lung lavage 2013 mas
DESCRIPTION
MAS / Meconium Aspiration Syndrome. Lung lavage rising as a new method to overcome this situation. This journal shows what kind of fluid we could use comparing surfactant and other fluid.TRANSCRIPT

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 1/31
Lung lavage for meconium aspiration syndrome in newborn
infants (Review)
Hahn S, Choi HJ, Soll R, Dargaville PA
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2013, Issue 4
http://www.thecochranelibrary.com
Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 2/31
T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1 ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9 AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
20DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
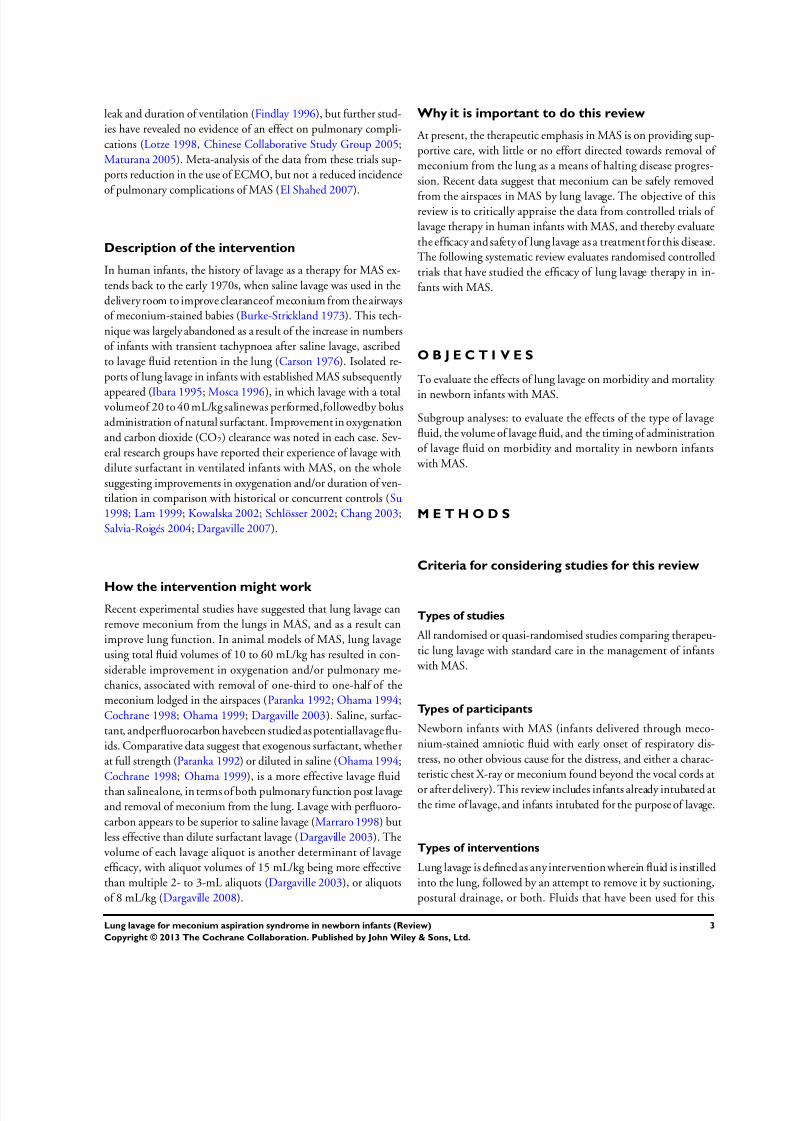
Analysis 1.1. Comparison 1 Lung lavage versus standard care, Outcome 1 Death. . . . . . . . . . . . . . 21
Analysis 1.2. Comparison 1 Lung lavage versus standard care, Outcome 2 Use of ECMO. . . . . . . . . . . 21
Analysis 1.3. Comparison 1 Lung lavage versus standard care, Outcome 3 Death or use of ECMO. . . . . . . 22
Analysis 1.4. Comparison 1 Lung lavage versus standard care, Outcome 4 Pneumothorax. . . . . . . . . . . 22
Analysis 1.5. Comparison 1 Lung lavage versus standard care, Outcome 5 Oxygenation index. . . . . . . . . 23
Analysis 1.6. Comparison 1 Lung lavage versus standard care, Outcome 6 Alveolar-arterial oxygen difference. . . . 24 Analysis 1.7. Comparison 1 Lung lavage versus standard care, Outcome 7 PaO2/FiO2. . . . . . . . . . . . 25
Analysis 2.1. Comparison 2 Lung lavage followed by surfactant bolus versus surfactant bolus, Outcome 1 Death. . . 26
Analysis 2.2. Comparison 2 Lung lavage followed by surfactant bolus versus surfactant bolus, Outcome 2 Pneumothorax. 26
26 ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
29INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iLung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 3/31
[Intervention Review]
Lung lavage for meconium aspiration syndrome in newborninfants
Seokyung Hahn1, Hyun Jin Choi2 , Roger Soll3, Peter A. Dargaville4
1Department of Medicine, Seoul National University College of Medicine, Seoul, Korea, South. 2 Department of Preventive Medicine,
Seoul National University College of Medicine, Seoul, Korea, South. 3Division of Neonatal-Perinatal Medicine, University of Vermont,
Burlington, Vermont, USA. 4 Department of Paediatrics, Royal Hobart Hospital, Hobart, Australia
Contact address: SeokyungHahn, Departmentof Medicine, Seoul NationalUniversityCollege of Medicine, 28 Yongon-dongChongno-
gu, Seoul, 110-744, Korea, South. [email protected].
Editorial group: Cochrane Neonatal Group.
Publication status and date: New, published in Issue 4, 2013.
Review content assessed as up-to-date: 15 February 2013.
Citation: Hahn S, Choi HJ, Soll R, Dargaville PA. Lung lavage for meconium aspiration syndrome in newborn infants. Cochrane
Database of Systematic Reviews 2013, Issue 4. Art. No.: CD003486. DOI: 10.1002/14651858.CD003486.pub2.
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Meconium aspiration syndrome (MAS) can occur when a newborn infant inhales a mixture of meconium and amniotic fluid into the
lungs around the time of delivery. Other than supportive measures, little effective therapy is available. Lung lavage may be a potentially
effective treatment for MAS by virtue of removing meconium from the airspaces and altering the natural course of the disease.
Objectives
To evaluate the effects of lung lavage on morbidity and mortality in newborn infants with MAS.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library ), MEDLINE, and EMBASE up
to December 2012; previous reviews including cross-references, abstracts, and conference proceedings; and expert informants. We
contacted authors directly to obtain additional data. We used the following subject headings and text words: meconium aspiration,
pulmonary surfactants, fluorocarbons, bronchoalveolar lavage, lung lavage, pulmonary lavage.
Selection criteria
Randomised controlled trials that evaluated the effects of lung lavage in infants with MAS, including those intubated for the purposeof lavage. Lung lavage was defined as any intervention in which fluid is instilled into the lung that is followed by an attempt to remove
it by suctioning and/or postural drainage.
Data collection and analysis
The review authors extracted from the reports of the clinical trial, data regarding clinical outcomes, including mortality, requirement
for extracorporeal membrane oxygenation (ECMO), pneumothorax, duration of mechanical ventilation and oxygen therapy, length of
hospital stay, indices of pulmonary function, and adverse effects of lavage. Data analysis was done in accordance with the standards of
the Cochrane Neonatal Review Group.
1Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 4/31
Main results
Only four small randomised controlled trials fulfilled the selection criteria. For one of these trials, no data are available for the control
group. Two studies compared lavage using diluted surfactant with standard care. Meta-analysis of these two studies did not show a
significant effect on mortality (typical relative risk 0.42, 95% confidence interval [CI] 0.12 to 1.46; typical risk difference -0.10, 95%
CI -0.24 to 0.04) or the use of ECMO (typical relative risk 0.27, 95% CI 0.04 to 1.86; typical risk difference -0.15, 95% CI -0.35 to
0.04). For the composite outcome of death or use of ECMO, a significant effect favoured the lavage group (typical relative risk 0.33,95% CI 0.11 to 0.96; typical risk difference -0.19, 95% CI -0.34 to -0.03; number needed to benefit [NNTB] 5). No other benefits
were reported. The other published study compared surfactant lavage followed by a surfactant bolus with surfactant bolus therapy alone
in MAS complicated by pulmonary hypertension. No significant improvements in mortality, pneumothorax, duration of mechanical
ventilation. or duration of hospitalisation were observed.
Authors’ conclusions
In infants with meconium aspiration syndrome, lung lavage with diluted surfactant may be beneficial, but additional controlled clinical
trials of lavage therapy should be conducted to confirm the treatment effect, to refine the method of lavage treatment, and to compare
lavage treatment with other approaches, including surfactant bolus therapy. Long-term outcomes should be evaluated in further clinical
trials.
P L A I N L A N G U A G E S U M M A R Y
Lung lavage for meconium aspiration syndrome in newborn infants
Meconium aspiration syndrome (MAS) is a disease of the newborn lung in which meconium, the fetal stool, is passed before birth and
then is inhaled into the lung. Little effective treatment is available, other than supportive measures including artifical respiration and,
occasionally, the use of heart-lung bypass. This review examined whether cleansing the lung using a natural chemical called surfactant,
or another similar fluid, is helpful in MAS. This cleansing procedure is known as lung lavage. Lung lavage with diluted surfactant may
help improve the clinical course of infants with MAS, in particular, the likelihood of survival without the need for heart-lung bypass.
More trials will be needed to properly evaluate lavage treatment in MAS.
B A C K G R O U N D
Description of the condition
Meconium aspiration syndrome (MAS) occurs when a newborn
infant inhales a mixture of meconium and amniotic fluid into the
lungs around the time of delivery. Intrapartum passage of meco-
nium, the viscid secretion of the fetal intestine, occurs in up to15% of deliveries at term ( Wiswell 1993). Aspiration of meco-
nium or meconium-stained amniotic fluid into the airways may
occur prenatally (during hypoxic fetal gasping), or immediately
after delivery as the first breaths are taken. Once inhaled, meco-
nium migrates down the tracheobronchial tree, causing a variable
degree of airway obstruction as it disperses into the distal airspaces
(Tran 1980). Thereafter a toxic pneumonitis ensues, with hem-
orrhagic edema and exudation of plasma proteins into the alve-
olar space (Tyler 1978; Dargaville 2001). The function of pul-
monary surfactant may be secondarily impaired, both by meco-
nium (Moses 1991), and by plasma protein (Fuchimukai 1987).
