lipo-meningocele ccase by ali akhter
TRANSCRIPT
Lipomeningocele Case Presentation
By
Dr Ali Akhter
Intern
Paediatric Surgery
Civil Hospital Karachi
1 year old male child resident of Mithi, brought in paediatric surgical OPD with presenting C/o Lump over the lower back since birth.
Lump was small initially that gradually increased in size over past one year.it was painless without any discharge, or change in colour of overlying skin.
No associated fever, no fecal or urinary retention or movement problem of lower limbs.
No significant past medical or surgical Hx.Antenatally mother was unregistered case with no proper antenatal visits or scan, didn’t took multivitamins or other medication, no Hx of illness during pregnancy.Baby was born at term via NVD at home with no postnatal issue except small swelling over lower back.Developmentally child was appropriate for his age.Product of uncosanguineous marriage having one other sib that is healthyNo Hx of familial illness, or congenital malformations

Vaccinated upto age.
Poor socio-economic background.

Young infant of average built and height sitting in mom’s lap
RR: 26 br/mint
HR:100b/mint
Temp:98 F
BP: 90/60 mmHg
No anemia, jaundice, edema, Deh, Cl, or cyanosis. Lymph nodes impalpable
Wt: 8 kgs
Height: 87 cm
MAC: 11 cm
OFC: 40 cm

Local exam of lump:An orange size ( 5X 6 cm) single swelling starting at about midline at lumbo sacral area extending towards left side upto middle of iliac crest with normal overlying skin. No hairs or other visible defect.It was nontender normothermic, soft swelling with well defined margins,attached to underlying structures; overlying skin was movable.Trans-illumination and fluctuation tests were negative.

There was no neurological deficit detected on examination of lower limbs.
Examination of CHEST; CVS; & ABDOMEN was unremarkable.

DD?

D/D:
- Lipoma
- Neural tube defect
(lipomeningocele/meningomyelocele)
- Sacrococcygeal teratoma

Lumbo-sacral MRI

MRI Findings
Spina bifida at L 3,4 &5
Protrusion of spinal nerve roots from the neural tube defect
Lipomatous tissue covering meningocele
Xray L/S Spine
Showed Spina bifida at L 3,4 &5
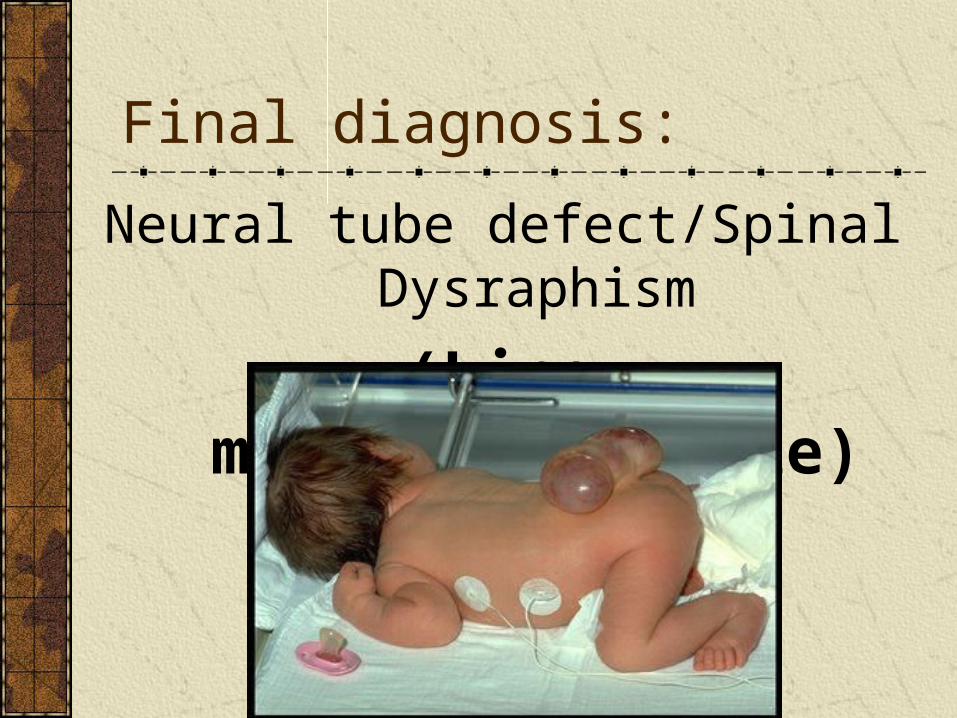
Final diagnosis:
Neural tube defect/Spinal Dysraphism
(Lipo-meningomyelocele)

Treatment ?
Neural Tube Defects:Congenital deformities involving the coverings
of the nervous system are called neural tube
defects Normal embryological development
Neural plate development -18th dayCranial closure 24th day (upper spine)Caudal closure 26th day (lower spine)

Etiology
The primary embryologic defect in all neural tube defects is failure of the neural tube to close (at days 17-30 of gestation.), affecting neural and cutaneous ectodermal structures.
This may result from:
Combination of environmental and genetic causes
Teratogens: (carbamazepine, valproic acid)
Nutritional deficiencies - notably, folic acid deficiency

