“l’insufficienza respiratoria acuta dal territorio … mondo scientifico/28-09-10/la psv...
TRANSCRIPT
Presidio Ospedaliero dei PellegriniU. O. Accettazione Medico-Chirurgica Responsabile: Dr. Vittorio Helzel
Dr. Ivan Curcio
“l’INSUFFICIENZA RESPIRATORIA ACUTA DAL TERRITORIOALLA MEDICINA D’URGENZA”
28 Settembre 2010Nola (NA)
La PSV nella BPCO
Noninvasive Ventilation : 3491 referencesAND Emergency : 196 references
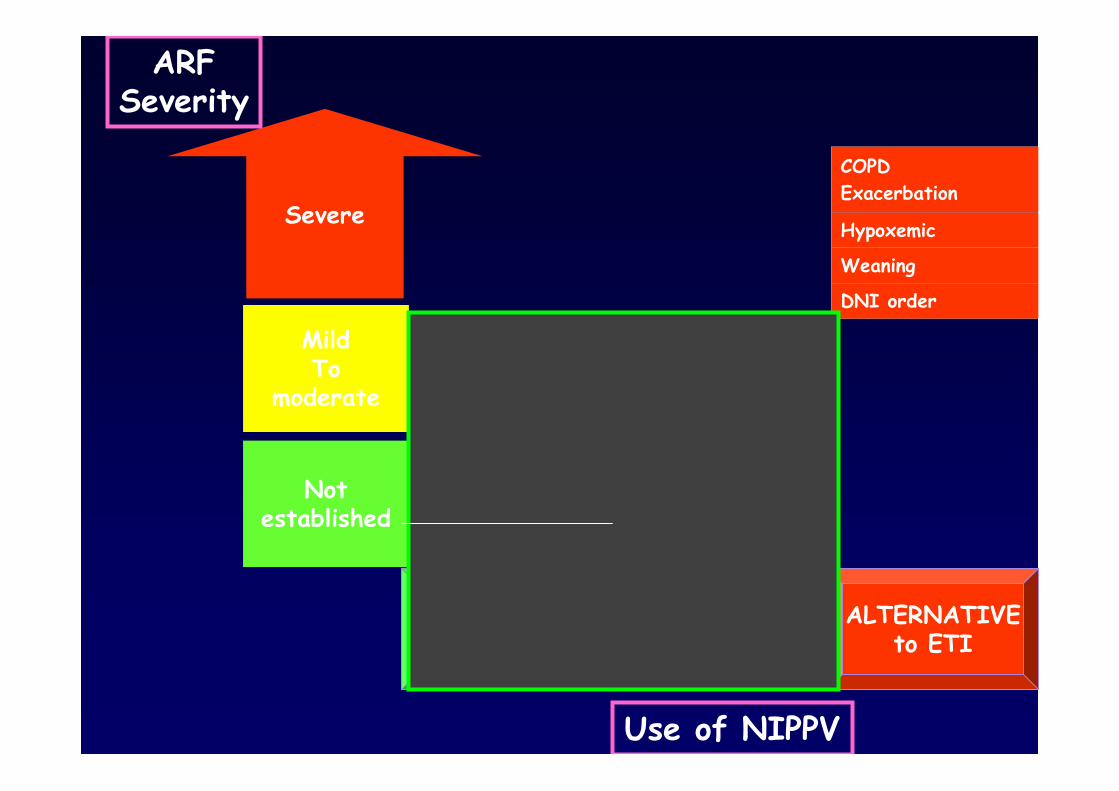
Severe
MildTo
moderate
Notestablished
COPDexacerbation
Post-extubation
hypoxemic
COPDexacerbation
Hypoxemic
Post-extubation
COPDExacerbation
Hypoxemic
Weaning
DNI order
Use of NIPPV
ARFSeverity
TO PREVENT TO AVOIDETI
ALTERNATIVEto ETI
Prevention of ETI in COPD patients
This is acttually the MAJOR indication for NIV andshould be considered the FIRST LINE TREATMENTfor those patients with a pH<7,35>7,30
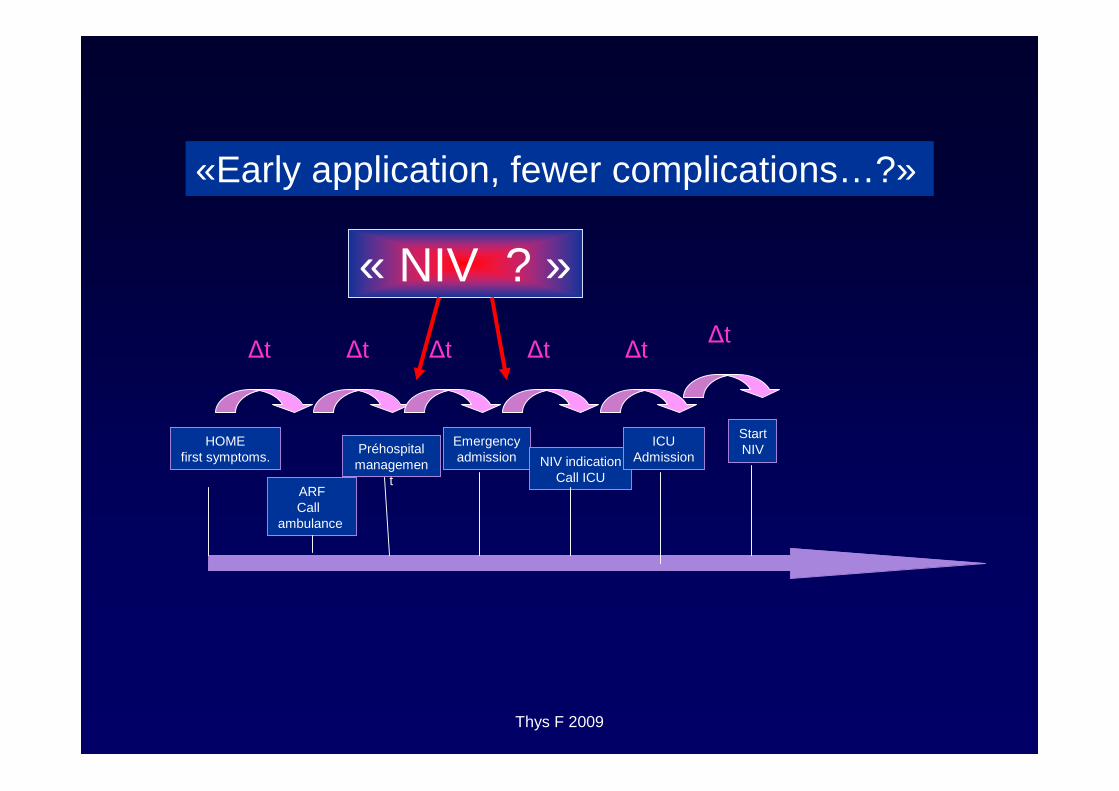
«Early application, fewer complications…?»
HOMEfirst symptoms.