In many infants with MAS, particularly those with coexisting as-
phyxia, there is an added component of pulmonary hypertension,
which may cause profound hypoxaemia. The reported incidence
of MAS varies widely, but is of the order of 1 to 2 per 1000 live
births ( Wiswell 1993).
Approximately one-third of infants with MAS need mechanical
ventilatory support ( Wiswell 1993), and many are treated with
high-frequency ventilation or nitric oxide, or both. Infants venti-
lated for MAS are often treated with exogenous surfactant, which
appears to reduce the use of extracorporeal membrane oxygena-
tion (ECMO), but has no clear effect on mortality (Findlay 1996;
Lotze 1998; El Shahed 2007). Data regarding the effect of bo-
lus surfactant therapy on pulmonary complications of MAS are
conflicting; one small trial demonstrated a benefit in terms of air
2Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 5/31
leak and duration of ventilation (Findlay 1996), but further stud-
ies have revealed no evidence of an effect on pulmonary compli-
cations (Lotze 1998, Chinese Collaborative Study Group 2005;
Maturana 2005). Meta-analysis of the data from these trials sup-
ports reduction in the use of ECMO, but not a reduced incidence
of pulmonary complications of MAS (El Shahed 2007).
Description of the intervention
In human infants, the history of lavage as a therapy for MAS ex-
tends back to the early 1970s, when saline lavage was used in the
delivery room to improve clearanceof meconium from the airways
of meconium-stained babies (Burke-Strickland 1973). This tech-
nique was largely abandoned as a result of the increase in numbers
of infants with transient tachypnoea after saline lavage, ascribed
to lavage fluid retention in the lung (Carson 1976). Isolated re-
ports of lung lavage in infants with established MAS subsequently
appeared (Ibara 1995; Mosca 1996), in which lavage with a totalvolumeof 20 to 40 mL/kg salinewas performed,followedby bolus
administration of natural surfactant. Improvement in oxygenation
and carbon dioxide (CO2) clearance was noted in each case. Sev-
eral research groups have reported their experience of lavage with
dilute surfactant in ventilated infants with MAS, on the whole
suggesting improvements in oxygenation and/or duration of ven-
tilation in comparison with historical or concurrent controls (Su
1998; Lam 1999; Kowalska 2002; Schlösser 2002; Chang 2003;
Salvia-Roigés 2004; Dargaville 2007).
How the intervention might work Recent experimental studies have suggested that lung lavage can
remove meconium from the lungs in MAS, and as a result can
improve lung function. In animal models of MAS, lung lavage
using total fluid volumes of 10 to 60 mL/kg has resulted in con-
siderable improvement in oxygenation and/or pulmonary me-
chanics, associated with removal of one-third to one-half of the
meconium lodged in the airspaces (Paranka 1992; Ohama 1994;
Cochrane 1998; Ohama 1999; Dargaville 2003). Saline, surfac-
tant, andperfluorocarbon havebeen studied as potentiallavage flu-
ids. Comparative data suggest that exogenous surfactant, whether
at full strength (Paranka 1992) or diluted in saline (Ohama 1994;
Cochrane 1998; Ohama 1999), is a more effective lavage fluid
than salinealone, in terms of both pulmonary function post lavage
and removal of meconium from the lung. Lavage with perfluoro-
carbon appears to be superior to saline lavage (Marraro 1998) but
less effective than dilute surfactant lavage (Dargaville 2003). The
volume of each lavage aliquot is another determinant of lavage
efficacy, with aliquot volumes of 15 mL/kg being more effective
than multiple 2- to 3-mL aliquots (Dargaville 2003), or aliquots
of 8 mL/kg (Dargaville 2008).
Why it is important to do this review
At present, the therapeutic emphasis in MAS is on providing sup-
portive care, with little or no effort directed towards removal of
meconium from the lung as a means of halting disease progres-
sion. Recent data suggest that meconium can be safely removed
from the airspaces in MAS by lung lavage. The objective of thisreview is to critically appraise the data from controlled trials of
lavage therapy in human infants with MAS, and thereby evaluate
the efficacy and safety of lung lavage as a treatment for this disease.
The following systematic review evaluates randomised controlled
trials that have studied the efficacy of lung lavage therapy in in-
fants with MAS.
O B J E C T I V E S
To evaluate the effects of lung lavage on morbidity and mortality
in newborn infants with MAS.
Subgroup analyses: to evaluate the effects of the type of lavage
fluid, the volume of lavage fluid, and the timing of administration
of lavage fluid on morbidity and mortality in newborn infants
with MAS.
M E T H O D S
Criteria for considering studies for this review
Types of studies
All randomised or quasi-randomised studies comparing therapeu-
tic lung lavage with standard care in the management of infants
with MAS.
Types of participants
Newborn infants with MAS (infants delivered through meco-
nium-stained amniotic fluid with early onset of respiratory dis-
tress, no other obvious cause for the distress, and either a charac-
teristic chest X-ray or meconium found beyond the vocal cords at
or after delivery). This review includes infants already intubated atthe time of lavage, and infants intubated for the purpose of lavage.
Types of interventions
Lung lavage is defined as any intervention wherein fluid is instilled
into the lung, followed by an attempt to remove it by suctioning,
postural drainage, or both. Fluids that have been used for this
3Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 6/31
purpose include saline, full-strength and dilute surfactant, and
perfluorocarbon.
Standard care is defined as no lavage therapy, but it does include
routine suction of the endotracheal tube to maintain its patency.
For some studies, bolus surfactant therapy may be mandated as
part of standard care.
Types of outcome measures
Primary outcomes
• Death.
• Use of ECMO.
• Death or use of ECMO.
• Pneumothorax.
• All air leak (pneumothorax, pneumomediastinum,
pneumopericardium, pneumoperitoneum, pulmonary interstitial
emphysema).
• Days of mechanical ventilation via an endotracheal tube.
• Days of supplemental oxygen.
• Length of stay in hospital.
• Total cost of hospitalisation.
The composite outcome of death or use of ECMO has been in-
cluded in recognition that mortality is influenced by the availabil-
ity of ECMO.
Secondary outcomes
• Indices of pulmonary function (including Oxygenation
Index, Alveolar-arterial oxygen difference, PF ratio) measured at
24, 48, and 72 hours.[definitions: Oxygenation index (OI) = (Mean airway pressure ×
FiO2)/PaO2; Alveolar-arterial oxygen difference (AaDO2)=FiO2
× 713 PaCO2/0.8 PaO2; PF Ratio = PaO2/FiO2]
Lung mechanics (compliance and resistance of the lung or the
respiratory system):
• Adverse effects of lavage (acute hypoxaemia, bradycardia,
hypotension).
Search methods for identification of studies
We used the standard search methods of the Cochrane Neonatal
Review Group.
Electronic searches
We used the standardized search strategy of the Neonatal Review
Group as outlined in The Cochrane Library. The followingsources
were searched between 1966 and December 2012 for eligible stud-
ies in any language:
• Cochrane Neonatal Review Group trials register.
• CENTRAL (The Cochrane Library , Issue 11, 2012).
• MEDLINE and EMBASE electronic searches.
We constructed search strategies using the following MeSH terms
or keywords: meconium, meconium aspiration syndrome, pul-monary surfactants, lung surfactant, fluorocarbons, bronchoalve-
olar lavage, lung lavage, and pulmonary lavage.
Searching other resources
We screened for trials in conference proceedings of annual meet-
ings of the American Thoracic Society, the Society for Pediatric
Research, the European Respiratory Society, and the European So-
ciety for Pediatric Research (December 2012); and in the reference
lists from the retrieved articles and from review articles. We had
personal communications with primary authors of the identified
studies to identify unpublished data. We searched for any ongoing or recently completed and un-
published trials using clinicaltrials.gov, controlled-trials.com, and
who.int/ictrp.
Data collection and analysis
We used the methods of the Cochrane Neonatal Review Group
for data collection and analysis.
Selection of studies
We included all randomised and quasi-randomised controlled tri-
als that fulfilled the selection criteria described in the previous sec-
tion. Two review authors independently reviewed the results of
the updated search and selected studies for inclusion. We resolved
any disagreement by discussion.
Data extraction and management
We used a standard form for data extraction, which included a
collection of descriptive data on the study design, the study pop-
ulation (baseline characteristics and inclusion and exclusion cri-
teria), and the method of intervention (type of lavage fluid, total
lavage volume, aliquot volume, and lavage fluid concentration),
and quantitativedata regarding the outcome measures.Pneumoth-
orax was counted only if it occurred after randomisation.
Two review authors independently extracted the data from in-
cluded studies, and results were compared. The investigators of
included studies were asked to provide unpublished outcome data
where necessary.
4Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 7/31
Assessment of risk of bias in included studies
The quality of eligible studies was assessed using The Cochrane
Collaboration’s tool for assessing the risk of bias for randomised
controlled trials (RCTs) (Higgins 2011). Two review authors per-
formed the assessment, and they resolved any difference of opin-
ion by involving coauthors in the discussion.The methodological quality of the studies was assessed using the
following criteria:
• Sequence generation (checking for possible selection bias):
For each included study, we categorized the method used to
generate the allocation sequence as follows:
◦ Low risk (any truly random process, e.g. random
number table; computer random number generator).
◦ High risk (any nonrandom process, e.g. odd or even
date of birth; hospital or clinic record number).
◦ Unclear risk.
• Allocation concealment (checking for possible selection
bias): For each included study, we categorized the method used
to conceal the allocation sequence as follows:◦ Low risk (e.g. telephone or central randomisation;
consecutively numbered sealed opaque envelopes).
◦ High risk (open random allocation; unsealed or non-
opaque envelopes, alternation; date of birth).
◦ Unclear risk.
• Blinding (checking for possible performance bias): For each
included study, we categorized the methods used to blind study
participants and personnel from knowledge of which
intervention a participant received. Blinding was assessed
separately for different outcomes or classes of outcomes. We
categorized the methods as follows:
◦ Low risk, high risk, or unclear risk for participants.
◦ Low risk, high risk, or unclear risk for personnel.◦ Low risk, high risk, or unclear risk for outcome
assessors.
