Dougan et al. (2009)
Lee et al. (2008).
Study Sources:Study #1: August et al. (2001)
Study #2: August et al. (2003)
1) Summer school (two summers, six weeks each summer); 2) Student mentorship program (offered during the school year).; 3) Family Program, in which parents and children are involved in separate sessions over the course of three years (12, two-hour sessions in year one, 11 sessions in year two, six sessions in year three). Occurs biweekly. Start with a meal, then separate sessions, after which parents and children come together for an activity. During the first two years, the parent component derives from The Incredible Years (e.g., Webster-Stratton et al., 2004). The second family component is FLEX, which is an individually-tailored program based upon the specific needs of the family. May include referrals for domestic violence, assistance
control group. Data from 1,364 classmates were also collected.
4 year follow-up.
August et al. (2006) re: sustaining Early Risers. Bloomquist et al (2008) re: transporting Early Risers to a community setting, data re: costs and implementation. Bloomquist et al. (2009) re: parent participation. Klimes et al. (2009) re: practitioner and site characteristics as they pertain to intervention fidelity. Lee et al. (2008) re: fidelity.

meeting tangible needs.
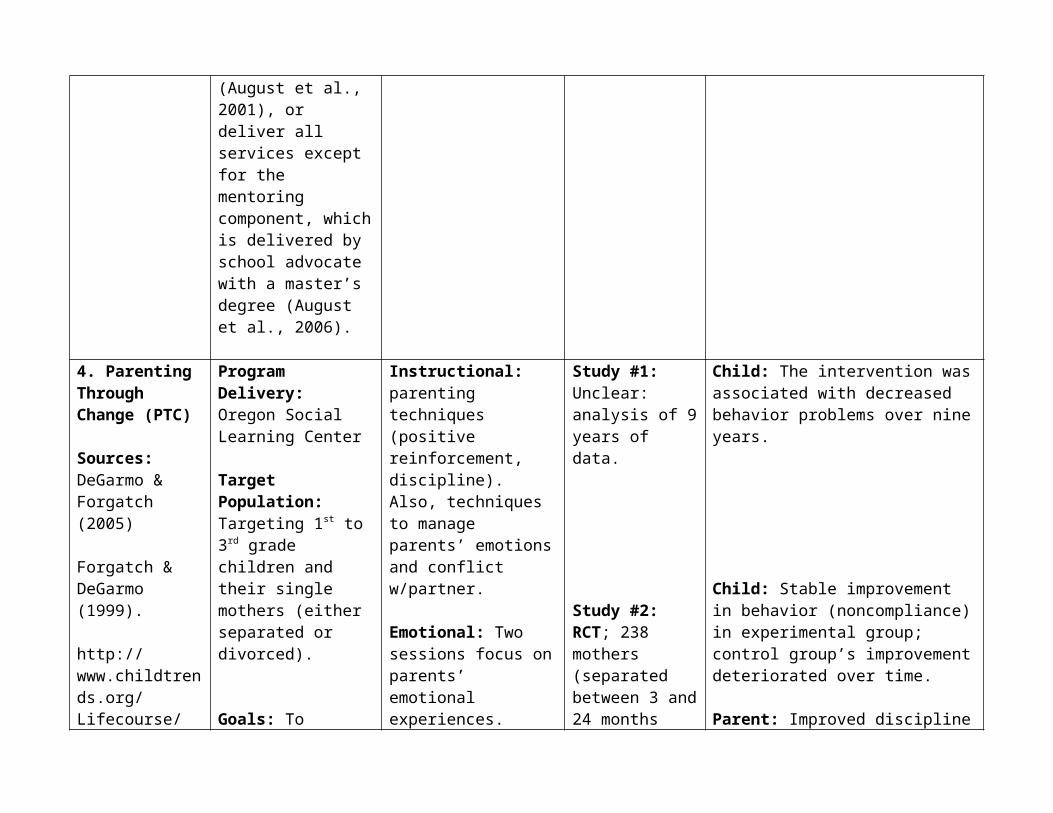
Delivered by a team: the family peer advocate may coordinate both child and family components, deliver the FLEX family intervention (August et al., 2001), or deliver all services except for the mentoring component, which is delivered by school advocate with a master’s degree (August et al., 2006).
4. Parenting Through Change (PTC)
Sources: DeGarmo & Forgatch (2005)
Forgatch & DeGarmo (1999).
http://www.childtrends.org/Lifecourse/programs/ptc.htm
http://
Program Delivery: Oregon Social Learning Center
Target Population: Targeting 1st to 3rd grade children and their single mothers (either separated or divorced).
Goals: To prevent behavioral and emotional problems and encourage healthy development through the provision of
Instructional: parenting techniques (positive reinforcement, discipline). Also, techniques to manage parents’ emotions and conflict w/partner.
Emotional: Two sessions focus on parents’ emotional experiences.
Instrumental: Under program costs, NREPP cites transportation, meals, child care.
Study #1: Unclear: analysis of 9 years of data.
Study #2: RCT; 238 mothers (separated between 3 and 24 months prior) and their sons. Random assignment: 2/3rds received the
Child: The intervention was associated with decreased behavior problems over nine years.
Child: Stable improvement in behavior (noncompliance) in experimental group; control group’s improvement deteriorated over time.
Parent: Improved discipline and positive parenting strategies evidenced in the treatment group over time in contrast