ARFCall
ambulance
Préhospitalmanagemen
t
Emergencyadmission NIV indication
Call ICU
ICUAdmission
StartNIV
Δt Δt Δt Δt ΔtΔt
« NIV ? »
Thys F 2009
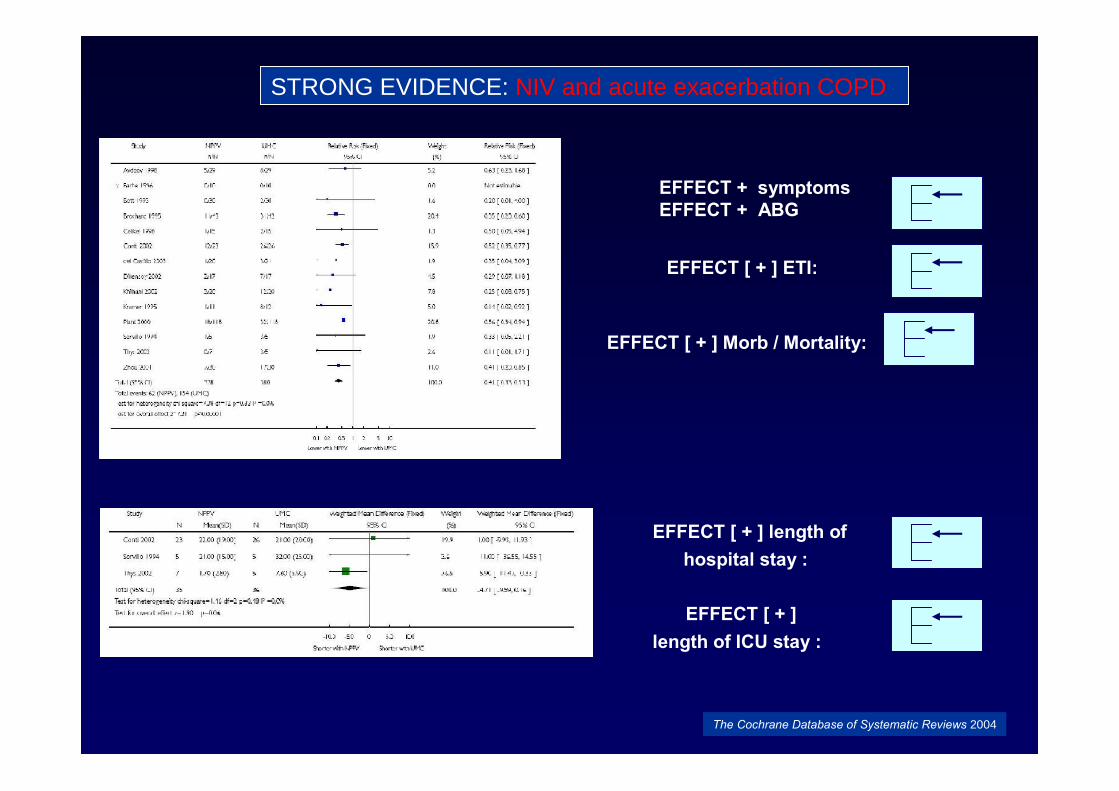
STRONG EVIDENCE: NIV and acute exacerbation COPD
EFFECT + symptomsEFFECT + ABG
EFFECT [ + ] ETI:
EFFECT [ + ] Morb / Mortality:
Intubation
Durée séjour USI
EFFECT [ + ] length ofhospital stay :
EFFECT [ + ]length of ICU stay :
The Cochrane Database of Systematic Reviews 2004
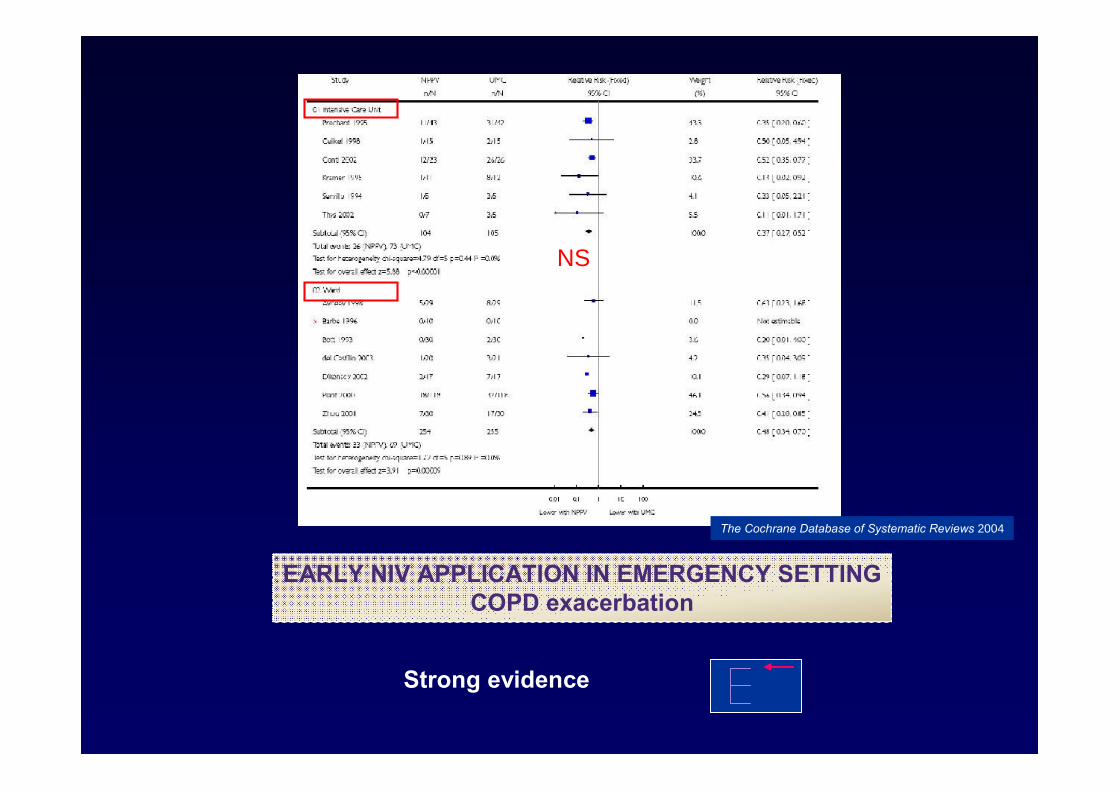
NS
Intubation
EARLY NIV APPLICATION IN EMERGENCY SETTINGCOPD exacerbation
Strong evidence
The Cochrane Database of Systematic Reviews 2004
