liz borders case study ppt
TRANSCRIPT

APPLICATION OF ASPEN GUIDELINES FOR INTIATING TPN: A CASE OF SPONTANEOUS
NONTRAUMATIC HEMOPERITONEUMBy Liz Borders

BACKGROUND INFORMATION
o 65 year old Caucasian male
o Married; Businessman
o Denies any past medical history
o Past surgical history:o Multiple inguinal hernia repairso Lipoma excision
o Appeared physically well-nourished
o 5’ 8” or 68”
o 175 lbs or 79 kg
o BMI of 26 kg/m2
o BMI within normal limits for age

(LACK OF) DIET PROGRESSION
10/11 – 10/17: NPO
10/17: Clear liquids
10/18: Prudent (low cholesterol). Ate 2 meals
10/19: NPO. Can have ice, hard candy, gum, popsicles, sips with medicine
10/21: Clear liquids
10/22-discharge: NPO. Can have ice chips and Italian ice

COURSE OF HOSPITAL STAY
o 10/11 – Came to the emergency department with complaints of abdominal pain and some non-bloody emesiso CT of abdomen and pelvis showed significant amount of hemoperitoneumo Became hypotensive and tachycardic and required massive blood transfusion

DIAGNOSIS: SPONTANEOUS NON-TRAUMATIC HEMOPERITONEUM
Computed tomography (CT) scan of blood in the peritoneal cavity.
COURSE OF HOSPITAL STAY
o10/11 – Admitted to ED, dx CT showing hemoperitoneum oBecame hypotensive and tachycardic and required massive blood transfusion
o 10/11 - Exploratory laparotomy (ex-lap) with omental resection, small bowel resection, repair of serosal tearso Abdomen left open – patient was unstable and surgeons wanted to prevent abdominal
compartment syndrome. Wound VAC was placed

EXPLORATORY LAPAROTOMY (EX-LAP) ON 10/11
o Procedure where a patient’s abdomen is cut open and surgeons look at the organs and structureso Called “exploratory” because surgeons are not
going in with specific procedures in mindo Objective is to obtain information that is not
available via clinical diagnostic methods
o Abdomen was left open as the patient was also unstable. Surgeons also wanted to prevent abdominal compartment syndrome

OMENTAL RESECTION & SMALL BOWEL RESECTION

NEGATIVE PRESSURE WOUND THERAPY
o Vacuum is placed over the wound to draw out fluid and increase blood flow to the area1
o Open abdomens require 1.5-2.5gm/kg of protein2
o Well-nourished patients with open abdomens/wound VACs should tolerate 7-10 days without nutrition support2
o During this time, enteral access should be obtained. If full enteral support can’t be attained by 7-10 days, PN should be used2
COURSE OF HOSPITAL STAY
o 10/11 – Admitted to ED, dx CT showing hemoperitoneum oBecame hypotensive and tachycardic and required massive blood transfusion
o 10/11 – Ex-lap with omental resection, small bowel resection, repair of serosal tearso Abdomen left open as patient was unstable, and wound VAC was placed
o10/11 – Patient had post-operative ST-segment elevation myocardial infarction (STEMI)

ST-ELEVATED MYOCARDIAL INFARCTION (STEMI)
o Also known as a heart attack. Occurs when the blood flow to the heart is stopped
o STEMI occurs by developing a complete occlusion of a major coronary artery previously affected by atherosclerosis
o Cardiac complications occur in up to 5% of patients 45 years or oldero Myocardial infarction is the most common complication4

COURSE OF HOSPITAL STAY
o 10/11 – Admitted to ED, dx CT showing hemoperitoneum oBecame hypotensive and tachycardic and required massive blood transfusion
o 10/11 – Ex-lap with omental resection, small bowel resection, repair of serosal tearso Abdomen left open as patient was unstable, and wound VAC was placed
o 10/11 – Patient had post-operative ST-segment elevation myocardial infarction (STEMI)
o 10/12 – Initial nutrition assessment