www.nrepp.samhsa.gov/ViewIntervention.aspx?id=67
Study Sources:Study #1: Forgatch & DeGarmo (1999)
Study #2: Martinez & Fogatch (2001)
Study #3: DeGarmo & Forgatch (2005)
parenting skills. Program Focus: PTC derives from the Parent Management Training-Oregon Model (PMT-O) (Patterson et al., 2004); provides parenting skills to single mothers who are recently separated or divorced.
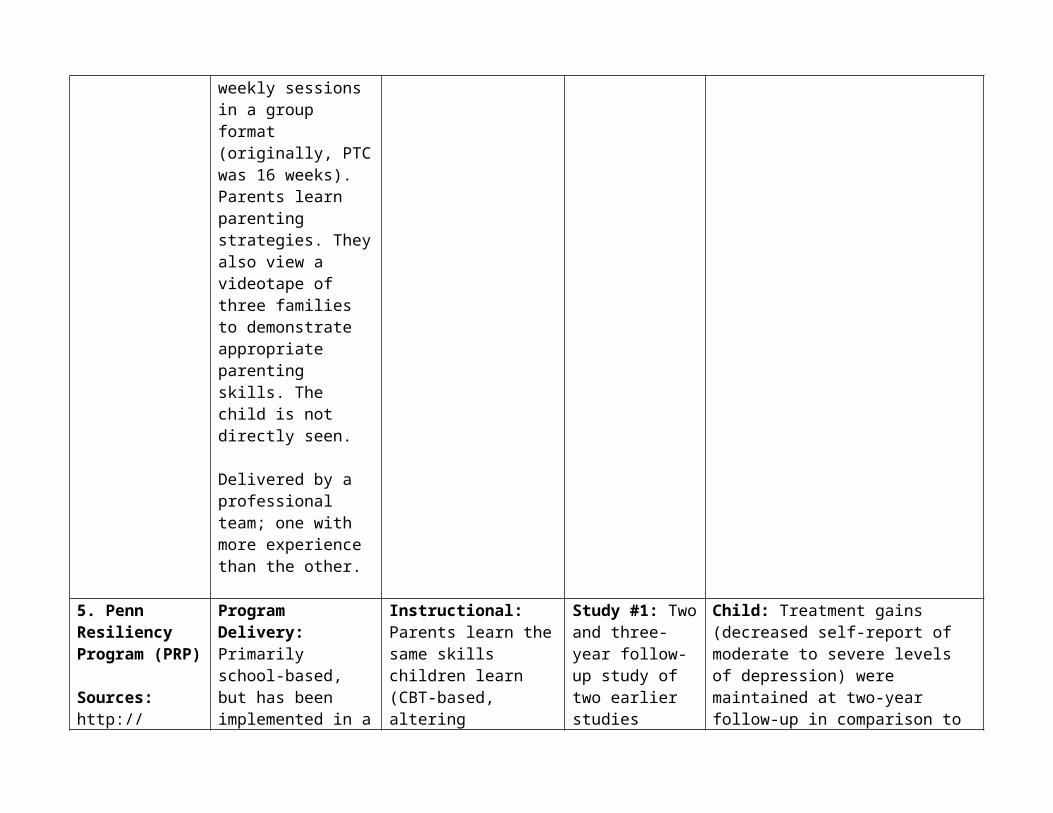
The program consists of 14 weekly sessions in a group format (originally, PTC was 16 weeks). Parents learn parenting strategies. They also view a videotape of three families to demonstrate appropriate parenting skills. The child is not directly seen.
Delivered by a professional team; one with more experience than the other.
intervention, the remaining 1/3rd was assigned to the control group (no treatment). Followed up to 36 months post-baseline.
Study #3: Same as #2.
to the control group, which declined over time.
Child: Youth in the intervention group had significant decreases in behavior problems and affiliation with deviant peers over the control group.
5. Penn Resiliency Program (PRP)
Sources:
Program Delivery: Primarily school-based, but has been implemented in a
Instructional: Parents learn the same skills children learn (CBT-based, altering emotions,
Study #1: Two and three-year follow-up study of two earlier studies
Child: Treatment gains (decreased self-report of moderate to severe levels of depression) were maintained at two-year follow-up in comparison to the control

