lr miscarriage booklet
TRANSCRIPT

Hormone Solutions
Understanding miscarriage
Table of ContentsWhat is miscarriage? 1What does not cause miscarriage? 1When is a miscarriage not a miscarriage? 2Why does miscarriage occur? 2Who develops miscarriage? 6How often does a miscarriage happen? 6Can I avoid a miscarriage? 8What are the signs and symptoms of miscarriage? 8How is miscarriage classified? 10How is miscarriage treated? 11How is surgery performed? 14What are the complications of a miscarriage? 15When can we try again? 16What is the role of progesterone in humans? 17What are the pros and cons of natural progesterone treatment versus synthetics? 18What about homeopathic treatment? 19Who should not use natural progesterone hormone cream? 19How do I use natural progesterone hormone cream? 19What are the side-effects of natural progesterone replacement therapy? 20Which progesterone cream is best for me? 21What can we expect at the reproductive endocrinologist’s? 24About Lawley Pharmaceuticals 25Our Mission Statement 26Completed Clinical Studies 26Where can I find out more? 27References for Medical Professionals 28Glossary 29

1
What is miscarriage?A miscarriage is a pregnancy that ends spontaneously before 20 weeks of pregnancy, when the fetus has no chance of living independently outside the womb. After 20 weeks, pregnancy loss is considered a stillbirth. A fetus that survives into the third trimester (weeks 28 to 40 of pregnancy) has a chance of survival.
The medical term for miscarriage is spontaneous abortion, abbreviated as SAB. The medical term for repeated miscarriages is habitual abortion. Your medical caregivers must use this terminology for correct diagnosis, treatment, billing, and to comply with legal regulations. They do not intend to be offensive by using the term ‘abortion’ with regard to your loss.
What does not cause miscarriage?You will not lose a pregnancy through working outside your home, unless it is in a dangerous environment. Dangerous work environments include:
• Farms that use insecticides and herbicides known to interfere with reproduction
• Hospitals, (especially sterilizers where the worker is exposed to ethylene oxide gas from 0.1 ppm to 250 ppm), laboratories, Nuclear Medicine, Radiology, and incinerator disposals
• Food processing plants with incinerators that produce CHCs• Workplaces near a source of radiation that delivers more than
100 mSv during the pregnancy
You will not lose a pregnancy from moderate exercise. You will not lose a fetus by having gentle sexual intercourse during your pregnancy. The common cold or a yeast (candida) infection will not cause you to lose your baby.
If you have a pre-existing condition like thyroid disease or diabetes and are taking your medications as prescribed, you have a good chance of bringing your pregnancy successfully to term.

2
When is a miscarriage not a miscarriage?You may not have actually had a miscarriage.
A blighted ovum means the gestational sac formed, but there is no baby in it. Your body may be slow to realize the absence because you have all the symptoms of a pregnancy, like nausea and tender breasts. Blighted ovum may only be discovered during an ultrasound.
A complete molar pregnancy means the sperm fertilized an empty egg, and no embryo formed. These are called moles. A partial molar pregnancy means two sperm fertilized the same egg, and only a little bit of placenta and embryo is formed.
In these cases, you have not lost a child, but just the products of conception.
Why does miscarriage occur?A pregnancy is most vulnerable during Weeks 7 to 13. Repeated miscarriages can result from problems with: Implantation; genetics; immune disorders; physiology; hormones; toxin exposure; lifestyle; trauma; the mother’s age; and infections. The fetus is abnormal in 70% of miscarriages.
Implantation problems mean the couple conceives but the fertilized egg cannot implant safely in the uterus for a full-term pregnancy.
A miscarriage that occurs in the first trimester of pregnancy (Day 1 to Week 12) is most likely to be caused by a genetic disorder with the fetus. For example, Turner’s syndrome is a genetic disorder that terminates 98% of affected pregnancies in the first trimester.
Late miscarriage in the second trimester (4 to 6 months) can happen from problems with the immune system or physiological problems. Examples of immune system problems are:
• Rh incompatibility, where the mother is Rh negative and the father and fetus are Rh positive. The mother’s antibodies attack the fetus as a foreign invader.
• Antiphospholipid antibodies that cause clots in the placenta. Between 10% and 15% of repeat miscarriages are caused by these antibodies, and the fetus often grows into the second trimester.

3
• Lupus, where the woman’s overactive immune system attacks her body. ANA antibodies are present in the bloodstream.
• Faulty fetal-blocking antibodies that cannot protect the baby from the mother’s immune system when the parents’ DNA is too similar. Multiple miscarriages will likely occur at exactly the same time each pregnancy, usually before Week 12.
Examples of physiological (mechanical) problems are:1. Uterine fibroid tumors – Although they are benign (non-cancerous),
fibroids can crowd out a pregnancy. Submucosal fibroids act like an IUD contraceptive to prevent the egg from implanting in the uterus.
2. Ectopic (tubal) pregnancy – In 2% of pregnancies, the egg does not implant in the uterus, but stays in the fallopian tube, which ruptures when the embryo outgrows it.
3. Incompetent cervix – In 1 out of every 100 pregnancies, the mother has a weak cervix due to a previous difficult delivery or miscarriage, or cervical surgery, D&C termination, birth defect, or exposure to the synthetic hormone DES (Diethylstilbestrol). The cervix is weak and opens before the fetus can survive outside the mother’s body, usually in the second trimester (Weeks 13 to 27 of pregnancy) or third trimester (Weeks 28 to delivery). One-quarter of babies lost in the second trimester are due to incompetent cervix.
4. Placenta previa – The placenta grows over the cervical opening and will tear in the second trimester.
Progesterone deficiency is a hormonal problem where the pregnancy cannot be sustained past the tenth week without progesterone supplements.
During the latter half of a woman’s menstrual cycle (luteal), the ovary naturally secretes progesterone from the empty follicle in the ovary where the egg was released. Progesterone prepares the woman’s uterus for implantation of a fertilized egg. If the woman conceives, the empty follicle forms a corpus luteum (yellow body) that supports the pregnancy until the placenta is big enough to take over progesterone production.
If the egg (ovum) is fertilized, the corpus luteum (yellow body) in the ovary secretes progesterone to maintain the pregnancy until the placenta is large enough to take over production. Progesterone levels increase to