• Incomplete outcome data (checking for possible attrition
bias through withdrawals, dropouts, and protocol deviations):
For each included study and for each outcome, we described the
completeness of data, including attrition and exclusions from the
analysis. We noted whether attrition and exclusions were
reported, the numbers included in the analysis at each stage
(compared with the total randomly assigned participants),
reasons for attrition or exclusion where reported, and whether
missing data were balanced across groups or were related to
outcomes. Where sufficient information was reported or
supplied by the trial authors, we included missing data in the
analyses again. We categorized the methods as follows:
◦ Low risk (< 20% missing data).
◦ High risk (≥ 20% missing data).
◦ Unclear risk.
• Selective reporting bias: For each included study, we
described how we investigated the possibility of selective
outcome reporting bias and what we found. We assessed the
methods as follows:
◦ Low risk (where it is clear that all of the study’s pre-
specified outcomes and all expected outcomes of interest to the
review have been reported).
◦ High risk (where not all of the study’s pre-specified
outcomes have been reported; one or more reported primary outcomes were not pre-specified; outcomes of interest are
reported incompletely and so cannot be used; or study fails to
include results of a key outcome that would have been expected
to have been reported).
◦ Unclear risk.
• Other sources of bias: For each included study, we
described any important concerns that we had about other
possible sources of bias (e.g. whether a potential source of bias
was related to the specific study design, or whether the trial was
stopped early as the result of some data-dependent process). We
assessed whether each study was free of other problems that
could put it at risk of bias as follows:
◦
Low risk; high risk; unclear risk.• Overall risk of bias [described in Table 8.5c in the
Handbook].
We made explicit judgements regarding whether studies were at
high risk of bias, according to the criteria given in The Cochrane
Handbook (Higgins 2011). With reference to (1) to (6) above,
we assessed the likely magnitude and direction of the bias, and
whether we considered it likely to influence the findings. If needed,
we planned to explore the impact of the level of bias by undertaking
sensitivity analyses (see Sensitivity analysis, later).
Measures of treatment effect
We performed statistical analyses using Review Manager software(RevMan 2011). Dicotomous data were analysed using relative
risk (RR), risk difference (RD), and the number needed to benefit
(NNTB) or the number needed to harm (NNTH). The 95%
confidence intervals (CIs) were reported on all estimates.
Some continuous outcomes are only descriptively presented in
a table without statistical pooling because of the skewed nature
of the data; the weighted mean difference (WMD) was used for
pooling otherwise.
Dealing with missing data
For included studies, levels of attrition were noted. The impact
of including studies with high levels of missing data in the overall
assessment of treatment effect was explored through sensitivity
analysis.
All outcome analyses were performed on an intention-to-treat
basis(i.e. we included all participants randomly assigned to each
group in the analyses). The denominator for each outcome in each
trial was the number randomly assigned minus any participants
whose outcomes were known to be missing.
5Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 8/31
Assessment of heterogeneity
We examined heterogeneity between trials by inspecting the forest
plots and quantifying the impact of heterogeneity using the I2
statistic. If noted, we planned to explore the possible causes of
statistical heterogeneity using pre-specified subgroup analyses (e.g.
differences in study quality, participants, intervention regimens,or outcome assessments).
Assessment of reporting biases
We planned to assess possible publication bias and other biases
using symmetry/asymmetry of funnel plots, but this was not ap-
plicable because an insufficient number of studies was included in
the meta-analysis for such an exploration.
For included trials that were recently performed (and there-
fore were prospectively registered), we explored possible selec-
tive reporting of study outcomes by comparing primary and sec-
ondary outcomes given in the reports versus primary and sec-ondary outcomes proposed at trial registration, using the Websites
www.clinicaltrials.gov and www.controlled-trials.com. If such dis-
crepancies were found, we planned to contact the primary investi-
gators to obtain missing outcome data on outcomes pre-specified
at trial registration.
Data synthesis
Where meta-analysis was judged to be appropriate, the analysis
was done using Review Manager software (RevMan 2011), as sup-
plied by The Cochrane Collaboration. We used the Mantel-Haen-
szel method to obtain estimates of typical relative risk and risk
difference. A fixed-effect model was primarily used for the meta-analysis after the statistical heterogeneity was investigated. Data
were analysed on an intention-to-treat basis.
Subgroup analysis and investigation of heterogeneity
Three subgroup analyses were planned a priori:
• Type of lavage fluid (saline, surfactant, perfluorocarbon,
other).
• Lavage aliquot volume (< 5 mL/kg, ≥ 5 mL/kg).
• Timing of lavage: early (< 6 hours of life) or late (≥ 6 hours
of life).
Sensitivity analysis
We planned sensitivity analyses for use in situations where this
might affect the interpretation of significant results (e.g. where
risk of bias is associated with the quality of some of the included
trials or missing outcome data). None were thought necessary in
this review.
R E S U L T S
Description of studies
See: Characteristicsof included studies; Characteristicsof excluded
studies; Characteristics of ongoing studies.
Results of the search
Four randomised controlled trials were identified, one of which
(Ogawa 1997) was excluded as data on the nonlavaged control
group were not reported andare not now obtainable. In that study,
which has been published only in conference proceedings format,
six infants underwent lavage with five aliquots each of 2 mL/kg of
Surfacten-TA (6 mg/mL), and a further four infants received an
identicallavage using saline. Oxygenation and CO2 clearance were
better in the group lavaged with dilute surfactant than with saline,
but no formal comparisons with the control group are reported.
Included studies
Three studies are included in this review ( Wiswell 2002;
Gadzinowski 2008; Dargaville 2011).
Wiswell 2002 performed a phase I/II randomised controlled trial
of surfactant lavage in conventionally ventilated infants with MAS
who were at least 35 weeks’ gestation and less than 72 hours of age,
and had an oxygenation index (OI) between 8 and 25 inclusive
on two separate blood gas analyses within a three-hour period.
Surfactant lavage was performed at a mean age of 14 hours using
6 aliquots of 8 mL/kg of KL4 (Surfaxin, Discovery Laboratories
Inc, Doylestown, PA). The concentration of surfactant phospho-lipid was 2.5 mg/mL for the first four aliquots, and 10 mg/mL
for the last two. Each lavage aliquot was instilled via the endotra-
cheal tube while positive end-expiratory pressure continued, fol-
lowed by closed endotracheal suctioning for 10 seconds, during
which positive-pressure ventilation was re-instituted. The infant’s
physiological state was allowed to recover after each lavage aliquot
before the next was administered. After the final aliquot, positive
end-expiratory pressure was maintained at 6 to 8 cm H2O for at
least two hours. Control infants received conventional mechanical
ventilation and standard supportive measures at the discretion of
the site study investigator. In both groups, a treatment failure cri-
terion (OI > 25 or OI 50% above baseline) had to be reached be-
fore rescue therapies such as high-frequency oscillatory ventilation
(HFOV), bolus surfactant therapy, inhaled nitric oxide (iNO),
and ECMO could be used.
Dargaville 2011 performed a multicenter randomised controlled
trial of diluted surfactant lavage in infants who had a diagnosis of
MAS. The infants were at least 36 weeks’ gestation and 2 kg birth
weight, less than 24 hours of age, and mechanically ventilated with
a mean airway pressure of at least 12 cm H2O and an alveolar-
6Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 9/31
arterial O2 difference (AaDO2) of at least 450 mmHg on two se-
quential blood gases. Surfactant lavage was performed at a mean
age of 13 hours using two aliquots of 15 mL/kg of bovine sur-
factant (Survanta, Abbott Laboratories, Columbus, OH) diluted
with saline to a phospholipid concentration of 5 mg/mL. Lavage
fluid was instilled over 20 seconds through a dispensing catheter with the ventilator circuit disconnected. Three positive-pressure
inflations were then administered, followed by disconnection of
the ventilator circuit and suctioning of the instilled fluid. Control
infants received mechanical ventilation and standard supportive
measures. In both groups, ventilator management and the use of
HFOV, iNO, and bolus surfactant therapy were at the discretion
of the site study investigator, as wasthe decision to refer to ECMO.
Gadzinowski 2008 performed a randomised controlledtrial of sur-
factant lavage followed by bolus surfactant treatment compared
with bolus surfactant treatment alone for MAS with pulmonary
hypertension. The infants were at least 35 weeks’ gestation and
less than 24 hours of age, and the diagnosis of pulmonary hyper-
tension was based on standardised echocardiographic parameters.Surfactant lavage was performed with a total lavage volume of 15
mL/kg and an aliquot volume of 3.75 mL/kg at the mean age of
9.7 hours, using diluted bovine surfactant (Survanta) at a phos-
pholipid concentration of 5 mg/mL. Lavage and suctioning were
conducted via a closed system in four body positions: on the right
and left sides, and in the Trendelenburg and anti-Trendelenburg
positions. After the lavage treatment, one dose of bolus surfactant
(Survanta, 100 mg/kg) was given. The control group received one
dose of bolus surfactant (Survanta, 100 mg/kg) and conventional
treatment. After an echocardiographic assessment was conducted,
iNO was administered to both groups.
Excluded studies
Twelve studies were excluded from the analysis (Burke-Strickland
1973; Carson 1976; Rosegger 1987; Ogawa 1997; Su 1998; Lam
1999; Schlösser 2002; Kowalska 2002; Chang 2003; Salvia-Roigés
2004; Dargaville 2007; Armenta 2011). The rationale for exclu-
sion is given in the table Characteristics of excluded studies.
Ongoing studies
Ongoing or unpublished trials are noted in the table
Characteristics of ongoing studies (McNamara 2006; Segal 2012;
Sur-Lu-Lav 2011).
Risk of bias in included studies
In the study by Wiswell et al ( Wiswell 2002), randomisation was
performed by drawinga randomisationslip froma closedenvelope,
with an allocation ratio of 2:1 (lavage:standard care). Treatment
was not blinded to the clinical team, although the one-year follow-
up was performed by an investigator who was blinded to the al-
location. No exclusions were noted after randomisation, although
three of the 15 infants randomly assigned to surfactant lavage did
not receive the complete lavage series, two infants received only
four of the scheduledsix lavage aliquots, andanother received only
two aliquots. For the purposes of analysis, allinfants were includedin their respective allocation groups. Other bias may have existed
in that the number of infants receiving rescue therapy exceeded
the number reaching treatment failure criteria, even though rescue
therapies were not permitted unless infants met treatment failure.
The study was conducted without a formal sample size calculation
and based on an estimate for assessing safety and potential efficacy
in a rather exploratory fashion.
The study by Dargaville et al (Dargaville 2011) described an
adequate process of randomisation and allocation concealment.