Spina bifida occulta: In which osseous fusion of one or more vertebral arches is lacking, without involvement of the underlying meninges or neural tissue.a skin lesion such as a hairy patch, dermal sinus tract, dimple, hemangioma, or lipoma points to the underlying spina bifida
Spina bifida cystica with meningocele: is simply herniation of the meninges through the bony defect (spina bifida). The spinal cord and nerve roots do not herniate into this dorsal dural sac.
Types of neural tube defects
Spina bifida cystica with Myelomeningocele is a condition in which the spinal cord and nerve roots herniate into a sac of meninges. This sac protrudes through the bone and musculocutaneous defect.
Certain neurologic anomalies, such as hydrocephalus and Chiari II malformation are associated with myelomeningocele., myelomeningoceles have a higher incidence of associated intestinal, cardiac, and esophageal malformations, as well as renal and urogenital anomalies
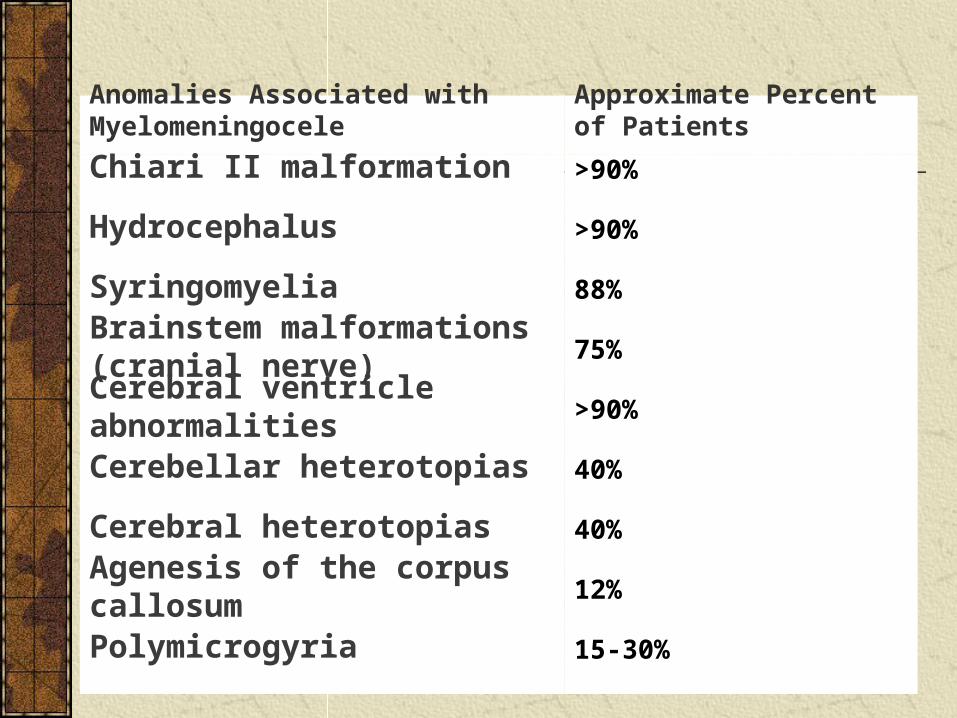
Anomalies Associated with Myelomeningocele
Approximate Percent of Patients
Chiari II malformation >90%
Hydrocephalus >90%
Syringomyelia 88%
Brainstem malformations (cranial nerve)
75%
Cerebral ventricle abnormalities >90%
Cerebellar heterotopias 40%
Cerebral heterotopias 40%
Agenesis of the corpus callosum 12%
Polymicrogyria 15-30%
Anencephaly and rachischisis are extremely severe forms, in which an extensive opening in the cranial and vertebral bone is present with an absence of variable amounts of the brain, spinal cord, nerve roots, and meninges.

lipomeningocele or lipomyelomeningocele -subtype of spina bifida:
These lesions have a lipomatous mass that herniates through the bony defect and attaches to the spinal cord, tethering the cord and often the associated nerve roots.
The lipomyelomeningocele can envelop both dorsal and ventral nerve roots, only the dorsal nerve roots, or simply the filum terminale and conus medullaris. These lesions do not have associated hydrocephalus but have a more guarded prognosis than simple meningoceles.
The surgical goal in treating these lesions is to detach the lipoma of the buttocks from the lipoma that emerges through the dura, fascia, and bony defect. All of the lipoma should not be removed. Take care to leave some lipoma on the cord in order to avoid injuring the underlying neural substrate. The filum terminale also is divided to further untether the cord. A patulous graft is then placed over the dural opening to establish a pool of CSF around the cord to help prevent retethering
Diagnostic Detection of Neural Tube Defects
measurement of AFP in the amniotic fluid or maternal bloodstream at 15-20 weeks' gestation which leak into the amniotic fluid from open neural tube defects such as anencephaly and myelomeningocele
Determining precise gestational age is essential because fetal AFP levels are age specific
Normal AFP concentration in the maternal serum is usually lower than 500 ng/mL.
fetal ultrasonography by a skilled person is usually 98% specific. False-positive findings can result from multiple pregnancies or inaccurate fetal dating. However, closed neural tube defects can sometimes remain undetected, especially in cases of skin-covered lipomyelomeningoceles and meningoceles, in which the AFP levels may also be normal. These closed neural tube defects comprise about 10% or more of total neural tube defects discovered.