http://www.ppc.sas.upenn.edu/prpsum.htm
Roberts et al. (2004)
Gillham et al. (2006)
Gillham et al. (2007)
Study Sources:
Study #1: Roberts et al. (2004)
Study #2: Gillham et al. (2006)
Study #3: Gillham et al. (2007)
variety of settings, including primary care (Gillham et al., 2006),
Target Population: Targeting children with depressive symptoms between 10 and 14 years of age (corresponding to the 6th
to 8th grades) and their families.
Goals: To prevent adolescent depression.
Program Focus: PRP derives from cognitive-behavioral theory and problem solving skills. The parent component consists of six group sessions, 90 minutes in duration. Child component delivered after school; 12 90-minute weekly sessions. Delivered by a range of professionals based on setting (e.g. teachers, counselors, graduate psychology and education students).
cognitive restructuring, problem solving).
(Gillham & Reivich, 1999; Gillham et al., 1995)-in the first study, the sample consisted of 341 youth between 11 and 13 years of age from 18 schools located in Australia. The second sample consisted of 404 students between 11-13 years of age from another 18 schools.
Study #2: RCT 211 11 and 12 year old children randomly assigned to PRP or usual services (primary care). Two-year follow-up.
Study #3: RCT. 693 youth from three schools assigned to PRP, the Penn
group, but no significant difference between groups at three years. The intervention group made fewer explanations regarding negative events comparative to the control group at both follow-up points, although no significant differences between groups at either follow-up periods.
Child: PRP was associated with improvements in explanatory style for positive events over time; no association between PRP and depression, depressive or anxiety disorders across the sample as a whole. However, PRP reduced onset of depression, anxiety, and adjustment disorders individuals with elevated symptoms. Child: PRP significantly decreased depressive symptoms among youth in two schools in comparison to PEP and the control group. The PRP group in the third school did not evidence reduced

