lowering mortality of acs with optimal therapy: doing it...
TRANSCRIPT

Lowering Mortality ofACS with Optimal Therapy:
Doing It Right from the Start
dr. Berlian Idriansyah Idris, SpJP(K), FIHA, MPH, DSc
RSUD Kota Tangerang

ACUTE CORONARY SYNDROME
Spectrum of clinical syndromes due to sudden, significantly compromised coronary circulation due to thrombosis, ranging from unstable angina to NSTEMI and STEMI.
Topol EJ, ed. Textbook of cardiovascular medicine 2007.
Hamm CW et al. Eur Heart J 2011;32:2999 – 3054
Acute thrombosis induced by a ruptured or eroded atherosclerotic coronary plaque, causing a sudden and critical reduction in blood flow

Normal
vessel
Minimal
CAD
Severe
CAD
Moderate
CAD
Progression
Pathophysiology

Autopsy
Stable plaque
Davies MJ. Heart 2000;83;361-366.
Thrombosis caused by erosion
Thrombosis caused by disruption
Thrombosis caused
by disruption

Cardiovascular
disease
Cerebrovascular
disease
PAD
24.7%
3.8% 11.8%
29.9%
3.3%
7.4%
19.2% A total of ~26% of patients
had manifestations of
atherothrombosis in
more than one arterial bed
26.2%†
Coccheri S. Eur Heart J 1998;19(Suppl):227.
Atherothrombosis is often found in more than one
arterial bed*
*Data from the Clopidogrel versus Aspirin in Patients
at Risk of Ischemic Events (CAPRIE) study (n=19,185)
†Total does not add up because of rounding
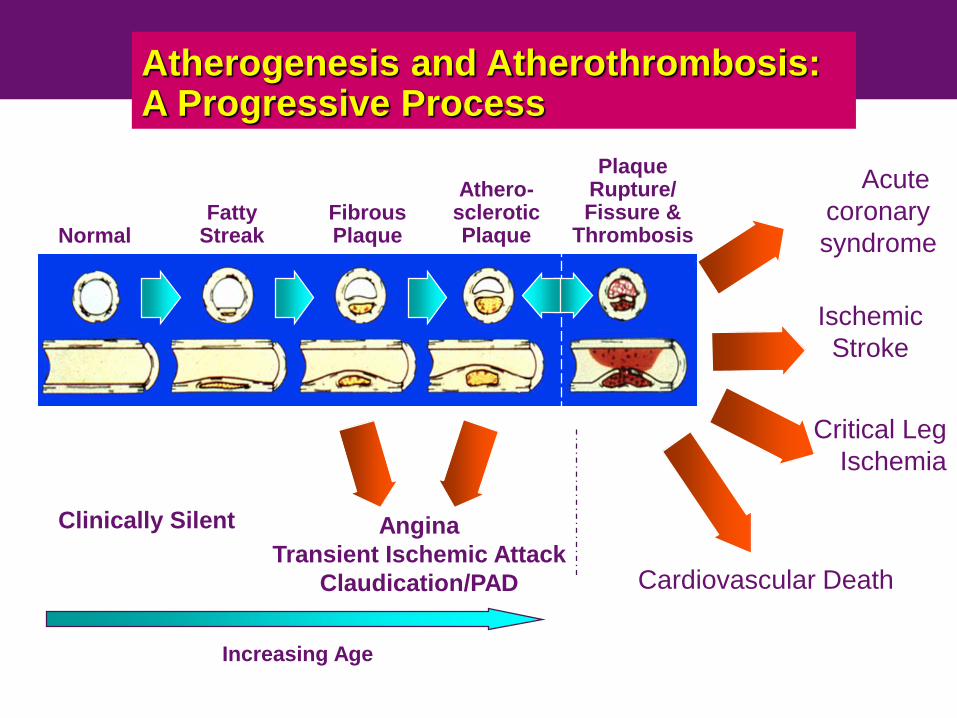
Atherogenesis and Atherothrombosis: A Progressive Process
NormalFatty
StreakFibrousPlaque
Athero-scleroticPlaque
PlaqueRupture/Fissure &
Thrombosis
Acute
coronary
syndrome
Ischemic
Stroke
Critical Leg
Ischemia
Clinically Silent
Cardiovascular Death
Increasing Age
Angina
Transient Ischemic Attack
Claudication/PAD

~1 IN 5 mortality in 5 years from index event:
2010 Global Registry
GRACE study: Analysis of UK and Belgian patients with ACS (n=3721)
Of the patients who died, death occurred post-discharge in 68%, 86% and 97% of STEMI, NSTEMI and UA patients, respectively. ACS, acute coronary
syndromes; GRACE, Global Registry of Acute Coronary Events; MI, myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI,
ST-segment elevation myocardial infarction; UA, unstable angina.
Fox KA et al. Eur Heart J 2010;31:2755–2764.