Among 66 enrolled infants, one infant randomly assigned to the
surfactant lavage group was too unstable to receive lavage and was
deemed to have been ineligible for enrolment. The intervention
was not blinded.In the study by Gadzinowski et al (Gadzinowski 2008), no infor-
mation is provided about random sequence generation, allocation
concealment, and blinding of the intervention.
Effects of interventions
LUNG LAVAGE VERSUS STANDARD CARE (Comparison
1)
Two studies compared lung lavage with standard care (Dargaville
2011; Wiswell 2002).
Death (Outcome 1.1)
Both studies reported on mortality, and one RCT reported no
events. No treatment effect on death was noted (typical RR 0.42,95% CI 0.12 to 1.46; typical RD -0.10, 95% CI -0.24 to 0.04)
( Analysis 1.1).
Use of ECMO (Outcome 1.2)
Both RCTs reported on the number of infants who needed
ECMO.Inonestudy(Dargaville 2011),only25 ofthe 66enrolled
infants were treated at centres at which ECMO was available. No
difference in the relative risk of ECMO was noted, although a
trend toward an interventional benefit was observed (typical RR
0.27, 95% CI 0.04 to 1.86; typical RD -0.15, 95% CI -0.35 to
0.04) ( Analysis 1.2).
Death or use of ECMO (Outcome 1.3)
For both studies, the numbers of infants who received ECMO or
died could be calculated. Surfactant lavage significantly decreased
the combined outcome of death or requirement for ECMO (typ-
ical RR 0.33, 95% CI 0.11 to 0.96: typical RD -0.19, 95% CI
-0.34 to -0.03; NNTB 5) ( Analysis 1.3). Each study showed a
result favouring the intervention.
Pneumothorax (Outcome 1.4)
Both studies reported on pneumothorax, but not on other air
leaks. No significant difference was observed between treatment
7Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 10/31
groups (typical RR 0.38, 95% CI 0.08 to 1.90, typical RD -0.07,
95% CI -0.19 to 0.05) ( Analysis 1.4).
Days of mechanical ventilation
Duration of ventilation showed wide variation in both studies.
Median duration for mechanical ventilation was shorter in the
intervention group for both studies (Dargaville 2011); median5.0versus6.3 days ( Wiswell 2002); median4.6 versus7.6 days) (Table
1).
Days of supplemental oxygen
Dargaville 2011 reported days of oxygen therapy only for
survivors.The values were a little different between groups:
(Dargaville 2011): median 14 versus 14 days ( Wiswell 2002):
mean 13.5 versus 12.1 days (Table 1).
Length of hospital stay
One study ( Wiswell 2002) reported length of stay in the Neonatal
Intensive Care Unit, which differed little between groups (mean
12.7 vs 13.1 days). In the other study, the length of hospital stay
was similar in the two groups (Dargaville 2011): median 17 versus
19 days (Table 1).Total cost of hospitalisation
None of the studies reported hospitalisation cost.
Indices of pulmonary function (Outcomes 1.5 and 1.6)
Both RCTs reported OI measured at 24, 48, and 72 hours. A
significant difference between groups was observed at 48 hours
after lavage treatment (WMD -6.20, 95% CI -12.11 to -0.29)
( Analysis 1.5). AaDO2 and pulmonary function (PF) ratio were
measured in one study (Dargaville 2011), which did not show
any significant differences between groups, although better results
appeared to be obtained in the treatment group over time after
use of lavage therapy ( Analysis 1.6). Lung mechanics were not
reported in either study.
Adverse effectsIn one study ( Wiswell 2002), the instillation and recovery of the
six lavage aliquots took 50 to 60 minutes. In two infants the hy-
poxaemia that occurred during lavage was sufficiently pronounced
to halt the lavage procedure. Overall 5 of 15 infants required hand
ventilation to recover oxygen saturation after lavage. In one other
infant, the lavage procedure was stopped because of hypotension,
although this infant had coincident gram-negative sepsis. The oc-
currence and severity of episodes of hypoxaemia or hypotension
are not reported in the control group, and thus it is not possible
to make direct comparisons between groups. In the other study
(Dargaville 2011), two infants experienced transient bradycardia
at less than 100 beats per minute during lavage, with recovery by
five minutes after lavage. Five infants had an oxygen saturationbelow 80% for longer than 10 minutes, with recovery to above
90% within 40 minutes in all cases. Six infants needed treatment
for hypotension during or immediately after lavage. Overall, car-
diopulmonary indices were affected transiently, and the lavaged
infants and the control infants showed similar blood gas indices at
four hours post lavage. One infant died of intractable pulmonary
hypertension three hours after lavage.
LUNG LAVAGE FOLLOWED BY SURFACTANT BOLUS
VERSUS SURFACTANT BOLUS THERAPY FOR MAS
WITH PULMONARY HYPERTENSION (Comparison 2)
One study compared lung lavage followed by surfactant bolus ver-
sus surfactant bolus therapy for MAS with pulmonary hyperten-
sion (Gadzinowski 2008).Death (Outcome 2.1)
Nodifference in therelative risk of mortalitywas noted;two deaths
were reported in the control group versus none in the lavage group
(RR 0.17, 95% CI 0.01 to 3.06) ( Analysis 2.1).
Pneumothorax (Outcome 2.2)
No difference in the relative risk of pneumothorax was noted; two
episodes of pneumothorax were reported in the control group but
nonein the lavagegroup(RR0.17, 95% CI0.01 to3.06) ( Analysis
2.2).
Days of mechanical ventilation
The difference between mean values in days of mechanical venti-
lation was less than one day (mean ± standard deviation [SD] 6.6
± 2.6 vs 7.3 ± 1.7 days) (Table 2).Length of the hospital stay
The length of hospital stay appeared to be shorter in the interven-
tion group (mean ± SD: 16.4 ± 5.4 vs 19.8 ± 2.9 days) (Table 2).
Indices of pulmonary function As a result of the small size of the study (7 vs 6 for treatment
vs control) and the skewed nature of the data (large difference
between reported mean and median values), we did not assess
the significance based on the test of means but just descriptively
presented the results (Table 3). The median value of OI measured
at 24 hours in the surfactant lavage group was lower than that
in the control group (2.8 vs 9.0). The OI measured at 48 hours
was, however,similar between groups (median 1.7 vs 1.8). AaDO2
measured at 24 and 48 hours in the lavage group appeared to belower than in the control group. Compliance and resistance are
not reported.
Adverse effectsExcept for pneumothorax and death, adverse effects were not re-
ported.
SUBGROUP ANALYSES
None of the planned subgroup analyses were possible.
Type of lavage fluid
All included studies used diluted surfactant for lavage.
Lavage aliquot volume
The aliquot volume was at least 5 mL/kg in all studies comparing
surfactant lavage with standard care, and less than 5 mL/kg in the
study comparing surfactant lavage followed by bolus surfactant with surfactant bolus therapy.
Timing of lavageThe mean age when lavage was performed was greater than six
hours in all included studies.
8Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 11/31
D I S C U S S I O N
Therapeutic lunglavage is an emergingtreatmentfor MAS,which,
by virtue of removal of meconium from the lung, would appear
to have a potential advantage over the supportive measures cur-
rently employed for thiscondition. Thisreview has identified three
small randomised controlled trials of lung lavage using surfactant( Wiswell 2002; Gadzinowski 2008; Dargaville 2011).
In the meta-analysis of the trials comparing surfactant lavage and
standard care ( Wiswell 2002; Dargaville 2011), a significant dif-
ference was noted in the composite outcome of death or use of
ECMO. Analysis of this outcome was necessary given that the
availability of ECMO clearly affects mortality. Any other primary
outcomes including mortality, pneumothorax, or use of ECMO
did not demonstrate a significant benefit. Among the secondary
outcomes examining pulmonary function, only OI at 48 hours
was improved significantly in the surfactant lavage group. In one
study in which a large total volume of lavage fluid was used, the
lavage procedure was relatively protracted and in some cases washalted because of concern regarding hypoxaemia or hypotension
( Wiswell 2002). In the other study, the lavage procedure was com-
pleted in all infants, but some experienced transient bradycardia
and hypotension.
The two studies comparing surfactant lavage with standard care
varied considerably in the severity of disease of enrolled infants
at the time of recruitment ( Wiswell 2002; Dargaville 2011). In
the study of Wiswell et al, infants with MAS of lesser severity
were targeted (mean OI 12 at enrolment), and no deaths and
relatively rapid weaning from ventilation were noted, in particular
in the lung lavage group. By contrast, the other study focused on
infants with severe disease (mean OI 25 at enrolment) (Dargaville2011). In this case, no difference was discernible in duration of
mechanical ventilation, which was relatively prolonged in both
groups, but fewer infants who underwent lavage died or required
ECMO. This suggests that lung lavage has the greatest potential
for benefit in infants with severe disease, although the possibility
of an impact in milder cases on duration of ventilation or other
pulmonary outcomes needs further exploration.
The study comparing surfactant lavage followed by bolus surfac-
tant with surfactant bolus therapy (Gadzinowski 2008) did not
show an effect on mortality, pneumothorax, days on mechanical
ventilation, or length of hospital stay. The intervention seemed to
improve oxygenation, with a lower OI at 24 hours.
Because of the small number of RCTs and the lack of sufficient
numbers of infantsrandomly assigned,the evidenceregarding lung
lavage in MAS is thought to be insufficient to allow firm conclu-
sions, although a beneficial effect is noted in some important out-
comes. A recent systematic review focusing on surfactant lavage
therapy reviewed existing RCTs together with non-randomisedcontrolled studies for supporting evidence; the results of meta-
analysis also suggested that surfactant lavage had significant effects
on mortality and morbidity for MAS (Choi 2012).
Subgroup analyses according to type of lavage fluid, lavage aliquot
volume, and timing of lavage were planned. However, none of the
planned subgroup analyses were possible. Additional studies will
be needed to fully assess the impact of these factors on the success
of lung lavage in MAS.
Of the few RCTs identified, only one was judged to have a low risk
of bias. The protocols of the other two studies were unavailable
for full assessment.
Further randomised controlled trials of lung lavage are needed toproperly evaluate the safety and efficacy of this treatment. A phase
III RCT (Segal 2012) evaluating the effect of surfactant lavage
compared with standard care had been registered, and is recorded
to have been terminated without completion. One trial compar-
ing lavage with diluted surfactant versus standard care is currently
under way (McNamara 2006) and is aiming to recruit 60 infants.
