london cancer: pathway specification for · london cancer: pathway specification for urological...
TRANSCRIPT
London Cancer:
Pathway specification for urological cancers
Originally published May 2012, updated December 2012
Version 2.0
2
Contents
1. Introduction ................................................................................................................................... 2 1.1. London Cancer ................................................................................................................................. 2 1.2. Pathway specifications .................................................................................................................... 3
2. Pelvic cancer pathway specification ................................................................................................. 5
3. Renal cancer pathway specification ............................................................................................... 13
Appendix: London Cancer Urology Technical Group .............................................................................. 19
1. Introduction
1.1. London Cancer
The cancer care providers of North East London and North Central London and West Essex agreed in July 2011 to develop an integrated cancer system in response to the requirements of London’s Strategic Health Authority and commissioners. Since April 2012 this integrated cancer system, London Cancer, has been commissioned to provide cancer services for a resident population of 3.2 million. Its mission is to drive superior outcomes and experience for our patients and local communities, and thereby position its staff as leaders in cancer care – locally, nationally and globally. London Cancer will be underpinned by patient-empowerment, research, evidence and information sharing. It will radically refocus hospitals into working in partnership with each other, primary care and patients, to deliver coordinated, comprehensive pathways of excellent care for every patient irrespective of where they access our system or the type of cancer that they have. The agreed priorities of the integrated cancer system are:
Being patient-focused through listening, communication, involvement, information, education, choice, and personalisation
Optimising care along a co-ordinated pathway – earlier diagnosis, exceptional treatment for all, local treatment where appropriate, compassionate aftercare and empowering/supporting patient self-management
Embedding research for personalised care, equitable access to trials, the discovery of new treatments and evaluating new ways of working together with patients
Increasing value – superior outcomes for patients per pound invested.

3
In addition to these priorities, London Cancer has carried out extensive research on what matters to patients and has distilled this work into ten key themes that will be central to everything that we do:
1. Diagnosis – patients are diagnosed at an earlier stage 2. Ethos – patients are treated holistically as individuals, and with dignity, sensitivity and respect, so that they do not feel that they are treated as a set of
cancer symptoms 3. Communication – patients receive written and verbal information about diagnosis and all treatment options, including side effects and quality of life
implications 4. Choice – patients and carers are fully involved in the choice of hospital and treatment options 5. Support – patients are given information on support groups, benefits entitlement and are offered emotional and psychosocial support 6. Carers – carers are fully involved and supported throughout the pathway 7. Holistic assessment – patients have holistic assessments at appropriate stages throughout the pathway, with action to meet their needs taken as a result 8. Seamless care – all patients are assigned a CNS when diagnosed and a community keyworker on discharge 9. Transport – patients should only travel when necessary and appropriate arrangements should be made for the immunosuppressed; patients should be
provided with free parking or transport vouchers 10. Discharge – patients and their GPs should be provided with discharge information and follow-up advice.
1.2. Pathway specifications
London Cancer will deliver a step-change in cancer services in North East London and North Central London and West Essex. It will do this through empowering clinicians and placing patients at the heart of cancer care. Clinically led pathway boards will be constituted for each cancer pathway and these boards will, under the leadership of a pathway director, lead service improvement and change across the pathway. The focus of pathway boards will be the whole patient pathway, including:
The diagnostic interface with the public
Primary care and accident and care in emergency departments
Initial assessment and appropriate rapid onward referral where necessary
The provision of various aspects of patient treatment
Follow-up or supporting end of life care. To instigate change pathway boards may constitute sub-groups, called technical groups, which are responsible for developing specifications for the future delivery of services along their pathways within the integrated cancer system. The organisations of London Cancer that contribute to the pathway will then be invited to demonstrate how they could meet the requirements of these specifications for the components of the pathway that they wish to provide. The London Cancer Urology Technical Group was the first to be constituted. It met during a four-month period between December 2011 and March 2012 to develop the specification for the future delivery of urological cancer services. A full list of those who sat on the group and the dates on which it met can be found in the appendix.
4
The resulting pathway specification was published internally to London Cancer in May 2012. In August trusts were invited to express their interest in hosting a local unit or specialist centre that met the specification. Following these expressions of interest, trusts were given further time to strengthen the clinical consensus on the proposed model and to try and achieve consensus on the location of the specialist centres. Consensus on the clinical model was achieved during these discussions in autumn 2012. It has been possible therefore to clarify the pathway specification in light of this consensus. This update has been carried out by the Urology Pathway Co-Directors and Pathway Manager. The update also provided opportunity to add further detail on key areas such as leadership and partnership working across the system as well as specialist MDT clinic, on-call and readmission arrangements.

5
2. Pelvic cancer pathway specification
Where a provider serves both as a local unit and specialist centre then it must meet both local unit and specialist centre specification.