Activated platelets are central to
thrombus formation in ACS
• Platelets do 3 things that promote thrombus formaton
– Adhesion
– Activation
– Aggregation
Plaque rupture leads
to platelet adhesion
to the exposed
subendothelium
Adherent platelet become activated
Activated platelets aggregate
and assemble a critical mass
of activated, pro-thrombotic
platelet membrane at the site
of injury
2
1
3
Vorchheimer DA, et al. Mayo Clin Proc. 2006;81:59-68; Davies MJ. Heart. 2000;83:361-366.
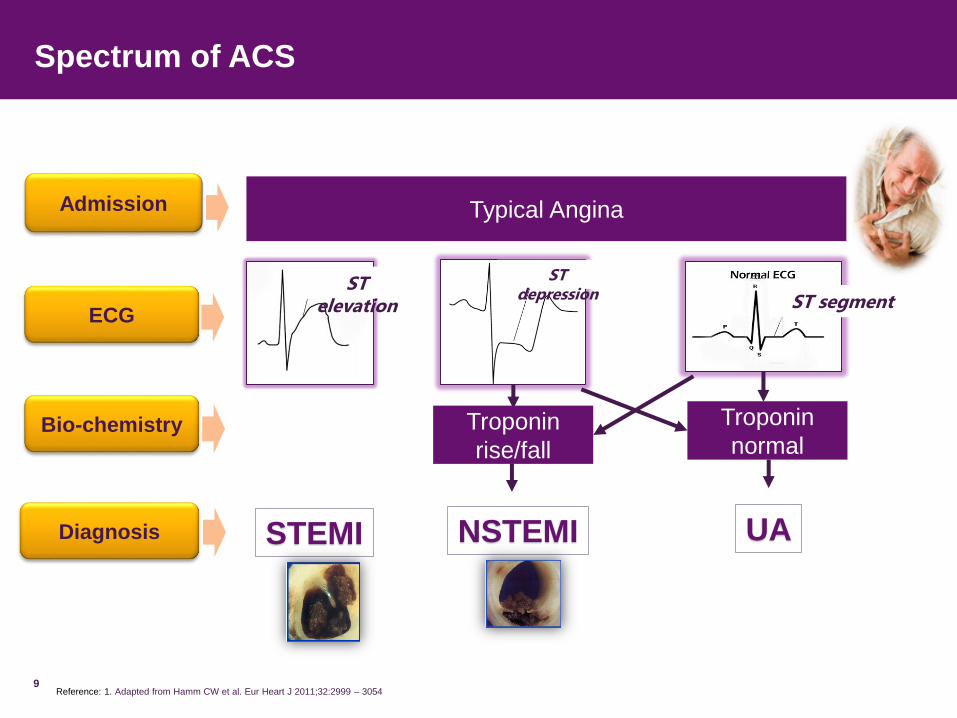
Spectrum of ACS
9Reference: 1. Adapted from Hamm CW et al. Eur Heart J 2011;32:2999 – 3054
Admission
ECG
Bio-chemistry
Diagnosis STEMI NSTEMI
ST segment
ST depression
ST elevation
UA
Typical Angina
Troponin
rise/fall
Troponin
normal

Clinical classification of chest pain
Typical angina (definite)
• Substernal chest discomfort with a characteristic quality and duration that is
• provoked by exertion or emotional stress and
• relieved by rest or nitroglycerin
Atypical angina (probable)
• meets 2 of the above characteristics
Noncardiac chest pain
• meets <=1 of the typical angina characteristics
10Diamond GA. J Am Coll Cardiol 1983;1:574

Management
• Monitor and support ABCs
• Check vital signs, including oxygen saturation
• Establish IV access
• Administer
– Oxygen 4L/min
– Aspirin 160-325 mg chewed
– Clopidogrel loading dose 300 mg or ticagrelor 180 mg
– NTG (ISDN) sublingual and intravenous if needed
– Morphine if pain not relieved with NTG
– Anticoagulant: UFH/enoxaparine/fondaparinux
• Urgent reperfusion as indicated in STEMI: fibrinolytic or primary PCI
11