4
400 ng/ml of blood, and taper off during the last month of pregnancy to 200 ng/ml.
When you become pregnant, the corpus luteum supports the pregnancy for about the first 10 weeks. The placenta is the organ that attaches mother and child during pregnancy, and is expelled as afterbirth following the delivery. At about 8 to 10 weeks of pregnancy, the placenta in pregnant females is usually big enough to take over progesterone production from the ovaries and support the pregnancy after the tenth week. This is the critical moment for sustainability of the pregnancy and the danger time if progesterone production from the corpus luteum does not keep pace with the requirements of the growing fetus. If the placenta does not produce sufficient progesterone to pick up the progesterone shortfall from the corpus luteum the placenta will become unstable and begin to breakdown. Spotting may occur and if not addressed with progesterone supplementation (e.g. ProFeme®) the pregnancy will usually miscarry. By week 13 the placenta is sufficiently developed to support its own progesterone production and production continues to steadily increase until the end of the 8th month.
Pre-pregnancy normal daily progesterone production is around 20 milligrams per day during the luteal phase. During pregnancy, your progesterone production increases sharply to 400 milligrams by the third trimester (7 – 9 months). Estrogen also increases during pregnancy, but not as much as progesterone.
The progesterone level in the blood is a good indicator of the health of the placenta. Low progesterone levels are associated with amnionitis, intrauterine death, premature rupture of the membranes, premature labor, and placental abruption.
Toxin exposure is likely to cause miscarriage. If you live or work near the flue gases of incinerators you are exposed to chlorinated hydrocarbons (CHC) that cause endometriosis, habitual abortion, and birth defects. CHCs are stored in body fat. Hospital and food processing workers are
��������
�������������������������������������
��������
�������������������������������������
��������
�����������������������������������������������������
�������������
�������
�
�
�
��
��
��
���
�
�������������������������������������������
5
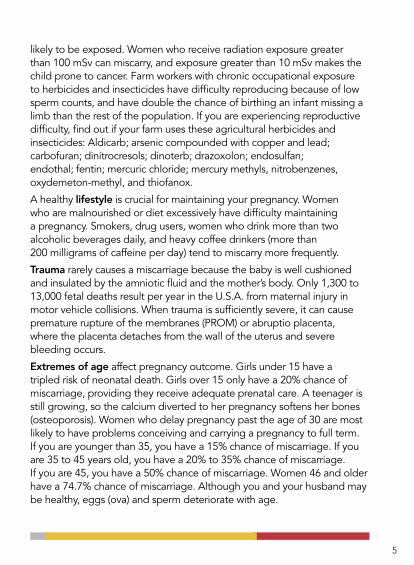
likely to be exposed. Women who receive radiation exposure greater than 100 mSv can miscarry, and exposure greater than 10 mSv makes the child prone to cancer. Farm workers with chronic occupational exposure to herbicides and insecticides have difficulty reproducing because of low sperm counts, and have double the chance of birthing an infant missing a limb than the rest of the population. If you are experiencing reproductive difficulty, find out if your farm uses these agricultural herbicides and insecticides: Aldicarb; arsenic compounded with copper and lead; carbofuran; dinitrocresols; dinoterb; drazoxolon; endosulfan; endothal; fentin; mercuric chloride; mercury methyls, nitrobenzenes, oxydemeton-methyl, and thiofanox.
A healthy lifestyle is crucial for maintaining your pregnancy. Women who are malnourished or diet excessively have difficulty maintaining a pregnancy. Smokers, drug users, women who drink more than two alcoholic beverages daily, and heavy coffee drinkers (more than 200 milligrams of caffeine per day) tend to miscarry more frequently.
Trauma rarely causes a miscarriage because the baby is well cushioned and insulated by the amniotic fluid and the mother’s body. Only 1,300 to 13,000 fetal deaths result per year in the U.S.A. from maternal injury in motor vehicle collisions. When trauma is sufficiently severe, it can cause premature rupture of the membranes (PROM) or abruptio placenta, where the placenta detaches from the wall of the uterus and severe bleeding occurs.
Extremes of age affect pregnancy outcome. Girls under 15 have a tripled risk of neonatal death. Girls over 15 only have a 20% chance of miscarriage, providing they receive adequate prenatal care. A teenager is still growing, so the calcium diverted to her pregnancy softens her bones (osteoporosis). Women who delay pregnancy past the age of 30 are most likely to have problems conceiving and carrying a pregnancy to full term. If you are younger than 35, you have a 15% chance of miscarriage. If you are 35 to 45 years old, you have a 20% to 35% chance of miscarriage. If you are 45, you have a 50% chance of miscarriage. Women 46 and older have a 74.7% chance of miscarriage. Although you and your husband may be healthy, eggs (ova) and sperm deteriorate with age.

6
Infections such as malaria, syphilis, toxoplasmosis, mycoplasma, fifth disease (erythema infectiosum, commonly called ‘slapped cheek’), and chicken pox can cause miscarriage.
Who develops miscarriage?Every healthy woman under the age of 35 has a 15% chance of miscarriage. A chemical pregnancy occurs when a woman loses a newly implanted egg at the expected time of her period. Up to three-quarters of miscarriages are chemical pregnancies. The woman may not even know she was pregnant.
If you had one previous miscarriage, your chance of another miscarriage is not tremendously increased. There is a 25% chance that you will miscarry a second time. There is a 20% chance that you will be a habitual aborter with multiple miscarriages.
Diabetes, autoimmune diseases, and antiphospholipid syndrome (APS) place a pregnancy at additional risk. Autoimmune disorders include rheumatoid arthritis, lupus, and scleroderma. The immune system defends the body against invaders, like viruses and bacteria. In autoimmune disorders, the immune system is overactive and attacks the body’s own tissues. Consequently, women with autoimmune disorders often have difficulty bringing a pregnancy to term.
Women with uterine fibroids, or who had a uterine fibroid embolization (UFE), or myomectomy to remove fibroids are at high risk for miscarriage.
The incidence of miscarriage is greater in females with a genetic disorder affecting their sex chromosomes. For example, 1 in every 2,500 to 10,000 live girls born in Australia has Turner’s syndrome, and is prone to miscarriage. It affects females only. Type II Diabetic women and girls with juvenile rheumatoid arthritis are more likely to have Turner’s syndrome.
How often does a miscarriage happen?Up to one-quarter of all confirmed pregnancies result in a miscarriage. Most miscarriages occur before Week 13 of pregnancy. Most countries do not include miscarriages in their pregnancy calculations because there is no way to count those that do not require in-patient hospitalization.

7
If this is your first pregnancy and you are one or two weeks pregnant, you have a 75% chance of miscarriage. You probably are unaware that you conceived because most home test kits detect a pregnancy no sooner than 14 days after ovulation. If you are three to six weeks pregnant, you have a 10% chance of miscarriage. If you are six to 12 weeks pregnant, you have a 5% chance of miscarriage. Once your obstetrician can hear the fetal heartbeat, your pregnancy is even safer. You only have a 3% chance of a second trimester miscarriage. In the third trimester, you only have a 1% chance of stillbirth.
If your first pregnancy miscarried, you have a 13% chance of recurrence. If you had at least one live birth and one miscarriage, you have a 10% chance of another spontaneous abortion (SAB). If you had multiple miscarriages and one live birth, you have a 13% chance of another miscarriage, providing you are younger than 35. However, if your first child was a live birth, followed by several SABs, your obstetrician must re-evaluate your risk. If you had two live births and two miscarriages, you have a 40% chance of another SAB. If you had three pregnancies that all ended in miscarriage, then you have a 60% chance of another SAB and must go for testing. If you had four consecutive pregnancies that all ended in miscarriage, then you have a 5% chance of delivering a live baby, at best – perhaps less. Ask your family doctor to refer you to a reproductive endocrinologist and then a fertility specialist.
Turner syndrome is responsible for 20% of all miscarriages that occur in the first trimester, and 98% of pregnancies affected by Turner’s syndrome end in miscarriage.
Many fetuses with hypogonadism have one or both kidneys missing (renal agenesis) and 10% to 33% of them will die in the uterus.
Infertility affects 15% of Australian couples. Infertility affects 12% of women aged 15 to 44 in the U.S.A., either because they cannot conceive, or they miscarry.
Mothers over 35 are more likely to miscarry.