ICU - RICUp
H
7,0
7,1
7,2
7,3
7,4 Resp. WARDBro
char
dKra
mer
Celik
elM
artin
Conti
Bott
Angus
Barbé
Plan
t
ED
Woo
dTh
ys
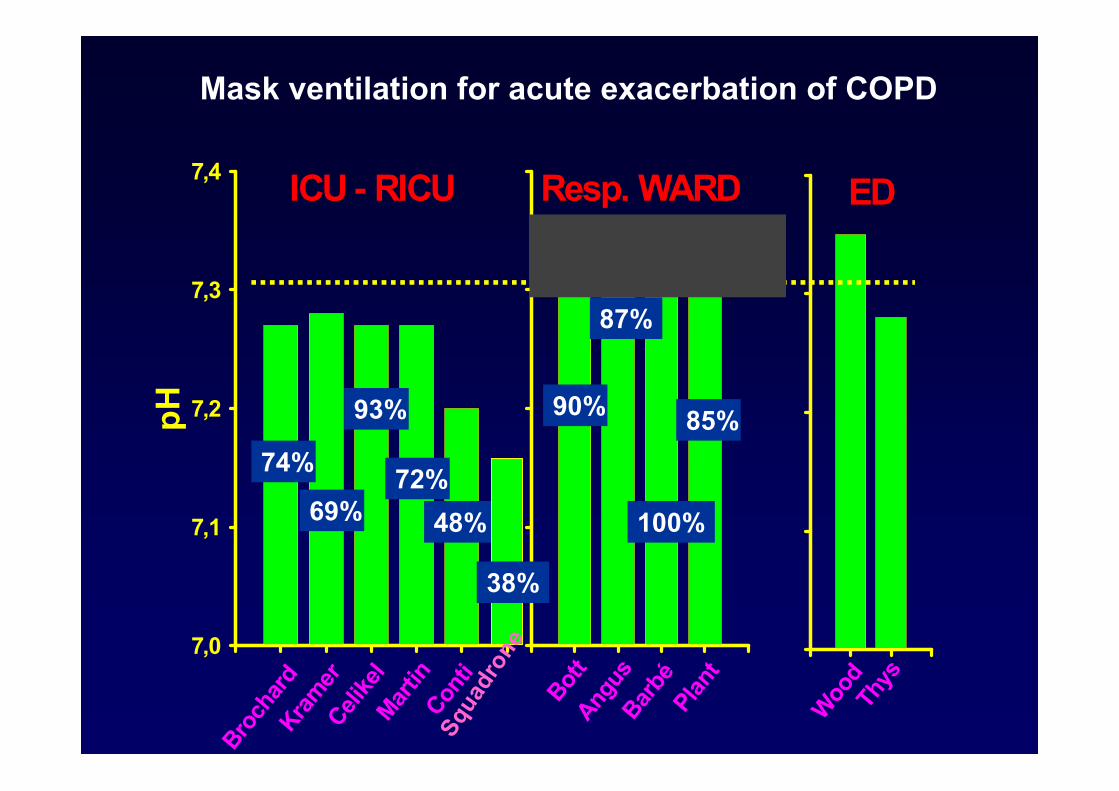
Mask ventilation for acute exacerbation of COPD
74%
69%
93%
72%
48%
90% 85%Sq
uadr
one
38%
87%
100%
Hill S; RESPIRATORY CARE • JANUARY 2009 VOL 54 NO 1
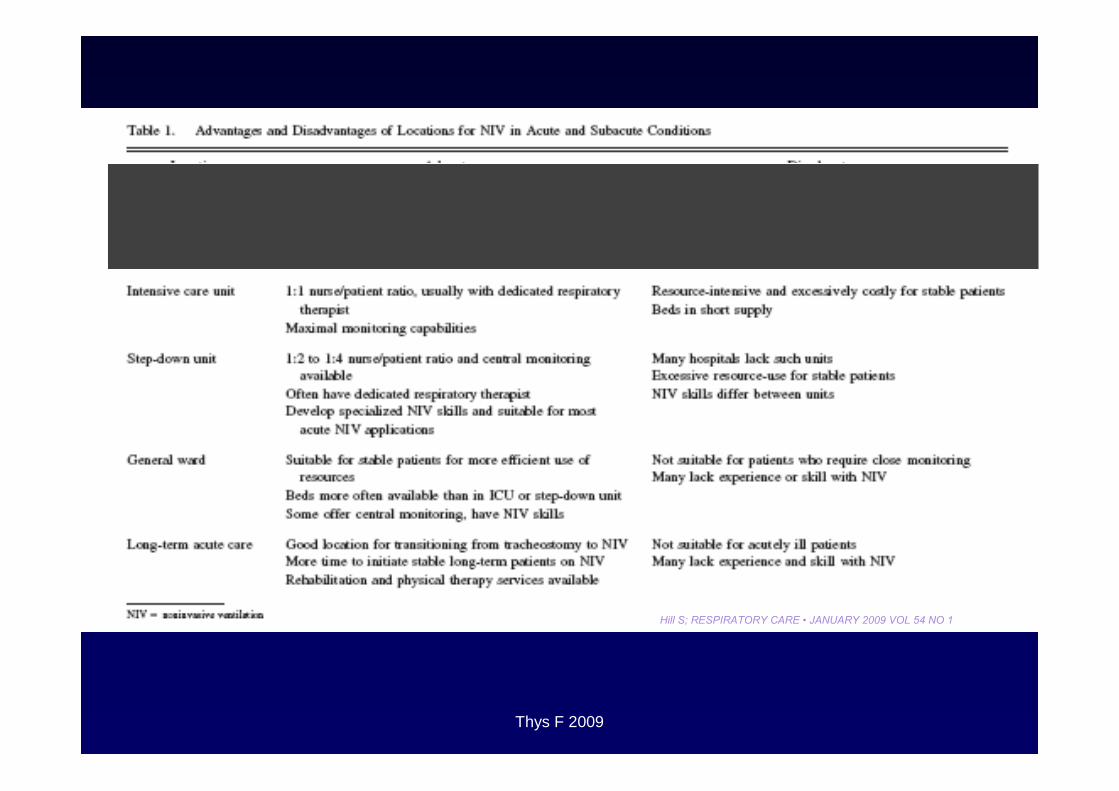
Thys F 2009
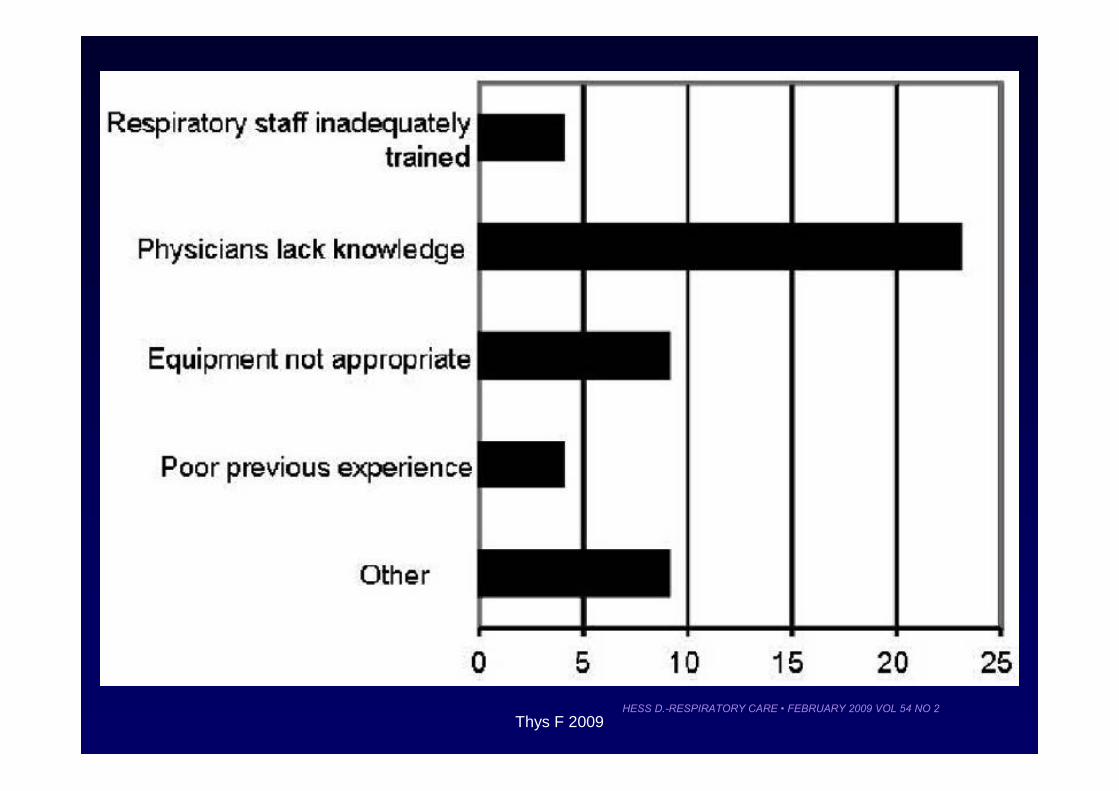
HESS D.-RESPIRATORY CARE • FEBRUARY 2009 VOL 54 NO 2Thys F 2009
Sottiaux T, Chest 1999
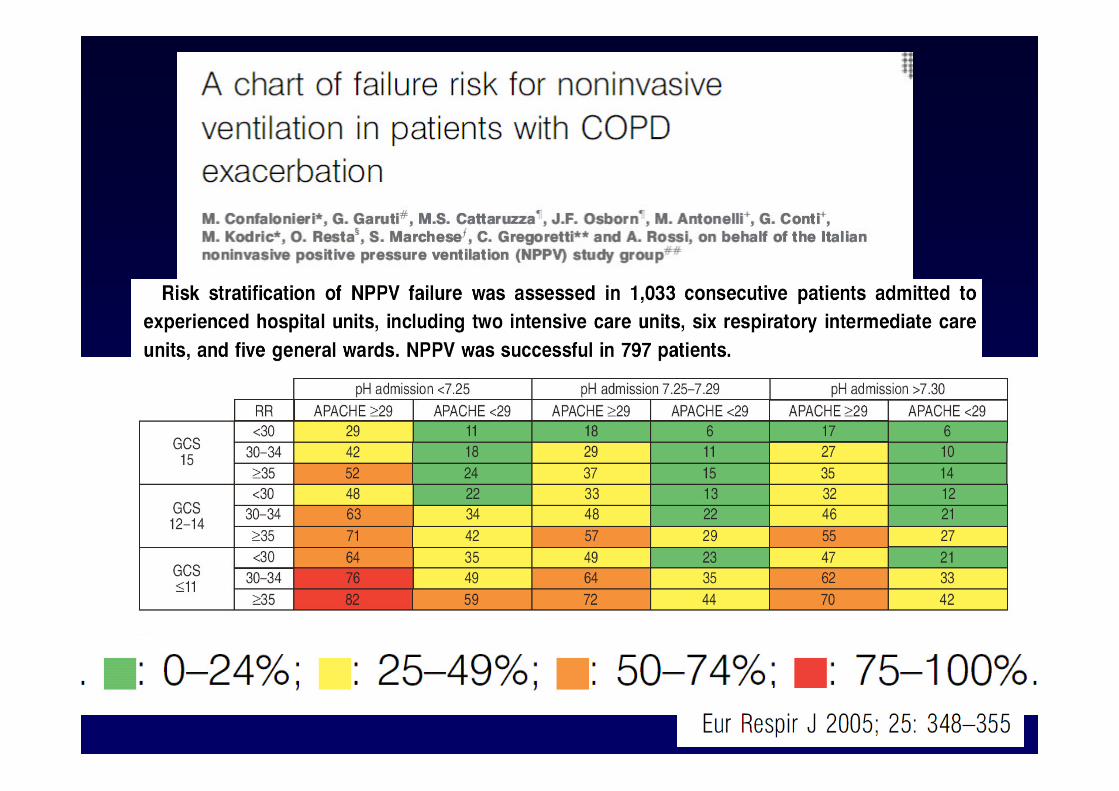
“We must identify patients in whom NIV is not likely to be effective,so avoiding a dangerous delay before effective therapy is applied.