Antiplatelet Agent


Metabolism P2Y12 inhibitor
(Pro drug vs active drug)
*Prasugrel is not yet approved and available in Indonesia Figure adapted from Schömig A (2009). CYP, cytochrome P450.
Schömig A. N Engl J Med 2009;361:1108–1111.
Binding
P2Y12
Platelet
No in vivo
biotransformation
Ticagrelor
(Active Drug)
Prasugrel*
(Prodrug)
Clopidogrel
(Prodrug)
CYP-dependent
oxidation
CYP3A4/5
CYP2B6
CYP2C19
CYP2C9
CYP2D6Hydrolysis
by esterase
CYP-dependent
oxidation
CYP1A2
CYP2B6
CYP2C19
CYP-dependent
oxidation
CYP2C19
CYP3A4/5
CYP2B6
Active compound
Intermediate metabolite
Pro-drug

CYP2C19 Polymorphisms
Ultrarapidmetabolizer
Intermediate Metabolizer
Poor Metabolizer
Reduced response of “pro drug” agent
Prevalence of Poor Metabolizer is higher in Asian 2 – 5% in Caucasian 4 – 8 % of african 11 - 12% of Asian
Sukasem C et al. Pharmacogenomics and
Personalized Medicine 2013:6 85–91
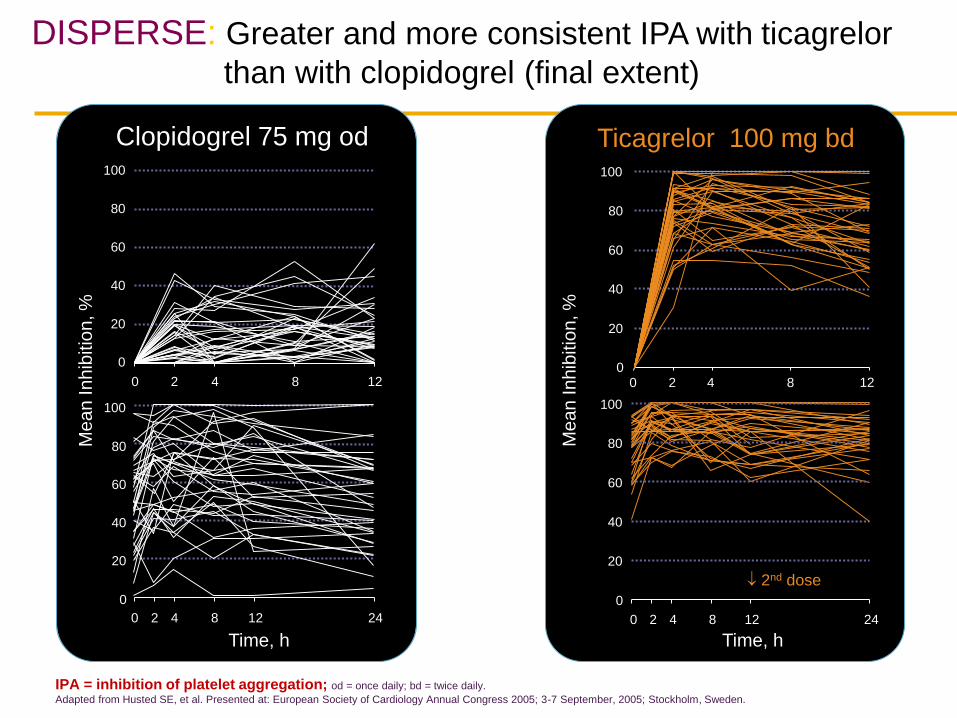
IPA = inhibition of platelet aggregation; od = once daily; bd = twice daily.
Adapted from Husted SE, et al. Presented at: European Society of Cardiology Annual Congress 2005; 3-7 September, 2005; Stockholm, Sweden.
DISPERSE: Greater and more consistent IPA with ticagrelor
than with clopidogrel (final extent)
Time, h
Clopidogrel 75 mg od
Me
an
In
hib
itio
n, %
Ticagrelor 100 mg bd
DAY 1
DAY 14
Time, h
Me
an
In
hib
itio
n, %
0
20
40
60
80
100
0 2 4 8 12
0
20
40
60
80
100
0 2 4 8 12
0
20
40
60
80
100
0 2 4 8 12 24
0
20
40
60
80
100
0 2 4 8 12 24
2nd dose