8
Can I avoid a miscarriage?Subfertile women who do fall pregnant may not be able to sustain the pregnancy past the tenth week. Progesterone is the hormone that supports a pregnancy. Before conceiving, a woman prone to miscarriage can try a low dose of natural progesterone cream from days 12 to 26 of her cycle until the pregnancy is confirmed. If spotting occurs at week 6 or 7 of pregnancy, a high dose of 100 to 200 mg progesterone cream is applied twice or three times daily. Often, women use natural progesterone cream until the baby is full term (40 weeks of gestation).
What are the signs and symptoms of miscarriage?A sign is something you can objectively see or measure, like vomiting or a fever. A symptom is something only you feel and report.
If you are pregnant and develop any of these signs and symptoms, go to the nearest Emergency Room immediately:
• Bright red or brownish bleeding from the vagina, which may be painless• Passing clots or tissue • Painful contractions every 5 to 20 minutes apart• Leaking clear fluid from the vagina (not urine from the bladder)
If you are pregnant and develop any of these signs and symptoms, phone your doctor as soon as possible:
• Back pain• Abdominal cramps• White or blood-tinged mucous from the vagina• Loss of pregnancy signs, like abdominal and breast swelling
• Fever over 101ºF or 38.33ºC, especially if accompanied by chills (rigors)
If your doctor is unavailable, ask for the obstetrician on call (locum tenens) or go to the nearest hospital Emergency Room immediately. If you have a high fever, take acetaminophen/paracetamol (Tylenol®/Panadol®) to reduce it, because prolonged high fever damages the fetus. The ER doctor can update your obstetrician when your condition has stabilized.

9
An ectopic pregnancy occurs in the fallopian tubes instead of the uterus. Often, the affected woman’s first pregnancy test will be positive, and then repeat tests will be negative, although the woman still has other pregnancy symptoms. If you have an ectopic pregnancy (tubal pregnancy), then your symptoms will be more dramatic than most:
• Bright red, spotty vaginal bleeding• Abdominal pain that increases in severity as the tube nears rupture• Referred shoulder pain• Dizziness• Fainting• Mass on the sides of the uterus (adnexal mass) instead
of within the uterus• Uterus that is smaller than expected for the stage of pregnancy• Urge to move the bowels
Go to the nearest Emergency Room immediately. Ectopic pregnancy is life-threatening for the mother. You must have surgery performed on the ruptured fallopian tube to stanch the bleeding.
If you have painless, bright red bleeding in your second or third trimester that stops and recurs again days or weeks later, you may have placenta previa. The placenta partly or completely grew over the opening to the birth canal.
On rare occasions, you may be unable to get medical attention immediately. If bleeding occurs and you cannot get to your doctor’s office right away, try these easy steps to control bleeding:
1. Bed rest.2. Drink several salty liquids, like V8, tomato juice, or bouillon soup.
Good fluid balance will help keep you from getting dizzy.3. Take one or two 200 mg tablets of ibuprofen every 4 to 6 hours.
Avoid taking aspirin, because it is an anticoagulant and could worsen your bleeding. Ibuprofen will lessen your cramps by decreasing prostaglandins and reduce the blood flow 25% to 30%.
4. Take one 300 mg tablet of ferrous gluconate or iron equivalent per day to prevent anemia.
10
The paramedics, triage nurse, ER doctor and obstetrician must all ask you how much blood you have lost. Try to be patient with their repetitive questions, as they are tracking your progress over time. An overnight pad or super tampon holds around 10 ml of blood. To calculate the approximate amount of blood you have lost, multiply the number of sanitary products you saturated by 10. For example:
5 extra-absorbent pads x 10 = 50 ml blood lost
If you are losing a blighted ovum, then your blood flow will be slow and brown. If you are losing a molar pregnancy (hydatidiform mole), you will bleed during Week 12, your ßhCG levels will be too high, and your uterus will be larger than normal for a 12-week pregnancy. Remember that you are only losing some poor genetic material, not a fully-formed child in either of these situations. Only 1 in every 1,000 pregnancies is molar.
How is miscarriage classified?A fetus is not necessarily present in every miscarriage. Blighted ovum and molar pregnancy are two conditions where there is no fetus, only the supporting tissues or abnormal growths.
These are the different stages of a true miscarriage:
1. If you are only spotting, and your cervix is still closed, it is called a threatened abortion. Your doctor will advise bed rest and abstaining from any activity that could aggravate your condition. This includes sexual intercourse until the problem resolves.
2. If you are actively bleeding, have back or abdominal pain, and your cervix is open, then you have an incomplete miscarriage.
3. If your cervix is dilated or effaced, or if your membranes have burst, you have an inevitable miscarriage.
4. If you have expelled the contents of your uterus, you have a complete miscarriage.
5. If the embryo is dead but remains in the uterus, you have a missed miscarriage.
6. If you have three or more first trimester miscarriages in a row, you have recurrent miscarriage (RM).

11
How is miscarriage treated?The paramedic will make you bed rest quietly and may give you medications to stop your uterus from contracting under the direction of the Emergency Room physician at the base hospital by phone. Bring all prescription drugs, herbs, and supplements you are taking with you to the hospital. Be honest with the ER doctor if you drink heavily or use street drugs. Your doctor may consult with a pharmacist to find out if your miscarriage could be the result of a drug interaction.
The nurse or midwife will record your vital signs (height, weight, blood pressure and temperature). If you have been bleeding excessively, the nurse will take your pulse twice:
• First when you have been lying down quietly for 5 minutes• Second when you have been standing fairly still for 1-3 minutes
The maximum amount your pulse should increase when standing is 20 beats per minute. If you have bled so much that your blood volume is depleted, it will increase more. You may require intravenous fluids (IV), antibiotics and a blood transfusion.
You will require a vaginal exam by a doctor or midwife. You must recline on the examination couch while your doctor inserts a clean clamp (speculum) to hold your vagina open and shines a bright light on your perineum to see well. If you have not had a pap smear in the past year, the doctor scrapes your cervix with a wooden Popsicle stick, smears the sample on a slide, and sends it to the Pathology Lab for expert examination.
Some miscarriages are inevitable. Remember, if your membranes break and you go into labour, that a baby can only survive outside the uterus if it weighs at least 500 grams (1.10 pounds) and is at least 24 weeks old.
If you have a molar pregnancy, remember that a proper fetus does not form, and the cellular mass cannot survive outside your body. Your uterus is more likely filled with clusters of bubbles. Your doctor will likely suggest a cervical dilatation and evacuation with suction (D&E) to remove the products of conception by the end of your first trimester (Week 12 of pregnancy). In 2-3% of molar pregnancies, the moles may develop into a cancer called choriocarcinoma which can spread to distant parts of the body and require methotrexate and limited cancer chemotherapy.