INITIAL NUTRITION ASSESSMENT – 10/12
o PES Statement: Increased nutrient needs (energy and protein) related to surgery, open abdomen, and STEMI as evidenced by labs, wounds, and estimated needs for recovery.
o Calculated needs:o 1975 – 2370kcal (25-30kcal/79kg)o Penn State Equation: 1763kcalo 119 – 158gm protein (1.5-2gm/kg)
oIntervention: Nutrition support options
INITIAL NUTRITION INTERVENTIONS – 10/12
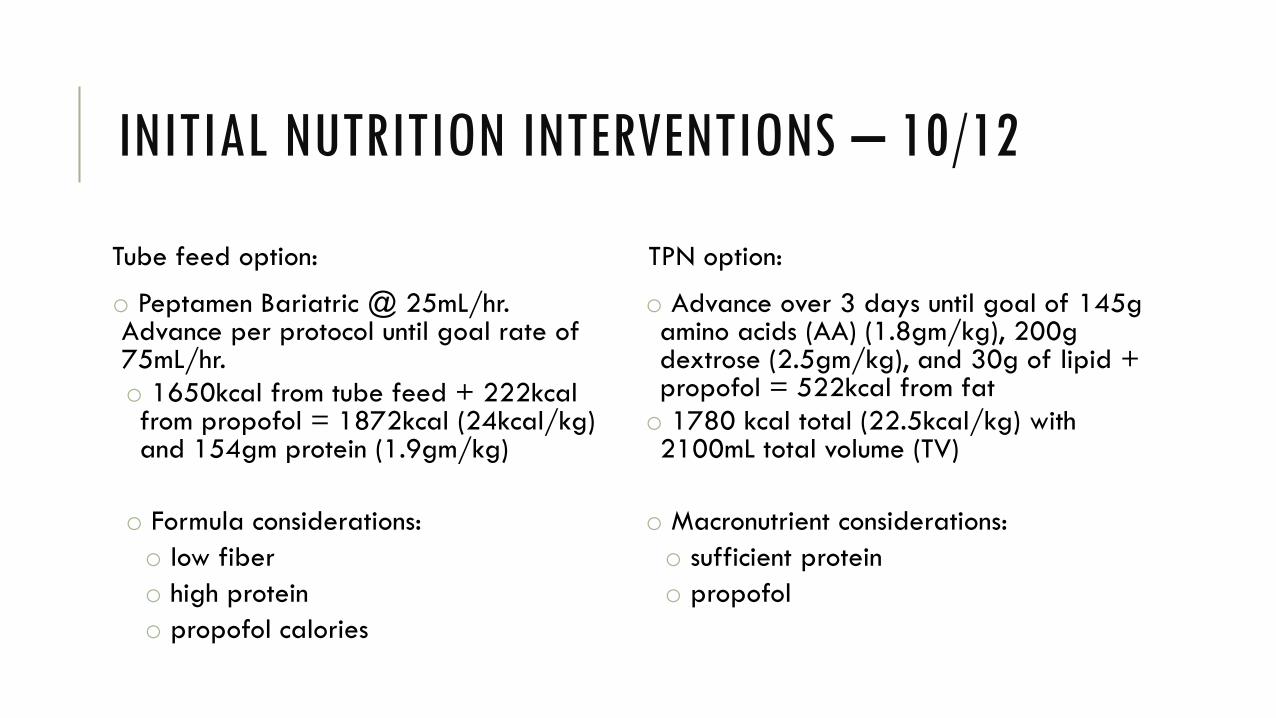
Tube feed option:
o Peptamen Bariatric @ 25mL/hr. Advance per protocol until goal rate of 75mL/hr.o 1650kcal from tube feed + 222kcal from propofol = 1872kcal (24kcal/kg) and 154gm protein (1.9gm/kg)
o Formula considerations:o low fibero high proteino propofol calories
TPN option:
o Advance over 3 days until goal of 145g amino acids (AA) (1.8gm/kg), 200g dextrose (2.5gm/kg), and 30g of lipid + propofol = 522kcal from fato 1780 kcal total (22.5kcal/kg) with 2100mL total volume (TV)
o Macronutrient considerations:o sufficient proteino propofol

COURSE OF HOSPITAL STAY
o 10/11 – Admitted to ED, dx CT showing hemoperitoneum oBecame hypotensive and tachycardic and required massive blood transfusion
o 10/11 – Ex-lap with omental resection, small bowel resection, repair of serosal tearso Abdomen left open as patient was unstable, and wound VAC was placed
o 10/11 – Patient had post-operative ST-segment elevation myocardial infarction (STEMI)
o 10/12 – Initial nutrition assessment
o 10/12 – Stabilized, returned to the operating room and had abdomen closed
o 10/13 – Extubated
o 10/16 – Nutrition follow-up assessment