POINT IN THE PATHWAY LOCAL PROSTATE/BLADDER UNIT SPECIALIST PROSTATE/BLADDER CENTRE
Leadership Named leader who takes responsibility for system-wide collaborative working to ensure availability of relevant specialist expertise at local units and equitable access to best practice and research
Implements the pathway across all providers
Demonstrates leadership in clinical and non-clinical innovations across the system
Maintains and develops the multidisciplinary team
Partnership working All providers work together in an integrated team
Demonstrates commitment to partnership when developing plans against the specification
All providers work together in an integrated team
Demonstrates commitment to partnership when developing plans against the specification
Primary care Makes specialist urological advice available to GPs by telephone and email
GPs use NICE 2-week urology referral criteria and London Cancer agreed forms and criteria
GPs use national guidelines for monitoring minor PSA rises
Diagnosis of cancer Adheres to agreed London Cancer diagnostic guidelines
Clinical nurse specialist present at all cancer diagnoses
Clinical workforce trained in advanced communication
Provides full written information about tumour type and treatment options through designated specialised staff skilled in counselling patients on treatment options
Rapid onward referral to specialist centre
Written confirmation of diagnosis and responsible consultant sent to GPs within 24 hours of patients being informed of new cancer diagnosis

6
POINT IN THE PATHWAY LOCAL PROSTATE/BLADDER UNIT SPECIALIST PROSTATE/BLADDER CENTRE
MDT Composition Local MDT with membership as per Peer Review measures
Weekly pelvic cancer-specific specialist MDT with professional constitution including:
Specialist surgeons
Specialist oncologists
Interventional radiologist
Organ-specific histopathologist
Clinical nurse specialist
Clinical trials nurses
Palliative care professional
MDT co-ordinator
Clinical nurse specialist
Provides access to a key worker for all patients (usually a clinical nurse specialist) who shares information freely with specialist centre
Clinical nurse specialists work as collective network across system
Provides access to a key worker for all patients (usually a clinical nurse specialist) who shares information freely and gives support and advice to referring unit
Clinical nurse specialists work as collective network across system
Holistic care Carries out holistic assessment, including palliative care and travel needs
Refers to appropriate cancer rehabilitation specialists
Carries out holistic assessment at key points in treatment pathway
Refers to appropriate cancer rehabilitation specialists
Information Capacity for reliable videoconferencing with specialist centre and other local units
Capacity for real-time electronic recording of discussions and decisions
Sends all MDT letters detailing decision and tests requested to GPs electronically (e.g. via systems such as Path Links)
Capacity for reliable videoconferencing with local units
Capacity for real-time electronic recording of discussions and decisions
Sends all MDT letters detailing decision and tests requested to GPs electronically (e.g. via systems such as Path Links)
Specialist MDT clinic Develops a network of multi-professional specialist MDT clinics across the system
Treatment decision
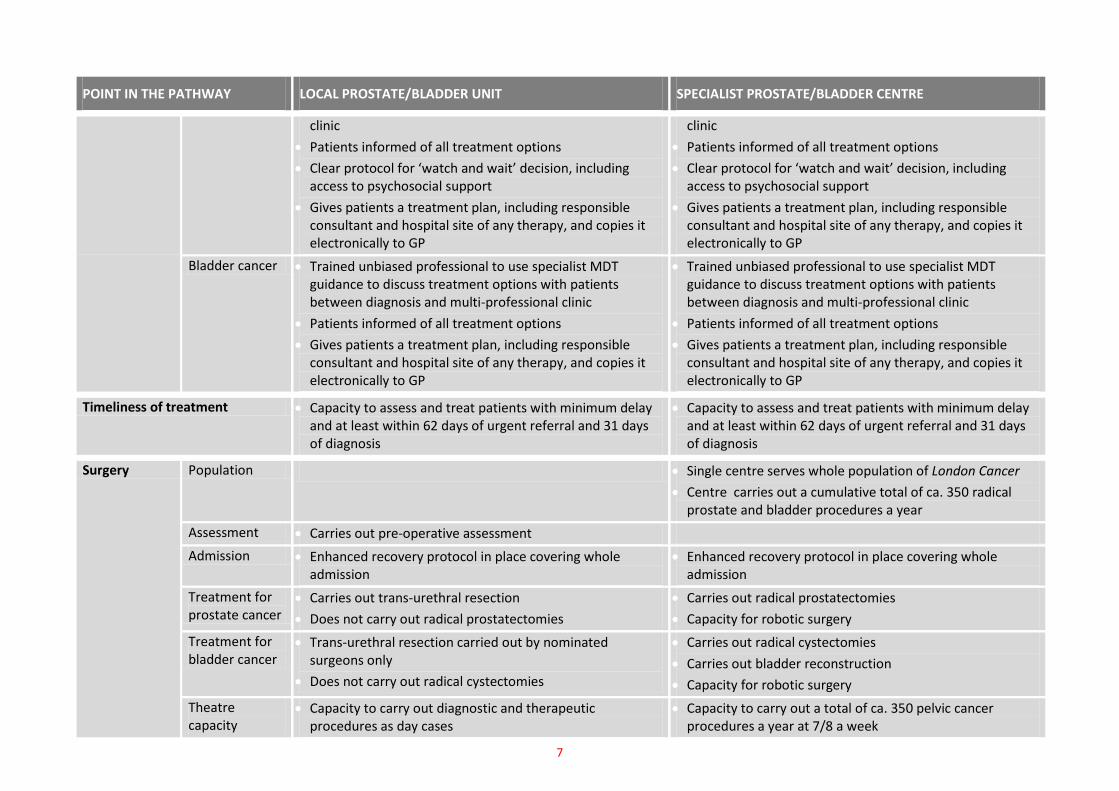
Prostate cancer Trained unbiased professional to use specialist MDT guidance to discuss treatment options with patients between diagnosis and multi-professional specialist MDT
Trained unbiased professional uses specialist MDT guidance to discuss treatment options with patients between diagnosis and multi-professional specialist MDT
7
POINT IN THE PATHWAY LOCAL PROSTATE/BLADDER UNIT SPECIALIST PROSTATE/BLADDER CENTRE
clinic
Patients informed of all treatment options
Clear protocol for ‘watch and wait’ decision, including access to psychosocial support