We must dissuade physicians from the indiscriminate use of NIV in ARF patients.”
SELECTED INDICATIONS FOR NIV IN ARF PATIENTS
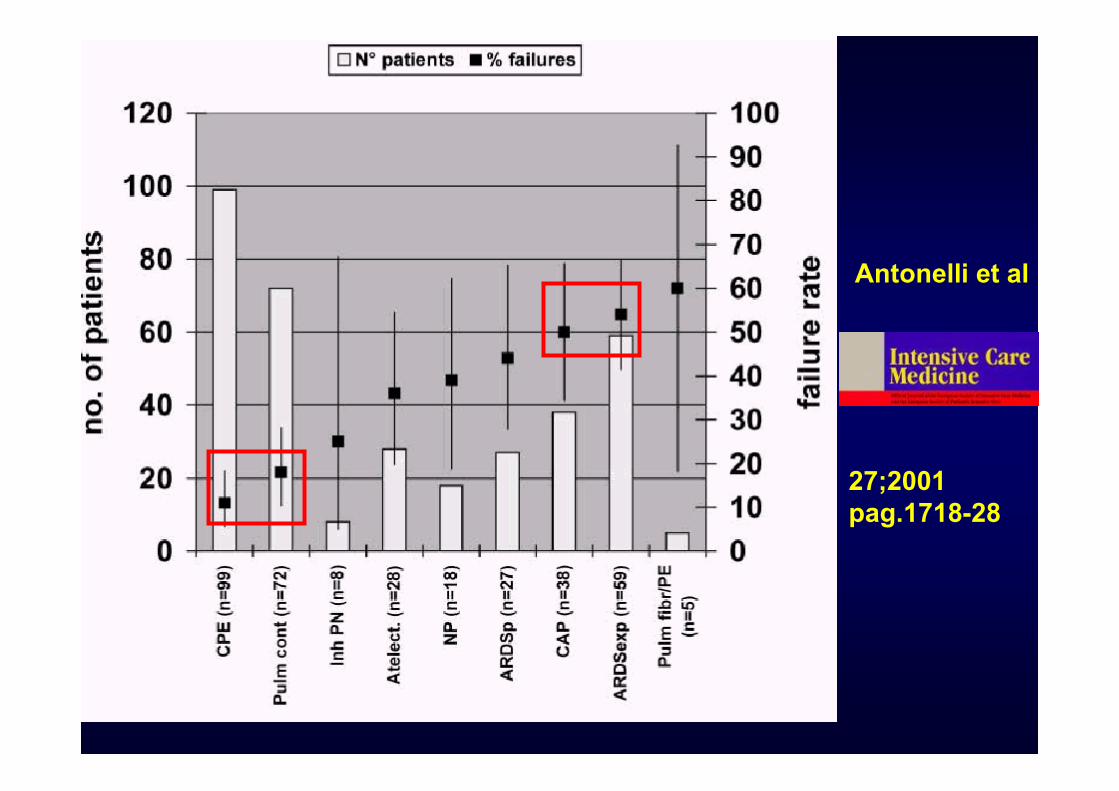
Antonelli et al
27;2001pag.1718-28
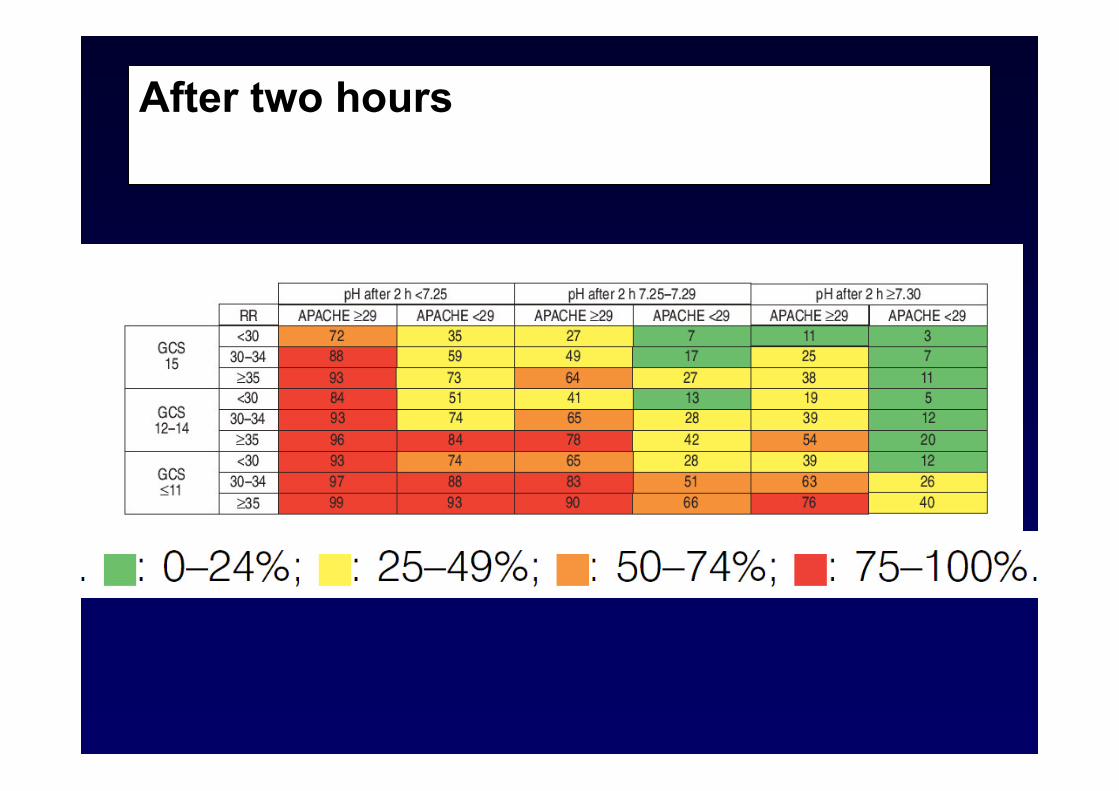
After two hours
ARF in COPD : NIV
• Success rates [ 80-85%]• Increases pH, reduces PaCO2, relieve symptoms
and dyspnea in first 4 h of treatment• Decreases the length of hospital and ICU stay• Mortality, Morbidity intubation rate are reduced
Depends on staff experience and availability of resources for monitoring, andmanaging complications