Another trial (Sur-Lu-Lav 2011) undertaken to investigate the ef-
fect of surfactant lavage compared with standard care is registered.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
In infants with MAS, lung lavage with diluted surfactant may be
of benefit, but more evidence is required to allow firm conclusions
to be drawn.
Implications for research
Further controlledclinical trialsof lung lavagein MAS are required
to confirm the treatment effect, refine the method of lavage, and
compare lung lavage versus other approaches, including surfactant
bolus therapy. Outcomes to be evaluated in further clinical trials
should include short- and long-term clinical outcomes, and any
adverse effects of lavage.
9Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 12/31
R E F E R E N C E S
References to studies included in this review
Dargaville 2011 {published data only}
Dargaville PA, Copnell B, Mills JF, Haron I, Lee JK,
Tingay DG, et al.Randomized controlled trial of lung lavage with dilute surfactant for meconium aspiration syndrome.
Journal of Pediatrics 2011;158(3):383–9.
Gadzinowski 2008 {published data only}
Gadzinowski J, Kowalska K, Vidyasagar D. Treatment of
MAS with PPHN using combined therapy: SLL, bolus
surfactant and iNO. Journal of Perinatology 2008;28(Suppl
3):S56–66.
Wiswell 2002 {published data only}
Wiswell TE, Knight GR, Finer NN, Donn SM, Desai H,
Walsh WF, et al.A multicenter, randomized, controlled trial
comparing Surfaxin (Lucinactant) lavage with standard care
for treatment of meconium aspiration syndrome. Pediatrics
2002;109(6):1081–7.
References to studies excluded from this review
Armenta 2011 {published data only}
Armenta JMV, Urbina EC, Herrera JC. Surfactant bronchial
lavage in meconium aspiration syndrome: A comparative
study. Intensive Care Medicine 2011;37:S317.
Burke-Strickland 1973 {published data only}
Burke-Strickland M, Edwards NB. Meconium aspiration in
the newborn. Minnesota Medicine 1973;56:1031–5.
Carson 1976 {published data only}
Carson BS, Losey RW, Bowes WAJ, Simmons MA.
Combined obstetric and pediatric approach to prevent
meconium aspiration syndrome. American Journal of
Obstetrics and Gynecology 1976;126(6):712–5.Chang 2003 {published data only}
Chang HY, Hsu CH, Kao HA, Hung HY, Chang JH,
Peng CC, et al.Treatment of severe meconium aspiration
syndrome with dilute surfactant lavage. Journal of the
Formosan Medical Association 2003;102(5):326–30.
Dargaville 2007 {published and unpublished data}
Dargaville PA, Mills JF, Copnell B, Loughnan PM,
McDougall PN. Therapeutic lung lavage in meconium
aspiration syndrome: a preliminary report. Journal of
Paediatric and Child Health 2007;43(7):539–45.
Kowalska 2002 {published data only}
Kowalska K, Szymankiewicz M, Gadzinowski J. An
effectiveness of surfactant lung lavage (SLL) in meconium
aspiration syndrome (MAS) [Skutecznosc plukania
drzewa tchawiczo–oskrzelowego roztworem naturalnego
surfaktantu (SLL) w leczeniu zespolu aspiracji smolki
(MAS) – doniesienie wstepne]. Przeglad Lekarski. 2002;
Vol. 59 Suppl 1:21–4.
Lam 1999 {published data only}
Lam BCC, Yeung CY. Surfactant lavage for meconium
aspiration syndrome: a pilot study. Pediatrics 1999;103(5
Pt 1):1014–18.
Ogawa 1997 {published data only}
Ogawa Y. Bronchial lavage with surfactant solution for
the treatment of meconium aspiration syndrome. Hot
Topics in Neonatology Conference Book. Chicago: Ross
Laboratories, 1997:259–64.
Rosegger 1987 {published data only}
Rosegger H, Engele H, Haas J. Tracheobronchial
lavage a supplementary measure in the initial
management of meconium aspiration syndrome
[Tracheobronchiallavage eine ergänzende Maßnahme
zur erstversorgung beim mekoniumaspirationssyndrom].
Wiener Klinische Wochenschrift 1987;99(24):843–7.
Salvia-Roigés 2004 {published data only}
Salvia-Roigés MD, Carbonell-Estrany X, Figueras-Aloy
J, Rodriguez-Miguélez JM. Efficacy of three treatment
schedules in severe meconium aspiration syndrome. Acta
Paediatrica 2004;93(1):60–5.
Schlösser 2002 {published data only}
Schlössser RL, Veldman A, Fischer D, Allendorf A, von
Loewenich V. Lavage with exogenous surfactant in neonatal
meconium aspiration syndrome [Lavage mit exogenem
surfactant bei neonataler mekoniumaspiration]. Zeitschrift
für Geburtshilfe und Neonatologie. 2002;206(1):15–8.
Su 1998 {published data only}
Su BH, Hu PS, Peng CT, Tsai CH. The effect of bronchial
lavage and surfactant supplement on severe meconium
aspiration syndrome. Mid-Taiwan Journal of Medicine
1998;3:191–7.
References to ongoing studies
McNamara 2006 {unpublished data only}
McNamara P. Surfactant lavage vs. Bolus surfactant in
neonates with meconium aspiration. ClinicalTrials.gov
(http://www.clinicaltrials.gov/ct2/show/NCT00312507?
term=McNamara&rank=1) (accessed 19.02.2013).
Segal 2012 {unpublished data only}
Wiswell TE. Phase III randomized study of lucinactant
in full term newborn infants with meconium aspiration
syndrome. ClinicalTrials.gov (http://clinicaltrials.gov/show/
NCT00004500) (accessed 19.02.2013).
Sur-Lu-Lav 2011 {unpublished data only}
Nangia S. Comparison of surfactant lung lavage with
standard care in the treatment of meconium aspiration
syndrome (Sur-Lu-Lav). ClinicalTrials.gov(http://
clinicaltrials.gov/ct2/show/NCT01310621?term=Sur-Lu-
Lav&rank=1) (accessed 19.02.2013).
Additional references
Chinese Collaborative Study Group 2005
Chinese Collaborative Study Group for Neonatal
respiratory Diseases. Treatment of severe meconium
aspiration syndrome with porcine surfactant: a multicentre,
10Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 13/31
randomized, controlled trial. Acta Paediatrica 2005;94(7):
896–902.
Choi 2012
Choi HJ, Hahn S, Lee J, Park BJ, Lee SM, Kim HS,
et al.Surfactant lavage therapy for meconium aspiration
syndrome: a systematic review and meta-analysis.
Neonatology 2012;101(3):183–91.
Cochrane 1998
Cochrane CG, Revak SD, Merritt TA, Schraufstatter IU,
Hoch RC, Henderson C, et al.Bronchoalveolar lavage
with KL4-surfactant in models of meconium aspiration
syndrome. Pediatric Research 1998;44(5):705–15.
Dargaville 2001
Dargaville PA, South M, McDougall PN. Surfactant and
surfactant inhibitors in meconium aspiration syndrome.
Journal of Pediatrics 2001;138(1):113–5.
Dargaville 2003
Dargaville PA, Mills JF, Headley BM, Chan Y, Coleman L,
Loughnan PM, et al.Therapeutic lung lavage in the piglet
model of meconium aspiration syndrome. American Journal of Respiratory and Critical Care Medicine 2003;168(4):
456–63.
Dargaville 2008
Dargaville PA, Copnell B, Tingay DG, Gordon MJ, Mills
JF, Morley CJ. Refining the method of therapeutic lung
lavage in meconium aspiration syndrome. Neonatology
2008;94(3):160–3.
El Shahed 2007
El Shahed AI, Dargaville P, Ohlsson A, Soll RF. Surfactant
for meconium aspiration syndrome in full term/near term
infants. Cochrane Database of Systematic Reviews 2007, Issue
3. [DOI: 10.1002/14651858.CD002054.pub2]
Findlay 1996
Findlay RD, Taeusch HW, Walther FJ. Surfactant
replacement therapy for meconium aspiration syndrome.
Pediatrics 1996;97(1):48–52.
Fuchimukai 1987
Fuchimukai T, Fujiwara T, Takahashi A, Enhorning G.
Artificial pulmonary surfactant inhibited by proteins.
Journal of Applied Physiology 1987;62(2):429–37.
Higgins 2011
Higgins JPT, Green S (editors). Cochrane Handbook
for Systematic Reviews of Interventions. Version 5.1.0
[updated March 2011]. The Cochrane Collaboration,
2011. Available from www.cochrane-handbook.org.
Ibara 1995
Ibara S, Ikenoue T, Murata Y, Sakamoto H, Saito T,Nakamura Y, et al.Management of meconium aspiration
syndrome by tracheobronchial lavage and replacement of
Surfactant-TA. Acta Paediatrica Japonica 1995;37(1):64–7.
Lotze 1998
Lotze A, Mitchell BR, Bulas DI, Zola EM, Shalwitz RA,
Gunkel JH, et al.Multicenter study of surfactant (beractant)
use in the treatment of term infants with severe respiratory
failure. Journal of Pediatrics 1998;132(1):40–7.
Marraro 1998
Marraro G, Bonati M, Ferrari A, Barzaghi MM, Pagani
C, Bortolotti A, et al.Perfluorocarbon broncho-alveolar
lavage and liquid ventilation versus saline broncho-alveolar
lavage in adult guinea pig experimental model of meconium
inhalation. Intensive Care Med 1998;24(5):501–8.
Maturana 2005
Maturana A, Torres-Pereyra J, Salinas R, Astudillo P, Moya
FR, The Chile Surf Group. A randomized trial of natural
surfactant for moderate to severe meconium aspiration
syndrome. PAS. 2005; Vol. 57:1545.
Mosca 1996
Mosca F, Colnaghi M, Castoldi F. Lung lavage with a saline
volume similar to functional residual capacity followed
by surfactant administration in newborns with severe
meconium aspiration syndrome. Intensive Care Med 1996;
22(12):1412–3.
Moses 1991
Moses D, Holm BA, Spitale P, Liu MY, Enhorning G.
Inhibition of pulmonary surfactant function by meconium. American Journal of Obstetrics and Gynecology 1991;164(2):
477–81.
Ohama 1994
Ohama Y, Itakura Y, Koyama N, Eguchi H, Ogawa Y.
Effect of surfactant lavage in a rabbit model of meconium
aspiration syndrome. Acta Paediatrica Japonica 1994;36(3):
236–8.