Onset P2Y12 inhibitor
Ticagrelor provide Faster Onset and offset vs high dose clopidogrel
IPA : Inhibition of Platelet Aggregation
Onset
100
90
80
70
60
50
40
30
20
10
0
IPA
%
Ticagrelor (n=54)
Clopidogrel (n=50)
0 0.5 1 2 4 8 24 6 weeks 0 2 4 8 24 48 72 120 168 240
Maintenance OffsetTime (hours))
Loading Dose
TICA 180 mg
CLO 600 mg
*
** * *
‡
†
** †
Last maintenance dose
TICA 90 mg bid
CLOPI 75 mg qd
** * P<0,0001
† P<0,005‡ P<0,05
Time (hours)
Catatan : penelitian ini dilakukan pada pasien CAD yang
mengkonsumsi aspirin tanpa riwayat ACS <1 tahun
Ticagrelor belum mendapatkan persetujuan untuk populasi
pasien ini.
18
Referensi Adapted from Gurbel PA, et al. Circulation. 2009;120:2577–2585.
41% ticagrelorVs.
8% clopidogrel
At 30 minutes
88% ticagrelorVs.
38% clopidogrel
At 2 hours
8

Balance between antiplatelet effect and bleeding risk

Balancing risk and benefit
INHIBITION OF PLATELET AGGREGATION
RIS
K O
F A
NY
EV
ENT
RIS
K O
F A
NY
EV
ENT
High Risk of Ischemic Event High Risk of Bleeding Event“Sweet Spot”
Ischemic risk Bleeding risk
Ferreiro Jl, Sibbing D, Angiolillo DJ. Thromb Haemost 2010; 103: 1128–1135

Factors Associated with Increased Ischemic and Bleeding Risk

PLATO Study
PLATO Study:
• 43 countries
• 862 sites
• 18,624 patients
43 countries862 sites
PLATO study tested the hypothesis that…
ticagrelor will result in a lower risk of recurrent thrombotic events in a broad
patient population with ACS as compared to clopidogrel and this would be
achieved with a clinically acceptable bleeding rate and overall safety profile
18,624 patients
Wallentin L, et al. N Engl J Med. 2009;361:1045–1057.

PLATO Trial: Reduction CV event of ticagrelor starts early and
continue until 12 months in ACS Patients vs. clopidogrel1
Reference: 1. Wallentin L, et al. N Engl J Med. 2009;361:1045–1057.
No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
Months After Randomization
8,521
8,628
8,362
8,460
8,124 6,650
6,743
5,096
5,161
4,047
4,1478,219
0 2 4 6 8 10 12
12
11
10
9
8
7
6
5
4
3
2
1
0
13
Cu
mu
lati
ve
In
cid
en
ce
of
(Co
mp
osit
e o
f
CV
De
ath
, M
I, o
r S
tro
ke
) %
11.7 Clopidogrel
9.8 Ticagrelor
HR: 0.88 (95% CI, 0.77−1.00); P=0.045
0–30 Days
4.8
5.4
Clopidogrel
Ticagrelor
0–12 Months
at 1 month
ARR=0.6%
RRR=12%
HR: 0.84 (95% CI, 0.77–0.92); P<0.001
at 12 months
ARR=1.9%
RRR=16%

Benefit CV Mortality P2Y12 Inhibitor
5.50 5.10
Plasebo Clopidogrel
CURE1
2.40 2.10
Clopidogrel Prasugrel *
TRITON TIMI 382
5.10
4.00
Clopidogrel Ticagrelor
PLATO3
P = NS
n = 12.562
NNT = 250
n = 13.608
NNT = 333
n = 18.624
NNT = 91
1.Yusuf S et al. N Engl J Med 2001;345; 2.Wiviott SD e tal. N Engl J Med 2007;357:2001-15; 3.Wallentin L, et al. N Engl J Med. 2009;361:1045–1057.
* Prasugrel is not yet approved and available in Indonesia
Rate
of C
V d
ea
th (
%)
Rate
of co
mp
osite C
V d
ea
th (
%) P = N/A P = 0.001

Real World Evidence DAPT in ACS
• Outcomes in Patients Treated With Ticagrelor
or Clopidogrel After Acute Myocardial
Infarction: Experiences From SWEDEHEART
Registry (The PRACTICAL study) Anders Sahlén, Christoph Varenhorst, Bo Lagerqvist, Henrik Renlund,
Elmir Omerovic, David Erlinge, Lars Wallentin, Stefan James, Tomas Jernberg
Referensi: 1. Salhén A et al. Eur Heart J 2016; 37; 3335 - 3342 14