For the first few hours, one-to-one monitoring by a skilled and experienced nurse,respiratory therapist, or physician is mandatory.
Immediate access to staff skilled in invasive airway management.
Conditions necessary for the NIV application in this particular setting
PREHOSPITAL SETTING and NIV ?
Very low level of evidence……..
No serious study published !
Feasibility:
Clinical benefit :
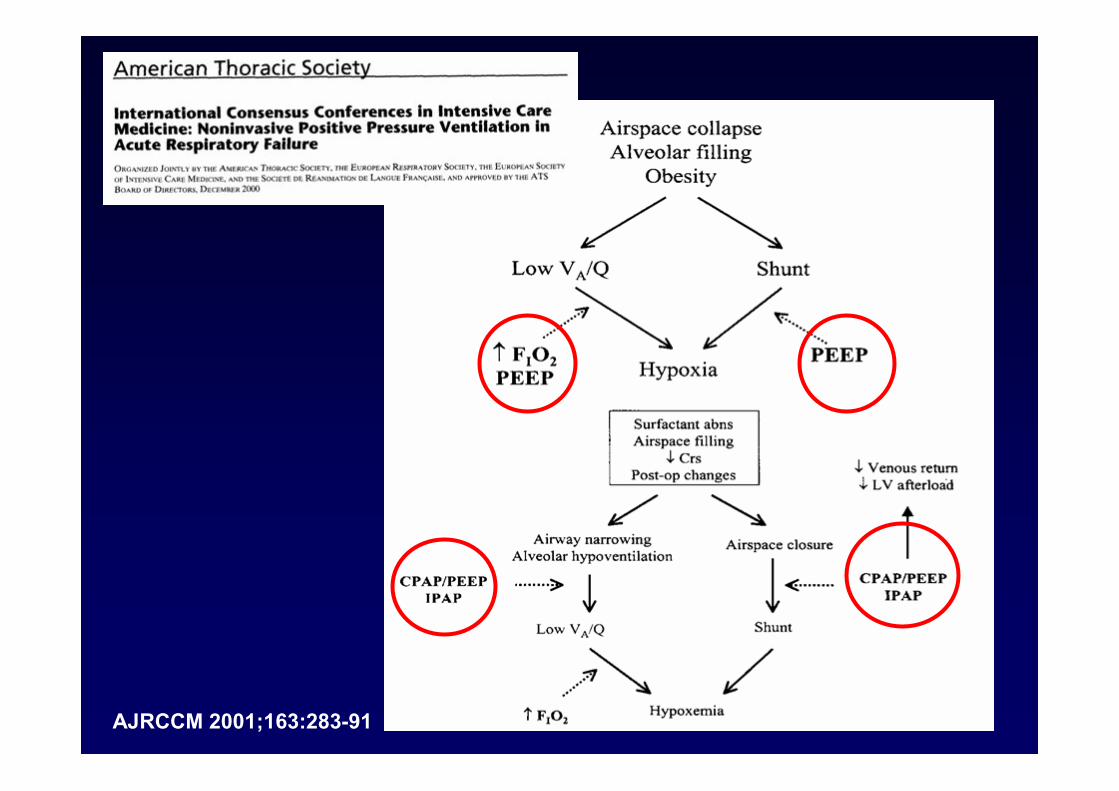
AJRCCM 2001;163:283-91
Caso clinico
Maschio 72 anni , PESO 82 KG BPCO stadio GOLD III Ipertensione arteriosa Terapia domiciliareOmeprazolo 20 mg, furosemide 20 mg,ramipril 10 mg,Tiotropio 1 puff/die, fluticasone + formoterolo
50/500 spray 1 puff b.i.d.