NUTRITION FOLLOW-UP – 10/16
o Patient had been NPO x5 dayso Diagnosed patient with mild malnutrition
o Per MD, awaiting bowel function with possible move towards clear liquids
Nutrition Recommendations:o Low fiber diet if tolerableo If unable to progress towards diet,
recommended tube feeding or TPN

(LACK OF) DIET PROGRESSION
10/11 – 10/17: NPO
10/17: Clear liquids
10/18: Prudent (low cholesterol). Ate 2 meals
10/19: NPO. Can have ice, hard candy, gum, popsicles, sips with medicine
10/21: Clear liquids
10/22-discharge: NPO. Can have ice chips and Italian ice

COURSE OF HOSPITAL STAY
o 10/16 – Nutrition follow-up assessment
o 10/18 – Abdominal X-ray noted ileus

ILEUS
o Early enteral nutrition after surgery to prevent post-op ileus – maintains intestinal barriers, improves blood flow and healing5
o Once ileus had formed, enteral nutrition was not an option during this time, as the gut is not functioning
o Ileus was treated nonoperativelyo Require bowel rest and hydration o Symptoms like nausea and abdominal distention
treated with antiemetics and nasogastric tube decompression
o Hypomotility of the gastrointestinal tract in the absence of mechanical bowel obstruction

(LACK OF) DIET PROGRESSION
10/11 – 10/17: NPO
10/17: Clear liquids
10/18: Prudent (low cholesterol). Ate 2 meals
10/19: NPO. Can have ice, hard candy, gum, popsicles, sips with medicine
10/21: Clear liquids
10/22-discharge: NPO. Can have ice chips and Italian ice

COURSE OF HOSPITAL STAY
o 10/16 – Nutrition follow-up assessment
o 10/18 – X-ray noted ileus
o 10/21 – Developed anastomotic leak and had ex-lap for lysis of adhesions (LoA), abscess drainage, fibrin reinforcement of staple line

EX-LAP ON 10/21
o Patient was having some return of bowel function in the form of loose, liquid stools
o It was decided to perform a CT scan due to continued delay of full bowel function and sustained leukocytosis
o Discovered fluid collection from a bowel anastomosis
o Surgeons were forced to perform another ex-lap to drain the purulent collection of fluid from the abdomen, lyse adhesions, and reinforce the anastomosis’ staple line

COURSE OF HOSPITAL STAY
o 10/16 – Nutrition follow-up assessment
o 10/18 – X-ray noted ileus
o 10/21 – Developed anastomotic leak and had ex-lap for lysis of adhesions (LoA), abscess drainage, fibrin reinforcement of staple line
o 10/22 – Nutrition follow-up. Started on total parenteral nutrition (TPN)

NUTRITION FOLLOW UP – 10/22
oPatient had been NPO or on clears for 11 dayso Diagnosed patient with moderate malnutrition
o Spoke with doctor about urgent need for nutritiono As patient did not have a functioning bowel (small bowel resection, ileus, anastomotic leak), TPN was
the only option
In the patient who was previously healthy prior to critical illness with no evidence of protein-calorie malnutrition, use of PN should be reserved and initiated only after the first 7 days of hospitalization (when EN is not available).3
PN therapy provided for a duration of <5-7 days would be expected to have no outcome effect and may result in increased risk to the patient. Thus, PN should be initiated only if the duration of therapy is anticipated to be ≥7 days.3

NUTRITION FOLLOW UP – 10/22
o New PES statement: Malnutrition related to decreased intakes, surgery, and altered GI as evidenced by NPO/clears x11 days except 2 meals, wounds, labs, and calculated needs.
o Patient had developed acute post-op moderate energy malnutrition from lack of nutrition for over a week, wounds, labs, and calculated needs
o Recommended slow advancement of TPN to prevent refeeding syndrome6

NUTRITION INTERVENTIONS– 10/22
Day 1 – 12.8kcal/79kg
50g AA
150g dextrose
30g lipids
1000 mL
Day 2
90g AA
180g dextrose
40g lipids
1400mL
Day 3
120g AA
205g dextrose
45g lipid
1800mL
Day 4
140g AA
245g dextrose
50g lipid
2100mL
Day 5 – GOAL
140g AA (1.7gm/79kg)
290g dextrose (3.7gm/kg)
65g lipid (0.8gm/kg)
2196kcal (28kcal/kg)
2200mL