Ohama 1999
Ohama Y, Ogawa Y. Treatment of meconium aspiration
syndrome with surfactant lavage in an experimental rabbit
model. Pediatric Pulmonology 1999;28(1):18–23.
Paranka 1992
Paranka MS, Walsh WF, Stancombe BB. Surfactant lavage
in a piglet model of meconium aspiration syndrome.Pediatric Research 1992;31(6):625–8.
RevMan 2011
The Nordic Cochrane Centre. The Cochrane Collaboration.
Review Manager (RevMan). 5.2. Copenhagan: The Nordic
Cochrane Centre. The Cochrane Collaboration, 2011.
Tran 1980
Tran N, Lowe C, Sivieri EM, Shaffer TH. Sequential effects
of acute meconium obstruction on pulmonary function.
Pediatric Research 1980;14(1):34–8.
Tyler 1978
Tyler DC, Murphy J, Cheney FW. Mechanical and chemical
damage to lung tissue caused by meconium aspiration.
Pediatrics 1978;62(4):454–9.
Wiswell 1993
Wiswell TE, Bent RC. Meconium staining and the
meconium aspiration syndrome. Unresolved issues.
Pediatric Clinics of North America 1993;40(5):955–81.
Wiswell 2000
Wiswell TE, Gannon CM, Jacob J, Goldsmith L, Szyld
E, Weiss K, et al.Delivery room management of the
apparently vigorous meconium-stained neonate: results of
11Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 14/31
the multicenter, international collaborative trial. Pediatrics
2000;105(1 Pt 1):1–7.∗ Indicates the major publication for the study
12Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 15/31
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Dargaville 2011
Methods International multicenter randomised controlled trial. 13 participating centres. Ran-
domisation blinded, with a 1:1 allocation ratio
Intervention not blinded to either clinical team or assessors of in-hospital outcomes.
Complete follow-up with blinded assessment of outcome at two years of age (not yet
reported)
Participants 66 infants from 13 participating centres, who were of at least 36 weeks’ gestation and 2
kg birth weight, less than 24 hours of age, with a diagnosis of MAS. The infants were
eligible for enrolment if they were mechanically ventilated with mean airway pressure
of at least 12 cm H2O and an alveolar-arterial oxygen difference of at least 450 mmHg
on two sequential blood gases. Subsequent improvement in oxygenation was allowableas long as FiO2 remained > 0.5 before randomisation. One infant randomly assigned
to the lavage group who did not receive lavage was found to be ineligible because of
cardiopulmonary instability. 30 infants received surfactant lavage and 35 received no
lavage
Interventions Surfactant lavage with total volume of 30 mL/kg, divided into two aliquots of 15 mL/
kg of bovine surfactant (Survanta, Abbott Laboratories, Columbus OH) with a phos-
pholipid concentration of 5 mg/mL. Lavage fluid was instilled over 20 seconds through
a dispensing catheter with the ventilator circuit disconnected. Three positive-pressure
inflations were then administered, followed by disconnection of the ventilator circuit
and suction of the instilled fluid with a standard suction catheter for up to 30 seconds
Outcomes Primary outcome: duration of respiratory support, defined as the cumulative durationof all periods of intubation and nasal continuous positive airway pressure (CPAP)
Secondary outcomes: death, pneumothorax, duration of intubation, oxygen therapy,
HFOV, iNO, hospitalisation
Evaluation of the physiologic effects and safety of lavage: heart rate, mean blood pressure,
SpO2, blood gas analyses
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Randomly permuted blocks of two or four,
stratified by study centre
Allocation concealment (selection bias) Low risk Pre-prepared sequentially numbered sealed
opaque envelopes
13Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 16/31
Dargaville 2011 (Continued)
Blinding of participants and personnel
(performance bias)
All outcomes
High risk Blinding of the intervention was not possi-
ble
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk All outcomes were measured by objective
means
Incomplete outcome data (attrition bias)
All outcomes
Low risk One infant was ineligible. Complete data
were available for 65 eligible infants
Selective reporting (reporting bias) Low risk The study protocol is available and all of
the study’s pre-specified outcomes that are
of interest in the review have been reported
in the pre-specified way
Other bias Low risk The study appears to be free of other
sources of bias
Gadzinowski 2008
Methods Single-centre randomised controlled trial. Randomisation blinded, with a 1:1 allocation
ratio
Intervention not blinded to clinicalteam or assessors of longer-termoutcomes. Complete
follow-up with assessment up to two years of age
Participants 13 neonates of gestational age > 34 weeks, postnatal age less than 24 hours, with MAS
complicated by pulmonary hypertension diagnosed on the basis of echocardiographicparameters. Seven infants received surfactant lavage followed by bolus surfactant treat-
ment, and 6 received bolus surfactant treatment only
Interventions Surfactant lavage with a total lavage volume of 15 mL/kg (aliquot volume 3.75 mL/kg)
of bovine surfactant (Survanta) at a phospholipid concentration of 5 mg/mL. Lavage
was conducted via a closed lavage and suctioning system, in four body positions: on the
right and left sides, and in the Trendelenburg and anti-Trendelenburg positions
After 2 mL of the solution was instilled, mechanical ventilation was continued
After 3 to 5 respiratory cycles, the secretions were suctioned
After lavage treatment, one dose of bolus Survanta (100 mg/kg) was given. Heart rate
and oxygen saturation were monitored
Outcomes Primary outcome: (1) PaO2; (2) fraction of inspired oxygen; (3) oxygenation index; and(4) alveolar-arterial oxygen difference
Secondary outcomes: length of time on mechanical ventilation; duration of iNO treat-
ment; length of hospital stay; complications; and mortality
Notes
Risk of bias
14Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 17/31
Gadzinowski 2008 (Continued)
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Unclear risk The study is described as randomised, butno information is provided about the se-
quence generation method
Allocation concealment (selection bias) Unclear risk Not reported
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Not reported (each group of infants was
managed by a different group of neonatol-
ogists)
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk All outcomes were measured by objective
means
Incomplete outcome data (attrition bias)
All outcomes
Low risk Complete data were available for all en-
rolled infants
Selective reporting (reporting bias) Low risk The study protocol is not available, and in-
formationis sufficient to permit judgement
Wiswell 2002
Methods Multicenter randomised controlled trial
15 participating centres
Randomisation blinded, with a 2:1 allocation ratio (lavage vs control). Intervention not
blinded to clinical team or assessors of longer-term outcomesComplete follow-up with assessment up to one year of age
Participants 22 infants (enrolledinnine participating centres) of gestational age > 34 weeks, postnatal
age up to 72 hours, with a diagnosis of MAS requiring mechanical ventilation
The infants were eligible for enrolment if oxygenation index (OI) was between 8 and
25, inclusive, on at least two of three consecutive blood gas analyses within a three-hour
period
15 infants received surfactant lavage and 7 received standard care
Interventions Lung lavage with a total lavage volume of 48 mL/kg, divided into 6 aliquots each of 8
mL/kg
Lavage fluid was lucinactant (Surfaxin), at a phospholipid concentration of 2.5 mg/mL
for the first four lavage aliquots, and 10 mg/mL for the last two aliquots
Each aliquot was instilled down the endotracheal tube with the chest alternately left and
right side down, with suctioning after each instillation using a closed suctioning system
Recovery of blood pressure, heart rate, and oxygen saturation was mandated before
proceeding with further lavage aliquots
15Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 18/31
Wiswell 2002 (Continued)
Outcomes Primary outcome: incidence of treatment failure, defined as an OI > 25 or an increase
in OI of 50% above baseline
Secondary outcomes: MAS-related mortality, oxygenation changes, need for rescue ther-apies (HFOV, bolus surfactant, iNO, ECMO), duration of ventilation
Longer-term outcomes: survival at 12 months, numbers of hospitalizations and respira-
tory illnesses in the first year of life, growth and development at 12 months
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk The study is described as randomised, but
no information about the sequence gener-
ation method is provided
Allocation concealment (selection bias) Low risk Randomisation was performed by drawing
a randomisation slip from a closedenvelope
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Not reported
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk All outcomes were measured by objective
means
Incomplete outcome data (attrition bias)
All outcomes
Low risk ITT analysis was carried out
Selective reporting (reporting bias) Unclear risk The study protocol is not available, and in-
formationis sufficient to permit judgement
Other bias High risk (1) The study was conducted without a for-
malsample size calculation but based on an
estimate for assessing safety and potential
efficacy in a rather exploratory fashion
(2) The number of infants receiving rescue
therapy was greater than the number of in-
fants with treatment failures, although res-cue therapies were not allowed unless in-
fants met treatment failure
16Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 19/31
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Armenta 2011 Surfactant lavage was compared with saline lavage
Burke-Strickland 1973 Nonrandomised case series
Carson 1976 Randomisation ofinfantsto receive salinelavage orno lavagementionedinmethods,butno results presented
Chang 2003 Nonrandomised study over two time epochs
Dargaville 2007 Nonrandomised study with concurrent controls
Kowalska 2002 Nonrandomised study over two time epochs
Lam 1999 Nonrandomised study over two time epochs
Ogawa 1997 Randomised controlled trial; no data reported or obtainable for nonlavaged control group
Six infants received 5 × 2 mL/kg lavage with Surfacten-TA (6 mg/mL phospholipid), and 4 infants received
identical lavage, but with saline
A significant difference was noted between the two groups in both oxygenation and CO2 clearance after
lavage, favouring the group lavaged with dilute surfactant
Rosegger 1987 Nonrandomised study with concurrent controls
Salvia-Roigés 2004 Nonrandomised study of two different treatment schedules involving lavage, compared with historical
controls
Schlösser 2002 Nonrandomised study with concurrent controls
Su 1998 Nonrandomised study, no control group
Characteristics of ongoing studies [ordered by study ID]
McNamara 2006
Trial name or title Surfactant Lavage versus Bolus Surfactant in Neonates With Meconium Aspiration
Methods RCT
Participants Meconium aspiration syndrome (n = 20)
Interventions Surfactant lavage or surfactant bolus treatment
Outcomes Primary outcome measures:
Change in oxygenation from baseline to one and six hours after treatment.
17Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 20/31
McNamara 2006 (Continued)
Change in dynamic pulmonary compliance from baseline to one and six hour after treatment.
Change in pulmonary artery pressure from baseline to one and six hour after treatment.
Measures of efficacy of ventilation and oxygenation at one hour and six hours after treatment.