Caso clinicoIn P.S.GCS 11, P.A. 150/80 mmhg, SPO2 85%
EOT: broncostenosi associata a ronchi,iniziale utilizzo muscolatura respiratoria
accessoria
ECG: ritmo sinusale, BBdx, EAS
RX TORACE: accentuazione della tramavascolare , iperdiafania diffusa
EGA all’ingresso
PH 7.26PaO2 94PaCO2 104HCO3 46.7FIO2 40%
Caso clinico
Sulla postazione monitorizzata
Inizia NIV in modalità PSV
PS 20 CMH20PEEP 6 CMH20FIO 28%
EGA DOPO 1 ORA
PH 7.33PaO2 100PaCO2 95HCO3 50FIO2 28%
Sulla postazione monitorizzata
PS 22 CMH20PEEP 6 CMH20FIO 28%
EGA DOPO 6 ORE
TRASFERIMENTO IN MEDICINA
PH 7.36PaO2 94PaCO2 78HCO3 48.6FIO2 28%
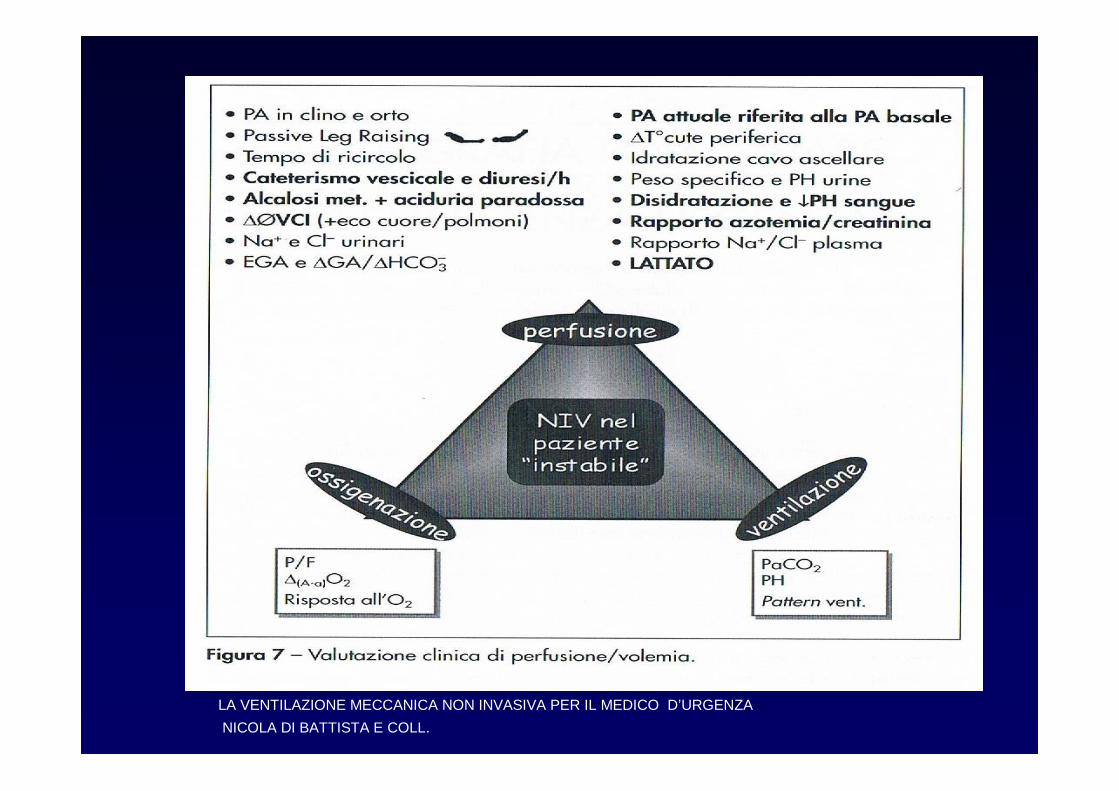
LA VENTILAZIONE MECCANICA NON INVASIVA PER IL MEDICO D’URGENZA
NICOLA DI BATTISTA E COLL.
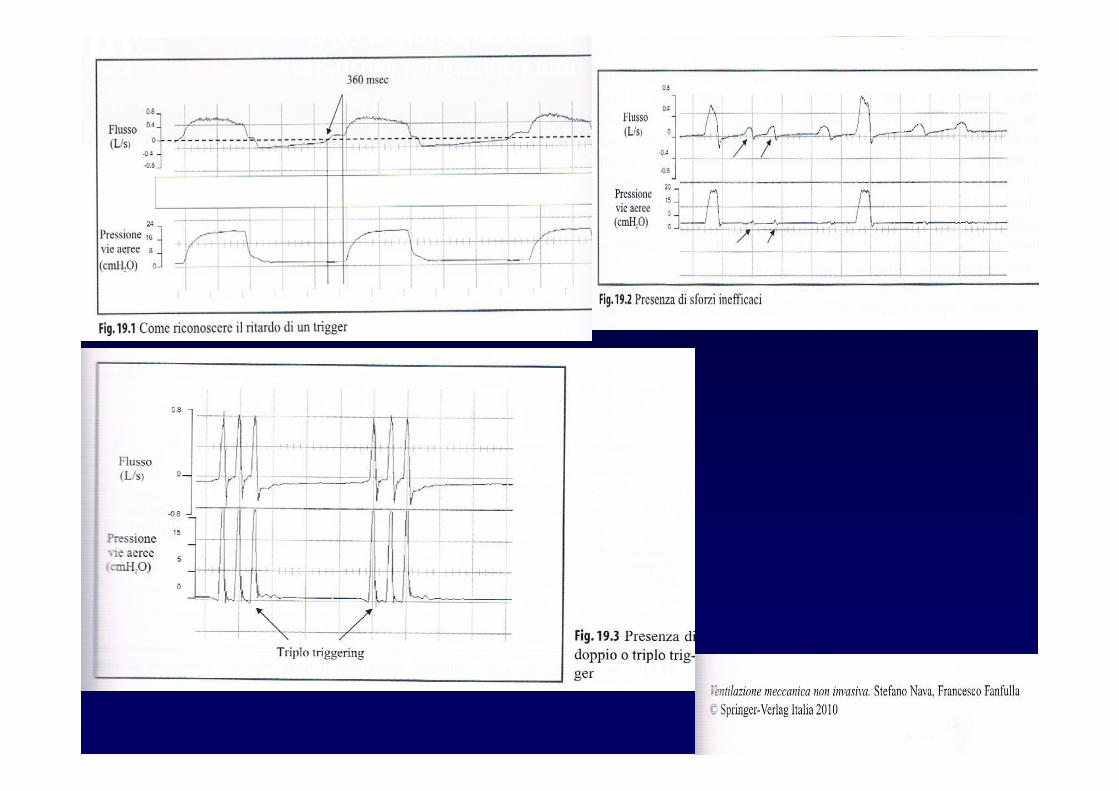
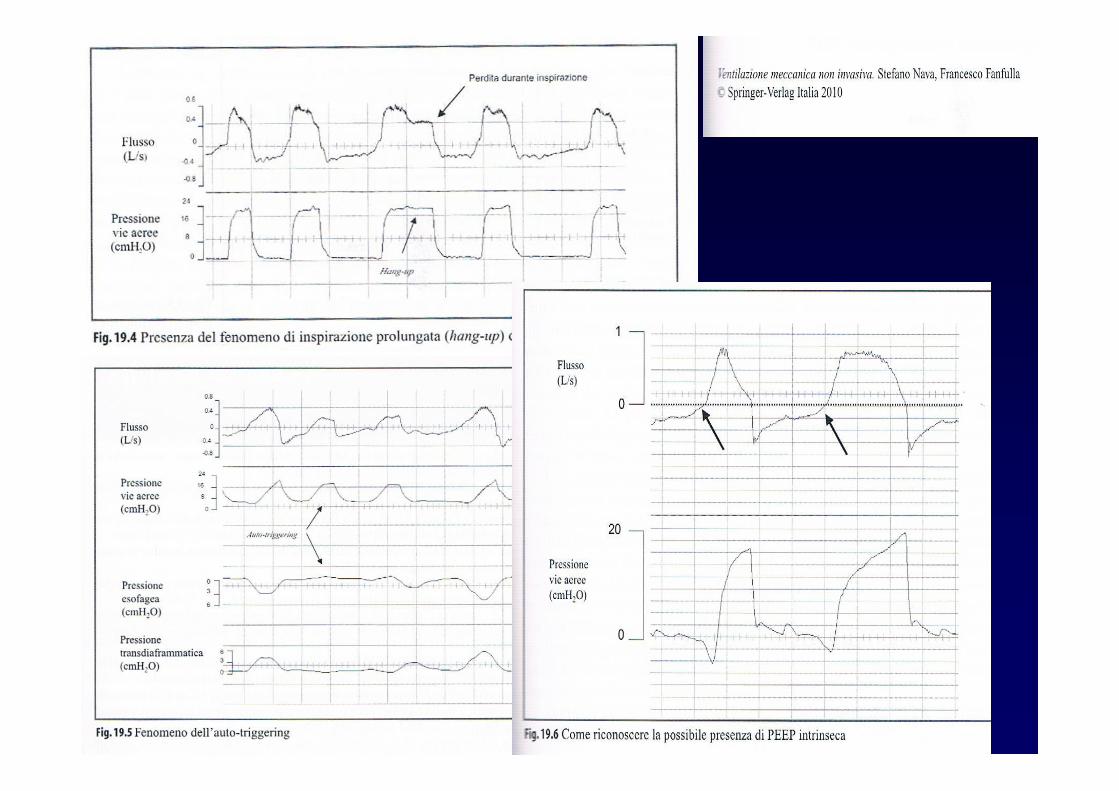
Reasons for asynchrony
Incorrect ventilator settings Ti too long Leak Intrinsic PEEP