PRACTICAL Study :Consistent effectiveness Ticagrelor in ACS showed in real-world setting1
Reduce
15%vs.
Clopidogrel
Cu
mu
lati
ve
in
cid
en
ce
Time (days)
0 100 200 300 365
0.00
0.02
0.04
0.06
0.08
0.10Clopidogrel
Ticagrelor 90 mg
Ticagrelor
90 mgClopidogrel
HR adjusted
(complete cases)*
95% confidence
interval
4.43% 3.85%1.178
(0.994–1.396)
All-cause death, MI or strokeBleeding requiring
hospitalization at 12 months
(sensitivity analysis)3
HR 0.85. 95% CI (0.77-0.94)
Referensi: 1. Salhén A et al. Eur Heart J 2016; 37; 3335 - 3342
45,073 consecutive patients who survived an acute MI
15

ESC STEMI 2017
Ticagrelor is preferred OAP before clopidogrel

28
ESC NSTEACS 2015:
Ticagrelor is preferred OAP before clopidogrel
A P2Y12 inhibitor is recommended, in addition to aspirin, for 12 months
unless there are contraindications such as excessive risk of bleeds.
Ticagrelor is recommended, in the absence of contraindications,
for all patients at moderate-to-high risk of ischaemic events (e.g.
elevated cardiac troponins), regardless of initial treatment strategy
and including those pretreated with clopidogrel (which should be
discontinued when ticagrelor is started).
Prasugrel is recommended in patients who are proceeding to PCI if
no contraindication).
Clopidogrel is recommended for patients who cannot receive
ticagrelor or prasugrel or who require oral anticoagulation.
1B
1B
1B
1A
Roffi M et al. Eur Heart J 2016;37(3):267-315

29
Summary
•ACS is a fatal condition, mortality is still high
•Platelet plays important role in
atherothrombosis pathophysiology of ACS
•Agressively treating atherothrombosis from
the start is the hallmark of therapy, while
taking into account bleeding bleeding risk
•Recent guidelines prefer ticagrelor for ACS
patients with better efficacy and similar safety
profile

THANK YOU…
30
31
• Thank you

Key Question
32
Switching DAPT in ACS, how ?
Bleeding with OAP, how to prevent and manage ?
How long DAPT ?

SWITCHING RECOMMENDATION BASED ON STEMI 2017
Valgimigli Marco et al. Europan Heart Journal . 2017;0: 1-48

PLATO Study : Switch in Acute from Ticagrelor to
Clopidogrel is allowed
Characteristic Ticagrelor
(n=9333)
Clopidogrel
(n=9291)
P value
Start of randomized treatment , %
Time after start of chest pain (hours) median 11.3 11.3 0.89
Time after start of hospitalization (hours), median 4.9 5.3 0.75
Clopidogrel start-up
Clopidogrel in hospital before randomization, n (%) 4293 (46.0) 4282 (46.1) 0.91
Clopidogrel dose given within 24 h before or after randomization, n (%) 0.65
No loading dose or missing information 4937 (52.9) 94 (1.0)
300-375 mg 1921 (20.6) 5528 (59.5)
600-675 mg 1282 (13.7) 1822 (19.6)
Other dose 697 (7.5) 1339 (14.4)
Same dose as before index event 496 (5.3) 508 (5.5)
Wallentin L, et al. N Engl J Med. 2009;361:1045-1057.

35
Greater IPA will achieved when switching from clopidogrel to ticagrelor
despite of patient respond or no respond to clopidogrel
Non Responders Responders
*p<0.0001, †p<0.001, ‡p<0.05.
Gurbel PA, et al. Circulation 2010;121:1188–1199.

Interruption and/or neutralization of both
anticoagulant and antiplatelet therapies is
indicated in case of major bleeding, unless it
can be adequately controlled by specific
haemostatic measures
Minor bleeding should preferably be managed
without interruption of active treatments.
Co-medication of PPI and antithrombotic agents
is recommended in patients at increased risk of
GI haemorrhage.
CLASS LEVEL
1 C
CLASS LEVEL
1 C
CLASS LEVEL
1 B
Hamm CW et al. Eur Heart J 2011;32:2999 – 3054
Bleeding Management

37
The proton pump inhibitor treatment algorithm in
patients with acute coronary syndrome
Agewall S et al. Eur Heart J 2013; 34, 1708–1715
ACS treated with DAPT in patients with a history of GI
hemorrhage or peptic ulcer, and/or high CRUSADE score or
multiple other risk factor for GI Bleeding
( Helicobacter Pylori infection, age ≥ 65 years , concurrent use
of anticoagulants or steroids)
Prasugrel
Ticagrelor
Clopidogrel Warfarin
Any PPI PPI with less CYP2C19 inhibitory
capacity (pantoprazole) rather
than a PPI with high inhibitory
capacity (omperazole
Any PPI,
With carefull
INR monitoring

How Long DAPT
Referensi: 1. Valgimigli M et al. European Heart Journal 2017; 0; 1–48