12
A miscarriage is often treatable if it is addressed immediately. Not every woman who spots during the first trimester has a miscarriage; 20% of women who spot bring the pregnancy to full term (40 weeks). If you are pregnant and spot or bleed visit your doctor or the nearest Emergency Department at an obstetric hospital as soon as possible. Bring any tissue you pass with you in a clean container. The lab can test the tissue for many abnormalities to pinpoint your problem.
Progesterone is the hormone that supports a pregnancy. If you do fall pregnant but are unable to sustain the pregnancy past the tenth week, then there is a high probability that you are progesterone-deficient.
Before conceiving, a woman prone to miscarriage can try a low dose of natural progesterone cream from days 12 to 26 of her cycle until the pregnancy is confirmed. If spotting occurs at week 6 or 7 of pregnancy, a high dose of 100 to 200 mg progesterone cream is applied twice or three times daily. Often, women use natural progesterone cream until the baby is full term (40 weeks of gestation).
If your problem is incompetent cervix, the treatment is simply to sew the cervix shut (cerclage) during Weeks 14 to 16 of your pregnancy. Your doctor must remove your stitches (sutures) between Weeks 36 to 38 so that you can give birth. Cerclage cannot avert an inevitable miscarriage, so your doctor cannot perform it if your cervix has already dilated to 4 centimeters or if your membranes have already ruptured. You are also ineligible for cerclage if your cervix is irritated. Cerclage is generally well tolerated by mother and baby, but it is not a cure-all. Be aware that cerclage can cause severe bleeding (hemorrhage) from lacerations of the cervix, rupture of the membranes, uterus or bladder, and premature labor.
Daily progesterone production jumps from a non pregnant 20mg to 400mg
during the third trimester

13
If the cause of your miscarriage is an immune problem, then the treatment varies:
• Rh incompatibility requires RhoGAM injections at 26 to 28 weeks of pregnancy and again within 72 hours after your delivery
• Antiphospholipid antibodies requires daily low dose aspirin or heparin, an anticoagulant
• Lupus requires prednisone, a powerful anti-inflammatory steroid • Faulty fetal-blocking antibodies require the mother to receive injections
of the father’s white blood cells, so sufficient paternal HLA antibodies in the maternal bloodstream will stimulate the fetal-blocking antibodies to protect the next baby
Many insurance companies will not cover immune testing until the woman has had at least three miscarriages. You may have to travel a long distance to get help for faulty fetal-blocking and HLA antibody problems, in particular.
The immune system contains several different types of white blood cells. Progesterone supplementation can help your immune system by influencing the way your white blood cells react to your pregnancy. The immune responses most likely to impair your pregnancy are:
1. T and B cells that can cause placental rejection 2. Natural killer cells that release tumor necrosis factor (TNF) that
damages the placenta and endometrium3. Lymphocytes that stick in the placenta and damage it
Progesterone soothes inflammation that scars and damages the placenta. Progesterone encourages the placenta to increase its HCG production, blocking NK cells’ killing power. Progesterone can prevent the uterus from producing irritating prostaglandins that make it contract far too early in the pregnancy. Progesterone encourages the cervix to make an antibody-rich plug to protect the baby and placenta from ascending germs.
Women with autoimmune disorders usually require progesterone supplementation until the end of Week 16 of pregnancy.
Sometimes, newly pregnant autoimmune women are allergic to their own hormones, including progesterone, because of a problem with their CD 19+5+ cells. Your doctor can test for allergies with a skin or blood

14
test. CD 19+5+ cells are usually suppressed by 10 weeks of gestation. Progesterone allergy is less of a concern after you have been pregnant for 10 weeks.
See a gynecologist with CREI (Certified Reproductive Endocrinology and Infertility) qualifications about repeated miscarriage (habitual abortion). Your doctor must rule out other causes besides progesterone deficiency. For example, Turner’s syndrome is a chromosomal abnormality affecting only girls, where one X chromosome is missing. Turner’s syndrome is responsible for 20% of all miscarriages that occur in the first trimester, and 98% of pregnancies affected by Turner’s syndrome end in miscarriage.
Women with reproductive difficulties may successfully deliver a baby through Assisted Reproductive Technology (ART). The cost of ART presently ranges from $8,000 to $15,000 per cycle, depending on the complexity of the method the doctor uses. ART is usually successful in three cycles. Ask your doctor to define ‘success’ before you make your down payment, because some clinics define success as any conception, and others define it as taking home a baby.
Two-thirds of infertile couples can have a baby. Your chances of success diminish as your age increases.
How is surgery performed?If you have an ectopic pregnancy, you must have surgery to remove the fetus and products of conception from the affected fallopian tube. In most cases, the surgeon is unable to salvage the delicate tube and will remove it (salpingectomy). You have a 9% chance of another ectopic pregnancy if you only have one fallopian tube left. If you retained your damaged fallopian tube, then you have a 12% chance of a repeat ectopic pregnancy.
MOTHER’S AGE ART SUCCESS RATE
Younger than 35 37.3%
35 - 37 30.2%
37 - 40 20.2%
41 - 42 11%
15
For unavoidable miscarriages, the method of choice is dilatation and curettage (D&C). The surgeon may place a black “matchstick” of seaweed called a laminaria tent in your cervix to open it gently overnight. When you are in the operating room the surgeon gradually makes the opening of your cervix bigger by spinning a series of increasingly larger dilator wands in it. The surgeon grasps your uterus with a tenaculum clamp to hold it steady. The surgeon scrapes the lining of your uterus clean with curettes, which resemble small rakes.
Dilatation and evacuation (D&E) with a suction device is the choice for molar pregnancy.
In all cases, you will be taken to a Recovery Room for the anesthetic to wear off. Your nurse will encourage you to get up and walk soon after the surgery to prevent pooling of body fluids and pneumonia. You cannot drive yourself home. Arrange for a friend to pick you up and monitor you overnight for complications.
You can take a shower the day after your surgery. Avoid baths, douching, swimming, and intercourse for a month. Avoid heavy lifting. Wear absorbent sanitary napkins for a few days up to several weeks after surgery to catch the drainage. Do not use tampons because infection could result. Expect breast discomfort and leaking milk to last a week.
Call the doctor if you develop fever, heavy bleeding or a foul-smelling discharge. You may need antibiotics to fight infection or ergometrine to stanch bleeding. Barring complications, you probably can return to work in two days, but book the week off work as a precaution. Most women can resume exercising in three weeks.
What are the complications of a miscarriage?Most miscarriages do not result in physical complications, but every surgery entails risk. Possible complications of salpingectomy, D&C and D&E include:
• Adverse reaction to the anesthetic• Bleeding• Infection• Damage to the cervix causing it to become incompetent• Perforation of the uterus, bowel or bladder