Gives patients a treatment plan, including responsible consultant and hospital site of any therapy, and copies it electronically to GP
clinic
Patients informed of all treatment options
Clear protocol for ‘watch and wait’ decision, including access to psychosocial support
Gives patients a treatment plan, including responsible consultant and hospital site of any therapy, and copies it electronically to GP
Bladder cancer Trained unbiased professional to use specialist MDT guidance to discuss treatment options with patients between diagnosis and multi-professional clinic
Patients informed of all treatment options
Gives patients a treatment plan, including responsible consultant and hospital site of any therapy, and copies it electronically to GP
Trained unbiased professional to use specialist MDT guidance to discuss treatment options with patients between diagnosis and multi-professional clinic
Patients informed of all treatment options
Gives patients a treatment plan, including responsible consultant and hospital site of any therapy, and copies it electronically to GP
Timeliness of treatment Capacity to assess and treat patients with minimum delay and at least within 62 days of urgent referral and 31 days of diagnosis
Capacity to assess and treat patients with minimum delay and at least within 62 days of urgent referral and 31 days of diagnosis
Surgery Population Single centre serves whole population of London Cancer
Centre carries out a cumulative total of ca. 350 radical prostate and bladder procedures a year
Assessment Carries out pre-operative assessment
Admission Enhanced recovery protocol in place covering whole admission
Enhanced recovery protocol in place covering whole admission
Treatment for prostate cancer
Carries out trans-urethral resection
Does not carry out radical prostatectomies
Carries out radical prostatectomies
Capacity for robotic surgery
Treatment for bladder cancer
Trans-urethral resection carried out by nominated surgeons only
Does not carry out radical cystectomies
Carries out radical cystectomies
Carries out bladder reconstruction
Capacity for robotic surgery
Theatre capacity
Capacity to carry out diagnostic and therapeutic procedures as day cases
Capacity to carry out a total of ca. 350 pelvic cancer procedures a year at 7/8 a week

8
POINT IN THE PATHWAY LOCAL PROSTATE/BLADDER UNIT SPECIALIST PROSTATE/BLADDER CENTRE
Inpatient care Capacity to carry out diagnostic and therapeutic procedures as day cases
Median lengths of stay of 2.5 days for radical prostatectomy and 12 days for radical cystectomy
Sufficient dedicated ring-fenced beds (estimated at 5 to 8 beds)
Capacity to deal with surgical readmissions efficiently and effectively within 24 hours of admission to local unit
Ward nursing capacity for level 1 patients
Intensive care capacity for median stay of 1 night for radical cystectomy
Provides access to specialist rehabilitation service adhering to NCAT rehab pathway
Skills and workforce
A minimum of 2 nominated surgeons to carry out transurethral resection of bladder
Dedicated team to carry out ca. 350 procedures a year across the system
Sufficient specialist pelvic surgeons
Consultant specialist pelvic surgical on-call rota (with no duties elsewhere)
Sufficient anaesthetists and skilled theatre teams
Enhanced recovery nurse
Co-locations Access to pelvic emergency surgeon
24-hour interventional radiology
Mandatory co-dependency with specialist gynaecological cancer surgery
Ablative therapies Provides ablative therapies or has a referral pathway to a site that does
Provides ablative therapies or has a referral pathway to a site that does
Specialist surgeon not required and delivery on specialist site not necessary
System-wide capacity for ca. 250 procedures a year on sites seeing sufficient volume to provide a critical mass
Systemic therapy
Treatment for prostate cancer
Delivers chemotherapy and hormone therapy where deemed appropriate by the specialist MDT
Issues patient-held records
Refers new cases of castrate-resistant prostate cancer for