Enhancement Program (PEP), or a control group.Three year follow-up.
symptoms of depression.
6. Queensland Early Intervention and Prevention Anxiety Project (QEIPAP)
Sources: Dadds et al. (1997)
Dadds et al. (1999)
Study Sources:Study #1: Dadds et al. (1997)
Study #2: Dadds et al. (1999)
Program Delivery: School setting.
Target Population: Targeting children between 7 and 14 years of age with anxiety symptoms and their families.
Goals: To decrease anxiety symptoms or the onset of an anxiety disorder.
Program Focus: QEIPAP derives from the Coping Koala Treatment Manual (Barrett, Dadds, & Rapee, 1991), a treatment for anxiety disorders.
Children and parents are seen concurrently; program for youth is 10 sessions; parent component is three weeks (corresponding
Instructional: Parents learn the same skills that are being taught to their children to decrease their own anxiety and model for their child
Study #1: RCT: 128 children from eight schools in Australia were assigned to QEIPAP or a comparison group (monitoring) based upon the random assignment of hteir school.Six month follow-up.
Study #2: Same study as above-longer-term follow-up (12 and 24 months)
Child: Both groups evidenced improvements at post re onset of new and existing anxiety disorders; intervention group evidenced a maintenance in treatment gains.
Child: Both groups were similar in prevalence of anxiety disorders and reduced incidence of new disorders; however, at 24 months posttest, the intervention group was superior to the control condition.
with the child’s third, sixth, and ninth session).
Delivered by mental health professionals (clinical psychologists).
MULTI LEVEL1. Adolescent Transition Program (ATP)
Sources:http://www.uoregon.edu/~cfc/atp.htm
http://www.whatcomcounts.org/whatcom/modules.php?op=modload&name=PromisePractice&file=promisePractice&pid=865
http://test.scripts.psu.edu/dept/prevention/ATP.htm
Connell et al. (2008)
Dishion et al.
Program Delivery: School setting, although home visits are provided to encourage participation.
Target Population: Targeting youth in middle school and their families.
Goals: To prevent behavior problems by targeting parent factors.
Program Focus: ATP indicated components (Each level builds on the previous one).
Universal: A Family Resource Center that provides information about parenting and factors that increase problem behaviors,
Informational: Information about risk factors associated with substance use and problem behaviors; information about parenting (universal level). Information also provided during selective level regarding parenting practices and how to alter behavior.
Instructional: Parenting skills (including monitoring behavior, limit setting, problem solving, communication and listening skills). (indicated level, e.g. the parenting group).
Instrumental: Case management services (indicated level).
Study #1: RCT: (all three components): subsample of 106 sixth grade youth from a larger prevention study (RCT) who were assessed as high risk for behavioral or emotional problems and randomly assigned to either ATP or control. Youth assessed during the 7th, 8th, and 9th grades.
Study #2: RCT: (Family Resource Room-part of a larger evaluation). RCT of 999 families to the intervention or control group.
Child: The family component was associated with decreased levels of depressive symptoms among youth identified as high-risk during the three assessment periods in comparison to high-risk control group youth.
Child: In comparison to the control group, intervention youth evidenced reduced antisocial behavior, substance use, and fewer deviant peers.

(2000)
Stormshack et al. (2005)
Study Sources:
Study #1: Connell et al. (2008)
Study #2: Dishion et al. (2000)
Study #3: Stormshack et al. (2005)
including substance use.
Selective: The Family Check-up (three sessions), which provides a family assessment to identify youth risk factors.
Indicated: The Parent Focus curriculum, which provides needed services as indicated by the assessment (e.g. case management, parenting sessions, family therapy).
Youth are also offered a six week program called SHAPe (Success, Health, and Peace Curriculum).
Delivered by professionals, called parent consultants who have a master’s degree or a doctorate.
Study #3: 789 youth in sixth grade across four schools. Data collected over three years. (Family Resource Center universal component only)
Child: The Family Resource Center was associated with significant reductions in behavioral problems over time.
2. Early Alliance
Sources:
Program Delivery: School setting for youth; home setting for
Informational: Education re: parenting.
No direct outcomes reported. Prinz et al. (2001) studied recruiting and retaining participants; Dumas et al. (2001)
Dumas et al. (1999)
Dumas et al. (2001)
Prinz et al. (2000)
Smith et al. (2001)
families.
Target Population: Targeting families of children residing in low income communities who are evidencing early-onset behavior problems. The intervention aims to intervene before the first grade.
Goals: To decrease academic failure, substance use, and conduct problems.
Program Focus: Universal and indicated prevention program.
One universal component: a) a weekly classroom component to encourage appropriate behavior through attention and positive reinforcement) (e.g., children participate in the Good Communication Game; parents participate in the Good News Note
Instructional: Parenting skills, Coping skills
Emotional: Last 20 minutes of family sessions are spent in supportive discussions with parent.
Advocacy: Assists parents to advocate for their child (e.g. at school), facilitates access to advocacy services for the child or family (e.g. legal aid).
provides preliminary results on content and process fidelity.