16
The drop in progesterone that accompanies a miscarriage in late second or third trimester may result in temporary depression. Emotional strain makes depression last longer.
Grief is a normal response to the death of a loved one. Many couples consider their fetus to be a person, and it is very disheartening if outsiders minimize the impact of a miscarriage. How a person deals with grief is very personal, and each person will grieve differently. Grief puts strain on a marriage. Elisabeth Kübler-Ross identified these five stages of grief in her landmark book, On Death and Dying:
1. Denial This can’t be happening2. Anger Why me!3. Bargaining I’ll do anything if...4. Depression I just can’t handle it5. Acceptance Everything will be all right
A person may not necessarily follow the stages in order, or go through each stage. A person should go through at least two of the five stages. If your grief is not progressing through the stages, or is prolonged, then see your doctor.
When can we try again?If you have had a molar pregnancy, wait at least 1 year before attempting another pregnancy. You must wait until your ßhCG level has returned to 0 to ensure that no moles have migrated to distant parts of your body (metastasized). In rare cases, your gynecologist will set the allowable ßhCG level at less than 2 mIU/ml if you can maintain it for a full year. Follow your gynecologist’s instructions exactly.
In all other cases, wait at least one and preferably three cycles before attempting another pregnancy. Allow yourself time to recover fully. Take a 400 micrograms (0.4 milligrams) folic acid supplement daily and eat a nutritious diet while you are waiting to try again. Reduce your caffeine intake. Avoid alcohol, smoking, contact sports, environmental hazards, and people with infectious diseases. Before you use an over-the-counter medication, check with your doctor or pharmacist.

17
What is the role of progesterone in humans?Progesterone is the hormone that regulates menstruation, supports pregnancy, and helps an embryo develop by providing a source of corticosteroids. Natural progesterone is a steroid hormone derived from cholesterol and is vital as a precursor hormone in the body’s production of corticosteroids and glucocorticoids – steroids that help us deal with stress and physical cellular/tissue repair. Progesterone is normally produced by the corpus luteum in the ovaries and in the brains of humans and animals. At about 8 to 10 weeks of pregnancy, the placenta in pregnant females takes over progesterone production from the ovaries. Progesterone is the pivotal hormone of pregnancy (see www.progesteroneinpregnancy.info).
Women in their childbearing years experience cyclical progesterone surges. In the beginning (follicular phase) of a menstrual cycle, women have low progesterone levels equivalent to that in men, children, and post menopausal women (less than 2 ng/ml of blood). The small amount of progesterone present in males does not have a feminizing effect on them. Progesterone decreases libido and calms mood in both sexes.
When a woman releases an egg for fertilization (ovulation), her progesterone level spikes (greater than 5 ng/ml of blood). If the egg (ovum) is fertilized, the corpus luteum (yellow body) in the ovary secretes progesterone to maintain the pregnancy until the placenta is large enough to take over production. Progesterone levels increase to 400 ng/ml of blood, and taper off during the last month of pregnancy to 200 ng/ml. After birth occurs and milk production (lactation) begins, women experience “baby blues” because the progesterone levels decrease abruptly.
Progesterone is a neurosteroid in the brain that affects functioning of the nerve synapses and the protective myelin sheath of nerves. Researchers are investigating the effects of progesterone on memory, cognition, and multiple sclerosis. Animal studies suggest progesterone may protect females from brain injury.
Progesterone molecule

18
Progesterone reduces spasms in smooth muscles. It is an anti-inflammatory and decreases immune response. Progesterone adjusts the body’s use of zinc, copper, fat, estrogen, collagen, and blood clotting factors. It is one of the hormones that regulate the uterus, gall bladder, thyroid, bones, teeth, skin, ligaments, tendons, and joints.
Women take progesterone to prevent excessive menstrual bleeding and to assist with in-vitro fertilization. A woman with a very short cervix who is prone to miscarriage can take progesterone to help maintain her pregnancies, because it has been proven to reduce pre-term births and the time babies spend in neonatal intensive care units.
What are the pros and cons of natural progesterone treatment versus synthetics?Natural hormone creams are absorbed through the skin (transdermally), so they avoid first-pass metabolism by the liver, a phenomenon where ingested drugs are absorbed through the stomach and intestine, travel to the liver, and are broken down to the extent that only a small fraction of the active drug circulates to the rest of the body. This first pass through the liver greatly reduces the bioavailability of the hormones by breaking them down into less active forms. Synthetic hormone pills are rapidly metabolized by the liver on the first pass, so the amount of hormone you receive is reduced. Oral hormones are excreted in the urine, so most of your dose is lost.
PRO-FEME® natural progesterone cream contains the hormone identical to that produced by the human ovary and application as a topical cream to the skin avoids the first-pass metabolism.
Other non-oral delivery methods of natural progesterone, such as lotions, sprays and troches have not proved as effective as cream for administering progesterone.
Wild yam treatments sold in health food stores contain a steroid substrate called diosgenin, which is chemically similar to progesterone, but does not act like progesterone within the body. Humans cannot convert diosgenin into progesterone – a point often misrepresented by marketers of wild yam products.
Unlike natural progesterone the synthetic progestins are contraindicated in pregnancy. Drug company Product Information profiles warn that
19
synthetic progestins should not be used in pregnancy due to the potential for causing birth defects. This is not the case with natural progesterone.
What about homeopathic treatment?Homeopathy is a complementary therapy. Homeopaths claim that like cures like. Essentially, homeopaths believe that if a substance causes a disease, then you can cure it by taking a very minute, diluted amount of the same substance. Homeopathic treatments contain NO progesterone, nor have they been demonstrated to cause any change in progesterone levels. Progesterone is the worldwide gold standard for pregnancy support.
Who should not use natural progesterone cream? Do not use PRO-FEME® progesterone cream if you have:
• A known allergy or sensitivity to any of the ingredients in the cream, especially macadamia or almond oil
• Yellow jaundice or liver disease• Undiagnosed vaginal bleeding• The immune disease herpes gestationis, which develops during
pregnancy and is also called pemphigoid gestationis (PG)• A clotting disorder, like deep vein thrombosis (DVT)• Severe heart, blood vessel, or liver disease• A personal history of carcinoma of the breast or endometrium
How do I use natural progesterone cream?The aim of hormone replacement therapy is to mimic your ovaries natural hormone production as much as possible. Lawley’s applicators are marked in unit doses. You must tailor the strength and amount of cream you apply and the number of days you apply it to your individual requirements. Your doctor may alter the dose recommended in the directions on the product insert.
• If you have premenstrual syndrome, apply 2 units of Pro-Feme® 3.2% cream from Day 12 - Day 26 of your menstrual cycle. This will give you 32 milligrams of progesterone daily. Your doctor may instruct you to