Protocols to allow specialist management of patients with safe local delivery where appropriate
Delivers targeted therapy and hormone targeted therapy
Reviews all new cases of castrate-resistant prostate cancer
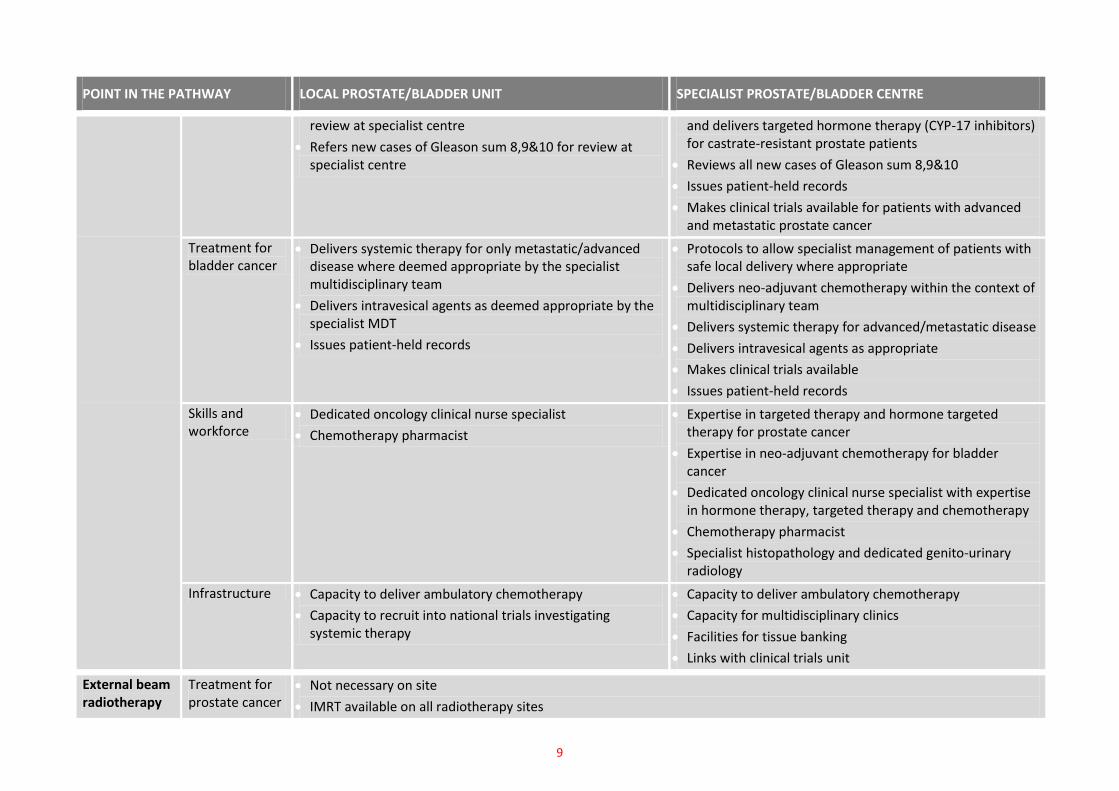
9
POINT IN THE PATHWAY LOCAL PROSTATE/BLADDER UNIT SPECIALIST PROSTATE/BLADDER CENTRE
review at specialist centre
Refers new cases of Gleason sum 8,9&10 for review at specialist centre
and delivers targeted hormone therapy (CYP-17 inhibitors) for castrate-resistant prostate patients
Reviews all new cases of Gleason sum 8,9&10
Issues patient-held records
Makes clinical trials available for patients with advanced and metastatic prostate cancer
Treatment for bladder cancer
Delivers systemic therapy for only metastatic/advanced disease where deemed appropriate by the specialist multidisciplinary team
Delivers intravesical agents as deemed appropriate by the specialist MDT
Issues patient-held records
Protocols to allow specialist management of patients with safe local delivery where appropriate
Delivers neo-adjuvant chemotherapy within the context of multidisciplinary team
Delivers systemic therapy for advanced/metastatic disease
Delivers intravesical agents as appropriate
Makes clinical trials available
Issues patient-held records
Skills and workforce
Dedicated oncology clinical nurse specialist
Chemotherapy pharmacist
Expertise in targeted therapy and hormone targeted therapy for prostate cancer
Expertise in neo-adjuvant chemotherapy for bladder cancer
Dedicated oncology clinical nurse specialist with expertise in hormone therapy, targeted therapy and chemotherapy
Chemotherapy pharmacist
Specialist histopathology and dedicated genito-urinary radiology
Infrastructure Capacity to deliver ambulatory chemotherapy
Capacity to recruit into national trials investigating systemic therapy
Capacity to deliver ambulatory chemotherapy
Capacity for multidisciplinary clinics
Facilities for tissue banking
Links with clinical trials unit
External beam radiotherapy
Treatment for prostate cancer
Not necessary on site
IMRT available on all radiotherapy sites

10
POINT IN THE PATHWAY LOCAL PROSTATE/BLADDER UNIT SPECIALIST PROSTATE/BLADDER CENTRE
Treatment for bladder cancer
Not necessary on site
Brachytherapy for prostate cancer
Referral Assesses suitability for brachytherapy
Written protocols for referral to brachytherapy centre(s)
Assesses suitability for brachytherapy
Written protocols for referral to brachytherapy centre(s )
Population Brachytherapy takes place in dedicated centre(s) with a minimum throughput of 50 patients per year
Brachytherapy centres do not need to be located with specialist prostate surgery centre(s)
Assessment Pre-operative assessment takes place at brachytherapy centre(s)
Treatment Takes place at brachytherapy centre(s)
Theatre capacity
System-wide capacity to carry out ca. 100 cases a year in dedicated brachytherapy theatre lists
Capacity to grow service as demand increases
Inpatient care – low dose rate
Median length of stay for low dose rate brachytherapy of 24 hours
Carries out morning lists to allow discharge on same day where possible
Dedicated radiation protection rooms for patients
Ward staff (including junior doctors) trained in radiation protection and radiation protection supervisor in place
Inpatient care – high dose rate
Median length of stay of 3 days for temporary high dose rate brachytherapy boost administered as a single fraction under spinal anaesthetic
No requirement for radiation protection on ward as applicators removed in theatre
Skills and workforce
Dedicated team(s) to carry out ca. 100 procedures a year system-wide
Brachytherapy centres have:
A minimum of 2 trained radiation oncologists
A training specialist registrar in clinical oncology
A minimum of 2 trained radiologists or urologists
A urologist specialised in dealing with urological complications following brachytherapy
A clinical nurse specialist