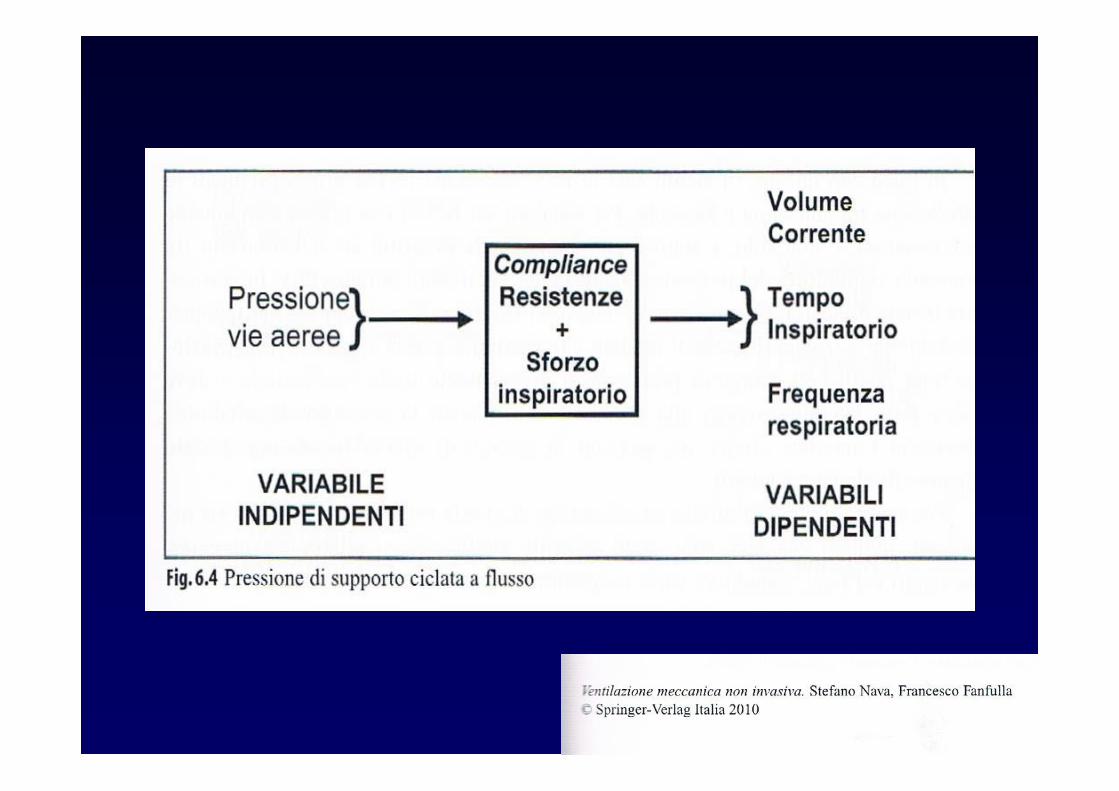
PSV
Metodica di ventilazione in cui ogni atto respiratoriospontaneo riceve un supporto pressorio inspiratorio. Lapressione inspiratoria delle vie aeree è mantenutacostante al livello stabilito dall’operatore , e poiché ilpassaggio alla fase espiratoria è ciclato a caduta diflusso, il paziente ha il controllo del timing respiratorio edel volume corrente. questo dovrebbe migliorarel’interazione paziente –macchina. L’aggiunta di PEEPesterna può ulteriormente ridurre il lavoro dei muscolirespiratori
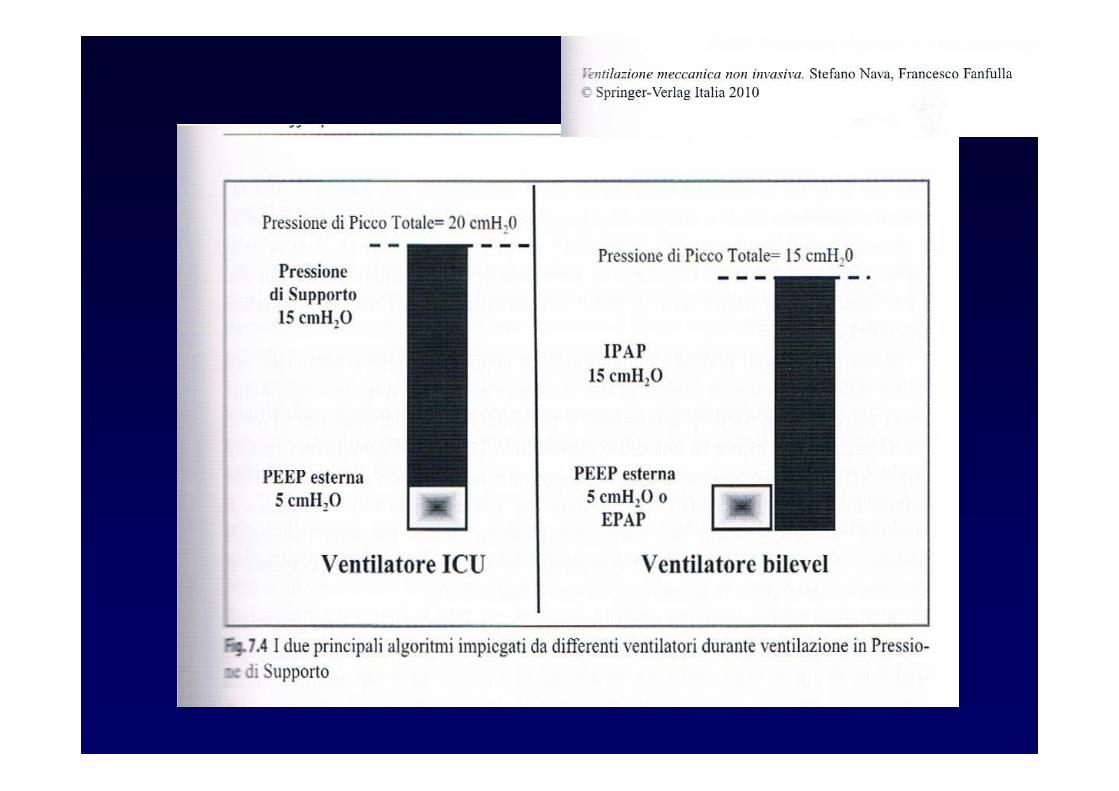
Pressione di supporto
Aiuto inspiratorio sovra-PEEP erogato dal ventilatore.Diverso signifacato ha il termine IPAP ( Inspiratory PeakAirways Pressure ) che definisce il valore totale dipressione inspiratoria comprendente anche il livello diPEEP
Quale pressione nel BPCO ?