Cardiac function by echocardiography at six hours after treatment
Secondary outcome measures:
Change in oxygenation, dynamic pulmonary compliance, and pulmonary vascular resistance from baseline
to 12, 24, and 48 hours after treatment
Measures of efficiency of ventilation and oxygenation at 12, 24, and 48 hours after treatment
Duration of mechanical ventilation, defined as the cumulative time of mechanical ventilation
Length of time on CPAP
Length of time with oxygen supplementation
Length of time on inotropes and maximum inotropic score
Need for and length of use of NO
Need for and length of use of ECMO
Time to full enteral feeds
Attainment of exit criteria
Development of significant pulmonary haemorrhage
Development of significant intracranial haemorrhage
Development of tension pneumothorax requiring drainage
Need for repeat surfactant
Length of stay in a level III NICU
Mortality
Starting date 2006
Contact information Patrick McNamara, MD, [email protected] .
The Hospital for Sick Children, Toronto, Ontario, Canada
Notes clinical trials.gov. identifier NCT00312507
Segal 2012
Trial name or title Phase III Randomized Study of Lucinactant in Full Term Newborn Infants with Meconium Aspiration
Syndrome
Methods Randomised controlled trial
Participants 69 infants (lucinactant n = 38; standard care n = 31)
Interventions Lucinactant via bronchoalveolar lavage
Outcomes Numbers of days receiving mechanical ventilation (lucinactant 10.2 ± 9.96; standard care 8.1 ± 8.52)
Air leak (lucinactant 2/38; standard care 0/31)
Intraventricular haemorrhage (lucinactant 0/38; standard care 1/31)
Death (lucinactant 0/38; standard care 0/31)
Starting date Recruitment occurred between March 2000 and October 2002
18Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 21/31
Segal 2012 (Continued)
Contact information Robert Segal; Discovery Laboratory
Notes Clinical trials.gov. identifier NCT00004500.Sponsored by Discovery Laboratories
Sur-Lu-Lav 2011
Trial name or title Comparison of Surfactant Lung Lavage with Standard Care in the Treatment of Meconium Aspiration
Syndrome (Sur-Lu-Lav)
Methods Randomised controlled trial
Participants Inclusion criteria:
• Gestation age ≥ 37 weeks
• Cephalic presentation• Singleton pregnancy
• Presence of meconium-stained amniotic fluid or staining of meconium in skin,umbilical cord, or nails
• Nonvigorous babies
• Presence of respiratory distress (Downes score ≥ 4)
• Presence of meconium below vocal cords or chest x-ray; suggestive of meconium aspiration
• Age < 2 hours
Exclusion criteria:
• Major congenital malformations
• Congenital heart disease
• Hydrops fetalis
• Air leaks
• Pulmonary haemorrhage
Interventions Lavage with 2 × 10 mL/kg aliquots of bovine surfactant or standard care
The diluted surfactant is instilled into the endotracheal tube over a period of 15 to 20 seconds
Once the instillation is complete, 5 manual breaths will be provided and the infant will be repositioned supine
The suction catheter will be inserted and advanced to a position approximately 5 mm past the end of the
endotracheal tube
Outcomes Primary outcome: duration of oxygen therapy, severity of respiratory distress, need for mechanical ventilation
Secondary outcome: duration of mechanical ventilation, complications, incidence of sepsis, mortality, dura-
tion of hospital stay
Starting date 2011
Contact information Sushma Nangia, MBBS, MD, DM [email protected] Saran Children’s Hospital, Lady Hardinge Medical College
Notes clinical trials.gov. identifier NCT01310621
19Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 22/31
D A T A A N D A N A L Y S E S
Comparison 1. Lung lavage versus standard care
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Death 2 88 Risk Ratio (M-H, Fixed, 95% CI) 0.42 [0.12, 1.46]
2 Use of ECMO 2 47 Risk Ratio (M-H, Fixed, 95% CI) 0.27 [0.04, 1.86]
3 Death or use of ECMO 2 88 Risk Ratio (M-H, Fixed, 95% CI) 0.33 [0.11, 0.96]
4 Pneumothorax 2 88 Risk Ratio (M-H, Fixed, 95% CI) 0.38 [0.08, 1.90]
5 Oxygenation index 2 Mean Difference (IV, Fixed, 95% CI) Subtotals only
5.1 measured at 24 hours 2 88 Mean Difference (IV, Fixed, 95% CI) -1.90 [-7.56, 3.77]
5.2 measured at 48 hours 2 88 Mean Difference (IV, Fixed, 95% CI) -6.20 [-12.11, -0.29]
5.3 measured at 72 hours 2 88 Mean Difference (IV, Fixed, 95% CI) -3.56 [-8.72, 1.60]
6 Alveolar-arterial oxygen
difference
1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
6.1 measured at 24 hours 1 66 Mean Difference (IV, Fixed, 95% CI) -12.0 [-109.19, 85.
19]
6.2 measured at 48 hours 1 66 Mean Difference (IV, Fixed, 95% CI) -57.0 [-162.96, 48.
96]
6.3 measured at 72 hours 1 66 Mean Difference (IV, Fixed, 95% CI) -41.0 [-132.59, 50.
59]
7 PaO2/FiO2 1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
7.1 measured at 24 hours 1 66 Mean Difference (IV, Fixed, 95% CI) -1.0 [-54.61, 52.61]
7.2 measured at 48 hours 1 66 Mean Difference (IV, Fixed, 95% CI) 27.0 [-26.63, 80.63]
7.3 measured at 72 hours 1 66 Mean Difference (IV, Fixed, 95% CI) 26.0 [-24.96, 76.96]
Comparison 2. Lung lavage followed by surfactant bolus versus surfactant bolus
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Death 1 13 Risk Ratio (M-H, Fixed, 95% CI) 0.18 [0.01, 3.06]
2 Pneumothorax 1 13 Risk Ratio (M-H, Fixed, 95% CI) 0.18 [0.01, 3.06]
20Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
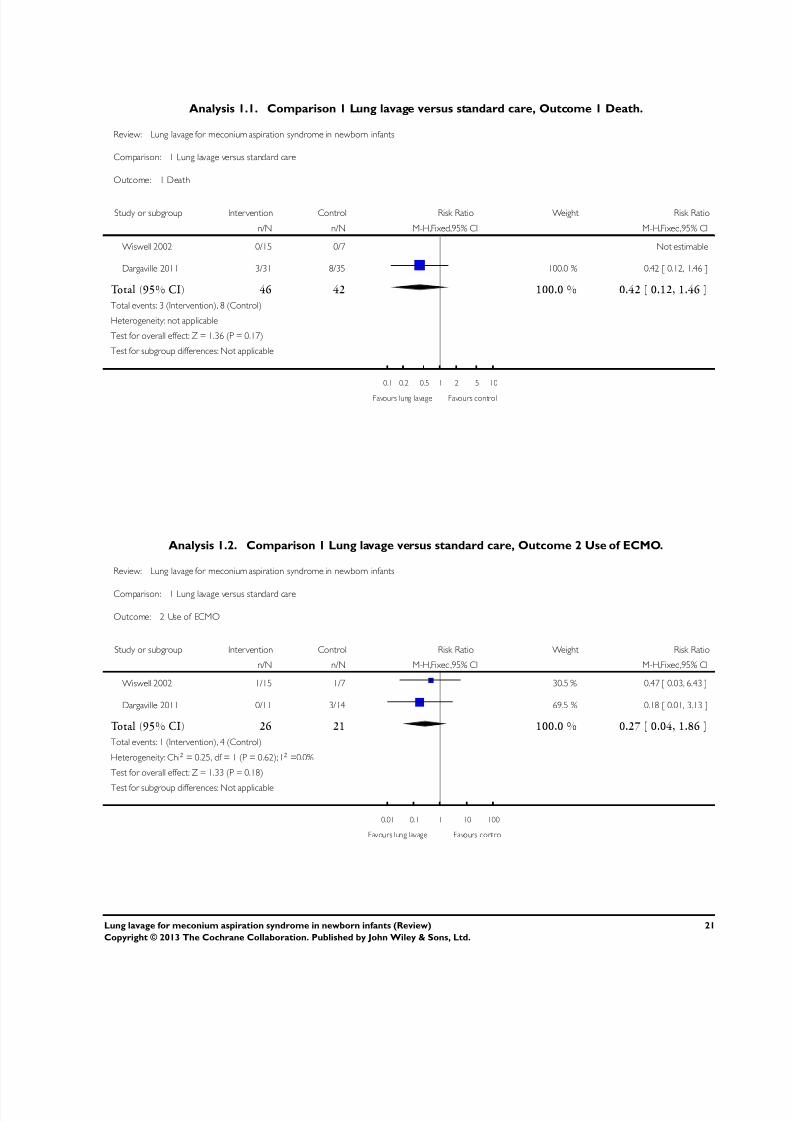
7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 23/31
Analysis 1.1. Comparison 1 Lung lavage versus standard care, Outcome 1 Death.
Review: Lung lavage for meconium aspiration syndrome in newborn infants
Comparison: 1 Lung lavage versus standard care
Outcome: 1 Death
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Wiswell 2002 0/15 0/7 Not estimable
Dargaville 2011 3/31 8/35 100.0 % 0.42 [ 0.12, 1.46 ]
Total (95% CI) 46 42 100.0 % 0.42 [ 0.12, 1.46 ]
Total events: 3 (Intervention), 8 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.36 (P = 0.17)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
Favours lung lavage Favours control
Analysis 1.2. Comparison 1 Lung lavage versus standard care, Outcome 2 Use of ECMO.
Review: Lung lavage for meconium aspiration syndrome in newborn infants
Comparison: 1 Lung lavage versus standard care
Outcome: 2 Use of ECMO
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Wiswell 2002 1/15 1/7 30.5 % 0.47 [ 0.03, 6.43 ]
Dargaville 2011 0/11 3/14 69.5 % 0.18 [ 0.01, 3.13 ]
Total (95% CI) 26 21 100.0 % 0.27 [ 0.04, 1.86 ]
Total events: 1 (Intervention), 4 (Control)
Heterogeneity: Chi2 = 0.25, df = 1 (P = 0.62); I2 =0.0%
Test for overall effect: Z = 1.33 (P = 0.18)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours lung lavage Favours control
21Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 24/31
Analysis 1.3. Comparison 1 Lung lavage versus standard care, Outcome 3 Death or use of ECMO.