A minimum of 3 trained physicists or dosimetrists (one of whom should be a trained radiation supervisor)
Trained theatre staff
Co-locations Access to radiation physics and urology
High dose rate brachytherapy for prostate co-located with brachytherapy procedures for other tumour types due to equipment

11
POINT IN THE PATHWAY LOCAL PROSTATE/BLADDER UNIT SPECIALIST PROSTATE/BLADDER CENTRE
Acute oncology Full acute oncology service that meets Peer Review standards
Full acute oncology service that meets Peer Review standards
Post-treatment
Discharge Clear procedures for receipt of patients discharged from care of the centre
Provides electronic end of treatment summaries with accessible record of treatment for GPs and patients
Discharge carried out by skilled professionals
Provides electronic end of treatment summaries with accessible record of treatment for local units, GPs and patients
Ability to readmit any patient with a complication within 24 hours of presentation to a local provider
Follow-up for prostate cancer
Capacity to host specialist outreach clinics Not necessary for patients to return to specialist centre after treatment
Follow-up for bladder cancer
Care for patients once discharged from specialist centres Follows up patients who have undergone radical cystectomy for up to 2 years before transferring care to local units
Follows up patients who have undergone neo-bladder reconstruction for up to 3 years
Primary care
Follows NICE guidance on transferring prostate follow-up to primary care
Provides GP with clear details of primary care follow-up required for prostate patients
Provides primary care with clear details of how to reaccess secondary care
Follows NICE guidance on transferring prostate follow-up to primary care
Provides GP with clear details of primary care follow-up required for prostate patients
Provides primary care with clear details of how to reaccess secondary care
Palliative care
Clear referral pathways for patients with palliative and specialist palliative care needs
Clear referral guidance for management of:
End of life care
Complex symptom control
GP and palliative care team to manage patient as appropriate
Clear referral pathways for patients with palliative and specialist palliative care needs
Clear referral guidance for management of:
End of life care
Complex symptom control
GP and palliative care team to manage patient as appropriate

12
POINT IN THE PATHWAY LOCAL PROSTATE/BLADDER UNIT SPECIALIST PROSTATE/BLADDER CENTRE
Research and innovation Access to multidisciplinary oncology service including:
Clinical trial research
Research nursing
Carries out prospective audit of service and publishes transparent outcomes data
Access to multidisciplinary oncology service including:
Tissue banking
Clinical trial research
Research nursing
Carries out prospective audit of service and publishes transparent outcomes data
Education and training Offers simulation training in new surgical techniques
Conducts training in delivery of systemic therapy
Patient travel Informs patients of support available for travel to specialist centre and radiotherapy units
Robust patient travel plan in place
13
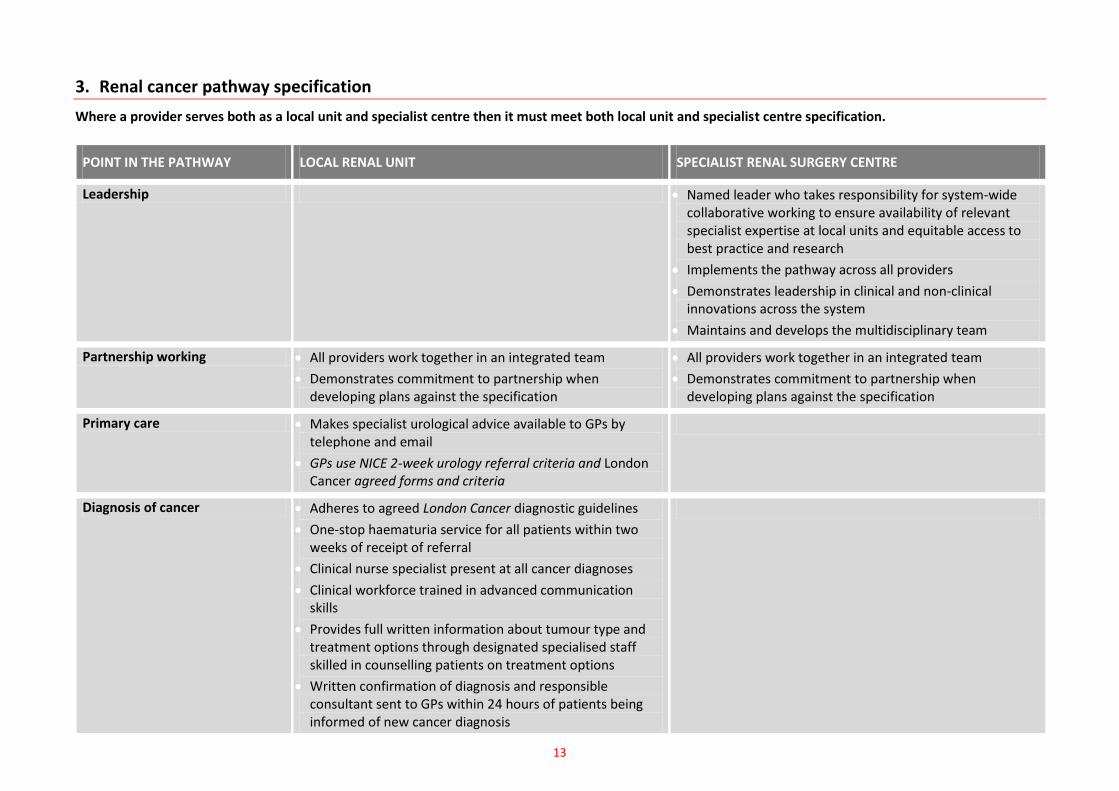
3. Renal cancer pathway specification
Where a provider serves both as a local unit and specialist centre then it must meet both local unit and specialist centre specification.
POINT IN THE PATHWAY LOCAL RENAL UNIT SPECIALIST RENAL SURGERY CENTRE
Leadership Named leader who takes responsibility for system-wide collaborative working to ensure availability of relevant specialist expertise at local units and equitable access to best practice and research
Implements the pathway across all providers
Demonstrates leadership in clinical and non-clinical innovations across the system
Maintains and develops the multidisciplinary team
Partnership working All providers work together in an integrated team
Demonstrates commitment to partnership when developing plans against the specification