20
alter this dose to create a crescendo effect 4 to 5 days prior to your menstrual period, when your symptoms are worst.
• If you are perimenopausal, apply 2 units of Pro-Feme® 3.2% cream from Day 12 to Day 26 of your menstrual cycle. If your period occurs after 5 to 10 days, cease application and start again 12 days later. This will give you 32 milligrams of progesterone daily.
• If you have endometriosis or postnatal depression, apply 3 units of Pro-Feme® 10% cream daily for 21 days in the calendar month.
• If you have a history of miscarriage the recommended dosing of Pro-Feme® to provide progesterone support and assist in preventing miscarriage is as follows:
Before conceiving, a woman prone to miscarriage should use Pro-Feme® 3.2% cream from days 12 to 26 of the cycle until the pregnancy is confirmed. If spotting occurs at week 6 or 7 of pregnancy, a high dose of 100 to 200 mg progesterone cream (Pro-Feme® 10%) twice or three times daily. Often, women use Pro-Feme® natural progesterone cream until the baby is full term (40 weeks of gestation).
What are the side-effects of natural progesterone replacement therapy?Progesterone is the hormone that supports a pregnancy (‘pro’ means for and ‘gestation’ means pregnancy). The most common problems associated with progesterone treatments are that they can cause symptoms similar to pregnancy:
• Tender breasts• Indigestion and vomiting• Fatigue• Mood swings• Vaginal discharge• Constipation or diarrhea• Headache• Muscle or joint pain• Runny nose, sneezing, and coughing• Problems urinating

21
Your doctor can adjust your dose if these minor symptoms do not clear up soon.
If you take estrogen with progesterone, you have an increased risk of breast cancer over taking estrogen alone.
Which progesterone cream is best for me?If one Googles “natural progesterone cream” or “progesterone gel” there are dozens of products claiming to be the “best” and “authentic” natural progesterone creams or gel. Just how does a woman determine which product is most suited to her requirements? The following is an outline of basic manufacturing processes to help you decide. The three quality standards of natural progesterone cream are:
1. Pharmaceutical Grade: The manufacturer operates to international standards of Good Manufacturing Practice (GMP). GMP means all production processes are standardized and controlled from the time the raw material is procured through to the expiry date printing on the finished product. The Australian government, like the U.S. and European regulators, enforces rigid government controls on the manufacturing facility and its equipment, processes, and packaging. PRO-FEME® natural progesterone creams are guaranteed stable, effective, and potent. The final product has detailed documentation and is backed by clinical trials that substantiate its therapeutic claims.
2. Cosmetic Grade: This is the quality sold over-the-counter in drug, department and grocery stores. Cosmetic grade products are 70% pure. Often, brand-names have exactly the same ingredients as generics, just with a different label. Cosmetic grade products are allowed a high bacterial content, so their shelf-life is very limited (usually 3 to 6 months). Cosmetic manufacturers are not required to register their products with the government because cosmetic products do not require clinical trials to prove their worth.

22
3. Compounded Product: Natural health products from pharmacists, herbalists, homeopaths, naturopaths, and practitioners of traditional Indian and Chinese medicines are compounded. This means the product is tailored to the patient’s individual needs in the delivery system most desired. Pharmacists compound drugs that are not commercially available, or in a different strength than that readily available. A compounded product may be needed to make a drug palatable. A compounded product may be needed if the patient reacts to dyes, preservatives, and allergens found in commercial products. Compounded products do not undergo any form of production control, concentration, impurity, stability or efficacy testing. Safe shelf-life is usually extremely short, if at all known. Compounded items are time-consuming to make, so generally they are more expensive.
The only pharmaceutical grade natural progesterone creams for women available worldwide are PRO-FEME® 3.2% and 10% creams from Lawley Pharmaceuticals, Australia. PRO-FEME® progesterone creams are specifically targeted for use in women with declined or lowered serum progesterone levels due to genetic disorders, surgical or chemical interventions, under- production by the ovaries or ageing. Low progesterone in women is associated with PMS, miscarriage, fatigue, lethargy, depression, irritability and mood changes.
Applied topically to the skin, PRO-FEME® Progesterone Creams for women are the world’s only clinically trialed and tested pharmaceutical grade progesterone creams using natural bio-identical progesterone. PRO-FEME® Progesterone Creams are listed with the Australian government (AUST L 95334 / L 70886).
PRO-FEME® Prescribing Information and Consumer Medicine Information can be downloaded from http://www.hormonesolutions.com.au (or by clicking on the hyperlinks).
��������
��������������������������������������
��������
��������������������������������������
��������
������������������������������������������������������
��������������
�������
�
�
�
��
��
��
���
�
��������������������������������������������
��������
�������������������������������������
��������
�������������������������������������
��������
�����������������������������������������������������
�������������
�������
�
�
�
��
��
��
���
�
�������������������������������������������

23
PROFILE TEST NORMAL ADULT – FEMALE VALUE
Thyroid T3 110 to 230 ng/dL
T4 5 to 10 µg/dL
TSH 1 to 4 µU/mL
Liver AST 5 to 40 IU/L
ALT 5 to 35 IU/L
ALP 30 to 85 ImU/mL
Bilirubin 0.1 to 1.0 mg/dL
Cholesterol 150 to 250 mg/dL
Kidney Creatinine 0.7 to 1.5 mg/dL
BUN 7 to 20 mg/dL
Adrenals Cortisol 2 to 28 µg/dL depending on time of day
ACTH 15 to 100 pg/mL
Hormones GH 0 to 8 ng/mL
FSH 3 to 20 mIU/mL
LH <7 mIU/mL
HCG Negative unless pregnant
Progesterone <2 ng/mL before ovulation>5 ng/mL after ovulation
Estradiol Varies from 25 pg/mL on Day 3 to 200 pg/mL at ovulation
Prolactin < 24 ng/mL
Testosterone 6 to 86 ng/dL
SHBG 18 to 114 nmol/L
Anemia Iron 60 to 190 µg/dL
Ferritin 12 to 300 mg/L
TIBC 250 to 420 µg/dL
Hemoglobin 12 to 16 g/dL
Hematocrit 37% to 47%
The usual preliminary blood tests are:

24
What can we expect at the reproductive endocrinologist’s?Your reproductive endocrinologist will perform a pregnancy blood test as a routine precaution to ensure you are not already pregnant. A routine urine drug test is required as a standard legal precaution before treatment.
Your doctor will likely order these blood tests to confirm that your hormones are in balance, that you are not anemic, and that you do not have an underlying infection: T3; T4; TSH; FSH; LH; estrogen; estradiol; testosterone; CBC; ferritin; TIBC; hepatitis; VDRL for syphilis; and HIV.
The nurse may book an abdominal ultrasound for you with the Radiology Department if your uterus is enlarged from retained products of conception, a new pregnancy, hyperplasia, fibroids, or another condition. If your endocrinologist suspects hormonal imbalance from the pituitary gland in your brain, you probably will require skull x-rays, a mammogram, and an ultrasound of your ovaries. You may be asked to get a CT, MRI or PET scan, or a biopsy.
These are guidelines only. Children and men have different normal values. Your laboratory adjusts its normal values for the local population it serves. It may use different units of measure. To find out more about diagnostic tests, visit Lab Tests Online: http://www.labtestsonline.org/understanding/index.html.