(LACK OF) DIET PROGRESSION
10/11 – 10/17: NPO
10/17: Clear liquids
10/18: Prudent (low cholesterol). Ate 2 meals
10/19: NPO. Can have ice, hard candy, gum, popsicles, sips with medicine
10/21: Clear liquids
10/22-discharge: NPO. Can have ice chips and Italian ice

NITROGEN BALANCE – 10/27
o 140g of protein intake
o +2.97 nitrogen balance
o Positive balance shows patient was anabolic with TPN at goal

COURSE OF HOSPITAL STAY
o 10/16 – Nutrition follow-up assessment
o 10/18 – X-ray noted ileus
o 10/21 – Developed anastomotic leak and had ex-lap for lysis of adhesions (LoA), abscess drainage, fibrin reinforcement of staple line
o 10/22 – Started on total parenteral nutrition (TPN)
o 10/30 – Began progressing TPN towards 12-hour cycle - at-home TPN use needed due to anastomotic leak wound healing
NUTRITION FOLLOW UP – 10/30
o Patient was anabolic at TPN goal, but needed to go home on TPN for anastomotic wound healing
o Cycled TPN for 18 hours the first night, and 12 hours the second
Discharge TPN Rx: 140g AA (1.7gm/79kg)290g dextrose (3.7gm/kg)65g lipid (0.8gm/kg)2196kcal (28kcal/kg)2200mL over 12 hours

COURSE OF HOSPITAL STAY
o 10/16 – Nutrition follow-up assessment
o 10/18 – X-ray noted ileus
o 10/21 – Developed anastomotic leak and had ex-lap for lysis of adhesions (LoA), abscess drainage, fibrin reinforcement of staple line
o 10/22 – Started on total parenteral nutrition (TPN)
o 10/30 – Began progressing TPN towards 12-hour cycle - at-home TPN use needed due to anastomotic leak wound healing
o11/5 – Patient was discharged with at-home TPN

USING TPN WHEN THE GUT IS NOT FUNCTIONING
o Although using enteral nutrition is preferred, sometimes it is not an option
o If the GI tract is not functioning, TPN use may be needed
o Per ASPEN guidelines, TPN should not be used until around 7 days after admission
o This patient did not receive TPN until 11 days, so he was acutely malnourished post-operatively
o However, he reached an anabolic state soon after reaching TPN goal
o Patient was on TPN for greater than 5-7 days, so guidelines show this as a beneficial treatment to the patient

Patient came in well-nourished
Ex-lap, small bowel resection, omental
resection
Patient was prescribed bowel
rest – minimal nutrition (POD1-7)
Patient developed post-op ileus –
unable to feed with gut (POD 7-10)
Developed anastomotic leak and had another ex-lap (POD 10)
Started TPN (POD 11)
Went home on TPN for adequate
nutrition while leak wound heals

WHAT DID I LEARN
o Post-op malnutrition
o Using TPN before tube feeding
o Early enteral nutrition as a possible benefit after abdominal/intestinal surgery

REFERENCES
1. Gestring, M. Negative pressure wound therapy. In: UpToDate, Post TW (Ed), UpToDate, Waltham, A. (Accessed on December 6, 2015.)
2. Friese, R. S. (2012). The open abdomen: Definitinos, management principles, and nutrition support considerations. JPEN J Parenter Enteral Nutr, 27(4), 492-498.
3. McClave, S. A. et. al. (2009). Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient. JPEN J Parenter Enteral Nutr, 33(3), 277-316.
4. Devereaux, PJ. Perioperative myocardial infarction after noncardiac surgery. In: UpToDate, Post TW (Ed), UpToDate, Waltham, A. (Accessed December 6, 2015).
5. Warren, J. et. al. (2011). Postoperative diet advancement: surgical dogma vs evidence-based medicine. JPEN J Parenter Enteral Nutr, 26(2), 115-125.
6. Boateng A. et. al. (2010). Refeeding syndrome: Treatment considerations based on collective analysis of literature case reports. Elsevier Nutr, 26, 156-167.