All providers work together in an integrated team
Demonstrates commitment to partnership when developing plans against the specification
Primary care Makes specialist urological advice available to GPs by telephone and email
GPs use NICE 2-week urology referral criteria and London Cancer agreed forms and criteria
Diagnosis of cancer Adheres to agreed London Cancer diagnostic guidelines
One-stop haematuria service for all patients within two weeks of receipt of referral
Clinical nurse specialist present at all cancer diagnoses
Clinical workforce trained in advanced communication skills
Provides full written information about tumour type and treatment options through designated specialised staff skilled in counselling patients on treatment options
Written confirmation of diagnosis and responsible consultant sent to GPs within 24 hours of patients being informed of new cancer diagnosis

14
POINT IN THE PATHWAY LOCAL RENAL UNIT SPECIALIST RENAL SURGERY CENTRE
Rapid onward referral to specialist centre, including for patients with ultrasound with incidental findings
MDT Composition Local MDT with membership as per Peer Review measures Weekly renal specific specialist multidisciplinary team with professional constitution including:
Specialist upper tract surgeons
Specialist upper tract oncologists
Specialist clinical oncologists
Interventional radiologist
Organ specific histopathologist
Clinical nurse specialist
Nephrologists/renal physicians
Clinical trials nurses
Palliative care professional
MDT co-ordinator
Clinical nurse specialist
Provides access to a key worker for all patients (usually a clinical nurse specialist) who shares information freely with specialist centre
Clinical nurse specialists work as collective network across system
Provides access to a key worker for all patients (usually a clinical nurse specialist) who shares information freely and gives support and advice to referring unit
Clinical nurse specialists work as collective network across system
Holistic care
Carries out holistic assessment, including palliative care and travel needs
Refers to appropriate cancer rehabilitation specialists
Carries out holistic assessment at key points in treatment pathway
Refers to appropriate cancer rehabilitation specialists
Information
Capacity for reliable videoconferencing with specialist centre and other local units
Capacity for real-time electronic recording of discussions and decisions
Sends all MDT letters detailing decision and tests requested to GPs electronically (e.g. via systems such as Path Links)
Capacity for reliable videoconferencing with local units
Capacity for real-time electronic recording of discussions and decisions
Sends all MDT letters detailing decision and tests requested to GPs electronically (e.g. via systems such as Path Links)

15
POINT IN THE PATHWAY LOCAL RENAL UNIT SPECIALIST RENAL SURGERY CENTRE
Specialist MDT clinic Develops a network of multi-professional specialist MDT clinics across the system
Treatment decision Trained unbiased professional to use specialist MDT guidance to discuss treatment options with patients between diagnosis and multi-professional specialist MDT clinic
Patients informed of all treatment options
Gives patients a treatment plan, including responsible consultant and hospital site of any therapy, and copies it electronically to GP
Trained unbiased professional to use specialist MDT guidance to discuss treatment options with patients between diagnosis and multi-professional specialist MDT clinic
Patients informed of all treatment options
Gives patients a treatment plan, including responsible consultant and hospital site of any therapy, and copies it electronically to GP
Timeliness of treatment Capacity to assess and treat patients with minimum delay and at least within 62 days of urgent referral and 31 days of diagnosis
Capacity to assess and treat patients with minimum delay and at least within 62 days of urgent referral and 31 days of diagnosis
Surgery Assessment Carries out pre-operative assessment