system, in which teachers send notes home praising positive behavior); Three indicated components: b) peer intervention (lasting one year), in a small group format to improve the quality of peer relationships; c) a reading-mentoring program that meets at the child’s school twice a week for 3 ½ hours to improve academic achievement. d) Family component: individually tailored, hourly meetings in which the first 40 minutes are dedicated to parenting techniques, and the last 20 minutes are supportive communication between the parent and a professional Family Consultant. Crisis sessions are also available.
Delivered by professionals (e.g. the classroom component is delivered by teachers,

Family Consultants provide the family-based component).
3. Fast Track
Sources: http://www.childtrends.org/Lifecourse/programs/FastTrackPrevention.htm
http://actagainstviolence.apa.org/specialtopics/fasttrack.html
Conduct Problems Prev Research Group (2007)
Nix et al. (2005)
Orrell-Valente et al. (1999)
Study Sources: Study #1: Conduct Problems Prev Research Group (2007)
Program Delivery: School and home-based
Target Population: Targeting high-risk children in the first to sixth grades and their families.
Goals: To decrease the onset of antisocial behavior through parent factors (e.g. parenting skills, the parent/school relationship) and enhancing youth capabilities.
Program Focus: Developed by the Conduct Problems Prevention Research Group, Fast Track is a multi-component prevention program for children at risk of conduct problems.
Universal, selective, and indicated prevention program.
Informational: Teachers occasionally join parent meetings to provide information about the child component and how parents can implement strategies.
Instructional: Parenting skills, communication and problem-solving.
Emotional: (for high risk families); during the home visits, parents discuss personal or other issues that might potentially interfere with supporting the child.
Instrumental: Transportation, food, childcare for siblings.
Advocacy: (high-risk families) Assist caregivers in being advocates for their child and family.
Study #1: RCTSample: 891 youth from high-risk schools (based upon poverty, neighborhood crime) in four areas were randomly assigned to Fast Track or a control group. Ten year intervention.
Child: No significant impact of the intervention upon conduct and oppositional defiant disorder and attention-deficit hyperactivity disorder), although significant interactions were found between the initial level of risk and the intervention (youth at highest risk who were assigned to the intervention group evidenced significant reductions in diagnoses and behavioral symptoms.
Additionally, Orrell-Valente et al. (1999) studied influences on parents’ participation in Fast Track; Nix et al. (2005) assessed the association between risk factors and participation. Bierman et al. (2006) studied the examination between clinical judgment (for home visits) and validity.

Consists of a universal classroom component.For high-risk youth, services include tutoring three times each week for two years, social skills groups to build skills (e.g. communication and problem solving skills) between two and three times a week for ½ hour per meeting, and a mentoring program.
High-risk families of children in the 1st through 3rd grade are eligible for group meetings, which meet between 5 to 22 times per year; parent-child sharing sessions after the family group meetings (30 minutes in length), and biweekly home visits to discuss any personal or other issues that could potentially interfere with the family’s progress.