25
About Lawley PharmaceuticalsLawley Pharmaceuticals is a privately owned pharmaceutical company which focuses on the transdermal administration of the naturally occurring
hormones progesterone, testosterone and estradiol. Founded in 1995 by pharmacist Michael Buckley, Lawley Pharmaceuticals has grown to become a world leader in research and development of transdermal hormone preparations. As the principal of Lawley Pharmaceuticals,
Mr. Buckley has presided over the development, research, clinical trial program, regulatory process, development and marketing of the company.
The Lawley Pharmaceuticals portfolio of products includes Andro-Feme® 1% cream testosterone for women
Andromen® 2% and Andromen®Forte 5% testosterone creams for men
PRO-FEME® 3.2% and 10% progesterone creams for women
��������
�������������������������������������
��������
�������������������������������������
��������
�����������������������������������������������������
�������������
�������
�
�
�
��
��
��
���
�
�������������������������������������������
��������
��������������������������������������
��������
��������������������������������������
��������
������������������������������������������������������
��������������
�������
�
�
�
��
��
��
���
�
��������������������������������������������
26
Our Mission StatementLawley Pharmaceuticals (www.lawleypharm.com.au) strives to provide the optimal delivery systems for the administration of naturally occurring hormones to counter endocrine deficiency states.
Our philosophy is based on the principle to use a bio-identical hormone in preference to a synthetic hormone analogue (when a viable clinical option) and to advance areas of clinical research using natural hormones.
Our goal is to establish, through evidence-based medical research, naturally occurring hormones as cornerstone treatments for diseases such as breast cancer, infertility, hypogonadism, post natal depression and endometriosis.
Lawley Pharmaceuticals has established strong links with centres of medical research excellence around the world and continues to push the boundaries of medical research.
Completed Clinical Studies1. The effectiveness of transdermal progesterone cream on menopausal
symptoms, lipids and bone markers2. The effects of sequential transdermal progesterone cream on
endometrium bleeding pattern and salivary levels in post-menopausal women
3. Evaluation of serum progesterone levels after topical applications of Andro-Feme® cream in post menopausal women with symptoms of progesterone deficiency
4. Systemic absorption after transdermal application of labeled Progesterone in rats
5. Plasma and saliva concentrations of progesterone in pre-and post menopausal women after topical application of progesterone cream
6. The effect of progesterone replacement therapy on sexuality, mood and cognition of post menopausal women
7. Long-Term pharmacokinetics and clinical efficacy of Andromen®Forte 5% cream for androgen replacement in hypogonadal women.
8. Transdermal progesterone therapy improves well-being, mood, and sexual function in premenopausal women.

27
9. The pharmacokinetics of Andro-Feme®1% progesterone cream following two week, once daily application in progesterone deficient women.
Where can I find out more?1. Lawley Pharmaceuticals
http://www.miscarriage-hormone-treatment.com2. Lawley Pharmaceuticals http://www.progesteroneinpregnancy.info
3. Henry Lerner, Alice D. Domar, Miscarriage: Why It Happens and How Best to Reduce Your Risks, Da Capo Press, 2003, ISBN 0738206342, 9780738206349, 291 pages
4. Stillbirth and Neonatal Death Support http://www.sands.org.au/5. Victorian Government Health Information http://www.health.vic.gov.
au/maternity/yourpregnancy/pregnancyloss.htm6. Simon Knowles, A passage through grief--the Western Australian
Rural Pregnancy Loss Team, BMJ 1994;309:1705-1708 (24 December) http://www.bmj.com/cgi/content/short/309/6970/1705
7. Pregnancy Help Australia http://www.pregnancysupport.com.au/8. Infertility Treatment Authority http://www.ita.org.au/9. National Women’s Health Information Center (NWHIC) at
1-800-994-9662 www.womenshealth.gov10. American College of Obstetricians and Gynecologists (ACOG)
http://www.acog.org11. Infertility Awareness Association of Canada
http://www.iaac.ca/en/home12. Medline (U.S. National Library of Medicine and the National Institutes
of Health) http://www.nlm.nih.gov/medlineplus/pregnancyloss.html13. Lab Tests Online http://www.labtestsonline.org/understanding/
analytes/progesterone/test.html

28
References for Medical Professionals 1. www.DoctorDirect.com.au. If in Australia call 1-800 62 506 or
08 9228 9033 to speak with a pharmacist, or e-mail [email protected]. If in the USA or Canada call toll-free on 1-800-961-7813 or Toll free fax: 1-800-961-7650
2. Clinical Trials for Miscarriage http://clinicaltrials.gov/ct2/results?term=miscarriage
3. American College of Obstetricians and Gynecologists, Progesterone Recommended In Certain High Risk Pregnancies to Help Prevent Preterm Birth. October 31, 2003 http://www.acog.org/from_home/publications/press_releases/nr10-31-03-2.cfm
4. Garrisi JG, Colls P, Ferry KM, Zheng X, Garrisi MG, Munné S. Effect of infertility, maternal age, and number of previous miscarriages on the outcome of preimplantation genetic diagnosis for idiopathic recurrent pregnancy loss. Fertil Steril. 2008 Aug 8.
5. M S Rein. Advances in uterine leiomyoma research: the progesterone hypothesis. Environ Health Perspect. 2000 October; 108 Suppl 5: 791–793.
6. Pope Paul VI Institute, The Medical & Surgical Practice of NaProTECHNOLOGY. 2006, Omaha, Nebraska. http://www.naprotechnology.com/progesterone.htm
7. Aboutanos MB, Aboutanos SZ, Dompkowski D, Duane TM, Malhotra AK, Ivatury RR. Significance of motor vehicle crashes and pelvic injury on fetal mortality: a five-year institutional review. J Trauma. 2008 Sep;65(3):616-20.
8. Nybo Andersen AM, Wohlfahrt J, Christens P, Olsen J, Melbye M. Maternal age and fetal loss: population based register linkage study. BMJ. 2000 Jun 24;320(7251):1708-12.
9. W Stuart A. Smellie, Cases in primary care laboratory medicine: testing pitfalls and summary of guidance on sex hormone testing. BMJ Jan 2007; 334: 91 - 94; DOI: 10.1136/bmj.39038.614317.AE
10. Faricelli R, Esposito S, Toniato E, Flacco M, Conti P, Martinotti S, Robuffo I. A new diagnostic approach to better identify antiphospholipid syndrome. Int J Immunopathol Pharmacol. 2008 Apr-Jun;21(2):387-92.
29
GlossaryYou may hear these terms discussed in reference to yourself, your spouse, or your daughter:
Alfa-fetoprotein (AFP): A tumor marker for certain cancers of the ovaries and testes. Adults should have less than 15 nanograms of alfa-fetoprotein per milliliter of blood.
Amenorrhea: The monthly menstrual cycle ceases due to one of these causes:
• Menopause• Pregnancy• Not eating enough (anorexia nervosa)• Exercising too much• Extreme stress• A serious underlying medical miscarriage, such as uremia from
end-stage renal disease (ESRD or kidney failure)
Anemia: Lack of blood, usually due to iron deficiency anemia. Anemic people feel tired and are withdrawn and pale. Dark skinned people have pale mucous membranes. Your family doctor orders a Complete Blood Count and ferritin levels to confirm that you have anemia, and will likely prescribe iron supplements.
Anosmia: Lacking all sense of smell, common in women with genetic disorders affecting the sex glands.
ßhCG (Beta Human Chorionic Gonadotropin): Pregnant women excrete this pregnancy hormone 10 days after conception. ßhCG is the hormone detected by home pregnancy kits. Most of them detect 25 to 50 milli-international units of ßhCG per milliliter (mIU/mL). Your midwife or doctor uses a more sensitive test that detects 5 to 10 mIU/mL. Labs use ßhCG to measure the age of the embryo. High levels can mean multiple pregnancy, or cancer, or molar pregnancy (greater than 100,000 mIU/mL). Low levels can mean death of the fetus, tubal (ectopic) pregnancy, or miscarriage. Males with carcinoma of the testicles excrete this hormone. Non-pregnant women and healthy males never excrete ßhCG.