Admission Enhanced recovery protocol covers whole admission Enhanced recovery protocol covers whole admission
Treatment of T1 and T2 disease
Does not carry out partial nephrectomies (nephron-sparing surgery) or nephro-ureterectomies
May carry out radical nephrectomies as agreed by specialist MDT and performed by specialist surgeons (i.e. those treating T3 and T4 disease at specialist centre)
Carries out appropriate surgery, including all nephron-sparing surgery and nephro-ureterectomies, with specialist team
Capacity for robotic surgery
Treatment of T3 and T4 disease
Carries out palliative treatments only Carries out appropriate surgery with specialist team
Capacity for robotic surgery
Benign disease Capacity to carry out surgery on complex benign renal disease (up to 100 cases per year)
Theatre capacity Capacity to carry out local radical nephrectomy, where appropriate
Capacity to carry out a total of ca. 400 procedures a year at 10 a week (includes up to 100 benign cases)
Inpatient care Capacity to care for patients following local radical nephrectomy, where appropriate
Median length of stay of 3.5 days for nephrectomy
Sufficient dedicated ring-fenced beds (estimated at 8 to 10 beds)
Capacity to deal with surgical readmissions efficiently and
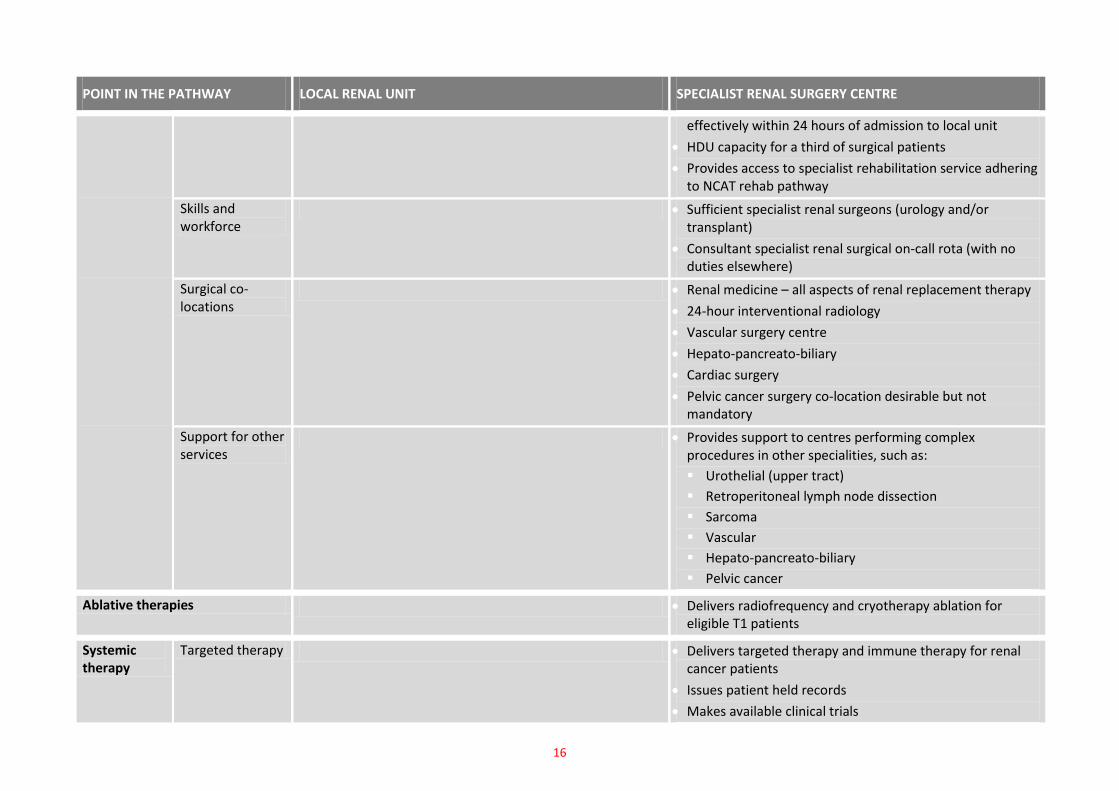
16
POINT IN THE PATHWAY LOCAL RENAL UNIT SPECIALIST RENAL SURGERY CENTRE
effectively within 24 hours of admission to local unit
HDU capacity for a third of surgical patients
Provides access to specialist rehabilitation service adhering to NCAT rehab pathway
Skills and workforce
Sufficient specialist renal surgeons (urology and/or transplant)
Consultant specialist renal surgical on-call rota (with no duties elsewhere)
Surgical co-locations
Renal medicine – all aspects of renal replacement therapy
24-hour interventional radiology
Vascular surgery centre
Hepato-pancreato-biliary
Cardiac surgery
Pelvic cancer surgery co-location desirable but not mandatory
Support for other services
Provides support to centres performing complex procedures in other specialities, such as:
Urothelial (upper tract)
Retroperitoneal lymph node dissection
Sarcoma
Vascular
Hepato-pancreato-biliary
Pelvic cancer
Ablative therapies Delivers radiofrequency and cryotherapy ablation for eligible T1 patients
Systemic therapy
Targeted therapy Delivers targeted therapy and immune therapy for renal cancer patients
Issues patient held records
Makes available clinical trials
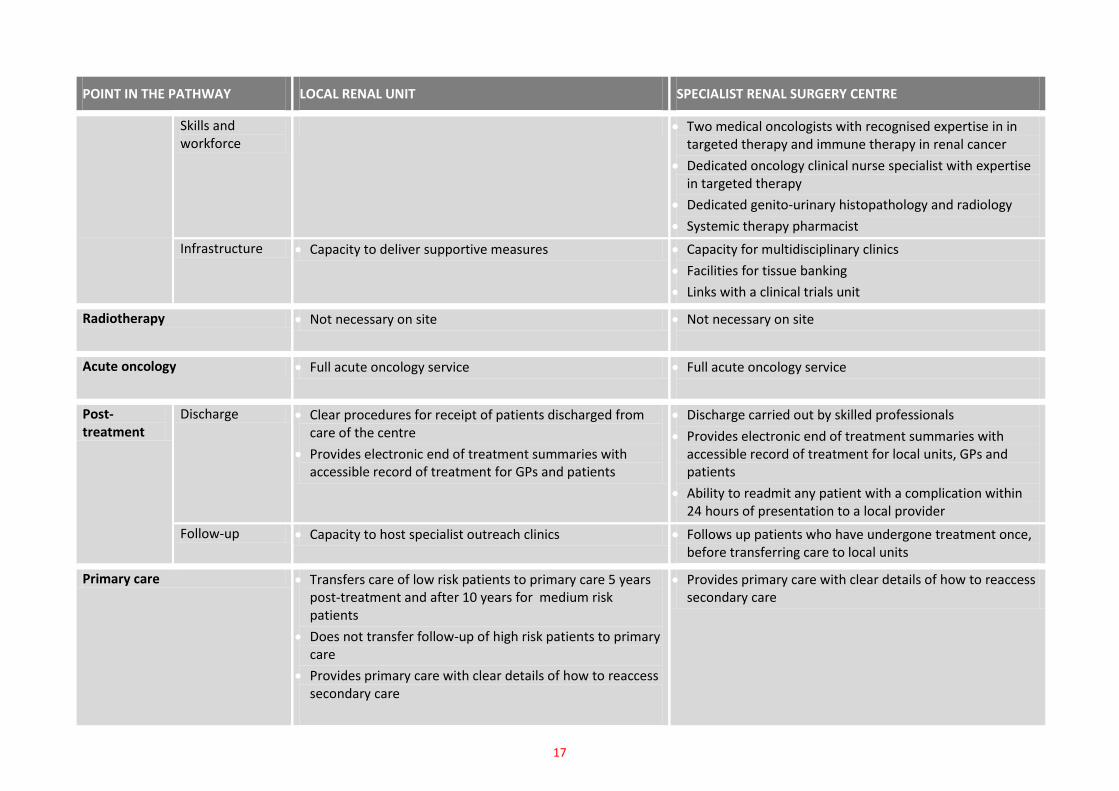
17
POINT IN THE PATHWAY LOCAL RENAL UNIT SPECIALIST RENAL SURGERY CENTRE
Skills and workforce
Two medical oncologists with recognised expertise in in targeted therapy and immune therapy in renal cancer
Dedicated oncology clinical nurse specialist with expertise in targeted therapy
Dedicated genito-urinary histopathology and radiology
Systemic therapy pharmacist
Infrastructure Capacity to deliver supportive measures Capacity for multidisciplinary clinics
Facilities for tissue banking
Links with a clinical trials unit
Radiotherapy Not necessary on site Not necessary on site
Acute oncology Full acute oncology service Full acute oncology service
Post-treatment
Discharge Clear procedures for receipt of patients discharged from care of the centre
Provides electronic end of treatment summaries with accessible record of treatment for GPs and patients
Discharge carried out by skilled professionals
Provides electronic end of treatment summaries with accessible record of treatment for local units, GPs and patients
Ability to readmit any patient with a complication within 24 hours of presentation to a local provider
Follow-up Capacity to host specialist outreach clinics Follows up patients who have undergone treatment once, before transferring care to local units
Primary care Transfers care of low risk patients to primary care 5 years post-treatment and after 10 years for medium risk patients
Does not transfer follow-up of high risk patients to primary care