Team-led: Teachers and former teachers (educational coordinators) deliver the classroom component; trained peers deliver the peer group intervention. Parent group component delivered by professionals (e.g. counselors, social workers)
Group format, individual, in home sessions.
4. Incredible Years
Sources:www.incredibleyears.com http://www.incredibleyears.com/program/Incredible-Years_factsheet.pdf
Study Sources: Study #1: Webster Stratton et
Program Delivery: Delivered across settings (e.g. schools, Head Start, daycares).
Target Population: Targeting families of children from birth to 12 years of age. The BASIC program focuses on children 3-6 and 6-12. The ADVANCED series focuses on children 6-12 whose parents who have interpersonal
Instructional: Parenting skills (e.g. positive reinforcement, discipline, setting limits) (BASIC Program). Communication, problem-solving, stress, anger reduction skills (ADVANCED series).
Instrumental: Food, childcare, transportation provided
Study #1: RCT
Sample: 78 families with children between three and eight years of age were randomly assigned to BASIC vs. Advance Parent Training.
Study #2: Review
Child: Both groups showed significant improvements at short term follow up on child adjustment, child knowledge of social skills. Advance Training showed added improvements in increased knowledge of prosocial solutions.
Parent: Both groups showed significant improvements at short term follow up on parent distress and communication and problem solving between parents. 1) Communication and problems solving skills; 2) Better consumer satisfaction.
Child/Parent: A synthesis of these studies shows they are effective for decreasing behavior problems and

al. (2004)
Study #2: Findings from www.incredibleyers.com
difficulties.
Goals: To prevent and prevent the exacerbation of emotional and behavioral problems among youth.
Program Focus: This selective/indicated prevention program consists of the BASIC and ADVANCED series. There are two BASIC parenting series: a) Preschool/Early Childhood (ages 3-6) and b) School-age (6-12). The BASIC Series for preschool children is delivered in a group format and focuses on building parenting skills. Child’s component includes skill development (e.g. social skills, preparing youth for school). The ADVANCED series training builds on the BASIC parenting program by focusing on
of studies to date, multiple RCTs.
improving functioning, and enhancing parenting skills. 80% of children who participate in Incredible Years evidence improved behavior.

the parent’s own interpersonal issues. This program can be delivered in nine to 11 weekly two-hour group sessions.
Used as a selective and indicated prevention program based upon population (e.g. children at risk because living in poverty, children evidencing behavioral problems).
Delivered by professionals.
5. Triple P Positive Parenting Program
Sources:http://www.triplep-america.com/documents/Effectiveness%20of%20the%20Triple%20P%20Positive%20Parenting%20Program%20on%20behavioural.pdf
Program Delivery: Delivered in multiple settings.
Target Population: Targeting families of children between 0 and 12 years of age who are at risk or evidencing behavioral problems. Additional program offered for families of adolescents between 13-16.
Goals: To decrease risk of emotional and behavioral problems
Informational: Information about parenting resources (Level 1), handouts about how to manage child behaviors (Level 2).
Instructional: Parenting strategies (Levels 2, 3, 4, 5). Parenting strategies (Levels 2-5). Also, Level 5 offers a Coping Skills Module: Identify and modify dysfunctional cognitions, coping skills (i.e. relaxation techniques) self-statements, and a Partner
Study #1: RCTSample: 305 preschool-aged youth and their caregivers were randomly assigned to either Enhanced (Level 5), Standard (Level 4), Self-Directed Triple P (Level 4) or WLC.
1 year follow-up
Child: Youth of caregivers receiving Enhanced and Standard Triple P evidenced greater decreases in disruptive behaviors compared to Self-Directed and WLC youth.
Youth receiving Enhanced Triple P evidenced the greatest gains at post. At one-year follow-up, all three experimental groups evidenced similar treatment gains (via observation), but the Enhanced and Standard Triple P groups reported greater improvements in the child’s behavior as reported by parent.
Parent: Caregivers receiving Enhanced and Standard Triple P evidenced greater gains in parenting, parenting
www.triplep.net
http://www.nrepp.samhsa.gov/ViewIntervention.aspx?id=1
Study Sources:Study #1:Sanders et al. (2000)
Study #2: Sanders et al. (2007)
Study #3: Prinz et al. (2009)
among children through parent skill building and knowledge.
Program Focus: Triple P is a multi-level prevention program (universal, selective, indicated).
Universal: Corresponds to level 1. Use of media, such as television and newspapers, to raise community understanding about positive parenting.
Selective: Level 2: Provision of parenting advice and information via handouts and videotapes to manage ordinary child behaviors and mild behavior issues. Provided in one or two meetings, 20 minutes in duration.
Indicated: Level 3 is designed for youth with a range of behavioral problems. Delivered in four sessions, 20
Support Module: Communication and listening skills, develop strategies to support partners, problem-solving skills.
Study #2: RCTSample: 139 families randomized to either Enhanced, Standard, or Self-Directed Triple P, or WLC.Pre/post/1 and 3 year follow-up.
Study #3: RCTSample: 18 counties randomly assigned to Triple P (Levels 1-5) or services as usual.
competence, and satisfaction in comparison to Self-Directed and WLC conditions.
Child: No significant difference between treatment conditions regarding the number of youth who met diagnostic criteria; all three groups evidenced significant decreases in youth meeting diagnostic criteria at one and three year follow-up in comparison to pre-test. Also examined pre-intervention predictors of three-year outcomes.
Child: Large effect sizes associated with the intervention for three outcomes: child maltreatment, injuries due to child maltreatment, and placements out of home.