Review: Lung lavage for meconium aspiration syndrome in newborn infants
Comparison: 1 Lung lavage versus standard care
Outcome: 3 Death or use of ECMO
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Wiswell 2002 1/15 1/7 11.7 % 0.47 [ 0.03, 6.43 ]
Dargaville 2011 3/31 11/35 88.3 % 0.31 [ 0.09, 1.00 ]
Total (95% CI) 46 42 100.0 % 0.33 [ 0.11, 0.96 ]
Total events: 4 (Intervention), 12 (Control)
Heterogeneity: Chi2 = 0.08, df = 1 (P = 0.78); I2 =0.0%
Test for overall effect: Z = 2.04 (P = 0.042)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours lung lavage Favours control
Analysis 1.4. Comparison 1 Lung lavage versus standard care, Outcome 4 Pneumothorax.
Review: Lung lavage for meconium aspiration syndrome in newborn infants
Comparison: 1 Lung lavage versus standard care
Outcome: 4 Pneumothorax
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Wiswell 2002 1/15 0/7 12.4 % 1.50 [ 0.07, 32.84 ]
Dargaville 2011 1/31 5/35 87.6 % 0.23 [ 0.03, 1.83 ]
Total (95% CI) 46 42 100.0 % 0.38 [ 0.08, 1.90 ]
Total events: 2 (Intervention), 5 (Control)
Heterogeneity: Chi2 = 1.00, df = 1 (P = 0.32); I2 =0.0%
Test for overall effect: Z = 1.17 (P = 0.24)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours lung lavage Favours control
22Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 25/31
Analysis 1.5. Comparison 1 Lung lavage versus standard care, Outcome 5 Oxygenation index.
Review: Lung lavage for meconium aspiration syndrome in newborn infants
Comparison: 1 Lung lavage versus standard care
Outcome: 5 Oxygenation index
Study or subgroup Inter vention ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 measured at 24 hours
Wiswell 2002 15 6.2 (15.5) 7 9.6 (11.1) 24.8 % -3.40 [ -14.76, 7.96 ]
Dargaville 2011 31 16.3 (13.7) 35 17.7 (13.3) 75.2 % -1.40 [ -7.93, 5.13 ]
Subtotal (95% CI) 46 42 100.0 % -1.90 [ -7.56, 3.77 ]
Heterogeneity: Chi2 = 0.09, df = 1 (P = 0.76); I2 =0.0%
Test for overall effect: Z = 0.66 (P = 0.51)
2 measured at 48 hours
Wiswell 2002 15 4.4 (4.3) 7 10.6 (13.8) 32.0 % -6.20 [ -16.65, 4.25 ]
Dargaville 2011 31 10.3 (11.6) 35 16.5 (17.8) 68.0 % -6.20 [ -13.37, 0.97 ]
Subtotal (95% CI) 46 42 100.0 % -6.20 [ -12.11, -0.29 ]
Heterogeneity: Chi2 = 0.0, df = 1 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 2.05 (P = 0.040)
3 measured at 72 hours
Wiswell 2002 15 3.3 (3.1) 7 8.4 (14.3) 23.2 % -5.10 [ -15.81, 5.61 ]
Dargaville 2011 31 9.9 (11.7) 35 13 (12.7) 76.8 % -3.10 [ -8.99, 2.79 ]
Subtotal (95% CI) 46 42 100.0 % -3.56 [ -8.72, 1.60 ]
Heterogeneity: Chi2 = 0.10, df = 1 (P = 0.75); I2 =0.0%
Test for overall effect: Z = 1.35 (P = 0.18)
-20 -10 0 10 20
Favours lung lavage Favours control
23Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 26/31
Analysis 1.6. Comparison 1 Lung lavage versus standard care, Outcome 6 Alveolar-arterial oxygen
difference.
Review: Lung lavage for meconium aspiration syndrome in newborn infants
Comparison: 1 Lung lavage versus standard care
Outcome: 6 Alveolar-arterial oxygen difference
Study or subgroup Inter vention ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 measured at 24 hours
Dargaville 2011 31 358 (202) 35 370 (200) 100.0 % -12.00 [ -109.19, 85.19 ]
Subtotal (95% CI) 31 35 100.0 % -12.00 [ -109.19, 85.19 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.24 (P = 0.81)
2 measured at 48 hours
Dargaville 2011 31 258 (222) 35 315 (216) 100.0 % -57.00 [ -162.96, 48.96 ]
Subtotal (95% CI) 31 35 100.0 % -57.00 [ -162.96, 48.96 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.05 (P = 0.29)
3 measured at 72 hours
Dargaville 2011 31 236 (189) 35 277 (190) 100.0 % -41.00 [ -132.59, 50.59 ]
Subtotal (95% CI) 31 35 100.0 % -41.00 [ -132.59, 50.59 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.88 (P = 0.38)
-200 -100 0 100 200
Favours lung lavage Favours control
24Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 27/31
Analysis 1.7. Comparison 1 Lung lavage versus standard care, Outcome 7 PaO2/FiO2.
Review: Lung lavage for meconium aspiration syndrome in newborn infants
Comparison: 1 Lung lavage versus standard care
Outcome: 7 PaO2/FiO2
Study or subgroup Inter vention ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 measured at 24 hours
Dargaville 2011 31 148 (109) 35 149 (113) 100.0 % -1.00 [ -54.61, 52.61 ]
Subtotal (95% CI) 31 35 100.0 % -1.00 [ -54.61, 52.61 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.04 (P = 0.97)
2 measured at 48 hours
Dargaville 2011 31 188 (110) 35 161 (112) 100.0 % 27.00 [ -26.63, 80.63 ]
Subtotal (95% CI) 31 35 100.0 % 27.00 [ -26.63, 80.63 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.99 (P = 0.32)
3 measured at 72 hours
Dargaville 2011 31 187 (110) 35 161 (100) 100.0 % 26.00 [ -24.96, 76.96 ]
Subtotal (95% CI) 31 35 100.0 % 26.00 [ -24.96, 76.96 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.00 (P = 0.32)
-100 -50 0 50 100
Favours control Favours lung lavage
25Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 28/31
Analysis 2.1. Comparison 2 Lung lavage followed by surfactant bolus versus surfactant bolus, Outcome 1
Death.
Review: Lung lavage for meconium aspiration syndrome in newborn infants
Comparison: 2 Lung lavage followed by surfactant bolus versus surfactant bolus
Outcome: 1 Death
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Gadzinowski 2008 0/7 2/6 100.0 % 0.18 [ 0.01, 3.06 ]
Total (95% CI) 7 6 100.0 % 0.18 [ 0.01, 3.06 ]
Total events: 0 (Intervention), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.19 (P = 0.23)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours lung lavage Favours control
Analysis 2.2. Comparison 2 Lung lavage followed by surfactant bolus versus surfactant bolus, Outcome 2
Pneumothorax.
Review: Lung lavage for meconium aspiration syndrome in newborn infants
Comparison: 2 Lung lavage followed by surfactant bolus versus surfactant bolus
Outcome: 2 Pneumothorax
Study or subgroup Intervention Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Gadzinowski 2008 0/7 2/6 100.0 % 0.18 [ 0.01, 3.06 ]
Total (95% CI) 7 6 100.0 % 0.18 [ 0.01, 3.06 ]
Total events: 0 (Intervention), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.19 (P = 0.23)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours lung lavage Favours control
26Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 29/31

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 30/31
H I S T O R Y
Protocol first published: Issue 1, 2002
Review first published: Issue 4, 2013
Date Event Description
30 August 2011 New citation required and conclusions have changed Search updated, studies added, analyses and texts
amended
20 July 2011 Amended Authorship amended
2 May 2011 Amended Converted to new review format.
30 August 2005 New citation required and conclusions have changed Substantive amendment
C O N T R I B U T I O N S O F A U T H O R S
Dr. Seokyung Hahn is the primary author of the review. She carried out study selection, assessment of study methodology, and data
extraction and wrote the review.
Dr. Hyun Jin Choi performed the initial search for the articles, assessed study methodology, extracted data, and collaborated with Dr.
Hahn in writing the review.
Dr. Peter Dargaville specified the objectives and the types of studies, participants, interventions, and outcomes to be included.
Dr. Roger Soll participated in assessing the study methodology, extracted data, and collaborated with Dr. Dargaville at an earlier stage
of the review.
D E C L A R A T I O N S O F I N T E R E S T
Dr. Hahn and Dr. Choi declared no conflict of interest.
Dr. P. Dargaville has received support for animal laboratory studies of therapeutic pulmonary lavage from Abbott Australasia, and has
also been supported as an invited speaker by Abbott, and by Chiesi Farmaceutici.
Dr. Dargaville was Chief Investigator of the lessMAS trial, which is funded independent of industry, but for which Abbott Laboratories
has provided surfactant free of charge.
Dr. R. Soll has acted as a consultant and an invited speaker for several of the pharmaceutical companies that manufacture or distribute
surfactant preparations (Abbott Laboratories, Ross Laboratories, Chiesi Pharmaceuticals, Dey Laboratories, Burroughs Wellcome).
28Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7/18/2019 Lung Lavage 2013 MAS
http://slidepdf.com/reader/full/lung-lavage-2013-mas 31/31
S O U R C E S O F S U P P O R T
Internal sources
• Menzies Research Institute Tasmania, Hobart, Australia.
External sources
• National Evidence-based Healthcare Collaborating Agency, Korea, South.
• National Research Foundation of Korea (NRF), Korea, South.
NRF grant funded by the Korea government (MEST); No. 2012-0000994.
• Eunice Kennedy Shriver National Institute of Child Health and Human Development National Institutes of Health,
Department of Health and Human Services, USA.
Editorial support of the Cochrane Neonatal Review Group has been funded with Federal funds from the Eunice Kennedy Shriver
National Institute of Child Health and Human Development National Institutes of Health, Department of Health and Human
Services, USA, under Contract No. HHSN275201100016C.
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
The composite outcome of death or use of ECMO was included as an outcome in view of the effects of ECMO, when available, on
mortality risk.
I N D E X T E R M S
Medical Subject Headings (MeSH)
Bronchoalveolar Lavage [∗methods]; Infant, Newborn; Meconium Aspiration Syndrome [mortality; ∗ therapy]; Pulmonary Surfactants
[∗therapeutic use]; Randomized Controlled Trials as Topic
MeSH check words
Humans
29Lung lavage for meconium aspiration syndrome in newborn infants (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.