Provides primary care with clear details of how to reaccess secondary care
Provides primary care with clear details of how to reaccess secondary care
18
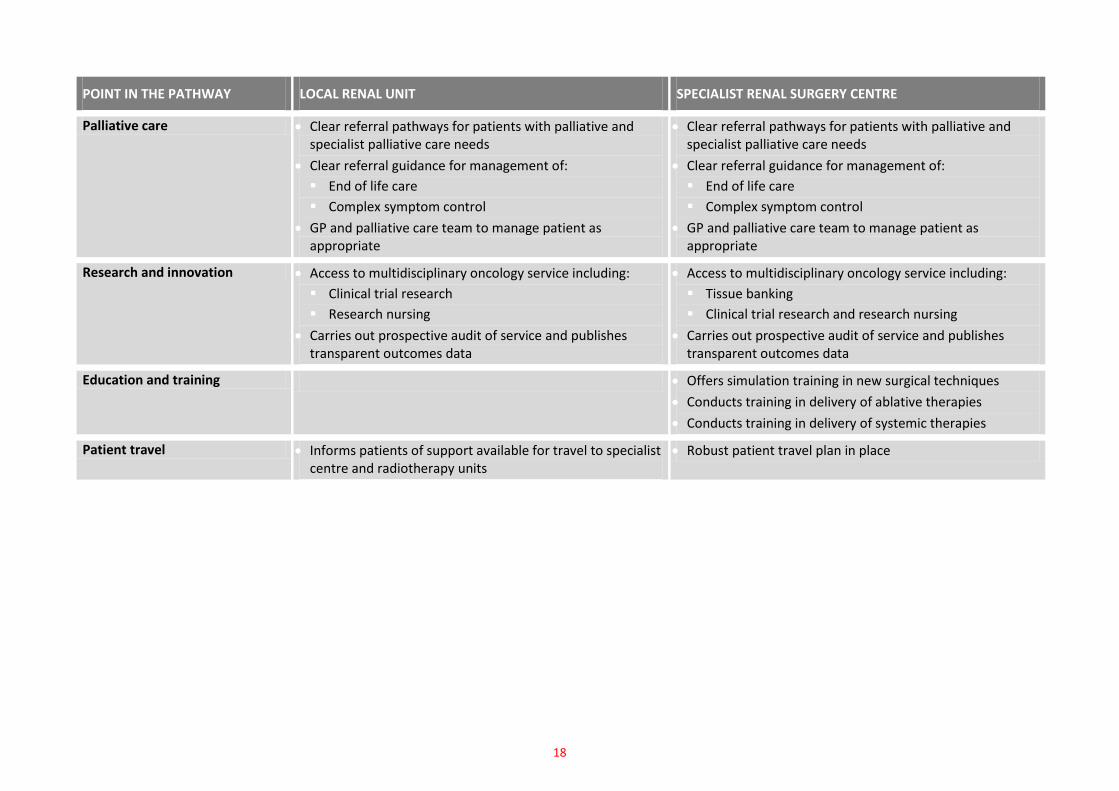
POINT IN THE PATHWAY LOCAL RENAL UNIT SPECIALIST RENAL SURGERY CENTRE
Palliative care Clear referral pathways for patients with palliative and specialist palliative care needs
Clear referral guidance for management of:
End of life care
Complex symptom control
GP and palliative care team to manage patient as appropriate
Clear referral pathways for patients with palliative and specialist palliative care needs
Clear referral guidance for management of:
End of life care
Complex symptom control
GP and palliative care team to manage patient as appropriate
Research and innovation Access to multidisciplinary oncology service including:
Clinical trial research
Research nursing
Carries out prospective audit of service and publishes transparent outcomes data
Access to multidisciplinary oncology service including:
Tissue banking
Clinical trial research and research nursing
Carries out prospective audit of service and publishes transparent outcomes data
Education and training Offers simulation training in new surgical techniques
Conducts training in delivery of ablative therapies
Conducts training in delivery of systemic therapies
Patient travel Informs patients of support available for travel to specialist centre and radiotherapy units
Robust patient travel plan in place
19
Appendix: London Cancer Urology Technical Group
London Cancer Urology Technical Group attendees
John Hines (Co-chair), Consultant Urologist, Whipps Cross University Hospital NHS Trust and London Cancer Urology Pathway Co-Director
Mark Emberton (Co-chair), Consultant Urological Surgeon, University College London Hospitals NHS Foundation Trust and London Cancer Urology Pathway Co-Director
Anand Kelkar, Consultant Urological Surgeon, Barking Havering and Redbridge Hospitals NHS Trust
Angela Lee, Clinical Nurse Specialist, Barking Havering and Redbridge Hospitals NHS Trust
Bruce Turner, Uro-oncology Nurse Practitioner, Homerton University Hospital NHS Foundation Trust
Colin Bunce, Consultant Urological Surgeon, Barnet and Chase Farm Hospitals NHS Trust
David Nicol, Consultant Urologist, The Royal Free Hampstead NHS Trust and University College London Hospitals NHS Foundation Trust
Faiz Mumtaz, Consultant Urologist, Barnet and Chase Farm Hospitals NHS Trust
Frank Chinegwundoh, Consultant Urological Surgeon, Newham University Hospital NHS Trust
Gillian Smith, Consultant Urological Surgeon, The Royal Free Hampstead NHS Trust
Guy Webster, Consultant Urologist, Barnet and Chase Farm Hospitals NHS Trust
Jaspal Virdi, Consultant Urological Surgeon, The Princess Alexandra Hospital NHS Trust
Jhumur Pati, Consultant Urological Surgeon, Homerton University Hospital NHS Foundation Trust
John Peters, Consultant Urologist, Whipps Cross University Hospital NHS Trust
Katharine Pigott, Consultant Clinical Oncologist, The Royal Free Hampstead NHS Trust
Maneesh Ghei, Consultant Urologist, The Whittington Hospital NHS Trust
Rateb Samman, Consultant Urologist, The Princess Alexandra Hospital NHS Trust
Sandeep Gujral , Consultant Urological Surgeon, Barking Havering and Redbridge Hospitals NHS Trust
Tim Briggs, Consultant Urologist, Barnet and Chase Farm Hospitals NHS Trust
Tom Powles, Consultant Medical Oncologist, Barts and the London NHS Trust
Patient representative input from:
Christopher Kennedy, Patient
Steve Johnson, Patient
Primary care input from:
Karen Sennet, General Practitioner, Islington
Mike Gocman, General Practitioner, Enfield
Palliative care input from:
Adrian Tookman, Consultant Physician in Palliative Medicine, The Royal Free Hampstead NHS Trust
Clare Phillips, Consultant in Palliative Medicine, Barts and the London NHS Trust and Newham University Hospital NHS Trust
London Cancer Urology Technical Group meeting dates
2nd December 2011 19th January 2012 20th February 2012 26th March 2012