minutes per session.
Level 4 (Standard Triple P, Group Triple P, Self-directed), for youth with severe behavioral problems, delivered in either 10 individual or eight group sessions, 10 hours total. Level 5 (Enhanced Triple P) for children with behavioral problems whose families have stressors (e.g. parental depression). Between 13 to 15 sessions (three to five sessions added onto Standard Triple P). Delivered by professionals (e.g. teachers, mental health providers, physicians, counselors).
6. Raising Healthy Children (RHC)
Sources:http://
Program Delivery: School setting (component of parent program delivered in home)
Informational: Workshops on raising children; helping child succeed in school, and encouraging abstinence from drugs. Newsletters
Study #1: RCT; 938 first and second graders were randomly assigned to RHC or control group.
Child: Children in the RHC group evidenced significantly better school-related outcomes (academics, investment in school), decreases in problem behaviors and improved social functioning comparative to the control

www.colorado.edu/cspv/publications/factsheets/blueprints/FS-BPP20.pdf
Catalano et al. (2003)
Haggerty et al. (2002)
Study Sources:
Study #1: Catalano et al. (2003)
Study #2: Brown et al. (2005)
Target Population: Targeting families of children in grades 1-12 (children recruited in the 1st and 2nd grades).
Goals: To encourage child development, reduce behavioral problemst, and decrease risk of long-term behavior and mental health difficulties and school failure.
Program Focus: Derives from the Seattle Social Development Project; offers universal and selective preventive components.
For parents: Universal workshops on parenting, how to raise healthy children, helping child succeed in school and remain free from drugs.
Child curriculum content varies based on age group (K-2nd grade,
are also sent to families to support learned content (part of the universal component).
Instructional: parenting strategies.
Reassessed 18 months post-intervention.
Study #2: 959 first and second graders were assigned to RHC or a control condition. Reassessed during the 6th to 10th grades.
group (teacher report). Parent report found youth in the RHC group evidenced more favorable school-related outcomes.
Child: Reduced alcohol use among youth in intervention group between the 8th and 10th grades comparative to the control group; no significant growth rates between groups regarding marijuana or cigarette use. Additionally, Haggerty et al. (2002) examine predictors of parent attendance, and Haggerty et al. (2006) investigates outcomes the impact of the program upon teen driving.

3rd grade, or 4th-6th grade). Parents who are determined to need additional support are provided with 12 home-based visits, which focus on parenting skills. Additionally, six booster sessions offered in the home to manage child’s entry into high school, issues around teen driving, etc…
For students: Tutoring, study clubs (for youth in the 4th to 6th grades), individual sessions and group workshops during middle and high school.
For teachers: Workshops and individual meetings re: classroom management.
Professionally delivered by school-home coordinators (teachers, professionals who have prior experience working with families).