Tale da non generare volumi correnti superiori a 8 mL/Kg
Pressione espiratoria
L’aggiunta di una pressione positiva espiratoria in PSVviene spesso definita come ventilazione bilevel
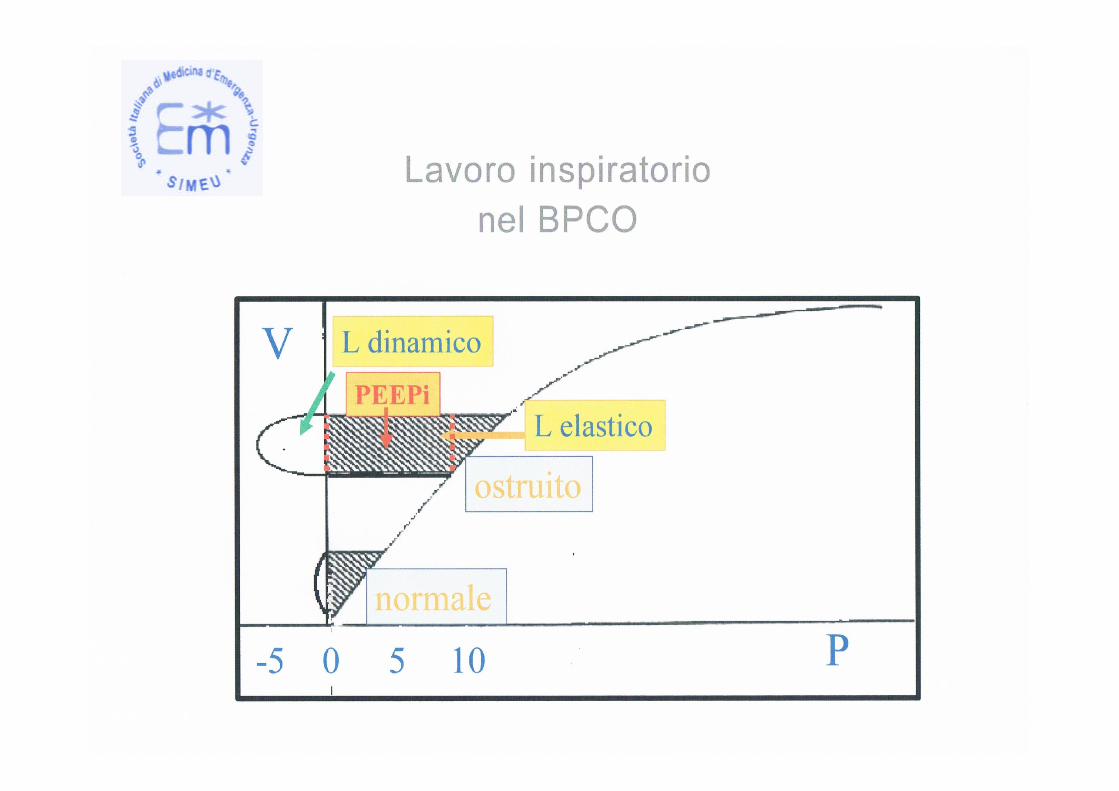
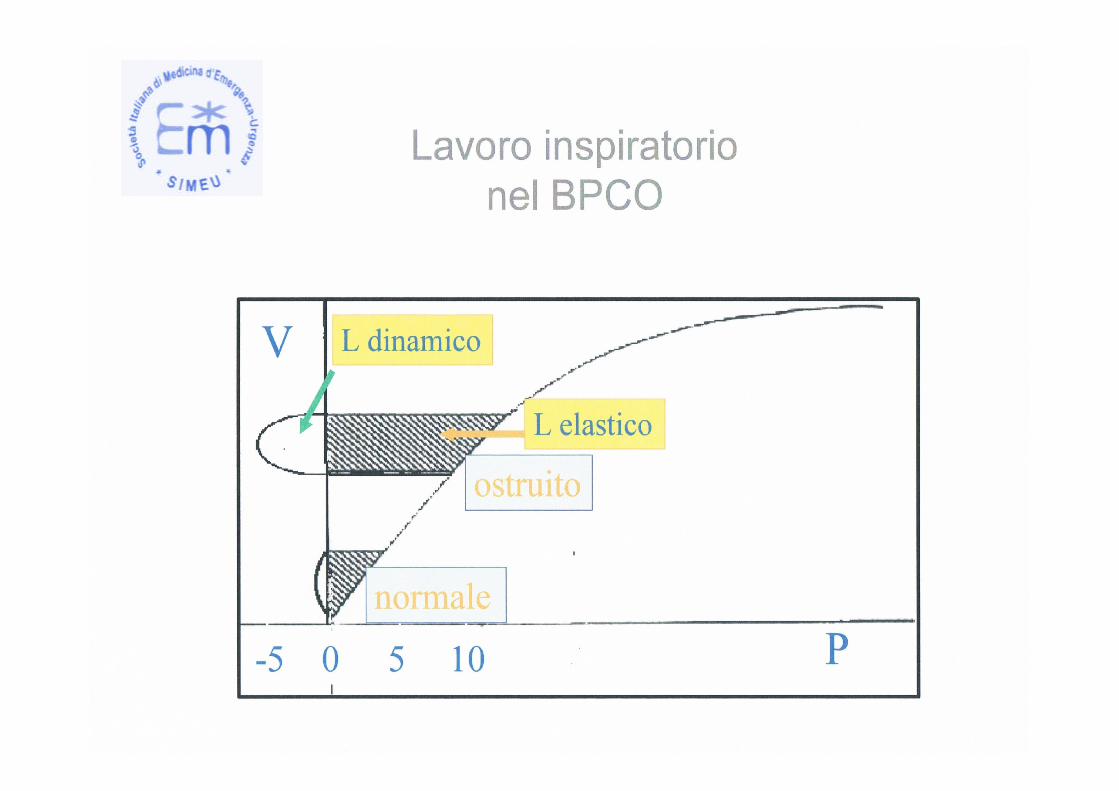
Lo scopo è ridurre il carico resistivo per eliminare lacomponente del lavoro respiratorio dovuta alla presenzadi PEEP intrinseca che è pari a circa il 50% del lavororespiratorio totale
Quale pressione espiratoria nel BPCO?
Una pressione tra 4 e 6 cmH2O
Trigger espiratorio
Ciclaggio tra fase inspiratoria ed espiratoriadeterminato dalla caduta di flusso inspiratorio ad undeterminato valore impostato ed è espresso comepercentuale del picco di flusso.settato di default al 25% , naturalmente influenza iltempo inspiratorioparticolarmente utile in presenza di perdite

OSSERVAZIONE PAZIENTE CRITICO
2008 2009
5%
respiratori2141
2009
39.00095%
4%
respiratori1554
2008
35.00096%