30
CA-15-3: Cancer Antigen 15-3, which is elevated in 3⁄4 of patients with metastatic breast cancer.
CA-125: Cancer Antigen 125 is a tumor marker for ovarian cancer.
CA-549: Cancer Antigen 549 is elevated in half of patients with advanced breast cancer.
D&C: Dilatation & Curettage, when the doctor scrapes the uterine lining to remove retained products of conception after a miscarriage. D&C is also used to examine the cells for endometrial cancer, to relieve the heavy buildup of the uterine lining (hyperplasia), and for abortions early in pregnancy.
Dysmenorrhea: Painful menstruation. If it is caused by excessive prostaglandins, dysmenorrhea can usually be relieved with ibuprofen (Motrin), massage, heat packs, adequate rest, and mild aerobic exercise, like walking. If it is caused by PCOS, hyperplasia, submucosal fibroids, or another uterine abnormality, the doctor must investigate further. Progesterone often relieves the pain associated with heavy menstruation from hyperplasia or fibroids.
Endometrial hyperplasia: Overgrowth of the womb’s lining because of: Overstimulation by estrogen during perimenopause; estrogen-mimicking chemical toxins in the environment, such as pesticides on produce and phthalates in cosmetics and plastics; antibiotics and growth hormones in meat and milk; and obesity. (see www.endometrialhyperplasia.info)
Fibroid tumors: Benign (non-cancerous) uterine tumors that can cause pain and heavy bleeding.
Fibrosis: Scar tissue replaces healthy tissue as a result of degeneration, injury, or infection.
FSH (follicular stimulating hormone): A hormone produced by the pituitary gland and the placenta, which stimulates the ovaries and controls reproduction.
Genotype: Genetic makeup, as opposed to appearance.

31
Gonadotropin levels: The pituitary gland secretes a group of hormones called gonadotropins, which stimulate the testicles and ovaries. Girls with Turner syndrome possess at least one extra X chromosome(s), which usually causes their pituitary glands to produce too much of the gonadotropins FSH (follicular stimulating hormone) and LH (luteinizing hormone).
Hyalinized: Healthy tissue is replaced by hyaline (clear or translucent white, glassy collagen fibers) due to degeneration.
Hyposmia: Decreased sense of smell, a sign of genetic problems.
Hypothalamus: The section of the brain that regulates body temperature, chemical balance, the pituitary gland, and the autonomic nervous system. The hypothalamus is part of the limbic system, so it regulates sexual appetite, eating, sleep, and emotions. It influences heart and breathing rates and blood pressure. The hypothalamus is located in the grey matter, below the thalamus, in the center of the brain. The pituitary gland hangs on a stalk below the hypothalamus.
Hypermenorrhea: Prolonged bleeding more than 7 days.
Hypomenorrhea: Scanty menstruation, saturating less than one pad per day.
Karyotype: Number, form, and size of chromosomes.
Mastectomy: Surgical removal of the breast.
Menorrhagia: Heavy bleeding more than 80 ml per cycle, or 16 soaked sanitary pads per cycle, leading to iron deficiency anemia.
LH (luteinizing hormone): A gonadotropic hormone released by the pituitary gland in the brain, which stimulates females to ovulate (release an egg).
Lymphedema: Swollen lymph glands.
Nystagmus: Erratic eye movement.
Osteoporosis: Bones that are brittle and break easily due to lack of calcium and sex hormones.
32
PCOS: Polycystic ovary syndrome. Painful, liquid-filled cysts on the ovaries that cause irregular menstruation, abnormal hair growth, skin tags, dark skin patches, insulin resistance, weight gain, infertility, and miscarriage. It may have a genetic component.
Phenotype: The physical characteristics of the boy comprised of his genetic makeup and his environment.
Pituitary gland: Connected to the hypothalamus, the pituitary controls growth hormone, prolactin for milk production, and follicle stimulating hormone (FSH) to stimulate testes. The pituitary stimulates the adrenal glands and the thyroid.
Polymenorrhea: One menstrual period every 2-3 weeks; this is too frequent.
Prostaglandin: Chemicals that control the contractions of the uterus. Prostaglandin level is highest when your menstrual period begins. Too much prostaglandin contracts the uterine muscle so hard that the blood supply is cut off, the uterus is starved for oxygen, and pain results. Prostaglandins from the uterus can leak into the bloodstream and cause nausea, vomiting, diarrhea, and headache.
Pterygium colli: Children with Turner or Noonan syndrome have a web of skin extending down the sides of their necks to their shoulders.
Renal agenesis: One or both kidneys are missing.
Salpingectomy: Removal of the fallopian tube.
Synkinesia: Involuntary movement at the same time as voluntary movement, common in genetic disorders.
T3, T4, and TSH: A panel of blood tests used to evaluate the thyroid gland in the neck. Women with thyroid imbalance do not ovulate (release eggs for fertilization).
Virilize: Encourage formation of male secondary sexual characteristics, such as beard growth, voice deepening, and strong muscle growth. Common in hormonal imbalance.

33
Notes

© Lawley Pharmaceuticals 2009
This publication is copyright. Other than for the purposes and subject to the Copyright Act, no part of it may in any form or by any means (electronic, mechanical, microcopying, photocopying, recording or otherwise) be reproduced, stored in a retrieval system or transmitted without prior written permission.
Enquiries should be addressed to: Lawley Pharmaceuticals, 61 Walcott Street, Mt Lawley, 6050, WA Australia
This brochure is presented by Lawley Pharmaceuticals 61 Walcott Street Mt Lawley Western Australia 6050 T. +61 (0)8 9228 9033 or 1800 627 506 F. +61 (0)8 9228 9455 E. [email protected] W. www.lawleypharm.com.au
USA and Canada Toll free phone: 1-800-961-7813 Toll free fax: 1-800-961-7650